Professor Ley Sander Department of Clinical and Experimental Epilepsy UCL Institute of Neurology National Hospital for Neurology & Neurosurgery Queen Square, London WC1N 3BG The Medical and Surgical Treatment of Epilepsy

Professor Ley Sander Department of Clinical and Experimental Epilepsy UCL Institute of Neurology National Hospital for Neurology & Neurosurgery Queen Square,
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Professor Ley SanderDepartment of Clinical and Experimental Epilepsy
UCL Institute of Neurology
National Hospital for Neurology & Neurosurgery
Queen Square, London WC1N 3BG
The Medical and Surgical Treatment of Epilepsy
The Treatment of Epilepsy
• The incidence and prevalence
• Aetiologies and risk factors
• Aims of treatment
• Clinical settings
• Principles of treatment – Medical treatment– Surgical treatment
• Guidelines
• Conclusions
Incidence and Prevalence
• Incidence of new cases of epilepsy:• 50/100,000/year
• Incidence of single seizures:• 20 - 30/100,000/year
• Prevalence of active epilepsy • 5 - 10/1,000 (50% because on AEDs)
• Severe epilepsy: 1 - 2/1,000
• Cumulative Incidence (lifetime prevalence):• 2 - 5%
Incidence and Prevalence in the UK
• 30 000 new cases a year
• 300 000 - 400 000 cases
• 72 000 - 80 000 cases of severe epilepsy
Incidence and Prevalence in the UK
• GP– 1 - 2 new cases of epilepsy/year– 10 - 12 cases of active epilepsy
• Neurologist– 150 cases of epilepsy/single seizures/year– 1,200 cases of active epilepsy
Epilepsy: Aetiologies and Risk Factors
• Risk factors varies with age and geographic location
– Congenital, developmental and genetic conditions in childhood, adolescence and young adults
– Head trauma, infection and tumours at any age although tumours more likely over age 40
– Cerebrovascular disease common in elderly
– Endemic infections are associated with epilepsy in certain areas – malaria, neurocysticercosis, paragonomiasis,
– no adequate large scale study of attributable risk yet
Antiepileptic Treatment
• AEDs are mainstay treatment
• Non-pharmacological options feasible in only few selected cases
– Surgery
• Curative
• Palliative
– Ketogenic diet (children)
– Behaviour modification– Avoidance therapy in cases with clear precipitants
Aims of Antiepileptic Treatment
• Complete seizure freedom• 50% seizure reduction of little benefit
• No adverse effects• long term treatment - long term effects ?• cognitive effects debilitating• teratogenicity
• Non-obtrusive treatment• once or twice daily• No PK or PD interactions
• Maintenance of a normal lifestyle
• Reduction in morbidity and mortality
AED Treatment: Clinical Settings
• Prophylactic Treatment
• Newly Diagnosed Epilepsy
• Single seizure
• Recurrent seizures
• Chronic Epilepsy
Prophylactic use of AEDs
• Often advocated after • Head injury• Craniotomy
There are considerable compliance problems
• There is no evidence of a protective effect of this policy• No place for this!
• Better wait for the event to happen
Is it Epilepsy ?
• Newly diagnosed or suspected cases at Primary Care
level > 50% not epilepsy
commonest differential diagnosis: syncope
• Chronic cases 15 - 20% not epilepsy
mostly psychological in nature
Careful diagnostic assessment a must in all cases
The Single Seizure
• A controversial area!
• Single unprovoked attack usually not treated: practice to defer treatment until 2 or more seizures, although patients at high risk may be treated after a first attack
• Incidence of epilepsy much greater than of single seizures
• Community-based studies show that overall risk of a second
seizure greater than previously accepted • selection bias
Patients Seizure type
time to entry bias
The Single Seizure
• AED treatment following a single seizure reduce risk of recurrence in the short term although long term prognosis not changed
• This may eventually lead to changes in the way single seizures are managed• treatment after first seizure• - for six months, for a year?
• tailored treatment and not symptomatic
• Meanwhile, involve patient and or guardians in the decision
Recurrent Seizures
• Treatment recommended after two or more seizures
Exceptions:
- Long interval between seizures
- Clear identifiable precipitant factor
- Patient against treatment
- Unlikely compliance
Precipitating Factors
Fever
Drugs
Alcohol
Photo-Sensitivity
Sleep Deprivation
Reflex Mechanisms
Acute Metabolic Stress
Emotional Stress/Major Life Events
Starting an AED
• Starting AED treatment is a major event and should not be undertaken without careful evaluation of all relevant factors
• Therapy is a long term prospect
• All implications must be fully explained to the individual and or guardian
• Paramount that the patient or guardians are kept informed about the treatment process and the rationale behind it

Starting Treatment
• Treatment should always be started with a single drug at a small dose
• All common side-effects must be discussed• teratogenicity and contraception if applicable
• Importance of compliance should be stressed
• Careful titration is a must
- start low, go slow
Choice of AEDs treatment
• Choice of AED influenced by:• Type of seizure and or epileptic syndrome • Individual circumstances of patient• Side effect profile of drug• Personal preferences
• No clear cut evidence based medicine is available!
• Clinical practice is based more on dogmatic teaching than on scientific knowledge
• Empirical rather than rational
Principles of AED treatment
• Diagnosis clearly established
• Appropriate first line drug for syndrome and patient
• One drug at a time as a rule:– If first drug ineffective add another first line drug and then
withdraw first drug
• Combination therapy only when single drug ineffective
What Is Chronic Epilepsy ?
• Active 2 years after onset
• Failed 2 first line AEDs
• Great number of seizure in early history
Chronic Epilepsy 1
• Review history of epilepsy- Obtain and review old notes if possible- Interview patient and witness- Classify seizures
• Review diagnosis- Non-epileptic events- Identifiable aetiology- High resolution MRI scanning
• Question Compliance- Check serum AED levels
• Review past and present AED treatment for efficacy and side-effects
Chronic Epilepsy 2
• Select the AED that is most likely to be efficacious and with the least side-effects
• Adjust the dose of the selected drug to the optimum
• Attempt to reduce and taper other AEDs
• If seizures continue despite a maximally tolerated dose of a first-line drug: - Check compliance- tablet count, serum levels, counselling
• Commence another first-line AED if there is one that has not been used to its optimum
Chronic Epilepsy 3
• If seizures continue try a combination of two AEDs
• If combination unhelpful, AED which appears most effective and with fewer side-effects should be continued and the other AED replaced
• If this drug is effective, withdrawal of the initial agent should be considered; if not, it should be replaced by another AED
• Consider the possibility of surgical treatment
• Consider using an experimental AED
Inappropriate use of AEDs
• Inappropriate treatment of people who do not have epilepsy
• Inappropriate drug treatment of patients who do have epilepsy• JME easily treated with some AEDs but poorly controlled with others• Partial epilepsies often misdiagnosed as generalised epilepsy
• Incorrect dosages or inappropriate use of polytherapy • Overzealous adherance to “therapeutic” AED drug levels
AED drug levels monitoring
Measurement of AED levels: • drug toxicity occurs and needs to be documented• suspected non-compliance• suspected drug interactions• during pregnancy (free levels)• during systemic illness• phenytoin therapy
Not a guide to dosing!
• Partial seizures: simple, complex, sec gen.
• Stereotyped onset
• No non-epileptic attacks
• No contraindication for Neurosurgery
• Active epilepsy for >2-3 yr, despite 3 + AEDs
• Inadequate seizure control: > 1-2 c p s /month
• Acceptance of best risk / benefit ratio
Who Should be Evaluated for Surgery
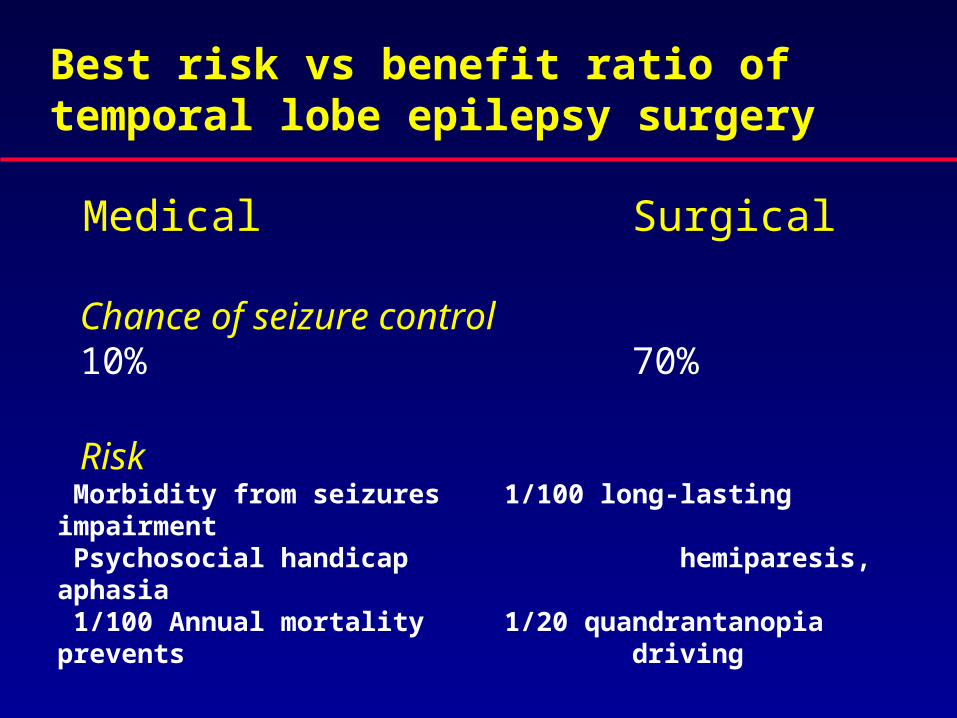
Best risk vs benefit ratio of temporal lobe epilepsy surgery
Medical Surgical
Chance of seizure control 10% 70%
Risk Morbidity from seizures 1/100 long-lasting impairment Psychosocial handicap hemiparesis, aphasia 1/100 Annual mortality 1/20 quandrantanopia prevents
driving
• 70% Anterior temporal lobe resection
• 20% Extra-temporal cortical resection Lesionectomy
• 10% Palliative Procedures • Hemispherectomy• Corpus callosotomy• Subpial transection• Vagal Nerve Stimulation
Range of Epilepsy Surgery
Convergence of data– One epileptogenic & dysfunctional area – Rest of brain normal
• Clinical• Neuro-Imaging• EEG• Neuropsychology• Neuropsychiatry • Psychosocial
Components of Presurgical Evaluation
Realistic expectations?• Improvement in life from seizure control? • Intelligence, memory will not improve• Not more attractive, employable• Need to continue AEDs after Social support• Family, friends, community, finances
Psychosocial
• Fundamental
• MRI predicts nature and extent of pathology
• Unusual to resect area with normal imaging
• Poor results if imaging normal
Neuro-imaging
TLE: Anterior Temporal Lobe resection • Focal pathology: 70% seizure free, 25% >90% reduced
• DNT, cavernoma>HS>AVM>trauma>MCD
• 20% seizure free if no focal pathology
Extra Temporal Lobe• Focal pathology: 60% seizure free, 20% >90% reduced
• DNT, cavernoma, glioma>AVM>trauma
• MCD 20-30% seizure free, if focal
• <20% seizure free if no focal pathology
Pathology and Outcome
Treatment Guidelines for Epilepsy
• NICE = www.nice.org.uk – National Institute for Clinical Excellence (England and Wales)
• SIGN = www.sign.ac.uk – Scottish Intercollegiate Guidelines Network (Scotland)
• AAN = www.aan.com – American Academy of Neurology (USA)
Primary Care Guidelines for Epilepsy
• Referral of ALL who experience a suspected seizure– Seen within 14 days by specialist
• Risk and safety precautions documented• Care Plan in place• At least a yearly review• Early re-referral if
– Treatment failure– Seizures not controlled– Diagnostic uncertainty – Considering pregnancy– Considering drug withdrawal
Managing People With Epilepsy
Holistic issues:- Interest and continuity of care- Clear plan- Information provision
- SUDEP
- Easy access
- Practical Issues: • Cooking, Bathing, Driving, Contraception, Conception
- Reasonable Expectations:• Prognosis, Independent Living, Employment
AED Treatment: Conclusions
Correct diagnosis and classification paramount to treatment
AEDs are mainstay treatment
Treatment empirical rather than rational!
> 70% of patients become seizure free
Potential complications: toxicity
Low threshold for s/effects
AED Treatment: Conclusions
Potential for misuse of AEDs not to be dismissed
New AEDs may be better tolerated, but more effective?
Chronic side effect profile of new AEDs not fully known
Surgical treatment very successful but only possible in a few selected cases
Consider stopping AED if seizure free for years
New treatment still needed!
Related Documents











