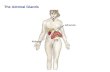
AJR:169, July 1997 169 Primary Adrenal Ganglioneuroma: CT Findings in Four Patients Gregory L. Johnson1 Ralph H. Hruban2 Fray F. Marshall3 Elliot K. Fishman1 OBJECTIVE. The purpose of this study was to characterize the appearance of adrenal ganglioneuroma on CT scans and to define the specific imaging features of the tumor. CONCLUSION. Adrenal ganglioneuroma is an uncommon benign tumor that is re- vealed as a solid adrenal mass on CT scans. Specific CT features such as calcification and le- sion enhancement may simulate a primary adrenal carcinoma. However. in our four patients. no signs of local invasion or vascular extension were noted. The specific diagnosis of adrenal ganglioneuroma requires either biopsy or surgical removal for documentation. Received October 2. 1996; accepted after revision November 26, 1996. tThe Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins Medical Institutions, Baltimore, MD 21287. Address correspon- dence to E. K. Fishman, Department of Radiology, Johns Hopkins Hospital, 600 N. Wolfe St., Baltimore, MD 21287. 2Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore, MD 21287. 3Department of Urology, The Johns Hopkins Medical Institutions, Baltimore, MD 21287. AJR 1997;169:169-171 0361-803X/97/1 691-169 © American Roentgen Ray Society A drenal ganglioneuroma is a be- nign neoplasm arising from neural crest tissue. Adrenal ganglioneuro- mas occur within the adrenal medulla and are composed of mature ganglion cells and Schwann’s cells in a fibrous stroma [I ]. Char- acteristically, ganglioneuromas do not secrete excess catecholamines or steroid hormones, and they are rarely associated with hyperten- sion [2]. Because of this lack of hormone production. ganglioneuromas are usually clinically silent lesions detected in patients undergoing abdominal imaging studies for unrelated reasons. Because it is an uncommon lesion. adrenal ganglioneuroma is not typi- cally included in the differential diagnosis of incidental asymptomatic adrenal masses. We have collected the records of four patients whom we treated for pathologically proven ganglioneuromas. and we present the CT de- scription of this unusual entity with patho- logic correlation. Materials and Methods Over a 10-year period, primary adrenal gangli- oneuromas were diagnosed in four patients for whom both CT and pathologic correlation were available at our institution. The patients were two men and two women (25-70 years old: mean age. 49 years old). Clinical presentations varied. Pa- tients typically presented with abdominal pain. but no patient was suspected of having an adrenal tu- mor before radiologic examination. One patient had a history of mild hypertension that was adequately managed with a single antihy- pertensive agent. None had clinical symptoms or biochemical evidence suggestive of adrenal corti- cal or medullary hyperfunction. No primary ma- lignancies or other evidence of metastatic disease were identified in any of the patients. Unenhanced and enhanced CT scans were ob- tamed in all four cases. Measurement of the CT at- tenuation values were available in two cases. In the other two cases. attenuation was defined rela- tive to the liver or kidney. Results The maximum diameter of the four tu- mors ranged from 5 to 9 cm. In all four pa- tients, the mass occurred in the right adrenal gland (Figs. 1-4). All lesions were fairly homogeneous in attenuation and ap- pearance on the unenhanced scans and in three cases on the enhanced scans. No evi- dence of necrosis or hemorrhage was seen. The lesions had smooth borders, and no ev- idence of local extension or invasion was noted. Clear planes were present between the liver and adrenal masses. No evidence of invasion of the renal vein, adrenal vein, or inferior vena cava was seen. In two of the four cases, areas of calcification were noted either centrally or in the periphery of the lesion. Definite enhancement was noted in two cases in which IV contrast material was administered. The range of enhance- Downloaded from www.ajronline.org by 27.70.129.20 on 03/22/23 from IP address 27.70.129.20. Copyright ARRS. For personal use only; all rights reserved

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Primary adrenal ganglioneuroma: CT findings in four patients.Primary Adrenal Ganglioneuroma: CT Findings in Four Patients
Gregory L. Johnson1 Ralph H. Hruban2 Fray F. Marshall3 Elliot K. Fishman1
OBJECTIVE. The purpose of this study was to characterize the appearance of adrenal
ganglioneuroma on CT scans and to define the specific imaging features of the tumor.
CONCLUSION. Adrenal ganglioneuroma is an uncommon benign tumor that is re-
vealed as a solid adrenal mass on CT scans. Specific CT features such as calcification and le-
sion enhancement may simulate a primary adrenal carcinoma. However. in our four patients.
no signs of local invasion or vascular extension were noted. The specific diagnosis of adrenal
ganglioneuroma requires either biopsy or surgical removal for documentation.
Received October 2. 1996; accepted after revision November 26, 1996.
tThe Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins Medical Institutions, Baltimore, MD 21287. Address correspon- dence to E. K. Fishman, Department of Radiology, Johns Hopkins Hospital, 600 N. Wolfe St., Baltimore, MD 21287.
2Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore, MD 21287.
3Department of Urology, The Johns Hopkins Medical Institutions, Baltimore, MD 21287.
AJR 1997;169:169-171
0361-803X/97/1 691-169
nign neoplasm arising from neural
crest tissue. Adrenal ganglioneuro-
composed of mature ganglion cells and
Schwann’s cells in a fibrous stroma [I ]. Char-
acteristically, ganglioneuromas do not secrete
excess catecholamines or steroid hormones,
and they are rarely associated with hyperten-
sion [2]. Because of this lack of hormone
production. ganglioneuromas are usually
undergoing abdominal imaging studies for
unrelated reasons. Because it is an uncommon
lesion. adrenal ganglioneuroma is not typi-
cally included in the differential diagnosis of
incidental asymptomatic adrenal masses. We
have collected the records of four patients
whom we treated for pathologically proven
ganglioneuromas. and we present the CT de-
scription of this unusual entity with patho-
logic correlation.
available at our institution. The patients were two
men and two women (25-70 years old: mean age.
49 years old). Clinical presentations varied. Pa-
tients typically presented with abdominal pain. but
no patient was suspected of having an adrenal tu-
mor before radiologic examination.
pertensive agent. None had clinical symptoms or
biochemical evidence suggestive of adrenal corti-
cal or medullary hyperfunction. No primary ma-
lignancies or other evidence of metastatic disease
were identified in any of the patients.
Unenhanced and enhanced CT scans were ob-
tamed in all four cases. Measurement of the CT at- tenuation values were available in two cases. In
the other two cases. attenuation was defined rela-
tive to the liver or kidney.
Results
The maximum diameter of the four tu-
mors ranged from 5 to 9 cm. In all four pa-
tients, the mass occurred in the right
adrenal gland (Figs. 1-4). All lesions were
fairly homogeneous in attenuation and ap-
pearance on the unenhanced scans and in
three cases on the enhanced scans. No evi-
dence of necrosis or hemorrhage was seen.
The lesions had smooth borders, and no ev-
idence of local extension or invasion was
noted. Clear planes were present between
the liver and adrenal masses. No evidence
of invasion of the renal vein, adrenal vein,
or inferior vena cava was seen. In two of
the four cases, areas of calcification were
noted either centrally or in the periphery of
the lesion. Definite enhancement was noted
in two cases in which IV contrast material
was administered. The range of enhance-
D ow
nl oa
de d
fr om
w w
w .a
jr on
lin e.
or g
by 2
7. 70
.1 29
.2 0
on 0
3/ 22
/2 3
fr om
I P
ad dr
es s
27 .7
0. 12
9. 20
. C op
yr ig
ht A
R R
S. F
or p
er so
170 AJR:169, July 1997
Fig. 1.-61-year-old woman with 5 x 4 cm right adrenal mass. A, Unenhanced CT scan shows homogeneous mass (solid arrow) measur- ing 20 H. Right adrenal mass displaces upper pole of right kidney (open
arrow) posteriorly. B, Enhanced CT scan shows enhancement of 51 H (solid arrow). Posteriorly displaced strongly enhancing upper pole of right kidney is again seen (open arrow). Adrenal ganglioneuroma was pathologically confirmed.
Fig. 2.-41-year-old man with incidentally detected 6 x 5 cm right ad- renal mass. A, Unenhanced CT scan shows mass as homogeneous and of solid at- tenuation, measuring 20 H. Left renal stone is incidentally seen. B, Enhanced CT scan shows enhancement to 57 H. Adrenal ganglio- neuroma was pathologically confirmed.
Fig. 3-70-year-old woman with 5 x 4 cm right adrenal mass. A, Unenhanced CT scan shows mass of attenuation equal to that of kid- ney. Note central area offaint calcification. Mass showed no significant enhancement Adrenal ganglioneuroma was pathologically confirmed. B, High-power photomicrograph shows histologically mature ganglion cells (arrows) embedded in matrix of irregular bundles of benign Schwann’s cells. (H and E, x 200)
Fig. 4-25-year-old man with 9 x 7 cm right adrenal mass. A, Unenhanced CT scan shows mass of lower attenuation than liver. Foci of calcification (arrow) are also presentwithin periphery of lesion. B, Enhanced CT scan shows mass as minimally enhanced. Adrenal ganglioneuroma was pathologically confirmed.
#{149}ft:1Patient Data and CT Characteristics of Primary Adrenal Ganglioneuromas
Patient Lesion
None
None
Central
Peripheral
AJR:169, July 1997 171
unenhanced CT scans the tumors typically
measured approximately 20 H, and, after
contrast material administration, they ranged
from 30 to 57 H (Table 1).
Discussion
sympathetic nervous system that occurs in
all age groups but is more common before
the age of 60 years. Ganglioneuromas may
arise anywhere along the paravertebral sym-
pathetic plexus and occasionally are found
within the adrenal medulla [2]. Rarely, neu-
roblastoma may mature into ganglioneu-
roma [11. Also, ganglioneuroma may occur in
association with other tumors such as pheo-
chromocytoma. These cases are not ad-
dressed in this report.
manifestation of disease would not be cx-
pected. The tumor is commonly identified
serendipitously in patients undergoing radio-
logic study for other reasons. This occult nature
often presents a challenge to the radiologist at-
tempting to differentiate adrenal ganglion-
euroma from other nonhyperfunctioning
cal carcinoma, myelolipoma, and hemangi-
oma. CT is an effective diagnostic tool for
asymptomatic cortical lesions such as my-
elolipomas or adenomas because of the pres-
ence of fat and low attenuation, respectively
[3-5]. Ganglioneuroma offers no such dis-
criminating components, but certain charact-
eristics may help to support or at least suggest
the diagnosis. These characteristics include a
solid round adrenal mass without evidence
of tumor invasion.
nal mass depends on many factors, includ-
ing lesion size, attenuation value, clinical
history of endocrine dysftmction (e.g., Cush-
ing’s disease), or the presence of a known pri-
mary tumor (e.g.. lung cancer). Most centers
will monitor an incidental adrenal mass that
is less than 4 cm in maximum diameter in the
absence of adrenal dysfunction or known pri-
mary cancer [6]. However, a lesion larger
than 4 cm even in these patients is more
problematic. Because adrenal carcinoma
ble to distinguish between a silent adrenal
cancer and a ganglioneuroma without biopsy
or surgical resection.
nal masses often includes scintigraphic evalu-
ation. Because of the lack of exogenous
hormone secretion, scintigraphic studies of
ganglioneuroma typically reveal discordant
the side with the mass) [6, 7]. However, this
scintigraphic pattern is also seen with adreno-
cortical carcinoma. Careful analysis of the
CT appearance of the lesion may help distin-
guish between the two entities. However, we
cautiously note that no single characteristic
could definitively distinguish between the
two lesions.
carcinoma are typically solid and may en-
hance with iodinated contrast material. How-
ever, in our series ganglioneuromas enhanced
homogeneously (three cases) or minimally
heterogeneously (one case), whereas a more
irregular enhancement pattern would be cx-
pected in cases of adrenal carcinoma. Local
invasion into vascular structures including
the adrenal vein, the renal vein, and the infe-
rior vena cava is present in more than 50% of
cases of adrenal carcinoma. No evidence of
vascular invasion by adrenal ganglioneuroma
was seen in this series, and the finding has
been reported as uncharacteristic by other
authors [2, 8]. The presence of calcification
can occur in either lesion and is not helpful in
differentiating these lesions.
in various areas of the body and noted that
many of the lesions were of low CT attenu-
ation [9], which does not appear to be the
case in our series of adrenal ganglioneu-
romas. The lesions appear to be generally
solid in attenuation, which would correlate
with the histopathology (Fig. 3B). All four
masses occurred in the right adrenal gland.
This occurrence, although interesting, is
likely attributed to the small sample size
of our study.
In conclusion, primary adrenal ganglio-
neuromas are uncommon benign neural crest tumors. In our series, the CT appearance was
usually that of a homogeneous solid mass
greater than 5 cm in maximum dimension
with enhancement after contrast media in-
jection. Although the appearance, including
the presence of calcification, may overlap
with that of primary adrenal carcinoma, the
lack of both clinical symptoms and local in-
vasion may help suggest the diagnosis of
adrenal ganglioneuroma.
with this work.
Semin Roentgenol 1988:23:205-215
2. Karsner HT. Thmors of the adrenal. In:Karsner
HT. ed. Atlas oftumorpatholog 2nd series. Be- thesda, MD: Armed Forces Institute ofTumor Pa-
thology, 1986:253-260 3. Korobkin M, Bmdeur FJ,Yutzy 0G. et al. Differen-
Dation of adrenal adenomas from nonadenomas us-
ing CT attenuation values. AiR 1996;166:53l-536 4. Dunnick NR, Korobkin M. Characterization of
adrenal masses. AJR 1995:164:637-642 5. Francis IR, Gros MD, Shapiro B. Korobkin M.
Quint LE. Integrated imaging of adrenal disease.
Radiology 1992:184:1-13
tally discovered adrenal masses: a functional and
morphological study. Ep Clin Endocrinol 1993:
101: 13 1-137
7. Nakajo M, Yshiaki N, Yonekura R, Iwashita S. Goto T. The role of adrenocortical scintigraphy in
the evaluation of unilateral incidentally discov-
ered adrenal and juxtadrenal masses. Ann NucI
Med 1993:7:157-166
patients. Pediatr Radio! 1983:313: 1 1-18
9. Kumar AJ, Kuhadja FP, Martinez CR. Fishman EK, Jezio DV, Siegleman SS. Computed tomog- raphy of extracranial nerve sheath tumors with
pathological correlation. J Comput Assist Tornogr
1983:7:857-865
Gregory L. Johnson1 Ralph H. Hruban2 Fray F. Marshall3 Elliot K. Fishman1
OBJECTIVE. The purpose of this study was to characterize the appearance of adrenal
ganglioneuroma on CT scans and to define the specific imaging features of the tumor.
CONCLUSION. Adrenal ganglioneuroma is an uncommon benign tumor that is re-
vealed as a solid adrenal mass on CT scans. Specific CT features such as calcification and le-
sion enhancement may simulate a primary adrenal carcinoma. However. in our four patients.
no signs of local invasion or vascular extension were noted. The specific diagnosis of adrenal
ganglioneuroma requires either biopsy or surgical removal for documentation.
Received October 2. 1996; accepted after revision November 26, 1996.
tThe Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins Medical Institutions, Baltimore, MD 21287. Address correspon- dence to E. K. Fishman, Department of Radiology, Johns Hopkins Hospital, 600 N. Wolfe St., Baltimore, MD 21287.
2Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore, MD 21287.
3Department of Urology, The Johns Hopkins Medical Institutions, Baltimore, MD 21287.
AJR 1997;169:169-171
0361-803X/97/1 691-169
nign neoplasm arising from neural
crest tissue. Adrenal ganglioneuro-
composed of mature ganglion cells and
Schwann’s cells in a fibrous stroma [I ]. Char-
acteristically, ganglioneuromas do not secrete
excess catecholamines or steroid hormones,
and they are rarely associated with hyperten-
sion [2]. Because of this lack of hormone
production. ganglioneuromas are usually
undergoing abdominal imaging studies for
unrelated reasons. Because it is an uncommon
lesion. adrenal ganglioneuroma is not typi-
cally included in the differential diagnosis of
incidental asymptomatic adrenal masses. We
have collected the records of four patients
whom we treated for pathologically proven
ganglioneuromas. and we present the CT de-
scription of this unusual entity with patho-
logic correlation.
available at our institution. The patients were two
men and two women (25-70 years old: mean age.
49 years old). Clinical presentations varied. Pa-
tients typically presented with abdominal pain. but
no patient was suspected of having an adrenal tu-
mor before radiologic examination.
pertensive agent. None had clinical symptoms or
biochemical evidence suggestive of adrenal corti-
cal or medullary hyperfunction. No primary ma-
lignancies or other evidence of metastatic disease
were identified in any of the patients.
Unenhanced and enhanced CT scans were ob-
tamed in all four cases. Measurement of the CT at- tenuation values were available in two cases. In
the other two cases. attenuation was defined rela-
tive to the liver or kidney.
Results
The maximum diameter of the four tu-
mors ranged from 5 to 9 cm. In all four pa-
tients, the mass occurred in the right
adrenal gland (Figs. 1-4). All lesions were
fairly homogeneous in attenuation and ap-
pearance on the unenhanced scans and in
three cases on the enhanced scans. No evi-
dence of necrosis or hemorrhage was seen.
The lesions had smooth borders, and no ev-
idence of local extension or invasion was
noted. Clear planes were present between
the liver and adrenal masses. No evidence
of invasion of the renal vein, adrenal vein,
or inferior vena cava was seen. In two of
the four cases, areas of calcification were
noted either centrally or in the periphery of
the lesion. Definite enhancement was noted
in two cases in which IV contrast material
was administered. The range of enhance-
D ow
nl oa
de d
fr om
w w
w .a
jr on
lin e.
or g
by 2
7. 70
.1 29
.2 0
on 0
3/ 22
/2 3
fr om
I P
ad dr
es s
27 .7
0. 12
9. 20
. C op
yr ig
ht A
R R
S. F
or p
er so
170 AJR:169, July 1997
Fig. 1.-61-year-old woman with 5 x 4 cm right adrenal mass. A, Unenhanced CT scan shows homogeneous mass (solid arrow) measur- ing 20 H. Right adrenal mass displaces upper pole of right kidney (open
arrow) posteriorly. B, Enhanced CT scan shows enhancement of 51 H (solid arrow). Posteriorly displaced strongly enhancing upper pole of right kidney is again seen (open arrow). Adrenal ganglioneuroma was pathologically confirmed.
Fig. 2.-41-year-old man with incidentally detected 6 x 5 cm right ad- renal mass. A, Unenhanced CT scan shows mass as homogeneous and of solid at- tenuation, measuring 20 H. Left renal stone is incidentally seen. B, Enhanced CT scan shows enhancement to 57 H. Adrenal ganglio- neuroma was pathologically confirmed.
Fig. 3-70-year-old woman with 5 x 4 cm right adrenal mass. A, Unenhanced CT scan shows mass of attenuation equal to that of kid- ney. Note central area offaint calcification. Mass showed no significant enhancement Adrenal ganglioneuroma was pathologically confirmed. B, High-power photomicrograph shows histologically mature ganglion cells (arrows) embedded in matrix of irregular bundles of benign Schwann’s cells. (H and E, x 200)
Fig. 4-25-year-old man with 9 x 7 cm right adrenal mass. A, Unenhanced CT scan shows mass of lower attenuation than liver. Foci of calcification (arrow) are also presentwithin periphery of lesion. B, Enhanced CT scan shows mass as minimally enhanced. Adrenal ganglioneuroma was pathologically confirmed.
#{149}ft:1Patient Data and CT Characteristics of Primary Adrenal Ganglioneuromas
Patient Lesion
None
None
Central
Peripheral
AJR:169, July 1997 171
unenhanced CT scans the tumors typically
measured approximately 20 H, and, after
contrast material administration, they ranged
from 30 to 57 H (Table 1).
Discussion
sympathetic nervous system that occurs in
all age groups but is more common before
the age of 60 years. Ganglioneuromas may
arise anywhere along the paravertebral sym-
pathetic plexus and occasionally are found
within the adrenal medulla [2]. Rarely, neu-
roblastoma may mature into ganglioneu-
roma [11. Also, ganglioneuroma may occur in
association with other tumors such as pheo-
chromocytoma. These cases are not ad-
dressed in this report.
manifestation of disease would not be cx-
pected. The tumor is commonly identified
serendipitously in patients undergoing radio-
logic study for other reasons. This occult nature
often presents a challenge to the radiologist at-
tempting to differentiate adrenal ganglion-
euroma from other nonhyperfunctioning
cal carcinoma, myelolipoma, and hemangi-
oma. CT is an effective diagnostic tool for
asymptomatic cortical lesions such as my-
elolipomas or adenomas because of the pres-
ence of fat and low attenuation, respectively
[3-5]. Ganglioneuroma offers no such dis-
criminating components, but certain charact-
eristics may help to support or at least suggest
the diagnosis. These characteristics include a
solid round adrenal mass without evidence
of tumor invasion.
nal mass depends on many factors, includ-
ing lesion size, attenuation value, clinical
history of endocrine dysftmction (e.g., Cush-
ing’s disease), or the presence of a known pri-
mary tumor (e.g.. lung cancer). Most centers
will monitor an incidental adrenal mass that
is less than 4 cm in maximum diameter in the
absence of adrenal dysfunction or known pri-
mary cancer [6]. However, a lesion larger
than 4 cm even in these patients is more
problematic. Because adrenal carcinoma
ble to distinguish between a silent adrenal
cancer and a ganglioneuroma without biopsy
or surgical resection.
nal masses often includes scintigraphic evalu-
ation. Because of the lack of exogenous
hormone secretion, scintigraphic studies of
ganglioneuroma typically reveal discordant
the side with the mass) [6, 7]. However, this
scintigraphic pattern is also seen with adreno-
cortical carcinoma. Careful analysis of the
CT appearance of the lesion may help distin-
guish between the two entities. However, we
cautiously note that no single characteristic
could definitively distinguish between the
two lesions.
carcinoma are typically solid and may en-
hance with iodinated contrast material. How-
ever, in our series ganglioneuromas enhanced
homogeneously (three cases) or minimally
heterogeneously (one case), whereas a more
irregular enhancement pattern would be cx-
pected in cases of adrenal carcinoma. Local
invasion into vascular structures including
the adrenal vein, the renal vein, and the infe-
rior vena cava is present in more than 50% of
cases of adrenal carcinoma. No evidence of
vascular invasion by adrenal ganglioneuroma
was seen in this series, and the finding has
been reported as uncharacteristic by other
authors [2, 8]. The presence of calcification
can occur in either lesion and is not helpful in
differentiating these lesions.
in various areas of the body and noted that
many of the lesions were of low CT attenu-
ation [9], which does not appear to be the
case in our series of adrenal ganglioneu-
romas. The lesions appear to be generally
solid in attenuation, which would correlate
with the histopathology (Fig. 3B). All four
masses occurred in the right adrenal gland.
This occurrence, although interesting, is
likely attributed to the small sample size
of our study.
In conclusion, primary adrenal ganglio-
neuromas are uncommon benign neural crest tumors. In our series, the CT appearance was
usually that of a homogeneous solid mass
greater than 5 cm in maximum dimension
with enhancement after contrast media in-
jection. Although the appearance, including
the presence of calcification, may overlap
with that of primary adrenal carcinoma, the
lack of both clinical symptoms and local in-
vasion may help suggest the diagnosis of
adrenal ganglioneuroma.
with this work.
Semin Roentgenol 1988:23:205-215
2. Karsner HT. Thmors of the adrenal. In:Karsner
HT. ed. Atlas oftumorpatholog 2nd series. Be- thesda, MD: Armed Forces Institute ofTumor Pa-
thology, 1986:253-260 3. Korobkin M, Bmdeur FJ,Yutzy 0G. et al. Differen-
Dation of adrenal adenomas from nonadenomas us-
ing CT attenuation values. AiR 1996;166:53l-536 4. Dunnick NR, Korobkin M. Characterization of
adrenal masses. AJR 1995:164:637-642 5. Francis IR, Gros MD, Shapiro B. Korobkin M.
Quint LE. Integrated imaging of adrenal disease.
Radiology 1992:184:1-13
tally discovered adrenal masses: a functional and
morphological study. Ep Clin Endocrinol 1993:
101: 13 1-137
7. Nakajo M, Yshiaki N, Yonekura R, Iwashita S. Goto T. The role of adrenocortical scintigraphy in
the evaluation of unilateral incidentally discov-
ered adrenal and juxtadrenal masses. Ann NucI
Med 1993:7:157-166
patients. Pediatr Radio! 1983:313: 1 1-18
9. Kumar AJ, Kuhadja FP, Martinez CR. Fishman EK, Jezio DV, Siegleman SS. Computed tomog- raphy of extracranial nerve sheath tumors with
pathological correlation. J Comput Assist Tornogr
1983:7:857-865
Related Documents