Processing speed mediates the relationship between verbal memory, verbal fluency, and functional outcome in chronic schizophrenia Natalia Ojeda a,b, ⁎ , Javier Peña a , Pedro Sánchez b , Edorta Elizagárate b , Jesús Ezcurra b a Department of Psychology, University of Deusto, Avda. Universidades, 24. 48007 Bilbao, Spain b Refractory Psychosis Unit, Hospital Psiquiátrico de Alava, C/ Alava, 43. 01006 Vitoria, Spain Received 4 October 2007; received in revised form 18 December 2007; accepted 20 December 2007 Available online 8 February 2008 Abstract Verbal fluency and verbal memory have been reported to be diminished in patients with schizophrenia. These deficits could partially predict functional disability in this pathology. However, processing speed often mediates the relationship among cognitive processes in the disorder. Our goal was to analyse the influence of processing speed as mediator of the relation between verbal fluency–verbal memory and functional disability in chronic schizophrenia. We examined 90 hospitalized patients and 30 healthy controls (matched for gender, age and years of education). The neuropsychological battery included tests for verbal fluency, verbal memory, motor speed and processing speed. Outcome measures included Disability Assessment Schedule (DAS-WHO) and number of hospitalizations (NH). Results confirmed chronicity on clinical symptoms (PANSS total X = 48.94 + 14.97 PANSS negative X = 27.81 + 10.18, PANSS positive X = 23.51 + 10.81) and impairment on functional disability (DAS-WHO X = 13.62 + 4.28). As expected, verbal fluency was severely impaired in patients and significantly predicted functional outcome. Immediate and Delayed Verbal Memory were also severely impaired and predicted functional outcome. However, when processing speed was entered in the regression analyses the significance of verbal fluency and verbal memory decreased significantly. Sobel's equation was significant, suggesting full mediation. Our findings suggest that processing speed may be a central factor in the relation between cognitive symptoms and functional outcome in chronic schizophrenia. © 2008 Elsevier B.V. All rights reserved. Keywords: Chronic schizophrenia; Neurocognition; Functional disability; Verbal fluency; Verbal memory; Processing speed 1. Introduction The presence of cognitive deficits in schizophrenia has been extensively reported as a core feature of the disorder (Heinrichs and Zakzanis, 1998; Wilk et al., 2005), and the average impairment can reach 2 standard deviations below normal performance (Bilder et al., 2000; Harvey and Keefe, 1997). The suggested evidence of cognition as best predictor of functional outcomes and disability in schizophrenia including work functioning and independent living (Gold et al., 2002; Hofer et al., 2005) provided further relevance to the study of these deficits, specially after the published weak relation with clinical symptoms (Green, 1996). Green additionally characterized the association between specific neurocognitive domains and different measures Available online at www.sciencedirect.com Schizophrenia Research 101 (2008) 225 – 233 www.elsevier.com/locate/schres ⁎ Corresponding author. Department of Psychology, University of Deusto, Avda. Universidades, 24, 48007 Bilbao, Spain. Tel.: +34 94 413 90 00x2671; fax: +34 94 413 90 89. E-mail address: [email protected] (N. Ojeda). 0920-9964/$ - see front matter © 2008 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2007.12.483

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Available online at www.sciencedirect.com
01 (2008) 225–233www.elsevier.com/locate/schres
Schizophrenia Research 1
Processing speed mediates the relationship between verbal memory,verbal fluency, and functional outcome in chronic schizophrenia
Natalia Ojeda a,b,⁎, Javier Peña a, Pedro Sánchez b, Edorta Elizagárate b, Jesús Ezcurra b
a Department of Psychology, University of Deusto, Avda. Universidades, 24. 48007 Bilbao, Spainb Refractory Psychosis Unit, Hospital Psiquiátrico de Alava, C/ Alava, 43. 01006 Vitoria, Spain
Received 4 October 2007; received in revised form 18 December 2007; accepted 20 December 2007Available online 8 February 2008
Abstract
Verbal fluency and verbal memory have been reported to be diminished in patients with schizophrenia. These deficits couldpartially predict functional disability in this pathology. However, processing speed often mediates the relationship among cognitiveprocesses in the disorder. Our goal was to analyse the influence of processing speed as mediator of the relation between verbalfluency–verbal memory and functional disability in chronic schizophrenia. We examined 90 hospitalized patients and 30 healthycontrols (matched for gender, age and years of education). The neuropsychological battery included tests for verbal fluency, verbalmemory, motor speed and processing speed. Outcome measures included Disability Assessment Schedule (DAS-WHO) andnumber of hospitalizations (NH). Results confirmed chronicity on clinical symptoms (PANSS total X=48.94+14.97 PANSSnegative X=27.81+10.18, PANSS positive X=23.51+10.81) and impairment on functional disability (DAS-WHO X=13.62+4.28). As expected, verbal fluency was severely impaired in patients and significantly predicted functional outcome. Immediate andDelayed Verbal Memory were also severely impaired and predicted functional outcome. However, when processing speed wasentered in the regression analyses the significance of verbal fluency and verbal memory decreased significantly. Sobel's equationwas significant, suggesting full mediation. Our findings suggest that processing speed may be a central factor in the relationbetween cognitive symptoms and functional outcome in chronic schizophrenia.© 2008 Elsevier B.V. All rights reserved.
Keywords: Chronic schizophrenia; Neurocognition; Functional disability; Verbal fluency; Verbal memory; Processing speed
1. Introduction
The presence of cognitive deficits in schizophrenia hasbeen extensively reported as a core feature of the disorder(Heinrichs and Zakzanis, 1998; Wilk et al., 2005), and
⁎ Corresponding author. Department of Psychology, University ofDeusto, Avda. Universidades, 24, 48007 Bilbao, Spain. Tel.: +34 94413 90 00x2671; fax: +34 94 413 90 89.
E-mail address: [email protected] (N. Ojeda).
0920-9964/$ - see front matter © 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2007.12.483
the average impairment can reach 2 standard deviationsbelow normal performance (Bilder et al., 2000; Harveyand Keefe, 1997).
The suggested evidence of cognition as best predictorof functional outcomes and disability in schizophreniaincluding work functioning and independent living (Goldet al., 2002; Hofer et al., 2005) provided further relevanceto the study of these deficits, specially after the publishedweak relation with clinical symptoms (Green, 1996).Green additionally characterized the association betweenspecific neurocognitive domains and different measures

226 N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
of outcome: 1. verbal memory (VM) associated with alltypes of functional outcome, 2. vigilance related to socialproblem solving and skill acquisition, and 3. executivefunctioning with community functioning. Bowie andHarvey (2005) also found a positive relation amongneurocognitive domains and adaptive/social skills, sug-gesting that negative symptoms and neurocognitivedomains are distinct and have differential pathways ofchange with treatment.
Since Green's findings of verbal memory as related toall functional outcomes, the interest to analyse it deeplyhas increased. Several studies have shown that both verbalmemory (VM) and verbal fluency (VF), as well as theprocessing speed (PS), are related to different measures ofoutcome: Bryson and Bell (2003) found that VM wasassociated to the improvement in work performance,while clinical symptoms did not. Dickerson et al. (1999)found that VM, VF and performance on trail making testpredicted changes in social and community outcome.Gold et al. (2002) reported that semantic fluency, VM, andsome measures of processing speed (PS) (as TMT-A andStroop) predicted job tenure, but not fine motor speed(Purdue Pegboard). Jaeger et al. (2003) discovered thatVF, attention and VM predicted work, school, andindependent living, even after controlling for negativesymptoms. In a more specific analysis Velligan et al.(2000) replicated Green's finding on VM predicting allmeasures of community outcome, vigilance predictingsocial outcomes, and executive functioning predictingwork and activities of daily living (ADLs). Daily problemsolving skills have also been found to be dependent onVM abilities, VF, and processing speed (PS) both, in atesting setting (Keefe et al., 2006; Revheim et al., 2006) orin a real context (Rempfer et al., 2003). Furthermore,some authors concluded that PS is strongly related to VM(Brébion et al., 2006) and VF (Van Beilen et al., 2004) inchronic schizophrenia.
The strong role played by PS in relation to VF andVM has been previously addressed. However, none ofthese studies analysed profoundly this interactionrelated to functional outcome. Given the reportedrelevance of processing speed (PS), we hypothesizedPS to be a putative mediator between the verbal memory(VM), verbal fluency (VF) and functional disability(FD) in chronic schizophrenia. That is to say, theassociation among VM, VF, and functional outcomes(FO) could be (at least partially) attributed to themediation effect of PS. Therefore, we aim first, todescribe the role played by VM and VF, in FO inpatients with chronic schizophrenia. Secondly, analysethe possible interaction between PS and VM–VF as realpredictors of FO.
2. Materials and methods
2.1. Participants
90 hospitalized patients were recruited from AlavaPsychiatric Hospital (76 males, 14 females; years ofeducation=10.17+2.8), ranged in age from 18 to 65(age=36.09+10.68). Mean time of hospitalization forpatients was very variable on the sample (646.24+1648.72 days).
Subjects met diagnostic criteria for schizophreniaaccording to the American Psychiatric Association'sDiagnostic and Statistical Manual of Mental Disorders,fourth edition (DSM-IV) (APA, 1994) criteria, using theStructured Clinical Interview for DSM-IV (SCID-I). Attime of recruitment all were under antipsychotic medica-tion. Exclusion criteria included previous history of lackof consciousness (N1 h), mental retardation, relevantneurological condition including cerebrovascular disease,hypertension, and significant sensorial deficits.
All participants underwent a general medical evalua-tion, and cognitive assessment described below. Patientsadditionally completed psychiatric interview and psychia-tric evaluation including Positive and Negative SymptomScale (PANSS), Brief Psychiatric Rating Scale (BPRS),Calgary Depression Scale, and Young Mania Scale.
Thirty healthy comparison participants were recruitedand screened to rule out past or current history ofpsychiatric disorder, medical conditions relevant to centralnervous system, and significant sensorial deficits. The twogroups did not significantly differ on age (t=−0.64,p=0.53), gender distribution (χ2=3.03, p=0.08) or yearsof education (t=0.21,p=0.83).All subjectswere voluntaryand gave written informed consent form approved by theinstitutional review board to participate in the study.
2.2. Measures
2.2.1. Verbal memory testThe Spanish version of Logical Memory I and II
(WMS-III) was used (Wechsler, 1987). In this test, theexaminer reads two stories, stopping after each readingfor an immediate free recall. Then, after 20 min thesubject is asked to recall the two stories read before.Two measures are obtained: Immediate Verbal Memory(IVM) and Delayed Verbal Memory (DVM).
2.2.2. Verbal fluency from testBarcelona (Peña-Casanova, 1990); reliability (con-
current validity with ADAS (Alzheimer's DiseaseAssessment Scale) r=0.87, r2 =0.76; test–retest relia-bility: r=0.92, interrater r=0.99).

227N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
2.2.2.1. Phonological fluency (PF). In this test theparticipant is asked to say as many words as possiblebeginning with letter P in a 3-minute time limit, ex-cluding proper nouns and the same word with a differentsuffix. The total number of words generated was used asa measure.
2.2.2.2. Semantic fluency (SF). The participant isasked to say as many nouns of animals as possible withina 1-minute time limit. As for the phonological fluency, thetotal number of words generated was used as a measure.
2.2.3. Processing speed tests
2.2.3.1. Stroop color naming test (Golden, 1978).Only the color naming condition of the Stroop test wasconsidered. Patients were presented a sheet displayedwith blocks of color (red, blue, green), and required toname the color of each block, column by column, asquickly as they could in 45 s limit. The total number ofcolors named was recorded.
2.2.3.2. Digit symbol substitution test from the WAIS-R(Wechsler, 1981). Subjects were presented with rowsof empty boxes labeled by a digit. They were required tofill out these boxes one by one, as quickly as they couldwith a corresponding symbol, according to a digit/symbol code that was permanently displayed. The totalnumber of boxes accurately filled in within 120 s wasused as a measure.
2.2.3.3. Trail making test— part A (Reitan and Wolfson,1985). Subjects were presented with a sheet withnumbers from 1 to 25 that were randomly displayed.They were required to draw a line between the numbersin ascending order as quickly as they could. The time inseconds for completion was recorded.
These three processing speed measures were con-verted into z-scores, and the sign of TMT-A wasadjusted so that higher score indicated better neuro-cognitive performance. Then, they were averaged tocreate a global measure of processing speed (PS) assuggested by Brébion et al. (2006). The internalconsistency of this scale was very high (Cronbach'salpha=0.95).
2.2.4. Fine motor speed
2.2.4.1. Grooved Pegboard Test (Mathews and Klove,1964). It contains 25 grooved holes and a set ofgrooved pegs. The holes are randomly positioned, andthe pegs must be rotated till they match the shape of the
hole and slot in. The time in seconds for completion wasrecorded.
2.2.4.2. Functional disability was assessed using theDisability Assessment Schedule (DAS-WHO; WHO,1988). The total number of hospitalizations since thefirst episode was added as measure of outcome, as inprevious literature (Fujii and Wylie, 2002).
2.3. Data analyses
Data were examined for normal distributions withKolmogorov–Smirnov Test and only TMT-A did notconform to the assumption of normality. It was normal-ized by log-transformation to reduce the influence ofoutliers. χ2 test was used to analyse any differencebetween the groups for gender and t-tests for age andyears of education. Multivariate analysis of variance(MANOVA) was used as the primary test of groupdifferences, with group as a between-subjects factor andneuropsychological scales as dependent variables.
To test the hypothesis that PS mediates the effect ofpredictor variables (VF and VM) on the FO, wefollowed previously published and recommended cri-teria (Baron and Kenny, 1986; Frazier et al., 2004). In afirst step, the predictors (VF and VM) must besignificantly associated with FO. In the second step,VF and VM must be significantly associated with thepotential mediating variable, in our case, PS. In the thirdstep, the mediator (PS) must be related to the outcomevariable (FO). The final step is to show that the strengthof the relation between the predictor and the outcome issignificantly reduced when the mediator is added to themodel. If perfect mediation is obtained, the VF and VMeffect will become zero, showing that PS fully mediatesthe relation. If the path between the predictors (VF andVM) and functional disability remains significant, itsuggests that PS variable is partial mediator. Separateanalyses were performed with semantic fluency, pho-nemic fluency, Immediate Verbal Memory and DelayedVerbal Memory as predictor variables. Significancelevel was set at 0.05. All tests were two-tailed.
3. Results
3.1. Differences between schizophrenic patients andnormal control group
Demographic and clinical characteristics of the sampleare described in Table 1. As expected, we found sta-tistically significant differences between the two groupsin all cognitive measures. Patients displayed worse
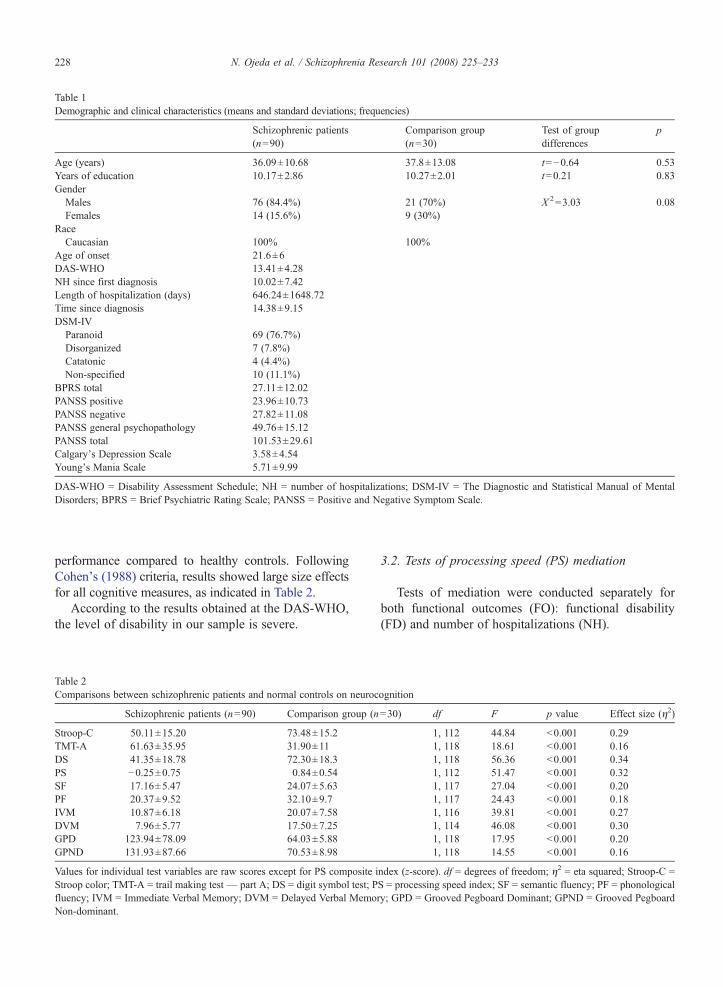
Table 1Demographic and clinical characteristics (means and standard deviations; frequencies)
Schizophrenic patients(n=90)
Comparison group(n=30)
Test of groupdifferences
p
Age (years) 36.09±10.68 37.8±13.08 t=−0.64 0.53Years of education 10.17±2.86 10.27±2.01 t=0.21 0.83GenderMales 76 (84.4%) 21 (70%) Χ 2=3.03 0.08Females 14 (15.6%) 9 (30%)
RaceCaucasian 100% 100%
Age of onset 21.6±6DAS-WHO 13.41±4.28NH since first diagnosis 10.02±7.42Length of hospitalization (days) 646.24±1648.72Time since diagnosis 14.38±9.15DSM-IVParanoid 69 (76.7%)Disorganized 7 (7.8%)Catatonic 4 (4.4%)Non-specified 10 (11.1%)
BPRS total 27.11±12.02PANSS positive 23.96±10.73PANSS negative 27.82±11.08PANSS general psychopathology 49.76±15.12PANSS total 101.53±29.61Calgary's Depression Scale 3.58±4.54Young's Mania Scale 5.71±9.99
DAS-WHO = Disability Assessment Schedule; NH = number of hospitalizations; DSM-IV = The Diagnostic and Statistical Manual of MentalDisorders; BPRS = Brief Psychiatric Rating Scale; PANSS = Positive and Negative Symptom Scale.
228 N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
performance compared to healthy controls. FollowingCohen's (1988) criteria, results showed large size effectsfor all cognitive measures, as indicated in Table 2.
According to the results obtained at the DAS-WHO,the level of disability in our sample is severe.
Table 2Comparisons between schizophrenic patients and normal controls on neuroc
Schizophrenic patients (n=90) Comparison group (n
Stroop-C 50.11±15.20 73.48±15.2TMT-A 61.63±35.95 31.90±11DS 41.35±18.78 72.30±18.3PS −0.25±0.75 0.84±0.54SF 17.16±5.47 24.07±5.63PF 20.37±9.52 32.10±9.7IVM 10.87±6.18 20.07±7.58DVM 7.96±5.77 17.50±7.25GPD 123.94±78.09 64.03±5.88GPND 131.93±87.66 70.53±8.98
Values for individual test variables are raw scores except for PS composite iStroop color; TMT-A = trail making test— part A; DS = digit symbol test; Pfluency; IVM = Immediate Verbal Memory; DVM = Delayed Verbal MemoNon-dominant.
3.2. Tests of processing speed (PS) mediation
Tests of mediation were conducted separately forboth functional outcomes (FO): functional disability(FD) and number of hospitalizations (NH).
ognition
=30) df F p value Effect size (η2)
1, 112 44.84 b0.001 0.291, 118 18.61 b0.001 0.161, 118 56.36 b0.001 0.341, 112 51.47 b0.001 0.321, 117 27.04 b0.001 0.201, 117 24.43 b0.001 0.181, 116 39.81 b0.001 0.271, 114 46.08 b0.001 0.301, 118 17.95 b0.001 0.201, 118 14.55 b0.001 0.16
ndex (z-score). df = degrees of freedom; η2 = eta squared; Stroop-C =S = processing speed index; SF = semantic fluency; PF = phonologicalry; GPD = Grooved Pegboard Dominant; GPND = Grooved Pegboard
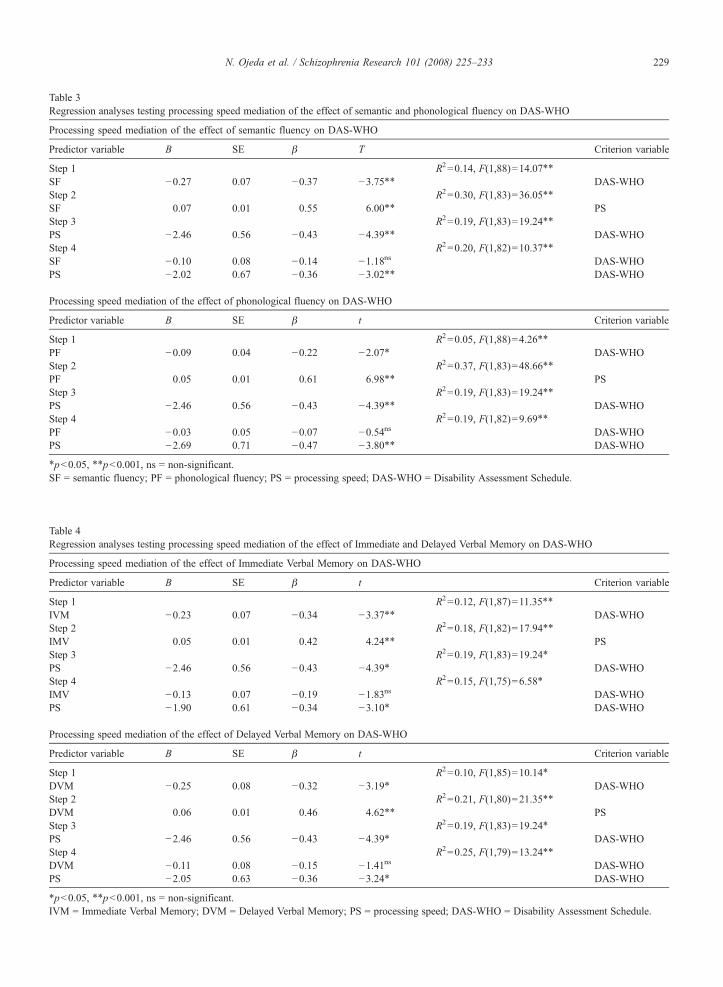
Table 3Regression analyses testing processing speed mediation of the effect of semantic and phonological fluency on DAS-WHO
Processing speed mediation of the effect of semantic fluency on DAS-WHO
Predictor variable B SE β T Criterion variable
Step 1 R2=0.14, F(1,88)=14.07⁎⁎
SF −0.27 0.07 −0.37 −3.75⁎⁎ DAS-WHOStep 2 R2=0.30, F(1,83)=36.05⁎⁎
SF 0.07 0.01 0.55 6.00⁎⁎ PSStep 3 R2=0.19, F(1,83)=19.24⁎⁎
PS −2.46 0.56 −0.43 −4.39⁎⁎ DAS-WHOStep 4 R2=0.20, F(1,82)=10.37⁎⁎
SF −0.10 0.08 −0.14 −1.18ns DAS-WHOPS −2.02 0.67 −0.36 −3.02⁎⁎ DAS-WHO
Processing speed mediation of the effect of phonological fluency on DAS-WHO
Predictor variable B SE β t Criterion variable
Step 1 R2=0.05, F(1,88)=4.26⁎⁎
PF −0.09 0.04 −0.22 −2.07⁎ DAS-WHOStep 2 R2=0.37, F(1,83)=48.66⁎⁎
PF 0.05 0.01 0.61 6.98⁎⁎ PSStep 3 R2=0.19, F(1,83)=19.24⁎⁎
PS −2.46 0.56 −0.43 −4.39⁎⁎ DAS-WHOStep 4 R2=0.19, F(1,82)=9.69⁎⁎
PF −0.03 0.05 −0.07 −0.54ns DAS-WHOPS −2.69 0.71 −0.47 −3.80⁎⁎ DAS-WHO
⁎pb0.05, ⁎⁎pb0.001, ns = non-significant.SF = semantic fluency; PF = phonological fluency; PS = processing speed; DAS-WHO = Disability Assessment Schedule.
Table 4Regression analyses testing processing speed mediation of the effect of Immediate and Delayed Verbal Memory on DAS-WHO
Processing speed mediation of the effect of Immediate Verbal Memory on DAS-WHO
Predictor variable B SE β t Criterion variable
Step 1 R2=0.12, F(1,87)=11.35⁎⁎
IVM −0.23 0.07 −0.34 −3.37⁎⁎ DAS-WHOStep 2 R2=0.18, F(1,82)=17.94⁎⁎
IMV 0.05 0.01 0.42 4.24⁎⁎ PSStep 3 R2=0.19, F(1,83)=19.24⁎
PS −2.46 0.56 −0.43 −4.39⁎ DAS-WHOStep 4 R2=0.15, F(1,75)=6.58⁎
IMV −0.13 0.07 −0.19 −1.83ns DAS-WHOPS −1.90 0.61 −0.34 −3.10⁎ DAS-WHO
Processing speed mediation of the effect of Delayed Verbal Memory on DAS-WHO
Predictor variable B SE β t Criterion variable
Step 1 R2=0.10, F(1,85)=10.14⁎
DVM −0.25 0.08 −0.32 −3.19⁎ DAS-WHOStep 2 R2=0.21, F(1,80)=21.35⁎⁎
DVM 0.06 0.01 0.46 4.62⁎⁎ PSStep 3 R2=0.19, F(1,83)=19.24⁎
PS −2.46 0.56 −0.43 −4.39⁎ DAS-WHOStep 4 R2=0.25, F(1,79)=13.24⁎⁎
DVM −0.11 0.08 −0.15 −1.41ns DAS-WHOPS −2.05 0.63 −0.36 −3.24⁎ DAS-WHO
*pb0.05, ⁎⁎pb0.001, ns = non-significant.IVM = Immediate Verbal Memory; DVM = Delayed Verbal Memory; PS = processing speed; DAS-WHO = Disability Assessment Schedule.
229N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
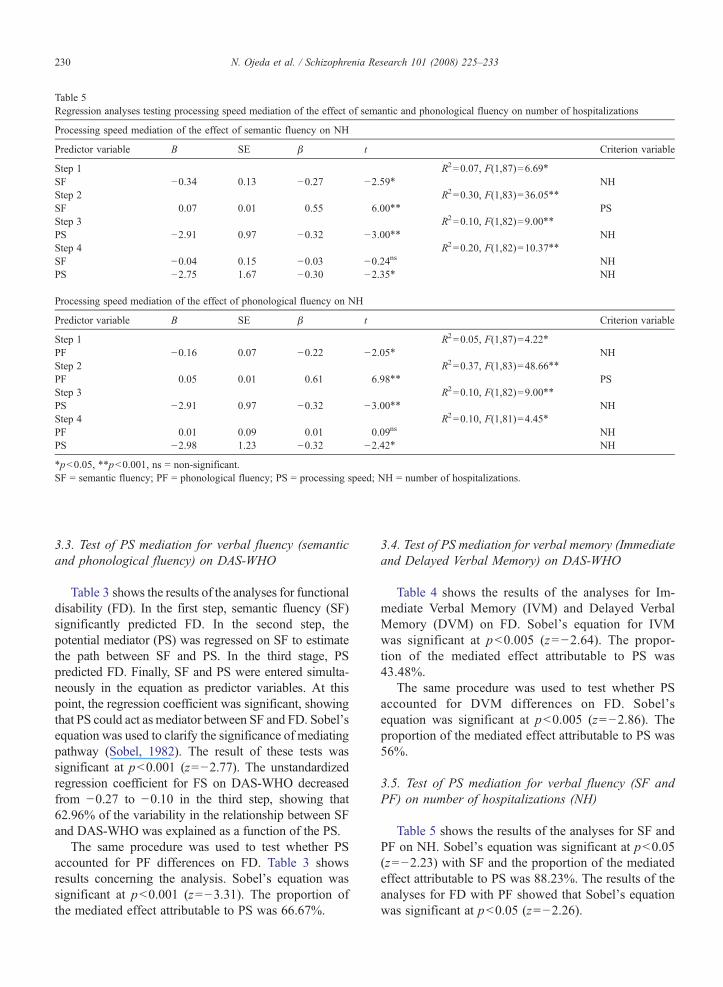
Table 5Regression analyses testing processing speed mediation of the effect of semantic and phonological fluency on number of hospitalizations
Processing speed mediation of the effect of semantic fluency on NH
Predictor variable B SE β t Criterion variable
Step 1 R2=0.07, F(1,87)=6.69⁎
SF −0.34 0.13 −0.27 −2.59⁎ NHStep 2 R2=0.30, F(1,83)=36.05⁎⁎
SF 0.07 0.01 0.55 6.00⁎⁎ PSStep 3 R2=0.10, F(1,82)=9.00⁎⁎
PS −2.91 0.97 −0.32 −3.00⁎⁎ NHStep 4 R2=0.20, F(1,82)=10.37⁎⁎
SF −0.04 0.15 −0.03 −0.24ns NHPS −2.75 1.67 −0.30 −2.35⁎ NH
Processing speed mediation of the effect of phonological fluency on NH
Predictor variable B SE β t Criterion variable
Step 1 R2=0.05, F(1,87)=4.22⁎
PF −0.16 0.07 −0.22 −2.05⁎ NHStep 2 R2=0.37, F(1,83)=48.66⁎⁎
PF 0.05 0.01 0.61 6.98⁎⁎ PSStep 3 R2=0.10, F(1,82)=9.00⁎⁎
PS −2.91 0.97 −0.32 −3.00⁎⁎ NHStep 4 R2=0.10, F(1,81)=4.45⁎
PF 0.01 0.09 0.01 0.09ns NHPS −2.98 1.23 −0.32 −2.42⁎ NH
*pb0.05, **pb0.001, ns = non-significant.SF = semantic fluency; PF = phonological fluency; PS = processing speed; NH = number of hospitalizations.
230 N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
3.3. Test of PS mediation for verbal fluency (semanticand phonological fluency) on DAS-WHO
Table 3 shows the results of the analyses for functionaldisability (FD). In the first step, semantic fluency (SF)significantly predicted FD. In the second step, thepotential mediator (PS) was regressed on SF to estimatethe path between SF and PS. In the third stage, PSpredicted FD. Finally, SF and PS were entered simulta-neously in the equation as predictor variables. At thispoint, the regression coefficient was significant, showingthat PS could act as mediator between SF and FD. Sobel'sequation was used to clarify the significance of mediatingpathway (Sobel, 1982). The result of these tests wassignificant at pb0.001 (z=−2.77). The unstandardizedregression coefficient for FS on DAS-WHO decreasedfrom −0.27 to −0.10 in the third step, showing that62.96% of the variability in the relationship between SFand DAS-WHO was explained as a function of the PS.
The same procedure was used to test whether PSaccounted for PF differences on FD. Table 3 showsresults concerning the analysis. Sobel's equation wassignificant at pb0.001 (z=−3.31). The proportion ofthe mediated effect attributable to PS was 66.67%.
3.4. Test of PS mediation for verbal memory (Immediateand Delayed Verbal Memory) on DAS-WHO
Table 4 shows the results of the analyses for Im-mediate Verbal Memory (IVM) and Delayed VerbalMemory (DVM) on FD. Sobel's equation for IVMwas significant at pb0.005 (z=−2.64). The propor-tion of the mediated effect attributable to PS was43.48%.
The same procedure was used to test whether PSaccounted for DVM differences on FD. Sobel'sequation was significant at pb0.005 (z=−2.86). Theproportion of the mediated effect attributable to PS was56%.
3.5. Test of PS mediation for verbal fluency (SF andPF) on number of hospitalizations (NH)
Table 5 shows the results of the analyses for SF andPF on NH. Sobel's equation was significant at pb0.05(z=−2.23) with SF and the proportion of the mediatedeffect attributable to PS was 88.23%. The results of theanalyses for FD with PF showed that Sobel's equationwas significant at pb0.05 (z=−2.26).

231N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
3.6. Test of PS mediation for verbal memory (Immediateand Delayed Verbal Memory) on NH
The same procedure was used to test whether PSaccounted for IVM and DVM differences on NH. In thisparticular analysis, IVM did not show a significantassociation with NH measure (r=−0.08ns) so furthermediation analysis was not possible. As with IVM,DVM did not show a significant association with NHmeasure (r=−0.16ns).
3.7. Test of motor speed (MS) mediation
Not surprisingly, MS did not correlate with outcomemeasures (DAS-WHO and NH). Thus, mediationanalyses were not possible. Only Grooved PegboardDominant Hand (GPD) correlated with NH (r=0.29⁎),but Sobel's equation was not significant for GPDmediation.
4. Discussion
As expected, our patients were impaired on allcognitive measures, including VF, VM, PS and MSwhen compared to normal controls, showing largeeffect sizes (Cohen, 1988). PS index was the moreseverely impaired cognitive domain. Results obtainedin this study confirmed the initial hypothesis: PS actsas a pathway through which VM and VF are asso-ciated with FO, as measured by the DAS-WHO ornumber of hospitalizations. The portion of the me-diated effect attributable to PS ranged between 43.48%and 66.67% (for verbal memory and verbal fluencyrespectively).
Regarding verbal memory, our results are compatiblewith Holthausen et al. (2003) who reported that bothprocessing speed and semantic organization wererelated to verbal memory efficiency in schizophrenia.One additional contribution of our study was that thepredictive value of PS was fairly constant across bothimmediate recall and long term recall, suggesting thatprocessing speed was pervasively related to memory allalong the recall temporal processing.
Our findings are consistent with McClure et al.(2007), Van Beilen et al. (2004), and Henry andCrawford (2005), who concluded that decreased PSwas related to impaired fluency performance in patientswith schizophrenia, but not in normal comparison group.Furthermore, once the role of speed is considered, verbalfluency has a non-significant role as predictor offunctional outcome in schizophrenia. This major findingadds the need of revision of previous studies which
concluded that VF has predictive value on functionaloutcome, but did not include the revision of PS onthe analysis (Zanello et al., 2006; Laes and Sponheim,2006).
Contrary to Bokat and Goldberg (2003), our datasuggest that both, semantic fluency (SF) and phoneticfluency (PF), are similarly impaired in chronic schizo-phrenia. Bokat and Goldberg (2003) found a greaterdeficit in SF vs PF in schizophrenia that could probablysuggest that the integrity of the semantic store wasspecifically compromised. This conclusion was repli-cated in a posterior meta-analysis with 84 studies usingthe English FAS version (Henry and Crawford, 2005).Part of the disparity could be explained by thedifferences between the FAS English version (1 minper task) and the Spanish version, which in thephonological fluency subtest asks the patient to producewords during 3 min. This cognitive demand on longertime would emphasize the deficit in the phonologicalfluency in schizophrenia. Also, this variation preventsfrom the direct comparison between raw scores on thetwo test versions.
Apart from this particular subtest, the cognitivemeasures employed in this study for verbal fluency,verbal memory, and processing speed are among thestandard measures included in this type of studies. Someauthors have suggested that particular subtests includedin the PS index could have a specific role in the PS indexas predictor of the different variables analysed (Brébionet al., 2006). Although a particular subtest could mainlycontribute to the predicting value in a particular study,the relation between PS and FO has been replicated withalmost all standard cognitive measures of PS (Bowieet al., in press; Gold et al., 2002; McClure et al., 2007).Negative or non-significant results have been associatedto the use of motor speed subtests (instead of non-motorspeed tests) in the same direction as our data (Brébionet al., 2006) with few exceptions (as Van Beilen et al.,2004). Although Van Beilen et al. (2004) concluded thatmotor speed significantly predict VF in schizophrenia,deeper review of their MS index shows that the only twosubtests included (Stroop and TMT-A), are frequentlyused as PS measures. Consistent with previous studies(Gold et al., 2002; Revheim et al., 2006), our dataconfirmed that all types of speed do not contributeequally. It is PS, and not motor speed (as measured byGrooved Pegboard), that acts as mediator and predictorof FO. Despite the strong impairment observed in motorspeed in our patient sample, MS does not mediate therelation between VF–VM and FO significantly. Ouradvantage is that, to the best of our knowledge, this is thefirst study which includes MS, SP, FO, and additional
232 N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
cognitive measures, to specify the role of each group ofvariables in the model. Studies that employmainly motorspeed tasks may therefore underestimate the role ofcognitive slowness in cognition in schizophrenia.
These findings also emphasize the relevance of themeasures employed for both, processing speed andfunctional outcome. When number of hospitalizations(NH) was considered as a measure of outcome, ourresults were consistent with previous findings (Fujii andWylie, 2002) where both SF and PF, but not VM (eitherIVM or DVM), predicted FO. As VM has been found bypast studies (since Green, 1996) to be significantlyrelated to specific measures of outcome different fromDAS-WHO, future studies should review the utility ofNH as unique measure of FO.
It could be criticized that the predictive effect variesaccording to the severity of the illness, as our data isbased on chronic patients with long time of hospitaliza-tion. Actually, McClure et al. (2007) and Gold et al.(2002) found similar results with samples of ambulatory(vs hospitalized) older and chronic patients withschizophrenia. A pending issue for the future wouldbe to analyse this relationship in studies with firstepisode psychosis (FEP) samples. Keshavan et al.(2003) and Malla et al. (2002) found in FEP a significantrelationship between cognition (including VF) and FObut did not include PS measures.
Despite these interesting findings, there are somelimitations in our study. First, a common limitation tothese type of studies: the tasks used as measures of speedof processing are only approximations of specific func-tions, rather than accurate measures. A second limitationis due to the cross-sectional nature of the study, so find-ings only indicate that cognitive and outcome variablesare statistically associated. Longitudinal data with firstepisode samples should be obtained to demonstrate if thispredictive role is confirmed on the changes on timeleading to specific impaired functional outcome.
Our data have shown that processing speed, and notmotor speed, is a strong predictor of functional outcomein patients with schizophrenia, despite their verbalabilities (Green et al., 2000). Taking back Green's dataand results published in the early 2000 in literaturewhich emphasized the role of VM in FOs, our resultssuggest that processing speed is the key variable whichmediates that relationship. As limitations are founddepending on the specific measures employed, futurelongitudinal studies should be performed to issue if PSequally predicts specific FO measures, such as commu-nity functioning, independent living, work performance,social problem solving or activities of daily living inchronic schizophrenia.
Role of funding sourceFunding for this study was provided by Basque Government Grant,
Department of Education; the Basque Government had no further rolein study design; in the collection, analysis and interpretation of data; inthe writing of the report; and in the decision to submit the paper forpublication.
ContributorsOjeda designed the study and wrote the protocol. Elizagarate
managed the literature searches and analyses. Ezcurra and Sanchezundertook the statistical analysis, and Peña wrote the first draft of themanuscript. All authors contributed to and have approved the finalmanuscript.
Conflict of interestAuthors declare that do not have and do not anticipate having any
conflict of interests, or competing financial interests.
AcknowledgementsThis research was partially supported by Basque Government
Department of Education, Universities and Research, Grant NumberBFI05.456 to J. Peña. Authors thank Dr. AB Yoller, who kindlyprovided data necessary for the analysis.
References
American Psychiatric Association, 1994. Diagnostic and StatisticalManual of Mental Disorders, fourth ed. APA, Washington, DC.
Baron, R.M., Kenny, D.A., 1986. The moderator–mediator variabledistinction in social psychological research: conceptual, strate-gic, and statistical considerations. J. Pers. Soc. Psychol. 51,1173–1182.
Bilder, R.M., Goldman, R.S., Robinson, D., Reiter, G., Bell, L., Bates,J.A., Pappadopoulos, E.,Willson, D.F., Alvir, J.M.,Woerner,M.G.,Geisler, S., Kane, J.M., Lieberman, J.A., 2000. Neuropsychologyof first-episode schizophrenia: initial characterization and clinicalcorrelates. Am. J. Psychiatry 157, 549–559.
Bokat, C.E., Goldberg, T.E., 2003. Letter and category fluency inschizophrenic patients: a meta-analysis. Schizophr. Res. 64, 73–78.
Bowie, C.R., Harvey, P.D., 2005. Cognition in schizophrenia:impairments, determinants, and functional importance. Psychiatr.Clin. North Am. 28, 613–633.
Bowie, C.R., Leung, W.W., Reichenberg, A., McClure, M.M.,Patterson, T.L., Heaton, R.K., Harvey, P.D., 2007. Predictingschizophrenia patients' real-world behavior with specific neurop-sychological and functional capacity measures. Biol. Psychiatry25.
Brébion, G., David, A.S., Bressan, R.A., Pilowsky, L.S., 2006.Processing speed: a strong predictor of verbal memory perfor-mance in schizophrenia. J. Clin. Exp. Neuropsychol. 28, 370–382.
Bryson, G., Bell, M.D., 2003. Initial and final work performance inschizophrenia: cognitive and symptompredictors. J. Nerv.Ment. Dis.191, 87–92.
Cohen, J., 1988. Statistical PowerAnalysis for the Behavioral Sciences,second ed. Erlbaum, Hillsdale, N. J.
Dickerson, F., Boronow, J.J., Ringel, N., Parente, F., 1999. Socialfunctioning and neurocognitive deficits in outpatients withschizophrenia: a 2-year follow-up. Schizophr. Res. 37, 13–20.
233N. Ojeda et al. / Schizophrenia Research 101 (2008) 225–233
Frazier, P.A., Tix, A.P., Barron, K.E., 2004. Testing moderator andmediator effects in counseling psychology research. J. Couns.Psychol. 51, 115–134.
Fujii, D.E., Wylie, A.M., 2002. Neurocognition and community out-come in schizophrenia: long-term predictive validity. Schizophr.Res. 59, 219–223.
Gold, J.M., Goldberg, R.W., McNary, S.W., Dixon, L.B., Lehman, A.F.,2002. Cognitive correlates of job tenure among patients with severemental illness. Am. J. Psychiatry 159, 1395–1402.
Golden, C.J., 1978. Stroop color and word test: a manual for clinicaland experimental uses. Stoelting Co, Chicago.
Green, M.F., 1996. What are the functional consequences of neurocog-nitive deficits in schizophrenia? Am. J. Psychiatry 153, 321–330.
Green, M.F., Kern, R.S., Braff, D.L., Mintz, J., 2000. Neurocognitivedeficits and functional outcome in schizophrenia: are wemeasuring the “right stuff”? Schizophr. Bull. 26, 119–136.
Harvey, P.D., Keefe, R.S.E., 1997. Cognitive impairment in schizo-phrenia and implications of atypical neuroleptic treatment. C.N.S.Spectr. 2, 1–11.
Heinrichs, R.W., Zakzanis, K.K., 1998. Neurocognitive deficit inschizophrenia: a quantitative review of the evidence. Neuropsy-chology 12, 426–445.
Henry, J.D., Crawford, J.R., 2005. A meta-analytic review of verbalfluency deficits in schizophrenia relative to other neurocognitivedeficits. Cogn. Neuropsychiatry 10, 1–33.
Hofer, A., Baumgartner, S., Bodner, T., Edlinger, M., Hummer, M.,Kemmler, G., Rettenbacher, M.A., Fleischhacker, W.W., 2005.Patient outcomes in schizophrenia II: the impact of cognition. Eur.Psychiat. 20, 395–402.
Holthausen, E.A., Wiersma, D., Sitskoorn, M.M., Dingemans, P.M.,Schene, A.H., Van den Bosch, R.J., 2003. Long-term memorydeficits in schizophrenia: primary or secondary dysfunction?Neuropsychology 17, 539–547.
Jaeger, J., Czobor, P., Berns, S.M., 2003. Basic neuropsychologicaldimensions in schizophrenia. Schizophr. Res. 65, 105–116.
Keefe, R.S., Bilder, R.M., Harvey, P.D., Davis, S.M., Palmer, B.W.,Gold, J.M., Meltzer, H.Y., Green, M.F., Miller del, D., Canive, J.M.,Adler, L.W., Manschreck, T.C., Swartz, M., Rosenheck, R., Perkins,D.O., Walker, T.M., Stroup, T.S., McEvoy, J.P., Lieberman, J.A.,2006. Baseline neurocognitive deficits in the CATIE schizophreniatrial. Neuropsychopharmacology 31, 2033–2046.
Keshavan, M.S., Haas, G., Miewald, J., Montrose, D.M., Reddy, R.,Schooler, N.R., Sweeney, J.A., 2003. Prolonged untreated illnessduration from prodromal onset predicts outcome in first episodepsychoses. Schizophr. Bull. 29, 757–769.
Laes, J.R., Sponheim, R.S., 2006. Does cognition predict communityfunction only in schizophrenia?: a study of schizophrenia patients,
bipolar affective disorder patients, and community controlsubjects. Schizophr. Res. 84, 121–131.
Malla, A.K., Norman, R.M.G., Manchanda, R., Towsend, L., 2002.Symptoms, cognition, treatment adherence and functional outcomein first-episode psychosis. Psychol. Med. 32, 1109–1119.
Mathews, C.G., Klove, N., 1964. Instruction Manual for the AdultNeuropsychological Test Battery. University of Madison MedicalSchool, Madison.
McClure, M.M., Bowie, C.R., Patterson, T.L., Heaton, R.K., Weaver,C., Anderson, H., Harvey, P.D., 2007. Correlations of functionalcapacity and neuropsychological performance in older patientswith schizophrenia: evidence for specificity of relationships?Schizophr. Res. 89, 330–338.
Peña-Casanova, J., 1990. Programa integrado de exploración neurop-sicológica. Manual, Barcelona, Masson.
Reitan, R., Wolfson, D., 1985. The Haldstead–Reitan Neuropsycho-logical Test Battery. Neuropsychology Press, Tucson.
Rempfer, M.V., Hamera, E.K., Brown, C.E., Cromwell, R.L., 2003.The relations between cognition and the independent living skillof shopping in people with schizophrenia. Psychiatry Res. 117,103–112.
Revheim, N., Schechter, I., Kim, D., Silipo, G., Alligham, B., Butler,P., Javitt, D.C., 2006. Neurocognitive and symptom correlates ofdaily problem-solving skills in schizophrenia. Schizophr. Res. 83,237–245.
Sobel, M.E., 1982. Asymptotic confidence intervals for indirect effectsin structural equation models. In: Leinhart, S. (Ed.), SociologicalMethodology. Jossey-Bass, San Francisco, pp. 290–312.
Van Beilen, M., Pijnenborg, M., Van Zomeren, E.H., Van den bosch,R.J., Withaar, F.K., Bruma, A., 2004. What is measured by verbalfluency tests in schizophrenia? Schizophr. Res. 69, 267–276.
Velligan, D.I., Bow-Thomas, C.C., Mahurin, R.K., Miller, A.L.,Halgunseth, L.C., 2000. Do specific neurocognitive deficits predictspecific domains of community function in schizophrenia? J. Nerv.Ment. Dis. 188, 518–524.
Wechsler, D., 1981. Wechsler Adult Intelligence Scale Revised.Psychological Corporation, San Antonio.
Wechsler, D., 1987. WMS-R:Wechsler Memory Scale Revised. ThePsychological Corporation, New York.
Wilk, C.M.,Gold, J.M.,McMahon,R.P., Iannone, V.N.,Buchanan,R.W.,2005. No, it is not possible to be schizophrenic yet neuropsycholo-gically normal. Neuropsychology 19, 778–786.
World Health Organization, 1988. Disability Assessment Schedule.WHO, Geneva.
Zanello, A., Perrig, L., Huguelet, P., 2006. Cognitive functions relatedto interpersonal problem-solving skills in schizophrenic patientscompared with healthy subjects. Psychiat. Res. 142, 67–78.
Related Documents











