PROXIMAL POLE SCAPHOID FRACTURES AND N ONUNION BY THOMAS E. TRUMBLE, MD, AND DUC VO, MD Proximal pole fractures and nonunions of the scaphoid present an extremely challenging treatment problem. Untreated, proximal pole fractures have a high rate of developing a nonunion that may lead to painful arthritis. Cast immo- bilization is not adequate, and surgery is recommended for the treatment of acute fractures and nonunions. The fractures are difficult to treat through a conven- tional volar approach, and the preferred treatment is open reduction and internal fixation using a dorsal approach with a screw that is specially designed for the scaphoid. The type of fixation implant used is important, because the end of the screw must be buried beneath the articular cartilage when the dorsal approach is used. The main blood supply of the scaphoid enters through the dorsoradial ridge of the scaphoid. By definition, proximal pole nonunions have partial ischemia or complete avascular necrosis, because the fracture line isolates the proximal pole from the perforating vessels. The definitive treatment for these fractures is a standard or vascularized bone graft, depending on the vascularity of the proximal pole of the scaphoid in addition to internal fixation via a dorsal approach. Using this treatment algorithm, the surgeon can optimize the success rate of achieving a successful scaphoid union in the shortest possible time of immobilization. Copyright © 2001 by the American Society for Surgery of the Hand A cute proximal pole scaphoid fractures and proximal pole scaphoid nonunions present a serious clinical problem. They frequently produce very few symptoms in the early stages and the success rate decreases with any delay to treatment. Of all scaphoid fractures, proximal pole fractures appear to have a higher rate of avascular necrosis and a lower success rate with treatment, especially when cast treat- ment is used for the acute fracture and internal fixa- tion without a vascularized bone graft is used for the proximal pole nonunion. 1-4 Untreated proximal pole scaphoid nonunions frequently cause late wrist pain with progressive arthrosis. 5-8 The natural history of scaphoid fractures that develop into nonunions has not been clearly delineated, because in most cases it is not possible to determine how long a nonunion has been present or how many patients with asymptomatic nonunions are present in a population. 8-10 Conse- quently, the risk for developing wrist arthrosis from a scaphoid nonunion cannot be calculated. There is, however, a growing body of data suggesting that most From the University of Washington Medical Center, Department of Orthopaedic Surgery and Sports Medicine, Seattle, WA. Address reprint requests to Thomas E. Trumble, MD, University of Washington Medical Center, Department of Orthopaedic Surgery and Sports Medicine, 1959 NE Pacific St, Box 356500, Seattle, WA 98195-6500. Copyright © 2001 by the American Society for Surgery of the Hand 1531-0914/01/0103-0003$35.00/0 doi:10.1053/jssh.2001.26183 JOURNAL OF THE AMERICAN SOCIETY FOR SURGERY OF THE HAND VOL. 1, NO. 3, AUGUST 2001 155

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PROXIMAL POLE SCAPHOID
FRACTURES AND NONUNION
BY THOMAS E. TRUMBLE, MD, AND DUC VO, MD
Proximal pole fractures and nonunions of the scaphoid present an extremelychallenging treatment problem. Untreated, proximal pole fractures have a highrate of developing a nonunion that may lead to painful arthritis. Cast immo-bilization is not adequate, and surgery is recommended for the treatment of acutefractures and nonunions. The fractures are difficult to treat through a conven-tional volar approach, and the preferred treatment is open reduction and internalfixation using a dorsal approach with a screw that is specially designed for thescaphoid. The type of fixation implant used is important, because the end of thescrew must be buried beneath the articular cartilage when the dorsal approach isused. The main blood supply of the scaphoid enters through the dorsoradial ridgeof the scaphoid. By definition, proximal pole nonunions have partial ischemia orcomplete avascular necrosis, because the fracture line isolates the proximal polefrom the perforating vessels. The definitive treatment for these fractures is astandard or vascularized bone graft, depending on the vascularity of the proximalpole of the scaphoid in addition to internal fixation via a dorsal approach. Usingthis treatment algorithm, the surgeon can optimize the success rate of achieving asuccessful scaphoid union in the shortest possible time of immobilization.
Copyright © 2001 by the American Society for Surgery of the Hand
Acute proximal pole scaphoid fractures andproximal pole scaphoid nonunions present aserious clinical problem. They frequently
produce very few symptoms in the early stages and thesuccess rate decreases with any delay to treatment. Ofall scaphoid fractures, proximal pole fractures appear
to have a higher rate of avascular necrosis and a lowersuccess rate with treatment, especially when cast treat-ment is used for the acute fracture and internal fixa-tion without a vascularized bone graft is used for theproximal pole nonunion.1-4 Untreated proximal polescaphoid nonunions frequently cause late wrist painwith progressive arthrosis.5-8 The natural history ofscaphoid fractures that develop into nonunions has notbeen clearly delineated, because in most cases it is notpossible to determine how long a nonunion has beenpresent or how many patients with asymptomaticnonunions are present in a population.8-10 Conse-quently, the risk for developing wrist arthrosis from ascaphoid nonunion cannot be calculated. There is,however, a growing body of data suggesting that most
From the University of Washington Medical Center, Department ofOrthopaedic Surgery and Sports Medicine, Seattle, WA.Address reprint requests to Thomas E. Trumble, MD, University ofWashington Medical Center, Department of Orthopaedic Surgery andSports Medicine, 1959 NE Pacific St, Box 356500, Seattle, WA98195-6500.
Copyright © 2001 by the American Society for Surgery of the Hand1531-0914/01/0103-0003$35.00/0doi:10.1053/jssh.2001.26183
JOURNAL OF THE AMERICAN SOCIETY FOR SURGERY OF THE HAND � VOL. 1, NO. 3, AUGUST 2001 155
nonunions develop a collapse deformity followed bywrist arthrosis over time.6,11-13 The past fifteen yearshave provided major advances in our ability to diag-nose scaphoid nonunions and evaluate the collapsedeformity using computerized tomography (CT). Inaddition, magnetic resonance imaging (MRI) hasmade it possible to determine whether avascular ne-crosis is present in the proximal pole before surgery.Therefore, the surgery to treat proximal pole scaphoidnonunions can be planned to include vascularizedbone grafts.14 Fracture fixation has advanced withspecially designed screws to meet the constraints ofstabilizing a bone that is covered by articular surfaceat both ends with a fragile blood supply enteringbetween the 2 articular surfaces.15 The screw has beenfurther modified by cannulation so that it may beplaced over a guide wire for greater accuracy. Thefollowing discussion on the etiology, diagnosis, andtreatment options for scaphoid nonunions aims toestablish a better understanding of this entity and itstherapeutic challenges.
ANATOMY AND MECHANISM OF INJURY
Pertinent AnatomyScaphoid is Greek for “canoe” or “boat.” To better
represent scaphoid anatomy, however, the adjectives“bent” and “twisted” should be added. The plane ofthe scaphoid is tilted both palmarward and radiallywith respect to the central axis of the forearm, and thisobliquity can add to the complexity of operative treat-ment. The proximal half of the scaphoid is largelycovered with articular surface with few, if any, perfo-
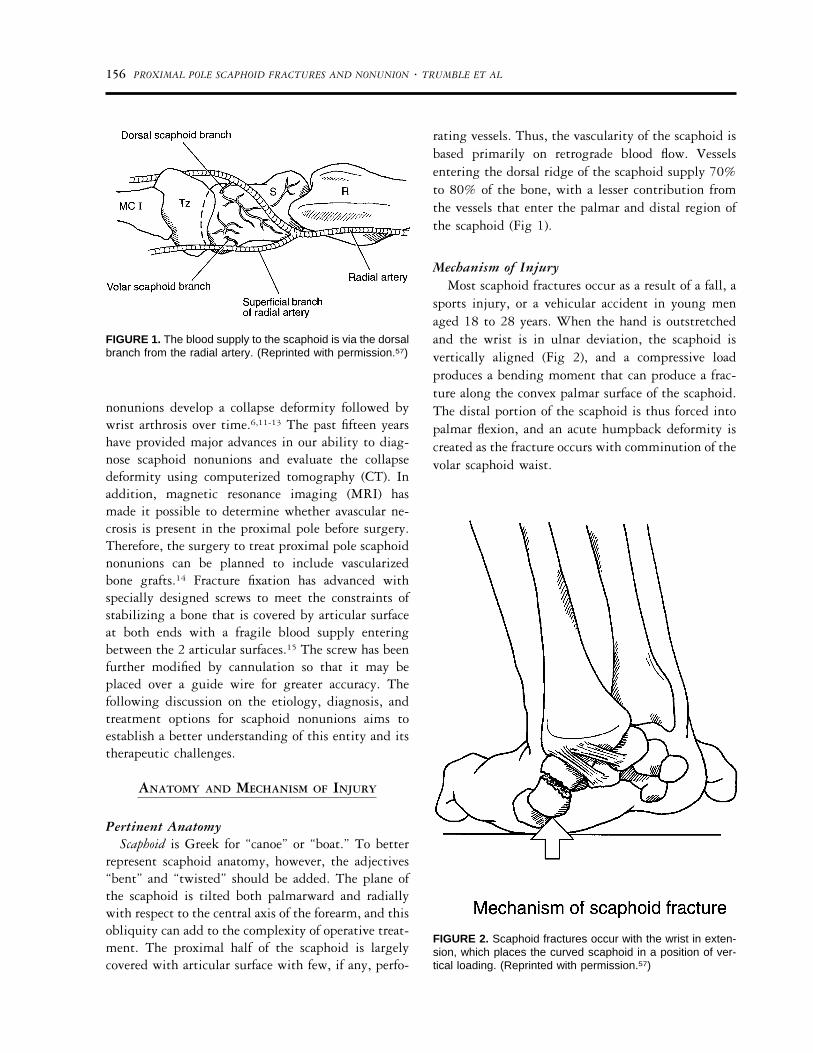
rating vessels. Thus, the vascularity of the scaphoid isbased primarily on retrograde blood flow. Vesselsentering the dorsal ridge of the scaphoid supply 70%to 80% of the bone, with a lesser contribution fromthe vessels that enter the palmar and distal region ofthe scaphoid (Fig 1).
Mechanism of InjuryMost scaphoid fractures occur as a result of a fall, a
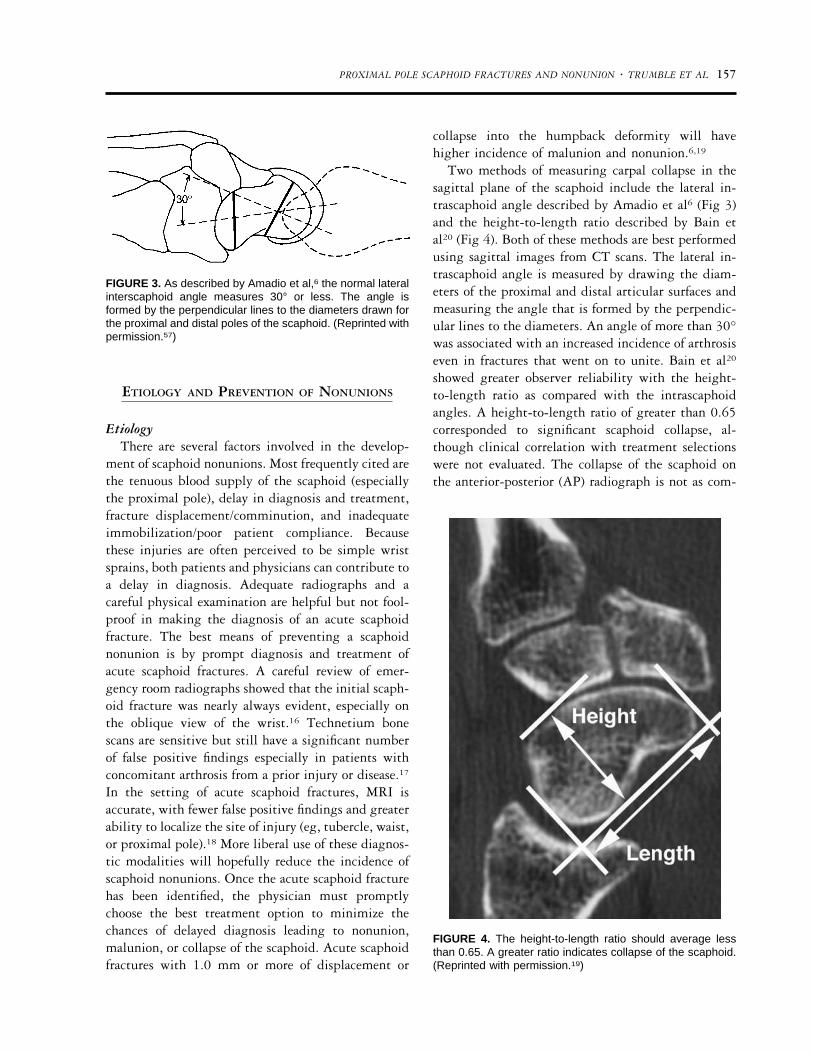
sports injury, or a vehicular accident in young menaged 18 to 28 years. When the hand is outstretchedand the wrist is in ulnar deviation, the scaphoid isvertically aligned (Fig 2), and a compressive loadproduces a bending moment that can produce a frac-ture along the convex palmar surface of the scaphoid.The distal portion of the scaphoid is thus forced intopalmar flexion, and an acute humpback deformity iscreated as the fracture occurs with comminution of thevolar scaphoid waist.
FIGURE 1. The blood supply to the scaphoid is via the dorsalbranch from the radial artery. (Reprinted with permission.57)
FIGURE 2. Scaphoid fractures occur with the wrist in exten-sion, which places the curved scaphoid in a position of ver-tical loading. (Reprinted with permission.57)
156 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL
ETIOLOGY AND PREVENTION OF NONUNIONS
EtiologyThere are several factors involved in the develop-
ment of scaphoid nonunions. Most frequently cited arethe tenuous blood supply of the scaphoid (especiallythe proximal pole), delay in diagnosis and treatment,fracture displacement/comminution, and inadequateimmobilization/poor patient compliance. Becausethese injuries are often perceived to be simple wristsprains, both patients and physicians can contribute toa delay in diagnosis. Adequate radiographs and acareful physical examination are helpful but not fool-proof in making the diagnosis of an acute scaphoidfracture. The best means of preventing a scaphoidnonunion is by prompt diagnosis and treatment ofacute scaphoid fractures. A careful review of emer-gency room radiographs showed that the initial scaph-oid fracture was nearly always evident, especially onthe oblique view of the wrist.16 Technetium bonescans are sensitive but still have a significant numberof false positive findings especially in patients withconcomitant arthrosis from a prior injury or disease.17
In the setting of acute scaphoid fractures, MRI isaccurate, with fewer false positive findings and greaterability to localize the site of injury (eg, tubercle, waist,or proximal pole).18 More liberal use of these diagnos-tic modalities will hopefully reduce the incidence ofscaphoid nonunions. Once the acute scaphoid fracturehas been identified, the physician must promptlychoose the best treatment option to minimize thechances of delayed diagnosis leading to nonunion,malunion, or collapse of the scaphoid. Acute scaphoidfractures with 1.0 mm or more of displacement or
collapse into the humpback deformity will havehigher incidence of malunion and nonunion.6,19
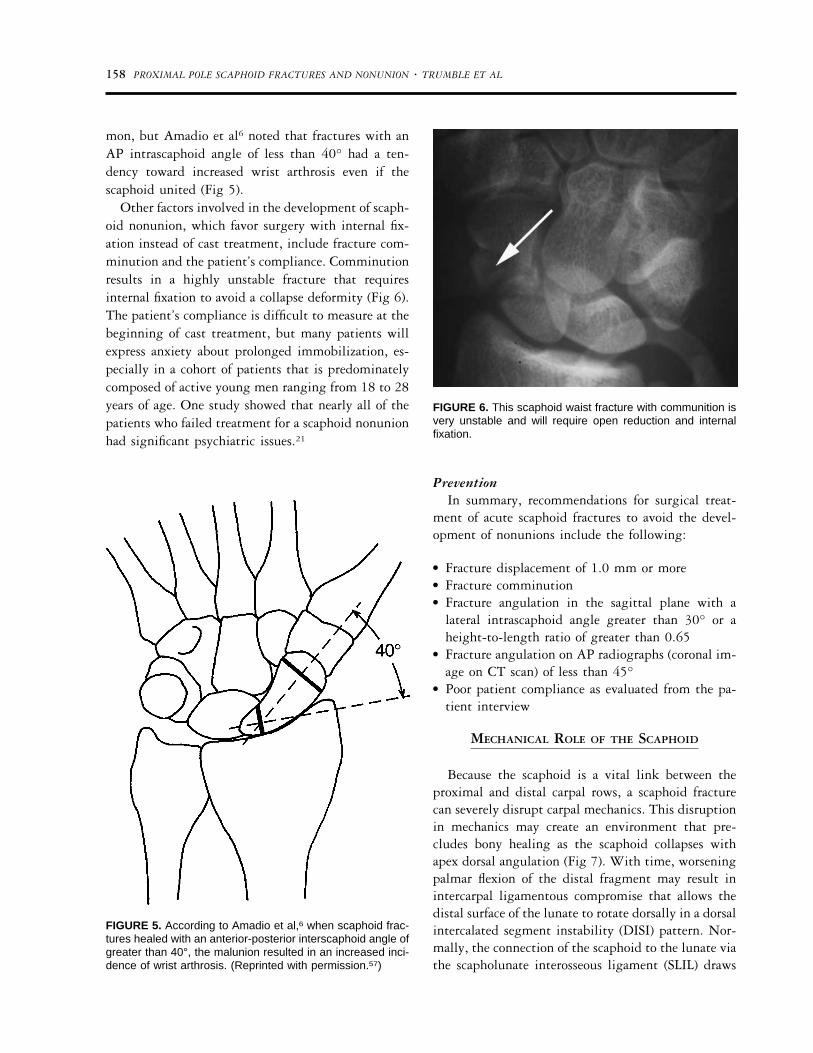
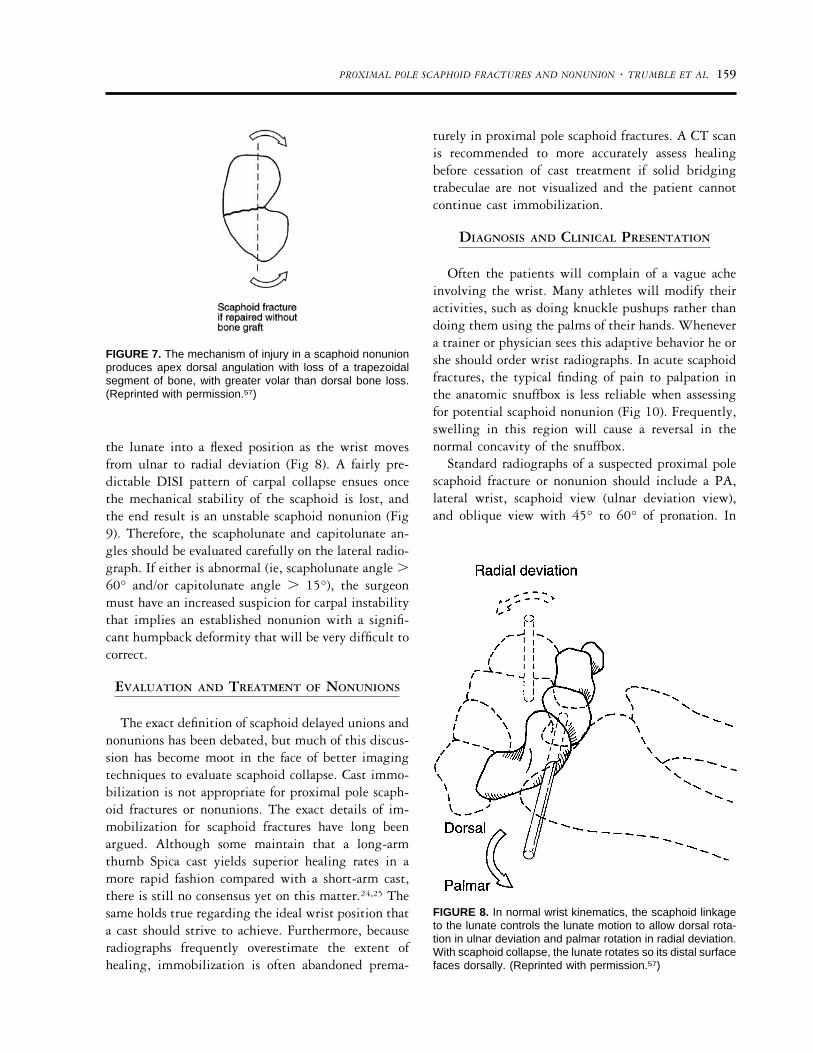
Two methods of measuring carpal collapse in thesagittal plane of the scaphoid include the lateral in-trascaphoid angle described by Amadio et al6 (Fig 3)and the height-to-length ratio described by Bain etal20 (Fig 4). Both of these methods are best performedusing sagittal images from CT scans. The lateral in-trascaphoid angle is measured by drawing the diam-eters of the proximal and distal articular surfaces andmeasuring the angle that is formed by the perpendic-ular lines to the diameters. An angle of more than 30°was associated with an increased incidence of arthrosiseven in fractures that went on to unite. Bain et al20
showed greater observer reliability with the height-to-length ratio as compared with the intrascaphoidangles. A height-to-length ratio of greater than 0.65corresponded to significant scaphoid collapse, al-though clinical correlation with treatment selectionswere not evaluated. The collapse of the scaphoid onthe anterior-posterior (AP) radiograph is not as com-
FIGURE 3. As described by Amadio et al,6 the normal lateralinterscaphoid angle measures 30° or less. The angle isformed by the perpendicular lines to the diameters drawn forthe proximal and distal poles of the scaphoid. (Reprinted withpermission.57)
FIGURE 4. The height-to-length ratio should average lessthan 0.65. A greater ratio indicates collapse of the scaphoid.(Reprinted with permission.19)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 157
mon, but Amadio et al6 noted that fractures with anAP intrascaphoid angle of less than 40° had a ten-dency toward increased wrist arthrosis even if thescaphoid united (Fig 5).
Other factors involved in the development of scaph-oid nonunion, which favor surgery with internal fix-ation instead of cast treatment, include fracture com-minution and the patient’s compliance. Comminutionresults in a highly unstable fracture that requiresinternal fixation to avoid a collapse deformity (Fig 6).The patient’s compliance is difficult to measure at thebeginning of cast treatment, but many patients willexpress anxiety about prolonged immobilization, es-pecially in a cohort of patients that is predominatelycomposed of active young men ranging from 18 to 28years of age. One study showed that nearly all of thepatients who failed treatment for a scaphoid nonunionhad significant psychiatric issues.21
PreventionIn summary, recommendations for surgical treat-
ment of acute scaphoid fractures to avoid the devel-opment of nonunions include the following:
● Fracture displacement of 1.0 mm or more● Fracture comminution● Fracture angulation in the sagittal plane with a
lateral intrascaphoid angle greater than 30° or aheight-to-length ratio of greater than 0.65
● Fracture angulation on AP radiographs (coronal im-age on CT scan) of less than 45°
● Poor patient compliance as evaluated from the pa-tient interview
MECHANICAL ROLE OF THE SCAPHOID
Because the scaphoid is a vital link between theproximal and distal carpal rows, a scaphoid fracturecan severely disrupt carpal mechanics. This disruptionin mechanics may create an environment that pre-cludes bony healing as the scaphoid collapses withapex dorsal angulation (Fig 7). With time, worseningpalmar flexion of the distal fragment may result inintercarpal ligamentous compromise that allows thedistal surface of the lunate to rotate dorsally in a dorsalintercalated segment instability (DISI) pattern. Nor-mally, the connection of the scaphoid to the lunate viathe scapholunate interosseous ligament (SLIL) draws
FIGURE 5. According to Amadio et al,6 when scaphoid frac-tures healed with an anterior-posterior interscaphoid angle ofgreater than 40°, the malunion resulted in an increased inci-dence of wrist arthrosis. (Reprinted with permission.57)
FIGURE 6. This scaphoid waist fracture with communition isvery unstable and will require open reduction and internalfixation.
158 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL
the lunate into a flexed position as the wrist movesfrom ulnar to radial deviation (Fig 8). A fairly pre-dictable DISI pattern of carpal collapse ensues oncethe mechanical stability of the scaphoid is lost, andthe end result is an unstable scaphoid nonunion (Fig9). Therefore, the scapholunate and capitolunate an-gles should be evaluated carefully on the lateral radio-graph. If either is abnormal (ie, scapholunate angle �60° and/or capitolunate angle � 15°), the surgeonmust have an increased suspicion for carpal instabilitythat implies an established nonunion with a signifi-cant humpback deformity that will be very difficult tocorrect.
EVALUATION AND TREATMENT OF NONUNIONS
The exact definition of scaphoid delayed unions andnonunions has been debated, but much of this discus-sion has become moot in the face of better imagingtechniques to evaluate scaphoid collapse. Cast immo-bilization is not appropriate for proximal pole scaph-oid fractures or nonunions. The exact details of im-mobilization for scaphoid fractures have long beenargued. Although some maintain that a long-armthumb Spica cast yields superior healing rates in amore rapid fashion compared with a short-arm cast,there is still no consensus yet on this matter.24,25 Thesame holds true regarding the ideal wrist position thata cast should strive to achieve. Furthermore, becauseradiographs frequently overestimate the extent ofhealing, immobilization is often abandoned prema-
turely in proximal pole scaphoid fractures. A CT scanis recommended to more accurately assess healingbefore cessation of cast treatment if solid bridgingtrabeculae are not visualized and the patient cannotcontinue cast immobilization.
DIAGNOSIS AND CLINICAL PRESENTATION
Often the patients will complain of a vague acheinvolving the wrist. Many athletes will modify theiractivities, such as doing knuckle pushups rather thandoing them using the palms of their hands. Whenevera trainer or physician sees this adaptive behavior he orshe should order wrist radiographs. In acute scaphoidfractures, the typical finding of pain to palpation inthe anatomic snuffbox is less reliable when assessingfor potential scaphoid nonunion (Fig 10). Frequently,swelling in this region will cause a reversal in thenormal concavity of the snuffbox.
Standard radiographs of a suspected proximal polescaphoid fracture or nonunion should include a PA,lateral wrist, scaphoid view (ulnar deviation view),and oblique view with 45° to 60° of pronation. In
FIGURE 7. The mechanism of injury in a scaphoid nonunionproduces apex dorsal angulation with loss of a trapezoidalsegment of bone, with greater volar than dorsal bone loss.(Reprinted with permission.57)
FIGURE 8. In normal wrist kinematics, the scaphoid linkageto the lunate controls the lunate motion to allow dorsal rota-tion in ulnar deviation and palmar rotation in radial deviation.With scaphoid collapse, the lunate rotates so its distal surfacefaces dorsally. (Reprinted with permission.57)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 159
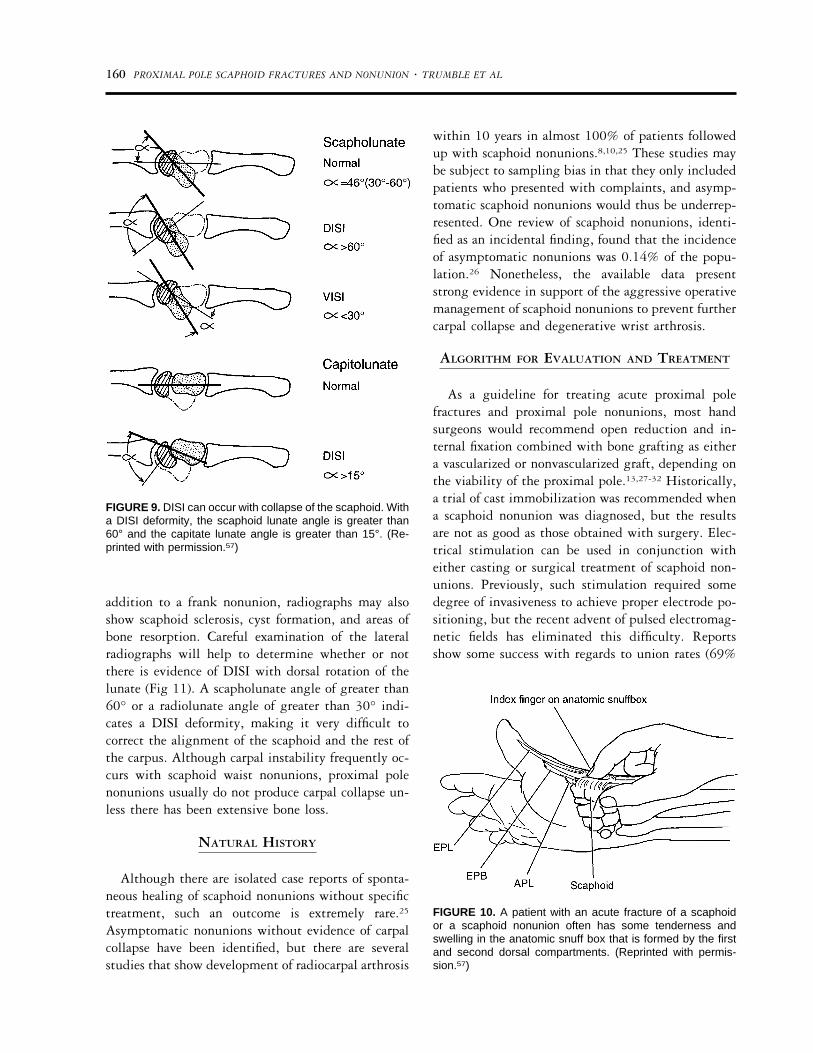
addition to a frank nonunion, radiographs may alsoshow scaphoid sclerosis, cyst formation, and areas ofbone resorption. Careful examination of the lateralradiographs will help to determine whether or notthere is evidence of DISI with dorsal rotation of thelunate (Fig 11). A scapholunate angle of greater than60° or a radiolunate angle of greater than 30° indi-cates a DISI deformity, making it very difficult tocorrect the alignment of the scaphoid and the rest ofthe carpus. Although carpal instability frequently oc-curs with scaphoid waist nonunions, proximal polenonunions usually do not produce carpal collapse un-less there has been extensive bone loss.
NATURAL HISTORY
Although there are isolated case reports of sponta-neous healing of scaphoid nonunions without specifictreatment, such an outcome is extremely rare.25
Asymptomatic nonunions without evidence of carpalcollapse have been identified, but there are severalstudies that show development of radiocarpal arthrosis
within 10 years in almost 100% of patients followedup with scaphoid nonunions.8,10,25 These studies maybe subject to sampling bias in that they only includedpatients who presented with complaints, and asymp-tomatic scaphoid nonunions would thus be underrep-resented. One review of scaphoid nonunions, identi-fied as an incidental finding, found that the incidenceof asymptomatic nonunions was 0.14% of the popu-lation.26 Nonetheless, the available data presentstrong evidence in support of the aggressive operativemanagement of scaphoid nonunions to prevent furthercarpal collapse and degenerative wrist arthrosis.
ALGORITHM FOR EVALUATION AND TREATMENT
As a guideline for treating acute proximal polefractures and proximal pole nonunions, most handsurgeons would recommend open reduction and in-ternal fixation combined with bone grafting as eithera vascularized or nonvascularized graft, depending onthe viability of the proximal pole.13,27-32 Historically,a trial of cast immobilization was recommended whena scaphoid nonunion was diagnosed, but the resultsare not as good as those obtained with surgery. Elec-trical stimulation can be used in conjunction witheither casting or surgical treatment of scaphoid non-unions. Previously, such stimulation required somedegree of invasiveness to achieve proper electrode po-sitioning, but the recent advent of pulsed electromag-netic fields has eliminated this difficulty. Reportsshow some success with regards to union rates (69%
FIGURE 9. DISI can occur with collapse of the scaphoid. Witha DISI deformity, the scaphoid lunate angle is greater than60° and the capitate lunate angle is greater than 15°. (Re-printed with permission.57)
FIGURE 10. A patient with an acute fracture of a scaphoidor a scaphoid nonunion often has some tenderness andswelling in the anatomic snuff box that is formed by the firstand second dorsal compartments. (Reprinted with permis-sion.57)
160 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL

to 80%).33,34 Similarly, periods of high-frequency ul-trasound have improved the healing of nonunions.Concomitant long arm casting has been associatedwith a higher likelihood of healing when bone stim-ulators are used. Not surprisingly, nonunions presentfor more than 5 years and proximal pole nonunionsfared the worst. Because these union rates are inferiorto those of operative treatment, pulsed electromag-netic field treatment is used mostly as an adjunct tosurgery or in cases where surgical intervention maynot be feasible and cast immobilization is the onlyoption. The key to treatment hinges on whether or notthere is avascular necrosis of the proximal pole (Fig12). Conventional bone grafts will work when theproximal pole is viable, whereas a vascularized bonegraft, usually performed by a dorsal approach, will benecessary when there is avascular necrosis of the prox-imal pole. When the proximal pole is viable, thefracture site determines the surgical approach. A dor-
sal approach is used for proximal pole nonunions,whereas a volar approach is used for nonunions ofthe scaphoid waist. Nonunions of the scaphoid waistwith avascular necrosis may also require a dorsal ap-proach.
Workup With Diagnostic Imaging StudiesOperative treatment of established scaphoid non-
unions should be advocated, given the high likelihoodof eventual development of radiocarpal arthrosis witha persistent scaphoid nonunion. Younger patientswith a shorter duration of the nonunion have the bestprognosis in the absence of avascular necrosis of theproximal pole. Although one study refutes this con-cept, the researchers did not have the advantage ofMRI studies to separate out the patients with avascu-lar necrosis of the proximal pole.13,14,35 The followingworkup is recommend for patients with minimal ar-throsis present on plain radiographs.
Indications for an MRI ScanMRI scans are of established value in detecting
occult acute scaphoid fractures.18 Their applicabilityhas also been expanded to determine the vascularity ofproximal fragments in scaphoid nonunions14 (Fig 12).Proximal fragments with absence of T1 marrow signalhave shown osteonecrosis, empty bone lacunae, andpoor uptake of fluorescent bone labels on biopsy14 (Fig13). In contrast, retention of some proximal pole
FIGURE 11. CT provides an excellent means of evaluatingdisplacement of carpal fractures and the degree of collapse.(Reprinted with permission.19)
FIGURE 12. On this MRI scan, the loss of signal from theproximal pole of the scaphoid is consistent with avascularnecrosis. (Reprinted with permission.14)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 161

signal has been associated with viable bone on histo-logic examination and normal uptake of fluorescentlabels (Figs 14 and 15). In one study based on directobservation of punctate bleeding at the time of sur-gery, the union rate decreases as the vascularity of thescaphoid decreases.4
Indications for a CT ScanCT scans can be useful in determining the presence
of nonunions or incomplete unions when radiographsare equivocal. CT scans are also helpful in planningsurgery in patients who have had extensive areas ofcollapse and/or bone resorption. The measurement ofintrascaphoid angles is also facilitated by CT scans(Fig 11). CT scans in the sagittal plane are the bestmethod of confirming fracture healing when the pa-tient needs a definitive evaluation before returning toheavy work or contact sports.
The workup can be summarized as follows:
● Obtain an MRI scan to evaluate for avascular ne-crosis when suspected to decide whether a vascular-ized bone graft is necessary.
● Obtain a CT scan for patients with significant col-lapse or bone resorption to plan for surgical recon-struction, especially if it is not clear whether or notthe fracture represents a proximal pole fracture.
SURGICAL MANAGEMENT OF SCAPHOID
NONUNIONS
Treatment OverviewWhen a scaphoid nonunion is present with normal
vascularity of the proximal pole, internal fixation andconventional bone grafting are recommended, withthe approach directed by the site of the fracture. (Thedorsal approach is used for proximal pole fractures,and the volar approach is used for waist fractures).Vascularized bone grafts are used when avascular ne-crosis is present, or when prior traditional bone graft-ing has failed to achieve union. Intercarpal instabilitynecessitates careful attention to correction of anyhumpback deformity at the nonunion site, usuallythrough placement of a volarly-based wedge graft.36
Salvage procedures such as radial styloidectomy, prox-imal row carpectomy, limited intercarpal arthrodesis,and complete wrist fusion are reserved for cases ofsevere degenerative arthrosis.
FIGURE 13. Biopsies from the scaphoid during the bonegrafting showed osteonecrosis with destruction of the normaltrabecular architecture and empty lacunae devoid of the nor-mal osteocytes. (Reprinted with permission.14)
FIGURE 14. This MRI scan shows normal signal intensityfrom the proximal pull to the scaphoid despite the fracture,indicating normal vascularity of the proximal pull. (Reprintedwith permission.14)
162 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL

Evolution of the Surgical Treatment of ScaphoidNonunions
Bone grafting has been—and still is—a verypopular form of treatment for a scaphoid nonunion.Matti introduced the concept of an inlay bone graftplaced via a dorsal approach in 1937. This proce-dure involved packing cancellous autograft into thenonunion defect after adequate excision of scleroticbone. Russe modified this method by advocating avolar approach and use of an oblong shaped graft. In1980, Russe reported another modification inwhich 2 matching corticocancellous iliac crestgrafts were implanted with their cancellous sidesfacing one another. One study reported that a care-fully followed technique advocated by Russeshowed a union rate of only 76% and that healingwas less likely with proximal pole nonunions or inthe presence of osteonecrosis.4 Another criticism oftraditional Matti-Russe grafting is the long periodof postoperative immobilization that is usually re-
quired, often over 6 months. For this reason, theaddition of supplemental internal fixation has re-cently gained favor, with a gratifying increase inunion rates (consistently �90%) and reduction induration of immobilization.13,15,37-40 When used inconjunction with bone grafting, internal fixationcan take various forms, including staples, wires, andscrews. Staples can maintain distraction of the frac-ture site and have fallen out of favor. MultipleKirschner wires can provide fixation, but not thecompressive effect achieved with screw fixation.Regardless of the type of screw used, accurate cen-tering of the implant is of critical importance. In aprevious studies, we found that successful position-ing of screws within the central third of the prox-imal pole was more likely to be achieved withcannulated implants, and this reduced the time tounion by over 50%.13,19 Although Kirschner wireswere used initially to stabilize the scaphoid, specialscrews, with threads at the proximal and distal endsor along their entire course, can be buried beneaththe cartilage, both proximally and distally, prevent-ing impingement from the screw. Wires that mi-grate or are left prominent may necessitate eventualremoval. Several screws have been specifically de-signed for use in the scaphoid. The Herbert screw(Zimmer Inc, Warsaw, IN) is a double-threadedscrew with a differential pitch that allows for com-pression at the fracture site. Its insertion can befacilitated with a positioning jig (Heune device)(Fig 16), and both of its ends are easily buriedwithin the bone. This particular jig was designedfor use with a volar Matti-Russe approach. Its can-nulated counterpart, the Herbert-Whipple screw(Zimmer Inc, Warsaw, IN), may allow for moreoptimal positioning via placement of an initialguide wire. The Acutrak Screw41,42 (Acumed, NJ) isa continuously variable-pitched, fully threadedscrew in which the diameter tapers along the lengthof the screw. A 3.0-mm cannulated screw withsmall profile screw head has been developed bySynthes Inc (Paoli, PA), although careful counter-sinking of the screw head is required.
PROXIMAL POLE NONUNIONS WITH A VIABLE
PROXIMAL POLE
For waist fractures the volar approach is favored,because it preserves the major vascular supply to the
FIGURE 15. Bone biopsy samples from the proximal pole ofpatients labeled with tetracycline before surgery for openreduction internal fixation of scaphoid nonunions showednormal uptake of the tetracycline with abundant osteoid (seearrow). This patient had a normal MRI signal from the prox-imal pole corresponding with an intact blood supply. (Re-printed with permission.14)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 163
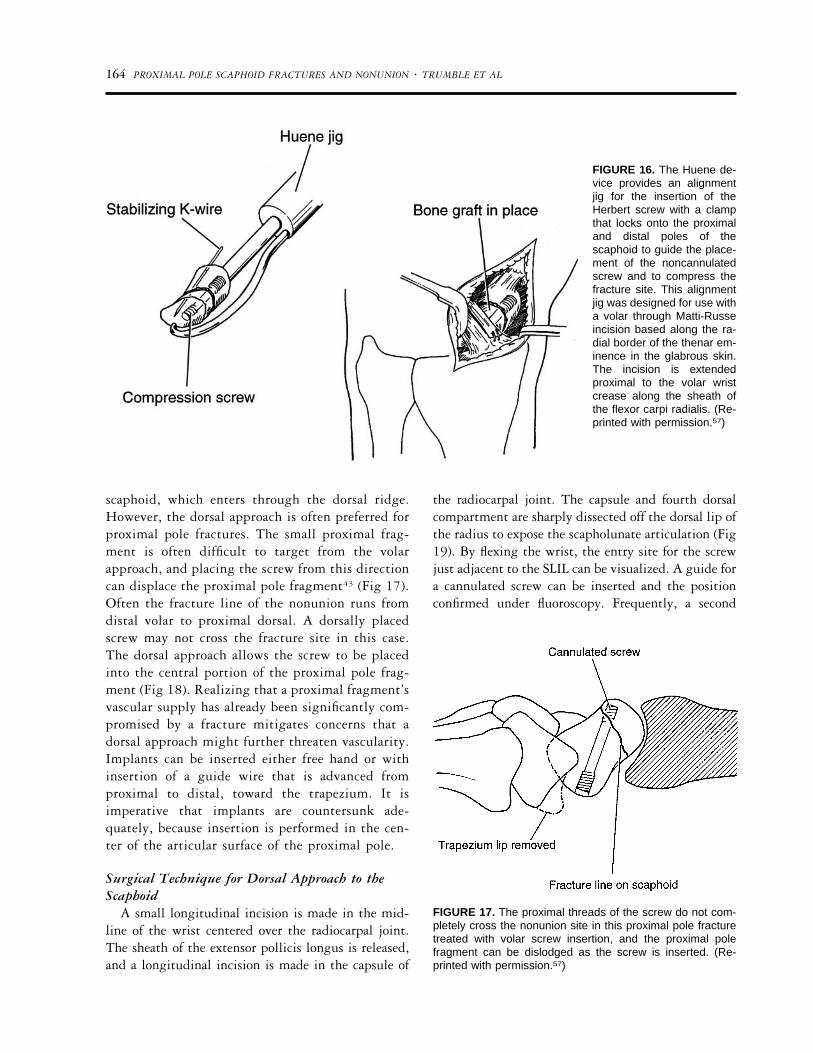
scaphoid, which enters through the dorsal ridge.However, the dorsal approach is often preferred forproximal pole fractures. The small proximal frag-ment is often difficult to target from the volarapproach, and placing the screw from this directioncan displace the proximal pole fragment43 (Fig 17).Often the fracture line of the nonunion runs fromdistal volar to proximal dorsal. A dorsally placedscrew may not cross the fracture site in this case.The dorsal approach allows the screw to be placedinto the central portion of the proximal pole frag-ment (Fig 18). Realizing that a proximal fragment’svascular supply has already been significantly com-promised by a fracture mitigates concerns that adorsal approach might further threaten vascularity.Implants can be inserted either free hand or withinsertion of a guide wire that is advanced fromproximal to distal, toward the trapezium. It isimperative that implants are countersunk ade-quately, because insertion is performed in the cen-ter of the articular surface of the proximal pole.
Surgical Technique for Dorsal Approach to theScaphoid
A small longitudinal incision is made in the mid-line of the wrist centered over the radiocarpal joint.The sheath of the extensor pollicis longus is released,and a longitudinal incision is made in the capsule of
the radiocarpal joint. The capsule and fourth dorsalcompartment are sharply dissected off the dorsal lip ofthe radius to expose the scapholunate articulation (Fig19). By flexing the wrist, the entry site for the screwjust adjacent to the SLIL can be visualized. A guide fora cannulated screw can be inserted and the positionconfirmed under fluoroscopy. Frequently, a second
FIGURE 16. The Huene de-vice provides an alignmentjig for the insertion of theHerbert screw with a clampthat locks onto the proximaland distal poles of thescaphoid to guide the place-ment of the noncannulatedscrew and to compress thefracture site. This alignmentjig was designed for use witha volar through Matti-Russeincision based along the ra-dial border of the thenar em-inence in the glabrous skin.The incision is extendedproximal to the volar wristcrease along the sheath ofthe flexor carpi radialis. (Re-printed with permission.57)
FIGURE 17. The proximal threads of the screw do not com-pletely cross the nonunion site in this proximal pole fracturetreated with volar screw insertion, and the proximal polefragment can be dislodged as the screw is inserted. (Re-printed with permission.57)
164 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL
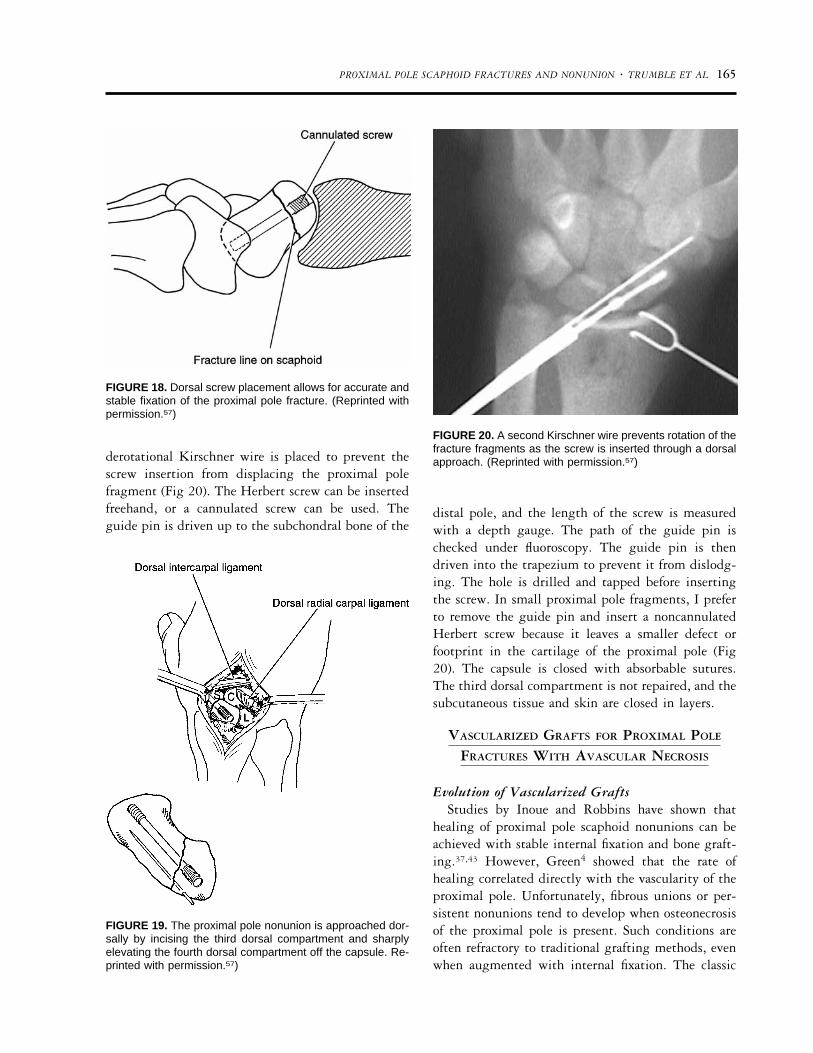
derotational Kirschner wire is placed to prevent thescrew insertion from displacing the proximal polefragment (Fig 20). The Herbert screw can be insertedfreehand, or a cannulated screw can be used. Theguide pin is driven up to the subchondral bone of the
distal pole, and the length of the screw is measuredwith a depth gauge. The path of the guide pin ischecked under fluoroscopy. The guide pin is thendriven into the trapezium to prevent it from dislodg-ing. The hole is drilled and tapped before insertingthe screw. In small proximal pole fragments, I preferto remove the guide pin and insert a noncannulatedHerbert screw because it leaves a smaller defect orfootprint in the cartilage of the proximal pole (Fig20). The capsule is closed with absorbable sutures.The third dorsal compartment is not repaired, and thesubcutaneous tissue and skin are closed in layers.
VASCULARIZED GRAFTS FOR PROXIMAL POLE
FRACTURES WITH AVASCULAR NECROSIS
Evolution of Vascularized GraftsStudies by Inoue and Robbins have shown that
healing of proximal pole scaphoid nonunions can beachieved with stable internal fixation and bone graft-ing.37,43 However, Green4 showed that the rate ofhealing correlated directly with the vascularity of theproximal pole. Unfortunately, fibrous unions or per-sistent nonunions tend to develop when osteonecrosisof the proximal pole is present. Such conditions areoften refractory to traditional grafting methods, evenwhen augmented with internal fixation. The classic
FIGURE 18. Dorsal screw placement allows for accurate andstable fixation of the proximal pole fracture. (Reprinted withpermission.57)
FIGURE 19. The proximal pole nonunion is approached dor-sally by incising the third dorsal compartment and sharplyelevating the fourth dorsal compartment off the capsule. Re-printed with permission.57)
FIGURE 20. A second Kirschner wire prevents rotation of thefracture fragments as the screw is inserted through a dorsalapproach. (Reprinted with permission.57)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 165
radiographic signs of sclerosis, cystic changes, andareas of significant bone resorption are not alwaysreliable indicators of the presence of osteonecrosis.Green advocated that intraoperative punctate bleed-ing of bony surfaces of the scaphoid be used to deter-mine vascularity.4 His recommendations were madebefore MRI scans were applied to scaphoid nonunions.As mentioned earlier, recent studies have establishedthe value of MRI signals in assessing for proximal polevascularity.14,44-46 Low signals on both T1- and T2-weighted images seem to be associated with the great-est compromise of vascular supply and poor healingrates with traditional nonvascularized grafts.
Early vascularized grafts were often based on apedicle from the pronator quadratus insertion on thedistal radius but this graft was difficult to placebecause of the short bulky muscle pedicle. More recentreports have advocated the use of a variety of sources,including the ulna artery, the first dorsal metacarpalartery, and even a free vascularized graft from the iliaccrest.7,47 As a variation on the vascularized grafttheme, Fernandez and Eggli implanted a vascularbundle from the second dorsal intermetacarpal artery
into nonunion sites.48 Although the grafts lacked abony component, union was achieved in 10 of 11patients within 10 weeks. Presently, the most fre-quently used donor sites include the dorsoradial aspectof the distal radius (first described by Zaidemberg)49
and the index metacarpal (based on the first dorsalmetacarpal artery).50,51
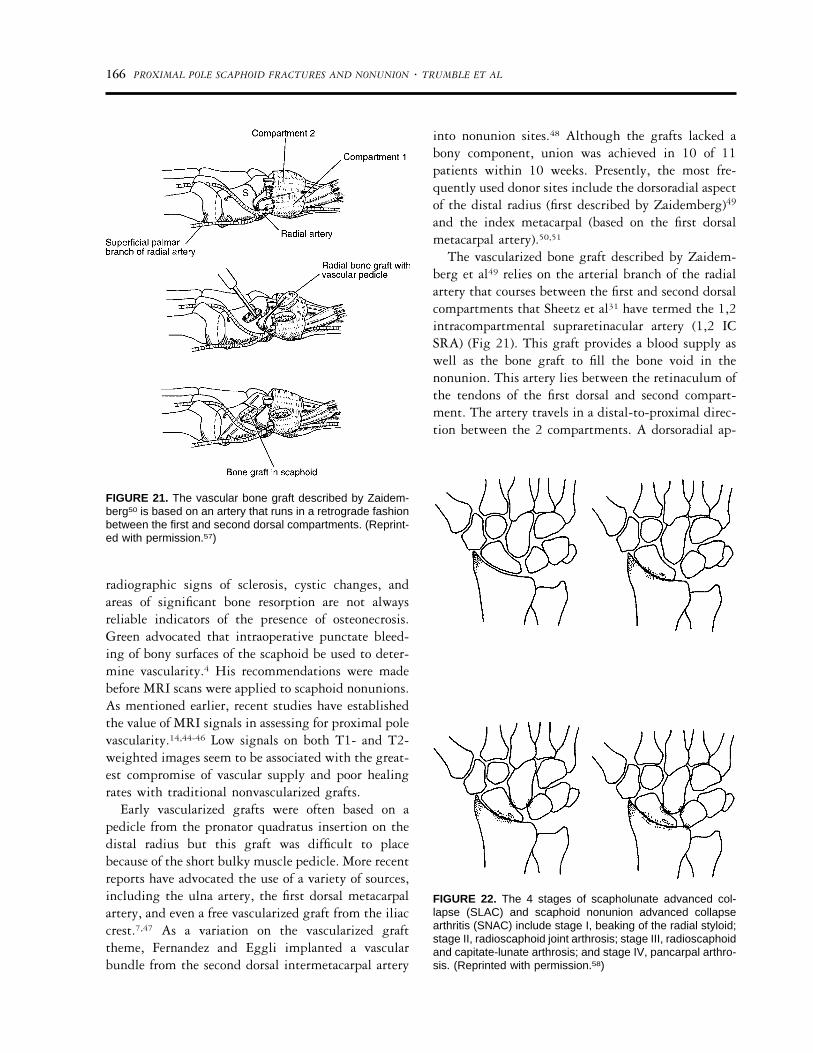
The vascularized bone graft described by Zaidem-berg et al49 relies on the arterial branch of the radialartery that courses between the first and second dorsalcompartments that Sheetz et al31 have termed the 1,2intracompartmental supraretinacular artery (1,2 ICSRA) (Fig 21). This graft provides a blood supply aswell as the bone graft to fill the bone void in thenonunion. This artery lies between the retinaculum ofthe tendons of the first dorsal and second compart-ment. The artery travels in a distal-to-proximal direc-tion between the 2 compartments. A dorsoradial ap-
FIGURE 21. The vascular bone graft described by Zaidem-berg50 is based on an artery that runs in a retrograde fashionbetween the first and second dorsal compartments. (Reprint-ed with permission.57)
FIGURE 22. The 4 stages of scapholunate advanced col-lapse (SLAC) and scaphoid nonunion advanced collapsearthritis (SNAC) include stage I, beaking of the radial styloid;stage II, radioscaphoid joint arthrosis; stage III, radioscaphoidand capitate-lunate arthrosis; and stage IV, pancarpal arthro-sis. (Reprinted with permission.58)
166 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL
proach allows for procurement of the graft andexposure of the scaphoid nonunion as an extension ofthe dorsal approach for the viable proximal pole. Theincision begins over the midline of the dorsal wristand curves proximal and radial over the interval be-tween the first and second dorsal compartments. Thethird dorsal compartment (containing the extensorpollicis longus) is released, and the extensor pollicislongus is retracted radially. The extensor carpi radialislongus is retracted ulnarly, and the capsule of thewrist is incised longitudinally to expose the scaphoid.
The vascularized bone graft is procured with anelliptical paddle of corticocancellous bone, perios-teum, and retinaculum supplied by the recurrent ves-sel from the radial artery. The 1,2 IC SRA is visible asa thin red line in the groove between the first andsecond dorsal compartments. The vessel takes off dis-tally from the radius and pierces the volar wall of thefirst dorsal compartment. The first dorsal compart-ment has to be released along its palmar surface, thetendons are retracted, and the artery is mobilized bymaking parallel incisions in the periosteum betweenthe 2 compartments tracing the course of the arteryfrom distal to proximal. Once a 2.0- to 2.5-cm pediclehas been prepared, the periosteum around the planneddonor site is incised as an ellipse or rectangle. A fineoscillating saw with constant irrigation is used to cut
the 3 side of the graft, excluding the side under thevascular pedicle. Small osteotomes are then used tocomplete the elevation of the graft. After preparationof the scaphoid nonunion site, the vascularized graft isrotated into the defect and secured with either Kirsch-ner wires or a scaphoid screw. The capsule is closedloosely to avoid strangulation of the vascular pedicle.The subcutaneous tissues and skin are closed in layers.Union was achieved in all 11 patients included inZaidemberg’s original article. In several of the original
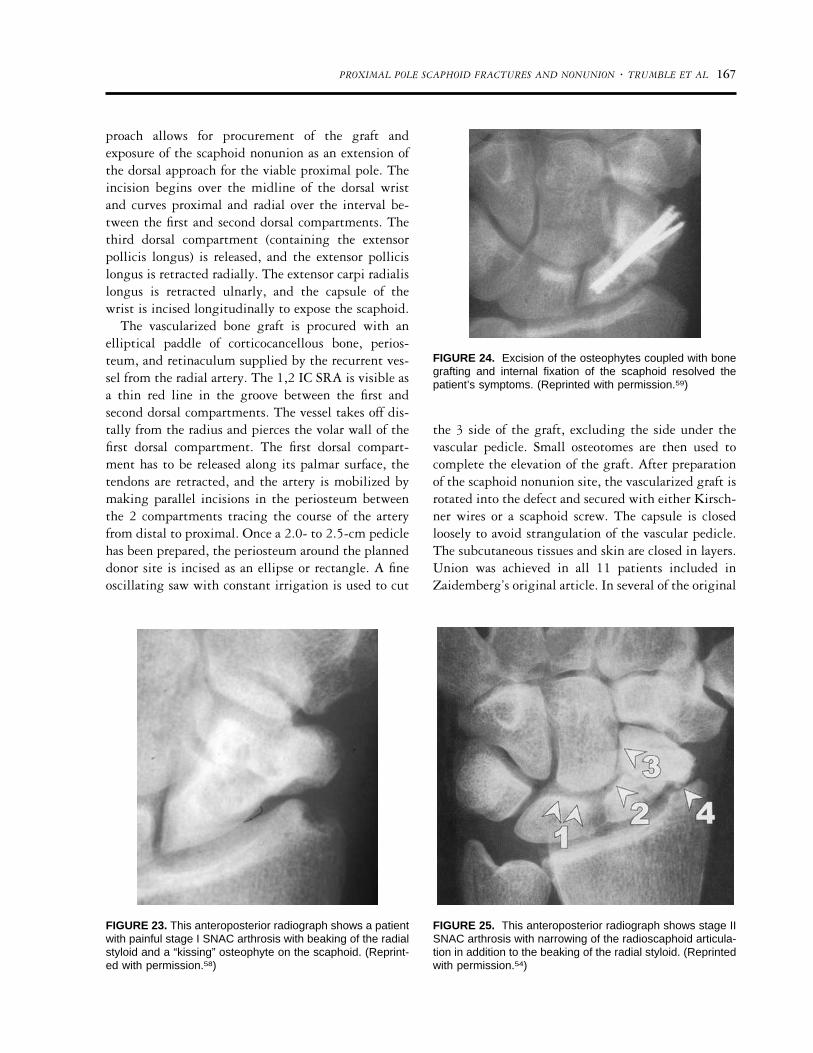
FIGURE 23. This anteroposterior radiograph shows a patientwith painful stage I SNAC arthrosis with beaking of the radialstyloid and a “kissing” osteophyte on the scaphoid. (Reprint-ed with permission.58)
FIGURE 24. Excision of the osteophytes coupled with bonegrafting and internal fixation of the scaphoid resolved thepatient’s symptoms. (Reprinted with permission.59)
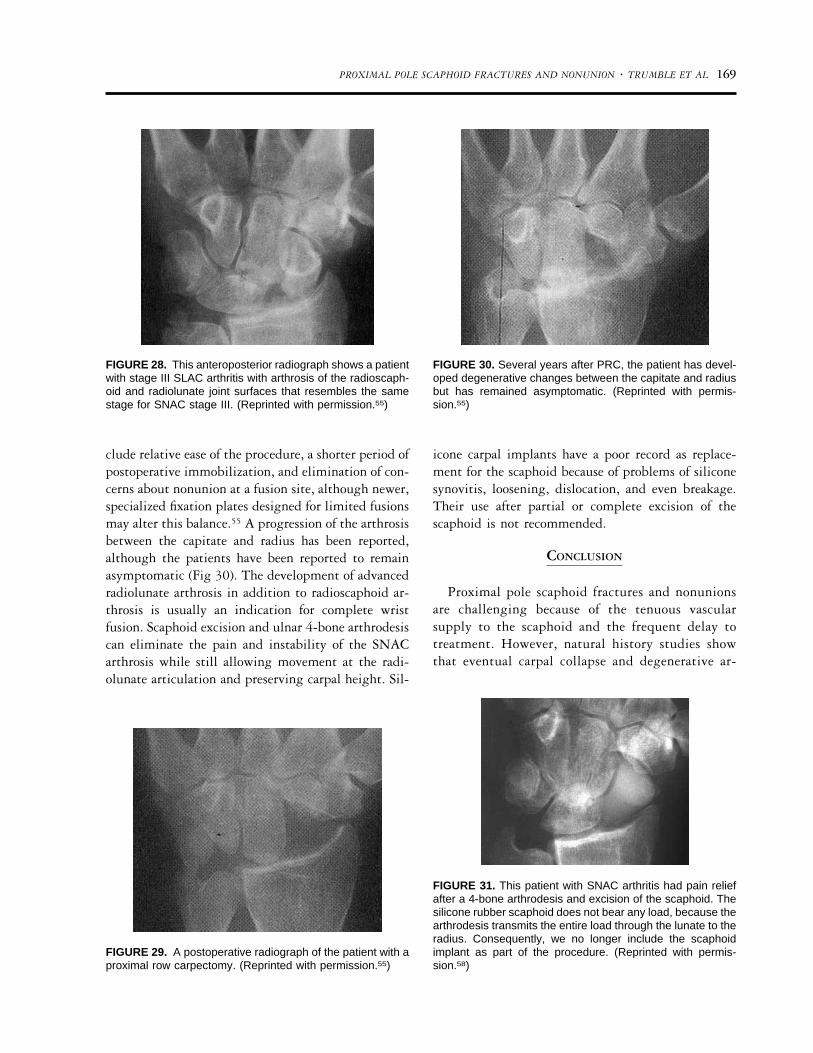
FIGURE 25. This anteroposterior radiograph shows stage IISNAC arthrosis with narrowing of the radioscaphoid articula-tion in addition to the beaking of the radial styloid. (Reprintedwith permission.54)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 167

cases, a concomitant palmar approach was required tofully address the flexion deformity of the distal scaph-oid fragment. This additional exposure has usuallybeen necessary in waist fractures with a severe hump-back deformity. In more recent cases, we have rotatedthe vascular pedicle into a volar defect through asingle approach.
Although union rates associated with the variousvascularized bone grafts appear to be high, the infre-quent use of these grafts will make it difficult todetermine the superiority of one technique over an-other. Long-term outcome studies with sufficient sam-ple size will not be easy to achieve. The complexity ofthe situation is heightened by the lack of a standard-ized definition for bony union. Although some sur-geons have used crossing trabeculae on 2 of 3 radio-graphs as sufficient criteria, others have been more
stringent, demanding that such trabeculae be presenton all radiographs to define union. Nonetheless, vas-cularized grafting clearly has a role in the treatment ofscaphoid nonunions that present with osteonecrosis orprove refractory to traditional grafting.
SALVAGE PROCEDURES FOR SCAPHOID
NONUNIONS WITH ARTHRITIS
Once significant radiocarpal or intercarpal arthrosishas developed because of a scaphoid nonunion, bonegrafting and/or internal fixation is unlikely to producea successful result. The surgeon must turn to a differ-ent armamentarium of salvage procedures to treatscaphoid nonunion advanced collapse (SNAC).
As the scaphoid collapses, the carpus rotates into afixed DISI pattern and a pattern of arthritis thatresembles the 4 stages of the arthritis from a scapholu-nate ligament disruption.52 In the first stage there isbeaking of the radial styloid (Fig 22). The secondstage is marked by arthrosis of the radioscaphoid joint.The third stage occurs when the arthrosis extends toinvolve the lunocapitate articulations. In the fourthstage, there is pancarpal arthrosis. In stage I, a radialstyloidectomy can be performed along with internalfixation and bone grafting of the scaphoid nonunion(Figs 23 and 24). In stage II arthritis there are severaloptions available. Malerich et al53 described excisionof the distal pole as the site of impingement (Figs 25and 26). The proximal pole was maintained to preventmigration of the capitate. Following this theory, Ruchet al performed arthroscopic excision of the radialstyloid and the distal pole of the scaphoid.54 Proximalcarpectomy (Figs 27 through 30) and ulnar 4-bonearthrodesis (capitate-lunate-triquetrum-hamate) withscaphoid excision have also been recommended (Fig31).55,56 Advantages of proximal row carpectomy in-
FIGURE 26. Excision of the distal pole of the scaphoidavoids impingement between the scaphoid and radius. (Re-printed with permission.54)
FIGURE 27. Proximal row car-pectomy is performed by piece-meal removal of the scaphoidfollowed by removal of the lu-nate and triquetrum. (Reprintedwith permission.58)
168 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL
clude relative ease of the procedure, a shorter period ofpostoperative immobilization, and elimination of con-cerns about nonunion at a fusion site, although newer,specialized fixation plates designed for limited fusionsmay alter this balance.55 A progression of the arthrosisbetween the capitate and radius has been reported,although the patients have been reported to remainasymptomatic (Fig 30). The development of advancedradiolunate arthrosis in addition to radioscaphoid ar-throsis is usually an indication for complete wristfusion. Scaphoid excision and ulnar 4-bone arthrodesiscan eliminate the pain and instability of the SNACarthrosis while still allowing movement at the radi-olunate articulation and preserving carpal height. Sil-
icone carpal implants have a poor record as replace-ment for the scaphoid because of problems of siliconesynovitis, loosening, dislocation, and even breakage.Their use after partial or complete excision of thescaphoid is not recommended.
CONCLUSION
Proximal pole scaphoid fractures and nonunionsare challenging because of the tenuous vascularsupply to the scaphoid and the frequent delay totreatment. However, natural history studies showthat eventual carpal collapse and degenerative ar-
FIGURE 28. This anteroposterior radiograph shows a patientwith stage III SLAC arthritis with arthrosis of the radioscaph-oid and radiolunate joint surfaces that resembles the samestage for SNAC stage III. (Reprinted with permission.55)
FIGURE 29. A postoperative radiograph of the patient with aproximal row carpectomy. (Reprinted with permission.55)
FIGURE 30. Several years after PRC, the patient has devel-oped degenerative changes between the capitate and radiusbut has remained asymptomatic. (Reprinted with permis-sion.55)
FIGURE 31. This patient with SNAC arthritis had pain reliefafter a 4-bone arthrodesis and excision of the scaphoid. Thesilicone rubber scaphoid does not bear any load, because thearthrodesis transmits the entire load through the lunate to theradius. Consequently, we no longer include the scaphoidimplant as part of the procedure. (Reprinted with permis-sion.58)
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 169

throsis will ensue. When recognized acutely, inter-nal fixation (most commonly with screw fixation)will yield union in a high percentage of cases wherethe proximal pole of the scaphoid is free of avascularnecrosis. The patients regain 80% of the motion ofthe contralateral wrist and over 70% of the strengthof the contralateral hand. Ninety percent of thepatients with painful scaphoid nonunions will notea significant decrease in wrist pain. A volar ap-proach is appropriate for waist nonunions, whereasa dorsal approach is required for proximal polefractures and nonunions to allow for proper implant
positioning. Restoration of scaphoid length andcorrection of existing humpback deformity shouldbe achieved to optimize results. Proximal pole non-unions that are accompanied by osteonecrosis ne-cessitate the addition of a vascularized bone graft.Vascularized grafts may also be useful for non-unions that fail to heal after adequate fixation andtraditional grafting methods. Salvage proceduressuch as radial styloidectomy, scaphoid excision withor without limited midcarpal fusion, proximal rowcarpectomy, and total wrist fusion are reserved forcases with severe carpal collapse and arthrosis.
REFERENCES
1. Smith K, Helm R, Tonkin MA. The Herbert screw for thetreatment of scaphoid fractures. Ann Chir Main Memb Super1991;10:556-563.
2. Osterman AL, Mikulics M. Scaphoid nonunion. Hand Clin1988;4:437-455.
3. Schneider LH, Aulicino P. Nonunion of the carpal scaphoid:the Russe procedure. J Trauma 1982;22:315-319.
4. Green DP. The effect of avascular necrosis on Russe bonegrafting scaphoid nonunion. J Hand Surg 1985;10:597-605.
5. Duppe H, Johnell O, Lundborg G, Karlsson M, RedlundJohnell I. Long-term results of fracture of the scaphoid. Afollow-up study of more than thirty years. J Bone Joint SurgAm 1994;76:249-252.
6. Amadio PC, Berquist TH, Smith DK, Ilstrup DM, CooneyWPd, Linscheid RL. Scaphoid malunion. J Hand Surg [Am]1989;14:679-687.
7. Gabl M, Reinhart C, Lutz M, et al. Vascularized bone graftfrom the iliac crest for the treatment of nonunion of theproximal part of the scaphoid with an avascular fragment.J Bone Joint Surg Am 1999;81:1414-1428.
8. Mack GR, Bosse MJ, Gelberman RH, Yu E. The naturalhistory of scaphoid non-union. J Bone Joint Surg Am 1984;66:504-509.
9. Gelberman RH, Wolock BS, Siegel DB. Fractures and non-unions of the carpal scaphoid. J Bone Joint Surg Am 1989;71:1560-1565.
10. Ruby LK, Stinson J, Belsky MR. The natural history ofscaphoid non-union. A review of fifty-five cases. J Bone JointSurg Am 1985;67:428-432.
11. Watson HK, Ryu J. Evolution of arthritis of the wrist. ClinOrthop 1986;202:57-67.
12. Herbert TJ. Natural history of scaphoid nonunion: a criticalanalysis [letter]. J Hand Surg [Am] 1994;19:155-156.
13. Trumble TE, Clarke T, Kreder HJ. Non-union of the scaph-oid. Treatment with cannulated screws compared with treat-ment with Herbert screws. J Bone Joint Surg Am 1996;78:1829-1837.
14. Trumble TE. Avascular necrosis after scaphoid fracture: acorrelation of magnetic resonance imaging and histology.J Hand Surg [Am] 1990;15A:757-764.
15. Herbert TJ, Fisher WE. Management of the fractured scaph-oid using a new bone screw. J Bone Joint Surg Br 1984;66:114-123.
16. Larsen CF, Brondum V, Skov O. Epidemiology of scaphoidfractures in Odense, Denmark. Acta Orthop Scand 1992;63:216-218.
17. Murphy DG, Eisenhauer MA, Powe J, Pavlofsky W. Can aday 4 bone scan accurately determine the presence or absenceof scaphoid fracture? Ann Emerg Med 1995;26:434-438.
18. Hunter JC, Escobedo EM, Wilson AJ, Hanel DP, Zink BrodyGC, Mann FA. MR imaging of clinically suspected scaphoidfractures. AJR Am J Roentgenol 1997;168:1287-1293.
19. Trumble TE, Gilbert M, Murray LW, Smith J, Rafijah G,McCallister WV. Displaced scaphoid fractures treated withopen reduction and internal fixation with a cannulated screw.J Bone Joint Surg Am 2000;82:633-641.
20. Bain GI, Bennett JD, MacDermid JC, Slethaug GP, RichardsRS, Roth JH. Measurement of the scaphoid humpback de-formity using longitudinal computed tomography: intra- andinterobserver variability using various measurement tech-niques. J Hand Surg [Am] 1998;23A:76-81.
21. Kim WC, Shaffer JW, Idzikowski C. Failure of treatment ofununited fractures of the carpal scaphoid. The role of non-compliance. J Bone Joint Surg Am 1983;65:985-991.
22. Gellman H, Caputo RJ, Carter V, Aboulafia A, McKay M.Comparison of short and long thumb-Spica casts for non-displaced fractures of the carpal scaphoid. J Bone Joint SurgAm 1989;71:354-357.
23. Falkenberg P. An experimental study of instability duringsupination and pronation of the fractured scaphoid. J HandSurg [Br] 1985;10:211-213.
24. Roolker W, Ritt MJ, Bos KE. Spontaneous healing of anon-union of the scaphoid. J Hand Surg [Br] 1998;23:86-87.
25. Lindstrom G, Nystrom A. Natural history of scaphoid non-union, with special reference to “asymptomatic” cases. J HandSurg [Br] 1992;17:697-700.
26. Sehat KR, Bannister GC. The prevalence of established scaph-oid fracture non-union found on incidental radiography. In-jury 2000;31:275-276.
27. Bunker TD, McNamee PB, Scott TD. The Herbert screw forscaphoid fractures. A multicentre study. J Bone Joint Surg Br1987;69:631-634.
28. Herbert TJ. Experience with the Herbert screw in the treat-ment of scaphoid fractures [letter]. J Hand Surg [Br] 1989;14:463.
29. Herbert TJ, Fisher WE, Leicester AW. The Herbert bone
170 PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL

screw: a ten year perspective. J Hand Surg [Br] 1992;17:415-419.
30. Kuhlmann JN, Mimoun M, Boabighi A, Baux S. Vascular-ized bone graft pedicled on the volar carpal artery for non-union of the scaphoid. J Hand Surg [Br] 1987;12:203-210.
31. Sheetz KK, Bishop AT, Berger RA. The arterial blood supplyof the distal radius and ulna and its potential use in vascu-larized pedicled bone grafts. J Hand Surg [Am] 1995;20:902-914.
32. Stark A, Brostrom LA, Svartengren G. Surgical treatment ofscaphoid nonunion. Review of the literature and recommen-dations for treatment. Arch Orthop Trauma Surg 1989;108:203-209.
33. Adams BD, Frykman GK, Taleisnik J. Treatment of scaphoidnonunion with casting and pulsed electromagnetic fields: astudy continuation. J Hand Surg [Am] 1992;17:910-914.
34. Frykman GK, Taleisnik J, Peters G, et al. Treatment ofnonunited scaphoid fractures by pulsed electromagnetic fieldand cast. J Hand Surg [Am] 1986;11:344-349.
35. Trezies AJ, Davis TR, Barton NJ. Factors influencing theoutcome of bone grafting surgery for scaphoid fracture non-union. Injury 2000;31:605-607.
36. Tomaino MM, King J, Pizillo M. Correction of lunate mal-alignment when bone grafting scaphoid nonunion withhumpback deformity: rationale and results of a techniquerevisited. J Hand Surg [Am] 2000;25:322-329.
37. Inoue G, Shionoya K. Herbert screw fixation by limited accessfor acute fractures of the scaphoid. J Bone Joint Surg Br1997;79:418-421.
38. Tsuyuguchi Y, Murase T, Hidaka N, Ohno H, Kawai H.Anterior wedge-shaped bone graft for old scaphoid fracturesor non-unions. An analysis of relevant carpal alignment.J Hand Surg [Br] 1995;20:194-200.
39. Stark HH, Rickard TA, Zemel NP, Ashworth CR. Treatmentof ununited fractures of the scaphoid by iliac bone grafts andKirschner-wire fixation. J Bone Joint Surg Am 1988;70:982-991.
40. Herbert TJ. Use of the Herbert bone screw in surgery of thewrist. Clin Orthop 1986;202:79-92.
41. Faran KJ, Ichioka N, Trzeciak MA, Han S, Medige J, MoyOJ. Effect of bone quality on the forces generated by com-pression screws. J Biomech 1999;32:861-864.
42. Toby EB, Butler TE, McCormack TJ, Jayaraman G. A com-parison of fixation screws for the scaphoid during applicationof cyclical bending loads. J Bone Joint Surg Am 1997;79:1190-1197.
43. Robbins RR, Ridge O, Carter PR. Iliac crest bone graftingand Herbert screw fixation of nonunions of the scaphoid withavascular proximal poles. J Hand Surg [Am] 1995;20:818-831.
44. Morgan WJ, Breen TF, Coumas JM, Schulz LA. Role ofmagnetic resonance imaging in assessing factors affectinghealing in scaphoid nonunions. Clin Orthop 1997;336:240-246.
45. Sakuma M, Nakamura R, Imaeda T. Analysis of proximalfragment sclerosis and surgical outcome of scaphoid non-union by magnetic resonance imaging. J Hand Surg [Br]1995;20:201-205.
46. Perlik PC, Guilford WB. Magnetic resonance imaging toassess vascularity of scaphoid nonunions. J Hand Surg [Am]1991;16:479-484.
47. Mathoulin C, Haerle M. Vascularized bone graft from thepalmar carpal artery for treatment of scaphoid nonunion.J Hand Surg [Br] 1998;23:318-323.
48. Fernandez DL, Eggli S. Non-union of the scaphoid. Revas-cularization of the proximal pole with implantation of avascular bundle and bone-grafting. J Bone Joint Surg Am1995;77:883-893.
49. Zaidemberg C, Siebert JW, Angrigiani C. A new vascularizedbone graft for scaphoid nonunion. J Hand Surg [Am] 1991;16:474-478.
50. Yuceturk A, Isiklar ZU, Tuncay C, Tandogan R. Treatmentof scaphoid nonunions with a vascularized bone graft based onthe first dorsal metacarpal artery. J Hand Surg [Br] 1997;22:425-427.
51. Mathoulin C, Brunelli F. Further experience with the indexmetacarpal vascularized bone graft. J Hand Surg [Br] 1998;23:311-317.
52. Watson HK, Ballet FL. The SLAC wrist: scapholunate ad-vanced collapse pattern of degenerative arthritis. J Hand Surg[Am] 1984;9:358-365.
53. Malerich MM, Clifford J, Eaton B, Eaton R, Littler JW.Distal scaphoid resection arthroplasty for the treatment ofdegenerative arthritis secondary to scaphoid nonunion.J Hand Surg [Am] 1999;24:1196-1205.
54. Ruch DS, Chang DS, Poehling GG. The arthroscopic treat-ment of avascular necrosis of the proximal pole followingscaphoid nonunion. Arthroscopy 1998;14:747-752.
55. Tomaino MM, Miller RJ, Cole I, Burton RI. Scapholunateadvanced collapse wrist: proximal row carpectomy or limitedwrist arthrodesis with scaphoid excision? J Hand Surg [Am]1994;19:134-142.
56. Watson HK, Weinzweig J, Zeppieri J. The natural progres-sion of scaphoid instability. Hand Clin 1997;13:39-49.
57. Trumble TE. Fractures and Dislocation of the Carpus. In:Trumble TE, ed. Principles of Hand Surgery and Therapy.Philadelphia: Saunders, 2000.
58. Trumble, TE. Arthritis. In: Trumble TE, ed. Principlesof Hand Surgery and Therapy. Philadelphia: Saunders,2000:401-435.
PROXIMAL POLE SCAPHOID FRACTURES AND NONUNION � TRUMBLE ET AL 171
Related Documents











