- Large patient cohort prospective study with more than 500 patients and more than 5 years follow up have shown that CyberKnife is equally effective as long coures RT - SBRT/ CyberKnife is now standard of care treatment for localized prostate cancer - Outcome of CyberKnife treatment is similar to long course RT - Side-effect after Cyberknife is less than 1% in prostate cancer - CyberKnife is safe, out patient, short course treatment in both primary and metastatic CyberKnife in prostate cancer

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
- Large patient cohort prospective study with more than 500 patients and more than 5
years follow up have shown that CyberKnife is equally effective as long coures RT
- SBRT/ CyberKnife is now standard of care treatment for localized prostate cancer
- Outcome of CyberKnife treatment is similar to long course RT
- Side-effect after Cyberknife is less than 1% in prostate cancer
- CyberKnife is safe, out patient, short course treatment in both primary and metastatic
diseases.
- High dose radiation may be effective in many of the ‘radioresistant’ disease.
CyberKnife in prostate cancer

• Most prevalent malignancy in males in western community
• 2nd MC cause of mortality in the west
• Uncommon in Asians, probably shorter lifespan
• In TMH, constitutes 2.4% of all registered pts in 2000
• In recent years, more early prostate cancer patients are diagnosed
with prostate cancer
• Prostate cancer is slow growing tumour, risk of bone metastasis is
high in ‘high risk’ group patient
Prostate cancer

Risk stratification
RISK STRATIFICATION
LOW RISK INTERMEDIATE HIGH
T1,2a, PSA < 10 ng/ml,GS</=6
T2b, GS=7
T3,4,PSA>20ng/ml,GS>7
Wait & watchSurgeryRadiation therapyHTRadiosurgery
Combination
SurgeryRadiation therapyHTRadiosurgery
Combination
SurgeryRadiation therapyHTRadiosurgery
Combination

Radiotherapy Radiation techniques: 2D Planning Conformal Radiation therapy - 3D-CRT - IMRT - SBRT
Target volume: CTV – prostate with capsule + SVT1 & small T2 with less PSA less GS only prostate is
sufficient.PTV – 1 cm margin.
Inclusion of pelvic lymph nodes still controversial.
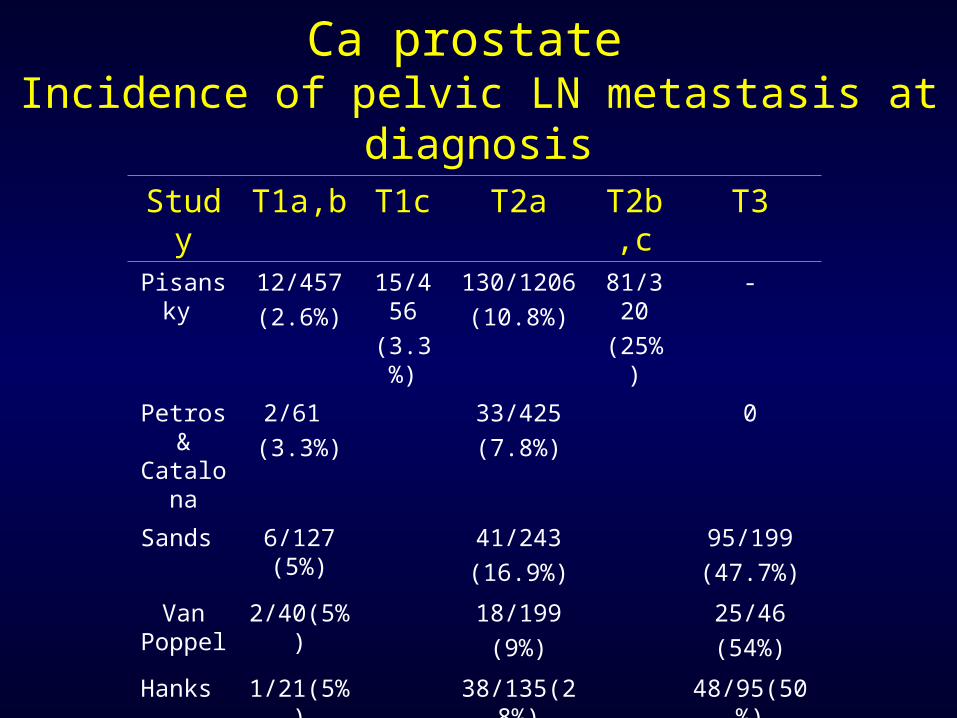
Ca prostate Incidence of pelvic LN metastasis at diagnosis
Study T1a,b T1c T2a T2b,c T3Pisansky 12/457
(2.6%)15/456(3.3%)
130/1206 (10.8%)
81/320(25%)
-
Petros & Catalona
2/61 (3.3%)
33/425(7.8%)
0
Sands 6/127 (5%) 41/243(16.9%)
95/199(47.7%)
Van Poppel
2/40(5%) 18/199(9%)
25/46(54%)
Hanks 1/21(5%) 38/135(28%) 48/95(50%)
Radiotherapy Radiation therapy schedules Conventional fractionation: - 70Gy/ 35# / 7 wk - 2Gy/# - Acute rectal & bladder toxicity
Hypofractionation schedule: - High dose per fraction, short course treatment - Equivalent loco-regional control
Ultra-hypofractionation schedule: - Very short course, high dose per fraction - Usual treatment duration 5 to 7 days

Conformal Radiation therapy reduces toxicity
• RCT• Royal Marsden Tait et al.
Gr 2 or more 5 Vs 15%.• Rotterdam trial Koper et al.
Grade 2 GI toxicity (32% vs. 19%, p = 0.02).
• M.D. Anderson Storey et al.No dif but Dose 78 vs 70.
• Nonrandomized trials• 15/27 improvement • Most pronounced when dose
escalation was not used.• When dose escalation was used, no
increased toxicity was demonstrated, except when the dose to the rectum >75 Gy.
• No article suggested increased toxicity with 3D-CRT for similar doses delivered compared withconventional RT.
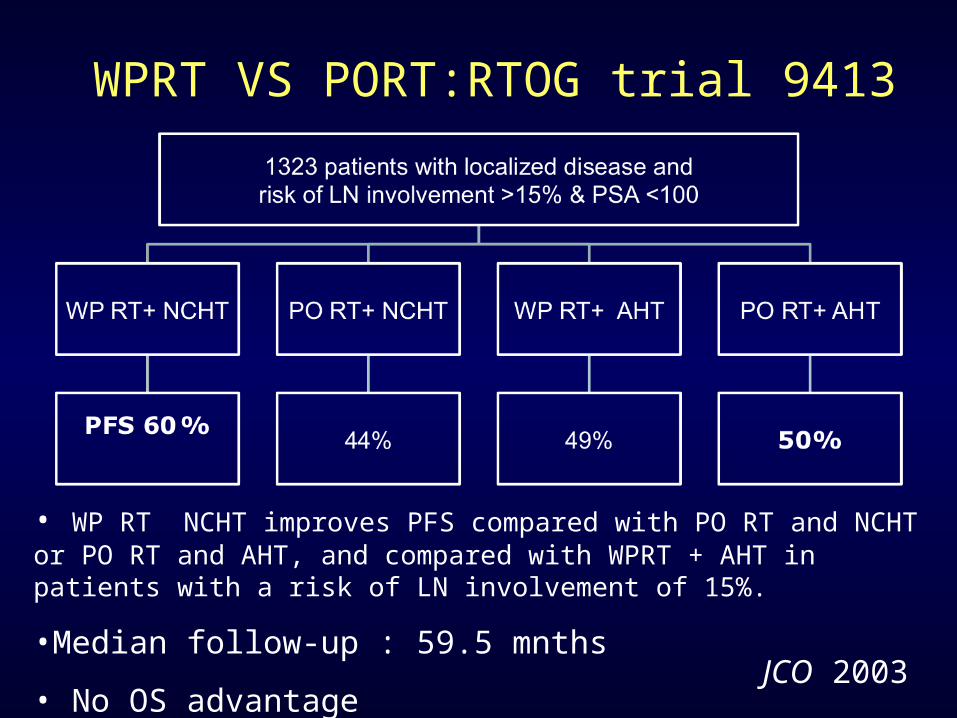
WPRT VS PORT:RTOG trial 9413
• WP RT NCHT improves PFS compared with PO RT and NCHT or PO RT and AHT, and compared with WPRT + AHT in patients with a risk of LN involvement of 15%.
•Median follow-up : 59.5 mnths
• No OS advantage JCO 2003
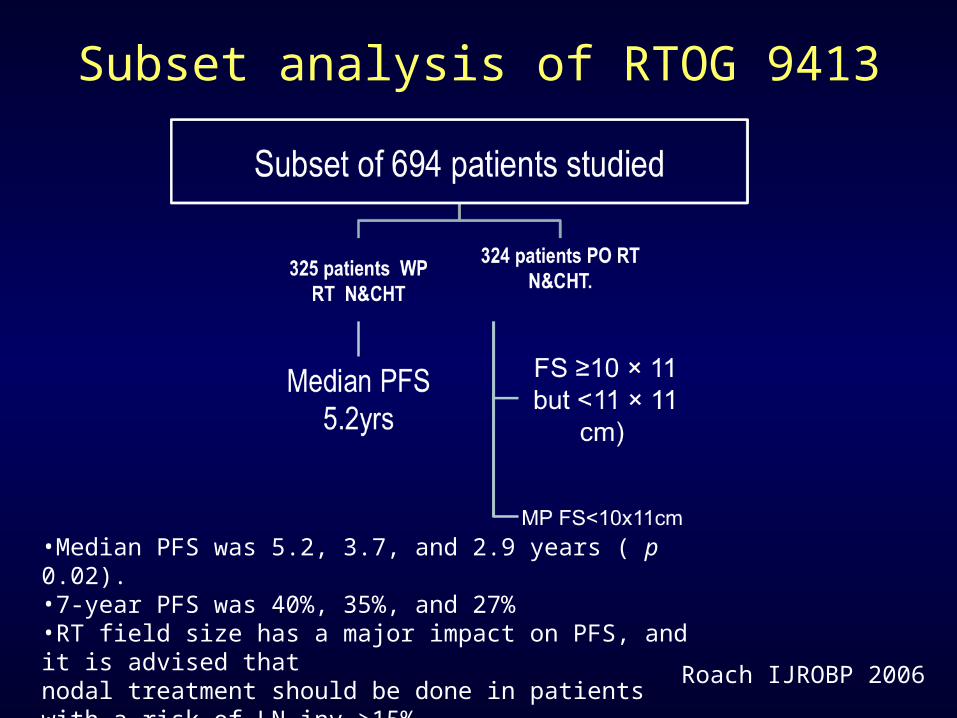
Subset analysis of RTOG 9413
•Median PFS was 5.2, 3.7, and 2.9 years ( p 0.02). •7-year PFS was 40%, 35%, and 27%•RT field size has a major impact on PFS, and it is advised thatnodal treatment should be done in patients with a risk of LN inv >15% .
Roach IJROBP 2006
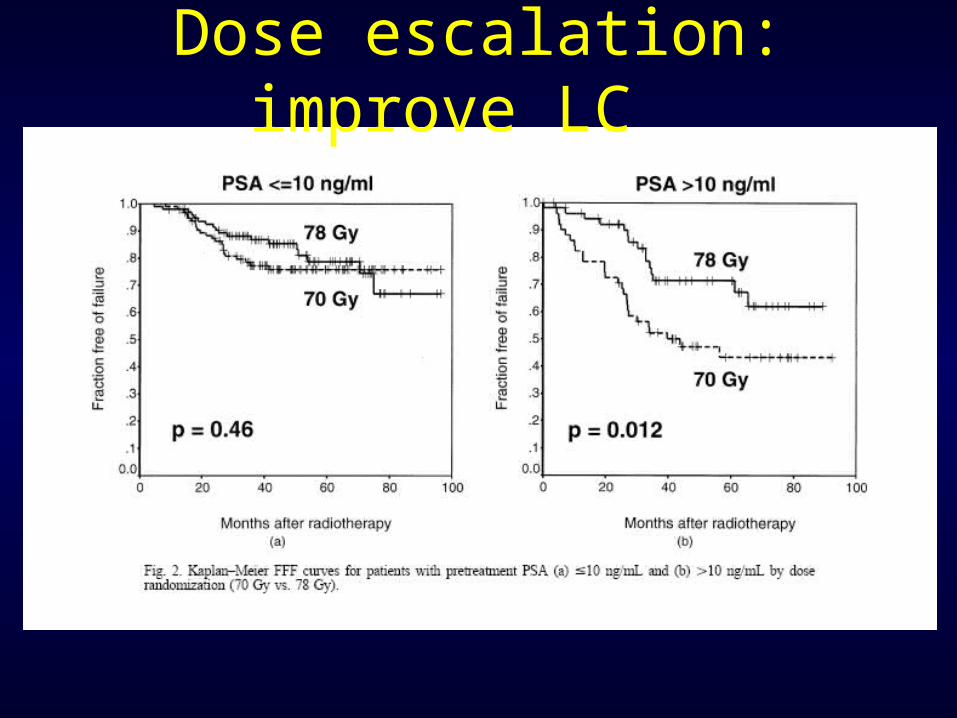
Dose escalation: improve LC

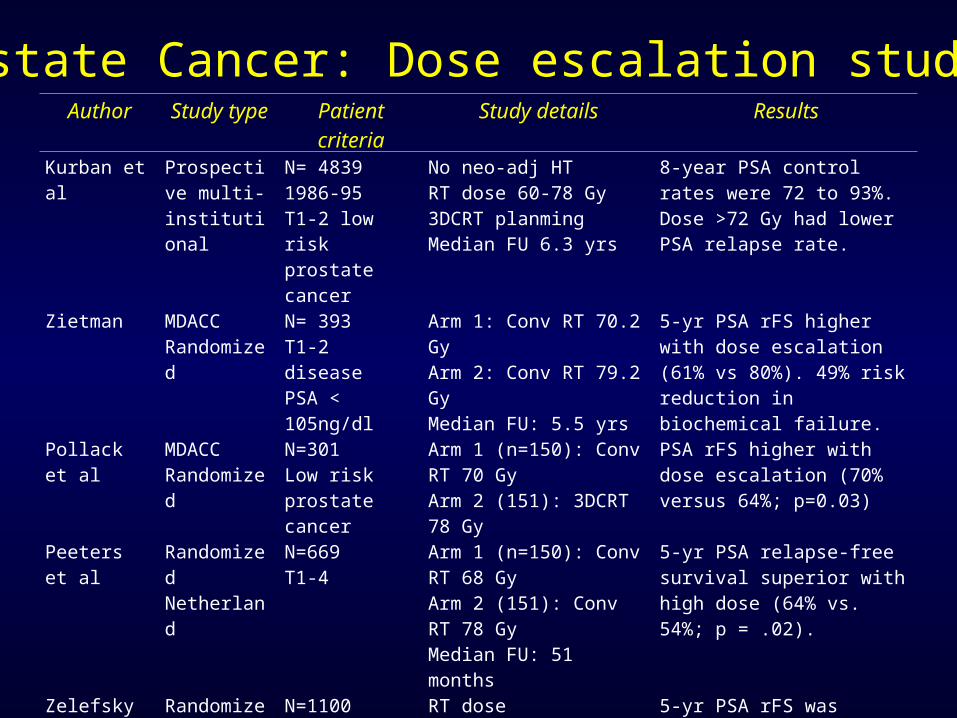
Author Study type Patient criteria Study details ResultsKurban et al Prospective
multi-institutional
N= 48391986-95T1-2 low risk prostate cancer
No neo-adj HTRT dose 60-78 Gy3DCRT planmingMedian FU 6.3 yrs
8-year PSA control rates were 72 to 93%. Dose >72 Gy had lower PSA relapse rate.
Zietman MDACCRandomized
N= 393T1-2 diseasePSA < 105ng/dl
Arm 1: Conv RT 70.2 GyArm 2: Conv RT 79.2 GyMedian FU: 5.5 yrs
5-yr PSA rFS higher with dose escalation (61% vs 80%). 49% risk reduction in biochemical failure.
Pollack et al MDACCRandomized
N=301Low risk prostate cancer
Arm 1 (n=150): Conv RT 70 GyArm 2 (151): 3DCRT 78 Gy
PSA rFS higher with dose escalation (70% versus 64%; p=0.03)
Peeters et al RandomizedNetherland
N=669T1-4
Arm 1 (n=150): Conv RT 68 GyArm 2 (151): Conv RT 78 GyMedian FU: 51 months
5-yr PSA relapse-free survival superior with high dose (64% vs. 54%; p = .02).
Zelefsky et al RandomizedMSKCC
N=11001988-98
RT dose systematically increased from 64.8 to 86.4 Gy by increments of 5.4 Gy in consecutive groups of pts.
5-yr PSA rFS was higher with dose escalation in favorable, intermediate and unfavourable groups.
Zelefsky et al Single arm N=5611996-2000
RT dose: 81 Gy to PTV 8-yr PSA rFS for favorable-, intermediate-, and unfavorable-risk groups were 85%, 76%, 72%
Prostate Cancer: Dose escalation studies
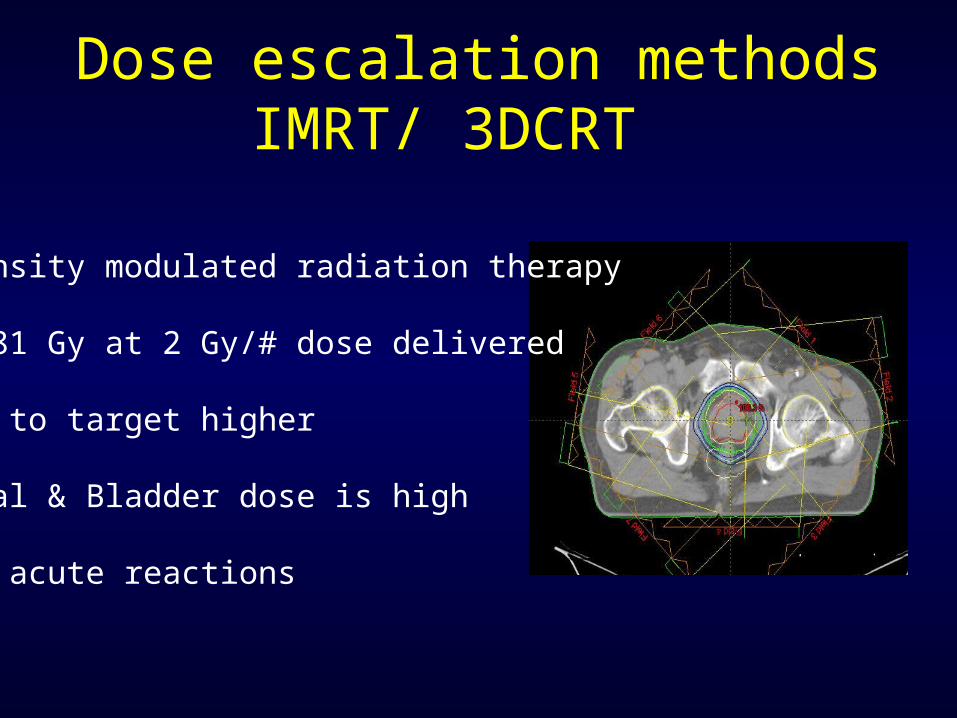
Intensity modulated radiation therapy
76- 81 Gy at 2 Gy/# dose delivered
Dose to target higher
Rectal & Bladder dose is high
High acute reactions
Dose escalation methodsIMRT/ 3DCRT
Toxicities after Radiation therapy
Rectal toxicity - Telengectasia - Bleeding - Bladder toxicity - Incontinence - Bleeding - Thimble bladder- Urethral stricture -Erectile dysfunction- Quality of life

Toxicity depends upon dose
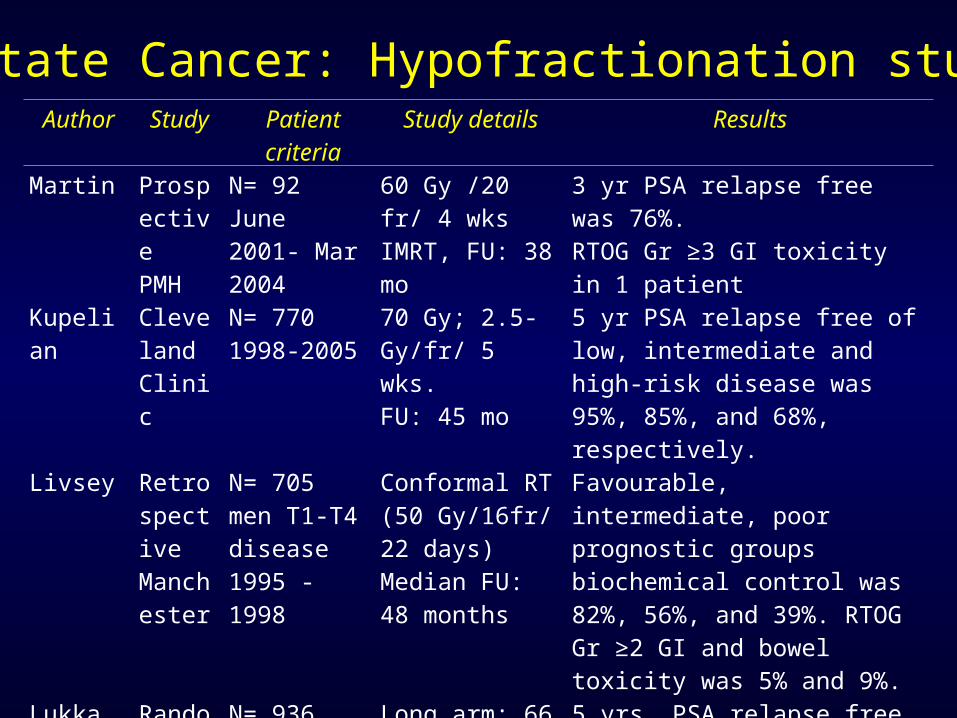
Author Study Patient criteria Study details ResultsMartin Prospect
ivePMH
N= 92June 2001- Mar 2004
60 Gy /20 fr/ 4 wksIMRT, FU: 38 mo
3 yr PSA relapse free was 76%.RTOG Gr ≥3 GI toxicity in 1 patient
Kupelian Cleveland Clinic
N= 7701998-2005
70 Gy; 2.5-Gy/fr/ 5 wks.FU: 45 mo
5 yr PSA relapse free of low, intermediate and high-risk disease was 95%, 85%, and 68%, respectively.
Livsey RetrospectiveManchester
N= 705 men T1-T4 disease 1995 -1998
Conformal RT (50 Gy/16fr/ 22 days)Median FU: 48 months
Favourable, intermediate, poor prognostic groups biochemical control was 82%, 56%, and 39%. RTOG Gr ≥2 GI and bowel toxicity was 5% and 9%.
Lukka RandomizedNCI Canada
N= 936Mar 1995- Dec1998
Long arm: 66 Gy/33 fr 45 days Short arm: 52.5 Gy/20 fr 28 days
5 yrs, PSA relapse free survival was 52.95% in long and 59.95% in short arm.GI toxicity higher with short arm (11% vs 7%)
Tsuji Chiba Japan
N=201June 1995-Feb 2004
Three clinical trials RTOG Gr ≥2 GI toxicity. 5-yr PSA relapse-free survival 83.2% without any local recurrence.
Prostate Cancer: Hypofractionation studies

Author Study Patient criteria Study details Results
King Prospective N=41Stanford
SBRT (CyberKnife)36.25 Gy/ 5 fr/ 1 weekMedian FU: 33 months
Biochemical control 100%At 12 months, 78% achieved PSA nadirRTOG Gr ≥3 rectal toxicity 4.8%
Friedland Prospective N=112NaplesFeb2005-Dec 2006
SBRT (CyberKnife)RT dose: 35-36 Gy/5 frMedian FU: 24 months
3 patients had failure (two local and one distant failure). 82% no erectile dysfunction
Brachytherapy
Galalae Three centre data
N=611Localized prostate cancer
HDR brachytherapy combined with EBRT
5-yr PSA relapse-free survival were 96%, 88%, and 69% for favorable-, intermediate-, and unfavorable-risk patients
Prostate Cancer: Ultra-hypofractionation studies

Fullar et al, IJROBP 2008
Radiosurgery mimicking brachytherapy

Fullar et al, IJROBP 2008
Radiosurgery mimicking brachytherapy

Fullar et al, IJROBP 2008
Radiosurgery vs brachytherapy: Dosimetry
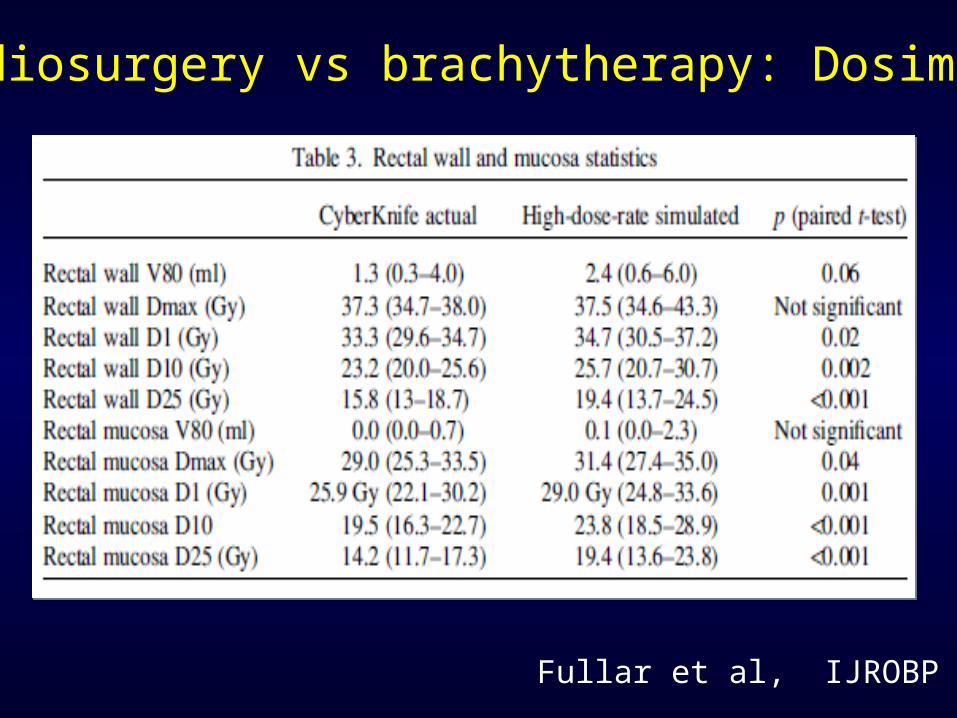
Radiosurgery vs brachytherapy: Dosimetry
Fullar et al, IJROBP 2008

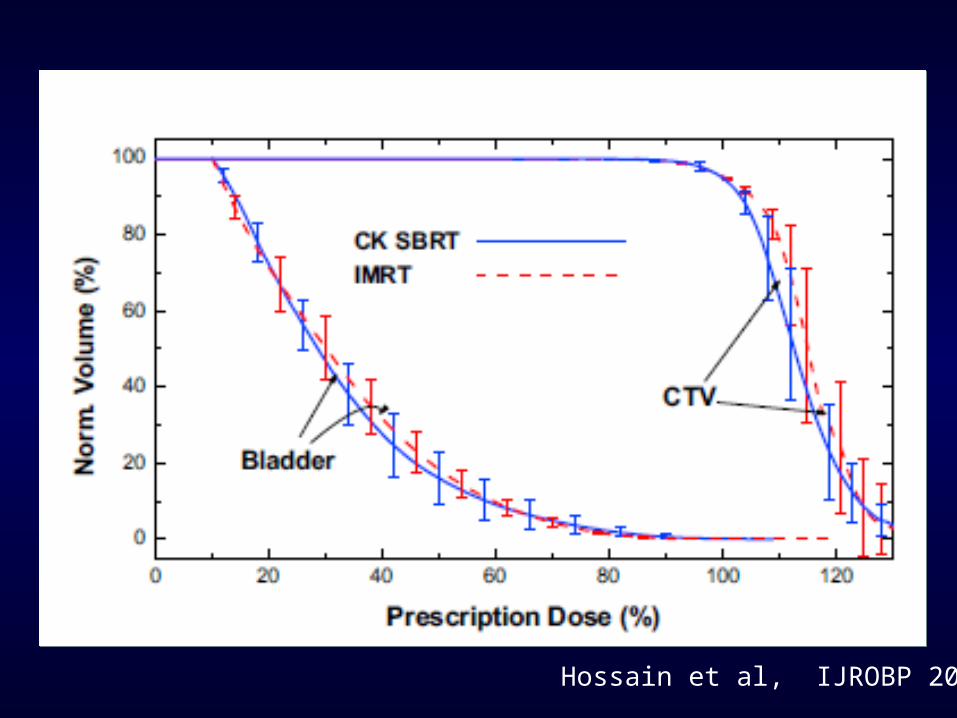
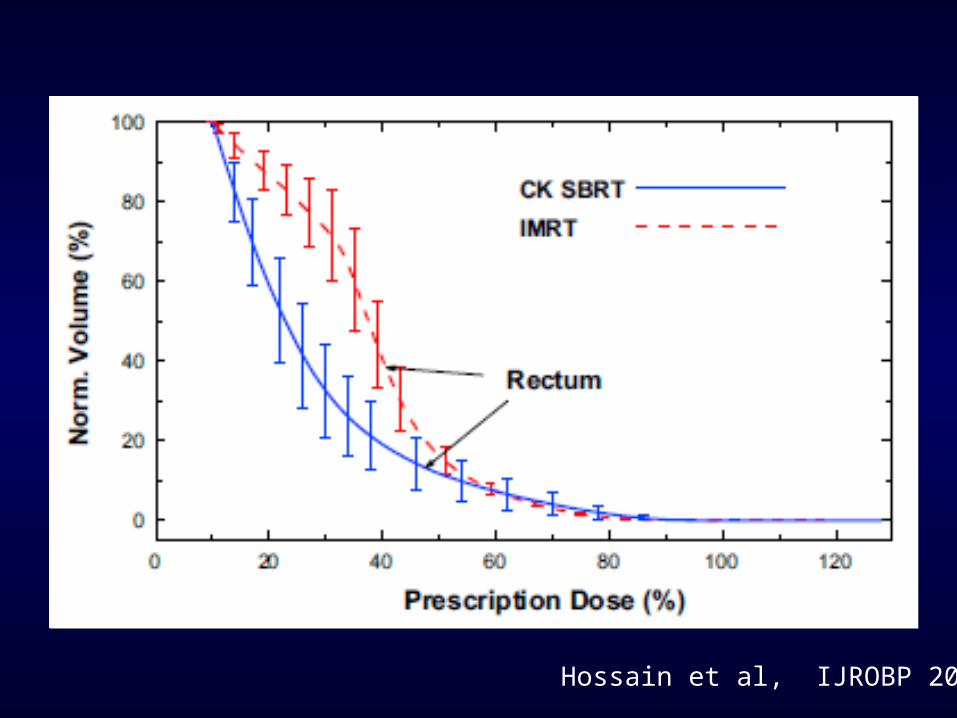
Hossain et al, IJROBP 2010
SBRT vs IMRT : Dosimetry
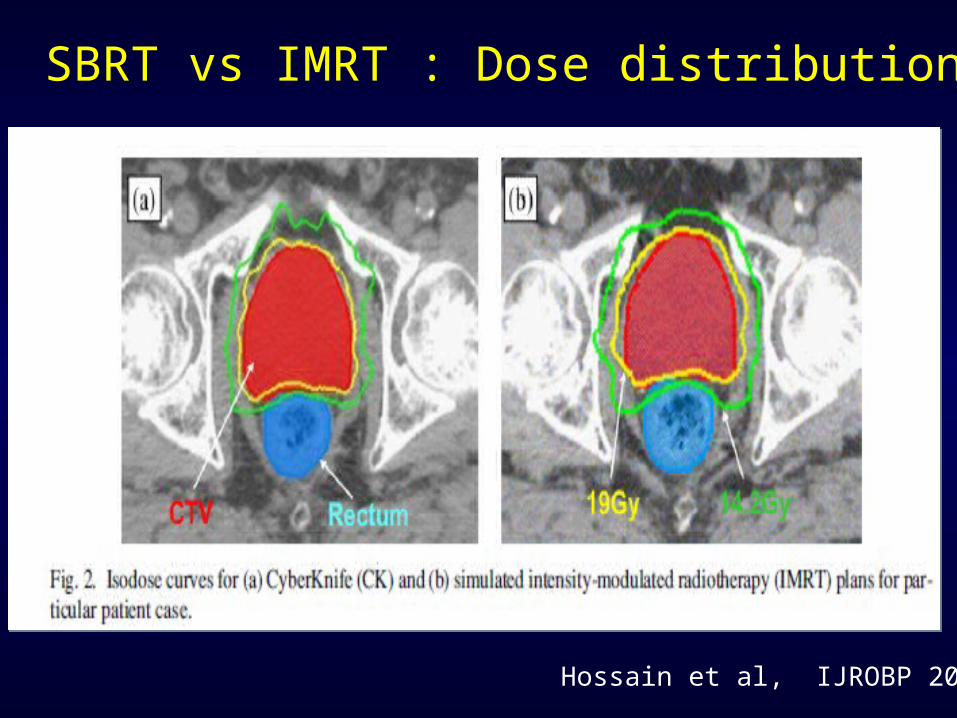
Hossain et al, IJROBP 2010
SBRT vs IMRT : Dose distribution
Hossain et al, IJROBP 2010
Hossain et al, IJROBP 2010

Hossain et al, IJROBP 2010

SBRT: Early outcome of Ph II study (n=45)
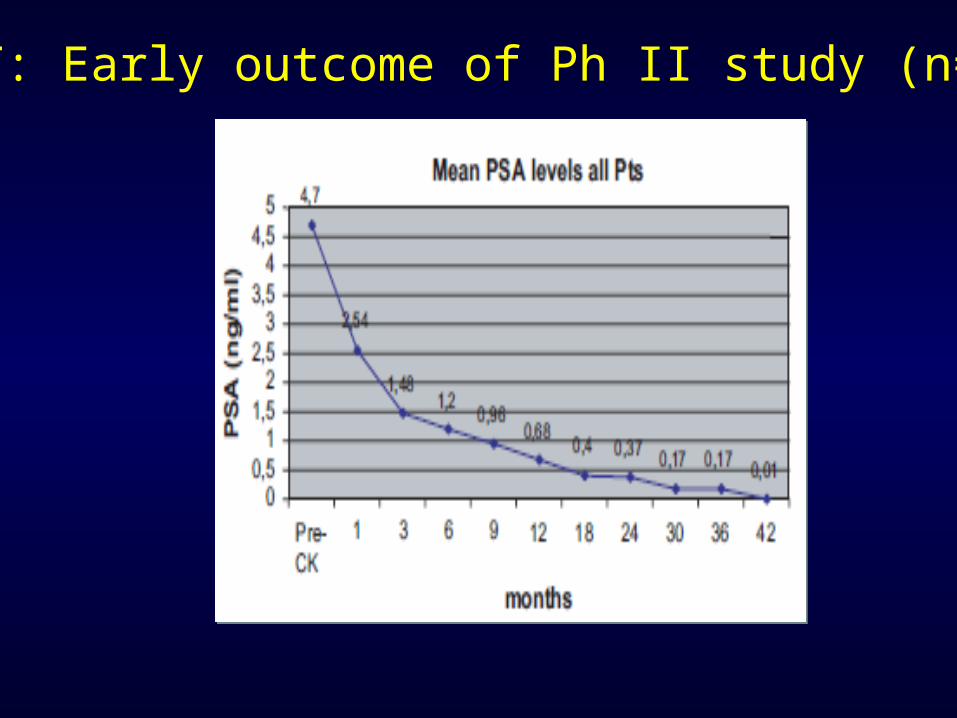
SBRT: Early outcome of Ph II study (n=45)
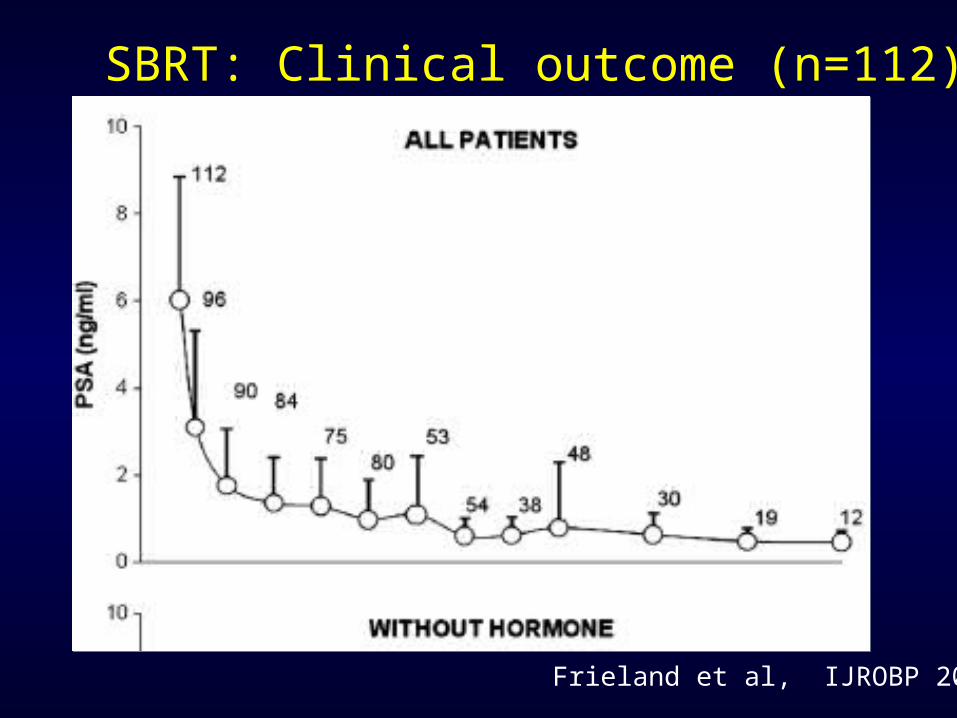
SBRT: Clinical outcome (n=112)
Frieland et al, IJROBP 2009

Probability of maintaining erectile function
Robinson et al IJROBP 2002
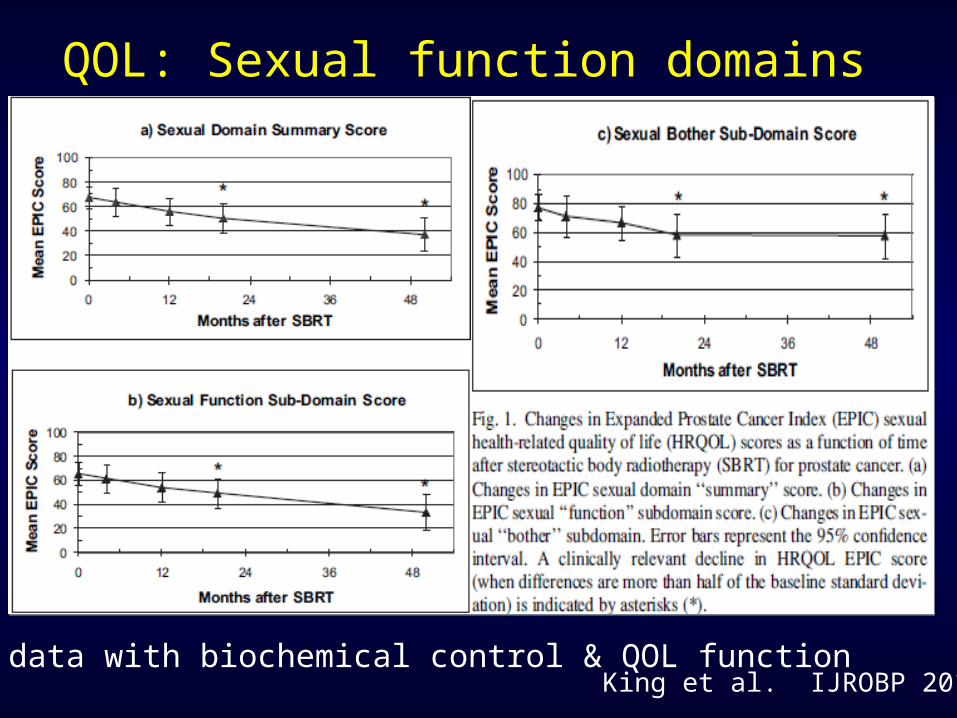
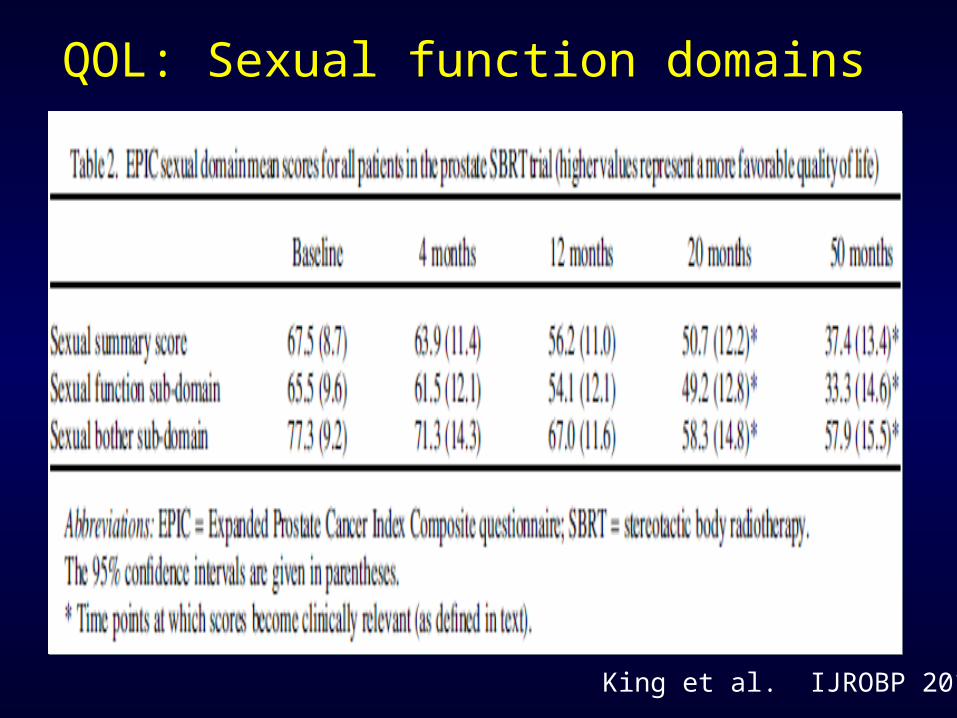
King et al. IJROBP 2010
QOL: Sexual function domains
5 yr FU data with biochemical control & QOL function
QOL: Sexual function domains
King et al. IJROBP 2010
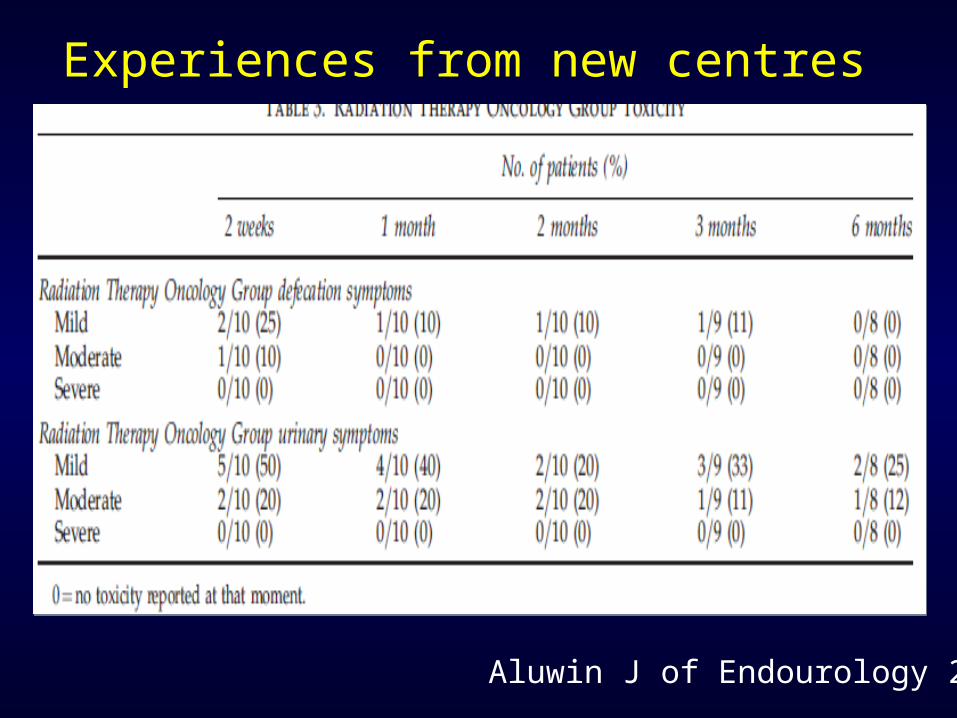
Aluwin J of Endourology 2010
Experiences from new centres

Conclusions
- Large patient cohort prospective study with more than 500 patients and more than 5
years follow up have shown that CyberKnife is equally effective as long coures RT
- SBRT/ CyberKnife is now standard of care treatment for localized prostate cancer
- Outcome of CyberKnife treatment is similar to long course RT
- Side-effect after Cyberknife is less than 1% in prostate cancer
- CyberKnife is safe, out patient, short course treatment in both primary and metastatic
diseases.
- High dose radiation may be effective in many of the ‘radioresistant’ disease.

Thank you
Dr Debnarayan Dutta, MDCyberKnife Specialist
Related Documents











