1 1 MINISTRY OF HEALTH MALAYSIA A PRESENTATION TO THE CONFERENCE ON THE NINTH MALAYSIA PLAN 15-17 FEBRUARY 2005 PROPOSED NATIONAL HEALTH CARE PROPOSED NATIONAL HEALTH CARE FINANCING MECHANISM FINANCING MECHANISM BY DATUK DR. HJ MOHD ISMAIL MERICAN DEPUTY DIRECTOR-GENERAL OF HEALTH (RESEARCH & TECHNICAL SUPPORT) MINISTRY OF HEALTH MALAYSIA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

11
MINISTRY OF HEALTH MALAYSIAA PRESENTATION TO
THE CONFERENCE ON THE NINTH MALAYSIA PLAN15-17 FEBRUARY 2005
PROPOSED NATIONAL HEALTH CARE PROPOSED NATIONAL HEALTH CARE FINANCING MECHANISMFINANCING MECHANISM
BY
DATUK DR. HJ MOHD ISMAIL MERICANDEPUTY DIRECTOR-GENERAL OF HEALTH
(RESEARCH & TECHNICAL SUPPORT)MINISTRY OF HEALTH MALAYSIA

22
OVERVIEWObjective of the presentationWhy we need a change?What we have done so far?Malaysian National Health AccountsHealth care financing model
The preferred choice for MalaysiaThe next step
Implementation plan
33
OBJECTIVE OF THE PRESENTATIONOBJECTIVE OF THE PRESENTATION
THE NEXT STEP
To inform participants on the proposed national health care
financing mechanism: principles & its current status

44
WHY DO WE NEED A CHANGE?
Current scenario
Future goal
MOH’s PROPOSALGAPSGAPS

55
WHY DO WE NEED A CHANGE?
Reduce “gaps” in the present healthcare delivery system
e.g. equity, accessibility, quality of services, lack of integration & long waiting time at government health facilities.
Ensure that all Malaysians continue to receive appropriate health care of good quality at affordable prices.

66
CURRENT SCENARIO-1
1. Highly subsidized services & overdependence on government health facilities (including those who can afford)+ heavy workload + long waiting time
2. Inadequate integration in health, especially between public & private sectors+ “brain drain” to private sector+ private sector concentrates in urban areas+ inequitable distribution of resources and services

77
CURRENT SCENARIO-2
3. Rising demand & expectations for high tech & quality medical care
4. Inability to better regulate private health care providers
5.Changing demographic & epidemiological patterns
Increase in the ageing populationIncrease in chronic diseases
88
CURRENT SCENARIO-3
6. Increasing healthcare costs+ greater inequity & public outcry if not controlled+ access to private health services is mainly for
those who can afford+ increasing trend of private health expenditure
(esp. out-of-pocket expenditure – financial risk upon unexpected health events)
+ ‘supplier-induced demand’ - inappropriate services / medication

Operating and Development Expenditure, MOH 1990-2003
-
1,000.0
2,000.0
3,000.0
4,000.0
5,000.0
6,000.0
7,000.0
8,000.0
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
RM
Mill
ion Operating
Development
Total
Note: Using Current Prices
Source: Finance Division, MOH

1010
PER CAPITA ALLOCATION FORMOH: 1998 -2003
191 19
9 212 24
8 257 30
2
0
50
100
150
200
250
300
350Allocation per capita (R
M)
1998 1999 2000 2001 2002 2003YearsNote: Using Current Prices
Source: Finance Division, MOH
1111
CURRENT SCENARIO-4
7.7. Challenges of globalization & liberalization:
cross border flow (human, life-stock, etc)transmission of diseases
more foreign workers utilizing subsidized serviceshealth insurance coverage not mandated currently

1212
MALAYSIAN NATIONAL HEATLH ACCOUNTS Definition & Chronology
A tool which describes the expenditure flows of both public & private within the health sector of a country, inclusive of the sources, uses & channels for all funds utilized in the whole health system
Time frame of the project: 2001-2005Approved by NDPC (chaired by KSN)Supported by EPUFunded by UNDPFuture plan: institutionalize in P&D of MOH

1313
MALAYSIAN NATIONAL HEATLH ACCOUNTS … preliminary results...
Total health expenditure @ 1997-2002:ranges from 2.2%-3.1% of GDP(total health expenditure for 2002: 3.1% of GDP)
Government health expenditure @ 1997-2002:ranges from 51.0%-63.7% of total health expenditure
Private health expenditure @ 1997-2002:ranges from 36.3%-49.0% of total health expenditure
GOVERNMENT SPENDING ON HEALTH IS MORE THAN PRIVATE SPENDING

1414
NATIONAL HEALTH FINANCING: MAIN OBJECTIVES
NHCF
Enhanceefficiency & quality
Greaterintegration in
Health:10 , 20 , 30
Public / private
Better regulationof health
care providers
Mobilize Resources“Risk sharing” &pooling of resources(Community rated NHI System) & manage rateof healthspending
Achieve greaterequity & accessibility
Enhance national integration, social solidarity and caring society

1515
PROPOSAL OF THE MOH
Introduction of a National Introduction of a National Health Financing Mechanism & Health Financing Mechanism &
restructuring of MOH hospitals & clinicsrestructuring of MOH hospitals & clinics

1616
PRINCIPLES OF HEALTH CARE FINANCING MECHANISM :
Superior than the existing systemSingle national health care financing system with single fund managerContribution
Mandatory- those who can afford to pay must payGovernment assistance - the poor, disabled, elderly, civil servants (& dependants + pensioners)
Viable & sustainableViable & sustainableIn line with: In line with:
National integrity, national solidarity & a caring society Vision 2020

1717
NATIONAL INTEGRITY& NATIONAL SOLIDARITY
APRIL 2004
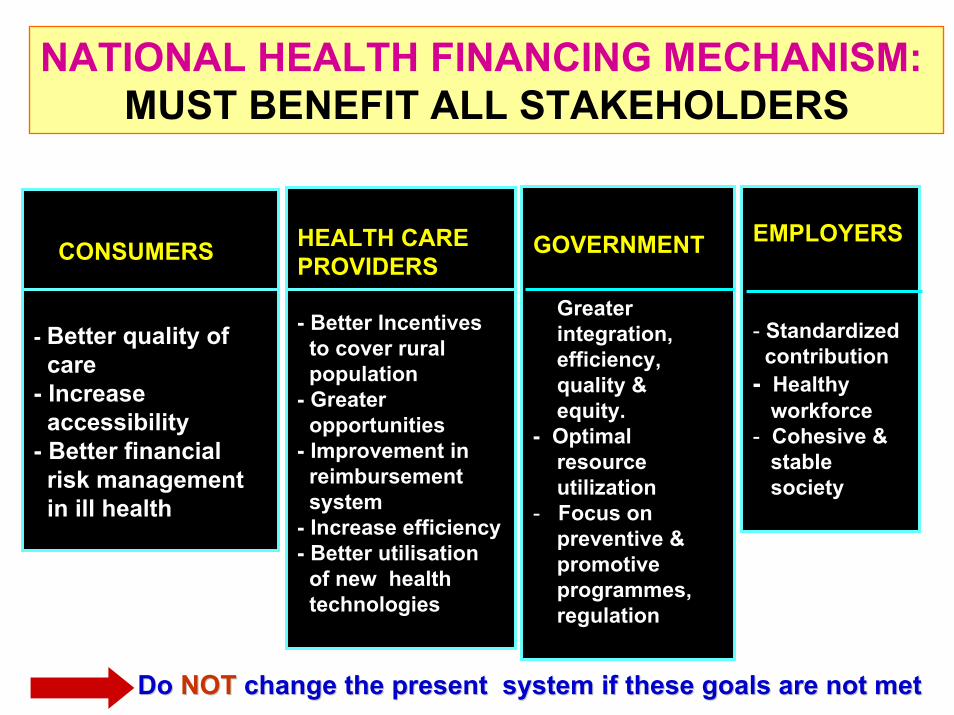
NATIONAL HEALTH FINANCING MECHANISM: MUST BENEFIT ALL STAKEHOLDERS
CONSUMERS
- Better quality of care
- Increase accessibility
- Better financial risk managementin ill health
HEALTH CAREPROVIDERS
- Better Incentives to cover rural population
- Greater opportunities
- Improvement in reimbursement system
- Increase efficiency- Better utilisation
of new health technologies
GOVERNMENT
Greater integration,efficiency,quality &equity.
- Optimal resourceutilization
- Focus on preventive & promotive programmes, regulation
EMPLOYERS
- Standardizedcontribution
- Healthy workforce
- Cohesive &stable society
Do Do NOTNOT change the present system if these goals are not metchange the present system if these goals are not met

1919
CAN WE STAY AS WE ARE?
Improvement or consolidation of the present system alone, will NOT be able to successfully achieve the desired objectives & benefits

2020
METHODOLOGYMETHODOLOGY
Review Review of various of various
relatedrelateddocumentsdocuments
Other Other Countries’Countries’
experiencesexperiences
Meetings / Meetings / forums / seminarsforums / seminars
involvinginvolvingstakeholdersstakeholders
in healthin health
PREPARATION OF THE NATIONAL HEALTH CARE FINANCING MECHANISM

2121
FEEDBACK FROM PROFESSIONAL ORGANISATIONS & NGOs
CAPCAPFOMCAFOMCAMMA MMA APHMAPHMPCDOMPCDOMCHICHIPDPKAPDPKAMTUCMTUCPhAMAPhAMAAMMAMMetc
Support National Health Support National Health Insurance Insurance Support NHFA Support NHFA
to govern health fundnnot to be privatisedot to be privatised
etc

2222
ORG. ACTIONS NEEDED / DECISIONDATES
NATIONAL HEALTH CARE FINANCING MECHANISM: -Chronology of events since MTR 4 MP (Early 1980s)
8.8.2000 EPU REACTIVATE THE DISCUSSION ON NHCF MECHANISM
30.11.2001 EPU - MEETING CHAIRED BY DG OF EPU ON NHCF27.03.2002 EPU - FOLLOW-UP MEETING WITH EPU :
TO PRESENT TO NDPC
13.06.2002 NDPC MOH TO PREPARE MEMOPRANDUM - TO CABINET
25.10.2002 YAB PM TO SEEK VIEWS OF PM; YAB PM SUPPORRTS NHI; NEED FURTHER DELIBRATION; MEMORANDUM CABINET
21.5.2003 MOF TO OBTAIN INPUT: TREASURY SUPPORTS NHCF
03.09.2003 CABINET AGREES IN PRINCIPLE, BUT IN VIEW OF IMPLICATIONSMEMBERS REQUEST SPECIAL SESSION
07.05.2004 YB HEALTH AGREES IN PRINCIPLES; SUPPORT NHI; WILL GET DATEMINISTER FOR PRESENTATION TO YAB PM
13.09.2004 NEAC MEETING ON SOCIAL SECURITY & PENSION REFORM(MTEN) CHAIRED BY YB DATO’ ,MUSTAPHA MOHAMED
02.11.2004 YAB AGREES WITH NHI; NHFA NOT TO BE PRIVATISED;PM NEEDS CONSULTANTS FOR IMPLEMENTATION

2323
NATIONAL HEALTHCARE FINANCING MECHANISM:
- THE SCOPE / SPECTRUM

2424
NATIONAL HEALTHCARE FINANCING MECHANISM
FFUUTTUURREE
HHEEAALLTTHH
SSYYSSTTEEM
Monitoring, Evaluation, Regulation & Enforcement
SOURCESOF
FINANCING
e.g. NationalHealth Insurance
NATIONALHEALTH
FUND
GOVERNANCEi.e INTER-MEDIARY
BODY(NHFA)
PROVIDERPAYMENT
MECHANISMHEALTHCARE DELIVERY SYSTEM
PATIENTS /CONSUMERS
MANDATORYCONTRIBUTION**
quantum &ceiling
ofcontribution
(**Health improvement contribution)
ESSENTIALHEALTHCARE BENEFITSPACKAGES
M
2525
NATIONAL HEALTH INSURANCE IS THE PREFERED CHOICE FOR MALAYSIA
a) Community-rated National Health Insurance (NHI)
- premium to be paid by those who can afford to pay, plus
b) Government Consolidated Revenue
- for the poor, disabled, elderly, civil servants (& dependants
+ pensioners)

2626
NATIONAL HEALTH INSURANCE -1
DEFINITION:-- ExpenditureExpenditure for for unpredictableunpredictable episodesepisodes are are
financed in advancefinanced in advance by by regularregular premiums, premiums, managed by a Government / Govt.managed by a Government / Govt.--appointed appointed authority (regulated by Govt.) toauthority (regulated by Govt.) to “cover” the “cover” the whole populationwhole population
-- Originated from Germany Originated from Germany (1893)-- Implemented in:Implemented in:
-- Europe: Europe: Germany, Belgium, France, Netherlands, etc
-- Latin America: Latin America: Chile, Argentina, Brazil, etc
-- Asia: Asia: Japan, Taiwan, Thailand, Korea, etc

2727
NATIONAL HEALTH INSURANCE-2
PARAMETERS PARAMETERS NATIONAL HEALTH INSURANCENATIONAL HEALTH INSURANCE
Contribution
Premium
Sharing of risk
Pooling of fund
Mandatory for those who can afford(employee, employer & self-employed)Government ( the poor, handicapped, elderly, civil servants & dependants, pensioners)
Community-rated(according to ability to pay & not risk-rated )Cap on income (e.g: 3%-4% of monthly income with a cap of RM 10,000)
Yes
Yes

2828
THE GOVERNANCE OF THE NATIONAL HEALTH FUND
NATIONAL HEALTH FINANCING AUTHORITY (NHFA)NATIONAL HEALTH FINANCING AUTHORITY (NHFA)
Owned by government, accountable to MOHSingle payerNot-for-profitNot to be privatisedStatutory BodyFunctions:
1. Policy, research & corporate health planning2. Health benefit packages & scope3. Assessment of health facilities & health providers - quality, efficiency, etc4. ICT planning & applications5. Health care financing data & analysis6. Fund collection & disbursement7. Strategic human resource planning & training

2929
ESSENTIAL HEALTH CARE BENEFITS PACKAGES
ESSENTIAL HEALTH CARE ESSENTIAL HEALTH CARE BENEFITS PACKAGEBENEFITS PACKAGESS-- must be in line with wellness paradigmmust be in line with wellness paradigm-- covers covers selected selected preventive, primary preventive, primary
andand hospital care serviceshospital care services-- obtainable from public & private obtainable from public & private
sectors (at sectors (at revised revised pricepricess)
SOURCE:NATIONALHEALTH
INSURANCE
OTHER SOURCES
)
OPTIONAL CARE PACKAGEOPTIONAL CARE PACKAGESS-- voluntaryvoluntary-- for optional coverage not coveredfor optional coverage not covered
in the essential health care packagesin the essential health care packages-- obtainable from public & private sectorsobtainable from public & private sectors

3030
RESTRUCTURING OF THEMOH HOSPITALS & CLINICS
(i.e. Health Care Delivery System)

3131
BENEFITS OF RESTRUCTURINGTHE MOH HOSPITALS & CLINICS
(MOH Health Care Delivery System)
Greater efficiency & competitiveness
Greater autonomy & flexibility in management &resource utilization
Flexible employment terms, better remuneration & working benefits
Promotion of professional competition & efficiency- reduction of “brain drain”
Decentralized management, yet integrated

3232
NEW ROLE OF MOH
Governmentshould
continueprovidingbudget toMOH for:
* * Regulatory, enforcement, policy formulation & monitoring to ensure quality, equity & accessibility
* Essential health care benefits packages for the poor, disabled, elderly, civil servants(& dependants + pensioners )
* Public health services (population health), research, training & development of new MOH facilities

3333
ROLE OF PRIVATE SECTOR, EPF & SOCSO
Complement the national Complement the national health financing mechanismhealth financing mechanism
this will be further deliberated this will be further deliberated in futurein future

3434
1. Consultant is needed to identify: - Financial implication to government- Appropriate level of contribution & means test- Benefit packages- Provider payment mechanism- Legal implications
2. Adopt an incremental approach- In phases (e.g. start with formal employment sector, in-patient
care etc.)- Social marketing
3. Review existing laws & formulate new ones
4. Establish the NHFA
5. Expedite & facilitate related functions of MOH which would have an impact on:
- Restructuring of the MOH hospitals & clinics
THE NEXT STEP

3535
CONCLUSION- PROPOSED HEALTH CARE SYSTEM
GovernmentConsolidated Revenue MOHMOH New New
role role of of MOHMOH
REDUCE
GAPS
MANDATORY
VOLUNTARY
NationalHealth Fund
Savings,Out-of-pocket,Private Insurance
NHFA
ESSENTIALHEALTH BENEFITPACKAGES
RESTRUCTU-RED MOHHOSPITALS & CLINICS
PRIVATESECTOR
PremiumEmployee Employer,
Self-employed,Foreign-workers
(Those who can afford)
EXTRACOVERAGE /ADDED VALUE PACKAGES

3636
Centella Asiatica
Related Documents











