Prognostic value of fragmented QRS in cardiac AL amyloidosis Stefano Perlini a, b, ⁎, Francesco Salinaro a , Francesco Cappelli c, d , Federico Perfetto c , Franco Bergesio c , Alessio Alogna a , Roberta Mussinelli a , Michele Boldrini a , Ambra Raimondi a , Francesco Musca a , Giovanni Palladini b , Giampaolo Merlini b a Clinica Medica II, Department of Internal Medicine, Fondazione IRCCS San Matteo, University of Pavia, Italy b Amyloidosis Research and Treatment Center and Department of Molecular Medicine, Fondazione IRCCS San Matteo, University of Pavia, Italy c Regional Amyloid Center, Azienda Ospedaliero Universitaria Careggi, Florence, Italy d Intensive Cardiac Care Unit, Heart and Vessel Department, Azienda Ospedaliero Universitaria Careggi, Florence, Italy abstract article info Article history: Received 9 April 2012 Received in revised form 16 May 2012 Accepted 27 May 2012 Available online xxxx Keywords: Amyloid Fragmented QRS Electrocardiography Echocardiography Prognosis Background: In light-chain (AL) cardiac amyloidosis, the 12-lead electrocardiogram (ECG) reflects myocardial amyloid infiltration with low limb voltages, pseudoinfarction patterns, and conduction abnormalities. Moreover, it is not unusual to see “aspecific” QRS complex abnormalities, such as notches and RsR′ pattern in the absence of QRS prolongation, i.e. a fragmentation of QRS complexes (fQRS), that has been associated with myocardial scars and prognosis. Since cardiomyocyte damage and interstitial fibrosis are associated with cardiac amyloid deposition, aim of the present study was to analyze the prevalence and the potential prognostic value of fQRS in patients with cardiac amyloidosis. Methods: We enrolled 375 consecutive untreated patients in whom a first AL amyloidosis diagnosis was concluded between 2008 and 2010, 264 with and 111 without heart involvement. Patients with a positive history of coronary disease were excluded from the analysis. Results: The prevalence of fQRS was significantly higher in patients with cardiac AL amyloidosis (28.5% vs. 11.7%; p = 0.0008). After a median follow-up of 561 days, Kaplan–Meier survival analysis revealed a significantly higher mortality in the fQRS group when compared with the “normal” QRS group (p = 0.0008). No association was found between the presence of fQRS and the duration of PQ, QRS, and QTc intervals, the presence of peripheral low voltages or pseudonecrosis, NT-proBNP serum levels or cardiac wall thickness. Conclusions: In patients with cardiac AL amyloidosis, the presence of fQRS at diagnosis has an independent prognos- tic value. Such a simple and cheap analysis in patients' diagnostic work-up may improve diagnosis and prognostic stratification. © 2012 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Amyloidoses constitute a large group of diseases in which aggregates of insoluble toxic protein are deposited in forms of fibrils in several tissues [1,2]. The most common form of systemic amyloidosis is AL amyloidosis, in which fibrils are composed mainly by the N-terminus of a monoclonal immunoglobulin light-chain; the incidence is approximately 1 case per 100,000 person‐years in Western countries and in such patients cardiac involvement is not only frequent but also the most common cause of death [3,4]. In primary (AL) amyloidosis, not only is survival dependent on the presence of cardiac involvement, but heart dysfunction also limits the feasibility of intensive and effective therapy [5–7]. The 12-lead electrocardiogram (ECG) reflects the generalized infiltrative nature of this disease with low voltages in the limb leads, pseudoinfarction patterns in the anterior precordial and/or the inferior limb leads, and conduction abnormalities such as fascicular block or atrioventricular block of varying degrees [4,8–10]. Moreover, it is not unusual to see “aspecific” abnormalities of the QRS complexes, such as notches and RsR′ pattern in the absence of QRS prolongation, that have been never described in detail. It has been suggested that alter- ations in QRS morphology, leading to a terminal conduction delay or a fragmentation of QRS complexes (fQRS) on the 12-lead ECG are associat- ed with regional myocardial scars, in the setting of ischemic heart dis- ease, dilated cardiomyopathy, and repaired tetralogy of Fallot [11–13]. In detail, the definition of fQRS includes various RSR′ patterns with differ- ent morphologies of the QRS complexes with or without the Q wave on a resting 12-lead ECG. Various patterns include an additional R wave (R′) or notching in the nadir of the S wave, or the presence of > 1 R′ fragmen- tation in 2 contiguous leads, corresponding to a major coronary artery territory [14]. These different fQRS morphologies probably represent intramyocardial conduction abnormalities and peri-infarction conduc- tion block due to myocardial necrosis or scar [15]. It is important to note that myocardial scar and/or fibrosis may alter QRS morphology International Journal of Cardiology xxx (2012) xxx–xxx ⁎ Corresponding author at: Clinica Medica II, Dipartimento di Medicina Interna, Università di Pavia, P. le Golgi 19, 27100 Pavia, Italy. Tel.: +39 0382 502285; fax: +39 0382 526897. E-mail address: [email protected] (S. Perlini). IJCA-14930; No of Pages 6 0167-5273/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijcard.2012.05.097 Contents lists available at SciVerse ScienceDirect International Journal of Cardiology journal homepage: www.elsevier.com/locate/ijcard Please cite this article as: Perlini S, et al, Prognostic value of fragmented QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/ j.ijcard.2012.05.097

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

International Journal of Cardiology xxx (2012) xxx–xxx
IJCA-14930; No of Pages 6
Contents lists available at SciVerse ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Prognostic value of fragmented QRS in cardiac AL amyloidosis
Stefano Perlini a,b,⁎, Francesco Salinaro a, Francesco Cappelli c,d, Federico Perfetto c, Franco Bergesio c,Alessio Alogna a, Roberta Mussinelli a, Michele Boldrini a, Ambra Raimondi a, Francesco Musca a,Giovanni Palladini b, Giampaolo Merlini b
a Clinica Medica II, Department of Internal Medicine, Fondazione IRCCS San Matteo, University of Pavia, Italyb Amyloidosis Research and Treatment Center and Department of Molecular Medicine, Fondazione IRCCS San Matteo, University of Pavia, Italyc Regional Amyloid Center, Azienda Ospedaliero Universitaria Careggi, Florence, Italyd Intensive Cardiac Care Unit, Heart and Vessel Department, Azienda Ospedaliero Universitaria Careggi, Florence, Italy
⁎ Corresponding author at: ClinicaMedica II, Dipartimentdi Pavia, P. le Golgi 19, 27100 Pavia, Italy. Tel.: +39 0382 5
E-mail address: [email protected] (S. Perlini).
0167-5273/$ – see front matter © 2012 Elsevier Irelanddoi:10.1016/j.ijcard.2012.05.097
Please cite this article as: Perlini S, et al, Pj.ijcard.2012.05.097
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 9 April 2012Received in revised form 16 May 2012Accepted 27 May 2012Available online xxxxKeywords:AmyloidFragmented QRSElectrocardiographyEchocardiographyPrognosis
Background: In light-chain (AL) cardiac amyloidosis, the 12-lead electrocardiogram (ECG) reflects myocardialamyloid infiltration with low limb voltages, pseudoinfarction patterns, and conduction abnormalities.Moreover, it is not unusual to see “aspecific” QRS complex abnormalities, such as notches and RsR′ patternin the absence of QRS prolongation, i.e. a fragmentation of QRS complexes (fQRS), that has been associatedwith myocardial scars and prognosis. Since cardiomyocyte damage and interstitial fibrosis are associatedwith cardiac amyloid deposition, aim of the present study was to analyze the prevalence and the potentialprognostic value of fQRS in patients with cardiac amyloidosis.Methods:Weenrolled375 consecutive untreatedpatients inwhomafirst AL amyloidosis diagnosiswas concludedbetween 2008 and 2010, 264with and 111without heart involvement. Patientswith a positive history of coronarydisease were excluded from the analysis.Results: The prevalence of fQRS was significantly higher in patients with cardiac AL amyloidosis (28.5% vs. 11.7%;
p=0.0008). After a median follow-up of 561 days, Kaplan–Meier survival analysis revealed a significantly highermortality in the fQRS group when compared with the “normal” QRS group (p=0.0008). No association wasfound between the presence of fQRS and the duration of PQ, QRS, and QTc intervals, the presence of peripherallow voltages or pseudonecrosis, NT-proBNP serum levels or cardiac wall thickness.Conclusions: In patientswith cardiac AL amyloidosis, the presence of fQRS at diagnosis has an independent prognos-tic value. Such a simple and cheap analysis in patients' diagnostic work-up may improve diagnosis and prognosticstratification.© 2012 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Amyloidoses constitute a large group of diseases in which aggregatesof insoluble toxic protein are deposited in forms of fibrils in several tissues[1,2]. The most common form of systemic amyloidosis is AL amyloidosis,in which fibrils are composed mainly by the N-terminus of a monoclonalimmunoglobulin light-chain; the incidence is approximately 1 case per100,000 person‐years in Western countries and in such patients cardiacinvolvement is not only frequent but also the most common cause ofdeath [3,4]. In primary (AL) amyloidosis, not only is survival dependenton the presence of cardiac involvement, but heart dysfunction also limitsthe feasibility of intensive and effective therapy [5–7].
The 12-lead electrocardiogram (ECG) reflects the generalizedinfiltrative nature of this disease with low voltages in the limb
odiMedicina Interna, Università02285; fax: +39 0382 526897.
Ltd. All rights reserved.
rognostic value of fragmente
leads, pseudoinfarction patterns in the anterior precordial and/orthe inferior limb leads, and conduction abnormalities such as fascicularblock or atrioventricular block of varying degrees [4,8–10]. Moreover, itis not unusual to see “aspecific” abnormalities of the QRS complexes,such as notches and RsR′ pattern in the absence of QRS prolongation,that have been never described in detail. It has been suggested that alter-ations in QRS morphology, leading to a terminal conduction delay or afragmentation of QRS complexes (fQRS) on the 12-lead ECG are associat-ed with regional myocardial scars, in the setting of ischemic heart dis-ease, dilated cardiomyopathy, and repaired tetralogy of Fallot [11–13].In detail, the definition of fQRS includes various RSR′patternswith differ-entmorphologies of the QRS complexeswith orwithout the Qwave on aresting 12-lead ECG. Various patterns include an additional R wave (R′)or notching in the nadir of the Swave, or the presence of >1 R′ fragmen-tation in 2 contiguous leads, corresponding to a major coronary arteryterritory [14]. These different fQRS morphologies probably representintramyocardial conduction abnormalities and peri-infarction conduc-tion block due to myocardial necrosis or scar [15]. It is important tonote that myocardial scar and/or fibrosis may alter QRS morphology
d QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/

2 S. Perlini et al. / International Journal of Cardiology xxx (2012) xxx–xxx
without lengthening its duration, thereby resulting in an additional R′ ornotch in either the R or S wave within a narrow QRS complex. The pres-ence of fQRS has been correlated with prognosis in the setting ofischemic heart disease [16–19], dilated cardiomyopathy [19,20], and ac-quired long QT syndrome [21], although this is not predictive of success-ful response to cardiac resynchronization therapy [22], or prophylacticICD implantation [23]. Since in the setting of cardiac amyloidosis car-diomyocyte damage and amyloid deposition may contribute to similaralteration in QRS morphology, aim of the present study was on the onehand to analyze the prevalence of fQRS in patients with cardiac amyloid-osis, and on the other hand to assess whether this finding has a prognos-tic value in predicting advanced heart failure and sudden cardiac death.Indeed the majority of patients with cardiac amyloidosis die for majorcardiac events, which are often sudden cardiac death due to eithertachy- or bradyarrythmias leading to electromechanic dissociation [7].
To this aim, consecutive patients with AL amyloidosis were rec-ruited in the years 2008, 2009, and 2010, with a median follow-upof 18.7 months in order to assess the prevalence of fQRS, the relation-ship with clinical, structural, functional and biochemical data, andtheir possible prognostic significance.
2. Methods
We enrolled all consecutive untreated subjects undergoing extensive multiteamevaluation c/o the Amyloidosis Research and Treatment Center of Pavia and theRegional Amyloid Center of the Careggi Hospital of Florence, Italy in whom firstdiagnosis of primary AL amyloidosis was concluded between 2008 and 2010. Diagnosiswas made according to the International Society of Amyloidosis criteria, as well asassessment of organ involvement at baseline [24]. The presence of heart involvementwas defined according to either the demonstration of amyloid deposits on the endo-myocardial biopsy or by echocardiographic evidence of cardiac amyloidosis in the settingof a defined systemic disease. Echocardiographic features of amyloidosis includeddiastolic dysfunction, and a mean left ventricular wall thickness (septum and posteriorwall) greater than 12 mm in the absence of hypertension or other potential causes ofleft ventricular hypertrophy. The presence of low voltages on 12-lead electrocardiography(all limb leads less than 5 mm in height) was a clue to cardiac involvement by amyloid.Elevation of the N-terminal pro-brain natriuretic peptide (NT-proBNP), and elevation ofcardiac troponins were compared with echocardiography [25–29]. No patient withcardiac AL was found to have NT-proBNP in the normal range. Patients were also dividedaccording to the Mayo staging system as proposed by Dispenzieri and coworkers [30]. Atpresentation, all patients provided informed consent for anonymous publication ofscientific data. The authors of this manuscript have certified that they comply with the“Principles of Ethical Publishing in the International Journal of Cardiology” [31]
2.1. 12-lead ECG
Analysis of the standard 12-lead electrocardiogram (Esaote P8000 Power 1e30, fil-ter range 0.05 to 50 Hz, 25 mm/s, 10 mm/mV) was performed by 2 independentreaders (F.S. and F.C.) blinded to the organ involvement, echocardiographic data andlevels of cardiac biomarkers as well as clinical data. There was 97% concordance in de-fining fQRS between the 2 readers. Beyond the usual electrocardiographic parameters(PQ, QRS, QT intervals), peripheral and total QRS scores were also calculated as the sumof QRS voltages in all the 6 peripheral leads and in all the 12 peripheral and precordialleads, respectively.
2.2. fQRS definition criteria
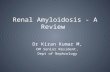
Fragmented QRS was defined by the presence of various RSR' patterns with orwithout a Q wave and included an additional R wave (R), notching of the R wave,notching of the downstroke or upstroke of the S wave, or the presence of >1 R′ in 2contiguous leads corresponding to a major coronary artery territory (Fig. 1) [14]. Elec-trocardiograms were compared with previous electrocardiograms (if available) to con-firm that fQRS or pathologic Q waves were of recent onset.
2.3. Echocardiography
Echocardiographic data were collected with the patient in a supine left lateraldecubitus position. Two-dimensionally targeted M-mode echocardiography was per-formed after the longitudinal parasternal view had been checked to avoid angulationof the ultrasonic beam and consequent changes in the LV shape. LV internal dimen-sions, posterior wall thickness, and interventricular septum thickness were analyzedby a single reader according to the standards of the American Society of Echocardiog-raphy [32]. LV mass was indexed to body surface area (g/m2). Endocardial shorteningfraction (SFendo) was calculated as the difference between the end-diastolic and theend-systolic diameters divided by the end-diastolic diameter and then multiplied by100. Transmitral flow velocity in early (E) and late (A) diastole was measured by
Please cite this article as: Perlini S, et al, Prognostic value of fragmentej.ijcard.2012.05.097
conventional pulsed Doppler in the apical 4-chamber view. Moreover, pulsed TDI-derived early diastolic peak velocity at lateral (E' lateral) mitral annulus was evaluatedas an index of LV relaxation [33]. The E to E′ ratio was also assessed.
2.4. Statistics
Continuous variables are expressed as median values and interquartile ranges, andcategorical variables as frequencies and percentages. Comparisons of continuous vari-ables were based on ANOVA followed by 2-tail Mann–Whitney's U test, and compari-sons of proportions were based on chi-square tests. Prevalence of fQRS was assessedas the number of patients showing this electrocardiographic abnormality divided bythe total study population. Survival curves were plotted according to Kaplan–Meierand differences in survival were tested for significance by the log-rank test. ReceiverOperator Characteristic (ROC) analysis was performed to assess the ability (by calculat-ing the area under the curve) of the biochemical, echo- and electrocardiographic pa-rameters to identify patients who died within 12 months from diagnosis. Coxproportional regression models were fitted to compute hazard ratios (HR) and 95%confidence interval for death for a series of potential predictors, namely the presenceof fQRS, NT-proBNP and Troponin I serum levels (as prognostically validated biochem-ical markers of cardiac dysfunction), LVMI (as an index of the extent of cardiac involve-ment), E/E′ ratio, and Endocardial Shortening Fraction (as indices of diastolic andsystolic dysfunctions, respectively). Moreover, Cox proportional regression modelswere fitted to compute hazard ratios (HR) for death for the presence of fQRS, and forthe Mayo staging system, that has been prognostically validated [30]. All analyseswere performed using MedCalc® version 11.6.1.0.
3. Results
3.1. Study population
The study population included 418 consecutive patients, diag-nosed between 2008 and 2010. To avoid any possible interferenceof ischemic heart disease on the presence of fQRS, patients with a pos-itive history of coronary disease were excluded from the analysis. 43patients without all echocardiographic, electrocardiographic and bio-chemical data were excluded. A cohort of 375 patients (age 65±17 years; 202 males) was included in the final analysis. The cohortwas divided into two groups depending on the presence (n=264)or absence (n=111) of heart involvement by amyloidosis. Patientswith bundle branch blocks (n=14) and with ICD or PM (n=3)were included, following the criteria for definition of fQRS in thiscase as suggested by Das et al. [18].
3.2. ECG presentation
As expected, the presence of cardiac involvement was associatedwith a peculiar electrocardiographic pattern, with a 63.9% proportionof low voltages and a 52.2% proportion of pseudonecrosis, as definedby the presence of a pathological Q wave in two or more contiguousleads in the absence of history of ischemic heart disease and/or evi-dence of akinetic/dyskinetic wall segments [4]. Moreover, when com-pared with patients without cardiac amyloidosis, the presence ofmyocardial involvement was associated with prolonged PQ, QRSand QT intervals. Overt atrio-ventricular block was present in 24.8%of patients with cardiac AL, and complete bundle branch block wasevident in 28% of patients with cardiac involvement. In both casesthe prevalence of atrio-ventricular and intra-ventricular conductiondelays was significantly higher than in patients without cardiac in-volvement (p=0.0295 and p=0.0306, respectively).
3.3. Echocardiographic presentation
Table 1 reports the values of septal and posterior wall end-diastolic thicknesses, left ventricular mass index, end-diastolic andend-systolic chamber volumes, ejection fraction, early-to-atrial trans-mitral flow velocity ratio (E/A ratio), and tissue Doppler E/E′. Asexpected, cardiac amyloidosis was associated with left ventricularconcentric hypertrophy with preserved ejection fraction and evidentdiastolic dysfunction (all pb0.01 vs. patients without cardiac involve-ment). This was associated with a marked increase in NT-proBNP and
d QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/

Fig. 1. The differentmorphologies of fQRSwhich include various RSR′ patterns are shown in this figure. Note that if RSR′ patterns are present in the right precordial leads (leads V1 and V2)with QRSmore than 100 ms (incomplete right bundle branch block) or QRSmore than 120 ms (complete right bundle branch block), and in left precordial lead (RSR′ in leads I, V5 andV6)with QRS more than 120 ms (left bundle branch block), they are defined as complete or incomplete bundle branch block and excluded from the definition of fQRS, whereas if the RSR′pattern is present in the mid precordial lead or in inferior leads, they are defined as fQRS. fQRS, fragmented QRS.Reproduced with permission from [43] (Das et al. Fragmented QRS on a 12-lead ECG: a predictor of mortality and cardiac events in patients with coronary artery disease. Heart Rhythm2007; 4:1385–1392).
3S. Perlini et al. / International Journal of Cardiology xxx (2012) xxx–xxx
TnI serum levels when compared with patients with non cardiac AL[6651 (2821–18133) vs. 190 (125–334)pg/ml and 0.150 (0.04–0.297)vs. 0.03 (0.004–0.019)ng/ml, pb0.01 for both comparisons].
3.4. fQRS distribution
In the whole study group (n=375), fQRS were observed in 88 pa-tients (23.5%), 28.4% with and 11.7% without cardiac involvement.The prevalence of fQRS was significantly higher in patients with car-diac AL amyloidosis (p=0.0008). As to the regional localization, themajority of fQRS were identified in the inferior (60%) or the anterior(26.7%) leads, with a minority in the lateral (13.3%) leads or inmore than one area. In a minority of patients, fQRS were concomitantto a complete bundle branch block (n=14) or to a paced rhythm(n=3). In these patients, the presence of fQRS was identified
Table 1Values of septal (IVS) and posterior wall (PW) end-diastolic thicknesses, end-diastolic(EDVLV) and end-systolic (ESVLV) chamber volumes, left ventricular mass index(LVMI), ejection fraction (EF). Early-to-atrial transmitral flow velocity ratio (E/Aratio), tissue Doppler E/E′, and peripheral and total QRS score of AL patients with andwithout cardiac involvement. Data are expressed as median (interquartile range).ANOVA followed by 2-tail Mann–Whitney's U test.
Non-cardiacAL (n=111)
Cardiac AL(n=264)
p
IVS (mm) 10.2 (9.7–11.8) 15.2 (13.7–16.7) b0.01PW (mm) 10.1 (9.5–11.6) 14.9 (12.7–16.7) b0.01EDVLV (ml) 91 (73–107) 75 (61–96) b0.01ESVLV (ml) 37 (29–42) 31 (24–41) b0.05EF (%) 61 (57–64) 58 (51–65) b0.05LVMI (g/m2) 109 (91–134) 175 (144–198) b0.01E/A ratio 0.78 (0.68–1.09) 1.33 (0.76–2.5) b0.01lateral E/E′ 5.04 (3.92–6.44) 9.44 (6.45–13.46) b0.01Total QRS score (mV) 9.85 (8.27–13.24) 8.33 (6.60–10.00) b0.01Peripheral QRS score (mV) 3.65 (2.55–4.85) 2.45 (1.90–3.25) b0.01
Please cite this article as: Perlini S, et al, Prognostic value of fragmentej.ijcard.2012.05.097
according to the criteria defined by Das and coworkers [18]. Accordingto the Mayo staging system [30], there was a progressive increase ofthe prevalence of fQRS from stage 1 (7.7%) to stage 2 (22.6%) andstage 3 (36.9%) (pb0.05). As reported in Table 2, no difference wasobserved in the echocardiographic and electrocardiographic para-meters when comparing cardiac AL patients with or without evidenceof fQRS. Given the known alterations of the electrocardiogram inducedby the presence of cardiac amyloidosis, the possible relationships be-tween fQRS and other electrocardiographic parameters were analyzed.No association was found between the presence of fQRS and either theduration of PQ, QRS, andQTc intervals, or the presence of peripheral lowvoltages, pseudonecrosis or a strain pattern. Moreover, the presence offQRS was not associated with different structural (i.e. wall thickness,volumes, left ventricularmass index) or functional (i.e. ejection fraction,SFendo, transmitral E/A ratio, lateral tissue Doppler E/E′) echo-cardiographic parameters. Furthermore, the possible association withprognostically validated [25,30,34] biochemical markers of cardiacdysfunction (i.e. BNP, NT-proBNP, and TnI), was excluded. Table 3shows the cutoff values of the different parameters as derived byReceiver Operator Characteristic (ROC) analyses, aimed at assessing
Table 2Values of PQ, QRS and QT intervals, peripheral and total QRS score, and left ventriclemass index (LVMI), endocardial Shortening Fraction (FSendo), and tissue Doppler E/Ein AL patients with and without fQRS. Data are expressed as median (interquartilerange). ANOVA followed by 2-tail Mann–Whitney's U test.
fQRS absent (n=287) fQRS present (n=88) p
PQ (ms) 170 (150–195) 173 (155–200) nsQRS (ms) 80 (78–95) 85 (80–100) nsQTc (ms) 445 (420–468) 450 (418–472) nsTotal QRS score (mV) 8.90 (7.05–10.92) 8.25 (6.82–11.20) nsPeripheral QRS score (mV) 2.87 (2.00–3.70) 2.77 (1.87–4.12) nsLVMI (g/m2) 150 (117–189) 165 (130–186) nsSF endo (%) 39 (31–45) 38 (29–45) nslateral E/E′ 7.26 (5.09–11.42) 7.51 (5.55–12.41) ns
d QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/

Table 4Kaplan–Meier univariable analysis for fQRS, NT-proBNP and Troponin I serum levels,LVMI, E/E′ ratio, and endocardial Shortening Fraction.
Hazard ratio 95% CI p
fQRS presence 2.7369 1.28–5.84 b0.001NT-proBNP>2692 pg/ml 11.0907 6.17–19.94 b0.0001TnI>0.13 ng/ml 5.5137 2.85–10.67 b0.0001LV mass>162 g/m2 3.1763 1.71–5.91 b0.001lateral E/E′>7.28 4.1350 2.26–7.57 b0.0001SF endo>38.23% 3.3123 1.81–6.08 b0.001
4 S. Perlini et al. / International Journal of Cardiology xxx (2012) xxx–xxx
the ability to identify patients who diedwithin 12 months from diagno-sis. Since ejection fraction failed to reach statistical significance as a pre-dictor of survival, endocardial shortening fraction was used as an indexof systolic function. The Kaplan–Meier univariable analysis confirmedthat all the considered parameters significantly predicted survivalafter a median follow-up of 561 days, i.e. the presence of fQRS, NT-proBNP and Troponin I serum levels, LVMI, E/E′ ratio, and EndocardialShortening Fraction (Table 4). In detail, a significantly higher mortalityin the fQRS group when compared with the “normal” QRS group(p=0.0008) was observed in all AL patients. The same trend was alsoconfirmed in the subgroup with cardiac involvement (p=0.0035)(Figs. 2 and 3). We then fitted a multivariable model including allthese parameters, observing that fQRS andNT-proBNPwere the only in-dependent prognostic determinants, while LVmass, TnI, and lateral E/E′, and SFendo did not enter the model (Table 5). When the model in-cluded both fQRS and the Mayo staging system, the presence of fQRSwas associated with a 1.572 death hazard ratio (1.028–2.404;p=0.0379). According to Kaplan–Meier analysis, the presence of fQRSadded to the Mayo staging system was able to differentiate stage II pa-tients' survival (p=0.0165), whereas it did not modify stage I or stageIII mortality (Fig. 4).
4. Discussion
The main result of our study is that patients with cardiac ALamylodosis have a much higher prevalence of fQRS when comparedwith patients without cardiac involvement. Moreover, the presenceof fQRS was associated with a worse prognosis, independent of indi-ces of the extent of amyloid infiltration (such as left ventricularmass index), systolic (SFendo) and diastolic (lateral E/E′) dysfunc-tions. In detail, the presence of fQRS was observed in 28.4% of cardiacAL patients. Such an electrocardiographic pattern has to be added tothe other already described typical features of cardiac AL amyloidosis,i.e. low peripheral voltages and pseudonecrosis, that in our serieswere respectively present in 63.9% and 52.2% patients.
Up to now, studies concerning the presence of fQRS have mainlyinvolved patients with coronary artery disease (CAD) and ischemicscarring. Das and colleagues demonstrated good sensitivity and speci-ficity (>86%) of fQRS for diagnosing myocardial scar in patients withknown or suspected CAD, and the poor prognosis associated with thisECG presentation [18]. More importantly, the presence of fQRS has ahigher negative predictive value for myocardial scar than does the Qwave [14]. Several studies have suggested that fragmentation of QRS oc-curs due to an alteration of the normal depolarization of the ventricles.Both necropsy and in vivo imaging (mainly cardiac magnetic resonanceimaging) studies of patients with myocardial infarction and left ventri-cle aneurysm have confirmed significant myocardial necrosis, with
Table 3The table shows the ROC-derived cut-off values of left ventricle mass index, ejectionfraction, endocardial Shortening Fraction, tissue Doppler E/E′, NT-proBNP, and TnIserum levels, with relative area under the curve, statistical significance, sensitivity,and specificity.
Area underthe ROCcurve
p Value Cut-offvalue
Sensitivity %(CI)
Specificity %(CI)
LV mass(g/m2)
0.631 0.0229 162 62.5 (40.6–81.2) 65.5 (56.0–74.2)
EF (%) 0.557 0.41 59.68 44.0 (24.4–65.1) 73.9 (64.9–81.2)SF endo(%)
0.708 b0.001 38.23 82.6 (61.2–95.0) 56.4 (46.6–65.8)
lateralE/E′
0.758 b0.001 7.28 79.2 (57.8–92.9) 63.2 (53.6–72.0)
NT-proBNP(pg/ml)
0.835 b0.001 2692 93.1 (77.2–99.2) 67.9 (59.4–75.6)
TnI(ng/ml)
0.83 b0.001 0.13 79.3 (60.3–92.0) 80.7 (73.2–86.9)
Please cite this article as: Perlini S, et al, Prognostic value of fragmentej.ijcard.2012.05.097
“islands” of viable myocardial tissue interspersed in abundant fibroustissue [35,36]. This feature is responsible for inhomogeneous activationof the ventricles and can further worsen heart function also in the pa-tientswith amyloidosis and heart involvement, inwhomamyloid depo-sition has been described as “patchy”, causing local alterations of theelectrical impulse conduction. Concomitant atrial involvement maywell be the cause of the observed PQ interval prolongation and of the in-creased incidence of overt atrio-ventricular block in patients with cardi-ac AL. Barasan and colleagues have also suggested that presence of fQRSin patients with narrow QRS can help identifying the presence andcorrectly locating the dyssynchrony and help patient selection for cardi-ac resynchronization therapy [36], although successful response to car-diac resynchronization therapy [22], or prophylactic ICD implantation[23] was not predicted by the presence of this ECG abnormality. Havingused echocardiographic parameters of morphology and function as anindirect estimate of the severity of amyloid heart disease, one possiblelimitation of the present study is the lack of data on cardiac magneticresonance imaging, which is considered the gold standard to preciselyidentify cardiac fibrosis. Therefore on the basis of our data, it is impossi-ble to extend the positive and negative predictive values of fQRS toidentify or exclude a worse heart involvement by amyloidosis. Howev-er, fQRS have a great importance for determining the prognosis of pa-tients with infiltrative cardiomyopathy by amyloidosis, as well as inCAD patients. It is important to note that the presence of fQRS was anindependent prognostic factor in AL patients. No significant associationwas indeed found between the presence of fQRS and cardiac echo-derived anatomic (thicknesses, volumes, LVmass) or functional param-eters (EF, E/A and E/E′), as well as with biochemical markers of cardiacdamage (NT-proBNP, and TnI), and other electrocardiographic parame-ters (PQ, QRS, and QTc intervals, presence of pseudonecrosis and lowvoltages). In the multivariable analysis, fQRS and NT-proBNP were theonly independent prognostic determinants (pb0.05), whereas LVmass, TnI, lateral E/E′, and SFendo did not enter the statistical model(Table 4). Moreover, the presence of fQRS further stratified survival inpatients with Mayo stage II classification. This finding indicates that
Fig. 2. Kaplan–Meier survival curves of AL amyloidosis patients with and without fQRSat the 12-lead ECG.
d QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/

Fig. 3. Kaplan–Meier survival curves of patients with cardiac AL amyloidosis with andwithout fQRS at the 12-lead ECG.
Fig. 4. Kaplan–Meier survival curves according to the Mayo stage and to the presenceor absence of fQRS at the 12-lead ECG.
5S. Perlini et al. / International Journal of Cardiology xxx (2012) xxx–xxx
the presence of fQRS adds a prognostic piece of information to the al-ready known and validated prognostic factors in cardiac amyloidosis,i.e. biochemical markers of cardiac involvement [25,30,34]. Notably,the exclusion of the 17 patients in whom fQRS was concomitant to acomplete bundle branch block (n=14) or to a paced rhythm (n=3)did not change these results. It has to be reminded that in this specificsubset of patients, the presence of fQRS was identified according tothe criteria defined by Das and coworkers [18].
Indeed, patients with cardiac amyloidosis presenting fQRS die morethan thosewithout fQRS.We donot know themechanisms of death, butit may well be due to myocardial damage-related heart failure or to asudden ventricular tachyarrhythmia event, since fQRS is associatedwith a significantly higher incidence of arrhythmic events in patientswith ischemic cardiomyopathy who receive an implantable cardiac de-fibrillator [37]. Depolarization abnormalities that predict sudden cardi-ac death (SCD) are late potentials on signal-averaged ECG (SAECG) andwide QRS aswell as fragmented QRS complexes [14] on routine 12-leadECG. Also repolarization abnormalities, such as the microwave T wavealternans (MTWA), QT prolongation and QT dispersion are predictorsof sudden cardiac death.
It has to be noted that the presence of fQRS is not specific forCAD, being also encountered in other myocardial diseases such asarrhythmogenic right ventricular dysplasia/cardiomyopathy [38],acquired long QT syndrome [21], repaired tetralogy of Fallot [13], andBrugada syndrome [39]. Moreover, recent studies demonstrate a higherprevalence of fQRS in patients with rheumatoid arthritis [40] and pul-monary sarcoidosis [41], as a possible index of myocardial structuralalteration development and/or of extracellularmatrix changes. The pre-sent study adds on this evidence in patients with cardiac AL amyloid-osis, setting the stage for further research in other forms of cardiacamyloid deposition, aswell as for future studies on the relationships be-tween fQRS and cardiac morbidity/mortality. It might be hypothesizedthat fQRS may be valuable in determining the risk for sudden cardiacdeath and for guiding selection for device therapy in patients withstructural heart disease (for example amyloidosis) or with Brugada
Table 5Cox proportional hazard multivariable analysis for fQRS, NT-proBNP and Troponin I serumlevels, LVMI, E/E′ ratio, and endocardial Shortening Fraction. pb0.001 for the model.
Hazard ratio 95% CI p
fQRS presence 2.4229 1.01–4.07 b0.05NT-proBNP>2692 pg/ml 9.1175 2.16–38.51 b0.0001TnI>0.13 ng/ml 1.2872 0.59–2.80 nsLV mass>162 g/m2 1.2563 0.57–2.76 nslateral E/E′>7.28 2.0589 0.83–5.09 nsSF endo>38.23% 2.0676 0.94–4.56 ns
Please cite this article as: Perlini S, et al, Prognostic value of fragmentej.ijcard.2012.05.097
syndrome. It is possible that the predictive value of fQRS for death canbe further enhanced by combining a marker of repolarization abnor-mality such as microwave T wave alternans [42]. This is beyond thescope of the present investigation.
Further studies are needed in order to evaluate the relationshipsbetween fQRS, pseudonecrosis pattern and cardiac involvement, sinceboth these electrocardiographic features have been shown to predictthe presence of myocardial fibrotic scars, at least in the setting of ische-mic cardiac disease. Although preliminary, the results of our studydemonstrate how a simple, cheap and easily feasible diagnostic tech-nique, such as the 12-lead ECG, can enable further characterization ofcardiac amyloid deposition, with a prognostically powerful parameter.Moreover, a thorough analysis of the ECG, focused on the search forfQRS can unveil yet unknown facets of the electrical features of cardiacamyloidosis, which are potentially related to the presence of fibrosisand dyssynchrony.
In conclusion, the search for the presence of fQRS in the 12-leadelectrocardiogram should be recommended in all AL patients, givenits prognostic role in the setting of a rare and ominous disease suchas AL amyloidosis. Moreover, its higher prevalence in patients withcardiac involvement adds on the other diagnostic markers such aslow voltages and pseudonecrosis.
Funding sources
The contributions of G.M., G.P., and S.P. were partially supported by:the EURAMY(“Systemic Amyloidoses in Europe”) project partially fundedby the European Community's Sixth Framework Program; CARIPLO(Fondazione Cassa di Risparmio delle Provincie Lombarde); NOBELProject “Transcriptomics and Proteomics Approaches to Diseases of HighSociomedical Impact: A Technology-Integrated Network”; AssociazioneItaliana per la Ricerca sul Cancro (AIRC) Special Program MolecularClinical Oncology 5 per mille n. 9965. F.S. was partially supported by aninvestigator fellowship from Collegio Ghislieri, Pavia.
References
[1] Merlini G, Bellotti V. Molecular mechanisms of amyloidosis. N Engl J Med2003;349:583–96.
[2] Falk RH. Diagnosis and management of the cardiac amyloidoses. Circulation2005;112:2047–60.
[3] Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory featuresin 474 cases. Semin Hematol 1995:45–59.
[4] Dubrey SW, Cha K, Anderson J, et al. The clinical features of immunoglobulinlight-chain (AL) amyloidosis with heart involvement. QJM 1998;91:141–57.
[5] Merlini G, Stone MJ. Dangerous small B-cell clones. Blood 2006;108:2520–30.[6] Kyle RA, Greipp PR. Amyloidosis (AL). Clinical and laboratory features in 229
cases. Mayo Clin Proc 1983;58:665–83.
d QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/

6 S. Perlini et al. / International Journal of Cardiology xxx (2012) xxx–xxx
[7] Rapezzi C, Merlini G, Quarta CC, et al. Systemic cardiac amyloidoses: disease pro-files and clinical courses of the 3 main types. Circulation 2009;120:1203–12.
[8] Buja LM, Khoi NB, Roberts WC. Clinically significant cardiac amyloidosis. Clinico-pathologic findings in 15 patients. Am J Cardiol 1970;26:394–405.
[9] Roberts WC, Waller BF. Cardiac amyloidosis causing cardiac dysfunction: analysisof 54 necropsy patients. Am J Cardiol 1983;52:137–46.
[10] Falk RH, Rubinow A, Cohen AS. Cardiac arrhythmias in systemic amyloidosis: cor-relation with echocardiographic abnormalities. J Am Coll Cardiol 1984;3:107–13.
[11] el-Sherif N. The rsR′ pattern in left surface leads in ventricular aneurysm. Br HeartJ 1970;32:440–8.
[12] Flowers NC, Horan LG, Thomas JR, Tolleson WJ. The anatomic basis forhigh-frequency components in the electrocardiogram. Circulation 1969;39:531–9.
[13] Park SJ, On YK, Kim JS, et al. Relation of fragmented QRS complex to right ventric-ular fibrosis detected by late gadolinium enhancement cardiac magnetic reso-nance in adults with repaired tetralogy of Fallot. Am J Cardiol 2012;109:110–5.
[14] Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J. Significance of a fragmentedQRS complex versus a Q wave in patients with coronary artery disease. Circula-tion 2006;113:2495–501.
[15] Shadaksharappa KS, Kalbfleisch JM, Conrad LL, Sarkar NK. Recognition and signif-icance of intraventricular block due to myocardial infarction (peri-infarctionblock). Circulation 1968;37:20–6.
[16] Ari H, Cetinkaya S, Ari S, Koca V, Bozat T. The prognostic significance of a fragmen-ted QRS complex after primary percutaneous coronary intervention. Heart Vessels2012;27:20–8.
[17] Erdogan T, Cetin M, Kocaman SA, et al. Relationship of fragmented QRS with prog-nostic markers and in-hospital MACE in patients undergoing CABG. Scand Cardi-ovasc J 2012;46:107–13.
[18] Das MK, Suradi H, Maskoun W, et al. Fragmented wide QRS on a 12-lead ECG: asign of myocardial scar and poor prognosis. Circ Arrhythm Electrophysiol2008;1:258–68.
[19] Das MK, MaskounW, Shen C, et al. Fragmented QRS on twelve-lead electrocardio-gram predicts arrhythmic events in patients with ischemic and nonischemic car-diomyopathy. Heart Rhythm 2010;7:74–80.
[20] Sha J, Zhang S, Tang M, Chen K, Zhao X, Wang F. Fragmented QRS is associatedwith all-cause mortality and ventricular arrhythmias in patient with idiopathicdilated cardiomyopathy. Ann Noninvasive Electrocardiol 2011;16:270–5.
[21] Haraoka K, Morita H, Saito Y, et al. Fragmented QRS is associated with torsades depointes in patients with acquired long QT syndrome. Heart Rhythm 2010;7:1808–14.
[22] Rickard J, Zardkoohi O, Popovic Z, et al. QRS fragmentation is not associated withpoor response to cardiac resynchronization therapy. Ann Noninvasive Ele-ctrocardiol 2011;16:165–71.
[23] Cheema A, Khalid A, Wimmer A, et al. Fragmented QRS and mortality risk in pa-tients with left ventricular dysfunction. Circ Arrhythm Electrophysiol 2010;3:339–44.
[24] Gertz MA, Comenzo R, Falk RH, et al. Definition of organ involvement and treat-ment response in immunoglobulin light chain amyloidosis (AL): a consensusopinion from the 10th International Symposium on Amyloid and Amyloidosis,Tours, France, 18–22 April 2004. Am J Hematol 2005;79:319–28.
[25] Palladini G, Campana C, Klersy C, et al. Serum N-terminal pro-brain natriureticpeptide is a sensitive marker of myocardial dysfunction in AL amyloidosis. Circu-lation 2003;107:2440–5.
[26] Palladini G, Perlini S, Merlini G. Imaging of systemic amyloidosis. In: Gertz MA,Rajkumar SV, editors. Amyloidosis: Diagnosis and Treatment. Humana Press;2010. p. 15–32.
Please cite this article as: Perlini S, et al, Prognostic value of fragmentej.ijcard.2012.05.097
[27] Palladini G, Barassi A, Klersy C, et al. The combination of high-sensitivity cardiactroponin T (hs-cTnT) at presentation and changes in N-terminal natriuretic pep-tide type B (NT-proBNP) after chemotherapy best predicts survival in AL amyloid-osis. Blood 2010;116:3426–30.
[28] Ghio S, Perlini S, Palladini G, et al. Importance of the echocardiographic evaluationof right ventricular function in patients with AL amyloidosis. Eur J Heart Fail2007;9:808–13.
[29] Cappelli F, Porciani MC, Bergesio F, et al. Right ventricular function in AL amyloid-osis: characteristics and prognostic implication. Eur Heart J Cardiovasc Imaging2012;13:416–22.
[30] Dispenzieri A, Gertz MA, Kyle RA, et al. Serum cardiac troponins and N-terminalpro-brain natriuretic peptide: a staging system for primary systemic amyloidosis.J Clin Oncol 2004;22:3751–7.
[31] Coats AJ, Shewan LG. Statement on authorship and publishing ethics in the Inter-national Journal of Cardiology. Int J Cardiol 2011;153:239–40.
[32] Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantita-tion in M-mode echocardiography: results of a survey of echocardiographic mea-surements. Circulation 1978;58:1072–83.
[33] Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quiñones MA. Doppler tissueimaging: a noninvasive technique for evaluation of left ventricular relaxationand estimation of filling pressures. J Am Coll Cardiol 1997;30:1527–33.
[34] Palladini G, Lavatelli F, Russo P, et al. Circulating amyloidogenic free light chainsand serum N-terminal natriuretic peptide type B decrease simultaneously in asso-ciation with improvement of survival in AL. Blood 2006;107:3854–8.
[35] Friedman PL, Fenoglio JJ, Wit AL. Time course for reversal of electrophysiologicaland ultrastructural abnormalities in subendocardial Purkinje fibers surviving ex-tensive myocardial infarction in dogs. Circ Res 1975;36:127–44.
[36] Basaran Y, Tigen K, Karaahmet T, et al. Fragmented QRS complexes are associatedwith cardiac fibrosis and significant intraventricular systolic dyssynchrony innonischemic dilated cardiomyopathy patients with a narrow QRS interval. Echo-cardiography 2011;28:62–8.
[37] Maskoun W, Suradi H, Mahenthiran J, Bhakta D, Das MK. Fragmented QRS com-plexes on a 12-lead ECG predict arrhythmic events in patients with ischemic car-diomyopathy who receive an ICD for primary prophylaxis. Heart Rhythm 2007;4:S211–2.
[38] Peters S, Trummel M, Koehler B. QRS fragmentation in standard ECG as a diagnos-tic marker of arrhythmogenic right ventricular dysplasia-cardiomyopathy. HeartRhythm 2008;5:1417–21.
[39] Morita H, Kusano KF, Miura D, et al. Fragmented QRS as a marker of conductionabnormality and a predictor of prognosis of Brugada syndrome. Circulation2008;118:1697–704.
[40] Kadi H, Inanir A, Habiboglu A, et al. Frequency of fragmented QRS on ECG is in-creased in patients with rheumatoid arthritis without cardiovascular disease: apilot study. Mod Rheumatol 2012;22:238–42.
[41] Schuller JL, Olson MD, Zipse MM, et al. Electrocardiographic characteristics in pa-tients with pulmonary sarcoidosis indicating cardiac involvement. J CardiovascElectrophysiol 2011;22:1243–8.
[42] Das MK, El Masry H. Fragmented QRS and other depolarization abnormalities as apredictor of mortality and sudden cardiac death. Curr Opin Cardiol 2010;25:59–64.
[43] Das MK, Saha C, El Masry H, et al. Fragmented QRS on a 12-lead ECG: a predictorof mortality and cardiac events in patients with coronary artery disease. HeartRhythm 2007;4:1385–92.
d QRS in cardiac AL amyloidosis, Int J Cardiol (2012), doi:10.1016/
Related Documents