PREVALENCE OF OPPORTUNISTIC INFECTIONS AMONG PATIENTS ATTENDING ART CLINIC AT RUHIIRA HEALTH CENTRE THREE, ISINGIRO DISTRICT BY MAWANDA BASHIR DCM/0129/143/DU A DISSERTATION SUB-MITTED TO THE SCHOOL OF ALLIED HEALTH SCIENCES IN PARTIAL FULLFILLMENT OF THE REQUIREMENTS FOR THE AWARD OF DIPLOMA IN CLINICAL MEDICINE AND COMMUNITY HEALTH OF KAMPALA INTERNATIONAL UNIVERSITY (WESTERN CAMPUS) JULY, 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PREVALENCE OF OPPORTUNISTIC INFECTIONS AMONG PATIENTS
ATTENDING ART CLINIC AT RUHIIRA HEALTH CENTRE THREE,
ISINGIRO DISTRICT
BY
MAWANDA BASHIR
DCM/0129/143/DU
A DISSERTATION SUB-MITTED TO THE SCHOOL OF ALLIED
HEALTH SCIENCES IN PARTIAL FULLFILLMENT OF THE
REQUIREMENTS FOR THE AWARD OF DIPLOMA IN CLINICAL
MEDICINE AND COMMUNITY HEALTH OF KAMPALA
INTERNATIONAL UNIVERSITY
(WESTERN CAMPUS)
JULY, 2017
i
DECLARATION
I Mawanda Bashir declare that this research report write up is my own and has never been submitted
to any institution for any academic award. Therefore the work presented here is in its original form.
Where the work of other people has been quoted, references have been made.
………………………………… …………………………………
Signature Date
ii
APPROVAL
This is to certify that this research proposal entitled “Prevalence and associated risk factors for
opportunistic infections among patients attending ART Clinic at Ruhiira health Centre 3,
Isingiro district” was prepared by Mawanda Bashir under my close supervision.
Dr. ODWEE AMBROSE
Department of Surgery, KIU-TH
……………………………. ……………… ………………
Signature Date

iii
DEDICATION
I dedicate this piece of work to the Almighty Allah, the sustainer of all mankind. Secondly to my
parents Mrs. Nakku Aisha and Mr. Mawanda Yusuf and most importantly to my big brother Mr.
Sahaki Kimera and lastly to all my family members and relatives, Mr. Siraje Masagazi and wife
Halima Masagazi and my Aunt, Sonny Zawedde.

iv
ACKNOWLEDGEMENT
This research exercise would not have been possible without the support of the various individuals
whose dedication and commitment influenced the success of the exercise. These include;
First and foremost the Almighty Allah, who has given me the gift of life and also made me the person
that I am today.
Secondly to my lovely parents, my beautiful mum Mrs. Nakku Aisha, my dad Mr. Mawanda Yusuf
and my elder brother Sahaki Kimera for all their care and support, both physically and financially.
Thirdly, my supervisor DR. Ambrose Odwee and Mr. Dickson who guided me throughout the entire
research process, as well as the In-Charge Ruhiira HC III Mr. Gordon Muhangi who assisted me in
the data collection process.
Not forgetting all classmates and good friends especially my close friends Kagugube Edward, Ategeka
Shaban, Namyalo Jackie, Walungama Faizal, SSengendo Peter, Luyiga Raymond K, H.E Lutaaya
Andrew Musisi, Lubanga George, Mungoma Derrick and all the rest for all their support and
encouragement throughout the entire course.
Lastly my lovely sisters Namiiro Sophie and Namuddu Asha for their endless affection.
May the Almighty Allah reward you all abundantly.

v
LIST OF ABBREVIATIONS
AIDS
AIS
ART
AUD
CDC
HAART
HC III
HIV
HR
KIU-WC
KSHV
NAIDS
MAC
MDGs
OIs
PLWHA
PPE
SDG
UNAIDS
WHO
Acquired Immune Deficiency Syndrome
AIDS Indicator Survey
Anti-Retro Viral Therapy
Alcohol Use Disorders
Centre for Disease Control
Highly Active Anti-Retro Viral Therapy
Health Centre Three
Human Immunodeficiency Virus
Hazard Ratio
Kampala International University- Western campus
Kaposi’s Sarcoma-associated herpes virus
Nutritional Acquired Immune Deficiency Syndrome
Mycobacterium Avium Complex
Millennium Development Goals
Opportunistic Infections
People Living With HIV/AIDS
Pruritic Parpular Eruptions
Sustainable Development Goals
The Joint United Nations Programme on HIV and AIDS
World Health Organization

vi
TABLE OF CONTENTS
DECLARATION ................................................................................................................................................. i
APPROVAL........................................................................................................................................................ii
DEDICATION .................................................................................................................................................. iii
ACKNOWLEDGEMENT ................................................................................................................................ iv
LIST OF ABBREVIATIONS ............................................................................................................................ v
TABLE OF CONTENTS .................................................................................................................................. vi
LIST OF TABLES............................................................................................................................................. ix
DEFINITION OF TERMS ................................................................................................................................. x
ABSTRACT ....................................................................................................................................................... xi
CHAPTER ONE ................................................................................................................................................. 1
1.0 Introduction ....................................................................................................................................................... 1
1.1 Background ....................................................................................................................................................... 1
1.2 Problem statement ............................................................................................................................................ 3
1.3 Justification of the study .................................................................................................................................. 4
1.4 General objective .............................................................................................................................................. 4
1.5 Specific objectives ............................................................................................................................................ 4
1.6 Research questions ........................................................................................................................................... 5
1.7 Conceptual frame work .................................................................................................................................... 6
1.8 SCOPE OF THE STUDY. ............................................................................................................................... 7
CHAPTER TWO ................................................................................................................................................ 8
2.0 Introduction ....................................................................................................................................................... 8
2.1 Prevalence of opportunistic infections among patients with HIV in Uganda. .......................................... 8
2.1.1 Status of the HIV epidemic in Uganda ........................................................................................................ 8
2.1.1.1 HIV prevalence in Uganda ........................................................................................................................ 8
2.1.1.2 HIV burden in Uganda ............................................................................................................................... 8
2.1.1.3 Prevalence of opportunistic infections among patients on ART in Uganda ........................................... 9
2.2 RISK FACTORS FOR OPPORTUNISTIC INFECTIONS AMONG PATIENTS WITH HIV. ............. 10
2.2.1 WHO staging and CD4 count ..................................................................................................................... 10
2.2.2 Age ............................................................................................................................................................... 10
2.2.3 Malnutrition ................................................................................................................................................. 10
2.3 HIGH RISK BEHAVIORS FOR OPPORTUNISTIC INFECTIONS AMONG PATIENTS WITH HIV.
................................................................................................................................................................................ 11
2.3.1 Sex workers.................................................................................................................................................. 11

vii
2.3.2 Alcohol consumption .................................................................................................................................. 11
2.3.3 Tobacco smoking......................................................................................................................................... 12
2.3.4 Unprotected sex. .......................................................................................................................................... 12
CHAPTER THREE .......................................................................................................................................... 14
3.0 General Introduction....................................................................................................................................... 14
3.1 Study Design ................................................................................................................................................... 14
3.2 Study area ........................................................................................................................................................ 14
3.3 Study population ............................................................................................................................................. 14
3.3.1 Inclusion criteria .......................................................................................................................................... 15
3.3.2 Exclusion criteria ......................................................................................................................................... 15
3.4 Sample size determination ............................................................................................................................. 15
3.5 Sampling procedure ........................................................................................................................................ 15
3.6 Study variables ................................................................................................................................................ 15
3.6.1 Dependent variable ...................................................................................................................................... 15
3.6.2 Independent variable ................................................................................................................................... 16
3.7 Data collection and management ................................................................................................................... 16
3.8 Data analysis ............................................................................................................................................... 16
3.9 Ethical considerations ................................................................................................................................ 16
CHAPTER FOUR ............................................................................................................................................ 17
4.0 Introduction ..................................................................................................................................................... 17
4.1 RESPONDENTS’ DEMOGRAPHIC CHARACTERISTICS. ................................................................... 17
4.2 PREVALENCE OF OPPORTUNISTIC INFECTIONS. ............................................................................ 18
4.2 Distribution of OIs with socio-demographic characteristics of the Participants attending ART clinic at
Ruhiira HC III, Isingiro District........................................................................................................................... 18
4.3 CLINICAL VARIABLES.............................................................................................................................. 19
4.3.1 Distribution of OIs with Clinical variables of the participants ................................................................. 19
4.4 HIGH RISK BEHAVIOUR ........................................................................................................................... 20
4.4.1 Distribution of OIs with different high risk behaviors exhibited by the study participants. .................. 20
4.4.2 Distribution of specific OIs with different high risk behaviors exhibited by the study participants. .... 21
CHAPTER FIVE .............................................................................................................................................. 22
5.1 INTRODUCTION .......................................................................................................................................... 22
5.2 PREVALENCE OF OPPORTUNISTIC INFECTIONS AMONG PATIENTS ATTENDING ART
CLINIC AT RUHIIRA HEALTH CENTER III, ISINGIRO DISTRICT. ....................................................... 22

viii
5.2.1 Frequency of opportunistic infections among study participants attending ART clinic at Ruhiira HC III,
Isingiro District. .................................................................................................................................................... 22
5.3 ASSOCIATED RISK FACTORS FOR THE DEVELOPMENT OF OPPORTUNISTIC INFECTIONS
AMONG HIV PATIENTS ATTENDING ART AT RUHIIRA HEALTH CENTRE III. .............................. 23
5.3.1 Selected Socio-Demographic characteristics of study participants attending ART clinic at Ruhiira HC
III, Isingiro District. .............................................................................................................................................. 23
5.3.2 Distribution of OIs with selected clinical variables of participants attending ART clinic at Ruhiira HC
III, Isingiro District. .............................................................................................................................................. 24
5.4 ASSOCIATION OF HIGH RISK BEHAVIOR WITH HIV & OI POSITIVE STATUS ........................ 25
5.4.1 Distribution of OIs with different high risk behaviors exhibited by the study participants. .................. 25
CONCLUSION ..................................................................................................................................................... 25
STRENGTHS AND WEAKNESSES ................................................................................................................. 26
RECOMMENDATIONS ..................................................................................................................................... 26
References ......................................................................................................................................................... 27
Appendix 1: Consent Form .............................................................................................................................. 30
Appendix 2: Questionnaire. Instructions; Tick the right option and fill in where necessary. ..................... 31
Appendix 3: DATA COLLECTION SHEET ..................................................................................................... 34
Appendix 5: Work Plan .................................................................................................................................... 35
Appendix 6: MAPS .......................................................................................................................................... 36
Map of Uganda showing Isingiro District at position # 26 ................................................................................ 36
MAP OF ISINGIRO SHOWING SUB-COUNTIES ..................................................................................... 37
LETTER OF PERMISSION ............................................................................................................................ 38
ix
LIST OF TABLES
Table 1: Selected Socio-Demographic characteristics of study participants attending ART clinic at
Ruhiira HC III, Isingiro District. .............................................................................................................. 17
Table 2: Frequency of opportunistic infections among study participants attending ART clinic at
Ruhiira HC III, Isingiro District. .............................................................................................................. 18
Table 3: shows the relationship between the socio-demographic characteristics and OIs among the
study participants attending ART clinic at Ruhiira HC III, Isingiro District. ....................................... 19
Table 4: Distribution of OIs with selected clinical variables of participants attending ART clinic at
Ruhiira HC III, Isingiro District. .............................................................................................................. 20
Table 5: The table below shows how the selected OIs were distributed among the four high risk
behaviors. ................................................................................................................................................... 21

x
DEFINITION OF TERMS
ART: Antiretroviral therapy (ART) is the combination of several medicines used to slow the rate at
which HIV makes copies of itself (multiplies) in the body.
HAART: Stands for highly active antiretroviral therapy. This refers to treatment with a very potent drug
to suppress the growth of HIV, the retrovirus responsible for AIDS.
Immune compromised: A state in which the body’s ability to fight infections or infectious disease and
cancer is reduced or entirely absent.
Morbidity: The condition of being diseased.
Mortality: The state or condition of being subject to death.
Opportunistic infection: Are infections that occur more frequently and are more severe in individuals
with weakened immune systems, including people with HIV.
Pathogen: A bacterium, virus, or other microorganism that can cause disease.
Super infection: Infection occurring after or on top of an earlier infection.

xi
ABSTRACT
INTRODUCTION: The introduction of antiretroviral therapy (ART) has led to decline in HIV and
HIV-related opportunistic infections (OIs). Knowledge of the most common OIs in Ruhiira will help
in implementing the preventive measures against those particular pathogens.
AIM: This study determined the prevalence of OIs among patients attending ART clinic at Ruhiira
HC III, Isingiro District.
METHOD: A retrospective cross-sectional study design was used.
RESULTS: According to the study, a total of 105 participants were involved and out of these 62 had
OIs, with majority of cases being oral thrush (24%), persistent diarrhea (18%), HSV infection (16%),
recurrent bacterial pneumonia (15%), TB (11%), HZ (10%) and the least number of cases (6%) being
for PPE. These were more common among females (34%) than males (25%) also among those aged
between 28-38 years (32%), single as well as unemployed individuals (49%) and (85%) respectively.
OIs were commonest among those with WHO HIV clinical stage 3 (74%) and 4 (100%), CD4 cell
count of less than 250 cell/µl (82%), malnutrition assessed by weight for age of less than 50kg (73%),
as well as low level of ART adherence <95% (100%), having multiple sexual partners (69%), alcohol
intake (67%), engaging in unprotected sexual intercourse (50%), as well as cigarette smoking (40%).
CONCLUSION: In this study, the overall prevalence of OIs was high 59%, compared to studies from
other researchers and the most common OIs identified were Oral thrush, persistent diarrhea, HSV
infection, recurrent bacterial pneumonia, TB, HZ, and PPE. And the associated risk factors for
developing OIs were identified as advanced WHO HIV clinical stage, malnutrition, and poor ART
adherence, while high risk behaviors namely; having multiple sexual partners, alcohol intake,
engaging in unprotected sexual intercourse, as well as cigarette smoking were also confirmed to have
a positive impact on the occurrence of OIs among patients on ART at Ruhiira HC III, Isingiro District.
RECOMMENDATIONS: In view of the above conclusions, the researcher recommended the
following; Health education talks be given to the clients regarding staying away from the high risk
behaviors as well as adhering to their ART treatment. Also further studies be done in higher health
facility setting like HC IV, district hospitals as well as referrals where there are large number of clients
and equipment to diagnose most OIs, are also available in these settings.
1
CHAPTER ONE
1.0 Introduction
This chapter will include the background, problem statement, study objectives, study
justification and research questions.
1.1 Background
The human immunodeficiency virus (HIV) epidemic remains one of the top global health
challenge of the 21st century. Currently HIV has no effective vaccine or curative therapy.
According to the Joint United Nations Programme on HIV/AIDS (UNAIDS), 36.7 million people
worldwide were estimated to be living with this deadly virus by end of 2015 of which 25.5 million
(69.5%) were in sub-Saharan Africa. Since its outbreak, an estimated 34 million people
worldwide have died with sub-Saharan Africa accounting for approximately 70% of the total
deaths. The report also shows that 17 million people living with HIV (50%) were on HAART by
end of 2015 with subsequent 43% reduction in mortality thus improving survival and quality of
life (UNAIDS, 2016).
Acquired Immunodeficiency Syndrome (AIDS) causes progressive decline in immunological
response in people living with HIV/AIDS (PLWHA) making them susceptible to a variety of
opportunistic infections which are responsible for morbidity and mortality (Goud, T Gangadhara;
Ramesh, 2014). With the changing scenario of AIDS epidemic, a host of opportunistic infections
add to the present endemic state of some already existing infections like tuberculosis (Agarwal,
Powar, Tankhiwale, & Rukadikar, 2015).
Opportunistic infections (OIs) are infections that are more frequent or more severe because of
immune-suppression in HIV-infected persons, and they are the major clinical manifestation of
HIV patients. These take the advantage of the immune suppression and they indirectly affect the
natural history of HIV disease, because HIV viral load increases in patients with acute
opportunistic diseases. Severely immune-compromised HIV patients may develop a variety of
opportunistic infections that have a significant impact on their well-being, quality of life, health
care costs, and their survival. (Moges NA, Kassa GM 2014).
The most common opportunistic diseases in HIV patients are Candida esophagitis, Pneumocystis
carinii pneumonia (PCP), disseminated Mycobacterium avium complex (MAC) infection,
2
cytomegalovirus (CMV), Cryptococcus, Kaposi sarcoma, herpes zoster, and tuberculosis (CDC,
2009). And majority of these OI are associated with an increased hazard of death in HIV patients.
Patients experiencing morbidity from opportunistic diseases may have interruptions in
antiretroviral therapy causing more rapid progression of HIV disease. In addition studies found
that opportunistic infections cause an up regulation in HIV replication and higher viral loads (P.
R, F, M, MJ, & Rivas, 2007)Thus increasing morbidity and mortality among patients with HIV
which considerably affect the health and quality of life of these individuals (Dabla et al, 2015).
Opportunistic infections are caused by bacteria, viruses, fungi, or protozoa and these take
advantage of an opportunity not normally available, such as a host with a weakened immune
system, an altered microbiota (such as a disrupted gut flora), or breached integumentary barriers.
Many of these pathogens do not cause disease in a healthy host that has a normal immune system
as earlier on stated, however, a compromised immune system, a penetrating injury, or a lack of
competition from normal commensals presents an opportunity for the pathogen to infect (CDC,
2015).
OIs that indicate that the HIV has progressed to AIDS irrespective of how many CD4 cells a
person has, however HIV treatment can help restore the person’s immune system. These include;
Aspergillus sp., Candida albicans, Clostridium difficile, Coccidioides immitis, Cryptococcus
neoformans, Cryptosporidium, Cytomegalovirus, Histoplasma capsulatum, Isospora belli,
Progressive multifocal leukoencephalopathy, Kaposi's Sarcoma, Legionella pneumophila,
Microsporidium, Mycobacterium avium complex (MAC) (Nontuberculosis Mycobacterium),
Mycobacterium tuberculosis, Pneumocystis jirovecii, f. hominis, Pseudomonas aeruginosa,
Salmonella spp, Staphylococcus aureus, Streptococcus pneumonia, Streptococcus pyogenes and
Toxoplasma gondii (B-Lajoie et al., 2016).
There’s generally a high prevalence of OIs amongst HIV patients globally. In Eastern Ethiopia,
Out of 358 patients, 172 had diagnosed OIs, yielding an overall prevalence of 48% (172/358).
(Mitiku H, F, & Z, 2015) while in India the prevalence was 50.63% with a significant positive
association with WHO clinical staging and CD4 count as associated risk factors (Bhuvana, Hema,
& Patil, 2015).

3
Other associated clinical risk factors for development of OIs included, first-line current drug
regimen, poor ARV adherence status, current CD4+ <200 cells/μL, and current Hb level <10g/dl
as observed in Addis Ababa (Eyasu, Berhane, & Yohannes, 2015).
Concerning the OIs in India, Tuberculosis was the most common OI with an incidence of 15.4
per 100 person-years, followed by oral candidiasis 11.3, herpes zoster 10.1, and cryptococcal
meningitis 1.7 per 100 person-years. Patients with baseline CD4 counts of <200/mm3 were six
times more likely to develop OIs compared to those with CD4 counts of >350/mm3 (p < 0.001).
(Manisha Ghate, Deshpande, & Tripathy, 2009).
In Uganda, the Mean annual prevalence for any OI in 2004 was 57.6% and in 2013 was 27.5%,
it was observed as well that the most commonly encountered OIs were geohelminths (35%),
diarrhea<1 month (18%) and mycobacterium tuberculosis (11%).The factors associated with any
OI after HAART were male gender, low education(<primary), baseline WHO stages III&IV,
stavudine ART regimen, baseline CD4 count <100cells/μl and low baseline weight <55 kg
(Rubaihayo, Tumwesigye, Konde-Lule, & Wamani, 2016).
1.2 Problem statement
Opportunistic infections (OIs) associated with HIV remain the single main cause of ill-health and
death among HIV/AIDS patients in resource poor settings. OIs lower the quality of life of HIV
infected persons, speeds up the rate of progression to fully blown AIDS, reduces patients’
response to antiretroviral treatment especially when HIV-positive patients are co-infected with
tuberculosis, increases stigma and limits one’s ability to work and are usually associated with
high medical care costs. OIs have therefore greatly contributed to poverty among those infected
and affected by HIV/AIDS and hence an impediment to the attainment of the sustainable
development goal (SDG) three on health in resource poor settings (Colindres et al., 2008).
In low- and middle-income countries (LMICs), the global rollout of ART has led to >15 million
patients on ART, and a decline in HIV-related deaths by 40% since 2004. OIs remain the major
driver of HIV-associated morbidity and mortality, accounting for the substantially higher
mortality observed in LMICs (B-Lajoie et al., 2016).
Uganda is one of the few sub-Saharan countries in which the magnitude of the HIV epidemic has
been substantially reduced and stabilized in the past decades, due to the use of HAART though

4
recent reports show a slight increase in HIV prevalence among adults from a national average of
6.4% in 2005 to 7.3% in 2011 (Uganda MOH, 2015).
HIV positive patients in resource poor settings like Uganda also suffer because of the high risk of
exposure to potential pathogens which are endemic in these settings and most patients suffer from
nutritional deficiency resulting in poor prognostic outcomes while on HAART and 40% of those
eligible for HAART present with late disease stage for treatment with increased risk of
opportunistic infections and death. The purpose of this study is to assess the prevalence of OIs
and their associated risk factors among HIV positive patients attending ART at Ruhiira health
center III, Isingiro district.
1.3 Justification of the study
The research will be used to establish the existence of opportunistic infections among patients
attending ART at Ruhiira HC III, Isingiro District and how these infections affect the socio-
economic status of these individuals. In addition, the research will also contribute to the efforts
being made by Isingiro district and the country as a whole to reduce on the cases of morbidity and
mortality rates in HIV patients due to opportunistic infections.
Furthermore, the information obtained from this study will also be used to provide sensitization
on how the way of life of these individuals predisposes them to various opportunistic infections
and so help them adopt behaviors that can help them reduce the risks of acquiring these infections
as well as create self-awareness among these individuals regarding the risks and complications
associated with the different OIs and finally to help stake holders plan effective intervention
formulate policies and developmental programs to help address the problems identified.
1.4 General objective
To assess the prevalence and associated risk factors for opportunistic infections among patients
attending ART clinic at Ruhiira Health Centre III, Isingiro District.
1.5 Specific objectives
To assess the prevalence of opportunistic infections among patients attending ART at Ruhiira
health center III, Isingiro District.

5
To determine the associated factors for the development of opportunistic infections among HIV
patients attending ART at Ruhiira Health Centre III.
To find out if there is existence of any association of high risk behavior with OI positive status.
1.6 Research questions
The research aims at answering the following questions;
What is the prevalence of opportunistic infections among patients attending ART at Ruhiira health
center III, Isingiro District?
What are the associated factors for development of opportunistic infections among HIV patients
attending ART at Ruhiira Health Center III?
Is there any association of high risk behavior with HIV & OI positive status?

6
1.7 Conceptual frame work
Behavioral factors
Alcoholism, number of
sexual partners, type of
sexual partners (spouse/ide
lover), Smoking, use/ non-
use of condoms,
abstinence from sexual
intercourse
Intervening factors.
Status of Immune system,
Circumcision status,
Drug adherence, practicing
safe sex, OI treatment
availability, availability and
uptake of condoms, ART
adherence counselling, OI
diagnosis and treatment.
SOCIO-DEMOGRAPHICS
Age, Sex,
Marital status,
Occupation, Level of
education, employment
status
Individual health factors
WHO clinical Staging,
Baseline CD4 count,
Baseline weight, Baseline
Hemoglobin, viral load
Prevalence of
Opportunistic
infections.

7
1.8 SCOPE OF THE STUDY.
The study was focused on clients who attend ART clinic at Ruhiira Health Centre III, Isingiro
District, and was aimed at assessing the prevalence and associated risk factors for OIs among
these individuals. The independent variables in this study included individual health factors,
behavioral factors, and socio-demographic factors as well as intervening factors and the
dependent variable of the study was the magnitude of prevalence of OIs. Among the factors that
were looked at in this study include the demographic factors such as sex, age bracket, marital
status and employment status. Other factors which the study focused on included clinical variables
such WHO clinical Staging, Baseline CD4 count, Baseline weight and level of ART adherence.
Behavioral factors such as Alcoholism, MSP, Smoking, Unprotected sex were also examined to
determine their effect on the dependent variable.

8
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
In this chapter, the researcher tried to review relevant literature to help in the understanding of
opportunistic infections among patients who tested HIV positive. The researcher acknowledged
the fact that there was some literature on opportunistic infections and their associated risk factors
among patients on ART in Uganda. The literature will be from different sources these include
articles, journals, text books and webpages.
2.1 Prevalence of opportunistic infections among patients with HIV in Uganda.
2.1.1 Status of the HIV epidemic in Uganda
2.1.1.1 HIV prevalence in Uganda
According to The Uganda HIV and AIDS Country Progress report (2014), the two rounds of
AIDS Indicator Survey show that HIV prevalence in the general population in Uganda increased
from 6.4% in 2004/5 to 7.3% by 2011, this tally with the 2013 HIV estimates which show that
HIV prevalence stabilized around 7.4% in 2012/2013. This stagnation of HIV prevalence could
be partly due to the high coverage of ART program where the number of PLHIV enrolled on ART
increased from about 330,000 in 2011 to about 750,896 in 2014 and the reduction in AIDS related
deaths from 67,000 to 63,000 in 2010 and 2013 respectively. However, there are still marked
variations in the prevalence rate by social dynamics and geographical areas. According to the AIS
(2016) geographically the central region of Uganda was shown to have the highest HIV
prevalence (10.6%), followed by mid-northern (8.3%) and then mid and south western (8–8.2%)
and lowest prevalence in mid-eastern (4.1%) Uganda.
2.1.1.2 HIV burden in Uganda
According to The Uganda HIV and AIDS Country Progress report (2014), Uganda is still
classified as a high burden country with high number of persons living with HIV which has
continued to increase. This is a result of continuing spread of HIV, and increased longevity among
persons living with HIV. The report further states that national projections based on Spectrum
9
estimates indicate an increasing number of people living with HIV; 1.4million in 2011 to 1.6M
in 2013, and to 1,500,000 in 2014 and high number of orphans due to AIDS of about one million.
HIV doesn't kill anybody directly. Instead, it weakens the body's ability to fight disease. Infections
which are rarely seen in those with normal immune systems are deadly to those with HIV. People
with HIV can get many of these infections which are referred to as opportunistic infections.
2.1.1.3 Prevalence of opportunistic infections among patients on ART in Uganda
According to a study made by Rubaihayo et al., (2016), the most common opportunistic infections
among patients with HIV in Uganda include Mycobacterium tuberculosis, oral candida, Herpes
zoster, genital ulcer and Crypotococcal meningitis. These were also considered to be the easiest
to diagnose in comparison to other opportunistic infections (Rubaihayo et al. 2015).
Another recent study in Uganda on patients attending ART stated that the most frequent OIs
before HAART were oral candida (34.6%), diarrhoeal infection (<1 month) (30.6%),
geohelminths (26.5%), Mycobacterium tuberculosis (TB) (17.7%), malaria (15.1%) and bacterial
pneumonia (11.2%) (Rubaihayo et al., 2016). In early HAART (2004–2008), the most frequent
OIs were geohelminths (32.4%), diarrhoeal infection (25.6%), TB (18.2%) and oral candida
(18.1%) (Rubaihayo et al., 2016). In late HAART (2009–2013), the most frequent OIs were
geohelminths (23.5%) and diarrhoeal infection (14.3%) (Rubaihayo et al., 2016).
According to Rubaihayo et al (2015), although the natural history of AIDS tends to be similar in
most patients, the patterns of OIs that largely define the symptomatic and clinical manifestation
of AIDS tend to vary in different regions of the world. Thus, while HIV patients in developed
countries rarely suffer from bacterial and protozoal infections, they are a major cause of morbidity
and mortality in resource-poor countries.
In another study in in North India, in a total of 80 patients, 38 (47.5%) HIV-positive patients
screened were found to have OI. There were 13.6% patients presenting with infections having a
CD4 count below 200 cells/μL. There were 4.0% patients with CD4 counts between 200 and 499
cells/μL and 0.49% patients with CD4 counts above 500 cells/μL. The following OI's were present
on testing. Oral candidiasis (40.8%), Cryptosporidiosis (23.68%), Tuberculosis (5.92%), and
CMV IgM, PCP, Isosporiasis and Cryptococcosis were (2.96%). Oral candidiasis was the most
10
common infection found in these patients followed by opportunistic stool infection,
Cryptosporidiosis (Mala & Aroma, 2015).
2.2 RISK FACTORS FOR OPPORTUNISTIC INFECTIONS AMONG PATIENTS
WITH HIV.
2.2.1 WHO staging and CD4 count
In India the prevalence of opportunistic infection was 50.63% with a significant positive
association with WHO clinical staging and CD4 count as associated risk factors (Bhuvana et al.,
2015). In Addis Ababa, among the patients with OIs, patients with stage III and II were with
higher frequency, 112(25.34%) and 55(12.44%), respectively. Patients with baseline WHO stage
III and stage IV, were 1.698 times odds of having OIs with a statistical significance (P= 0.016),
but the BMI (base line) had no significant association with the current occurrence of OIs. Patients
with poor ARV adherence were 4.04 times (P=0.004) more likely to acquire OIs as compared to
patients with good ARV adherence. Moreover, patients with the following variables had increased
likelihood of OIs: hypertension (COR: 5.457; P=0.010), and Hb level, < 10g/dL (COR: 13.442;
P= 0.014) and patients under first-line ART regimen, 343 (77.5%) (Eyasu et al., 2015).
2.2.2 Age
According to Goud, T Gangadhara Ramesh, (2014), in the present study majority of the HIV
positive patients with opportunistic infections were in the age group of 30-39 years and all the
patients fell below the age of 60 years comparable to results of Garcia Ordonez MA et al (1998).
So it was observed that the frequency of opportunistic infections was highest in the sexually active
age group of the society.
2.2.3 Malnutrition
HIV causes immune impairment leading to malnutrition which leads to further immune
deficiency, and contributes to rapid progression of HIV infection to AIDS. A malnourished person
after acquiring HIV is likely to progress faster to AIDS, because his body is weak to fight infection
whereas a well-nourished person can fight the illness better. It has been proved that good nutrition
increases resistance to infection and disease, improves energy, and thus makes a person stronger
11
and more productive. Nutritional improvement measures must be initiated before a patient reaches
this stage.
Malnutrition is considered to be the most common cause of immunodeficiency worldwide.
Malnutrition, immune system, and infectious diseases are interlocked in a complex negative
cascade, malnutrition elicits dysfunctions in the immune system and promotes increased
vulnerability of the host to infections (Morley, 2007). These immune dysfunctions are referred to
as nutritional-acquired immune deficiency syndrome (NAIDS), every type of immunological
deficiency induced by malnutrition can be included under the NAIDS umbrella (Shalini Duggal,
Chugh, & 2Ashish Kumar Duggal, 2012).
2.3 HIGH RISK BEHAVIORS FOR OPPORTUNISTIC INFECTIONS AMONG
PATIENTS WITH HIV.
2.3.1 Sex workers
According to UNAIDS (2016), evidence shows that HIV prevalence among sex workers is 12
times greater than among the general population. Even in very high prevalence countries, HIV
prevalence among sex workers is much higher than among the general population. An analysis of
16 countries in sub-Saharan Africa in 2012 showed a pooled prevalence of more than 37% among
sex workers. Stigma and discrimination, violence and punitive legal and social environments are
key determinants of this increased HIV vulnerability. Punitive environments have been shown to
limit the availability, access and uptake of HIV prevention, treatment, care and support for sex
workers and their clients.
2.3.2 Alcohol consumption
The prevalence of alcohol use disorders (AUDs) appears to be high among people living with
HIV (PLHIV) compared to the general population (Selnes OA, 2010). AUDs are associated with
premature mortality in PLHIV (Bryant KJ et al.,2010), thought to occur due to alcohol enhancing
the toxicity of antiretroviral treatment (ART), increasing liver damage from concurrent infection
with hepatitis C virus, and increasing the risk of opportunistic infection due to decreased
effectiveness of ART and exacerbation of immune suppression (Braithwaite, 2010).

12
A study made by Matiwos and the colleagues (2013) showed that the overall prevalence of AUDs
was 32.6%, with hazardous use, harmful use and alcohol dependence accounting for 24.7%, 2.8%
and 5.1% of the total, respectively. There was no significant difference in the prevalence of AUDs
in persons receiving antiretroviral treatment compared to those who were antiretroviral therapy
naïve (32.6% vs. 38.6%). AUDs were identified in 26.0% and 44.1% of females and males,
respectively. Male gender, smoking cigarettes and psychological distress were positively
associated independently with AUDs.
2.3.3 Tobacco smoking
As mortality due to AIDS-related causes has decreased with the use of antiretroviral therapy, there
has been a rise in deaths related to non–AIDS-defining illnesses (S. R et al., 2011). Given the
exceedingly high prevalence of cigarette smoking among individuals living with HIV infection,
tobacco has been implicated as a major contributor to this paradigm shift (S. R et al., 2011).
Evidence suggests that smoking-related illnesses, such as cardiovascular disease, respiratory
illnesses, and certain malignancies, contribute substantially to morbidity and mortality among
HIV-infected persons (S. R et al., 2011).
Evidence demonstrates that cigarette smoking adversely affects the immunologic response to
ART. In a longitudinal study of a large HIV-infected cohort, Feldman and coworkers (2006)
found that, compared with nonsmokers, smokers receiving ART had poorer viral responses (HR,
0.79; 95% CI, 0.67–0.93), poorer immunologic response (HR, 0.85; 95% CI, 0.73–0.99), greater
risk of virologic rebound (HR, 1.39; 95% CI, 1.06–1.69), and more frequent immunologic failure
(HR, 1.52; 95% CI, 1.18–1.96).
2.3.4 Unprotected sex.
Alcorn (2009) stated that current guidance for people with HIV from many sources is that
unprotected sex poses a risk of superinfection – infection with a new strain of HIV that over-runs
the existing virus population due to lack of immunity to that virus, Superinfection seems to happen
not only in people who have been recently infected with HIV, but also in those with longstanding
HIV infection.
A recently reported study in Kenyan women estimated an annual incidence of superinfection of
at least 4%, but no evidence of disease progression as a consequence of superinfection. A study

13
in gay men reported an incidence of 5% per year (Alcorn, 2009). Superinfection has been
associated with CD4 cell declines, and a handful of cases of transmitted drug resistance among
people with HIV (Alcorn, 2009). There is much stronger evidence that unprotected sex with other
HIV-infected people is harmful for people with HIV where it involves the risk of exposure to
sexually transmitted infections (Alcorn, 2009).
14
CHAPTER THREE
STUDY METHODOLOGY
3.0 General Introduction
This chapter outlined the major approaches in the study methodology including the methods and
tools that were used to conduct the research, design, data collection methods, tools and research
sample sizes.
3.1 Study Design
The study employed a retrospective and cross-sectional study designs where the retrospective
design was used to assess the prevalence of opportunistic infections while the cross-sectional
design was used to establish the associated risk factors for opportunistic infections, among
patients attending ART at Ruhiira HC III.
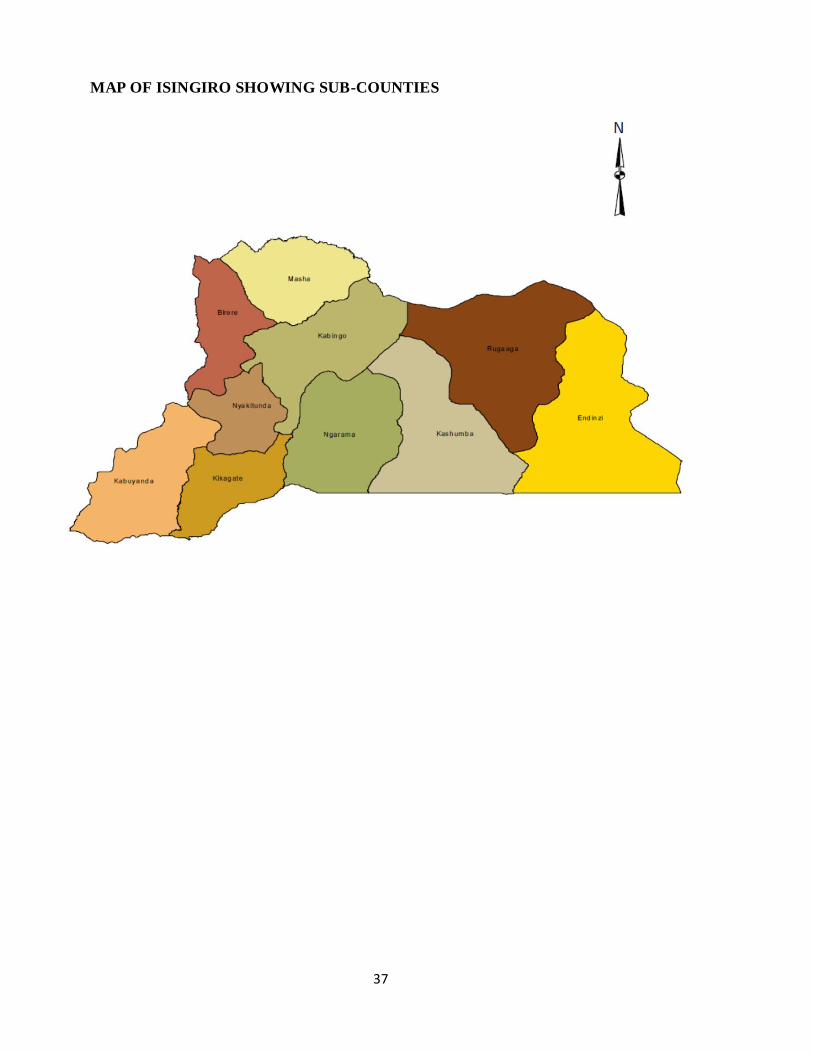
3.2 Study area
The study area was Ruhiira HC III where HIV positive clients attended ART services every
Wednesday of the week throughout the study period. Ruhiira HC III is a government owned and
funded hospital situated in Ruhiira village, Nyakitunda sub-county, Isingiro district, which is one
of the districts that make up the Ankole sub-region in Western Uganda. The 2014 national housing
and population census estimated the population of Isingiro District at 486,360. Majority of the
locals in Ruhiira are farmers and this is their major source of income and majority of the residents
do not attain adequate education in their youthful age since their parents prefer sending them to
gardens than studying so majority of residents are illiterates.
3.3 Study population
The study population was from patients who attend ART clinic at Ruhiira HC III who are
estimated to be about 550 clients.
15
3.3.1 Inclusion criteria
Patients who were confirmed to be HIV positive and were enrolled for ART. Study will also
include both married and single/unmarried individuals with all participants in age bracket
between 18 – 60 years and have stayed in Ruhiira for at least the past three years.
3.3.2 Exclusion criteria
Clients who did not consent to the study, as well as HIV positive patients who were not enrolled
for ART, those patients who were critically ill and unable to speak as well as those that were not
mentally stable.
3.4 Sample size determination
The sample was obtained directly from Krejcie and Morgan Table for Determining Sample Size
for Finite Population (Aulawi, 2017).
The total number of clients who attend ART services at Ruhiira HC III is approximately 550,
therefore using Morgan tables, a total of 226 participants were to be used in the study, however
due to limited time and manpower a total sample size of 105 participants was used.
3.5 Sampling procedure
A systematic randomized sampling technique was used to enroll participants in the study. The
ART book register was used as a sampling frame using an interval of 2 calculated by (N/n) where
N- total population and n – required sample size. The researcher closed the eyes and chose the
start number and then include participants with an interval of 2 until the required total number of
participants was obtained. If the final had incomplete records then the one next to it would be
included instead.
3.6 Study variables
3.6.1 Dependent variable
Prevalence of opportunistic infections.
16
3.6.2 Independent variable
Socio demographics, clinical variables and high risk behavior.
3.7 Data collection and management
Data was collected using a structured questionnaire and data collection sheet. Data collection
sheets were used to establish the prevalence, commonest opportunistic infection among HIV
patients and associated risk factors while the questionnaire was used to assess participants for
high risk behaviors such as alcohol consumption and multiple sexual partners as well as other
predisposing factors to opportunistic infections such as employment status and other socio-
economic factors. Records were reviewed for completeness and errors.
3.8 Data analysis
Data was first analyzed manually using electronic calculators. The data was then presented in
lists, tables, bar charts and pie charts. Direct quotes from the respondents were also used.
3.9 Ethical considerations
Permission to conduct research was sought from the office of the administrator, school of Allied
Health Sciences, KIU-WC, confidentiality was ensured whereby the names of the respondents
were not included and information given by the respondent was not disclosed to anyone, informed
consent forms will be availed and respondents will not be forced to participate and finally the
benefits of the research were also explained to the respondents
17
CHAPTER FOUR
FINDINGS OF THE STUDY
4.0 Introduction
This chapter contains results for data collected which were analyzed manually and interpreted in
form of tables, pie charts, bar graphs, histograms, line graphs and simple statements. The sample
size of the study was 105 participants attending ART Clinic at Ruhiira HC III, Isingiro District.
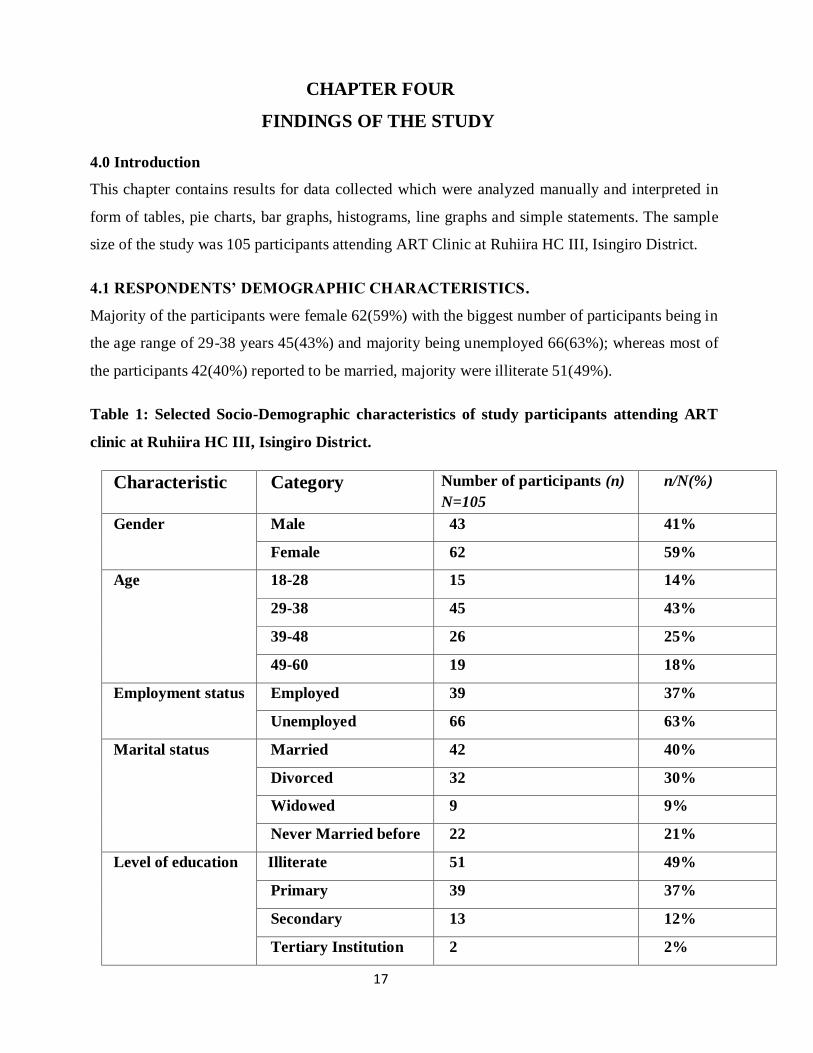
4.1 RESPONDENTS’ DEMOGRAPHIC CHARACTERISTICS.
Majority of the participants were female 62(59%) with the biggest number of participants being in
the age range of 29-38 years 45(43%) and majority being unemployed 66(63%); whereas most of
the participants 42(40%) reported to be married, majority were illiterate 51(49%).
Table 1: Selected Socio-Demographic characteristics of study participants attending ART
clinic at Ruhiira HC III, Isingiro District.
Characteristic Category Number of participants (n)
N=105
n/N(%)
Gender Male 43 41%
Female 62 59%
Age
18-28 15 14%
29-38 45 43%
39-48 26 25%
49-60 19 18%
Employment status Employed 39 37%
Unemployed 66 63%
Marital status Married 42 40%
Divorced 32 30%
Widowed 9 9%
Never Married before 22 21%
Level of education Illiterate 51 49%
Primary 39 37%
Secondary 13 12%
Tertiary Institution 2 2%

18
4.2 PREVALENCE OF OPPORTUNISTIC INFECTIONS.
The most number of cases of OIs recorded were of oral thrush 15(24%) followed by persistent
diarrhea 11(18%) then HSV infections with 10(16%) of cases and recurrent bacterial pneumonia
with 9(15%) of the cases, tuberculosis with 7(11%) of cases, Herpes Zoster cases being 6(10%) and
the least OIs recorded were PPE infections 4(6%).
Table 2: Frequency of opportunistic infections among study participants attending ART
clinic at Ruhiira HC III, Isingiro District.
Opportunistic infection Frequency
n= 62
(%)
Chronic Diarrhea 11 18
HSV infection 10 16
Tuberculosis 7 11
Oral thrush 15 24
Recurrent bacterial
pneumonia
9 15
Herpes Zoster 6 10
PPE 4 6
4.2 Distribution of OIs with socio-demographic characteristics of the Participants attending
ART clinic at Ruhiira HC III, Isingiro District.
In this study, majority of OIs were found among females (58%) compared to the males (42%), and
according to age, majority of cases of OIs were found amongst participants between the ages 29-38
years, while regarding employment status (85%) and according to marital status, majority of OIs
were found among the participants who were divorced (27%) and finally, regarding the level of
education, majority of cases of OIs were found among illiterates (35%) as shown in the table below.

19
Table 3: shows the relationship between the socio-demographic characteristics and OIs among
the study participants attending ART clinic at Ruhiira HC III, Isingiro District.
Characteristic Category OIs
(n=62)
YES NO
Gender Male 42% 58%
Female 58% 42%
Age
18-28 11% 89%
29-38 32% 68%
39-48 10% 90%
49-60 6% 94%
Employment status Employed 15% 85%
Unemployed 85% 15%
Marital status Married 10% 90%
Divorced 27% 73%
Widowed 2% 98%
Never Married
before
20% 80%
Level of education Illiterate 35% 65%
Primary 21% 79%
Secondary 3% 97%
Tertiary Institution 0% 100%
4.3 CLINICAL VARIABLES
4.3.1 Distribution of OIs with Clinical variables of the participants
All participants in WHO HIV clinical stage 4 (100% of cases) and those with level of drug
adherence of less than 95% (100% of cases) were found to be having OIs, followed by majority
of the participants who were in WHO HIV clinical stage 3 (71%), participants with a CD4 count
of less than 250 cells/µL (82%), and also participants with weight of less than 50kg (73% of
cases) as shown in the table below.
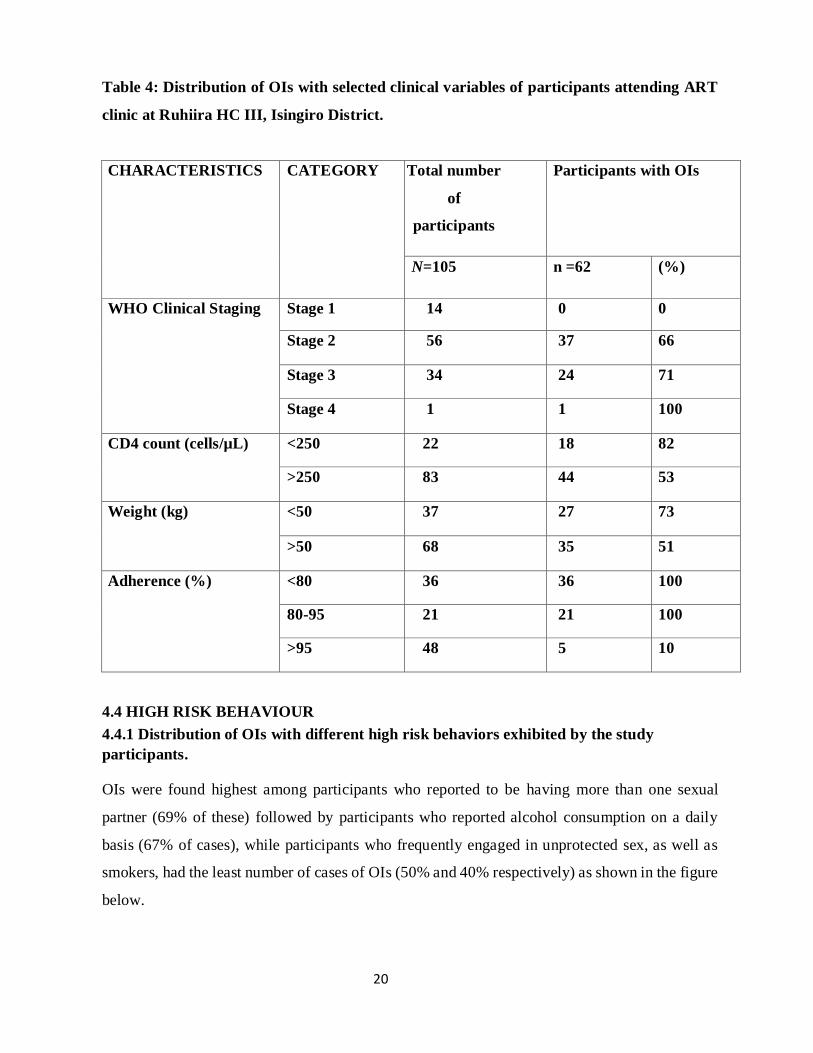
20
Table 4: Distribution of OIs with selected clinical variables of participants attending ART
clinic at Ruhiira HC III, Isingiro District.
CHARACTERISTICS CATEGORY Total number
of
participants
Participants with OIs
N=105 n =62 (%)
WHO Clinical Staging Stage 1 14 0 0
Stage 2 56 37 66
Stage 3 34 24 71
Stage 4 1 1 100
CD4 count (cells/µL) <250 22 18 82
>250 83 44 53
Weight (kg) <50 37 27 73
>50 68 35 51
Adherence (%) <80 36 36 100
80-95 21 21 100
>95 48 5 10
4.4 HIGH RISK BEHAVIOUR
4.4.1 Distribution of OIs with different high risk behaviors exhibited by the study
participants.
OIs were found highest among participants who reported to be having more than one sexual
partner (69% of these) followed by participants who reported alcohol consumption on a daily
basis (67% of cases), while participants who frequently engaged in unprotected sex, as well as
smokers, had the least number of cases of OIs (50% and 40% respectively) as shown in the figure
below.

21
Figure 1: Distribution of OIs with different high risk behaviors exhibited by the study
participants attending ART Clinic at Ruhiira HC III, Isingiro District.
4.4.2 Distribution of specific OIs with different high risk behaviors exhibited by the study
participants.
Of participants that reported MSP, majority (29%) had Oral thrush and HSV infection (25%); of
those that reported frequent unprotected sex, majority (14%) had HSV infection, while majority
of alcohol consumers had TB (33%) and of the smokers, (50%) had oral thrush and 50% TB.
Table 5: The table below shows how the selected OIs were distributed among the four high
risk behaviors.
HIGH RISK BEHAVIOURS
More than 1
sexual partner
Unprotected sex Alcohol
consumption
smoking
Chronic diarrhea 5 2 1 nil
Herpes Zoster 1 1 2 nil
Herpes simplex 6 4 nil nil
Oral thrush 7 2 2 1
Recurrent bacterial
pneumonia
3 3 nil nil
TB 1 nil 3 1
PPE 1 2 nil nil
35
28
12
5
69%
50%
67%
40%
0%
10%
20%
30%
40%
50%
60%
70%
80%
More than 1 sexualpartner
Unprotected sex Alcohol consumers smokers
0
5
10
15
20
25
30
35
40
number of participants in category number of respondents in this category with OIs
OP
PO
RTU
NIT
IC IN
FEC
TIO
N
22
CHAPTER FIVE
DISCUSSIONS, CONCLUSIONS AND RECOMMENDATIONS
5.1 INTRODUCTION
Research study was targeting HIV patients attending ART clinic at Ruhiira HC III, Isingiro
District, from the age of 18- 60 years, irrespective of their sex, tribe, religion, education
background, marital status or even occupation, however age limit of above 18 years because it’s
the age at which one is considered an adult by law in Uganda and can consent on their own, and
not above 60 years because beyond this age one’s immunity is usually lowered and hence higher
chances of contracting various OIs which interferes with the results of the study.
Sample size of the study was 105 study participants and out of these, majority (62) were found to
be having OIs.
5.2 PREVALENCE OF OPPORTUNISTIC INFECTIONS AMONG PATIENTS
ATTENDING ART CLINIC AT RUHIIRA HEALTH CENTER III, ISINGIRO
DISTRICT.
In this study the overall prevalence of OIs among patients on ART at Ruhiira HC III, Isingiro
District was 59%, which is similar to that of Rubaihayo (57%) conducted in Uganda in 2004 but
which is higher compared to studies from other researchers like of Bhuvana et al 2015 in which
the prevalence was only 50%, Other similar studies revealed a prevalence of 47.6% both in
Taiwan and South Africa. This difference and high prevalence may be attributed to the difference
in the study setting Ruhiira being a rural area where locals are still naïve about some facts about
OIs in HIV whereas other studies were conducted in urban or semi-urban settings where
individuals are much more informed; other reasons could be due to difference in the socio
demographic characteristics and sample size difference.
5.2.1 Frequency of opportunistic infections among study participants attending ART clinic
at Ruhiira HC III, Isingiro District.
In this study, most common OIs identified were oral thrush with majority of cases and prevalence
of (24%) followed by chronic diarrhea with a prevalence of (18%), HSV infections (16%),

23
recurrent bacterial pneumonia (15%), Tuberculosis (11%), HZ (10%) and finally the least
prevalent OI being PPE with a prevalence of (6%). These findings are similar to those of
Rubaihayo et al 2015 in Uganda where he identified oral candida (oral thrush) and diarrhea as the
most common OIs in patients with HIV, same applies to a study by Moges et al. in their study
found that oral candidiasis and chronic diarrhea were among the most common OIs encountered,
this may be because their diagnosis is relatively easy to identify from patients than other OIs, on
the contrary, the study by Goud and Ramesh showed TB as the commonest OI and another study
by Ghate et al showed TB was the most common OI, followed by oral candidiasis, herpes zoster,
and cryptococcal meningitis. These differences can be attributed to the difference in the
geographical setting that is Asia versus Africa, as well as the level of health facility where the
study was conducted from, as their studies were conducted in a hospital setting where facilities
for diagnosis of most OIs were available unlike in Ruhiira HC III.
5.3 ASSOCIATED RISK FACTORS FOR THE DEVELOPMENT OF
OPPORTUNISTIC INFECTIONS AMONG HIV PATIENTS ATTENDING ART AT
RUHIIRA HEALTH CENTRE III.
5.3.1 Selected Socio-Demographic characteristics of study participants attending ART
clinic at Ruhiira HC III, Isingiro District.
In this study, the risk of OIs was loosely associated with gender, age, level of education and
marital status; majority of opportunistic infections were found among respondents aged 29-38
years (32% of cases) and this can be attributed to the fact that this is a sexually active age group
and majority of participants were from this age range. These findings are in line with those from
a similar study by Goud, T Gangadhara Ramesh (2014), where majority of the HIV positive
patients with opportunistic infections were in the age group of 30-39 years this is because this is
a sexually active age group in society.
According to gender, majority of OIs were found among females (34%), this can be attributed to
the genetic makeup of women having a lower immunity than men which poses a higher risk of
them contracting OIs as well as the fact that they were the biggest population (59%) among the
study participants compared to the males (41%). Contrarily, male gender was found to be strongly
associated with the occurrence of OIs in other reports.

24
According to marital status, majority of OIs were among the divorced (27%) and the never
married participants (20%) whereas the least number of cases of OIs were found among the
married (10%) and widowed participants (2%). This is because the divorced and the never married
participants are all taken to be under broad category of “single” and these individuals usually
have no limit to the number of sexual partners they have and this is one of the predisposing factors
to contracting OIs especially those that are sexually transmitted.
5.3.2 Distribution of OIs with selected clinical variables of participants attending ART
clinic at Ruhiira HC III, Isingiro District.
In this study, risk factors identified for OIs were WHO HIV clinical stage 3 (71%) and 4 (100%
of cases) and those with level of drug adherence of less than 95% (100% of cases), participants
with a CD4 count of less than 250 cells/µL (82%), and also participants with weight for age of
less than 50kg (73% of cases) which is indicative of malnutrition; This is because the higher the
WHO clinical stage, the lower ones immunity tends to fall and the more likely to acquire OI while
low drug adherence leads to an increase in the viral load of an individual which is a high risk
factor for development of OIs among HIV seropositive clients. Similarly a reduced CD4 cell
count below 250cells/µ implies that the person’s body’s defense mechanisms against infections
are down hence an increased chance of acquiring OIs. The results above are similar with those
from a similar study by, Moges et al. (2014) where in their study assessed the factors associated
with occurrence of OIs among HIV-infected patients taking ART and accordingly, younger age,
advanced baseline WHO stage, ART adherence, recent hemoglobin status, and recent weight were
found to be associated factors for OIs occurrence and in another study in India the prevalence was
50.63% with a significant positive association with WHO clinical staging and CD4 count as
associated risk factors (Bhuvana et al., 2015). This is because of lower immunity with higher
WHO staging and CD4 cell count of less than 250 as well as poor treatment outcomes which
result from poor drug adherence and all these factors further predispose to OIs.

25
5.4 ASSOCIATION OF HIGH RISK BEHAVIOR WITH HIV & OI POSITIVE STATUS
5.4.1 Distribution of OIs with different high risk behaviors exhibited by the study
participants.
The study also showed that high risk behaviors were highly associated with developing OIs,
majority of OIs were found among participants who reported to be having more than one sexual
partner (69% of these) followed by participants who reported alcohol consumption on a daily
basis (67% of cases), while participants who frequently engaged in unprotected sex, as well as
smokers, had the least number of cases of OIs (50% and 40% respectively) a study in the USA
revealed that There is much stronger evidence that unprotected sex with other HIV-infected
people is harmful for people with HIV where it involves the risk of exposure to sexually
transmitted infections (Alcorn, 2009). Similarly a study by Feldman and coworkers (2006) found
that, compared with nonsmokers, smokers receiving ART had poorer viral responses (HR, 0.79;
95% CI, 0.67–0.93), poorer immunologic response (HR, 0.85; 95% CI, 0.73–0.99), greater risk
of virologic rebound (HR, 1.39; 95% CI, 1.06–1.69), and more frequent immunologic failure (HR,
1.52; 95% CI, 1.18–1.96), hence a high chance of acquiring OIs.
CONCLUSION
According to the study, the overall prevalence of OIs among study participants was 59%, with
majority of cases being oral thrush (24%), followed by persistent diarrhea (18%), HSV infection
(16%), recurrent bacterial pneumonia (15%), TB (11%), HZ (10%) and the least number of cases
(6%) being for PPE. These were more common among females (34%) than males (25%) and other
predisposing factors identified were the sexually active age group between 28-38 years (32%),
being single as well as unemployment were also associated with majority of cases of OIs (49%)
and (85%) respectively. The study also revealed that the risk factors for developing OIs among
HIV clients attending ART included, advanced WHO HIV clinical stage 3 (74%) and 4 (100%),
CD4 cell count of less than 250 cell/µl (82%), malnutrition assessed by weight for age of less
than 50kg (73%), as well as low level of ART adherence <95% (100%). The study also
demonstrated that engaging in any of the four high risk behaviors increased one’s chances of
getting an OI by over 50%; that is to say, having multiple sexual partners (69%), alcohol intake
(67%), engaging in unprotected sexual intercourse (50%), as well as cigarette smoking (40%).

26
STRENGTHS AND WEAKNESSES
Among the strengths, included this being the first study about OIs among patients on Art, to be
carried in Isingiro District. Of the weaknesses, the required ample size was not met due to limited
time as well as man power.
RECOMMENDATIONS
In view of the above conclusions, the researcher recommends the following; Health education
talks be given to the clients regarding staying away from the high risk behaviors as well as
adhering to their ART treatment.
Also further studies be done in higher health facility settings like HC IV, district hospitals as well
as referrals where there are large number of clients and equipment to diagnose most OIs.
27
References
Agarwal, S. G., Powar, R. M., Tankhiwale, S., & Rukadikar, A. (2015). Study of Opportunistic
Infections in HIV-AIDS Patients and their Co-Relation with CD4+Cell Count.
Int.J.Curr.Microbiol.App.Sci, 4(6), 848–861. Retrieved from http://www.ijcmas.com/vol-
4-6/Saurabh G Agarwal, et al.pdf
Andrea Low, Georgios Gavriilidis, Natasha Larke, Marie-Renee B-Lajoie, Olivier Drouin, John
Stover, Lulu Muhe, Philippa Easterbrook (2016) ; Incidence of Opportunistic Infections
and the Impact of Antiretroviral Therapy Among HIV-Infected Adults in Low- and
Middle-Income Countries: A Systematic Review and Meta-analysis. Clin Infect Dis; 62
(12): 1595-1603.
Aulawi, A., & Krejcie, M. (2017). Method for determining sample size of a population.
Retrieved from http://downloadkemanx.blogspot.ug/2010/06/krejcie-and-morgan-method-
for.html
B-Lajoie, M.-R., Drouin, O., Bartlett, G., Nguyen, Q., Low, A., Gavriilidis, G., … Muhe, L.
(2016). Incidence and Prevalence of Opportunistic and Other Infections and the Impact of
Antiretroviral Therapy Among HIV-infected Children in Low- and Middle-income
Countries: A Systematic Review and Meta-analysis. Clinical Infectious Diseases, 62(12),
1586–1594. https://doi.org/10.1093/cid/ciw139
Bhuvana, K. B., Hema, N. G., & Patil, R. T. (2015). Prevalence and risk factors for
opportunistic infections in HIV patients who developed adverse drug reactions ( ADRs )
to antiretroviral therapy ( ART ) in a tertiary-care teaching hospital, 5(3), 200–206.
https://doi.org/10.5455/njppp.2015.5.0301201517
Braithwaite RS, Bryant KJ: Influence of alcohol consumption on adherence to and toxicity of
antiretroviral therapy and survival. Alcohol Res Health. 2010, 33 (3): 280-
286.PubMedPubMed Central
Bryant KJ, Nelson S, Braithwaite S, Roach D: Integrating HIV/AIDS and alcohol research.
Alcohol Res Health. 2010, 33 (3): 165-255.Google Scholar
CDC. (2015). Chlamydial Infections in Adolescents and Adults. Retrieved from
https://www.cdc.gov/std/tg2015/chlamydia.htm
Colindres, R., Mermin, J., Ezati, E., Kambabazi, S., Buyungo, P., Sekabembe, L., … Quick, R.
(2008). Utilization of a basic care and prevention package by HIV-infected persons in

28
Uganda. AIDS Care, 20(2), 139–145. https://doi.org/10.1080/09540120701506804
Eyasu, M., Berhane, A., & Yohannes, S. (2015). Spectrum and Associated Risk Factors of
Opportunistic infections among antiretroviral therapy experienced HIV/AIDS patients in
Addis Ababa, Ethiopia. World Journal of Pharmacy and Pharmaceutical Sciences, 4(10),
347–366.
John Rubaihayo, Nazarius M. Tumwesigye, and Joseph Konde-Lule, Henry Wamani et.al
(2016): Frequency and distribution patterns of opportunistic infections associated with
HIV/AIDS in Uganda. BMC Research Notes. 9:501
Goud, T Gangadhara; Ramesh, K. (2014). Opportunistic infections among HIV patients
attending Tertiary Care hospital , Karnataka , India. Internal Journal of Current
Microbiology and Applied Sciences, 3(4), 824–829.
Mala, E., & Aroma, O. (2015). Opportunistic infections in relation to CD4 counts in human
immunodeficiency virus seropositive patients in a tertiary care hospital in North India.
Retrieved from http://www.cjhr.org/article.asp?issn=2348-
3334;year=2015;volume=2;issue=3;spage=199;epage=202;aulast=Mala
Manisha Ghate, Deshpande, S., & Tripathy, S. (2009). Incidence of common opportunistic
infections in HIV-infected individuals in Pune, India. Incidence of Common Opportunistic
Infections in HIV-Infected Individuals in Pune, India, 13(1), e1--e8.
Mitiku H, F, W., & Z, T. (2015). Magnitude of opportunistic infections and associated factors
in HIV-infected adults on antiretroviral therapy in eastern Ethiopia. Research and
Palliative Care, 7, 137–144.
Morley, J. E. (2007). Protein-energy malnutrition definition. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3132791
R, P., F, J.-O., M, A., MJ, G., & Rivas. (2007). Impact of syphilis infection on HIV viral load
and CD4 cell counts in HIV-infected patients.
R, S., E, W. M., S, K., N, R., A, F., & P, D. (2011). Cigarette Smoking in the HIV-Infected
Population.
Rubaihayo, J., Tumwesigye, N. M., Konde-Lule, J., & Wamani, H. (2016). Frequency and
distribution patterns of opportunistic infections associated with HIV/AIDS in Uganda.
Selnes OA. (2010). Impact of HIV infection and alcohol on cognition. Neurobehav Hiv Med,
85–95.
Shalini Duggal, Chugh, T. Das, & 2Ashish Kumar Duggal. (2012). HIV and Malnutrition.
29
Effects on Immune System.
Uganda Ministry of Health. National AIDS indicator survey 2011. Kampala: Uganda Ministry
of Health; 2011.
Uganda MOH. (2015). The HIV And AIDS Uganda Country Progress Report 2014, 73.
Retrieved from
http://www.unaids.org/sites/default/files/country/documents/UGA_narrative_report_2015.
UNAIDS. (2016). Global AIDS update. WHO/UNAIDS.

30
Appendix 1: Consent Form
I MAWANDA BASHIR a student at Kampala International University pursuing a Diploma in
Clinical Medicine and Community Health is conducting a research on prevalence and associated
risk factors for opportunistic infections among patients attending ART clinic at Ruhiira Healt h
Centre Three, Isingiro District.
Part I- Information
Dear participant,
Following consultation with administration of the Health Centre and administration of the Faculty
of Allied Health Sciences, Kampala International University- Western Campus, and authority has
been given to me to interview patients attending ART Clinic. The participants are required to
consent to voluntarily participate in this study.
I the under signed;
I have read the information sheet above about the planned study and the explanation given to me,
and I understand what I have been requested to do in respect to this study.
I have discussed and asked questions about the study and got satisfied with the answers. I have
after due consideration agreed to voluntarily participate in the study.
Participant’s signature………………………………..Date……………….………………..
Investigators name ……………………………...Signature ………………..Date……………

31
Appendix 2: Questionnaire.
Instructions; Tick the right option and fill in where necessary.
PART A: Bio-data
1. Age ……….
2. Sex…………
3. Tribe ………………………
4. Religion…………………….
5. Marital status?
1. Married
2. Single
3. Separated
4. Widowed
5. Level of education;
a. None
b. Primary school
c. Secondary
d. Tertiary
6. Occupation of the respondent
a. Business person.
b. House wife
c. Student
d. Peasant
e. Civil servant
Others (specify)
…………………………………………………………………………………………………

32
PART B: PATIENTS LIFE-STYLE
For the patient attending ART.
1. A) Do you smoke tobacco cigarettes?
a. Yes
b. I used to but stopped
c. No
B) If yes, how many sticks per day, on average?
a. 1-2
b.3-5
c. 5-10
d.More than 10
C) If you stopped, please specify when and the reason for stopping
……………………………………………………………………………………………………
………………………………………………………………………………….……………
2. A) Do you take alcohol?
a. Yes
b. I used to take but stopped
c. No
B) If yes, how many bottles per day on average?
a. 1-2
b. 3-5
c. 5-10
d. More than 10
e. None
C) If you stopped please specify when and the reason for stopping
……………………………………………………………………………………………………
………………………………………………………………………………………………
33
3. A) How often do you engage in sexual intercourse?
a. Once in a week
b. 3-5 times in a week
c. More than 5 times in a week
d. None
B) Besides your spouse, how many other sexual partners do you have?
a. 1-2
b. 3-5
c. 5-10
d. More than 10
e. None
C) Do you know how to use a condom?
a. Yes
b. No
D) If yes, do you always use a condom when engaging in sexual intercourse?
a. Yes, but with my spouse only
b. Yes, but with my side-dish(es) only
c. Always
d. Never

34
Appendix 3: DATA COLLECTION SHEET
No. Age sex Type of
OIs
WHO
clinical
stage
Baseline
CD4
Baseline
Weight
Drug
compliance
Marital
status
First
line
regime
n

35
Appendix 5: Work Plan
MONTH/
ACTIVITY
FEB MAR APR MAY JUNE JULY
Proposal writing
approval
Data collection
Analysis/documenta
tion
Report writing
Submission of report

36
Appendix 6: MAPS
Map of Uganda showing Isingiro District at position # 26
INSINGIRO DISTRICT
37
MAP OF ISINGIRO SHOWING SUB-COUNTIES

38
LETTER OF PERMISSION
Related Documents











