Program Management Of DR-TB (PMDT) “Diagnose, Treat and Cure All Missing TB Cases” Dr Mohan K Prasai Consultant Chest Physician NTC

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Program Management Of DR-TB (PMDT)
“Diagnose, Treat and Cure All Missing TB Cases”
Dr Mohan K PrasaiConsultant Chest Physician
NTC

Global Burden Of MDR-TB: 2012
Global Estimation 310,000Diagnosed cases 86,000

Types of Drug Resistance
• Mono-resistance : resistance to single first line drug
• Poly-resistance: resistance to more than one drug other than HR together
• Multi- Drug resistance (MDR): resistance to at-least Rifampicin & Isoniazide or RIF Resistance confirmed by GeneXpert.
• Pre-XDR: MDR with resistance to one of injectable or floroquinolone.
• Extensive Drug resistance (XDR): resistance to floroquinolone and injectable second line in addition with MDR TB.
• XXDR: Resistance to almost all ATT.

Types of Resistance (By Treatment history)Initial resistance ( New cases - never have
prior ATT or less than one month)
Acquired resistance (Re-treatment or new case with more than one month of ATT)

Multi Drug resistant Tuberculosis
• MDR TB is an increasing health problem.• A serious challenge to TB control programm.• It is regarded as a result of failure of
effective implementation of Tuberculosis control program.
• Minimize the transmission of DR-TB by Infection control measures.
• GeneXpert is a gold standard diagnosis tool for early and confirmatory diagnosis of MDR-TB.
How is it caused ?
It is the result of inadequate or poorly administered treatment regimen.
Causes of inadequate treatment: 1. Health care providers- inadequate
regimens2. Drugs -inadequate supply or quality3. Patients -inadequate drugs intake

When to Suspect of MDR TB ?Failure of Re-treatment Regimen
Persistent positive sputum
Fall and Rise Phenomenon
Clinical and radiological Deterioration

DR-TB(M/XDR) Management sites
Rx Centres: 13 Rx Sub-centres: 71
50% Treatment Centers and 25% Sub Treatment Centers in private sector

Key Policies of PMDT
• GeneXpert test is gold standard test• Provision of free quality assured second
line drugs• Fully supervised treatment• Prepare the patient for treatment • Clinical monitoring, treatment and
documentation of side effects• Regular sputum microscopy and culture
monitoring• Standardized recording and reporting
system• Monitoring of treatment outcome and
evaluation of program progress through cohort analysis

Candidates for Second line DST(SLDST)
Any patient who has had a past history of previous second line drugs
Any patient who remains culture positive on or after four months of the standard regimen used for MDR TB
Contacts of an individual documented with XDR TB.

Where To Refer ?
Near by GeneXpert centre
National Reference Lab, GENETUP, Kalimati
National Tuberculosis Center, Thimi
Line Probe Assay (LPA)
GeneXpert

Nepal Report In % (MDR-TB)
1999 2002 2007 20110
5
10
15
20
25
30
35
40
45
28.2
40.93
25.3 25.4
11.96
20.46
11.72
15.4
Acquired Any Resistance Acquired MDR
1999 2002 2007 20110
2
4
6
8
10
12
14
16
13.32
10.99
14.71
9.3
3.74
1.32
2.862.2
Initial Any Resistance Initial MDR

Nepal Report In % (XDR-TB)
2009 20100
5
10
15
20
25
30
5 %
8 %
24 %
28 %
XDR Ofl Res
2005 - DOTS PLUS Pilot Program started with 350 pts for 2 yrs(Treatment Centers- 5, Sub Centers – 11)
2007 - GLC review and permission for expansion (300/year)
2010 - XDR-TB Treatment started 2011 - Treatment Centre - 12, Sub-Centre - 62 (8
DRTB Hostels established in 5 regions (EDR-1, CDR-3, WDR-1, MWDR-2, FWR-1)
2012 - 2 hostels planned2013 - Treatment centre 13,sub-centre-71, DR Home
in Bandipur
DR TB Program Milestones
1. National TB centre,Thimi (G)2. National Medical College,Birgunj (NG)3. Lalgadh Hospital (G)4. NATA Morang (NG)5. BPKIHS Dharan(NG)6. Regional TB centre, Kaski(G)7. Bhim Hospital,Bhairawa(G)8. Lumbini Zonal Hospital, Butwal(G)9. NATA,Banke (NG)10. Mahakali Zonal Hospital, Mahendra Nagar (G)11. Seti Zonal Hospital,Dhangadhi(NG)12. TEAM Hospital- Dadeldhura(NG)13. NATA/GENETUP-Kathmandu(NG)
List of DR-TB centers

Differences between DR Centre and Sub centre
Treatment centre
Facility of Medicines Facility of Sputum examination Facility of Baseline investigations Responsible for filling all the
documents required for enrollment and follow-up
Responsible to transport the sputum samples to NRL for C/S
Facility of management of severe side effects
Responsible to Quarterly reporting to Regional monitoring & evaluation WS
Sub centre
Facility of medicinesFacility of management of
minor side effectsResponsibility of referring
the patient to DR Centre for each monitoring investigations
Responsible to Quarterly reporting to Treatment centre (DR-TB management WS)

Responsibilities of DR TB centre
1. Counseling to the patient2. Registration of the patients3. Baseline and follow-up investigations4. Collection & transportation of the samples
to NRL5. Provide DOT6. Management of the side effects7. Supervision of DR Sub centers8. Participation in the National monitoring and
evaluation workshop

Responsibilities of DR TB Sub-centre
1. Counseling to the patient2. Provide DOT3. Refer the patients to DR centre for
regular investigations 4. Management of minor side effects

Standard MDR-TB Treatment Regimens
First Phase 8 – 12 months (intensive phase)
1. Kanamycin (KM)2. Pyrazinamide(Z)3. Levofloxacin (Lfx)4. Ethionamide (Eto)5. Cycloserine (Cs)
Second Phase 12 – 14 months (continuation phase)
All the drugs except the injectables.

Extensively Drug Resistance (XDR )TB
XDR-TB is a form of TB which is resistant to at least four of the core anti-TB drugs.
XDR-TB involves resistance to the two most potential anti TB drugs, that is Isonized & Rifampicin, also known as MDR-TB in addition to resistance to any of the floroquinolone (ofloxacin,Moxifloxacin) and any injectable aminoglycosides (Capreomycin, Kanamycin).
Take substantially longer to treat than ordinary(drug susceptible).
Require the use of second line anti TB drugs ,which are more expensive and have more side effects.

Management of XDR TB cases
Started since Feb 2010Much more difficult to treat than MDR TB casesStandard regimen (but individualization is
implemented in the substitution of drugs for severe side effects)
Intensive phase for 12 months and continuation for another 12 months. (Injectable first 8 months six days a week ,and then 4 months thrice a week)
Standard XDR –TB Treatment Regimens
First Phase 12 – 16 months (intensive phase)
1. Capreomycin(CM)2. Pyrazinamide(Z)3. Moxifloxacin(Mfx)4. Amoxycillin/
clavunate(Amoxy/clav)5. Cycloserine (Cs)6. Paraaminosalicylic Acid
(PAS)7. Clofazamine(cfz)
Second Phase 12 – 14 months (continuation phase)
All the drugs except Injectables one.

Drug Resistance Survey Report
Year Initial Any Resistance
Initial MDR
Acquired Any Resistance
Acquired MDR
1999 13.32% 3.74% 28.20% 11.96%
2002 10.99% 1.32% 40.93% 20.46%
2007 14.71% 2.86% 25.3% 11.72%
2011 9.6% 2.2% 25.4% 15.4%

Estimation Of MDR/XDR TB In Nepal
DRS- 2011 2013-14 2014-15 2015-16
Estimated MDR-TB cases among new cases 2.2% 553 557 561
Estimated MDR-TB cases among retreatment cases 15.4% 455 464 467
Total estimated MDR-TB among notified cases 1008 1021 1027
XDR-TB cases targeted for enrolment 35 40 45
Pre-XDR
63 95 120
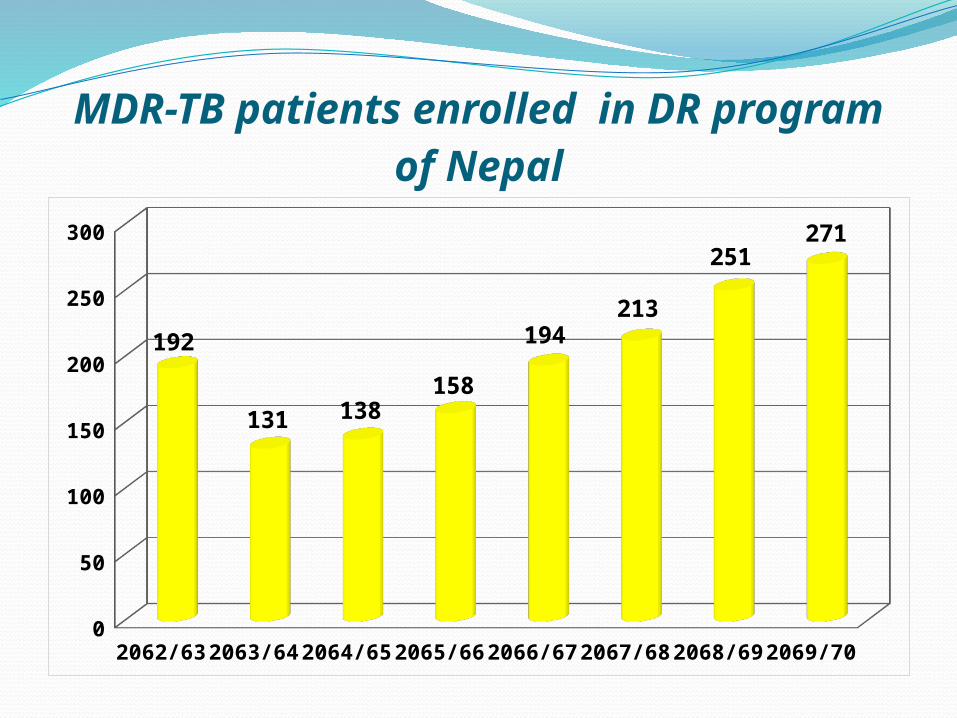
MDR-TB patients enrolled in DR program of Nepal
2062
/63
2063
/64
2064
/65
2065
/66
2066
/67
2067
/68
2068
/69
2069
/70
0
50
100
150
200
250
300
192
131 138158
194213
251271
2062 2063 2064 2065 2066 2067
60.00
62.00
64.00
66.00
68.00
70.00
72.00
74.00
76.00
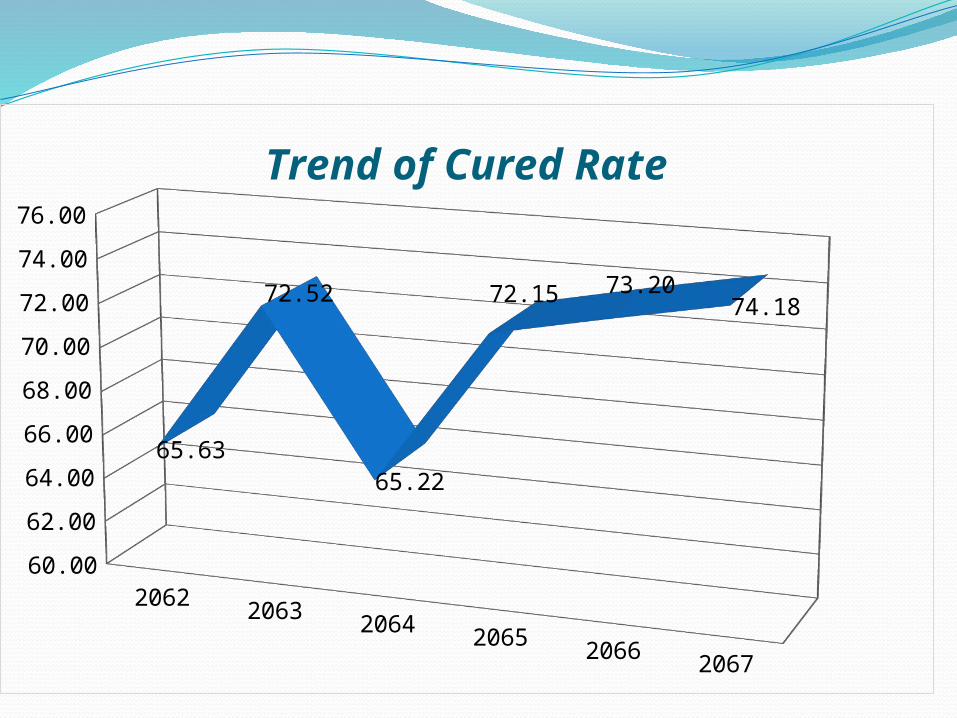
65.63
72.52
65.22
72.15 73.2074.18
Trend of Cured Rate

2062 2063 2064 2065 2066 2067
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
11.6
13.0
8.70
5.705.15 6.57
Trend of Death Rate

2062 2063 2064 2065 2066 2067
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
4.69
4.58
7.97 8.23
9.79
7.98
Trend of Failure Rate

2062 2063 2064 2065 2066 2067
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
18.00
20.0017.4
10.0
18.1
13.3
11.86
11.27
Trend of Defaulter Rate
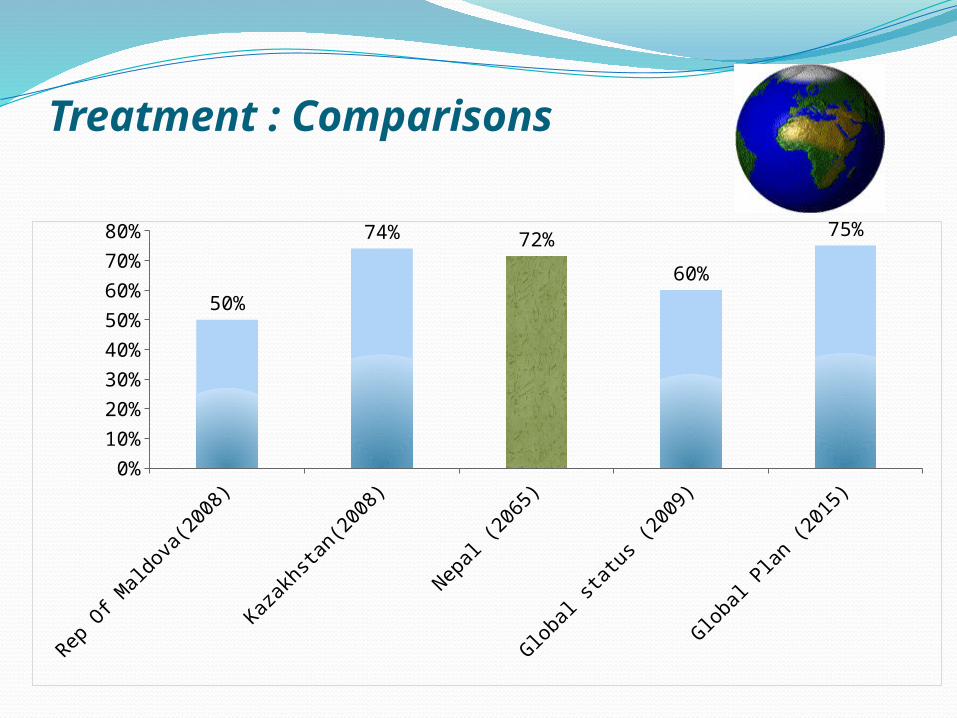
Treatment : Comparisons
Rep O
f Mal
dova
(200
8)
Kazak
hsta
n(20
08)
Nep
al (2
065)
Globa
l sta
tus (
2009
)
Globa
l Pla
n (2
015)
0%
10%
20%
30%
40%
50%
60%
70%
80%
50%
74% 72%
60%
75%

Facility/Support
To Health Care Providers:Health Hazard (Nrs.1000 per month)Supply of PPE (N-95 mask and gloves).
To the patientsNutritional support (Nrs.1500 per month)
throughout the treatment period.Supply of surgical mask

Prevention of MDR TB ?????Rapid diagnosis and adequate treatment of TB
with qualitative drugsSound implementation of DOTS programIdentify contacts who could have contracted TB,
i.e family members, people in close contact etc.Patients with HIV/AIDS should be identified and
diagnosed ASAP.Contact tracing for MDR -TB cases in placeEarly diagnosis of DR-TB cases referring
suspected cases for GeneXpertInfection control measures taken where all DR-
TB patients will be treatedIndoor Facilities ( Isolation) during Ss positive

What Improves Outcomes:• Early identification (and treatment)
of MDR-TB• Use of an “effective” regimen• Adequate patient support• DOT• Prompt management of side-effects• Social economic support

REQUESTDrug resistant tuberculosis is entirely the end
results of a number of different Failures, which is possible to Avoid by providing qualitative service .
LET us work all together for the sake of future generation.
Be sincere towards to own responsibilities
“ STOP TB IN MY LIFETIME”

Challenges !!!
• Ignorance/Poverty• Low MDR-TB case finding• Limitation of sample currier system• Limitation of Diagnostic centers• Insufficient socio-economic support to
patients• High prevalence of Floroquinolone
Resistance• Infection control measures are not in place• Limitation of qualified health personnel in
DR centres• Social stigma
I am Stopping TB
We Must Stop TB

Thank you
Thank you for your kind Attention
Related Documents











