Original article Primary gastrointestinal lymphoma in an Egyptian district: A study using a population-based cancer registry Magdy M. Saber a , Ahmed A. Zeeneldin a , Mohamed A. Samra a, * , Sarah A. Farag b a Department of Medical Oncology, National Cancer Institute, Cairo University, Egypt b Department of Medical Oncology, Tanta Cancer Center, Gharbiah, Egypt Received 11 January 2013; accepted 17 March 2013 Available online 28 April 2013 KEYWORDS Gastrointestinal lymphoma; Egypt; Gharbiah population-based cancer registry; Treatment; Outcomes; Survival Abstract Introduction: Gastrointestinal lymphoma (GIL) is the most common extranodal form of non-Hodgkin’s lymphoma (NHL) with geographical and age variation of its various subtypes. Aim: To study GIL in Gharbiah, Egypt and to recognize the treatments employed and their out- comes including survival. Methods: This is a retrospective study. Between 2000 and 2002, 40 adult patients with GIL were identified in the Gharbiah population based cancer registry (GPBCR); 26 cases of whom were trea- ted at Tanta Cancer Center (TCC). Results: GIL in Gharbiah, Egypt represented 6.2% of all GIT cancers. The median age was 47 years with slight male predominance. The commonest primary site was the stomach followed by the colon/rectum then the small intestine (67.5%, 25% and 7.5%, respectively). The commonest histological subtypes were the diffuse large B-cell (41.5%) followed by marginal zone B-cell (39%). The commonest symptoms were abdominal pains followed by vomiting. Only 18% of GILs were surgically resected. Most patients (77%) received chemotherapy with a 60% complete response (CR) rate. Once in CR, relapses are occasional. The median overall survival (OS) and progression free survival (PFS) were 31 and 14 months (95% CI, 13.2–48.7 and 6.4–21.6 months, respectively). Gastric primary site and diffuse large B cell subtype carry a non-significant worse OS and PFS than those of other sites and subtypes. * Corresponding author. Address: Department of Medical Oncology, National Cancer Institute, Cairo University, Kasr Eleini St., Foum El- Khalig square, Cairo, Egypt. E-mail address: [email protected] (M.A. Samra). Peer review under responsibility of The National Cancer Institute, Cairo University. Production and hosting by Elsevier Journal of the Egyptian National Cancer Institute (2013) 25, 95–101 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com 1110-0362 ª 2013 Production and hosting by Elsevier B.V. on behalf of National Cancer Institute, Cairo University. http://dx.doi.org/10.1016/j.jnci.2013.03.006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Original article
Primary gastrointestinal lymphoma in an Egyptian
district: A study using a population-based cancer registry
Magdy M. Saber a, Ahmed A. Zeeneldin a, Mohamed A. Samra a,*,
Sarah A. Farag b
a Department of Medical Oncology, National Cancer Institute, Cairo University, Egyptb Department of Medical Oncology, Tanta Cancer Center, Gharbiah, Egypt
Received 11 January 2013; accepted 17 March 2013Available online 28 April 2013
KEYWORDS
Gastrointestinal lymphoma;
Egypt;
Gharbiah population-based
cancer registry;
Treatment;
Outcomes;
Survival
Abstract Introduction: Gastrointestinal lymphoma (GIL) is the most common extranodal form of
non-Hodgkin’s lymphoma (NHL) with geographical and age variation of its various subtypes.
Aim: To study GIL in Gharbiah, Egypt and to recognize the treatments employed and their out-
comes including survival.
Methods: This is a retrospective study. Between 2000 and 2002, 40 adult patients with GIL were
identified in the Gharbiah population based cancer registry (GPBCR); 26 cases of whom were trea-
ted at Tanta Cancer Center (TCC).
Results: GIL in Gharbiah, Egypt represented 6.2% of all GIT cancers. The median age was
47 years with slight male predominance. The commonest primary site was the stomach followed
by the colon/rectum then the small intestine (67.5%, 25% and 7.5%, respectively). The commonest
histological subtypes were the diffuse large B-cell (41.5%) followed by marginal zone B-cell (39%).
The commonest symptoms were abdominal pains followed by vomiting. Only 18% of GILs were
surgically resected. Most patients (77%) received chemotherapy with a 60% complete response
(CR) rate. Once in CR, relapses are occasional. The median overall survival (OS) and progression
free survival (PFS) were 31 and 14 months (95% CI, 13.2–48.7 and 6.4–21.6 months, respectively).
Gastric primary site and diffuse large B cell subtype carry a non-significant worse OS and PFS than
those of other sites and subtypes.
* Corresponding author. Address: Department of Medical Oncology,
National Cancer Institute, Cairo University, Kasr Eleini St., Foum El-
Khalig square, Cairo, Egypt.
E-mail address: [email protected] (M.A. Samra).
Peer review under responsibility of The National Cancer Institute,
Cairo University.
Production and hosting by Elsevier
Journal of the Egyptian National Cancer Institute (2013) 25, 95–101
Cairo University
Journal of the Egyptian National Cancer Institute
www.nci.cu.adu.egwww.sciencedirect.com
1110-0362 ª 2013 Production and hosting by Elsevier B.V. on behalf of National Cancer Institute, Cairo University.
http://dx.doi.org/10.1016/j.jnci.2013.03.006

Conclusions: GILs in Gharbiah, Egypt are characterized by predominance of male gender, gastric
site and marginal zone histology. Survival is worse for gastric and diffuse large B-cell GILs com-
pared to other sites and histologies.
ª 2013 Production and hosting by Elsevier B.V. on behalf of National Cancer Institute, Cairo University.
Introduction
Gastrointestinal tract is the most common extranodal site in-volved by lymphoma accounting for 5%–20% of all cases[1,2]. However, primary gastrointestinal lymphoma (GIL) is
very rare, constituting only about 1%–4%of all gastrointestinalmalignancies. Although lymphoma can involve any part of thegastrointestinal tract, the most frequent sites among adults are
the stomach followed by the small intestine and ileocecal region[3]. In the pediatric age group, small and large intestines are themost frequent sites [4].Diffuse largeB-cell (DLBC) lymphoma is
the most common pathological subtype in all sites of the gastro-intestinal tract. Nevertheless, the frequency of other subtypeshas recently increased in certain regions of the world [3].
GILs can be associated with chronic inflammation that
forms the basis of understanding the mucosa associated lym-phoid tissue (MALT) lymphomas. However, chronic inflam-mation can also pose diagnostic difficulties [5,6]. While
chronic gastritis due to Helicobacter pylori is the best-studiedprecursor of MALT lymphoma, other parts of the GIT dem-onstrate precursor inflammatory lesions that lead to specific
types of lymphoma [7].The diagnostic difficulties for GILs are compounded by the
fact that often only small biopsies are available for examina-
tion and the morphology of a particular type of lymphomamay differ in the GIT compared to the lymph node. Several re-cent large series describing the epidemiological and clinico-pathological features of primary GIT lymphomas have been
published [3,8–14]. The advent of wireless capsule endoscopyand double balloon enteroscopy has made previously inacces-sible portions of GIT visible and changed our perceptions
about some types of GILs. Finally, the increasing number ofimmunosuppressed patients (either due to HIV or iatrogenic)is associated with increasing incidence of some types of GILs
that were very rarely seen previously [15–18].Staging of GILs is a matter of debate due to various avail-
able staging systems. Although the modified Ann Arbor classi-fication is feasible and relevant for prognosis, certain demerits
in terms of disseminated and incurable infiltration of the GITprompted development of the Paris staging system, which candifferentiate distant lymphoma manifestations depending on
the involved organ (using endoscopic ultrasound), and furthersubdivide lymph node involvement [19].
In this retrospective study, we reviewed the clinicopatho-
logic characteristics and treatment outcomes of 40 adult pa-tients with GIL identified at the Gharbiah population basedcancer registry (GPBCR) in Egypt.
Methods
This is a retrospective study. Patients with GILs were identified
through GPBCR. Data on age, sex, sub-site, histology, grade,stage and treating center were obtained from the registry.Further data on complaints, comorbidities, treatment modali-
ties (surgery, radiotherapy and chemotherapy), response to
therapy, dates of diagnosis, surgery and relapse; and survivalwere obtained for that subset of patients treated at Tanta Can-cer Center (TCC). The study was approved by the IRB of the
Egyptian National Cancer Institute.Inclusion criteria were patients with GIL (site codes) and a
malignant histology [histology codes (ICD-O-3)] between 2000and 2002. Exclusion criteria were non-confirmed histologic
subtype as those diagnosed based on death certificate, radiol-ogy or malignant neoplasm unspecified.
Between 2000 and 2002, 42 cases with GILs contained in
GPBCR were identified. Two cases were excluded; one diag-nosed from death certificate and another had the diagnosisof NHL with no subtype identified. Patients’ files were re-
viewed for clinical and pathologic data, details of treatmentsand their outcome including response and survival.
Statistical analysis
All analyses were done using SPSS� software program version15 (Chicago, USA). Nominal and categorical data were com-
pared for different histologies (Diffuse large B vs. others)and subsites (gastric vs. others) using the Chi squared test orFisher’s exact test. Survival was calculated using the KaplanMeier method and groups were compared using the Log-rank
test. A probability (p) < 0.05 (two sided) was considered sta-tistically significant.
Results
GPBCR patients
GILs represented 6.2% of GIT cancers in GPBCR. All GILswere of the non-Hodgkin’s lymphoma (NHL) type. The med-
ian age was 47 years (range, 20–77 years) with slight male pre-dominance (male to female ratio of 1.2:1). The stomach wasthe commonest involved site followed by the colon/rectum
and small intestine (67.5%, 25% and 7.5%, respectively).The gastric antrum and the cecum were the commonest sub-sites. Most patients (29/40) had either local or regional disease.Seven patients had a widespread disease to the liver (2 cases),
lungs (2 cases), bone (1 case) or unknown sites (2 cases). Dif-fuse large B-cell (DLBC) subtype was the commonest subtype(41.5%) followed by the marginal-zone B-cell (MZ) subtype
(39%). Other subtypes included diffuse mixed small and largecell (3 cases), B-cell Small lymphocytic (2 cases), mantel cell (1case) and follicular (1 case). Most DLBC (11/17) and MZ (13/
16) were located in the stomach. Table 1 shows the character-istics of the 40 GIL patients identified through GPBCR.
Tanta Cancer Center (TCC) patients
We could identify 26 cases treated at TCC, the main oncologycenter in Gharbiah governorate, Egypt. Their characteristics
96 M.M. Saber et al.
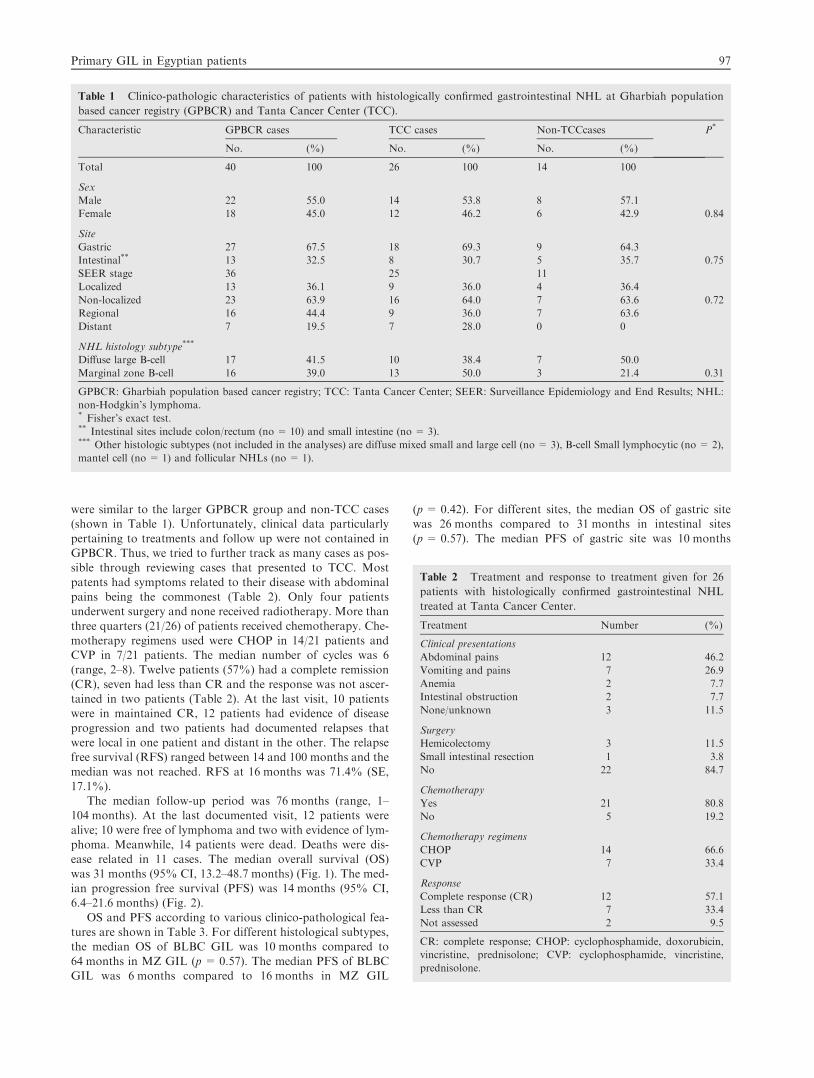
were similar to the larger GPBCR group and non-TCC cases(shown in Table 1). Unfortunately, clinical data particularly
pertaining to treatments and follow up were not contained inGPBCR. Thus, we tried to further track as many cases as pos-sible through reviewing cases that presented to TCC. Most
patents had symptoms related to their disease with abdominalpains being the commonest (Table 2). Only four patientsunderwent surgery and none received radiotherapy. More than
three quarters (21/26) of patients received chemotherapy. Che-motherapy regimens used were CHOP in 14/21 patients andCVP in 7/21 patients. The median number of cycles was 6(range, 2–8). Twelve patients (57%) had a complete remission
(CR), seven had less than CR and the response was not ascer-tained in two patients (Table 2). At the last visit, 10 patientswere in maintained CR, 12 patients had evidence of disease
progression and two patients had documented relapses thatwere local in one patient and distant in the other. The relapsefree survival (RFS) ranged between 14 and 100 months and the
median was not reached. RFS at 16 months was 71.4% (SE,17.1%).
The median follow-up period was 76 months (range, 1–104 months). At the last documented visit, 12 patients were
alive; 10 were free of lymphoma and two with evidence of lym-phoma. Meanwhile, 14 patients were dead. Deaths were dis-ease related in 11 cases. The median overall survival (OS)
was 31 months (95% CI, 13.2–48.7 months) (Fig. 1). The med-ian progression free survival (PFS) was 14 months (95% CI,6.4–21.6 months) (Fig. 2).
OS and PFS according to various clinico-pathological fea-tures are shown in Table 3. For different histological subtypes,the median OS of BLBC GIL was 10 months compared to
64 months in MZ GIL (p = 0.57). The median PFS of BLBCGIL was 6 months compared to 16 months in MZ GIL
(p= 0.42). For different sites, the median OS of gastric sitewas 26 months compared to 31 months in intestinal sites
(p= 0.57). The median PFS of gastric site was 10 months
Table 2 Treatment and response to treatment given for 26
patients with histologically confirmed gastrointestinal NHL
treated at Tanta Cancer Center.
Treatment Number (%)
Clinical presentations
Abdominal pains 12 46.2
Vomiting and pains 7 26.9
Anemia 2 7.7
Intestinal obstruction 2 7.7
None/unknown 3 11.5
Surgery
Hemicolectomy 3 11.5
Small intestinal resection 1 3.8
No 22 84.7
Chemotherapy
Yes 21 80.8
No 5 19.2
Chemotherapy regimens
CHOP 14 66.6
CVP 7 33.4
Response
Complete response (CR) 12 57.1
Less than CR 7 33.4
Not assessed 2 9.5
CR: complete response; CHOP: cyclophosphamide, doxorubicin,
vincristine, prednisolone; CVP: cyclophosphamide, vincristine,
prednisolone.
Table 1 Clinico-pathologic characteristics of patients with histologically confirmed gastrointestinal NHL at Gharbiah population
based cancer registry (GPBCR) and Tanta Cancer Center (TCC).
Characteristic GPBCR cases TCC cases Non-TCCcases P*
No. (%) No. (%) No. (%)
Total 40 100 26 100 14 100
Sex
Male 22 55.0 14 53.8 8 57.1
Female 18 45.0 12 46.2 6 42.9 0.84
Site
Gastric 27 67.5 18 69.3 9 64.3
Intestinal** 13 32.5 8 30.7 5 35.7 0.75
SEER stage 36 25 11
Localized 13 36.1 9 36.0 4 36.4
Non-localized 23 63.9 16 64.0 7 63.6 0.72
Regional 16 44.4 9 36.0 7 63.6
Distant 7 19.5 7 28.0 0 0
NHL histology subtype***
Diffuse large B-cell 17 41.5 10 38.4 7 50.0
Marginal zone B-cell 16 39.0 13 50.0 3 21.4 0.31
GPBCR: Gharbiah population based cancer registry; TCC: Tanta Cancer Center; SEER: Surveillance Epidemiology and End Results; NHL:
non-Hodgkin’s lymphoma.* Fisher’s exact test.** Intestinal sites include colon/rectum (no = 10) and small intestine (no = 3).*** Other histologic subtypes (not included in the analyses) are diffuse mixed small and large cell (no = 3), B-cell Small lymphocytic (no = 2),
mantel cell (no = 1) and follicular NHLs (no = 1).
Primary GIL in Egyptian patients 97

compared to 16 months in intestinal sites (p = 0.94). Patientswho received CHOP had a median OS of 64 months comparedto 31 months in those who received CVP (p = 0.75). The med-
ian PFS was 64 months with CHOP compared to 9 monthswith CVP (p = 0.48).
Discussion
In our series, GILs represented a minority of all GIT cancers(6.2%), which is comparable to an incidence of 4% reported
by the literature [20–22].Males were slightly more affected than females in our study
with a male to female ratio of 1.2:1 which is lower than whathas been reported from the West (1.74:1) [23]; Jordon
(2.8:1)[24]; and India (1.9:1) [20,25]; but it is close to the ratioreported from Thailand (1.4:1) [26]; China (1.2:1) (1.18:1)[27,28]; and Japan (1.2:1) [8].
The median age of patients in our study was 47 years. Thisage was relatively younger than that shown in 2 studies fromChina reporting a median age of 53 years [26,28]; and of
56 years in Singapore [29]. Other studies revealed youngerage of patients e.g. mean age 21 and 34 years in two studiesfrom India respectively [20,25] and of 35 years in Saudi Arabia
[30] reflecting the variable geographic characteristics of the dis-ease. H. pylori infection, immunosuppression after solid-organtransplantation, celiac disease, inflammatory bowel disease,and human immunodeficiency virus (HIV) infection may be
risk factors for GILs [21]. Given the retrospective nature ofthe current study, data on these risk factors especially H. pyloriinfection were not documented.
The commonest symptoms in our series were abdominalpains (46%) followed by vomiting (27%), similar to commonsymptoms reported by other studies [25,27,31–34].
A difference in prognosis and distribution of GILs has beenreported in Western and Middle Eastern countries. GILs werereported to be located more frequently in the stomach in the
West, but more frequently in the small intestine in the East,although this was shown to be contrary in the recent years. In-creased incidence of GIL in the small intestine was thought to
be due to higher incidence of immunoproliferative small intes-tinal disease in the Middle East [35]. Stomach is the common-est involved site in our study (69%). This finding is comparableto most studies of GILs [8,26–29,31,36,37] reporting gastric
involvement that ranges between 56% and 81%. Series fromJordon [38]; Kuwait [39] and Nigeria [40] reported higher prev-alence of small intestinal GILs. However, other investigators
from the Middle East i.e. Saudi Arabia, reported involvementof gastric site in 51% of patients [30]. Unlike Cirillio et al. [37]and Koniaris et al. [41], our large intestine GILs (27%) ex-
ceeded those of the small intestine (4%). Our low figures ofsmall intestinal GILs are mainly because of exclusion of pedi-atric patients where intestinal GILs predominate [42,43]. Thismay also be a random variation associated with a relatively
low number of cases.Similar to most studies, diffuse large B-cell (DLBC) NHL
was the commonest subtype followed by marginal zone (MZ)
NHL [26–27,29,44]. In Japan, MZ subtype slightly exceededDLBC subtype [8] and this may reflect the geographic varia-tion [33].
Similar to many studies [28–29,31], most patients (81%) ofthe current study received chemotherapy. However, surgerywas less encountered in our study (16%) and this may reflect
temporal evolution of the treatment of GILs with a decreasingrole of surgery and increasing that of radiation therapy andsystemic therapy [8]. The complete response (CR) rate afterchemotherapy in our series was 57% which is comparable to
Figure 1 Overall survival of the 26 patients with gastrointestinal NHL treated at Tanta Cancer Center (TCC).
98 M.M. Saber et al.

that seen in other studies [28–29,32,45] reporting CR rates thatrange between 52% and 67%.
In our study, the median OS and PFS rates were 31 and14 months respectively; and the two-year OS and PFS rates
were 56% and 41% respectively. Survival rates in the currentstudy were similar to those reported by many studies [29,32–
33,45–46]. Higher 2-year OS (67%) was reported in a studyfrom Singapore [29]. Also, Cirillio et al. [37] reported a median
Figure 2 Progression-free survival of 26 patients with gastrointestinal NHL treated at Tanta Cancer Center (TCC).
Table 3 Overall survival (OS) and progression free survival (PFS) of patients with gastrointestinal NHL treated at Tanta Cancer
Center.
Variable No. OS PFS
Median
(months)
1-y rate (SE)
(%)
2-y rate (SE)
(%)
p Median
(months)
1-y rate (SE)
(%)
2-y rate (SE)
(%)
p
All patients 26 31 62 (10.1) 56 (10.6) – 14 51 (10.2) 41 (10.6) –
Sex
Female 12 26 70.0 (14.5) 58.3 (16.1) 0.95 10 45.8 (15.0) 27.5 (13.5) 0.41
Male 14 42 55.6 (13.6) 55.6 (13.6) 42 55.6 (13.6) 55.6 (13.6)
Site
Gastric 18 26 62.7 (12.1) 53.8 (13.3) 10 47.2 (12.1) 39.4 (12.4)
Intestinal 8 31 62.5 (17.1) 62.5 (17.1) 0.57 16 62.5 (17.1) 46.9 (18.7) 0.96
Histologic subtypes*
DLBC 10 10 44.4 (16.6) 44.4 (16.6) 6 40.0 (15.5) 26.7 (15.0)
MZ 13 64 65.3 (14.2) 65.3 (14.2) 0.37 16 56.3 (14.8) 45.0 (15.6) 0.42
Stage
I 9 64 58.3 (18.6) 58.3 (18.6) 64 51.9 (17.6) 51.9 (17.6)
II 9 42 50.8 (17.7) 50.8 (17.7) 10 44.4 (16.6) 44.4 (16.6)
IV 7 26 71.4 (17.1) 53.6 (20.1) 0.8 14 57.1 (18.7) 19.0 (16.8) 0.94
Chemotherapy regimen
CVP 7 31 66.7 (19.2) 66.7 (19.2) 9 50.0 (20.4) 25 (20.4)
CHOP 14 64 76.2 (12.1) 66.6 (13.8) 0.75 64 62.9 (13.3) 53.9 (14.1) 0.48
1-y rate: one-year rate; 2-y rate: two-year rate; SE: standard error; NR: not reached; MZ: marginal zone NHL; DLBC: diffuse large B cell NHL;
CVP: cyclophosphamide, vincristine, prednisolone; CHOP: cyclophosphamide, doxorubicin, vincristine, prednisolone.* Other histologic subtypes are not included in the analyses.
Primary GIL in Egyptian patients 99

OS of 54 months, with 46% of patients surviving at 5 years.Liang et al. [28] reported the experience in the managementof 425 Chinese patients with primary GILs in Hong Kong over
a period of 18 years. The OS of all patients was 45% at 5 years.Multivariate analysis revealed that age below 60 years, lowgrade histology, stage I or II disease and absence of bulky tu-
mor were independent prognostic factors predicting better OS.Similar to several studies [28,46,47], MZ subtype had a bet-
ter prognosis than other subtypes included in our study partic-
ularly DLBC.In our study, gastric involvement had a better OS and PFS
than intestinal involvement. However, the difference did notreach statistical significance. In a 15-year review of 75 cases of
GILs from North India and after a mean follow-up of 4 years,the 5-year OS rates were 34%, 25% and 16% for stages I, II,or >II, respectively. The survival rate was significantly better
for gastric location (44%) compared to other sites (24%)(p < 0.01) [25]. The 30-year experience of primary GILs (49cases) at the Cancer Institute, Madras, India revealed that 5-
year OS and DFS rates were 47% and 40%, respectively. Therewas no overall significant difference in survival between the dif-ferent treatment groups. Stage, extent of surgical resection, re-
sponse to treatment, serosal involvement, multimodalitytreatment, and performance status were significant prognosticfactors. Achievement of complete remission and complete surgi-cal resection were the most favorable independent prognostic
factors on multivariate analyses [45]. In a study of the 185 pa-tients with primaryGILs fromSaudiArabia, patientswith intes-tinal lymphoma had a 10-year survival rate of 48% comparable
to 53% in those with gastric lymphoma (p = 0.431) [30].Our study has strengths and limitations. To the best our
knowledge, it is the first study fromEgypt that addresses the issue
ofGILs on the population level. The retrospective nature impliessomemissing data as these data were originally collected for rea-sons other than research.Moreover, the medical service in Egypt
is spannedamongmanyproviders like theministry of health,mil-itary, educational aswell as private hospitalsmaking accessibilityto complete patients’ information in all of these settings a difficulttask. However, the study accurately reflects the practice of the
oncology community within the jurisdictions of the study.In conclusions, in our trial, GIT NHL represents 6.2% of
all GIT cancers. The median age is 47 years with slight male
predominance. The commonest primary site is the stomachfollowed by the colon/rectum. The commonest histologicalsubtype is Marginal zone B-cell followed by the diffuse large
B-cell. Most patients are treated with chemotherapy that gives60% complete response rate. Once in CR, relapses are occa-sional. The median OS and PFS are relatively short as 31and 14 months, respectively. Gastric primary site and diffuse
large B cell subtype carry a non-significant worse OS andPFS that other sites and subtypes. Better classification of theprimary GILs and more refined stratification of the patients
according to the prognostic variables may allow individualiza-tion of treatment. Prospective studies are essential to define theunderlying causative or risk factors as well as the relative roles
of surgery, chemotherapy and radiotherapy.
References
[1] d’Amore F, Brincker H, Gronbaek K, Thorling K, Pedersen M,
Jensen MK, et al. Non-Hodgkin’s lymphoma of the
gastrointestinal tract: a population-based analysis of incidence,
geographic distribution, clinicopathologic presentation features,
and prognosis. Danish lymphoma study group. J Clin Oncol
1994;12:1673–84.
[2] Wu XC, Andrews P, Chen VW, Groves FD. Incidence of
extranodal non-Hodgkin lymphomas among whites, blacks, and
Asians/Pacific Islanders in the United States: anatomic site and
histology differences. Cancer Epidemiol 2009;33:337–46.
[3] Ghimire P, Wu P, Zhu L. Primary gastrointestinal lymphoma.
World J Gastroenterol 2011;17(6):697–707.
[4] Ford EG. Gastrointestinal tumors. In: Andrassy R, editor.
Pediatric surgical oncology. Philadelphia, PA: WB Saunders
Co.; 1998. p. 289–304.
[5] Isaacson PG. Mucosa-associated lymphoid tissue lymphoma.
Semin Hematol 1999;36:139–47.
[6] Isaacson PG, Du MQ. MALT lymphoma: from morphology to
molecules. Nat Rev Cancer 2004;4:644–53.
[7] Cardona DM, Layne A, Lagoo AS. Lymphomas of the gastro-
intestinal tract – pathophysiology, pathology, and differential
diagnosis. Indian J Pathol Microbiol 2012;55:1–16.
[8] Nakamura S, Matsumoto T, Iida M, Yao T, Tsuneyoshi M.
Primary gastrointestinal lymphoma in Japan: a
clinicopathologic analysis of 455 patients with special reference
to its time trends. Cancer 2003;97:2462–73.
[9] Wong MT, Eu KW. Primary colorectal lymphomas. Colorectal
Dis 2006;8:586–91.
[10] Dionigi G, Annoni M, Rovera F, Boni L, Villa F, Castano P,
et al. Primary colorectal lymphomas: review of the literature.
Surg Oncol 2007;16(Suppl. 1):S169–71.
[11] Gustafsson BI, Siddique L, Chan A, Dong M, Drozdov I, Kidd
M, et al. Uncommon cancers of the small intestine, appendix
and colon: an analysis of SEER 1973–2004, and current
diagnosis and therapy. Int J Oncol 2008;33:1121–31.
[12] Schottenfeld D, Beebe-Dimmer JL, Vigneau FD. The
epidemiology and pathogenesis of neoplasia in the small
intestine. Ann Epidemiol 2009;19:58–69.
[13] Arora N, Manipadam MT, Pulimood A, Ramakrishna BS,
Chacko A, Kurian SS, et al. Gastrointestinal lymphomas:
pattern of distribution and histological subtypes: 10 years’
experience in a tertiary center in South India. Indian J Pathol
Microbiol 2011;54:712–9.
[14] Kassira N, Pedroso FE, Cheung MC, Koniaris LG, Sola JE.
Primary gastrointestinal tract lymphoma in the pediatric patient:
review of 265 patients from the SEER registry. J Pediatr Surg
2011;46:1956–64.
[15] Nguyen DD, Loo Jr BW, Tillman G, Natkunam Y, Cao TM,
Vaughan W, et al. Plasmablastic lymphoma presenting in a
human immunodeficiency virus-negative patient: a case report.
Ann Hematol 2003;82:521–5.
[16] Nicol I, Boye T, Carsuzaa F, Feier L, Collet Villette AM, Xerri
L, et al. Post-transplant plasmablastic lymphoma of the skin. Br
J Dermatol 2003;149:889–91.
[17] Dong HY, Scadden DT, de Leval L, Tang Z, Isaacson PG,
Harris NL. Plasmablastic lymphoma in HIV-positive
patients: an aggressive Epstein-Barr virus-associated
extramedullary plasmacytic neoplasm. Am J Surg Pathol
2005;29:1633–41.
[18] Castillo J, Pantanowitz L, Dezube BJ. HIV-associated
plasmablastic lymphoma: lessons learned from 112 published
cases. Am J Hematol 2008;83:804–9.
[19] Di Raimondo F, Caruso L, Bonanno G, Naso P, Chiarenza A,
Fiumara P, Bari A, Palumbo GA, Russo A, Giustolisi R. Is
endoscopic ultrasound clinically useful for follow-up of gastric
lymphoma? Ann Oncol 2007;18:351–6.
[20] Gupta S, Pant GC, Gupta S. A clinicopathological study of
primary gastrointestinal lymphoma. J Surg Oncol
1981;16(1):49–58.
[21] Crump M, Gospodarowicz M, Shepherd FA. Lymphoma of the
gastrointestinal tract. Semin Oncol 1999;26(3):324–37.
100 M.M. Saber et al.

[22] Rajesh KN. Clinicopathologic characteristics and therapeutic
outcome of primary gastrointestinal lymphoma in Cuddalore
district in India. Int J Biol Med Res 2012;2(4):1419–22.
[23] Ducreux M, Boutron1 M-C, Piard F, Carli P-M, Faivre J. A 15-
year series of gastrointestinal non-Hodgkin’s lymphomas: a
population-based study. Br J Cancer 1998;77(3):511–4.
[24] Bani-Hani KE, Yaghan RJ, Matalka II. Primary gastric
lymphoma in Jordan with special emphasis on descriptive
epidemiology. Leuk Lymphoma 2005;46(9):1337–43.
[25] Singh DP, Sharma SC, Sandhu AP, Goenka MK, Kochhar R,
Nagi B, Sur RK, Patel FD, Ayyagari S, Bhatia SS,
Mukhopadhyay P, Xavier S, Bhasin D, Singh K, Wig JD,
Gupta NM, Das A, Gupta BD. Primary gastrointestinal
lymphoma–disease spectrum and management: a 15-year
review from north India. Indian J Gastroenterol
1997;16(3):88–90.
[26] Sukpanichnant S, Udomsakdi-Auewarakul C, Ruchutrakool T,
Leelakusolvong S, Boonpongmanee S, Chinswangwatanakul V.
Gastrointestinal lymphoma in Thailand: a clinicopathologic
analysis of 120 cases at Siriraj Hospital according to WHO
classification. Southeast Asian J Trop Med Public Health
2004;35(4):966–76.
[27] Todd D. Fourth Seah Cheng Siang Memorial Lecture. Primary
gastrointestinal lymphoma in Hong Kong. Ann Acad Med
Singapore 1994;23(3):430–6.
[28] Liang R, Todd D, Chan TK, Chiu E, Lie A, Kwong YL, Choy
D, Ho FC. Prognostic factors for primary gastrointestinal
lymphoma. Hematol Oncol 1995;13(3):153–63.
[29] Au E, Ang PT, Tan P, Sng I, Fong CM, Chua EJ, Ong YW.
Gastrointestinal lymphoma–a review of 54 patients in
Singapore. Ann Acad Med Singapore 1997;26(6):758–61.
[30] Amer MH, El-Akkad S. Gastrointestinal lymphoma in adults:
clinical features and management of 300 cases. Gastroenterology
1994;106(4):846–58.
[31] Rackner VL, Thirlby RC, Ryan Jr JA. Role of surgery in
multimodality therapy for gastrointestinal lymphoma. Am J
Surg 1991;161(5):570–5.
[32] Shukla K, Patel T, Shukla J, Palanki S. Primary gastrointestinal
lymphoma–a clinicopathologic study. Indian J Pathol Microbiol
2007;50(2):296–9.
[33] Feng L, Zhang G, Hu Z, Zou Y, Chen F, Zhang G, Tang L.
Diagnosis and treatment of 81 patients with primary
gastrointestinal lymphoma. J Cent S Univ Med Sci
2009;34(7):582–8.
[34] Boot H. Diagnosis and staging in gastrointestinal lymphoma.
Best Pract Res Clin Gastroenterol 2010;24:3–12.
[35] Atalay C, Kanlıoz M, Demir S, Pak I, Altınok M. Primary
gastrointestinal lymphomas. Acta Chir Belg 2003;103:616–20.
[36] Aozasa K, Tsujimoto M, Inoue A, Nakagawa K, Hanai J,
Kurata A, Nosaka J. Primary gastrointestinal lymphoma. A
clinicopathologic study of 102 patients. Oncology
1985;42(2):97–103.
[37] Cirillo M, Federico M, Curci G, Tamborrino E, Piccinini L,
Silingardi V. Primary gastrointestinal lymphoma: a
clinicopathological study of 58 cases. Haematologica
1992;77(2):156–61.
[38] Tarawneh MS. Non-Hodgkin’s lymphomas in Jordanians: a
histopathological study of 231 cases. Hematol Oncol
1986;4:91–9.
[39] Omar YT, Al-Nakib B, Jacob GS, Ali SM, Temmim L,
Radhakrishnan S, Fayaz MS. Primary gastrointestinal
lymphoma in Kuwait. An 11-yr retrospective analysis of 108
cases. Eur J Cancer Clin Oncol 1985;21(5):573–7.
[40] Afolayan EA, Anjorin AS. Incidence of primary extranodal
lymphoma involving gastrointestinal tract by histological type at
Ilorin. Niger J Med 2001;10:135–8.
[41] Koniaris LG, Drugas G, Katzman PJ, Salloum R. Management
of gastrointestinal lymphoma. J Am Coll Surg 2003
Jul;197(1):127–41.
[42] Takahashi H, Hansmann ML. Primary gastrointestinal
lymphoma in childhood (up to 18 years of age). A
morphological, immunohistochemical and clinical study. J
Cancer Res Clin Oncol 1990;116(2):190–6.
[43] Morsi A, Abd El-Ghani Ael-G, El-Shafiey M, Fawzy M, Ismail
H, Monir M. Clinico-pathological features and outcome of
management of pediatric gastrointestinal lymphoma. J Egypt
Natl Cancer Inst 2005;17(4):251–9.
[44] Harris NL, Jaffe ES, Stein H, et al. A revised European-
American classification of lymphoid neoplasms: a proposal from
the international lymphoma study group. Blood
1994;84:1361–92.
[45] Chandran RR, Raj EH, Chaturvedi HK. Primary
gastrointestinal lymphoma: 30-year experience at the Cancer
Institute, Madras, India. J Surg Oncol 1995;60(1):41–9.
[46] Song LP, Hou HL, Zhao H, Zheng W, Zhang L, Gao J. Clinical
study of 22 cases of primary gastrointestinal lymphoma. Ai
Zheng 2004;23(6):685–8.
[47] Nakamura S, Akazawa K, Yao T, Tsuneyoshi M. A
clinicopathologic study of 233 cases with special reference to
evaluation with the MIB-1 index. Cancer 1995;76:1313–24.
Primary GIL in Egyptian patients 101
Related Documents











