Page 1/17 Preventing and arresting primary tooth enamel lesions using self-assembling peptide P 11 -4 in vitro Nour Wahba Department of Pediatric and Dental Public health, Faculty of Dentistry, Ain Shams University, Cairo Falk Schwendicke Department of Oral Diagnostics, Digital Health and Health Services Research, Charitè - Universitätmedizin Berlin Mohamed Amr Kamel Department of Operative Dentistry, Faculty of Dentistry, Ain Shams University Gehan Allam Department of Pediatric Dentistry and Dental Public Health, Faculty od Dentistry, Ain Shams University, Cairo Sebastian Paris Department of Operative and Preventive Dentistry, Charitè - Universitätmedizin Berlin Noha Kabil Department of Pediatric Dentistry and Dental Public Health, Faculty of Dentistry, Ain Shams University, Cairo Paul-Georg Jost-Brinkmann Department of Orthodontics, Dentofacial Orthopedics and Pedodontics, Charitè - Universitätmedizin Berlin Karim Elhennawy ( [email protected] ) Charite Universitatsmedizin Berlin https://orcid.org/0000-0002-5216-9452 Research article Keywords: Caries, prevention, self-assembling peptides, primary teeth, microradiography, demineralization Posted Date: February 16th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-228625/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Page 1/17
Preventing and arresting primary tooth enamellesions using self-assembling peptide P11-4 in vitroNour Wahba
Department of Pediatric and Dental Public health, Faculty of Dentistry, Ain Shams University, CairoFalk Schwendicke
Department of Oral Diagnostics, Digital Health and Health Services Research, Charitè - UniversitätmedizinBerlinMohamed Amr Kamel
Department of Operative Dentistry, Faculty of Dentistry, Ain Shams UniversityGehan Allam
Department of Pediatric Dentistry and Dental Public Health, Faculty od Dentistry, Ain Shams University,CairoSebastian Paris
Department of Operative and Preventive Dentistry, Charitè - Universitätmedizin BerlinNoha Kabil
Department of Pediatric Dentistry and Dental Public Health, Faculty of Dentistry, Ain Shams University, CairoPaul-Georg Jost-Brinkmann
Department of Orthodontics, Dentofacial Orthopedics and Pedodontics, Charitè - Universitätmedizin BerlinKarim Elhennawy ( [email protected] )
Charite Universitatsmedizin Berlin https://orcid.org/0000-0002-5216-9452
Research article
Keywords: Caries, prevention, self-assembling peptides, primary teeth, microradiography, demineralization
Posted Date: February 16th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-228625/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. ReadFull License
Page 2/17
AbstractBackground: Self-assembling peptides (SAP) may prevent and/or arrest caries lesions. The aim of the studywas to evaluate SAP for caries prevention and arrest in primary tooth enamel in vitro.
Methods: 215 extracted primary teeth were used. In the prevention experiment, self-assembling peptide forprevention (SAPP), �uoride varnish/mouthwash (FV/FMW), casein-phosphopeptide amorphous-calciumphosphate (CPP-ACP), nanohydroxy-apatite (nHA) were applied. Samples were subjected to a demineralizingpH-cycling for 14-days. In the arrest experiment, 60 samples were pre-demineralized and induced lesionstreated using self-assembling peptide for repair (SAPR), FV, CPP-ACP plus �uoride and resin in�ltration (RI),and submitted to pH-cycling. Thirty-�ve samples were used as negative controls (NC). Mineral loss and itsdifferences (Δ/ΔΔZ) were determined using transversal microradiography.
Results: FV (ΔZ median: -46 [interquartile range: 189] vol%×µm) and FMW (-28 [129] vol%×µm) preventedcaries signi�cantly more effective than all other groups (p<0.05), which did not show signi�cant preventiveeffects compared with NC (ΔZ=1446 [378] vol%×µm). RI (ΔΔZ=1808 [2193] vol%×µm) and FV (ΔΔZ=1494[4274] vol%×µm) arrested lesions compared with NC (ΔΔZ=5605 [1371] vol%×µm; p<0.05), while SAPR andCPP-ACPF did not show such arrest.
Conclusions: FV and FMW showed the largest caries-preventive effect, while RI and FV arrested lesionprogression in primary tooth enamel in vitro.
Clinical signi�cance: Preventing and arresting caries lesion allows decreasing invasive treatment needs andpatient’s morbidity and fosters the application of minimal invasive dentistry approach.
BackgroundCaries in the primary dentition is one of the most prevalent conditions of humankind [1] with over 500 millionuntreated cases and over 120 million incident cases each year. Conventional treatment of caries lesions inprimary teeth using restorative approaches is challenging due to a combination of behavioral and micro- andmacro-anatomic factors, and failure rates of most restorations in the primary dentition being high [2].Dentists frequently refrain from restoring caries lesions in the primary dentition at all, even if cavitated. Cariesin the primary dentition is a major reason for hospitalization for both routine treatments and emergencies [3,4].
Hence, there is a great need for both preventing and arresting caries lesions in the primary dentition. The mostaccepted strategies for prevention are the delivery of �uoride, mainly via toothpaste or, in high-risk individuals,varnishes, gels or mouthwashes, as well as routine oral hygiene care and dietary control. The use of�uoridated toothpaste for caries prevention is supported by a large body of evidence [5]. Similarly, �uoridevarnish (FV) application has been found highly e�cacious for caries prevention [6] and, if applied risk-adjusted, cost-effective [7]. The use of �uoride mouthwash (FMW) also has been supported by a range ofstudies [8]. However, and especially in smaller children, the delivery of �uoride is limited by the risks ofchronic and acute toxicity.
Page 3/17
Alternative interventions to control the balance between de- and remineralization on the surface of primaryteeth, speci�cally enamel, have been sought, among them casein-phosphopeptide amorphous calciumphosphate (CPP-ACP) with or without the addition of �uoride for home and in-o�ce use, nanohydroxyapatite(nHA) or self-assembling peptides P11-4 (SAP) [9]. SAP are oligomer β-sheet-forming peptides (Ace-Gln-Gln-Arg-Phe-Glu-Trp-Glu-Phe-Glu-Gln-Gln-Nh2), which when subjected to speci�c environmental conditions havethe ability to self-assemble into �brillar scaffolds thereby creating β-sheet called ‘nanotapes’ [10]. Theprocess of self-assembly continues while the nanotapes connect by pairing and transform into ribbons,which further self-assemble to form �brils and �bers [11], leading to scaffold-like structures attractingcalcium and phosphate deposition [12–14]. SAP thereby is supposed to facilitate biomimeticremineralization of hard dental tissue [13] and has been found e�cacious clinically, too [15].
Similarly, for lesion arrest, the in-o�ce application of FV or CPP-ACP, for example in higher concentrations[16], or SAP has been suggested [17]. Alternatively, resin in�ltration (RI), where the lesion is in�ltrated withlowly �lled resins, which are light-cured and subsequently block any acid diffusion into the lesion body andhence mineral loss from it, can be applied to inhibit caries lesion progression [18]. There is a robust body ofclinical data supporting RI, for example to arrest proximal lesions, mainly in the permanent dentition [19].
Overall, the majority of studies on preventing and/or arresting lesions using the described measures wereconducted in the permanent, not the primary dentition. The body of evidence comparing �uoride applications,other mineral suppliers, RI or SAP is extremely limited. Therefore, we aimed to compare caries prevention andinhibition of lesion progression using SAP against those of other established measures in vitro, hypothesizingSAP to have signi�cantly superior caries-preventive and arresting properties.
Methods
Study designThis study followed the CRIS (checklist for reporting In-vitro studies) guidelines [20] and was based on thefundamentals of ethical research practice. An informed consent was obtained from all patients’ legalguardians in order to include her/his extracted teeth in the experiments. This study assessed the caries-preventive and arresting effect of SAP and various alternatives, namely FV, FMW, CPP-ACP, CPP-ACP with�uoride (CPP-ACPF) and nHA for caries prevention, and FV, CPP-ACPF and RI for lesion arrest in primary toothenamel in vitro (Table 1).
Page 4/17
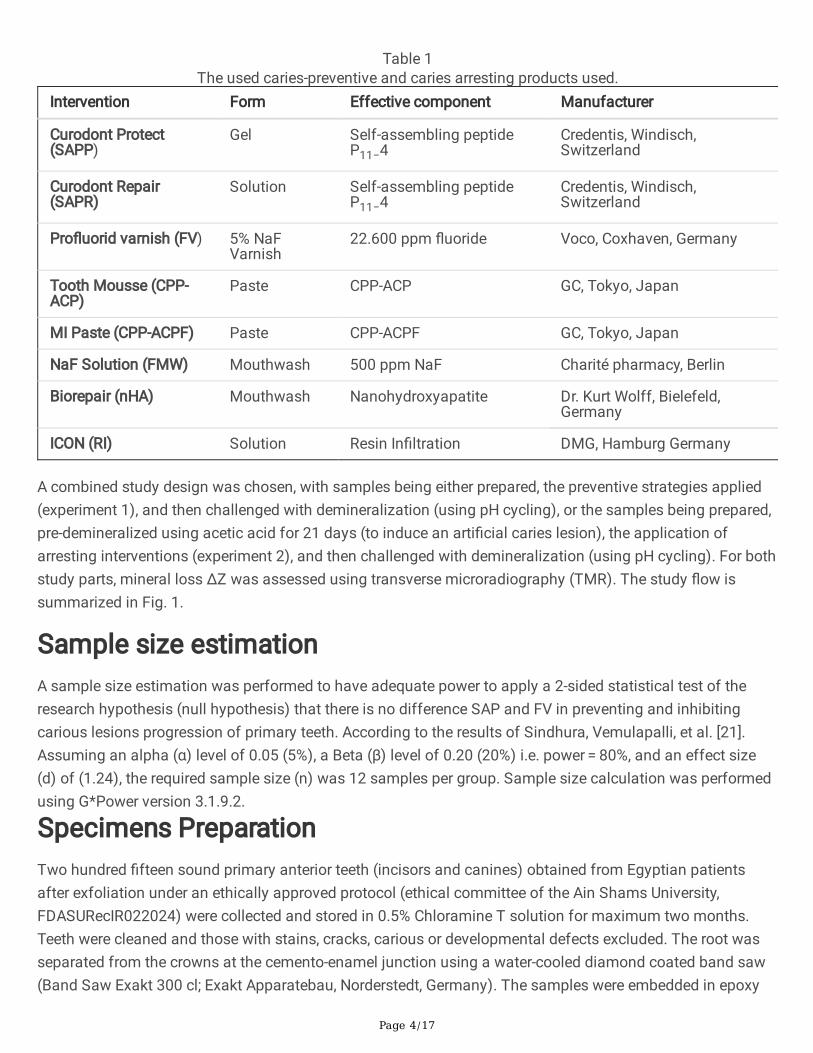
Table 1The used caries-preventive and caries arresting products used.
Intervention Form Effective component Manufacturer
Curodont Protect(SAPP)
Gel Self-assembling peptideP11−4
Credentis, Windisch,Switzerland
Curodont Repair(SAPR)
Solution Self-assembling peptideP11−4
Credentis, Windisch,Switzerland
Pro�uorid varnish (FV) 5% NaFVarnish
22.600 ppm �uoride Voco, Coxhaven, Germany
Tooth Mousse (CPP-ACP)
Paste CPP-ACP GC, Tokyo, Japan
MI Paste (CPP-ACPF) Paste CPP-ACPF GC, Tokyo, Japan
NaF Solution (FMW) Mouthwash 500 ppm NaF Charité pharmacy, Berlin
Biorepair (nHA) Mouthwash Nanohydroxyapatite Dr. Kurt Wolff, Bielefeld,Germany
ICON (RI) Solution Resin In�ltration DMG, Hamburg Germany
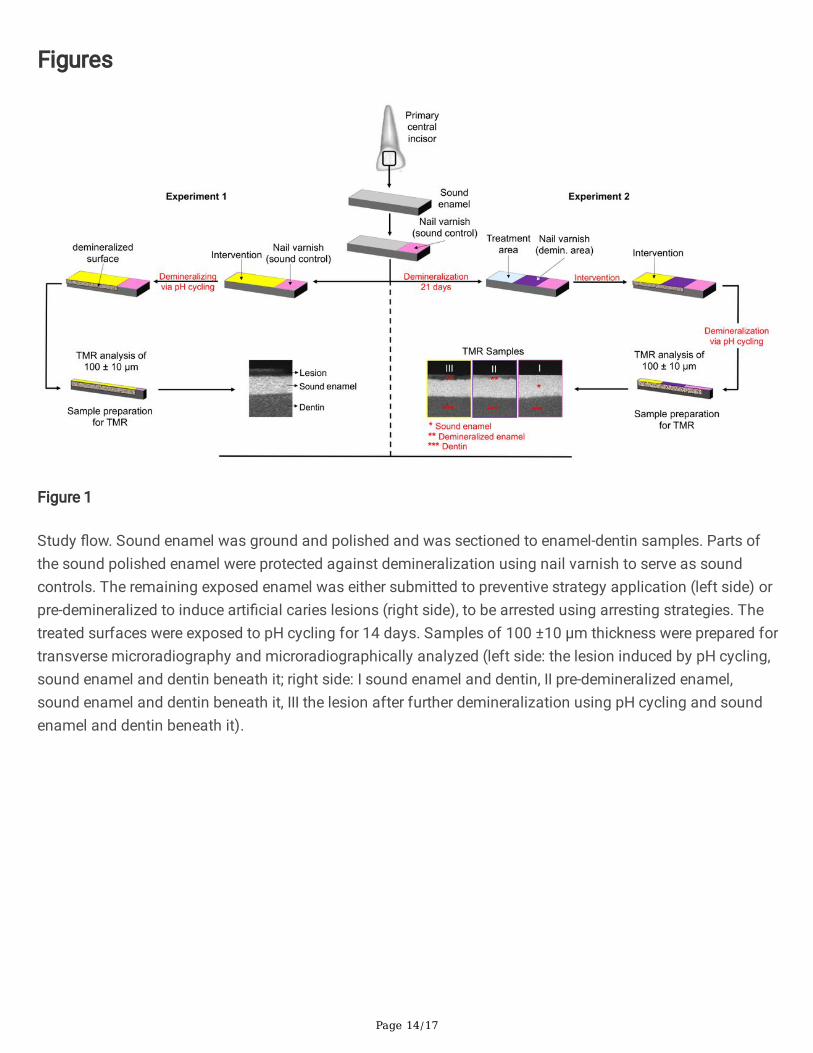
A combined study design was chosen, with samples being either prepared, the preventive strategies applied(experiment 1), and then challenged with demineralization (using pH cycling), or the samples being prepared,pre-demineralized using acetic acid for 21 days (to induce an arti�cial caries lesion), the application ofarresting interventions (experiment 2), and then challenged with demineralization (using pH cycling). For bothstudy parts, mineral loss ΔZ was assessed using transverse microradiography (TMR). The study �ow issummarized in Fig. 1.
Sample size estimationA sample size estimation was performed to have adequate power to apply a 2-sided statistical test of theresearch hypothesis (null hypothesis) that there is no difference SAP and FV in preventing and inhibitingcarious lesions progression of primary teeth. According to the results of Sindhura, Vemulapalli, et al. [21].Assuming an alpha (α) level of 0.05 (5%), a Beta (β) level of 0.20 (20%) i.e. power = 80%, and an effect size(d) of (1.24), the required sample size (n) was 12 samples per group. Sample size calculation was performedusing G*Power version 3.1.9.2.
Specimens PreparationTwo hundred �fteen sound primary anterior teeth (incisors and canines) obtained from Egyptian patientsafter exfoliation under an ethically approved protocol (ethical committee of the Ain Shams University,FDASURecIR022024) were collected and stored in 0.5% Chloramine T solution for maximum two months.Teeth were cleaned and those with stains, cracks, carious or developmental defects excluded. The root wasseparated from the crowns at the cemento-enamel junction using a water-cooled diamond coated band saw(Band Saw Exakt 300 cl; Exakt Apparatebau, Norderstedt, Germany). The samples were embedded in epoxy
Page 5/17
resin (Technovit 4071, Heraeus Kulzer, Hanau, Germany), with the labial surfaces of incisors and the lingualsurfaces of canines facing upward, ground �at and polished sequentially (Mikroschleifsystem; AbrasivePaper WS �ex 18C, SiC 1200–4000, Exakt Apparatebau, Norderstedt, Germany) until a surface ofapproximately 2 mm x 2 mm enamel was exposed.
InterventionsThe 215 samples were divided into the two experimental arms; 120 were used to assess the caries preventiveeffect, 60 to assess lesion arrest, and 35 served as negative control group (NC), where 20 were used for the1st experiment and 15 for the 2nd experiment. One third of the exposed surfaces of all samples wasprotected against the subsequent demineralization challenge using a nail varnish (Maybelline New YorkExpress Finish 40, New York, USA), serving as sound control.
Experiment 1:To test the caries preventive effect, the remaining two thirds of the exposed surfaces of the 120samples were treated using one of six interventions (n = 20/group, Table 1) before being challenged fordemineralization: (1) SAPP (Curodont Protect, Credentis, Windisch, Switzerland), (2) FV (5% NaF Pro�uorid,Voco, Cuxhaven, Germany), (3) CPP-ACP (Tooth Mousse, GC, Tokyo, Japan), (4) CPP-ACP plus �uoride (CPP-ACPF, MI Paste Plus, GC, Tokyo, Japan), (5) 500 ppm sodium Fluoride Mouthwash (FMW) (pharmacy of theCharité - Universitätsmedizin Berlin), (6) nHA mouthwash (Biorepair Mouth Wash, Dr. Kurt Wolff, Bielefeld,Germany). Curodont Protect gel was applied on a semi-dry surface with a microbrush, rubbed in and left for acouple of minutes to dry. It was then washed away as instructed by the manufacturer. FV, CPP-ACP and CPP-ACPF were applied on a dry surface with a microbrush and left 30 min to set, then rinsed off with water tomimic the conditions of the oral cavity. Both mouthwashes were utilized once daily after the demineralizationcycle for 15 minutes by storing the samples in them, while the other samples were stored in distilled waterduring that time.
Experiment 2: To test lesion arrest, the remaining two thirds of the exposed surfaces of the 60 samples werepre-demineralized using 3 mM CaCl2, 3 mM KH2PO4, 0,006 mM methylhydroxydiphosphanate (MHDP),50 mM CH3COOH, 10M KOH. The pH was adjusted to 4.95 using KOH for 21 days (Carl Roth, Karlsruhe,Germany) [22]. Half of the demineralized surface was covered with a nail varnish to allow the assessment ofthe mineral loss of the lesions after the �rst and prior to the second demineralization challenge. Theremaining one third of the exposed surface of the sample received one of four interventions (n = 15/group,Table 1) prior to being challenged again for demineralization: (1) SAPR (Curodont Repair, Credentis, Windisch,Switzerland), (2) 5% FV (5% NaF Pro�uorid, Voco, Cuxhaven, Germany), (3) CPP-ACPF (MI Paste Plus, GC), (4)RI (Icon DMG, Hamburg, Germany). For SAPR, samples were etched with 37% phosphoric acid (Fine Etch 37,Spident, Korea) for �ve s and rinsed with tap water. After drying the surface, Curodont Repair (In Vitro Vial,Credentis, Windisch, Switzerland) was dissolved without any further puri�cation in 50 µL distilled waterapplied on each sample and left 5 min for setting. FV and CPP-ACPF were applied as described. Before RI,samples were etched using 37% phosphoric acid (FineEtch 37) for �ve s. The specimens were thereafterwashed and dried using Icon Dry for 30 s and in�ltrated using Icon In�ltrant for 3 min. After removing theexcess material, light-curing was performed using a LED curing light (Valo, Ultradent, Salt Lake City, USA) withan intensity of 1400 mW/cm2 for 40 s from < 1 mm distance. The procedure was repeated, with the in�ltrantbeing applied for only 1 min, as recommended by the manufacturer. For both groups, an untreated negative
Page 6/17
control (NC) (n = 35) was carried along the experiments, where 20 samples were utilized for experiment no.1and 15 for experiment no.2.
Demineralization challenge using pH cyclingAll samples were subsequently subjected to a pH cycling using a demineralization solution containing2.2 mM CaCl2, 2.2 mM NaH2PO4 and 50 mM acetic acid adjusted to a pH of 4.8 by NaOH (Carl Roth,Karlsruhe, Germany). The remineralizing solution contained 1.5 mM CaCl2, 0.9 mM NaH2PO4 and 0.15 M KCladjusted to a pH of 7.0 by KOH (Carl Roth, Karlsruhe, Germany). Each group was cycled separately for 8 h in100 ml demineralizing solution and 16 h in 100 ml remineralizing solution for 14 days at room temperaturewithout agitation. Between the de-and remineralizing cycles, the samples were washed with distilled water.The mouthwashes in the prevention groups were renewed daily [23].
Transversal Microradiography (TMR)Samples were cut along their longitudinal axes (Band Saw Exakt, Exakt Apparatebau, Norderstedt, Germany)and thereafter, thin plano-parallel slices with a thickness of 100 ± 10 µm prepared (Mikroschleifsystem, ExaktApparatebau, Norderstedt, Germany). During the sample preparation, �ve samples were lost. The sampleswere placed on �lm holders and exposed to a nickel-�ltered copper radiation source operating at 20 kV and20 mA with an exposure time of 10 s. Films (Fine 71337, Fuji�lm, Tokyo, Japan) were developed according tothe manufacturer’s instructions under standardized conditions. The microradiographs were analyzed with adigital image-analyzing system (XC 77 CE, Sony, Tokyo, Japan) interfaced with a universal microscope(Axioskop 60318, Zeiss, Oberkochen, Germany) and a personal computer (TMR for Windows 2.0.27.2,Inspector, Research, Amsterdam, Netherland). Calibration standardization was done using an aluminum step-wedge with different aluminum thicknesses and a calibration curve between aluminum thickness and greylevels was constructed.
Statistical AnalysisStatistical analysis was performed using SPSS 20 (IBM, Armonk, NY, USA). Data were controlled for normaldistribution using Shapiro-Wilk-test. Mineral loss ΔZ was calculated for each group as the median ΔZtogether with interquartile deviations (ID) and expressed as vol.%/µm. In addition, the lesion depth (LD) wasdetermined. Analyses of variance and post-hoc Tukey’s honestly signi�cant difference (HSD) test were usedto compare Δ/ΔΔZ between groups. The level of signi�cance was set at p < 0.05.
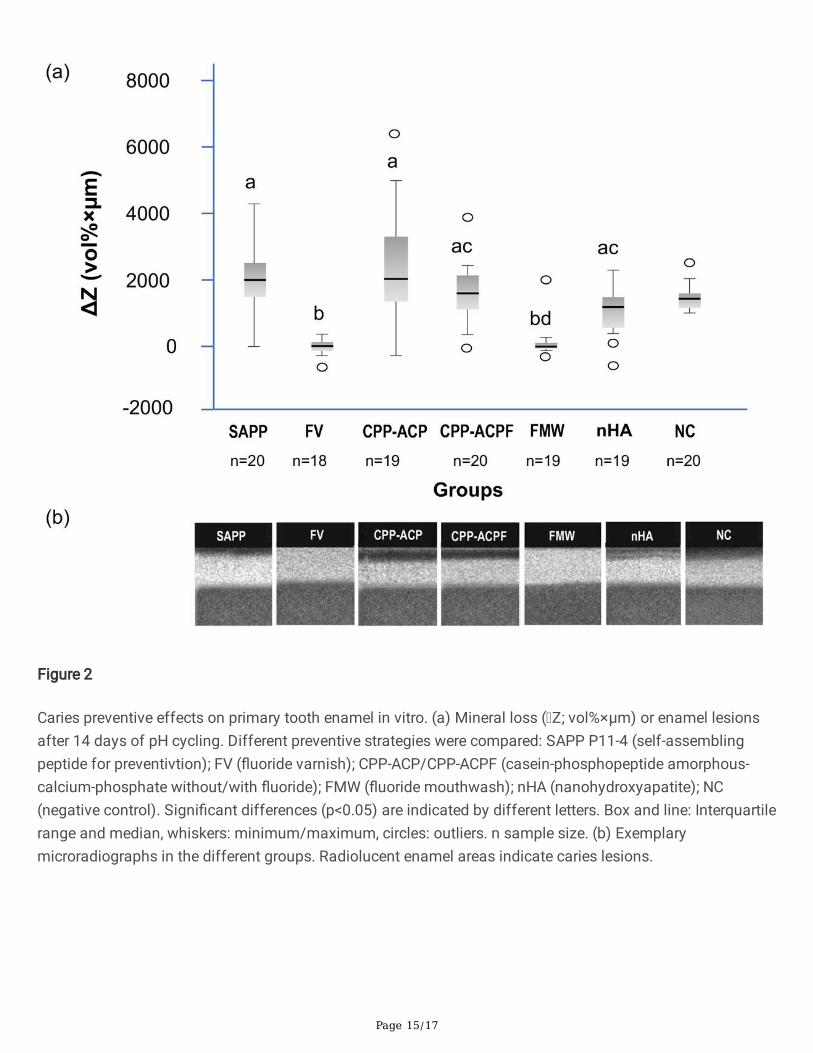
ResultsWhen preventing the development of caries lesions, ΔZ was signi�cantly lower for FV (median: -46[interquartile range: 189] vol%×µm) and FMW (-28 [129] vol%×µm) than all other groups (p < 0.05). SAPP(1956 [11826] vol%×µm) and CPP-ACPF (ΔZ = 1606 [935] vol%×µm), CPP-ACP (ΔZ = 2099 [2042] vol%×µm)and nHA (ΔZ = 1074 [971] vol%×µm) did not show signi�cantly different ΔZ than untreated controls (ΔZ = 1446 [378] vol%×µm; p < 0.001, Fig. 2). Exemplary microradiographs are shown in Fig. 2.
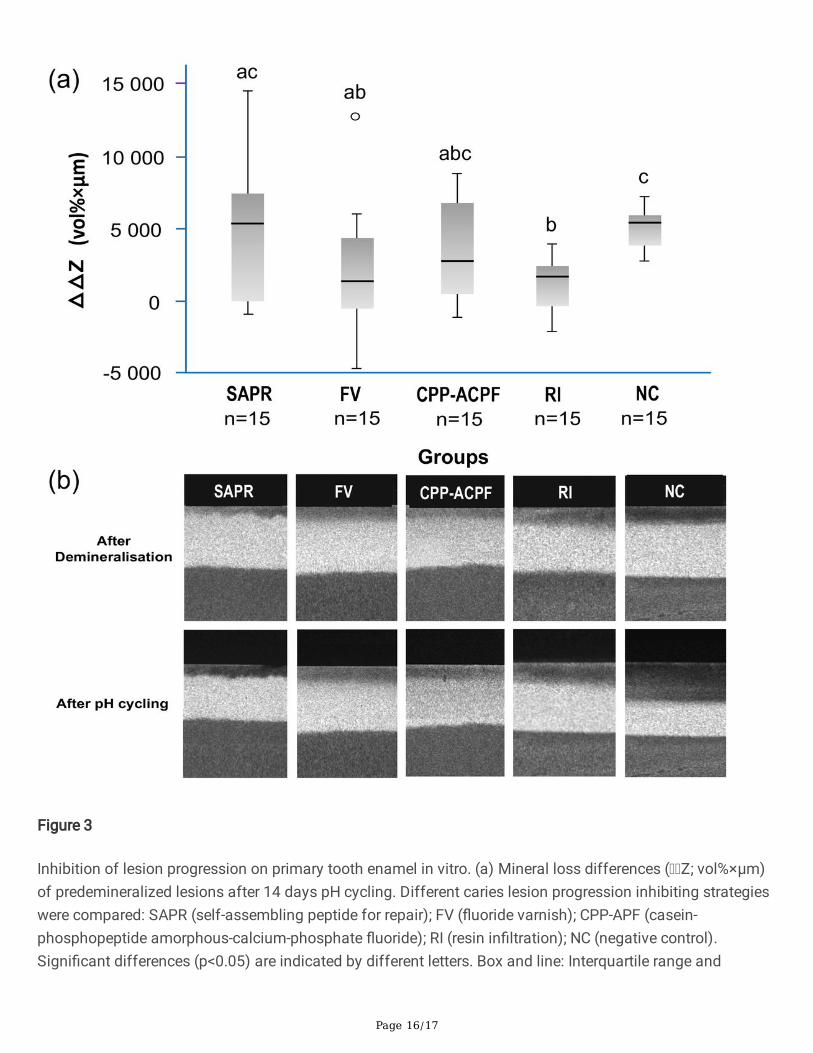
When arresting caries lesions, ΔΔZ was signi�cantly lower in RI (ΔΔZ = 1808 [2193] vol%×µm) than SAPR(ΔΔZ = 5293 [7804] vol%×µm) and NC (ΔΔZ = 5605 [1371] vol%×µm); FV (ΔΔZ = 1494 [4274] vol%×µm) also
Page 7/17
showed ΔΔZ lower than NC. No signi�cant differences were found between the other groups (p > 0.05; Fig. 3).Exemplary microradiographs are shown in Fig. 3.
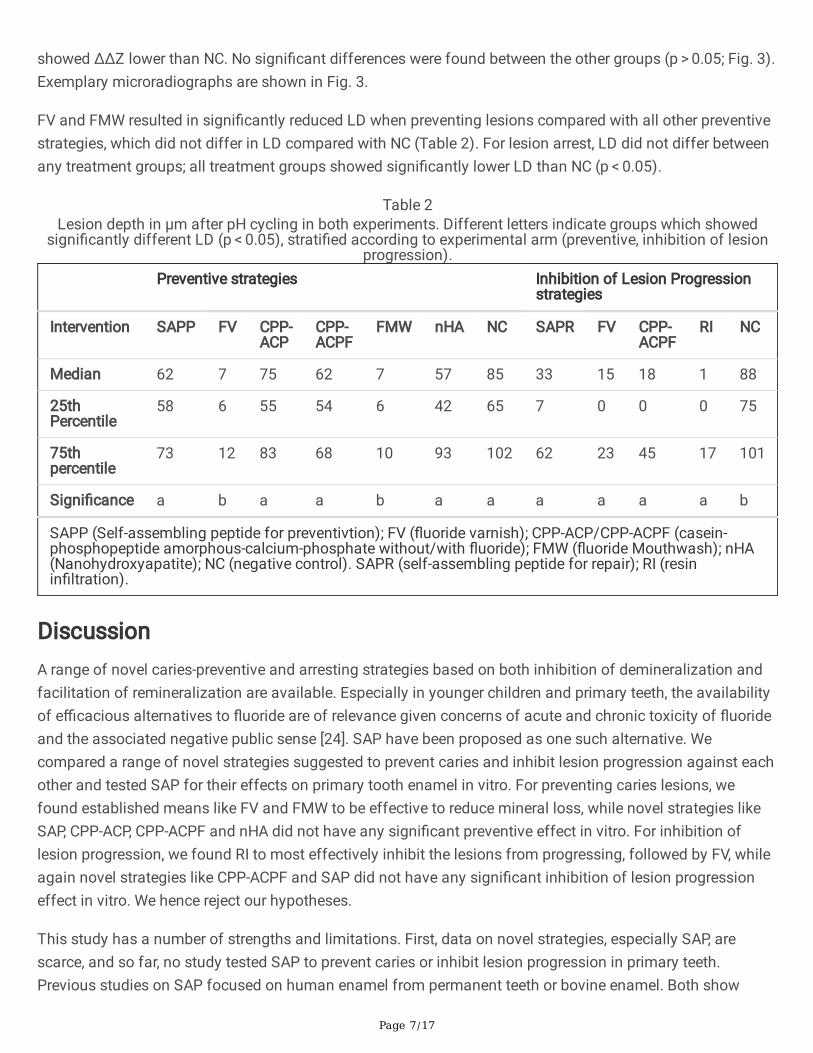
FV and FMW resulted in signi�cantly reduced LD when preventing lesions compared with all other preventivestrategies, which did not differ in LD compared with NC (Table 2). For lesion arrest, LD did not differ betweenany treatment groups; all treatment groups showed signi�cantly lower LD than NC (p < 0.05).
Table 2Lesion depth in µm after pH cycling in both experiments. Different letters indicate groups which showed
signi�cantly different LD (p < 0.05), strati�ed according to experimental arm (preventive, inhibition of lesionprogression).
Preventive strategies Inhibition of Lesion Progressionstrategies
Intervention SAPP FV CPP-ACP
CPP-ACPF
FMW nHA NC SAPR FV CPP-ACPF
RI NC
Median 62 7 75 62 7 57 85 33 15 18 1 88
25thPercentile
58 6 55 54 6 42 65 7 0 0 0 75
75thpercentile
73 12 83 68 10 93 102 62 23 45 17 101
Signi�cance a b a a b a a a a a a b
SAPP (Self-assembling peptide for preventivtion); FV (�uoride varnish); CPP-ACP/CPP-ACPF (casein-phosphopeptide amorphous-calcium-phosphate without/with �uoride); FMW (�uoride Mouthwash); nHA(Nanohydroxyapatite); NC (negative control). SAPR (self-assembling peptide for repair); RI (resinin�ltration).
DiscussionA range of novel caries-preventive and arresting strategies based on both inhibition of demineralization andfacilitation of remineralization are available. Especially in younger children and primary teeth, the availabilityof e�cacious alternatives to �uoride are of relevance given concerns of acute and chronic toxicity of �uorideand the associated negative public sense [24]. SAP have been proposed as one such alternative. Wecompared a range of novel strategies suggested to prevent caries and inhibit lesion progression against eachother and tested SAP for their effects on primary tooth enamel in vitro. For preventing caries lesions, wefound established means like FV and FMW to be effective to reduce mineral loss, while novel strategies likeSAP, CPP-ACP, CPP-ACPF and nHA did not have any signi�cant preventive effect in vitro. For inhibition oflesion progression, we found RI to most effectively inhibit the lesions from progressing, followed by FV, whileagain novel strategies like CPP-ACPF and SAP did not have any signi�cant inhibition of lesion progressioneffect in vitro. We hence reject our hypotheses.
This study has a number of strengths and limitations. First, data on novel strategies, especially SAP, arescarce, and so far, no study tested SAP to prevent caries or inhibit lesion progression in primary teeth.Previous studies on SAP focused on human enamel from permanent teeth or bovine enamel. Both show

Page 8/17
different mineralization and maturation potential than human primary tooth enamel. Second, SAP havelargely been tested for lesion arrest (i.e. facilitation of remineralization), not prevention [25], and this study isone of few testing this novel strategy for preventive applications as well as caries arrest. Third, theassessment of mineral loss using transverse microradiography is highly sensitive and a valid method thatwas not employed in previous studies on SAP. Instead, scanning electron microscopy (SEM), surfacemicrohardness or laser �uorescence, which are all only determining proxies for mineral loss [26, 27] had beenused. Fourth, and as a limitation, the employed in vitro protocol may have biased our �ndings to somedegree. Notably, grinding and polishing the enamel surface has removed the aprismatic enamel surface layerwhich is hypothesized to be required for SAP and SAPR action: On prismatic enamel, columnar calcium of thehydroxyapatite crystal is not available any longer; it is assumed that peptide matrix development may beimpeded to some degree in prismatic compared with aprismatic enamel. We nevertheless used the describedsetup, as only then valid mineral loss measurements in TMR are possible. Moreover, and notable, theaprismatic outermost layer of enamel is usually gradually worn off in a clinical setting, too, at leastocclusally, and any clinical e�cacy of self-assembling peptides might be reduced if strongly relying on thisaprismatic enamel being available. In addition, previous studies had by large employed polished specimens,which is why we aimed to retain this concept for reasons of comparability [26, 27, 25]. Fifth, we applied SAPonly once, i.e. before the 14d pH cycling period for reasons for standardization (other materials, e.g. FV, werealso only applied once). The manufacturer recommends applying it 1–2 times per week. Also, we neitheremployed human nor arti�cial saliva, which has been suggested to be required for full action of SAP, as the 3-dimensional matrix formed by the peptides increases the surface area for calcium and phosphate deposition,present in the saliva, thereby allowing the formation of de novo hydroxyapatite crystals [13, 14, 12].Application frequency and the availability of saliva might explain the differences between our �ndings andthose yielded in situ and in vivo (8), with saliva also being a relevant source of mineralization related to�uoride applications, for instance. Furthermore, we employed an etching step when testing lesion arrest usingSAP to mimic its clinical application. Etching of our polished samples might have removed the remainingpseudo-intact surface layer of the lesion claimed to be needed for SAP to effectively remineralize the enamel.The etching step was suggested in vivo to clean the pseudo-intact surface of enamel from pellicle andremove mineral debris; both are not present in arti�cially induced enamel lesions.
A range of �ndings needs to be discussed. SAP were not effective to prevent caries or inhibit lesionprogression. A limited body of evidence on SAP is available, as discussed, and our �ndings align with some,but not all of the reported studies. This might be partially due to the mentioned methodological reasons(application time and frequency, absence of aprismatic enamel, lack of saliva and pellicle formation).However, especially for SAP, there remain a number of questions towards its hypothesized preventivemechanism: SAP are designed to assemble in the acidic environment of an active caries lesion and thenattract minerals present in human saliva. It is unclear how this mechanism should apply to prevent lesions. Inour study, it cannot be excluded that the material was washed away during the �rst demineralization cycles,or that only very thin peptide layers formed on the sound enamel surfaces, possibly insu�cient to protect theenamel from subsequent demineralization.
Topical �uoride is considered the gold standard for caries prevention and lesion arrest (9). This wascon�rmed by our study. There is evidence suggesting that SAP should be combined with �uoride to harness
Page 9/17
their complementary mechanism and location of action when it comes to inhibiting lesion progression(�uoride mainly acts on the pseudo-intact surface of initial lesions (9), while SAP is suggested to diffuse intothe subsurface body of the lesion (1)). In our study, a possible advantage of the used FV was its consistencyand stickiness. It is possible that FV not only had a chemical but also mechanical effect by “sealing” thesurface, thereby protecting it from demineralization. Such sealing effect has been described for FV in studieson root caries prevention [28]. Given that we also found FMW to be e�cacious, this explanation may not fullyapply, though (notably, however, FMW was provided daily in contrast to most other alternatives).
RI is well known for its lesion progression inhibition in non-cavitated lesions by in�ltrating carious enamelporosities and thereby occluding the diffusion pathways leading to caries arrest [29]. RI has beendemonstrated to be superior to �uoride-based alternatives for lesion arrest by a range of clinical studies [19],also in the primary dentition [30], and our data also point into this direction. Notably, the application of RI istechnique-sensitive, something which may be relevant especially in the primary dentition and in children.
CPP-ACP and CPP-ACPF did not show any caries preventive or lesion progression inhibiting effect in ourstudy, which may be attributed to the fact that their effect is thought to be enhanced by the presence of abio�lm, which acts as a reservoir for the delivered calcium and phosphate ions and hence prevents mineralloss in intermittent periods of demineralization. Moreover, and as discussed for SAP, the applicationfrequency of CPP-ACP and CPP-ACPF might have been insu�cient.
Based on our results, a range of future directions can be derived. First, future in vitro studies assessing SAPshould aim to mimic the aprismatic enamel layer even when using ground specimens. Second, theapplication of saliva prior to remineralization may be recommended in an in vitro setting to allow pellicleformation and simulate clinical conditions as far as possible. Alternative, in situ designs may be employed.Third, mineral loss measurement should not focus on artifact-prone methods (like laser-�uorescence) orunsuitable proxies (like SEM evaluation), but strive to truly determine the mineralization effects, for exampleusing TMR, transverse wavelength-independent microradiography or micro-CT. Last, clinical studies should beemployed before translating our �ndings into any clinical recommendations; so far, clinical data largelyfocused on lesion remineralization, as described.
ConclusionIn conclusion, and within the described limitations, FV and FMW showed consistent and signi�cant cariespreventive effects on human primary teeth enamel in vitro, while RI and FV were shown to be effective toinhibit caries lesion progression in this set-up. SAP, CPP-ACP and CPP-ACPF and nHA did not show anysigni�cant caries preventive or progression inhibition effects.
AbbreviationsSAPSelf-assembling peptidesSAPPSelf-assembling peptides for prevention
Page 10/17
FVFluoride varnishFMWFluoride mouthwashCPP-ACPCasein-phosphopeptide amorphous-calcium phosphatenHANanohydroxy-apatiteRIResin in�ltrationNCUntreated controlsSAPRSelf-assembling peptides for repairAce-Gln-Gln-Arg-Phe-Glu-Trp-Glu-Phe-Glu-Gln-Gln-Nh2
oligomer β-sheet-forming peptidesCRISChecklist for reporting In-vitro studiesCPP-ACPFCasein -phosphopeptide amorphous-calcium phosphate with �uorideTMRTransverse microradiographyIDInterquartile deviationsLDLesion depthHSDPost-hoc Tukey’s honestly signi�cant differenceSEMScanning electron microscopy
DeclarationsEthics approval:
The study was approved by the ethical committee of the Ain Shams University, FDASURecIR022024. Thisarticle does not contain any studies with human participants or animals performed by any of the authors.
Consent to participate:
An informed consent was obtained from the patients’ guardians in order to include her/his extracted teeth inthe experiments.
Page 11/17
Consent for publication:
Not applicable
Availability of data and materials:
All data generated or analyzed during this study are included in this published article.
Competing Interests:
All authors declare that they have no competing interests.
Funding:
The work was supported by the Department of Orthodontics, Dentofacial Orthopedics and Pedodontics,Charité - Universitätsmedizin Berlin, Germany. The funding body was not involved in study design, datacollection, analysis and writing of the study.
Authors’ contributions:
The study was conceived by KE, FS, SP, NW, NK, GA and SP, FS, KE, PG JB, MK planned the analysis. NW andKE collected the data. FS, PG JB und KE performed the analysis. NW, KE, FS, NK and PG JB wrote themanuscript. All authors read and approved the manuscript.
Acknowledgments:
The authors would like to thank and acknowledge the contribution of Annette Steinke, Carola Schweynochand Rainer Toll, Department of Operative and Preventive Dentistry, for their valuable technical support duringsample preparation and microradiography.
References1. Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, Alipour V, Amini S, Arabloo J, Are� Z, Arora A,
Ayanore MA, Bärnighausen TW, Bijani A, Cho DY, Chu DT, Crowe CS, Demoz GT, Demsie DG, DibajiForooshani ZS, Du M, El Tantawi M, Fischer F, Folayan MO, Futran ND, Geramo YCD, Haj-Mirzaian A,Hariyani N, Hasanzadeh A, Hassanipour S, Hay SI, Hole MK, Hostiuc S, Ilic MD, James SL, Kalhor R,Kemmer L, Keramati M, Khader YS, Kisa S, Kisa A, Koyanagi A, Lalloo R, Le Nguyen Q, London SD,Manohar ND, Massenburg BB, Mathur MR, Meles HG, Mestrovic T, Mohammadian-Hafshejani A,Mohammadpourhodki R, Mokdad AH, Morrison SD, Nazari J, Nguyen TH, Nguyen CT, Nixon MR, OlagunjuTO, Pakshir K, Pathak M, Rabiee N, Ra�ei A, Ramezanzadeh K, Rios-Blancas MJ, Roro EM, Sabour S,Samy AM, Sawhney M, Schwendicke F, Shaahmadi F, Shaikh MA, Stein C, Tovani-Palone MR, Tran BX,Unnikrishnan B, Vu GT, Vukovic A, Warouw TSS, Zaidi Z, Zhang ZJ, Kassebaum NJ. Global, Regional, andNational Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis forthe Global Burden of Disease 2017 Study. J Dent Res. 2020;99:362-373.doi:10.1177/0022034520908533
Page 12/17
2. Schwendicke F, Gostemeyer G, Blunck U, Paris S, Hsu LY, Tu YK. Directly Placed Restorative Materials:Review and Network Meta-analysis. J Dent Res. 2016;doi:10.1177/0022034516631285
3. Pitts NB, Chestnutt IG, Evans D, White D, Chadwick B, Steele JG. The dentinal caries experience ofchildren in the United Kingdom, 2003. Br Dent J. 2006;200:313-320. doi:10.1038/sj.bdj.4813377
4. Pine CM, Harris RV, Burnside G, Merrett MC (2006) An investigation of the relationship between untreateddecayed teeth and dental sepsis in 5-year-old children. Br Dent J. 2006;200:45-47; discussion 29.doi:10.1038/sj.bdj.4813124
5. Walsh T, Worthington HV, Glenny AM, Appelbe P, Marinho VC, Shi X (2010) Fluoride toothpastes ofdifferent concentrations for preventing dental caries in children and adolescents. Cochrane DatabaseSyst Rev (1):Cd007868. doi:10.1002/14651858.CD007868.pub2
�. Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries inchildren and adolescents. Cochrane Database Syst Rev. 2013;doi:10.1002/14651858.CD002279.pub2
7. Schwendicke F, Splieth CH, Thomson W, Reda S, Stolpe M, Foster Page LA (2017) Cost-effectiveness ofcaries-preventive �uoride varnish applications in clinic settings among patients of low, moderate, andhigh risk Community Dentistry Oral Epidemiology. 2017;doi: 10.1111/cdoe.12320
�. Marinho VC, Chong LY, Worthington HV, Walsh T. Fluoride mouthrinses for preventing dental caries inchildren and adolescents. Cochrane Database Syst Rev. 2016;doi:10.1002/14651858.CD002284.pub2
9. Urquhart O, Tampi MP, Pilcher L, Slayton RL, Araujo MWB, Fontana M, Guzman-Armstrong S, NascimentoMM, Novy BB, Tinanoff N, Weyant RJ, Wolff MS, Young DA, Zero DT, Brignardello-Petersen R, Ban�eld L,Parikh A, Joshi G, Carrasco-Labra A. Nonrestorative Treatments for Caries: Systematic Review andNetwork Meta-analysis. J Dent Res. 2019;98:14-26. doi:10.1177/0022034518800014
10. Aggeli A, Bell M, Boden N, Keen JN, Knowles PF, McLeish TC, Pitkeathly M, Radford SE. Responsive gelsformed by the spontaneous self-assembly of peptides into polymeric beta-sheet tapes. Nature.1999;386:259-262. doi:10.1038/386259a0
11. Aggeli A, Fytas G, Vlassopoulos D, McLeish TC, Mawer PJ, Boden N. Structure and dynamics of self-assembling beta-sheet peptide tapes by dynamic light scattering. Biomacromolecules. 2001;2:378-388.doi:10.1021/bm000080z
12. Kind L, Stevanovic S, Wuttig S, Wimberger S, Hofer J, Muller B, Pieles U. Biomimetic Remineralization ofCarious Lesions by Self-Assembling Peptide. J Dent Res. 2017;96:790-797.doi:10.1177/0022034517698419
13. Kirkham J, Firth A, Vernals D, Boden N, Robinson C, Shore RC, Brookes SJ, Aggeli A (2007) Self-assembling peptide scaffolds promote enamel remineralization. J Dent Res. 2007;86:426-430.doi:10.1177/154405910708600507
14. Deyhle H, Dziadowiec I, Kind L, Thalmann P, Schulz G, Muller B. Mineralization of Early Stage CariousLesions In Vitro-A Quantitative Approach. Dent J. (Basel). 2015;3:111-122. doi:10.3390/dj3040111
15. Alkilzy M, Tarabaih A, Santamaria RM, Splieth CH (2018) Self-assembling Peptide P11-4 and Fluoride forRegenerating Enamel. J Dent Res. 2018;97:148-154. doi:10.1177/0022034517730531
1�. Schwendicke F, Splieth C, Breschi L, Banerjee A, Fontana M, Paris S, Burrow MF, Crombie F, Page LF,Gaton-Hernandez P, Giacaman R, Gugnani N, Hickel R, Jordan RA, Leal S, Lo E, Tassery H, Thomson WM,
Page 13/17
Manton DJ. When to intervene in the caries process? An expert Delphi consensus statement. Clin OralInvestig. 2019;doi:10.1007/s00784-019-03058-w
17. Brunton PA, Davies RPW, Burke JL, Smith A, Aggeli A, Brookes SJ, Kirkham J. Treatment of early carieslesions using biomimetic self-assembling peptides – a clinical safety trial. Br Dent J. 2013;215:E6-E6.doi:10.1038/sj.bdj.2013.741
1�. Paris S, Meyer-Lueckel H, Kielbassa AM (2007) Resin In�ltration of Natural Caries Lesions. J Dent Res.2007;86:662-666. doi:10.1177/154405910708600715
19. Krois J, Gostemeyer G, Reda S, Schwendicke F. Sealing or in�ltrating proximal carious lesions. J Dent.2018;74:15-22. doi:10.1016/j.jdent.2018.04.026
20. Krithikadatta J, Gopikrishna V, Datta M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): Aconcept note on the need for standardized guidelines for improving quality and transparency in reportingin-vitro studies in experimental dental research. J Conserv Dent. 2014;17:301-304. doi:10.4103/0972-0707.136338
21. Sindhura V, Uloopi KS, Vinay C, Chandrasekhar R (2018) Evaluation of enamel remineralizing potential ofself-assembling peptide P(11)-4 on arti�cially induced enamel lesions in vitro. J Indian Soc Pedod PrevDent. 2018;36:352-356. doi:10.4103/jisppd.Jisppd_255_18
22. Wierichs RJ, Kogel J, Lausch J, Esteves-Oliveira M, Meyer-Lueckel H (2017) Effects of Self-AssemblingPeptide P11-4, Fluorides, and Caries In�ltration on Arti�cial Enamel Caries Lesions in vitro. Caries Res.2017;51:451-459. doi:10.1159/000477215
23. Marquezan M, Corrêa FN, Sanabe ME, Rodrigues Filho LE, Hebling J, Guedes-Pinto AC, Mendes FM.Arti�cial methods of dentine caries induction: A hardness and morphological comparative study. ArchOral Biol. 2009;54:1111-1117. doi:10.1016/j.archoralbio.2009.09.007
24. Oh HJ, Kim CH, Jeon JG (2020) Public Sense of Water Fluoridation as Re�ected on Twitter 2009-2017. JDent Res. 2020;99:11-17. doi:10.1177/0022034519885610
25. Jablonski-Momeni A, Korbmacher-Steiner H, Heinzel-Gutenbrunner M, Jablonski B, Jaquet W, BottenbergP. Randomised in situ clinical trial investigating self-assembling peptide matrix P11-4 in the prevention ofarti�cial caries lesions. Scienti�c Reports. 2019;9:269. doi:10.1038/s41598-018-36536-4
2�. Ceci M, Mirando M, Beltrami R, Chiesa M, Colombo M, Poggio C. Effect of self-assembling peptide P11 -4on enamel erosion: AFM and SEM studies. Scanning. 2016;38:344-351. doi:10.1002/sca.21276
27. Soares R, De Ataide IN, Fernandes M, Lambor R. Assessment of Enamel Remineralisation AfterTreatment with Four Different Remineralising Agents: A Scanning Electron Microscopy (SEM) Study. JClin Diagn Res. 2017;11:Zc136-zc141. doi:10.7860/jcdr/2017/23594.9758
2�. Gostemeyer G, Schulze F, Paris S, Schwendicke F. Arrest of Root Carious Lesions via Sodium Fluoride,Chlorhexidine and Silver Diamine Fluoride In Vitro. Materials (Basel). 2017;doi:10.3390/ma11010009
29. Paris S, Hopfenmuller W, Meyer-Lueckel H. Resin In�ltration of Caries Lesions. J Dent Res. 2010;89:823-826. doi:10.1177/0022034510369289
30. Ekstrand KR, Bakhshandeh A, Martignon S. Treatment of Proximal Super�cial Caries Lesions on PrimaryMolar Teeth with Resin In�ltration and Fluoride Varnish versus Fluoride Varnish Only: E�cacy after 1Year. Caries Research. 2010;44 (1):41-46
Page 14/17
Figures
Figure 1
Study �ow. Sound enamel was ground and polished and was sectioned to enamel-dentin samples. Parts ofthe sound polished enamel were protected against demineralization using nail varnish to serve as soundcontrols. The remaining exposed enamel was either submitted to preventive strategy application (left side) orpre-demineralized to induce arti�cial caries lesions (right side), to be arrested using arresting strategies. Thetreated surfaces were exposed to pH cycling for 14 days. Samples of 100 ±10 µm thickness were prepared fortransverse microradiography and microradiographically analyzed (left side: the lesion induced by pH cycling,sound enamel and dentin beneath it; right side: I sound enamel and dentin, II pre-demineralized enamel,sound enamel and dentin beneath it, III the lesion after further demineralization using pH cycling and soundenamel and dentin beneath it).
Page 15/17
Figure 2
Caries preventive effects on primary tooth enamel in vitro. (a) Mineral loss ( Z; vol%×µm) or enamel lesionsafter 14 days of pH cycling. Different preventive strategies were compared: SAPP P11-4 (self-assemblingpeptide for preventivtion); FV (�uoride varnish); CPP-ACP/CPP-ACPF (casein-phosphopeptide amorphous-calcium-phosphate without/with �uoride); FMW (�uoride mouthwash); nHA (nanohydroxyapatite); NC(negative control). Signi�cant differences (p<0.05) are indicated by different letters. Box and line: Interquartilerange and median, whiskers: minimum/maximum, circles: outliers. n sample size. (b) Exemplarymicroradiographs in the different groups. Radiolucent enamel areas indicate caries lesions.
Page 16/17
Figure 3
Inhibition of lesion progression on primary tooth enamel in vitro. (a) Mineral loss differences ( Z; vol%×µm)of predemineralized lesions after 14 days pH cycling. Different caries lesion progression inhibiting strategieswere compared: SAPR (self-assembling peptide for repair); FV (�uoride varnish); CPP-APF (casein-phosphopeptide amorphous-calcium-phosphate �uoride); RI (resin in�ltration); NC (negative control).Signi�cant differences (p<0.05) are indicated by different letters. Box and line: Interquartile range and

Page 17/17
median, whiskers: minimum/maximum, circles: outliers. n sample size. (b) Exemplary microradiographs inthe different groups. Radiolucent enamel areas indicate caries lesions.
Related Documents








![Enamel and Dentin Carious Lesions...classified into a superficial lesion [dental plaque & acquired pellicle, in close association with the surface layer (2 - 3 m)], deep lesions (between](https://static.cupdf.com/doc/110x72/5e68547868b2a32bb7246bcc/enamel-and-dentin-carious-lesions-classified-into-a-superficial-lesion-dental.jpg)


