Competition in Health Care and Health Insurance Lessons from the US and Elsewhere Martin Gaynor E.J. Barone Professor of Economics and Public Policy Heinz College Carnegie Mellon University Freedom of Choice and Competition in Health Care Annual VATT Seminar Helsinki, Finland, November 1, 2016 1

Prof. Martin Gaynor: Competition in Health Care and Health Insurance - Lessons from the US and Elsewhere
Feb 09, 2017
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Competition in Health Care and
Health Insurance Lessons from the US and Elsewhere
Martin Gaynor E.J. Barone Professor of Economics and Public Policy
Heinz College
Carnegie Mellon University
Freedom of Choice and Competition in Health Care
Annual VATT Seminar
Helsinki, Finland, November 1, 2016
1

Introduction • Health care spending is high and rising around the world
– US: $3 trillion; $9,523 per capita, 17.5% of GDP
• Larger than the entire economy of France
• Can’t be sustained without serious strain/harm
– Gov’t spends ~1/3 of revenues on healthcare; projected to rise to ~1/2
– Recent slowdown, but unclear how likely this is to last
• Hospital, physician services, health insurance are ~10% of GDP (more than computers, cars, beer)
– Finland: $19.8 billion, $3,628 per capita, 9.6% of GDP
– OECD: $162 billion, $3,470 per capita, 9.0% of GDP
• There are also serious concerns about the quality of care, waiting times and access to care, and innovation and responsiveness.
2
>

Well, At Least It’s Art
3
by Andy Warhol Pittsburgh native, Carnegie Mellon ‘49 ~ 1985-86 was available via Christie’s $15-20,000

Health Reform • There have been regular attempts at health reform
– Motivated by spending, waiting times,…
• Most of these efforts work for a while, but then spending resumes growing as before (waiting times..?)
– Stakeholders figure out the new system and how to “game” it
• This puts governments in the position of having to keep tightening their belts
– Unpopular with the citizenry and with stakeholders
• Competition is viewed as an alternative
– “Let the market take care of it”
• Competition has important virtues
– Deliver the products/services that consumers value at the lowest feasible cost
• Competitive markets don’t always work well
– Market imperfections (asymmetric information, market power,..) • Characterize health care
– Equity/distribution
4

Competition in Health Care and Health Insurance
• Competition as a system/reform
– United States • Uses markets for provision of care (~100%), for financing (~50%)
– Netherlands • Uses markets for provision of care (<100%), for financing (~100%)
– Switzerland • Uses markets for financing of care (~100%)
– United Kingdom • Uses markets for provision of care (<100%); for financing (small %)
– South Africa • Private and public systems for provision and financing
5

Competition in Health Care and Health Insurance
• Key feature
– Patient choice
• Differences in competitive systems
– Market determined prices • US private health care, private insurance
• UK private health care, private insurance
• Netherlands health care, insurance
• South Africa private health care, private insurance
– Administered prices • US Medicare (public); UK NHS
6

United States • The US relies on markets for the provision and financing (~1/2) of
health care
– That means that the health care system will only work as well as the markets that support it, but...
– Those markets don’t work as well as they could/should
• Prices are high and rising, there are quality problems, there’s too little organizational innovation
• Fragmented delivery system, need for coordination of care
– Consolidation, concentration, and market power have a large part to do with that
• Markets are highly concentrated
• More consolidation is happening
– Matters for the Affordable Care Act and for health reform generally – depends on markets
7

What’s Happening in the US? • Health spending
– High and rising (but recent “slowth”)
– Private spending driven by prices; public spending driven by volume
• Prices
– Competition among providers or insurers drives prices down
– But… lots of consolidation, concerns over market power
• Quality
– Concerns over quality: too low, too much variation, too much “inappropriate care”
– Competition among providers seems to improve quality
• Relevant for public as well as private patients
• Consolidation may harm competition and patients
• Innovation, Efficiency, Service
– Health system characterized as sclerotic, unresponsive, uncreative
8

What’s Happening in the US?
• Competition
– Lots of consolidation • Horizontal (hospital-hospital, physician-physician, insurer-insurer)
• Vertical (hospital-physician; insurer-hospital, physician)
– Anticompetitive practices • Anti-tiering, anti-steering, gag clauses
• Most favored nations clauses
– Lack of entry, dynamism
9

0,00%
2,00%
4,00%
6,00%
8,00%
10,00%
12,00%
14,00%
16,00%
18,00%
Pe
rce
nta
ge C
han
ge
Year
National Health Expenditures Annual Growth Rate
US Health Care Cost Growth 1961-2014
2013; 2.9%
2007; 6.4%
10
2014; 5.3%
Source: CMS, National Health Expenditure Accounts, Historical Data

What’s Driving the Growth in US Private Health Spending? It’s the Prices
11
Changes in Utilization and Prices of Medical Service Categories, 2014 Source: Health Care Cost Institute

Factors Accounting For Growth In Per Capita National Health Expenditures, 2004–14
It’s The Prices – Over Time
Source: CMS

What’s Driving Geographic Variation in US Private Health Spending? It’s the Prices
13
Wage and Risk Adjusted Hospital Prices, 2008-2011
http://www.healthcarepricingproject.org

Private Knee MRI Prices
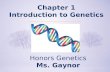
National Variation in US Private Prices and Medicare Fees: Knee MRI
Note: Each column is a hospital; Medicare prices are calculated using Medicare Impact Files
Medicare Knee MRI Prices Mean 353
Min - Max 293 - 546
p10-p90 325 - 389
IQR 335 - 366
p90/10 ratio 1.2
IQR ratio 1.09
Coefficient of Variation 0.08
Gini Coefficient 0.04
Mean 1,331
Min - Max 260 - 3,174
p10-p90 745 - 2,036
IQR 960 - 1,629
p90/10 ratio 2.73
IQR ratio 1.70
Coefficient of Variation 0.38
Gini Coefficient 0.21

Colonoscopy Facility Prices Within US Markets Denver, CO Atlanta, GA Manhattan, NY
Columbus, OH Philadelphia, PA Houston, TX
Note: Each column is a hospital. Prices are regression-adjusted, measured from 2008 – 2011, and presented in 2011 dollars.
Private Price Medicare Reimbursement

US Hospital Consolidation • A lot of consolidation
– Over 1,200 mergers since 1994
– 457 mergers from 2010-2014
– Most urban areas are now dominated by 1-3 large hospital systems • Typical area: 1 dominant system, 2-3 smaller systems, small independents
• Boston, Cleveland, Pittsburgh, San Francisco
139
110
86 83
58
38
59 51 57 58 60
52
72 90
107
88 100
287
175
132 118
101
56
236
88
249
149
78 80
125
156
244
296
178
0
50
100
150
200
250
300
350
98 99 00 01 02 03 04 05 06 07 08 09 10 11 12 13 14
Number of Deals Number of Hospitals
Source: American Hospital Association

US Physician-Hospital Consolidation • Lots of acquisitions of physician practices by hospitals.
– 32% increase in # of doctors employed by hospitals over last decade. – 33% of physicians now employed by hospitals. – Share of spending from hospital owned practices rose from 16.9% in 2007
to 26.5% in 2013. – Growth of ACOs.
• Acquisitions of physician practices by hospitals can reduce competition in the physician services market. – Example: town with 2 hospitals, 10 physician practices in 10 specialties.
• Hospital acquisition: 10 practices per specialty → 2 practices. • Physician integration: 10 practices per specialty → 10 multispecialty practices.
– St. Luke’s case (FTC v. St. Luke’s/Salzer, 2014) • Largest health system in the state (St. Luke’s); largest multispecialty group (Salzer) • Physician practices were each other’s closest competitor • Benefits of merger (care coordination, EMR, evidence based medicine, risk based
contracts) – Plausible, but speculative – Merger not necessary to achieve benefits
17

US Insurer Consolidation, National
18/16
Source: NAIC & CCIIO. Excludes California.
NAIC CCIIO
Market Share of Top 4 Insurers, Fully-insured Commercial

• Figures reflect self + full-insurance, by state and MSA
• Nationwide, 2-firm concentration ratio (CR) is .28
• And if we could subdivide by customer segment, higher still
US, Local Market Concentration Higher
19/16
State 2-firm CR (N=51) MSA 2-firm CR (N=388)
Source: 2014 AMA Competition in health insurance report
.66 .7

How Does Competition in US Private Health Care Work?
• Consumers don’t pay for the product directly, due to insurance
– Not like markets for toothpaste, air travel, etc.
• Two-Stage Competition
– Hospitals and doctors compete to be included in insurers’ networks • Price, Quality, Service
– Compete to attract patients • Quality, Service, Price
20

How Does Competition in US Private Health Care Work?
• Employers buy health insurance from insurers – Insurers compete to sell insurance to employers
• Compete on premiums, benefits, provider networks, service
– Employees enroll in plans offered by their employers
• Pay part of premium directly
• Pay part indirectly (lower pay or increase)
• Insurers contract with providers to be part of the networks for enrollees
– Providers compete to be included in insurers’ networks • Compete on prices, quality, services, reputation
– Providers compete with others in the network to attract patients
• Compete on quality, services, reputation, location
21

How Does Competition in US Private Health Care Work?
• Higher insurance premiums
– Get passed through to workers
– Cause employers to reduce workers’ coverage, reduce their contributions
• Higher provider prices
– Increase insurers’ expenses
– Lead to increased premiums to employers,…
22

Evidence on Competition: US
• Prices
– Prices higher in more concentrated markets • Hospitals
• Physicians
• Insurers
– Mergers between close competitors lead to large price increases • Hospitals
– No difference between not-for-profits and for-profits • Hospitals
• Quality
– Medicare (administered prices) • Quality (mortality) lower in more concentrated markets
– Private (market determined prices) • Mixed evidence
• Strongest evidence is that quality lower in more concentrated markets
23

Evidence on Competition: US Hospital Prices
• Federal Trade Commission retrospectives
– Haas-Wilson and Garmon (2011)
• Merger of Evanston Northwestern and Highland Park hospitals.
• Four out of five insurers experienced substantial price increases due to the merger.
• 20.1%, 26.5%, 35.1%, 64.9% (relative to non-merging Chicago hospitals).
• Merger of St. Therese and Victory Memorial didn’t increase prices.
– Tenn (2011)
• Merger of Sutter and Summit hospital systems in SF Bay area.
• Summit prices increase post-merger by 28.4%, 28.7%, 44.2% for 3 insurers.
– Thompson (2011)
• Merger of Cape Fear and New Hanover hospitals in Wilmington, NC.
• Price increases of 56.5%, 65.3% for two insurers, no effect for one insurer, price decrease of 30% for one insurer.
24
®

Evidence on Competition: US Hospital Prices
• Vita and Sacher (2001) – Merger of Dominican Santa Cruz and AMI-Community hospitals in Santa Cruz, CA.
– Only 2 hospitals in Santa Cruz; 1 other hospital (Watsonville) in Santa Cruz county.
– Price increases of 23% at Dominican, 17% at Watsonville.
• Gaynor and Vogt (2003) – Merger of Tenet and Ornda hospital corporations.
– 2 Tenet hospitals in San Luis Obispo county (Sierra Vista, Twin Cities); one Ornda hospital (French).
– 3 hospitals in SLO itself (French, General, Sierra Vista).
– Five hospitals in San Luis Obispo county, two more within 50 miles.
– Merger would have led to price increases of 53% at French, 32% at Sierra Vista, 33% at Twin Cities, 5% at General, 5% Arroyo Grande.
• Dafny (2009) – Hospitals increase price by 40% following mergers of nearby rivals.
• Nevo, Gowrisankaran, and Town (2014) – Merger of Inova Health System and Prince William hospital in Northern Virginia.
– Price increase of 30.5% at Prince William.
• Increased insurance premiums – Trish and Herring (2015): 3 to 2 hospital merger 4.2% increase in premiums.
25
®

Evidence on Competition: US Physician Prices
• Physician practice mergers
– Can lead to substantial price increases (Dunn and Shapiro, 2014, Baker et al., 2014a)
– Can lead to higher price growth (Baker et al., 2014a)
• Hospital acquisitions of physician practices
– Higher spending (Robinson and Miller, 2014, Baker et al., 2014b)
– Higher prices (Baker et al., 2014b, Capps et al., 2015)
– Changed referral patterns (Baker et al., 2015)
• To acquiring hospital
• More likely to go to high cost, low quality hospital
26

Evidence on Competition: US Insurer Prices
• Increased market concentration leads to substantial premium increases – Commercial, large group insurance market (Dafny et al. 2012)
• Increase in concentration led to 7% increase in premiums 1998-2006 • ~$34 billion per year; $200 per insured person
– Small group insurance market (Guardado et al. 2013) • Merger of United and Sierra in Nevada • 13.7% increase in premiums due to the merger
– Individual exchange market (Dafny et al. 2014) • Premiums would have decreased by 5.4% had United participated in the
exchanges • Exchange premiums would have been 11.1% lower if all insurers in a state
had participated
– Medicare Advantage bids (Song et al. 2012) • Each additional insurer in a market lowered bids by $1.28
• Changes in concentration are correlated with premium increases – Employer-sponsored, fully-insured (Trish and Herring 2015) – 3 to 4 merger leads to 4.67% increase in premiums(~$215)
27

Evidence on Competition: US Insurers
• Individual demand elasticity
– Initial choices responsive to premiums, plan features
– Lots of inertia thereafter
• Recent studies suggest high switching costs (Handel, 2010) or large preference heterogeneity (Carlin and Town, 2009); imply low demand elasticity
– Suggests market power
• Firm demand elasticity
– -7.9 (Dowd and Feldman, 1994)
– -4.57 (Atherly, 2004)
28

Evidence on Competition: Netherlands, Switzerland, Germany
• High degree of price dispersion in premiums, with little reduction over time
– Switzerland (Frank and Lamiraud, 2009)
– Netherlands (Bolhaar, Lindeboom, van der Klaauw, 2010)
– Suggests lack of competition
• Relatively little plan switching
– Less switching in markets with more plans (Frank and Lamiraud, 2009)
• Insurance firm’s demand elasticity – Netherlands: -0.10 to -0.38 (van Dijk et al, 2008)
– Netherlands: -0.41 (Schut et al, 2003)
– Germany: -3.45 (Schut et al, 2003)
– Germany: -0.45 short run, -12 long run (Tamm et al, 2007)
29

Evidence on Competition: Provider Quality
• Consolidation can lead to substantially lower quality – Medicare (administered prices)
– 1.46 percentage points higher mortality rate in most concentrated markets for Medicare heart attack patients (Kessler and McClellan, 2000)
– Higher mortality rates in more concentrated physician markets for Medicare PCI patients (Eisenberg, 2015)
• Consolidation can lead to lower quality –Private (market determined prices) [but some studies go the other way]
– Hospital merger (Evanston) had no effect on some quality indicators, harmed others (Romano and Balan, 2011)
– Hospital mergers in New York state had no impacts on many quality indicators, led to increases in mortality for AMI, heart failure patients (Capps, 2005)
– Removal of barriers to entry led to increased market shares for low mortality rate CABG surgeons in Pennsylvania (Cutler et al., 2010)
30

Evidence on Competition: Innovation
• Not much evidence on this for either providers or insurers
• One piece of evidence on insurers’ offerings of provider networks
– Primary innovation of late is narrow or “high performance” networks
• Data on physician network breadth provides glimpse into link between insurance competition and product variety
• Areas with more concentrated insurance markets have substantially less variation in the breadth of provider networks offered (Dafny and Ody, 2016)
31

Summary and Conclusions
• Competition in health care is a popular option for health reform
• How well does competition in health care work? – Provider price competition (US)
• Can work very well
• Doesn’t seem to compromise quality
• Access for the poor?
– Provider quality competition (US) • Works well where there are administered prices
• Less clear for market determined prices
• Limited measures of quality, types of services
– Insurer price competition (US, Germany, Netherlands, Switzerland) • More competition leads to lower premiums (US)
• Demand not highly elastic, may be inelastic (?)
• Incomplete, possibly inconsistent evidence
32

Summary and Conclusions
• Consolidation (US)
– Harmful when between close competitors
– Much higher prices
– Little evidence of countervailing benefits
– Strongest evidence for hospital prices
– Less evidence on physicians, insurers, quality
• Policy
– Competition can work
– Needs an accompanying public infrastructure • Support for choice, competition
• Vigilant antitrust/competition authority
• Other parts of government must facilitate, support entry and competition
– Health ministry,…
– Sometimes work at cross purposes to competition (e.g., consolidation, centralization)
33

END
34
Related Documents