Prevention and Treatment of Venous Thromboembolism National Performance Measures And Recent Guidelines Dale W. Bratzler, DO, MPH QIOSC Medical Director Dale W. Bratzler, DO, MPH Professor and Associate Dean, College of Public Health Professor of Medicine, College of Medicine Chief Quality Officer – OU Physicians Group University of Oklahoma Health Sciences Center August 3, 2012

Prevention and Treatment of Venous Thromboembolism National Performance Measures And Recent Guidelines Dale W. Bratzler, DO, MPH QIOSC Medical Director.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prevention and Treatment of Venous Thromboembolism
National Performance Measures And Recent Guidelines
Dale W. Bratzler, DO, MPH
QIOSC Medical Director
Dale W. Bratzler, DO, MPHProfessor and Associate Dean, College of Public Health
Professor of Medicine, College of MedicineChief Quality Officer – OU Physicians Group
University of Oklahoma Health Sciences Center
August 3, 2012

2
Outline
• The problem – VTE in US hospitals
• Need for national performance standards
• Update on National Guidelines for Prevention of VTE
• Strategies for prevention of VTE

Venous thromboembolism (VTE) = Deep vein thrombosis (DVT) and Pulmonary embolism (PE)

“The best estimates indicate that 350,000 to 600,000 Americans each year suffer from DVT and PE, and that at least 100,000 deaths may be directly or indirectly related to these diseases. This is far too many, since many of these deaths can be avoided. Because the disease disproportionately affects older Americans, we can expect more suffering and more deaths in the future as our population ages–unless we do something about it.”

5
Annual Incidence of VTE in Olmsted County, MN: 1966-1995
By Age and Gender
Annu
al in
cide
nce/
100,
000
Annu
al in
cide
nce/
100,
000
Age group (yr)Age group (yr)
0
200
400
600
800
1,000
1,200
MenMen
WomenWomen

6
Prevention of Venous ThromboembolismIntroduction
• VTE Remains a major health problem– In addition to the risk of sudden death
• 30% of survivors develop recurrent VTE within 10 years
• 28% of survivors develop venous stasis syndrome within 20 years
Goldhaber SZ. N Engl J Med. 1998;339:93-104.Silverstein MD, et al. Arch Intern Med. 1998;158:585-593.
Heit JA, et al. Thromb Haemost. 2001;86:452-463.Heit JA. Clin Geriatr Med. 2001;17:71-92.
Heit JA, et al. Mayo Clin Proc. 2001;76:1102-1110.

7
Risk of DVT in Hospitalized Patients
Patient group DVT incidence Medical patients 10 - 20 % Major gyne/urol/gen surgery 15 - 40 % Neurosurgery 15 - 40 % Stroke 20 - 50 % Hip/knee surgery 40 - 60 % Major trauma 40 - 80 % Spinal cord injury 60 - 80 % Critical care patients 15 - 80 %
No prophylaxis + routine objective screening for DVT

Associated Illnesses that are a Consequence of VTE events
• Chronic thromboembolic pulmonary hypertension– Mean pulmonary artery pressure greater than 25
mm Hg that persists 6 months after PE– 2-4% of patients after PE
• Post-thrombotic syndrome– Calf swelling and skin pigmentation; venous
ulceration in severe cases• Up to 43% of patients within 2 years – most mild
Goldhaber SZ, Bounameaux H. Lancet. 2012 May 12; 379:1835-46.

9
Prevention of Venous Thromboembolism
• The majority (93%) of estimated VTE-related deaths in the US were due to sudden, fatal PE (34%) or followed undiagnosed VTE (59%)
Heit JA, Cohen AT, Anderson FA on behalf of the VTE Impact Assessment Group. [Abstract] American Society of Hematology Annual Meeting, 2005.
For many patients, the first symptom of VTE is sudden death!
How many of those patients with sudden death in the hospital or after discharge attributed to an acute coronary
event actually died of acute pulmonary embolism?

10
National Body Position Statements
• Leapfrog1:
PE is “the most common preventable cause of hospital death in the United States”
• Agency for Healthcare Research and Quality (AHRQ)2:
Thromboprophylaxis is the number 1 patient safety practice
• American Public Health Association (APHA)3:
“The disconnect between evidence and execution as it relates to DVT prevention amounts to a public health crisis.”
The Leapfrog Group Hospital Quality and Safety Survey. Available at: www.leapfrog.medstat.com/pdf/Final/docShojania KG, et al. Making Healthcare Safer: A Critical Analysis of Patient Safety Practices. AHRQ, 2001. Available
at: www.ahrq.gov/clinic/ptsafety/White Paper. Deep-vein thrombosis: Advancing awareness to protect patient lives. 2003. Available at:
www.alpha.org/ppp/DVT_White_Paper.pdf

11
Annual cost to treat VTE
• $11,000 per DVT episode per patient• $17,000 per PE episode per patient• Recurrence increases hospitalization costs by
20%• Complications of anticoagulation• Time lost from work
– Quality of life: venous stasis and pulmonary HTN

12
Consequences of Surgical Complications
• Dimick and colleagues demonstrated increased costs of care:– infectious complications was $1,398– cardiovascular complications $7,789– respiratory complications $52,466– thromboembolic complications $18,310
Dimick JB, et al. J Am Coll Surg 2004;199:531-7.

Do venous and arterial diseases have shared risk factors?
“…..4 years after surviving a PE, fewer than half will remain free of MI, stroke, PAD, recurrent VTE, cancer or chronic thromboembolic pulmonary hypertension.”
VTE and atherothrombosis have a common pathophysiology that includes inflammation, hypercoagulability, and endothelial injury.
Goldhaber SZ, Bounameaux H. Lancet. 2012 May 12; 379:1835-46.

14
Inherited risk factors for DVT
Group 1 disorders• Protein C deficiency (2.5-6%)• Protein S deficiency (1.3-5%)• Antithrombin deficiency (0.5-
7.5%)
Group 2 disorders• Factor V leiden (6%)• Prothrombin (G20210A) (5-
10%)• Elevated VIII, IX, XI• Hyperhomocysteinemia• Arteriosclerosis

15
Acquired Risk FactorsRisk Factor Attributable Risk
Hospitalization/Nursing home 61.2
Active malignant neoplasm 19.8
Trauma 12.5
CHF 11.8
CV catheter 10.5
Neurologic disease with paresis 8.2
Superficial vein thrombosis 4.3
Varicose veins/stripping 6
Many others….
Being in the hospital is the greatest risk factor for VTE!

16
Risk Factors for DVT or PENested Case-Control Study (n=625 case-control pairs)
Surgery
Trauma
Inpatient
Malignancy with chemotherapy
Malignancy without chemotherapy
Central venous catheter or pacemaker
Neurologic disease
Superficial vein thrombosis
Varicose veins/age 45 yr
Varicose veins/age 60 yr
Varicose veins/age 70 yr
CHF, VTE incidental on autopsy
CHF, antemortem VTE/causal for death
Liver disease
0 5 10 15 20 25 50
Odds ratio

17
Independent Risk Factors for VTE afterMajor Surgery*:
Olmsted County 1988-97 (n=163)Risk Factor OR 95% CI P-value
Age (per 10 years) 1.26 1.07, 1.50 0.007
BMI (kg/m2, per 2-fold increase) 2.95 1.49, 5.82 0.002
ICU Length of Stay > 6 Days 3.97 1.46, 10.80 0.007
Central Venous Catheter 2.46 1.21, 5.03 0.013
Immobility Requiring Physical Therapy 2.18 1.17, 4.06 0.014
Varicose Veins 1.87 1.08, 3.23 0.025
Any Infection 1.68 1.01, 2.82 0.046
Anticoagulation Prophylaxis 0.27 0.12, 0.59 0.001
*Controlled for Surgery Type, Active Cancer, and Event Year
Heit, et al. J Thromb Haemost 2005

18
VTE is a Disease of Hospitalized and Recently Hospitalized Patients
1000
100
1
10
Hospitalized patients Community residents
Recently hospitalized
Heit JA. Mayo Clin Proc. 2001;76:1102
Ca
ses
per
10,0
00 p
ers
on-
year
s
VTE 100X more common in hospitalized patients!

19
Cumulative Incidence of VTE After Primary Hip or Knee Replacement
VTEevents
(%)
3.5
3.0
1.0
0.5
0.00 7 14 21 28 35
Days
Primary hipPrimary knee
42 49 56 63 9170 77 84
2.5
2.0
1.5
White RH, et al. Arch Intern Med. 1998; 158: 1525-1531

Many events occur after hospital discharge.
• IMPROVE Registry– 15,156 medical patients admitted to the hospital
• 184 patients had VTE events– 45% developed VTE after discharge
• Other studies have shown that up to two-thirds of VTE events occur in patients after discharge
Spyropoulos AC, et al. Chest 2011; 140:706-14.

VTE Facts
• Almost half of the outpatients with VTE had been recently hospitalized
• Less than half of the recently hospitalized patients had received VTE prophylaxis during their hospitalizations
• About half had a length of stay (LOS) of < 4 days Medical
Hospitalization Only
Hospitalization with Surgery
Ou
tpat
ien
ts W
ith
VT
E,
% 70
60
50
40
30
20
10
0
Days After Discharge
0-29 30-59 60-90
Goldhaber S. Arch Intern Med. 2007;167:1451-2.Spencer FA et al. Arch Intern Med. 2007;167(14):1471-5.

22
Prevention of Venous Thromboembolism
• Despite the well known risk of VTE and the publication of evidence-based guidelines for prevention, multiple medical record audits have demonstrated underuse of prophylaxis
Anderson FA Jr, et al. Ann Intern Med. 1991;115:591-595.Anderson FA Jr, et al. J Thromb Thrombolysis. 1998; 5 (1 Suppl):7S-11S.
Bratzler DW, et al. Arch Intern Med. 1998;158:1909-1912.Stratton MA, et al. Arch Intern Med. 2000;160:334-340.

Published Audits of VTE ProphylaxisGeneral Surgery
0
40
80
120
160
200
240
280
Moderate High Very High
Ca
se
s
Received Prophylaxis No Prophylaxis
30/86 (35%) 33/83 (40%)
97/250 (39%)
Use of any form of prophylaxis based on level of risk for venous thromboembolism among 419 Medicare patients from 20 hospitals undergoing major abdominothoracic surgery. Measures were implemented for patients at moderate risk (35%; 95% CI, 25-46%), at high risk (40%; 95% CI, 29-51%), and at very high risk (39%; 95% CI, 33-45%). Overall
utilization rate for prophylaxis was 38% (95% CI, 33-43%).
Bratzler DW, et al. Arch Intern Med. 1998;158:1909-1912.

24
Thromboprophylaxis Use in Practice1992-2002
Prophylaxis Patient Group Studies Patients Use (any)
Orthopedic surgery 4 20,216 90 % (57-98)
General surgery 7 2,473 73 % (38-98)
Critical care 14 3,654 69 % (33-100)
Gynecology 1 456 66 %
Medical patients 5 1,010 23 % (14-62)
How many patients with COPD, CVA, heart failure, pneumonia, etc do you have in your hospital that are not on DVT prophylaxis?

Prevention of VTE in Medical Patients
Amin A, Stemkowski S, Lin J, Yang G. J Thromb Haemost 2007; 5: 1610–6.

Prevention of VTE in Medical Patients
Amin A, Stemkowski S, Lin J, Yang G. J Thromb Haemost 2007; 5: 1610–6.

Diagnosis of VTE
• D-dimer (rule out only)
• Compression ultrasound
• CT angiography
Goldhaber SZ, Bounameaux H. Lancet. 2012 May 12; 379:1835-46.

Diagnosis of VTE
Goldhaber SZ, Bounameaux H. Lancet. 2012 May 12; 379:1835-46.

Prophylaxis and Treatment

30
Prophylaxis Modalities• Mechanical
– Graduated compression stockings (GCS) (e.g., “white hose”)
– Sequential compression devices• Venous foot pumps (currently recommended only for orthopedic
surgery in patients with bleeding risk)
In most studies, less effective than pharmacologic prophylaxis and patient compliance rates are
generally low.
Rates of compliance with mechanical forms of prophylaxis in many studies is less than 50% - has become a new target of malpractice litigation.
31
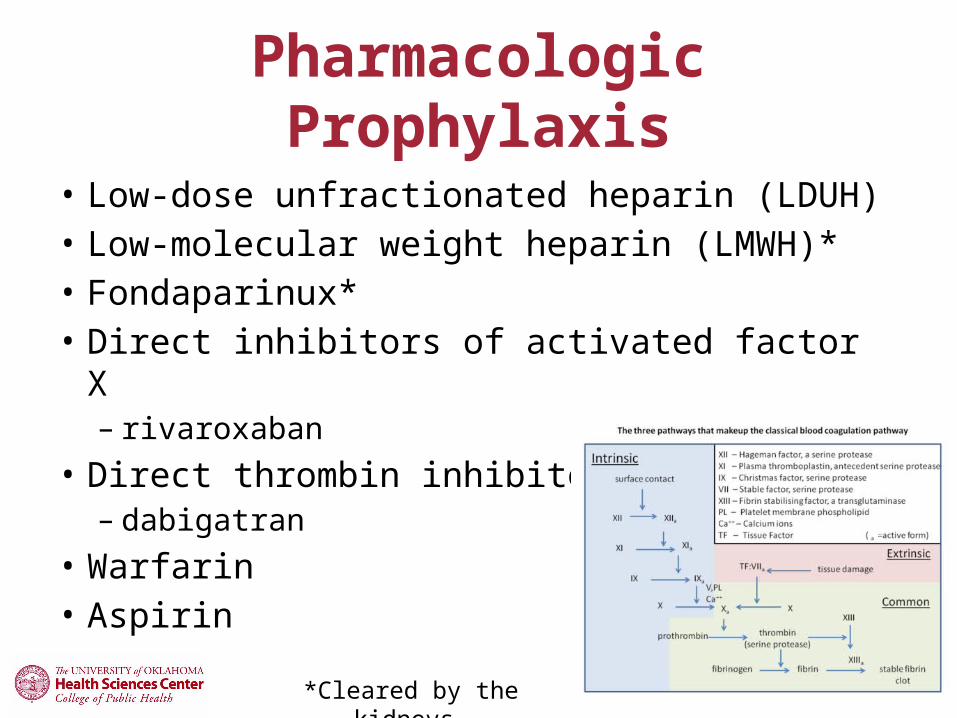
Pharmacologic Prophylaxis
• Low-dose unfractionated heparin (LDUH)• Low-molecular weight heparin (LMWH)*• Fondaparinux*• Direct inhibitors of activated factor X
– rivaroxaban• Direct thrombin inhibitors
– dabigatran• Warfarin• Aspirin
*Cleared by the kidneys.

Approach to Treatment

How long do you treat?
Duration of TreatmentEvidence
GradeFirst VTE event secondary to a reversible factor (“provoked”)
3 months 1A
First idiopathic (“unprovoked) VTE At the end of initial 3-month period In the absence of contraindication During long-term treatment
At least 3 monthsAssess for long-term RxLong-term RxAssess risk/benefit balance
1A1C1A1C
Recurrent VTE or strong thrombophilia Long-term Rx 1A
VTE secondary to cancer Long-term Rx, preferentially with LMWH during the first 3-6 months, then anticoagulate as long as the cancer is considered “active”
1A1C
Kearon C, et al. Chest 2008; 133 (6 suppl):454S-545S.

Do we have to use warfarin long-term?
Multicenter, double-blind study, patients with first-ever unprovoked venous thromboembolism who had completed 6 to 18 months of oral anticoagulant treatment were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years
Becattini C, et al. N Engl J Med 2012;366:1959-67.

35
Development of National Performance Measures to Prevent and Treat VTE

36
Why the need for performance measures?
• Despite widespread publication and dissemination of guidelines, practices have not changed at an acceptable pace– There are still far too many needless deaths from
VTE in the US
• Reasonably good evidence that using performance measures for accountability can accelerate the rate of change

37

38
Venous ThromboembolismStatement of Organization Policy
“Every healthcare facility shall have a written policy appropriate for its scope, that is evidence-based and that drives continuous quality improvement related to VTE risk assessment, prophylaxis, diagnosis, and treatment.”

39
Venous ThromboembolismCharacteristics of Preferred Practices
General• Protocol selection by multidisciplinary teams• System for ongoing QI• Provision for RA/stratification, prophylaxis,
diagnosis, treatment• QI activity for all phases of care• Provider education

40
Venous ThromboembolismCharacteristics of Preferred Practices
(cont.)
Risk Assessment/Stratification• RA on all patients using evidence-based policy• Documentation in patient record that done
Prophylaxis• Based on assessment & risk/benefit, efficacy/safety• Based on formal RA, consistent with accepted,
evidence-based guidelines

41
Venous ThromboembolismCharacteristics of Preferred Practices
(cont.)
Diagnosis• Objective testing to justify continued initial therapy
Treatment and Monitoring• Ensure safe anticoagulation, consider setting• Incorporate Safe Practice 29 • Patient education; consider setting and reading levels• Guideline-directed therapy• Address care setting transitions in therapy

42
Surgical Care Improvement ProjectFirst Two VTE Measures Endorsed by NQF
• Prevention of venous thromboembolism• Proportion who have recommended VTE
prophylaxis ordered
• Proportion who receive appropriate form of VTE prophylaxis (based on ACCP Consensus Recommendations) within 24 hours before or after surgery

43
Venous ThromboembolismTechnical Advisory Panel (TAP) charge
• Vet the 19 potential measures, agreed upon by the Steering Committee, through TAP and The Joint Commission survey processes
• Identify a subset of measures that help address the identified gaps within the endorsed VTE domains
• Oversee final development and testing of measures for Steering Committee and NQF endorsement consideration

44
6 Refined Measures That Were Endorsed
Risk Assessment/Prophylaxis domain Prophylaxis w/in 24 hours of admission or surgery,
OR a documented risk assessment showing that the patient does not need prophylaxis
Prophylaxis/documentation w/in 24 hours after ICU admission or surgery

45
6 Refined Measures That Were Endorsed
Patients w/overlap of anticoagulation therapy At least five calendar days of overlap and discharge with INR
> 2.0, or discharge on overlap therapy
Patient receiving UFH with dosage/platelet count monitoring by protocol/nomogram Nomogram/protocol incorporates routine platelet count
monitoring

46
6 Refined Measures Endorsed (cont.)
Treatment/Monitoring Domain (cont.)
– Discharge instructions consistent with Joint Commission safety goals (Follow-up Monitoring, Compliance Issues, Dietary Restrictions, Potential for Adverse Drug Reactions/Interactions)
Outcome Incidence of potentially-preventable VTE – proportion of
patients with hospital-acquired VTE who had NOT received VTE prophylaxis prior to the event
New Guidelines and Controversies

New Guidelines
http://www.chestnet.org/accp/guidelines/accp-antithrombotic-guidelines-9th-ed-now-available

The ACCP recommends that performance measures for quality improvement, performance-based reimbursement, and public reporting purposes should be based on rigorously developed guideline recommendations. However, not all recommendations graded highly according to the ACCP grading system (1A, 1B) are necessarily appropriate for development into such performance measures, and each one should be analyzed individually for importance, feasibility, usability, and scientific acceptability (National Quality Forum criteria). Performance measures developers should exercise caution in basing measures on recommendations that are graded 1C, 2A, 2B, and 2C, according to the ACCP Grading System1 as these should generally not be used in performance measures for quality improvement, performance-based reimbursement, and public reporting purposes.
ACCP Disclaimer

ACCP 9th EditionGeneral Overview
• For acutely ill hospitalized medical patients at increased risk of thrombosis, we recommend anticoagulant thromboprophylaxis with LMWH, LDUH, or fondaparinux (Grade 1B)– Mechanical prophylaxis (GCS or IPC) if bleeding or
high risk for bleeding• Similar recommendation for critically ill
patients

ACCP 9th EditionGeneral Overview
• For patients undergoing non-orthopedic surgery– Generally recommend the use of a risk assessment
tool (Rogers score or Caprini score) to determine need for prophylaxis
• Low risk of VTE (Rogers score < 7.0, Caprini score 0) no prophylaxis recommended other than early ambulation

Bahl V, et al. Ann Surg. 2010; 251:344-50.


Bahl V, et al. Ann Surg. 2010; 251:344-50.

Rogers SO, et al. J Am Coll Surg 2007;204:1211–1221.

Rogers SO, et al. J Am Coll Surg 2007;204:1211–1221.

ACCP 9th EditionGeneral Overview
• Patients undergoing major orthopedic surgery (THA, TKA, or HFS) recommend LMWH, fondaparinux, apixaban, dabigatran, rivaroxaban, LDUH, adjusted-dose warfarin, aspirin (all Grade 1B), or an IPC device (Grade 1C).– Subsequently recommend in THA, TKA, or HFS
LMWH the preferred agent (Grade 2B)

ACCP Guidelines
• The technical expert panel is evaluating new guidelines to consider revisions– No revisions likely before January 2014– Many of the recommendations in guidelines do
not have 1A and 1B grades and remain very controversial
– Most hospitalized patients have additional risk factors for VTE

59
Strategies for Improvement

60
Strategies to Improve VTE Prophylaxis
• Hospital policy of risk assessment or routine prophylaxis for all admitted patients– Most will have risk factors for VTE and should
receive prophylaxis– Preprinted protocols for surgical patients

61
Electronic Alerts to Prevent VTE among Hospitalized Patients
Control Alert group group P
No. 1,251 1,255
Any prophylaxis 15 % 34 % <0.001
VTE at 90 days 8.2 % * 4.9 % 0.001
Major bleeding 1.5 % 1.5 % NS
Kucher – N Engl J Med 2005;352:969
• Hospital computer system identified patient VTE risk factors• RCT: no physician alert vs physician alert

62
Electronic Alerts to Prevent VTE among Hospitalized Patients
Kucher – N Engl J Med 2005;352:969
• Among hospitalized patients with risk factors for VTE and not receiving prophylaxis, use of a physician VTE risk alert:– Improved use of prophylaxis by 130%
– Reduced symptomatic VTE by 41%
– Did not increase bleeding

Improving Compliance with Treatment Protocols
• Use of standardized protocols, nomograms, algorithms, or preprinted orders– Address overlap (either 5 days in hospital or
discharge on overlap)– When used, UFH should be managed by
nomogram/protocol, and the protocol should ensure routine platelet count monitoring

Essential Elements for Improvement
• Institutional support
• A multidisciplinary team or steering committee
• Reliable data collection and performance tracking
• Specific goals or aims
• A proven QI framework
• Protocols
SHM Resource Room. http://www.hospitalmedicine.org. Accessed September 2009.

Risk Assessment Prophylaxis
Low Ambulatory patient without VTE risk factors; observation patient with expected LOS 2 days; same day surgery or minor surgery
Early ambulation
Moderate All other patients (not in low-risk or high-risk category); most medical/surgical patients; respiratory insufficiency, heart failure, acute infectious, or inflammatory disease
UFH 5000 units SC q 8 hours; OR LMWH q day; OR UFH 5000 units SC q 12 hours (if weight < 50 kg or age > 75 years); AND suggest adding IPC
High Lower extremity arthroplasty; hip, pelvic, or severe lower extremity fractures; acute SCI with paresis; multiple major trauma; abdominal or pelvic surgery for cancer
LMWH (UFH if ESRD); OR fondaparinux 2.5 mg SC daily; OR warfarin, INR 2-3; AND IPC (unless not feasible)
Maynard GA, et al. J Hosp Med 2009 Sep 14. [Epub ahead of print]

Maynard GA, et al. J Hosp Med 2009 Sep 14. [Epub ahead of print]

Conclusions
• VTE remains a substantial health problem in the US
• VTE prophylaxis remains underutilized
• National performance measures may address both prophylaxis and treatment of VTE across broad hospital populations
67

Related Documents











