Procalcitonin as an early indicator of outcome in sepsis: a prospective observational study E.J. Giamarellos-Bourboulis a, * , I. Tsangaris b , Th. Kanni a , M. Mouktaroudi a , I. Pantelidou a , G. Adamis c , S. Atmatzidis d , M. Chrisofos e , V. Evangelopoulou f , F. Frantzeskaki b , P. Giannopoulos g , G. Giannikopoulos h , D. Gialvalis i , G.M. Gourgoulis a , K. Kotzampassi j , K. Katsifa k , G. Kofinas l , F. Kontopidou a , G. Koratzanis m , V. Koulouras n , A. Koutsikou o , M. Koupetori p , I. Kritselis q , L. Leonidou r , A. Mega s , V. Mylona m , H. Nikolaou t , S. Orfanos b , P. Panagopoulos a , E. Paramythiotou b , A. Papadopoulos a , X. Papanikolaou l , M. Pavlaki u , V. Polychronopoulos v , A. Skoutelis w , A. Theodotou x , M. Vassiliaghou y , E.E. Douzinas z , C. Gogos r , A. Armaganidis b on behalf of the Hellenic Sepsis Study Group a 4th Department of Internal Medicine, University of Athens, Medical School, Athens, Greece b 2nd Department of Critical Care, University of Athens, Medical School, Athens, Greece c 1st Department of Internal Medicine, ‘G. Gennimatas’ Athens Hospital, Athens, Greece d 2nd Department of Surgery, University of Thessaloniki, Medical School, Thessaloniki, Greece e 2nd Department of Urology, ‘Sismanogleion’ Athens Hospital, Athens, Greece f Intensive Care Unit, ‘Korgialeneion-Benakeion’ Hospital of Athens, Athens, Greece g 1st Department Propedeutic Surgery, University of Athens, Medical School, Athens, Greece h Department of Internal Medicine, Chios General Hospital, Chios, Greece i 2nd Department of Surgery, ‘Evangelismos’ Athens General Hospital, Athens, Greece j 1st Department Prop. Surgery, University of Thessaloniki, Medical School Thessaloniki, Greece k Intensive Care Unit, ‘Tzaneion’ Hospital of Piraeus, Piraeus, Greece l Intensive Care Unit, ‘Hippokrateion’ Athens General Hospital, Athens, Greece m 2nd Department of Internal Medicine, ‘Sismanogleion’ Athens Hospital, Athens, Greece n Department of Critical Care, University of Ioannina Medical School, Ioannina, Greece o Intensive Care Unit, ‘Thriassio’ Elefsina General Hospital, Elefsina, Greece p 1st Department of Internal Medicine, ‘Thriassio’ Elefsina General Hospital, Elefsina, Greece q Department of Surgery, Nafplion General Hospital, Nafplion, Greece r 1st Department of Internal Medicine, University of Patras, Medical School, Patras, Greece s Intensive Care Unit, ‘Laikon’ Athens General Hospital, Athens, Greece t Intensive Care Unit, ‘Aghia Olga’ Athens General Hospital, Athens, Greece u Department of Internal Medicine, Argos General Hospital, Argos, Greece v 3rd Department of Pulmonary Medicine, ‘Sismanoglion’ Athens Hospital, Athens, Greece w 5th Department of Internal Medicine, ‘Evangelismos’ Athens Hospital, Athens, Greece x Intensive Care Unit, Karditsa General Hospital, Karditsa, Greece y Intensive Care Unit, ‘G. Gennimatas’ Thessaloniki General Hospital, Thessaloniki, Greece z 3rd Department of Critical Care, University of Athens, Medical School, Athens, Greece article info Article history: Received 11 November 2009 Accepted 30 July 2010 Available online 4 December 2010 Keywords: Procalcitonin Prognosis Sepsis summary This study explores the role of procalcitonin (PCT) in predicting the outcome of sepsis. In a prospective multicentre observational investigation, blood was sampled within 24 h of onset of sepsis in 1156 hospitalised patients; 234 were in the intensive care unit (ICU) at the point of presentation of sepsis while 922 were not. PCT was estimated in serum by the ultrasensitive Kryptor assay in a double-blinded fashion. Among patients outside the ICU, mortality was 8% in those with PCT 0.12 ng/mL but 19.9% in those with PCT >0.12 ng/mL [P < 0.0001, odds ratio (OR) for death: 2.606; 95% confidence interval (CI): 1.553e4.371]. Among patients whose * Corresponding author. Address: 4th Department of Internal Medicine, ATTIKON University General Hospital, 124 62 Athens, Greece. Tel.: þ30 210 58 31 994; fax: þ30 210 53 26 446. E-mail address: [email protected] (E.J. Giamarellos-Bourboulis). Available online at www.sciencedirect.com Journal of Hospital Infection journal homepage: www.elsevierhealth.com/journals/jhin 0195-6701/$ e see front matter Ó 2010 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jhin.2010.07.026 Journal of Hospital Infection 77 (2011) 58e63

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ww.sciencedirect.com
Journal of Hospital Infection 77 (2011) 58e63
Available online at w
Journal of Hospital Infection
journal homepage: www.elsevierhealth.com/journals / jh in
Procalcitonin as an early indicator of outcome in sepsis: a prospectiveobservational study
E.J. Giamarellos-Bourboulis a,*, I. Tsangaris b, Th. Kanni a, M. Mouktaroudi a, I. Pantelidou a, G. Adamis c,S. Atmatzidis d, M. Chrisofos e, V. Evangelopoulou f, F. Frantzeskaki b, P. Giannopoulos g,G. Giannikopoulos h, D. Gialvalis i, G.M. Gourgoulis a, K. Kotzampassi j, K. Katsifa k, G. Kofinas l,F. Kontopidou a, G. Koratzanis m, V. Koulouras n, A. Koutsikou o, M. Koupetori p, I. Kritselis q, L. Leonidou r,A. Mega s, V. Mylonam, H. Nikolaou t, S. Orfanos b, P. Panagopoulos a, E. Paramythiotou b,A. Papadopoulos a, X. Papanikolaou l, M. Pavlaki u, V. Polychronopoulos v, A. Skoutelis w, A. Theodotou x,M. Vassiliaghou y, E.E. Douzinas z, C. Gogos r, A. Armaganidis b on behalf of the Hellenic Sepsis Study Groupa4th Department of Internal Medicine, University of Athens, Medical School, Athens, Greeceb 2nd Department of Critical Care, University of Athens, Medical School, Athens, Greecec1st Department of Internal Medicine, ‘G. Gennimatas’ Athens Hospital, Athens, Greeced2nd Department of Surgery, University of Thessaloniki, Medical School, Thessaloniki, Greecee 2nd Department of Urology, ‘Sismanogleion’ Athens Hospital, Athens, Greecef Intensive Care Unit, ‘Korgialeneion-Benakeion’ Hospital of Athens, Athens, Greeceg 1st Department Propedeutic Surgery, University of Athens, Medical School, Athens, GreecehDepartment of Internal Medicine, Chios General Hospital, Chios, Greecei 2nd Department of Surgery, ‘Evangelismos’ Athens General Hospital, Athens, Greecej 1st Department Prop. Surgery, University of Thessaloniki, Medical School Thessaloniki, Greecek Intensive Care Unit, ‘Tzaneion’ Hospital of Piraeus, Piraeus, Greecel Intensive Care Unit, ‘Hippokrateion’ Athens General Hospital, Athens, Greecem 2nd Department of Internal Medicine, ‘Sismanogleion’ Athens Hospital, Athens, GreecenDepartment of Critical Care, University of Ioannina Medical School, Ioannina, Greeceo Intensive Care Unit, ‘Thriassio’ Elefsina General Hospital, Elefsina, Greecep1st Department of Internal Medicine, ‘Thriassio’ Elefsina General Hospital, Elefsina, GreeceqDepartment of Surgery, Nafplion General Hospital, Nafplion, Greecer 1st Department of Internal Medicine, University of Patras, Medical School, Patras, Greeces Intensive Care Unit, ‘Laikon’ Athens General Hospital, Athens, Greecet Intensive Care Unit, ‘Aghia Olga’ Athens General Hospital, Athens, GreeceuDepartment of Internal Medicine, Argos General Hospital, Argos, Greecev 3rd Department of Pulmonary Medicine, ‘Sismanoglion’ Athens Hospital, Athens, Greecew5th Department of Internal Medicine, ‘Evangelismos’ Athens Hospital, Athens, Greecex Intensive Care Unit, Karditsa General Hospital, Karditsa, Greecey Intensive Care Unit, ‘G. Gennimatas’ Thessaloniki General Hospital, Thessaloniki, Greecez3rd Department of Critical Care, University of Athens, Medical School, Athens, Greece
a r t i c l e i n f o
Article history:Received 11 November 2009Accepted 30 July 2010Available online 4 December 2010
Keywords:ProcalcitoninPrognosisSepsis
* Corresponding author. Address: 4th Department oUniversity General Hospital, 124 62 Athens, Greecefax: þ30 210 53 26 446.
E-mail address: [email protected] (E.J. Giam
0195-6701/$ e see front matter � 2010 The Hospitaldoi:10.1016/j.jhin.2010.07.026
s u m m a r y
This study explores the role of procalcitonin (PCT) in predicting the outcome of sepsis. Ina prospective multicentre observational investigation, blood was sampled within 24 h of onsetof sepsis in 1156 hospitalised patients; 234 were in the intensive care unit (ICU) at the point ofpresentation of sepsis while 922 were not. PCT was estimated in serum by the ultrasensitiveKryptor assay in a double-blinded fashion. Among patients outside the ICU, mortality was 8% inthose with PCT �0.12 ng/mL but 19.9% in those with PCT >0.12 ng/mL [P< 0.0001, odds ratio(OR) for death: 2.606; 95% confidence interval (CI): 1.553e4.371]. Among patients whose
f Internal Medicine, ATTIKON. Tel.: þ30 210 58 31 994;
arellos-Bourboulis).
Infection Society. Published by Elsevier Ltd. All rights reserved.

E.J. Giamarellos-Bourboulis et al. / Journal of Hospital Infection 77 (2011) 58e63 59
sepsis presented in ICU, mortality was 25.6% in those with PCT �0.85 ng/mL but 45.3% in thosewith PCT >0.85 ng/mL (P¼ 0.002; OR for death: 2.404; 95% CI: 1.385e4.171). It is concludedthat PCT cut-off concentrations can contribute to predicting the outcome of sepsis and mightbe of particular value in identifying patients who would benefit from ICU admission.
� 2010 The Hospital Infection Society. Published by Elsevier Ltd. All rights reserved.
Introduction
The incidence of sepsis has increased over the last decade. Thishas been attributed to various factors including the increasedincidence of diabetes mellitus, increasing numbers of long-stayintensive care unit (ICU) patients, increasing use of immunosup-pressive therapies and increasing antimicrobial resistance.1
Numerous studies have attempted to define the role of procalci-tonin (PCT) as a diagnostic biomarker in sepsis.2e4 Although levelsof PCT in serum are generally greater among patients with sepsisthan among those with non-infectious systemic inflammatoryresponse, meta-analyses have failed to determine a thresholdabove which PCT can safely discriminate sepsis.5 A serious limita-tion of all these studies is the limited number of enrolled patientsand the heterogeneity of PCT assays used, although there isevidence that serial PCT measurement might be of value in deter-mining the prognosis of the septic patient.3,6
More recently, the role of PCT in sepsis has been explored ina series of prospective trials.7e10 For instance, using an ultrasensi-tive assay, PCT has been shown to be useful in the decision toinitiate empiric antibiotics in patients with lower respiratory tractinfection.
In an attempt to study the problem of sepsis in Greece, theHellenic Sepsis Study Group was convened in May 2006 with theparticipation of various ICUs, departments of internal medicine anddepartments of surgery across the country. Twenty-six of thesedepartments participated in the present study. The aim of the studywas to define thresholds of PCT that can safely discriminate risk ofdeath separately for patients presenting with sepsis outside an ICUand for those developing sepsis after ICU admission.
Methods
Study design
This prospective multicentre study was conducted in 26departments across Greece from January 2007 to September 2008.The participating departments were 11 ICUs, eight departments ofinternal medicine, one department of pulmonary medicine, fivedepartments of surgery and one department of urology. Some areuniversity departments and some are departments of the Greeknational health system. The aim of the study was to define PCTthresholds that can safely discriminate the prognosis of sepsis.
Patients admitted with sepsis to the emergency department,patients with sepsis presenting during hospitalisation outside theICU and patients with sepsis presenting during hospitalisation inthe ICU were eligible. In total, 1156 patients were enrolled.Mortality was similar among non-ICU departments and amongICUs. Written informed consent was provided by the patients ortheir first-degree relatives for patients unable to consent. The studyprotocol was approved by the Ethics Committees of the hospitals ofparticipating centres. Each patient was enrolled once in the study.
Inclusion criteria were: (a) age �18 years; (b) sepsis due to lowerrespiratory tract infection, acute pyelonephritis, intra-abdominalinfection or primary bacteraemia, and (c) blood sampling within 24 hfrom onset of sepsis. Exclusion criteria were: (a) human immunode-ficiency virus infection, and (b) neutropenia (<1000 neutrophils/mL).
Patientswere classifiedas suffering fromsepsis, severe sepsis or septicshock, according to standard definitions.11
Ventilator-associated pneumonia was diagnosed in patientsintubated for more than two days with all of the following: (a) coretemperature >38 �C or <36 �C; (b) purulent tracheobronchialsecretions; and (c) new chest X-ray infiltrates.12e14
Acute lower respiratory tract infection was diagnosed inpatients with all of the following: (a) core temperature >38 �C or<36 �C; (b) white blood cell (WBC) count>12 000/mL; and (c) chestX-ray findings consistent with acute lower respiratory tract infec-tion.8 This was divided into community-acquired pneumonia (CAP)or hospital-acquired pneumonia (HAP).
Acute pyelonephritis was diagnosed in patients with all of thefollowing: (a) core temperature >38 �C or <36 �C; (b) lumbartenderness or radiological evidence consistent with acute pyelo-nephritis; and (c) �10 WBC/high power field of spun urine or �2þin dipstick test for WBCs and nitrates.15
Acute intra-abdominal infection was diagnosed in patients withall of the following: (a) core temperature >38 �C or <36 �C; (b)WBC count >12 000/mL; and (c) radiological evidence consistentwith intra-abdominal infection.16
Primary bacteraemia was diagnosed in patients presentingwith all of the following: (a) peripheral blood culture positivefor Gram-positive or Gram-negative bacteria (coagulase-negativestaphylococci and other skin commensals were consideredcontaminants unless isolated on at least two separate occasions orfrom both a peripheral vein and a central catheter); and (b)absence of any primary site of infection after extensiveinvestigation.16
For every patient a complete diagnostic work-up was performedcomprising history, thorough physical examination, WBC count,blood biochemistry, arterial blood gas, blood cultures fromperipheral veins and central lines, urine cultures, chest X-ray andchest and abdominal computed tomography if appropriate. Ifnecessary, quantitative cultures of tracheobronchial secretionswere performed and evaluated as previously described.12 Progresswas recorded for 28 days. Clinical and demographic data wererecorded in a case report form (CRF). All CRFs weremonitored by anindependent monitor blind to the study design.
Blood sampling and laboratory procedure
A volume of 3 mL of blood was sampled from every patientwithin 24 h of onset of sepsis. In 47 patients blood sampling wasrepeated within the first 24 h upon disease worsening. Blood wascollected into sterile, pyrogen- and anticoagulant-free tubes(Vacutainer, Becton Dickinson, Cockeysville, MD, USA). Tubes weretransported by courier within a day to the Laboratory of Immu-nology of Infectious Diseases of the 4th Department of InternalMedicine at ATTIKON University Hospital, Athens. Tubes werecentrifuged and serum was kept refrigerated at e70 �C untilassayed. PCT was estimated in duplicate by immuno-time-resolvedamplified cryptate technology assay (Kryptor PCT; BRAHMS GmbH,Henningdorf, Germany) with a functional assay sensitivity of0.06 ng/mL. This assay applies a six-point standard curve and twocontrols with known concentrations per run. All estimations wereperformed and reported by two technicians who were blind to the
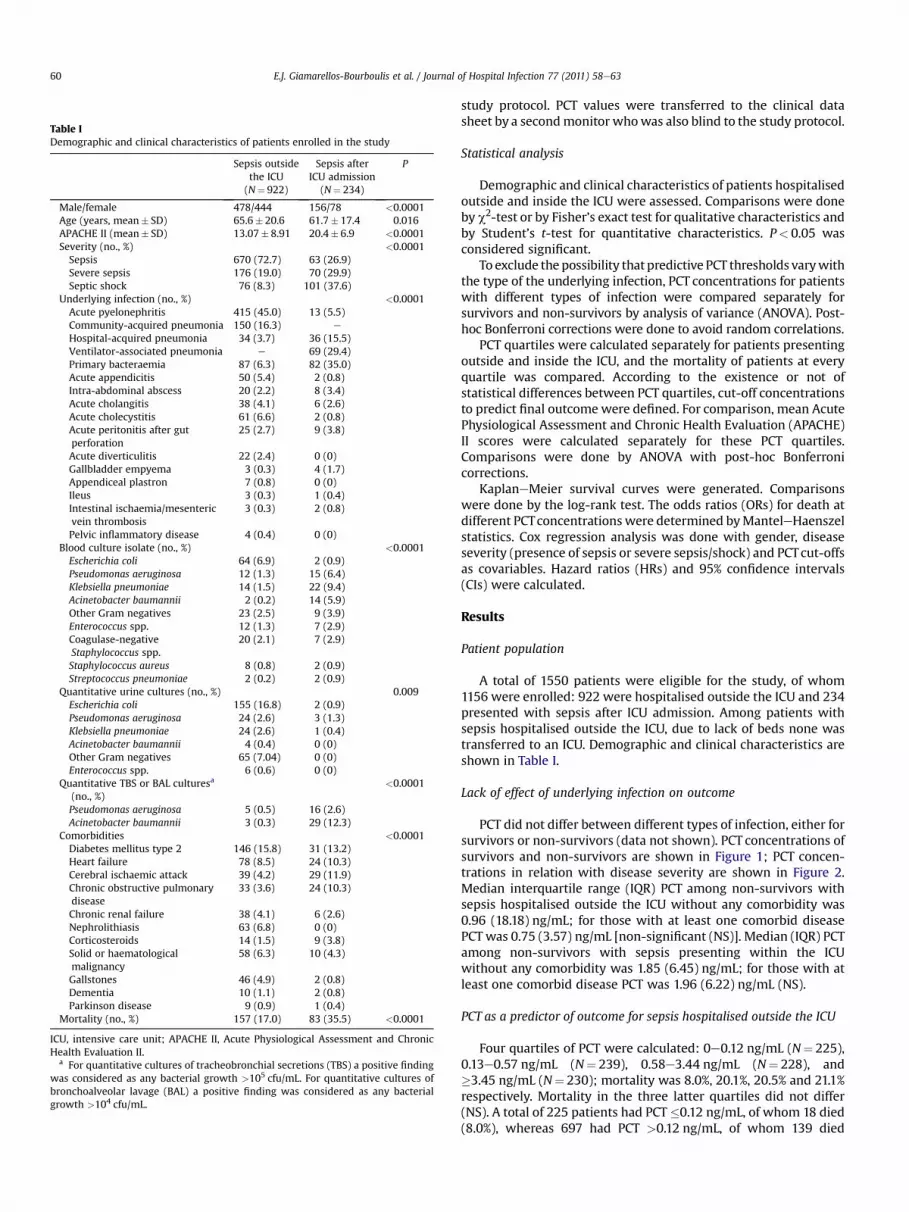
Table IDemographic and clinical characteristics of patients enrolled in the study
Sepsis outsidethe ICU(N¼ 922)
Sepsis afterICU admission
(N¼ 234)
P
Male/female 478/444 156/78 <0.0001Age (years, mean� SD) 65.6� 20.6 61.7� 17.4 0.016APACHE II (mean� SD) 13.07� 8.91 20.4� 6.9 <0.0001Severity (no., %) <0.0001Sepsis 670 (72.7) 63 (26.9)Severe sepsis 176 (19.0) 70 (29.9)Septic shock 76 (8.3) 101 (37.6)
Underlying infection (no., %) <0.0001Acute pyelonephritis 415 (45.0) 13 (5.5)Community-acquired pneumonia 150 (16.3) e
Hospital-acquired pneumonia 34 (3.7) 36 (15.5)Ventilator-associated pneumonia e 69 (29.4)Primary bacteraemia 87 (6.3) 82 (35.0)Acute appendicitis 50 (5.4) 2 (0.8)Intra-abdominal abscess 20 (2.2) 8 (3.4)Acute cholangitis 38 (4.1) 6 (2.6)Acute cholecystitis 61 (6.6) 2 (0.8)Acute peritonitis after gutperforation
25 (2.7) 9 (3.8)
Acute diverticulitis 22 (2.4) 0 (0)Gallbladder empyema 3 (0.3) 4 (1.7)Appendiceal plastron 7 (0.8) 0 (0)Ileus 3 (0.3) 1 (0.4)Intestinal ischaemia/mesentericvein thrombosis
3 (0.3) 2 (0.8)
Pelvic inflammatory disease 4 (0.4) 0 (0)Blood culture isolate (no., %) <0.0001Escherichia coli 64 (6.9) 2 (0.9)Pseudomonas aeruginosa 12 (1.3) 15 (6.4)Klebsiella pneumoniae 14 (1.5) 22 (9.4)Acinetobacter baumannii 2 (0.2) 14 (5.9)Other Gram negatives 23 (2.5) 9 (3.9)Enterococcus spp. 12 (1.3) 7 (2.9)Coagulase-negativeStaphylococcus spp.
20 (2.1) 7 (2.9)
Staphylococcus aureus 8 (0.8) 2 (0.9)Streptococcus pneumoniae 2 (0.2) 2 (0.9)
Quantitative urine cultures (no., %) 0.009Escherichia coli 155 (16.8) 2 (0.9)Pseudomonas aeruginosa 24 (2.6) 3 (1.3)Klebsiella pneumoniae 24 (2.6) 1 (0.4)Acinetobacter baumannii 4 (0.4) 0 (0)Other Gram negatives 65 (7.04) 0 (0)Enterococcus spp. 6 (0.6) 0 (0)
Quantitative TBS or BAL culturesa
(no., %)<0.0001
Pseudomonas aeruginosa 5 (0.5) 16 (2.6)Acinetobacter baumannii 3 (0.3) 29 (12.3)
Comorbidities <0.0001Diabetes mellitus type 2 146 (15.8) 31 (13.2)Heart failure 78 (8.5) 24 (10.3)Cerebral ischaemic attack 39 (4.2) 29 (11.9)Chronic obstructive pulmonarydisease
33 (3.6) 24 (10.3)
Chronic renal failure 38 (4.1) 6 (2.6)Nephrolithiasis 63 (6.8) 0 (0)Corticosteroids 14 (1.5) 9 (3.8)Solid or haematologicalmalignancy
58 (6.3) 10 (4.3)
Gallstones 46 (4.9) 2 (0.8)Dementia 10 (1.1) 2 (0.8)Parkinson disease 9 (0.9) 1 (0.4)
Mortality (no., %) 157 (17.0) 83 (35.5) <0.0001
ICU, intensive care unit; APACHE II, Acute Physiological Assessment and ChronicHealth Evaluation II.
a For quantitative cultures of tracheobronchial secretions (TBS) a positive findingwas considered as any bacterial growth >105 cfu/mL. For quantitative cultures ofbronchoalveolar lavage (BAL) a positive finding was considered as any bacterialgrowth >104 cfu/mL.
E.J. Giamarellos-Bourboulis et al. / Journal of Hospital Infection 77 (2011) 58e6360
study protocol. PCT values were transferred to the clinical datasheet by a secondmonitor whowas also blind to the study protocol.
Statistical analysis
Demographic and clinical characteristics of patients hospitalisedoutside and inside the ICU were assessed. Comparisons were doneby c2-test or by Fisher’s exact test for qualitative characteristics andby Student’s t-test for quantitative characteristics. P< 0.05 wasconsidered significant.
To exclude the possibility that predictive PCT thresholds varywiththe type of the underlying infection, PCT concentrations for patientswith different types of infection were compared separately forsurvivors and non-survivors by analysis of variance (ANOVA). Post-hoc Bonferroni corrections were done to avoid random correlations.
PCT quartiles were calculated separately for patients presentingoutside and inside the ICU, and the mortality of patients at everyquartile was compared. According to the existence or not ofstatistical differences between PCT quartiles, cut-off concentrationsto predict final outcome were defined. For comparison, mean AcutePhysiological Assessment and Chronic Health Evaluation (APACHE)II scores were calculated separately for these PCT quartiles.Comparisons were done by ANOVA with post-hoc Bonferronicorrections.
KaplaneMeier survival curves were generated. Comparisonswere done by the log-rank test. The odds ratios (ORs) for death atdifferent PCTconcentrations were determined byManteleHaenszelstatistics. Cox regression analysis was done with gender, diseaseseverity (presence of sepsis or severe sepsis/shock) and PCTcut-offsas covariables. Hazard ratios (HRs) and 95% confidence intervals(CIs) were calculated.
Results
Patient population
A total of 1550 patients were eligible for the study, of whom1156 were enrolled: 922 were hospitalised outside the ICU and 234presented with sepsis after ICU admission. Among patients withsepsis hospitalised outside the ICU, due to lack of beds none wastransferred to an ICU. Demographic and clinical characteristics areshown in Table I.
Lack of effect of underlying infection on outcome
PCT did not differ between different types of infection, either forsurvivors or non-survivors (data not shown). PCT concentrations ofsurvivors and non-survivors are shown in Figure 1; PCT concen-trations in relation with disease severity are shown in Figure 2.Median interquartile range (IQR) PCT among non-survivors withsepsis hospitalised outside the ICU without any comorbidity was0.96 (18.18) ng/mL; for those with at least one comorbid diseasePCT was 0.75 (3.57) ng/mL [non-significant (NS)]. Median (IQR) PCTamong non-survivors with sepsis presenting within the ICUwithout any comorbidity was 1.85 (6.45) ng/mL; for those with atleast one comorbid disease PCT was 1.96 (6.22) ng/mL (NS).
PCT as a predictor of outcome for sepsis hospitalised outside the ICU
Four quartiles of PCT were calculated: 0e0.12 ng/mL (N¼ 225),0.13e0.57 ng/mL (N¼ 239), 0.58e3.44 ng/mL (N¼ 228), and�3.45 ng/mL (N¼ 230); mortality was 8.0%, 20.1%, 20.5% and 21.1%respectively. Mortality in the three latter quartiles did not differ(NS). A total of 225 patients had PCT �0.12 ng/mL, of whom 18 died(8.0%), whereas 697 had PCT >0.12 ng/mL, of whom 139 died

Non-ICU
16
12
PCT
con
cent
ratio
n (n
g/m
L)
8
4
0
16
12
PCT
con
cent
ratio
n (n
g/m
L)
8
4
0
Survivors Non-survivors Survivors Non-survivors
ICU
P = 0.001P = 0.004
Figure 1. Boxplots of procalcitonin (PCT) concentrations among survivors and non-survivors. Circles denote outliers and asterisks denote extremes. P-values reflect significantdifferences between survivors and non-survivors. Results are given separately for patients with sepsis presenting outside an intensive care unit (non-ICU; P¼ 0.004) and for patientswith sepsis presenting after ICU admission (ICU; P¼ 0.001).
E.J. Giamarellos-Bourboulis et al. / Journal of Hospital Infection 77 (2011) 58e63 61
(19.9%) (Figure 3). OR for death at PCT >0.12 ng/mL was 2.606 (95%CI: 1.553e4.371; P< 0.0001). In consequence we propose thata cut-off of 0.12 ng/mL may be predictive of final outcome.
Mean� SD APACHE II score among patients with PCT �0.12ng/mL was 10.23� 6.95, and among those with PCT >0.12 ng/mLwas 13.81�9.20 (P< 0.0001). Mean� SD WBC counts were13 521.9� 5138.6 and 15 111.4� 9435.7/mL respectively (P¼ 0.034).
Among cases of primary bacteraemia, seven had PCT �0.12 ng/mL and 80 had PCT >0.12 ng/mL. Nil and 24 (30.0%) died respec-tively (P¼ 0.041).
The implicated pathogenwas identified in 51 of the 225 patientswith PCT �0.12 ng/mL (22.7%); in 47 of these (92.2%) at least one ofthe initially prescribed antimicrobials was active in vitro against theorganism. The implicated pathogenwas identified in 298 of the 697patients with PCT >0.12 ng/mL (42.8%); in 285 of these (95.6%, NS)at least one of the initially prescribed antimicrobials was active invitro against the pathogen.
In an attempt to define whether the calculated PCT cut-off maybe an independent predictor of outcome, two different approacheswere used. In the first approach, mean� SD of APACHE II scores
Non-ICU
P < 0.001
P < 0.001
30
20
10
0
PCT
con
cent
ratio
n (n
g/m
L)
Sepsis Severe sepsis Septic shock
Figure 2. Boxplots of procalcitonin concentrations according to sepsis severity. Circles dcompared to patients with sepsis. Results are given separately for patients with sepsis preseafter ICU admission (ICU).
were calculated for patients belonging to each PCT quartile,i.e. 0e0.12, 0.13e0.57, 0.58e3.44, and �3.45 ng/mL. Mean� SDAPACHE II scores were 10.26� 6.84,12.88� 10.75,14.32� 9.59, and14.28� 7.22 respectively. APACHE II scores of patients whose PCTlevels were in the lowest quartile were lower than those of patientswhose PCT levels were in the other three quartiles (P< 0.0001),whereas scores of the patients in the second, third and fourth PCTquartiles did not differ from each other (NS).
In the second approach, Cox regression survival analysis wasdone. By this method, the only factor in the equation affectingoutcome was disease severity (HR: 9.04; 95% CI: 6.00e13.62;P< 0.0001) as opposed to gender (1.10; 0.78e1.56; NS) or the PCT0.12 ng/mL cut-off (1.26; 0.73e2.21; NS).
PCT as a predictor of outcome for sepsis presenting after ICUadmission
Four quartiles of PCT were calculated: 0e0.28 ng/mL (N¼ 57),0.28e0.85 ng/mL (N¼ 60), 0.86e3.55 ng/mL (N¼ 59), �3.56 ng/mL(N¼ 58); mortality was 22.8%, 28.3%, 43.4% and 49.3% respectively.
ICU
P < 0.00130
20
10
0
PCT
con
cent
ratio
n (n
g/m
L)
Sepsis Severe sepsis Septic shock
enote outliers and asterisks denote extremes. P-values reflect significant differencesnting outside an intensive care unit (non-ICU) and for patients with sepsis presenting

1.0
0.8
0.6
0.4
0.2
0.0
0 4 8 12 16 20 24 28Survival (days)
Cum
ulat
ive
surv
ival
log-rank: 14.027
P < 0.0001
Figure 3. Survival curves of patients with sepsis hospitalised outside the intensive careunit in relation to procalcitonin (PCT) concentration. Solid line: �0.12; dashed line:>0.12. P-values correspond to comparisons between patients below or above theindicated PCT threshold.
E.J. Giamarellos-Bourboulis et al. / Journal of Hospital Infection 77 (2011) 58e6362
Mortality did not differ between the first and the second quartiles(NS), nor between the third and the fourth quartiles (NS). A total of117 patients had PCT �0.85 ng/mL, of whom 30 died (25.6%), andanother 117 had PCT >0.85 ng/mL, of whom 53 died (45.3%)(Figure 4). OR for death at PCT >0.85 ng/mL was 2.404 (95% CI:
1.0
0.8
0.6
0.4
0.2
0.0
0 4 8 12 16 20 24 28Survival (days)
Cum
ulat
ive
surv
ival
log-rank: 9.683
P = 0.002
Figure 4. Survival curves of patients with sepsis presenting in the ICU in relation toprocalcitonin (PCT) concentration. Solid line: �0.85; dashed line: >0.85. P-valuescorrespond to comparisons between patients below or above the indicated PCTthreshold.
1.385e4.171; P< 0.0001). In consequence we propose that a cut-offof 0.85 ng/mL may be predictive of final outcome in patients whodevelop sepsis on ICU.
Themean� SDAPACHE II scorewas 18.59� 7.21 among patientswith PCT �0.85 ng/mL, and 22.10� 6.30 (P< 0.0001) amongpatients with PCT> 0.85 ng/mL. Mean� SD WBC counts were12 988.8� 7804.3 and 16 342.7�13 323.4/mL respectively (P¼ 0.032).
Among cases of primary bacteraemia, 40 had PCT �0.85 ng/mLand 42 had PCT >0.85 ng/mL. Eight (20%) and 19 (45.2%) diedrespectively (P¼ 0.029).
The implicated pathogenwas identified in 50 of the 117 patientswith PCT �0.85 ng/mL (42.7%); in 37 of these (74%) at least one ofthe initially prescribed antimicrobials was active in vitro against thepathogen. The implicated pathogen was identified in 48 of the 117patients with PCT>0.85 ng/mL (41.0%); in 35 of these (72.9%, NS) atleast one of the initially prescribed antimicrobials was active in vitroagainst the pathogen.
In an attempt to define whether the calculated PCT cut-off maybe an independent factor for outcome, again two differentapproaches were used as above. For patients in each PCT quartile(i.e. 0e0.28, 0.28e0.85, 0.86e3.55, and �3.56 ng/mL), mean� SDAPACHE II scores were 17.43� 5.42, 19.85� 8.41, 20.55� 6.65, and23.59� 5.62 respectively. APACHE II scores among patients in thefirst PCT quartile were lower compared with those in the fourthquartile (P< 0.0001) but did not differ compared with the secondand third quartiles. APACHE II scores among patients in the secondPCT quartile were lower compared with those in the fourth quartile(P¼ 0.029) but did not differ compared with the other quartiles.APACHE II scores among patients in the third quartile did not differcompared with other quartiles.
Using the Cox regression survival analysis method, both diseaseseverity and PCT >0.85 ng/mL were independently associated withfinal outcome. HR for death was 3.02 in the event of severe sepsis orshock (95% CI: 1.36e6.73; P¼ 0.007) and 2.31 (95% CI: 1.32e4.05;P¼ 0.003) when PCT >0.85 ng/mL.
Changes in PCT with worsening disease
PCT measurement was repeated for nine patients on progressionfrom septic shock to multi-organ failure; for 19 patients onprogression from sepsis to septic shock; for 10 patients uponprogression from sepsis to severe sepsis; and for nine patients uponprogression from severe sepsis to septic shock. In the first group(shock to organ failure), median (IQR) PCT on day 1 was 0.40(1.78) ng/mL and on worsening it was 0.52 (28.56) ng/mL (NS). Inthe second group (sepsis to septic shock), median (IQR) PCTon day 1was 0.53 (1.25) ng/mL and on worsening it was 0.60 (12.37) ng/mL(NS). In the third group (sepsis to severe sepsis), median (IQR) PCTon day 1 was 0.19 (2.57) ng/mL and on worsening it was 0.86(2.28) ng/mL (NS). In the fourth group (severe sepsis to septicshock), median (IQR) PCT on day 1 was 0.54 (0.46) ng/mL and onworsening it was 0.61 (0.68) ng/mL (NS).
Discussion
Early and reliable recognition of sepsis is essential for successfulmanagement, prompting great interest in the role of biomarkers.Although numerous studies have explored the role of PCT in earlydiagnosis, to our knowledge no study has investigated whether PCTcan be predictive of outcome.
Our results suggest that PCT can be useful in the early predictionof patients at risk of death. The PCT cut-off estimated within thefirst 24 h of onset of sepsis differed according to the type of nursingfacility. Among patients hospitalised outside the ICU, a PCT level of�0.12 ng/mL was predictive of death, whereas for patients in the

E.J. Giamarellos-Bourboulis et al. / Journal of Hospital Infection 77 (2011) 58e63 63
ICU a PCT level of >0.85 ng/mL was predictive of death. Thediscrepancy may reflect differences between the two groups in theresponse to sepsis, or the effectiveness of its management (Table I).The PCT threshold of 0.12 ng/mLmay provide powerful informationto the attending physician outside the ICU.
The validity of these cut-offs is supported by four observations:(a) the lack of effect of the type of underlying infection or thepresence of comorbid conditions; (b) the significant differences inAPACHE II scores and in WBC counts between groups of patientsdefined by these cut-offs; (c) the lack of effect of the activity of theadministered antimicrobial regimens; and (d) the stability of PCTlevels on disease worsening.
The proposed cut-offs seem to provide additional prognosticvalue to the widespread APACHE II score especially for ICUpatients. For patients with sepsis developing outside the ICU,APACHE II scores increased in parallel with the increase in PCTquartile. APACHE II is not widely used outside the ICU so PCTmight still be a powerful tool. For patients developing sepsis afterICU admission, the 0.85 ng/mL PCT cut-off proved to be animportant predictor of final outcome. In these patients, APACHE IIscore did not increase in parallel with PCT quartiles and Coxregression analysis revealed the proposed threshold to be anindependent predictor of mortality.
Our study has some limitations. For instance, the predominanceof Gram-negative bacteria causing sepsis in our patients raisesconcerns about whether our results would apply to sepsis of othercauses. Furthermore, no patient with sepsis presenting outside theICU was subsequently admitted to an ICU, preventing us fromexploring whether the proposed PCT cut-offs translate to earlierICU admission.
This is the first large multicentre study clearly showing thatPCT may be useful in the early discrimination of the septic patientat risk of unfavourable outcome and providing specific concen-tration cut-offs to aid this prognostication. Although previousstudies have shown that PCT early in the septic process is greateramong non-survivors than among survivors, they did not identifypractical cut-off concentrations nor did they define survivalcurves.17,18 Our results strongly support the use of PCT in theroutine management of the septic patient.
Conflict of interest statementNone declared.
Funding sourceThis study was supported by an unrestricted educational grantby Brahms GmbH, Germany. The funding source had no role inthe collection and analysis of data nor inwriting themanuscript.
References
1. Wenzel RP. Treating sepsis. N Engl J Med 2002;347:966e967.2. Jones AE, Fiechtl JF, Brown MD, Ballew JJ, Kline JA. Procalcitonin test in the
diagnosis of bacteremia: a meta-analysis. Ann Emerg Med 2007;50:34e41.3. Giamarellos-Bourboulis EJ, Mega A, Grecka P, et al. Procalcitonin: a marker to
clearly differentiate systemic inflammatory response syndrome and sepsis inthe critically ill patient? Intensive Care Med 2002;28:1351e1356.
4. Becker KL, Snider R, Nylen ES. Procalcitonin assay in systemic inflammation,infection, and sepsis: clinical utility and limitations. Crit Care Med2008;36:941e952.
5. Tang BMP, Eslick GD, Craig JC, McLean AS. Accuracy of procalcitonin for sepsisdiagnosis in critically ill patients: systematic review and meta-analysis. LancetInfect Dis 2007;7:210e217.
6. Dahaba AA, Hagara B, Fall A, Rehak PH, List WF, Metzler H. Procalcitonin forearly prediction of survival outcome in postoperative critically ill patients withsevere sepsis. Br J Anesth 2006;97:503e508.
7. Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-guidedtreatment on antibiotic use and outcome in lower respiratory tract infections:cluster-randomized, single-blinded intervention trial. Lancet2004;363:600e607.
8. Christ-Crain M, Stolz D, Bingisser R, et al. Procalcitonin guidance of antibiotictherapy in community-acquired pneumonia. A randomized trial. Am J Resp CritCare Med 2006;174:84e93.
9. Stolz D, Christ-Crain M, Bingisser R, et al. Antibiotic treatment of exacerbationsof COPD. A randomized controlled trial comparing procalcitonin-guidance withstandard therapy. Chest 2007;131:9e19.
10. Briel M, Schuetz P, Mueller B, et al. Procalcitonin-guided antibiotic use vsstandard approach for acute respiratory tract infections in primary care. ArchIntern Med 2008;168:2000e2007.
11. Levy M, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS interna-tional sepsis definitions conference. Crit Care Med 2003;31:1250e1256.
12. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med2002;165:867e903.
13. KollefMH.Appropriateantibiotic therapy forventilator-associatedpneumoniaandsepsis: a necessity, not an issue for debate. Intensive Care Med 2003;29:147e149.
14. Rello J, Paiva JA, Baraibar J, et al. International conference for the developmentof consensus on the diagnosis and treatment of ventilator-associated pneu-monia. Chest 2001;120:955e970.
15. Pinson AG, Philbrick JT, Lindbeck GH, Schorling JB. Fever in the clinical diag-nosis of acute pyelonephritis. Am J Emerg Med 1997;15:148e151.
16. Calandra T, Cohen J. The International Sepsis Forum Consensus definitions ofinfections in the intensive care unit. Crit Care Med 2005;33:1639e1648.
17. Rau MB, Frigerio I, Büchler MW, et al. Evaluation of procalcitonin for predictingseptic multiorgan failure and overall prognosis in secondary peritonitis. Aprospective, international multicenter study. Arch Surg 2007;142:134e142.
18. Hirakata Y, Yanagihara K, Kurihara S, et al. Comparison of usefulness of plasmaprocalcitonin and C-reactive protein measurements for estimation of severityin adults with community acquired pneumonia. Diagn Microbiol Infect Dis2008;61:170e174.
Related Documents







![Procalcitonin · 2014-02-17 · 1 What is Procalcitonin? Healthy 0.05 0.52 10 Local infections Septic shock Severe sepsis Systemic infections (sepsis) Clinical condition PCT [ng/mL]](https://static.cupdf.com/doc/110x72/5e973e26f8ba5342184eaef4/procalcitonin-2014-02-17-1-what-is-procalcitonin-healthy-005-052-10-local-infections.jpg)



