Promoting Primary Care Smoking- Cessation Support with Quitlines The QuitLink Randomized Controlled Trial Stephen F. Rothemich, MD, MS, Steven H. Woolf, MD, MPH, Robert E. Johnson, PhD, Kelly J. Devers, PhD, Sharon K. Flores, MS, Pamela Villars, MEd, LPC, Vance Rabius, PhD, Tim McAfee, MD, MPH Background: Counseling by clinicians promotes smoking cessation, but in most U.S. primary care practices, it is diffıcult to provide more than brief advice to quit in the course of routine work. Telephone quitlines can deliver effective intensive counseling, but few collaborate closely with clinicians. Purpose: This study aimed to determine whether cessation support in practices is enhanced by a systems approach, in partnership with quitlines. Design: A cluster RCT was used. Setting/participants: Participants included 1817 adult smokers from 16 primary care practices in the Virginia Ambulatory Care Outcomes Research Network. Intervention: An expanded tobacco-use “vital sign” intervention (identify smokers, advise cessation, and assess readiness to quit) that was combined with fax referral of preparation-stage smokers to a quitline providing feedback to practices was compared to a traditional tobacco-use vital sign alone. Main outcome measures: The frequency of cessation support (in-offıce discussion of methods to quit or quitline referral) reported by patients in an exit survey (September 2005–July 2006, analyzed in 2008) was measured. Results: The adjusted percentage of smokers who reported receiving cessation support differed by 12.5% in intervention and control practices (40.7% vs 28.2%, respectively; p0.001). Both in-offıce discussion of methods to quit and quitline referral increased signifıcantly with the intervention. Post hoc analysis revealed that the increase in cessation was stable for both patient gender and visit type and was more pronounced with patients aged 35–54 years and with male and more experienced clinicians. Conclusions: A systems approach to identifying smokers, advising and assessing readiness to quit, combined with a partnership with a quitline, increases delivery of cessation support for primary care patients beyond that accomplished by traditional tobacco-use vital sign screening alone. Clinical trial registration: NCT00112268. (Am J Prev Med 2010;38(4):367–374) © 2010 American Journal of Preventive Medicine Introduction F ew interventions provide greater health benefıt than smoking cessation. Tobacco use is the leading cause of death in the U.S. 1 and is a major risk factor for a number of chronic diseases. 2 Clinicians have long been viewed as important catalysts for promoting smok- ing cessation. At least 70% of smokers see a physician each year, 3 and smokers cite physician advice as a major determinant in quitting. 4,5 Clinicians fınd it diffıcult to offer additional counsel- ing, however, because of lack of time, skills, staff, and reimbursement. 6,7 These missed opportunities are im- From the Departments of Family Medicine (Rothemich, Woolf, Johnson, Flores), Epidemiology and Community Health (Rothemich, Woolf), and Biostatistics (Johnson), Virginia Commonwealth University, Richmond, Virginia; Health Policy Center (Devers), Urban Institute, Washington, DC; American Cancer Society (Villars, Rabius), Atlanta, Georgia; and Depart- ment of Health Services (McAfee), School of Public Health, University of Washington; and Free & Clear, Inc., Seattle, Washington Address correspondence and reprint requests to: Stephen F. Rothemich, MD, MS, Department of Family Medicine, Virginia Commonwealth Uni- versity, 1200 East Broad Street, P.O. Box 980251, Richmond VA 23298- 0251. E-mail: [email protected]. 0749-3797/00/$17.00 doi: 10.1016/j.amepre.2010.01.008 © 2010 American Journal of Preventive Medicine • Published by Elsevier Inc. Am J Prev Med 2010;38(4)367–374 367

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

FFBVAmW
Mv0
©
Promoting Primary Care Smoking-Cessation Support with QuitlinesThe QuitLink Randomized Controlled Trial
Stephen F. Rothemich, MD, MS, Steven H. Woolf, MD, MPH, Robert E. Johnson, PhD,Kelly J. Devers, PhD, Sharon K. Flores, MS, Pamela Villars, MEd, LPC,
Vance Rabius, PhD, Tim McAfee, MD, MPH
Background: Counseling by clinicians promotes smoking cessation, but in most U.S. primary carepractices, it is diffıcult to providemore than brief advice to quit in the course of routine work. Telephonequitlines can deliver effective intensive counseling, but few collaborate closely with clinicians.
Purpose: This study aimed to determine whether cessation support in practices is enhanced by asystems approach, in partnership with quitlines.
Design: A cluster RCT was used.
Setting/participants: Participants included 1817 adult smokers from 16 primary care practices inthe Virginia Ambulatory Care Outcomes Research Network.
Intervention: An expanded tobacco-use “vital sign” intervention (identify smokers, advise cessation,andassess readiness toquit) thatwas combinedwith fax referral ofpreparation-stage smokers toaquitlineproviding feedback to practices was compared to a traditional tobacco-use vital sign alone.
Main outcome measures: The frequency of cessation support (in-offıce discussion of methodsto quit or quitline referral) reported by patients in an exit survey (September 2005–July 2006,analyzed in 2008) was measured.
Results: The adjusted percentage of smokers who reported receiving cessation support differed by12.5% in intervention and control practices (40.7% vs 28.2%, respectively; p�0.001). Both in-offıcediscussion ofmethods to quit and quitline referral increased signifıcantly with the intervention. Post hocanalysis revealed that the increase in cessation was stable for both patient gender and visit type and wasmore pronounced with patients aged 35–54 years and withmale andmore experienced clinicians.
Conclusions: A systems approach to identifying smokers, advising and assessing readiness to quit,combined with a partnership with a quitline, increases delivery of cessation support for primary carepatients beyond that accomplished by traditional tobacco-use vital sign screening alone.
Clinical trial registration: NCT00112268.(Am J Prev Med 2010;38(4):367–374) © 2010 American Journal of Preventive Medicine
I
Ffbied
i
rom the Departments of Family Medicine (Rothemich, Woolf, Johnson,lores), Epidemiology and Community Health (Rothemich, Woolf), andiostatistics (Johnson), Virginia Commonwealth University, Richmond,irginia; Health Policy Center (Devers), Urban Institute,Washington, DC;merican Cancer Society (Villars, Rabius), Atlanta, Georgia; and Depart-ent of Health Services (McAfee), School of Public Health, University ofashington; and Free & Clear, Inc., Seattle, WashingtonAddress correspondence and reprint requests to: Stephen F. Rothemich,D, MS, Department of Family Medicine, Virginia Commonwealth Uni-ersity, 1200 East Broad Street, P.O. Box 980251, Richmond VA 23298-251. E-mail: [email protected].
r0749-3797/00/$17.00doi: 10.1016/j.amepre.2010.01.008
2010 American Journal of Preventive Medicine • Published by El
ntroductionew interventions provide greater health benefıtthan smoking cessation. Tobacco use is the leadingcause of death in theU.S.1 and is amajor risk factor
or a number of chronic diseases.2 Clinicians have longeen viewed as important catalysts for promoting smok-ng cessation. At least 70% of smokers see a physicianach year,3 and smokers cite physician advice as a majoreterminant in quitting.4,5
Clinicians fınd it diffıcult to offer additional counsel-ng, however, because of lack of time, skills, staff, and
eimbursement.6,7 These missed opportunities are im-sevier Inc. Am J Prev Med 2010;38(4)367–374 367

ptcaiswtet
sbUaafStter
pttgiFatsb
sifArrfspefssnccacm
sa
ftpp
tptnswrfwcsr
MTwS
S
PApmctc
TtGU
368 Rothemich et al / Am J Prev Med 2010;38(4):367–374
ortant because half of all clinical encounters occur8 inhe primary care setting, in which short offıce visits andompeting demands impede delivery of more than briefdvice to quit. Treating tobacco use as a “vital sign” canncrease delivery of brief advice to quit,9 which helpsome smokers,10 but it does not increase the frequencyith which clinicians provide the additional assistancehat many smokers need.11 Reconfıguring practices tonable physicians or other staff to offer intensive cessa-ion counseling is feasible in exceptional settings only.12
Clinicians unable to provide intensive counseling them-elves can refer patients to telephone quitlines, an evidence-ased intervention13,14 explicitly recommended in theSDHHS smoking-cessation guideline.3 Quitlines arevailable in all states, and clinicians can refer patients bydvising smokers to call themselves or in many states byaxing/emailing a referral directly from the practice.15
mokers who call directly may be more likely to enrollhan those referred, but the infrequency with which pa-ients place such calls may ultimately make referral moreffective.16 By either means, quitline services in the U.S.emain substantially underutilized.Clinician enthusiasm for referral is more likely if therocess is easy to accomplish during busy clinical opera-ions, with available infrastructure and offıce procedureso expedite referrals. Clinicians alsowant counseling pro-rams to collaborate as partners by keeping cliniciansnformed of patients’ progress and coordinating logistics.ew quitlines routinely provide feedback to cliniciansbout the results of intensive counseling or request thathe physician provide prescriptions for medications;ome arrange classes and nonprescription medicationut do so independently of the physician.Elements of this partnership model exist in some
tates,16,17 where clinicians can refer patients for counsel-ng and pharmacotherapy, sometimes with clinicianeedback, or vouchers or direct mailings for medications.n Oregon health system16 uses an electronic medicalecord to systematize counseling and generate fax refer-als to the quitline. Practices inMichigan18 used clinicianeedback to promote quitline referrals. A trial in Minne-ota19 made quitline referrals a feature of its pay-for-erformance program. These experiments reported anffect on referrals, but few studies have documented ef-ects on in-offıce cessation support. An Australiantudy20 found that access to a quitline was helpful tomokers but was not associated with more-intensive cli-ician advice to quit. The Oregon study21 reported in-reased documentation of counseling when clinicians re-eived performance feedback. AMassachusetts study22 ofn electronic health record–based intervention that in-luded availability of fax referral found that patients were
ore often referred, predominantly via email to a healthystem counselor, and overall made more contacts withny cessation counselor.Few of these models combine all of the ideal features
or implementation in primary care. Some rely on elec-ronic prompts, but most primary care practices remainaper-based. Some require counseling to be delivered byhysicians, who face competing demands.We report a cluster RCT of the “QuitLink” interven-
ion, designed to address the above defıciencies, in whichractices used a paper-based, systems approach to iden-ify smokers, provide advice to quit, and assess willing-ess to quit (A1–3 of the 5A’s framework, see Table 1). Formokers ready to attempt quitting and willing to workith a quitline, the system also accommodated fax refer-al for free proactive telephone counseling and feedbackrom the quitline to the practices. This study examinedhether such a system increased the delivery of in-offıceessation support (a proxy for A4–5), defıned as a discus-ion of methods to quit (e.g., medications, quit date) oreferral to a quitline.
ethodshe study was approved by the IRBs of Virginia Common-ealth University and Bon Secours Richmond Healthystem.
etting
ractices were recruited under the auspices of the Virginiambulatory Care Outcomes Research Network. Eligibleractices included those within a 35-mile radius of Rich-ond (VA) with the full-time equivalent of at least twolinicians (family physicians, general internists, nurse prac-itioners, or physician assistants) who specialized in primaryare and saw at least some adult patients. From the potential
able 1. 5A’s counseling framework recommended inhe U.S. Public Health Service 2008 Clinical Practiceuideline: Treating Tobacco Use and Dependencepdate3
A1 Ask Identify and document tobacco use statusfor every patient at every visit
A2 Advise In a clear, strong, and personalizedmanner, urge every tobacco user to quit
A3 Assess Determine whether the tobacco user iswilling to make a quit attempt at thistime
A4 Assist For the patient willing to make a quitattempt, use counseling andpharmacotherapy to help him or her quit
A5 Arrange Schedule follow-up contact, in person orby telephone, preferably within the first
week after the quit datewww.ajpm-online.net

paadscotivcyo
D
Twwatsvpw
Aqsd
dssadnTvn
cvc
P
Apotits(trdsww
C
BapmQpwiedisps
Fi
To
a
b
Rothemich et al / Am J Prev Med 2010;38(4):367–374 369
A
ool of 51 sites, 29 practices were targeted for recruitmentnd 16 were enrolled. See Appendixes A–B, available onlinetwww.ajpm-online.net, for additional practice recruitmentetails. The 16 practices (three urban, four rural, and nineuburban) included 11 family medicine, two internal medi-ine, and three dual-specialty practices. Themedian numberf clinicians per practice (n�4, range�2–7) reflected na-ional norms.23,24 Only one practice used an electronicmed-cal record. Practices randomized to the control and inter-ention groups did not differ signifıcantly by the number oflinicians per practice or by the clinicians’ gender, specialty,ears since licensure, or race (see Appendix C, availablenline at www.ajpm-online.net).
ata Sources
he percentage of adult smokers who received counselingas determined by patient self-report via exit surveys, whichere administered by trained research assistants rotatingmong the practices. Research assistants asked patients athe conclusion of clinical encounters to describe the coun-eling they had just received. Eligible subjects for the inter-iew and the methods used by research assistants to visitractices are detailed in Appendix A, available online atww.ajpm-online.net.The one-page survey included questions for A1 (Ask) and2 (Advise), adapted from previous instruments,9 and twouestions designed to concisely address in-offıce cessationupport (A4 and A5): asking patients if the clinician had
able 2. Relationships among intervention, mainutcomes, 5A’s, and exit survey questions
5A’s3 Survey question
Interventiona
A1: Ask Did anyone ask you today if yousmoke?
A2: Advise If you smoke, did anyone adviseyou today to stop smoking?
A3: Assess Not assessed on the exit survey
Main outcome:in-office cessationsupport
A4: Assist; A5:Arrangeb
Discussion: If you smoke, didanyone talk with you todayabout ideas or plans to helpyou quit smoking?
Referral: If you smoke, were youreferred today to a quit line?
The stamp for the intervention practices addressed A1–3, whereasthe control stamp addressed A1 only.The two questions together addressed aspects of A4 and A5, actingas a proxy for both (1) offering pharmacotherapy, setting quit dates,arranging follow-up, and (2) offering referral to a quitline.
iscussed methods to quit (e.g., pharmacotherapy, quit p
pril 2010
ates) or had referred them to a quitline (see Table 2). Theurvey also inquired about patient age and gender, smokingtatus, counseling about other health behaviors, visit type,nd clinician seen. To limit respondent burden, the surveyid not explore additional issues, such as the patient’s readi-ess to change or which practice staff offered counseling.he survey was self-administered; research assistants pro-ided limited assistance with incomplete entries and offeredo cessation counseling.Semi-structured interviews were conducted with eight
linicians and 12 staff from four intervention practices witharying fax referral volumes, to elicit their experiences withessation counseling in general and QuitLink in particular.
re-Intervention Period
2-month “wash in” period (April–May 2005) allowedarticipating practices to incorporate the vital sign method-logy and thereby begin the study with the control condi-ion. Rooming staff (e.g., nurses, medical assistants) werenstructed to ask and record patients’ smoking status using araditional tobacco-use vital sign stamp3 (Figure 1). Exiturveys were administered for 6 weeks pre-interventionJune–July 2005) to establish each practice’s baseline cessa-ion support for visiting smokers, a statistic needed for blockandomization to reduce practice-level variation. Furtheretails about the use of these data to generate six analytictrata are provided in Appendix A, available online at ww-.ajpm-online.net. Clinicians, patients, and investigatorsere not blinded to the intervention.
omparison Period
efore the intervention, a nurse liaison trained rooming stafft all intervention practices on QuitLink implementationrocedures; the sessions were also attended by most offıceanagers and some physicians. Rooming staff were given auitLink rubber stamp (Figure 2) and instructed to (1) askatients’ smoking status; (2) advise current smokers to quitith a short sentence (e.g., “Quitting smoking is the mostmportant thing you can do for your health”); (3) ask smok-rs whether they planned to quit within 30 days; and (4)ocument responses on the stamp imprint. The noticeswerentended to prompt counseling, but no effort was made totandardize the script or protocol. The intervention alsorovided the means for fax referral to a free quitline formokers who were both ready to quit and willing to use a
igure 1. Traditional tobacco-use vital sign stamp (usedn all practices during the wash-in period and by control
ractices during the comparison period)
qdoppQoVri
(wtiirtV
vasrlwAtaqp
D
Pt8fdo
am
rdntatmwappacoa
R
P
TpwwAQtpwibmnsw
C
D1tpgtt
steaac
F(p
370 Rothemich et al / Am J Prev Med 2010;38(4):367–374
uitline, and for two forms of practice feedback (see Appen-ix A, available online at www.ajpm-online.net). Either staffr clinicians could offer referrals. When this study waslanned, Virginia did not operate a state quitline, so studyatients were referred to the American Cancer Societyuitline®, with the goal of later applying the model withther quitline programs, including those now available inirginia and throughout the country. Patients interested ineferral completed a fax referral form, providing contactnformation and necessary consents.Outcomes were measured during the comparison period
September 2005–July 2006), duringwhich referred patientsere contacted by quitline staff and offered four proactiveelephone counseling sessions (the number of calls offeredn most of the trials demonstrating effectiveness25). Whenndicated, a counselor contacted the patient’s clinician toequest a prescription for bupropion SR, the only prescrip-ion cessation medication covered by most health plans inirginia when the study was planned.Control practices continued to use only the traditional
ital sign stamp, and fax referral was unavailable. Researchssistants collected exit surveys at control and interventionites, as described above, over the 9-month comparison pe-iod. Three months into the comparison period, the stateaunched a quitline. The availability of the new state quitlineas not addressed with intervention or control practices.lthough clinicians in either control or intervention prac-ices could invite patients to use the state quitline, it was notvailable by fax referral to either group. The exit survey’suitline referral question did not specify to which quitline aatient was referred.
ata Analysis
ower analysis indicated that 16 practices and 200 pa-ients (50 in pre-intervention) per practice would provide0% power (one-sided, ��0.05) to detect an increaserom 32% to 40%. Assumptions for the power analysis areetailed in Appendix A, available online at www.ajpm-nline.net.In-offıce cessation supportwas defıned as patient report ofdiscussion of methods to quit (e.g., quit dates, arranging
igure 2. QuitLink enhanced tobacco-use vital sign stampused in intervention practices during the comparisoneriod)
edications) or quitline referral. The proportion of patients r
eceiving cessation support among all adult smokers wasetermined for each practice. Data were weighted, and aested hierarchic logistic regression was performed, the de-ails of which are provided in Appendix A, available onlinet www.ajpm-online.net. Because the hypotheses are direc-ional, signifıcance for the outcome measures was deter-ined by computing the one-sided p-value associatedith the coeffıcient of the treatment-arm independent vari-ble. Post hoc analyses examined associations betweenatient/clinician characteristics and in-offıce cessation sup-ort. The overall change (unadjusted); the overall changedjusted for patient’s gender and age, visit type, and clini-ian’s gender and years since licensure; and change by levelsf patient, visit, and clinician characteristics were measureds ORs.
esults
re-Intervention Period
he exit survey was administered for 3 months to 3203atients (581 smokers) at the 16 practices. The frequencyith which practices offered in-offıce cessation supportas divided into six ranges that defıned the strata (seeppendixA, available online atwww.ajpm-online.net). TheuitLink interventionwas assigned randomly to eight prac-ices, and there was no attrition of intervention or controlractices before or after randomization. The one practiceith an EMR was randomized to the control group. Pre-ntervention survey data revealed no signifıcant differencesetween intervention and control practices prior to imple-enting the intervention or differences with nationalorms. Further details about the pre-intervention compari-ons are provided in Appendix A, available online atww.ajpm-online.net.
omparison Period
uring the comparison period, research assistants spent8–40 days (median�21.5) at each practice. Among po-entially eligible patients at the 16 practices, 36% did notarticipate because they refused, were too ill, had lan-uage or vision diffıculties, or were designated by recep-ionists as inappropriate subjects. Participation propor-ions did not differ between study arms.Across the 16 practice sites, 10,395 patients (1817
mokers)—including 4726 patients from control prac-ices and 5669 from intervention practices—completedxit surveys during the comparison period. Respondentge, the prevalence of current smokers, and the percent-ge of visits for general checkups did not differ signifı-antly between the two groups. The intervention group
espondents included more women (Table 3).www.ajpm-online.net

d6icav
PS
Pncpjs
SS
Toabda
P
Ppbfnmtcsvt
T
a
b
c
d
e
I
Td
Na
b
c
Rothemich et al / Am J Prev Med 2010;38(4):367–374 371
A
Consistentwith the study plan, therewas no signifıcantifference in tobacco screening, which was reported by1.2% of smokers in intervention practices and by 66.5%n control practices (p�0.45). There was also no signifı-ant difference in the percentages of patients receivingdvice to quit: 58.2% and 55.3%, respectively, in the inter-ention and control sites (p�0.39).
able 4. Outcomes of intervention, stratified by counselin
Counseling behavior
Affirmativ
ICCbControl(%)c
Interventio(%)d
Ask 0.105 66.5 61.2
Advise 0.062 55.3 58.2
Main outcome: in-officecessation support
0.024 28.2 40.7
Secondary outcomes
Discussion 0.021 27.7 34.4
Referral 0.024 8.7 21.4
Data weighted to adjust for uneven patient sampling over the comhierarchic logistic regression.Estimate of the ICCEight practices with denominators of n�958 smokersEight practices with denominators of n�857 smokersThe CI for each of Ask and Advise is two sided. The CI for each of tsided and the 95% lower confidence bound is reported.
able 3. Characteristics of study groups surveyeduring exposure to intervention
Control Intervention p-valuea
Number ofpractices
8 8
Number ofpatients
4726 5669
Mean age (years[range])b
50 (18–100) 52 (18–100) 0.20
Gender (female,%)c
56 63 0.04
Office visits forgeneralcheckup (%)c
61 60 0.95
Patients whocurrentlysmoke (%)c
21 (n�958) 16 (n�857) 0.11
ote: Boldface values indicate significance.Two-sample independent t-test accounting for within- and between-practice variationMean of practice-level mean ages. Ranges represent actual agesreported by patients.Mean of practice-level percentages
CC, intracluster correlation
pril 2010
rimary Outcome: In-Office Cessationupport
atients at the QuitLink intervention practices were sig-ifıcantly more likely to report the receipt of in-offıceessation support (Table 4). Intervention and controlractices differed by 12.5% (40.7% vs 28.2%) in the ad-usted percentage of patients who reported receiving suchupport (p�0.001).
econdary Outcomes: Cessation Supportubcomponents
he effect of the intervention on cessation support wasbserved for both in-offıce discussion of methods to quitnd referral for quitline counseling (Table 4). Analyzedy cluster, the adjusted percentage of patients reporting aiscussion of methods to quit differed by 6.7% (p�0.001)nd for quitline referral differed by 11.8% (p�0.001).
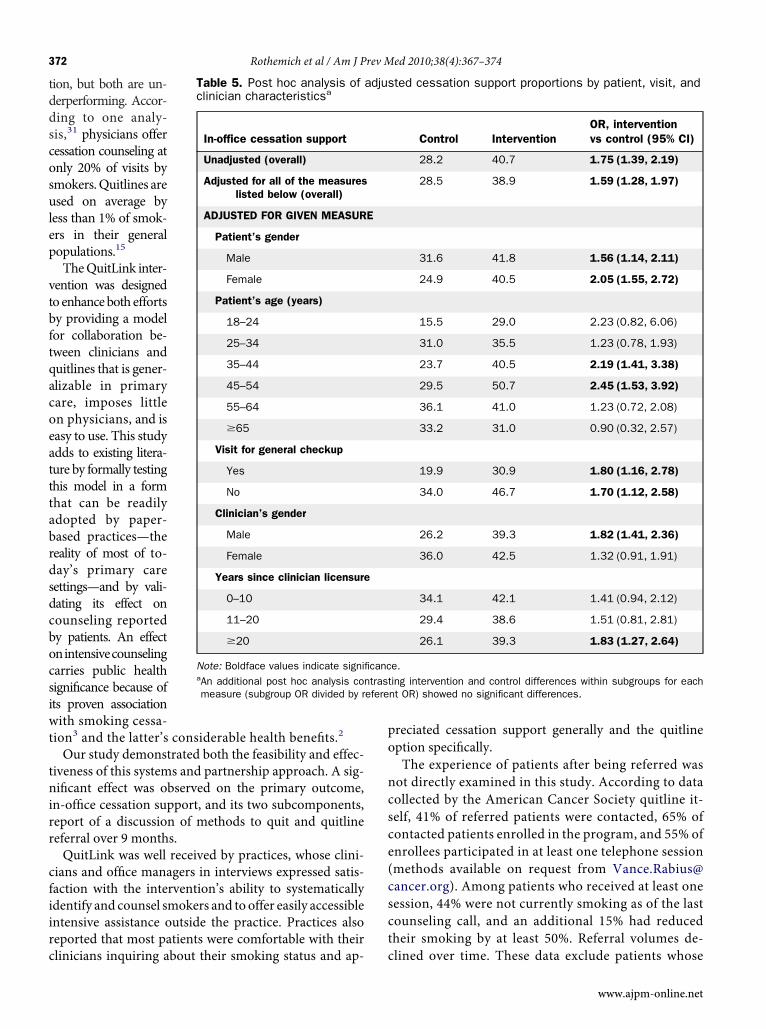
ost Hoc Comparisons
ost hoc comparison of the intervention and controlractices (Table 5) showed that the effect was stable foroth male and female patients (OR�1.56 and 2.05) andor offıce visits reported as checkups or health mainte-ance and as other visits (OR�1.80 and 1.70). Improve-ent in the main outcome was more likely among pa-
ients aged 35–54 years (OR�2.19 and 2.45); malelinicians (OR�1.82); and clinicians at least 20 yearsince licensure (OR�1.83). However, within the inter-ention group, there were no signifıcant differences inhe main outcome across levels of these patient, visit,
or clinician charac-teristics. The OR de-creased slightly (from1.75 to 1.59) but re-mained signifıcant af-ter multivariate (col-lective) adjustment forpatient characteris-tics (gender and age);visit type; and cliniciancharacteristics (genderand years since licen-sure; Table 5).
DiscussionCurrent guide-lines3,26–30 empha-size the need for themedical communityand quitlines to pro-
tivities (5A’s framework3)
ponsea
Difference(95% CI; %)e p-value
5.3 (�20.5, 9.9) 0.45
3.0 (�4.7, 10.7) 0.39
12.5 (>8.7) <0.001
6.7 (>4.2) 0.001
11.8 (>8.8) <0.001
on period and analyzed with nested
ain and secondary outcomes is one
g ac
e res
n
paris
he m
mote smoking cessa-
tddscosulep
vtbftqacoeatttabrdsdcbocsiwt
tnirr
cfiirc
po
ncsce(csct
efere
372 Rothemich et al / Am J Prev Med 2010;38(4):367–374
ion, but both are un-erperforming. Accor-ing to one analy-is,31 physicians offeressation counseling atnly 20% of visits bymokers.Quitlines aresed on average byess than 1% of smok-rs in their generalopulations.15
TheQuitLink inter-ention was designedoenhanceboth effortsy providing a modelor collaboration be-ween clinicians anduitlines that is gener-lizable in primaryare, imposes littlen physicians, and isasy to use. This studydds to existing litera-ure by formally testinghis model in a formhat can be readilydopted by paper-ased practices—theeality of most of to-ay’s primary careettings—and by vali-ating its effect onounseling reportedy patients. An effectnintensivecounselingarries public healthignifıcance because ofts proven associationith smoking cessa-ion3 and the latter’s considerable health benefıts.2
Our study demonstrated both the feasibility and effec-iveness of this systems and partnership approach. A sig-ifıcant effect was observed on the primary outcome,n-offıce cessation support, and its two subcomponents,eport of a discussion of methods to quit and quitlineeferral over 9 months.QuitLink was well received by practices, whose clini-
ians and offıce managers in interviews expressed satis-action with the intervention’s ability to systematicallydentify and counsel smokers and to offer easily accessiblentensive assistance outside the practice. Practices alsoeported that most patients were comfortable with their
Table 5. Post hoc analysis ofclinician characteristicsa
In-office cessation support
Unadjusted (overall)
Adjusted for all of the measureslisted below (overall)
ADJUSTED FOR GIVEN MEASUR
Patient’s gender
Male
Female
Patient’s age (years)
18–24
25–34
35–44
45–54
55–64
�65
Visit for general checkup
Yes
No
Clinician’s gender
Male
Female
Years since clinician licensure
0–10
11–20
�20
Note: Boldface values indicate signifiaAn additional post hoc analysis conmeasure (subgroup OR divided by r
linicians inquiring about their smoking status and ap- c
reciated cessation support generally and the quitlineption specifıcally.The experience of patients after being referred wasot directly examined in this study. According to dataollected by the American Cancer Society quitline it-elf, 41% of referred patients were contacted, 65% ofontacted patients enrolled in the program, and 55% ofnrollees participated in at least one telephone sessionmethods available on request from [email protected]). Among patients who received at least oneession, 44% were not currently smoking as of the lastounseling call, and an additional 15% had reducedheir smoking by at least 50%. Referral volumes de-
ted cessation support proportions by patient, visit, and
Control InterventionOR, interventionvs control (95% CI)
28.2 40.7 1.75 (1.39, 2.19)
28.5 38.9 1.59 (1.28, 1.97)
31.6 41.8 1.56 (1.14, 2.11)
24.9 40.5 2.05 (1.55, 2.72)
15.5 29.0 2.23 (0.82, 6.06)
31.0 35.5 1.23 (0.78, 1.93)
23.7 40.5 2.19 (1.41, 3.38)
29.5 50.7 2.45 (1.53, 3.92)
36.1 41.0 1.23 (0.72, 2.08)
33.2 31.0 0.90 (0.32, 2.57)
19.9 30.9 1.80 (1.16, 2.78)
34.0 46.7 1.70 (1.12, 2.58)
26.2 39.3 1.82 (1.41, 2.36)
36.0 42.5 1.32 (0.91, 1.91)
34.1 42.1 1.41 (0.94, 2.12)
29.4 38.6 1.51 (0.81, 2.81)
26.1 39.3 1.83 (1.27, 2.64)
e.ing intervention and control differences within subgroups for eachnt OR) showed no significant differences.
adjus
E
canctrast
lined over time. These data exclude patients whose
www.ajpm-online.net

cl
amsotfnpeto
mteitbsclwosfodlai(Fto
cwbWqoIliwcsca
fa
TA5baJMoAaFTclrPPmcTPlan
p
a
R
Rothemich et al / Am J Prev Med 2010;38(4):367–374 373
A
linician may have directed them to the Virginia quit-ine after it became available.Partnerships between clinicians and quitlines presentwin–win scenario for patients, clinicians, and com-unity programs. Patients obtain more-intensive as-istance. Clinicians, who recognize the importancef behavior change but frequently cannot provide in-ensive counseling themselves,32 welcome a practice-riendly solution that limits intrusion but easily con-ects patients with the help they need. Communityrograms, which often struggle to attract clients viaxpensive media campaigns, welcome referrals fromhemedical community and the additional imprimaturf the smoker’s physician.The present trial has several limitations. First, as inost prior studies, counseling was measured rather
han cessation, but the close linkage between the two isxtensively documented.3 Second, like previous stud-es, patient report of counseling was relied on ratherhan direct observation (e.g., audiotaping), the lattereing too intrusive and expensive for the currenttudy. Third, a Hawthorne effect was possible if clini-ians knew that research assistants were onsite (lessikely given the unannounced visits). Fourth, effectsere measured for 9 months; therefore, sustainabilityver longer periods cannot be predicted. Fifth, mea-urement was made of patients’ reports of being re-erred rather than contacts with the quitline or receiptf counseling. Sixth, patients’ reports of being referredid not discriminate between referral to the study quit-ine and referral to the state quitline, which becamevailable during the study. Seventh, intervention fıdel-ty might have improved with longer training sessionsours lasted 1 hour) or if more clinicians participated.inally, as QuitLink was a multicomponent interven-ion, the current study cannot dissect the contributionf individual components.Themodel presented here bears signifıcance because it
ould improve the intensity of counseling providedmoreidely to primary care patients, not only for tobacco useut for other important risk factors (e.g., obesity).hether the current fındings are generalizable will re-uire replication in other settings and the measurementf effects on not only counseling but smoking prevalence.n addition, some state-sponsored quitlines face chal-enges in accommodating referral volume, because ofnadequate funding,14,33making it vital for states to fınd aay to share costs with appropriate private payers. Theurrent fındings add to a growing literature that empha-izes the need for collaboration between clinicians andommunity partners to improve the quality of preventive
nd chronic illness care. Investing in the infrastructurepril 2010
or such collaboration may yield important public healthnd economic benefıts.
his study was funded through a grant from thegency for Healthcare Research and Quality (GrantR21HS014854-02). The authors thank the Virginia Am-ulatory Care Outcomes Research Network; the researchssistants who administered the exit surveys (Melissaohnson Becker, Deidre Henley, Ann Luck, Carolynitchell); and the clinicians, staff, managers and patientsf the participating practices: Ashland Medical Center,shland; Aylett Medical Center, Aylett; Bowles, Bowlesnd Short Family Physicians, Sandy Hook; Cold Harboramily Practice, Mechanicsville; Drs. Titus, Hendrix,urner, Pahle and Christensen, Richmond; Green Medi-al Center, Richmond; Huguenot Primary Care, Mid-othian; Laburnum Medical Center, Richmond; Memo-ial Medical Center, Mechanicsville; Midlothian Familyractice, Inc.—Powhatan, Powhatan; Midlothian Familyractice, Inc.—Watercove, Midlothian; Midlothian Pri-ary Care, Ltd., Midlothian; Powhatan Family Physi-ians, Powhatan; Richmond Family Practice, Richmond;idewater Physicians Multispeciality Group—Westoint, West Point; Village Green Family Medicine, Mid-othian. The authors also thank Amy Burgett, RN, forssistance with survey data collection and Paul Mazma-ian, PhD, for assistance conducting interviews.TM owns stock in Free & Clear, a quitline servicerovider.No other fınancial disclosures were reported by the
uthors of this paper.
eferences1. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual
causes of death in the U.S., 2000. J Am Med Assoc 2004;291(10):1238–45.
2. USDHHS. The health consequences of smoking: a report ofthe Surgeon General. Atlanta: USDHHS, CDC, National Cen-ter for Chronic Disease Prevention and Health PromotionOffıce on Smoking and Health, 2004.
3. Fiore MC, Jean CR, Baker TB, et al. Treating tobacco use anddependence: 2008 update. Rockville MD: USDHHS. PublicHealth Service, 2008.
4. Duncan CL, Cummings SR, Hudes ES, Zahnd E, Coates TJ.Quitting smoking: reasons for quitting and predictors of ces-sation among medical patients. J Gen Intern Med 1992;7(4):398–404.
5. Ossip-Klein DJ, McIntosh S, Utman C, Burton K, Spada J,Guido J. Smokers ages 50�: who gets physician advice to quit?Prev Med 2000;31(4):364–9.
6. Vogt F, Hall S, Marteau TM. General practitioners’ and familyphysicians’ negative beliefs and attitudes towards discussingsmoking cessation with patients: a systematic review. Addic-
tion 2005;100(10):1423–31.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
A
S
Sf
374 Rothemich et al / Am J Prev Med 2010;38(4):367–374
7. Hu S, McAlister AL, Meshack AF, Margolis JA. Physicians’views and practice of smoking cessation. Texas Med 2003;99(11):57–63.
8. Bernstein AB, Hing E, Moss AJ, Allen KF, Siller AB, Tiger RB.Health care in America: trends in utilization. Hyattsville MD:National Center for Health Statistics, 2003.
9. Rothemich SF, Woolf SH, Johnson RE, et al. Effect on cessa-tion counseling of documenting smoking status as a routinevital sign: an ACORN study. Ann FamMed 2008;6(1):60–8.
0. RussellMAH,WilsonC, TaylorC, BakerCD. Effect of general-practitioners advice against smoking. Br Med J 1979;2(6184):231–5.
1. Schroeder SA. What to do with a patient who smokes. JAMA2005;294(4):482–7.
2. Orleans CT, Woolf SH, Rothemich SF, Marks JS, Isham GJ.The top priority: building a better system for tobacco-cessationcounseling. Am J Prev Med 2006;31(1):103–6.
3. Stead LF, Perera R, Lancaster T. Telephone counselling forsmoking cessation. Cochrane Database Syst Rev 2006;3:CD002850.
4. McAfee TA. Quitlines a tool for research and dissemination ofevidence-based cessation practices. Am J Prev Med 2007;33(6S):S357–67.
5. Cummins SE, Bailey L, Campbell S, Koon-Kirby C, Zhu SH.Tobacco cessation quitlines in North America: a descriptivestudy. Tob Control 2007;16(1S):i9–15.
6. Bentz CJ, Bayley KB, Bonin KE, Fleming L, Hollis JF, McAfeeT. The feasibility of connecting physician offıces to a state-leveltobacco quit line. Am J Prev Med 2006;30(1):31–7.
7. SwanGE,McAfee T, Curry SJ, et al. Effectiveness of bupropionsustained release for smoking cessation in a healthcaresetting—a randomized trial. Arch Intern Med 2003;163(19):2337–44.
8. WadlandWC,Holtrop JS,Weismantel D, Pathak PK, Fadel H,Powell J. Practice-based referrals to a tobacco cessation quitline: assessing the impact of comparative feedback vs generalreminders. Ann FamMed 2007;5(2):135–42.
9. An LC, Bluhm JH, Foldes SS, et al. A randomized trial of apay-for-performance program targeting clinician referral to astate tobacco quitline. Arch Int Med 2008;168(18):1993–9.
0. Borland R, Balmford J, Bishop N, et al. In-practice manage-ment versus quitline referral for enhancing smoking cessationin general practice: a cluster randomized trial. Fam Pract2008;25(5):382–9.
1. Bentz CJ, Bayley KB, Bonin KE, et al. Provider feedback toimprove 5A’s tobacco cessation in primary care: a cluster ran-
domized clinical trial. Nicotine Tob Res 2007 Mar;9(3):341–9. 02. Linder JA,RigottiNA,SchneiderLI,Kelley JH,BrawarskyP,HaasJS. An electronic health record-based intervention to improvetobacco treatment in primary care: a cluster-randomized con-trolled trial. Arch InternMed 2009;169(8):781–7.
3. Hing E, Burt CW. Offıce-based medical practices: methodsand estimates from the National Ambulatory Medical CareSurvey. Adv Data 2007;(383):1–15.
4. Burt CW, Sisk JE. Which physicians and practices are usingelectronic medical records? Health Aff (Millwood) 2005;24(5):1334–43.
5. Rabius V, Pike KJ, Hunter J, Wiatrek D, McAlister AL. Effectsof frequency and duration in telephone counseling for smok-ing cessation. Tob Control 2007;16(1S):i71–4.
6. CDC. Best practices for comprehensive tobacco control pro-grams, 2007. 2nd ed. U.S.: Atlanta GA: USDHHS, CDC, Na-tional Center for Chronic Disease Prevention and Health Pro-motion, Offıce on Smoking and Health, 2007.
7. NIH State-of-the-Science Panel. NIH State-of-the-Scienceconference statement: tobacco use: prevention, cessation, andcontrol. Ann Intern Med 2006;145(11):839–44.
8. Bonnie RJ, Stratton K, Wallace RB. Ending the tobacco prob-lem: a blueprint for the nation. 2008;18(6):69–12.
9. Robert Wood Johnson Foundation. Innovations in buildingconsumer demand for tobacco-cessation products and ser-vices. National conference,May 3–4, 2007. PrincetonNJ: Rob-ert Wood Johnson Foundation, 2007.
0. National Business Group on Health. Reducing the burden ofsmoking on employee health and productivity. WashingtonDC: Center for Prevention and Health Services, 2006. Reportnr Vol. I, No. 5.
1. Thorndike AN, Regan S, Rigotti NA. The treatment of smok-ing by U.S. physicians during ambulatory visits: 1994–2003.Am J Public Health 2007;97(10):1878–83.
2. Yarnall KSH, Pollak KI, Ostbye T, Krause KM, Michener JL.Primary care: is there enough time for prevention?Am JPublicHealth 2003;93(4):635–41.
3. CDC. State-specifıc prevalence and trends in adult cigarettesmoking—U.S., 1998–2007. JAMA 2009;302(3):250–2.
ppendix
upplementary data
upplementary data associated with this article can beound, in the online version, at doi:10.1016/j.amepre.2010.
1.008.www.ajpm-online.net
Related Documents











