P-annotatePDF-v11 INSTRUCTIONS ON THE ANNOTATION OF PDF FILES To view, print and annotate your article you will need Adobe Reader version 9 (or higher). This program is freely available for a whole series of platforms that include PC, Mac, and UNIX and can be downloaded from http://get.adobe.com/reader/ . The exact system requirements are given at the Adobe site: http://www.adobe.com/products/reader/tech-specs.html . Note: if you opt to annotate the file with software other than Adobe Reader then please also highlight the appropriate place in the PDF file. PDF ANNOTATIONS Adobe Reader version 9 Adobe Reader version X and XI When you open the PDF file using Adobe Reader, the Commenting tool bar should be displayed automatically; if not, click on ‘Tools’, select ‘Comment & Markup’, then click on ‘Show Comment & Markup tool bar’ (or ‘Show Commenting bar’ on the Mac). If these options are not available in your Adobe Reader menus then it is possible that your Adobe Acrobat version is lower than 9 or the PDF has not been prepared properly. (Mac) PDF ANNOTATIONS (Adobe Reader version 9) The default for the Commenting tool bar is set to ‘off’ in version 9. To change this setting select ‘Edit | Preferences’, then ‘Documents’ (at left under ‘Categories’), then select the option ‘Never’ for ‘PDF/A View Mode’. (Changing the default setting, Adobe version 9) To make annotations in the PDF file, open the PDF file using Adobe Reader XI, click on ‘Comment’. If this option is not available in your Adobe Reader menus then it is possible that your Adobe Acrobat version is lower than XI or the PDF has not been prepared properly. This opens a task pane and, below that, a list of all Comments in the text. These comments initially show all the changes made by our copyeditor to your file.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

P-annotatePDF-v11
INSTRUCTIONS ON THE ANNOTATION OF PDF FILES
To view, print and annotate your article you will need Adobe Reader version 9 (or higher). This program is freely available for a whole series of platforms that include PC, Mac, and UNIX and can be downloaded from http://get.adobe.com/reader/. The exact system requirements are given at the Adobe site: http://www.adobe.com/products/reader/tech-specs.html.
Note: if you opt to annotate the file with software other than Adobe Reader then please also highlight the appropriate place in the PDF file.
PDF ANNOTATIONS
Adobe Reader version 9 Adobe Reader version X and XI
When you open the PDF file using Adobe Reader, the Commenting tool bar should be displayed automatically; if not, click on ‘Tools’, select ‘Comment & Markup’, then click on ‘Show Comment & Markup tool bar’ (or ‘Show Commenting bar’ on the Mac). If these options are not available in your Adobe Reader menus then it is possible that your Adobe Acrobat version is lower than 9 or the PDF has not been prepared properly.
(Mac) PDF ANNOTATIONS (Adobe Reader version 9)
The default for the Commenting tool bar is set to ‘off’ in version 9. To change this setting select ‘Edit | Preferences’, then ‘Documents’ (at left under ‘Categories’), then select the option ‘Never’ for ‘PDF/A View Mode’.
(Changing the default setting, Adobe version 9)
To make annotations in the PDF file, open the PDF file using Adobe Reader XI, click on ‘Comment’.
If this option is not available in your Adobe Reader menus then it is possible that your Adobe Acrobat version is lower than XI or the PDF has not been prepared properly.
This opens a task pane and, below that, a list of all Comments in the text. These comments initially show all the changes made by our copyeditor to your file.
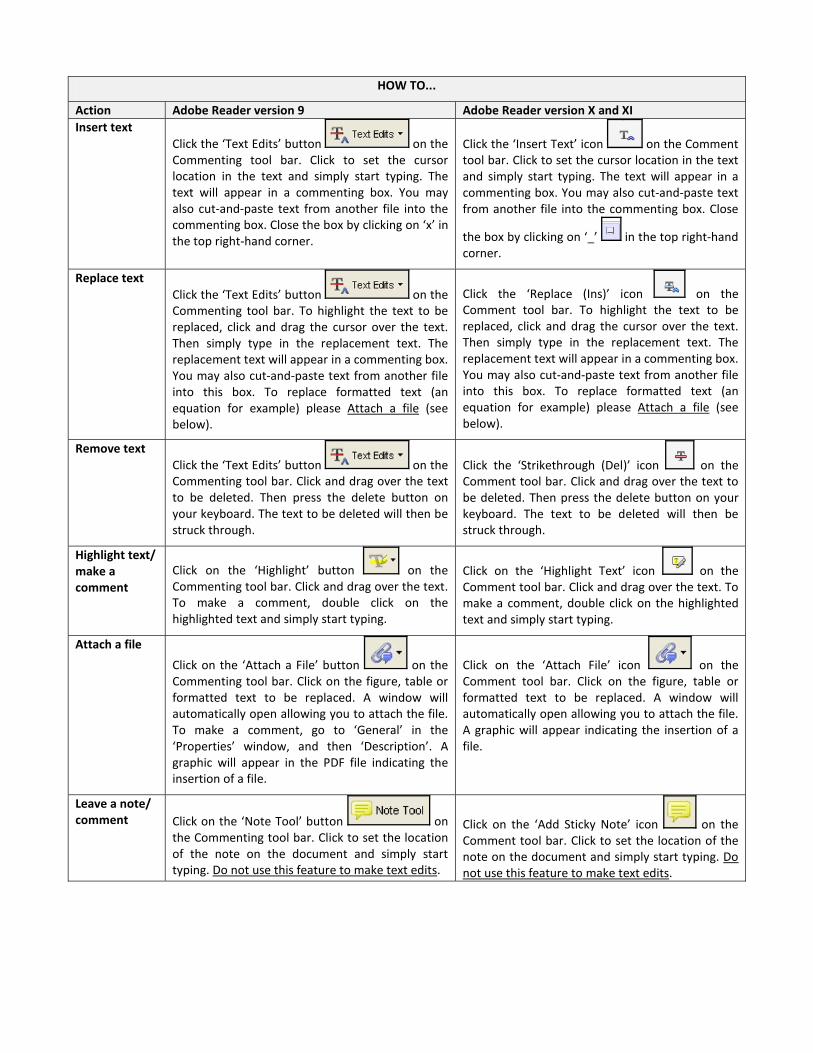
Action
HOW TO...
Adobe Reader version 9 Adobe Reader version X and XI Insert text Click the ‘Text Edits’ button on the
Commenting tool bar. Click to set the cursor location in the text and simply start typing. The text will appear in a commenting box. You may also cut-and-paste text from another file into the commenting box. Close the box by clicking on ‘x’ in the top right-hand corner.
Click the ‘Insert Text’ icon on the Comment tool bar. Click to set the cursor location in the text and simply start typing. The text will appear in a commenting box. You may also cut-and-paste text from another file into the commenting box. Close
the box by clicking on ‘_’ in the top right-hand corner.
Replace text Click the ‘Text Edits’ button on the Commenting tool bar. To highlight the text to be replaced, click and drag the cursor over the text. Then simply type in the replacement text. The replacement text will appear in a commenting box. You may also cut-and-paste text from another file into this box. To replace formatted text (an equation for example) please Attach a file (see below).
Click the ‘Replace (Ins)’ icon on the Comment tool bar. To highlight the text to be replaced, click and drag the cursor over the text. Then simply type in the replacement text. The replacement text will appear in a commenting box. You may also cut-and-paste text from another file into this box. To replace formatted text (an equation for example) please Attach a file (see below).
Remove text Click the ‘Text Edits’ button on the Commenting tool bar. Click and drag over the text to be deleted. Then press the delete button on your keyboard. The text to be deleted will then be struck through.
Click the ‘Strikethrough (Del)’ icon on the Comment tool bar. Click and drag over the text to be deleted. Then press the delete button on your keyboard. The text to be deleted will then be struck through.
Highlight text/ make a comment
Click on the ‘Highlight’ button on the Commenting tool bar. Click and drag over the text. To make a comment, double click on the highlighted text and simply start typing.
Click on the ‘Highlight Text’ icon on the Comment tool bar. Click and drag over the text. To make a comment, double click on the highlighted text and simply start typing.
Attach a file
Click on the ‘Attach a File’ button on the Commenting tool bar. Click on the figure, table or formatted text to be replaced. A window will automatically open allowing you to attach the file. To make a comment, go to ‘General’ in the ‘Properties’ window, and then ‘Description’. A graphic will appear in the PDF file indicating the insertion of a file.
Click on the ‘Attach File’ icon on the Comment tool bar. Click on the figure, table or formatted text to be replaced. A window will automatically open allowing you to attach the file. A graphic will appear indicating the insertion of a file.
Leave a note/ comment Click on the ‘Note Tool’ button on
the Commenting tool bar. Click to set the location of the note on the document and simply start typing. Do not use this feature to make text edits.
Click on the ‘Add Sticky Note’ icon on the Comment tool bar. Click to set the location of the note on the document and simply start typing. Do not use this feature to make text edits.

Action
HOW TO...
Adobe Reader version 9 Adobe Reader version X and XI Review To review your changes, click on the ‘Show’
button on the Commenting tool bar. Choose ‘Show Comments List’. Navigate by clicking on a correction in the list. Alternatively, double click on any mark-up to open the commenting box.
Your changes will appear automatically in a list below the Comment tool bar. Navigate by clicking on a correction in the list. Alternatively, double click on any mark-up to open the commenting box.
Undo/delete change
To undo any changes made, use the right click button on your mouse (for PCs, Ctrl-Click for the Mac). Alternatively click on ‘Edit’ in the main Adobe menu and then ‘Undo’. You can also delete edits using the right click (Ctrl-click on the Mac) and selecting ‘Delete’.
To undo any changes made, use the right click button on your mouse (for PCs, Ctrl-Click for the Mac). Alternatively click on ‘Edit’ in the main Adobe menu and then ‘Undo’. You can also delete edits using the right click (Ctrl-click on the Mac) and selecting ‘Delete’.
SEND YOUR ANNOTATED PDF FILE BACK TO ELSEVIER
Save the annotations to your file and return as instructed by Elsevier. Before returning, please ensure you have answered any questions raised on the Query Form and that you have inserted all corrections: later inclusion of any subsequent corrections cannot be guaranteed.
FURTHER POINTS
Any (grey) halftones (photographs, micrographs, etc.) are best viewed on screen, for which they are optimized, and your local printer may not be able to output the greys correctly.
If the PDF files contain colour images, and if you do have a local colour printer available, then it will be likely that you will not be able to correctly reproduce the colours on it, as local variations can occur.
If you print the PDF file attached, and notice some ‘non-standard’ output, please check if the problem is also present on screen. If the correct printer driver for your printer is not installed on your PC, the printed output will be distorted.

Prognostic Meaning of Coronary MicrovascularDisease in Type 2 Diabetes Mellitus: A Transthoracic
Doppler Echocardiographic Study
Q2 Lauro Cortigiani, MD, Fausto Rigo, MD, Sonia Gherardi, MD, Maurizio Galderisi, MD, Francesco Bovenzi, MD,and Rosa Sicari, MD, PhD, FESC, Lucca, Mestre, Cesena, Naples, and Pisa, Italy
Background: The prognostic value of Doppler-derived coronary flow velocity reserve (CFVR) of the left anteriordescending coronary artery in patients with type 2 diabetes with preserved left ventricular systolic function andwithout flow-limiting stenoses on angiography remains undetermined.
Methods: The study sample consisted of 144 patients with type 2 diabetes (82 men; mean age 626 10 years)with chest pain or angina-equivalent symptoms, no histories of coronary artery disease, and echocardio-graphic ejection fractions $ 50%. All patients underwent dipyridamole stress echocardiography with CFVRassessment of the left anterior descending coronary artery by transthoracic Doppler echocardiography andcoronary angiography showing normal coronary arteries or nonobstructive coronary artery disease.
Results:Mean CFVRwas 2.446 0.57. On individual patient analysis, 109 patients (76%) had CFVR > 2, and 35(24%) had CFVR # 2. During a median follow-up period of 29 months (interquartile range, 14–44 months), 17hard events (five deaths, 12 nonfatal myocardial infarctions) occurred. The annual hard-event rate was 13.9%in subjects with CFVR# 2 and 2.0% in those with CFVR > 2. The annual event rate associated with CFVR# 2was significantly higher both in patients with left ventricular hypertrophy (P < .0001) and in those without leftventricular hypertrophy (P = .048). On Cox analysis, CFVR # 2 (hazard ratio, 11.20; 95% confidence interval,3.07–40.92), and male sex (hazard ratio, 7.80; 95% confidence interval, 1.74–34.97) were independentprognostic indicators, whereas nonobstructive coronary artery disease was not an independent predictor ofoutcomes.
Conclusions:Microvascular dysfunction before the occurrence of coronary artery involvement is a strong andindependent predictor of outcomes in patients with type 2 diabetes. Vasodilator stress CFVR is a suitable toolto assess microvascular dysfunction in routine clinical practice. (J Am Soc Echocardiogr 2014;-:---.)
Keywords: Diabetes, Vasodilator stress echocardiography, Coronary flow velocity reserve, Prognosis,Microvascular disease
Diabetes mellitus provokes functional and morphologic alterations ofthe coronary microcirculation even in the absence of epicardialcoronary atherosclerosis. In fact, vasomotor function is impaired inpatients with type 2 diabetes because of decreased bioavailability ofthe potent vasodilator endothelium-derived nitric oxide1,2 andincreased secretion of vasoconstrictor mediators such as endothelin-13 and angiotensin II.4 Diabetic autonomic neuropathy contributes toalter coronary vasoreactivity.5 In addition, hyalinization6 or wallthickening of intramural arterioles6,7 and reduced density of capillary
vessels8 have been reported as structural changes of the diabetic heart.Most patients with type 2 diabetes have associated arterial hyperten-sion,9 dyslipidemia,10 and obesity,11 contributing to coronarymicrovas-cular damage.12-15 Previous evidence shows both reduced maximalcoronary vasodilation and impairment in the regulation of coronaryflow in response to submaximal increases in myocardial demand inpatients with diabetes mellitus.16 These microvascular abnormalitiesmay lead to myocardial ischemia in the absence of epicardial coronaryatherosclerosis in some circumstances and thus contribute to adversecardiovascular events in patients with diabetes. Functionally, microvas-cular disease in patients with diabetes translates into reduced coronaryflow reserve, as demonstrated with different techniques such as intra-coronary Doppler,16,17 transesophageal Doppler echocardiography,18
and positron emission tomography (PET).19,20 Unfortunately, thesetechniques do not apply to daily practice. However, coronary flowreserve measurement in patients with diabetes is of potential clinicalinterest, as invasively detected impaired coronary flow reserve is anestablished prognostic predictor in unselected cohorts of patientswith normal or mildly diseased coronary arteries.21 Moreover,perfusion defects on single-photon emission computed tomographywere associated with markedly increased risk in asymptomatic patients
From the Cardiology Division, Campo di Marte Hospital, Lucca, Italy (L.C., F.B.);
Cardiology Division, Umberto I Hospital, Mestre, Italy (F.R.); Cardiology Division,
Cesena Hospital, Cesena, Italy (S.G.); Department of Clinical and Experimental
Medicine, Federico II University Hospital, Naples, Italy (M.G.); CNR, Institute of
Clinical Physiology, Pisa, Italy (R.S.).
Reprint requests: Rosa Sicari, MD, PhD, FESC, CNR, Institute of Clinical
Physiology, Via G. Moruzzi, 1, 56124 Pisa, ItalyQ1 (E-mail: [email protected]).
0894-7317/$36.00
Copyright 2014 by the American Society of Echocardiography.
http://dx.doi.org/10.1016/j.echo.2014.02.010
1
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
1234
567
8910
11121314
151617
181920
212223
24252627
282930
313233
343536
37383940
414243
444546
47484950
515253
545556
575859
6061
62636465
666768
697071
72737475
767778
798081
828384
85868788
899091
929394
959697
9899100101
102103104
105106107
108109110111
112113114
115116117
118119120
121122
Original text:
Inserted Text
given name
Original text:
Inserted Text
surname
Original text:
Inserted Text
given name
Original text:
Inserted Text
surname
Original text:
Inserted Text
given name
Original text:
Inserted Text
surname
Original text:
Inserted Text
given name
Original text:
Inserted Text
surname
Original text:
Inserted Text
given name
Original text:
Inserted Text
surname
Original text:
Inserted Text
given name
Original text:
Inserted Text
surname
adonhers
Typewritten Text
adonhers
Typewritten Text
Funding: institutional funding of the CNR, Institute of Clinical Physiology, Pisa, Italy
adonhers
Typewritten Text
ok
adonhers
Typewritten Text
adonhers
Typewritten Text
adonhers
Typewritten Text
adonhers
Typewritten Text
adonhers
Highlight
adonhers
Sticky Note
Please modify affiliation for Fausto Rigo (FR) as follows: Divisione di Cardiologia, Ospedale dell'Angelo, Mestre-Venezia and Maurizio Galderisi (MG): Department of Medical Translational Science, Federico II University Hospital, Naples, Italy
adonhers
Highlight

with diabetes without knowncoronary artery disease(CAD),22 while the presence ofcoronary vascular dysfunction, asassessed using PET, indepen-dently predicted cardiac andall-cause mortality in patientswith and those without dia-betes.23 Intriguingly, patientswith diabetes without knownCAD with visually normal resultson PET but impaired coronaryflow reserve experienced a car-
diac mortality rate comparable with that in patients with knownCAD23; conversely, patients with diabetes without known CAD andvisually normal results on PET who had preserved coronary flowreserve experienced a cardiac mortality rate comparable with that inpatients without diabetes free of CADwith normal imaging findings.23
Lately, transthoracic Doppler echocardiography associated withvasodilatory stress has proved to be a highly feasible and effectivemodality for assessing risk in a general diabetic population,24 as wellas in unselected25 and hypertensive26 patients without obstructiveCAD. The aim of this prospective, multicenter, observational studywas to investigate the prognostic implications of Doppler-derivedcoronary flow velocity reserve (CFVR) of the left anterior descendingcoronary artery (LAD) in patients with type 2 diabetes withangiographically normal or near normal coronary arteries andpreserved systolic left ventricular (LV) function.
METHODS
Patients
From January 2006 to December 2009, 144 patients (82 men; meanage, 62 6 10 years) with type 2 diabetes27 were prospectivelyenrolled at 5 Italian cardiology institutions (in Lucca, Mestre,Cesena, Pisa, and Naples), fulfilling the following inclusion criteria:(1) chest pain or angina-equivalent symptoms, (2) no history ofCAD (i.e., acute coronary syndrome, coronary revascularization,and/or angiographic evidence of$50% diameter coronary stenosis),(3) LV ejection fraction on resting echocardiography $ 50%, (4) nosignificant valvular or congenital heart disease, (5) no prognosticallyrelevant noncardiac diseases (cancer, end-stage renal or liver disease,or severe obstructive pulmonary disease), (6) adequate acousticwindow for imaging the left ventricle (for two-dimensional echocardi-ography) and LAD flowDoppler (for CFVR assessment), (7) dipyrida-mole stress echocardiography with CFVR assessment of the LAD bytransthoracic Doppler echocardiography performed before (within15 days) coronary angiography, and (8) coronary angiographyshowing normal coronary arteries or nonobstructive CAD.Follow-up information was available for all patients. Part of thissample (45 patients [31%]) was previously published24 and repre-sents an extension of follow-up.
Arterial hypertension,28 hypercholesterolemia,29 overweight orobesity,30 and smoking habit were considered associated cardiacrisk factors and defined according to standard definition. Accordingto individual needs and physicians’ choices, 59 patients (41%) wereevaluated after antianginal drugs had been discontinued, and 85patients (59%) were evaluated during antianginal treatment(Table 1). Phylline-containing drugs or beverages were discontinued$24 hours before testing. The decision to perform coronary
angiography in the face of negative results on stress echocardiographywasmade by the referring physician on the basis of the clinical picture.The study was approved by the institutional review board. All patientsgave written informed consent when they underwent stress echocar-diography. When patients provided consent, they also authorizedphysicians to use their clinical data. Stress echocardiographic datawere collected and analyzed by stress echocardiographers notinvolved in patient care.
Resting Echocardiography
Two-dimensional targeted M-mode echocardiography was carriedout under resting conditions for LV measurements, includinginterventricular septal thickness at end-diastole, LV internal dimensionat end-diastole, and posterior wall thickness at end-diastole.Measurements were made in accordance with recommendationsfrom the American Society of Echocardiography.31 LV mass was
Table 1 Clinical, echocardiographic, and angiographicfindings for patients with CFVR of the LAD > 2 and #2
Variable
CFVR > 2
(n = 109)
CFVR # 2
(n = 35) P
Age (y) 62 6 10 65 6 12 .14Men 63 (58%) 19 (54%) .72
Duration of diabetes (y) 8 6 4 10 6 6 .12Glycated hemoglobin
(mg/dL)
7.8 6 0.8 7.7 6 1.1 .59
Insulin therapy 33 (30%) 14 (40%) .29
Body mass index (kg/m2) 27.5 6 2.8 27.0 6 2.7 .42
Overweight or obesity 96 (88%) 28 (80%) .23
Arterial hypertension 78 (72%) 27 (77%) .52
Hypercholesterolemia 56 (51%) 30 (86%) .0003
Smoking habit 37 (34%) 8 (23%) .22
Number of associated
risk factors
2.4 6 1.0 2.7 6 0.9 .25
Left bundle branch block 8 (7%) 3 (9%) .81
LV ejection fraction (%) 59 6 6 58 6 8 .69
LV mass index (g/m2) 114 6 25 122 6 27 .11
LV hypertrophy 61 (56%) 24 (69%) .19Resting heart rate
(beats/min)
69 6 8 69 6 10 .95
Resting systolic blood
pressure (mm Hg)
138 6 16 149 6 17 .001
Resting rate-pressure
product
9,579 6 1,751 10,325 6 2,224 .04
Resting wall motion
abnormalities
11 (10%) 9 (26%) .02
Test performed on
antianginal therapy
62 (57%) 23 (66%) .36
b-blocking agents 38 (35%) 15 (43%) .39
Calcium antagonists 34 (31%) 15 (43%) .21
Long-acting nitrates 14 (13%) 5 (14%) .83
Resting velocity in the
LAD (cm/sec)
29 6 9 37 6 15 <.0001
Peak velocity in the LAD
(cm/sec)
76 6 23 66 6 24 .04
CFVR of the LAD 2.64 6 0.49 1.80 6 0.18 <.0001
Normal coronary arteries 88 (81%) 17 (49%) .0002Nonobstructive CAD 21 (19%) 18 (51%) .0002
Data are expressed as mean 6 SD or number (percentage).
Abbreviations
CAD = Coronary arterydisease
CFVR = Coronary flowvelocity reserve
LAD = Left anterior
descending coronary artery
LV = Left ventricular
PET = Positron emissiontomography
2 Cortigiani et al Journal of the American Society of Echocardiography- 2014
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
123124125126
127128129
130131132
133134135136
137138139
140141142
143144145
146147148149
150151152
153154155
156157158
159160161162
163164165
166167168
169170171172
173174175
176177178
179180181
182183
184185186187
188189190
191192193
194195196197
198199200
201202203
204205206
207208209210
211212213
214215216
217218219
220221222223
224225226
227228229
230231232233
234235236
237238239
240241242
243244

calculated using the following formula32: LV mass (g) = 0.80� [1.04� (interventricular septal thickness at end-diastole +LV internaldimension at end-diastole + posterior wall thickness at end-diastole)3
� (LV internal dimension at end-diastole)3] + 0.6 g. Dividing LV massby body surface area derived LV mass index. LV mass index> 116 g/m2 in men and >104 g/m2 in women was the criterion forLV hypertrophy.33 Ejection fraction was obtained using Simpson’srule.31
Stress Echocardiography
Transthoracic stress echocardiographic studies were performed usingcommercially available ultrasound machines (Sonos 7500 or iE33,Philips Medical Systems, Andover, MA; Vivid System 7, GEMedical Systems, Milwaukee, WI; Acuson Sequoia C256, SiemensMedical Solutions USA, Inc, Mountain View, CA) equipped withmultifrequency phased-array sector scan probes (S3-S8 or V3-V7)and with second-harmonic technology. Two-dimensional echocardi-ography and 12-lead electrocardiographic monitoring wereperformed in combination with high-dose dipyridamole (up to 0.84mg over 6 min).34 Echocardiographic images were semiquantitativelyassessed using a 17-segment, four-point scale model of the leftventricle.35 A wall motion score index was derived by dividing thesum of individual segment scores by the number of interpretablesegments. Ischemia was defined as stress-induced new wall motionabnormality. CFVR was assessed during the standard stress echocar-diographic examination by intermittent imaging of both wall motionand LAD flow.34 Coronary flow in the mid-distal portion of the LADwas sought in the low parasternal long-axis section under the guid-ance of color Doppler flow mapping.34 All studies were digitallystored to simplify offline reviewing and measurements. Coronaryflow parameters were analyzed offline using the built-in calculationpackage of the ultrasound unit. Flow velocities were measured at leasttwice for each study: at baseline and at peak stress (before aminoph-ylline injection). At each time point, three optimal profiles of peakdiastolic Doppler flow velocities were measured, and the resultswere averaged. CFVR was defined as the ratio between hyperemicpeak and basal peak diastolic coronary flow velocities. CFVR # 2was considered abnormal.24 All observers were trained by the samesenior investigator (F.R.), providing consistency in data acquisition,storage, and interpretation, and also through intensive joint readingsessions. All investigators from contributing centers passed qualitycontrol criteria for regional wall motion and Doppler interpretationbefore entering the study, as previously described.36 The previouslyassessed intraobserver and interobserver variability for measurementsof Doppler recordings and regional wall motion analysis assessmentwere <10%.37 In our previous experience, the assessment of CFVRof the LAD had 94% feasibility.24
Coronary Angiography
Coronary angiography in multiple views was performed according tothe standard Judkins technique, adopting femoral or radial approach.At least five views (including two orthogonal views) were acquired forthe left and at least two orthogonal views for the right coronary artery.Additional appropriate projections were obtained in case of superim-position of side branches or foreshortening of the segment of interest.Obstructive CAD was defined as a quantitatively assessed coronarystenosis of $50%. Normal coronary arteries were defined as 0%stenosis in any major vessel or secondary branch. NonobstructiveCAD was defined as any irregularity between 1% and 9% or vesselstenosis between 10% and 40% stenosis in any coronary artery.
The previously assessed intraobserver and interobserver variabilityof the method were 7% and 6%, respectively.38
Follow-Up Data
Outcomes were determined from patient interviews at the outpatientclinic, hospital chart reviews, and telephone interviews with patients,their close relatives, or referring physician. Death and nonfatalmyocardial infarction were registered as clinical events. Coronaryrevascularization (surgery or percutaneous interventions) was alsorecorded. To avoid misclassification of the cause of death,39 overallmortality was considered. Myocardial infarction was defined bytypical symptoms, electrocardiographic evidence, and cardiacenzyme changes. Follow-up data were analyzed for the predictionof hard events (death or nonfatal myocardial infarction).
Statistical Analysis
Continuous variables are expressed as mean 6 SD. Differencesbetween groups were compared using Student’s t and c2 tests, asappropriate. Linear regression was used to assess the correlationbetween CFVR and LV mass index. Hard event rates were estimatedusing Kaplan-Meier curves and compared using the log-rank test.Only the first event was taken into account. Patients undergoingcoronary revascularization (n = 9) were censored at the time of theprocedure. Annual event rates were obtained from Kaplan-Meierestimates to take censoring of the data into account. The associationsof selected variables with outcomes were assessed using Coxproportional-hazards modeling with univariate and stepwise multivar-iate procedures. A significance level of .05 was required for a variableto be included into the multivariate model, while a level of .10 was thecutoff for exclusion. Hazard ratios with corresponding 95% confidenceintervals were estimated. Statistical significance was set at P < .05. SPSSversion 16 (SPSS, Inc, Chicago, IL) was used for analysis.
RESULTS
Themain clinical, echocardiographic, and angiographic findings in thestudy group are listed in Table 1.
Stress Echocardiographic Findings
No complications or limiting side effects occurred. Stress echocardio-graphic results were negative for ischemia in all patients.
Mean CFVR in the entire study group was 2.44 6 0.57. Onindividual patient analysis, 109 patients (76%) had CFVR > 2, and35 (24%) had CFVR # 2. Compared with patients with CFVR > 2,those with CFVR # 2 more frequently had hypercholesterolemia,had higher resting and lower peak LAD flow velocities, and had agreater frequency of nonobstructive CAD (Table 1). In the subsetwith abnormal CFVR, rate-pressure products were significantly higherunder resting conditions because of a higher mean systolic bloodpressure (see Table 1).
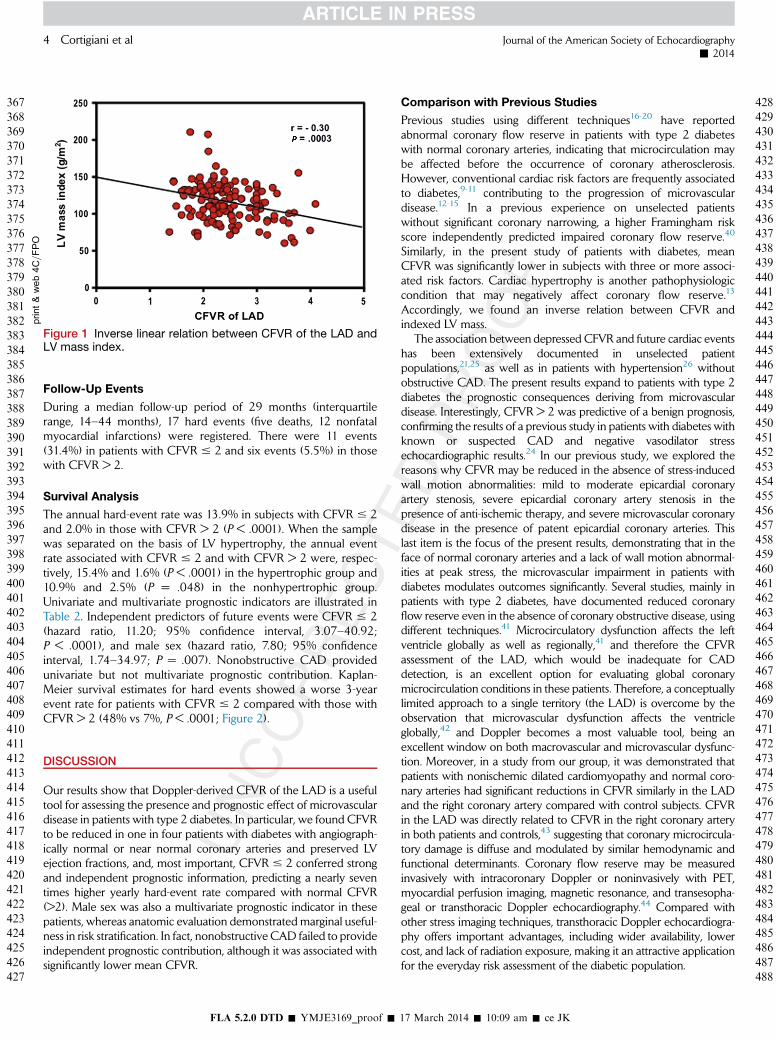
CFVRwas inversely related with LVmass index (Figure 1), as well asthe number of associated cardiac risk factors, 2.546 0.61 in the groupof 68 patients with two or fewer risk factors and 2.34 6 0.50 in thegroup of 76 patients with three or more risk factors (P = .03). Thenumber of risk factors was comparable in the 105 patients with normalcoronary arteries and 39 patients with nonobstructive CAD (2.461.0vs 2.66 0.8, P= .27). However, CFVRwasmarkedly lower in the lattergroup (2.56 6 0.57 vs 2.11 6 0.40, P < .0001).
Journal of the American Society of EchocardiographyVolume - Number -
Cortigiani et al 3
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
245246247248
249250251
252253254
255256257258
259260261
262263264
265266267
268269270271
272273274
275276277
278279280
281282283284
285286287
288289290
291292293294
295296297
298299300
301302303
304305
306307308309
310311312
313314315
316317318319
320321322
323324325
326327328
329330331332
333334335
336337338
339340341
342343344345
346347348
349350351
352353354355
356357358
359360361
362363364
365366
Follow-Up Events
During a median follow-up period of 29 months (interquartilerange, 14–44 months), 17 hard events (five deaths, 12 nonfatalmyocardial infarctions) were registered. There were 11 events(31.4%) in patients with CFVR # 2 and six events (5.5%) in thosewith CFVR > 2.
Survival Analysis
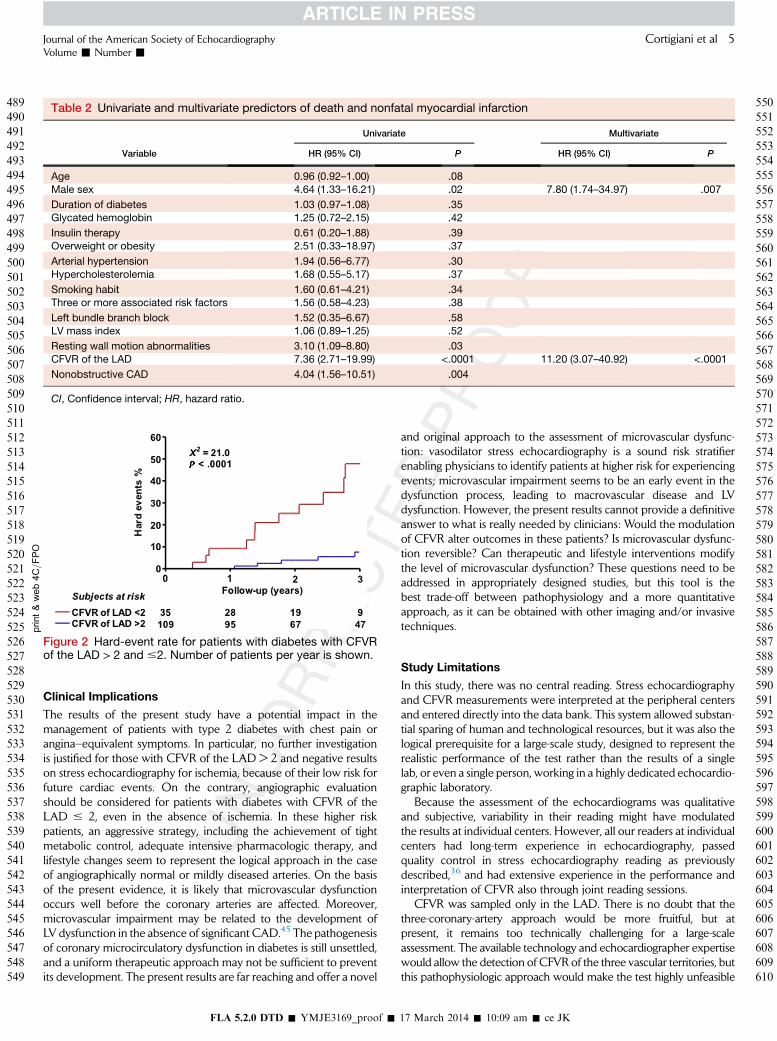
The annual hard-event rate was 13.9% in subjects with CFVR # 2and 2.0% in those with CFVR > 2 (P < .0001). When the samplewas separated on the basis of LV hypertrophy, the annual eventrate associated with CFVR # 2 and with CFVR > 2 were, respec-tively, 15.4% and 1.6% (P < .0001) in the hypertrophic group and10.9% and 2.5% (P = .048) in the nonhypertrophic group.Univariate and multivariate prognostic indicators are illustrated inTable 2. Independent predictors of future events were CFVR # 2(hazard ratio, 11.20; 95% confidence interval, 3.07–40.92;P < .0001), and male sex (hazard ratio, 7.80; 95% confidenceinterval, 1.74–34.97; P = .007). Nonobstructive CAD providedunivariate but not multivariate prognostic contribution. Kaplan-Meier survival estimates for hard events showed a worse 3-yearevent rate for patients with CFVR # 2 compared with those withCFVR > 2 (48% vs 7%, P < .0001; Figure 2).
DISCUSSION
Our results show that Doppler-derived CFVR of the LAD is a usefultool for assessing the presence and prognostic effect of microvasculardisease in patients with type 2 diabetes. In particular, we found CFVRto be reduced in one in four patients with diabetes with angiograph-ically normal or near normal coronary arteries and preserved LVejection fractions, and, most important, CFVR # 2 conferred strongand independent prognostic information, predicting a nearly seventimes higher yearly hard-event rate compared with normal CFVR(>2). Male sex was also a multivariate prognostic indicator in thesepatients, whereas anatomic evaluation demonstrated marginal useful-ness in risk stratification. In fact, nonobstructive CAD failed to provideindependent prognostic contribution, although it was associated withsignificantly lower mean CFVR.
Comparison with Previous Studies
Previous studies using different techniques16-20 have reportedabnormal coronary flow reserve in patients with type 2 diabeteswith normal coronary arteries, indicating that microcirculation maybe affected before the occurrence of coronary atherosclerosis.However, conventional cardiac risk factors are frequently associatedto diabetes,9-11 contributing to the progression of microvasculardisease.12-15 In a previous experience on unselected patientswithout significant coronary narrowing, a higher Framingham riskscore independently predicted impaired coronary flow reserve.40
Similarly, in the present study of patients with diabetes, meanCFVR was significantly lower in subjects with three or more associ-ated risk factors. Cardiac hypertrophy is another pathophysiologiccondition that may negatively affect coronary flow reserve.13
Accordingly, we found an inverse relation between CFVR andindexed LV mass.
The association between depressed CFVR and future cardiac eventshas been extensively documented in unselected patientpopulations,21,25 as well as in patients with hypertension26 withoutobstructive CAD. The present results expand to patients with type 2diabetes the prognostic consequences deriving from microvasculardisease. Interestingly, CFVR > 2 was predictive of a benign prognosis,confirming the results of a previous study in patients with diabetes withknown or suspected CAD and negative vasodilator stressechocardiographic results.24 In our previous study, we explored thereasons why CFVR may be reduced in the absence of stress-inducedwall motion abnormalities: mild to moderate epicardial coronaryartery stenosis, severe epicardial coronary artery stenosis in thepresence of anti-ischemic therapy, and severe microvascular coronarydisease in the presence of patent epicardial coronary arteries. Thislast item is the focus of the present results, demonstrating that in theface of normal coronary arteries and a lack of wall motion abnormal-ities at peak stress, the microvascular impairment in patients withdiabetes modulates outcomes significantly. Several studies, mainly inpatients with type 2 diabetes, have documented reduced coronaryflow reserve even in the absence of coronary obstructive disease, usingdifferent techniques.41 Microcirculatory dysfunction affects the leftventricle globally as well as regionally,41 and therefore the CFVRassessment of the LAD, which would be inadequate for CADdetection, is an excellent option for evaluating global coronarymicrocirculation conditions in these patients. Therefore, a conceptuallylimited approach to a single territory (the LAD) is overcome by theobservation that microvascular dysfunction affects the ventricleglobally,42 and Doppler becomes a most valuable tool, being anexcellent window on both macrovascular and microvascular dysfunc-tion. Moreover, in a study from our group, it was demonstrated thatpatients with nonischemic dilated cardiomyopathy and normal coro-nary arteries had significant reductions in CFVR similarly in the LADand the right coronary artery compared with control subjects. CFVRin the LAD was directly related to CFVR in the right coronary arteryin both patients and controls,43 suggesting that coronary microcircula-tory damage is diffuse and modulated by similar hemodynamic andfunctional determinants. Coronary flow reserve may be measuredinvasively with intracoronary Doppler or noninvasively with PET,myocardial perfusion imaging, magnetic resonance, and transesopha-geal or transthoracic Doppler echocardiography.44 Compared withother stress imaging techniques, transthoracic Doppler echocardiogra-phy offers important advantages, including wider availability, lowercost, and lack of radiation exposure, making it an attractive applicationfor the everyday risk assessment of the diabetic population.
print&web4C=FPO
Figure 1 Inverse linear relation between CFVR of the LAD andLV mass index.
4 Cortigiani et al Journal of the American Society of Echocardiography- 2014
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
367368369370
371372373
374375376
377378379380
381382383
384385386
387388389
390391392393
394395396
397398399
400401402
403404405406
407408409
410411412
413414415416
417418419
420421422
423424425
426427
428429430431
432433434
435436437
438439440441
442443444
445446447
448449450
451452453454
455456457
458459460
461462463
464465466467
468469470
471472473
474475476477
478479480
481482483
484485486
487488
Clinical Implications
The results of the present study have a potential impact in themanagement of patients with type 2 diabetes with chest pain orangina–equivalent symptoms. In particular, no further investigationis justified for those with CFVR of the LAD > 2 and negative resultson stress echocardiography for ischemia, because of their low risk forfuture cardiac events. On the contrary, angiographic evaluationshould be considered for patients with diabetes with CFVR of theLAD # 2, even in the absence of ischemia. In these higher riskpatients, an aggressive strategy, including the achievement of tightmetabolic control, adequate intensive pharmacologic therapy, andlifestyle changes seem to represent the logical approach in the caseof angiographically normal or mildly diseased arteries. On the basisof the present evidence, it is likely that microvascular dysfunctionoccurs well before the coronary arteries are affected. Moreover,microvascular impairment may be related to the development ofLV dysfunction in the absence of significant CAD.45 The pathogenesisof coronary microcirculatory dysfunction in diabetes is still unsettled,and a uniform therapeutic approach may not be sufficient to preventits development. The present results are far reaching and offer a novel
and original approach to the assessment of microvascular dysfunc-tion: vasodilator stress echocardiography is a sound risk stratifierenabling physicians to identify patients at higher risk for experiencingevents; microvascular impairment seems to be an early event in thedysfunction process, leading to macrovascular disease and LVdysfunction. However, the present results cannot provide a definitiveanswer to what is really needed by clinicians: Would the modulationof CFVR alter outcomes in these patients? Is microvascular dysfunc-tion reversible? Can therapeutic and lifestyle interventions modifythe level of microvascular dysfunction? These questions need to beaddressed in appropriately designed studies, but this tool is thebest trade-off between pathophysiology and a more quantitativeapproach, as it can be obtained with other imaging and/or invasivetechniques.
Study Limitations
In this study, there was no central reading. Stress echocardiographyand CFVR measurements were interpreted at the peripheral centersand entered directly into the data bank. This system allowed substan-tial sparing of human and technological resources, but it was also thelogical prerequisite for a large-scale study, designed to represent therealistic performance of the test rather than the results of a singlelab, or even a single person, working in a highly dedicated echocardio-graphic laboratory.
Because the assessment of the echocardiograms was qualitativeand subjective, variability in their reading might have modulatedthe results at individual centers. However, all our readers at individualcenters had long-term experience in echocardiography, passedquality control in stress echocardiography reading as previouslydescribed,36 and had extensive experience in the performance andinterpretation of CFVR also through joint reading sessions.
CFVR was sampled only in the LAD. There is no doubt that thethree-coronary-artery approach would be more fruitful, but atpresent, it remains too technically challenging for a large-scaleassessment. The available technology and echocardiographer expertisewould allow the detection of CFVR of the three vascular territories, butthis pathophysiologic approach would make the test highly unfeasible
Table 2 Univariate and multivariate predictors of death and nonfatal myocardial infarction
Variable
Univariate Multivariate
HR (95% CI) P HR (95% CI) P
Age 0.96 (0.92–1.00) .08Male sex 4.64 (1.33–16.21) .02 7.80 (1.74–34.97) .007
Duration of diabetes 1.03 (0.97–1.08) .35Glycated hemoglobin 1.25 (0.72–2.15) .42
Insulin therapy 0.61 (0.20–1.88) .39Overweight or obesity 2.51 (0.33–18.97) .37
Arterial hypertension 1.94 (0.56–6.77) .30Hypercholesterolemia 1.68 (0.55–5.17) .37
Smoking habit 1.60 (0.61–4.21) .34Three or more associated risk factors 1.56 (0.58–4.23) .38
Left bundle branch block 1.52 (0.35–6.67) .58LV mass index 1.06 (0.89–1.25) .52
Resting wall motion abnormalities 3.10 (1.09–8.80) .03CFVR of the LAD 7.36 (2.71–19.99) <.0001 11.20 (3.07–40.92) <.0001
Nonobstructive CAD 4.04 (1.56–10.51) .004
CI, Confidence interval; HR, hazard ratio.
print&web4C=FPO
Figure 2 Hard-event rate for patients with diabetes with CFVRof the LAD > 2 and #2. Number of patients per year is shown.
Journal of the American Society of EchocardiographyVolume - Number -
Cortigiani et al 5
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
489490491492
493494495
496497498
499500501502
503504505
506507508
509510511
512513514515
516517518
519520521
522523524
525526527528
529530531
532533534
535536537538
539540541
542543544
545546547
548549
550551552553
554555556
557558559
560561562563
564565566
567568569
570571572
573574575576
577578579
580581582
583584585
586587588589
590591592
593594595
596597598599
600601602
603604605
606607608
609610

on a routine basis. Our main aim was to test not only the efficacy butalso the effectiveness of the combined information onwall motion andCFVR in a single test.
The average body mass index of the sample under investigationwas 27 kg/m2. It is conceivable that a selection bias may have beenintroduced, because only patients with good acoustic windowswere entered into the data bank. Moreover, in Italy, obesity doesnot have the characteristics of an epidemic, as in the United States,and this may be another reason for the low enrollment rate of obesepatients.
CONCLUSIONS
Microvascular dysfunction before the occurrence of coronary arteryinvolvement is a strong and independent predictor of outcomes inpatients with type 2 diabetes. Vasodilator stress CFVR is a suitabletool to assess microvascular dysfunction in routine clinical practice.In particular, CFVR of the LAD# 2 represents a strong and indepen-dent predictor of the combined event of death and nonfatal myocar-dial infarction.
REFERENCES
1. Williams SB, Cusco JA, Roddy MA, Johnstone MT, Creager MA. Impairednitric oxide-mediated vasodilation in patients with non-insulin-dependentdiabetes mellitus. J Am Coll Cardiol 1996;27:567-74.
2. De Vriese AS, Verbeuren TJ, Van de Voorde J, Lameire NH,Vanhoutte PM. Endothelial dysfunction in diabetes. Br J Pharmacol2000;130:963-74.
3. Park J-Y, Takahara N, Gabriele A, Chou E, Naruse K, Suzuma K, et al. In-duction of endothelin-1 expression by glucose. An effect of protein kinaseC activation. Diabetes 2000;49:1239-48.
4. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis. Epidemi-ology, pathophysiology, and management. JAMA 2002;287:2570-81.
5. Takahashi T, Nishizawa Y, Emoto M, Kawagishi T, Matsumoto N,Ishimura E, et al. Sympathetic function test of vasoconstrictor changes infoot arteries in diabetic patients. Diabetes Care 1998;21:1495-501.
6. Sutherland CG, Fisher BM, Frier BM, Dargie HJ, Lindop GB.Endomyocardial biopsy pathology in insulin-dependent patients withabnormal ventricular function. Histopathology 1988;14:593-602.
7. Zarich SW, Nesto RW. Diabetic cardiomyopathy. Am Heart J 1989;118:1000-12.
8. Yarom R, Zirkin H, Stammler G, Rose AG. Human coronary microvesselsin diabetes and ischaemia. Morphometric study of autopsy material.J Pathol 1992;166:265-70.
9. Geiss LS, Rolka DB, Engelgau MM. Elevated blood pressure among U.S.adults with diabetes 1988-1994. Am J Prev Med 2002;22:42-8.
10. Rubins HB, Robins SJ, Collins D, Iranmanesh A, Wilt TJ, Mann D, et al.,Department of Veterans Affairs HDL Intervention Trial Study Group.Distribution of lipids in 8,500 men with CAD. Am J Cardiol 1995;75:1196-201.
11. Must A, Spadano J, Coakley CH, Field AE, Colditz G, Dietz WH. Thedisease burden associated with overweight and obesity. JAMA 1999;282:1523-9.
12. Schwartzkopff B, Frenzel H, Dieckerhoff J, Betz P, Flasshove M,Schulte HD, et al. Morphometric investigation of human myocardium inarterial hypertension and valvular aortic stenosis. Eur Heart J 1992;13(suppl):17-23.
13. Marcus ML. Importance of abnormalities in coronary flow reserve tothe pathophysiology of left ventricular hypertrophy secondary tohypertension. Clin Cardiol 1989;12(suppl):IV34-5.
14. Egashira K, Hirooka Y, Kai H, Sugimachi M, Suzuki S, Inou T, et al.Reduction in serum cholesterol with pravastatin improves
endothelium-dependent coronary vasomotion in patients withhypercholesterolemia. Circulation 1994;89:2519-24.
15. GrangerDN, Rodrigues SF, YildirimA, Senchenkova EY.Microvascular re-sponses to cardiovascular risk factors. Microcirculation 2010;17:192-205.
16. Nasher PJ Jr., Brown RE, Oskarsson H, Winniford MD, Rossen JD.Maximal coronary flow reserve and metabolic coronary vasodilation inpatients with diabetes mellitus. Circulation 1995;91:635-40.
17. Nitenberg A, Valensi P, Sachs R, DaliM, Aptecar E, Attali JR. Impairment ofcoronary vascular reserve and Ach-induced coronary vasodilation indiabetic patients with angiographically normal coronary arteries andnormal left ventricular systolic function. Diabetes 1993;42:1017-25.
18. Kranidis A, Zamanis N, Mitrakou A, Patsilinakos S, Bouki T, Tountas N,et al. Coronary microcirculation evaluation with transesophageal echocar-diography Doppler in type II diabetics. Int J Cardiol 1997;59:119-24.
19. Di Carli F, Janisse J, Grunberger G, Ager J. Role of chronic hyperglicemia inthe pathogenesis of coronary microvascular dysfunction in diabetes. J AmColl Cardiol 2003;41:1387-93.
20. Kjaer A, Meyer C, Nielsen FS, Parving HH, Hesse B. Dipyridamole, coldpressor test, and demonstration of endothelial dysfunction: a PET studyof myocardial perfusion in diabetes. J Nucl Med 2003;44:19-23.
21. Lerman A, Zeiher AM. Endothelial function: cardiac events. Circulation2005;111:363-8.
22. De Lorenzo A, Lima RS, Siqueira-Filho AG, Pantoja MR. Prevalence andprognostic value of perfusion defects detected by stress technetium-99msestamibi myocardial perfusion single-photon emission computedtomography in asymptomatic patients with diabetes mellitus and noknown coronary artery disease. Am J Cardiol 2002;90:827-32.
23. Dorbala S, Di Carli MF, Beanlands RS, Merhige ME, Williams BA,Veledar E, et al. Prognostic value of stress myocardial perfusion positronemission tomography: results from a multicenter observational registry.J Am Coll Cardiol 2013;61:176-84.
24. Cortigiani L, Rigo F, Gherardi S, Sicari R, Galderisi M, Bovenzi F, et al.Additional prognostic value of coronary flow reserve in diabetic andnondiabetic patients with negative dipyridamole stress echocardiographyby wall motion criteria. J Am Coll Cardiol 2007;50:1354-61.
25. Sicari R, Rigo F, Cortigiani L, Gherardi S, Galderisi M, Picano E. Additiveprognostic value of coronary flow reserve in patients with chest painsyndrome and normal or near-normal coronary arteries. Am J Cardiol2009;103:626-31.
26. Cortigiani L, Rigo F, Galderisi M, Gherardi S, Bovenzi F, Picano E, et al.Diagnostic and prognostic value of Doppler echocardiographic coronaryflow reserve in the left anterior descending artery in hypertensive andnormotensive patients [published erratum appears in Heart2012;98:92]. Heart 2011;97:1758-65.
27. Ryd�en L, Standl E, Bartnik M, Van den Berghe G, Betteridge J, de Boer MJ,et al, Task Force on Diabetes and Cardiovascular Diseases of the EuropeanSociety of Cardiology (ESC), European Association for the Study ofDiabetes (EASD). Guidelines on diabetes, pre-diabetes, and cardiovasculardiseases: executive summary. The Task Force on Diabetes and Cardiovas-cular Diseases of the European Society of Cardiology (ESC) and of theEuropean Association for the Study of Diabetes (EASD). Eur Heart J2007;28:88-136.
28. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, GermanoG,et al. Management of Arterial Hypertension of the European Society ofHypertension; European Society of Cardiology 2007 guidelines for themanagement of arterial hypertension: the Task Force for the Managementof Arterial Hypertension of the European Society of Hypertension (ESH)and of the European Society of Cardiology (ESC). J Hypertens 2007;25:1105-87.
29. National Cholesterol Education Program Expert Panel. Third report of theExpert Panel onDetection, Evaluation andTreatment ofHighBloodCholes-terol in Adults (Adult Treatment Panel III): full report. Available at: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp3full.pdf. Accessed March3, 2014.
30. Wilson PWF, D’Agostino RB, Sullivan L, Parise H, Kannel WB.Overweight and obesity as determinants of cardiovascular risk. Arch IntMed 2002;162:1867-72.
6 Cortigiani et al Journal of the American Society of Echocardiography- 2014
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
611612613614
615616617
618619620
621622623624
625626627
628629630
631632633
634635636637
638639640
641642643
644645646
647648649650
651652653
654655656
657658659660
661662663
664665666
667668669
670671
672673674675
676677678
679680681
682683684685
686687688
689690691
692693694
695696697698
699700701
702703704
705706707
708709710711
712713714
715716717
718719720721
722723724
725726727
728729730
731732

31. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA,et al, Chamber Quantification Writing Group, American Society ofEchocardiography’s Guidelines and Standards Committee, EuropeanAssociation of Echocardiography. Recommendations for chamberquantification: a report from the American Society of Echocardiography’sGuidelines and Standards Committee and the Chamber QuantificationWriting Group, developed in conjunction with the European Associationof Echocardiography, a branch of the European Society of Cardiology.J Am Soc Echocardiogr 2005;18:1440-63.
32. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al.Echocardiographic assessment of left ventricular hypertrophy: compari-son to necropsy findings. Am J Cardiol 1986;57:450-8.
33. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognosticimplications of echocardiographically determined left ventricular massin the Framingham Heart Study. N Engl J Med 1990;322:1561-6.
34. Sicari R, Nihoyannopoulos P, Evangelista A, Kasprzak J, Lancellotti P,Poldermans D, et al. Stress echocardiography expert consensus statementfrom the European Association of Echocardiography. Eur J Echocardiogr2008;9:415-37.
35. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK,et al., American Heart Association Writing Group on MyocardialSegmentation and Registration for Cardiac Imaging. Standardizedmyocardial segmentation and nomenclature for tomographic imaging ofthe heart: a statement for healthcare professionals from the CardiacImaging Committee of the Council on Clinical Cardiology of the Amer-ican Heart Association. Circulation 2002;105:539-42.
36. Picano E, Mathias W, Pingitore A, Bigi R, Previtali M, on behalf of theEDIC Study Group. Safety and tolerability of dobutamine-atropine stress
echocardiography: a prospective, large scale, multicenter trial. Lancet1994;344:1190-2.
37. Rigo F, RichieriM, Pasanisi E, Cutaia V, Zanella C, Della Valentina P, et al. Use-fulness of coronary flow reserve over regional wall motion when added todual-imaging dipyridamole echocardiography. Am JCardiol 2003;91:269-73.
38. Picano E, ParodiO, Lattanzi F, Sambuceti G, AndradeMJ,Marzullo P, et al.Assessment of anatomic and physiological severity of single-vesselcoronary artery lesions by dipyridamole echocardiography. Comparisonwith positron emission tomography and quantitative arteriography.Circulation 1994;89:753-61.
39. Lauer MS, Blackstone EH, Young JB, Topol EJ. Cause of death in clinicalresearch: time for a reassessment? J Am Coll Cardiol 1999;34:618-20.
40. Rubinshtein R, Yang EH,Rihal CS, PrasadA, LennonRJ, Best PJ, et al. Assess-ment of endothelial function by non-invasive peripheral arterial tonometrypredicts late cardiovascular adverse events. Eur Heart J 2010;31:936-42.
41. L’Abbate A. Large and micro coronary vascular involvement in diabetes.Pharmacol Rep 2005;57(suppl):3-9.
42. Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med2007;356:830-40.
43. Rigo F, Ciampi Q, Ossena G, Grolla E, Picano E, Sicari R. Prognostic valueof left and right coronary flow reserve assessment in nonischemic dilatedcardiomyopathy by transthoracic Doppler echocardiography. J Card Fail2011;17:39-46.
44. Pries AR, Habazettl H, Ambrosio G, Hansen PR, Kaski JC, Sch€achinger V,et al. A review ofmethods for assessment of coronarymicrovascular diseasein both clinical and experimental setting. Cardiovasc Res 2008;80:165-74.
45. LaaksoM. Heart in diabetes: a microvascular disease. Diabetes Care 2011;34(suppl):145-9.
Journal of the American Society of EchocardiographyVolume - Number -
Cortigiani et al 7
FLA 5.2.0 DTD � YMJE3169_proof � 17 March 2014 � 10:09 am � ce JK
733734735736
737738739
740741742
743744745746
747748749
750751752
753754755
756757758759
760761762
763764765
766767768
769770771772
773774775
776777778
779780781782
783784785
786787788
789790791
792793
794795796797
798799800
801802803
804805806807
808809810
811812813
814815816
817818819820
821822823
824825826
827828829
830831832833
834835836
837838839
840841842843
844845846
847848849
850851852
853854

Our reference: YMJE 3169 P-authorquery-v9
AUTHOR QUERY FORM
Journal: YMJE
Article Number: 3169
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen
annotation in the PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than
Adobe Reader then please also highlight the appropriate place in the PDF file. To ensure fast publication of your paper please
return your corrections within 48 hours.
For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in
the proof.
Location
in articleQuery / Remark: Click on the Q link to find the query’s location in text
Please insert your reply or correction at the corresponding line in the proof
If there are any drug dosages in your article, please verify them and indicate that you have done so by
initialing this query
Q1 Please disclose any conflict of interests or funding for this article.
Q2 Please confirm that given names and surnames have been identified correctly.
Please check this box or indicate
your approval if you have no
corrections to make to the PDF file ,
Thank you for your assistance.
Related Documents