Hepatitis C in Australian Prisons Professor Michael Levy AM Australian National University, Canberra

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Hepatitis C in Australian Prisons
Professor Michael Levy AM
Australian National University, Canberra
Hepatitis C in Australian Prisons
• Australian prisoners gained access to Direct Acting Antiviral medications for Hepatitis C infection on 1 March 2016 • Early access to these medications has already raised some
interesting issues for prisoner health services • Harm minimisation implementation in Australian prisons will be
reassessed by custodial authorities, utilising a limited evidence base • Hepatitis C will continue to reveal strengths and weaknesses in the
Australian health/ corrective services interface
What is Hepatitis C?
Hepatitis virus, is a virus like no other! First described in 1991 The hepatitis C virus does not kill liver cells directly, but the immune response to the virus in the liver, can cause liver inflammation and cell death. And this leads to cirrhosis (scar formation)…. and this to liver cancer. There is no adequate immune response for most infections, … but total for some! There is no acquired immunity, and no vaccine. Non-protective antibodies remain as markers of previous infection, … but not always!
Hepatitis C in Australian Prisons
• 6 genetic varients, which respond to specific treatments differently (genotypes 1 and 3 and currently covered)
• Genotype 3 is more connected to hepatic cell carcinoma
• Pre-cirrhotic treatment is critical; post-cirrhotic surveillance is critical
Hepatitis C Transmission
• Injecting drug use
• Tattoos
• Fights
• Sharing shaving and hairdressing equipment
Hepatitis C in Australian Prisons
• Australian Government has committed $1 billion for HCV treatment – irrespective of severity of disease, including prisoners; “silent” on re-treatment of reinfection
• 5-year agreement with pharmaceutical industry
• A 12 week, curative course of treatment costs ~$110,000

Hepatitis C in Australian Prisons
• There are ~233,000 Australians infected with hepatitis C, ~9,000 new infections annually
• Prior to March 2016, <3,000 were receiving treatment (annually); interferon-based treatments were unpopular, selective and cure was not guaranteed
• Between March and July 2016, nearly 22,500 Australians received treatment
Hepatitis C in Australian Prisons
• Genotype 1a, >8 viral load – 12 weeks, not 8 weeks
• Fibroscan > 40 years of age (risk of cirrhosis prior to this age is very low)
• AST to platelet ratio (APRI) instead of fibroscan, especially in young patients
Benefits of Treating in the prison-clinical ‘space’
• Proximity of the health service to the patient
• Support from mental health, close at hand
• “Shared Care” is tailored to the environment – efficiency
• Supervision of every dose – compliance, side-effects
• Peer support
• Alcohol is reasonably well controlled
• Access to pharmacotherapies – but not in all jurisdictions
• Less ‘chaos’ benefits individuals with poorer social function (sic: compliance)
• Aboriginal incarceration, cannot be ignored
Risks of Treating in the prison-clinical ‘space’
• Access to the full range of harm minimisation strategies is limited • Re-infection is a real risk • Side-effects of treatment in a closed environment, .. too easily
‘punished’ • Transition to community / loss to follow-up • Will DAAs find a “price” in the prison-drug market?
Hepatitis C in Australian Prisons
• Treatment should occur in a setting where re-infection is minimised.
• How can this be achieved in prison? • Bring your contacts for treatment (snow-ball recruitment within
networks) • Re-treat reinfection ($110,000 per episode) • Continue to re-test post-treatment induced cure • Do all doses need to be supervised?
Hepatitis C in Australian Prisons
• Currently – “low hanging fruit”
• What is next?
• 1 visit -> treatment; the future of fibroscan; escorts to appointments; treatment targets
• Sterilised environment – by when, how maintained?
• Treat 40/1000 for 15 years will halve prevalence – is this acceptable?
Luciani et al, Addiction 2014; 109: 1695-1706
• Almost half the cohort reported IDU during follow-up (103 subjects; 49.1%) and 65 (31%) also reported sharing of the injecting apparatus. There were 38 HCV incident cases in 269.94 person-years (py) of follow-up with an estimated incidence of 14.08 per 100 py [confidence interval (CI) = 9.96–19.32].
• Incident infection was associated independently with Indigenous background, injecting daily or more and injecting heroin. Three subjects were RNA-positive and antibody-negative at the incident time-point, indicating early infection, which provided a second incidence estimate of 9.4%.
• Analysis of continuously incarcerated subjects (n = 114) followed over 126.73 py, identified 13 new HCV infections (10.26 per 100 py, CI = 5.46–17.54).
• Bleach-cleansing of injecting equipment and opioid substitution treatment were not associated with a significant reduction in incidence.
INHSU – September 2016
PRISONS COULD UNLOCK HEPATITIS C FREE FUTURE • Treatment in prisons is a public health priority
• “it is clear that prisons act as incubators of hepatitis C, driving the epidemic both within the prison system and in the community at large.” Professor Andrew Lloyd (September 2016)
• Australia is one of the only countries to look at the mass scale up of new hepatitis C treatment combined with prevention programs in a prison setting.
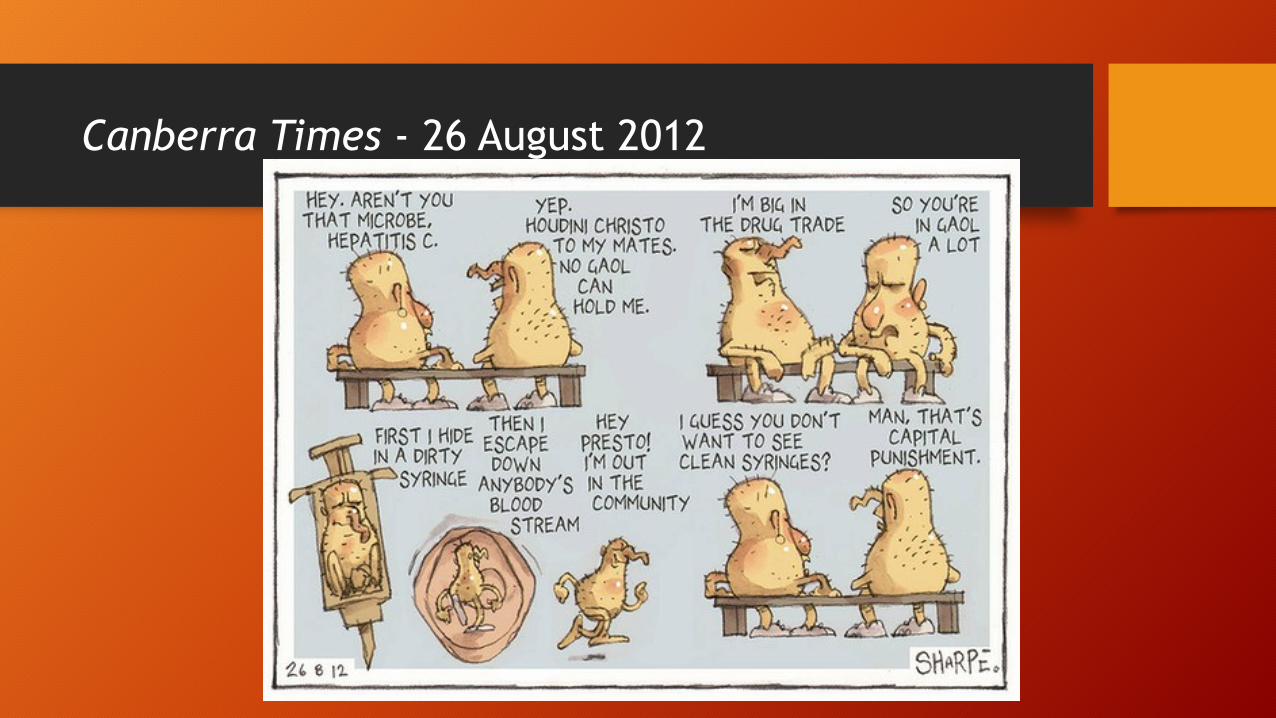
Canberra Times - 26 August 2012
For if you suffer your people to be ill-educated, and their manners to be corrupted from their infancy, and then punish them for those crimes to which their first education disposed them, what else is to be concluded from this, but that you first make thieves and then punish them. Utopia, Sir Thomas More (1478 - 1535
Related Documents











