4/19/2018 1 ©2016 MFMER | slide-1 Progressive Speech and Language Disorders Rene L. Utianski, PhD, CCC-SLP [email protected] ©2016 MFMER | slide-2 Outline • Part One: Background • Primary Progressive Aphasias (PPA) • Semantic Variant of PPA • Logopenic Variant • Agrammatic/ non-fluent variant of PPA • Primary Progressive Apraxia of Speech (PPAOS) • Part Two: Differential Diagnosis/ Case Studies • Part Three: Treatment ©2016 MFMER | slide-3 Part One Primary Progressive Aphasias and Primary Progressive Apraxia of Speech ©2016 MFMER | slide-4 Three General Components of Speaking 1 • Cognitive linguistic processing 2 • Sensorimotor planning/programming 3 • Neuromuscular execution

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
4/19/2018
1
©2016 MFMER | slide-1
Progressive Speech and Language DisordersRene L. Utianski, PhD, [email protected]
©2016 MFMER | slide-2
Outline • Part One: Background
• Primary Progressive Aphasias (PPA) • Semantic Variant of PPA• Logopenic Variant• Agrammatic/ non-fluent variant of PPA
• Primary Progressive Apraxia of Speech (PPAOS)
• Part Two: Differential Diagnosis/ Case Studies• Part Three: Treatment
©2016 MFMER | slide-3
Part OnePrimary Progressive Aphasias and Primary
Progressive Apraxia of Speech
©2016 MFMER | slide-4
Three General Components of Speaking
1• Cognitive linguistic processing
2• Sensorimotor
planning/programming
3• Neuromuscular execution
4/19/2018
2
©2016 MFMER | slide-5
What if something goes wrong?• Brain lesion
• Cerebrovascular Accident or Stroke (CVA)• Ischemic due to thrombosis or embolism• Hemorrhagic due to aneurysm or AVM
• Trauma (TBI)• Tumor• Infection
©2016 MFMER | slide-6
Three General Components of Speaking: What if something goes wrong?
1• Cognitive linguistic processing
• Aphasia
2• Sensorimotor planning/programming
• Apraxia of speech
3• Neuromuscular execution
• Dysarthria
©2016 MFMER | slide-7
What if something goes wrong?• Brain lesion
• Cerebrovascular Accident or Stroke (CVA)• Occlusive (ischemic) due to thrombosis or
embolism• Hemorrhagic due to aneurysm or AVM
• Trauma (TBI)• Neoplasm (tumor)• Infection/Toxin• Disease Process
©2016 MFMER | slide-8
Three General Components of Speaking:What if something goes wrong?
1• Cognitive linguistic processing
• Dementia• Progressive aphasia
2• Sensorimotor planning/programming
• Progressive apraxia of speech
3• Neuromuscular execution
• Dysarthria

4/19/2018
3
©2016 MFMER | slide-9
Primary Progressive Aphasia (PPA)
©2016 MFMER | slide-10
Primary Progressive Aphasia (PPA)• A rare degenerative, neurological syndrome. • Insidious onset. • Progressive. • Primary and initial complaint of language
difficulties.
©2016 MFMER | slide-11
Gorno-Tempini et al. Diagnosis Criteria (2011)
• Pattern of deficits are not accounted for by other nondegenerative nervous system, medical, or disorder at onset.
• Absence of episodic memory, visual memory, and visuo-perceptual impairments at onset.
• Absence of behavioral disturbance at onset.
©2016 MFMER | slide-12
Variants of PPA• Semantic variant• Logopenic• Agrammatic/ Non-fluent variant
4/19/2018
4
©2016 MFMER | slide-13
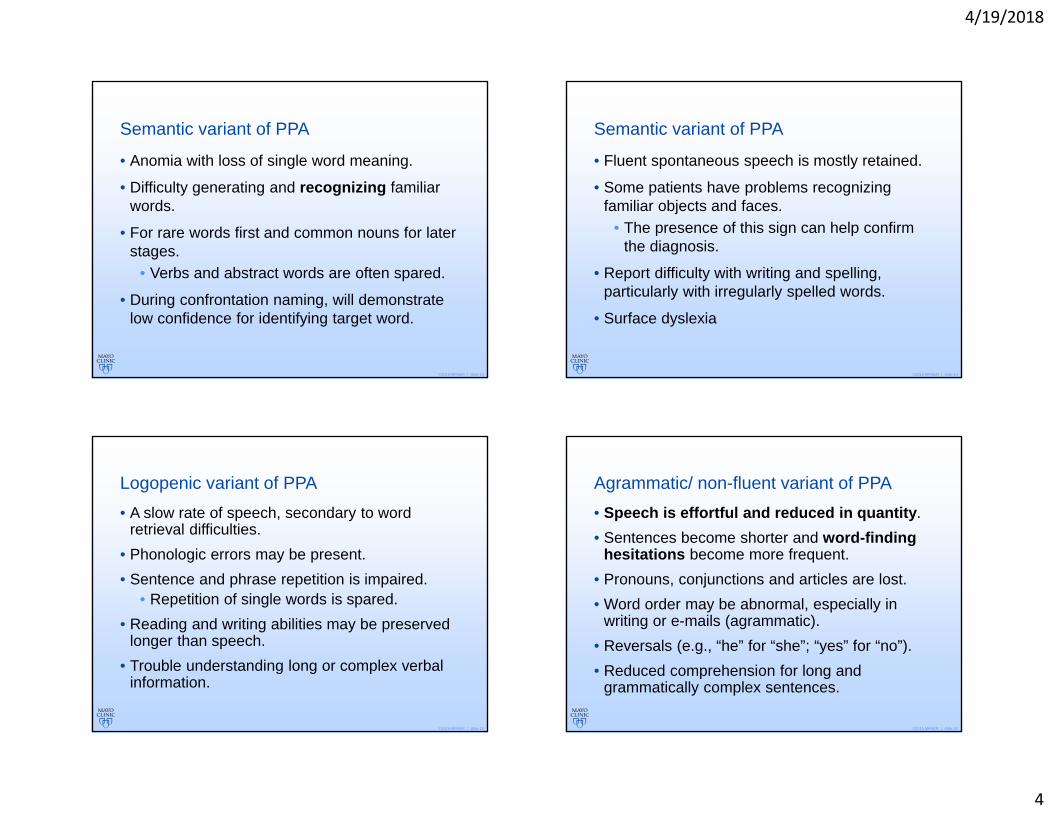
Semantic variant of PPA
• Anomia with loss of single word meaning.
• Difficulty generating and recognizing familiar words.
• For rare words first and common nouns for later stages.
• Verbs and abstract words are often spared.
• During confrontation naming, will demonstrate low confidence for identifying target word.
©2016 MFMER | slide-14
Semantic variant of PPA
• Fluent spontaneous speech is mostly retained.
• Some patients have problems recognizing familiar objects and faces.
• The presence of this sign can help confirm the diagnosis.
• Report difficulty with writing and spelling, particularly with irregularly spelled words.
• Surface dyslexia
©2016 MFMER | slide-15
Logopenic variant of PPA• A slow rate of speech, secondary to word
retrieval difficulties.• Phonologic errors may be present.• Sentence and phrase repetition is impaired.
• Repetition of single words is spared.• Reading and writing abilities may be preserved
longer than speech.• Trouble understanding long or complex verbal
information.
©2016 MFMER | slide-16
Agrammatic/ non-fluent variant of PPA• Speech is effortful and reduced in quantity.• Sentences become shorter and word-finding
hesitations become more frequent. • Pronouns, conjunctions and articles are lost. • Word order may be abnormal, especially in
writing or e-mails (agrammatic). • Reversals (e.g., “he” for “she”; “yes” for “no”). • Reduced comprehension for long and
grammatically complex sentences.
4/19/2018
5
©2016 MFMER | slide-17
PPA implies a disorder of language impairment.Aphasia may not even be present!
©2016 MFMER | slide-18
Primary Progressive Apraxia of Speech
©2016 MFMER | slide-19 ©2016 MFMER | slide-20
PPAOS
Insidious
Progressive
Motor planning difficulty
4/19/2018
6
©2016 MFMER | slide-21
PPAOS Diagnostic Criteria• Initial complaint of speech difficulty.• Unequivocal AOS.• No evidence of aphasia.• Normal neurological examination.• Normal neuropsychological testing.
©2016 MFMER | slide-22
Patient Perceptions and Complaints• “Pure” AOS:
• “my speech won’t come out right”• “know what I want to say but doesn’t come out right”• not as fluent as before• mispronounce words• with mild or moderate AOS, patients report being
surprised by errors that “sneak into” narratives • complaints usually center around articulation problems• some patients report having to speak slowly or more
carefully to prevent errors• predict errors on multi-syllabic or difficult to pronounce
words• recognize errors and attempt to correct them• problems may be more obvious when stressed or
fatigued
©2016 MFMER | slide-23
Motor processes of speech
Prosody
Articulation
Resonance
Phonation
Respiration
©2016 MFMER | slide-24
PPAOS Types
PPAOS
Prosodic Phonetic

4/19/2018
7
©2016 MFMER | slide-25
Classification is not dichotomous, but a relative predominance
Phonetic abnormalities
Prosodic abnormalities
©2016 MFMER | slide-26
Clinical Information• Demographics• Severity• Language• Cognition• Neurologic
©2016 MFMER | slide-27
How does the initial presentation influence disease progression?
ProsodicPhonetic
©2016 MFMER | slide-28
Some ideas…

4/19/2018
8
©2016 MFMER | slide-29
Part TwoDifferential Diagnosis
©2016 MFMER | slide-30
THE MAIN FOCUS: Differential diagnosis
Progressive
Apraxia of
Speech
Aphasia
©2016 MFMER | slide-31
Assessment and differential diagnosisStep 1: Is aphasia present?
Step 2: Is apraxia of speech present? If so, what dominates?
Step 3: Is dysarthria present?
Largely completed simultaneously!
©2016 MFMER | slide-32
First step• Is aphasia present?
4/19/2018
9
©2016 MFMER | slide-33
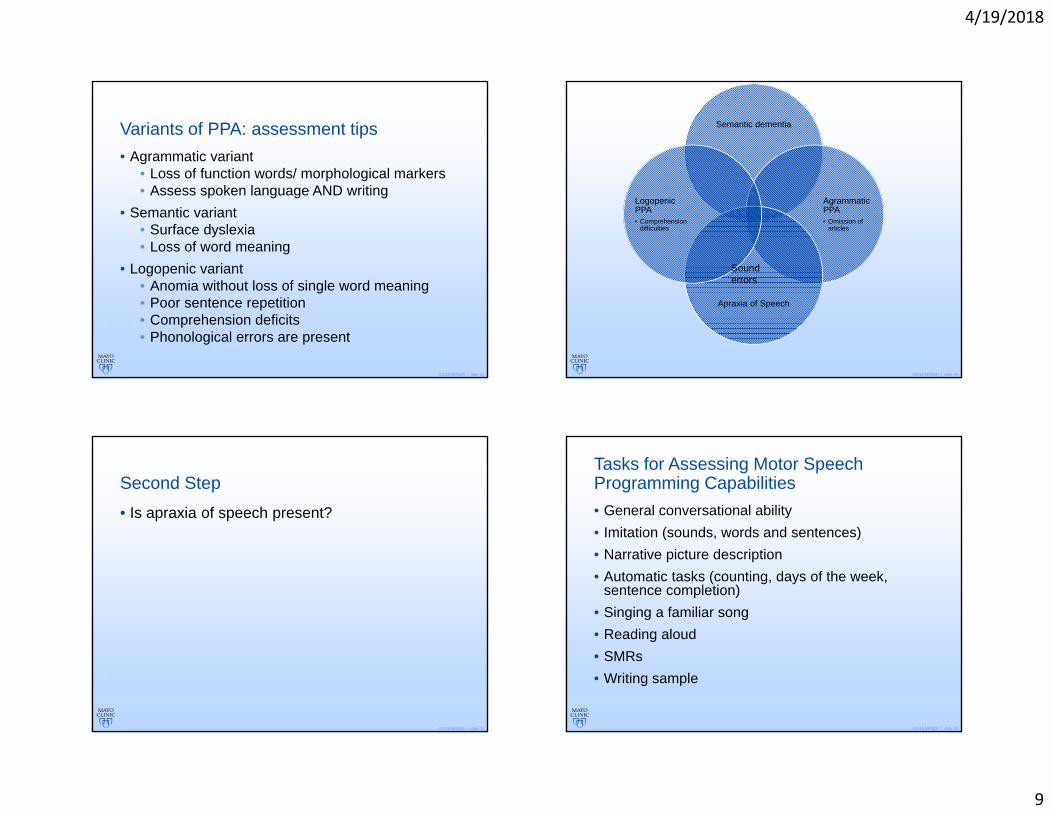
Variants of PPA: assessment tips• Agrammatic variant
• Loss of function words/ morphological markers• Assess spoken language AND writing
• Semantic variant• Surface dyslexia• Loss of word meaning
• Logopenic variant• Anomia without loss of single word meaning • Poor sentence repetition• Comprehension deficits• Phonological errors are present
©2016 MFMER | slide-34
Semantic dementia
Agrammatic PPA• Omission of
articles
Apraxia of Speech
LogopenicPPA• Comprehension
difficulties
Sound errors
©2016 MFMER | slide-35
Second Step• Is apraxia of speech present?
©2016 MFMER | slide-36
Tasks for Assessing Motor Speech Programming Capabilities• General conversational ability• Imitation (sounds, words and sentences)• Narrative picture description• Automatic tasks (counting, days of the week,
sentence completion)• Singing a familiar song• Reading aloud• SMRs• Writing sample
4/19/2018
10
©2016 MFMER | slide-37
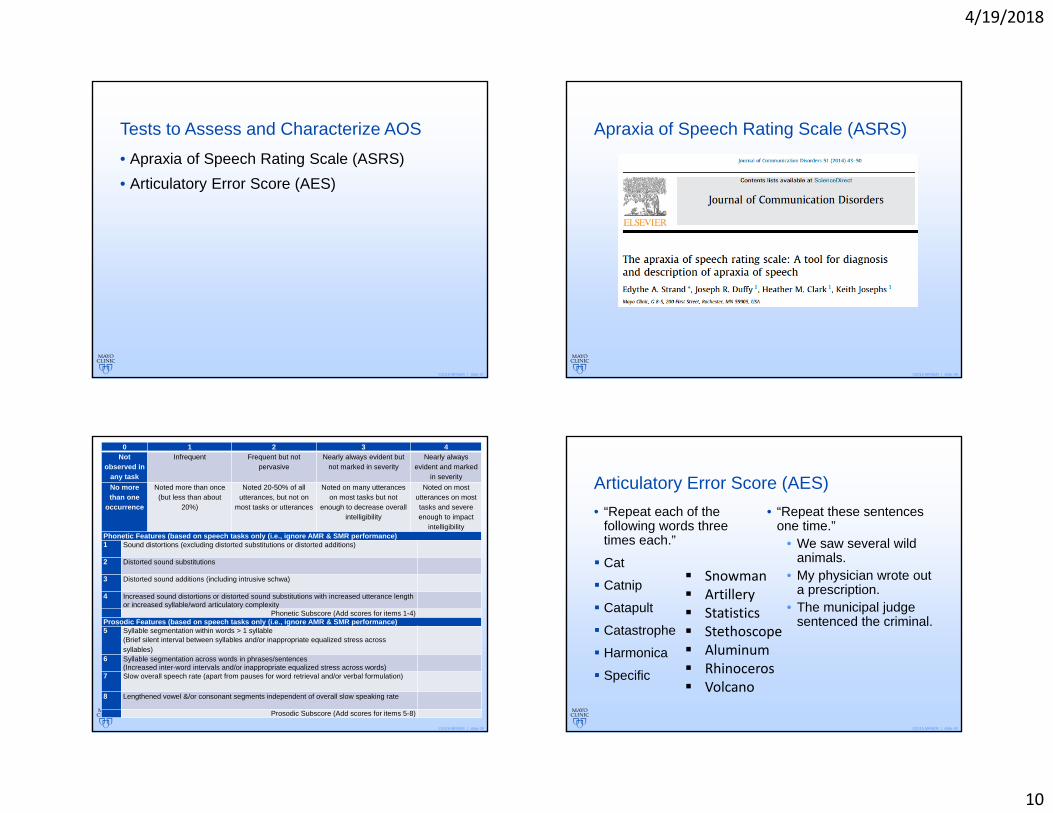
Tests to Assess and Characterize AOS• Apraxia of Speech Rating Scale (ASRS)• Articulatory Error Score (AES)
©2016 MFMER | slide-38
Apraxia of Speech Rating Scale (ASRS)
©2016 MFMER | slide-39
0 1 2 3 4Not
observed in any task
Infrequent Frequent but not pervasive
Nearly always evident but not marked in severity
Nearly always evident and marked
in severityNo more than one
occurrence
Noted more than once (but less than about
20%)
Noted 20-50% of all utterances, but not on
most tasks or utterances
Noted on many utterances on most tasks but not
enough to decrease overall intelligibility
Noted on most utterances on most tasks and severe enough to impact
intelligibilityPhonetic Features (based on speech tasks only (i.e., ignore AMR & SMR performance)1 Sound distortions (excluding distorted substitutions or distorted additions)
2 Distorted sound substitutions
3 Distorted sound additions (including intrusive schwa)
4 Increased sound distortions or distorted sound substitutions with increased utterance length or increased syllable/word articulatory complexity
Phonetic Subscore (Add scores for items 1-4)Prosodic Features (based on speech tasks only (i.e., ignore AMR & SMR performance)5 Syllable segmentation within words > 1 syllable
(Brief silent interval between syllables and/or inappropriate equalized stress across syllables)
6 Syllable segmentation across words in phrases/sentences(Increased inter-word intervals and/or inappropriate equalized stress across words)
7 Slow overall speech rate (apart from pauses for word retrieval and/or verbal formulation)
8 Lengthened vowel &/or consonant segments independent of overall slow speaking rate
Prosodic Subscore (Add scores for items 5-8)
©2016 MFMER | slide-40
Articulatory Error Score (AES)• “Repeat each of the
following words three times each.”
Cat
Catnip
Catapult
Catastrophe
Harmonica
Specific
• “Repeat these sentences one time.”
• We saw several wild animals.
• My physician wrote out a prescription.
• The municipal judge sentenced the criminal.
Snowman Artillery Statistics Stethoscope Aluminum Rhinoceros Volcano

4/19/2018
11
©2016 MFMER | slide-41 ©2016 MFMER | slide-42
Third step• Is dysarthria present?
©2016 MFMER | slide-43
Differential diagnosis: Dysarthria• Oral mechanism examination• AMRs• SMRs• Groping?• Distortions v. substitutions v. distorted
substitutions
©2016 MFMER | slide-44
Other tips for diagnosis• History is critical!
• Insidious onset• Progression over time
• Asking the right questions is crucial

4/19/2018
12
©2016 MFMER | slide-45
Case History Question Suggestions• Any difficulties with speech or language as a
child?• How would you describe the difficulties you
have been having?• How long have the difficulties been occurring? • Was the onset sudden? Or gradual?• Any worse over time?
©2016 MFMER | slide-46
Case History: Speech• Speech better at any time of the day?• Things that make it worse?• Does alcohol have any effect?• Any point at which it completely returns to
normal?• Any situation in which people have a difficult
time understanding you? • Difficulty producing words, despite knowing
what you want to say?• Difficulty with longer/ harder words?
©2016 MFMER | slide-47
Case History: Language• Difficulty understanding?• Difficulty thinking of words?• Mean to say one words and another word
comes out? i.e. dog for cat or cone for comb?• Hear a word and not know what it means?• Difficulty with yes/ no?• Difficulty with left/ right?• Ever leave words out in speaking or writing?
©2016 MFMER | slide-48
Case History: Other• Any changes in handwriting?• Any changes in behavior or personality? • Laughing or crying more easily? At
inappropriate times?• Any difficulty chewing or swallowing liquids or
solids?
4/19/2018
13
©2016 MFMER | slide-49
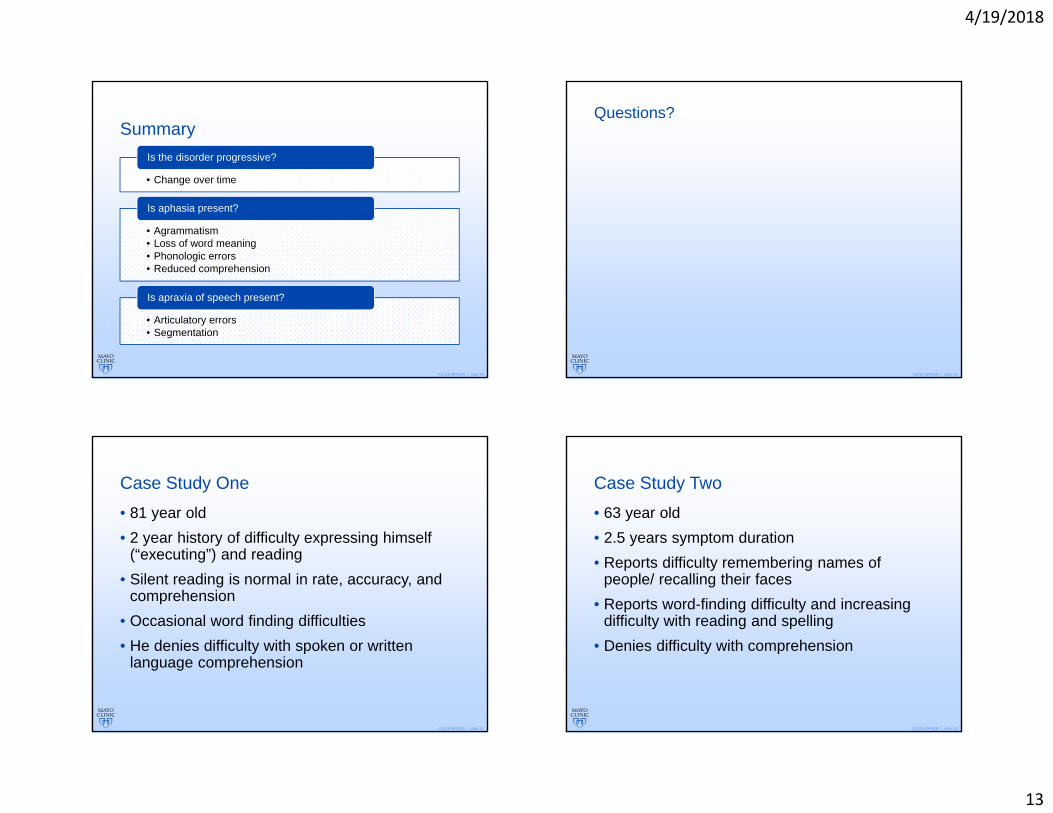
Summary
• Change over time
Is the disorder progressive?
• Agrammatism• Loss of word meaning• Phonologic errors• Reduced comprehension
Is aphasia present?
• Articulatory errors• Segmentation
Is apraxia of speech present?
©2016 MFMER | slide-50
Questions?
©2016 MFMER | slide-51
Case Study One• 81 year old• 2 year history of difficulty expressing himself
(“executing”) and reading• Silent reading is normal in rate, accuracy, and
comprehension• Occasional word finding difficulties • He denies difficulty with spoken or written
language comprehension
©2016 MFMER | slide-52
Case Study Two• 63 year old• 2.5 years symptom duration• Reports difficulty remembering names of
people/ recalling their faces• Reports word-finding difficulty and increasing
difficulty with reading and spelling• Denies difficulty with comprehension
4/19/2018
14
©2016 MFMER | slide-53
Case Study Three• 62 year old• 2.5 year history of speech difficulty (noticeable
to others only in the last 6 months)• Longstanding lisp• Denies difficulty with word retrieval• Reports changes in handwriting (more
laborious; larger print)
©2016 MFMER | slide-54
Case Study Four• 69 year old• 1.5 year history of “missing words,” confusing
tenses, word order, and pronouns• Denies difficulty with comprehension
©2016 MFMER | slide-55
Part ThreeTreatment
Using a Theoretical Framework to Guide the Clinical Management of Intelligibility Disorders
©2016 MFMER | slide-56
What is an intelligibility disorder?
4/19/2018
15
©2016 MFMER | slide-57
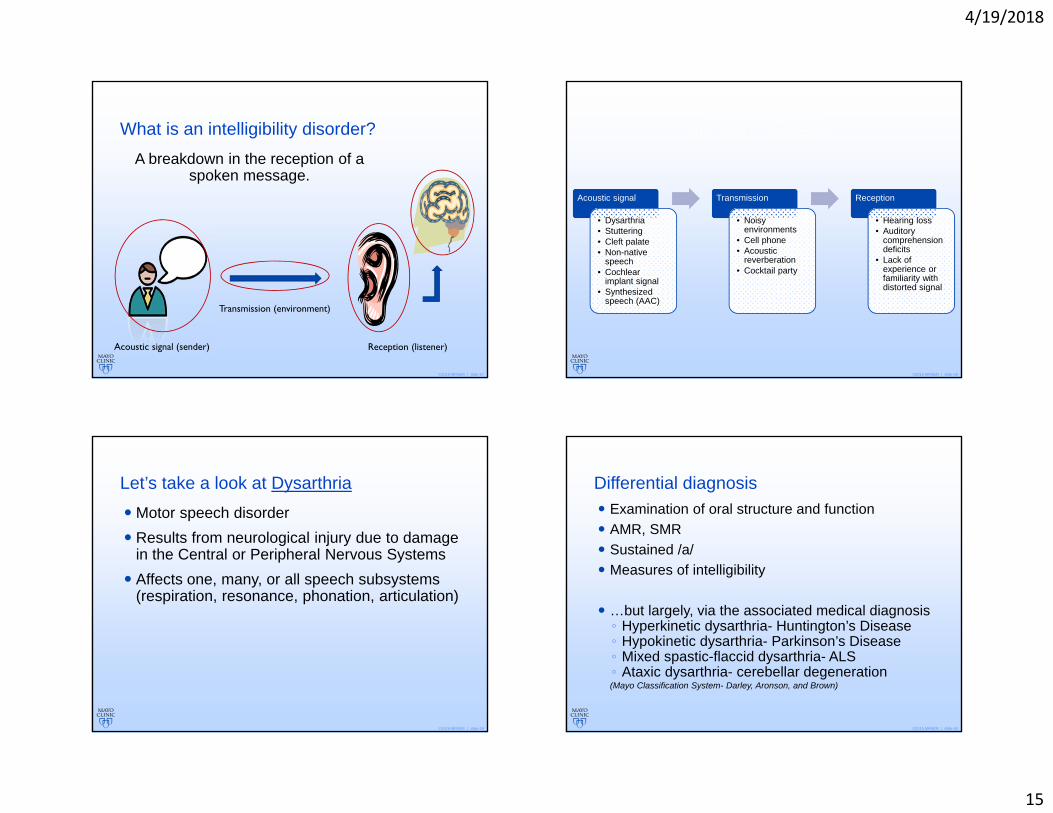
What is an intelligibility disorder?A breakdown in the reception of a
spoken message.
Acoustic signal (sender)
Transmission (environment)
Reception (listener)
©2016 MFMER | slide-58
POSSIBLE SOURCES OF INTELLIGIBILITY BREAKDOWNS
Acoustic signal
• Dysarthria• Stuttering• Cleft palate• Non-native
speech• Cochlear
implant signal• Synthesized
speech (AAC)
Transmission
• Noisy environments
• Cell phone• Acoustic
reverberation• Cocktail party
Reception
• Hearing loss• Auditory
comprehension deficits
• Lack of experience or familiarity with distorted signal
©2016 MFMER | slide-59
Let’s take a look at Dysarthria Motor speech disorder Results from neurological injury due to damage
in the Central or Peripheral Nervous Systems Affects one, many, or all speech subsystems
(respiration, resonance, phonation, articulation)
©2016 MFMER | slide-60
Differential diagnosis Examination of oral structure and function AMR, SMR Sustained /a/ Measures of intelligibility
…but largely, via the associated medical diagnosis◦ Hyperkinetic dysarthria- Huntington’s Disease◦ Hypokinetic dysarthria- Parkinson’s Disease◦ Mixed spastic-flaccid dysarthria- ALS◦ Ataxic dysarthria- cerebellar degeneration(Mayo Classification System- Darley, Aronson, and Brown)

4/19/2018
16
©2016 MFMER | slide-61
Mayo clinic classification approach
Hyperkinetic
Hypokinetic
Ataxic
Mixed
Flaccid
Spastic HarshnessStrained-strangled
Articulatory imprecisionHypernasalHyponasalMonotoneMonopitch
©2016 MFMER | slide-62
But does it matter?• Does the “dysarthria subtype” dictate your
clinical decision making?
• Probably not.
©2016 MFMER | slide-63
Mayo Clinic approach1) there is considerable overlap in speech symptoms among the classification categories, and
2) speech symptoms within a given classification may differ along the severity dimension.
This classification approach does not map well to the resulting communication disorders or to intervention targets. It does help diagnose neurologic disease!
Bottom line: we can’t treat the diagnosis, we need to treat the resulting intelligibility disorder!
©2016 MFMER | slide-64
What do I mean by that?• We identify what is wrong and we try and fix it!
• Theory will tell us what will have the largest impact on the listener.
4/19/2018
17
©2016 MFMER | slide-65
Speech Perception Theory
A theory is a set of interrelated principles and definitions that present a systematic view of phenomena by specifying relationships among variables with the purpose of explainingnatural phenomena.
©2016 MFMER | slide-66
“Intelligibility is as much in the ear of the listener as it is in the mouth
of the speaker.” (Martin & Weismer, 1992)
©2016 MFMER | slide-67
Theoretical perspective Dysarthria interferes with perceptual processes:◦ Activation of an optimal lexical candidate pool◦ Competition among lexical candidates◦ Application of strategies to lexically segment
the connected speech
©2016 MFMER | slide-68
How does it do that? To understand this interference, let’s take a look
at “normal” speech perception
Namely: How do listeners understand single words? and
connected speech? How does dysarthria interfere with these
processes?
4/19/2018
18
©2016 MFMER | slide-69
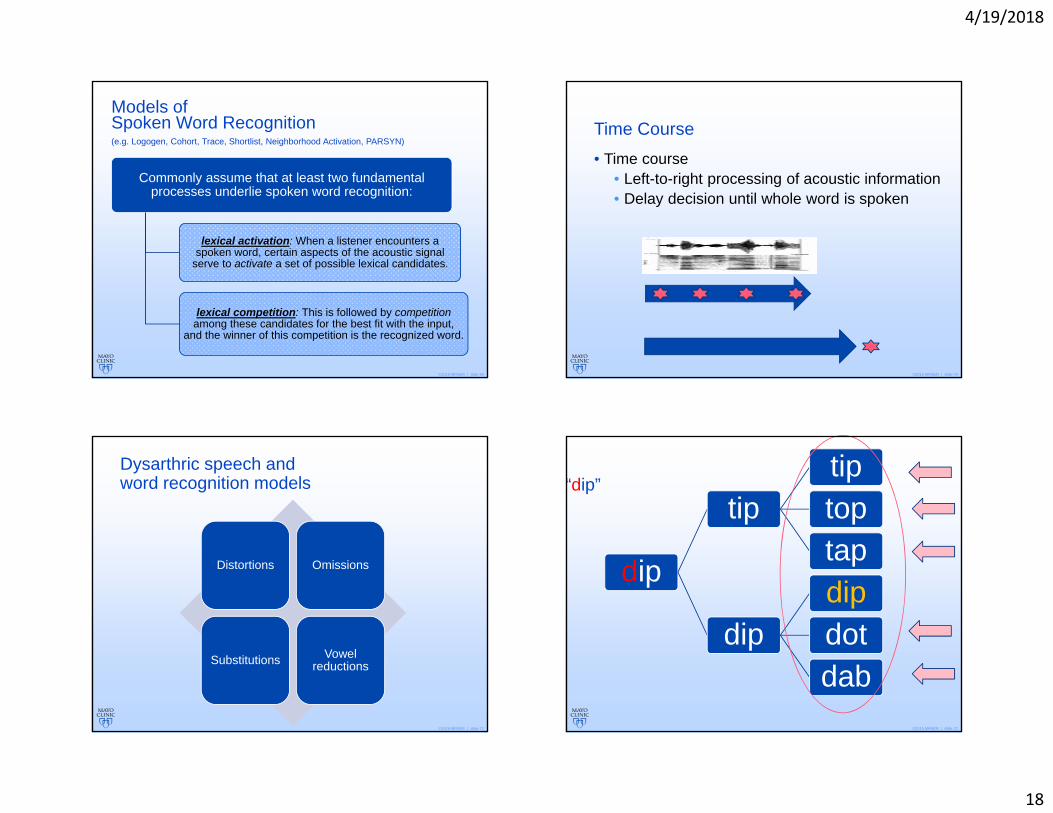
Models of Spoken Word Recognition(e.g. Logogen, Cohort, Trace, Shortlist, Neighborhood Activation, PARSYN)
Commonly assume that at least two fundamental processes underlie spoken word recognition:
lexical activation: When a listener encounters a spoken word, certain aspects of the acoustic signal
serve to activate a set of possible lexical candidates.
lexical competition: This is followed by competitionamong these candidates for the best fit with the input,
and the winner of this competition is the recognized word.
©2016 MFMER | slide-70
Time Course• Time course
• Left-to-right processing of acoustic information• Delay decision until whole word is spoken
©2016 MFMER | slide-71
Dysarthric speech and word recognition models
Distortions Omissions
Substitutions Vowel reductions
©2016 MFMER | slide-72
dip
tiptiptoptap
dipdipdotdab
“dip”
4/19/2018
19
©2016 MFMER | slide-73
“_ip”
_ipit
inill
if is
©2016 MFMER | slide-74
Single word
intelligibility
Acoustic information Word
frequency effects
©2016 MFMER | slide-75
There is very little predictive value in single word intelligibilityPerceiving connected speech is a very different beast!
©2016 MFMER | slide-76
Connected speech
intelligibility
Acoustic signal quality
Syntactic probabilities
Semantic priming
Listener expectations
about the message

4/19/2018
20
©2016 MFMER | slide-77
Deciphering Connected Speech Lexical activation and lexical competition are
strongly influenced by the message Semantics, syntactics, knowledge of topic
and speaker: prime the lexical candidates and facilitate efficient competition
The quality of the acoustic signal is not critical as listeners listen for words, not phonemes◦ Phonemic restoration
Listeners perform “lexical segmentation”
©2016 MFMER | slide-78
Lexical Segmentation• A fundamental process in deciphering degraded
speech that determines “word size frames” for lexical access.
Every thing I say is easy to under stand.
©2016 MFMER | slide-79
Metrical Segmentation Strategy (Cutler & Norris, 1987)
When listeners encounter degraded speech
They listen for STRONG (stressed) syllables
Treat them as WORD ONSETS
And they’ll most often be right in English
©2016 MFMER | slide-80
Lexical Segmentation • Semantically anomalous, syntactically correct
4/19/2018
21
©2016 MFMER | slide-81
Cues to syllable strength
Fundamental frequency variation
Syllable/vowel duration
Strong versus reduced vowels
Loudness variation
©2016 MFMER | slide-82
If you don’t “chop up” the acoustic stream into words correctly…
You have no chance at using all available acoustic and top-down information to make a best match for the words.
©2016 MFMER | slide-83
Regardless of “dysarthria type,” different types of degradation patterns
(e.g. slow rate, reduced pitch and loudness variation, consonant
imprecision), yield different perceptual errors.
THIS is the intelligibility disorder!
©2016 MFMER | slide-84
Listeners are flexible• Use available acoustic cues, even when they’re degraded;
• Can switch the amount of reliance on various cues, depending on which are most robust and systematic;
• They use their “higher level” knowledge to facilitate and guide speech understanding
• Semantics, syntax, phonotactics, knowledge of topic/ speaker
Context
Acoustic
4/19/2018
22
©2016 MFMER | slide-85
“Signal-Complementary Information” Lindblom, 1990
• Speech Signal transmitted
Listener manipulation
• Listener applies information
Augmented perceptual processing • Improved
performance
Increased intelligibility
©2016 MFMER | slide-86
Activating optimal lexical candidates• Alphabet cueing
• e.g. Hustad, Jones, & Dailey, 2003; Hustad, 2005
• Providing topic cues• e.g. Hustad, Auker, Natale, & Carlson, 2003; Jones, Mathy, Azuma, &
Liss, 2004; Utianski, Azuma, and Liss, 2010
• Providing semantic context• e.g. Dongilli, 1994; Hammen, Yorkston, & Dowden, 1991
©2016 MFMER | slide-87
Lexical competition• Providing a syntactic template or structure• Creating semantically and syntactically
predictable utterances• Using supplementary cues such as first-letter,
word-class cues, or gestures
©2016 MFMER | slide-88
Perceptual training• Training material
• Talker-specific• Disorder-specific
• Feedback type and frequency• Passive exposure vs. training• Generalization of minimal exposure/training
• Training regimen and intensity
4/19/2018
23
©2016 MFMER | slide-89
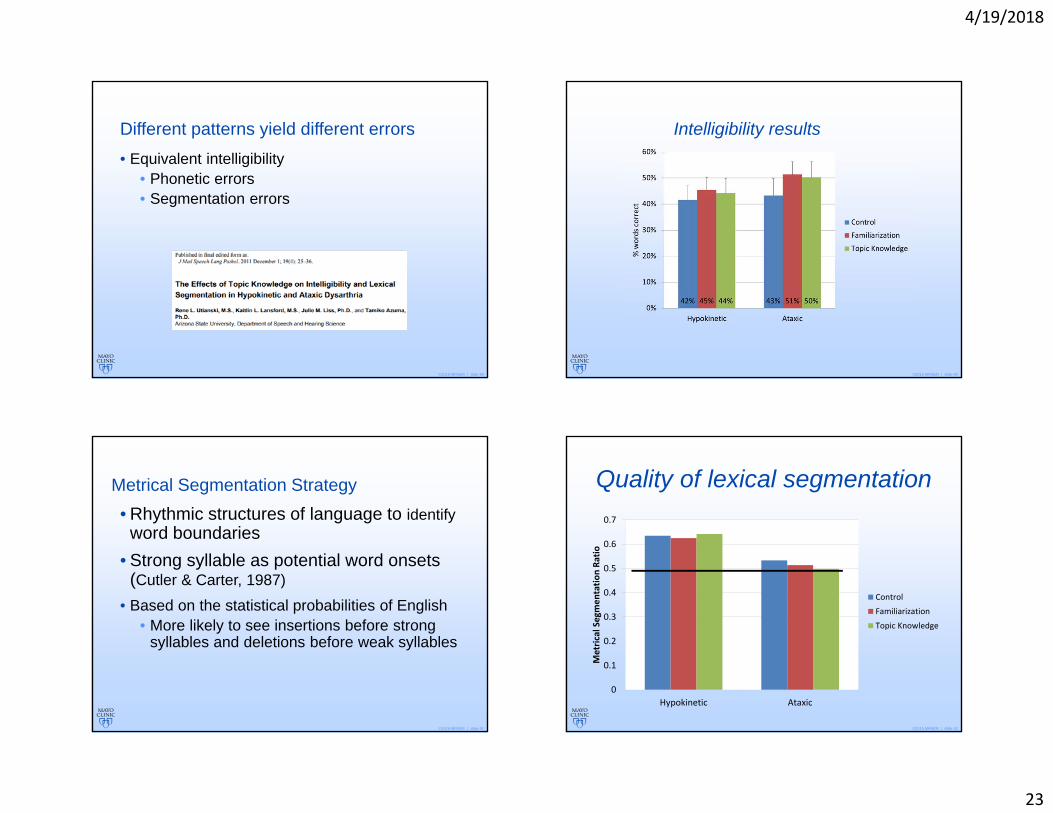
Different patterns yield different errors• Equivalent intelligibility
• Phonetic errors• Segmentation errors
©2016 MFMER | slide-90
Intelligibility results
©2016 MFMER | slide-91
Metrical Segmentation Strategy• Rhythmic structures of language to identify
word boundaries• Strong syllable as potential word onsets
(Cutler & Carter, 1987)• Based on the statistical probabilities of English
• More likely to see insertions before strong syllables and deletions before weak syllables
©2016 MFMER | slide-92
Quality of lexical segmentation
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Hypokinetic Ataxic
Metrical Segmen
tatio
n Ra
tioControl
Familiarization
Topic Knowledge

4/19/2018
24
©2016 MFMER | slide-93
Identifying the potential source of benefit
• Do listeners more correctly transcribe topic words, regardless of a lack of overall intelligibility for hypokinetic speech?
• Does the dysarthria type difference disappear when we look at the listener’s ability to use topic knowledge?
©2016 MFMER | slide-94
Topic words correct
27% 26%29% 34%30% 39%0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Hypokinetic Ataxic
% words correct
Control
Familiarization
Topic Knowledge
©2016 MFMER | slide-95
Take away points
• Topic knowledge and familiarization offer equal perceptual benefits for ataxic speech
• Sources of benefits for each speaker group• Listeners of hypokinetic speech rely on
syllabic stress to segment words• Listeners of ataxic speech utilize lexical
access and acoustic- phonetic remapping to segment words
©2016 MFMER | slide-96
Research-practice divideCurrent pitfalls in the remediation of intelligibility disorders

4/19/2018
25
©2016 MFMER | slide-97
Theoretical andClinical Perspectives
Theoretical Goal: Advance
knowledge about basic
mechanisms and processes
Clinical Goal: Determines how characteristics of
a particular clinical
population relate to
hypotheses generated from a theory or model.
(Bernstein & Weismer, 2000)
©2016 MFMER | slide-98
Clinic Theory
©2016 MFMER | slide-99
Treating Intelligibility Disorders
IntelligibilityIntelligibility
SpeakerSpeaker ListenerListener
©2016 MFMER | slide-100
Speaker-based approaches to remediation• Subsystem Approach
• Respiration• Phonation• Resonance• Articulation
• Global Approaches

4/19/2018
26
©2016 MFMER | slide-101
Respiration• Modify posture, tone, strength• Improve control of exhalation• Use biofeedback or visual feedback• Modify abnormal breathing pattern• Compensation (breath groups)
©2016 MFMER | slide-102
Phonation• Hyperadduction: relax• Hypoadduction: pushing/pulling, maximum
performance tasks• Traditional voice therapy
©2016 MFMER | slide-103
Resonance• Prosthetic device/surgery• Tactile/ kinesthetic feedback• Visual feedback• Contrast drills• CPAP
©2016 MFMER | slide-104
Articulation• Articulation drills• Contrast drills• Oral strengthening • Range-of-motion exercises

4/19/2018
27
©2016 MFMER | slide-105
Modification of speech signal• Reducing speaking rate• Speaking louder
• Is reduced loudness the problem?• Modifying prosody
• Reduced pitch loudness and variation? Monopitch and monoloud?
©2016 MFMER | slide-106
Typical Approaches to Characterizing Intelligibility
• Single-word intelligibility tests• Sentence intelligibility tests• Estimates from reading passages or spontaneous
connected speech
The estimates of single-word intelligibility are generally poor predictors of connected
speech intelligibility, except at very mild and very severe ends of the continuum.
©2016 MFMER | slide-107
Why is this the case? Listeners don’t listen for phonemes in connected
speech. They listen for words or even phrases.
Listeners apply their knowledge of syntax, semantics, and phonotactics, and knowledge of the speaker to problem-solve degraded stretches of speech.
©2016 MFMER | slide-108
Treating Motor speech disorders
IntelligibilityIntelligibility
SpeakerSpeaker ListenerListener

4/19/2018
28
©2016 MFMER | slide-109
How can we use a theoretical framework to guide clinical practice?
©2016 MFMER | slide-110
Face-to-face communication
• Face the listener
• Get the listener's attention before speaking
• Audio-visual enhancement for comprehensibility
©2016 MFMER | slide-111
Transmission:Minimize environmental interference
• Optimize the environment
• Reduce background noise (the dishwasher, too; not just the tv!)
• Avoid communication over a distance
©2016 MFMER | slide-112
Activate optimal lexical pool:Alphabet Supplementation• Use an alphabet supplementation board,
pointing to the first letter of each word as it is spoken.

4/19/2018
29
©2016 MFMER | slide-113
• What if hypernasality is interfering with activation of the target lexical item?
©2016 MFMER | slide-114
Syllable segmentation• Slow speaking rate • Pausing between words but without separating
syllables within words
©2016 MFMER | slide-115
Influence of familiarity• Measures of speech intelligibility are subject to bias.• Are speakers improving, or are you becoming a
better listener?
©2016 MFMER | slide-116
Is PPAOS a special case?

4/19/2018
30
©2016 MFMER | slide-117
Ways to quantify change to overcome bias• Rate• Segmentation• Loudness
• Digital advances
©2016 MFMER | slide-118
Praat
©2016 MFMER | slide-119
Cases? Questions? Comments?
Related Documents











