INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT, VOL. 10,11%128 (1995) PRINCIPLES OF HEALTH INFRASTRUCTURE PLANNING IN LESS DEVELOPED COUNTRIES J.-P. UNGER AND BART CRIEL Public Health Research and Training Unit, Prince Leopold Institute of Tropical Medicine, Nationalestraat 185, B-2000 Antwerp, Belgium SUMMARY This article proposes a number of key principles for health infrastructure planning, based on a literaturereview on the one hand, and on a process of internal deduction on the other. The principles discussed are the following: an integrated health system; a thrifty planning of tiers within that health system; a specificity of tiers; a homogeneity of the tiers’ structures; a minimum package of activities; a territorial responsibility and/or an explicit and discrete responsibility for a well-defined population; a necessary and suflicient population basis; a partial separation of administrative and public health planning bases; and, finally, rules for a geographical division and integration of non- governmental organizations. The definition of two strategies, primary health care and district health systems, is also revisited. KEY WORDS: Less Developed Countries; Integrated Health System; District Management; Primary Health Care INTRODUCTION The budget crises that health ministries are experiencing in less developed countries are such that not much more than paying salaries to staff can be done. Moreover, these salaries are often grossly insufficient. The subsequent scarcities of drugs and other consumables has led to a gradual decrease in the utilization of public health services by the population. The maintenance of health care facilities is threatened. Health manpower is concentrated mainly in large urban areas and many hospitals and health centres in rural areas are ‘functioning’ without doctors or nurses. There may, however, be a positive aspect linked to this crisis. Indeed, it offers Ministries of Health an opportunity to rationalize their health care pyramid and to concentrate the (scarce) resources on the most efficient entities in their respective health systems. The goal of this article is to review the principles guiding the identification of these entities; the definition of their functions and relationships with the other entities in the health system; the identification of the resources they need; and, finally, the identification of their interaction with the communities they serve. CCC 07494753/95/020113-16 01995 by John Wiley & Sons, Ltd.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT, VOL. 10,11%128 (1995)
PRINCIPLES OF HEALTH INFRASTRUCTURE PLANNING IN LESS DEVELOPED
COUNTRIES
J.-P. UNGER AND BART CRIEL Public Health Research and Training Unit, Prince Leopold Institute of Tropical Medicine,
Nationalestraat 185, B-2000 Antwerp, Belgium
SUMMARY
This article proposes a number of key principles for health infrastructure planning, based on a literature review on the one hand, and on a process of internal deduction on the other. The principles discussed are the following: an integrated health system; a thrifty planning of tiers within that health system; a specificity of tiers; a homogeneity of the tiers’ structures; a minimum package of activities; a territorial responsibility and/or an explicit and discrete responsibility for a well-defined population; a necessary and suflicient population basis; a partial separation of administrative and public health planning bases; and, finally, rules for a geographical division and integration of non- governmental organizations. The definition of two strategies, primary health care and district health systems, is also revisited.
KEY WORDS: Less Developed Countries; Integrated Health System; District Management; Primary Health Care
INTRODUCTION
The budget crises that health ministries are experiencing in less developed countries are such that not much more than paying salaries to staff can be done. Moreover, these salaries are often grossly insufficient. The subsequent scarcities of drugs and other consumables has led to a gradual decrease in the utilization of public health services by the population. The maintenance of health care facilities is threatened. Health manpower is concentrated mainly in large urban areas and many hospitals and health centres in rural areas are ‘functioning’ without doctors or nurses.
There may, however, be a positive aspect linked to this crisis. Indeed, it offers Ministries of Health an opportunity to rationalize their health care pyramid and to concentrate the (scarce) resources on the most efficient entities in their respective health systems. The goal of t h i s article is to review the principles guiding the identification of these entities; the definition of their functions and relationships with the other entities in the health system; the identification of the resources they need; and, finally, the identification of their interaction with the communities they serve.
CCC 07494753/95/020113-16 01995 by John Wiley & Sons, Ltd.
114 J.-P. UNGER AND B. CRIEL
KEY PRINCIPLES
An integrated health system
This principle argues the need for a specificity of, and a complementarity between, the various tiers in the health system.
Not all facilities are equally fit to provide a given service. This is a quite straightforward statement which seems obvious at first glance; yet, notwithstanding its common sense, it often lacks operationalization in health planning terms. The arguments underlying this statement are twofold: there is an economic rationale on the one hand, and a functional or technical one on the other. Nobody questions the relevancy of having hospitals to host and centralize technology and expertise. There is far less of a consensus, however, when the question arises whether hospitals are to deliver first-line health care, i.e. the care traditionally delivered by polyvalent health workers (e.g. a general practitioner). The assumption that hospitals should do so is often an implicit one. Indeed, many authors do describe ‘primary programmes’ to include those delivered by hospitals (Pearson, 1985; De Boer and McNeil, 1989; Jacobson et al., 1989; Chiphangwi, 1987). In the case of Zimbabwe for instance, it is illustrative that the facilities in the vast majority of the districts are either ‘rural health centres’ or ‘district hospitals’. For the urban or semi-urban population living around the location of the hospital, it is taken for granted that the hospital is the place to provide primary care to its surrounding communities. The implicit assumption is that a health centre is a valid option for the delivery of primary care to rural communities; but not so for urban communities where the district hospitals’ out-patients departments will take up that role.
We challenge this belief and offer the following arguments. Identical health care becomes increasingly expensive when it is delivered by
‘higher’ levels in the health care system (Van Lerberghe and Lafort, 1990). There must, thus, be one type of facility that is more efficient and more effective than others when it comes to solve a given health problem. We think that a hospital is not fit to provide first-line health care. Indeed:
- a hospital is too big a structure for staff and community members to know each other, and comprehensive and continuous care are thus jeopardized from the start (for instance, the population served by hospitals is so large that home visits meant to ensure continuity of care are impracticable);
-integrated care is hampered by the division of labour inherent to large entities;
- the technical and organizational complexity of hospital operations is hardly compatible with a process of participatory management;
- a high number of primary cases presenting at the hospital level results in the underutilization of the qualifications of its staff; and,
- an involvement of the hospital into primary care fosters the perception in the community that a health centre really is only the ‘second best’ solution; it will thus jeopardize the health centre’s credibility.

HEALTH INFRASTRUCTURE PLANNING 115
The role of first-line health services is to deliver care that is comprehensive, continuous and integrated (EVO, 1971), a principle which was implemented in the Kasongo project (1981). Many of the factors conditioning comprehensiveness, continuity and integration of care can only be met by a health facility responding to the following characteristics: a modestly sized building (human dimensions!) with not too big a staff; a relatively small population to care for; and, a close relationship between staff and people.
A sick person is more than a sick liver or a tired heart; he or she is also anxious for what the future will bring. A child with measles is more than merely the victim of a virus; he or she may also become malnourished. A woman with a tenth child may be very eager not to have future pregnancies, but she does not dare to express it in a straightforward way. The process of decreasing the suffering (present or potential) is greatly enhanced when the intervention proposed by the health worker takes into consideration the multiple dimensions of the health problem (i.e. including elements apart from the purely biological one). Because of this complexity, the management of a patient must be holistic if it is to be effective (Armstrong, 1979).
Care leading to a useful end is called continuous. It should not be limited to the issuing of a prescription. For instance, if a patient has no money, then he will not purchase the drugs. Or, if he is not convinced about the usefulness of the prescription, he is likely to throw it away. Similarly, a patient with tuberculosis, in the absence of conditions that would motivate him to complete his treatment, is likely to stop his treatment as soon as he feels better. If care is to be continuous, then it should be holistic. A holistic approach also implies that the health worker can offer the most appropriate type of care for the problem the patient presents at a given time and in a given context; curative or preventive or promotional care, or a combination of them. It is, other things remaining equal, easier to offer such an integrated care, if curative and preventive care are being coordinated within one single small unit.
Continuity of care also implies more than merely an interested attitude of the health worker. It is likely to succeed only if a number of structural and organizational changes are met: for instance, the existence of a real dialogue between health service and community, the organization of ‘defaulter tracing’ with the possibility of carrying out home visits, the implementation of a continuity ‘friendly’ fee system etc. (Criel and Van Balen, 1993). Integration of care, in itself a condition for having holistic care implies a good knowledge of the patient and of his social environment, an appropriate individual information system, and so on. The point to be made here is that holistic, integrated and continuous care can only be delivered under certain structural and organizational conditions; factories such as hospitals do not fit these conditions and are therefore the wrong structures to deliver that kind of care.
These arguments, together with the trade-off between the need to centralize technicity on the one hand, and the need for health facilities to be readily accessible, strengthen the idea that each level within the health pyramid should provide a given type of care. Each level should provide these services for which it is most fit, without offering at the same time the services for which another
116 J.-P. UNGER AND B. CRIEL
level is most appropriate. Let the cobbler stick to his last! In other words, an overlap of activities should be avoided. An occasional diversity of functions can be accepted if, for instance, a multiplication of urban hospital facilities is to be avoided.
While nobody denies the usefulness of a consistent health care pyramid, the principle of the specificity of each level of care is described only exceptionally. For instance, Balique (1989) includes level 1 activities (immunization, tuberculosis and leprosy control, diarrhoea1 disease control) in level 2 establishments.
Since the levels of health care services must be specific, and since it is desirable that people are treated as close as possible to their domicile (Jolly and King, 1966), the links between the different health care levels must be defined unequivocally, corresponding to the definition of an integrated system. In practice, a health system should meet the following four criteria:
(a) The system should contain no functional gaps: most of the situations must be covered in such a way that the vast majority of the health problems encountered can find an appropriate solution somewhere within the existing health pyramid. The overall effectiveness of the system can thus be ensured. The identification of the system’s functions should start from the intersection of the community’s demand (curative care being the most straightforward one) and the needs (as defined by professionals).
(b)The system should avoid any functional overlapping among its different levels (principle of specificity), with a few exceptions, like, for instance, the function of a district hospital being fulfilled by higher level hospitals (e.g. provincial or regional hospital).
(c) The patients should be taken care of at the very level best fit to manage their problems. An organizational consequence is that barriers (financial, intra-institutional, psychological, geographical) hindering the flow of referred patients within the system should be avoided as much as possible. The first level of care should be the entry gate into the system. Indeed, the likelihood that health problems will be solved under the jurisdiction of level 1 infrastructure is very high (90-95%). The problem will not only be solved in a more efficient way, but also in a more effective way. A World Bank study, carried out nine years ago, expressed the importance of health posts as follows: ‘But even in their present, imperfect state, health post programs are quite possibly competitive with the other available modes of service delivery when compared with them in cost-effectiveness terms’ (Gwatkin et al., 1986). Other studies have yielded similar conclusions (Van Lerberghe and Pangu, 1988; Adekolv, 1979). Because of the principle of specificity, barriers to a direct access to second-line professionals (e.g. through higher fees, system of appointments, etc.) should be used as incentives for an appropriate channelling of patients in the system. Great Britain and the Netherlands apply this principle (OECD, 1992), named the ‘~helonage’ (hierarchy of tiers) (Peeters et al., 1985).
.
HEALTH INFRASTRUCTURE PLANNING 117
(d) Finally, the relevant information on the patient’s problem should accompany the patient as he or she travels between the different levels in the system.
Homogeneity of the structures at each level
Each problem (e.g. a delivery, a trauma, an infection) requires specific techniques that can be reasonably decentralized so as to increase their geographical accessibility. Activities and techniques requiring staff with a given skill and materials of a certain type should be decentralized in similar infrastructures, constituting thereby a ‘tier’ of the health system. Decentralization obviously is constrained by an increase in costs (i.e. the economic limit to decentralization) and by a reduction in quality of care (i.e. the technical limit to decentralization). The latter refers to the fact that difficult techniques or complex diagnostic procedures cannot be practised regularly enough in small populations. Each technique or diagnostic act thus requires an optimal degree of decentralization. But, it would obviously not be very efficient to eventually have a health system with a large number of different facilities, each of them being adapted to one given technique or act. If the system is to be efficient, then these facilities should be grouped together in homogeneous structures (principle of the homogeneity of a level’s structures) because this simplifies planning of resources.
Thrifty planning of tiers
The system should have the necessary amount of different tiers (and not more than that) enabling it to solve, in an effective and efficient way, the majority of the health problems people experience. Thrifty planning means that the system should be as simple as possible. It is crucial to acknowledge that, a priori, the more tiers a system has, the more complex is its management, the more costly is its functioning, and the more likely will be the occurrence of delays in care at the appropriate tier in that same system. Hence, the system should be as simple as possible and only as complex as is really needed. If health planners intend to increase the number of tiers, then this decision should be strongly motivated. The expected advantages should be high enough to outweigh the already well- established disadvantages! This may be the case now and then (for instance, in the case of extremely scattered populations); but, there is solid empirical evidence that a two-tier system really is the most appropriate solution in the vast majority of situations.
Contrary to the schemes advocated by Balique (1989) and others, we think that the district should usually include no more than two levels. More specifically, we think that intermediate-level facilities (i.e. structures between health centres and hospitals) do not strengthen the system’s problem-solving capacity and that they increase the costs of the system.

118 J.-P. UNGER AND B. CRIEL
The following (not exhaustive) arguments may illustrate this position:
- if one such intermediate facility covers about 80000 people, then it will usually require more staff than eight distinct health centres covering 10 000 inhabitants: indeed, it will require approximately one doctor, 20 nurses and midwives instead of eight times one nurse, eight times one nurse-aid and eight times one clerk;
- the utilization of the buildings foreseen for these intermediate facilities has a poor efficiency, since generally one specific room is allocated to one specific activity (e.g. antenatal care, immunization, family planning, etc.). In a health centre, two rooms largely suffice for medical and nursing duties, provided that a proper timetable is designed (for instance, scheduling preventive activities in the afternoons);
- the quality of communication between staff and population is poor because it is less personalized; comprehensiveness and continuity of care are thus jeopardized;
- the care is as poorly integrated as it is in a hospital environment; - several health centres for that same population will obviously be located
much nearer to the communities they serve; a dialogue with the community; a necessary condition for community participation, then becomes possible;
- simulations show that overhead and operating budgets increase when the number of tiers increases;
- intermediate levels reduce the access to facilities located further upstream; and,
- the marginal benefit of in-patient facilities at an intermediate structure is low; in case of emergencies, patients will need to be referred to the hospital anyhow.
Minimal package of activities
If each level’s functions must be specific and its structures identical, then it is possible to describe a set of minimum activities common to all structures of a given level, i.e. the minimum activities package (MAP) (Unger and Dujardin, 1992). The MAP of a level is the standard medical output common to all structures bearing the same name in a given country. The definition of the MAP is important for planning purposes; more specifically, for a rational resource allocation minimizing opportunity costs. This implies that an efficient set of activities needs to be defined, matching the technologies and skills of each tier.
The World Bank (1993) has adopted the concept of the ‘essential clinical package’: ‘the most important factors in selecting the essential package should be the relative cost-effectiveness of interventions, the size and distribution of the health problems affecting the population, and the resources available’. This rationale - cost-effectiveness - is partly conflicting with another approach which consists of a planning of the health services’ package starting from the
HEALTH INFRASTRUCTURE PLANNING 119
bulk of the intersection between the community demands on the one hand and the needs defined by professionals on the other.
In fact, the two methods end up proposing a different array of activities (broad versus narrow MAP), one of them ruling out the possibility of delivering versatile curative care in public services. From this point of view, the public services of Northern Europe health systems (the Netherlands, the UK, Finland) strikingly contrast with the medical services of the USA. In Great Britain, for instance, Morrel (1 989) has proposed curative out-patient care, care and follow-up of chronic patients, preventive care, the organization of an information system, antenatal consultations, under-five clinics, care for the elderly, vaccination and screening activities. In countries such as Peru and Morocco, until recently, only prevention was allocated to first-line units. Curative medicine was delivered in ‘upper’ tiers, as if the health centres were unable to do so.
A broader scope of activities, including general practice curative care, has been advocated for first-line health services on the grounds of the following arguments:
- families are ‘health producing’ units. Physicians and nurses can only discuss the features of this production with them, provided that the health services meet the individual demands. Only then will services be able to deliver care acceptable to the patients;
- self-financing, even partial, cannot be considered if the services do not respond to the community demands (Abel Smith and Dua, 1988);
- the activities of health centres and hospitals cannot be defined by cost- effectiveness analysis. The identification of the MAP should find its roots in the features of managerial practice. Indeed, the MAP has been refined gradually over time. For instance, the versatile use of surgical tools in a district hospital has virtually yielded, in all African hospitals, a similar problem-solving capacity (Caesarean sections, extra-uterine pregnancies, appendectomy and strangulated hernias). Clearly, the rationale guiding the definition of the MAP shouid be a technical and managerial one, and not only a micro-economic one.
The definition of the MAP of the peripheral units is also shaped on practical experiences. In other words, it should be seen in a dynamic perspective. The MAP is a sum of activities that, once implemented in a given health centre, enables new interventions to be integrated without deeply modifying the organization or the cost of the structure. For instance, if a health centre is capable of providing continuous care for tuberculous patients, it can also ensure the follow-up of lepers without major changes.
MAPS are fairly homogeneous across subcontinent ensembles. In Africa, for instance, the health centre MAP should include curative care, under-five clinics, antenatal care, care and follow-up of chronic patients, nutritional rehabilitation, and family planning services. The MAP of a district hospital should include in-patient facilities with nursing expertise, a referral

120 3.4’. UNGER AND B. CRIEL
consultation, appropriate care for common medical and surgical emergencies (e.g. Caesarean section, strangulated hernia, extra-uterine pregnancy, appendectomy), maternity cases where complicated deliveries can be dealt with, laboratory and X-ray facilities.
Territorial responsibility and a discrete responsibility for populations
The population for which a given facility is responsible must be clearly and explicitly defined. In addition, tools should be designed so as to allow health centre staff to identify patients as being members (or not) of that population. The following arguments support this position:
- a more equitable distribution of care is possible; - an optimal ratio of population size per facility can be ensured; - an explicit responsibility for the health care of a population can only be
effective when it is clear for whom the staff are responsible; and, - in addition to the argument of effectiveness, efficiency is important: a scatter
of scarce resources over too large a population should be avoided, users must be brought to prefer to use ‘their’ facilities over any other (Wollast and Mercenier, 1971).
These facilities must have a territorial responsibility, or a population defined on the grounds of free affiliation or subscription up to a maximum figure, as in Great Britain or the Netherlands (GON, 1992). In the developing world, though, territorial responsibility is easier to implement due to transportation difficulties. The health centre will offer the entire gamut of minimal package activities to this well-defined population. This population will be the health services’ interlocutor and partner in a continuous process of dialogue: the health committee’s ‘constituency’ is thus defined. Finally, a clear identification of the population for which the health centre takes an explicit responsibility allows for an evaluation of the services delivered (knowledge of a denominator).
It is clear that it is impossible for a health centre to commit itself to deliver continuous, comprehensive and integrated care to people not belonging to that well-defined population. The health centre will never be able to achieve that commitment.
A necessary and sufficient population base
Simulations may be used to derive the increase in fixed costs when the number of facilities on a given level is increased. The population base per facility should be neither too small nor too large. If it is too small, it will be incompatible with the country’s resources. It will also threaten the technical quality of the care delivered. For example, the general practitioner of a small hospital that covers, say, 40000 people will perform approximately only 17 Caesarean sections a year (birth rate =0.043; rate of Caesarean sections= 1 %) and thus will gradually lose his surgical skills. Too large a population size reduces the
HEALTH INFRASTRUCTURE PLANNING 121
feasibility of a genuine dialogue between the health professional, the patients and their community. This balance is a local one, and will thus differ from one country to another. However, figures of one health centre per 10000 inhabitants and one district hospital per 150 000-300 000 inhabitants are recommendable for countries with very limited resources (manpower, equipment, financial resources). Assessments of the workload and the fixed costs of health centres and hospitals support that planning basis. For instance, an urban health centre covering 10000 people should be able to deliver each year approximately 12 000 curative consultations (30/day), 900 antenatal consultations (1 8/week), full immunizations and under-five clinics for 400 children.
Partial separation of the administrative and public health planning bases
Adopting administrative boundaries as the only basis of health planning generates great disparity in the facility/population ratios. The starting point for the planning of infrastructures should not be an adaptation of the structures’ sizes to the population of a given administrative area. The identification of the ‘catchment’ area (present or potential), i.e. an assessment of what population is using (or is going to use) which facility, is a more equitable and more rational basis. In some cases, there may be an entire overlap between the population of a given administrative area and the catchment population; in some cases, there is none or only a partial one. One should renounce the idea of superimposing per se operational health care units on administrative units.
It is advisable to divide up the country into operational health care units using a set of criteria referring to three different logics: (1) a demographic logic, which acknowledges the fact that the population size should be sufficiently small and sufficiently large at the same time; (2) an administrative logic, which acknowledges the fact that an overlap between administrative and operational units greatly facilitates the administration’s support for the public health services; and, (3) a sociological logic, which acknowledges the fact that a certain homogeneity of the population covered by an operational unit facilitates the processes of dialogue and community participation. The potential divergencies between the first two logics will remain limited in the planning process at regional or provincial level, but may be more pronounced at the lower levels of the health care pyramid (i.e. districts and health centres). Indeed, the increasing importance of community financing for the structures’ survival (in a context of local tax crisis) has made their geographical accessibility an overruling concern. In other words, the identification of the health centre’s areas does not have to match the administrative boundaries per se; this does not hamper the functioning of these first-line health services.
Balique (1989) advocates superimposing administrative entities and operational health care units. This enables one to abide by political pressures while claiming decisions to be in line with the planning basis. Decisions may then be justified by a scenario foreseeing a correction of non-priority deficiencies later on. However, these future adjustments are usually
122 J.-P. UNGER AND B. CRIEL
hypothetical due to resource constraints. The result is likely to be a very high proportion of ill-planned health facilities.
The rules of geographical division
When hospitals are too numerous, the following criteria may be used for the selection of future district hospitals among the existing structures: (1) the population size (financial viability of the district hospital and sufficient workload); (2) the distance between the most remote health centre and the district hospital, the transportation network and the existence of geographical barriers (geographical accessibility of the district hospital); (3) the amount of marginal investments required for the structure to function as a district hospital and the resources available.
The upper limit of the population to be covered by a district hospital is more relative than that of health centres. The following reasons support that position: a district hospital's costs are much higher and a larger population basis will increase its efficiency; moreover, it is generally much easier to increase its staff when this proves to be necessary. But, the main argument is really a conceptual one: a higher population basis for a district hospital, within reasonable limits of course, does not jeopardize the quality of the hospital services delivered. This is definitely not the case for a health centre, where too large a population precisely puts in jeopardy the very comprehensive and integrated nature of care at that level.
The geographical separation of health care facilities should also take into account current utilization patterns and natural population movements. This requires the occasional presence of national planners in the field. This approach, which consists of carving up the national territory into districts, is diametrically opposed to a scheme in which facilities are set up like supermarkets, i.e. based on market radii.
A given district should be divided into health areas along the following criteria (Pangu, 1988). The boundaries of the areas should be contiguous and respect the social and cultural population units. All the inhabitants of the area must have easy access to the health centre. The population of a given area must fit the one foreseen by the national model. The facility must be accessible to supervisors, preferably located in the main settlement of the area (and, thus, not necessarily at the geographic centre of the area), close to social and economical activity centres like markets. Existing buildings must be used when possible, but if they are ill-located it is more appropriate to build a new facility elsewhere (see, also, Assam et al., 1986).
Integrating non-governmental organizations (NGOs) into the system
An integration of NGO hospitals into national planning has considerable advantages: it allows governments to save on investment and operating costs, and it associates highly committed and skilled people in a national endeavour. The integration of NGOs should, however, be conditioned by the NGOs'
HEALTH INFRASTRUCTURE PLANNING 123
agreement to accept overall and explicit responsibility for a well-defined population and to operate within a system perspective: this may oppose a charitable approach to health care where a spontaneous reaction to human suffering overwhelms rational planning and action and it may run against proselytism.
HEALTH CARE STRATEGIES
The primary health care strategy
The Alma-Ata Conference of 1978 defined the primary health care strategy by generous principles, such as: reliance on community participation, decentralization of services, harmony between the health services’ characteristics and the country’s resources, importance of cultural aspects, search for equity, and integration of vertical programmes. On the basis of the previous principles, it is now possible to specify the interpretation of this concept, which is a strategy involving the reorientation of the entire health pyramid. Its main elements are as follows:
(a) Primary health care implies the development of $first-line health services (i.e. dispensaries or health centres) so as to make them accessible and functional through an improvement of curative care and by adding preventive activities to build the MAP. Later, health promotion activities can be added according to local possibilities and needs. Primary health care should not be reduced to social marketing, nor merely to the delivery of simple technologies such as all oral rehydration, malaria prophylaxis and breast-feeding, as suggested by Walsh and Warren (1979). Primary health care does not simply mean the deployment of village health workers, since they are unable to deliver care that would complement the existing skills and expertise of communities themselves.
Village health workers, however, can contribute to improve the action of first-line health services in remote or very scattered populations. Village health workers are to be seen as a specific solution for a specific, situational problem, but not more than that. Primary health care should not be confused with the implementation of one or two vertical programmes, nor with an isolated health promotion initiative such as the construction of latrines. Because the principle of specificity is usually overlooked, planners do not foresee urban health centres, arguing that their function can be taken over by the existing hospitals. In Africa, this leads to a very poor urban first-line coverage. Another common mistake is the development of vast first-line infrastructures (clinics) in urban settings, justified by the huge size of the covered population. The alternative option is to increase the number of units while reducing dramatically their size and population; as argued above, this would definitely benefit the quality of care provided.
(b) The second element of this strategy lies in the reorientation of hospital functions. The hospitals’ operations must be redirected to complement what is
124 J.-P. UNGER AND B. CRIEL
being done in the health centres (according to the principle of the specificity of each level). These structures should progressively increase their technology to solve more problems of referred patients; and, at the same time, reduce their first-line activities. Hence, the primary health care strategy does not mean a denial of technology: rather, this technology should be availed at the appropriate structure within the health system (Gentilini, 1989). Nor should primary health care be an exclusive choice between dispensaries and hospitals. On the contrary, the strategy implies a complementarity between hospitals and dispensaries.
(c) The third element is participation. The health centre really is the most appropriate level for community participation to take place. Indeed, the technical imperative of decisions made in a hospital inevitably transforms participation into community manipulation. Participation is a means to allow the population’s demands to be taken into account. Participation can only take place if a process of continuous dialogue between health services and community exists. The existence of such a dialogue is obviously conditioned by the extent to which the services provided are accepted by people, i.e. the extent to which they respond to people’s own demands. Only then may a participatory management of resources, a planning of activities fitting people’s preferences, a development of self-sufficiency and autonomy become possible.
District health systems
The provision of primary health care has stumbled over the lack of fine resource management and good knowledge of the particularities of the terrain. This has led to the insight that decision making should be decentralized (Vaughan et al., 1984). For several years, WHO has advocated a pivotal role for the district in service management and planning (WHO, 1987; PAHO, 1988).
The country representatives who attended the 1987 Harare Conference were mainly concerned with the wish to have their national structures legitimized by the label ‘district’. In a quest for consensus, while emphasizing the complementarity between the primary health care strategy, decentralization and strong district management teams, WHO (1985) had earlier remained vague and thus ambiguous on the district definition: ‘the lowest fully structured tier of a local government or of a decentralized administration’. On the basis of this definition, one could not rule out an interpretation of the district as a health centre surrounded by a network of village health workers. Later WHO documents, however, stated that the district should represent units defined on geographical and demographical grounds, conceived to facilitate the delivery of services and to enable an integration of the resources available (PaganiniJ989). One of these documents also stated that the district is to handle and manage the issue of community participation and that the districts should be fairly autonomous (WHO, 1986).
In fact, the district concept derives from two rationales: on the one hand, the implementation of the primary health care strategy, requesting a decentralized
HEALTH INFRASTRUCTURE PLANNING 125
management; and, on the other hand, the organization of integrated systems, which implies that one single team manages simultaneously the district hospital and the network of dispensaries. At the district level, the operational pyramid should closely overlap the administrative one, to enable professionals to identify deficiencies in the realm of health structures and to correct them through managerial changes.
In a broader sense, this managerial change requires one to:
- centralize and decentralize techniques from health centres to hospital and vice versa along the lines of continuous evaluation and resource fluctuation; and, to
-carry out activities on an integrated basis or a non-integrated basis, by respectively health centres and mobile team according to evaluation and political pressures. Thus, there is a very strong case for considering the hospital as an element cipart entiire of the district: district management also means district hospital management. This is in contradiction with Vaughan et al. (1984), according to whom the presence of a district hospital is facultative.
Commonly, the district represents the best level to merge bottom-up and top-down planning. The top-down planning generates a broad framework of standards, norms, instructions, programmes, definition of MAP, and so on. The bottom-up planning takes into account the specific desiderata and features of the population. Both should be married to allow optimal strategies to be designed that are adapted to the local context and that comply with the centrally designed framework.
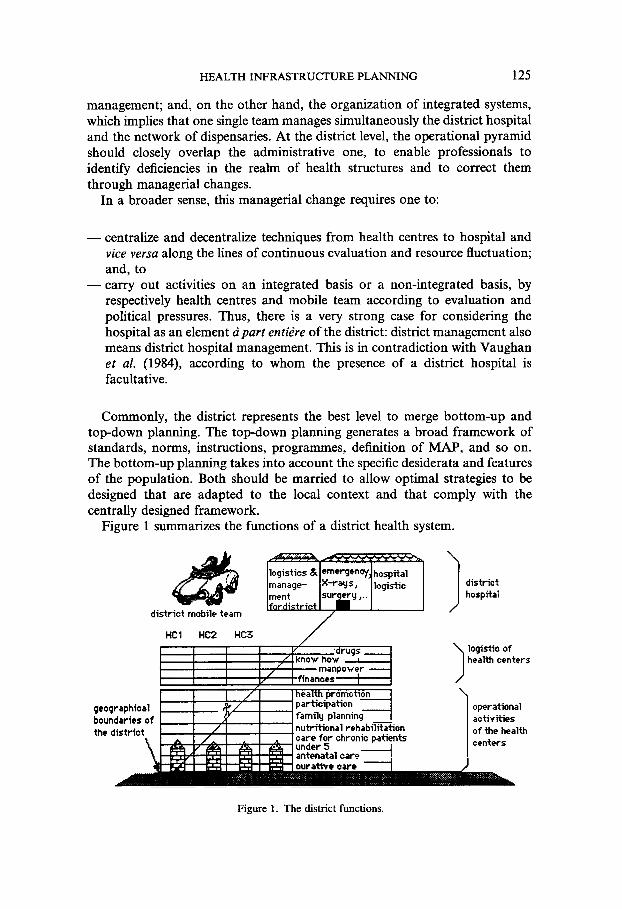
Figure 1 summarizes the functions of a district health system.
district hospital I logistic o f health centers
geographical boundaries o f the district
antenatal car
operational activities o f the health centers
Figure 1. The district functions.
126 J.-P. UNGER AND B. CRIEL
This scheme allows one to visualize:
(1) the responsibility of the district and its health centres for a geographically
(2) the delivery of a set of activities to be implemented in each dispensary (the
(3) the logistical and organizational functions which allow each unit to deliver
(4) the hierarchical relationships; and, ( 5 ) the patient flow in the system (referral and counter-referral).
well-defined population;
MAP);
these activities;
This scheme does not, however, show some of the functions the district hospital fulfils (Vaughan et al., 1984): indeed, very often the hospital is the place where medical assistants and students are trained, where first-line services are evaluated, where standardized clinical pathways are designed, where the epidemiological surveillance is centralized. In addition, it is often the venue where district decision-makers meet.
A district may also have a mobile team:
- to offer preventive activities to communities living too far from a health
- to deliver activities that cannot be integrated (yet); - to deliver activities that should not be integrated (e.g. epidemiological
surveillance, vector control, some health promotion activities like water and sanitation engineering);
centre;
- for emergency interventions (outbreaks for instance); and, - as a buffer to absorb priorities dictated by the agendas of donor agencies
and to avoid imbalances in health centres resulting from a process of crash integration (dracunculiasis control in Western Africa, for instance).
Again, just as for the health centre, the district’s size is a compromise, a trade-off between ‘smallness’ and ‘largeness’. It should be sufficiently small so as to mirror the local cultural, socioeconomic and demographic particularities of the area; and, to make bottom-up planning a feasible and sensible policy. It should be large enough to be an efficient entity with the necessary resources for a proper functioning of two tiers (at least in the vast majority of situations): i.e. a network of first-line health services and a hospital (Twaha et al., 1989).
The size of most districts in sub-Saharan Africa could vary between approximately 150 000 and 300 000 inhabitants and count from 10 to 30 health centres. If the resources available increase, it may be justified to pool them at a smaller scale: districts could then progressively become smaller without, however, going below a threshold where technical quality of care becomes endangered.
In areas with a scattered population, districts may be smaller if reasonable access to the district hospital is to be guaranteed. In such a situation, a three- tier system may be acceptable. A heterogeneous basis for planning districts
HEALTH INFRASTRUCTURE PLANNING 127
(two or three different types per country) is thus perfectly acceptable. It is an expression of a necessary flexibility vis-a-vis different situations. Obviously, smaller districts imply that the resources needed for their functioning are pooled for a smaller population base: this supposes some kind of national solidarity where relatively more resources are allocated to such districts.
In conclusion, the ‘reference system’, described as early as 1966 by Jolly and King, as a group of dispensaries and a reference hospital, corresponds to the district. However, if the whole is to function in an integrated way, then it is crucial that this group of structures is managed as a system. A team of health professionals, gathering both ‘hospital’ and ‘district’ staff, has 3 key role to play in that process. A consistent district management team is not only a more effective and efficient management body than an isolated district medical officer, it is also a more appealing and challenging way of working.
REFERENCES
Abel Smith, B., Dua, A. (1988). Community financing in developing countries: potential
Adekolu, J. (1979). The role of dispensaries in community health care in the Kainzi
Armstrong, D. (1979). The emancipation of biographical medicine. SOC. Sci. Med. 13A,
Assam, B. H., Akhtar, R., Askew, I. D. (1986). Applying operation research to health planning: locating health centres in Zambia. Health Policy and Planning 1(4), 326- 334.
Balique, H. (1989). Organisation ginirale des actions de santi au niveau piriphirique. In: La Sante‘ en Pays Tropicaux. Sous la direction de A. Rougemont et J. Brunet- Jailly. Doin kditeurs, Paris, 133.
Chiphangwi, J. (1987). Antenatal care in a district hospital. Trop. Doc. 17(3), 124-127. Criel, B., Van Balen, H. (1993). Paying for the Kasongo hospital in ZaYre: a conceptual
framework. Health Policy and Pfunning 8(1), 61-71. De Boer, C. N., McNeil, M. (1989). Hospital outreach community based health care:
the case of Chogoria, Kenya. SOC. Sci. Med. 28, 1007-1017. EVO (1971). Pour une politique de la santk. Groupe d‘itude pour une riforme de la
macine. Bruxelles. Gentilini (1989), quoted by J.-Y. Nau. Afrique: recherche mkdicale en souffrance. Le
Monde . GON (1992). Choices in Health Care. A report by the Government Committee on
choices in health care. The Netherlands: The Hague. Gwatkin, D. R., Berman, P., Burger, S. E. (1986). Health posts: are they contributing to
better health? PHN Technical Note 86-4. The World Bank, Washington. Jacobson, M. L., Labbok, M. H., Parker, R. L., Stevens, D. L., Carter, S. A. (1989). A
case study of the Tenwek hospital community health programme in Kenya. SOC. Sci. Med. 28, 1059-1062.
Jolly, R., King, M. (1966). The organization of health services. In: King, M. (Ed.). Medical Care in Developing Countries. A symposium from Makerere. Oxford University Press, Nairobi (2:4).
Kasongo (1981). Equipe du projet Kasongo. Le projet Kasongo. Ann. SOC. Belg. Med. Trop. 60, suppliment.
for the health sector. Health Policy and Planning 3(2), 95-108.
Lake area of Nigeria. J . Epi. Comm. Health 33, 145-149.
1-8.
128 J.-P. UNGER AND B. CRIEL
Morrel, D. (1989) The new general practitioner contract: is there an alternative? Br. Med. J. 289, 1005-1007.
OECD (1992). The Reform of Health Care: A Comparative Analysis of Seven Countries. Health Policy Studies No. 2, OECD, Paris (ch. 7 Netherlands, ch. 9 England).
Paganini, J. M. (1989). La salud en las grandes ciudades y 10s sistemas locales de salud. Bol sanit panam. 107(1), 65-73.
PAHO (1988). Organizacion Panamericana de la Salud. El desarrollo y fortalechiento de 10s sistemas locales de salud en la transfomacion de 10s sistemas nacionales de salud. Documento de trabajo CD33/14, XXXIII reunion del consejo directivo, Washington DC, septiembre-octubre 1988.
Pangu, K. A. (1988). Les soins de santt pour tous en l'an 2000, c'est possible. Thkse de doctorat B l'UniversitC Libre de Bruxelles.
Pearson, C. A. (1985). The role of hospitals in community health. In: Sofoluwe, G. O., Bennett, F. J. (Eds). Principles and Practice of Community Health in Africa. University Press Limited, Ibadan, 482.
Peeters, R. F., Stevens, F. C. J., Van der Zee, J. (1985). Basisgegevens van de Nederlanse en Belgische systemen van gezondheidszorg en sociale zekerheid bij ziekte en invaliditeit. Van Loghum Slaterus (Ed.).
Twaha, A., Ebrahim, G. J., Vogel, G. C. J., van Praagt, E. (1989). Lessons for national health systems from small-scale projects: a case study from Tanzania. J . Trop. Ped. 35, 4 w 3 .
Unger, J.-P., Dujardin, B. (1992). Epidemiology's contribution to health service management and planning in developing countries. Bulletin of WHO 70(4), 487-497.
Van Lerberghe, W. and Lafort, Y. (1990). The role of the hospital in the district: Current concerns. SHS paper, number 2. WHO/SHS/CC/90.2, WHO, Geneva, 5.
Van Lerberghe, W., Pangu, K. (1988). Comprehensive can be effective: the influence of coverage with a health centre network on the hospitalization patterns in the rural area of Kasongo, Zaire. SOC. Sci. Med, 26, 949-955.
Vaughan, J. P., Mills, A., Smith, D. (1984a). The importance of decentralised management. World Health Forum 5, 27-29.
Vaughan, P., Mills, A., Smith, D. (1984b). District health planning and management. EPC Publication No. 2. The London School of Hygiene and Tropical Medicine. Autumn 1984, 20.
Walsh, J. A., Warren, K. S. (1979). Selective primary health care. An interim strategy for disease control in developing countries. New Engl. J . Med. 301(18), 967-974.
WHO (1985). Renforcement des ministkres de la santt dans la perspective des soins de santt primaires. OMS, publication offset No. 82, Genke.
WHO (1986). WHO global program committee. Geneva. Doct WHO/SHS/DH/88.1/ Rev 1, 9.
WHO (1987a). Hbpitaux et santC pour tous. Strie de rapports techniques 744. Genkve. WHO (1987b). Report on the Interregional Meeting on Strengthening District Health
Systems Based on Primary Health Care. Harare, Zimbabwe, 3-7 August 1987. Geneva.
Wollast, E., Mercenier, P. (1971). Pour une rtgionalisation de l'organisation des soins. In: Groupe dktude pour une rtforme de la mkdecine. Pour une poh'tique a'e santt. Ed la revue nouvelle, Bruxelles, 95.
World Bank (1993). World Development Report. Investing in Health. The World Bank, Oxford University Press, Washington.
Related Documents











