-
8/10/2019 Primary Cleft Lip Repair
1/16
CME
Primary Repair of Bilateral Cleft Lip andNasal Deformity
John B. Mulliken, M.D.
Boston, Mass.
Learning Objectives: After studying this article, the participant should be able to: 1. List five principles that guidesynchronous repair of bilateral complete cleft lip and nasal deformity. 2. Explain how different growth rates for theprincipal nasolabial features are applied during primary repair. 3. Describe two approaches for positioning the alarcartilages to form the columella. 4. Discuss the influences on referral patterns for a newborn with bilateral cleft lip.
Traditional repair of bilateral cleft lip focused on labialclosure but accentuated the nasal deformities, which wereaddressed later. By the end of the past century, single-staged labial closure had replaced the old multistagedprocedures and the technical emphasis had begun to shiftfrom secondary to primary nasal correction. Now, presur-gical maxillary orthopedics sets the bony foundation forsynchronous nasolabial repair and for closure of the al-veolar clefts. The study of normal nasolabial growth andthe typical stigmata of the conventional methods providesthe necessary foreknowledge to guide surgical sculpture inthree dimensions and to anticipate the fourth dimension.The convergence of several forces are changing referral
lines for children born with bilateral cleft lip. These in-clude affirmation of centers of excellence, surgeons self-regulation, prenatal diagnosis, economics of health-caredelivery, and increasing parental sophistication. Thesepressures are not necessarily in conflict. Care by a sub-specialized plastic surgeon and experienced team is in thebest interests of the child and the third-partypayer. (Plast. Reconstr. Surg. 108: 181, 2001.)
James Barrett Brown and colleagues intro-duced their 1947 article with the pithy state-ment that a bilateral cleft lip is twice as difficult
to repair as a unilateral cleft and the results areonly half as good.1 Indeed, techniques for cor-rection of bilateral cleft lip have lagged behindthose for unilateral cleft lip. The infant withbilateral cleft lip has been subjected to multi-ple procedures only to endure sundry revisionsthroughout childhood. Despite the surgeonsbest efforts, the childs diagnosis was painfullyobvious to alleven at a distanceand thesestigmata were not easily erased by revisions.
These branded children beckoned surgeons tochange their traditional operative strategies.
Over the past decade, two important ad-vances have been made in the repair of bilat-eral cleft lip and nasal deformity: (1) evolutionto single-stage nasolabial closure with position-ing of the alar cartilages and sculpting of thesoft tissues to shape the columella and nasallobule, and (2) improved techniques for pre-surgical maxillary alignment to permit closureof the alveolar clefts and facilitate primary na-solabial repair. Although the principles for sin-gle-stage repair are established, craftsmanshipcontinues to evolve. Now, over a half centuryafter Barrett Browns discomfortable observa-tion, it can be said that the outcome for theinfant born with bilateral cleft lip is equal toand can surpass that of its unilateral counter-part.2 Furthermore, given the preoperative ad-vantage of nasolabial symmetry, these childrenrequire very few revisions.
Before undertaking primary repair of dou-ble cleft lip, there are some lessons to review.
LESSONS FROM SURGICALHISTORY
Many complex malformations, once onlyreparable by staged operations, can be cor-rected, usually more successfully, in a singleprocedure. This lesson is illustrated in the an-nals of the bilateral cleft lip and nasal defor-mity. Emphasis had focused on labial closureand ignored nasal distortion. Surgical text rec-
From the Division of Plastic Surgery and Craniofacial Centre, Childrens Hospital, Harvard Medical School. Received for publication August4, 2000; revised October 17, 2000.
181
-
8/10/2019 Primary Cleft Lip Repair
2/16
ommended staged repair, one side of the cleftand then the other. There was a misconceptionthat the diminutive prolabium lacks the poten-tial for growth. Techniques for repairing thedouble-labial cleft were adapted from thoseused for the more common unilateral form,
and they typically involved the introduction ofa rectangular or triangular flap from the laterallabial elements to augment prolabial height.These procedures left geometric (often asym-metric) labial scars and usually resulted in along-lip deformity and a tight upper lip.Straight-line repair minimized vertical elonga-tion of the central lip but produced an abnor-mally wide and shield-shaped philtrum. Therewas longstanding controversy over whether ornot to preserve the prolabial vermilion, leave itas a tiny strip, or excise it completely. Apposi-
tion of the orbicularis oris muscle was usuallynot mentioned. Some surgeons thought mus-cular closure would inhibit premaxillarygrowth.3 Nevertheless, with increasing atten-tion to muscular closure in the unilateral de-formity, reports began to underscore the im-portance of orbicular repair in bilateralclefts.4 8
Surgeons conceded to the complexity of thebilateral cleft nasal deformity and deferred cor-rection.911 The conventional teaching was thatthe columella is inadequate, and numerous
secondary procedures were devised to elon-gate the short columella. There are two ma-jor strategies.12 The first, popularized by Cro-nin, involves rotating bipedicled straps of tissuefrom the nostril sills.13 This method gives mod-est columellar length. A second method, theforked-flap procedure of Millard, involves re-cruiting labial tissue to the columella.5,9,14
There are two permutations of this method. Ininfants with a wide prolabium, the tines of theforked flap are banked at the time of labialclosure and transposed to the columella inearly childhood. More often, Millard prefersthree-stage columellar lengthening: (1) bilat-eral labial adhesions to stretch the prolabium;(2) elevation, rotation, and banking the tineswhile narrowing the philtrum (at age 18months); and, finally, (3) retrieval of the pro-labial prongs and elevation, along with the me-dial crura, to augment the columella (at age 2years).15
The forked-flap method, like all secondaryprocedures, causes peculiar tertiary distor-tions.16 Most techniques introduce a nexus ofscars across the columellar-labial junction. This
produces a midline nasolabial crease thatdeepens with smiling. The circumferentialphiltral scar produces a bulge rather than adimple. The best prolabial scars follow repairin infancy, done under minimal tension. Re-cruiting tines of a forked flap from the central
lip in a child can cause thickened and perma-nently wide philtral scars. Even in the best ofhands, the staged forked-flap procedure resultsin an unusual appearance: (1) a rectangularcolumella (with a broad base and without awaist); (2) a sharp columellar-labial angle; 3)abnormally elongated/enlarged nostrils; (4) atendency to columellar over-elongation with adisproportionate ratio of nostril length-to-nasaltip; and, sometimes, (5) a downward drift ofthe columellar base.1618 Furthermore, the me-dial crura become unnaturally positioned in
the tip, resulting in a break at the columellar-lobular connection. Because of these prob-lems, some surgeons began to wonder whetherlabial skin belongs in the columellaor ifmore tissue is needed at all.
Whereas delayed nasal repair was customaryfor the repair of bilateral cleft lip, the simulta-neous correction of the unilateral left lip andnasal deformity became accepted practice. Fur-thermore, there was no evidence that earlymanipulation of the alar cartilage impairs thedevelopment of the nasal tip.
LESSONS FROM BILATERALCLEFT STIGMATA
Every child with a repaired bilateral cleft liphas a characteristic appearance whose originsare both intrinsic to the malformation and ia-trogenic. The philtrum is bowed, wide, un-dimpled, overly long, often asymmetric, andlacking a white ridge. If the prolabial vermil-ion-mucosa is preserved, the free margins ofthe lateral labial elements hang like swags,flanking a thin median tubercle that is coveredby insufficient vermilion and chapped mucosa(whistling lip deformity).19 In profile, the up-per lip is flat or convex, whereas the lower lipeverts (cleft lip lower lip deformity).20 Thechild struggles to obtain bilabial closure over aprotrusive, retroclined, and vertically elon-gated premaxilla. The accompanying nasal de-formities are primarily deformational but arealso postsurgical. The tip is broad, the medialcrura are pulled inferior-posteriorly, the nos-trils are slumped, the alar domes are buckledand splayed, and the alae nasi are flared, some-times likened to cats knees.19 Often the alarlobules are hypoplastic (a primary deformity).
182 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
3/16
The caudal margin of the alar cartilage pro-trudes into the lateral vestibule, producing anoblique ridge or web.21Without amends for the
vertically long lateral labial elements and nor-mal muscular attachment of the alar bases, anunnatural elevation of the alae nasi will occur
and become more pronounced whenever thechild smiles.22 But of all the nasolabial distor-tions, the short columella is most obvious.
Principles that guide the surgical repair ofbilateral cleft lip and nasal deformity havebeen induced from the stigmata of conven-tional techniques and by study of the litera-ture19: (1) Symmetry. This is foremost. Stagedrepair portends asymmetry. Even the smallestnasolabial difference on the two sides will mag-nify with growth. (2) Primary muscular continu-ity. Orbicularis oris muscular bundles must be
completely mobilized from the lateral labialelements and apposed throughout the verticalextent of the upper lip. (3) Proper philtral sizeand shape. The constructed philtrum widensremarkably (in the upper portion more so thaninferiorly) and displays considerable verticalgrowth. (4)Formation of median tubercle from lat-eral labial elements. There is no prolabial whiteroll in the complete deformity, and both cen-tral vermilion and mucosa are deficient. (5)Primary positioning of alar cartilages to construct thenasal tip and columella. Techniques based onthis principle have dramatically changed thefaces of children born with bilateral cleft lip.
THEKEY: PRIMARYREPAIR OF THENASALDEFORMITY
Nasal dissection of stillborn infants with bi-lateral labial clefting reveals that the alardomes and middle crura are splayed, caudallyrotated like a bucket handle,23 and subluxedfrom their normal anatomic position overlyingthe upper lateral cartilages.19,23 Broadbent andWoolf24 described a case of primary medialadvancement of the alar domes combined withexcision of skin from the broad tip. However, itwas McComb who led the vanguard for primarycolumellar elongation. He initially tried pri-mary elevation of a forked flap21 and publishedhis follow-up analysis 10 years later, includingmeasurements of columellar growth.23 By thenhe had become disenchanted with this strategyand presented a revised technique for primarynasal repair in 1990without a forked flap.19
In the first stage, McComb used an externalincision (flying bird) to open the nasal tipand allow the apposition and suspension of the
splayed alar cartilages. The nasal tip was nar-rowed by V-Y plasty. Bilateral adhesions weredone, followed by definitive labial repair at asecond stage. The columellae looked quitenormal in McCombs assessment at 4 years.25
Mulliken also focused on early positioning of
the alar cartilages. This was initially done at asecond stage in conjunction with intranasaltransposition of the banked tines of a forkedflap.19 By l987, banking had been abandoned,and primary columellar lengthening and nasal-tip projection were achieved solely by apposi-tion and elevation of the alar domes and bysculpting the nasal soft tissues.22 Other sur-geons were on the same track to primary nasalcorrection. In 1991, Trott and Mohan wereworking in Malaysia, where socioeconomic fac-tors made multistaged repairs impractical.
They devised a single-stage nasolabial repair,based on open rhinoplastic exposure of thedislocated alars.26 Cutting and associates de-scribed another variation on the open-tip ap-proach and added presurgical stretching orelongation of the columella.27
The columella is in the nose became theshibboleth of surgeons who advocated primarynasal repair.16,25 The old, non-anatomic tech-niques that involved secondary recruitment ofprolabial skin into the columella were wrong.Instead, the alar cartilages should be placed inthe proper position at the time of labial repair,followed by trimming and redraping the softtissues of the nasal tip. No longer would thecolumella include labial (often hair-bearing)skin, the nasolabial junction be transgressed byscars, or the philtrum be encircled by scartissue.
LESSONS FROM THEFOURTHDIMENSION
Unlike the sculptor who works in stone, thesurgeon must work with a patient who growsand whose nasolabial proportions change.Thus, the surgeon must conceptualize thechilds appearance as a young adult. To do so,the surgeon must have a thorough understand-ing of three-dimensional form and fourth-dimensional alterations that occur with normalgrowth. Thankfully, Farkas and colleagues doc-umented the changes in the important nasola-bial features, between 1 and 18 years, in 1593North American Caucasians.28 Nasal height (n-sn) and width (al-al) develop early, reaching amean of 76.9 and 87 percent of adult size,respectively, by age 5 years. In contrast, nasal-tip protrusion (sn-prn) and columellar length
Vol. 108, No. 1 / CLEFT LIP AND NASAL DEFORMITY 183
-
8/10/2019 Primary Cleft Lip Repair
4/16
(sn-c') develop slowly, attaining a mean of onlytwo-thirds of adult size by 5 years of age. All thelabial landmarks grow rapidly, reaching ap-proximately 90 percent of adult proportions byage 5 years. The cutaneous upper lip attainsadult height by 3 years in girls and by 6 years in
boys.30
A working fourth-dimensional hypothesis forthe repair of bilateral cleft lip is to craft on asmall scale those features that are programmedfor rapid growth, compared with normal, age-matched infants. The corollary premise is thatslow-growing features can be constructed ofnormal size or slightly larger than normalsize.16 This accounting for temporal changesmust also include the nasolabial distortionsthat are particular to children with repairedbilateral cleft lip. Such knowledge can be
gained only by observation of older patients,ones own and those of predecessors and col-leagues. The fast-growing features grow evenfaster in the child with bilateral cleft lip, withthe exception of the median tubercle. Con-versely, the slow-growing features, specificallynasal-tip projection and columella, seem togrow more slowly in the child with bilateralcleft lip.29
PRESURGICALPREMAXILLARYMAXILLARYMANIPULATION
Synchronous nasolabial repair can be ac-complished only after proper alignment of thethree maxillary segments. Most bilateral cleftlips are complete, but sometimes there is a tinyband on one side that causes rotation of thepremaxilla. The protrusive premaxilla must beretracted and centralized, whereas the lateralmaxillary segments usually require expansion.There are two basic strategies for presurgicalpremaxillary orthopedic manipulation, activeand passive. The latter method is favored bythose who are concerned about the potentialdeleterious effects of forcing the segments intoposition. The passive molding plate is retainedby undercuts; this maintains the transversewidth of the maxillary segments. Because thereis no expansion, space is often inadequate forthe premaxilla. External force is needed toretract the premaxilla, using either adhesivetape, an elastic band attached to a headcap, orbilateral labial adhesion. Because there is nomuscle in the prolabial element of a bilateralcomplete cleft lip, preliminary labial adhesionsare prone to dehisce. Furthermore, externaltraction techniques tend to focus pressure in-
ferior to the basilar premaxilla, causing it tolingually incline and causing the vomer to bow.
The most commonly used active presurgicaldevice is based on the prototypic design ofGeorgiade and associates,30,31 refined and pop-ularized by Latham while working in collabo-
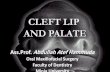
ration with Millard (Fig. 1).32,33
The acrylicplates of the custom-made appliance arepinned to the maxillary shelves. A looped wireis passed transversely through the neck of thepremaxilla, just behind the premaxillary alveo-lus and well anterior to the premaxillary-vomerine suture. The maxillary segments areexpanded by a ratcheted screw in the midplaneof the device, which is turned daily by thechilds parents. Elastic chains on each side areconnected to the trans-vomerine wire, loopedaround a pulley in the posterior section of the
appliance, and attached to a cleat on the mostanterior point of the maxillary acrylic plates.Tension on the elastic chain retracts the pre-maxilla; tension may be periodically adjusted.Typically it takes about 6 weeks to align thepremaxilla with the expanded palatal segmentsto effect closure of the alveolar clefts (gingivo-periosteoplasty). Lathams device is most suc-cessful in correcting the premaxillary antero-posterior position; however, the movement ismore retroclination than retroposition. Thedevice is somewhat less successful in amendingrotation and is least successful in preventingvertical elongation.
FIG. 1. The Latham pin-retained presurgical orthopedicappliance. Tightening the elastic chain retrudes the premax-illa; turning the screw expands the palatal shelves.
184 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
5/16
Some orthodontists think there are no advan-tages to premaxillary orthopedics in the manage-ment of bilateral cleft lip.34 However, proponentsof active versus passive techniques constitute thetwo major sides of the ongoing debate. Earlylongitudinal studies of children managed with a
Latham device show no serious deleterious ef-fects on occlusion and growth.33,35 However, crit-ics of active premaxillary orthopedics documentlong-term evidence for minor midfacial retru-sion.36,37 Whatever the outcome in terms of mid-facial position, three advantages of presurgicalalignment of the maxillary segments must beunderscored: (1) it permits philtral design ofproper proportions, (2) it facilitates primary na-sal correction, and (3) it allows closure of thealveolar gaps, thus preventing fistulas and (possi-bly) permitting bony ingrowth and stabilization
of the arch. Furthermore, if there is a near-normal maxillary foundation, there could be lesspostoperative prolabial distortion and interalarwidening. If the child exhibits midfacial retru-sion, maxillary advancement is a predictably suc-cessful procedure when done after completion ofgrowth. In the near future, it is likely that maxil-lary distraction with an entirely internal devicewill be available for patients who might benefit inchildhood.
PRIMARYREPAIR OF THEPRIMARYPALATE
Markings
The infant is typically 4 to 5 months old atthe time of synchronous repair. The philtralflap is designed with slightly biconcave sidesand a dart-shaped tip. The size of the flapdepends on the race and age of the infant andon the appearance of the parents. For a Cau-casian infant 4 to 6 months of age, suggesteddimensions are 6 to 8 mm for philtral flaplength: 3 to 4 mm wide between the peaks ofCupids bow and 2 mm wide at the columellar-labial junction. A strip of skin is drawn on eachside of the philtral flap; these will be deepithe-lialized to simulate the philtral ridges. The pro-posed Cupids bow peak-points are sited on thelateral labial elements so there will be sufficientcentral white roll for the handle of the Cupidsbow and enough vermilion to construct themedian tubercle. The alar base flaps are drawnat their junction with the lateral labial ele-ments. The vermilion-mucosal line is tattooed,as are the other important anatomic points tobe preserved during repair (Fig. 2, above, left).
Dissection
The philtral flap is incised, the flanking tabsare deepithelialized, and the remaining prola-bial skin is discarded. The lateral white line-vermilion-mucosal flaps are incised, and thealar base flaps are elevated. Orbicular muscular
bundles are dissected from the lateral labialelements (Fig. 2,above, center). The splayed alarcartilages are exposed through the rim inci-sions; it is helpful to support the cartilages witha cotton-tipped swab (Fig. 2, above, right).
Labial Closure
Mucosal flaps are elevated from the lateraland medial sides of the cleft defects to con-struct the nasal floors. Gingivomucoperiostealflaps are apposed, closing the alveolar clefts.The premaxillary vermilion-mucosa is trimmedto shorten the anterior wall of the gingivolabialsulcus (Fig. 2, second row, left). The remainingpremaxillary mucosa is sutured to the perios-teum to form the posterior wall of the anteriorgingivolabial sulcus. The lateral labial elementsare advanced medially as the buccal sulci areclosed. The lateral mucosal flaps form the an-terior wall of the central sulcus. The orbicularmuscles are apposed, inferiorly-to-superiorly,throughout the vertical height of the lip. Theuppermost suture suspends pars peripheralisto the periosteum of the anterior nasal spine
(Fig. 2, second row, right, left panel).The redundant tips of the lateral labial flaps
are trimmed to form the median tubercle (Fig.2, second row, right, right panel). The distal endof the philtral flap is inset. The philtral flap issecured to the muscular layer. This helps todepress the philtral flap and to raise the laterallabial flaps in an effort to simulate philtralridges. Yet, a realistic philtral dimple and flank-ing columns seem just beyond the surgeonscraft. The cephalic margin of the cutaneousflaps must be trimmed to correct for lateral
labial height; rarely is adjustment necessary atthe medial edges. These final steps in cutane-ous closure should be done after nasalcorrection.
Nasal Repair
A midline nasal-tip incision is not necessary,for with experience, it is possible to fully visu-alize the dislocated alar cartilages through bi-lateral rim incisions.29 An interdomal mattresssuture is placed to appose the middle cruraand genua. One or two mattress sutures sus-
Vol. 108, No. 1 / CLEFT LIP AND NASAL DEFORMITY 185
-
8/10/2019 Primary Cleft Lip Repair
6/16
pend each lateral genu (and lateral crus) tothe ipsilateral upper lateral cartilage (Fig. 2,third row, left). A cinch suture is placed througheach alar base and is tightened until the inter-alar distance is less than 25 mm (Fig. 2, thirdrow, right). The tips of the alar base flaps aretrimmed to form the nasal sills. A suture placedthrough the dermis of each alar base to theunderlying muscle serves to (1) prevent alarelevation with smiling and normal action of thedepressor alae nasi muscles, and (2) form the
normal cymal shape of the lateral sill (Fig. 2,third row, right panel).
Once the alar cartilages are in proper posi-tion, extra skin in the soft triangles becomesobvious and should be excised, including theskin of the lateral columella (Fig. 2, below, left,left panel). This resection narrows the tip, de-fines the columellar-lobular junction, elon-gates the nostrils, and narrows the columellarwaist. There is also redundancy in the vestibu-lar lining that becomes apparent after position-
FIG. 2. The Mulliken method of single-stage nasolabialrepair: the semi-open approach to nasal-tip cartilagesthrough bilateral rim incisions.
186 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
7/16
-
8/10/2019 Primary Cleft Lip Repair
8/16
complete deformity. Careful attention should
be given to the width of the philtral flap be-cause it has the same tendency to overgrowtransversely, as in the complete deformity.
Positioning the alar cartilages may not benecessary unless the columella measures shortand the genua are slumped. Another caveat isto sufficiently narrow the interalar dimension,for it will widen with time.
Asymmetric (Complete/Incomplete)
There is a range of severity in the asymmetriccomplete/incomplete bilateral cleft lip, de-
pending on the extent of soft-tissue bridging
and underlying alveolopalatal disjunction. Ifa tiny cutaneomucosal band on the incom-plete side pulls over the premaxilla, it is usu-ally best to divide it to allow presurgical cen-tralization of the premaxilla and symmetricrepair.
If one side is only partially cleft, the com-plete side should be addressed first. Unilateraldentofacial orthopedics, followed by a lip-nasal adhesion on the complete side, levelsthe surgical field before simultaneous bilat-eral nasolabial (and unilateral alveolar) clo-
FIG. 4 . (Above, left) Newborn with bilateral cleft lip, right cutaneous band, and intact rightalveolus and secondary palate. (Above, right; below) Appearance of the patient at age 5.5 years.
188 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
9/16
sure. During the second stage, the surgeonshould emphasize (overcorrect) repair onthe more severely involved side. Further-more, it is easier to match the good side tothe bad side than vice versa.
Complete Bilateral with Intact Secondary Palate
The rare complete bilateral cleft lip with anintact secondary palate is a particular chal-lenge. Neither external elastic traction nordentofacial orthopedics is possible because thepremaxilla is rigidly procumbent. There aretwo alternatives: (1) try to accomplish bilateralnasolabial repair over the protruding premax-illa; or (2) perform a premaxillary-vomerineostectomy and positioning and bilateral gingi-voperiosteoplasty, in conjunction with nasola-bial repair. A word of caution: the risk of pre-
maxillary necrosis is real. The incisions forpremaxillary ostectomy/positioning and alveo-lar closure impair the premaxillary blood sup-ply and limit venous drainage to the septalmucosa and preserved vomerine mucosa. Pri-mary premaxillary positioning in an infant withbilateral complete cleft lip can cause midfacialretrusion.39,40 However, this is unlikely in achild with an intact secondary palate.
Other Technical Variations on the Theme of Single-Stage Repair
Open rhinoplasty is another way to accessand primarily position the subluxed alar carti-lages, as first described by Trott and Mohan in1993.26 Their dissection plane is anterior to themedial crura. The prolabial-columellar unit ispedicled on the dorsal nasal skin and based onthe paired columellar arteries.4143 Their phil-tral flap is designed to correspond to the widthof the columellar base. Because the lateral phil-tral incisions extend across the columellarbase, this tissue cannot be used to construct themedial sills; the sills are formed almost entirelyfrom the alar flaps. Redundant skin is removedfrom the lateral labial elements. The inter-domal fat is elevated, the middle crura areapposed and secured to the septum, and thesoft tissues are gathered to enhance tip projec-tion (Fig. 5). Their postoperative photographsshow normally proportioned columellar lengthand nasal-tip protrusion. The philtra appear tobe wide. Perhaps this is acceptable in Asianchildren, who have a slightly broader Cupidsbow than Caucasian children.44 Distal ischemiais a potential problem if the philtral flap wereto be designed smaller using Trotts method.
Furthermore, this technique requires suturalreconstitution of the columellar labial angle,and this could also impede philtral circulation.
Nakajima and coworkers introduced presur-gical and postsurgical molding to minimize the
bilateral cleft nasal deformity.
45,46
Cutting andassociates extended this strategy to preopera-tive stretching of the columella. They fabri-cated an acrylic, double outrigger and prola-bial band, attached it to a passive palatalmolding plate, and secured it to the cheekswith tape.27,47 Their labial markings are similarto those of Trott and Mohan.26 However, theiropen-tip approach differs in that the prolabial-columellar flap is elevated at a deeper plane(membranous septum). This dissection is lesslikely to compromise the vascularity of the dis-tal prolabium. Their placement of interdomalsutures is done from the underside of the alarcartilages (Fig. 6). Cutting and associates un-derscore that preoperative expansion of nasallining is as important as columellar elongationbecause it lessens tension on the interdomalapposition and mimimizes widening of the na-sal tip.48 They emphasize that the moldingprongs must push anteriorly because of thetendency to produce a turned up nasal tip.Neither the Trott nor the Cutting methodsinclude cutaneous excision of the domal-columellar rims or resection of vestibular
lining.
REVISIONS
Symmetry is the major preoperative advan-tage of a bilateral cleft lip over a unilateralcleft. In part for this reason, the number ofrevisions for a double cleft lip should be lessthan for a single cleft lip. The most commonsecondary problem is extra mucosa (festoon-ing) in the lateral labial elements. Often this isassociated with minor vertical deficiency of themedian tubercle. It is best to wait until after the
FIG. 5. The Trott method of open approach to nasal-tipcartilages.26 The philtral-columellar flap (with rim exten-sions) is turned upward to expose the anterior surface of thedislocated middle crura and genua.
Vol. 108, No. 1 / CLEFT LIP AND NASAL DEFORMITY 189
-
8/10/2019 Primary Cleft Lip Repair
10/16
permanent central incisors have erupted and,if possible, after the premaxilla is in the correctsagittal position and angulation before adjust-ing the free labial margin to give proper dentalshow. There is a litany of procedures for thewhistling lip deformity (e.g., V-Y advance-ments, double/single Z-plasty, mucosal graft-ing). Particularly effective is the technique ofdeepithelialized, medially based submucosalflaps, tunnelled across the midline, to augmentthe central red lip.49 If there is insufficientlateral submucosa, a thick dermal graft servesto plump the median tubercle. Any excess mu-cosa can be trimmed to give a normal contourof the free margin in relation to the centralincisors.
An uncommon, annoying problem is pro-lapse of the posterior wall of the anterior gin-givolabial sulcus. Resuspension of the sulcalmucosa to the premaxillary periosteum is easilyaccomplished.
Nasal revisions in childhood are rarelyneeded. The most common is correction of an
abnormally wide nose, requiring readvance-ment of the alar bases. Sometimes domal diver-gence must be addressed. The alar cartilagescan be readjusted through rim incisions with-out the need for open rhinoplastic exposure.Final nasal adjustments are done after comple-tion of growth and maxillary advancement (ifnecessary) (e.g., tip reduction, nasomaxillarynarrowing, and septal resection).
OBLIGATION TOPERIODIC ASSESSMENT
Not only must surgeons prefigure the rate ofgrowth of nasolabial features, compounded bythe distortion of the deformity, but they alsoare obligated to periodically assess thesechanges to learn whether or not the predic-tions are accurate. Photography is the minimaldocumentation needed. Frontal and lateralviews (with the head in a neutral position) arenot enough; there must also be a basal view.For the latter, Pigott recommends that the na-sal dome be placed well above a line drawnbetween the medial canthi.50 Lehman suggests
FIG. 6. The Cutting method29 of open approach to nasal-tip cartilages. The philtral-medialcrural-columella complex (incised through the membranous septum with extensions into theintercartilaginous ridges) is reflected by retrograde dissection to display the underside of thesplayed middle crura and genua.
190 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
11/16
that McCombs rule be followed in publishingphotographs in support of a new method ofcleft lip repair, i.e., show 10 consecutive pa-tients with follow-up of 10 or more years.51
Although admirable, this rule is unrealistic,particularly if applied to the repair of bilateral
cleft lip. Less than 10 percent of cleft lips arebilateral, so even a high-volume surgeon mightsee only a few such new patients each year.Thus, in an average professional career of 25 to30 years, a surgeon will follow a relatively smallnumber of these children to adulthood.
What is needed is a convenient, objective,and rapid way to evaluate nasolabial symmetryand proportions throughout the growing years.Although clumsy, a panel can be convened toassess the photographs, using a rating scale.52
Other methodologies are direct anthropome-
try and computer-aided photogrammetry (in-direct anthropometry). There is great poten-tial for laser scanning or a similar advancedtechnology to assess results.53,54 This technol-ogy will likely incorporate the soft-tissue land-marks used in medical anthropometry, so untilit becomes available, anthropometry can bedone the old-fashioned way, by handheld ver-nier caliper.16,55,56
Intraoperative anthropometry provides base-line values for subsequent documentation ofchanges in the nasolabial dimensions. This was
done for 45 consecutive infants undergoingsingle-stage repair of bilateral complete cleftlip and nasal deformity.29 Fast-growing fea-tures, and nasal length and nasal width, wereset 88 percent and 96 percent, respectively,shorter than those of age-matched control in-fants. Slow-growing features, nasal protrusionand columellar length, were constructedlonger than normal (130 percent and 167 per-cent, respectively). Because all labial featuresgrow rapidly, these were downsized, with theexception of central vermilion-mucosal heightthat was deliberately made full.
Follow-up anthropometry required first mea-suring a cohort of normal children; thisshowed no differences16 from the results of thelarger samples determined by Farkas and col-leagues.28 Thirty-two children with repaired bi-lateral complete cleft lip were assessed fromage 1 to 12 years.16 Nasal-tip protrusion andcolumellar height were at the mean or longer.Interalar distance was about 2 SD above themean. Cutaneous upper labial height re-mained short in children younger than age 5years but tended to scatter around the mean in
the older children. A short cutaneous upper lipis attractive, provided there is sufficient heightof the central red lip. Although vermilion-mucosal height was made full, in one-half ofthe older children this dimension was just be-low the mean. Nevertheless, the total upper
labial height was either normal or slightly morethan normal. Admittedly, there are problemswith this study. First, the authors techniqueevolved through three technical phases in thestudy period, from two-stage to single-stage re-pairbut the principles did not change. Sec-ond, the study was serial and retrospective, sothe measurements in the three phases cannotbe compared at the same point in time. Third,only 12 of 32 children had undergone theone-stage repair described herein, and theirmean age at evaluation was 2.5 years.
A proviso for any anthropometric study isthat normal scalar measurements do not nec-essarily equate with normal appearance. Nev-ertheless, it is the authors strong impressionthat a child with measurements within 1 SD ofnormal looks better than a child with abnormalvalues. Furthermore, inclination of the upperlip influences appearance; i.e., a vertical upperlip looks longer than a protrusive lip. Thus, ifthe premaxilla is lingually inclined, whichmany are, this causes the upper lip to appearlonger than it may be by mensuration.
It is difficult to compare one surgicalmethod with another without a standard way toassess anatomic outcome. Kohout and col-leagues used photogrammetric analysis of twosurgeons results; one used the Mullikenmethod (group I) and the other used the Trottmethod (group II).57 The authors attempted todistinguish results attributable to method-ologic design from those produced by execu-tion of the particular method. Nasal-tip projec-tion was above normal with both methods butmore so in group I. Interalar dimension wasabnormally wide in both groups. Columellarlength, as a proportion of tip projection, ap-proached normal in group I but was short ingroup II. Philtral width (in proportion to nasalwidth) was normal in group I but abnormallyhigh in group II. An overly wide Cupids bow ingroup II was attributed to design.
Photogrammetry also permits the determi-nation of nasolabial angle and nasal-tip angle,provided the head is not rotated. Kohout andassociates found that the nasolabial angle wasobtuse in early childhood but narrowed in latechildhood and adolescence, presumably be-
Vol. 108, No. 1 / CLEFT LIP AND NASAL DEFORMITY 191
-
8/10/2019 Primary Cleft Lip Repair
12/16
cause of an increase in upper labial and colu-mellar obliquity. Nasal-tip angle was bluntedafter both the Mulliken and Trott methods;there were no long-term measures of possiblechange in the slow-growing lobule.57
EPILOGUE
Older children with bilateral cleft lip con-tinue to walk through the doors of cleft centershaving undergone many procedures and re-quiring more. They are unhappy because oftheir appearance and functional problems, butthe patterns of cleft care are changing. Fewergeneral plastic surgeons take on primary cleftlip repair. Two possible reasons for this trendare (1) established postgraduate fellowshiptraining in pediatric plastic surgery, and (2)increased number of craniofacial teams and
opportunities for pediatric plastic surgeons.Remarkably, this increased focus on care by afew is occurring despite diminished reimburse-ment for cleft work.
Outcome analyses in other pediatric surgicalspecialities underscore the value of subspecial-ization and high-volume operators. For exam-ple, there are lower inpatient costs and fewercomplications if ureteroneocystostomy is doneby fellowship-trained pediatric urologists ascompared with general urologists.58 For pedi-atric cardiac surgeons, there is an inverse rela-
tionship between the annual number of proce-dures (or a surgeons case load) and inpatientmortality.59,60 In these examples, the determi-nant of outcome is indisputable; the results ofcleft treatment are more difficult to assess.
Surely every infant born with cleft lip/palate,particularly a complete deformity, deserves thecare of an experienced team. Scandinavia hasthe longest tradition of centralized cleft care,beginning in 1933. There is only one center inDenmark, two in Finland, two in Norway, andsix in Sweden. The six-center Euro Cleft Studyshowed that standardization, centralization,and participation of high-volume operatorswere associated with good outcomes (andfewer revisions).61 In the United Kingdom, thethreshold volume for primary cleft repair hasrecently been mandated, the result of an out-come assessment of the countrys cleft centersunder the auspices of the National Health Ser-vice. The investigating committee concludedthat the number of cleft units should be re-duced drastically and that children should besent only to teams composed of two surgeons,each seeing 40 to 50 new patients annually.62
Boorman goes further by raising the questionof whether the rarity of the bilateral deformityand its attendant problems might argue forfurther control of referral.62
Such sweeping regulations would be unlikelyin Americas decentralized health-care system,
where change occurs slowly and, usually, vol-untarily. Parameters for cleft care have beenestablished by the American Cleft Palate-Craniofacial Association (ACPA).63 This orga-nization also surveyed North American teamsand determined standards-of-care delivery.64
Of 220 responding teams, the mean number ofnew cleft lip cases seen per year was 17. How-ever, 37 percent of U.S. and Canadian centersreported performing fewer than 10 primarylabial repairs each year. These numbers wouldbe even lower with more than one plastic sur-
geon on a team. The ACPA evaluation did notaddress the level of activity necessary to main-tain competency or provide optimal care.These issues are on the agenda of the Cranio-facial Outcomes Registry, which is supportedby a grant from The National Institute of Den-tal and Craniofacial Research. This program isbeing conducted with the cooperation ofACPA and its members. Prospective data, col-lected, and centralized by the Craniofacial Out-comes Registry, will permit inter-team compar-isons of outcome, the purpose being to
promote higher-quality care in the future.In the meantime, the traditional referrallines for a newborn with cleft lip/palate arechanging at the grassroots level. Rather than apediatrician, the prenatal ultrasonographer orperinatologist is increasingly the first to guideparents to a plastic surgeon. Savvy parents of-ten seek information (albeit nonpeer-re-viewed) in medical cyberspace, and parentalnetworks advise these Internauts where tosearch. Having completed a cram course incleft care, parents are likely to demand to taketheir infant to a cleft specialist outside theirinsurance network. Countercurrent to this ris-ing tide of parental self-referral stand thehealth maintenance organizations that insistthat all children stay within the network andaccept assignment to their general plasticsurgeon.
Rather than take up arms against third-partypayers, why not join them? Consider collabora-tive outcome studies. One hypothesis would bethat primary repair of a cleft lip in a restrictiveinsurance setting is penny-wise and pound-foolish. Perhaps if initial closure were done by
192 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
13/16
subspecialists, there would be fewer proce-dures and revisions, and decreased costs to allparties. It is easy to document efficacy in termsof speech, dentition, and facial growth. Stan-dardized evaluation of aesthetic results shouldsoon be possible using advanced technology,
such as laser scanning. A childs happiness andparental acceptance could be assessed by aquality-of-life outcome study.65
Who should care for an infant with cleft lip?At a societal level, this question exemplifies thelarger issue of what we want our health-caresystem to beand for whom. But the samequestion also could be asked by the surgeoncalled to see a newborn with cleft lip. Remem-ber the golden rule of pediatric care: Do for thechild what you would want done for your own.
John B. Mulliken, M.D.
Division of Plastic SurgeryChildrens Hospital300 Longwood AvenueBoston, Mass. [email protected]
REFERENCES
1. Brown, J. B., McDowell, F., and Byars, L. T. Doubleclefts of the lip. Surg. Gynecol. Obstet.85: 20, 1947.
2. Mulliken, J. B. Repair of bilateral complete cleft lip andnasal deformity: State of the art.Cleft Palate Craniofac.
J.37: 342, 2000.3. Manchester, W. M. The repair of double cleft lip as part
of an integrated program. Plast. Reconstr. Surg.45: 207,1970.
4. Glover, D. M., and Newcomb, M. R. Bilateral cleft liprepair and the floating premaxilla. Plast. Reconstr. Surg.28: 365, 1961.
5. Millard, D. R., Jr. Closure of bilateral cleft lip and elon-gation of columella by two operations in infancy. Plast.Reconstr. Surg.47: 324, 1971.
6. Duffy, M. M. Restoration of orbicularis oris muscle con-tinuity in therepair of thebilateral cleft lip. Br. J. Plast.Surg.24: 48, 1971.
7. Randall, P., Whitaker, L. A., and LaRossa, D. The impor-tance of muscle reconstruction in primary and second-ary cleft lip repair. Plast. Reconstr. Surg.54: 316, 1974.
8. Rehrmann, A. Construction of the upper lip, colu-
mella, and orbicularis musclein bilateral clefts.J. Max-illofac. Surg.3: 2, 1975.9. Millard, D. R., Jr. Cleft Craft: The Evolution of Its Surgery,
Vol. 2. Boston: Little, Brown, 1977.10. Black, P. W., and Scheflan, M. Bilateral cleft lip repair:
Putting it all together. Ann. Plast. Surg. 12: 118, 1984.11. Noordhoff, M. S. Bilateral cleft lipreconstruction. Plast.
Reconstr. Surg.78: 45, 1986.12. Cronin, T. D., and Upton, J. Lengthening of the short
columella associated with bilateral cleft lip.Ann. Plast.Surg.1: 75, 1978.
13. Cronin, T. D. Lengthening columella by use of skin fromnasal floor and alae. Plast. Reconstr. Surg.21: 417, 1958.
14. Millard, D. R., Jr. Columella lengthening by a forkedflap. Plast. Reconstr. Surg. 22: 454, l958.
15. Millard, D. R., Cassisi, A., and Wheeler, J. J. Designs forcorrection and camouflage of bilateral clefts of the lipand palate. Plast. Reconstr. Surg. 105: 1609, 2000.
16. Mulliken, J. B. Bilateral complete cleft lip and nasaldeformity: An anthropometric analysis of staged tosynchronous repair. Plast. Reconstr. Surg. 96: 9, 1995.
17. Pigott, R. W. Aesthetic considerations related to repairof bilateral cleft lip nasal deformity.Br. J. Plast. Surg.41: 593, 1988.
18. McComb, H. Primary repair of the bilateral cleft lipnose: A 15-year review anda new treatment plan. Plast.Reconstr. Surg.86: 882, 1990.
19. Mulliken, J. B. Principles and techniques of bilateral com-plete cleft lip repair.Plast. Reconstr. Surg.75: 477, 1985.
20. Pensler, J. M., and Mulliken, J. B. The cleft lip lower-lipdeformity.Plast. Reconstr. Surg. 82: 602, 1988.
21. McComb, H. Primary repair of the bilateral cleft lipnose.Br. J. Plast. Surg. 28: 262, 1975.
22. Mulliken, J. B. Correction of the bilateral cleft lip nasaldeformity: Evolution of a surgical concept. Cleft PalateCraniofac. J.29: 540, 1992.
23. McComb, H. Primary repair of the bilateral cleft lip nose:
A 10-year review.Plast. Reconstr. Surg.77: 701, 1986.24. Broadbent, T. R., and Woolf, R. M. Cleft lip nasal de-
formity. Ann. Plast. Surg.12: 216, 1984.25. McComb, H. Primary repair of the bilateral cleft lip
nose: A 4-year review. Plast. Reconstr. Surg. 94: 37, 1994.26. Trott, J. A.,and Mohan, N. A preliminary report on one
stage open tip rhinoplasty at the time of lip repair inbilateral cleft lip and palate: The Alor Setar experi-ence.Br. J. Plast. Surg.46: 215, 1993.
27. Cutting, C., Grayson, B., Brecht, L., Santiago, P., Wood,R., and Kwon, S. Presurgical columellar elongationand primary retrograde nasal reconstruction in one-stage bilateral cleft lip and nose repair.Plast. Reconstr.Surg.101: 630, 1998.
28. Farkas, L. G., Posnick, J. C., Hreczko, T. M., and Pron,G. E. Growth patterns of the nasolabial region: A mor-phometric study.Cleft Palate Craniofac. J. 29: 318, 1992.
29. Mulliken, J. B., Burvin, R., and Farkas, L. G. Repair ofbilateral complete cleft lip: Intraoperative nasolabialanthropometry.Plast. Reconstr. Surg. 107: 307, 2001.
30. Georgiade, N. G., and Latham, R. A. Maxillary archalignment in bilateral cleft lip and palate infant, usingpinned coaxial screw appliance. Plast. Reconstr. Surg.56: 52, 1975.
31. Georgiade, N. G., Mason, R., Riefkohl, R., et al. Preop-erative positioning of the protruding premaxilla in thebilateral cleftlip patient. Plast.Reconstr.Surg. 83:32, 1989.
32. Millard, D. R., Jr., and Latham, R. A. Improved primarysurgical and dental treatment of clefts.Plast. Reconstr.
Surg.86: 856, 1990.33. Millard, D. R., Latham, R., Huifen, X., et al. Cleft lipand palate treated by presurgical orthopedics, gingi-voperiosteoplasty, and lip adhesions (POPLA) com-pared with previous lip adhesion method: A prelim-inary study of serial dental casts. Plast. Reconstr. Surg.103: 1630, l999.
34. Ross, R. B., and MacNamera, M. C. Effect of presurgicalinfant orthopedics on facial esthetics in complete bi-lateral cleft lip and palate. Cleft Palate Craniofac. J.31:68, 1994.
35. Bitter, K. Lathams appliance for presurgical reposi-tioning of the protruded premaxilla in bilateral cleftlip and palate. J. Craniomaxillofac. Surg.20: 99, 1992.
36. Berkowitz, S. A comparison of treatment results in com-
Vol. 108, No. 1 / CLEFT LIP AND NASAL DEFORMITY 193
-
8/10/2019 Primary Cleft Lip Repair
14/16
plete bilateral cleft lip and palate using a conservativeapproach versus Millard-Latham PSOT procedure.Se-min. Orthod.2: 169, l996.
37. Henkel, K.-O., and Gundlach, K. K. H. Analysisof primarygingivoperiosteoplasty in alveolar cleft repair. Part I: Fa-cial growth.J. Craniomaxillofac. Surg.25: 266, 1997.
38. Mulliken, J. B. Primary repair of bilateral cleft lip and
nasal deformity. In G. S. Georgiade, R. Riefkohl, andL. S. Levin (Eds.), Georgiade Plastic and ReconstructiveSurgery, 3rd Ed. Baltimore: Williams & Wilkins, 1997.Pp. 230238.
39. Vargervik, K. Growth characteristics of the premaxillaand orthodontic treatment principles in bilateral cleftlip and palate. Cleft Palate J. 20: 289, 1983.
40. Friede, H., and Pruzansky, S. Long-term effects of pre-maxillary setback on facial skeletal profile in completebilateral cleft lip and palate.Cleft Palate J.22: 97, 1985.
41. Slaughter, W. B., Henry, J. W., and Berger, J. C.Changes in blood vessel pattern in bilateral cleft lip.Plast. Reconstr. Surg. 26: 166, 1960.
42. Fra, M. Anatomy and arteriography of cleft lips instillborn children. Plast. Reconstr. Surg. 42: 29, 1968.
43. Bennun, R. D., and Dogliotti, P. L. Anatomical basis forone-stage repair of bilateral cleft lip. InProceedings ofthe 8th Congress of the European Association for Maxillo-
facial Surgery,Madrid, 1986. P. 240.44. Farkas, L. G. (Ed.). Anthropometry of the Head and Face,
2nd Ed. New York: Raven Press, 1994. P. 344.45. Nakajima, T., Yoshimura, Y., and Sakakibara, A. Aug-
mentation of the nostril splint for retaining the cor-rected contour of the cleft lip nose. Plast. Reconstr.Surg.85: 182, 1990.
46. Nakajima, T., Yoshimura, Y., Nakanishi, Y., Kuwahara, M.,and Oka, T. Comprehensive treatment of bilateralcleft lip by multidisciplinary team approach. Br. J.Plast. Surg.44: 486, 1991.
47. Grayson, B. H., Santiago, P. E., Brecht,L. E., andCutting,C. B. Presurgical nasoalveolar molding in infantswith cleft lip and palate. Cleft Palate Craniofac. J. 36:486, 1999.
48. Cutting, C., Grayson, B., and Brecht, L. Columellarelongation in bilateral cleft lip (Letter). Plast. Reconstr.Surg.102: 1761, 1998.
49. Rodgers, C. M., and Mulliken, J. B. De-epithelializedmucosal-submucosal flaps to correct the whistlinglip deformity. Cleft Palate J. 26: 136, 1989.
50. Pigott, R. W. Alar leapfrog: A technique for reposi-tioning the total alar cartilage at primary cleft liprepair.Clin. Plast. Surg. 12: 643, 1985.
51. Lehman, J. A., Jr. Tulip flap for reconstruction of the
central tubercle in cleft lip (Discussion). Plast. Recon-str. Surg.101: 1349, 1998.
52. Tobiasen, J. M., and Hiebert, J. M. Facial impairmentscales for clefts. Plast. Reconstr. Surg. 93: 31, 1994.
53. Aung, S. C., Ngim, R. C. K., and Lee, S. T. Evaluationof the laser scanner as a surface measuring tool and itsaccuracy compared with direct facial anthropometricmeasurements. Br. J. Plast. Surg. 48: 551, 1995.
54. Bush, K., and Antonyshyn, O. Three-dimensional facialanthropometry using a laser surface scanner: Validationof the technique. Plast. Reconstr. Surg. 98: 226, 1996.
55. Farkas, L. G., and Lindsay, W. K. Morphology of theadult face following repair of bilateral cleft lip andpalate in childhood.Plast. Reconstr. Surg.47: 25, 1971.
56. Farkas, L. G., Hajnis, K., and Posnick, J. C. Anthropomet-ric and anthroposcopic findings of the nasal and facialregion in cleft patients before and after primary lip andpalate repair.Cleft Palate Craniofac. J.30: 1, l993.
57. Kohout, M. P., Aljaro, L. M., Farkas, L. G., and Mulliken,J. B. Photogrammetric comparison of two methodsfor synchronous repair of bilateral cleft lip and nasaldeformity.Plast. Reconstr. Surg. 102: 1339, 1998.
58. Snow, B. W., Cartwright, P. C., and Young, M. D. Doessurgical subspecialization in pediatrics provide high-quality, cost-effective care? Pediatrics97: 14, 1996.
59. Jenkins, K. J., Newburger, J. W., Lock, J. E., et al. In-hospital mortality for surgical repair of congenitalheart defects: Preliminary observations of variation byhospital caseload. Pediatrics95: 323, 1995.
60. Hannan, E. L., Racz, M., Kavey, R.-E., et al. Pediatric car-diac surgery: The effect of hospital and surgeon volumeon in-hospital mortality. Pediatrics101: 963, 1998.
61. Shaw, W. C., Dahl, E., Asher-McDade, C., et al. A six-center international study of treatment outcome inpatients with clefts of the lip and palate: Part 5. Gen-eral discussion and conclusions. Cleft Palate Craniofac.
J.29: 413, 1992.
62. Boorman, J. G. Treatment of cleft lip and/or palate inthe U.K. (Guest Editorial). Br. J. Plast. Surg. 51: 167,1998.
63. Peterson-Falzone, S. (Ed.). Parameters for the evalua-tion and treatment of patients with cleft lip/palate orother craniofacial anomalies. Cleft Palate Craniofac J. 30(Suppl. 1): S1, 1993.
64. Strauss, R. P. Cleft palate and craniofacial teams in theUnited States and Canada: A national survey of teamorganization and standards of care. Cleft Palate Cranio-
fac. J. 35: 473, 1998.65. Luce, E. A. Outcome studies and practice guidelines in
plastic surgery (Editorial). Plast. Reconstr. Surg. 104:1187, 1999.
Self-Assessment Examination follows onpage 195.
194 PLASTIC AND RECONSTRUCTIVE SURGERY,July 2001
-
8/10/2019 Primary Cleft Lip Repair
15/16
Self-Assessment Examination
Primary Repair of Bilateral Cleft Lip and Nasal Deformityby John B. Mulliken, M.D.
1. ALL THE FOLLOWING ARE COMMON STIGMATA AFTER TRADITIONAL REPAIR OF BILATERAL CLEFTLIP, EXCEPT:A) Slumped genuB) Elevated alae nasiC) Bowed philtrumD) Proclined premaxillaE) Thin median tubercle
2. THE FOLLOWING ARE CRITICISMS OF THE FORKED FLAP PROCEDURE FOR COLUMELLARELONGATION, EXCEPT:A) Scars at columellar-labial angleB) Inadequate columellar lengthC) Wide philtral scarsD) Abnormal columellar shapeE) Medial crura at nostril-lobular junction
3. PRINCIPLES FOR PRIMARY REPAIR OF BILATERAL COMPLETE CLEFT LIP AND NOSE INCLUDE THEFOLLOWING, EXCEPT:A) Maintain symmetryB) Secure primary muscular continuityC) Design proper prolabial size and configurationD) Construct median tubercle from prolabial vermilion-mucosaE) Form columella and nasal tip by positioning alar cartilages
4. ALL OF THE FOLLOWING ARE POTENTIAL ADVANTAGES OF PRESURGICAL ORTHOPEDICS, EXCEPT:A) Permit gingivoperiosteoplastyB) Correct protrusive basal premaxillaC) Facilitate primary nasal correctionD) Stabilize dental archE) Allow proper design of philtrum
5. ALL OF THE FOLLOWING ARE FAST-GROWING NASOLABIAL FEATURES, EXCEPT:A) Interalar widthB) Columellar lengthC) Cutaneous upper lip heightD) Cupids bow widthE) Median tubercle
6. WHICH OF THE FOLLOWING NASOLABIAL FEATURES IN A CHILD WITH REPAIRED BILATERALCOMPLETE CLEFT LIP IS LEAST LIKELY TO APPROXIMATE THE AGE-MATCHED NORMALMEASUREMENT?A) Interalar widthB) Nasal protrusionC) Columellar lengthD) Width of Cupids bow
E) Total upper lip height
-
8/10/2019 Primary Cleft Lip Repair
16/16
7. WHICH OF THESE NASOLABIAL FEATURES SHOULD BE CONSTRUCTED CONTRARY TO ITS PREDICTEDGROWTH RATE?A) Nasal-tip protrusionB) Columellar lengthC) Interalar widthD) Cupids bowE) Median tubercle
8. WHICH IS THE EASIEST AND MOST AVAILABLE METHODOLOGY TO ASSESS NASOLABIAL FEATURESAFTER REPAIR OF BILATERAL CLEFT LIP?A) AnthropometryB) Computer-aided photogrammetry (indirect anthropometry)C) Laser surface scanningD) Panel evaluationE) Digital three-dimensional photography
9. WHICH (OR WHO) IS LEAST LIKELY TO GUIDE PARENTS OF AN INFANT WITH A BILATERAL COMPLETECLEFT LIP TO A SUBSPECIALIST PLASTIC SURGEON?A) American Cleft Palate-Craniofacial AssociationB) Health maintenance organizationC) General plastic surgeonD) InternetE) Another parent
To complete the examination for CME credit, turn to page 283 for instructions and the response form.