Promises and perils of group clinics for young adults living with diabetes: a realist review Journal: Diabetes Care Manuscript ID Draft Manuscript Type: Systematic Review Date Submitted by the Author: n/a Complete List of Authors: Papoutsi, Chrysanthi; University of Oxford, Nuffield Department of Primary Care Health Sciences Colligan, Grainne; Queen Mary University of London, Blizard Institute, Barts and The London School of Medicine and Dentistry Hagell, Ann; Association for Young People's Health Hargreaves, Dougal; University College London, UCL Great Ormond St. Institute of Child Health Marshall, Martin; Department of Primary Care and Population Health Vijayaraghavan, Shanti; Barts Health NHS Trust Greenhalgh, Trish; University of Oxford, Nuffield Department of Primary Care Health Sciences Finer, Sarah; Queen Mary University of London, Blizard Institute, Barts and The London School of Medicine and Dentistry; Barts Health NHS Trust CONFIDENTIAL-For Peer Review Only Diabetes Care brought to you by CORE View metadata, citation and similar papers at core.ac.uk provided by UCL Discovery

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Promises and perils of group clinics for young adults living with diabetes: a realist review
Journal: Diabetes Care
Manuscript ID Draft
Manuscript Type: Systematic Review
Date Submitted by the Author: n/a
Complete List of Authors: Papoutsi, Chrysanthi; University of Oxford, Nuffield Department of Primary Care Health Sciences Colligan, Grainne; Queen Mary University of London, Blizard Institute, Barts and The London School of Medicine and Dentistry Hagell, Ann; Association for Young People's Health Hargreaves, Dougal; University College London, UCL Great Ormond St. Institute of Child Health Marshall, Martin; Department of Primary Care and Population Health Vijayaraghavan, Shanti; Barts Health NHS Trust Greenhalgh, Trish; University of Oxford, Nuffield Department of Primary Care Health Sciences Finer, Sarah; Queen Mary University of London, Blizard Institute, Barts and The London School of Medicine and Dentistry; Barts Health NHS Trust
CONFIDENTIAL-For Peer Review Only
Diabetes Care
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by UCL Discovery
1
Promises and perils of group clinics for young adults living with diabetes: a realist review Chrysanthi Papoutsi PhD,1 Grainne Colligan MSc,2 Ann Hagell PhD,3 Dougal Hargreaves,4 Martin Marshall MD,5 Shanti Vijayaraghavan FRCP,6 Trisha Greenhalgh FMedSci ,1 Sarah Finer PhD2,6 1 Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, England, UK 2 Centre for Primary Care and Public Health, Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, England, UK 3 Association for Young People’s Health, London, England, UK 4 UCL Great Ormond St. Institute of Child Health, University College London, London, England, UK
5 Department of Primary Care and Population Health, University College London, London, England, UK 6 Barts Health NHS Trust, London, England, UK
Corresponding author:
Dr Sarah Finer, Centre for Primary Care and Public Health, Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, United Kingdom, Yvonne Carter Building, 58 Turner Street, London, E1 2AB, +44 (0)20 7882 7326, [email protected]
Page 1 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
2
Abstract
Background: Group clinics are becoming popular as a new care model. This evidence
synthesis, using realist review methodology, examined the potential role of group clinics in
meeting the complex needs of young adults living with diabetes.
Research Design and Methods: We followed a theory-driven, realist approach to evidence
synthesis. Three reviewers screened the articles resulting from a systematic literature search
across 10 databases. To draw on lessons from a broader literature, we also included studies
on wider group-based processes such as structured diabetes education. Included papers were
coded and iteratively analysed using a realist logic. By following the established RAMESES
quality standards, we developed theoretically-informed explanations of how and why group
clinics could work for young people with diabetes.
Results: 131 papers met our inclusion criteria. Models of group-based care varied
significantly and incorporated different degrees of clinical and educational input. Providing a
safe space for interaction in a developmentally appropriate way was deemed important for
sustained engagement of young adults with their care. Group clinics were valued by patients
when they brokered connections and facilitated useful exchange of experiences. However,
engagement was not always sustained if individual needs were not fulfilled in a timely and
time-efficient manner. Substantial invisible work was required to overcome implementation
challenges.
Conclusions: In contrast to widespread rhetoric proposing group clinics as a solution to
increasing demand and financial pressures in health systems, this review suggests that
successful implementation requires careful work to address complex patient needs and
sustain engagement.
Page 2 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
3
Introduction
The global rise in diabetes prevalence is expected to have serious consequences across
healthcare systems. It is estimated that by 2045, healthcare expenditure on diabetes will reach
USD 776 billion (1). In the UK the cost of diabetes care is expected to account for 17% of the
total health resource expenditure in 2035⁄2036 (2). A large proportion of these costs relates to
managing diabetes complications, such as retinopathy, neuropathy, diabetic foot and
cardiovascular disease, which lead to reduced quality of life and premature mortality (1).
Alternative approaches to care provision are necessary to stem what has been described as a
‘titanic struggle’ against the burgeoning personal and systemic impact of diabetes (3).
Group clinics (also known as shared medical appointments) have been proposed as a way to
address rising healthcare costs and diminishing resources, with the potential to improve
efficiency and to provide opportunities for peer support and social learning, compared to
usual care focused on one-to-one interactions between patients and healthcare professionals
(4, 5). Numerous studies discuss group clinics delivered in a variety of formats and targeted
at different patient populations (6-8).
In diabetes, experimental studies of group-based care for adults have shown improvements in
glycaemic control, problem-solving ability and quality of life and reduced time commitment
for clinicians, compared to standard one-to-one consultations (9, 10). Similarly, systematic
reviews of group care for diabetes highlight clinical benefits (lower HbA1c, blood pressure)
and improvement in patient-reported outcomes (7, 8). Story-sharing interventions for
minority ethnic groups have also resulted in higher attendance and patient enablement,
compared to structured self-management education (11, 12).
Page 3 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

4
With diabetes prevalence (both type 1 and 2) rising in young adults (13) there is a need to
learn from alternative models of care and to re-design service delivery to better support this
patient group. In England, despite overall improvements in diabetes care processes for young
people under 25, emergency hospital admissions increased for the 20-24 age group between
2005/6 to 2015/16 (14). This increase is explained by a range of poor health outcomes across
a variety of clinical and psychosocial parameters for this patient group, including widening
inequalities (14-16). There are recognised barriers to regular clinic attendance and
engagement for young adults, such as diabetes-related psychological distress, lack of care
continuity and poor satisfaction with the health service, lack of developmentally appropriate
consultations and fear of complications (17, 18). In addition to the direct impact of unmet
healthcare need in this age group, evidence suggests that patterns of poor engagement with
health services in adolescence and young adulthood often persist into adult life (19). Novel
approaches to care delivery are urgently needed to address the specific health and self-care
needs of young adults in tune with their developmental stage and life circumstances, and to
improve their outcomes and experiences.
In this paper we use a realist approach to synthesise evidence on group clinics for young
adults with diabetes, rather than older age groups. A realist review allows us to extend
beyond de-contextualised lists of barriers and facilitators to understand ‘how, why, for whom
and in what circumstances’ group clinics might work for this age group (20). This approach
follows the tradition of narrative reviews that aim to increase understanding, rather than
summarise data (21). We aim to build on previous evidence of clinical benefit to understand
how group clinics need to be implemented in practice so these benefits can be realised for
different types of patients and in different circumstances. The realist review underpins a
theoretical and participatory approach to the co-design and evaluation of group clinics as part
Page 4 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
5
of the Together study, a wider programme of work testing feasibility and implementation of
group clinics for young adults living with diabetes (22).
Aims
This review aims to explore how, why, for whom and in what circumstances group clinics
may work for young adults living with diabetes (type 1 and 2).
Review questions
1. What are the ‘mechanisms’ by which group clinics (could) meet the complex health and
social needs of young people living with diabetes?
2. What are the important ‘contexts’ which (could) determine whether the different
mechanisms produce intended outcomes?
3. In what circumstances are group clinics likely to provide a better way of supporting
diabetes self-management than traditional care?
Methods
Our methods are based on previous realist reviews and on the RAMESES standards (20, 23).
Realist reviews typically start with an initial set of assumptions, i.e. a programme theory,
about how an intervention is assumed to be working. These assumptions are developed
further by drawing on secondary qualitative and quantitative data (theory building) and
become refined as the analysis of this data progresses (theory refinement). A basic principle
for scaffolding the analysis of the literature is that the resources offered by programmes
interact with the underlying reasoning of individuals (mechanisms). This interaction leads to
Page 5 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
6
certain outcomes depending on pre-existing contextual or structural factors (also see Glossary
in Appendix 1).
Data sources and searches
We performed literature searches in Embase (OvidSP), MEDLINE (OvidSP), PsycINFO
(OvidSP), Web of Science Core Collection, ASSIA (Proquest), Cinahl (EBSCOHost)
Cochrane Database of Systematic Reviews (Cochrane Library), Cochrane Central Register of
Controlled Trials (Cochrane Library) and Dissertations & Theses Global (Proquest). An
information specialist devised and tested the search strategy based on previous systematic
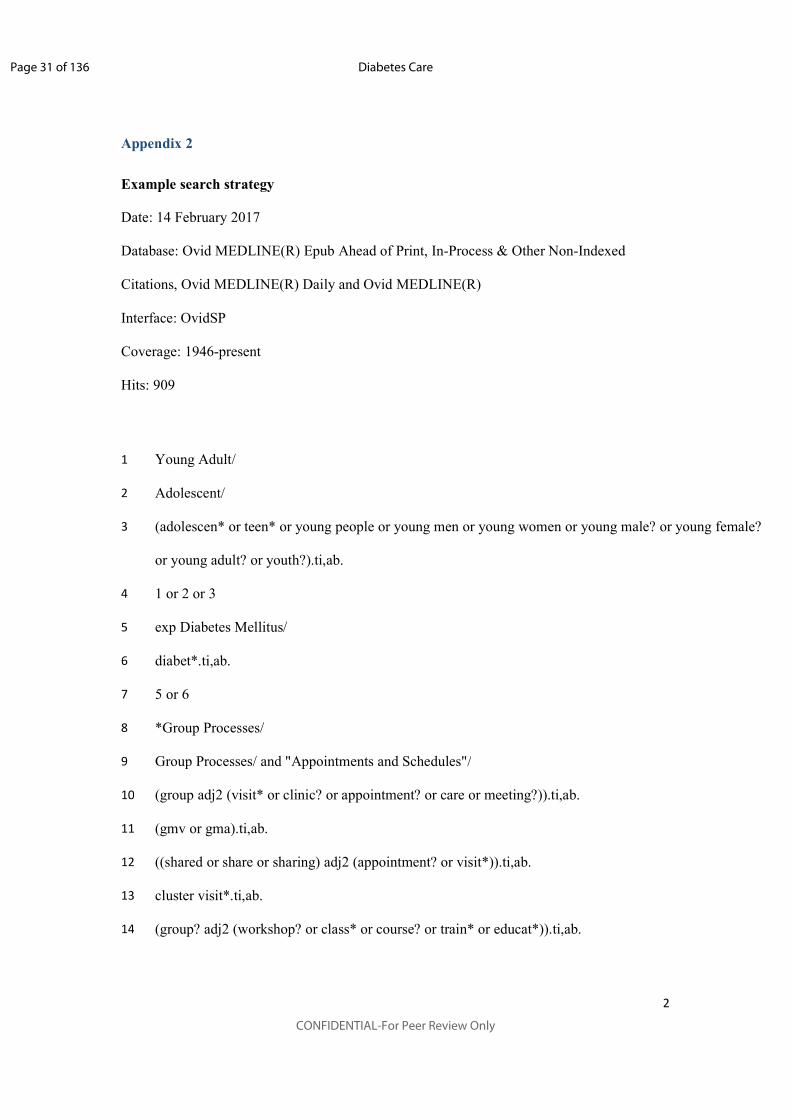
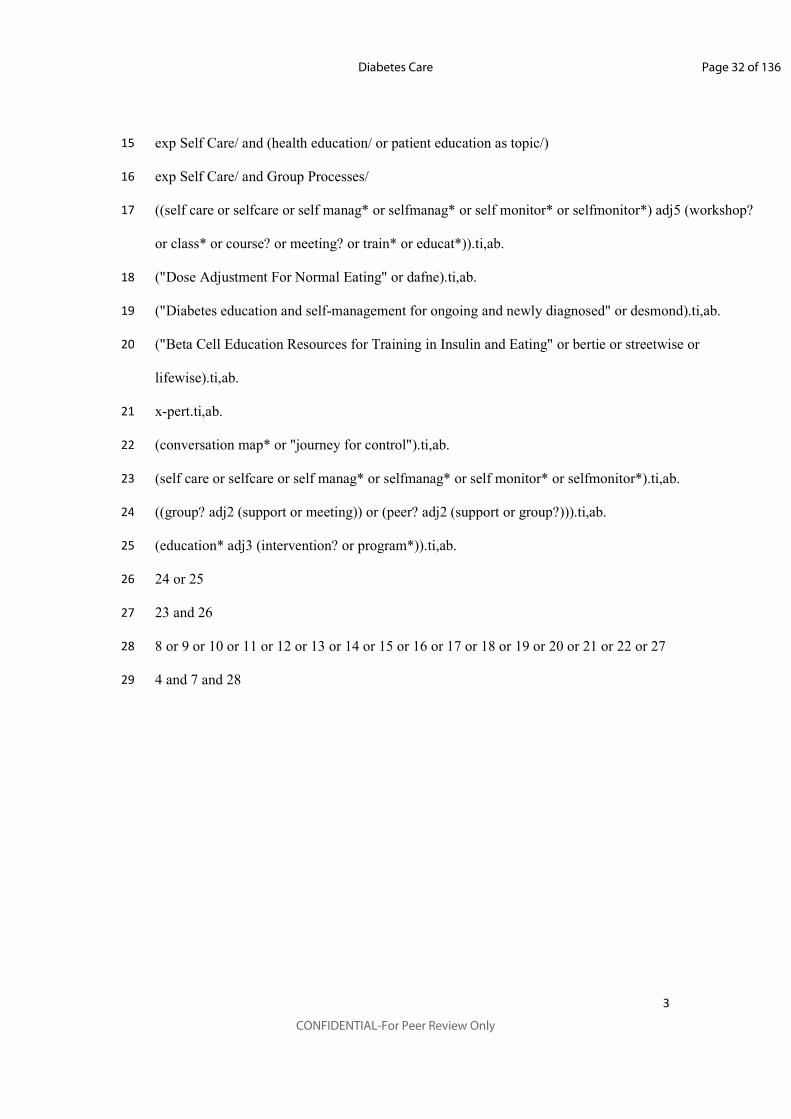
reviews (see Appendix 2 for an example of the search strategy) (24).
Study selection
Following two rounds of screening (title/abstract and full-text) by one reviewer (CP), articles
meeting inclusion criteria were classified as core (i.e. on group clinics primarily focusing on
16-25 year olds), highly relevant (e.g. on group education for 16-25 year olds or similar age
groups) and less relevant (e.g. group visits or education in very different age groups) – based
on their potential to contribute to programme theory. A 10% random sub-sample of papers
was reviewed by two additional reviewers with different expertise (GC, AH) to ensure
consistency.
As is standard in realist reviews, inclusion and exclusion criteria were refined as screening
progressed (20, 25). Studies published in English from 1999 were included if they focused on
Page 6 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
7
group-based care (in any setting) for young people (aged 16-25) with diabetes, other group-
based processes such as group education, and qualitative experiences of young patients living
with diabetes and transition to adult services. Studies were excluded when they described
one-to-one interventions or educational programmes without a component of group
interaction, when they referred to patient groups radically different to young adults (e.g.
much younger children or older adults), when they only discussed in-patient or home-based
education, when they had a very specific focus (e.g. exercise programmes or family
planning), or when they described low-resourced healthcare systems.
Data extraction and quality assessment
One reviewer (CP) read all articles included in full-text screening and conceptually coded
data relevant for programme theory development using the qualitative data management
software NVivo 11 (QSR International) until theoretical saturation was reached. A 10%
random sub-sample of coded articles was reviewed by a second reviewer (GC) for
consistency and disagreements were solved by discussion. Descriptive study characteristics
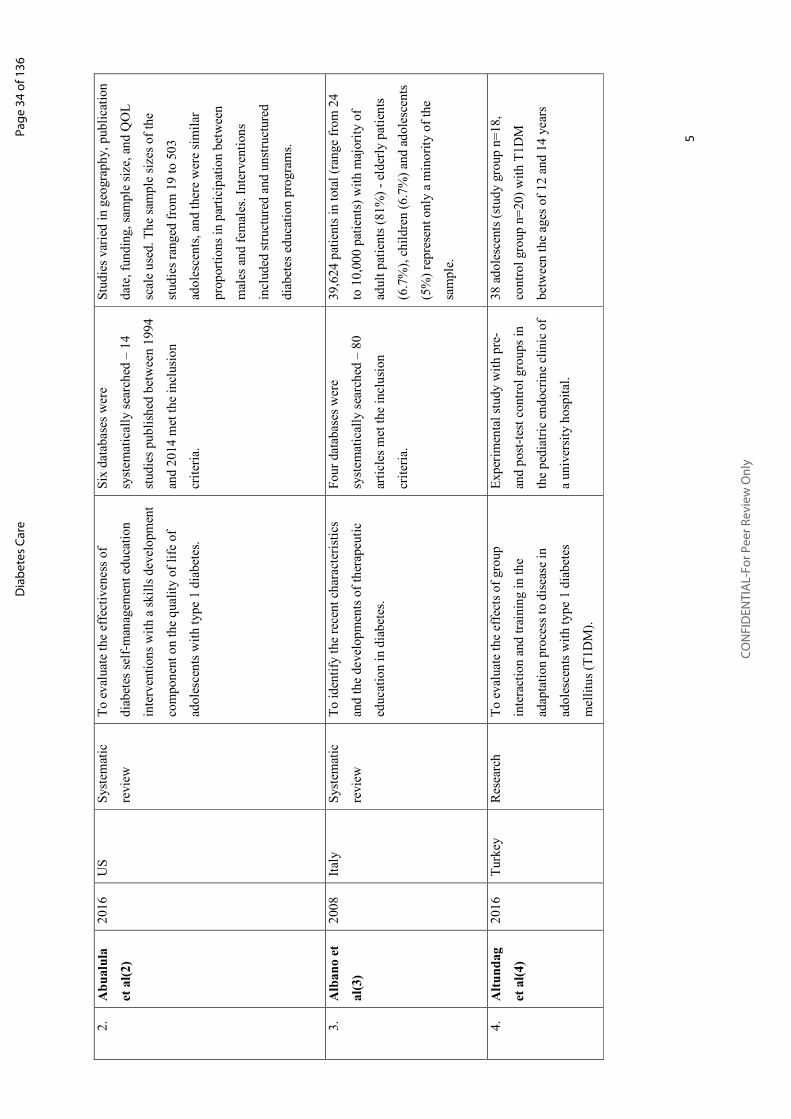
are presented in Appendix 3. At the point of inclusion based on relevance, the trustworthiness
and rigour of each study was assessed as appropriate for different study designs (20).
Data synthesis and analysis
Following conceptual coding, we applied a realist logic of analysis which meant iteratively
identifying sections of coded text and interpreting if they functioned as Contexts (C),
Mechanisms (M), Outcomes (O), or if they supported the configurations between them
(Context-Mechanism-Outcome Configurations or CMOCs). In doing this, we sought to
interpret and explain young adults’ reasoning and responses (i.e. mechanisms in a realist
Page 7 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
8
logic of analysis) to ‘resources’ becoming available through group clinics and to identify the
specific contexts where these mechanisms are more likely to be ‘triggered’. By moving
between data and programme theory, we were able to refine our explanations of why certain
patterns seemed to be occurring under specific contexts, related to group-based care. The
final programme theory consists of evidence-informed propositions, drawing on literature,
substantive theory and professional and patient expertise. Our synthesis was also informed by
substantive theory, mainly ecological theories of supported self-management and strong
structuration theory (26-28), critical perspectives on patient expertise and experiential
knowledge (29) and articulation work to denote the ‘hidden’, invisible adjustments and
alignments necessary to successfully carry out tasks in socio-cultural settings (30, 31).
Stakeholder input
Refinement of the programme theory was discussed repeatedly as part of a wider co-designed
research programme, with representation from people living with diabetes, health
professionals and wider stakeholders (e.g. policy makers).
Findings
Search results
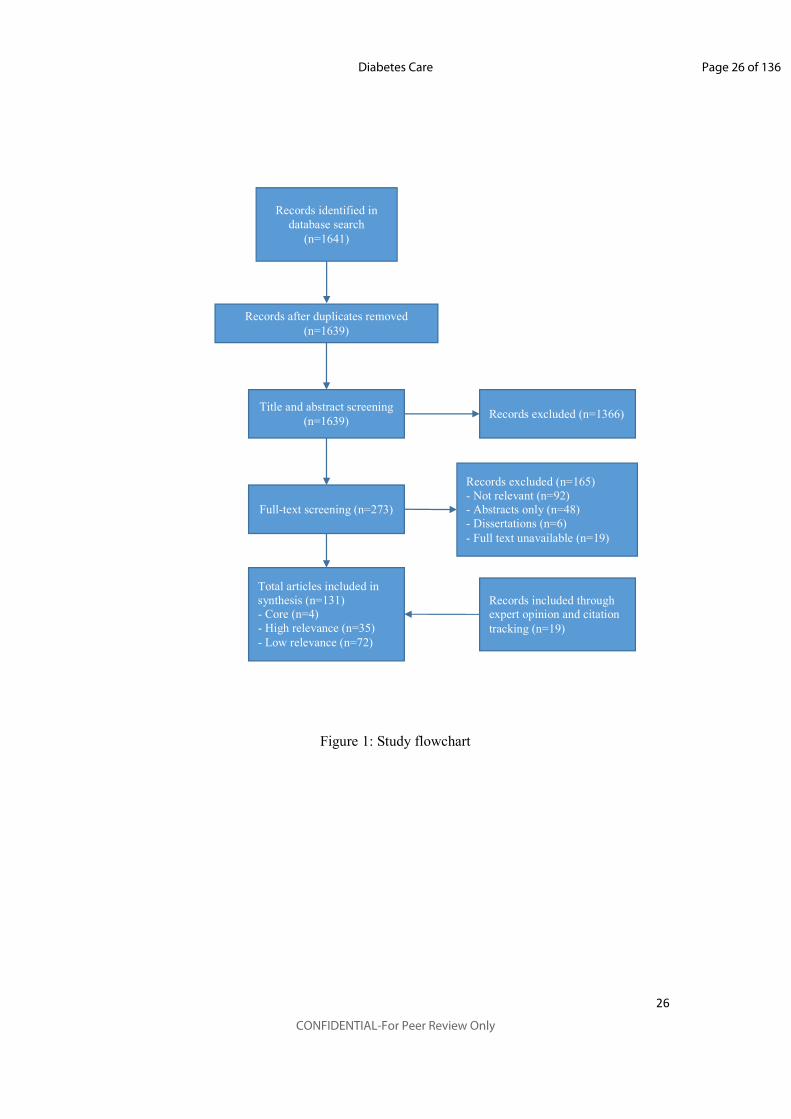
The database search identified 1641 potentially relevant records. Two articles were removed
as duplicate entries. Title and abstract screening excluded 1366 records that did not fulfil the
inclusion criteria. Subsequent full-text screening resulted in 112 references, which were
further categorised according to their potential to contribute to programme theory
development (4 core papers, 35 of high relevance, 73 of low relevance – as explained in the
methods section). An additional 19 articles were added following recommendation from
Page 8 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
9
experts, targeted searches (e.g. on peer support) and citation tracking. A total of 131 papers
were reviewed for programme theory building and refinement. The flowchart diagram for the
study is presented in Figure 1.
[Figure 1 here]
Of the 131 articles, 32 used quantitative and 29 used qualitative methods, 12 employed mixed
methods, and there were also 2 books, 45 reviews, 6 position papers and 5 papers describing
frameworks or models of group-based care interventions. Distinct literature on group clinics
for young adults with diabetes was sparse, but studies of group-based structured education
and group clinics in a wider age group offered additional sources of data, along with work on
young people’s experiences living with the condition and on transitional care. Group clinics
were described differently: as group clinics, shared medical appointments, group medical
visits, cluster visits, and drop-in groups. Some papers describe group care for young people
that involved a clinical component (32-35), but in most cases group interactions were only
discussed as part of educational programmes (36-39), or as a component of larger
multifaceted interventions (40). Intervention studies provided little detail on how group-based
care was set-up and delivered within existing services.
Group clinics for young adults with diabetes – how, why, for whom and in what
circumstances?
The following sections present the synthesis of the literature across a number of areas, each
underpinned by one or more CMOCs explaining how and why group clinics may (or may
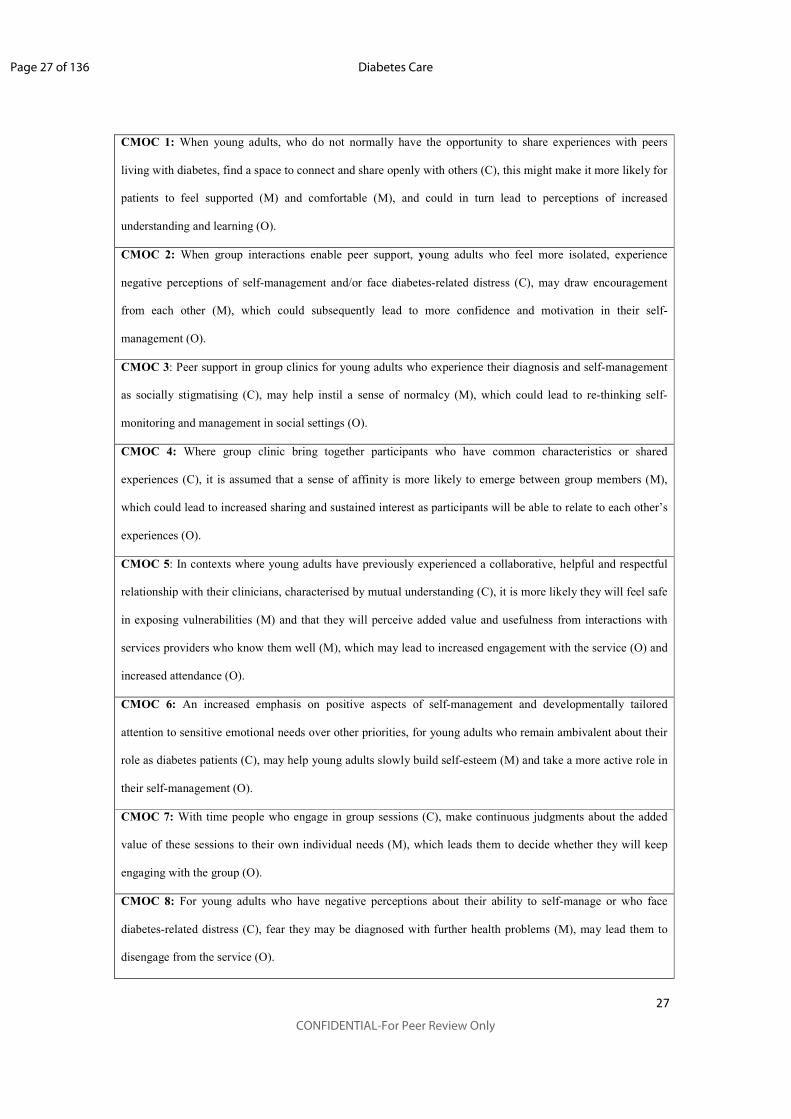
not) work for young people living with diabetes. The 8 CMOCs are described in Table 1 with
illustrative quotes supporting our interpretations. Selected supporting references can be found
in Appendix 1.
Page 9 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
10
[Table 1 here]
Sharing experiences
As a model of care that intends to bring patients together to engage in meaningful sharing and
interaction, group clinics play a symbolic role in recognising the significance of patient
expertise and supportive peer relationships. This shift towards care as a site for collective
action is generally well received by younger patients, who report high levels of satisfaction
(34, 35, 40). Sharing the experience of diabetes self-management between peers leads to
increased understanding and learning (CMOC1) (32, 34-36, 41, 42). Real personal
experiences help contextualise abstract medical advice which can lead to better self-
management (32, 42).
Young adults who feel isolated in or negative about their self-management, and with diabetes
distress may draw encouragement from peer support in group interactions, subsequently
leading to more confidence and motivation (CMOC2) (32, 36, 42, 43). This is often assumed
to result from role-modelling by patients who present themselves as more successful (43).
The literature commonly highlights empowerment as a way to explain how group clinics and
other peer interactions contribute to behaviour change (44). However, emphasis on individual
empowerment of behaviour change and self-management may neglect the social, professional
and cultural contexts in which patients are embedded.
Self-management as a social practice
Negotiating established norms in social settings with the need to effectively organise self-
management may require additional support and guidance. Group clinics are assumed to
provide a space for experimentation and reassurance – when a behaviour is normalised in the
group, it might become easier to perform it in public (45, 46). Group interactions also allow
Page 10 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
11
clinicians to acquire a sense of how young adults interact with their peers in the context of
self-management and to identify opportunities for supporting patients’ emotional and
motivational needs (43, 47). Especially for those experiencing their diagnosis and self-
management practices as stigmatising, peer support in group clinics may help instil a sense of
normalcy, which could lead to re-thinking self-monitoring and management in social settings
(CMOC3) (24, 25, 36, 41, 45, 46, 48, 49).
What counts as shared experience?
For group clinics to work, the literature suggests a need to instil a sense of connection and
affiliation between participants, and that this is most likely to develop when group
participants are invited on the basis of common characteristics or shared experiences so that
patients can relate to each other (CMOC4) (32, 50, 51). This is reinforced in a previous realist
review which suggests there is an ‘implied need for homogeneity within the group in order to
harness shared norms and values’ (25). What homogeneity means for young adults living
with diabetes is less clear. ‘Homophily’ – i.e. the degree to which people perceive others to
be similar to them – may be a more suitable concept to underpin an analysis of group
influence, as described in the diffusion of innvations theory (52).
Developmental stage, time since diagnosis, life stage (e.g. moving to university) or treatment
options (e.g. insulin pump therapy) are assumed to be important in allowing young adults to
interact more easily (51). There is, however, little data to show which of these characteristics
may actually make a difference in practice. Group homogeneity or homophily does not just
relate to creating a sense of affinity based on pre-existing characteristics, but also to ensuring
that topics of interest to all participants are discussed in the group (32).
Diffusion of innovations theory also highlights that ideas may flow less readily within a
Page 11 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
12
social system when there are too many similarities between people, therefore ‘heterophily’
also becomes important (52). In practice it may be difficult to match participants based on
background so building a sense of affinity will depend on how discussions are facilitated to
foreground commonalities and build on differences (6). Knowing patients well enough to be
able to understand how they might fit (or not) into a specific (albeit diverse) group and
fostering interactions in ways that not only focus on shared experiences but also help
reconcile contradictions may help young people feel affinity with others (53).
The role of relationships
Bringing people together in a way that allows connection and affinity to develop requires
significant skills and in-depth relational knowledge of patients and their circumstances. The
literature suggests that successful group clinics emerge from good pre-existing relationships
between patients and clinicians (53-55). Young adults feel they can trust their clinician, who
knows them well enough to suggest group clinics as a way to benefit their own individual
circumstances and to bring them together with other people who can share valuable expertise.
This relational introduction to group clinics could also counteract potential anxieties for
patients who may fear that group clinics are purely used a means to cut costs compared to
one-to-one care.
When young adults have a good relationship with their clinicians and perceive service
provision to be collaborative, helpful, respectful and characterised by mutual understanding,
it is more likely they will feel safe in exposing vulnerabilities and that they will perceive
added value and usefulness from their interactions with services providers. In turn, this may
may lead to increased engagement with the service and increased attendance (CMOC5) (53-
55).
Page 12 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
13
Provision of developmentally appropriate care
The literature further acknowledges that young adults are going through a life stage where
they are experimenting with their identities in-between childhood, adolescence and
adulthood, testing boundaries and keeping their options open (53, 55). Although necessary
for their development, this experimentation often ‘become[s] labelled as problematic [and]
problem saturated stereotypes of young people are allowed to dominate’ (48). Young adults
living with diabetes may have specific vulnerabilities in addition to their diabetes, including
experiencing eating disorders and mental health difficulties, a lack of supportive
relationships, and perceptions of low self-efficacy and control (55). In a healthcare system
that values consistency, attendance and adherence, adapting services for the needs of young
adults needs to be an ongoing and flexible process, and should recognise the physical,
cognitive, symbolic and socio-emotional work involved in self-management (49).
Service providers are commonly advised to deliver young adult care in an age- and
developmentally-appropriate manner, using a confidential and non-judgmental way manner
(56); ‘empathic, non-confrontational’ interventions and careful use of language (55); and
emphasising emotional and motivational needs (43, 47). Studies also recognise that young
adults may prioritise short-term gain over long-term implications and may respond more
positively when care extends beyond biomedical aspects of living with diabetes to include
young adults’ personal and professional priorities (53, 54, 56). In this way, young adults may
see added value in attending, which could in turn lead to increased engagement (48, 49, 53).
Group clinics have the potential to support this developmentally-appropriate care, creating a
safe space for discovering what it means to be living with diabetes, through one’s own
experiences and through the experiences and interpretations of others. Emphasis on positive
aspects of self-management, such as how it can help young adults achieve dietary freedom or
better manage their exercise regime, is also deemed important in building confidence, self-
Page 13 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

14
esteem and optimism (CMOC6) (57). Participation, however, needs to be treated as a
dynamic process and priorities need to be continuously reassessed and negotiated to
maximise the potential for continued engagement.
Engagement and sustainability
Existing literature indicates wide variability in group attendance, with interest dissipating as
patient needs and circumstances change (25, 32, 35, 45, 50, 58). Despite their benefits, group
clinics may not be sustainable if patients feel their individual needs are not fulfilled to the
extent needed and in a timely manner (58). According to the literature, it is often individual
attention as part of group-based care that leads to improvement and satisfaction. With time,
people who engage in group sessions, make continuous judgments about the added value of
these sessions to their own individual needs, which leads them to decide whether they will
keep engaging with the group (CMOC7) (25, 32, 35, 45, 58).
Therefore, group clinics need to ensure expectations are managed and individual needs are
adequately attended to, rather than focusing on a collective approach alone. This generates
questions about the potential for group clinics to replace individual appointments (25, 35, 45,
58). Although previous studies with adult diabetes groups report positive effects on clinical
and patient-reported outcomes, such improvements have not yet been identified in younger
groups (7, 8). Given the lack of long-term studies, it remains unclear whether engagement in
group clinics translates to improved glycaemic control or perceived quality of life for young
adults, especially for those transitioning to adult care (34, 45).
Other questions arise when considering group clinics for age groups <19 years; literature
suggests parents are active participants who attend the majority of group clinic appointments,
and whose presence increases discussion of significant diabetes-related topics (35). There are
Page 14 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
15
concerns, however, as to whether having parents in the group clinic may lead young patients
to take a more passive stance (33). Some interventions include separate parent-only groups to
allow ongoing parental involvement where needed, while still allowing space for young
adults to take ownership of their care and share openly with their peers (32, 48). A combined
approach may also help manage family relationships without detracting from the value of
group clinics as a peer-based model (48, 57).
Unintended consequences
Evidence on the potential of group clinics to support people to ask questions is contradicting:
some patients feel more comfortable contributing questions, while others are more reserved
in a group context (34, 35).Others have suggested peer support may negatively affect an
individual’s sense of self (48). Mismatch of expectations may lead young adults to feel they
cannot rely on their peers and may have negative consequences on group formation and
engagement.
Some studies suggest that young adults in most need (e.g. those with the highest HbA1c, low
self-esteem, or more signs of diabetes-related distress) are less likely to engage with diabetes
services, whether individual- or group-based (40, 54). For young adults who have negative
perceptions about their ability to self-manage or who face diabetes-related distress, fear they
may be diagnosed with complications or that they will be judged by fellow patients, may lead
to further disengagement (CMOC8) (40, 54).
Group clinics may also have other unintended consequences by normalising risky behaviours,
sharing negative experiences detrimental to diabetes care, or reacting adversely to advice
given by figures of authority. Managing these group dynamics is important to avoid negative
outcomes (59).
Page 15 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
16
Hidden implementation work and practical considerations
Running group-based care in healthcare services traditionally designed to deliver one-to-one
consultations is described as challenging. Established infrastructure and administrative
processes have to be adjusted to fit the new approach, while continuing to support
individualised care. This requires significant effort and introduces additional workload, which
some studies suggest balances out any time efficiencies gained through group-based care
(50). Despite best efforts to coordinate group clinics and ensure good group composition,
non-attendance, late cancellation and participation attrition are common and result in resource
waste (50).
Practical constraints to group-based clinics are widely reported, such as the lack of suitable
space to accommodate groups and need to use external facilities (42, 57). ‘Hidden’
operational work is necessary to ensure clinics are set up appropriately, with health
professionals briefed, content planned, and attendance confirmed, among other tasks (6).
‘Hidden’ clinical work is also required as clinicians will need to ‘triage’ for patients requiring
further individual attention in the context of the group interactions (25).
Delivery of group clinics require a wider skill set, different from that required when carrying
out individual clinical consultations. Groups need to be led by someone in a facilitator role
who can engage patients in discussion and manage group dynamics to allow experiences to
be shared, to ensure patient needs are met either as part of the clinic or individually; to
resolve any contradictions or disagreements with sensitivity; and to sustain a pleasant,
positive and safe learning environment (25, 36, 41, 42, 51). These skills expose additional
training needs that need to be fulfilled for staff to be able to deliver group clinics for young
adults (53, 55).
Page 16 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
17
Discussion
Summary of findings and comparison with previous literature
The 8 CMOCs described above synthesise a broad range of literature and allow us to explore
the mechanisms by which group clinics might meet the needs of young people living with
diabetes, the contexts in which this might work, and the circumstances in which this is likely
to add value over traditional care models. The following themes emerge when consolidating
and summarising the CMOCs:
1. Placing relationships at the core, without forgetting the individual
In line with other reviews on group-based care, we highlight the important role of therapeutic
relationships in the care of young adults with diabetes, not just between doctors and patients,
but also between peers (25). Whilst group clinics may seem to offer an opportunity to harness
these different therapeutic relationships, our review suggests that reality is more complex.
Peer support does not emerge automatically in group interactions, but occurs as a result of
carefully crafted interventions that take in account the need to draw on homophily and to
harness difference. In-depth knowledge of patients’ circumstances and good pre-existing
relationships with clinicians allow attention to socio-ecological aspects of coping with
diabetes, rather than focusing solely on self-management as an individual behaviour (28).
This means that emphasis on role modelling may be beneficial but can be sustained only
when the social aspects of self-management are not neglected (49).
Despite significant policy interest in group clinics as a replacement for one-to-one
consultations, our review reinforces that individual attention should be equally valued and
prioritised. Group clinics seem to work only on the basis of addressing individual patient
needs – either by bringing together groups homogeneous enough to be able to discuss issues
Page 17 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
18
of common interest or by addressing individual needs outside the group clinics. There is little
evidence to suggest that replacing individualised care with group clinics would lead to
positive experiences for young adults. Booth et al suggest that group clinics may be more
successful for specific period of times to fulfil clearly identified needs, rather than as a long-
term solution for patient care (25). More work is needed in this area to investigate the right
balance between one-to-one and group-based care specifically for young adults with diabetes.
2. Negotiating patient knowledge and identity
Beyond therapeutic relationships, group clinics become sites for collectively framing,
normalising or contesting the different types of biomedical and patient knowledge underlying
diabetes management (29, 60). Patients bring their own practical knowledge about how to
deal with aspects of their condition and debate their techniques with others who have devised
different ways of doing things and with clinicians who might be trying to reconcile
experiential aspects with core biomedical concepts. This process of ‘knowing together’
evolves as people compare their experiences and translate clinical knowledge, for example by
discussing the devices they use to support diabetes self-management (29). The group clinic
makes it easier to bring to focus competing priorities and to articulate ways for situating these
in the context of living with diabetes. Other studies have discussed this process by framing it
as ‘vicarious learning’ or ‘learning by doing’, but they have not adequately considered the
influence of the group on negotiating knowledge and patient identities (24, 25).
Many young adults will have recently arrived at a stage of independence in their diabetes
self-management. Instead of just sharing practical knowledge about the condition, group
clinics also act as a platform to collectively develop values and norms about what it means to
Page 18 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
19
attend adult diabetes care and being an adult diabetes patient. In the existing literature there is
more emphasis on group clinics modelling a notion of patients as empowered, in that they can
responsibly and proactively negotiate their care (and fulfil their individual needs) in the
context of a group interaction. This draws attention to specific dimensions of patient-hood
and may require careful management to ensure young adults are benefiting.
3. Hidden implementation work
Our review suggests that thinking about group clinics as the sum of multiple individual
consultations is misguided. Group clinics constitute a completely different way of organising
care and with this come different requirements for operational and administrative resources,
space for consultations, facilitation skills, documentation systems, as well as time investment
in getting to know patients and bringing them together in groups meaningfully. This includes
careful co-ordination between members of the multidisciplinary team and appropriate
individual management of patients who seem to require extra attention. Given the additional
work required, the role of group clinics in creating efficiencies in the health service requires
further research.
It is easy to underestimate the effort required in setting up and delivering good care through
group clinics, because it remains unarticulated and hidden. Temporal, material and integrative
aspects of articulation (31) are all present in research examining the feasibility of running
group clinics. However, few of these studies report on the interventions in enough depth to
allow full appreciation of the complexities involved in setting up and sustaining this new
model of care. There is need to better understand how wider cultural, professional and
material changes are required to establish group clinics as a mainstream model of care.
Page 19 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
20
Lessons learned
Group clinics have been studied across a range of conditions but have received less attention
in the context of diabetes care for young adults, despite the urgent need for better care models
to improve the poor health outcomes in this patient group. Drawing on a broad literature, this
review presents lessons learned towards tailoring group-based care interventions for the
specific needs and requirements of this age group.
Involvement in group clinics on the basis of good pre-existing relationships with health
professionals seems to be key in retaining young adults’ engagement with the service.
Carefully crafted therapeutic relationships between patients and health professionals are
based on flexibility, openness, non-judgmental language and understanding of developmental
goals and competing priorities. Group composition and facilitation relies on good knowledge
about patients – not just clinical information, but relational knowledge about their
personality, motivations and social context.
There are significant challenges to implementation and substantive invisible work is required
to establish successful group clinics for young adults. Resource implications, impact on pre-
existing processes, additional skills and infrastructure requirements would need to be
evaluated and costed. Iterative co-design of group-based care may help towards a clear value
statement for patients that would enhance the perceived usefulness of the model and would
lead to sustained engagement and sustainability.
Strengths and limitations
This review fulfils a clear and specific need in generating actionable evidence on how and
why group clinics may work for young adults living with diabetes. To do this we are drawing
our interpretations on a wider range of data than previous realist reviews, which looked
Page 20 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
21
across conditions or focused only on a small number of studies. Although this has
significantly expanded the evidence base feeding into this review, many of our interpretations
derive from literature on group-based education and would need to be examined further.
Under-reporting of the content and delivery of interventions in the published literature and
emphasis on clinical outcomes rather than psychosocial measures have also hindered a more
detailed analysis.
Further research
Better reporting of interventions and more long-term ethnographic studies would provide a
more detailed understanding of how and why group clinics work (or not) for young adults.
This realist review has already provided a foundation for the ongoing development and
evaluation of a new care model using group clinics for young adults with diabetes as part of a
larger programme of work undertaken in a multidisciplinary diabetes clinic in the UK.
Page 21 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
22
Acknowledgements
Author contributions: SF and DH conceptualised the study with input from MM, TG, AH,
SV and GC. CP led the design and conduct of the realist review, development of the
programme theory, and writing the manuscript. GC and AH acted as second reviewers, and
reviewed the manuscript. SF, TG, DH, MM and SV contributed to the interpretation of
findings and to writing the manuscript.
Statement of assistance: We would like to express our thanks to Nia Roberts, Geoff Wong
and Alexandra Christopher (University of Oxford) for methodological help. The paper has
greatly benefited from discussions with the steering group and participants in co-design
groups for the Together study.
Guarantor: SF is the guarantor for this study.
Funding: This work was funded by the UK National Institute for Health Research Health
Services and Delivery Research Programme (ref. 15/25/20). TG is part-funded by the
National Institute for Health Research Biomedical Research Centre, Oxford, UK (NIHR
BRC-1215-20008). CP is partly supported by an Academy of Medical Sciences Health of the
Public 2040 award, funded by the Wellcome Trust (HOP001\1049). The views and opinions
expressed therein are those of the authors and do not necessarily reflect those of the funders,
National Health Service or the Department of Health.
Ethics approval: The project has been approved by the Office for Research Ethics
Committees Northern Ireland (reference 17/NI/0019).
Conflict of interest statement: No competing interests to declare.
PROSPERO registration number: CRD42017058726
Page 22 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
23
References
1. International Diabetes Federation. Diabetes Atlas 2017 [Available from: http://www.diabetesatlas.org/. 2. Hex N, Bartlett C, Wright D, Taylor M, Varley D. Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabetic Medicine. 2012;29(7):855-62. 3. Anonymous. Editorial - Diabetes: mapping the titanic struggle ahead The Lancet Diabetes & Endocrinology. 2018;6(1):1. 4. Hayhoe B, Verma A, Kumar S. Shared medical appointments. BMJ. 2017;j4034. 5. Ramdas K, Darzi A. Adopting Innovations in Care Delivery-The Case of Shared Medical Appointments. The New England journal of medicine. 2017;376(12):1105-7. 6. Noffsinger EB. Running Group Visits in Your Practice. New York, NY: Springer; 2009. 7. Edelman D, McDuffie JR, Oddone E, Gierisch JM, Williams JW. Shared medical appointments for chronic medical conditions: a systematic review. VA-ESP Project #09-010. Durham, NC: Evidence-based Synthesis Program Center; 2012. 8. Housden L, Wong ST, Dawes M. Effectiveness of group medical visits for improving diabetes care: a systematic review and meta-analysis. CMAJ Canadian Medical Association Journal. 2013;185(13):E635-44. 9. Trento M, Passera P, Borgo E, Tomalino M, Bajardi M, Cavallo F, et al. A 5-Year Randomized Controlled Study of Learning, Problem Solving Ability, and Quality of Life Modifications in People With Type 2 Diabetes Managed by Group Care. Diabetes Care. 2004;27(3):670-5. 10. Trento M, Passera P, Tomalino M, Bajardi M, Pomero F, Allione A, et al. Group Visits Improve Metabolic Control in Type 2 Diabetes. A 2-year follow-up. 2001;24(6):995-1000. 11. Greenhalgh T, Campbell-Richards D, Vijayaraghavan S, Collard A, Malik F, Griffin M, et al. New models of self-management education for minority ethnic groups: pilot randomized trial of a story-sharing intervention. Journal of Health Services Research & Policy. 2011;16(1):28-36. 12. Greenhalgh T, Collard A, Begum N. Sharing stories: complex intervention for diabetes education in minority ethnic groups who do not speak English. Bmj. 2005;330(7492):628. 13. Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002–2012. New England Journal of Medicine. 2017;376(15):1419-29. 14. Kossarova L, Cheung R, Hargreaves D, Keeble E. Admissions of inequality: emergency hospital use for children and young people. London: Nuffield Trust; 2017. 15. Constantino MI, Molyneaux L, Limacher-Gisler F, Al-Saeed A, Luo C, Wu T, et al. Long-Term Complications and Mortality in Young-Onset Diabetes: Type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care. 2013;36(12):3863-9. 16. Browne JL, Nefs G, Pouwer F, Speight J. Depression, anxiety and self-care behaviours of young adults with Type 2 diabetes: results from the International Diabetes Management and Impact for Long-term Empowerment and Success (MILES) Study. Diabetic Medicine. 2015;32(1):133-40. 17. Hynes L, Byrne M, Dinneen SF, McGuire BE, O'Donnell M, Mc Sharry J. Barriers and facilitators associated with attendance at hospital diabetes clinics among young adults (15–30 years) with type 1 diabetes mellitus: a systematic review. Pediatric Diabetes. 2016;17(7):509-18. 18. Hargreaves DS, Viner RM. Children's and young people's experience of the National Health Service in England: a review of national surveys 2001–2011. Archives of Disease in Childhood. 2012;97(7):661-6. 19. Hargreaves DS, Elliott MN, Viner RM, Richmond TK, Schuster MA. Unmet Health Care Need in US Adolescents and Adult Health Outcomes. Pediatrics. 2015;136(3):513-20. 20. Wong G, Greenhalgh T, Westhrop G, Pawson R. Development of methodological guidance, publication standards and training materials for realist and meta-narrative reviews: The RAMESES (Realist And Meta-narrative Evidence Syntheses: Evolving Standards) project. Health Serv Deliv Res. 2014;2(30).
Page 23 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
24
21. Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews? European Journal of Clinical Investigation. 2018;48(6):e12931. 22. Papoutsi C, Hargreaves D, Colligan G, Hagell A, Patel A, Campbell-Richards D, et al. Group clinics for young adults with diabetes in an ethnically diverse, socioeconomically deprived setting (TOGETHER study): protocol for a realist review, co-design and mixed methods, participatory evaluation of a new care model. BMJ Open. 2017;7(6):e017363. 23. Papoutsi C, Mattick K, Pearson M, Brennan N, Briscoe S, Wong G. Social and professional influences on antimicrobial prescribing for doctors-in-training: a realist review. Journal of Antimicrobial Chemotherapy. 2017;72(9):2418-30. 24. Kirsh SR, Aron DC, Johnson KD, Santurri LE, Stevenson LD, Jones KR, et al. A realist review of shared medical appointments: How, for whom, and under what circumstances do they work? BMC Health Services Research. 2017;17(1):113. 25. Booth A, Cantrell A, Preston L, Chambers D, Goyder E. What is the evidence for the effectiveness, appropriateness and feasibility of group clinics for patients with chronic conditions? A systematic review. Health Services and Delivery Research. 2015;3(46). 26. Glass TA, McAtee MJ. Behavioral science at the crossroads in public health: extending horizons, envisioning the future. Social science & medicine. 2006;62(7):1650-71. 27. Stones R. Structuration theory. Basingstoke: Palgrave-Macmillan; 2005. 28. Greenhalgh T, Clinch M, Afsar N, Choudhury Y, Sudra R, Campbell-Richards D, et al. Socio-cultural influences on the behaviour of South Asian women with diabetes in pregnancy: qualitative study using a multi-level theoretical approach. BMC medicine. 2015;13(1):120. 29. Pols J. Knowing Patients. Science, Technology, & Human Values. 2013;39(1):73-97. 30. Strauss A. Work and the division of labor. The sociological quarterly. 1985;26(1):1-19. 31. Allen D. The Invisible Work of Nurses: Hospitals, Organisation and Healthcare. New York: Routledge; 2014. 32. Mejino A, Noordman J, van Dulmen S. Shared medical appointments for children and adolescents with type 1 diabetes: perspectives and experiences of patients, parents, and health care providers. Adolescent Health Medicine & Therapeutics. 2012;3:75-83. 33. Noordman J, van Dulmen S. Shared Medical Appointments marginally enhance interaction between patients: an observational study on children and adolescents with type 1 diabetes. Patient Education & Counseling. 2013;92(3):418-25. 34. Raymond JK, Shea JJ, Berget C, Cain C, Fay-Itzkowitz E, Gilmer L, et al. A novel approach to adolescents with type 1 diabetes: The team clinic model. Diabetes Spectrum. 2015;28(1):68-71. 35. Rijswijk C, Zantinge E, Seesing F, Raats I, van Dulmen S. Shared and individual medical appointments for children and adolescents with type 1 diabetes; differences in topics discussed? Patient Education & Counseling. 2010;79(3):351-5. 36. Lawton J, Rankin D. How do structured education programmes work? An ethnographic investigation of the dose adjustment for normal eating (DAFNE) programme for type 1 diabetes patients in the UK. Social Science & Medicine. 2010;71(3):486-93. 37. Lovell N. The 'SKIP' course: A programme for children and young people with diabetes. Journal of Diabetes Nursing. 2012;16(6):247-52. 38. Price K, Knowles J, Fox M, Wales J, Heller S, Eiser C, et al. Effectiveness of the Kids in Control of Food (KICk-OFF) structured education course for 11-16 year olds with Type 1 diabetes. Diabetic medicine : a journal of the British Diabetic Association [Internet]. 2016; 33(2):[192-203 pp.]. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/592/CN-01133592/frame.html
http://onlinelibrary.wiley.com/store/10.1111/dme.12881/asset/dme12881.pdf?v=1&t=izef2wm4&s=423664531d3ba0a3ff801d987785715125e25cd1. 39. Beer R, Eiser C, Johnson B, Bottrell K, Whitehead V, Elliott J, et al. WICKED: The development and evaluation of a psycho-education programme for young people with type 1 diabetes. Journal of Diabetes Nursing. 2014;18(6):233-7. 40. Graue M, Wentzel-Larsen T, Hanestad BR, Sovik O. Evaluation of a programme of group visits and computer-assisted consultations in the treatment of adolescents with Type 1 diabetes. Diabetic Medicine. 2005;22(11):1522-9.
Page 24 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
25
41. Céspedes-Knadle YM, Munoz CE. Development of a group intervention for teens with type 1 diabetes. The Journal for Specialists in Group Work. 2011;36(4):278-95. 42. Wong ST, Browne A, Lavoie J, Macleod MLP, Chongo M, Ulrich C. Incorporating group medical visits into primary healthcare: Are there benefits? Healthcare Policy. 2015;11(2):27-42. 43. Newman D. School nurse-facilitated group meetings for adolescents with diabetes. NASN School Nurse. 2012;27(1):15-7. 44. Murphy K, Casey D, Dinneen S, Lawton J, Brown F. Participants' perceptions of the factors that influence diabetes self-management following a structured education (DAFNE) programme. Journal of Clinical Nursing. 2011;20(9-10):1282-92. 45. Løding RN, Wold JE, Skavhaug A, Graue M. Evaluation of peer-group support and problem-solving training in the treatment of adolescents with type 1 diabetes. European Diabetes Nursing. 2007;4(1):28-33. 46. Plante WA, Lobato DJ. Psychosocial group interventions for children and adolescents with type 1 diabetes: the state of the literature. Children's Health Care. 2008;37(2):93-111. 47. Robinson E. Being diagnosed with type 1 diabetes during adolescence. How do young people develop a healthy understanding of diabetes? Practical Diabetes. 2015;32(9):339-44a. 48. Dovey-Pearce G, Doherty Y, May C. The influence of diabetes upon adolescent and young adult development: a qualitative study. British Journal of Health Psychology. 2007;12(Pt 1):75-91. 49. Hinder S, Greenhalgh T. " This does my head in". Ethnographic study of self-management by people with diabetes. BMC Health Services Research. 2012;12(1):83. 50. Sawtell M, Jamieson L, Wiggins M, Smith F, Ingold A, Hargreaves K, et al. Implementing a structured education program for children with diabetes: lessons learnt from an integrated process evaluation. BMJ Open Diabetes Research & Care. 2015;3(1):e000065. 51. Day E. Group education for young people with diabetes. Journal of Diabetes Nursing. 2007;11(3):5p-p. 52. Rogers EM. Diffusion of innovations: Simon and Schuster; 2010. 53. Dovey�Pearce G, Hurrell R, May C, Walker C, Doherty Y. Young adults’(16–25 years) suggestions for providing developmentally appropriate diabetes services: a qualitative study. Health & social care in the community. 2005;13(5):409-19. 54. Hynes L, Byrne M, Casey D, Dinneen SF, O'Hara MC. 'It makes a difference, coming here': A qualitative exploration of clinic attendance among young adults with type 1 diabetes. British Journal of Health Psychology. 2015;20(4):842-58. 55. Doherty Y, Dovey-Pearce G. Understanding the developmental and psychological needs of young people with diabetes. Implications for providing engaging and effective services. Practical Diabetes International. 2005;22(2):59-64. 56. Dovey-Pearce G. Improving care for young people: Ask them and they will tell you. Practical Diabetes. 2015;32(4):147. 57. Chaney D, Coates V, Shevlin M, Carson D, McDougall A, Long A. Diabetes education: what do adolescents want? Journal of Clinical Nursing. 2012;21(1-2):216-23. 58. Rankin D, Cooke DD, Elliott J, Heller SR, Lawton J, Group UNDS. Supporting self-management after attending a structured education programme: a qualitative longitudinal investigation of type 1 diabetes patients' experiences and views. BMC Public Health. 2012;12:652. 59. Wiggins M, Bonell C, Sawtell M, Austerberry H, Burchett H, Allen E, et al. Health outcomes of youth development programme in England: prospective matched comparison study. BMJ. 2009;339:b2534. 60. Greenhalgh T, Collard A, Campbell-Richards D, Vijayaraghavan S, Malik F, Morris J, et al. Storylines of self-management: narratives of people with diabetes from a multiethnic inner city population. Journal of Health Services Research & Policy. 2011;16(1):37-43.
Page 25 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
26
Records identified in database search
(n=1641)
Records after duplicates removed (n=1639)
Title and abstract screening (n=1639)
Full-text screening (n=273)
Total articles included in synthesis (n=131) - Core (n=4) - High relevance (n=35) - Low relevance (n=72)
Records excluded (n=165) - Not relevant (n=92) - Abstracts only (n=48) - Dissertations (n=6) - Full text unavailable (n=19)
Records excluded (n=1366)
Records included through expert opinion and citation tracking (n=19)
Figure 1: Study flowchart
Page 26 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
27
CMOC 1: When young adults, who do not normally have the opportunity to share experiences with peers
living with diabetes, find a space to connect and share openly with others (C), this might make it more likely for
patients to feel supported (M) and comfortable (M), and could in turn lead to perceptions of increased
understanding and learning (O).
CMOC 2: When group interactions enable peer support, young adults who feel more isolated, experience
negative perceptions of self-management and/or face diabetes-related distress (C), may draw encouragement
from each other (M), which could subsequently lead to more confidence and motivation in their self-
management (O).
CMOC 3: Peer support in group clinics for young adults who experience their diagnosis and self-management
as socially stigmatising (C), may help instil a sense of normalcy (M), which could lead to re-thinking self-
monitoring and management in social settings (O).
CMOC 4: Where group clinic bring together participants who have common characteristics or shared
experiences (C), it is assumed that a sense of affinity is more likely to emerge between group members (M),
which could lead to increased sharing and sustained interest as participants will be able to relate to each other’s
experiences (O).
CMOC 5: In contexts where young adults have previously experienced a collaborative, helpful and respectful
relationship with their clinicians, characterised by mutual understanding (C), it is more likely they will feel safe
in exposing vulnerabilities (M) and that they will perceive added value and usefulness from interactions with
services providers who know them well (M), which may lead to increased engagement with the service (O) and
increased attendance (O).
CMOC 6: An increased emphasis on positive aspects of self-management and developmentally tailored
attention to sensitive emotional needs over other priorities, for young adults who remain ambivalent about their
role as diabetes patients (C), may help young adults slowly build self-esteem (M) and take a more active role in
their self-management (O).
CMOC 7: With time people who engage in group sessions (C), make continuous judgments about the added
value of these sessions to their own individual needs (M), which leads them to decide whether they will keep
engaging with the group (O).
CMOC 8: For young adults who have negative perceptions about their ability to self-manage or who face
diabetes-related distress (C), fear they may be diagnosed with further health problems (M), may lead them to
disengage from the service (O).
Page 27 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

28
Table 1: Context-Mechanism-Outcome Configurations (CMOCs).
Page 28 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
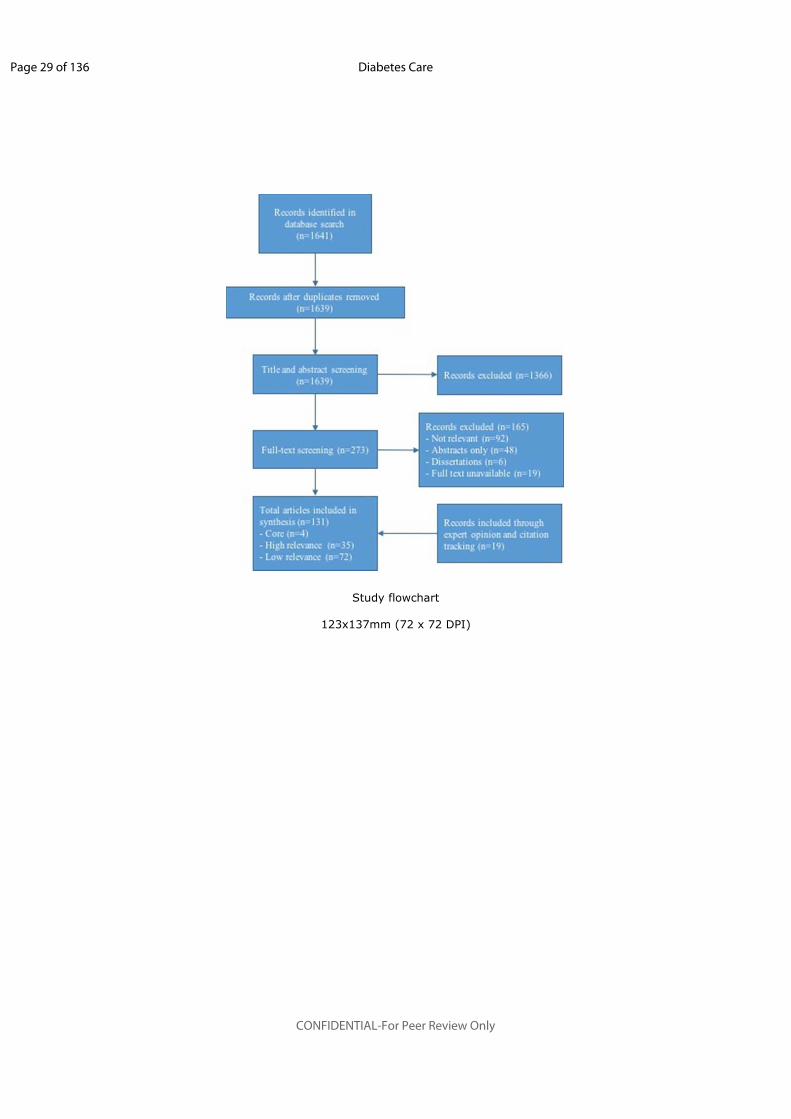
Study flowchart
123x137mm (72 x 72 DPI)
Page 29 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
1
Online-Only Supplemental Material
Appendix 1
Glossary
Contexts: settings, structures, environments, conditions or circumstances that trigger
behavioural and emotional responses (i.e. mechanisms) for those affected.
Mechanisms: the way in which individuals respond to and reason about the resources,
opportunities or challenges offered by a particular programme, intervention or process.
Mechanisms are triggered in specific contexts and lead to changes in behaviour.
Outcomes: impacts or behaviours resulting from the interaction between mechanisms and
contexts.
Context-Mechanism-Outcome Configurations (CMOCs): relationships between the building
blocks of realist analysis, i.e. how mechanisms are triggered under specific contexts to result
in particular outcomes.
Programme theory: a set of theoretical explanations or assumptions about how a particular
programme, process or intervention is expected to work.
Page 30 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
2
Appendix 2
Example search strategy
Date: 14 February 2017
Database: Ovid MEDLINE(R) Epub Ahead of Print, In-Process & Other Non-Indexed
Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R)
Interface: OvidSP
Coverage: 1946-present
Hits: 909
1 Young Adult/
2 Adolescent/
3 (adolescen* or teen* or young people or young men or young women or young male? or young female?
or young adult? or youth?).ti,ab.
4 1 or 2 or 3
5 exp Diabetes Mellitus/
6 diabet*.ti,ab.
7 5 or 6
8 *Group Processes/
9 Group Processes/ and "Appointments and Schedules"/
10 (group adj2 (visit* or clinic? or appointment? or care or meeting?)).ti,ab.
11 (gmv or gma).ti,ab.
12 ((shared or share or sharing) adj2 (appointment? or visit*)).ti,ab.
13 cluster visit*.ti,ab.
14 (group? adj2 (workshop? or class* or course? or train* or educat*)).ti,ab.
Page 31 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
3
15 exp Self Care/ and (health education/ or patient education as topic/)
16 exp Self Care/ and Group Processes/
17 ((self care or selfcare or self manag* or selfmanag* or self monitor* or selfmonitor*) adj5 (workshop?
or class* or course? or meeting? or train* or educat*)).ti,ab.
18 ("Dose Adjustment For Normal Eating" or dafne).ti,ab.
19 ("Diabetes education and self-management for ongoing and newly diagnosed" or desmond).ti,ab.
20 ("Beta Cell Education Resources for Training in Insulin and Eating" or bertie or streetwise or
lifewise).ti,ab.
21 x-pert.ti,ab.
22 (conversation map* or "journey for control").ti,ab.
23 (self care or selfcare or self manag* or selfmanag* or self monitor* or selfmonitor*).ti,ab.
24 ((group? adj2 (support or meeting)) or (peer? adj2 (support or group?))).ti,ab.
25 (education* adj3 (intervention? or program*)).ti,ab.
26 24 or 25
27 23 and 26
28 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 27
29 4 and 7 and 28
Page 32 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
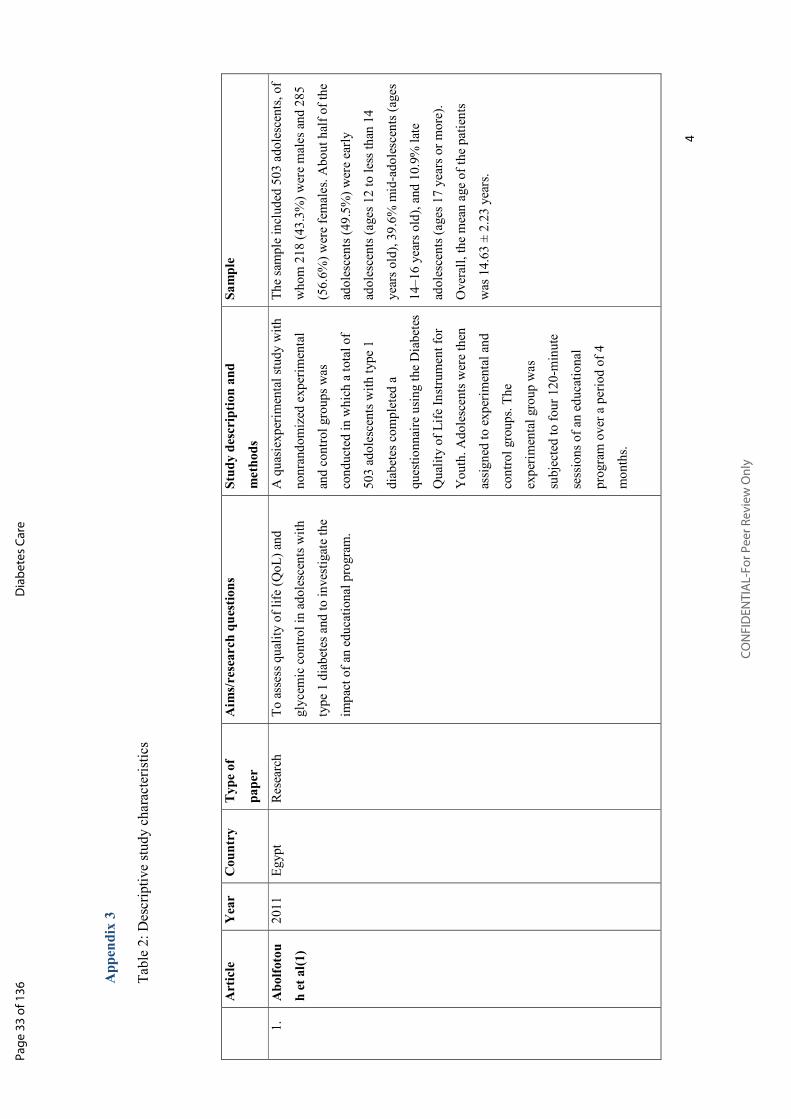
4 A
ppen
dix
3
Tabl
e 2:
Des
crip
tive
stud
y ch
arac
teris
tics
A
rtic
le
Yea
r C
ount
ry
Type
of
pape
r
Aim
s/re
sear
ch q
uest
ions
St
udy
desc
ript
ion
and
met
hods
Sam
ple
1.
Abo
lfoto
u
h et
al(1
)
2011
Eg
ypt
Res
earc
h To
ass
ess q
ualit
y of
life
(QoL
) and
glyc
emic
con
trol i
n ad
oles
cent
s with
type
1 d
iabe
tes a
nd to
inve
stig
ate
the
impa
ct o
f an
educ
atio
nal p
rogr
am.
A q
uasi
expe
rimen
tal s
tudy
with
nonr
ando
miz
ed e
xper
imen
tal
and
cont
rol g
roup
s was
cond
ucte
d in
whi
ch a
tota
l of
503
adol
esce
nts w
ith ty
pe 1
diab
etes
com
plet
ed a
ques
tionn
aire
usi
ng th
e D
iabe
tes
Qua
lity
of L
ife In
stru
men
t for
You
th. A
dole
scen
ts w
ere
then
assi
gned
to e
xper
imen
tal a
nd
cont
rol g
roup
s. Th
e
expe
rimen
tal g
roup
was
subj
ecte
d to
four
120
-min
ute
sess
ions
of a
n ed
ucat
iona
l
prog
ram
ove
r a p
erio
d of
4
mon
ths.
The
sam
ple
incl
uded
503
ado
lesc
ents
, of
who
m 2
18 (4
3.3%
) wer
e m
ales
and
285
(56.
6%) w
ere
fem
ales
. Abo
ut h
alf o
f the
adol
esce
nts (
49.5
%) w
ere
early
adol
esce
nts (
ages
12
to le
ss th
an 1
4
year
s old
), 39
.6%
mid
-ado
lesc
ents
(age
s
14–1
6 ye
ars o
ld),
and
10.9
% la
te
adol
esce
nts (
ages
17
year
s or m
ore)
.
Ove
rall,
the
mea
n ag
e of
the
patie
nts
was
14.
63 ±
2.2
3 ye
ars.
Page
33
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
5
2.
Abu
alul
a
et a
l(2)
2016
U
S Sy
stem
atic
revi
ew
To e
valu
ate
the
effe
ctiv
enes
s of
diab
etes
sel
f-m
anag
emen
t edu
catio
n
inte
rven
tions
with
a sk
ills d
evel
opm
ent
com
pone
nt o
n th
e qu
ality
of l
ife o
f
adol
esce
nts w
ith ty
pe 1
dia
bete
s.
Six
data
base
s wer
e
syst
emat
ical
ly se
arch
ed –
14
stud
ies p
ublis
hed
betw
een
1994
and
2014
met
the
incl
usio
n
crite
ria.
Stud
ies v
arie
d in
geo
grap
hy, p
ublic
atio
n
date
, fun
ding
, sam
ple
size
, and
QO
L
scal
e us
ed. T
he sa
mpl
e si
zes o
f the
stud
ies r
ange
d fr
om 1
9 to
503
adol
esce
nts,
and
ther
e w
ere
sim
ilar
prop
ortio
ns in
par
ticip
atio
n be
twee
n
mal
es a
nd fe
mal
es. I
nter
vent
ions
incl
uded
stru
ctur
ed a
nd u
nstru
ctur
ed
diab
etes
edu
catio
n pr
ogra
ms.
3.
Alb
ano
et
al(3
)
2008
Ita
ly
Syst
emat
ic
revi
ew
To id
entif
y th
e re
cent
cha
ract
eris
tics
and
the
deve
lopm
ents
of t
hera
peut
ic
educ
atio
n in
dia
bete
s.
Four
dat
abas
es w
ere
syst
emat
ical
ly se
arch
ed –
80
artic
les m
et th
e in
clus
ion
crite
ria.
39,6
24 p
atie
nts i
n to
tal (
rang
e fr
om 2
4
to 1
0,00
0 pa
tient
s) w
ith m
ajor
ity o
f
adul
t pat
ient
s (81
%) -
eld
erly
pat
ient
s
(6.7
%),
child
ren
(6.7
%) a
nd a
dole
scen
ts
(5%
) rep
rese
nt o
nly
a m
inor
ity o
f the
sam
ple.
4.
Altu
ndag
et a
l(4)
2016
Tu
rkey
R
esea
rch
To e
valu
ate
the
effe
cts o
f gro
up
inte
ract
ion
and
train
ing
in th
e
adap
tatio
n pr
oces
s to
dise
ase
in
adol
esce
nts w
ith ty
pe 1
dia
bete
s
mel
litus
(T1D
M).
Expe
rimen
tal s
tudy
with
pre
-
and
post
-test
con
trol g
roup
s in
the
pedi
atric
end
ocrin
e cl
inic
of
a un
iver
sity
hos
pita
l.
38 a
dole
scen
ts (s
tudy
gro
up n
=18,
cont
rol g
roup
n=2
0) w
ith T
1DM
betw
een
the
ages
of 1
2 an
d 14
yea
rs
Page
34
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
6
5.
And
erso
n
et a
l.(5)
2003
U
S R
esea
rch
Th
is st
udy
pres
ents
a c
linic
al
pers
pect
ive
on th
e ch
alle
nge
of
impr
ovin
g di
abet
es e
duca
tion
and
care
durin
g th
e yo
ung
adul
t per
iod,
focu
ssin
g on
the
impo
rtanc
e of
the
deve
lopm
enta
l cha
nges
that
occ
ur
durin
g th
is tr
ansi
tiona
l pha
se o
f life
. It
pres
ents
dev
elop
men
tally
-bas
ed
prac
tice
prin
cipl
es fo
r the
you
ng a
dult
perio
d.
The
auth
ors t
ook
a
deve
lopm
enta
l per
spec
tive
on
youn
g ad
ulth
ood
to u
nder
stan
d
its im
pact
on
diab
etes
man
agem
ent a
nd e
ngag
emen
t in
ther
apy.
n/a
Page
35
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
7
6.
Atta
ri et
al(6
)
2006
Ir
an
Res
earc
h To
inve
stig
ate
the
effe
ct o
f stre
ss
man
agem
ent t
rain
ing
on g
lyca
emic
cont
rol i
n pa
tient
s liv
ing
with
Typ
e 1
diab
etes
A q
uasi
exp
erim
enta
l stu
dy w
ith
nonr
ando
miz
ed e
xper
imen
tal
and
cont
rol g
roup
s was
cond
ucte
d in
whi
ch 6
0 pa
tient
s
com
plet
ed a
26
item
stre
ss
man
agem
ent q
uest
ionn
aire
.
HbA
1 le
vels
wer
e m
easu
red
sim
ulta
neou
sly
for a
ll
parti
cipa
nts b
efor
e th
e st
udy.
The
stud
y gr
oup
atte
nded
8, 2
hour
sess
ions
with
10-
15
parti
cipa
nts,
over
a 3
mon
th
perio
d on
stre
ss m
anag
emen
t.
The
clas
s for
mat
was
dis
cuss
ion
and
mut
ual t
alk,
und
er th
e
supe
rvis
ion
of a
psy
chia
trist
. At
the
end
of e
ach
sess
ion
ther
e
was
hom
ewor
k to
pre
pare
for
the
next
vis
it.
60 ty
pe 1
dia
betic
s (16
-30
year
s) w
ere
mat
ched
for a
ge a
nd se
x an
d di
vide
d in
to a
stud
y gr
oup
(n-=
30, m
ean
19.7
(3.2
9) [1
6-30
]) a
nd a
con
trol g
roup
(n=3
0, m
ean
20.8
(9.5
2 [1
6-30
]).
Page
36
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
8
7.
Bee
r et
al(7
)
2014
U
K
Res
earc
h To
dev
elop
, tria
l and
eva
luat
e an
age
-
appr
opria
te se
lf-m
anag
emen
t
prog
ram
me
calle
d W
orki
ng w
ith
Insu
lin, C
arbs
, Ket
ones
and
Exe
rcis
e to
Man
age
Dia
bete
s (W
ICK
ED)
Phas
e 1:
Par
ticip
ants
atte
nded
a
one-
wee
k D
AFN
E co
urse
, and
wer
e of
fere
d fo
llow
-up
at si
x
wee
ks. A
focu
s gro
up w
ith th
e
parti
cipa
nts t
ook
plac
e at
the
end
of th
e co
urse
and
inte
rvie
ws
wer
e ca
rrie
d ou
t with
faci
litat
ors
both
bef
ore
and
afte
r the
cou
rse.
Phas
e 2:
Dev
elop
men
t of a
stru
ctur
ed e
duca
tion
cour
se
spec
ific
to th
e re
quire
men
ts o
f
youn
g pe
ople
with
dia
bete
s.
Phas
e 3:
Eva
luat
ion
of th
e ne
w
cour
se u
sing
writ
ten
acco
unts
from
par
ticip
ants
and
con
tent
anal
ysis
.
Phas
e 1:
Sev
en y
oung
peo
ple
aged
16–
21.
Phas
e 2
and
3: N
ine
youn
g pe
ople
age
d
16–2
1 ye
ars a
ttend
ed th
e on
e-w
eek
cour
se a
nd to
ok p
art i
n ev
alua
tion.
Page
37
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
9
8.
Ble
akly
&
McK
ee(8
)
2010
N
orth
ern
Irel
and
Res
earc
h To
dis
cuss
the
deve
lopm
ent a
nd re
sults
of a
n ed
ucat
ion
prog
ram
me
for
adol
esce
nts w
ith ty
pe 1
dia
bete
s.
Focu
s gro
up to
incl
ude
adol
esce
nts i
n st
ruct
urin
g th
eir
own
educ
atio
n se
ssio
ns.
Four
2-h
our a
fter s
choo
l
sess
ions
at w
eekl
y in
terv
als i
n
the
loca
l lei
sure
cen
tre. T
he
sess
ions
invo
lved
a m
ixtu
re o
f
grou
p di
scus
sion
s, re
flect
ion,
and
prac
tical
app
licat
ion.
The
lear
ning
nee
ds o
f eac
h
indi
vidu
al w
ere
asse
ssed
thro
ugh
an in
itial
mul
tiple
choi
ce k
now
ledg
e qu
estio
nnai
re
adap
ted
by th
e di
abet
es te
am,
whi
ch in
clud
ed q
uest
ions
on
carb
ohyd
rate
food
s, in
sulin
actio
n an
d hy
pogl
ycae
mia
treat
men
t. A
n id
entic
al
ques
tionn
aire
at t
he e
nd o
f the
4
wee
ks p
rovi
ded
a to
ol to
ass
ess
know
ledg
e ga
ined
.
Eigh
t ado
lesc
ents
and
four
par
ents
atte
nded
and
rece
ived
info
rmat
ion
rega
rdin
g th
e pr
opos
ed c
onte
nt o
f the
educ
atio
n se
ssio
ns. O
f the
se a
dole
scen
ts
five
atte
nded
the
educ
atio
nal p
rogr
amm
e
on fo
ur c
onse
cutiv
e se
ssio
ns. T
he ta
rget
age
grou
p w
as 1
4- to
16-
year
olds
with
type
1 d
iabe
tes o
n m
ultip
le d
aily
inje
ctio
n (M
DI)
ther
apy
or w
ishi
ng to
com
men
ce M
DI t
hera
py.
Page
38
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
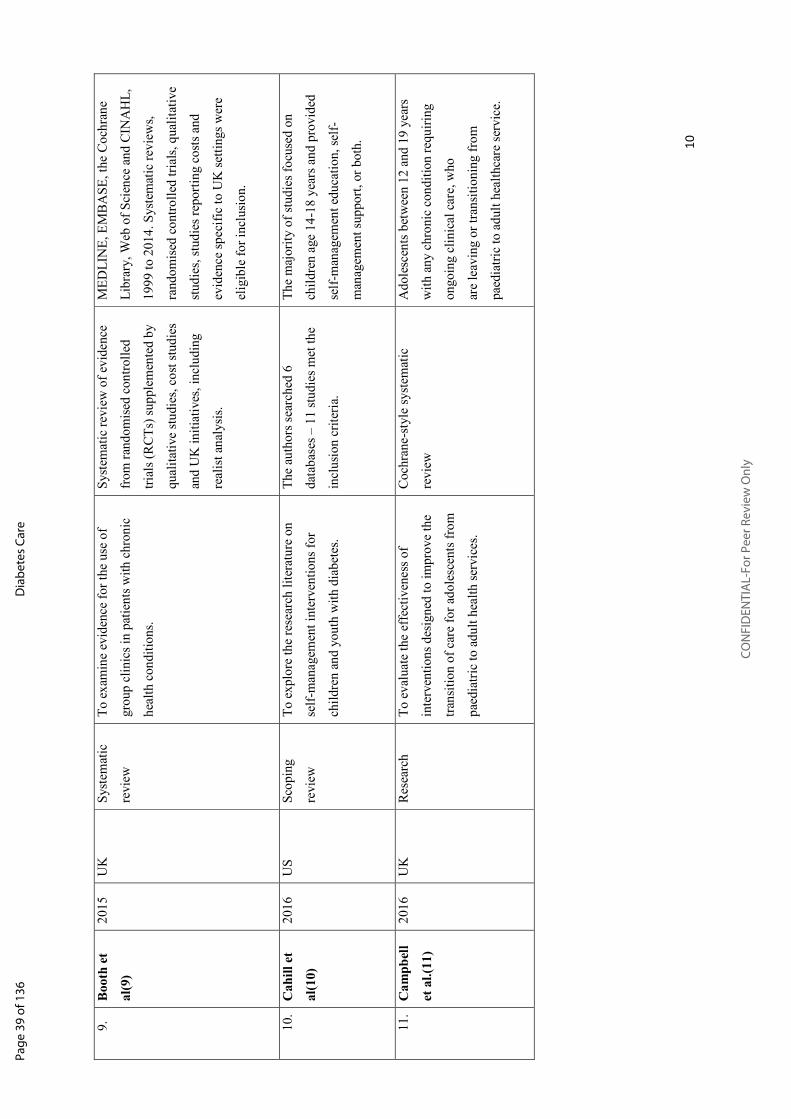
10
9.
Boo
th e
t
al(9
)
2015
U
K
Syst
emat
ic
revi
ew
To e
xam
ine
evid
ence
for t
he u
se o
f
grou
p cl
inic
s in
patie
nts w
ith c
hron
ic
heal
th c
ondi
tions
.
Syst
emat
ic re
view
of e
vide
nce
from
rand
omis
ed c
ontro
lled
trial
s (R
CTs
) sup
plem
ente
d by
qual
itativ
e st
udie
s, co
st st
udie
s
and
UK
initi
ativ
es, i
nclu
ding
real
ist a
naly
sis.
MED
LIN
E, E
MB
ASE
, the
Coc
hran
e
Libr
ary,
Web
of S
cien
ce a
nd C
INA
HL,
1999
to 2
014.
Sys
tem
atic
revi
ews,
rand
omis
ed c
ontro
lled
trial
s, qu
alita
tive
stud
ies,
stud
ies r
epor
ting
cost
s and
evid
ence
spec
ific
to U
K se
tting
s wer
e
elig
ible
for i
nclu
sion
.
10.
Cah
ill e
t
al(1
0)
2016
U
S Sc
opin
g
revi
ew
To e
xplo
re th
e re
sear
ch li
tera
ture
on
self-
man
agem
ent i
nter
vent
ions
for
child
ren
and
yout
h w
ith d
iabe
tes.
The
auth
ors s
earc
hed
6
data
base
s – 1
1 st
udie
s met
the
incl
usio
n cr
iteria
.
The
maj
ority
of s
tudi
es fo
cuse
d on
child
ren
age
14-1
8 ye
ars a
nd p
rovi
ded
self-
man
agem
ent e
duca
tion,
self-
man
agem
ent s
uppo
rt, o
r bot
h.
11.
Cam
pbel
l
et a
l.(11
)
2016
U
K
Res
earc
h
To e
valu
ate
the
effe
ctiv
enes
s of
inte
rven
tions
des
igne
d to
impr
ove
the
trans
ition
of c
are
for a
dole
scen
ts fr
om
paed
iatri
c to
adu
lt he
alth
serv
ices
.
Coc
hran
e-st
yle
syst
emat
ic
revi
ew
Ado
lesc
ents
bet
wee
n 12
and
19
year
s
with
any
chr
onic
con
ditio
n re
quiri
ng
ongo
ing
clin
ical
car
e, w
ho
are
leav
ing
or tr
ansi
tioni
ng fr
om
paed
iatri
c to
adu
lt he
alth
care
serv
ice.
Page
39
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
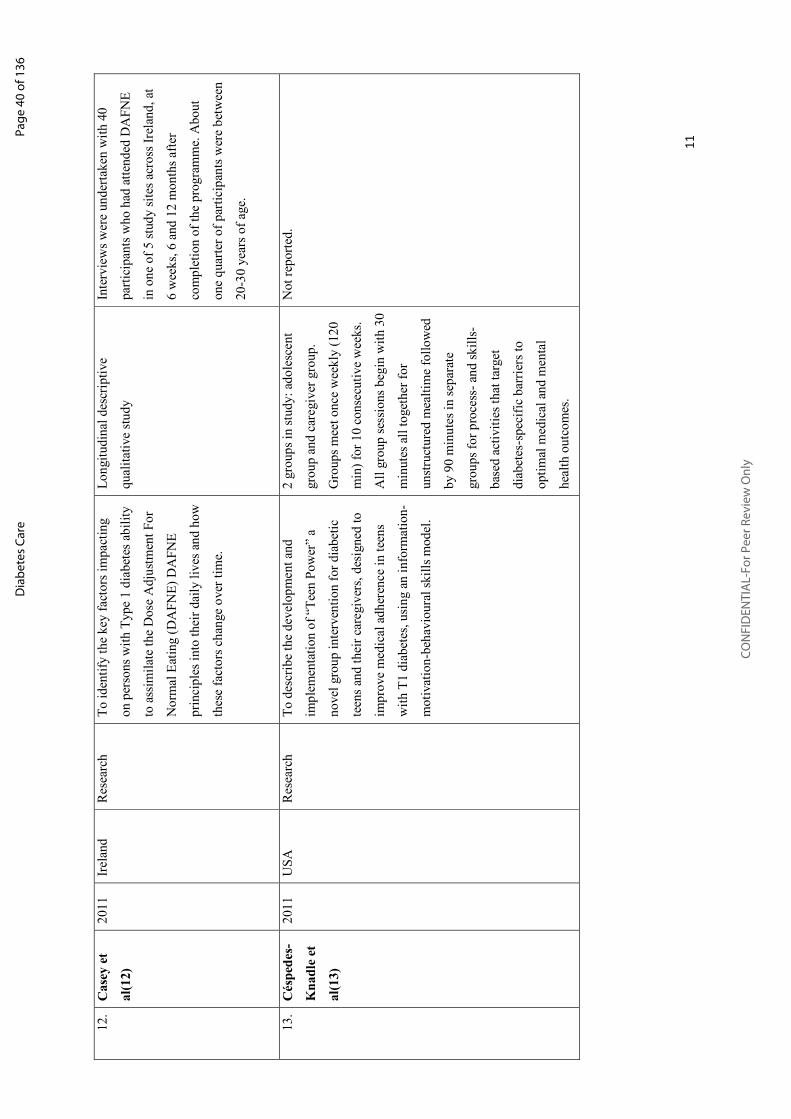
11
12.
Cas
ey e
t
al(1
2)
2011
Ir
elan
d R
esea
rch
To id
entif
y th
e ke
y fa
ctor
s im
pact
ing
on p
erso
ns w
ith T
ype
1 di
abet
es a
bilit
y
to a
ssim
ilate
the
Dos
e A
djus
tmen
t For
Nor
mal
Eat
ing
(DA
FNE)
DA
FNE
prin
cipl
es in
to th
eir d
aily
live
s and
how
thes
e fa
ctor
s cha
nge
over
tim
e.
Long
itudi
nal d
escr
iptiv
e
qual
itativ
e st
udy
Inte
rvie
ws w
ere
unde
rtake
n w
ith 4
0
parti
cipa
nts w
ho h
ad a
ttend
ed D
AFN
E
in o
ne o
f 5 st
udy
site
s acr
oss I
rela
nd, a
t
6 w
eeks
, 6 a
nd 1
2 m
onth
s afte
r
com
plet
ion
of th
e pr
ogra
mm
e. A
bout
one
quar
ter o
f par
ticip
ants
wer
e be
twee
n
20-3
0 ye
ars o
f age
.
13.
Cés
pede
s-
Kna
dle
et
al(1
3)
2011
U
SA
Res
earc
h To
des
crib
e th
e de
velo
pmen
t and
impl
emen
tatio
n of
“Te
en P
ower
” a
nove
l gro
up in
terv
entio
n fo
r dia
betic
teen
s and
thei
r car
egiv
ers,
desi
gned
to
impr
ove
med
ical
adh
eren
ce in
teen
s
with
T1
diab
etes
, usi
ng a
n in
form
atio
n-
mot
ivat
ion-
beha
viou
ral s
kills
mod
el.
2 gr
oups
in st
udy:
ado
lesc
ent
grou
p an
d ca
regi
ver g
roup
.
Gro
ups m
eet o
nce
wee
kly
(120
min
) for
10
cons
ecut
ive
wee
ks.
All
grou
p se
ssio
ns b
egin
with
30
min
utes
all
toge
ther
for
unst
ruct
ured
mea
ltim
e fo
llow
ed
by 9
0 m
inut
es in
sepa
rate
grou
ps fo
r pro
cess
- and
skill
s-
base
d ac
tiviti
es th
at ta
rget
diab
etes
-spe
cific
bar
riers
to
optim
al m
edic
al a
nd m
enta
l
heal
th o
utco
mes
.
Not
repo
rted.
Page
40
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
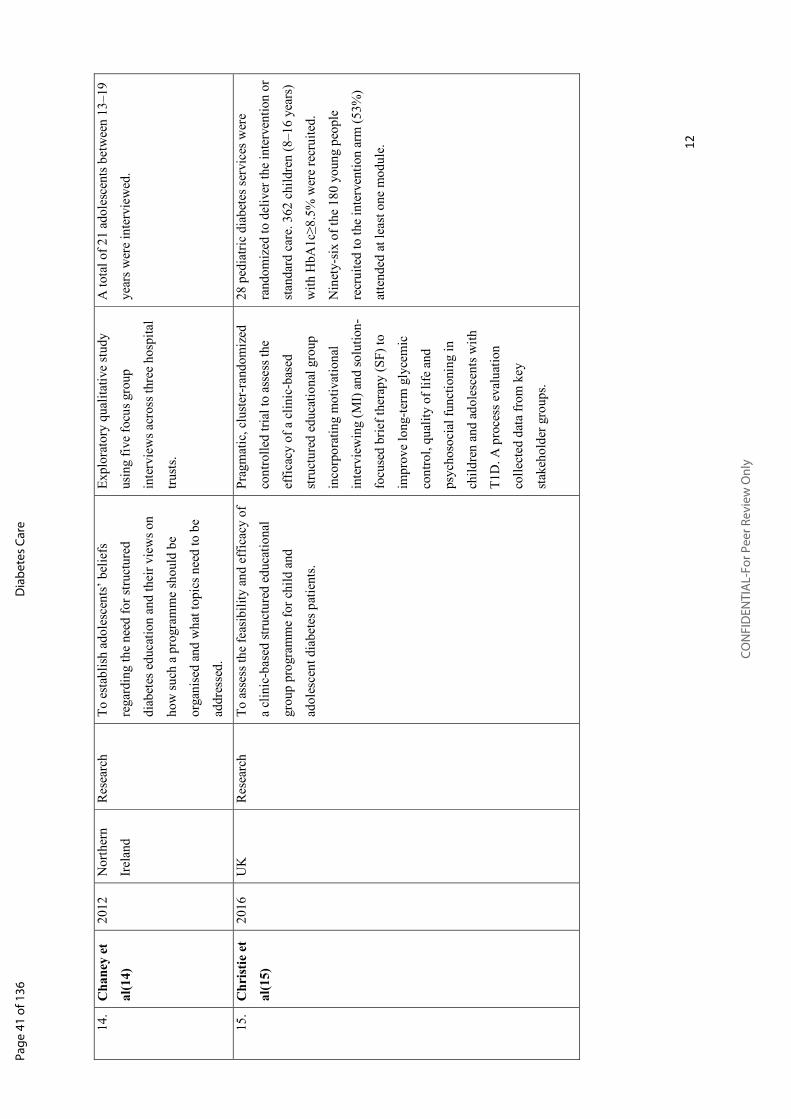
12
14.
Cha
ney
et
al(1
4)
2012
N
orth
ern
Irel
and
Res
earc
h To
est
ablis
h ad
oles
cent
s’ b
elie
fs
rega
rdin
g th
e ne
ed fo
r stru
ctur
ed
diab
etes
edu
catio
n an
d th
eir v
iew
s on
how
such
a p
rogr
amm
e sh
ould
be
orga
nise
d an
d w
hat t
opic
s nee
d to
be
addr
esse
d.
Expl
orat
ory
qual
itativ
e st
udy
usin
g fiv
e fo
cus g
roup
inte
rvie
ws a
cros
s thr
ee h
ospi
tal
trust
s.
A to
tal o
f 21
adol
esce
nts b
etw
een
13–1
9
year
s wer
e in
terv
iew
ed.
15.
Chr
istie
et
al(1
5)
2016
U
K
Res
earc
h To
ass
ess t
he fe
asib
ility
and
eff
icac
y of
a cl
inic
-bas
ed st
ruct
ured
edu
catio
nal
grou
p pr
ogra
mm
e fo
r chi
ld a
nd
adol
esce
nt d
iabe
tes p
atie
nts.
Prag
mat
ic, c
lust
er-r
ando
miz
ed
cont
rolle
d tri
al to
ass
ess t
he
effic
acy
of a
clin
ic-b
ased
stru
ctur
ed e
duca
tiona
l gro
up
inco
rpor
atin
g m
otiv
atio
nal
inte
rvie
win
g (M
I) a
nd so
lutio
n-
focu
sed
brie
f the
rapy
(SF)
to
impr
ove
long
-term
gly
cem
ic
cont
rol,
qual
ity o
f life
and
psyc
hoso
cial
func
tioni
ng in
child
ren
and
adol
esce
nts w
ith
T1D
. A p
roce
ss e
valu
atio
n
colle
cted
dat
a fr
om k
ey
stak
ehol
der g
roup
s.
28 p
edia
tric
diab
etes
serv
ices
wer
e
rand
omiz
ed to
del
iver
the
inte
rven
tion
or
stan
dard
car
e. 3
62 c
hild
ren
(8–1
6 ye
ars)
with
HbA
1c≥8
.5%
wer
e re
crui
ted.
Nin
ety-
six
of th
e 18
0 yo
ung
peop
le
recr
uite
d to
the
inte
rven
tion
arm
(53%
)
atte
nded
at l
east
one
mod
ule.
Page
41
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
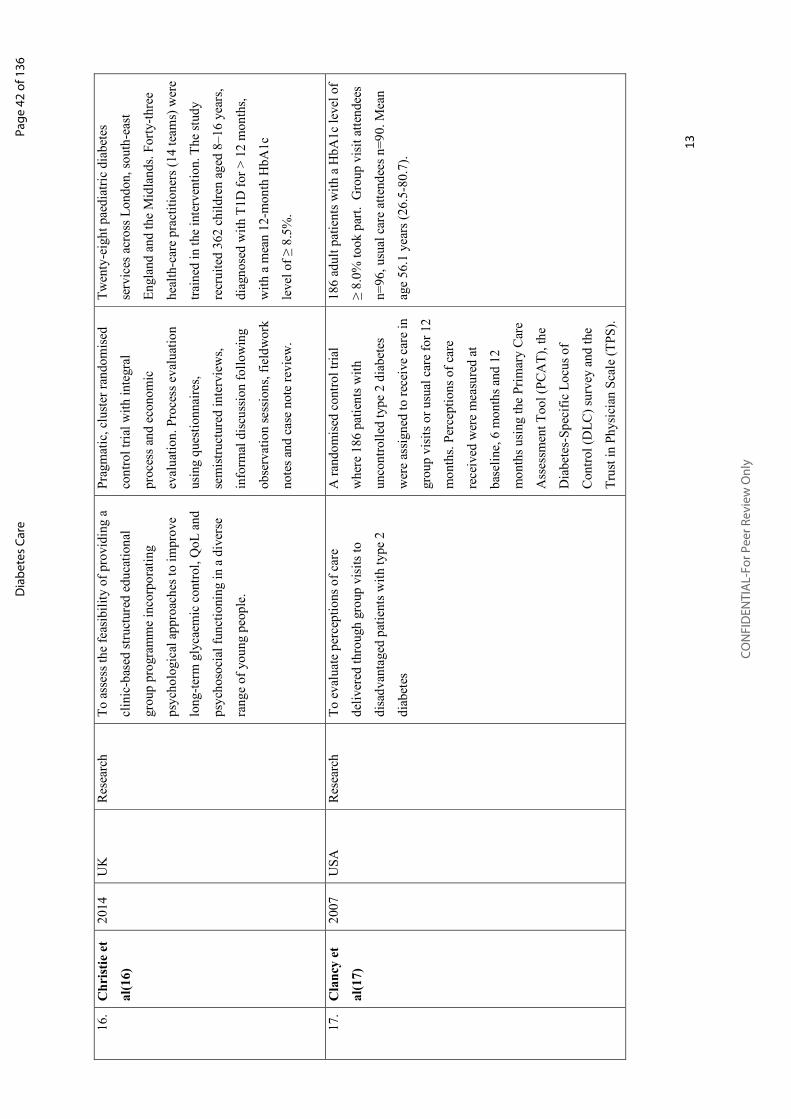
13
16.
Chr
istie
et
al(1
6)
2014
U
K
Res
earc
h To
ass
ess t
he fe
asib
ility
of p
rovi
ding
a
clin
ic-b
ased
stru
ctur
ed e
duca
tiona
l
grou
p pr
ogra
mm
e in
corp
orat
ing
psyc
holo
gica
l app
roac
hes t
o im
prov
e
long
-term
gly
caem
ic c
ontro
l, Q
oL a
nd
psyc
hoso
cial
func
tioni
ng in
a d
iver
se
rang
e of
you
ng p
eopl
e.
Prag
mat
ic, c
lust
er ra
ndom
ised
cont
rol t
rial w
ith in
tegr
al
proc
ess a
nd e
cono
mic
eval
uatio
n. P
roce
ss e
valu
atio
n
usin
g qu
estio
nnai
res,
sem
istru
ctur
ed in
terv
iew
s,
info
rmal
dis
cuss
ion
follo
win
g
obse
rvat
ion
sess
ions
, fie
ldw
ork
note
s and
cas
e no
te re
view
.
Twen
ty-e
ight
pae
diat
ric d
iabe
tes
serv
ices
acr
oss L
ondo
n, so
uth-
east
Engl
and
and
the
Mid
land
s. Fo
rty-th
ree
heal
th-c
are
prac
titio
ners
(14
team
s) w
ere
train
ed in
the
inte
rven
tion.
The
stud
y
recr
uite
d 36
2 ch
ildre
n ag
ed 8
–16
year
s,
diag
nose
d w
ith T
1D fo
r > 1
2 m
onth
s,
with
a m
ean
12-m
onth
HbA
1c
leve
l of ≥
8.5
%.
17.
Cla
ncy
et
al(1
7)
2007
U
SA
Res
earc
h To
eva
luat
e pe
rcep
tions
of c
are
deliv
ered
thro
ugh
grou
p vi
sits
to
disa
dvan
tage
d pa
tient
s with
type
2
diab
etes
A ra
ndom
ised
con
trol t
rial
whe
re 1
86 p
atie
nts w
ith
unco
ntro
lled
type
2 d
iabe
tes
wer
e as
sign
ed to
rece
ive
care
in
grou
p vi
sits
or u
sual
car
e fo
r 12
mon
ths.
Perc
eptio
ns o
f car
e
rece
ived
wer
e m
easu
red
at
base
line,
6 m
onth
s and
12
mon
ths u
sing
the
Prim
ary
Car
e
Ass
essm
ent T
ool (
PCA
T), t
he
Dia
bete
s-Sp
ecifi
c Lo
cus o
f
Con
trol (
DLC
) sur
vey
and
the
Trus
t in
Phys
icia
n Sc
ale
(TPS
).
186
adul
t pat
ient
s with
a H
bA1c
leve
l of
≥ 8.
0% to
ok p
art.
Gro
up v
isit
atte
ndee
s
n=96
, usu
al c
are
atte
ndee
s n=9
0. M
ean
age
56.1
yea
rs (2
6.5-
80.7
).
Page
42
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
14
18.
Cof
fen
&
Dah
lqui
st(
18)
2009
U
S Sy
stem
atic
revi
ew
To d
emon
stra
te th
e co
mpl
exity
of t
he
type
1 d
iabe
tes r
egim
en a
nd to
high
light
the
role
of t
he d
iabe
tes
educ
ator
s.
Thre
e da
taba
ses w
ere
sear
ched
for a
rticl
es a
bout
self-
man
agem
ent o
f typ
e 1
diab
etes
in y
oung
peo
ple.
Tas
k an
alys
is
to b
reak
dow
n th
e di
ffer
ent
activ
ities
invo
lved
in d
iabe
tes
man
agem
ent w
as c
ondu
cted
,
draw
ing
on re
leva
nt li
tera
ture
.
Littl
e in
form
atio
n is
pro
vide
d on
the
spec
ific
proc
esse
s fol
low
ed
in th
e re
view
.
The
pape
r foc
uses
on
child
ren
and
adol
esce
nts b
ut d
oes n
ot d
efin
e th
e
grou
p fu
rther
.
19.
Col
son
et
al(1
9)
2016
Fr
ance
Sy
stem
atic
revi
ew
To d
escr
ibe
the
cont
ent a
nd o
utco
mes
of st
ruct
ured
dia
bete
s edu
catio
n
prog
ram
mes
and
to a
sses
s com
patib
ility
with
reco
mm
enda
tions
of t
he
Inte
rnat
iona
l Soc
iety
for P
edia
tric
and
Ado
lesc
ent D
iabe
tes.
Inte
grat
ive
revi
ew b
ased
on
Coc
hran
e re
com
men
datio
ns.
Thirt
een
data
base
s wer
e
sear
ched
for e
valu
atio
ns o
f
educ
atio
n pr
ogra
ms (
2009
-
2014
) and
43
pape
rs m
et th
e
incl
usio
n cr
iteria
.
Educ
atio
nal p
rogr
amm
es fo
r you
ths w
ith
T1D
M <
18 y
ears
old
and
thei
r fam
ilies
.
Page
43
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
15
20.
Dav
idso
n
et a
l.(20
)
2004
U
S R
esea
rch
To d
escr
ibe
stre
ssor
s and
self-
care
chal
leng
es re
porte
d by
ado
lesc
ents
with
type
1 d
iabe
tes w
ho w
ere
unde
rgoi
ng in
itiat
ion
of in
tens
ive
man
agem
ent.
Con
tent
ana
lysi
s of c
opin
g sk
ills
train
ing
trans
crip
ts g
ener
ated
by
Gre
y an
d as
soci
ates
wer
e us
ed
to d
escr
ibe
adol
esce
nts’
pers
pect
ives
of s
tress
ors a
nd
self-
care
cha
lleng
es a
ssoc
iate
d
with
hav
ing
type
1 d
iabe
tes.
A c
onve
nien
ce sa
mpl
e of
six
teen
s (5
mal
es a
nd 1
fem
ale)
age
d 13
-17.
7 ye
ars
with
type
1 d
iabe
tes w
ere
draw
n fr
om a
wid
er st
udy,
“N
ursi
ng In
terv
entio
n to
Impl
emen
t DC
CT
Ther
apy
in Y
outh
(Gre
y et
al.,
199
8”
base
d on
the
avai
labi
lity
of tr
ansc
ripts
.
21.
Dav
is &
Vita
glia
no(
21)
2015
U
S
Posi
tion
pape
r/com
me
ntar
y
To in
trodu
ce th
e m
odel
of g
roup
vis
its
for a
dole
scen
ts w
ith ty
pe 1
dia
bete
s.
n/a
n/a
Page
44
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
16
22.
Dav
is et
al(2
2)
2008
U
SA
Res
earc
h R
evie
w o
f 9 p
aper
s on
“gro
up v
isits
in
diab
etes
” an
d ex
plor
atio
n of
ass
ocia
ted
prac
tical
issu
es.
Pilo
t stu
dy to
test
out
prac
tical
ities
of g
roup
vis
its fo
r
diab
etes
in a
Mid
wes
t aca
dem
ic
med
ical
cen
tre a
nd a
Wes
t Coa
st
fam
ily m
edic
ine
resi
denc
y. 2
orga
nisa
tiona
l mod
els:
a 9
0-
min
ute
nurs
e-pr
actit
ione
r led
grou
p vi
sit o
f six
to n
ine
patie
nts,
and
a se
cond
app
roac
h
usin
g a
prel
imin
ary
med
ical
assi
stan
t vis
it an
d th
ree
patie
nts
seen
toge
ther
by
a pr
imar
y ca
re
phys
icia
n in
an
hour
long
sess
ion.
Not
repo
rted
Page
45
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
17
23.
Day
(23)
20
07
UK
R
evie
w a
nd
inte
rven
tion
desc
riptio
n
The
pape
r dis
cuss
es c
urre
nt g
roup
educ
atio
n pr
ogra
mm
es a
vaila
ble
to
youn
g pe
ople
with
dia
bete
s and
pres
ents
a n
ew in
terv
entio
n.
Phas
e 1:
The
edu
catio
n
prog
ram
me
was
des
igne
d fo
r
use
with
gro
ups o
f bet
wee
n tw
o
and
six
indi
vidu
als a
ged
13–1
8
year
s, w
ith th
e ol
dest
par
ticip
ant
to d
ate
bein
g 17
yea
rs. W
ithou
t
exce
ptio
n, y
oung
peo
ple
wer
e
chan
ging
from
a re
gim
en o
f
mix
ed in
sulin
giv
en tw
ice
a da
y
befo
re b
reak
fast
and
bef
ore
even
ing
mea
l to
MD
I.
Phas
e 2:
Gro
ups o
f up
to 2
0
youn
g pe
ople
with
type
1
diab
etes
age
d 11
yea
rs a
nd o
ver
wer
e in
vite
d to
atte
nd tw
o
form
al e
duca
tion
sess
ions
, the
first
hel
d du
ring
the
sum
mer
holid
ay b
efor
e th
ey c
hang
ed to
seni
or sc
hool
and
the
seco
nd
arou
nd 2
–3 m
onth
s afte
r the
y
had
chan
ged
scho
ol.
Phas
e 1:
The
upt
ake
of th
ese
sess
ions
was
app
roxi
mat
ely
98 %
, mai
nly
beca
use
the
youn
g pe
ople
had
alre
ady
requ
este
d th
e ch
ange
to th
e ne
w re
gim
en
and
wer
e th
eref
ore
high
ly m
otiv
ated
to
atte
nd th
e se
ssio
ns.
Phas
e 2:
Var
ious
atte
ndan
ce le
vels
hav
e
been
seen
from
30–
80%
.
[no
furth
er in
form
atio
n on
the
sam
ple
or
parti
cipa
nts p
rovi
ded]
Page
46
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
18
24.
Deb
aty
et
al(2
4)
2008
Fr
ance
R
esea
rch
To a
sses
s qua
lity
of li
fe in
adu
lt ty
pe 1
diab
etic
pat
ient
s for
one
yea
r fol
low
ing
a ho
spita
l edu
catio
nal p
rogr
amm
e
Pros
pect
ive
sing
le-c
entre
stud
y
usin
g th
e D
QO
L sc
ale,
sent
by
post
and
com
plet
ed
anon
ymou
sly
by th
e pa
tient
s
befo
re th
e st
art o
f the
prog
ram
me,
and
thre
e, si
x an
d
12 m
onth
s afte
rwar
ds.
77 p
atie
nts i
nclu
ded
– 46
men
(60%
)
and
31 w
omen
(40%
), w
ith a
mea
n ag
e
36.9
±13.
5 ye
ars
25.
DeC
oste
r
&
Cum
min
gs
(25)
2005
U
S R
evie
w o
f
inte
rven
tions
To d
emon
stra
te th
e po
tent
ial o
f clin
ical
soci
al w
orke
rs to
mee
t psy
chos
ocia
l
need
s of a
dults
with
type
2 d
iabe
tes.
Thre
e da
taba
ses w
ere
sear
ched
for a
rticl
es o
n ev
iden
ce-b
ased
inte
rven
tions
or p
rogr
ams
appr
opria
te fo
r clin
ical
soci
al
wor
k in
dia
bete
s. 27
pap
ers
wer
e in
clud
ed in
the
revi
ew.
27 e
vide
nce-
base
d in
terv
entio
ns o
r
prog
ram
s app
ropr
iate
for c
linic
al so
cial
wor
k. V
arie
ty o
f sam
ples
incl
uded
in
each
of t
he st
udie
s.
Page
47
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
19
26.
Di B
attis
ta
et a
l.(26
)
2009
U
S an
d
Can
ada
Res
earc
h
To e
xam
ine
the
asso
ciat
ion
betw
een
soci
al a
nxie
ty a
nd a
dher
ence
to d
iabe
tes s
elf-
care
and
qual
ity o
f life
and
to d
eter
min
e th
e
effe
cts o
f fea
r of
hypo
glyc
emia
on
thes
e as
soci
atio
ns in
adol
esce
nts w
ith
type
1 d
iabe
tes.
Que
stio
nnai
res w
ere
adm
inis
tere
d: S
ocia
l anx
iety
scal
e fo
r ado
lesc
ents
, the
diab
etes
qua
lity
of li
fe sc
ale,
and
the
sum
mar
y of
dia
bete
s
self-
care
act
iviti
es
ques
tionn
aire
, and
the
hypo
glyc
aem
ia fe
ar su
rvey
.
Pear
son
corr
elat
ions
wer
e
com
pute
d to
test
the
hypo
thes
is
that
soci
al a
nxie
ty w
ould
resu
lt
in d
ecre
ased
adh
eren
ce a
nd
diab
etes
rela
ted
qual
ity o
f life
and
mul
tiple
regr
essi
ons w
ere
perf
orm
ed to
exa
min
e th
e
rela
tions
hip
betw
een
soci
al
anxi
ety
and
adhe
renc
e
beha
viou
rs.
Boy
s and
girl
s wer
e
com
pare
d on
thei
r lev
el o
f soc
ial
anxi
ety.
Seve
nty-
six
adol
esce
nts (
33 b
oys,
43
girls
), be
twee
n 13
-18
year
s of a
ge (
mea
n ag
e 15
.9 (1
.44)
yea
rs),
with
type
1
diab
etes
recr
uite
d fr
om 2
ped
iatri
c
outp
atie
nt c
linic
s in
Tenn
esse
e an
d
Toro
nto.
Page
48
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
20
27.
Dic
kins
on
&
O’R
eilly
(2
7)
2004
U
S R
esea
rch
To g
ain
a be
tter
unde
rsta
ndin
g of
wha
t it m
eans
for
adol
esce
nt
fem
ales
to li
ve w
ith ty
pe 1
dia
bete
s
Van
Man
en’s
phe
nom
enol
ogic
al
fram
ewor
k w
as
used
to g
uide
the
proj
ect o
f
inqu
iry. U
nstru
ctur
ed, o
ne-o
n-
one
inte
rvie
ws w
ere
cond
ucte
d
and
parti
cipa
nts’
acc
ount
s wer
e
trans
crib
ed a
nd a
naly
zed
for
them
es
10 a
dole
scen
t
fem
ales
, age
d 16
and
17
year
s, w
ith ty
pe
1 di
abet
es re
crui
ted
from
a d
iabe
tes
cam
p.
Page
49
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e

21
28.
Doe
(28)
20
16
UK
R
esea
rch
To in
vest
igat
e ho
w th
e ty
pe o
f sup
port
prov
ided
by
peer
s may
mod
erat
e th
e
rela
tions
hips
bet
wee
n pe
er su
ppor
t and
diab
etes
out
com
es
A c
ross
-sec
tiona
l res
earc
h
desi
gn is
util
ised
. Par
ticip
ants
wer
e as
ked
to c
ompl
ete
a
ques
tionn
aire
bat
tery
whi
ch
incl
uded
the
Ber
lin S
ocia
l
Supp
ort S
cale
, the
Dia
bete
s
Soci
al S
uppo
rt Q
uest
ionn
aire
-
Frie
nds V
ersi
on, t
he S
elf-
Car
e
Inve
ntor
y –R
evis
ed.
A re
cent
mea
sure
of H
bA1c
was
als
o
take
n.
Line
ar re
gres
sion
s wer
e us
ed to
look
at t
he im
pact
of g
loba
l pee
r
supp
ort o
n se
lf-ca
re, g
lyca
emic
cont
rol,;
dia
bete
s spe
cific
supp
ort,
self-
care
and
gly
caem
ic
cont
rol.
Fina
lly, t
hose
with
hig
h
vers
us lo
w H
BA
1c w
ere
com
pare
d on
thei
r lev
els o
f
soci
al su
ppor
t.
90 p
artic
ipan
ts, a
ged
15–1
8 ye
ars a
nd
wer
e re
crui
ted
from
two
gene
ral
hosp
itals
in E
ngla
nd. T
here
wer
e 37
mal
es a
nd 5
3 fe
mal
es.
Page
50
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
22
29.
Doh
erty
&
Dov
ey-
Pear
ce(2
9)
2005
U
K
Res
earc
h
(Rev
iew
(?) )
To p
rovi
de a
brie
f ove
rvie
w o
f rec
ent
rese
arch
into
the
impa
ct o
f dia
bete
s upo
n
adol
esce
nt d
evel
opm
ent a
nd th
e
spec
ific
psyc
holo
gica
l
diff
icul
ties a
ssoc
iate
d w
ith d
iabe
tes.
n/a
n/a
30.
Dov
ey-
Pear
ce e
t
al(3
0)
2005
U
K
Res
earc
h To
des
crib
e an
d un
ders
tand
the
cons
ider
ed o
pini
ons o
f 19
youn
g ad
ults
with
dia
bete
s who
wer
e re
ceiv
ing
seco
ndar
y ca
re se
rvic
es a
bout
the
prov
isio
n of
dia
bete
s ser
vice
s for
you
ng
peop
le.
Qua
litat
ive
user
invo
lvem
ent
stud
y us
ing
sem
i-stru
ctur
ed
inte
rvie
ws a
nd a
focu
s gro
up
with
serv
ice
user
s.
n =
19; m
ale
n =
8; fe
mal
e n
= 11
; age
rang
e =
16–
25 y
ears
; mea
n ag
e =
19.9
year
s; S
D ±
3.1
2 ye
ars
31.
Dov
ey-
Pear
ce e
t
al.(3
1)
2007
U
K
Res
earc
h Fi
rst,
to d
escr
ibe
and
unde
rsta
nd th
e
influ
ence
of d
iabe
tes u
pon
psyc
hoso
cial
deve
lopm
ent a
nd se
cond
, to
high
light
the
impl
icat
ions
for h
ealth
care
team
s.
Qua
litat
ive
sem
i-stru
ctur
ed
inte
rvie
ws w
ere
used
.
Peop
le a
ged
16–2
5 re
gist
ered
with
one
seco
ndar
y ca
re d
iabe
tes s
ervi
ce,
acro
ss tw
o di
stric
ts in
nor
th-e
ast
Engl
and
wer
e co
ntac
ted.
Nin
etee
n
inte
rvie
ws w
ere
cond
ucte
d an
d an
alys
ed u
sing
a
Fram
ewor
k A
ppro
ach.
32.
Dov
ey-
Pear
ce(3
2)
2015
U
K
Com
men
tary
To
con
tribu
te to
deb
ates
abo
ut
impr
ovin
g ca
re fo
r you
ng p
eopl
e.
n/a
n/a
Page
51
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
23
33.
Due
-
Chr
isten
se
n et
al(3
3)
2011
D
enm
ark
Res
earc
h To
test
whe
ther
pat
ient
s with
Typ
e 1
diab
etes
wou
ld jo
in su
ppor
t gro
ups a
nd
bene
fit b
y im
prov
ing
psyc
hoso
cial
func
tioni
ng, r
egar
dles
s of t
heir
HbA
1c
leve
ls.
Con
curr
ent m
ixed
met
hods
stud
y.
Self-
repo
rted
psyc
hoso
cial
func
tioni
ng a
nd H
BA
1c w
ere
mea
sure
d at
the
begi
nnin
g an
d
end
of th
e su
ppor
t gro
up a
nd a
t
6- a
nd 1
2-m
onth
follo
w-u
p. A
t
the
last
sess
ion,
the
patie
nts
answ
ered
five
ope
n-en
ded
ques
tions
abo
ut th
eir p
erce
ptio
n
of th
e fo
rmat
and
out
com
e of
the
inte
rven
tion.
Afte
r eac
h
supp
ort g
roup
, a fo
cus g
roup
inte
rvie
w w
as c
ondu
cted
betw
een
1 w
eek
and
2 m
onth
s
afte
r the
last
sess
ion.
Con
veni
ence
sam
ple
n= 5
4 pa
tient
s (43
wom
en a
nd 1
1 m
en).
The
mea
n ag
e of
the
parti
cipa
nts w
as
43.8
(10.
5) y
ears
34.
Ede
lman
et a
l(34)
Syst
emat
ic
revi
ew
To su
mm
ariz
e th
e ef
fect
s of S
hare
d
Med
ical
App
oint
men
ts (S
MA
s) o
n
staf
f, pa
tient
, and
eco
nom
ic o
utco
mes
and
to e
valu
ate
whe
ther
the
impa
ct
varie
d by
clin
ical
con
ditio
n or
spec
ific
inte
rven
tion
com
pone
nts.
25 a
rticl
es w
ere
incl
uded
in th
e
revi
ew.
16 st
udie
s eva
luat
ed S
MA
inte
rven
tions
in p
atie
nts w
ith d
iabe
tes m
ellit
us a
nd 3
eval
uate
d SM
As i
n ol
der a
dults
with
high
util
izat
ion
of m
edic
al re
sour
ces.
Page
52
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
24
35.
Elli
s et
al.(3
5)
2016
U
K
Syst
emat
ic
revi
ew
The
revi
ew a
ddre
ssed
the
follo
win
g
ques
tion:
‘Wha
t are
ado
lesc
ents
’ vie
ws
or e
xper
ienc
es o
f liv
ing
with
type
1
diab
etes
?’
Five
dat
abas
es se
arch
ed fo
r
rele
vant
arti
cles
bet
wee
n 20
04-
2014
, with
8 p
aper
s inc
lude
d in
the
revi
ew a
nd fi
ndin
gs
pres
ente
d in
nar
rativ
e fo
rm.
Ado
lesc
ents
with
dia
bete
s typ
e 1
aged
13-1
7 ye
ars,
alth
ough
som
e st
udie
s
incl
uded
par
ticip
ants
age
d 11
-18
year
s.
36.
Elw
yn e
t
al(3
6)
2001
U
K
Boo
k A
ims t
o pr
ovid
e a
prac
tical
gui
de to
smal
l gro
up w
ork
in o
rgan
isat
iona
l,
educ
atio
nal a
nd re
sear
ch se
tting
s.
n/a
n/a
37.
Ers
ig e
t
al.(3
7)
2015
U
S R
esea
rch
The
purp
ose
of th
is st
udy
was
to
iden
tify
stre
ssor
s of t
eens
with
Typ
e 1
diab
etes
(T1D
M) a
nd th
eir p
aren
ts
rela
ted
to th
e im
pend
ing
trans
ition
to
adul
thoo
d.
Qua
litat
ive
inte
rvie
win
g. O
pen
ende
d qu
estio
ns w
ere
aske
d to
iden
tify
ever
y da
y an
d ill
ness
-
rela
ted
stre
ssor
s am
ong
teen
ager
s with
Typ
e 1
diab
etes
and
thei
r par
ents
. Qua
litat
ive
desc
riptiv
e an
alys
is id
entif
ied
them
es in
inte
rvie
w tr
ansc
ripts
15 te
ens w
ith T
1DM
and
25
pare
nts s
een
in o
ne p
aedi
atric
dia
bete
s clin
ic.
Page
53
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
25
38.
Fern
ande
s
et a
l.(38
)
2014
U
S R
esea
rch
To
det
erm
ine
patie
nts’
and
par
ents
’
perc
eptio
ns re
gard
ing
the
deliv
ery
of
trans
ition
edu
catio
n an
d pe
rcei
ved
barr
iers
to tr
ansf
er to
adu
lt or
ient
ed
care
.
Self-
repo
rt su
rvey
(30
mul
tiple
choi
ce a
nd o
ne fr
ee re
spon
se
ques
tion)
. Par
ent a
nd p
atie
nt
resp
onse
s wer
e co
mpa
red.
Con
tent
ana
lysi
s was
em
ploy
ed
for t
he fr
ee re
spon
se q
uest
ion.
155
16–2
5 ye
ars o
ld w
ith v
ario
us
child
hood
ons
et c
hron
ic d
isea
ses
(con
veni
ence
sam
ple)
and
thei
r
pare
nts/
guar
dian
s (10
4).
39.
Fitz
patr
ick
et a
l(39)
2013
U
S Sy
stem
atic
revi
ew
To e
xam
ine
the
publ
ishe
d lit
erat
ure
on
the
effe
ct o
f pro
blem
-sol
ving
inte
rven
tions
on
diab
etes
self-
man
agem
ent a
nd d
isea
se c
ontro
l.
Two
data
base
s wer
e se
arch
ed
and
the
auth
ors f
ollo
wed
cita
tions
from
refe
renc
e lis
ts.
Twen
ty-f
our s
tudi
es m
et
incl
usio
n cr
iteria
.
Adu
lt an
d ch
ildre
n po
pula
tions
,
incl
udin
g m
ultie
thni
c sa
mpl
es o
r
raci
al/e
thni
c m
inor
ities
Page
54
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
26
40.
Floy
d et
al(4
0)
2016
U
SA
Res
earc
h To
det
erm
ine
whe
ther
shar
ed m
edic
al
appo
intm
ents
(SM
As)
with
mul
ticom
pone
nt in
terv
entio
ns u
tilis
ing
mul
tidis
cipl
inar
y te
ams,
impr
ove
glyc
aem
ic c
ontro
l and
psy
chos
ocia
l
outc
omes
in p
oorly
con
trolle
d
adol
esce
nt ty
pe 1
dia
bete
s.
In th
is p
ilot s
tudy
, gro
ups o
f 3-6
subj
ects
and
thei
r fam
ilies
cam
e
toge
ther
to 3
SM
As a
nd 1
indi
vidu
al a
ppoi
ntm
ent e
very
3
mon
ths o
ver a
9 m
onth
per
iod.
Gro
up se
ssio
n co
nten
t was
guid
ed b
y pa
rtici
pant
s and
pee
r
supp
ort e
nabl
ed th
roug
h
disc
ussi
on. S
tatis
tical
ana
lysi
s
look
ed a
t QO
L, a
dher
ence
and
retro
spec
tive
and
pros
pect
ive
glyc
aem
ic c
ontro
l as o
utco
me
mea
sure
s.
37 su
bjec
ts e
nrol
led
and
32 c
ompl
eted
3
of 4
vis
its. S
ubje
cts w
ere
aged
bet
wee
n
12-1
6 (m
ean
13.7
± 1.
1)ye
ars w
ith ty
pe 1
diab
etes
for ≥
1 y
ear a
nd a
HbA
1c 0
f
7.5-
11%
Page
55
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
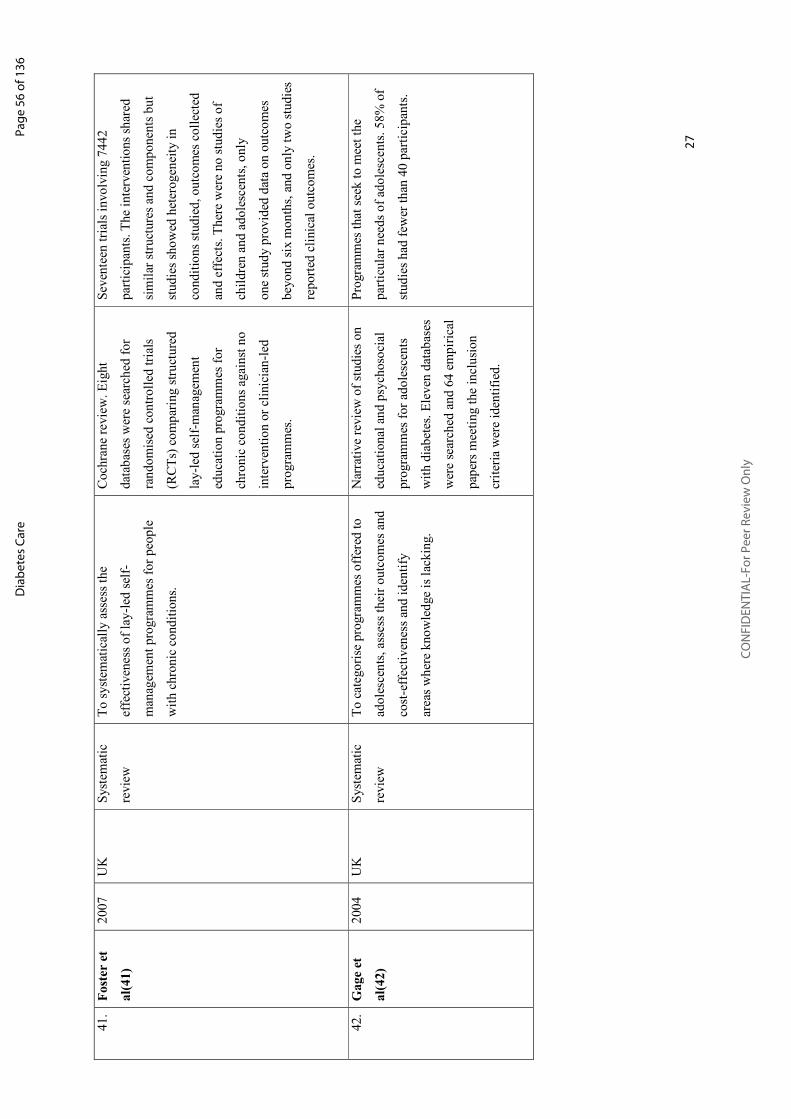
27
41.
Fost
er e
t
al(4
1)
2007
U
K
Syst
emat
ic
revi
ew
To sy
stem
atic
ally
ass
ess t
he
effe
ctiv
enes
s of l
ay-le
d se
lf-
man
agem
ent p
rogr
amm
es fo
r peo
ple
with
chr
onic
con
ditio
ns.
Coc
hran
e re
view
. Eig
ht
data
base
s wer
e se
arch
ed fo
r
rand
omis
ed c
ontro
lled
trial
s
(RC
Ts) c
ompa
ring
stru
ctur
ed
lay-
led
self-
man
agem
ent
educ
atio
n pr
ogra
mm
es fo
r
chro
nic
cond
ition
s aga
inst
no
inte
rven
tion
or c
linic
ian-
led
prog
ram
mes
.
Seve
ntee
n tri
als i
nvol
ving
744
2
parti
cipa
nts.
The
inte
rven
tions
shar
ed
sim
ilar s
truct
ures
and
com
pone
nts b
ut
stud
ies s
how
ed h
eter
ogen
eity
in
cond
ition
s stu
died
, out
com
es c
olle
cted
and
effe
cts.
Ther
e w
ere
no st
udie
s of
child
ren
and
adol
esce
nts,
only
one
stud
y pr
ovid
ed d
ata
on o
utco
mes
beyo
nd si
x m
onth
s, an
d on
ly tw
o st
udie
s
repo
rted
clin
ical
out
com
es.
42.
Gag
e et
al(4
2)
2004
U
K
Syst
emat
ic
revi
ew
To c
ateg
oris
e pr
ogra
mm
es o
ffer
ed to
adol
esce
nts,
asse
ss th
eir o
utco
mes
and
cost
-eff
ectiv
enes
s and
iden
tify
area
s whe
re k
now
ledg
e is
lack
ing.
Nar
rativ
e re
view
of s
tudi
es o
n
educ
atio
nal a
nd p
sych
osoc
ial
prog
ram
mes
for a
dole
scen
ts
with
dia
bete
s. El
even
dat
abas
es
wer
e se
arch
ed a
nd 6
4 em
piric
al
pape
rs m
eetin
g th
e in
clus
ion
crite
ria w
ere
iden
tifie
d.
Prog
ram
mes
that
seek
to m
eet t
he
parti
cula
r nee
ds o
f ado
lesc
ents
. 58%
of
stud
ies h
ad fe
wer
than
40
parti
cipa
nts.
Page
56
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
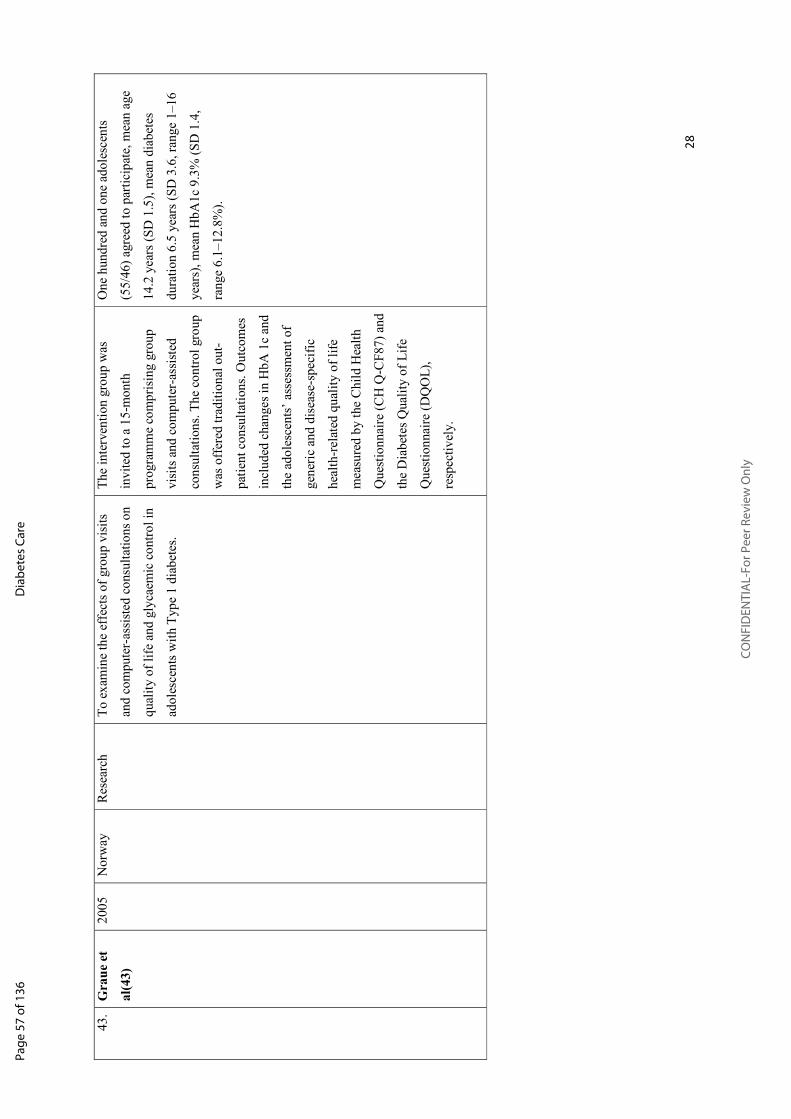
28
43.
Gra
ue e
t
al(4
3)
2005
N
orw
ay
Res
earc
h To
exa
min
e th
e ef
fect
s of g
roup
vis
its
and
com
pute
r-as
sist
ed c
onsu
ltatio
ns o
n
qual
ity o
f life
and
gly
caem
ic c
ontro
l in
adol
esce
nts w
ith T
ype
1 di
abet
es.
The
inte
rven
tion
grou
p w
as
invi
ted
to a
15-
mon
th
prog
ram
me
com
pris
ing
grou
p
visi
ts a
nd c
ompu
ter-
assi
sted
cons
ulta
tions
. The
con
trol g
roup
was
off
ered
trad
ition
al o
ut-
patie
nt c
onsu
ltatio
ns. O
utco
mes
incl
uded
cha
nges
in H
bA 1
c an
d
the
adol
esce
nts’
ass
essm
ent o
f
gene
ric a
nd d
isea
se-s
peci
fic
heal
th-r
elat
ed q
ualit
y of
life
mea
sure
d by
the
Chi
ld H
ealth
Que
stio
nnai
re (C
H Q
-CF8
7) a
nd
the
Dia
bete
s Qua
lity
of L
ife
Que
stio
nnai
re (D
QO
L),
resp
ectiv
ely.
One
hun
dred
and
one
ado
lesc
ents
(55/
46) a
gree
d to
par
ticip
ate,
mea
n ag
e
14.2
yea
rs (S
D 1
.5),
mea
n di
abet
es
dura
tion
6.5
year
s (SD
3.6
, ran
ge 1
–16
year
s), m
ean
HbA
1c 9
.3%
(SD
1.4
,
rang
e 6.
1–12
.8%
).
Page
57
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
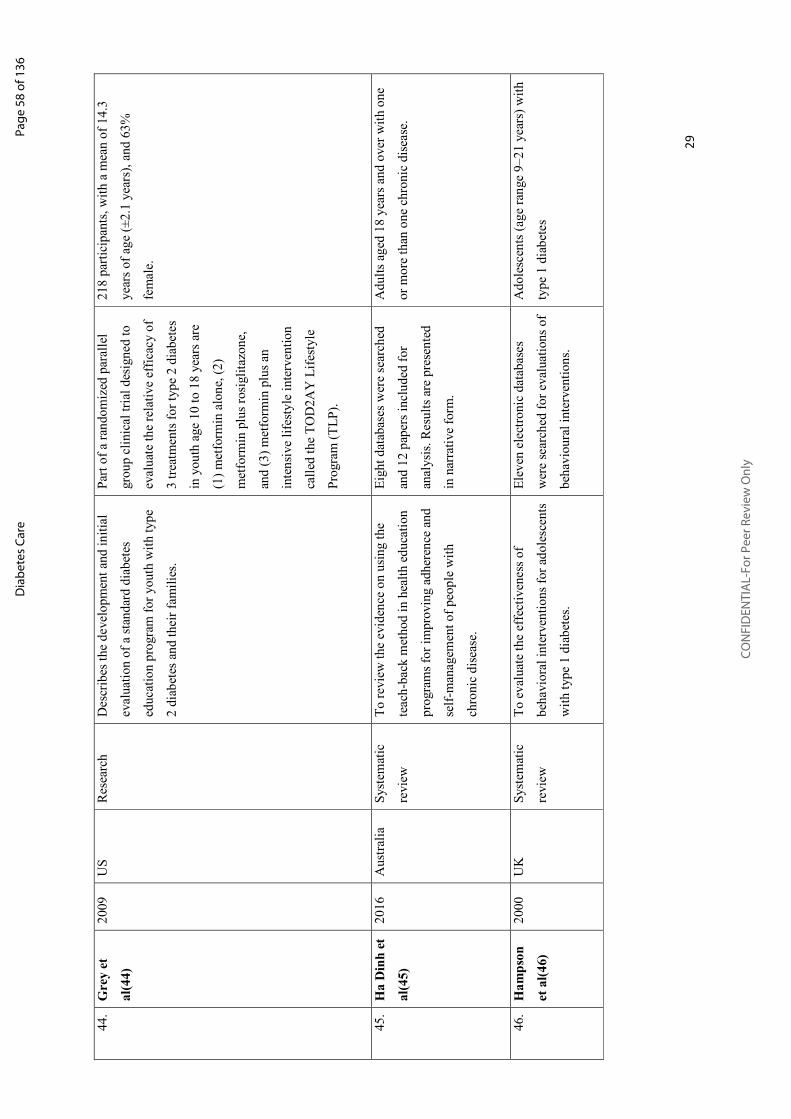
29
44.
Gre
y et
al(4
4)
2009
U
S R
esea
rch
D
escr
ibes
the
deve
lopm
ent a
nd in
itial
eval
uatio
n of
a st
anda
rd d
iabe
tes
educ
atio
n pr
ogra
m fo
r you
th w
ith ty
pe
2 di
abet
es a
nd th
eir f
amili
es.
Part
of a
rand
omiz
ed p
aral
lel
grou
p cl
inic
al tr
ial d
esig
ned
to
eval
uate
the
rela
tive
effic
acy
of
3 tre
atm
ents
for t
ype
2 di
abet
es
in y
outh
age
10
to 1
8 ye
ars a
re
(1) m
etfo
rmin
alo
ne, (
2)
met
form
in p
lus r
osig
litaz
one,
and
(3) m
etfo
rmin
plu
s an
inte
nsiv
e lif
esty
le in
terv
entio
n
calle
d th
e TO
D2A
Y L
ifest
yle
Prog
ram
(TLP
).
218
parti
cipa
nts,
with
a m
ean
of 1
4.3
year
s of a
ge (±
2.1
year
s), a
nd 6
3%
fem
ale.
45.
Ha
Din
h et
al(4
5)
2016
A
ustra
lia
Syst
emat
ic
revi
ew
To re
view
the
evid
ence
on
usin
g th
e
teac
h-ba
ck m
etho
d in
hea
lth e
duca
tion
prog
ram
s for
impr
ovin
g ad
here
nce
and
self-
man
agem
ent o
f peo
ple
with
chro
nic
dise
ase.
Eigh
t dat
abas
es w
ere
sear
ched
and
12 p
aper
s inc
lude
d fo
r
anal
ysis
. Res
ults
are
pre
sent
ed
in n
arra
tive
form
.
Adu
lts a
ged
18 y
ears
and
ove
r with
one
or m
ore
than
one
chr
onic
dis
ease
.
46.
Ham
pson
et a
l(46)
2000
U
K
Syst
emat
ic
revi
ew
To e
valu
ate
the
effe
ctiv
enes
s of
beha
vior
al in
terv
entio
ns fo
r ado
lesc
ents
with
type
1 d
iabe
tes.
Elev
en e
lect
roni
c da
taba
ses
wer
e se
arch
ed fo
r eva
luat
ions
of
beha
viou
ral i
nter
vent
ions
.
Ado
lesc
ents
(age
rang
e 9–
21 y
ears
) with
type
1 d
iabe
tes
Page
58
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
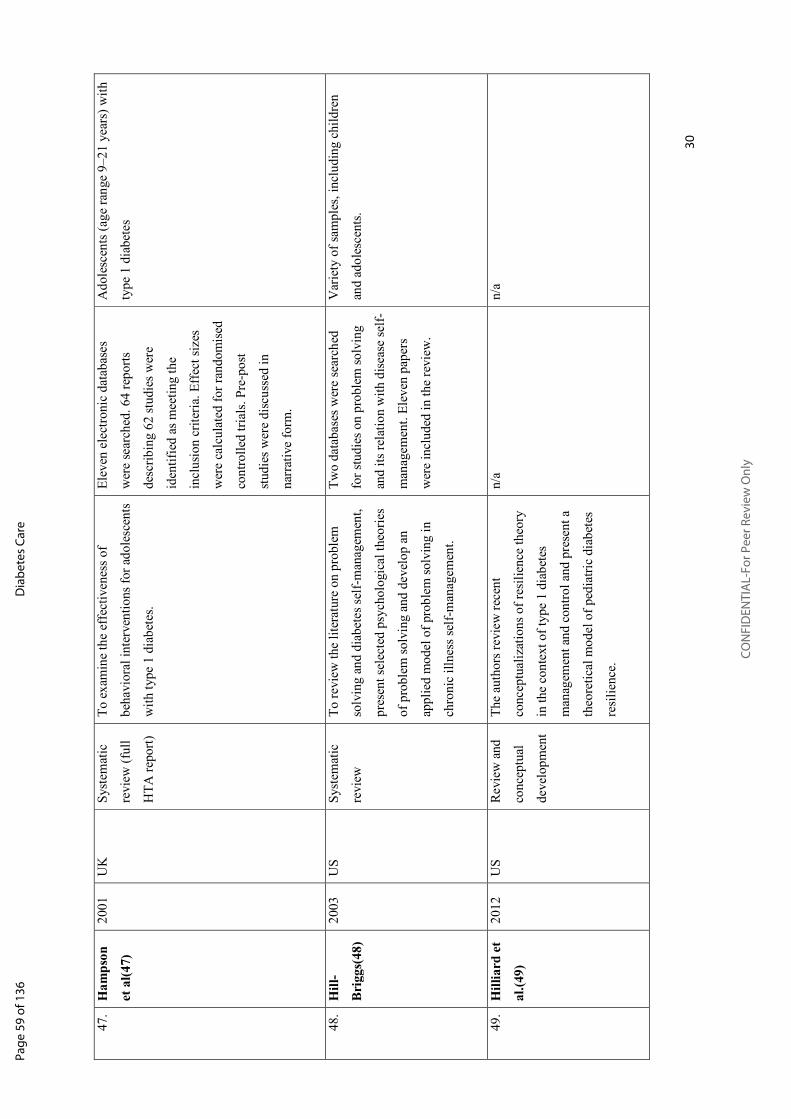
30
47.
Ham
pson
et a
l(47)
2001
U
K
Syst
emat
ic
revi
ew (f
ull
HTA
repo
rt)
To e
xam
ine
the
effe
ctiv
enes
s of
beha
vior
al in
terv
entio
ns fo
r ado
lesc
ents
with
type
1 d
iabe
tes.
Elev
en e
lect
roni
c da
taba
ses
wer
e se
arch
ed. 6
4 re
ports
desc
ribin
g 62
stud
ies w
ere
iden
tifie
d as
mee
ting
the
incl
usio
n cr
iteria
. Eff
ect s
izes
wer
e ca
lcul
ated
for r
ando
mis
ed
cont
rolle
d tri
als.
Pre-
post
stud
ies w
ere
disc
usse
d in
narr
ativ
e fo
rm.
Ado
lesc
ents
(age
rang
e 9–
21 y
ears
) with
type
1 d
iabe
tes
48.
Hill
-
Bri
ggs(
48)
2003
U
S Sy
stem
atic
revi
ew
To re
view
the
liter
atur
e on
pro
blem
solv
ing
and
diab
etes
self-
man
agem
ent,
pres
ent s
elec
ted
psyc
holo
gica
l the
orie
s
of p
robl
em so
lvin
g an
d de
velo
p an
appl
ied
mod
el o
f pro
blem
solv
ing
in
chro
nic
illne
ss se
lf-m
anag
emen
t.
Two
data
base
s wer
e se
arch
ed
for s
tudi
es o
n pr
oble
m so
lvin
g
and
its re
latio
n w
ith d
isea
se se
lf-
man
agem
ent.
Elev
en p
aper
s
wer
e in
clud
ed in
the
revi
ew.
Var
iety
of s
ampl
es, i
nclu
ding
chi
ldre
n
and
adol
esce
nts.
49.
Hill
iard
et
al.(4
9)
2012
U
S R
evie
w a
nd
conc
eptu
al
deve
lopm
ent
The
auth
ors r
evie
w re
cent
conc
eptu
aliz
atio
ns o
f res
ilien
ce th
eory
in th
e co
ntex
t of t
ype
1 di
abet
es
man
agem
ent a
nd c
ontro
l and
pre
sent
a
theo
retic
al m
odel
of p
edia
tric
diab
etes
resi
lienc
e.
n/a
n/a
Page
59
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
31
50.
Hill
iard
et
al(5
0)
2016
U
S R
evie
w o
f
inte
rven
tions
The
pape
r sum
mar
izes
the
evid
ence
base
for e
stab
lishe
d di
abet
es sk
ills
train
ing
prog
ram
s, fa
mily
inte
rven
tions
,
and
mul
tisys
tem
ic in
terv
entio
ns, a
nd
intro
duce
s em
ergi
ng e
vide
nce
for
tech
nolo
gy a
nd m
obile
hea
lth
inte
rven
tions
and
hea
lth c
are
deliv
ery
syst
em in
terv
entio
ns.
Des
crip
tive
over
view
of
inte
rven
tions
Chi
ldre
n an
d ad
oles
cent
s with
Typ
e 1
diab
etes
(T1D
) and
Typ
e 2
diab
etes
(T2D
) and
thei
r fam
ilies
.
51.
Hin
der
&
Gre
enha
lg
h(51
)
2012
U
K
Res
earc
h To
pro
duce
a ri
cher
und
erst
andi
ng o
f
how
peo
ple
live
with
dia
bete
s and
why
self-
man
agem
ent i
s cha
lleng
ing
for
som
e.
Ethn
ogra
phic
stud
y
supp
lem
ente
d w
ith b
ackg
roun
d
docu
men
ts o
n so
cial
con
text
.
Parti
cipa
nts w
ere
shad
owed
at
hom
e an
d in
the
com
mun
ity fo
r
2-4
perio
ds o
f sev
eral
hou
rs
inte
rvie
wed
(som
etim
es w
ith a
fam
ily m
embe
r or c
arer
) abo
ut
thei
r sel
f-m
anag
emen
t eff
orts
and
supp
ort n
eeds
; and
take
n ou
t
for a
mea
l. D
etai
led
field
not
es
wer
e m
ade
and
anno
tate
d. D
ata
anal
ysis
was
info
rmed
by
stru
ctur
atio
n th
eory
.
30 p
eopl
e w
ith d
iabe
tes (
15 ty
pe 1
, 15
type
2),
aged
5-8
8, fr
om a
rang
e of
ethn
ic
and
soci
o-ec
onom
ic g
roup
s
Page
60
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
32
52.
Hod
dino
tt
et a
l(52)
2010
U
K
Res
earc
h To
pro
pose
a fr
amew
ork
for t
he d
esig
n
and
proc
ess e
valu
atio
n of
hea
lth
impr
ovem
ent i
nter
vent
ions
occ
urrin
g in
a gr
oup
setti
ng to
ass
ist p
ract
ition
ers,
rese
arch
ers a
nd p
olic
y m
aker
s.
Bas
ed o
n te
am e
xper
ienc
es o
f
cond
uctin
g sy
stem
atic
revi
ews,
inte
rven
tion,
mix
ed m
etho
d an
d
ethn
ogra
phic
stud
ies o
f gro
ups
for b
reas
tfeed
ing
and
wei
ght
man
agem
ent a
nd a
lite
ratu
re
revi
ew, a
fram
ewor
k fo
r hea
lth
impr
ovem
ent g
roup
des
ign
and
deliv
ery
evol
ved.
The
fram
ewor
k w
as d
evel
oped
usi
ng
stud
ies t
he te
am h
ad b
een
invo
lved
in.
53.
Hou
sden
&
Won
g(53
)
2016
Syst
emat
ic
revi
ew
(upd
ate)
To id
entif
y as
soci
atio
n be
twee
n
deliv
ery
of g
roup
med
ical
vis
its
(GM
Vs)
and
phy
siol
ogic
, sel
f-ca
re a
nd
syst
em o
utco
mes
.
8 da
taba
ses w
ere
sear
ched
and
33 a
rticl
es w
ere
incl
uded
in th
e
revi
ew
Patie
nts a
ged
16–8
0 ye
ars w
ith ty
pe 1
or
2 di
abet
es.
54.
Hou
sden
et
al(5
4)
2013
Syst
emat
ic
revi
ew
To a
sses
s the
eff
ectiv
enes
s of g
roup
visi
ts fo
r pat
ient
s with
dia
bete
s.
Syst
emat
ic re
view
and
met
a-
anal
ysis
– 8
dat
abas
es w
ere
sear
ched
and
26
stud
ies w
ere
incl
uded
in th
e re
view
.
Patie
nts a
ged
16–8
0 ye
ars w
ith ty
pe 1
or
2 di
abet
es.
Page
61
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
33
55.
Hyn
es e
t
al.(5
5)
2015
Ir
elan
d R
esea
rch
To d
evel
op a
theo
ry e
xpla
inin
g
atte
ndan
ce o
f you
ng a
dults
at a
hosp
ital-b
ased
dia
bete
s clin
ic
Inte
rvie
ws c
ondu
cted
with
youn
g pe
ople
with
dia
bete
s and
thei
r ser
vice
pro
vide
rs.
Inte
rvie
ws w
ere
audi
o-re
cord
ed,
trans
crib
ed a
nd a
naly
sed
acco
rdin
g to
gro
unde
d th
eory
met
hodo
logy
.
You
ng a
dults
(21)
with
type
1 d
iabe
tes
and
serv
ice
prov
ider
s (8)
from
one
hosp
ital-b
ased
dia
bete
s clin
ic
56.
Hyn
es e
t
al(5
6)
2016
Ir
elan
d Sy
stem
atic
revi
ew
To sy
nthe
sise
find
ings
on
barr
iers
and
faci
litat
ors t
o cl
inic
atte
ndan
ce a
mon
g
youn
g ad
ults
(15–
30 y
ears
) with
type
1
diab
etes
.
Four
ele
ctro
nic
data
base
s wer
e
sear
ched
and
a to
tal 1
2 st
udie
s
met
the
incl
usio
n cr
iteria
.
Find
ings
are
pre
sent
ed in
the
form
of n
arra
tive
synt
hesi
s.
You
ng a
dults
(15–
30 y
ears
) with
type
1
diab
etes
mel
litus
.
Page
62
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
34
57.
Jabe
r et
al(5
7)
2006
U
SA
Res
earc
h Su
mm
ary
of c
urre
nt g
roup
vis
it
rese
arch
and
dev
elop
men
t of
sugg
estio
ns fo
r fur
ther
ing
this
car
e
mod
el.
Syst
emat
ic, e
lect
roni
c re
view
of
the
liter
atur
e, 1
974
– 20
04 v
ia
PubM
ed a
nd M
edlin
e da
taba
ses.
Furth
er a
rticl
es w
ere
obta
ined
by re
view
ing
bibl
iogr
aphi
es o
f
artic
les g
athe
red
thro
ugh
the
data
base
sear
ch. T
he q
ualit
ativ
e
revi
ew w
as o
rgan
ised
by
sequ
entia
lly d
escr
ibin
g th
e
effe
ct o
f all
revi
ewed
inte
rven
tions
on
each
of t
he
follo
win
g he
alth
out
com
es (i
f
mea
sure
d): p
atie
nt sa
tisfa
ctio
n,
heal
th se
rvic
es u
tiliz
atio
n,
qual
ity o
f car
e, h
ealth
beha
viou
rs, p
hysi
cal
func
tion
/dep
ress
ion
/qua
lity
of
life,
dis
ease
-spe
cific
out
com
es,
phys
icia
n sa
tisfa
ctio
n, a
nd c
ost
of c
are.
16 p
aper
s inc
ludi
ng p
rosp
ectiv
e
obse
rvat
iona
l
stud
ies a
nd ra
ndom
ized
con
trolle
d
clin
ical
trial
s.
Page
63
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
35
58.
Jabe
r et
al(5
8)
2006
U
SA
Res
earc
h To
des
crib
e cu
rren
t gro
up v
isit
mod
els
and
to d
iscu
ss th
e un
ique
adv
anta
ges
and
chal
leng
es g
roup
vis
its p
rese
nt fo
r
phys
icia
ns b
ased
on
four
-yea
r
expe
rienc
e.
Des
crip
tion
of lo
cally
dev
elop
ed
grou
p vi
sit p
rogr
ams f
or a
sthm
a,
oste
opor
osis
and
lipi
ds
man
agem
ent.
Cha
lleng
es
iden
tifie
d in
clud
ed: 1
) bill
ing
2)
wai
ting
time
and
patie
nt fl
ow 3
)
conf
iden
tialit
y 4)
dro
pout
rate
s.
≥ 24
0 pa
tient
s (m
ostly
fem
ale
in th
eir
mid
-50’
s)
Page
64
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
36
59.
Kee
rs J
et
al(5
9)
2004
Th
e
Net
herla
nd
s
Res
earc
h To
det
erm
ine
the
effe
ct o
f the
Mul
tidis
cipl
inar
y In
tens
ive
Educ
atio
n
Prog
ram
(MIE
P) o
n gl
ycae
mic
con
trol
and
qual
ity o
f life
and
gai
n in
sigh
t int
o
the
mec
hani
sms o
f eff
ect.
This
pilo
t stu
dy to
ok 5
1 pa
tient
s
thro
ugh
the
MIE
P ov
er 1
2 da
ys
with
gro
up se
ssio
ns a
nd
indi
vidu
al c
ouns
ellin
g
faci
litat
ed b
y th
e di
abet
es
educ
atio
n te
am.
Prim
ary
outc
ome
varia
bles
wer
e
glyc
aem
ic c
ontro
l (H
BA
1c) a
nd
qual
ity o
f life
mea
sure
d w
ith th
e
RA
BN
D-3
6 sc
ale.
The
Dia
bete
s
Sym
ptom
Che
cklis
t (D
SC)
mea
sure
d di
abet
es re
late
d
sym
ptom
s and
a D
utch
ver
sion
of th
e he
alth
locu
s of c
ontro
l
scal
e w
ere
used
alo
ng w
ith th
e
num
ber o
f sev
ere
hypo
glyc
aem
ic o
ccur
renc
es to
asse
ss se
cond
ary
outc
omes
. The
data
was
anl
ysis
ed u
sing
pai
red
T-te
sts a
nd re
gres
sion
ana
lysi
s.
58 p
atie
nts,
18-7
0 ye
ars (
mea
n 49
.10)
enro
lled
and
51 p
atie
nts c
ompl
eted
the
prog
ram
and
wer
e ev
alua
ted.
To
fit th
e
crite
ria H
BA
1c h
ad to
be>
7.5%
for a
t
leas
t a y
ear a
nd/o
r fre
quen
t or s
ever
e
hypo
glyc
aem
ia a
nd/o
r psy
chos
ocia
l
limita
tions
resu
lting
from
dia
bete
s.
Sele
ctio
n w
as b
ased
on
med
ical
repo
rts
and
an a
dmis
sion
inte
rvie
w
Page
65
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
37
60.
Kee
rs J
et
al(6
0)
2006
Th
e
Net
herla
nd
s
Res
earc
h Th
e st
udy
has 2
aim
s. 1)
to d
eter
min
e
the
effe
cts o
f the
Mul
tidis
cipl
inar
y
Inte
nsiv
e ed
ucat
ion
Prog
ram
(MIE
P) o
n
glyc
aem
ic c
ontro
l, H
r-Q
ol a
nd in
faci
litat
ors o
f em
pow
erm
ent (
i.e.
copi
ng a
nd a
ttrib
utio
n of
con
trol o
ver
diab
etes
), im
med
iate
ly a
fter t
he
inte
rven
tion
and
at a
1 y
ear f
ollo
w u
p.
2) to
det
erm
ine
whe
ther
inte
nded
incr
ease
s in
empo
wer
men
t are
rela
ted
to a
pos
itive
HB
A1c
and
Hr-
Qol
outc
omes
dire
ctly
afte
r MIE
P an
d at
1
year
follo
w u
p.
MIE
P w
as m
ade
up o
f 10
days
of g
roup
sess
ions
(6-9
patie
nts/
grou
p) a
nd so
me
indi
vidu
al su
ppor
t. Fo
llow
up
visi
ts ta
ke p
lace
at 6
wee
ks, 1
2
wee
ks a
nd 1
yea
r. Pa
rtici
pant
s
in th
e pr
ogra
m c
ompl
eted
a
base
line
asse
ssm
ent a
nd h
ad
thei
r firs
t mea
sure
men
ts ta
ken
follo
win
g a
succ
essf
ul
adm
issi
on in
terv
iew
. Fol
low
up
ques
tionn
aire
s wer
e m
aile
d to
parti
cipa
nts a
t 3m
onth
s and
1
year
. The
dat
a w
as a
nlys
ised
usin
g in
depe
nden
t T-te
sts a
nd
regr
essi
on a
naly
sis.
99 p
atie
nts c
ompl
eted
MIE
P an
d 23
1
non-
refe
rred
out
patie
nts c
onse
nted
to
prov
ide
refe
renc
e va
lues
.
Page
66
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
38
61.
Keo
ugh
et
al.(6
1)
2011
U
S R
esea
rch
Th
e pu
rpos
e of
this
stud
y w
as to
exam
ine
diff
eren
ces i
n se
lf-
man
agem
ent b
ehav
iors
(Col
labo
ratio
n
with
Par
ents
,Dia
bete
s Car
e A
ctiv
ities
,
Dia
bete
s Pro
blem
Sol
ving
, Dia
bete
s
Com
mun
icat
ion,
and
Goa
ls) b
etw
een
early
, mid
dle,
and
late
ado
lesc
ence
. The
role
of r
egim
en a
nd g
ende
r as
cova
riate
s in
self-
man
agem
ent
beha
vior
s was
als
o ex
amin
ed.
Seco
ndar
y an
alys
is o
n
dem
ogra
phic
, illn
ess-
rela
ted
and
self-
man
agem
ent v
aria
bles
, with
a cr
oss-
sect
iona
l des
crip
tive
surv
ey d
esig
n.
Parti
cipa
nts w
ere
anal
ysed
to
dete
rmin
e se
lf-m
anag
emen
t
beha
viou
rs in
the
early
, mid
dle
and
late
ado
lesc
ence
.
Una
djus
ted
diff
eren
ces b
y st
age
of a
dole
scen
ce in
self-
man
agem
ent b
ehav
iour
s wer
e
estim
ated
usi
ng A
NO
VA
.
504
parti
cipa
nts a
ged
13-2
1 ye
ars f
rom
the
Self-
Man
agem
ent o
f Dia
bete
s-
Ado
lesc
ent i
nstru
men
t dev
elop
men
t
stud
y, w
ho h
ad b
een
diag
nose
d w
ith
Type
1 d
iabe
tes f
or a
t lea
st a
yea
r, w
ere
not p
regn
ant a
nd h
ad n
o
cond
ition
/chr
onic
illn
ess t
hat c
ould
affe
ct h
ow th
e in
divi
dual
car
ed fo
r
his/
her d
iabe
tes.
Page
67
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
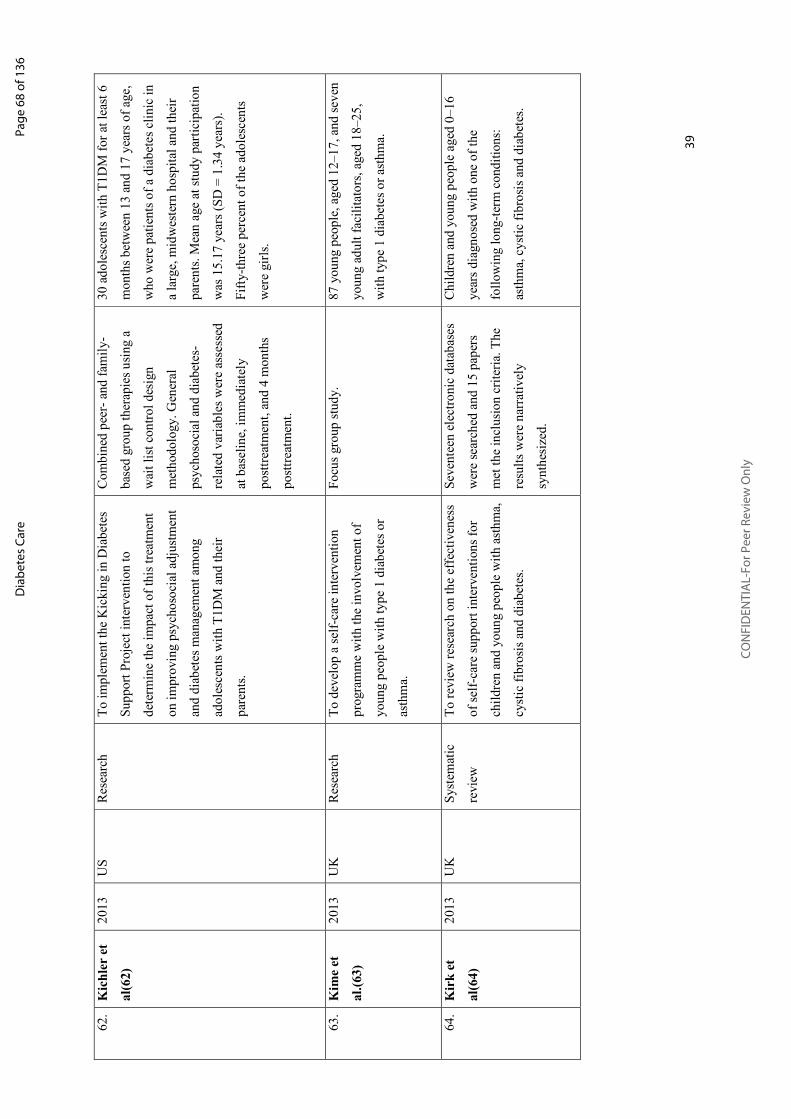
39
62.
Kic
hler
et
al(6
2)
2013
U
S R
esea
rch
To im
plem
ent t
he K
icki
ng in
Dia
bete
s
Supp
ort P
roje
ct in
terv
entio
n to
dete
rmin
e th
e im
pact
of t
his t
reat
men
t
on im
prov
ing
psyc
hoso
cial
adj
ustm
ent
and
diab
etes
man
agem
ent a
mon
g
adol
esce
nts w
ith T
1DM
and
thei
r
pare
nts.
Com
bine
d pe
er- a
nd fa
mily
-
base
d gr
oup
ther
apie
s usi
ng a
wai
t lis
t con
trol d
esig
n
met
hodo
logy
. Gen
eral
psyc
hoso
cial
and
dia
bete
s-
rela
ted
varia
bles
wer
e as
sess
ed
at b
asel
ine,
imm
edia
tely
post
treat
men
t, an
d 4
mon
ths
post
treat
men
t.
30 a
dole
scen
ts w
ith T
1DM
for a
t lea
st 6
mon
ths b
etw
een
13 a
nd 1
7 ye
ars o
f age
,
who
wer
e pa
tient
s of a
dia
bete
s clin
ic in
a la
rge,
mid
wes
tern
hos
pita
l and
thei
r
pare
nts.
Mea
n ag
e at
stud
y pa
rtici
patio
n
was
15.
17 y
ears
(SD
= 1
.34
year
s).
Fifty
-thre
e pe
rcen
t of t
he a
dole
scen
ts
wer
e gi
rls.
63.
Kim
e et
al.(6
3)
2013
U
K
Res
earc
h
To d
evel
op a
self-
care
inte
rven
tion
prog
ram
me
with
the
invo
lvem
ent o
f
youn
g pe
ople
with
type
1 d
iabe
tes o
r
asth
ma.
Focu
s gro
up st
udy.
87
you
ng p
eopl
e, a
ged
12–1
7, a
nd se
ven
youn
g ad
ult f
acili
tato
rs, a
ged
18–2
5,
with
type
1 d
iabe
tes o
r ast
hma.
64.
Kir
k et
al(6
4)
2013
U
K
Syst
emat
ic
revi
ew
To re
view
rese
arch
on
the
effe
ctiv
enes
s
of se
lf-ca
re su
ppor
t int
erve
ntio
ns fo
r
child
ren
and
youn
g pe
ople
with
ast
hma,
cyst
ic fi
bros
is a
nd d
iabe
tes.
Seve
ntee
n el
ectro
nic
data
base
s
wer
e se
arch
ed a
nd 1
5 pa
pers
met
the
incl
usio
n cr
iteria
. The
resu
lts w
ere
narr
ativ
ely
synt
hesi
zed.
Chi
ldre
n an
d yo
ung
peop
le a
ged
0–16
year
s dia
gnos
ed w
ith o
ne o
f the
follo
win
g lo
ng-te
rm c
ondi
tions
:
asth
ma,
cys
tic fi
bros
is a
nd d
iabe
tes.
Page
68
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
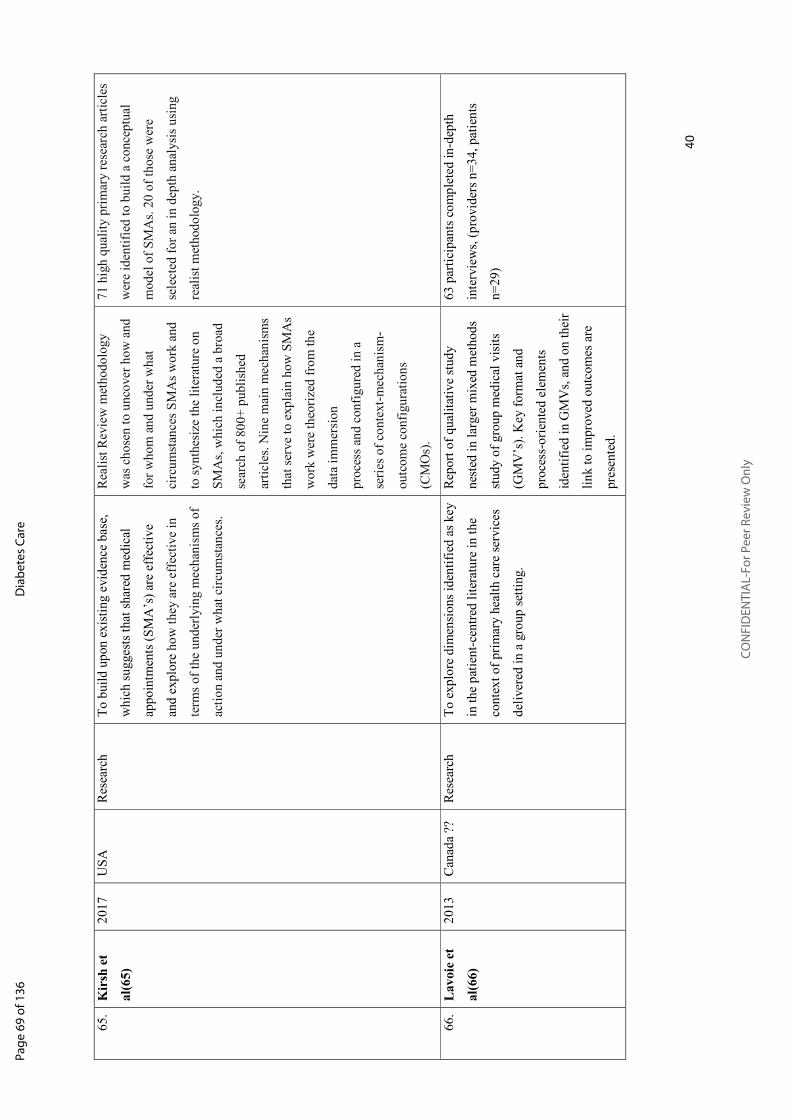
40
65.
Kir
sh e
t
al(6
5)
2017
U
SA
Res
earc
h To
bui
ld u
pon
exis
ting
evid
ence
bas
e,
whi
ch su
gges
ts th
at sh
ared
med
ical
appo
intm
ents
(SM
A’s
) are
eff
ectiv
e
and
expl
ore
how
they
are
eff
ectiv
e in
term
s of t
he u
nder
lyin
g m
echa
nism
s of
actio
n an
d un
der w
hat c
ircum
stan
ces.
Rea
list R
evie
w m
etho
dolo
gy
was
cho
sen
to u
ncov
er h
ow a
nd
for w
hom
and
und
er w
hat
circ
umst
ance
s SM
As w
ork
and
to sy
nthe
size
the
liter
atur
e on
SMA
s, w
hich
incl
uded
a b
road
sear
ch o
f 800
+ pu
blis
hed
artic
les.
Nin
e m
ain
mec
hani
sms
that
serv
e to
exp
lain
how
SM
As
wor
k w
ere
theo
rized
from
the
data
imm
ersi
on
proc
ess a
nd c
onfig
ured
in a
serie
s of c
onte
xt-m
echa
nism
-
outc
ome
conf
igur
atio
ns
(CM
Os)
.
71 h
igh
qual
ity p
rimar
y re
sear
ch a
rticl
es
wer
e id
entif
ied
to b
uild
a c
once
ptua
l
mod
el o
f SM
As.
20 o
f tho
se w
ere
sele
cted
for a
n in
dep
th a
naly
sis u
sing
real
ist m
etho
dolo
gy.
66.
Lav
oie
et
al(6
6)
2013
C
anad
a ??
R
esea
rch
To e
xplo
re d
imen
sion
s ide
ntifi
ed a
s key
in th
e pa
tient
-cen
tred
liter
atur
e in
the
cont
ext o
f prim
ary
heal
th c
are
serv
ices
deliv
ered
in a
gro
up se
tting
.
Rep
ort o
f qua
litat
ive
stud
y
nest
ed in
larg
er m
ixed
met
hods
stud
y of
gro
up m
edic
al v
isits
(GM
V’s
). K
ey fo
rmat
and
proc
ess-
orie
nted
ele
men
ts
iden
tifie
d in
GM
Vs,
and
on th
eir
link
to im
prov
ed o
utco
mes
are
pres
ente
d.
63 p
artic
ipan
ts c
ompl
eted
in-d
epth
inte
rvie
ws,
(pro
vide
rs n
=34,
pat
ient
s
n=29
)
Page
69
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
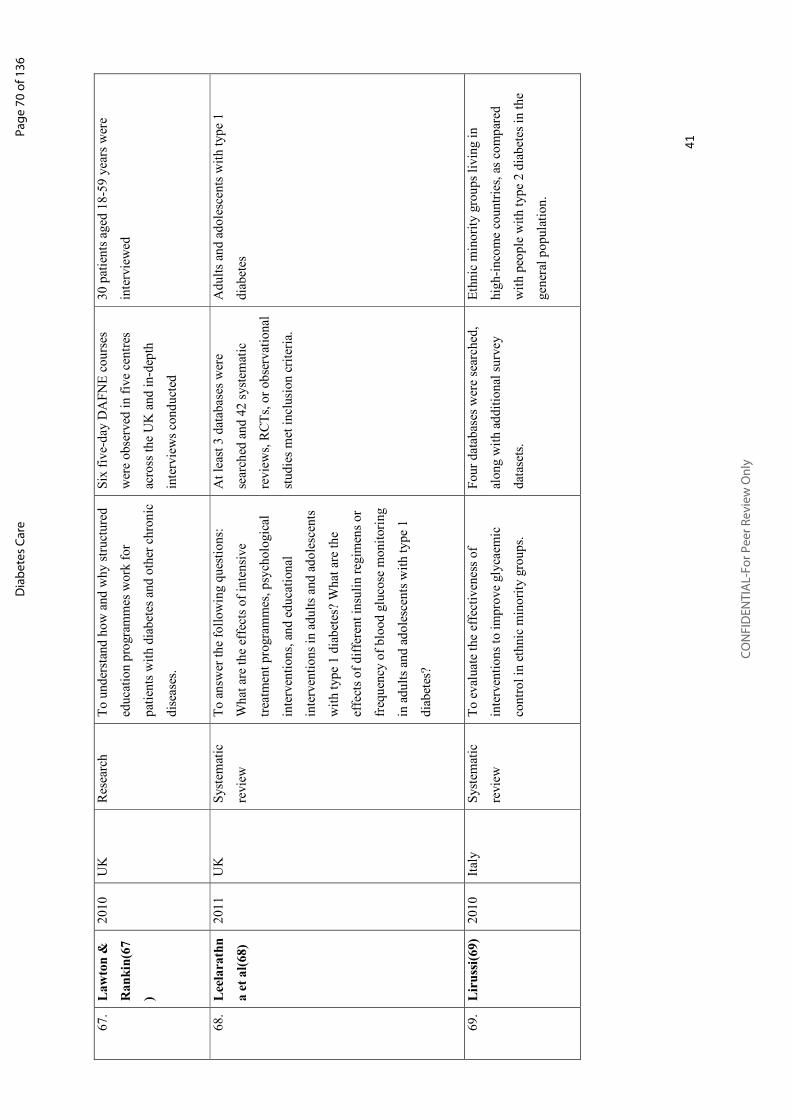
41
67.
Law
ton
&
Ran
kin(
67
)
2010
U
K
Res
earc
h To
und
erst
and
how
and
why
stru
ctur
ed
educ
atio
n pr
ogra
mm
es w
ork
for
patie
nts w
ith d
iabe
tes a
nd o
ther
chr
onic
dise
ases
.
Six
five-
day
DA
FNE
cour
ses
wer
e ob
serv
ed in
five
cen
tres
acro
ss th
e U
K a
nd in
-dep
th
inte
rvie
ws c
ondu
cted
30 p
atie
nts a
ged
18-5
9 ye
ars w
ere
inte
rvie
wed
68.
Lee
lara
thn
a et
al(6
8)
2011
U
K
Syst
emat
ic
revi
ew
To a
nsw
er th
e fo
llow
ing
ques
tions
:
Wha
t are
the
effe
cts o
f int
ensi
ve
treat
men
t pro
gram
mes
, psy
chol
ogic
al
inte
rven
tions
, and
edu
catio
nal
inte
rven
tions
in a
dults
and
ado
lesc
ents
with
type
1 d
iabe
tes?
Wha
t are
the
effe
cts o
f diff
eren
t ins
ulin
regi
men
s or
freq
uenc
y of
blo
od g
luco
se m
onito
ring
in a
dults
and
ado
lesc
ents
with
type
1
diab
etes
?
At l
east
3 d
atab
ases
wer
e
sear
ched
and
42
syst
emat
ic
revi
ews,
RC
Ts, o
r obs
erva
tiona
l
stud
ies m
et in
clus
ion
crite
ria.
Adu
lts a
nd a
dole
scen
ts w
ith ty
pe 1
diab
etes
69.
Lir
ussi
(69)
20
10
Italy
Sy
stem
atic
revi
ew
To e
valu
ate
the
effe
ctiv
enes
s of
inte
rven
tions
to im
prov
e gl
ycae
mic
cont
rol i
n et
hnic
min
ority
gro
ups.
Four
dat
abas
es w
ere
sear
ched
,
alon
g w
ith a
dditi
onal
surv
ey
data
sets
.
Ethn
ic m
inor
ity g
roup
s liv
ing
in
high
-inco
me
coun
tries
, as c
ompa
red
with
peo
ple
with
type
2 d
iabe
tes i
n th
e
gene
ral p
opul
atio
n.
Page
70
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
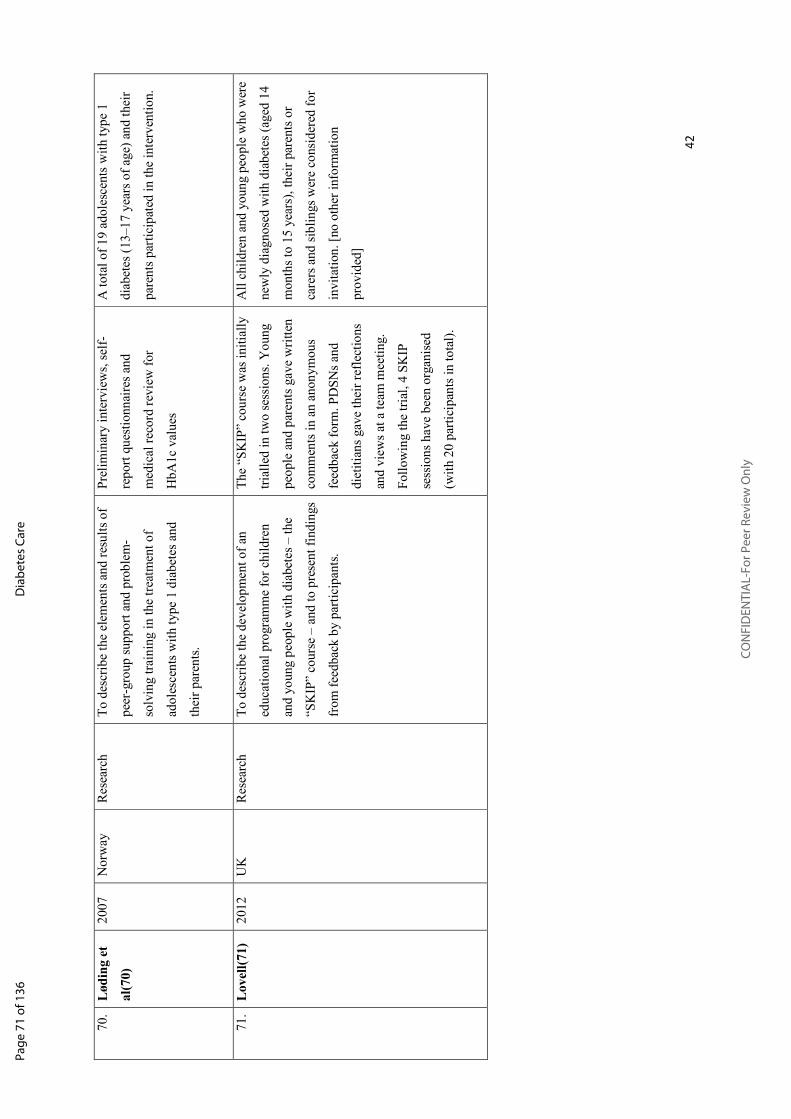
42
70.
Lød
ing
et
al(7
0)
2007
N
orw
ay
Res
earc
h To
des
crib
e th
e el
emen
ts a
nd re
sults
of
peer
-gro
up su
ppor
t and
pro
blem
-
solv
ing
train
ing
in th
e tre
atm
ent o
f
adol
esce
nts w
ith ty
pe 1
dia
bete
s and
thei
r par
ents
.
Prel
imin
ary
inte
rvie
ws,
self-
repo
rt qu
estio
nnai
res a
nd
med
ical
reco
rd re
view
for
HbA
1c v
alue
s
A to
tal o
f 19
adol
esce
nts w
ith ty
pe 1
diab
etes
(13–
17 y
ears
of a
ge) a
nd th
eir
pare
nts p
artic
ipat
ed in
the
inte
rven
tion.
71.
Lov
ell(7
1)
2012
U
K
Res
earc
h To
des
crib
e th
e de
velo
pmen
t of a
n
educ
atio
nal p
rogr
amm
e fo
r chi
ldre
n
and
youn
g pe
ople
with
dia
bete
s – th
e
“SK
IP”
cour
se –
and
to p
rese
nt fi
ndin
gs
from
feed
back
by
parti
cipa
nts.
The
“SK
IP”
cour
se w
as in
itial
ly
trial
led
in tw
o se
ssio
ns. Y
oung
peop
le a
nd p
aren
ts g
ave
writ
ten
com
men
ts in
an
anon
ymou
s
feed
back
form
. PD
SNs a
nd
diet
itian
s gav
e th
eir r
efle
ctio
ns
and
view
s at a
team
mee
ting.
Follo
win
g th
e tri
al, 4
SK
IP
sess
ions
hav
e be
en o
rgan
ised
(with
20
parti
cipa
nts i
n to
tal).
All
child
ren
and
youn
g pe
ople
who
wer
e
new
ly d
iagn
osed
with
dia
bete
s (ag
ed 1
4
mon
ths t
o 15
yea
rs),
thei
r par
ents
or
care
rs a
nd si
blin
gs w
ere
cons
ider
ed fo
r
invi
tatio
n. [n
o ot
her i
nfor
mat
ion
prov
ided
]
Page
71
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
43
72.
Lyo
ns e
t
al.(7
2)
2013
U
S R
evie
w
The
revi
ew id
entif
ies b
arrie
rs to
succ
essf
ul tr
ansi
tion
and
prov
ides
a
chec
klis
t for
stre
amlin
ing
the
proc
ess.
Rev
iew
of a
rticl
es re
late
d to
trans
ition
to a
dult
diab
etes
car
e
and
phys
ical
and
psy
chos
ocia
l
asse
ssm
ent o
f ado
lesc
ents
with
diab
etes
– o
ne d
atab
ase
sear
ched
. Des
ktop
revi
ew
(“in
tern
et se
arch
”) o
f onl
ine
trans
ition
reso
urce
s.
You
th w
ith d
iabe
tes m
ellit
us.
73.
Mal
low
et
al(7
3)
2015
U
SA
Res
earc
h Th
e ai
m o
f the
stud
y w
as to
exp
lore
the
impa
ct o
f Dia
bete
s Gro
up M
edic
al
Vis
its (D
GM
Vs)
on
biop
hysi
cal
outc
omes
of c
are
in u
nins
ured
per
sons
with
dia
bete
s.
Ret
rosp
ectiv
e st
udy
usin
g
conv
enie
nce
sam
plin
g of
thos
e
who
atte
nded
DG
MV
s and
usu
al
care
. Int
erve
ntio
n gr
oup
patie
nts
rece
ived
DG
MV
s dur
ing
the
stud
y tim
e fr
ame
and
met
incl
usio
n cr
iteria
. Usu
al c
are
patie
nts w
ere
rand
omly
sele
cted
from
dia
bete
s pat
ient
s rec
eivi
ng
usua
l car
e in
the
stud
y tim
e
fram
e w
ho m
et th
e in
clus
ion
crite
ria.
53 p
atie
nts a
ttend
ed D
GM
Vs a
nd 5
8
atte
nded
usu
al c
are
in th
e st
udy.
All
wer
e ag
ed 1
8 or
ove
r.
Page
72
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
44
74.
Man
nucc
i
et a
l(74)
2005
Ita
ly
Res
earc
h To
ass
ess t
he fe
asib
ility
and
eff
icac
y of
an In
tera
ctiv
e Ed
ucat
iona
l and
Sup
port
Gro
up p
rogr
amm
e (I
ESG
) for
pat
ient
s
with
type
1 d
iabe
tes.
The
Inte
ract
ive
Educ
atio
nal a
nd
Supp
ort G
roup
(IES
G) w
as
desi
gned
as a
sem
i-stru
ctur
ed,
long
-term
, ope
n, g
roup
educ
atio
n pr
ogra
mm
e. T
he
prog
ram
me
incl
uded
feat
ures
of
a se
lf-he
lp g
roup
, but
als
o
prov
ided
stru
ctur
ed in
form
atio
n
abou
t the
con
ditio
n. P
re- a
nd
post
ass
essm
ent o
f met
abol
ic
cont
rol a
nd d
iabe
tes r
elat
ed
qual
ity o
f life
.
Age
rang
e: 3
0.7±
8.4
(mea
n±SD
)
Page
73
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e

45
75.
Mar
kow
itz
&
Lef
fel(7
5)
2011
U
S R
esea
rch
Th
e au
thor
s im
plem
ente
d an
d ev
alua
ted
a su
ppor
t gro
up fo
r you
ng a
dults
with
Type
1 d
iabe
tes a
s a p
ilot p
roje
ct
You
th w
ith d
iabe
tes p
artic
ipat
ed
in m
onth
ly, p
rofe
ssio
nally
led
supp
ort g
roup
s for
5 m
onth
s.
Que
stio
nnai
res w
ere
com
plet
ed
pre-
and
post
-gro
up a
nd c
hart
revi
ew d
ata
wer
e co
llect
ed
rega
rdin
g gl
ycae
mic
con
trol a
nd
visi
t fre
quen
cy in
the
year
befo
re a
nd a
fter g
roup
parti
cipa
tion.
15 y
oung
adu
lts w
ith T
ype
1 di
abet
es
(18–
30 y
ears
) (93
% fe
mal
e, 9
2% w
hite
).
Mea
n ag
e w
as 2
6 +
3.3
year
s, di
abet
es
dura
tion
was
10.
6 +
8.0
year
s (ra
nge
1–
22 y
ears
). Pa
rtici
pant
s w
ere
high
ly
educ
ated
(> 8
5%
obta
ined
a b
ache
lor’
s deg
ree
or h
ighe
r),
80%
wer
e si
ngle
and
93%
had
no
child
ren.
The
maj
ority
wer
e se
en in
an
adul
t
diab
etes
clin
ic (7
5%),
with
the
rem
aind
er tr
eate
d by
pae
diat
ric
prov
ider
s. Th
e m
ajor
ity (8
6%) h
ad n
ever
befo
re p
artic
ipat
ed in
any
dia
bete
s
supp
ort g
roup
or c
omm
unity
-bas
ed
prog
ram
me.
76.
Mea
d &
Mac
Nei
l(7
6)
2004
U
SA
Res
earc
h To
pre
sent
a p
ersp
ectiv
e on
pee
r
supp
ort t
hat d
efin
es it
s diff
eren
ce a
nd
also
mai
ntai
ns it
s int
egrit
y to
the
mov
emen
t fro
m w
hich
it c
ame.
Writ
ten
refle
ctio
n to
off
er so
me
thin
king
abo
ut p
ract
ice
and
eval
uatio
n st
anda
rds t
hat
may
hel
p di
ffer
ent t
ypes
of p
eer
initi
ativ
es su
stai
n re
al p
eer
supp
ort v
alue
s in
actio
n.
N/A
Page
74
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
46
77.
Mej
ino
et
al(7
7)
2012
N
ethe
rland
s
Res
earc
h Th
is st
udy
exam
ined
the
pers
pect
ives
and
expe
rienc
es o
f pat
ient
s, pa
rent
s,
and
heal
th c
are
prov
ider
s with
shar
ed
med
ical
app
oint
men
ts (S
MA
s) fo
r
child
ren
and
adol
esce
nts w
ith ty
pe 1
diab
etes
.
Surv
ey q
uest
ionn
aire
s and
an
onlin
e fo
cus g
roup
Fifty
-two
patie
nts,
8 pa
rent
s, an
d 36
heal
th c
are
prov
ider
s par
ticip
ated
.
Parti
cipa
ting
patie
nts (
26 b
oys,
26 g
irls)
wer
e be
twee
n 8
and
18 y
ears
old
(mea
n
[M] =
13.
08, s
tand
ard
devi
atio
n [S
D] =
2.51
). O
ne o
r tw
o pa
rent
s (n
= 41
) per
patie
nt w
ere
pres
ent i
n si
x SM
As (
rang
e
4 to
11
pare
nts)
, reg
ardl
ess o
f the
patie
nts’
age
. How
ever
, pat
ient
s und
er
the
age
of 1
2 ye
ars (
n =
14) w
ere
alw
ays
acco
mpa
nied
by
thei
r par
ent(s
) dur
ing
an S
MA
.
78.
Mul
vane
y
et a
l.(78
)
2008
U
S R
esea
rch
To
doc
umen
t bar
riers
and
faci
litat
ors o
f sel
f-m
anag
emen
t as
perc
eive
d by
ado
lesc
ents
with
type
2 d
iabe
tes.
Bet
wee
n 20
03 a
nd 2
005,
6 fo
cus
grou
ps w
ere
used
to e
licit
resp
onse
s fro
m a
dole
scen
ts w
ith
type
-2 d
iabe
tes r
elat
ed
to th
eir s
elf-
man
agem
ent.
Tran
scrip
ts w
ere
code
d by
3
revi
ewer
s. Q
ualit
ativ
e an
alys
es
wer
e co
nduc
ted
usin
g N
VIV
O
softw
are.
Ado
lesc
ents
age
d 13
to 1
9
year
s wer
e re
crui
ted
from
an
acad
emic
med
ical
cen
ter d
iabe
tes c
linic
.
Page
75
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
47
79.
Mur
phy
et
al(7
9)
2011
Ir
elan
d R
esea
rch
To u
nder
stan
d th
e ex
perie
nce
of
parti
cipa
nts i
n th
e D
ose
Adj
ustm
ent f
or
Nor
mal
Eat
ing
prog
ram
me
and
to
iden
tify
fact
ors t
hat i
nflu
ence
parti
cipa
nts'
impl
emen
tatio
n of
the
self-
man
agem
ent g
uide
lines
.
Qua
litat
ive
inte
rvie
ws w
ith 4
0
parti
cipa
nts i
n Ir
elan
d.
Adu
lts w
ith ty
pe 1
dia
bete
s who
had
com
plet
ed a
Dos
e A
djus
tmen
t for
Nor
mal
Eat
ing
prog
ram
me
(aro
und
one
quar
ter o
f par
ticip
ants
wer
e ag
ed
betw
een
20-3
0 ye
ars)
.
80.
Mur
phy
et
al(8
0)
2006
U
K
Syst
emat
ic
revi
ew
To u
pdat
e th
e ex
istin
g da
taba
se o
f
psyc
hoed
ucat
iona
l int
erve
ntio
ns (p
ost
1999
).
27 a
rticl
es d
escr
ibin
g th
e
eval
uatio
n of
24
psyc
ho-
educ
atio
nal i
nter
vent
ions
. Eff
ect
size
s are
cal
cula
ted
and
data
sum
mar
y ta
bles
pre
sent
ed.
Chi
ldre
n an
d yo
ung
peop
le w
ith T
ype
1
diab
etes
(chi
ldre
n de
fined
as t
hose
age
d
5–11
yea
rs a
nd y
oung
peo
ple
as a
ged
12–1
8 ye
ars)
.
81.
New
man
(8
1)
2012
U
S C
omm
enta
ry
Pres
ents
the
pers
pect
ive
of a
scho
ol
nurs
e on
the
need
s of a
dole
scen
ts w
ith
diab
etes
and
exp
erie
nce
with
gro
up
mee
tings
.
n/a
Stud
ents
with
dia
bete
s typ
e 1
or 2
, age
d
15-1
7 ye
ars o
ld.
82.
Nof
fsin
ger
(82)
2009
U
S B
ook
Pres
ents
the
hist
ory
of g
roup
vis
it
mod
els a
nd p
ropo
ses w
ays t
o
succ
essf
ully
impl
emen
t gro
up c
linic
s.
n/a
n/a
Page
76
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
48
83.
Noo
rdm
an
& v
an
Dul
men
(83
)
2013
N
ethe
rland
s
Res
earc
h To
exa
min
e in
form
atio
nal a
nd
emot
iona
l pat
ient
–pro
vide
r and
pat
ient
–
patie
nt c
omm
unic
atio
n
sequ
ence
s (i.e
. cue
s and
subs
eque
nt
resp
onse
s) d
urin
g Sh
ared
Med
ical
App
oint
men
ts (S
MA
s) fo
r chi
ldre
n an
d
adol
esce
nts w
ith ty
pe 1
Dia
bete
s
Mel
litus
(T1D
M) a
nd th
eir p
aren
ts.
Vid
eo-r
ecor
ding
s wer
e m
ade.
Com
mun
icat
ion
sequ
ence
s, in
clud
ing
info
rmat
iona
l and
em
otio
nal
cues
and
resp
onse
s wer
e ra
ted
usin
g an
ada
ptat
ion
of
the
Med
ical
Inte
rvie
w A
ural
Rat
ing
Scal
e.
57 c
hild
ren/
adol
esce
nts w
ith T
1DM
and
36 h
ealth
care
pro
vide
rs p
artic
ipat
ed in
ten
SMA
s in
seve
n D
utch
hos
pita
ls.
Mea
n ag
e in
yea
rs (S
D; r
ange
) 14
year
s
(SD
: 2.6
;
rang
e: 8
–18)
. One
or b
oth
pare
nts (
n =
41, r
ange
: 4–1
1 pa
rent
s) fr
om 3
5
child
ren/
adol
esce
nts w
ere
pres
ent i
n si
x pr
otoc
olle
d SM
As.
Dur
ing
four
SM
As n
one
of th
e pa
rent
s wer
e
pres
ent.
84.
Nor
ris e
t
al(8
4)
2002
U
S Sy
stem
atic
revi
ew
To re
view
the
effe
ctiv
enes
s and
econ
omic
eff
icie
ncy
of se
lf-
man
agem
ent e
duca
tion
inte
rven
tions
for p
eopl
e w
ith d
iabe
tes,
incl
udin
g
inte
rven
tions
in se
tting
s out
side
the
hom
e, c
linic
, sch
ool,
or w
orks
ite.
Five
dat
abas
es w
ere
sear
ched
and
30 st
udie
s wer
e in
clud
ed in
the
revi
ew.
Var
ious
, inc
ludi
ng a
dults
, you
ng p
eopl
e
and
child
ren.
85.
O'H
ara
et
al(8
5)
2016
Ir
elan
d Sy
stem
atic
revi
ew
To sy
nthe
size
the
evid
ence
rega
rdin
g
the
effe
ctiv
enes
s of i
nter
vent
ions
aim
ed
at im
prov
ing
clin
ical
, beh
avio
ural
or
psyc
hoso
cial
out
com
es fo
r you
ng a
dults
with
Typ
e 1
diab
etes
.
Five
ele
ctro
nic
data
base
s wer
e
sear
ched
and
18
pape
rs w
ere
incl
uded
in n
arra
tive
synt
hesi
s.
You
ng a
dults
age
d be
twee
n 15
-30
year
s
with
Typ
e 1
diab
etes
Page
77
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
49
86.
Pals
et
al(8
6)
2016
D
enm
ark
Res
earc
h Th
e ob
ject
ive
of th
e st
udy
is to
exp
lore
the
effe
cts o
f Nex
t edu
catio
n (N
EED
),
a pa
rtici
pato
ry p
atie
nt e
duca
tion
appr
oach
in d
iabe
tes e
duca
tion.
A q
uasi
exp
erim
enta
l des
ign
usin
g in
terv
entio
n an
d co
ntro
l
site
s was
use
d to
car
ry o
ut a
real
ist e
valu
atio
n on
NEE
D to
help
gai
n in
sigh
t int
o th
e
mec
hani
sms b
y w
hich
the
patie
nt e
duca
tion
appr
oach
func
tione
d. D
ata
wer
e co
llect
ed
thro
ugh
ques
tionn
aire
s,
inte
rvie
ws a
nd o
bser
vatio
ns.
Dat
a w
as a
naly
sed
usin
g
desc
riptiv
e st
atis
tics,
logi
stic
regr
essi
on a
nd sy
stem
atic
text
cond
ensa
tion.
8 in
terv
entio
n sit
es n
=193
, 6 c
ontro
l
site
s, n=
58.
Page
78
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
50
87.
Pate
rson
&
Tho
rne(
87
)
2000
C
anad
a R
esea
rch
To
des
crib
e th
e de
velo
pmen
tal
evol
utio
n of
exp
ertis
e in
the
self-
man
agem
ent o
f dia
bete
s as i
t
was
por
traye
d in
a re
sear
ch st
udy
abou
t
expe
rt se
lf-m
anag
emen
t
of p
erso
ns w
ith lo
ng-s
tand
ing
Type
1
diab
etes
.
Gro
unde
d th
eory
stud
y w
hich
ass
umed
that
the
insi
der p
ersp
ectiv
e on
the
com
plex
pro
cess
of s
elf-
man
agem
ent i
s
acce
ssib
le th
roug
h in
terp
retiv
e re
sear
ch
met
hods
Parti
cipa
nts h
ad a
n in
itial
inte
rvie
w a
nd su
bseq
uent
ly
audi
o-ta
ped
thei
r dai
ly se
lf-
man
agem
ent d
ecis
ions
for 3
lots
of o
ne w
eek
perio
ds (t
hrou
ghou
t
one
year
). Tr
ansc
ripts
wer
e us
ed
as p
rom
pts f
or a
dditi
onal
inte
rvie
ws.
At t
he e
nd o
f the
rese
arch
, all
parti
cipa
nts
atte
nded
a 2
hou
r foc
us g
roup
inte
rvie
w w
here
find
ings
wer
e
shar
ed a
nd p
artic
ipan
ts w
ere
invi
ted
to re
flect
on
them
.
Ana
lysi
s of t
he tr
ansc
ripts
was
guid
ed b
y tra
ditio
nal c
onst
ant
com
para
tive
anal
ytic
tech
niqu
es.
22 in
divi
dual
s with
long
stan
ding
(>15
year
s) T
ype
1 di
abet
es, i
dent
ified
as
expe
rt se
lf-m
anag
emen
t dec
isio
n
mak
ers.
Cau
casi
an. 1
4 w
omen
and
8
men
, ran
ged
24-8
1 ye
ars (
M=4
3.3)
. 18
had
high
-sch
ool o
r pos
t-sec
onda
ry
educ
atio
n an
d 8
had
one
or m
ore
diab
etes
-rel
ated
com
plic
atio
n.
Page
79
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
51
88.
Pian
a et
al(8
8)
2010
Ita
ly
Res
earc
h To
intro
duce
a n
arra
tive-
auto
biog
raph
ical
app
roac
h in
the
care
and
educ
atio
n of
ado
lesc
ents
with
type
-
1 di
abet
es.
Ado
lesc
ents
atte
ndin
g on
e 9-
day
sum
mer
cam
p in
200
4, 2
005,
or
2006
par
ticip
ated
in st
ruct
ured
daily
self-
writ
ing
prop
osal
s on
diab
etes
, int
egra
ted
with
dai
ly
inte
ract
ive
self-
man
agem
ent
educ
atio
n. T
hey
late
r fill
ed in
ques
tionn
aire
s on
thei
r
expe
rienc
es a
t the
cam
p an
d
usin
g th
e au
tobi
ogra
phic
al
appr
oach
(50
resp
onse
s/53
.2%
resp
onse
rate
). El
icite
d te
xts
wer
e al
so a
naly
sed
usin
g
cont
ent a
naly
sis.
Nin
ety-
four
ado
lesc
ents
with
type
-1
diab
etes
(age
13–
18 y
ears
).
89.
Pilla
y et
al(8
9)
2015
C
anad
a Sy
stem
atic
revi
ew
To d
eter
min
e th
e ef
fect
s of b
ehav
iora
l
prog
ram
s for
pat
ient
s with
type
1
diab
etes
on
beha
vior
al, c
linic
al, a
nd
heal
th o
utco
mes
and
to in
vest
igat
e
fact
ors t
hat m
ight
mod
erat
e ef
fect
.
Six
elec
troni
c da
taba
ses w
ere
sear
ch a
nd 4
7 pa
pers
wer
e
incl
uded
in th
e re
view
.
Stud
ies f
ocus
ing
on y
outh
s (m
edia
n 13
.5
year
s) a
nd a
dults
(30-
49).
No
stud
ies
focu
sed
on y
oung
or o
lder
adu
lts.
Page
80
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
52
90.
Plan
te &
Lob
ato(
90)
2008
U
S Sy
stem
atic
revi
ew
To re
view
the
effic
acy
of g
roup
-bas
ed
psyc
holo
gica
l int
erve
ntio
ns fo
r
child
ren
and
adol
esce
nts w
ith ty
pe 1
diab
etes
.
Two
elec
troni
c da
taba
ses w
ere
sear
ched
and
31
artic
les w
ere
incl
uded
in th
e re
view
.
Chi
ldre
n an
d yo
ung
adul
ts (a
ge ra
nge
8-
23 y
ears
) with
type
1 d
iabe
tes.
91.
Povl
sen
&
Rin
gsbe
rg(
91)
2008
Sw
eden
R
esea
rch
To
exp
lore
how
you
ng a
dults
with
a
non-
wes
tern
imm
igra
nt b
ackg
roun
d an
d
type
1 d
iabe
tes s
ince
child
hood
/ado
lesc
ence
hav
e pe
rcei
ved
lear
ning
to li
ve w
ith th
e di
seas
e, w
ith
spec
ial f
ocus
on
heal
th e
duca
tion
and
supp
ort
A m
ixed
qua
ntita
tive
and
qual
itativ
e de
sign
was
app
lied.
This
incl
uded
data
on
met
abol
ic c
ontro
l for
2002
–200
6 an
d se
mi-s
truct
ured
inte
rvie
ws i
n 20
06
with
ele
ven
stra
tegi
cally
sele
cted
you
ng im
mig
rant
s.
Dat
a w
ere
anal
ysed
usi
ng
qual
itativ
e co
nten
t ana
lysi
s
Elev
en n
on-w
este
rn im
mig
rant
s, de
fined
as p
erso
ns o
r des
cend
ants
of p
erso
ns
with
imm
igra
nt o
r ref
ugee
bac
k-gr
ound
orig
inat
ing
from
cou
ntrie
s out
side
Wes
tern
Eur
ope,
Nor
th A
mer
ica
and
Aus
tralia
, par
ticip
ated
in th
e st
udy.
Thes
e w
ere
six
wom
en a
nd fi
ve m
en
aged
17–
28 y
ears
, who
had
bee
n
diag
nose
d w
ith ty
pe 1
dia
bete
s bet
wee
n
the
age
of
10 a
nd 1
7 ye
ars.
92.
Pow
ell e
t
al(9
2)
2015
U
S R
evie
w
To p
rovi
de a
n ov
ervi
ew o
f new
appr
oach
es to
dia
bete
s car
e
n/a
n/a
Page
81
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
53
93.
Pric
e et
al(9
3)
2016
U
K
Res
earc
h To
ass
ess t
he e
ffec
t of a
5-d
ay
stru
ctur
ed e
duca
tion
cour
se (K
ids i
n
Con
trol o
f Foo
d; K
ICk-
OFF
) on
biom
edic
al a
nd p
sych
olog
ical
out
com
es
in y
oung
peo
ple
with
Typ
e 1
diab
etes
.
Clu
ster
-ran
dom
ized
tria
l
invo
lvin
g 31
UK
pae
diat
ric
cent
res
Parti
cipa
nts w
ere
11-1
6 ye
ars o
f age
and
had
Type
1 d
iabe
tes f
or a
t lea
st o
ne y
ear.
Page
82
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
54
94.
Pyat
ak e
t
al.(9
4)
2016
U
S R
esea
rch
The
auth
ors i
dent
ified
and
trea
ted
youn
g ad
ults
with
type
1 d
iabe
tes w
ho
had
been
lost
to
follo
w-u
p du
ring
thei
r tra
nsfe
r fro
m
paed
iatri
c to
adu
lt ca
re, c
ompa
ring
thei
r
clin
ical
, psy
chos
ocia
l,
and
heal
th c
are
utili
zatio
n ou
tcom
es to
parti
cipa
nts r
ecei
ving
con
tinuo
us c
are
(CC
) thr
ough
out t
he tr
ansi
tion
to a
dult
care
.
Indi
vidu
als i
n th
eir l
ast y
ear o
f
paed
iatri
c ca
re (C
C g
roup
, n ¼
51) a
nd in
divi
dual
s los
t to
follo
w-u
p in
the
trans
fer t
o ad
ult
care
(“la
psed
car
e” [L
C] g
roup
,
n ¼
24)
wer
e fo
llow
ed
pros
pect
ivel
y fo
r 12
mon
ths.
All
parti
cipa
nts w
ere
prov
ided
deve
lopm
enta
lly ta
ilore
d
diab
etes
educ
atio
n, c
ase
man
agem
ent,
and
clin
ical
car
e th
roug
h a
stru
ctur
ed tr
ansi
tion
prog
ram
.
The
grou
ps w
ere
then
com
pare
d
on d
iabe
tes c
are
visi
ts,
glyc
emic
con
trol,
epis
odes
of
seve
re h
ypog
lyce
mia
(def
ined
as
requ
iring
ass
ista
nce
and/
or c
hang
e in
men
tal s
tatu
s),
emer
genc
y de
partm
ent v
isits
,
hosp
italis
atio
ns, a
nd
psyc
hoso
cial
out
com
es.
Parti
cipa
nt c
riter
ia: a
ge 1
9-25
yea
rs a
t
the
time
of st
udy
enro
lmen
t; (2
) dia
gnos
is o
f
type
1 d
iabe
tes
acco
rdin
g to
Am
eric
an D
iabe
tes
Ass
ocia
tion
crite
ria fo
r at l
east
2 ye
ars;
and
(3) p
artic
ipan
t not
pre
gnan
t
at th
e tim
e of
stud
y
enro
lmen
t or p
lann
ing
preg
nanc
y w
ithin
the
next
12
mon
ths
Page
83
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
55
95.
Ram
das &
Dar
zi(9
5)
2017
U
K
Res
earc
h To
exp
lore
why
giv
en th
e ef
fect
iven
ess
of g
roup
inte
rven
tions
, doc
tors
are
not
rout
inel
y
usin
g th
em to
trea
t phy
sica
l and
men
tal
cond
ition
s?
Shor
t rep
ort,
whi
ch i
dent
ified
and
disc
usse
s fou
r cru
cial
com
pone
nts (
(1) r
igor
ous
scie
ntifi
c
evid
ence
supp
ortin
g th
e va
lue
of
shar
ed a
ppoi
ntm
ents
, 2) e
asy
way
s to
pilo
t and
refin
e sh
ared
-
appo
intm
ent m
odel
s bef
ore
appl
ying
them
in p
artic
ular
car
e
setti
ngs,
3) re
gula
tory
chan
ges o
r inc
entiv
es th
at
supp
ort t
he u
se o
f suc
h m
odel
s,
4) re
leva
nt p
atie
nt a
nd c
linic
ian
educ
atio
n), w
hich
may
be
mi s
sing
from
gro
up
inte
rven
tions
and
the
auth
ors
belie
ve a
re n
eces
sary
for a
ny
high
ly in
nova
tive
serv
ice-
deliv
ery
mod
el to
bec
ome
stan
dard
.
N/A
Page
84
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
56
96.
Ran
kin
et
al.(9
6)
2011
U
K
Res
earc
h To
info
rm fu
ture
edu
catio
nal
inte
rven
tions
, the
aut
hors
exp
lore
d
patie
nts’
acc
ount
s of t
he e
duca
tion
and
info
rmat
ion
they
had
rece
ived
sinc
e
diag
nosi
s, an
d th
e re
ason
s beh
ind
gaps
in th
eir d
iabe
tes k
now
ledg
e
Sem
i-stru
ctur
ed in
terv
iew
s wer
e
cond
ucte
d w
ith 3
0 ty
pe 1
diab
etes
pat
ient
s enr
olle
d on
a
stru
ctur
ed e
duca
tion
prog
ram
me
in th
e U
K. D
ata
wer
e an
alys
ed
usin
g an
indu
ctiv
e, th
emat
ic
appr
oach
.
30 p
artic
ipan
ts a
ged
18-5
6 (1
6 fe
mal
es
and
14 m
ales
) wer
e re
crui
ted
from
six
cour
ses a
cros
s fiv
e di
abet
es c
entre
s in
the
UK
.
97.
Ran
kin
et
al(9
7)
2014
U
K
Res
earc
h To
exp
lore
pat
ient
s' ex
perie
nces
of,
view
s abo
ut a
nd n
eed
for,
soci
al
supp
ort a
fter a
ttend
ing
a st
ruct
ured
educ
atio
n pr
ogra
mm
e fo
r typ
e 1
diab
etes
.
Rep
eat q
ualit
ativ
e in
terv
iew
s
follo
win
g co
mpl
etio
n of
the
Dos
e A
djus
tmen
t for
Nor
mal
Eatin
g co
urse
and
gro
unde
d
theo
ry a
naly
sis.
30 a
dult
patie
nts w
ith ty
pe 1
dia
bete
s
recr
uite
d fr
om D
ose
Adj
ustm
ent f
or
Nor
mal
Eat
ing
cour
ses (
age:
36.
1mea
n±
11.6
SD; r
ange
18–
56).
98.
Ran
kin
et
al(9
8)
2012
U
K
Res
earc
h To
exp
lore
the
supp
ort n
eeds
of p
atie
nts
with
type
1 d
iabe
tes a
fter a
ttend
ing
a
stru
ctur
ed e
duca
tion
prog
ram
me.
Rep
eat q
ualit
ativ
e in
terv
iew
s
follo
win
g co
mpl
etio
n of
the
Dos
e A
djus
tmen
t for
Nor
mal
Eatin
g co
urse
. Dat
a w
ere
anal
ysed
indu
ctiv
ely.
30 a
dult
patie
nts w
ith ty
pe 1
dia
bete
s
recr
uite
d fr
om D
ose
Adj
ustm
ent f
or
Nor
mal
Eat
ing
cour
ses (
age:
36.
1mea
n±
11.6
SD; r
ange
18–
56).
Page
85
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
57
99.
Ray
mon
d
et a
l(99)
2015
U
S R
esea
rch
Feas
ibili
ty a
nd a
ccep
tabi
lity
pilo
t stu
dy
of T
eam
Clin
ics t
hat w
as c
arrie
d ou
t
befo
re b
egin
ning
a ra
ndom
ized
,
cont
rolle
d tri
al o
f thi
s pro
gram
.
Satis
fact
ion
surv
ey
92 p
atie
nts p
artic
ipat
ed in
Tea
m C
linic
(mea
n ag
e 15
.82
± 2.
1 ye
ars,
43%
fem
ale,
60%
non
-His
pani
c w
hite
, 24%
His
pani
c/La
tino,
6%
blac
k; re
flect
ive
of th
e ov
eral
l clin
ic
popu
latio
n)
Page
86
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
58
100.
Rei
tz e
t
al(1
00)
2012
U
SA
Res
earc
h Th
e pu
rpos
e of
the
stud
y w
as to
eval
uate
the
effe
ct o
f a d
iabe
tes s
uppo
rt
and
educ
atio
n gr
oup
visi
t pro
gram
on,
HB
A1c
con
cent
ratio
n, lo
w-d
ensi
ty
lipop
rote
in c
once
ntra
tion,
BP
targ
ets
and
wei
ght c
hang
es se
vera
l mon
ths
afte
r pro
gram
com
men
cem
ent.
A q
uasi
-exp
erim
enta
l mat
ched
cont
rolle
d pr
e- a
nd p
ost-s
tudy
desi
gn w
as u
sed
to c
ompa
re
diff
eren
ces i
n th
e m
easu
red
outc
omes
bet
wee
n th
e di
abet
ic
patie
nts i
n th
e gr
oup
visi
t
prog
ram
and
thos
e in
a m
atch
ed
com
paris
on g
roup
. The
bas
elin
e
varia
bles
of e
ach
grou
p, a
nd th
e
chan
ges f
rom
bas
elin
e, w
ith
adju
stm
ent f
or b
asel
ine
valu
es
durin
g th
e fo
llow
-up
perio
d of
7
mon
ths,
wer
e co
mpa
red
with
the
Coc
hran
Man
tel H
aens
zel
(CM
H) s
tatis
tic. T
he n
umbe
r of
offic
e vi
sits
dur
ing
the
follo
w-
up p
erio
d w
as a
lso
com
pare
d.
The
leve
l of s
igni
fican
ce fo
r
grou
p co
mpa
rison
s was
set a
t an
alph
a va
lue
of le
ss th
an 0
.05.
SAS
Ente
rpris
e G
uide
4.1
was
used
for d
ata
anal
ysis
.
Gro
up v
isit
prog
ram
(n=5
2) a
nd
com
paris
on g
roup
pat
ient
s (n=
236)
wer
e
draw
n fr
om fa
mily
pra
ctic
e, ≥
18 y
ears
and
had
type
2 d
iabe
tes w
ith a
t lea
st o
ne
visi
t to
the
prac
tice
in th
e pr
eced
ing
year
.
Page
87
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e

59
101.
Rijs
wijk
et
al(1
01)
2010
N
ethe
rland
s
Res
earc
h Th
e fo
llow
ing
rese
arch
que
stio
ns w
ere
addr
esse
d:
1. W
hat a
re th
e di
ffer
ence
s bet
wee
n a
tradi
tiona
l ind
ivid
ual
outp
atie
nt v
isit
and
an S
MA
for
child
ren
and
adol
esce
nts w
ith
type
1 d
iabe
tes i
n:
a. th
e am
ount
of d
iabe
tes-
rela
ted
topi
cs
disc
usse
d?
b. th
e co
nver
satio
nal c
ontri
butio
ns o
f
the
parti
cipa
nts?
2. H
ow d
o ch
ildre
n an
d ad
oles
cent
s
asse
ss th
e so
cial
and
info
rmat
iona
l asp
ects
of a
n SM
A?
Vid
eota
pes o
f 42
indi
vidu
al
outp
atie
nt v
isits
and
5 S
MA
s
with
31
child
ren
or a
dole
scen
ts
wer
e co
llect
ed a
nd o
bser
ved
usin
g a
chec
klis
t of t
opic
s.
Surv
ey q
uest
ionn
aire
on
view
s
abou
t par
ticip
atio
n in
the
SMA
s.
Parti
cipa
ting
patie
nts w
ere
betw
een
6
year
s and
19
year
s of a
ge a
nd
parti
cipa
ted
in d
iffer
ent a
ge g
roup
s, of
6–12
(chi
ldre
n) a
nd 1
3–19
yea
rs
(ado
lesc
ents
). //
The
patie
nts w
ere
on
aver
age
12.8
(SD
2.8
; ran
ge 6
–19)
yea
rs
of a
ge in
the
indi
vidu
al c
onsu
ltatio
ns
and
12.3
(SD
2.7
; ran
ge 8
–18)
yea
rs in
the
SMA
s (ns
). Pa
rent
s par
ticip
ated
in
all S
MA
s.
102.
Rith
olz
et
al(1
02)
2011
U
S Sy
stem
atic
revi
ew
To u
nder
stan
d ho
w q
ualit
ativ
e re
sear
ch
cont
ribut
es to
an
incr
ease
d
unde
rsta
ndin
g f b
ehav
iour
al d
iabe
tes.
The
pape
r syn
thes
ises
find
ings
in n
arra
tive
form
.
Chi
ldre
n, a
dole
scen
ts, a
nd a
dult
patie
nts
with
bot
h ty
pe 1
and
type
2 d
iabe
tes
Page
88
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
60
103.
Rob
inso
n(
103)
2015
U
K
Res
earc
h
To g
ain
grea
ter i
nsig
ht in
to th
e
expe
rienc
e of
bei
ng d
iagn
osed
with
type
1 d
iabe
tes d
urin
g ad
oles
cenc
e, a
nd
the
fact
ors t
hat i
nflu
ence
how
a y
oung
pers
on m
akes
sens
e of
the
cond
ition
over
tim
e.
Uns
truct
ured
inte
rvie
ws w
ere
cond
ucte
d an
d re
sults
wer
e
anal
ysed
usi
ng In
terp
reta
tive
phen
omen
olog
ical
ana
lysi
s
Eigh
t adu
lts, a
ged
28–3
6 ye
ars w
ho w
ere
diag
nose
d w
ith
diab
etes
dur
ing
adol
esce
nce
104.
Ros
tam
i et
al.(1
04)
2014
Ir
an
Res
earc
h Th
is st
udy
escr
ibes
and
exp
lore
s the
expe
rienc
es o
f sup
port
in Ir
ania
n
adol
esce
nts w
ith T
1DM
in o
rder
to
prov
ide
cultu
re a
nd c
onte
xt sp
ecifi
c
rese
arch
of T
1DM
in o
rder
to im
prov
e
know
ledg
e of
how
cul
tura
l fac
tors
influ
ence
the
prov
isio
n of
supp
ort t
o
adol
esce
nts w
ith T
1DM
.
Sem
i-stru
ctur
ed in
terv
iew
s wer
e
used
and
con
tent
ana
lysi
s was
cond
ucte
d
A se
mi-s
truct
ured
inte
rvie
w
sche
dule
was
dev
elop
ed to
guid
e gr
oup
disc
ussi
ons
base
d on
the
rese
arch
que
stio
ns
Purp
osiv
e sa
mpl
ing
was
use
d to
iden
tify
parti
cipa
nts w
ho w
ere
10-1
9 ye
ars o
ld,
had
T1D
M fo
r at l
east
two
year
s and
had
no o
ther
chr
onic
dis
ease
s. 7
mal
es a
nd 3
fem
ales
wer
e re
crui
ted
at tw
o di
abet
es
man
agem
ent c
linic
s in
Iran
.
Page
89
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
61
105.
Sadu
r et
al(1
05)
1999
U
SA
Res
earc
h To
eva
luat
e th
e ef
fect
iven
ess o
f a
clus
ter v
isit
mod
el le
d by
a d
iabe
tes
nurs
e ed
ucat
or fo
r del
iver
ing
outp
atie
nt
care
man
agem
ent t
o ad
ult p
atie
nts w
ith
poor
ly c
ontro
lled
diab
etes
.
Ran
dom
ised
con
trol t
rial.
Inte
rven
tion
subj
ects
rece
ived
mul
tidis
cipl
inar
y ou
tpat
ient
diab
etes
car
e m
anag
emen
t in
clus
ter v
isit
setti
ngs o
f 10–
18
patie
nts/
mon
th fo
r 6 m
onth
s.
The
outc
omes
ava
ilabl
e fo
r the
stud
y in
clud
ed p
ost i
nter
vent
ion
HbA
1c le
vels
; sel
f-re
porte
d
mea
sure
s of s
elf-
care
pra
ctic
es,
self-
effic
acy,
and
satis
fact
ion
with
gen
eral
med
ical
car
e an
d
with
dia
bete
s spe
cific
car
e;
mea
sure
s of u
tiliz
atio
n of
inpa
tient
and
out
patie
nt se
rvic
es
befo
re ,
durin
g, a
nd a
fter t
he 6
-
mon
th in
terv
entio
n th
roug
h th
e
end
of 1
997;
and
tota
l cos
ts o
f
care
for t
he sa
me
perio
ds
Parti
cipa
nts a
ged
16-7
5 ye
ars w
ith
HB
A1c
con
cent
ratio
n >8
.5%
or n
o
HB
A1c
mea
sure
men
t for
the
prev
ious
year
, wer
e ra
ndom
ised
to a
n in
terv
entio
n
grou
p (n
=97)
or a
usu
al c
are
grou
p
(n=8
8).
Page
90
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
62
106.
Satt
oe e
t
al(1
06)
2015
N
ethe
rland
s
Syst
emat
ic
revi
ew
To p
rovi
de a
syst
emat
ic o
verv
iew
of
self-
man
agem
ent i
nter
vent
ions
(SM
I)
for y
oung
peo
ple
with
chr
onic
cond
ition
s.
Six
data
base
s wer
e se
arch
ed a
nd
86 st
udie
s wer
e in
clud
ed in
the
revi
ew –
of t
hose
16
artic
les
refe
rred
to d
iabe
tes.
You
ng p
eopl
e (a
ged
7–25
yea
rs) w
ith
som
atic
chr
onic
con
ditio
ns o
r phy
sica
l
disa
bilit
y, in
clud
ing
diab
etes
.
107.
Saw
tell
et
al(1
07)
2015
U
K
Res
earc
h To
ass
ess t
he fe
asib
ility
, acc
epta
bilit
y,
fidel
ity, a
nd p
erce
ived
impa
ct o
f the
stru
ctur
ed e
duca
tiona
l gro
up p
rogr
am
Chi
ld a
nd A
dole
scen
t Stru
ctur
ed
Com
pete
ncie
s App
roac
h to
Dia
bete
s
Educ
atio
n (C
ASC
AD
E).
Mix
ed m
etho
ds p
roce
ss
eval
uatio
n, e
mbe
dded
with
in a
clus
ter r
ando
miz
ed c
ontro
l tria
l
in 2
8 pe
diat
ric d
iabe
tes c
linic
s
acro
ss E
ngla
nd. T
he e
valu
atio
n
used
mul
tiple
met
hods
,
incl
udin
g qu
estio
nnai
res,
obse
rvat
ion
and
qual
itativ
e
inte
rvie
ws.
362
child
ren
parti
cipa
ted,
age
d 8-
16
year
s with
type
1 d
iabe
tes.
108.
Schi
lling
et
al(1
08)
2002
U
S Sy
stem
atic
revi
ew
To c
larif
y th
e co
ncep
t of s
elf-
man
agem
ent o
f typ
e 1
diab
etes
in
child
ren
and
adol
esce
nts.
Thre
e da
taba
ses w
ere
sear
ched
and
nine
ty n
ine
refe
renc
es w
ere
revi
ewed
.
Chi
ldre
n an
d ad
oles
cent
s age
d 6-
17
year
s.
Page
91
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
63
109.
Schi
lling
er
et a
l(109
)
2008
U
SA
Res
earc
h To
exa
min
e w
heth
er ta
ilore
d se
lf-
man
agem
ent s
uppo
rt (S
MS)
stra
tegi
es
reac
h pa
tient
s in
a sa
fety
net
syst
em.
Var
iatio
n by
lang
uage
, lite
racy
and
insu
ranc
e w
as e
xplo
red.
An
effe
ctiv
enes
s stu
dy o
f SM
S
nest
ed w
ithin
a ra
ndom
ized
tria
l
amon
g di
vers
e di
abet
es p
atie
nts
in a
safe
ty n
et sy
stem
. Eng
lish-
,
Span
ish-
and
Can
tone
se-
spea
king
dia
bete
s pat
ient
s wer
e
rand
omiz
ed to
wee
kly
auto
mat
ed te
leph
one
dise
ase
man
agem
ent (
ATD
M) o
r
mon
thly
gro
up m
edic
al v
isits
(GM
Vs)
. Tho
se ra
ndom
ised
to
AD
TM re
ceiv
ed w
eekl
y ph
one
calls
(6-1
2min
s) in
thei
r nat
ive
lang
uage
for 9
mon
ths.
Thos
e in
the
GM
V a
rm re
ceiv
ed la
ngua
ge
spec
ific
GM
Vs m
onth
ly fo
r 9
mon
ths.
Thes
e se
ssio
ns’ 6
-10
parti
cipa
nts a
nd la
sted
appr
oxim
atel
y 90
min
utes
.
Patie
nts w
ho w
ere
olde
r tha
n ag
e 17
;
had
ICD
-9 c
odes
con
sist
ent w
ith ty
pe 2
diab
etes
; spo
ke E
nglis
h, S
pani
sh, o
r
Can
tone
se; m
ade
≥1 p
rimar
y ca
re v
isit
in th
e pr
ior y
ear;
and
had
≥1 h
emog
lobi
n
A1c
val
ue (H
bA1c
) - A
ge (y
ears
): M
(SD
) 55.
4 (1
1.9)
Page
92
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
64
110.
Schm
idt e
t
al.(1
10)
2016
G
erm
any
R
esea
rch
To
test
the
effe
cts o
f a g
ener
ic
trans
ition
-orie
nted
pat
ient
edu
catio
n
prog
ram
on
adol
esce
nts’
hea
lth se
rvic
e
parti
cipa
tion
and
qual
ity o
f life
(QoL
).
The
auth
ors c
ondu
cted
a
cont
rolle
d tri
al c
ompa
ring
parti
cipa
nts o
f 29
trans
ition
wor
ksho
ps w
ith
treat
men
t as u
sual
. A
two-
day
trans
ition
wor
ksho
p w
as c
arrie
d
out a
t 12
sites
in G
erm
any,
focu
sing
in st
anda
rdiz
ed
mod
ules
on
adju
stm
ent t
o ad
ult
care
setti
ngs,
orga
niza
tion
of
futu
re d
isea
se m
anag
emen
t,
care
er c
hoic
es a
nd p
artn
ersh
ip.
Stud
y ou
tcom
es w
ere
heal
th-
rela
ted
trans
ition
com
pete
nce,
self-
effic
acy,
satis
fact
ion
with
care
, pat
ient
act
ivat
ion
and
QoL
.
Mea
sure
s wer
e as
sess
ed a
t
base
line
and
six-
mon
th fo
llow
-
up.
Rep
eate
d m
easu
rem
ent
cova
rianc
e an
alys
is u
sing
age
as
a co
varia
te w
as c
ondu
cted
.
274
adol
esce
nts (
16.8
mea
n ag
e, S
D =
1.76
) dia
gnos
ed w
ith ty
pe I
diab
etes
(DM
), C
ystic
fibr
osis
(CF)
or
infla
mm
ator
y bo
wel
dis
ease
(IB
D)
Page
93
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
65
111.
Schu
ltz e
t
al.(1
11)
2017
U
S R
esea
rch
To e
xam
ine
whi
ch c
ompo
nent
s of
trans
ition
pro
gram
s are
eff
ectiv
e in
impr
ovin
g ou
tcom
es
follo
win
g tra
nsfe
r
Syst
emat
ic re
view
/met
a-an
alys
is
11-2
6 ye
ars o
ld w
ith ty
pe 1
dia
bete
s
Page
94
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
66
112.
Sequ
eira
et
al.(1
12)
2015
U
S R
esea
rch
To e
valu
ate
the
effic
acy
of a
stru
ctur
ed
trans
ition
pro
gram
com
pare
d w
ith u
sual
care
in im
prov
ing
rout
ine
follo
w-u
p,
clin
ical
, and
psy
chos
ocia
l out
com
es
amon
g
youn
g ad
ults
with
type
1 d
iabe
tes
You
ng a
dults
with
type
1
diab
etes
in th
eir l
ast y
ear o
f
pedi
atric
car
e w
ere
recr
uite
d
from
thre
e cl
inic
s. In
terv
entio
n
grou
p pa
rtici
pant
s (n
= 51
)
rece
ived
a st
ruct
ured
trans
ition
pro
gram
inco
rpor
atin
g
tailo
red
diab
etes
edu
catio
n, c
ase
man
agem
ent,
grou
p ed
ucat
ion
clas
ses,
and
acce
ss to
a n
ewly
deve
lope
d yo
ung
adul
t dia
bete
s
clin
ic a
nd tr
ansi
tion
web
site
.
Con
trol g
roup
par
ticip
ants
(n =
30) r
ecei
ved
usua
l car
e. T
he
prim
ary
outc
ome
was
the
num
ber o
f rou
tine
clin
ic v
isits
.
Seco
ndar
y
outc
omes
incl
uded
gly
caem
ic
cont
rol,
hypo
glyc
aem
ia, h
ealth
care
use
, and
psy
chos
ocia
l
wel
l-bei
ng. A
sses
smen
ts w
ere
cond
ucte
d at
bas
elin
e, a
nd 6
and
12
mon
ths.
81 y
oung
adu
lts (5
1 in
inte
rven
tion
grou
p an
d 30
in c
ontro
l gro
up)
diag
nose
d w
ith ty
pe 1
dia
bete
s for
at
leas
t tw
o ye
ars,
aged
19-
25.
Parti
cipa
nts h
ad to
be
rece
ivin
g
rout
ine
diab
etes
car
e by
an
assi
gned
pro
vide
r, an
d 4)
in th
e la
st
year
of p
edia
tric
care
, def
ined
as
antic
ipat
ing
trans
ition
to a
dult
care
with
in th
e ne
xt y
ear.
Page
95
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
67
113.
Serl
achi
us
et a
l.(11
3)
2011
A
ustra
lia
Res
earc
h To
exp
lore
stre
ssor
s in
peop
le w
ith
T1D
M a
nd g
ain
feed
back
on
adap
ting
a
gene
ric c
opin
g sk
ills p
rogr
amm
e.
Focu
s gro
ups w
ere
cond
ucte
d
13 a
dole
scen
ts (1
3-17
) with
T1D
M
114.
Skin
ner
et
al.(1
14)
2000
U
K
Res
earc
h To
exa
min
e w
heth
er p
eer s
uppo
rt an
d
illne
ss re
pres
enta
tion
med
iate
the
link
betw
een
fam
ily su
ppor
t, se
lf-
man
agem
ent a
nd w
ell-b
eing
.
Parti
cipa
nts w
ere
recr
uite
d an
d
follo
wed
ove
r 6 m
onth
s. Th
ey
com
plet
ed q
uest
ionn
aire
asse
ssm
ents
on
self-
man
agem
ent,
wel
l-bei
ng a
nd
soci
al su
ppor
t.
52 a
dole
scen
ts(1
2-18
yea
rs o
ld) w
ith
Type
1 d
iabe
tes
115.
Smal
done
et a
l(115
)
2006
U
S R
esea
rch
To e
xam
ine
char
acte
ristic
s of p
atie
nts
with
type
1 a
nd ty
pe 2
dia
bete
s and
conc
lude
whe
ther
gro
up e
duca
tion
clas
ses s
houl
d be
sepa
rate
d by
type
of
diab
etes
.
Qua
ntita
tive
stud
y m
easu
ring
clin
ical
mar
kers
, sel
f-ca
re
beha
viou
rs, p
sych
osoc
ial
outc
omes
, foo
d ch
oice
s and
phys
ical
act
ivity
.
101
patie
nts w
ith ty
pe 1
dia
bete
s (m
ean
age
44 a
nd S
D 1
2.4
year
s) a
nd 1
07
patie
nts w
ith ty
pe 2
dia
bete
s (m
ean
age
57 a
nd S
D 9
.2 y
ears
).
116.
Soni
&
Ng(
116)
2014
U
K
Syst
emat
ic
revi
ew
To e
xam
ine
the
key
aspe
cts o
f
impr
ovin
g m
etab
olic
con
trol i
n ch
ildre
n
and
youn
g pe
ople
.
Find
ings
are
des
crib
ed in
narr
ativ
e fo
rm –
oth
er
met
hodo
logi
cal d
etai
ls a
re
mis
sing
.
Chi
ldre
n an
d yo
ung
adul
ts <
20
year
s.
Page
96
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
68
117.
Spen
cer
et
al.(1
17)
2013
U
K
Res
earc
h To
exp
lore
the
soci
al e
nviro
nmen
ts
youn
g pe
ople
with
type
1 d
iabe
tes
inha
bit,
and
the
pote
ntia
l inf
luen
ce o
f
thes
e en
viro
nmen
ts o
n th
eir g
lyca
emic
cont
rol.
In-d
epth
inte
rvie
ws w
ere
cond
ucte
d. A
n in
terp
retiv
e
phen
omen
olog
ical
app
roac
h w
as
take
n to
exp
lore
the
expe
rienc
es
of y
oung
peo
ple
with
type
1dia
bete
s and
thei
r par
ents
.
20 W
hite
Brit
ish
peop
le (9
mal
e, 1
1
fem
ale)
age
d 13
-16
year
s atte
ndin
g a
paed
iatri
c cl
inic
in N
orth
-Wes
t Eng
land
and
27 p
aren
ts (7
mal
e, 2
0 fe
mal
e).
The
fem
ale
pare
nt/g
uard
ian
alon
e to
ok p
art
in 1
3 in
terv
iew
s, an
d bo
th p
aren
ts
took
par
t in
seve
n in
terv
iew
s.
118.
Spen
cer
et
al.(1
18)
2013
U
K
Res
earc
h To
exp
lore
ado
lesc
ents
’ and
par
ents
’
expe
rienc
es o
f liv
ing
with
Typ
e 1
diab
etes
from
an
inte
rpre
tive
phen
omen
olog
ical
per
spec
tive
In-d
epth
inte
rvie
ws w
ere
cond
ucte
d, u
nder
pinn
ed b
y
inte
rpre
tive
phen
omen
olog
y
20 a
dole
scen
ts (1
3-16
, 9 m
ale,
9 fe
mal
e)
with
Typ
e 1
diab
etes
from
a d
iabe
tes
clin
ic in
Nor
th W
est E
ngla
nd, a
nd 2
7 of
thei
r par
ents
119.
Tho
rpe
et
al(1
19)
2013
U
S Sy
stem
atic
revi
ew
O
ne d
atab
ase
was
sear
ched
and
129
artic
les m
et c
riter
ia fo
r
incl
usio
n.
Patie
nts w
ith ty
pe 1
or 2
dia
bete
s and
no
rest
rictio
ns o
n ag
e.
Page
97
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
69
120.
Tie
rney
et
al.(1
20)
2008
U
K
Res
earc
h
To e
xplo
re p
atie
nts’
resp
onse
s to
deve
lopi
ng a
nd m
anag
ing
cyst
ic fi
bros
is-r
elat
ed d
iabe
tes a
nd to
cont
rast
thei
r vie
ws w
ith th
ose
of
indi
vidu
als w
ith ty
pe 1
dia
bete
s
mel
litus
.
Sem
i-stru
ctur
ed te
leph
one
or
face
-to-f
ace
inte
rvie
ws w
ere
cond
ucte
d w
ith p
atie
nts w
ho
had
cyst
ic fi
bros
is-r
elat
ed
diab
etes
or t
ype
1 di
abet
es
mel
litus
, dur
ing
whi
ch, t
hey
disc
usse
d di
agno
sis
and
man
agem
ent o
f dia
bete
s.
Fram
ewor
k an
alys
is w
as
empl
oyed
to id
entif
y th
emes
and
to c
onsi
der s
imila
ritie
s and
diff
eren
ces b
etw
een
the
two
grou
ps.
Parti
cipa
nts w
ere
deriv
ed fr
om a
larg
er
sam
ple
of p
atie
nts t
akin
g pa
rt in
a
ques
tionn
aire
-bas
ed st
udy
com
parin
g
epis
odes
of h
ypog
lyca
emia
and
qua
lity
of li
fe b
etw
een
patie
nts w
ith C
FRD
and
T1D
M. P
artic
ipan
ts h
ad to
be
18-6
0,
diag
nose
d w
ith d
iabe
tes f
or a
t lea
st 3
mon
ths a
nd b
eing
trea
ted
with
insu
lin.
23 in
terv
iew
s wer
e co
nduc
ted
with
11
CFR
D (5
mal
e, 6
fem
ale)
and
12
T1D
M
(6 m
ale)
par
ticip
ants
.
Page
98
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
70
121.
Vac
hon
et
al(1
21)
2007
U
SA
Res
earc
h To
des
crib
e th
e de
velo
pmen
t and
impl
emen
tatio
n of
a m
ultif
acet
ed
prog
ram
in a
n in
ner-
city
hea
lthca
re
cent
re d
esig
ned
to im
prov
e ac
cess
to
care
and
em
pow
er p
atie
nts t
o ta
ke a
mor
e ac
tive
role
in m
anag
ing
diab
etes
.
Des
crip
tion
of D
iabe
tic R
ewar
ds
Issu
ed V
ia E
very
one
(DR
IVE)
,
a m
onth
ly o
pen-
acce
ss, m
ulti-
stat
ion
grou
p vi
sit p
rogr
am
base
d in
an
econ
omic
ally
depr
ived
nei
ghbo
urho
od w
est
Chi
cago
. The
gro
up v
isit
form
at
inte
nded
to m
axim
ize
prov
ider
prod
uctiv
ity, i
ncre
ase
the
clin
ic's
capa
city
to se
e a
grea
ter
num
ber o
f pat
ient
s, pr
ovid
e
patie
nts a
setti
ng in
whi
ch to
lear
n m
ore
abou
t dia
bete
s,
nutri
tion
and
self-
man
agem
ent a
nd to
leve
rage
the
inte
ract
ions
am
ong
patie
nts i
n gr
oup
mee
tings
to
help
pro
mpt
cha
nges
in th
eir
self-
man
agem
ent t
hrou
gh p
eer
influ
ence
and
exp
erie
nce.
DR
IVE
day
parti
cipa
nts n
=294
, pat
ient
s
with
dia
bete
s who
hav
e no
t atte
nded
a
DR
IVE
day
n=44
3
Page
99
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
71
122.
Vik
lun
&
Wik
blah
(1
22)
2009
Sw
eden
R
esea
rch
To
exp
lore
teen
ager
s’ p
erce
ptio
ns o
f
fact
ors a
ffec
ting
deci
sion
-mak
ing
com
pete
nce
in d
iabe
tes m
anag
emen
t.
Qua
litat
ive
inte
rvie
ws w
ith
teen
ager
s with
type
1 d
iabe
tes
shor
tly a
fter t
hat c
ompl
eted
an
empo
wer
men
t edu
catio
n
prog
ram
me.
Inte
rvie
ws w
ere
anal
ysed
usi
ng q
ualit
ativ
e
cont
ent a
naly
sis.
31 te
enag
ers (
17 g
irls a
nd 1
5 bo
ys) w
ith
type
1 d
iabe
tes,
aged
12–
17 y
ears
.
123.
Vik
lund
et
al(1
23)
2007
a Sw
eden
R
esea
rch
To d
eter
min
e th
e ef
fect
s of a
n
empo
wer
men
t pro
gram
me
on
glyc
aem
ic c
ontro
l and
em
pow
erm
ent.
Ran
dom
ised
pre
-/pos
t-tes
t
desi
gn w
ith re
peat
ed m
easu
res.
The
empo
wer
men
t edu
catio
n
prog
ram
me
cons
iste
d of
six
2-h
grou
p se
ssio
ns. M
ain
outc
ome
mea
sure
s: H
bA1c
,
empo
wer
men
t and
par
enta
l
invo
lvem
ent.
Thirt
y-tw
o te
enag
ers w
ith T
ype
1
diab
etes
(12-
17 y
ears
), in
clud
ing
invo
lvem
ent f
rom
par
ents
.
Page
100
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
72
124.
Vik
lund
et
al(1
24)
2007
b Sw
eden
R
esea
rch
To e
valu
ate
whe
ther
dia
betic
teen
ager
s
parti
cipa
ting
in a
gro
up e
duca
tiona
l
prog
ram
me,
‘the
scho
oner
pro
gram
me’
,
diff
er fr
om n
on-p
artic
ipan
ts in
atti
tude
s
tow
ards
dia
bete
s and
self-
care
, and
to
eval
uate
the
impa
ct o
n th
e at
titud
es,
HbA
1c a
nd tr
eatm
ent o
f the
prog
ram
me.
Inte
nsiv
e ed
ucat
iona
l
prog
ram
me
run
on a
saili
ng
ship
. The
stud
y us
ed a
‘ref
eren
ce’ g
roup
and
com
pare
d
attit
udes
tow
ards
dia
bete
s and
self-
care
, gly
caem
ic c
ontro
l and
look
ed a
t the
role
of s
ocia
l
netw
orks
.
A to
tal o
f 90
youn
g pe
ople
(mea
n ag
e
15.5
yea
rs (S
D =
0.9
) atte
nded
the
prog
ram
me
Page
101
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
73
125.
Vis
senb
erg
et a
l(125
)
2016
Res
earc
h To
stud
y w
heth
er th
e gr
oup-
base
d
inte
rven
tion
Pow
erfu
l Tog
ethe
r with
Dia
bete
s (PT
WD
) cha
nged
soci
al
supp
ort a
nd so
cial
influ
ence
s, an
d
whi
ch e
lem
ents
of t
he in
terv
entio
n
cont
ribut
ed to
this
.
Qua
litat
ive
Proc
ess e
valu
atio
n.
Soci
al n
etw
ork-
base
d
inte
rven
tion
PTW
D d
evel
oped
,
whi
ch a
imed
to st
imul
ate
soci
al
supp
ort f
or se
lf-m
anag
emen
t
and
dim
inis
h hi
nder
ing
soci
al
influ
ence
s on
self-
man
agem
ent
amon
g so
cioe
cono
mic
ally
depr
ived
pat
ient
s. Th
e
inte
rven
tion
grou
p (I
G) w
as
com
pare
d w
ith a
stan
dard
grou
p-ba
sed
educ
atio
nal
inte
rven
tion
(con
trol g
roup
,
CG
). Q
ualit
ativ
e in
-dep
th
inte
rvie
ws w
ith p
artic
ipan
ts a
nd
inte
rvie
ws w
ith g
roup
lead
ers
wer
e co
nduc
ted.
51 in
-dep
th in
terv
iew
s wer
e ca
rrie
d ou
t
(par
ticip
ants
n=2
7, g
roup
lead
ers n
=24)
126.
Wal
ler
et
al(1
26)
2005
U
K
Res
earc
h To
ass
ess a
dole
scen
ts’ a
nd th
eir
pare
nts’
vie
ws o
n th
e ac
cept
abili
ty a
nd
desi
gn o
f a n
ew d
iabe
tes e
duca
tion
prog
ram
me.
Focu
s gro
up st
udy.
Tw
enty
-fou
r chi
ldre
n an
d 29
par
ents
atte
nded
one
of e
ight
sepa
rate
focu
s
grou
ps.
Page
102
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
74
127.
Wei
nger
K(1
27)
2003
U
SA
Rep
ort/
rese
arch
Des
crip
tion
of d
iffer
ent g
roup
med
ical
visi
t mod
els
Sum
mar
y of
seve
n pa
pers
look
ing
at fi
ve g
roup
med
ical
visi
t mod
els
n/a
128.
Wile
y et
al(1
28)
2014
A
ustra
lia
Res
earc
h To
des
crib
e th
e ex
perie
nce
of d
iabe
tes
educ
atio
n fr
om th
e pe
rspe
ctiv
e of
youn
g ad
ults
with
type
1 d
iabe
tes.
Surv
ey q
uest
ionn
aire
and
focu
s
grou
p st
udy.
150
resp
onde
nts t
o th
e su
rvey
ques
tionn
aire
(30.
5% a
ged
18–2
4 ye
ars)
and
33 p
artic
ipan
ts in
the
focu
s gro
ups
(mea
n ag
e w
as 2
5.1
year
s).
129.
Will
iam
s
&
Pace
(129
)
2009
C
anad
a Sy
stem
atic
revi
ew
To d
eter
min
e w
heth
er p
robl
em b
ased
lear
ning
(PB
L) is
an
effe
ctiv
e
educ
atio
nal s
trate
gy in
chr
onic
dis
ease
man
agem
ent.
Inte
grat
ive
liter
atur
e re
view
-
five
data
base
s wer
e se
arch
ed
and
thirt
een
pape
rs w
ere
incl
uded
in th
e re
view
.
Six
stud
ies i
nvol
ved
child
ren,
adol
esce
nts o
r adu
lts w
ith d
iabe
tes
130.
Won
g S
al(1
30)
2015
C
anad
a R
esea
rch
To re
port
whe
ther
gro
up m
edic
al v
isits
(GM
Vs)
for c
hron
ic c
ondi
tions
, hav
e
tang
ible
ben
efits
for p
rovi
ders
and
patie
nts
Des
crip
tive
stud
y in
clud
ing
in-
dept
h in
terv
iew
s with
pat
ient
s
atte
ndin
g an
d pr
ovid
ers
faci
litat
ing
GM
Vs a
nd d
irect
obse
rvat
ion.
Fiv
e pr
imar
y ca
re
prac
tices
in ru
ral t
owns
and
four
Firs
t Nat
ions
com
mun
ities
parti
cipa
ted.
Inte
rpre
tive,
them
atic
ana
lysi
s was
cond
ucte
d.
34 p
rovi
ders
and
29
patie
nts w
ere
inte
rvie
wed
. Mea
n ag
e of
pat
ient
s was
62 y
ears
old
, mos
tly fe
mal
e an
d m
arrie
d.
The
thre
e m
ost c
omm
on c
hron
ic
cond
ition
s rep
orte
d by
pat
ient
s wer
e
diab
etes
(n =
9),
high
blo
od p
ress
ure
(n
= 8)
and
arth
ritis
(n =
7).
Page
103
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e
75
131.
Yeo
h et
al(1
31)
2015
U
K
Syst
emat
ic
revi
ew
To re
view
edu
catio
nal,
tech
nolo
gica
l
and
phar
mac
olog
ical
inte
rven
tions
aim
ed a
t res
torin
g hy
pogl
ycem
ia
awar
enes
s (H
A) i
n ad
ults
with
type
1
diab
etes
.
Syst
emat
ic re
view
and
met
a-
anal
ysis
- se
ven
data
base
s wer
e
sear
ched
and
43
stud
ies m
et th
e
incl
usio
n cr
iteria
.
Adu
lts o
ver 1
8 ye
ars.
Page
104
of 1
36
CON
FID
ENTI
AL-F
or P
eer R
evie
w O
nly
Dia
bete
s Car
e

76
Page 105 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

77
Appendix 4
Table 3: Illustrative quotes
Page 106 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
78
CMOC 1 When young adults, who do not normally have the opportunity to share experiences with
peers living with diabetes, find a space to connect and share openly with others (C), this
might make it more likely for patients to feel supported (M) and comfortable (M), and could
in turn lead to perceptions of increased understanding and learning (O). (13, 21, 67, 74, 77,
99, 101, 115, 130)
Most patients (87%) indicated they had learned from fellow patients, fellow
patients helped them to understand the information better (75%), and they
learned to ask questions (42%) (Table 6). (77)
Group programmes of patient education have the advantage of stimulating
interactions among participants, which enhance the efficacy of education:
peer listening improves learning, while the opportunity to share one’s
experience about the disease with others provides an effective psychological
support [6]. Interactive formats are thought to be superior to more
traditional, lesson-style group programmes, because they are more effective
in enhancing interaction among patients [7]. (74)
Teen Power offered teens and caregivers the opportunity to negotiate this
balance through dialogue with others who share similar life experiences. In
this way, the group promoted social support and networking. Indeed, this was
the first opportunity for the majority of participants to meet other diabetic
teens and to dialogue with a young adult diabetes mentor. Effective diabetes
management can be particularly difficult for teens at a young developmental
stage. The Teen Power intervention offers these adolescents specific activities
and workshops, as well as an opportunity to learn from their peers. (13)
A self administered satisfaction survey from patients indicated that 96% felt
more supported, 82% better understood information compared to during
Page 107 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
79
regular appointments, 82% felt more comfortable asking questions, 88%
would recommend Team Clinic to others, and 84% wanted to attend another
Team Clinic. (99)
Surrogate question answering Wider evidence suggests that patients will often
be reluctant to ask questions within a one-toone consultation. Within a group
context they may find that a more active participant is more able to vocalise
their own concerns. Patients therefore become vicariously exposed to
information that would not otherwise be forthcoming. (9)
As an SMA lasts longer than an individual appointment and mutual
interaction is actively sought, SMAs may provide more opportunity to discuss
relevant diabetes-related topics and to invite patients to raise current health
issues themselves. In this way, SMA patients learn from each other and pick
up information about topics they were afraid to ask or never thought of
asking. We therefore expect that the children and the adolescents feel more at
ease and more stimulated to contribute to the conversation when they hear
their fellow patients talking about a certain topic. (101)
In the majority of the patients, their fellow patients also helped them to
understand the information better, which is highly relevant given the complex
and multidimensional nature of the disease. Yet, contrary to expectations, in
only a minority of the patients the presence of others helped them to ask
questions.(101)
The participants’ conversational contributions in the different types of visits
suggest that there is more balance in the input of the different participants
during SMAs. This could, however, be ascribed primarily to the higher
Page 108 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
80
conversational contribution of the team members and does, so far, not
indicate that SMAs provide a more safe environment for child patients to
speak up. In addition, the fact that in SMAs silences lasted half as long as in
individual visits, may suggest a more effective use of time, but may also
diminish opportunities of communicating empathy and providing space,
which are both strongly related to silences [18]. (101)
A programme that would engage young people was stated as being essential.
The use of practical sessions was considered to be very important as it was
felt that young people learned more by doing than just talking. Lectures about
the subject areas to be addressed were discouraged with many adolescents
stating that they would simply ‘turn off’ or not return after the first session.
Group discussion, practical demonstrations and fun activities were identified
as the most fruitful means of delivery for this age group (14)
Rather than repeating health education messages (e.g., reasons for a high
HbA1c) across several individual visits, providers taught to the whole group
at once, witnessed reinforcement of key messages by patients sharing their
own experience and, in addition, reported more opportunities for in-depth
patient–provider interactions. (130)
According to the providers, patients react more openly during SMAs and
thereby facilitate this learning process. (77)
Furthermore, parents (37.5%) want their child to attend SMAs in order to
enhance their relationship with other patients with type 1 diabetes. (77)
Group education classes stimulate learning by allowing adults to incorporate
their own experiences with diabetes into class discussion and, thus, actively
Page 109 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

81
engage in the learning process (5). (115)
Both learning communities and SMAs foster increased knowledge, self-
efficacy, a greater understanding of the medical condition, and coping skills.
(21)
Page 110 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
82
CMOC2 When group interactions enable peer support, young adults who feel more isolated,
experience negative perceptions of self-management and/or face diabetes-related distress (C),
may draw encouragement from each other (M), which could subsequently lead to more
confidence and motivation in their self-management (O). (67, 77, 81, 130)
Patients attending GMVs reported increased confidence and skills in
managing their health within their personal and social context. One patient
stated: “… you come out of the group feeling much more self-confident …
you’ve got your batteries recharged and you can really go till the next group
… it’s [GMV] more motivating … you want to do more yourself and rely less
on others … but then you always realize there’s others out there to help you if
needed.” (Patient #16) (130)
As well as helping to raise their self-esteem, and overcome feelings of
isolation, patients talked about how the group interactions had also enhanced
their capacity to comprehend and assimilate information during the course.
(67)
“Group was the one place I could really open up and talk about my diabetes
and feel good about it.” (81)
Openness like this encouraged the group to talk about relationships and
sharing responsibilities. (70)
According to the parents (37.5%), SMAs are only useful when children act
openly and are committed, not when SMAs are seen as unpleasant. (77)
For young adults who experience denial towards their diagnosis – group
clinics can provide a safe space to discover what it means to live with
diabetes. (81)
Page 111 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
83
CMOC 3 Peer support in group clinics for young adults who experience their diagnosis and self-
management as socially stigmatising (C), may help instil a sense of normalcy (M), which
could lead to re-thinking self-monitoring and management in social settings (O). (9, 13, 31,
51, 65, 67, 70, 90)
Injecting insulin was not a value-neutral medical procedure but a social
practice which people with diabetes deemed appropriate or inappropriate in
different contexts. (51)
Also, compared to individual treatment, practice of key diabetes management
skills within the social context of a therapeutic group may be more effective
for generalization of the skills adolescents need to apply in peer social
settings. (90)
A review of behavioral interventions found that almost one half of the
treatments for adolescents with diabetes were delivered in group formats
(Hampson et al., 2000). Interactions with peers who share the experience of
diabetes, which may be more difficult to arrange through individual therapy,
may foster a sense of normalcy (Citrin, Zigo, LaGreca, & Skyler, 1982). (90)
SMAs help patients break from their cognitive dissonance pertaining to their
illness, and coming out of concealing or normalizing their conditions [29].
(65)
[…] the selfcare behaviours that they are being encouraged to pursue are
likely to feel at odds with the prevailing social norms for their age group (31)
In this context involvement of patients in their own monitoring, particularly
where this requires hands-on engagement with monitoring equipment, may be
Page 112 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
84
both a practical and symbolic way of getting them to start to engage with
their own management. (9)
For example, teens who openly engaged in diabetes management behaviors
within the group setting appeared to have a positive influence on peers who
were reluctant. (13)
Some adolescents reported that they had fewer objections to measuring their
glucose values and injecting insulin in public after the intervention [peer-
group support and problem-solving training]. (70)
[…]interactions not only enhanced the depth and breadth of learning which
took place, but also, at a deeper and more fundamental level, they led to
transformations in course participants’ perceptions of, and orientations to
risk (and risk-taking), and, associatedly, their conversion into insulin dose-
adjusting subjects. (67)
Page 113 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
85
CMOC4 Where group clinic bring together participants who have common characteristics or shared
experiences (C), it is assumed that a sense of affinity is more likely to emerge between group
members (M), which could lead to increased sharing and sustained interest as participants
will be able to relate to each other’s experiences (O). (21, 23, 77, 107, 115)
[…] patients can benefit from attending a group which offers an accumulated
pool of experience. However, this consideration needs to be balanced against
that of ensuring that group sizes are not so large that opportunities for
interactions between participants, or for the daily review of individual data,
are compromised, as this may reduce a SEP’s effectiveness. (67)
For parents (62.5%), SMAs should preferably be attended by patients with
similar ages, attitudes, problems, and types of insulin treatment. (77)
[intended to ensure topics of interest to all participants will be covered in
full.]
To maximize the benefit of group education, participants must be able to
relate to each other’s shared experiences to inform or influence their own
behavior (5). (Smaldone, Ganda et al. 2006)
SMAs for adolescents who continue to meet together are similar to those that
participate in a learning community. The group bonding and camaraderie
that develop over time can lead to identity within the group, and give
adolescents the opportunity to share common struggles (Eisenstat et al.,
2012). (21)
They did not perceive age-banding as having the function of allowing
interaction with peers in the clinic setting. This is supported by the findings
from a qualitative study carried out by Datta (2003). She suggested that older
Page 114 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
86
adolescents and young adults are not generally comfortable with shared
activities, and that these have limited attractiveness, especially when
arranged by staff. (30)
During SMAs with adolescents, the team and group members address
transition issues over time, making the process less stressful. (Davis and
Vitagliano 2015)
For adolescents, an SMA can be seen as a step to independence. As one
parent reacted: “My influence during medical visits is gradually decreasing.
This is very important”. (77)
Difficulties in delivering the intervention particularly occurred when sessions
had groups of participants with a wide age range or group numbers were
very small. ‘The first group that we ran had two girls and a boy and the boy
was at the younger end of the teenage years and the girls were at the older, it
was unfortunate because we didn’t have that many patients as part of the
study so it was very difficult then to get the groups sorted out so we kind of
had to put them together. […] He was just a bit of a silly boy in that…I don’t
mean horribly, he was lovely, but just kind of played the fool a little bit
whereas the girls were older and a similar age and a lot more grown up
about it all.’ (Site educator) (107)
According to an equal number of parents, the topics discussed during an
individual appointment are more tailored to the individual patient. If their
child experiences unusual problems, these problems are more easily
addressed during an individual appointment. It is important to parents that
their children receive sufficient individual attention from health care
Page 115 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

87
providers during an SMA. (77)
Our opinion is that the time built into our SMA model for individual attention
during goal setting, history and physical, and wrap-up allowed for flexibility
to personalize group sessions based on recurrent themes among the
individuals, leading to these improvements. (40)
At times there were common issues and therefore group discussion of blood
glucose levels were relevant but on the whole this component became less
rather than more important as time went on. (12)
There were a few patients who thought if the GMV had too many people that
patients’ time was not used appropriately because they needed to listen to too
many patients’ health concerns. (130)
SMAs were also valued negatively by some parents (25%) when patients are present
who do not want to participate or when patients do not interact with each other. (77)
Page 116 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
88
CMOC5 In contexts where young adults have previously experienced a collaborative, helpful and
respectful relationship with their clinicians, characterised by mutual understanding (C), it is
more likely they will feel safe in exposing vulnerabilities (M) and that they will perceive
added value and usefulness from interactions with services providers who know them well
(M), which may lead to increased engagement with the service (O) and increased attendance
(O). (29, 30, 55)
Meeting service providers at appointments with whom young adults had a
relationship reinforced their engagement with the clinic, indicating that a
reciprocal relationship existed between relationships and engagement. In
addition, engagement positively influenced young adults’ diabetes-related
perceptions and behaviours, preventing a cycle of inadequate self-
management, distress, and non-attendance from developing.
‘If you were having a tough time with your bloods they’ll schedule times to
ring you over a few weeks and they’ll keep in contact with you until you have
it under control again, which is great like, so you always have somebody
there.’ Young adult 6, female, age 26, 50–75% attendance (55)
By continuing to deliver diabetes services to young adults using existing
models, high rates of clinic non-attendance are likely to persist, as the
findings of this study suggest that young adults actively respond only after
experiencing collaboration with, and support from, service providers. (55)
Once a relationship existed, experiences with supportive and understanding
service providers made young adults more likely to attend the diabetes clinic
despite feelings of distress, due to the knowledge and confidence they had that
they would benefit from attending.(55)
Other participants, who relied more on secondary care services, described a
Page 117 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
89
level of disengagement because of the lack of staff continuity, characterised
by feeling like a passive participant in consultations and questioning the
benefits of the advice given or of attending appointments: … [Y]ou’re telling
this doctor about your diabetes, and the next time, you’re telling another
doctor and they just preach to you the same things … If there’s not a patient–
doctor build-up, then you think, ‘Well, why should I bother coming?’ (Female,
22 years) (30)
Participants highlighted continuity of contact as helpful:
… [T]he trust and everything is already there … If not, that’s a slight
resentment: someone walks through the door, and 5 minutes later, they’re
telling you to cut this out and do that. It’s like, ‘Who are you to tell me?’
(Male, 21 years)
She was there on the end of the phone … I could talk to her and she knew the
basic background of my family, how I had become pregnant, everything – that
I’d lost a baby beforehand … and she was with me through that as well, so
she was brilliant … just listened and helped. (Female, 22 years) (30)
The data suggest that continuity of contact would allow a young person to feel
that their situation was understood without the need to retell their history.
This would appear to result in an increased level of trust, perceived
usefulness of contact, ease with which the young person can negotiate the
practicalities of clinics, make telephone contact between clinics and the
amount of rapport within the relationship. (30)
The quality of the relationship with the health care professional was seen to
be essential. The style of the consultation and the attitude of the health care
Page 118 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

90
professional working with the young person were seen to be at the core. This
involved seeing the same person and developing trust and rapport as well as
including family, friends and partners when required, in a manner that was
flexible and responsive. (29)
Page 119 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
91
CMOC6 An increased emphasis on positive aspects of self-management and developmentally tailored
attention to sensitive emotional needs over other priorities, for young adults who remain
ambivalent about their role as diabetes patients (C), may help young adults slowly build self-
esteem (M) and take a more active role in their self-management (O). (14)
A majority of our time, however, was devoted to focusing on the emotional
and motivational needs of the students, which are equally important. As one
teen remarked in one of the meetings, “We know about diabetes care, we
learned that at the hospital. If we don’t want to take care of ourselves, no one
is going to make us do it. Only we will, when we are ready.” (81)
Participants also highlighted the importance of having a programme which
could inspire and motivate them to take an active role in their diabetes
management because they want to, rather than because they have to. (113)
The Teen Power curriculum was designed to promote the development of
health promoting behaviors among Type 1 diabetic teens by simultaneously
targeting medical adherence and psychosocial barriers in order to optimize
positive treatment outcomes.(13)
Ambivalence appears to be an issue and it seems ‘clinical styles that are
respectful, acknowledge choices and ambivalence and do not increase
resistance seem to be logical’.33 Interventions are empathic,
nonconfrontational, use reflections, develop self-efficacy and highlight
discrepancies from the young person’s perspective. (29)
Sensitive use of language is also essential; for example, we can discuss
‘choices and behaviours’ rather than ‘problems or issues’ unless labelled by
the young person in that way. (29)
Page 120 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
92
[…] an adolescent at a stage of development prior to the development of
more abstract styles of thinking would not find discussions about the long-
term complications of diabetes meaningful. Instead he or she might feel
confused and overwhelmed and may withdraw as a means of self-protection.
(29)
[…] during regular follow-up visits, young patients often behave in a passive
way to back out of their responsibility to take care of their disease(101)
the effect this has on their engagement with services can be hard for health
care professionals to manage as it can result in the young person oscillating
between engagement and interest in diabetes and detachment and disinterest.
(29)
It is suggested that this results in blurred social boundaries where young
people in these age groups are sometimes considered as children and
sometimes considered as adults, rather than being allowed to flourish in their
own right, somewhere in-between. As a result, the oscillation, transaction and
ambiguity, normative and necessary for development, become labelled as
problematic, as they do not clearly fit with the social constructions of
childhood or of adulthood, and problem saturated stereotypes of young
people are allowed to dominate. (31)
Doctors often spend much time and effort trying to achieve control, minimise
disease progression, and reduce complications of chronic illness. Young
people, on the other hand, are far more interested in achieving the
developmental tasks of adolescence.’ They conclude that broadening the
disease-focused perspective would achieve better health outcomes and reduce
Page 121 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care

93
the conflict between the perspective of the professional and the young person.
(29)
They could also have additional, specific psychological vulnerabilities to
manage, associated with the demands of diabetes, such as eating problems,
social isolation, fear of stigma, poor intimate relationships, depression, poor
self-efficacy and low perceived control (29)
“When I went into college I think as most people do, diabetes became the last
thing on my mind, I didn’t care, I didn’t want to know about it.” Young adult
6, female, age 26, 50–75% attendance (55)
‘He tells me he plays football and goes to the gym. He doesn’t make any
special preparation for doing sports. Mum says he takes Lucozade with him.
Asghar insists he doesn’t and then Mum says he drank a whole bottle before
football. She gets frustrated with him “What about the time I chased after you
because you’d taken four bottles!”“I was taking them for my mates” Mum
looks disgruntled - “They’re too expensive to give them to your mates”.’
Field notes from home visit to Asghar, age 16, type 1 diabetes for 7 years,
IMD score 67.1 Lucozade is a commercial carbonated carbohydrate drink
which many participants used to treat hypoglycaemic attacks, but which is
also marketed as a sports drink. By handing out bottles to his friends, Asghar
may have successfully de-medicalised his treatment and achieved social gain,
but this trade-off had a very different social meaning for his mother, who was
struggling to feed a family of six on state benefits. (51)
Page 122 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
94
CMOC7 With time people who engage in group sessions (C), make continuous judgments about the
added value of these sessions to their own individual needs (M), which leads them to decide
whether they will keep engaging with the group (O). (9, 12, 70, 74, 77, 98, 101, 109)
However, while patients, in their follow-up interviews, highlighted some
benefits to be gained from attending follow-up sessions in a group, most
indicated a preference and need for one-to-one support. This included M7,
who described group-based follow-ups as mitigating opportunities for
patients to: “talk about their own individual circumstances ... everyone’s an
individual and I think everyone has individual needs... and events happening
in their lives” (M7.3). Several patients also expressed dissatisfaction with
reviews of blood glucose readings at six week follow-up sessions. While
patients had collected blood glucose data for six weeks, the requirement for
all patients’ readings to be reviewed meant there was only time to examine
their most recent results. M14, for instance, described how educators had
reviewed blood glucose readings that he had gathered over the preceding two
or three days, which, he suggested, could result in a focus applied to an
unrepresentative sample of results collected over “a very small period of that
six weeks”. (98)
Self-help groups can improve the psychological status and health-related QoL
of patients [10–12], but fail to modify metabolic control [10, 12]. In fact, the
format of the self-help group is not efficient for the transmission of structured
knowledge, which is also required for the improvement of metabolic control
[3]. Interactive group programmes which also include the provision of
technical information by health professionals in a more structured format,
with a pre-defined schedule of topics, could be more effective in the
Page 123 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
95
improvement of metabolic control [13]. (74)
Parents (25%) also value the privacy of an individual visit, particularly when
discussing personal problems. (77)
[…] some patients also identified themselves as not wanting to attend more
Gmvs because they did not want to talk about their issues, nor hear other
patients’ issues in a group. (130)
Any instance in which such public disclosure is bad for the patient may result
in negative outcomes. For some patients who already have high levels of self-
efficacy and who are private by nature, the SMA environment may prove to be
stressful in ways that private clinical encounters are not. (65)
A relevant proportion of patients invited did not attend group sessions. A low
participation rate seems to be common for long-term educational
programmes, particularly when dealing with established cases. (74)
In other accounts, patients sought and/or expressed a preference for
individualised and tailored support, provided by specialists, that was
responsive to changes in their personal circumstances and lifestyles. For
example, F2 described having needed, and received, regular and intensive
educator support after she became pregnant, to review and change quick-
acting ratios and basal insulin doses, to control unstable and fluctuating
blood glucose readings. (98)
Most of these participants reported that they rarely met outside the group and
interest in the group appeared less important as time went on. Over time for
many participants there was a shift from working and learning with others to
Page 124 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
96
solving my issues and the need to focus on me again. “Not really I mean at
this stage I’m not sure how much more group work would actually be of
benefit to me” (P9-096 12 months). “I think I find now after all this time the
group session there’s not as much said as before, because it’s the same kind
of people having the same kind of problems. And you kind of think now it
might be better off just to speak to the expert rather than listen to - again like
in the beginning it was - you learnt an awful lot from everybody else, but now
I don’t think so much now"(P13-100 12 months). (12)
Most participants reported that the group education sessions became less
important over time as participants required individual one to one responsive
practical support and advice available as needed, focusing on their unique
concerns. These findings are substantiated in other studies [8,48,49]. In
particular, participants in this study reported that they wanted timely access
to the right health professional when they were making real efforts to change
but were being hampered by a transient problem they did not know how to
manage. The need for timely support to resolve crises that threaten patients’
ability to self manage has also been highlighted by other writers [33,36]. (12)
To add, although patients did not mind the extra time investment and they
would recommend others to participate in an SMA as well, only half of them
would choose an SMA again next time. This latter finding may suggest that
SMAs and individual visits complement rather than replace each other, and
may therefore need to be offered interchangeably to guarantee high quality
diabetes care as well as visit adherence.(101)
The present study shows that group interventions for adolescents with type 1
Page 125 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
97
diabetes are effective when combined with individual consultations.
Discussing certain personal issues may feel more appropriate in an
individual consultation, while other issues may be more suitable for
discussion with peers in groups.(70)
Our qualitative study adds to Smith et al’s concerns about promoting group-
based support in diabetes clinical practice, particularly if this support is
offered in isolation from other types of inputs and interventions. We have also
provided insights into why group-based follow-ups may not necessarily be a
popular or effective approach – albeit in this instance, through a focus on
type 1 diabetes patients. Specifically, we have shown that a group-based
approach may be incompatible with patients’ need for individualised input
from health professionals post-course, to accommodate their specific and
personal experiences of applying their treatment regimens in everyday life.
(98)
There were few long-term studies examining the effectiveness of group
medical visits for diabetes care. Fifteen of the 26 studies were 12 months or
less in duration, and 6 studies were up to 2 years in duration. The study with
the longest duration followed patients for 5 years after the intervention.
Therefore, the long-term or sustainable outcomes of group medical visits are
unclear, and it is difficult to know if the outcomes were maintained for a
substantial length of time after the intervention. (54)
A significant proportion of those invited decline, largely because they do not
recognise benefits against the perceived advantages of an individual
consultation. (9)
Page 126 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
98
However, effort should be put into ways of improving access to the
intervention. First, more personalised information about the intervention and
advantages of participation could have been presented to the adolescents and
parents. Second, more effort might have been put into the issue of motivating
them to be willing to meet with others unfamiliar to them. Third, using
incentives and various forms of rewards for participation might encourage
participation. (70)
When comparing the two forms of SMS [self-management support], we found
that the ATDM [automated telephone disease management] model not only
reached a greater proportion of the target population than the group medical
visit model, but it also yielded particularly high rates of engagement for those
with limited literacy and limited English proficiency. For health system
planners and practitioners in health education and health promotion, this
suggests that the relative accessibility and targeting of the ATDM technology,
combined with its proactive nature and hierarchical logic, can provide a
strategy to reverse the inverse care law and reduce health care disparities.
(109)
Most patients (n = 45) appeared to be satisfied with the SMA directly after
having attended the SMA (M = 4.22, SD = 0.81). Their satisfaction tended to
decrease after 3 months (M = 3.76, SD = 1.15; t (28) = 1.94, P = 0.06) (77)
Perversely those least likely to communicate or engage in a group setting may
be the very ones who are most need supplemental individualised care. (9)
Page 127 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
99
CMOC8 For young adults who have negative perceptions about their ability to self-manage or who
face diabetes-related distress (C), fear they may be diagnosed with further health problems
(M), may lead them to disengage from the service (O). (15, 43, 55)
Even with the moderate intensity of our programme, a certain number of
adolescents chose not to participate or were lost during follow-up, giving the
intervention a completion rate of 39 of 55 patients, or 71%. Adolescents lost
during follow-up in both the intervention and control groups had significantly
lower scores on self-reported self-esteem and general health in the generic
measurement, a worse perception of diabetes-related impact, and higher
HbA1c. These adolescents appeared to have less self-confidence and
perceived a greater impact of the disease than did the other participants. This
suggests that there might be problems in reaching adolescents with these
particular problems. (43)
Dissatisfaction among young adults with the perceived quality of their self-
management was described by some young adults as a motivator, and by
others as a significant barrier, to clinic attendance. ‘I should be going to the
clinics, but the fear that I have is that they’re [service providers] going to
turn around and go well you’ve the signs of diabetes eye disease or your
kidney function isn’t as good as it should be; that’s what terrifies me.’ Young
adult 7, female, age 22, <50% attendance (55)
Take up was particularly low for those young people with the highest HbA1c.
Those who attended had significantly lower mean baseline HbA1c scores than
those who did not attend (9.52% (81 mol/mol) vs 10.33% (89 mmol/ mol),
p<0.01). (15)
Page 128 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
100
Previous research has highlighted that seemingly innocuous behaviours have
been interpreted as intrusive and an accusation of incapability by adolescents
when delivered by parents (Seiffge-Krenke et al., 2013). It is possible that
these behaviours elicit the same reaction when conveyed by peers. (28)
Close friends that can take a supportive role in a measured way are seen as
helpful but those that worry about diabetes or overly monitor the young
person’s self-care behaviours, are seen as unhelpful. (31)
Page 129 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
101
References
1. Abolfotouh MA, Kamal MM, El-Bourgy MD, Mohamed SG. Quality of life and glycemic control in adolescents with type 1 diabetes and the impact of an education intervention. International Journal of General Medicine. 2011;4:141-52. 2. Abualula NA, Jacobsen KH, Milligan RA, Rodan MF, Conn VS. Evaluating Diabetes Educational Interventions With a Skill Development Component in Adolescents With Type 1 Diabetes: A Systematic Review Focusing on Quality of Life. Diabetes Educator. 2016;42(5):515-28. 3. Albano MG, Crozet C, d'Ivernois JF. Analysis of the 2004-2007 literature on therapeutic patient education in diabetes: results and trends. Acta Diabetologica. 2008;45(4):211-9. 4. Altundag S, Bayat M. Peer Interaction and Group Education for Adaptation to Disease in Adolescents with Type 1 Diabetes Mellitus. Pakistan Journal of Medical Sciences. 2016;32(4):1010-4. 5. Anderson BJ, Wolpert HA. A developmental perspective on the challenges of diabetes education and care during the young adult period. Patient Education and Counseling. 2004;53(3):347-52. 6. Attari A, Sartippour M, Amini M, Haghighi S. Effect of stress management training on glycemic control in patients with type 1 diabetes. Diabetes Research and Clinical Practice. 2006;73(1):23-8. 7. Beer R, Eiser C, Johnson B, Bottrell K, Whitehead V, Elliott J, et al. WICKED: The development and evaluation of a psycho-education programme for young people with type 1 diabetes. Journal of Diabetes Nursing. 2014;18(6):233-7. 8. Bleakly R, McKee A. Outcomes of a local adolescent education programme in Northern Ireland. Journal of Diabetes Nursing. 2010;14(3):96-101. 9. Booth A, Cantrell A, Preston L, Chambers D, Goyder E. What is the evidence for the effectiveness, appropriateness and feasibility of group clinics for patients with chronic conditions? A systematic review. Health Services and Delivery Research. 2015;3(46). 10. Cahill SM, Polo KM, Egan BE, Marasti N. Interventions to Promote Diabetes Self-Management in Children and Youth: A Scoping Review. American Journal of Occupational Therapy. 2016;70(5):7005180020p1-8. 11. Campbell F, Biggs K, Aldiss SK, O'Neill PM, Clowes M, McDonagh J, et al. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database of Systematic Reviews. 2016;4:CD009794. 12. Casey D, Murphy K, Lawton J, White FF, Dineen S. A longitudinal qualitative study examining the factors impacting on the ability of persons with T1DM to assimilate the Dose Adjustment for Normal Eating (DAFNE) principles into daily living and how these factors change over time. BMC Public Health. 2011;11:672. 13. Céspedes-Knadle YM, Munoz CE. Development of a group intervention for teens with type 1 diabetes. The Journal for Specialists in Group Work. 2011;36(4):278-95. 14. Chaney D, Coates V, Shevlin M, Carson D, McDougall A, Long A. Diabetes education: what do adolescents want? Journal of Clinical Nursing. 2012;21(1-2):216-23. 15. Christie D, Thompson R, Sawtell M, Allen E, Cairns J, Smith F, et al. Effectiveness of a structured educational intervention using psychological delivery methods in children and adolescents with poorly controlled type 1 diabetes: a cluster-randomized controlled trial of the CASCADE intervention. BMJ Open Diabetes Research & Care. 2016;4(1):e000165. 16. Christie D, Thompson R, Sawtell M, Allen E, Cairns J, Smith F, et al. Structured, intensive education maximising engagement, motivation and long-term change for children and young people with diabetes: a cluster randomised controlled trial with integral process and economic evaluation - the CASCADE study. Health Technology Assessment (Winchester, England). 2014;18(20):1-202. 17. Clancy DE, Yeager DE, Huang P, Magruder KM. Further evaluating the acceptability of group visits in an uninsured or inadequately insured patient population with uncontrolled type 2 diabetes. The Diabetes Educator. 2007;33(2):309-14.
Page 130 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
102
18. Coffen RD, Dahlquist LM. Magnitude of type 1 diabetes self-management in youth: health care needs diabetes educators. Diabetes Educator. 2009;35(2):302-8. 19. Colson S, Cote J, Gentile S, Hamel V, Sapuppo C, Ramirez-Garcia P, et al. An Integrative Review of the Quality and Outcomes of Diabetes Education Programs for Children and Adolescents. Diabetes Educator. 2016;42(5):549-84. 20. Davidson M, Penney ED, Muller B, Grey M. Stressors and self-care challenges faced by adolescents living with type 1 diabetes [corrected] [published erratum appears in APPL NURS RES 2004 Aug;17(3):221]. Applied Nursing Research. 2004;17(2):72-80. 21. Davis LM, Vitagliano CP. Shared Medical Appointments for Adolescents With Type 1 Diabetes Mellitus: Important Learning Communities. Journal of Pediatric Nursing. 2015;30(4):632-4. 22. Davis AM, Sawyer DR, Vinci LM. The Potential of Group Visits in Diabetes Care. Clinical Diabetes. 2008;26(2):58-62. 23. Day E. Group education for young people with diabetes. Journal of Diabetes Nursing. 2007;11(3):5p-p. 24. Debaty I, Halimi S, Quesada JL, Baudrant M, Allenet B, Benhamou PY. A prospective study of quality of life in 77 type 1 diabetic patients 12 months after a hospital therapeutic educational programme. Diabetes & Metabolism. 2008;34(5):507-13. 25. DeCoster VA, Cummings SM. Helping adults with diabetes: a review of evidence-based interventions. Health & Social Work. 2005;30(3):259-64. 26. Di Battista AM, Hart TA, Greco L, Gloizer J. Type 1 diabetes among adolescents: reduced diabetes self-care caused by social fear and fear of hypoglycemia. Diabetes Educator. 2009;35(3):465-75. 27. Dickinson JK, O'Reilly MM. The lived experience of adolescent females with type 1 diabetes. Diabetes Educator. 2004;30(1):99-107. 28. Doe E. An analysis of the relationships between peer support and diabetes outcomes in adolescents with type 1 diabetes. Journal of Health Psychology. 2016;07:07. 29. Doherty Y, Dovey-Pearce G. Understanding the developmental and psychological needs of young people with diabetes. Implications for providing engaging and effective services. Practical Diabetes International. 2005;22(2):59-64. 30. Dovey-Pearce G, Hurrell R, May C, Walker C, Doherty Y. Young adults’(16–25 years) suggestions for providing developmentally appropriate diabetes services: a qualitative study. Health & social care in the community. 2005;13(5):409-19. 31. Dovey-Pearce G, Doherty Y, May C. The influence of diabetes upon adolescent and young adult development: a qualitative study. British Journal of Health Psychology. 2007;12(Pt 1):75-91. 32. Dovey-Pearce G. Improving care for young people: Ask them and they will tell you. Practical Diabetes. 2015;32(4):147. 33. Due-Christensen M, Zoffmann V, Hommel E, Lau M. Can sharing experiences in groups reduce the burden of living with diabetes, regardless of glycaemic control? Diabetic Medicine. 2012;29(2):251-6. 34. Edelman D, McDuffie JR, Oddone E, Gierisch JM, Williams JW. Shared medical appointments for chronic medical conditions: a systematic review. VA-ESP Project #09-010. Durham, NC: Evidence-based Synthesis Program Center; 2012. 35. Ellis M, Jayarajah C. Adolescents' view and experiences of living with type 1 diabetes. Nursing Children & Young People. 2016;28(6):28-34. 36. Elwyn G, Greenhalgh T, Macfarlane F. Groups: A guide to small group work in healthcare, management, education and research: Radcliffe Publishing; 2001. 37. Ersig AL, Tsalikian E, Coffey J, Williams JK. Stressors in Teens with Type 1 Diabetes and Their Parents: Immediate and Long-Term Implications for Transition to Self-Management. Journal of Pediatric Nursing. 2016;31(4):390-6.
Page 131 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
103
38. Fernandes SM, O'Sullivan-Oliveira J, Landzberg MJ, Khairy P, Melvin P, Sawicki GS, et al. Transition and transfer of adolescents and young adults with pediatric onset chronic disease: The patient and parent perspective. Journal of Pediatric Rehabilitation Medicine. 2014;7(1):43-51. 39. Fitzpatrick SL, Schumann KP, Hill-Briggs F. Problem solving interventions for diabetes self-management and control: a systematic review of the literature. Diabetes Research & Clinical Practice. 2013;100(2):145-61. 40. Floyd BD, Block JM, Buckingham BB, Ly T, Foster N, Wright R, et al. Stabilization of glycemic control and improved quality of life using a shared medical appointment model in adolescents with type 1 diabetes in suboptimal control. Pediatric Diabetes. 2016;26:26. 41. Foster G, Taylor SJC, Eldridge SE, Ramsay J, Griffiths CJ. Self-management education programmes by lay leaders for people with chronic conditions. Cochrane Database of Systematic Reviews. 2007(4). 42. Gage H, Hampson S, Skinner TC, Hart J, Storey L, Foxcroft D, et al. Educational and psychosocial programmes for adolescents with diabetes: approaches, outcomes and cost-effectiveness. Patient Education & Counseling. 2004;53(3):333-46. 43. Graue M, Wentzel-Larsen T, Hanestad BR, Sovik O. Evaluation of a programme of group visits and computer-assisted consultations in the treatment of adolescents with Type 1 diabetes. Diabetic Medicine. 2005;22(11):1522-9. 44. Grey M, Schreiner B, Pyle L. Development of a diabetes education program for youth with type 2 diabetes. Diabetes Educator. 2009;35(1):108-16. 45. Ha Dinh TT, Bonner A, Clark R, Ramsbotham J, Hines S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: A systematic review. JBI Database of Systematic Reviews and Implementation Reports. 2016;14(1):210-47. 46. Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al. Behavioral interventions for adolescents with type 1 diabetes - How effective are they? Diabetes Care. 2000;23(9):1416-22. 47. Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al. Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: A systematic review. Health Technology Assessment. 2001;5(10):i+iii-iv+1-69. 48. Hill-Briggs F. Problem solving in diabetes self-management: A model of chronic illness self-management behavior. Annals of Behavioral Medicine. 2003;25(3):182-93. 49. Hilliard ME, Harris MA, Weissberg-Benchell J. Diabetes resilience: a model of risk and protection in type 1 diabetes. Current Diabetes Reports. 2012;12(6):739-48. 50. Hilliard ME, Powell PW, Anderson BJ. Evidence-based behavioral interventions to promote diabetes management in children, adolescents, and families. American Psychologist. 2016;71(7):590-601. 51. Hinder S, Greenhalgh T. " This does my head in". Ethnographic study of self-management by people with diabetes. BMC health services research. 2012;12(1):83. 52. Hoddinott P, Allan K, Avenell A, Britten J. Group interventions to improve health outcomes: a framework for their design and delivery. BMC Public Health. 2010;10(1):800. 53. Housden LM, Wong ST. Using Group Medical Visits With Those Who Have Diabetes: Examining the Evidence. Current Diabetes Reports. 2016;16 (12) (no pagination)(134). 54. Housden L, Wong ST, Dawes M. Effectiveness of group medical visits for improving diabetes care: a systematic review and meta-analysis. CMAJ Canadian Medical Association Journal. 2013;185(13):E635-44. 55. Hynes L, Byrne M, Casey D, Dinneen SF, O'Hara MC. 'It makes a difference, coming here': A qualitative exploration of clinic attendance among young adults with type 1 diabetes. British Journal of Health Psychology. 2015;20(4):842-58. 56. Hynes L, Byrne M, Dinneen SF, McGuire BE, O'Donnell M, Mc Sharry J. Barriers and facilitators associated with attendance at hospital diabetes clinics among young adults (15-30 years) with type 1 diabetes mellitus: a systematic review. Pediatric Diabetes. 2016;17(7):509-18.
Page 132 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
104
57. Jaber R, Braksmajer A, Trilling JS. Group visits: a qualitative review of current research. JABFM. 2006;19. 58. Jaber R, Braksmajer A, Trilling J. Group visits for chronic illness care: models, benefits and challenges. Family practice management. 2006;13(1):37. 59. Keers JC, Blaauwwiekel EE, Hania M, Bouma J, Scholten-Jaegers SM, Sanderman R, et al. Diabetes rehabilitation: Development and first results of a Multidisciplinary Intensive Education Program for patients with prolonged self-management difficulties. Patient Education and Counseling. 2004;52(2):151-7. 60. Keers JC, Bouma J, Links TP, ter Maaten JC, Gans RO, Wolffenbuttel BH, et al. One-year follow-up effects of diabetes rehabilitation for patients with prolonged self-management difficulties. Patient Education and Counseling. 2006;60(1):16-23. 61. Keough L, Sullivan-Bolyai S, Crawford S, Schilling L, Dixon J. Self-management of Type 1 Diabetes Across Adolescence. Diabetes Educator. 2011;37(4):486-500. 62. Kichler J, Kaugars A, Marik P, Nabors L, Alemzadeh R. Effectiveness of groups for adolescents with type 1 diabetes mellitus and their parents. Families, systems & health : the journal of collaborative family healthcare [Internet]. 2013; 31(3):[280-93 pp.]. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/294/CN-00995294/frame.html. 63. Kime N, McKenna J, Webster L. Young people's participation in the development of a self-care intervention--a multi-site formative research study. Health Education Research. 2013;28(3):552-62. 64. Kirk S, Beatty S, Callery P, Gellatly J, Milnes L, Pryjmachuk S. The effectiveness of self-care support interventions for children and young people with long-term conditions: a systematic review. Child: Care, Health & Development. 2013;39(3):305-24. 65. Kirsh SR, Aron DC, Johnson KD, Santurri LE, Stevenson LD, Jones KR, et al. A realist review of shared medical appointments: How, for whom, and under what circumstances do they work? BMC Health Services Research. 2017;17(1):113. 66. Lavoie JG, Wong ST, Chongo M, Browne AJ, MacLeod ML, Ulrich C. Group medical visits can deliver on patient-centred care objectives: results from a qualitative study. BMC Health Services Research. 2013;13(1):155. 67. Lawton J, Rankin D. How do structured education programmes work? An ethnographic investigation of the dose adjustment for normal eating (DAFNE) programme for type 1 diabetes patients in the UK. Social Science & Medicine. 2010;71(3):486-93. 68. Leelarathna L, Guzder R, Muralidhara K, Evans ML. Diabetes: glycaemic control in type 1. Clinical Evidence. 2011;09:09. 69. Lirussi F. The global challenge of type 2 diabetes and the strategies for response in ethnic minority groups. Diabetes/Metabolism Research Reviews. 2010;26(6):421-32. 70. Løding RN, Wold JE, Skavhaug A, Graue M. Evaluation of peer-group support and problem-solving training in the treatment of adolescents with type 1 diabetes. European Diabetes Nursing. 2007;4(1):28-33. 71. Lovell N. The 'SKIP' course: A programme for children and young people with diabetes. Journal of Diabetes Nursing. 2012;16(6):247-52. 72. Lyons SK, Libman IM, Sperling MA. Diabetes in the adolescent: Transitional issues. Journal of Clinical Endocrinology and Metabolism. 2013;98(12):4639-45. 73. Mallow JA, Theeke LA, Barnes ER, Whetsel T. Examining dose of Diabetes Group Medical Visits and characteristics of the uninsured. Western Journal of Nursing Research. 2015;37(8):1033-61. 74. Mannucci E, Pala L, Rotella CM. Long-term interactive group education for type 1 diabetic patients. Acta Diabetologica. 2005;42(1):1-6. 75. Markowitz JT, Laffel LM. Transitions in care: support group for young adults with Type 1 diabetes. Diabetic Medicine. 2012;29(4):522-5. 76. Mead S, MacNeil C. Peer support: what makes it unique? Int J Psychosoc Rehabil. 2006;10.
Page 133 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
105
77. Mejino A, Noordman J, van Dulmen S. Shared medical appointments for children and adolescents with type 1 diabetes: perspectives and experiences of patients, parents, and health care providers. Adolescent Health Medicine & Therapeutics. 2012;3:75-83. 78. Mulvaney SA, Mudasiru E, Schlundt DG, Baughman CL, Fleming M, VanderWoude A, et al. Self-management in type 2 diabetes: the adolescent perspective. Diabetes Educator. 2008;34(4):674-82. 79. Murphy K, Casey D, Dinneen S, Lawton J, Brown F. Participants' perceptions of the factors that influence diabetes self-management following a structured education (DAFNE) programme. Journal of Clinical Nursing. 2011;20(9-10):1282-92. 80. Murphy HR, Rayman G, Skinner TC. Psycho-educational interventions for children and young people with Type 1 diabetes. Diabetic Medicine. 2006;23(9):935-43. 81. Newman D. School nurse-facilitated group meetings for adolescents with diabetes. NASN School Nurse. 2012;27(1):15-7. 82. Noffsinger EB. Running Group Visits in Your Practice. New York, NY: Springer; 2009. 83. Noordman J, van Dulmen S. Shared Medical Appointments marginally enhance interaction between patients: an observational study on children and adolescents with type 1 diabetes. Patient Education & Counseling. 2013;92(3):418-25. 84. Norris SL, Nichols PJ, Caspersen CJ, Glasgow RE, Engelgau MM, Jack L, et al. Increasing diabetes self-management education in community settings. A systematic review. American Journal of Preventive Medicine. 2002;22(4 Suppl):39-66. 85. O'Hara MC, Hynes L, O'Donnell M, Nery N, Byrne M, Heller SR, et al. A systematic review of interventions to improve outcomes for young adults with Type 1 diabetes. Diabetic Medicine. 2016;20:20. 86. Pals RA, Olesen K, Willaing I. What does theory-driven evaluation add to the analysis of self-reported outcomes of diabetes education? A comparative realist evaluation of a participatory patient education approach. Patient Education and Counseling. 2016;99(6):995-1001. 87. Paterson B, Thorne S. Developmental evolution of expertise in diabetes self-management. Clinical Nursing Research. 2000;9(4):402-19. 88. Piana N, Maldonato A, Bloise D, Carboni L, Careddu G, Fraticelli E, et al. The narrative-autobiographical approach in the group education of adolescents with diabetes: a qualitative research on its effects. Patient Education & Counseling. 2010;80(1):56-63. 89. Pillay J, Armstrong MJ, Butalia S, Donovan LE, Sigal RJ, Chordiya P, et al. Behavioral Programs for Type 1 Diabetes Mellitus: A Systematic Review and Meta-analysis. Annals of Internal Medicine. 2015;163(11):836-47. 90. Plante WA, Lobato DJ. Psychosocial group interventions for children and adolescents with type 1 diabetes: the state of the literature. Children's Health Care. 2008;37(2):93-111. 91. Povlsen L, Ringsberg KC. Learning to live with type 1 diabetes from the perspective of young non-western immigrants in Denmark. Journal of Clinical Nursing. 2008;17(11c):300-9. 92. Powell PW, Corathers SD, Raymond J, Streisand R. New approaches to providing individualized diabetes care in the 21st century. Current Diabetes Reviews. 2015;11(4):222-30. 93. Price K, Knowles J, Fox M, Wales J, Heller S, Eiser C, et al. Effectiveness of the Kids in Control of Food (KICk-OFF) structured education course for 11-16 year olds with Type 1 diabetes. Diabetic medicine : a journal of the British Diabetic Association [Internet]. 2016; 33(2):[192-203 pp.]. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/592/CN-01133592/frame.html
http://onlinelibrary.wiley.com/store/10.1111/dme.12881/asset/dme12881.pdf?v=1&t=izef2wm4&s=423664531d3ba0a3ff801d987785715125e25cd1. 94. Pyatak EA, Sequeira PA, Vigen CL, Weigensberg MJ, Wood JR, Montoya L, et al. Clinical and Psychosocial Outcomes of a Structured Transition Program Among Young Adults With Type 1 Diabetes. Journal of Adolescent Health. 2017;60(2):212-8.
Page 134 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
106
95. Ramdas K, Darzi A. Adopting Innovations in Care Delivery — The Case of Shared Medical Appointments. New England Journal of Medicine. 2017;376(12):1105-7. 96. Rankin D, Heller S, Lawton J. Understanding information and education gaps among people with type 1 diabetes: a qualitative investigation. Patient Education & Counseling. 2011;83(1):87-91. 97. Rankin D, Barnard K, Elliott J, Cooke D, Heller S, Gianfrancesco C, et al. Type 1 diabetes patients' experiences of, and need for, social support after attending a structured education programme: a qualitative longitudinal investigation. Journal of Clinical Nursing. 2014;23(19-20):2919-27. 98. Rankin D, Cooke DD, Elliott J, Heller SR, Lawton J, Group UNDS. Supporting self-management after attending a structured education programme: a qualitative longitudinal investigation of type 1 diabetes patients' experiences and views. BMC Public Health. 2012;12:652. 99. Raymond JK, Shea JJ, Berget C, Cain C, Fay-Itzkowitz E, Gilmer L, et al. A novel approach to adolescents with type 1 diabetes: The team clinic model. Diabetes Spectrum. 2015;28(1):68-71. 100. Reitz JA, Sarfaty M, Diamond JJ, Salzman B. The effects of a group visit program on outcomes of diabetes care in an urban family practice. Journal of Urban Health. 2012;89(4):709-16. 101. Rijswijk C, Zantinge E, Seesing F, Raats I, van Dulmen S. Shared and individual medical appointments for children and adolescents with type 1 diabetes; differences in topics discussed? Patient Education & Counseling. 2010;79(3):351-5. 102. Ritholz MD, Beverly EA, Weinger K. Digging deeper: The role of qualitative research in behavioral diabetes. Current Diabetes Reports. 2011;11(6):494-502. 103. Robinson E. Being diagnosed with type 1 diabetes during adolescence. How do young people develop a healthy understanding of diabetes? Practical Diabetes. 2015;32(9):339-44a. 104. Rostami S, Parsa-Yekta Z, Najafi Ghezeljeh T, Vanaki Z. Supporting adolescents with type 1 diabetes mellitus: a qualitative study. Nursing & Health Sciences. 2014;16(1):84-90. 105. Sadur CN, Moline N, Costa M, Michalik D, Mendlowitz D, Roller S, et al. Diabetes management in a health maintenance organization. Efficacy of care management using cluster visits. Diabetes Care. 1999;22(12):2011-7. 106. Sattoe JNT, Bal MI, Roelofs P, Bal R, Miedema HS, van Staa A. Self-management interventions for young people with chronic conditions: A systematic overview. Patient Education and Counseling. 2015;98(6):704-15. 107. Sawtell M, Jamieson L, Wiggins M, Smith F, Ingold A, Hargreaves K, et al. Implementing a structured education program for children with diabetes: lessons learnt from an integrated process evaluation. BMJ Open Diabetes Research & Care. 2015;3(1):e000065. 108. Schilling LS, Grey M, Knafl KA. The concept of self-management of type 1 diabetes in children and adolescents: an evolutionary concept analysis. Journal of Advanced Nursing. 2002;37(1):87-99. 109. Schillinger D, Hammer H, Wang F, Palacios J, McLean I, Tang A, et al. Seeing in 3-D: examining the reach of diabetes self-management support strategies in a public health care system. Health Education & Behavior. 2008;35(5):664-82. 110. Schmidt S, Herrmann-Garitz C, Bomba F, Thyen U. A multicenter prospective quasi-experimental study on the impact of a transition-oriented generic patient education program on health service participation and quality of life in adolescents and young adults. Patient Education & Counseling. 2016;99(3):421-8. 111. Schultz AT, Smaldone A. Components of Interventions That Improve Transitions to Adult Care for Adolescents With Type 1 Diabetes. Journal of Adolescent Health. 2017;60(2):133-46. 112. Sequeira PA, Pyatak EA, Weigensberg MJ, Vigen CP, Wood JR, Ruelas V, et al. Let's Empower and Prepare (LEAP): Evaluation of a Structured Transition Program for Young Adults With Type 1 Diabetes. Diabetes Care. 2015;38(8):1412-9. 113. Serlachius A, Northam E, Frydenberg E, Cameron F. Adapting a generic coping skills programme for adolescents with type 1 diabetes: a qualitative study. Journal of Health Psychology. 2012;17(3):313-23.
Page 135 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
107
114. Skinner TC, John M, Hampson SE. Social support and personal models of diabetes as predictors of self-care and well-being: a longitudinal study of adolescents with diabetes. Journal of Pediatric Psychology. 2000;25(4):257-67. 115. Smaldone A, Ganda OP, McMurrich S, Hannagan K, Lin S, Caballero AE, et al. Should group education classes be separated by type of diabetes? Diabetes Care. 2006;29(7):1656-8. 116. Soni A, Ng SM. Intensive diabetes management and goal setting are key aspects of improving metabolic control in children and young people with type 1 diabetes mellitus. World Journal of Diabetes. 2014;5(6):877-81. 117. Spencer J, Cooper H, Milton B. Type 1 diabetes in young people: The impact of social environments on self-management issues from young people's and parents' perspectives. Journal of Diabetes Nursing. 2014;18(1):22-31. 118. Spencer JE, Cooper HC, Milton B. The lived experiences of young people (13-16 years) with Type 1 diabetes mellitus and their parents--a qualitative phenomenological study. Diabetic Medicine. 2013;30(1):e17-24. 119. Thorpe CT, Fahey LE, Johnson H, Deshpande M, Thorpe JM, Fisher EB. Facilitating healthy coping in patients with diabetes: a systematic review. Diabetes Educator. 2013;39(1):33-52. 120. Tierney S, Deaton C, Webb K, Jones A, Dodd M, McKenna D, et al. Isolation, motivation and balance: Living with type 1 or cystic fibrosis-related diabetes. Journal of Clinical Nursing. 2008;17(7b):235-43. 121. Vachon GC, Ezike N, Brown-Walker M, Chhay V, Pikelny I, Pendergraft TB. Improving access to diabetes care in an inner-city, community-based outpatient health center with a monthly open-access, multistation group visit program. Journal of the National Medical Association. 2007;99(12):1327-36. 122. Viklund G, Wikblad K. Teenagers' perceptions of factors affecting decision-making competence in the management of type 1 diabetes. Journal of Clinical Nursing. 2009;18(23):3262-70. 123. Viklund G, Ortqvist E, Wikblad K. Assessment of an empowerment education programme. A randomized study in teenagers with diabetes. Diabetic Medicine. 2007a;24(5):550-6. 124. Viklund GE, Rudberg S, Wikblad KF. Teenagers with diabetes: self-management education and training on a big schooner. International Journal of Nursing Practice. 2007b;13(6):385-92. 125. Vissenberg C, Stronks K, Nijpels G, Uitewaal P, Middelkoop B, Kohinor M, et al. Impact of a social network-based intervention promoting diabetes self-management in socioeconomically deprived patients: a qualitative evaluation of the intervention strategies. BMJ open. 2016;6(4):e010254. 126. Waller H, Eiser C, Heller S, Knowles J, Price K. Adolescents' and their parents' views on the acceptability and design of a new diabetes education programme: a focus group analysis. Child: Care, Health & Development. 2005;31(3):283-9. 127. Weinger K. Group medical appointments in diabetes care: is there a future? Diabetes Spectrum. 2003;16(2):104-7. 128. Wiley J, Westbrook M, Long J, Greenfield JR, Day RO, Braithwaite J. Diabetes education: the experiences of young adults with type 1 diabetes. Diabetes Therapy Research, Treatment and Education of Diabetes and Related Disorders. 2014;5(1):299-321. 129. Williams B, Pace AE. Problem based learning in chronic disease management: A review of the research. Patient Education and Counseling. 2009;77(1):14-9. 130. Wong ST, Browne A, Lavoie J, Macleod MLP, Chongo M, Ulrich C. Incorporating group medical visits into primary healthcare: Are there benefits? Healthcare Policy. 2015;11(2):27-42. 131. Yeoh E, Choudhary P, Nwokolo M, Ayis S, Amiel SA. Interventions That Restore Awareness of Hypoglycemia in Adults With Type 1 Diabetes: A Systematic Review and Meta-analysis. Diabetes Care. 2015;38(8):1592-609.
Page 136 of 136
CONFIDENTIAL-For Peer Review Only
Diabetes Care
Related Documents











