Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript








468 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Prevalence of measles antibody inchildren of different ages in Shiraz,Islamic Republic of IranA. Karimi,1 A. Arjomandi,1 A. Alborzi,1 M. Rasouli,1 M.R. Kadivar,1 B. Obood1 and B.Pourabbas1
1Clinical Microbiology Research Centre, Shiraz University of Medical Sciences, Shiraz, Islamic Republic ofIran.Received : 10/10/02; accepted: 21/09/03
ABSTRACT An outbreak of measles due to secondary vaccine failure prompted this investigation into theprevalence of measles antibody in children. We studied 608 children in 7 different age groups: 6, 9, 14 and 18months and 6, 10 and 15 years. Children in the 2 youngest groups received no vaccination; the rest werevaccinated at 9 months and 15 months. The 15-year-old age group received an additional vaccination.Transplacental measles antibody (Ab) decreased from 10.0% at 6 months to 0% at 9 months. Measles Abwas positive in 52.9% (14 months), 89.4% (18 months), 60.8% 96 years), 45.0% (10 years) and 96.8% (15years). To increase Ab levels, a booster vaccination is recommended, administered either with the secondDPT booster or at pre-high school age.
Prévalence des anticorps antirougeoleux chez des enfants de différents âges à Chiraz (Répu-blique islamique d’Iran)RÉSUMÉ Une flambée de rougeole due à l’échec de la vaccination secondaire a conduit à effectuer uneétude de la prévalence des anticorps antirougeoleux chez les enfants. Nous avons étudié 608 enfants danssept groupes d’âge différents : 6, 9, 14 et 18 mois et 6, 10 et 15 ans. Les enfants des deux groupes d’âge lesplus jeunes n’avaient pas été vaccinés ; le reste des enfants avaient été vaccinés à l’âge de 9 et 15 mois. Legroupe des enfants de 15 ans avait eu une vaccination supplémentaire. Les anticorps transplacentairesdiminuaient, passant de 10,0 % à l’âge de 6 mois à 0 % à l’âge de 9 mois. Dans les groupes d’âge étudiés,la proportion des enfants présentant des anticorps antirougeoleux par âge était de 52,9 % (14 mois), 89,4%(18 mois), 60,8 % (6 ans), 45,0 % (10 ans) et 96,8 % (15 ans). Afin d’augmenter les taux d’anticorps, unevaccination de rappel est recommandée, à administrer soit avec le deuxième rappel DTC soit à l’âgecorrespondant au cycle d’enseignement pré-secondaire.
01 Prevalence of measles.pmd 8/17/2005, 11:03 AM468

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 469
Introduction
Prevention of measles using vaccination isstill the most important task in developingcountries. The disease is a substantialcause of mortality and morbidity in chil-dren. It is highly contagious but prevent-able [1]. Mortality has declined drama-tically since the introduction of a live atten-uated vaccine. Despite an 85% decrease inmortality, however, outbreaks of measleshave been reported due to secondary vac-cine failure in older age groups (10–24years), e.g. in a study of measles epidemi-ology by the Iranian Minister of Health andMedical Education in 1998 [2]. This has ledsome countries, including the United Statesof America, to introduce an additional doseof vaccine in school-age children. In the Is-lamic Republic of Iran, the decline in mea-sles incidence due to the vaccinationprogramme has been noticed in children;cases in older age groups are, however, stillemerging. This might be due to immigra-tion from neighbouring countries such asAfghanistan and Pakistan, which have avaccine coverage of less than 80% (unpub-lished report, Ministry of Health and Medi-cal Education, 1988).
Our study was conducted to disclosethe prevalence of measles antibodies in dif-ferent age groups and to evaluate the ne-cessity of administering additional doses ofvaccine. The study was prompted by anoutbreak of measles in our country in 1997.
Methods
Over the period 2001–02 we enrolled 608children into the study in 7 different agegroups. Details of the groups and their vac-cination history are given in Table 1. Thechildren were selected by random clustersampling of children referred to the Motah-hari out-patient clinic or from primary
schools in Shiraz. The epidemiological dataincluding sex, age, socioeconomic status,number of family members and vaccinationhistory were obtained. For antibody (Ab)testing, 5 mL of blood was drawn and se-rum was separated and frozen at –20 °C.The sera were examined using an enzyme-linked immunosorbent assay IgG kit (Mor-billio, Radim SpA, Pomezia, Italy). Sampleswith optical density (OD) lower than thecut-off control (OD < 0.200) were consid-ered non-reactive for measles IgG antibod-ies. Samples with OD higher than thecut-off control (OD > 0.700) were consid-ered reactive for measles IgG antibodies.Samples with absorbance values ± 10% ofthe cut-off (OD 0.200 to 0.700) controlwere considered questionable and were re-tested for confirmation.
Results
We enrolled 608 children, 52% male and48% female, in the study. Table 2 shows
Table1 Vaccination history for children inseven different age groups
Group No. Age Vaccination history
1 70 6 m No vaccination
2 62 9 m No vaccination
3 70 14 m Vaccinated at 9 m
4 66 18 m Vaccinated at 9 mand 15 m
5 97 6 y Vaccinated at 9 mand 15 m
6 149 10 y Vaccinated at 9 mand 15 m
7 94 15 y Vaccinated at 9 m,15 months and 9 mprior to the study
m = months. y = years.
01 Prevalence of measles.pmd 8/17/2005, 11:03 AM469

470 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
the frequency of measles Ab prevalence ineach age group. Antibody prevalence washigher in girls, although the result was notstatistically significant. The Ab prevalencewas significantly different in all consecu-tive age groups (P = 0.00001). The P-val-ues for the different age groups are shownin Table 2. Number of family members, so-cioeconomic status and literacy of parentswere not significant (data not shown).
Transplacental IgG from mothers de-clined from 10.0% at 6 months to 0% at 9months of age in non-vaccinated children.Although this is unusual and we do nothave good explanation for it, it is possiblethe titre of measles Ab in our pregnantwomen was very low due to low contactwith wild measles viruses. However, in in-fants more than 9 months old, the preva-lence of Ab increased owing to vaccinationat 9 months and 15 months of age, and de-clined over time thereafter.
Primary vaccine failure is defined as ano detectable antibody after vaccination. Itcan be caused by interaction of maternalantibody to the vaccine by immunologicalresponse, technical problems, and so on.Primary vaccine failure in our study was
47.1% in the 14-month-old group, reduc-ing to about 10.6% in the 18-month-oldgroup due to the second dose of vaccinegiven at 15 months. Primary vaccine failurewas 55% at age 10, reducing to 3.2% at 15due to the third vaccine administration.
Discussion
Measles is a highly contagious, preventabledisease. The incidence has shown a re-markable decline in our county over recentyears due to routine administration of live,attenuated vaccine at the ages of 9 monthsand 15 months, but several reports of dis-ease outbreak in older age groups havebeen documented [2,3]. The presence ofmeasles Ab indicates previous infection,active immunization or, at ages below 9months, maternal Ab transmission, all ofwhich offer immunity.
Our study was conducted to determinethe pattern of Ab prevalence in different agegroups of children. In this study, transpla-cental Ab was detected in only 10.0% of 6-month-old infants, declining to 0% at 9months. This finding is in accord with pre-
Table 2 Prevalence of measles antibody (Ab) in children in seven different agegroups in Shiraz
Age Total Ab positive Ab negative P-values between different age groupsNo. No. % No. %
6 m 70 7 10.0 63 90.0
9 m 62 0 – 62 100.0 6 m and 9 m 0.014
14 m 70 37 52.9 33 47.1 9 m and 14 m 0.00001
18 m 66 59 89.4 7 10.6 18 m and 6 y 0.00006
6 y 97 59 60.8 38 39.2 6 y and 10 y 0.016
10 y 149 67 45.0 82 55.0 10 y and 15 y 0.00001
15 y 94 91 96.8 3 3.2 All age groups 0.00001
Total 608 320 50.7 288 49.3
m = months. y = years.
01 Prevalence of measles.pmd 8/17/2005, 11:03 AM470

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 471
vious studies from Iran [4,5]. The declineof maternal antibody in infants in differentgeographic areas is dependent on socioeco-nomic states, catabolism of antibody,amount of antibody transmission to fetus,level of maternal antibody, and so on. Insome studies it was shown to be between0% and 10% at about 11 months of age[2,4]. Therefore, a high percentage of chil-dren at 6 months of age are also susceptiblein an outbreak of the disease. It has beendocumented that the Schwarz type vaccinethat is used in the Islamic Republic of Iranis not so effective for 6-month-old infants[6,7]. The absence of Abs during outbreakswas 47.1% at 14 months, 1 month beforethe second vaccination and 10.6% 3months afterwards. This finding was in ac-cordance with previous studies [8–10].High primary vaccine failure at 9 months ofage might be related to trans-placental Abfrom mothers [8].
Other possible factors responsible forthis high primary vaccine failure includenutritional status of children [11], acutedisease during vaccination [12–14] andconcomitant administration of gammaglobulin [15], race, environmental factors[16,17], sex [18] and immunity status ofthose being vaccinated [19,20]. In ourstudy, sex and literacy were not statisticallyimportant factors in primary vaccine fail-
ure. Measles Ab was positive in 89.4% ofthe 18-month-old children and 60.8% at 6years of age, which was statistically signif-icant (P < 0.001). In the 10-year-old group,only 45.0% of the children were positivefor measles Ab (P = 0.016). This Ab-waning phenomenon is reported to beabout 2%–20% in several studies [21–24].The presence of Ab may be due to the vac-cine effect or to previous infection withwild virus. The waning of Ab titre is greaterin subjects who produce lower initial Ab ti-tres. Accordingly, a single vaccination pro-duces more significant Ab waning [25]. Animportant observation was the significantrise in the Ab titre of the 15-year-old agegroup following the administration of anadditional booster dose of the vaccine,compared to the 10-year-old age group (P< 0.00001) (Table 2). The necessity for anadditional immunization is also emphasizedin a report from Singapore [26] and in oth-er countries [27,28]. Therefore, an addi-tional dose of measles vaccine isrecommended for Iranian children aroundhigh-school age.
Acknowledgement
The authors wish to thank Dr A. Japoni forhis help in preparing the manuscript.
References
1. Issacs D, Menser M. Modern vaccines,measles, mumps, rubella, and varicella.Lancet, 1990, 335:1384–7.
2. Study of measles epidemiology in Iranduring 1991 to 1998. Annual report of theMinister of Health and Medical Educa-tion. Tehran, Ministry of Health and Medi-cal Education, 1998.
3. Health picture. Annual report of the Min-ister of Health and Medical Education.
Tehran, Ministry of Health and MedicalEducation, 2002.
4. Mirchamsy H et al. Age of measles im-munization in tropics. Developments inbiological standardization, 1978, 41:191–4.
5. Mokhtariazad T. Evaluation of measlesvaccination in 6-month infants [thesis].Tehran, Tehran University of MedicalSciences, 1982.
01 Prevalence of measles.pmd 8/17/2005, 11:03 AM471

472 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
6. Markowitz LE et al. Immunization of six-month-old infants to different dosesof Edmonston–Zagreb and Schwarzmeasles vaccine New England journalof medicine, 1990, 322:580–7.
7. Tidjani O et al. Serological effects ofEdmonston–Zagreb, Schwarz and AIK-C measles vaccine strains given at ages4–5 or 8–10 months. Lancet, 1989, 11:1357–60.
8. Shelton JD et al. Measles vaccine effi-cacy: Influence of age at vaccination vsduration of time since vaccination. Pedi-atrics, 1978, 62:961–4.
9. Mirchamsy H et al. Comparative field trialof five measles vaccines produced inhuman diploid cell, MRC-S. Journal ofbiological standardization, 1977, 5:1–18.
10. Mirchamsy H et al. Mass immunization ofchildren in Iran with live attenuatedSugiyama virus adapted to calf kidneycell cultures. Japanese journal of experi-mental medicine, 1971, 41:39–40.
11. Wesley A, Coovadia HM, Henderson L.Immunological recovery after measles.Clinical and experimental immunology,1978, 32:540–4.
12. Krober MS, Stracener CE, Bass JW. De-creased measles antibody response af-ter measles–mumps–rubella vaccine ininfants with colds. Journal of the Ameri-can Medical Association, 1991, 265(16):2095–6.
13. Halsey NA et al. Response to measlesvaccine in Haitian infants 6 to12 monthsold. New England journal of medicine,1985, 313(9):544–9.
14. Ndikuyeze A et al. Immunogenicity andsafety of measles vaccines in ill Africanchildren. International journal of epide-miology, 1988, 17(2):448–55.
15. Krugman S. Present studies of measlesand rubella immunization in the United
States: a medical program report. Pediat-rics, 1971, 78:1–16.
16. Black FL et al. Geographic variation ininfant loss of maternal measles antibodyand in prevalence of rubella antibody.American journal of epidemiology, 1986,124(3):442–52.
17. Neiburg P, Dibley MJ. Risk factors forfatal measles infection. Internationaljournal of epidemiology, 1980, 15(3):309–11.
18. Bromberg K et al. Maternal immunity tomeasles and infant immunity at less thantwelve months of age relative to mater-nal place of birth. Journal of pediatracs,1994, 125(4):579–81.
19. Dai B et al. Duration of immunity follow-ing immunization of live measles vac-cine. Bulletin of the World HealthOrganization, 1991, 69(4):415–23.
20. Markowitz LE et al. Persistence ofmeasles antibody after revaccination.Journal of infectious diseases, 1992,166(1):205–8.
21. Climie A, Andre FE. Field trial of heat-stable measles vaccine in Papua NewGuinea. Journal of tropical medicine andhygiene, 1984, 87(6):249–55.
22. Zhuji Measles Vaccine Study Group. Epi-demiologic examination of immunityperiod of measles vaccine. Chinesemedical journal, 1987, 67:19–22 [in Chi-nese].
23. Xiang JZ, Chen AH. Measles vaccine inthe People’s of Republic of China. Re-views of infectious diseases, 1983, 5(3):506–10.
24. Gdalevich M et al. Measles epidemicin Israel—successful containment inthe military. Preventive medicine, 2000,31(6):469–51.
25. Smith FR et al. Reported measles in per-sons immunologically primed by prior
01 Prevalence of measles.pmd 8/17/2005, 11:03 AM472

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 473
vaccination. Journal of pediatrics, 1982,101(3):391–3.
26. Goh D et al. Resurgence of measles inSingapore: profile of hospital cases.Journal of paediatrics and child health,1999, 35(5):493–6.
27. Christenson B, Bottiger M. Measles anti-body comparison of long-term vaccina-
tion titer, early vaccination titers andnaturally acquired immunity. Vaccine,1994, 12(2):129–33.
28. Olsha M et al. Measles immunity in Is-raeli young adults. Israel journal of medi-cal sciences, 1994, 30:596–9.
Measles mortality reduction
Measles remains a leading cause of death among young children,despite the availability of a safe and effective vaccine for the past40 years. More than half a million people, the majority of them chil-dren, died from measles in 2003; in the Eastern Mediterranean Re-gion (EMR) there were an estimated 69 000 deaths from measles.WHO and UNICEF have developed a joint Strategic Plan for MeaslesMortality Reduction and Regional Elimination 2001–2005. The over-riding goal of this plan is to reduce the number of global measlesdeaths (from the 1999 level) by 50% by the end of 2005. The prioritycountries in EMR are Afghanistan, Djibouti, Pakistan, Somalia andSudan. The four-pronged strategy for sustainable measles mortalityreduction is based on: providing strong routine immunization; pro-viding a “second opportunity” for measles immunization to all chil-dren; surveillance; improvement in the clinical management ofmeasles cases. Thus, from 1999 to 2003, more than 350 millionchildren globally received measles vaccine through supplementaryimmunization activities. Moreover, improvements were made in rou-tine immunization over this period. These accelerated activitieshave resulted in a significant reduction in estimated global measlesdeaths. Overall, global measles mortality decreased by 39% be-tween 1999 and 2003. Given the progress made to date, it is ex-pected that the 2005 global measles mortality reduction goal will beachieved.
Source: WHO Fact sheet No. 286Available at: http://www.who.int/mediacentre/factsheets/fs286/en/
01 Prevalence of measles.pmd 8/17/2005, 11:03 AM473

474 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Évaluation de la réponse vaccinalecontre la poliomyélite et la rougeolechez les enfants malnutris au MarocH. Caidi, 1 F. Bennis, 2 N. Mouan 2 et R. El Aouad 1
1Département d’Immuno-Virologie, Institut national d’Hygiène, Rabat (Maroc).Courriel : [email protected] de Pédiatrie III, C.H.U. Avicenne, Rabat (Maroc).Reçu : 07/02/02 ; accepté : 26/10/03
RÉSUMÉ Il s’agit d’une étude comparative de la séroprévalence des anticorps anti-poliovirus type 1, anti-poliovirus type 2, anti-poliovirus type 3 et des anticorps anti-rougeole chez les enfants malnutris (37) etcomplètement vaccinés et les enfants dont l’état nutritionnel est normal (34). L’âge est compris entre10 mois et 5 ans. Les enfants souffrant d’une malnutrition protéino-calorique présentaient un tauxd’immunisation vis-à-vis du vaccin poliomyélitique et du vaccin antirougeoleux très faible en comparaisonavec les enfants témoins. En effet, 94,1 % des enfants témoins sont immunisés contre le poliovirus type 1,97,1 % contre le poliovirus type 2 et 91,2 % contre le poliovirus type 3. Chez les enfants malnutris, ces tauxétaient dans certains cas significativement plus faibles : 40,5 % (p = 0,001), 59,5 % (p = 0,001) et 40,5 %respectivement. La même baisse de la réponse vaccinale a été notée concernant le vaccin antirougeo-leux: le taux d’immunisation est de 82,4 % chez les enfants témoins contre 35,1 % chez les enfantsmalnutris. La malnutrition est le facteur majeur de l’échec de la réponse vaccinale qui nous interpelle pouradopter les attitudes adéquates en vue d’éviter les échecs de vaccination.
Evaluation of the response to vaccination against poliomyelitis and measles in malnourished chil-dren in MoroccoABSTRACT We made a comparative survey of the poliovirus antibodies (anti-poliovirus type 1, anti-poliovirustype 2 and anti-poliovirus type 3) and the measles antibodies in malnourished but completely vaccinatedchildren (37) and control children (34). The age range was 10 months to 5 years. Immunization in children withprotein–energy malnutrition was low for both vaccines. Seroprevalence rates of the polio 1, polio 2, polio 3antibodies and the measles antibodies in the control group were 94.1%, 97.1%, 91.2% and 82.4% respectively.In malnourished children the respective rates were in some cases significantly lower being: 40.5% (P = 0.001),59.5% (P = 0.001), 40.5% and 35.1%. Malnutrition is a major determinant of the humoral response to oral polioand measles vaccines and must be given due consideration to prevent vaccination failure.
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM474

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 475
Introduction
La malnutrition protéino-calorique (MPC)représente dans les pays en développementl’un des principaux problèmes de santépublique, responsable d’une forte mortalitéinfantile [1,2]. D’après des analyses ré-centes des causes de décès chez l’enfant, lamalnutrition, mesurée par les paramètresanthropométriques, serait associée audécès dans près de la moitié des cas dansles pays en développement [1]. Elle est parailleurs fréquemment associée sous uneforme grave ou modérée à de très nom-breuses affections où elle intervient commefacteur aggravant [1,2,3].
Plusieurs mécanismes immunitairessont défaillants chez les enfants malnutrisqui, de ce fait, sont victimes de sévères in-fections et du cycle vicieux infection-malnutrition [4]. La malnutrition constitueun problème majeur de l’échec des pro-grammes de vaccination dans les pays où lamalnutrition est répandue.
Des études ont montré la faible réponseau vaccin vivant atténué contre la rougeoleet la poliomyélite en comparaison avec lesenfants témoins [5,2,6,7].
L’objectif de notre étude consiste àévaluer la séroprévalence des anticorpsanti-poliovirus type 1, anti-poliovirus type2 et anti-poliovirus type 3 ainsi que des an-ticorps anti-rougeole chez les enfantsmalnutris, complètement vaccinés. Laprévalence de ces mêmes anticorps est dé-terminée en parallèle chez les enfantscomplètement vaccinés et dont l’état nutri-tionnel est normal.
Méthodes
Enfants malades etenfants témoinsL’étude est réalisée sur 37 enfants(20 garçons et 17 filles) âgés de 10 mois à
5 ans auprès du service de Pédiatrie III,Hôpital d’enfants du Centre hospitalier uni-versitaire (C.H.U.) de Rabat. Tous ces en-fants sont vaccinés contre la poliomyélite(vaccin antipoliomyélitique oral trivalent ;fabricants : Bucham & Clyron) et la rou-geole (vaccin antirougeoleux ; fabricants :Serum Institut of India et Aventis) et rem-plissent les critères de malnutrition qui sontvérifiés au préalable grâce à un question-naire validé par le clinicien. Ils sont alorsclassés selon l’âge (Tableau 1), le type demalnutrition (Tableau 2) et le degré de mai-greur (Tableau 3).
Le calendrier vaccinal au Maroc prévoitune première dose de vaccin poliomyéli-tique oral à la naissance et 3 doses de rappelà un intervalle d’un mois, et une dose devaccin antirougeoleux à 9 mois.
Le groupe témoin a été recueilli égale-ment auprès du même service. Il s’agit de20 garçons et 14 filles (34 enfants) âgés de10 mois à 5 ans. Ces enfants sont tous vac-cinés contre la poliomyélite et la rougeole etne présentent aucun signe de malnutrition.Le prélèvement sanguin est fait dans le ca-dre d’un bilan destiné à l’exploration de lapathologie qui a motivé leur hospitalisation.
Tableau 1 Répartition des enfants malnutriset des enfants témoins en fonction de l’âgeet du sexe
Variable Enfants malnutris Enfants témoinsNombre % Nombre %
Âge (mois)10-12 16 34,2 14 41,113-15 10 27,0 9 26,416-24 7 18,9 6 17,6>24 4 10,8 5 14,7
SexeMasculin 20 54,0 20 58,8Féminin 17 45,9 14 41,1
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM475

476 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Prélèvement sanguinUn prélèvement sanguin (5 ml) veineux estrecueilli dans un tube sec pour chaque en-fant. Le sang est centrifugé (500 g pendant10 minutes) et le sérum est stocké congeléà - 80 °C jusqu’à son utilisation.
Titrage des anticorps anti-polio 1,2 et 3 et des anticorps anti-rougeoleLe titrage des anticorps anti-poliovirus 1, 2et 3 ainsi que des anticorps anti-rougeoleest réalisé par réaction de séroneutralisationsur cultures cellulaires. Deux lignées sontutilisées : la lignée HEp-2 pour le titrage desanticorps anti-poliovirus 1, 2 et 3, et lalignée Vero pour le titrage des anticorpsanti-rougeole. Le choix de ces techniquesétait justifié par leur grande maîtrise dansnotre laboratoire.
Pour le poliovirus, le titre du sérum estdonné par la plus forte dilution sérique quineutralise 50 % des cultures cellulairescontre 100 DI50 de virus d’épreuve. Les ré-sultats des titres d’anticorps sont normale-ment exprimés par leur réciproque (Manualfor the virological investigation of the po-liomyelitis).
La DCP 50 % est calculée par la mé-thode de Reed et Munch.
Log DCP 50% = log (dilution 50 %d’effet cytopathogène) + DP corrigé
Pour le titrage du taux d’anticorps con-tre le vaccin antirougeoleux, le titre dusérum est calculé par la méthode de Kärber(Manual for the laboratory diagnosis ofmeasles virus infection).
Log10 (inverse) de la plus grande dilution - (somme des moyennes des plages de lyse (UFP) ÷ titre inverse du virus contrôle - 0,5) × log10 du facteur de dilution.
Résultats
La tranche d’âge la plus touchée par lacarence nutritionnelle se situe entre 9 moiset 2 ans et touche aussi bien le sexe mascu-lin que le sexe féminin.
Tableau 2 Répartition des enfants malnutrisen fonction du type de malnutrition
Type de Garçons Filles Totalmalnutrition (%)
Kwashiorkor 2 2 4 (10,8)
Marasme 6 0 6 (16,2)
Autres hypotrophies 12 15 27 (27,9)
Syndromes anémiques 3 0 3
Vomissements associésà une béancedu cardia 1 1 2
Infections parasitaires 2 0 2
Infectionsmycobactériennes 0 1 1
Avitaminose 2 0 2
Maladie cœliaque 4 3 7
Cardiopathie congénitale 1 0 1
Diarrhées avecdéshydratation 6 4 10
Total (%) 20 (54) 17 (45,9) 37 (100)
Tableau 3 Répartition des enfants malnutrisen fonction du degré de maigreur
Degré de Nombre %maigreur (%) de cas
< 60 14 37,8
70 10 27,0
80 8 21,6
90 5 13,5
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM476

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 477
Les résultats de séroneutralisation pourle vaccin antipoliomyélitique chez les en-fants témoins montrent qu’après trois do-ses de vaccin antipoliomyélitique oraltrivalent (VPOT), la proportion d’enfantstémoins présentant des titres ≥ 8 est de94,1 % (32/34) pour le type 1, de 97,1 %(33/34) pour le type 2 et de 91,2 % (31/34)pour le type 3.
Chez les 37 enfants de notre étude souf-frant d’une malnutrition protéino-caloriqueet en comparaison avec le groupe témoin, letaux d’immunisation est beaucoup plusfaible aussi bien pour le poliovirus type 1que pour le poliovirus type 2 et le poliovirustype 3. En effet, la séroconversion est de40,5 % (15/37) pour le poliovirus type 1,59,5 % (22/37) pour le poliovirus type 2 et40,5 % (15/37) pour le poliovirus type 3.Le pourcentage d’enfants triple positifs estde 37,8 % (14/37) seulement (Tableau 4).
Pour le vaccin antirougeoleux, les résul-tats de la séroneutralisation ont révélé quemalgré une couverture vaccinale de 100 %chez les enfants témoins, le taux de séro-conversion contre le vaccin est de 82,4 %(28/34) ; 70 % présentent un tauxd’anticorps compris entre 120 et 899 UFPet seulement 12,4 % des enfants présententun titre supérieur à 900 UFP. Le taux de
séroconversion négatif chez ce grouped’enfants est de 17,6 % (6/34).
Chez les enfants malades, le tauxd’immunisation contre la rougeole estbeaucoup plus abaissé par rapport augroupe témoin. Ainsi, la présence d’anti-corps neutralisant le virus de la rougeolerévélé par la réaction de séroneutralisationest notée chez seulement 35,1 % (13/37)des enfants, le titre des anticorps étant en-tre 120 et 899 UFP. La majorité des enfantsde ce groupe sont séronégatifs (24/34), soitun pourcentage de 64,8 % ; le titre des anti-corps neutralisants est inférieur à 8 UFP.Par ailleurs, aucun enfant ne présente untaux d’anticorps supérieur à 900 UFP.
On a également pu comparer le tauxd’immunisation contre la poliomyélite et larougeole chez les enfants malnutris enfonction de deux paramètres : le type demalnutrition et le degré de maigreur.
Chez les cas de kwashiorkor (4 cas) etde marasme (6 cas), le taux d’immunisa-tion est nul aussi bien pour les trois typesde poliovirus que pour le virus de la rou-geole. Pour les autres hypotrophies (27cas), 12 présentent un statut immunitairenormal pour le vaccin antipoliomyélitique etle vaccin antirougeoleux avec un pourcen-tage de 44,4 % et 13 enfants ont des testsnégatifs pour la poliomyélite et la rougeole,soit un pourcentage de 48,1 %. Les deuxhypotrophes restants ont des tests positifspour la poliomyélite et négatifs pour la rou-geole (7,4 %).
L’immunisation la plus défaillante estcelle trouvée chez les enfants avec un degréde maigreur < 60 % et un degré de mai-greur de 90 % : 3 enfants seulement sur 14(21,4 %) avec un degré de maigreur< 60 % présentent une séroconversion vis-à-vis du vaccin antipoliomyélitique contre2 cas (14,2 %) pour le vaccin antirougeo-leux ; un seul cas sur 5 (20,0 %) avec undegré de maigreur de 90 % (les enfantsavec un degré de maigreur de 90 % sont
Tableau 4 Taux d’immunisation contre lepoliovirus et le virus de la rougeole chez lesenfants témoins et les enfants malnutris
Immunisation Enfants Enfants pcontre témoins malnutris
% %
PoliovirusType 1 94,0 40,5 < 0,001Type 2 97,0 59,0 < 0,001Type 3 91,0 40,5 < 0,001
Virus de larougeole 82,3 35,1 < 0,001
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM477

478 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
tous des formes œdémateuses où le degréde maigreur n’est pas un bon indicateur del’état nutritionnel du malade) est séropositifaussi bien pour le virus poliomyélitique quepour le virus de la rougeole.
Trois cas sur 10 (30,0 %) avec un de-gré de maigreur de 70 % montrent uneséroconversion positive vis-à-vis du polio-virus et 4 enfants sur 10 (40,0 %) uneséroconversion positive vis-à-vis du virusde la rougeole ; 7 enfants sur 8 ayant undegré de maigreur de 80 % sont séroposi-tifs pour le poliovirus (87,5 %) contre6 cas (75,0 %) pour le virus de la rougeole.
Discussion
Comme déjà mentionné, la tranche d’âge laplus touchée par la carence nutritionnelle sesitue entre 10 mois et deux ans ; cetteprédilection trouve son explication dans lesevrage de l’allaitement au sein et la grandefréquence des maladies associées à cet âge[2,3]. Par ailleurs, la malnutrition toucheaussi bien les garçons (54 %) que les filles(45,9 %), la différence n’étant pas statis-tiquement significative (p = 0,48). Pour lesrésultats de séroneutralisation, notre étudemontre que le taux d’immunisation aussibien pour le vaccin antipoliomyélitique quepour le vaccin antirougeoleux chez les en-fants malnutris est plus faible en comparai-son avec les enfants dont l’état nutritionnelest normal. Pour le vaccin antipoliomyéli-tique, le taux de séroconversion pour letype 1 est de 94 % chez les enfants té-moins, alors que chez les enfants malades ilest de 40,5 %, la différence étant statis-tiquement très significative (p = 0,001).Pour le poliovirus type 2, la proportiond’enfants présentant des titres d’anticorps≥ 8 est de 97 % chez les enfants témoinscontre 59 % chez les enfants malades (p =0,001). Il n’en reste pas moins quel’immunité contre le poliovirus type 1
constitue un atout majeur dans la lutte con-tre la poliomyélite antérieure aiguë puisqu’ils’agit à la fois du type le plus fréquent et leplus pathogène. La même différence estnotée pour le poliovirus type 3 : 91 % pourles témoins contre 40,5 % pour les enfantssouffrant d’une malnutrition protéino-calorique (p = 0,001). Ces résultats sonttout à fait comparables à ceux rapportéspar d’autres auteurs, le poliovirus type 3étant connu pour sa faible immunogénicité[8].
En effet, les carences en protéines et enapport énergétique ont une influence di-recte sur l’immunité et plus particulière-ment sur la production d’anticorps qui sontdes glycoprotéines [4]. Ainsi l’absence deréponse immunitaire vaccinale, plus parti-culièrement dans les formes œdémateuses(kwashiorkor) où le taux d’immunisationest nul aussi bien pour le vaccin antipo-liomyélitique que pour le vaccin antirougeo-leux, trouve son explication dans le défautde protéosynthèse. Dans ces formes œdé-mateuses, la protidémie est très basse, elleatteint 38 g/L ; l’électrophorèse des frac-tions protéiques a révélé une hypoalbumi-némie (< 18 g/L) et une hypogammaglo-bulémie (< 3 g/L).
Dans la malnutrition protéino-énergé-tique, le système du complément, surtout lafraction C3, est déficiente et par con-séquent la production d’anticorps est dé-ficiente elle aussi. Cette déficience en pro-duction des anticorps aussi bien pour levaccin trivalent oral (VPOT) que pour levaccin antirougeoleux est beaucoup plusmarquée chez les cas de kwashiorkor et demarasme [9] ; ceci explique la susceptibi-lité sinon la confirmation d’une réinfectionpar la poliomyélite et par la rougeole chezles enfants souffrant de MPC.
D’autres facteurs peuvent expliquer lafaible réponse vaccinale antipoliomyéli-tique, comme les diarrhées chroniques et
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM478

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 479
l’interférence des entérovirus non po-liomyélitiques qui sévissent pendant la pé-riode sèche. Deux études ont permisd’illustrer le rôle de ces deux facteurs. Ain-si, une étude menée en Tunisie en 1997 sur121 enfants ayant reçu 3 doses du vaccinVPOT a montré que les taux de sérocon-version pour le poliovirus type 1, le poliovi-rus type 2 et le poliovirus type 3 sont de94,7 %, 100 % et 89,5 % respectivement.Le faible taux de séroconversion a été notésurtout pour le poliovirus 3 comparé à celuidu poliovirus 2 et du poliovirus 1. L’inter-férence virale avec les entérovirus a éténotée dans 50 % de la non-réponse à untype de poliovirus ou à un autre. L’étude amontré que la faible réponse vaccinale peutaussi être associée à d’autres facteurscomme la présence d’anticorps maternelset la malnutrition [10].
Une étude menée en Chine (province deGuangdong) a permis d’illustrer le rôle de lasaison de vaccination dans la séroconver-sion vaccinale antipoliomyélitique chez82 enfants vaccinés en été et 106 enfantsvaccinés en hiver. Le dosage des anticorpsa été testé avant et après vaccination. Letaux de séroconversion est de deux à septfois plus important en hiver qu’en été.L’interférence virale avec les entérovirusnon poliomyélitiques a été notée dans75,6 % et 38 % des cas en été et en hiverrespectivement ; ceci laisse apparaître quela fréquence des infections à entéroviruspendant la période sèche, période oùl’incidence de la malnutrition est à son pic,peut être la cause principale de l’échec de laréponse vaccinale antipoliomyélitique. Unesuggestion proposée par l’auteur de l’étudeest de donner une dose de vaccin supplé-mentaire en dehors de la période sèche,surtout chez les enfants à risque de malnu-trition [11]. Ceci donc laisse comprendreque l’infection par des virus autres que lepoliovirus pourra diminuer la réponse vac-
cinale vis-à-vis du vaccin contre la po-liomyélite, surtout chez les enfants à risquepour la malnutrition où l’infection pard’autres virus est plus fréquente [12].
La malnutrition et les maladies diar-rhéiques très fréquentes dans les pays endéveloppement sont les causes majeures del’échec vaccinal. Une étude similaire a étéréalisée en 1996 aux Philippines surl’évaluation de la réponse vaccinale vis-à-vis du vaccin poliomyélitique oral chez lesenfants dénutris suite à des diarrhées chro-niques. Les résultats montrent que le tauxd’immunisation chez les enfants est di-minué de 26 à 34 % en comparaison avec legroupe témoin (p < 0,002) [13]. En effet,les diarrhées fréquentes chez les enfantssouffrant de MPC peuvent expliquer lanon-fixation du virus dans la paroi intesti-nale, soit par un phénomène d’inférence vi-rale avec les anticorps en réponse au VPOT(l’adénovirus, l’entérovirus et le rotavirus),bactérienne ou parasitaire, soit en favo-risant une élimination trop rapide du virus[10,14].
Pour le vaccin antirougeoleux commepour le vaccin antipoliomyélitique, la séro-conversion vis-à-vis du virus de la rougeoleest bien plus diminuée dans le cas d’unedénutrition sévère. Ainsi, le taux d’immuni-sation chez les témoins est de 82,3 % (28/34) ; ce taux est abaissé à 35,1 % (13/37)chez les enfants malnutris (p = 0,001).
Une étude sur la réponse vaccinale vis-à-vis du vaccin vivant atténué de la rou-geole a été réalisée au Soudan chez35 enfants malnutris en comparaison avec35 enfants témoins dont l’état nutritionnelest normal. Un prélèvement sanguin a étéeffectué avant et après vaccination, et ledosage des anticorps a été réalisé par réac-tion d’inhibition d’hémagglutination. Letaux de séroconversion chez les enfantsmalnutris et les enfants témoins est de92 % et 96 % respectivement (p < 0,02) ;
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM479

480 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
le faible taux de séroconversion a été notéchez les cas de kwashiorkor [15].
La baisse de la réponse vaccinale est laconséquence d’un état nutritionnel défail-lant. Des études ont rapporté que le tauxd’immunisation ou de séroconversion vis-à-vis du virus de la rougeole est beaucoupplus abaissé chez les enfants malnutris [16]en comparaison avec les enfants dont l’étatnutritionnel est normal. Ainsi, une bonnecouverture vaccinale ne garantit pas unebonne immunité sérologique chez les en-fants souffrant de MPC.
La supplémentation en vitamine A chezles mères après l’accouchement et lesnouveau-nés pourra remédier à ceproblème et pourra augmenter la produc-tion des anticorps en réponse à la vaccina-tion. Une étude menée en Inde consistait àdonner de la vitamine A (60 mg de rétinol)aux mères ainsi qu’à leur bébé (7,5 mg) àchaque administration d’une dose de VPO.Cette supplémentation a amélioré le tauxd’immunisation vis-à-vis du vaccin de lapoliomyélite, surtout pour le poliovirus detype 3 [17].
Conclusion
Au vu de ces résultats qui démontrent lesfaibles taux de séroconversion vis-à-vis duvaccin poliomyélitique oral et du vaccin an-tirougeoleux chez les enfants malnutriscomparés à des enfants témoins, il nousparaît urgent de discuter d’une conduitepour améliorer l’état vaccinal de ces en-fants et de s’assurer que les taux satisfai-sants de couverture vaccinale (> 95 %pour la poliomyélite et 92 % pour la rou-geole à l’échelle nationale) permettrontd’atteindre les objectifs assignés, à savoir
l’éradication de la poliomyélite d’ici l’an2005 et l’élimination de la rougeole d’ici2010. Si la malnutrition protéino-caloriquea légèrement reculé ces dernières années auMaroc (de 28 % à 24 %), il n’en reste pasmoins que les cas de malnutrition que l’oncontinue à enregistrer constituent un obsta-cle qui ralentit, voire compromet, le succèsdes programmes d’éradication de la po-liomyélite et d’élimination de la rougeole.
L’évaluation de l’importance de la mal-nutrition protéino-calorique au Maroc per-mettrait de proposer une attitude adaptéepour prévenir ces échecs de la vaccination.L’impact de la supplémentation en vitamineA, qui est actuellement intégrée dans lesactivités du programme de vaccination, surla séroconversion vis-à-vis du VPO et duvaccin antirougeoleux chez les enfants mal-nutris doit être apprécié lorsque l’admi-nistration d’une dose supplémentaire devaccin antipoliomyélitique et antirougeo-leux, une fois la malnutrition protéino-calorique jugulée, pourrait être une alterna-tive pour prévenir ces échecs de vaccina-tion. Ceci suppose néanmoins qu’undépistage ciblé de la malnutrition protéino-calorique dans les régions à risque doit êtreentrepris, ce qui pourrait être d’une grandeimportance à la phase finale d’éradicationde la poliomyélite et d’élimination de la rou-geole.
Remerciements
Nous tenons à remercier tout le personneldu service de Pédiatrie III pour leur aideprécieuse. Nous tenons à remercier égale-ment nos collègues du laboratoire de virolo-gie de l’Institut national d’Hygiène à Rabat.
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:04 AM480

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 481
Références
1. Rice AL et al. Malnutrition as an underly-ing cause of childhood deaths associ-ated with infectious diseases in develo-ping countries. Bulletin of the WorldHealth Organization, 2000, 78(10):1207–21.
2. El Khaier A. Etude épidémiologiqueétiologique clinique évolutive et théra-peutique des malnutritions protéino-caloriques de l’enfant. Thèse n° 376 ;1987
3. Bhaskaram P. Nutritional modulation ofimmunity to infection. Indian journal ofpathology and microbiology, 1992,35(4):392–40.
4. Pastoret PP. Nutrition et réponse im-mune. In : Pastoret PP, Govaerts A, BazinH. Immunologie animale. Paris, Flamma-rion Médecine Sciences, 1990.
5. Bhaskaram P. Measles and malnutrition.Indian journal of medical research,1995, 102:195–9
6. Powell GM. Response to live attenuatedmeasles vaccine in children with severekwashiorkor. Annals of tropical paedia-trics, 1982, 2(3):143–5.
7. Chandra RK. Reduced secretoryantibody response to live attenuatedmeasles and poliovirus vaccines in mal-nourished children. British medical jour-nal, 1975, 2(5971):583–5.
8. Jody R et al. Sabin inactivated trivalentpoliovirus vaccine : first clinical trial andseroimmunity survey. Pediatric infectiousdiseases journal, 1988, 7:760–5.
9. Hafez M et al. Antibody production andcomplement system in protein energymalnutrition. Journal of tropical medicineand hygiene, 1977, 80(2):36–9
10. Triki H, Abdallah MV, Ben Aissa R. Influ-ence of host related factors on the anti-
body response to trivalent oral polio vac-cine in Tunisian infants. Vaccine, 1997,15(10):1123–9.
11. Wu CM, Zheng HY, Ren YL. [Immune in-terference of enteroviruses to immuneresponse of TOPV in subtropical areas.]Zhonghua liu xing bing Xne za zhi, 1996,17(4): 233–5 [In Chinese].
12. Faden H, Duffy L. Effect of concurrent vi-ral infection on systemic and local anti-body response to live attenuated andenhanced-potency inactivated poliovi-rus vaccines. American journal ofdiseases of children, 1992, 146(11):1320–3
13. Yoon PW, Black RE, Moulton LH. The ef-fect of malnutrition on the risk of diar-rheal and respiratory mortality inchildren < 2 years of age in Cebu, Philip-pines. American journal of clinical nutri-tion, 1997, 65(4):1070–7.
14. Myaux JA et al. Effect of diarrhea on thehumoral response to oral polio vaccina-tion. Pediatric infectious diseases jour-nal, 1996, 15(3):204–9.
15. Idriss S, El Seed AM. Measles vaccina-tion in severely malnourished Sudanesechildren. Annals of tropical pediatrics,1983, 3(2):6–7.
16. Halsey NA et al. Response to measlesvaccine in Haitian infants 6 to 12 monthsold. Influence of maternal antibodies,malnutrition and concurrent illnesses.New England journal of medicine, 1985,313(9):544–9.
17. Bahl R et al. Effect of vitamin A adminis-tered at Expanded Programme on Immu-nization contacts on antibody responseto oral polio vaccine. European journalof clinical nutrition, 2002, 56(4):321–5.
02 Evaluation de la rÈponse.pmd 8/17/2005, 11:05 AM481

482 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Detection of pneumonia amongchildren under six years by clinicalevaluationH. Shamo’on,1 A. Hawamdah,1 R. Haddadin1 and S. Jmeian 2
1Department of Paediatrics; 2Ear, Nose and Throat Department, Queen Alia Military Hospital, RoyalMedical Services, Amman, Jordan.Received: 09/12/03; accepted: 17/03/04
ABSTRACT To determine the most useful clinical symptoms and signs for detection of pneumonia in children,we carried out a prospective clinical study at Queen Alia Hospital, Amman, on 147 children admitted betweenAugust 2002 and January 2003 with clinical pneumonia. All the children had chest X-rays, which were readby the same radiologist. The most sensitive and specific signs and symptoms for prediction of pneumoniawere coughing, tachypnoea (respiratory rate > 50/min) and chest wall indrawing. We found that presence oftachypnoea and lower chest wall indrawing can detect most cases of pneumonia. If all clinical signs arenegative, chest X-ray findings are unlikely to be positive.
Dépistage de la pneumonie chez des enfants de moins de six ans par évaluation cliniqueRÉSUMÉ Afin de déterminer les symptômes et les signes cliniques les plus utiles pour le dépistage de lapneumonie chez l’enfant, nous avons réalisé une étude clinique prospective à l’hôpital Reine Alia d’Ammanchez 147 enfants hospitalisés entre août 2002 et janvier 2003 pour un épisode de pneumonie avec diagnos-tic clinique. Tous les enfants ont eu des radiographies pulmonaires interprétées par le même radiologue. Latoux, la tachypnée (rythme respiratoire > 50/min) et le tirage respiratoire étaient les signes et les symptômesles plus sensibles et les plus spécifiques pour prédire une pneumonie. Nous avons trouvé que la présencede tachypnée et d’un tirage sous-sternal permet de dépister la plupart des cas de pneumonie. Si tous lessignes cliniques sont négatifs, il est peu probable que les résultats de la radiographie pulmonaire soientpositifs.
03 Detection of pneumonia.pmd 8/17/2005, 11:05 AM482

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 483
Introduction
Acute lower respiratory tract illness(ALRI) is common among children seen inprimary care [1], and accounts for slightlyless than 50% of deaths in children under 1year and about 20% of deaths in all hospi-talized children under 15 years [2].
The physical differences between thechests of children and adults account forsome of the differences in physical signs[3]. Small children find it difficult to takelarge breaths, so crackles and wheezeswhich may be expected only during such amanoeuvre will not be heard. In ALRI,when the history and physical examinationsuggest the same diagnosis, chest radiogra-phy is rarely necessary; when the 2 are in-consistent, then a radiograph may behelpful [4]. The identification of signs suchas rapid breathing and chest retraction isvery important in deciding who needs ex-pensive treatment and who does not [5].Also important is the decision to refer achild to hospital, which may be many milesaway for many people living in rural areasin developing countries.
Our aim was to emphasize the impor-tance of using simple clinical signs such asrespiratory rate and chest wall indrawing indetecting ALRI, especially pneumonia, inchildren.
Methods
We did a prospective clinical observationstudy at Queen Alia Military Hospital, Am-man, Jordan over a 6-month period (Au-gust 2002–January 2003) for all childrenbelow 6 years of age admitted with clinicalpneumonia (most cases admitted were be-low this age). All patients were admitted viathe outpatient clinic at Marqa, which isabout 20 km from the hospital. This clinicsees patients from areas surrounding Am-
man (suburban areas) but does not alwayshave radiology facilities available. The pae-diatrician admitted all cases on a clinicalbasis according to World Health Organiza-tion criteria: cough with tachypnoea (respi-ratory rate > 50/min in infants or > 40/minin older children), indrawing or wheezing.The respiratory rate was counted for a fullminute after lowering the temperature (us-ing cold compresses or paracetamol) to< 38 °C rectally or 37.5 °C axillary and be-fore the routine extraction of blood.
All children admitted were examined bya specialist in paediatrics and the same ear,nose and throat specialist to exclude severeupper respiratory tract infection and all hadchest X-rays which were assessed by thesame radiologist. No clinical findings werewritten on the X-ray request.
Exclusion criteria from the study werechildren with immune deficiency, thoseknown to have asthma, history of foreignbody aspiration or chemical pneumonitis,children with failure to thrive and malnutri-tion, and children with severe upper res-piratory tract infection. Malnourished chil-dren were excluded because tachypnoeaand lower chest wall indrawing are not suf-ficiently sensitive as predictors of pneumo-nia in these children [6].
The 147 patients in our study were di-vided into 2 groups according to the chestX-ray findings: those having lobar pneumo-nia or bronchopneumonia in 1 or morelobes, and those having normal or hyperin-flated chest X-rays. The clinical signs andsymptoms of the 2 groups were analysedand compared with the radiological evi-dence of pneumonia (gold standard) andtheir sensitivity and specificity calculated.
Results
Our study included 147 children admittedwith clinical pneumonia, 72 (49%) male
03 Detection of pneumonia.pmd 8/17/2005, 11:05 AM483

484 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
and 75 (51%) female. The ages of the chil-dren were: 1–12 months 92 (63%), 13–36months 47 (32%) and 37–72 months 8(5%). Mean duration of admission was 5days for the first and second age groupsand 2 days for the third age group.
From the chest X-ray findings, 40 chil-dren (27%) had lobar pneumonia in 1 or 2lobes and 50 children (34%) had broncho-pneumonia, a total of 90 children (61%)with pneumonia diagnosed on a radiologicalbasis. Fifty-seven children (39%) had nor-mal or hyperinflated chest X-rays. A familyhistory of bronchial asthma or allergy wasdiscovered in 15 children (10%).
Table 1 shows the overall frequency ofsymptoms and signs of pneumonia and Ta-ble 2 shows their sensitivity and specificitycompared with radiology results (goldstandard). Cough, fever, tachypnoea andchest indrawing were the most frequentlyobserved signs and symptoms, while tac-hypnoea was both the most sensitive(99%) and most specific (88%) sign ofpneumonia and cough the most sensitive(98%) symptom. Most of the children(146) received antibiotics; 2 patients need-ed a respirator (1 developed pneumotho-
rax) and 3 had pleural effusion. There wereno deaths.
Discussion
In developing countries, the case fatalityrate from ALRI in children could to be re-duced if the most serious forms of ALRIwere identified and dealt with appropriately.
Our study showed that the most sensi-tive symptom was cough 98%, with 70%specificity. The most sensitive signs in de-creasing order were: tachypnoea (99%),chest wall indrawing (88%), and fever(78%), while the most specific were tachy-pnoea (88%) followed by chest wall in-drawing (77%).
Anadol found that tachypnoea had aspecificity of 99% and a sensitivity of 61%and was the most important sign in diag-nosing pneumonia [7]. Another studyshowed that the best screen for pneumoniawas the presence of fever along withtachypnoea [8]. A study done in Chinashowed that tachypnoea was more reliablethan auscultation in predicting pneumonia[9].
Most of our children were infants, so inour study clinical signs appear to predictpneumonia in infants more reliably than inolder children. A study done by Redd et al.comparing the clinical and radiological di-agnosis of pneumonia found that childrenwith a radiographic diagnosis tended tohave been ill longer and to be older becausemothers may have tended to take febrilechildren with mild ALRI to the health centreor hospital more often than non-febrile chil-dren with mild ALRI [10]. In the absenceof respiratory signs, febrile infants are un-likely to have abnormal chest radiography[11,12].
Wheezing was found in 33% of the chil-dren in our study and was not a useful sign
Table 1 Frequency of symptoms and signs inchildren with pneumonia (n = 147)
Clinical sign or symptom No. %
Cough 105 71
Fever 103 70
Tachypnoea 96 65
Chest indrawing 92 63
Poor feeding 79 54
Grunting 79 54
Diminished air entry 58 40
Crepitation 52 35
Wheezes 49 33
03 Detection of pneumonia.pmd 8/17/2005, 11:05 AM484

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 485
for determining pneumonia in children.This is in agreement with a study done byMahabee-Gittens et al., who found that inwheezy infants and toddlers, gruntingalong with oxygen saturation is highly spe-cific and can be used to help diagnosepneumonia in wheezing infants and tod-dlers [13].
We did not differentiate ALRI frombronchial asthma so it is possible that chil-dren were overtreated for ALRI and under-treated for asthma. In regions wherewheezing illness is prevalent, the specifici-ty of the World Health Organization pneu-monia algorithm is reduced and this maylead to unnecessary use of antibiotics orunderutilization of bronchodilators [14].Simple physical signs that require minimalexpertise to recognize can be used to deter-mine oxygen therapy and to aid in screen-ing for referral [15–17].
There may be poor agreement, evenamong experienced physicians, on thepresence of rales in young children, and
this was the case in our study. Subcostal orintercostal recessions (difficulty in breath-ing) are generally more often seen in infantsthan in older children because the chestwall is more compliant than that of the old-er child.
The most useful single factor for rulingout pneumonia in an infant is the absence oftachypnoea [18]. We found that tachyp-noea and chest wall indrawing in the pres-ence of cough can help the clinician todetermine the need for chest radiography inthe paediatric emergency clinic. A studydone in Brazil showed that the clinicalsymptoms taken together contribute morethan the signs and are on a par with X-rayin importance [19]. Another study foundthat age-specific respiratory rate (recom-mended by the World Health Organization,with or without chest wall indrawing) is asensitive and specific indicator of pneumo-nia in almost all age groups [20]. Carefulattention to specific clinical factors and useof adjunct radiographs and laboratory tests
Table 2 Sensitivity and specificity of clinical symptoms and signs atpresentation for predicting pneumonia
Clinical sign or Chest X-ray Sensitivity Specificitysymptom Pneumonia Normal or (%) (%)
detected hyperinflated(n = 90) (n = 57)
No. positive for No. positive forsymptom/sign symptom/sign
Tachypnoea 89 7 99 88
Cough 88 17 98 70
Chest indrawing 79 13 88 77
Fever 70 33 78 42
Poor feeding 52 27 58 53
Grunting 52 27 58 53
Diminished air entry 30 28 33 51
Crepitation 27 25 30 56
Wheezes 20 29 22 49
03 Detection of pneumonia.pmd 8/17/2005, 11:05 AM485

486 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
should guide physicians in selection of anti-biotics and decisions regarding hospitaliza-tion [21].
The employment of simple clinical cri-teria gives a good indication of pneumoniaand can decrease unnecessary referral andadmissions to hospital and thus result incost-savings.
Most of the children in our study re-ceived antibiotics, which appear to be usedin a high percentage of cases, even if inap-propriate for the condition, because theseclinical signs do not distinguish viral frombacterial pneumonia, nor do chest X-ray,temperature measurement or duration offever [22].
Our study justifies the premise thatpneumonia case detection does not requireauscultation, chest X-ray or laboratorytesting, and that observation of the respira-tory rate and lower chest wall indrawingare the key elements of assessment inyoung children.
Conclusions
Initial observation of the infant may be themost critical component for the diagnosisof pneumonia.
Tachypnoea is the most valuable of theindividual clinical signs for prediction ofradiological pneumonia and can be a sensi-tive and reasonably specific indicator ofrespiratory infection.
The absence of tachypnoea and chestwall indrawing can safely be used to reducethe number of chest X-rays ordered forchildren under investigation. These find-ings have relevance for assessment proto-cols and resulting treatment decisionswhen chest X-ray is not routinely available.
These methods for pneumonia case de-tection could be taught to primary carephysicians, nurses and even mothers, al-lowing them to seek medical advice early.This would lead to a decrease in the pneu-monia mortality rate in children.
References
1. Margolis P, Gadomski A. Does this infanthave pneumonia? Journal of the Ameri-can Medical Association, 1998, 279(4):308–13.
2. Larsen GL et al. Respiratory tract andmediastinum. In: Hay WW et al., eds. Cur-rent pediatric diagnosis and treatment,13th ed. Stamford City, Appleton &Lange, 1997:420–74.
3. Helms P, Henderson J, eds. Respiratorydisorders. In: Campbell AGM, McIntoshN, eds. Forfar and Arneil’s textbook ofpediatrics, 5th ed. London, ChurchillLivingstone, 1998, 12:489–583.
4. Alario AJ et al. Usefulness of chest radio-graphs in children with acute lowerrespiratory tract disease. Journal of pedi-atrics, 1987, 111(2):187–93.
5. Cherian T et al. Evaluation of simpleclinical signs for the diagnosis of acutelower respiratory tract infections. Lancet,1988, 2(8603):125–8.
6. Falade AG et al. Use of simple clinicalsigns to predict pneumonia in youngGambian children: the influence of mal-nutrition. Bulletin of the World Health Or-ganization, 1995, 73(3):299–304.
7. Anadol D, Aydin YZ, Gocmen A. Over-diagnosis of pneumonia in children.Turkish journal of pediatrics, 43(3):205–9.
8. Zukin DD et al. Correlation of pulmonarysigns and symptoms with chest radio-graphs in the pediatric age group.Annals of emergency medicine, 1986,15(7):792–6.
03 Detection of pneumonia.pmd 8/17/2005, 11:05 AM486

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 487
9. Dai Y et al. Respiratory rate and signs inroentgenographically confirmed pneu-monia among children in China. Pediat-ric infectious disease journal, 1995, 14(1):48–50.
10. Redd SC et al. Comparison of the clinicaland radiographic diagnosis of paediatricpneumonia. Transactions of the RoyalSociety of Tropical Medicine and Hy-giene, 1994, 88(3):307–10.
11. Crain EF et al. Is a chest radiograph nec-essary in the evaluation of every febrileinfant less than 8 weeks of age? Pediat-rics, 1991, 88(4):821–4.
12. Taylor JA et al. Establishing clinically rel-evant standards for tachypnea in febrilechildren younger than 2 years. Archivesof pediatrics & adolescent medicine,1995, 149(3):283–7.
13. Mahabee-Gittens EM et al. Clinical fac-tors associated with focal infiltrates inwheezing infants and toddlers. Clinicalpediatrics, 2000, 39(7):387–93.
14. Nascimento-Carvalho CM et al. Child-hood pneumonia: clinical aspects asso-ciated with hospitalization or death.Brazilian journal of infectious diseases,2002, 6(1):22–8.
15. Margolis PA et al. Accuracy of the clinicalexamination in detecting hypoxemia ininfants with respiratory illness. Journal ofpediatrics, 1994, 124(4):552–60.
16. Usen S et al. Clinical predictors ofhypoxaemia in Gambian children withacute lower respiratory tract infection:prospective cohort study. British medicaljournal, 1999, 318(7176):86–91.
17. Weber MW et al. Predictors of hypo-xaemia in hospital admission with acutelower respiratory tract infection in a de-veloping country. Archives of disease inchildhood, 1997, 76(4):310–4.
18. Bloomfield D. Tachypnea. Pediatrics inreview, 2002, 23(8):294–5.
19. Pereira JC, Escuder MM. The importanceof clinical symptoms and signs in the di-agnosis of community-acquired pneu-monia. Journal of tropical pediatrics,1998, 44(1):18–24.
20. Singhi S et al. Validity of clinical signs forthe identification of pneumonia in chil-dren. Annals of tropical paediatrics,1994, 14(1):53–8.
21. Lichenstein R, Suggs AH, Campbell J.Pediatric pneumonia. Emergency medi-cine clinics of North America, 2003,21(2):437–51.
22. Korppi M et al. Comparison of radiologi-cal findings and microbial aetiology ofchildhood pneumonia. Acta paediatrica,1993, 82(4):360–3.
03 Detection of pneumonia.pmd 8/17/2005, 11:05 AM487

488 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Group A streptococci in children withacute pharyngitis in Sousse, TunisiaR. Mzoughi,1 O. Bouallègue,1 H. Selmi,2 H. Ben Said,3 A.S. Essoussi2 and M. Jeddi1
1Microbiology Laboratory; 2Paediatric Service, Farhat Hached Hospital, Sousse, Tunisia.3Centre de Protection Maternelle et Infantile (Centre PMI), Erriadh, Sousse, Tunisia.Received: 16/01/03; accepted: 07/10/03
ABSTRACT A 1-year prospective study in 2 paediatric outpatient clinics in Sousse, Tunisia, aimed todetermine the presence of group A streptococci in acute pharyngitis cases and carriers, and the distributionof the serotypes and biotypes. Group A streptococci were found in 9.0% of throat swabs from 155 controlsand 17.7% from 474 patients (P < 0.05). Of 43 strains isolated from patients and submitted for typing, 15different types were identified, the most common being M75 (14 strains; 32.5%), M9 (6 strains; 14.0%), M76(5 strains; 11.6%) and M12 (4 strains; 9.3%). Three strains were non-typeable (7.0%). Biotyping of thestrains showed 3 predominant biotypes: biotype 3 (n = 14), biotype 2 (n = 11), and biotype 1 (n = 7).
Les streptocoques du groupe A chez des enfants atteints de pharyngite aiguë à Sousse (Tunisie)RÉSUMÉ Une étude prospective sur un an réalisée dans deux services de consultations externespédiatriques à Sousse (Tunisie) avait pour objectif de déterminer la présence de streptocoques du groupeA dans les cas de pharyngite aiguë et chez les porteurs, ainsi que la répartition des sérotypes et biotypes.On a trouvé des streptocoques du groupe A dans 9,0 % des prélèvements de gorge de 155 sujets témoinset chez 17,7 % des 474 patients (p < 0,05). Parmi les 43 souches isolées chez les patients et soumises autypage, 15 types différents ont été identifiés, les plus courants étant M75 (14 souches ; 32,5 %), M9(6 souches ; 14,0 %), M76 (5 souches ; 11,6 %) et M12 (4 souches ; 9,3 %). Trois souches étaient nontypables (7,0 %). Le biotypage des souches a montré trois biotypes prédominants : le biotype 3 (n = 14), lebiotype 2 (n = 11) et le biotype 1 (n = 7).
04 Group A streptococci.pmd 8/17/2005, 11:05 AM488

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 489
Introduction
Streptococcus pyogenes (group A strepto-coccus) is still the most frequent cause ofpharyngitis in children and can lead to se-vere post-infection sequelae includingrheumatic fever and glomerulonephritis[1]. The incidence of rheumatic fever hasdeclined rapidly in developed countrieswhere improved living conditions and sys-tematic antibiotic therapy with penicillinhave limited the spread of bacterial strainsin the population [2–4]. However, unex-pected outbreaks of rheumatic fever haveoccurred in the United States of America[5]. The changing epidemiology of group Astreptococci and rheumatic fever is said tobe related to changes in the distribution ofserotypes [6,7], where certain virulent Mtypes have been associated with invasivedisease [5,8–10]. Thus, it is important toestablish the epidemiological patterns ofgroup A streptococci in different countriesand regions, and especially to serotype thestrains that have been isolated. This knowl-edge will be important for the developmentand use of vaccines [11].
In Tunisia, rheumatic fever remains animportant health problem in children, withan incidence of 57 cases per 100 000 in-habitants in 2001 [12]. As a part of the na-tional effort to clarify the epidemiologicalpattern of group A streptococci in ourcountry the present study was conductedto determine the presence of group A strep-tococci in acute pharyngitis cases and incarriers in the city of Sousse, and the dis-tribution of serotypes and biotypes.
Methods
A 1-year prospective study, between 1 Oc-tober 1994 and 20 September 1995, wasconducted in 2 paediatric outpatient clinics
in Sousse: Farhat Hached Hospital andCentre de Protection Maternelle et Infantile(Centre PMI) Erriadh. Samples were col-lected from patients with acute pharyngitis,diagnosed on the basis of fever over 38 °C,sore throat, pharyngeal exudates and acuteinflammatory tonsillitis.
A total of 474 patients, age 2 to 8 years,living in a populous district around Soussewere monitored by 3 general practitionersand 1 paediatrician. Samples were also col-lected from 155 healthy paediatric patientswho were attending for vaccination. Aswab was applied over both tonsils and theposterior pharynx and was transferred tothe Microbiology Laboratory of FarhatHached Hospital as soon as possible (2 to 3hours after sampling). Samples were col-lected from patients before any antibiotictherapy.
All swabs were inoculated onto 5%horse blood agar plates, with nalidixic acidand colistin and incubated in a CO2-en-riched atmosphere for 24 hours at 37 °C.The cultures negative for beta-haemolyticstreptococci were incubated during 24hours under the same conditions. The pos-itive beta-haemolytic colonies were isolatedand applied to a 0.04 U bacitracin disk, thehalo was measured and the strains wereidentified by latex agglutination (Strepto-kit, bioMérieux, France). Forty-three (43)strains of group A streptococci isolatedfrom the patients were serotyped by stan-dard methods [13] at the Institut Für Ex-perimentelle Mikrobiologie, Jena, Germany.The biotypes were determined with a com-mercially available identification system(rapid ID 32 STREP, bioMérieux, France),using the classification of Bouvet et al.[14].
Statistical analysis was carried outusing chi-squared tests.
04 Group A streptococci.pmd 8/17/2005, 11:05 AM489

490 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Results
Streptococcal strains were found in 12.9%of the controls and 20.7% of the patients.Group A streptococci had a frequency of9.0% and 17.7% in the controls and thepatients respectively (significant differ-ence, P < 0.05) (Table 1).
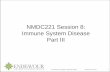
The isolation rates of group A strepto-cocci peaked twice during the year fromOctober to December and in June (Figure1).
Of the 43 strains analysed, 93.0% weretypeable. Fifteen different types were iden-tified, the most common being M75(32.5% of strains), M9 (14.0%), M76(11.6%), and M12 (9.3%) (Figure 2). Theremaining serotypes (< 3% each) were:M1, M14, M25, M2, M3, M11, M28, M8and M49. Only 3 strains (7.0%) were non-typeable.
Three biotypes were predominant: bio-type 3, biotype 2 and biotype 1 (Table 2).
Table 1 Throat swab culture results in patients with acute pharyngitis andhealthy controls
Patient group No. of Group A Group C, G, F Positive culturepatients streptococci streptococci
No. of % No. of % No. of %strains strains strains
Acute pharyngitis 474 84 17.7 14 3.0 98 20.7
Controls (carrier state) 155 14 9.0 6 3.9 20 12.9
Figure 1 Monthly isolation rates of group A streptococci in patients with pharyngitis
04 Group A streptococci.pmd 8/17/2005, 11:05 AM490

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 491
Discussion
Little is known about the group A strepto-cocci serotypes circulating in the Maghrebarea and North Africa. To the best of ourknowledge, the present study is the firstTunisian report of the serotypes of group Astreptococci isolated from children withpharyngitis.
M serotyping might not adequately re-flect the clonal diversity of bacterialstrains, as suggested by the finding that
isolates expressing the same M serotypecan be distinguished by genetic methods[15–17]. Our results suggest that strepto-coccal pharyngitis is caused by a wide vari-ety of strains, although 4 serotypespredominated (M75, M9, M76 and M12).Continued study may help define the epide-miology of group A streptococci in Tunisia.
Most isolates of group A streptococcidescribed in developing countries, especial-ly in the Middle East region, are untypeable[7,18]. Among typeable strains, M type 1 isusually one of the predominant serotypes,as it was reported in Kuwait [7], IslamicRepublic of Iran [18], and the United ArabEmirates [19].
In contrast, the high rate of typeableisolates in our study (93.0%) suggests thatgroup A streptococci strains in our city aresimilar but not necessarily related to thosecommonly found in Europe and NorthAmerica. Furthermore, our findings high-light the low rate (< 3%) of M type 1,which has been associated with seriousdiseases such as rheumatic fever, a recog-nized problem in Tunisia, and toxic shocksyndrome [9,20], which has not yet beenreported from our area.
Although the number of isolates wasnot sufficient to make any epidemiologicalconclusions, this data could be useful forfurther understanding the epidemiology ofgroup A streptococcal infections, and forthe development and use of a vaccine.
Acknowledgements
This work was supported by the TunisianMinistry of Scientific Research. We thankDrs E. Günther and E. Straube (Institut Fürexperimentelle Mikrobiologie, Jena, Ger-many) for their help in serotyping thestrains.
Table 2 Biotype distribution of group Astreptococci associated with acutepharyngitis (n = 43 strains)
Biotype 1 2 3 4 5 8 10
No. of strains 7 11 14 5 4 1 1
Figure 2 Distribution of M types of group Astreptococci associated with acutepharyngitis (n = 43 strains)
04 Group A streptococci.pmd 8/17/2005, 11:05 AM491

492 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
References
1. Bisno AL. Group streptococcal infectionsand acute rheumatic fever. New Englandjournal of medicine, 1991, 325:783–93.
2. Bach JF et al. 10-year educationalprogramme aimed at rheumatic fever intwo French Caribbean islands. Lancet,1996, 347:644–8.
3. Markowitz M, Gerber MA, Kaplan EL.Treatment of streptococcal pharyngoton-sillitis: reports of penicillin’s demise arepremature. Journal of pediatrics, 1993,123:679–85.
4. Massel BF et al. Penicillin and themarked decrease in morbidity and mor-tality from rheumatic fever in the UnitedStates. New England journal of medi-cine, 1988, 318:280–6.
5. Veasy LG et al. Resurgence of acuterheumatic fever in the intermountainarea of the United States. New Englandjournal of medicine, 1987, 316:421–7.
6. Kaplan EL, Wotton JT, Johnson DR. Dy-namic epidemiology of group A strepto-coccal serotypes associated withpharyngitis. Lancet, 2002, 358:1334–7.
7. Majeed HA et al. The concurrent asso-ciations of group A streptococcal sero-types in children with acute rheumaticfever or pharyngitis-associated glom-erulonephritis and their families in Ku-wait. Zentralblatt für Bakteriologie,Mikrobiologie, und Hygiene. Series A,1986, 262:346–56.
8. Bryant AE, Hayes-Schroer SM, StevensDL. M type 1 and 3 group A streptococcistimulate tissue factor-mediated pro-coagulant activity in human monocytesand endothelial cells. Infection and im-munity, 2003, 71:1903–10.
9. Schwartz B, Facklam RR, Breiman RF.Changing epidemiology of group Astreptococcal infection in the USA. Lan-cet, 1990, 336:1167–71.
10. Stollerman GH. Rheumatic group Astreptococci and the return of rheumaticfever. Archives of internal medicine,1990, 35:1–26.
11. Olive C et al. Protection of mice fromGroup A streptococcal infection by intra-nasal immunisation with a peptide vac-cine that contains a conserved M proteinB cell epitope and lacks a T cell epitope.Vaccine, 2002, 20:2816–25.
12. Bulletin épidémiologique. Direction dessoins de santé de base. Tunis, Ministèrede la Santé Publique, 2001.
13. Johnson DR et al. Laboratory diagnosisof group A streptococcal infections.Geneva, World Health Organization,1997.
14. Bouvet A et al. Restricted associationbetween biotypes and serotypes withingroup A streptococci. Journal of clinicalmicrobiology, 1994, 32:1312–7.
15. Muotiala A et al. Molecular comparisonof group A streptococci of T1M1 serotypefrom invasive and non invasive infec-tions in Finland. Journal of infectious dis-eases, 1997, 175:392–9.
16. Nguyen L et al. Molecular epidemiologyof streptococcus pyogenes in an areawhere acute pharyngotonsillitis is en-demic. Journal of clinical microbiology,1997, 35:2111–4.
17. Murase T et al. Characteristics of Strepto-coccus pyogenes serotype M1 and M3isolates from patients in Japan from1981 to 1997. Journal of clinical microbi-ology, 1999, 37:4131–34.
18. Fazeli MR et al. Group A streptococcalserotypes isolated from healthy schoolchildren in Iran. European journal ofclinical microbiology and infectious dis-eases, 2003, 22:475–8.
04 Group A streptococci.pmd 8/17/2005, 11:05 AM492

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 493
19. Ameen AS et al. Serotypes of group Astreptococci isolated from healthyschoolchildren in the United Arab Emir-ates. Bulletin of the World Health Organi-zation, 1997, 75(4):355–9.
20. Johnson DR, Stevens DL, Kaplan EL.Epidemiologic analysis of group A strep-
tococcal serotypes associated with se-vere systemic infections, rheumatic fe-ver, or uncomplicated pharyngitis.Journal of infectious diseases, 1992,166:374–82.
Active tuberculosis among Iraqi schoolchildren with positive skin tests and their householdcontacts. W. Al Kubaisy, A. Al Dulayme and D.S. Hashim. Eastern Mediterranean Health Journal,2003, Vol. 9 No. 4, pages 675–88.The authors’ names in Arabic should read:
The affiliation of Professor Al Kubaisy should read: College of Medicine, Al Nahrain University, Baghdad,Iraq.
CorrectionKnowledge, attitudes and practices survey among health care workers and tuberculosis patients inIraq. D.S. Hashim, W. Al Kubaisy and A. Al Dulayme. Eastern Mediterranean Health Journal, 2003,Vol. 9 No. 4, pages 718–31.The authors’ names in Arabic should read:
The affiliation of Professor Al Kubaisy should read: College of Medicine, Al Nahrain University, Baghdad,Iraq.
04 Group A streptococci.pmd 8/17/2005, 11:05 AM493

494 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Cryptosporidiosis in children in anorth Jordanian paediatric hospitalE.S. Mahgoub,1 A. Almahbashi2 and B. Abdulatif3
1Department of Microbiology, Faculty of Medicine; 2Faculty of Applied Medical Science; 3Faculty ofVeterinary Science, Jordan University of Science and Technology, Irbid, Jordan.Received: 27/10/02; accepted: 14/09/03
ABSTRACT We investigated the rate of infection by Cryptosporidium parvum among children from birth to 12years attending Princess Rahma Teaching Hospital in Irbid, Jordan and evaluated various diagnostic meth-ods. We collected single stool specimens from 300 children; 7 specimens were from children undergoingchemotherapy treatment for cancer. Diagnostic methods used for detection of infection were direct wetmount preparation, flotation concentration, cold Kinyoun Ziehl–Neelsen stain and direct immunofluores-cence. We detected C. parvum oocysts in 112 samples (37.3%) using direct immunofluorescence, whichshowed the highest sensitivity. Source of drinking water appeared to be an important risk factor for transmis-sion of infection. A higher incidence of infection was recorded during January–May, the rainy season.
La cryptosporidiose chez l’enfant dans un hôpital pédiatrique du nord de la JordanieRÉSUMÉ Nous avons étudié le taux d’infection par Cryptosporidium parvum chez des enfants de la nais-sance à l’âge de 12 ans consultant à l’hôpital universitaire Princesse Rahma d’Irbid (Jordanie) et évaluédiverses méthodes diagnostiques. Nous avons recueilli un échantillon unique de selles chez 300 enfants ;7 échantillons provenaient d’enfants sous chimiothérapie anticancéreuse. Les méthodes de diagnostic uti-lisées pour le dépistage de l’infection était l’examen direct de préparation à l’état frais, la concentration parflottation, la coloration de Ziehl-Neelsen, la coloration de Kinyoun à froid et l’immunofluorescence directe.Nous avons détecté des oocystes de C. parvum dans 112 échantillons (37,3 %) par immunofluorescencedirecte, méthode qui a montré la plus forte sensibilité. La source d’eau de boisson semblait être un importantfacteur de risque de transmission de l’infection. Une incidence plus élevée de l’infection a été enregistréeentre janvier et mai, la saison des pluies.
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM494

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 495
Introduction
Cryptosporidium parvum is a coccidianprotozoan parasite found in the brush-border of the enterocytes of the small intes-tine in many vertebrates, including humans[1]. Cryptosporidiosis is recognized as acause of diarrhoeal illness in man and sev-eral mammalian species [2]. The first casesof human cryptosporidiosis were reportedin 1976, and there are increasing numbersof reports of patients with documented in-fection with C. parvum. It is now consid-ered a common enteric pathogen in humansand domestic animals worldwide [3]. Cry-ptosporidiosis can induce self-limiting diar-rhoea in immunocompetent people orsevere and prolonged diarrhoea in immuno-compromised patients, such as those withAIDS, transplant recipients, those receiv-ing chemotherapy for cancer, institutional-ized patients, and patients with immuno-suppressive infectious disease [4].
A study in the same area of Jordan in1994 reported that the rate of infectionamong elementary-school children was 7%[5].
Diagnosis of the infection generally re-quires the observation of the infective stage(oocysts 4–6 µm). Owing to the small sizeof the oocysts, the routine wet mount prep-aration and concentration methods havelimited value for detection of C. parvum infaecal samples, where oocysts can easilybe confused with other materials present inthe sample [6].
We conducted this study because of theincreasing international documentation ofinfection by C. parvum and the fact that itis under-diagnosed in most Jordanian hos-pital laboratories. We also wanted to com-pare the different methods used for thediagnosis of C. parvum including the directimmunofluorescence test which was usedfor the first time in Jordan in this study. In
addition, we tried to focus on some epide-miological factors that lead to infection inchildren.
Methods
PatientsOver a period of 11 months, 300 singlestool specimens were collected from chil-dren attending outpatient clinics as well asinpatients in Princess Rahma TeachingHospital. Requests for stool examinationswere made by paediatricians who deemed itnecessary for diagnosis and follow-up oftheir patients. Princess Rahma TeachingHospital is the hospital for medical care ofchildren under 12 years of age. Faecal sam-ples were taken from children with diar-rhoea who were sent to the laboratory forinvestigation. Seven of the children wereundergoing chemotherapy for cancer.There were no exclusion criteria.
The purpose of the study was verballyexplained to the parents who agreed to givesamples from their children. Paeditriciansfilled in the clinical information andsupplied data on drugs as well as chemo-therapeutic agents used for treatment. Ad-ditional information about the children wasobtained by means of a questionnaire filledin with the assistance of the parents. Infor-mation requested included name, age, sexand residence (urban/rural). The source ofdrinking water was also ascertained (well,spring, tap, filtered, boiled). Parents werealso asked whether they kept animals in thehome.
Laboratory testsStool specimens were collected in the labo-ratory facilities at Princess Rahma Teach-ing Hospital and transported in a cool boxto the laboratory in the Department of Mi-crobiology at Jordan University of Science
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM495

496 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
and Technology in Irbid. Each sample,whether liquid, semi-solid or formed, wasdivided in 4 aliquots and processed accord-ing to each of the 4 methods describedhere. In all methods used, a positive slidewas read by at least 2 of the investigators.
Direct wet mountThe direct wet mount preparation was usedaccording to the World Health OrganizationBench aids for the diagnosis of intestinalparasites [7]. Lugol’s 1% iodine was usedto differentiate C. parvum oocysts fromyeast cells: C. parvum oocysts do not ac-cept the iodine stain, so they appear trans-parent; yeast cells accept the stain andappear deep yellow.
Sugar flotation concentration methodSheather’s sugar flotation technique wasused (specific gravity of solution 1.20–1.25). The high specific gravity allows theoocysts to float on the top of the solution inthe test tube. Briefly, a suspension of stoolin sugar solution was made in a test tubefilled to the brim with Sheather’s sugar so-lution. A cover slip was put on top of thetest tube in contact with the solution for 15minutes. The cover slip was placed down-wards on a microscope slide and the oo-cysts were visualized microscopically at× 400 magnification [8,9].
Cold Kinyoun stainingDifferential staining using a modified Ziehl–Neelsen technique, the cold Kinyountechnique (TCS Biosciences Limited,Buckingham, United Kingdon), was em-ployed to differentiate C. parvum oocystsfrom other cells and artefacts. The oocystsare acid-fast so they accept the stain andappear pink to red in colour (4–6 mm)against a blue background of debris.
Direct immunofluorescent antibodystainingMeriFluor™ Cryptosporidium/Giardia(Meridian Diagnostic Incorporated, Cincin-nati, United States of America) is an in vitrodirect immunofluorescence kit for the si-multaneous detection of Cryptosporidiumoocysts and Giardia cysts in faecal materi-al. The detection reagent contains a mixtureof fluorescein isothiocynate-labelled mono-clonal antibodies directed against cell wallantigens of Cryptosporidium oocysts. Pos-itive and negative controls were providedwith the kit by the manufacturing companyand manufacturer’s instructions were fol-lowed.
Statistical analysisStatistical analysis was performed usingSPSS.
Results
Of 300 stool samples, 112 (37.3%) werepositive for C. parvum. According to theconsistency of the sample, oocysts weredetected in 27.2% of liquid samples, 51.1%of semi-solid samples and 12.5% offormed samples. Among the 7 childrenwho were on chemotherapy for cancer, C.parvum was detected in the stools of 4(57.1%).
The monoclonal direct immunofluores-cence method gave the highest rate of pos-itive samples (37.3%) (Table 1) and wasstatistically the most sensitive comparedwith the other 3 methods (Table 2). In addi-tion, under ultraviolet light, the direct im-munofluorescence slide showed clear,oval, fluorescent green oocysts against anorange to dark background.
When the results were examined ac-cording to the children’s age, the highest
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM496

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 497
rate of infection (57%) was noted amongthose in the age group 5–< 7 years (Figure1).
The relation of infection to locality, sex,presence of animals in the home and sourceof drinking water is illustrated in Table 3.There was no significant difference in thedistribution of cases between males and fe-males. Out of 138 samples from childrenwho lived in rural areas, 60 (43.5%) werepositive for C. parvum oocysts, whereasof the 162 samples from children who livedin urban areas only 52 (32.1%) were posi-tive. In regard to the presence of animals,the infection rate was 36.2% among chil-dren who lived in compounds with no ani-
mals in comparison with 45.0% amongthose who lived in association with ani-mals. In the children who drank tap water,the infection rate was 35.3%. In those whodrank well water or spring water, however,infection rates were 48.4% and 42.9% re-spectively.
The seasonal pattern of C. parvum in-fection showed that a higher rate of inci-dence was recorded in the periods fromJanuary to July 2001, the first 5 months ofwhich represent the rainy months for thatyear (Figure 2).
Table 2 shows the comparative resultsbetween the 4 methods usually used for di-agnosis of C.parvum in stools. Comparisonof the various methods revealed the superi-ority of immunofluorescence followed bythe modified Ziehl–Neelsen, sugar flotationand the direct methods.
Discussion
Our findings showed a high incidence ofcryptosporidiosis in the 300 childrenwhose stools we examined. Oocysts of C.parvum were detected in 37.3% of samplesusing the immunofluorescence technique.This is the first time the immunofluores-
Table 1 Comparison of four methods fordiagnosis of Cryptosporidium parvum
Method Samples positive,n = 300
No. %
Direct wet mount 52 17.3
Sheather’s flotation 68 22.6
Cold Kinyoun stain 92 30.6
Direct immunofluorescence 112 37.3
Table 2 Specificity, sensitivity and efficiency of the 4diagnostic methods used for the detection ofCryptosporidium parvum oocysts in stool samplesfrom children in Irbid
Method Specificity Sensitivity Efficiency(%) (%) (%)
Direct wet mount 95 47 81
Sheather’s flotation 96 61 85
Cold Kinyoun stain 100 82 94
Directimmunofluorescence 100 98 99
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM497

498 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
cence test has been used in Jordan. Al-though this figure is higher than the one re-ported before from Jordan [10], it is similarto high figures from other countries as cit-ed below. It is also worth noting that previ-ous workers from Jordan took specimensfrom healthy schoolchildren while ourswere sick children reporting to a paediatrichospital. Our colleagues used a singlemethod, namely the modified Ziehl–Neelsen, while we used 4 methods.
A number of other studies on preva-lence of cryptosporidiosis have been re-ported from different parts of the world.The incidence rates vary according to sam-ple collection, which depends on clinicaljudgement; diagnostic tests, where somemethods are better than others; availabilityof facilities; and reporting systems. Inci-dence rates of 13.5% to 19.5% have beenreported from Egypt [11,12], and 10% inKuwaiti children [13]. Very high rates havebeen reported in Israeli children 48% [14],from the Texas–Mexico border 70.2% [15]and from the Republic of Korea 57% [16].
Figure 1 Incidence of cryptosporidiosis according to age
Table 3 The rate of infection byCryptosporidium parvum in relation tosociodemographic characteristics andsource of drinking water
Variable PositiveNo. %
Sexa
Male 72/186 38.7Female 40/114 35.1
Localityb
Rural 60/138 43.5Urban 52/162 32.1
Animals at residencec
With 18/40 45.0Without 94/206 36.2
Source of drinking waterd
Well water 31/64 48.4Spring water 3/7 42.9Tap water 73/207 35.3Filtered water 4/14 28.6Boiled water 0/7 –
aP = 0.529, degrees of freedom = 1, χ2 = 0.40.bP = 0.042, degrees of freedom = 1, χ2 = 4.12.cP = 0.282, degrees of freedom = 1, χ2 = 1.16.dP = 0.425, degrees of freedom = 3, χ2 = 1.71.
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM498

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 499
A review of several human population-based studies, especially on immunocom-promised patients in less-developedcountries, reported prevalence rangingfrom 9% to 48% in Africa and Asia [17].
In this study, 4 different methods wereused to detect and identify C. parvum oo-cysts in children’s stool samples. The di-rect wet mount with iodine identified thelowest number of samples, 52 (17.3%),positive for oocysts. The C. parvum oo-cyst is very small in size and can easily bemistaken in stool debris for artefacts. Also,it is easy to confuse with other oocysts,such as those of Cyclospora spp., andcells, especially yeast cells, which resembleC. parvum oocysts in size and morphology[18].
The number of oocysts detected in-creased to 68 (22.6%) using the flotationconcentration method. This procedureshowed a clear slide picture during micro-scopic examination yet the oocysts did notappear pink and refractile, and other para-
sites cannot be detected by this method.Also, this procedure necessitated readingthe results within 15 minutes of preparationbecause the oocysts tend to collapse anddisappear if left for a long time. Moreover,the presence of Sheather’s sugar solutioninhibits the staining procedure [19].
The cold Kinyoun acid-fast stainingtechnique yielded a higher rate of oocystidentification, 92 (30.6%). Using this meth-od we could differentiate between C. par-vum oocysts, which take a red to pinkcolour, and other faecal components, espe-cially yeast cells, which take the colour ofthe counterstain, i.e. blue if using methyl-ene blue, or green using malachite green.
The direct immunofluorescence meth-od gave the highest number of positivesamples, 112 (37.3%). In comparison withother methods, this method showed highsensitivity so we were able to detect oo-cysts even when present in low numbers inthe samples and large numbers of samplescould be scanned.
Figure 2 Seasonal variation of cryptosporidiosis, November 2000 to September 2001
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM499

500 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Our findings support and agree withother studies which reported that using flu-orescent monoclonal reagents increasedthe sensitivity and specificity of the detec-tion of C. parvum oocysts. It provides anexcellent screening method and offers auseful technique for epidemiological stud-ies, and hence, control of the parasite [20–22]
Source of drinking water plays an im-portant role in the transmission of infec-tion. Many people in Irbid depend onuntreated rainwater collected directly fromthe roof, then stored in metal or cementtanks. This is why most of our cases werediagnosed during April–May, during therainy season. Some families use wells orspring water for drinking. The resultsshowed that the rate of infection amongthose who drink from wells was 48.4%,compared to those who use only tap water,35.3%. We know that the oocysts ofCryptosporidium spp. can survive in con-centrations of chlorine used for watertreatment, let alone untreated water [23].
Considering the locality, we found thatthe infection rate in children who lived inrural areas was 43.5% whereas in childrenin urban areas it was 32%.
Seasonal or temporal trends associatedwith increased incidence vary from coun-try to country. Our result agrees with otherstudies from Central America, South Afri-ca, and India that reported a high peak inci-dence in rainy season [24]. Also, ourfindings were similar to those of anotherstudy conducted in Kuwait to detect the in-cidence and seasonality of cryptosporidio-sis in Kuwaiti children. The results of thatstudy showed that the maximum numbersof cases were recorded during the monthsJanuary to April [13].
Acknowledgement
This study was supported by the Deanshipof Research, Jordan University of Scienceand Technology.
References
1. Tzipori S. Cryptosporidiosis in animalsand humans. Microbiological reviews,1983, 47(1):84–96.
2. Fayer R, Ungar BL. Cryptosporidium spp.and cryptosporidiosis. Microbiologicalreviews, 1986, 50(4):458–83.
3. Meisel JL et al. Overwhelming waterydiarrhea associated with a cryptospo-ridium in an immunosuppressed patient.Gastroenterology, 1976, 70(6):1156–60.
4. Fayer R, Morgan U, Upton SJ. Epidemi-ology of Cryptosporidium: transmission,detection and identification. Interna-tional journal for parasitology, 2000,30(12–13):1305–22.
5. Nemri LF and Hijazi SS. Cryptospo-ridium a cause of gastroenteritis in pre-
school children in Jordan. Journal ofclinical gastroenterology, 1994, 19(4):288–91.
6. Weber R et al. Threshold of detection ofCryptosporidium oocysts in human stoolspecimens: evidence for low sensitivityof current diagnostic methods. Journalof clinical microbiology, 1991, 29(7):1323–7.
7. O‘Donoghue JP. Cryptosporidium andcryptosporidiosis in man and animals.International journal for parasitology,1995, 25(2):139–95.
8. Bench aids for the diagnosis of intestinalparasites. Geneva, World Health Organi-zation, 1994.
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM500

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 501
9. Garcia LS. Practical guide to diagnosticparasitology. Washington DC, ASMPress, 1999.
10. Nimri LF, Batchoun R. Prevalence ofCryptosporidium species in elementaryschool children. Journal of clinical mi-crobiology, 1994, 32(4):1040–2.
11. Stazzone AM et al. Frequency of Giardiaand Cryptosporidium infections in Egyp-tian children as determined by con-ventional and immunofluorescencemethods. Pediatric infectious diseasejournal, 1996, 15(11):1044–6.
12. Abdel-Maboud AI et al. Cryptospori-diosis in Benha; study of some modali-ties in diagnosis and treatment. Journalof the Egyptian Society of Parasitology,2000, 30(3):717–25.
13. Iqbal J et al. Cryptosporidiosis in Kuwaitichildren: seasonality and endemicity.Clinical microbiology and infection,2001, 7(5):261–6.
14. Robin G et al. Cryptosporidium infectionin Bedouin infants assessed by prospec-tive evaluation of anticryptosporidialantibodies and stool examination.American journal of epidemiology,2001, 153(2):194–201.
15. Leach CT et al. Prevalence of Crypto-sporidium parvum infection in childrenalong the Texas–Mexico border and as-sociated risk factors. American journal oftropical medicine and hygiene, 2000,62(5):656–1.
16. Cha JY et al. High prevalence and sea-sonality of cryptosporidiosis in a smallrural village occupied predominantly byaged people in the Republic of Korea.American journal of tropical medicineand hygiene, 2001, 65:518–22.
17. Ungar BLP. Cryptosporidium. In: MandellGL, Bennett JE, Dolin R, eds. Mandell,
Douglas and Bennett’s principles andpractice of infectious diseases, 5thed. Philadelphia, Churchill Livingstone,1999:2903–15.
18. Fayer R, Speer SA, Dubey JP. The gen-eral biology of Cryptosporidium. In: FayerR, ed. Cryptosporidium and cryptospo-ridiosis. Boca Raton, Florida, CRCPress, 1997:1–41.
19. Weber R et al. Threshold of detection ofCryptosporidium oocysts in human stoolspecimens: evidence for low sensitivityof current diagnostic methods. Journal ofclinical microbiology, 1991, 29(7):1323–7.
20. Garcia LS, Brewer TC, and Bruckner DA.Fluorescence detection of Cryptospo-ridium oocysts in human fecal speci-mens by using monoclonal antibodies.Journal of clinical microbiology, 1987,25(1):119–21.
21. Xiao L, Herd RP. Quantitation of Giardiacysts and Cryptosporidium oocysts in fe-cal sample by direct immunofluores-cence assay. Journal of clinicalmicrobiology, 1993, 31(11):2944–6.
22. Alles AJ et al. Prospective comparison ofdirect immunofluorescence and conven-tional staining methods for detection ofGiardia and Cryptosporidium spp. in hu-man fecal specimens. Journal of clinicalmicrobiology, 1995, 33(6):1632–4.
23. Korich DJ et al. Effects of ozone, chlorineand monochloromine on Crypto-sporidium parvum oocyst viability. Ap-plied and environmental microbiology,1990, 56:1423–8.
24. Casemore DP, Wright SE, Coop RL.Cryptosporidiosis—human and animalepidemiology. In: Fayer R, ed. Cryptospo-ridium and cryptosporidiosis. BocaRaton, Florida, CRC Press, 1997.
05 Cryptosporidiosis in children.pmd 8/18/2005, 11:18 AM501

502 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Handicap among children in Saudi Arabia: prevalence, distribution, type, determinants and relatedfactorsABSTRACT We determined the prevalence, distribution and determinants of handicap among children inSaudi Arabia. A field survey was carried out from 1417 to 1420 AH (1997–2000 AD) of 60 630 children under16 years selected from all regions of the country. Information was collected by questionnaire for all childrenand those with a handicap, or suspected of having a handicap, were referred for confirmatory diagnosis. Ofthe total sample, 3838 (6.33%) were recorded as handicapped. The region with the highest proportion ofhandicapped children was Jazan (9.90%); Riyadh had the lowest (4.36%). Motor disability was the common-est kind of handicap (3.0% of the total sample), followed by learning disability (1.8%). The highest proportionof disability was found among children with handicapped parents, those whose mothers were older at thetime of their birth and those whose mothers had not had medical care and necessary vaccination duringpregnancy.
*M.B. Al-Hazmy,1 B. Al Sweilan2 and N.B. Al-Moussa3
1Department of Medical Biochemistry, Faculty of Medicine, King Saud University, Riyadh, Saudi Arabia.2Red Crescent Society, Riyadh, Saudi Arabia.3Special Education, Ministry of Health, Riyadh, Saudi Arabia.Received: 25/02/03; accepted: 23/02/04
Le handicap chez l’enfant en Arabie saoudite : prévalence, répartition, type, déterminants etfacteurs associésRÉSUMÉ Cette étude a déterminé la prévalence, la répartition et les déterminants du handicap chez l’enfanten Arabie saoudite. Une enquête sur le terrain a été réalisée de 1417 à 1420 de l’Hégire (1997-2000) auprèsde 60 630 enfants de moins de 16 ans sélectionnés dans toutes les régions du pays. Des informations ontété recueillies à l’aide d’un questionnaire pour tous les enfants, et ceux ayant un handicap ou suspectésd’avoir un handicap ont été adressés à un laboratoire pour diagnostic de confirmation. Dans l’échantillontotal, 3838 enfants (6,33 %) ont été recensés comme handicapés. La région ayant le plus fort pourcentaged’enfants handicapés était Jazan (9,90 %) ; Riyad avait le plus faible pourcentage (4,36 %). Le handicapmoteur était le type d’handicap le plus courant (3,0 % de l’échantillon total), suivi par les troubles del’apprentissage (1,8 %). Le pourcentage d’incapacités le plus élevé a été constaté chez les enfants deparents handicapés, chez ceux dont la mère était plus âgée à leur naissance et ceux dont la mère n’avait pasbénéficié d’une surveillance médicale ni reçu les vaccinations nécessaires pendant la grossesse.
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM502

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 503
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM503

504 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM504

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 505
[7, 6]
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM505

506 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM506

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 507
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM507

508 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM508

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 509
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM509

510 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM510

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 511
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM511

512 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM512

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 513
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM513

514 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM514

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 515
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM515

516 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM516

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 517
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM517

518 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM518

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 519
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM519

520 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM520

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 521
2. WHO Expert Committee on Disability Prevention and Rehabilitation. Geneva, WorldHealth Organization, 1981 (Technical Report Series No. 668):1–39.
3. Hutchison T, Nicoll A. Developmental screening and surveillance. British journal of hospitalmedicine, 1988, 39(1):22–9.
4. Cochran WG. Sampling techniques, 3rd ed. New York, John Wiley, 1977.
5. Wilson JM, Jungner G. Principles and practice of screening for disease. Geneva, WorldHealth Organization, 1968 (Public Health Papers, No. 34):11.
6. Fleiss JL. Statistical methods for rates and proportions, 2nd ed. New York, John Wiley, 1981.
7. SPSS 6.0 for Windows. Chicago, SPSS Inc., 1995.
8. Schneiderman ED et al. A PC program for computing confidence band for average andindividual growth curves. Computers, biology and medicine, 1994, 24(2):119–27.
06 Handicap among children in Saudi Arabia.pmd 8/17/2005, 11:06 AM521

522 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Attitudes of a high-risk group ofpregnant Saudi Arabian women toprenatal screening for chromosomalanomaliesZ.A. Babay1
1Department of Obstetrics and Gynaecology, King Saud University, King Khaled University Hospital,Riyadh, Saudi Arabia.Received: 30/04/03; accepted: 14/01/04
ABSTRACT The attitude of 550 pregnant Saudi Arabian women aged > 35 years to prenatal screening forchromosomal anomalies was investigated. A total of 336 women (61.1%) accepted the general idea ofprenatal screening while 160 (29.1%) did not; 54 women (9.8%) were undecided. There was a high accep-tance of non-invasive methods such as ultrasound (61.3%) and biochemical screening (53.0%) but a lowacceptance of invasive methods (34.2%). The main reason for refusal of screening was the unacceptabilityof termination of pregnancy as a treatment option. There were statistically significant differences betweenthose who accepted the idea of screening and those who did not with regard to their awareness of theavailability of prenatal screening, their rejection of pregnancy termination, their doubt of the accuracy of thetests and in their belief that chromosomal abnormalities need no be screened for.
Attitudes d’un groupe de femmes enceintes saoudiennes à haut risque vis-à-vis du dépistageprénatal des anomalies chromosomiquesRÉSUMÉ On a examiné l’attitude de 550 femmes enceintes saoudiennes âgées de plus de 35 ans vis-à-visdu dépistage prénatal des anomalies chromosomiques. Au total, 336 femmes (61,1 %) acceptaient l’idéegénérale du dépistage prénatal tandis que 160 (29,1 %) ne l’acceptaient pas ; 54 femmes (9,8 %) étaientindécises. Il y avait une forte acceptation des méthodes noninvasives telles que l’échographie (61,3 %) et ledépistage biochimique (53,0 %) mais une faible acceptation des méthodes invasives (34,2 %). La raisonprincipale du refus du dépistage était l’inacceptabilité de l’interruption de grossesse comme option thérapeu-tique. Il y avait des différences statistiquement significatives entre les femmes qui acceptaient l’idée dudépistage et celles qui ne l’acceptaient pas pour ce qui concerne la connaissance de l’existence dudépistage prénatal, leur rejet de l’interruption de grossesse, leur doute au sujet de l’exactitude des tests etleur opinion concernant le fait que les anomalies chromosomiques ne nécessitent pas de dépistage.
07 Attitudes of a high-risk.pmd 8/18/2005, 11:11 AM522

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 523
Introduction
Genetic diseases affect all populations andhave been apparent since antiquity. In re-cent years many advances have been madein the field of prenatal screening for chro-mosomal anomalies. Techniques now avail-able for such screening include secondtrimester biochemical screening (α-feto-protein, β human chorionic gonadotropin(HCG) and unconjugated estrogen), firsttrimester biochemical screening (pregnan-cy associated plasma protein A (PAPPA),and β HCG), ultrasound fetal nuchal trans-lucency measurement, in addition to theolder invasive techniques such as amnio-centesis and chorionic villus sampling.Some of the non-invasive methods havehigh sensitivity, especially if combined withultrasound nuchal translucency measure-ment (90% sensitivity and 3.1% false posi-tive rate) [1] in addition to causing no harmto the fetus. The use of these tests has re-sulted in a significant decrease in the preva-lence of children with chromosomalabnormalities [2].
The incidence of Down syndrome inSaudi Arabia is 1.8 per 1000 live births [3],which is similar to the reported incidence inHawaii but higher than the rest of the Unit-ed States of America (10 per 10 000 livebirths) [4]. Some modern Islamic opinionand rulings have accepted prenatal diagno-sis and approved severe congenital anoma-lies and malformations per se as a reasonfor termination of pregnancy before en-soulment (120 days from conception or134 days from last menstrual period) [5,6].However, in spite of the availability of thesescreening tests, there are no reports in liter-ature about their use in Saudi Arabia nor theawareness of Saudi Arabian women ofsuch tests and their attitudes to them.Therefore, this study was carried out toassess the awareness and acceptance of
such screening methods among pregnantSaudi Arabian women.
Methods
King Khalid University Hospital (KKUH)Riyadh, Saudi Arabia is the largest teachinghospital in the central region in Saudi Ara-bia, with an average delivery rate of 4500babies per month. All pregnant womenaged 35 years or older attending the Satur-day afternoon antental clinic at KKUH be-tween October 2002 and January 2003were included in the study and were admin-istered a questionnaire devised by the au-thor. The questionnaire was conductedverbally and it included information on age,parity, personal or family history of a childwith chromosomal anomalies, awarenessof the availability of prenatal screening forsuch conditions and their acceptance ofsuch screening in the next pregnancy, inaddition to reasons for non-acceptance.None of the women refused to participate.Statistical analysis was done using SPSS,version 10. The Student t-test was used tocompare between variables and a P-valueof ≤ 0.01 was considered significant.
Results
A total of 1680 pregnant women attendedthe antental clinic during the study period.Of those, 550 (32.7%) women were aged35 years or older and were included in thestudy. The mean age and standard deviation(SD) was 37 (2.34) years (range 35–44years) and mean parity was 4 (3.23) (range1–7). In all, 284 women (51.6%) knewabout the availability of prenatal screening,28 women (5.1%) had a positive familyhistory of a child with chromosomal anom-alies and 13 women (2.4%) had a history ofgiving birth to an affected child. A total of
07 Attitudes of a high-risk.pmd 8/18/2005, 11:11 AM523

524 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
336 women (61.1%) accepted the generalidea of prenatal screening in the next preg-nancy while 160 women (29.1%) did notand 54 women (9.8%) could not decide(Table 1). Among the women who accept-ed the idea of screening, 53.0% acceptedthe idea of biochemical screening, 61.3%accepted the idea of ultrasound screeningand 34.2% accepted the idea of invasiveprocedures such as amniocentesis andchorionic villus sampling.
Further questioning of the women whodid not accept the idea of screeningshowed that 76% did not accept termina-tion of pregnancy as an option in the eventof an abnormal result, 22% did not acceptscreening in general as they doubted theaccuracy of the tests, 19% did not believethat they would have an abnormal child and6% did not believe chromosomal anoma-lies were an abnormality that should bescreened for (Table 2).
Table 3 shows a comparison betweenthose who accepted the idea of screening inpregnancy versus those who did not. Therewas a statistically significant difference be-
tween the 2 groups in their awareness ofthe availability of prenatal screening(57.7% versus 42.1%) (P = 0.0005), intheir rejection of pregnancy termination(65.5% versus 92.5%) (P = 0.001), in theirdoubt of the accuracy of the tests (8.9%versus 42.5%) (P = 0.001) and in theirbelief that chromosomal abnormalitieswere not an abnormality that should bescreened for (0.3% versus 15.0%) (P =0.001). There was no significant differencein acceptance or rejection of prenatalscreening between those who had a posi-tive family history of a child with chromo-somal anomalies, those who had positivepersonal history of having a child withchromosomal anomalies, and those whobelieved that they would not have a childwith chromosomal anomalies.
A comparison was made between thewomen who had positive family history ofa child with a chromosomal anomaly, thosewith a positive personal history of having achild with a chromosomal anomaly, andthose who did not have any such history(Table 4). There was a statistically signifi-cant difference between the 3 groups inacceptance of termination of pregnancy(75.0%, 69.2% and 76.2% respectively)(P = 0.001), in the belief in the possibility
Table 1 Characteristics of the study sample
Charactersitic No. (n = 550) %
Had a positive personalhistory of a child withchromosomal anomaly 13 2.4
Had a positive familyhistory of a child withchromosomal anomaly 28 5.1
Was aware of the availabilityof prenatal screening 284 51.6
Found screening:Acceptable 336 61.1Unacceptable 160 29.1Undecided 54 9.8
Table 2 Reasons for finding prenatalscreening unacceptable
Reason %
Did not accept termination ofpregnancy as an option 76
Doubted the accuracy of the tests 22
Did not believe that they would have achild with chromosomal anomalies 19
Did not believe chromosomalabnormality was an abnormalitythat should be screened for 6
07 Attitudes of a high-risk.pmd 8/18/2005, 11:11 AM524

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 525
of delivering a child with chromosomalanomalies (64.3%, 84.6% and 14.9%respectively) (P = 0.001), in the accep-tance of chromosomal anomalies as an ab-normality that should be screened for(7.1%, 38.5% and 5.1% respectively)(P = 0.001), in the acceptance of bio-chemical screening during pregnancy(71.4%, 53.8% and 29.7% respectively)(P = 0.001), in the acceptance of ultra-sound screening during pregnancy (71.4%,61.5% and 25.5% respectively) (P =0.001), and in the acceptance of an inva-sive investigation (25.0%, 100.0%, 43.4%respectively) (P = 0.001).
Discussion
The old adage that prevention is better thancure applies as much to genetic as to ac-quired diseases. Primary prevention of ab-normal genotypes would need to act priorto conception. Prenatal diagnosis with se-lective termination (secondary prevention)alters the birth frequency of the conditionbut is really only a holding measure pendingthe development of primary prevention ofgenetic disease. Currently the only primaryprevention available is pre-implantationgenetic diagnosis which requires in vitro
Table 3 Comparison of women who accepted the idea of prenatal screening for chromosomalabnormalities and those who did not
Variable Accepted Did not accept Odds 95% CI P-valuescreening screening/was ratio(n = 336) undecided
(n = 214)No. % No. %
Had a positive familyhistory of a child withchromosomal anomaly 20 6.9 8 3.7 1.63 0.67–4.11 0.3407
Had a positive personalhistory of a child withchromosomal anomaly 8 2.4 5 2.3 1.02 0.29–4.02 0.7992
Was aware of theavailability of prenatalscreening 194 57.7 90 42.1 1.88 1.31–2.70 0.0005**
Did not accept terminationof pregnancy as an option 220 65.5 198 92.5 0.15 0.08–0.28 0.001**
Doubted the accuracy ofprenatal screening tests 30 8.9 91 42.5 0.13 0.08–0.22 0.001**
Did not believe that theywould have a child withchromosomal anomalies 56 16.7 49 22.9 0.67 0.43–1.06 0.0889
Did not believe chromosomalanomaly was an abnormalitythat should be screened for 1 0.3 32 15.0 0.02 0.0–0.1 0.001**
**Statistically significant at P ≤ 0.01.CI = confidence interval.
07 Attitudes of a high-risk.pmd 8/18/2005, 11:11 AM525

526 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
fertilization and this is not suitable as ascreening test. The principle for any test tobe used for screening populations is that itshould be sensitive, relatively specificand harmless. In addition, the disorderscreened for should be of appreciablefrequency and early diagnosis should be anadvantage. In our study almost two-thirds(61.1%) of the women questioned accept-ed the idea of screening. Of those accept-ing the idea of screening, all acceptedultrasound screening, probably because itis part of the antenatal care in Saudi Arabiaand is therefore familiar to them and does
Table 4 Comparison of the women with a positive family history, those with a positive personalhistory and those with no history of a child with a chromosomal anomaly
Variable Positive family Positive personal No history P-valuehistory (n = 28) history (n = 13) (n = 509)
No. % No. % No. %
Accepted the idea ofprenatal screening 20 71.4 8 61.5 308 60.5 0.263
Was aware of the availabilityprenatal screening 15 53.6 10 76.9 259 50.9 0.0639
Did not accept terminationof pregnancy as an option 21 75.0 9 69.2 388 76.2 0.0019**
Doubted the accuracy ofprenatal screening tests 5 17.9 3 23.1 113 22.2 0.86
Did not believe that theywould have a child withchromosomal anomalies 18 64.3 11 84.6 76 14.9 0.001**
Did not believe chromosomalanomaly was an abnormalitythat should be screened for 2 7.1 5 38.56 26 5.1 0.001**
Accepted the idea of biochemicalscreening 20 71.4 7 53.8 151 29.7 0.001**
Accepted the idea of ultrasoundscreening 20 71.4 8 61.5 130 25.5 0.001**
Accepted the idea of invasivescreening (aminocentesis andchorionic villus sampling 7 25.0 13 100.0 221 43.4 0.001**
**Statistically significant at P ≤ 0.01.
not carry any risk of abortion. The accep-tance rate for biochemical screening waslower (53.0%). This rate is similar to thereported acceptance rate in other parts ofthe world [7,8]. The acceptance rate ofinvasive procedures was much lower(34.2%) probably because as it carries therisk of abortion. On the other hand, 29.1%of the women did not accept the idea ofscreening; the main reason was that theydid not accept termination of pregnancy asa treatment option.
Factors such as socioeconomic struc-ture, education and religion affect the
07 Attitudes of a high-risk.pmd 8/18/2005, 11:11 AM526

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 527
acceptability of prenatal diagnosis. Thesefactors are very important in Saudi Arabiaas all Saudi Arabians are Muslims and highparity is a characteristic feature of thecommunity. At the same time, the physi-cian’s attitude towards such tests is impor-tant as they share the same religiousbackground.
Public awareness of the risks and diffi-culties facing a child with chromosomalanomalies and the effect on their futurehealth and living is of great importance foracceptance of prenatal screening. In ourstudy 19% of the women believed that theywould not have a child with chromosomalanomalies although, because of their age(> 35 years), this was a high-risk popula-tion for certain such conditions. In addi-tion, the difference between those whoaccepted screening and those who did notwas statistically significant in regards to
their awareness of the availability of prena-tal screening and in their belief in theaccuracy of the tests (Table 3), whichreflects a lack of health knowledge.
From this study we conclude that com-bined biochemical screening and ultra-sound nuchal translucency are the mostacceptable prenatal genetic screening testsfor Saudi Arabian women bearing in mindthe religious and social background. Prena-tal diagnosis of such anomalies is importantfor both the parents and physicians even iftermination is not undertaken. Physiciansshould be encouraged to offer these testand to give appropriate counseling as thishigh-risk group constituted 32.7% of thewomen attending the antental clinic. Publicawareness should also be raised about theissues of genetic abnormalities and prenatalscreening until suitable primary preventionis available.
References
1. Benn PA et al. Combined second trimes-ter biochemical and ultrasound screen-ing for Down syndrome. Obstetrics andgynecology, 2002, 100(6):1168–76.
2. Cheffins T et al. The impact of maternalserum screening on the birth prevalenceof Down syndrome and the use of am-niocentesis and chorionic villus sam-pling in south Australia. British journalof obstetrics and gynaecology, 2000,107(12):1453–9.
3. Niazi MA et al. Down’s syndrome inSaudi Arabia: incidence and cytogenet-ics. Human heredity, 1995, 45(2):65–9.
4. Forrester MB, Merz RD. Epidemiology ofDown syndrome (trisomy 21) in Hawaii,1986–97. Teratology, 2002, 65(5):207–12.
5. Ghanem I. [Abortion as a necessity]. AlFaisal medical journal, 1984, 9:6–15 [inArabic].
6. [Regarding termination of pregnancy forcongenital abnormality (No. 4)]. TwelfthSession of the Moslem World LeagueConference of Jurists, Mecca 10–17February 1990 [In Arabic].
7. DeGraaf IM et al. Women’s preference inDown syndrome screening. Prenatal di-agnosis, 2002, 22(7):624–9.
8. Lam YH et al. Acceptability of serumscreening as an alternative to cytoge-netic diagnosis of Down syndromeamong women 35 years or older in HongKong. Prenatal diagnosis, 2000, 20(6):487–90.
07 Attitudes of a high-risk.pmd 8/18/2005, 11:11 AM527

528 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Validity of vision screening by schoolnurses in seven regions of OmanR. Khandekar,1 S. Al Harby,1 T. Abdulmajeed,1 S.A. Helmi2 and I.S. Shuaili3
1Eye and Ear Health Care Department; 2School Health Department, Directorate General of Health Affairs;3Department of Noncommunicable Diseases, Ministry of Health, Muscat, Oman.Received: 23/06/03; accepted: 20/10/03
ABSTRACT We tested the validity of vision screening in schools in 7 regions of Oman in 2003. Two research-ers tested 1719 randomly selected students in 4 school grades using the Snellen E acuity test. Trainedschool nurses had previously screened 182 233 students. The visual status recorded in the 2 screeningswas compared. Sensitivity of screening by nurses was 68.34% (95% CI: 67.30–69.38) and specificity99.23% (95% CI: 99.19–99.27). The positive predictive value was 85.42% (95% CI: 84.63–86.21) andnegative predictive value was 97.93% (95% CI: 97.87–98.00). The sensitivity of the vision test was signifi-cantly higher in females, older students and in North Sharqiya region. In general, the vision screening ofschool students in Oman has satisfactory validity. Periodic training of nurses and supervision of the screen-ing procedures could improve its sensitivity. Underlying causes of the high numbers of false negative casesshould be further investigated.
Validité du dépistage visuel réalisé par des infirmières scolaires dans sept régions d’OmanRÉSUMÉ Nous avons testé la validité du dépistage visuel dans des écoles de sept régions d’Oman en 2003.Deux chercheurs ont testé 1719 élèves choisis de manière aléatoire dans quatre classes à l’aide du test deSnellen (test du E). Des infirmières scolaires formées avaient examiné auparavant 182 233 élèves. Le bilanvisuel noté lors des deux examens a été comparé. La sensibilité de l’examen visuel réalisé par les infirmièresétait de 68,34 % (IC 95 % : 67,30-69,38) et la spécificité de 99,23 % (IC 95 % : 99,19-99,27). La valeurprédictive positive était de 85,42 % (IC 95 % : 84,63-86,21) et la valeur prédictive négative était de 97,93 %(IC 95 % : 97,87-98,00). La sensibilité du test de vision était significativement plus élevée chez les filles, chezles élèves plus âgés et dans la région septentrionale de Sharqiya. De manière générale, le dépistage visueldes écoliers et écolières à Oman avait une validité satisfaisante. La formation périodique des infirmières etle contrôle des procédures d’examen pourraient améliorer sa sensibilité. Les causes sous-jacentes dunombre élevé de cas faux négatifs devraient faire l’objet d’études approfondies.
08 Validity of vision.pmd 8/17/2005, 11:06 AM528

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 529
Introduction
Despite the widespread acceptance of vi-sion screening programmes as a means ofdetecting ocular disorders in children, therehas been little formal assessment of theirvalidity and reliability [1]. This is morechallenging as different methods are usedfor vision screening, e.g. the Snellen letteracuity and Modified Clinical Technique vi-sion screening kits, the Random Dot E ste-reogram and the hand-held autorefractor[2].
A study to assess the predictive abilityof school screening programmes suggest-ed the need for a detailed prospective studyto review predictability of both test-positiveand test-negative findings [3]. In our study,the validity of the school vision screeningprogramme was evaluated using specificityand sensitivity parameters. First levelscreening was performed by trained nursesand was compared with screening bypractising optometrists. Validating visionscreening by estimating the number of falsenegatives was also done [4].
In Oman, the eye health care pro-gramme is aimed at the early detection ofcommon and blinding eye diseases. Hence,trained nurses conduct vision screening an-nually, targeting students in 4 grades in allschools in Oman. Refractionists in each re-gion recheck the students shortlisted withdefective vision, refract them in schoolsand prescribe visual aids [5]. In 2002, thenumber of students with defective visionreferred by nurses and subsequently foundto be normal was high for 1st primary stu-dents but lower for 1st secondary students[6]. Rapid turnover of the health staff in-volved in this activity has raised seriousdoubts concerning the quality of thescreening procedures. The programmetherefore evaluated the validity of visionscreening using sensitivity and specificityparameters, reviewed the predictability of
vision screening for detection of refractiveerror and recommended steps to furtherstrengthen the vision screening activities.
Methods
We carried out a cross-sectional agreementstudy on 182 233 students in 7 regions ofOman during school year 2002–2003. Thestudy population was from 4 schoolgrades: 1st primary (6–7 years), 4th prima-ry (9–10 years), 1st preparatory (12–13years) and 1st secondary (16–17 years).
The list of schools in each region andthe number of students in each grade wereprovided by the Ministry of Education. Thevisual status of a randomly selected samplewas examined by the study investigators.The visual status of the same students thathad been noted by the school nurses duringschool year 2002–2003 was recoveredfrom school health records.
Hypothesis: the vision screening doneby school health staff matched the super-visor’s screening in 90% or more ofstudents. Null hypothesis: the visionscreening done by school health staff doesnot match the supervisor’s screening in90% or more of the students.
The study aimed to achieve a goal of90% power of the study and 95% signifi-cance level among a study populationwhich ranged from 15 000 to 45 000 perregion. With an acceptable error of 7%, thesample required was 137. To compensatefor the clustering effect of students in se-lected schools and to cover loss of data, thesample was multiplied by a factor of 1.8.Thus, the minimum sample in each regionwas 250.
The list of schools was used to random-ly select 4–6 schools in each region. Sincethe proportion of male and female studentsis almost equal, equal numbers of boys’ andgirls’ schools were selected. In each
08 Validity of vision.pmd 8/17/2005, 11:06 AM529

530 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
school, 1 class from each grade was ran-domly selected. If the class had less than50 students, an additional sample was en-rolled from another randomly selectedclass of the same grade. The aim was toenrol and examine 50 students in all 4grades in 1 region and give an equal oppor-tunity to all students of that grade in theschool to participate in the study.
The field staff comprised 2 national eyehealth care supervisors who had at least 5years of experience of vision screening.
The vision testing procedure and meth-od of response were explained to allstudents. Each student then was called ac-cording to his or her serial number. TheSnellen distant vision E chart was placed 6metres away from the student. The visionof the right eye was tested first followed bythe left and the results immediately notedon a standard form. Personal details of thestudents such as age, sex, area of residenceand visual status of each eye with and with-out visual aids were collected. History ofcheck-ups by an optician or ophthalmolo-gist was obtained from students who haddefective vision.
The school nurse had tested vision 3months prior to the study and the visualstatus of each student had been recorded inthe student’s health booklet. These recordswere referred to after the vision testing wascompleted by the supervisors.
Definitions: if vision screening in 1 eyewas found to have no more than 1 line dif-ference in the 2 screenings, it was definedas being in agreement. If vision screeningin 1 eye differed by more than 1 line in the 2screenings, the vision screening of that stu-dent was defined as being in disagreement.The disagreement was further graded ac-cording to the difference in visual status.Sensitivity was defined as ability of visionscreening by the nurse to correctly identifythe students with defective vision. Speci-
ficity was defined as ability of visionscreening by the nurse to correctly identifythe students without defective vision. Posi-tive predictive value was defined as abilityof vision screening to correctly predictcases of defective vision among studentswith suspected defective vision. Negativepredictive value was defined as ability ofthe test to correctly predict students with-out defective vision among those declaredto have normal vision.
The data was computed using EpiData.Univariate analysis was conducted usingSPSS, version 11. Agreement and disagree-ment rates per student were calculated.The sensitivity, specificity, false positives,false negatives, positive predictive and neg-ative predictive values of the vision screen-ing were estimated. The rates of validityparameters were projected for the studypopulation. They were also adjusted bysex, school grade and region using indirectstandardization. The determinants of theseparameters by sex, school grade and regionof residence were also evaluated. The fre-quencies, percentage proportions, odds ra-tios and 95% confidence intervals wereestimated to validate the results.
To ensure a high and uniform quality ofthe study, a standardization workshop wasconducted for the field staff. A pilot studywas carried out in schools not selected forthe study; on the basis of the pilot study,the methodology, data collection form anddata entry format were revised. Field staffhaving at least 5 years experience in visionscreening and supervision work wereselected for the study. The study wassupervised by the study investigators atvarious stages. During the pilot study,inter-observer variation was evaluated andwas found to be minimal. The supervisors’skills in vision screening were also com-pared to those of optometrists and werefound to match.
08 Validity of vision.pmd 8/17/2005, 11:06 AM530

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 531
The authorities in the Department ofSchool Health, Ministry of Health and Min-istry of Education were approached andtheir consent was obtained for the study.Verbal consent of school principals wasalso taken. The results of the study wereused to improve the vision screening ofstudents. The results were also distributedto regional health authorities and healthmanagers of related health programmes.
Due to logistic problems, the studycould not be conducted in Dhofar, Musun-dam and Al Wousta regions of Oman.Hence, the result of the study should be ex-trapolated to the whole of Oman with cau-tion. There was a gap of around 3 monthsbetween the vision screening done by thenurse and that done by the supervisors. It isassumed that vision status between the 2screenings had not changed in most of thestudents. However, a marginal increase inrefractive error or progress in pathologycausing further deterioration of visual sta-tus in a limited number of cases cannot beruled out.
Results
The profile of the study population and thesample we examined is given in Table 1.The total study population comprised 182233 students in 4 school grades in 7 regionsof Oman during the school year 2002–2003. We enrolled a sample of 1720 stu-dents as participants in our study. Onestudent did not complete the vision testingas he had to leave the school. Of the 1719students examined, 861 (50.1%) were maleand 858 (49.9%) were female. The samplewas evenly distributed between the 4grades and the 7 health regions. The pro-portion of the study population and thesample differed by region so adjusted ratesshould be used for comparison.
The vision of 1599 students (93.0%)was 6/6 in both eyes in both screenings. In74 (4.30%) students, vision was impairedin at least 1 eye. In 13 (0.76%) students,the screening by the nurse suggested im-paired vision but screening by the supervi-sor showed 6/6 vision. In 33 (1.92%)students the screening by the nurse sug-gested either 6/6 or 6/9 vision, but on re-screening by a supervisor, these studentswere found to have a higher grade of de-fective vision. Based on these findings, wecalculated validity parameters for the sam-ple and for the study population as a whole.For the statistical validation, 95% confi-dence intervals were also estimated (Table2).
The validity parameters of visionscreening by sex are given in Table 3. Thespecificity of screening was high for bothsexes. However, the sensitivity of vision
Table 1 Profile of the study population andthe sample
Variable Study population Sample(N = 182 233) (n = 1719)
No. % No. %
SexMale 94 276 51.7 861 50.1Female 87 957 48.3 858 49.9
School grade1st primary 40 437 22.2 415 24.14th primary 48 396 26.6 416 24.21st preparatory 51 043 28.0 479 27.91st secondary 42 357 23.2 409 23.8
RegionMuscat 34 056 18.7 250 14.5Dhakhiliya 29 101 16.0 237 13.8North Sharqiya 14 542 8.0 255 14.8South Sharqiya 15 750 8.6 228 13.3North Batinah 45 280 24.8 235 13.7South Batinah 26 621 14.6 259 15.1Dhahirah 16 883 9.3 255 14.8
08 Validity of vision.pmd 8/17/2005, 11:06 AM531

532 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
screening was significantly higher in fe-male than in male students.
The agreement and disagreement ratesfor 1st primary and 4th primary were de-termined and compared to those for 1st
preparatory and 1st secondary students(Table 4). The screening of students inhigher grades by school nurses had signifi-cantly higher specificity than that for pri-mary students.
Table 2 Parameters of validity
Parameter No. Crude Adjusted 95% CIOR OR
True positives 74 4.30 4.24 3.79–4.69
False positives 13 93.02 93.07 92.95–93.19
False negatives 33 0.76 0.72 0.26–1.18
True negatives 1599 1.92 1.96 1.51–2.41
% %
Sensitivity 69.16 68.34 67.30–69.38
Specificity 99.19 99.23 99.19–99.27
Positive predictive value 85.06 85.42 84.63–86.21
Negative predictive value 97.98 97.93 97.87–98.00
Rates are adjusted for sex, school grade and region.The false positive rate was 13/1719 × 100 = 0.76%.The false negative rate was 33/1719 × 100 = 1.92%.OR = odds ratio; CI = confidence interval.
Table 3 Validity of vision screening by sex
Variable Males (n = 861) Females (n = 858)No. % No. %
True positives 32 4.0 42 4.5
False positives 2 0.3 11 1.2
False negatives 18 2.2 15 1.7
True negatives 809 93.5 790 92.6
% (95% CI) % (95% CI)
Sensitivity 64.87 (63.35–66.39) 72.09 (70.68–73.49)
Specificity 99.73 (99.69–99.76) 98.69 (98.62–98.77)
Positive predictivevalue 94.02 (93.29–94.75) 78.46 (77.32–79.60)
Negative predictivevalue 97.72 (97.62–97.81) 98.17 (98.08–98.26)
Rates are adjusted for school grade and region.CI = confidence interval.
08 Validity of vision.pmd 8/17/2005, 11:06 AM532

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 533
The validity parameters (adjusted forsex and school grade) for each region werecompared (Table 5). Sensitivity rangedfrom 57.29% in Dhahirah to 80.08% inNorth Sharqiya.
Discussion
After 10 years of annual vision screening inschools, a review was needed. Our studytested the validity of vision screening. Onthe basis of our results, the programmewould be able to strengthen the strategy forreducing eye strain in schoolchildren.Thus, the study was crucial for the eyecare programme.
Since the sample was evenly distributedin all regions and the number of school stu-dents varied in different regions andgrades, the study results were adjusted be-fore outcomes of variants were compared.This also helped to minimize the confound-ing effects of school grade, sex, region andother related confounders on the validity.
The cooperation of students could bethe effect modifiers in such a study [7].Proper explanation of the procedures alongwith help from teachers ensured the fullcooperation of all participants.
The vision screening done by the nurseshad a specificity of 99.23%. Thus, visionscreening by nurses could accurately iden-tify students who did not have vision de-fects. The test had 68.34% sensitivity.Thus, the vision screening proceduresmissed a substantial proportion of studentswith defective vision.
In a study in New York State in the Unit-ed States of America (USA), using a visionscreening battery, the Snellen test was100% specific but it missed 75.5% of thechildren found to have vision problemswhen given a complete visual examination[8]. Although the methodology is differentin the 2 studies, our study had a higher rateof specificity and a relatively low sensitivi-ty. The World Health Organization has rec-ommended that vision screening should
Table 4 Validity of vision screening by school grade
Variable 1st & 4th primary Preparatory and(n = 831) secondary (n = 888)
No. % No. %
True positives 14 1.67 60 6.68
False positives 4 0.53 9 0.91
False negatives 11 1.36 22 2.54
True negatives 802 96.43 797 89.87
% (95% CI) % (95% CI)
Sensitivity 55.08 (52.55–57.61) 72.49 (71.39–73.60)
Specificity 99.45 (99.40–99.50) 99.00 (98.93–99.07)
Positive predictivevalue 75.87 (73.97–77.76) 88.06 (87.30–88.81)
Negative predictivevalue 98.61 (98.53–98.68) 97.26 (97.15–97.36)
Rates are adjusted for sex and region.CI = confidence interval.
08 Validity of vision.pmd 8/17/2005, 11:06 AM533

534 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
have at least 80% specificity and sensitivityfor it to be cost-effective (A. Choudhury,unpublished data, 2003).
Vision screening of 652 elementary stu-dents by lay volunteers was compared tothat of optometrists in the USA. The Modi-fied Clinical Technique was used in thisstudy. It showed 5.5% false positives and4.3% false negatives [9]. Our study had avery low number of false positives (0.76%)and false negatives (1.92%). Considering adifference of 1 line as normal in our studycould be a lenient criterion resulting inthese low rates.
There is no evidence to suggest that amore complex protocol would improve thedetection of ocular disorders in screening.Rather, a more effective implementation ofthe current screening procedure gives bet-ter results [1]. In our study, simple visiontesting methods were used and still had val-id outcomes. This is in agreement with theobservations of earlier studies [1,9].
In view of the shortage of qualified opti-cians, it would be impossible to screen thelarge number of children in the presentschool population. Wong found that fol-lowing an educational programme and col-laboration with optometrists, nurses wereable to correctly refer a high percentage of
children [10]. Therefore, first level screen-ing should be conducted by nurses or otherschool staff trained in such procedures.Oman has adopted a similar model of usingsimple vision screening tools, annual train-ing of nurses and active supervision by op-ticians. This has resulted in a reasonablequality of screening. Countries with limitedresources should focus on strengtheningvision screening procedures using similarmodels and strategies instead of investingin costly equipment and using complicatedscreening methods.
Bailey compared vision screening pro-cedures done by optometric students withthose done by licensed opticians using theModified Clinical Technique. They werefound to have less satisfactory validity. Itwas proposed that the limited experience ofthe first level vision screeners was mainlyresponsible for the low predictive ability ofthis test [3]. The staff involved in our studyhad been trained in vision screening fre-quently. This could have accounted for thehigh validity in our study.
Vision screening of schoolchildren inmany states of the USA has suggested thateven if different procedures and criteria areused, school screening may show a falsepositive rate of 30% or more [11,12]. In
Table 5 Validity of vision screening by region
Region Specificity Sensitivity Positive predictive Negative predictive(%) (%) value (%) value (%)
Muscat 67.64 98.92 84.21 97.30
Dhakhiliya 75.84 99.19 84.23 98.55
North Sharqiya 80.08 97.83 73.22 98.51
South Sharqiya 67.38 98.52 74.00 97.97
North Batinah 62.71 98.72 75.25 97.71
South Batinah 74.78 99.98 99.61 98.29
Dhahirah 57.29 99.97 99.09 97.53
Rates are adjusted for sex and school grade.
08 Validity of vision.pmd 8/17/2005, 11:06 AM534

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 535
our study, the rate for false positives andfalse negatives was less than 2%. The lowrate of refractive error and the high qualityof vision screening in our study could ac-count for these observations.
The vision screening carried out bynurses could accurately predict the pres-ence of refractive error in almost 70% ofthe students with this problem. The num-ber of students declared as having normalvision by a nurse after vision screening wasalmost 98% accurate. This high rate couldbe due to the large number of students inour study sample who did not have defec-tive vision.
Refractive errors, which often becomemanifest during school age, rarely carryany serious prognostic implications. Ex-perts disagree on whether an uncorrectedrefractive error that would be detected byscreening has any adverse effects on aca-demic performance in school-age children[13,14]. Hence, the 1.92% asymptomaticrefractive error cases that were missed inschools might be of minimal importance.
The sensitivity of vision screening inour study was significantly higher for fe-male than for male students. Differences inthe attitudes of male and female students tocooperating with female nurses and malesupervisors could be responsible for thisobservation.
Refractive error may be marginal inchildren of primary-school age comparedto students in preparatory and secondarygrades. Difference in prevalence in these 2groups of students and differential under-standing of vision screening proceduresmay have resulted in high specificity in stu-dents of higher grades.
Differences in the training of the nursesas well as in the quality of vision screeningby different nurses could account for theregional variation in the validity.
Vision screening by nurses and secondlevel screening performed by school re-fractionists in Oman is similar to the modelproposed in the USA [15]. This would cer-tainly reduce unnecessary referrals to theophthalmologist.
Vision screening in schools by trainednurses in a large part of Oman has veryhigh validity. However, false negative casesobserved in this study could be further re-duced through vigilant screening. Furtheroperational research is needed to determineyield and efficiency for the low rate of re-fractive error cases in 1st primary grade.
Recommendations
Vision screening in schools is an importantstrategy in many countries to detect andmanage defective vision in the early stages.The use of primary staff for first levelscreening needs to be validity tested. InOman, screening sensitivity was 68.3%and specificity 99.2.% The large number offalse negative cases compromised the qual-ity of vision screening. The underlyingcauses of low sensitivity should be identi-fied and addressed. Further training andperiodic supervision of vision screening bynurses could improve the validity of the vi-sion test. The sensitivity of vision screen-ing in primary school and validity waslower than in preparatory and secondarystudents. It could be improved throughtraining and more thorough screening
Vision screening of school students inOman has satisfactory validity. Its low sen-sitivity needs to be improved. Periodictraining of nurses and supervision of thescreening procedures could improve thequality of vision screening. Because of thelow yield, vision screening of primary-school students should perhaps be discon-
08 Validity of vision.pmd 8/17/2005, 11:06 AM535

536 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
tinued and replaced by preschool visionscreening. Determinants of low sensitivitysuch as being male and of young age, as
well as regional variation, should be furtherinvestigated to strengthen the quality ofscreening.
References
1. Macfarlane DJ, Fitzgerald WJ, Stark DJ.Assessment of the Queensland SchoolHealth Service vision screening pro-gramme. Australian and New Zealandjournal of ophthalmology, 1987, 15(3):175–80.
2. Hammond RS, Schmidt PP. A RandomDot E stereogram for the vision screen-ing of children. Archives of ophthalmol-ogy, 1986, 104(1):54–60.
3. Bailey RN. Assessing the predictive abil-ity of the test-positive findings of anelementary school vision screening. Op-tometry and vision science, 1998, 75(9):682–91.
4. Robinson B et al. Measurement of thevalidity of a preschool vision screeningprogram. American journal of publichealth, 1999, 89(2):193–8.
5. Eye health care manual, 1st ed. Muscat,Oman, Ministry of Health and United Na-tions Children’s Fund, 1995:55–7.
6. Annual health report year 2002. Muscat,Oman, Ministry of Health, 2003:1–41.
7. Elimination of avoidable visual disabilitydue to refractive errors. Geneva, WorldHealth Organization, 2000 (WHO/PBL/00.79).
8. Lieberman S et al. Validation study of theNew York State Optometric Association(NYSOA) vision screening battery.American journal of optometry and phy-siological optics, 1985, 62(3):165–8.
9. Wick B, O’Neal M, Ricker P. Comparisonof vision screening by lay and profes-sional personnel. American journal ofoptometry and physiological optics,1976, 53(9 Pt 1):474–8.
10. Wong SG. Comparison of vision screen-ing performed by optometrists andnurses. American journal of optometryand physiological optics, 1978, 55(6):384–9.
11. Appelboom TM. A history of visionscreening. Journal of school health,1985, 55(4):138–41.
12. Romano PE. Summary and conclusions.Symposium on preschool/school visionand eye screening: current techniquesand future trends. American orthopticjournal, 1988, 38:73–80.
13. Halveston EM et al. Visual function andacademic performance. American jour-nal of ophthalmology, 1985, 99(3):346–55.
14. Rosner J, Rosner J. Comparison of vi-sual characteristics in children with andwithout learning difficulties. Americanjournal of optometry and physiologicaloptics, 1987, 64(7):531–3.
15. Donaldson LA et al. Pediatric communityvision screening with combined optom-etric and orthoptic care: a 64-monthreview. Ophthalmic and physiologicaloptics, 2002, 22(1):26–31.
08 Validity of vision.pmd 8/17/2005, 11:06 AM536

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 537
Schoolteachers’ knowledge ofcommon health problems in BahrainF.A. Alnasir1 and J.H. Skerman2
1Department of Family and Community Medicine, College of Medicine and Medical Sciences, Arabian GulfUniversity, Bahrain.2Department of Anaesthesia and Intensive Care, College of Medicine and Medical Sciences, Arabian GulfUniversity and Salmaniya Medical Complex, Bahrain.Received: 01/07/03; accepted: 29/10/03
ABSTRACT Schoolteacher could be a useful source of health information for students but that they them-selves would have to possess adequate and accurate knowledge of health issues. We assessed Bahrainischoolteachers’ knowledge of some common health problems using a pre-tested, structured questionnairewhich requested information on schools, teachers’ demographic data, and knowledge about 5 commonhealth problems in Bahrain: bronchial asthma, sickle-cell anaemia, hypertension, diabetes mellitus and thedangers of smoking. We analysed the data on 1140 respondents from a random selection of teachers in allschools in Bahrain. The schoolteachers scored only around 50% on average for knowledge about commonhealth problems which indicates a need to educate schoolteachers about health in order to improve theirknowledge and their capability to disseminate health knowledge and information to students.
Connaissance des problèmes de santé courants par les enseignants scolaires à BahreïnRÉSUMÉ Les enseignants scolaires pourraient représenter une source utile d’information sur la santé pourles élèves mais il devraient eux-mêmes posséder des connaissances suffisantes et exactes sur les ques-tions de santé. Nous avons évalué les connaissances des enseignants scolaires Bahreïnites concernantdes problèmes de santé courants à l’aide d’un questionnaire structuré, testé au préalable, qui cherchait àrecueillir des informations sur les écoles, des données démographiques concernant les enseignants et laconnaissance de cinq problèmes de santé courants à Bahreïn : l’asthme bronchique, la drépanocytose,l’hypertension, le diabète sucré et les dangers du tabagisme. Nous avons analysé les données de1140 répondants dans une sélection aléatoire d’enseignants de toutes les écoles de Bahreïn. Les ensei-gnants n’ont obtenu qu’un score d’environ 50 % en moyenne pour les connaissances concernant cesproblèmes de santé courants, ce qui indique une nécessité d’éduquer les enseignants en matière de santéafin d’améliorer leurs connaissances et leur capacité à diffuser des connaissances et des informations surla santé aux élèves.
09 Schoolteachers knowledge.pmd 8/17/2005, 11:06 AM537

538 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Introduction
Schoolteachers form a group with greatpotential for influencing the health knowl-edge and attitudes of students and otherpopulation groups. Schoolteachers’ per-ceptions of health, their attitudes and prac-tices, and their knowledge of commonhealth problems could be essential factorsin optimizing their roles as health educatorsin society.
Many adult behaviour patterns and atti-tudes develop in early childhood. In addi-tion there is a growing acceptance of theneed for health education at primary schoolage. For example, it has been found thatvarious interventions such as improvingteachers’ awareness of cancer educationissues and providing appropriate cancer ed-ucation resources might increase the levelof primary school-based cancer education[1].
Schoolteachers are expected to be rolemodels so that students can emulate andadopt their behaviour and attitudes. InSweden, the majority of school pupilsthought that schoolteachers were the bestsources of information for sexually trans-mitted infections and sexuality [2]. School-teachers are also considered the majorsource of information for their studentsand would appear to be suitable as healtheducators [3]. In Australia, teachers andthe clergy have been identified as “gate-keepers” who might serve as a first line ofassistance for distressed young people [4].
Since current emphasis in health educa-tion is on prevention of serious illnessthrough lifestyles that promote wholeness,teachers are well placed professionally tocarry out health education at school [5,6].Teachers’ education is considered a majorfactor in the effective implementation ofcomprehensive school health [7]. Atti-tudes, behaviour and general knowledgeare disseminated to the students from the
teachers, either deliberately or uncon-sciously. In order to raise students’ healthknowledge and improve their attitudes to-ward health, they should be placed in anappropriate environment that is based on 3main determining factors: teachers, schooland society (including home).
School and health professionals shouldcontinue to advocate school-wide policiesand programmes that support both stu-dents and teachers if the goal of an inte-grated healthy school environment is to berealized [8]. Ministries of education andhealth should organize seminars on healtheducation [9]. Educational health packagescould be developed with collaboration be-tween teachers who have an understandingof the principles of curriculum design andhealth professionals who are fully aware ofhealth problems [10]. Development effortsby teachers, including training and ongoingreinforcement to increase their sense ofpreparedness, have significant effects inthe classroom [11]. In Nigeria, most teach-ers felt that health education was importantand should be an integral part of the curri-culum [12]. Multicultural attitudes andknowledge on the part of teachers changedin a positive direction when candidates at-tended a teacher preparation programme[13].
It is reported that the formation of apopulation’s healthy lifestyle, which is oneof the main tasks of Soviet medicine, canbe accomplished with the help of schoolhealth education teams [14]. It has beendocumented, however, that in Bahrainschool health education is not includedin the curriculum [15]. Few states in theUnited States of America include health ed-ucation in their state tests, and elementaryschool teachers often do not feel it is animportant subject and therefore spend in-sufficient time on health instruction in theclassroom [16].
09 Schoolteachers knowledge.pmd 8/17/2005, 11:06 AM538

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 539
It was our goal to study teachers’awareness about common health problemsin Bahrain. We hypothesized that the teach-ers were well informed about these prob-lems and hence would be able todisseminate information to others, specifi-cally students.
Methods
Information was collected about theschools in Bahrain and permission for con-ducting the study was obtained from theMinistry of Education, who sent out an in-formation circular to all schools in thecountry. The study was carried out during1997–1998. The target population was allBahraini teachers of all disciplines in 49randomly selected schools.
Schools in the 5 geographic regions ofBahrain (Muharraq, Manama, Northernarea, Central area and Western area) wereselected for this study. The total number ofschools in these areas is 152, with a total of3360 teachers. A random sample of 49schools was selected. Stratified randomsampling was done, giving appropriate rep-resentation to the 5 regions, and taking intoaccount the number of Bahraini teachers ineach school, the type of school, and the lo-cality. All 1248 Bahraini teachers in thoseschools were included in the study.
The study tool for this investigation wasa questionnaire. Based on a comprehensivereview of the literature, a 4-item surveywas designed. Items addressed each of thefollowing areas: information about theschool, teachers’ demographic characteris-tics, teachers’ health perceptions, andhealth knowledge. The questionnaire wasadapted to the local language and designedin a simple way to make it easy for the se-lected teachers to read and complete. Theface value and content validity of the ques-tionnaire were tested by distributing it to
doctors in various specialties and obtainingtheir feedback. It was also tested for re-peatability by sending it again to the samedoctors after a 1-week lapse. A pilot studywas done to test the various areas of thequestionnaire.
The health information portion of thequestionnaire was aimed at collecting infor-mation about the teachers’ health status andtheir experiences of illness. Five commonhealth problems in Bahrain (asthma, sickle-cell anaemia, hypertension, diabetes melli-tus and the dangers of smoking) werechosen because of their high prevalenceamong Bahrainis. The teachers were askedquestions (a total of 48: 8 questions for thesmoking problem and 10 for each of theothers) related to signs, symptoms andcomplications of those problems. Someuntrue information for each problem wasincluded to test the teachers’ knowledge.The teachers were asked to give their re-sponse to the pre-set questions by writing“Yes” (agree), “No” (do not agree) or “Donot know” to the answer. Each blank spacewas considered a missing value (i.e. teach-ers did not respond to it).
After analysing the responses, a scoreof 1 was given for the correct answer and0 for other answers (wrong, missing or“Do not know” answers).
No questions inquiring about whetherthe teachers had received any formal train-ing or special education about commonhealth problems were included.
The head teacher of each school wasgiven complete information on the study,either by telephone or through direct con-tact. The questionnaires were delivered tothe teachers in the selected schools in themorning and collected at the end of thesame day or after a maximum of 2 days. Anaccompanying letter was written to theteachers giving them information on thestudy, its aims, how to complete the ques-tionnaire and requesting their cooperation.
09 Schoolteachers knowledge.pmd 8/17/2005, 11:06 AM539

540 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Data were analysed using SPSS. Resultswere cross-tabulated and chi-squared cal-culated. The knowledge portions of thedata were scored and assessed as percent-age scores.
Results
Of the 1254 teachers included in the sam-ple, 1140 (91%) responded and 114 (9%)did not. Efforts were made to obtain thequestionnaire from the non-respondents,but without success. The general charac-teristics of these non-respondents, such asage, sex and type of school, were investi-gated and were not found to differ fromthose of the respondents. There were 679(60%) female respondents and 461 (40%)male. Age range was 20–58 years (mean32.7 years, median 32 years, standard devi-ation [SD] 6.17). Only 15% of the teachersstated they were above 40 years of age. Ofthe 220 teachers who did not wish to dis-close their ages (19%), the majority (94%)were female. Of the responding teachers,78% were married, 20% were single and2% were either divorced or widowed.There were 774 teachers who were mar-ried and had children (range 1–16 children,mean 3). More male teachers than femaleteachers had children (65% compared to35%).
Of the 1091 who responded to thequestion related to the teachers’ level of ed-ucation, 19% had only high school educa-tion and 81% had higher education, whichincludes a Diploma or Bachelor’s degree.Teachers in primary and intermediateschools were younger (≤ 32 years) (P <0.01) and more of them had degres thansecondary school teachers. More femalesthan males had higher education. Of the to-tal, 29% taught science subjects, includingmathematics, and 71% taught arts sub-jects. There were 1068 responses (94%) to
the question about the duration of occupa-tion. Duration ranged from 1 year to 35years (mean 12.3 years, SD 7.3). Only 6%of the teachers were smokers, of whomthe majority (94%) were male, while 4%were ex-smokers. Regarding alcohol con-sumption, since it is not usual in an Islamiccountry, not all who drink admit to it, andthe others may find the question offensive.Of the 98% who responded to this ques-tion, only 14 (1%), all of whom were male,admitted to drinking alcohol. Some 40% ofthe teachers were the heads of the house-hold, and 35% said they shared that re-sponsibility.
Table 1 shows the teachers’ responsesto questions on their own health and health-related attitudes. The health status of theteachers was satisfactory as only 16% hadany acute illness during the past 6 months.
The total scores for each teacher,which represented correct answers,ranged between 0 and 41 (mean 21.9, me-dian 24, SD 9.3). Only 1 teacher obtainedthe highest score, but there were 39 teach-ers (3%) who scored 0, i.e. no knowledgeat all. Table 2 shows the scores for eachhealth problem. The total scores for knowl-edge, after categorizing into 2 groups(group 1 = ≤ 24, group 2 = > 24) accordingto the median, were studied in relation to allother variables in the study (Table 3). Therewere a large number of missing values onthe topics of sickle-cell anaemia and asth-ma, while there were no missing values onknowledge related to hypertension, diabe-tes mellitus or the dangers of smoking.
A higher percentage of females thanmales were teaching science, 23% com-pared with 16% (chi-squared 7.225, P< 0.5). More of the younger teachers (≤ 32years) were teaching science subjects(46%), while more of the older teachers(> 32 years) were teaching arts subjects(77%) (chi-squared 20.81, P < 0.001).
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM540

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 541
In general, teachers who had no chron-ic illness had better health knowledge foreach category of health knowledge (chi-squared 15.8, P < 0.001). Of the 93% ofteachers who had not had any recent ill-ness, 88% perceived their general health assatisfactory (chi-squared 67.1, P < 0.001).
With regard to the dangers of smoking,surprisingly, it was found that there was norelationship between the smoking habit andknowledge about smoking (P < 0.9). How-ever knowledge about smoking increasedas the number of years of occupation in-creased (chi-squared 11.673, P < 0.001).
Table 1 Health and health-related attitudes of teachers
Variable Yes No Did notrespond
No. % No. % No. %
Suffered from any acuteillness during the past6 months 179 16 936 82 25 2
Any chronic illness 344 30 759 67 37 3
Family illness 322 28 785 69 33 3
Doing exercise 191 17 862 76 87 8
Hospital admissionsa 137 12 963 85 40 4
Good Unsatisfactory Noknowledge
Teachers’ perception oftheir general healthb 930 82 100 9 68 6
Perception of healthservices in Bahrain 762 67 265 23 113 10
aMore females (72%) than males (28%) reported having been admittedto hospital.b42 (4%) teachers did not respond.
Table 2 Teachers’ scores on knowledge of five common health problems inBahrain
Health problem Respondents No. of Score SD(n = 1140) questionsNo. % Range Mean Median
Sickle-cell anaemia 1053 92 10 0–10 4.88 5 1.980
Smoking 1067 94 8 0–8 5.28 6 1.852
Asthma 1029 90 10 0–10 5.16 5 2.185
Hypertension 969 85 10 0–10 3.00 3 1.899
Diabetes mellitus 1064 93 10 0–10 5.34 6 2.133
SD = standard deviation.
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM541

542 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Table 4 shows some characteristics thatwere found to have a significant relation-ship with teachers having adequate knowl-edge (≥ mean) about diabetes mellitus.Knowledge of other health problems was
found not to be related to the teachers’characteristics.
There was no relationship between suf-fering from chronic illness and knowledgeabout asthma, sickle-cell anaemia or the
Table 3 Correlation of some characteristics of teachers to betterknowledge of five common health problems in Bahrain
Characteristic Better knowledge P-value
Duration of occupation as a teacher Fewer years > more years < 0.05
Type of school Primary + intermediate > secondary < 0.02
Sex Female > male < 0.001
Marital status Married > single < 0.02
Teaching discipline Science > arts < 0.02
Recent illness No recent illness > having recent illness < 0.05
Chronic illness No chronic illness > having chronic illness < 0.001
Family size Smaller family size > larger family size < 0.01
Table 4 Relationship between characteristics of teachers andhaving adequate (≥≥≥≥≥ mean) knowledge about diabetes
Characteristic Teachers with P-value χχχχχ 2
adequate knowledge,%
SexMale 90 < 0.001 33.927Female 77
Discipline taughtScience 90 < 0.05 4.505Art 84
Family illnessYes 89 < 0.05 5.240No 83
Perception of ownhealth
Satisfactory 84 < 0.05 3.897Unsatisfactory 93
Drinking alcoholYes 76 < 0.002 5.040No 85
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM542

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 543
dangers of smoking. There was a signifi-cant relationship between suffering fromchronic illness and knowledge about diabe-tes mellitus (chi-squared 9.2, P < 0.02) andknowledge about hypertension (chi-squared 6.4, P < 0.001)
Discussion
The majority of the teachers who partici-pated in this study were young adults, andmost had a university degree, either a Di-ploma or Bachelor degree. Most of theteachers were female, and we found theyhad better health knowledge than the males.A study done in the United States of Amer-ica indicated that students’ attitudes im-proved if their teachers were moreeducated and older. It was reported that thestudents’ perception and attitude regardingadolescent homosexuality varied with theteacher’s sex, age, educational level andteaching status [17].
The overall knowledge of the school-teachers was found to be average in the ar-eas related to sickle-cell anaemia, asthmaand diabetes mellitus. While it was poor(< mean) in the area of hypertension, theyhad a good (≥ mean) knowledge of the dan-gers of smoking. Considering that the prev-alence of these problems is high in Bahrainand the surrounding areas (3%–5% forsickle-cell anaemia, 25% for diabetes melli-tus, 5% for bronchial asthma and approxi-mately 15% for hypertension) [18], it isalarming that schoolteachers are not moreaware of the problems. It is not surprisingtherefore if students lack information aboutsuch problems.
Teachers who had personal experienceof illness, i.e. chronic or acute illness, ei-ther at the time of the study or earlier in life,or who had a family member with a signif-icant illness, knew more in the areas of dia-betes mellitus and hypertension. Both of
these are chronic conditions and are verycommon in our community. This could ex-plain why teachers were more informed inthese 2 areas than the other areas
There was no relationship betweenteachers’ perceptions regarding their ownhealth or the health services in Bahrain andtheir knowledge of common health prob-lems. This finding was supported by re-sults of another study which found thatteachers’ health beliefs are not linked towhether teachers teach health generally[19].
Surprisingly, primary and intermediateschool teachers had better knowledge thansecondary school teachers. This could beexplained by the fact that they may beyounger and more of them have universitydegrees. Such findings regarding knowl-edge about common diseases are supportedby studies in other parts of the world. Astudy in Brazil found that in areas wherehelminthic diseases are known to have beenpresent for a long time, teachers and pupilsstill had little information on them, norwere they aware of the mechanism oftransmission [20].
Another barrier to quality health instruc-tion is when little or no in-service training isavailable for teachers. Several conditionsare necessary for the development of learn-ing opportunities allowing teachers free-dom to develop new understandings ofteaching and learning. Poor knowledge ofhealth can be attributed to the fact thathealth education is not a priority at manyschools, and can also be related to the factthat health education questions are usuallyabsent from end of year examinations [16].Most teachers in our study were self-taught with regard to health education asthere is no formal training, and relied pri-marily on traditional teacher-centred in-struction methods. In order to delivereffective health education in schools,
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM543

544 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
teachers require a substantial body ofknowledge and a variety of skills [21,22].The type of training programme offeredusually has a marked influence on thelength and type of programme they offer totheir students [23].
Our findings are in agreement withthose of several other reports which indi-cated that teachers’ health knowledge isdeficient and this may ultimately affecttheir ability either to deliver health educa-tion or to manage acute health problems inschool. In one study it was found that themajority of teachers encounter child abuseamong their students although they did notreceive sufficient education on how to ad-dress it [24]. In another study it wasreported that teachers needed more knowl-edge regarding head lice and were signifi-cantly more knowledgeable as teachingexperience increased [25]. In an Indianstudy about sex education, pupils in oneschool were reassessed after a health talkand distribution of a handout. Despite hav-ing had no formal sex education, most re-spondents were reasonably well informedabout the transmission of HIV. Mediateachers and health workers were quoted
as the main sources of knowledge [26]. Ina Canadian study on the effectiveness ofschool-based sexual health education, itwas found that it depended in part on thepreparation of the teachers [24]. The deliv-ery of consistently high quality sexualhealth education in schools requires that allteachers of sexual health education are ade-quately prepared and acquire a substantialbody of knowledge.
Conclusion
We found that there was a deficiency inteachers’ health knowledge and thereforethere is a need to educate schoolteachersabout health, particularly about health prob-lems prevailing in the society. There shouldbe regular pre-service and in-service train-ing regarding such problems. Health andeducation ministries in Bahrain should or-ganize joint seminars for schoolteachers onhealth education to improve their level ofhealth awareness. This would help teachersto develop health education packages incollaboration with the curriculum designersand health professionals to tackle currentknowledge about health-related problems.
References
1. Carey P et al. Cancer education and theprimary school teacher in England andWales. Journal of cancer education,1995, 10(1):48–52.
2. Persson E, Sandstrom B, Jarlbro G.Sources of information, experiences andopinions on sexuality, contraception andSTD protection among young Swedishstudents. Advances in contraception,1992, 8(1):41–9.
3. McGovern M, Barry MM. Death educa-tion: knowledge, attitudes and perspec-tives of Irish parents and teachers. Deathstudies, 2000, 24(4):325–33.
4. Leane W, Shute R. Youth suicide: theknowledge and attitudes of Australianteachers and clergy. Suicide and life-threatening behaviour, 1998, 28(2):165–73.
5. Mull, SS. The role of the health educatorin development of self-esteem. Journalof health education, 1991, 22:349–51.
6. Masvidal RM et al. La educación sani-taria en la escuela [Health education inschool]. Atención primaria 1995, 15(6):369–70, 372.
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM544

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 545
7. Wood DN. Teacher credential candi-dates’ perceptions of the need forpre-service training in comprehensivehealth education. Paper presented at theannual meeting of the American SchoolHealth Association, Milwaukee, Wiscon-sin, 1995.
8. Kubik MY et al. Food-related beliefs, eat-ing behavior, and classroom food prac-tices of middle school teachers. Journalof school health, 2002, 72(8):339–45.
9. Brook U. Teachers’ attitudes towardsAIDS: an explorative study in Israel. Pa-tient education and counseling, 1994,24(3):337–40.
10. Henry RL et al. Integrated health andeducation input in the development ofeducational resources about asthma forschools. Journal of paediatric and childhealth, 1994, 30(6):492–6.
11. Hausman AJ, Ruzek SB. Implementationof comprehensive school health educa-tion in elementary schools: focus onteacher concerns. Journal of schoolhealth, 1995, 65(3):81–6.
12. Fabiyi AK, Blumenthal DS. Health edu-cation in Nigerian secondary schools.Journal of community health, 1991,16(3):151–8.
13. Capella-Santana N. Voices of teachercandidates: positive changes inmulticultural attitudes and knowledge.Journal of educational research, 2003,96(3):182–92.
14. Tsurikov VT, Gavriushenko VV. Izopyta organizatsii smotra-konkursashkol’nykh sanprosvetagitbrigad. [Expe-rience in organizing competition ofschool health education teams].Sovetskoe zdravookhranenie, 1991, (5):54–6.
15. Roemer R. Legislative action to combatthe world tobacco epidemic, 2nd ed.Geneva, World Health Organization,1993:210.
16. Telljohann SK et al. Effects of an inser-vice workshop on the health teachingself-efficacy of elementary school teach-ers. Journal of school health, 1996,66(7):261–5.
17. Telljohann SK et al. Teaching aboutsexual orientation by secondary healthteachers. Journal of school health, 1995,65(1):18–22.
18. Health Information Directorate. Healthstatistics report – 2003. Bahrain, Ministryof Health, 2003.
19. Carey P et al. Is health locus of controlrelated to health education activity? Psy-chological reports, 1995, 76(3 pt 2):1389–90.
20. Dos Santos MG et al. Educacao emsaúde em escolas públicas de 1 grau daperiferia de Belo Horizonte, MG, Brasil.II - Conhecimentos, opinioes e pre-valencia de helmintiases entre alunos eprofessors. [Health education in 1stgrade public schools at the periphery ofBelo Horizonte, Brazil. II. Knowledge,opinion and prevalence of helminthiasisamong students and teachers]. Revistado Instituto de Medicina Tropical de SãoPaulo, 1993, 35(6):573–9.
21. Gingiss PL, Basen-Engquist K. HIV edu-cation practices and training needs ofmiddle school and high school teachers.Journal of school health, 1994, 64(7):285–90.
22. McKay A, Barrett M. Pre-service sexualhealth education training of elementary,secondary, and physical health educa-tion teachers in Canadian faculties ofeducation. Canadian journal of humansexuality, 1999, 8(2):91–101.
23. Sequier A, Demarteau M, Pereira M.L’analyse des représentations: unmoyen d’évaluer la formation desenseignants en éducation pour la santé.[Representational analysis: a means to
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM545

546 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
evaluate teacher training in health edu-cation]. Promotion & education, 1994,1(3):14–8.
24. Abrahams N, Casey K, Daro D. Teachers’knowledge, attitudes and beliefs aboutchild abuse and its prevention. Childabuse and neglect, 1992, 16(2):229–38.
25. Kirchofer GM, Price JH, Telljohann SK.Primary grade teachers’ knowledge and
perceptions of head lice. Journal ofschool health, 2001, 71(9):448–52.
26. Agrawal KH et al. Knowledge of and atti-tudes to HIV/AIDS of senior secondaryschool pupils and trainee teachers inUdupi District, Karanataka, India. Annalsof tropical paediatrics, 1999, 19(2):143–9.
Note from the Editor
We would like to inform our readers that the next issue of EMHJ(Volume 10 No. 6) will be a Special Issue on Nutrition.
09 Schoolteachers knowledge.pmd 8/17/2005, 11:07 AM546

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 547
Comparison of prostaglandin E2tablets or Foley catheter for labourinduction in grand multiparasM.I. Al-Taani1
1Department of Obstetrics and Gynaecology, Queen Alia Military Hospital, Royal Medical Services,Amman, Jordan.Received: 04/05/03; accepted: 23/10/03
ABSTRACT The efficacy, safety and outcome of prostaglandin (PG)E2 was compared with Foley catheterfor labour induction in grand multiparous women. At a hospital in Jordan, 147 women with Bishop score ≤ 5were randomized to receive 3 mg PGE2 vaginal tablets (n = 75) or 50 mL intracervical Foley catheter (n = 72).The change in Bishop score was significantly higher in the PGE2 group than the catheter group, and timefrom induction to delivery was significantly shorter in the PGE2 group. Significantly more women neededoxytocin for labour augmentation in the catheter than the PGE2 group and fetal distress was significantlymore frequent. For grand multiparas, PGE2 vaginal tablets may be preferable for ripening the cervix as wellas for labour induction.
Comparaison des ovules de prostaglandine E2 et de la sonde de Foley pour le déclenchement dutravail chez des grandes multiparesRÉSUMÉ L’efficacité, l’innocuité et l’effet de la prostaglandine (PG) E2 ont été comparés avec la sonde deFoley pour le déclenchement du travail chez des grandes multipares. Dans un hôpital en Jordanie,147 femmes dont le score de Bishop était inférieur ou égal à 5 ont été randomisées pour recevoir des ovulesvaginaux de PGE2 de 3 mg (n = 75) ou une sonde de Foley intracervicale de 50 mL (n = 72). La modificationdu score de Bishop était significativement plus importante dans le groupe de la PGE2 que dans le groupe dela sonde, et le temps entre le début du travail et l’accouchement était significativement plus court dans legroupe de la PGE2. Un nombre significativement plus important de femmes a eu besoin d’ocytocine pouraugmenter le travail dans le groupe de la sonde que dans le groupe de la PGE2 et la souffrance foetale étaitsignificativement plus fréquente. Chez les grandes multipares, les ovules vaginaux de PGE2 peuvent êtrepréférables pour la maturation cervicale ainsi que pour l’induction du travail.
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM547

548 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Introduction
The process of cervical ripening usuallycommences before labour begins; the cer-vix undergoes significant biochemicalchanges over a period lasting from 12hours to 6–8 weeks [1]. It is believed to becontrolled by certain hormones (in particu-lar prostaglandin E2) that play a role in trig-gering uterine contractile activity [2]. Sothe state of the cervix has been suggestedto be the most important factor in predict-ing the success rate of labour induction [3–5].
Calder et al. reported an increasing ma-ternal and neonatal morbidity when labourinduction begins with a Bishop score ≤ 3[6]. Trofatter in 1992 reported a decreasein induction failure when using a variety ofmethods to ripen the cervix [7]. The use ofprostaglandins for cervical ripening admin-istered by any route has been reported toimprove the rate of vaginal delivery and de-crease the rate of caesarean section and in-strument deliveries [8]. In addition, the useof a cervical catheter has been shown ef-fective for cervical priming and leads to afavourable outcome [9].
Grand multiparity is considered a riskfactor for maternal and neonatal morbidity.However, the subject is still under debate,with several authors reporting conflictingresults as to whether a pregnancy is highrisk or not because of its associated medi-cal and obstetric complications [10–13].Labour induction using prostaglandins inthis high parity group has been viewed as astressful and potentially dangerous proce-dure. Other reports on the use of prosta-glandins in grand multiparas contradict thisnotion and have yielded a safe and effectivemethod of labour induction [14–16].
Grand multiparity is common in Jordan.The total number of deliveries conducted inQueen Alia Military Hospital during the
study period (12 months) was 3684 and1547 (42%) of these were to grand multip-arous women. The number of inductionsof labour conducted was 590 (16%). It istherefore important to study the efficacy,safety and outcome of vaginal prostaglan-din (PG)E2 tablet compared with intracer-vical Foley catheter insertion for inductionof labour in this high parity group.
Methods
This prospective randomized study wascarried out at Queen Alia Military Hospital,Amman, Jordan. Between September 2001and August 2002, 147 grand multiparouswomen who had a clinically unfavourablecervix and indications for labour inductionwere recruited for the study. Patients wereeligible for inclusion if they had a singletonpregnancy at term, vertex presentation, in-tact membranes, reassuring fetal hearttracings and Bishop score ≤ 5. Womenwith previous caesarean section, rupturedmembranes, contraindications for vaginalbirth, suspected cephalopelvic dispropor-tion or unexplained antepartum haemor-rhage were excluded.
After written informed consent was ob-tained, patients were randomized to one ofthe 2 methods, using a random number ta-ble. For the first method, 75 women weregiven PGE2 3 mg vaginal tablet, inserted inthe posterior vaginal fornix. This was re-peated at 6-hour intervals, if needed. Forthe second method, 72 women were givena size 18 Foley catheter, inserted intracervi-cally in order to pass the internal os using asterile speculum technique. This was inflat-ed with 50 mL distilled water and taped tothe inner side of the thigh to produce asmall traction.
For all women, vital signs were record-ed on admission and blood was drawn for
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM548

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 549
complete blood count and cross-matching.General and systemic examinations fol-lowed by pelvic examination were per-formed. A fetal heart rate tracing wasobtained upon admission and after the initi-ation of the induction method for a mini-mum time of 45 minutes. Abdominal andcervical examinations were performed at4–6 hour intervals to diagnose the start oflabour and to measure Bishop score chang-es, unless these were indicated at earliertimes. Amniotomy was performed within1–2 hours of the diagnosis of labour or assoon as clinically feasible.
The progress of labour was monitoredevery 2 hours. Labour abnormalities weredefined by Friedman’s criteria [16]. Forthese cases, oxytocin infusion was startedfor augmentation of labour, administered inthe manner outlined by O’Driscoll andMeagher [17]. Intrapartum continuous fe-tal heart rate monitoring was performed.
The primary outcome measures werethe route of delivery and the time requiredfrom beginning of the induction method todelivery. The secondary outcome measureswere the change in Bishop score, intrapar-tum complications or the need for oxytocinfor labour augmentation.
Comparison of continuous variableswas made with Student t-test. Categoricalvariables were compared using the chi-squared or Fisher exact test. P < 0.05 wasconsidered to indicate a significant differ-ence.
Results
There were no significant differences inpresenting characteristics between the 2study groups (Table 1) and both groupshad similar indications for labour induction(Table 2). Postdates and pre-eclampsiawere the most frequent indications in both
groups. The frequency of postdate preg-nancies was significantly higher in thecather group than the PGE2 group (P =0.029).
As shown in Table 3, the change inBishop score was statistically significantlyhigher in the PGE2 group than the Foleycatheter group (mean 3.95 ± SD 2.20 ver-sus 3.10 ± 1.10) (P < 0.01). Significantlymore women in the catheter group (49%)needed oxytocin for labour augmentationthan in the PGE2 group (20%) (P < 0.001).
The time from initiation of the inductionmethod to delivery was significantly short-er in the PGE2 group compared with thecatheter group (16.5 ± 2.2 versus 20.5 ±3.9 hours) (P < 0.01). Of women that wererandomized to use PGE2, 61% deliveredwithin 16 hours after initiation of inductioncompared with 42% of those randomizedto use the Foley catheter. This was a statis-tically significant difference (P < 0.01).There were 21 women who delivered after24 hours in the catheter group, comparedwith 5 women in the PGE2 group. This dif-ference was highly statistically significant(P < 0.001).
Table 1 Presenting characteristics of grandmultiparas treated with Foley catheter orprostaglandin E2 (PGE2) vaginal tablet forinduction of labour
Characteristic Catheter PGE2 group P-group (n = 72) (n = 75) value
Maternal age(years) 27.7 (5.5) 27.1 (5.7) 0.438
Gestational age(weeks) 39.4 (1.9) 39.5 (1.7) 0.721
Parity (No.) 7.7 (2.1) 7.4 (1.9) 0.176
Initial Bishopscore 2.56 (1.40) 2.61 (1.30) 0.873
Values are shown as mean (standard deviation).n = number of patients.
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM549

550 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Table 2 Indications for induction of labour in grand multiparastreated with Foley catheter or prostaglandin E2 (PGE2) vaginaltablet for induction of labour
Indication Catheter group PGE2 group P-value(n = 72) (n = 75)
No. % No. %
Postdates 29 40 23 31 0.029
Pre-eclampsia 20 28 24 32 0.164
Diabetes 8 11 12 16 0.118
Suspected IUGR 10 14 11 15 0.693
Suspected macrosomia 5 7 5 7 0.999
IUGR = intrauterine growth restriction.n = number of patients.
Table 3 Labour and delivery outcomes of grand multiparas treatedwith Foley catheter or prostaglandin E2 (PGE2) vaginal tablet forinduction of labour
Outcome Catheter group PGE2 group P-value(n = 72) (n = 75)
No. % No. %
Change in Bishop scoreMean (SD) 3.10 (1.10) 3.95 (2.20) < 0.01
Oxytocin required 35 49 15 20 < 0.001
Time from induction to delivery< 16 hours 30 42 46 61 < 0.0116–24 hours 21 29 24 32 0.228> 24 hours 21 29 5 7 < 0.001Mean (SD) 20.5 (3.9) 16.5 (2.2) < 0.01
Intrapartum complicationsFetal distress 11 15 6 8 0.01Pyrexia 0 0 1 1 0.105Failure to progress 6 8 7 9 0.617Haemorrhage 3 4 5 7 0.91
Delivery typeSpontaneous vaginal 52 72 57 76 0.166Forceps 3 4 2 3 0.581Vacuum 5 7 6 8 0.611Caesarean section 12 17 10 13 0.147
SD = standard deviation.n = number of patients.
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM550

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 551
There were no significant differencesbetween the groups in intrapartum compli-cations or in type of delivery but the fre-quency of fetal distress was significantlyhigher in the catheter group than the PGH2group (P = 0.01) (Table 3). In addition,there were no statistically significant diffe-rences in fetal outcomes (Apgar scores at 5minutes, birth weight, admissions to theneonatal intensive care unit or meconiumaspiration) between the 2 groups (Table 4).No more than 2 × 3 mg PGE2 vaginal tab-lets were needed to achieve a clinically fea-sible cervix for amniotomy. No womanneeded a blood transfusion. All women andtheir babies were discharged home in goodcondition.
Discussion
This study demonstrates that cervical rip-ening as well as labour induction in grandmultiparas is safe using either PGE2 or Fo-ley catheter. Both methods were effective,but use of PGE2 3 mg vaginal tablets ap-peared to be superior to the intracervicalinsertion of a Foley catheter, in view of thehigher change in Bishop score, shorter in-
terval from initiation to delivery and lessneed of oxytocin for labour augmentation.The current study agrees with other re-ports regarding the use and safety of PGE2vaginal tablets for labour induction in grandmultiparas [14,18,19].
These findings contradict Sciscione etal. [9] who used PGE2 intracervical gelcompared with intracervical insertion ofFoley catheter; however this gel is notreadily available in our hospital. It is wellknown that some factors might affect thesafety, absorption and efficacy of PGE2,such as the vehicle, oily lubrication, humid-ity and possibly vaginal pH [20,21]. Thedifference in results may be attributed tothe type of PGE2 used, as the main effectof PGE2 gel is cervical ripening and its con-tractile effect is considered to be small[22,23].
The most hazardous major complica-tion of labour induction in grand multiparasis rupture of the uterus. Suggested risk fac-tors for uteruine rupture include multipari-ty, oxytocin use and the state of the cervix.The present study revealed no major com-plications. Comparison of intrapartumcomplications between groups showed no
Table 4 Fetal outcomes of grand multiparas treated with Foleycatheter or prostaglandin E2 (PGE2) vaginal tablet for inductionof labour
Outcome Catheter group PGE2 group P-value(n = 72) (n = 75)
No. % No. %
Mean (SD) birth weight (g) 3503 (575) 3452 (530) 0.319
Apgar score < 6 at 5 min 5 6.9 3 4.0 0.094
Admission to NICU 6 8.3 5 6.7 0.259
Meconium present 13 18.1 15 20.0 0.293
NICU = neonatal intensive care unit.SD = standard deviation.n = number of patients.
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM551

552 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
significant differences except for fetal dis-tress which was significantly higher in thecatheter group. Oxytocin was needed forlabour augmentation in 48.6% and 20.0%of the Foley and PGE2 groups, respectively.Outcome of labour and delivery comparedfavourably well in both groups. This dem-onstrates an equivalent safety of bothmethods, a finding that has been confirmedby others [14,24].
Furthermore, labour induction in grandmultiparas with previous caesarean sectionhas been reported to be safe, so too is theuse of oxytocin when there is no contrain-dication for repeating the caesarean section[25,26]. However, in the current study
there were no cases of previous caesareansection. This might eliminate grand multi-parity as a risk factor in the genesis of rup-ture of the uterus and in the increasingincidence of intrapartum complications asother studies indicate [12,13,27].
In the view of these findings, it can beconcluded that cervical priming as well aslabour induction in grand multiparouswomen is safe and effective when using ei-ther PGE2 tablets or Foley catheter, togeth-er with the use of oxytocin if needed forlabour augmentation, but in the absence ofany contraindications to induction. The useof PGE2 3 mg vaginal tablets is preferred tothe intracervical Foley catheter.
References
1. Steiner AL, Creasy RK. Methods of cervi-cal ripening. Clinical obstetrics and gy-necology, 1983, 26:37–46.
2. Garfield RE. Cellular and molecularbases for dystocia. Clinical obstetricsand gynecology, 1987, 30:3–18.
3. Garrett WJ. Prognostic signs of surgicalinduction of labour. Medical journal ofAustralia, 1960, 49:29.
4. Bishop EH. Pelvic scoring for elective in-duction. Obstetrics and gynecology,1964, 24:266–8.
5. Anderson AM, Turnbull AC. Relationshipbetween the length of gestation and cer-vical dilatation, uterine contractility andother factors during pregnancy. Ameri-can journal of obstetrics and gynecol-ogy, 1969, 105:1207–14.
6. Calder AA, Embrey MP, Tait T. Ripeningof the cervix with extra-amniotic prostag-landin E
2 in viscous gel before induction
of labour. British journal of obstetrics andgynaecology, 1977, 84:264–8.
7. Trofatter KF. Cervical ripening. Clinicalobstetrics and gynecology, 1992, 35:476–85.
8. Keirse MJ N. Prostaglandins in prein-duction cervical ripening. Meta-analysisof worldwide clinical experience. Jour-nal of reproductive medicine, 1993, 38(1 suppl.):89–100.
9. Sciscione AC et al. A prospective ran-domized comparison of Foley catheterinsertion versus intracervical prostag-landin E
2 gel for preinduction cervical
ripening. American journal of obstetricsand gynecology, 1999, 180(1 Pt 1):55–60.
10. Mwambingu FT, Al-Meshari AA, Akiel A.The problem of grandmultiparity in cur-rent obstetric practice. International jour-nal of gynaecology and obstetrics, 1988,26(3):355–9.
11. Evaldson GR. The grandmultipara inmodern obstetrics. Gynecologic and ob-stetric investigation, 1990, 30(4):217–23.
12. Babinszki A et al. Perinatal outcome ingrand and great-grand multiparity: ef-fects of parity on obstetric risk factors.American journal of obstetrics and gyne-cology, 1999, 181(3):669–74.
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM552

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 553
13. Goldman GA et al. The grandmultipara.European journal of obstetrics, gynecol-ogy, and reproductive biology, 1995,61(2):105–9.
14. Abou el-Leil LA, Nasrat AA, Fayed HM.Prostaglandin E2 vaginal pessaries inthe grandmultipara with an unripe cer-vix, a comparison of different paritygroups. International journal of gynaeco-logy and obstetrics, 1993, 40(2):119–22.
15. Yamani TY, Rouzi AA. Induction of laborwith vaginal prostaglandin-E2 in grandmultiparous women. International jour-nal of gynaecology and obstetrics, 1998,62(3):255–9.
16. Friedman EA. The labour curve. Clinics inperinatology, 1981, 8(1):15–25.
17. O’Driscoll K, Meagher D. Active manage-ment of labour. The Dublin experience,2nd ed. London, Baillière Tindall, 1986.
18. Sobande AA, Al-Bar HM, Archibong EI. Acomparison of spontaneous labor withinduced vaginal tablets prostaglandinE2 in grand multiparae. Saudi medicaljournal, 2001, 22(8):698–701.
19. Yamani TY, Rouzi AA. Induction of laborwith vaginal prostaglandin-E2 in grandmultiparous women with one previouscesarean section. International journalof gynaecology and obstetrics, 1999,65(3):251–3.
20. Lyrenas S, Clason I, Ulmsten U. In vivocontrolled release of PGE2 from a vagi-nal insert (0.8 mm, 10 mg) during induc-tion of labour. British journal of obstetricsand gynaecology, 2001, 108(2):169–78.
21. Ramsey PS et al. Effect of vaginal pH onefficacy of the dinoprostone gel for cervi-cal ripening/labor induction. Americanjournal of obstetrics and gynecology,2002, 186(4):843–6.
22. Seeras RC. Induction of labor utilizingvaginal vs. intracervical prostaglandinE2. International journal of gynaecologyand obstetrics, 1995, 48(2):163–7.
23. Nuutila M, Kajanoja P. Local administra-tion of prostaglandin E2 for cervicalripening and labor induction: the appro-priate route and dose. Acta obstetricia etgynecologica scandinavica, 1996, 75(2):135–8.
24. St Onge RD, Connors GT. Preinductioncervical ripening: a comparison of intrac-ervical prostaglandin E2 gel versus theFoley catheter. American journal of ob-stetrics and gynecology, 1995, 172(2 Pt1):687–90.
25. Abu-Heija AT, Ali AM. Induction of laborin grand multiparous women and previ-ous cesarean section: is it safe? Gyneco-logic and obstetric investigation, 2002,53(2):121–4.
26. Ben-Aroya Z et al. Oxytocin use in grand-multiparous patients: safety and compli-cations. Journal of maternal–fetal medi-cine, 2001, 10(5):328–31.
27. Toohey JS et al. The “dangerous multi-para”: fact or fiction? American journal ofobstetrics and gynecology, 1995, 172(2Pt 1):683–6.
10 Comparison of prostaglandin E2.pmd 8/17/2005, 11:07 AM553

554 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Low-dose quinine for treatment ofchloroquine-resistant falciparummalaria in Sudanese pregnant womenI. Adam,1 M.H. Ibrahim,1 I.A. A/elbasit 2 and M.I. Elbashir 2
1New Halfa Hospital, New Halfa, Sudan.2Faculty of Medicine, University of Khartoum, Khartoum, Sudan.Received: 14/07/03; accepted: 28/10/03
ABSTRACT Pregnant Sudanese women who presented at a hospital in eastern Sudan with chloroquine-resistant falciparum malaria were randomly allocated to one of two quinine regimens: low-dose (10 mg/kg 2times/day) (18 patients) or standard (10 mg/kg 3 times/day) (24 patients). Treatment was for 7 days andfollow-up for 28 days. Significantly fewer patients in the low-dose group reported vomiting and abdominal painthan the standard regimen group. Hypoglycaemia, preterm labour and recrudescence were slightly but notsignificantly higher in patients in the standard group than low-dose group. There were no significant differenc-es between the groups in the mean time from admission to remission of fever and parasite clearance. Wetentatively advocate the use of quinine 2 times/day to reduce side-effects and improve compliance.
Quinine à faible dose pour le traitement du paludisme à falciparum chloroquino-résistant chez desfemmes enceintes soudanaisesRÉSUMÉ Des femmes enceintes soudanaises atteintes de paludisme à falciparum chloroquino-résistant quiont consulté dans un hôpital du Soudan oriental ont été réparties de manière aléatoire entre les deuxschémas thérapeutiques de quinine suivants : faible dose, 10 mg/kg 2 fois/jour (18 patientes), ou standard,10 mg/kg 3 fois/jour (24 patientes). Le traitement durait 7 jours et le suivi 28 jours. Un nombre significative-ment moindre de patientes dans le groupe du traitement à faible dose a signalé des vomissements et desdouleurs abdominales par rapport aux patientes recevant le traitement standard. L’hypoglycémie, le travailprématuré et la recrudescence étaient légèrement, mais non significativement, plus élevés chez les pa-tientes du groupe du traitement standard que dans le groupe du traitement à faible dose. Il n’y avait aucunedifférence significative entre les deux groupes pour ce qui est du temps moyen entre l’admission, la rémis-sion de la fièvre et l’élimination du parasite. Nous recommandons provisoirement l’utilisation de la quininedeux fois par jour pour réduire les effets secondaires et améliorer l’observance du traitement.
11 Low-dose quinine.pmd 8/17/2005, 11:07 AM554

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 555
Introduction
In Sudan, falciparum malaria has been re-ported to cause a number of adverse mater-nal and fetal outcomes, such as maternalanaemia, low birth weight, preterm labourand perinatal mortality [1–6]. It is the lead-ing cause of maternal mortality [5,6].
The treatment of falciparum infectionremains the main means available to limitthe impact of malaria on pregnancy [7].The spread of chloroquine and sulfadox-ine–pyrimethamine resistance in Sudan [8–10] necessitates the use of alternative drugsfor the treatment of falciparum infections,such as quinine which is the second mostprescribed antimalarial drug in Sudan [11].Quinine is the treatment of choice for se-vere and chloroquine-resistant falciparummalaria.
The standard dose of quinine is 10 mg/kg, 3 times per day for 7 days [12]. Thisdose has been reduced effectively in chil-dren without impairing its efficacy, andwith marked improvement in compliancewith drug use [13]. The side-effects of qui-nine treatment that can lead to poor compli-ance are tinnitus, nausea, vomiting,diarrhoea, hypoglycaemia and acute hyper-sensitivity. Physicians in central and east-ern Sudan are now also giving quinine topregnant women 2 times daily rather than 3times, with apparently good outcomes. Thepresent study was carried out to verify theefficacy and safety of this ongoing clinicalpractice.
Methods
We performed a prospective clinical trial inNew Halfa Hospital in eastern Sudan fromthe period November 2002 to March 2003.After verbal consent, all pregnant womenpresenting with failure of chloroquine ther-apy for the treatment of falciparum malaria
were successively enrolled to the study.Those with one or more manifestations ofsevere falciparum malaria were excluded[14].
For both groups, quinine (LaboratoiresRenaudin, France) was given under strictsupervision, first by intravenous infusion in5% dextrose solution over 2–4 hours, andwhen the patient could tolerate it, therapywas continued orally in the form of tablets.For this phase of the study, patients wererandomized into 2 treatment groups: qui-nine 10 mg/kg 2 times/day for 7 days (BDgroup) and quinine 10 mg/kg 3 times/dayfor 7 days (TDS group).
A detailed record was made for eachpatient, including: personal data, medicaland obstetric history, physical examinationand use of antimalarials in the 3 weeks be-fore entry to the study. During the follow-up, all patients were asked daily about theexpected side-effects of quinine (tinnitus,vomiting and abdominal pain). Axillary tem-perature was recorded every 8 hours until itfell to normal (37.5 °C), and then daily untilday 7. All patients were kept in the hospitalfor at least 7 days and then followed upweekly in the antenatal clinic for 28 days.
Laboratory investigationsUsing finger prick blood samples, thick andthin blood smears were prepared from eachpatient in both groups, stained with Giemsa(pH 7.0, diluted in phosphate-buffered sa-line) and counted against 200 white bloodcells assuming that the number of cells is6000/mm3 of blood. Thin blood films, fixedin methanol and Giemsa-stained were madewhen the parasite species was doubtful.The blood films were repeated every 8hours until 2 consecutive films were nega-tive, then daily until day 7 and then on days14, 21 and 28. Haemoglobin concentrationand capillary blood glucose level were de-termined on presentation. Capillary blood
11 Low-dose quinine.pmd 8/17/2005, 11:07 AM555

556 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
glucose was estimated 2 hours after admin-istration of the drug.
All patients were resident in the samearea during the follow-up period. There-fore, the possibility of re-infection or re-crudescence could not be ruled out. Threespots of blood were taken on filter paperinitially and later if parasites reappeared mi-croscopically during the follow-up period.Primers from 3 polymorphic Plasmodiumfalciparum antigens; merozoite surfaceprotein-1 and 2 (MSP-1 and MSP-2) andglutamate-rich protein (GLURP) were usedin polymerase chain reaction analysis(PCR) to differentiate between true recru-descence and re-infection as described pre-viously [15].
Evaluation criteriaThe efficacy and side-effects of the 2 regi-mens of quinine were assessed accordingto parasite clearance time, fever clearancetime, occurrence of side-effects (tinnitus,vomiting, abdominal pain and hypoglycae-mia) and recrudescence. Parasite clearancetime was defined as the time between startof treatment until 2 consecutive negativeblood smears were obtained. Fever remis-sion time was defined as the time betweenadmission and achievement of normal bodytemperature.
StatisticsData was entered into the computer usingSPSS/PC batching for data analysis. Simplefrequency distribution cross-tabulation, de-scriptive statistics, mean, t-test and chi-squared with probability ≤ 0.05 was usedfor testing the hypotheses.
EthicsInformed consent was obtained from thewomen who participated in the study. Ethi-cal clearance for the study was obtainedfrom the Faculty Research Board, Faculty
of Medicine, University of Khartoum andthe National Ethical Committee at theSudanese Federal Ministry of Health.
Results
Sixty-five pregnant women presented toNew Halfa hospital with manifestations ofchloroquine-resistant falciparum malariaduring the study period. After confirmationof the infection, 14 patients were excludedfrom the study because they had severemanifestations of the disease. Initially, 25patients were enrolled in the BD group, and26 patients in the TDS group. However, 7/25 of the BD and 2/26 of the TDS group (P= 0.05) were excluded from the follow-upand evaluation as they chose to leave hospi-tal and continue the treatment at home afterthe first or the second dose of quinine.
Table 1 shows the major characteristicsof the remaining women on presentation.There were no significant differences be-tween the 2 groups in age, parity, weight,temperature, haemoglobin level, parasitecount and random blood glucose level atpresentation.
A slightly higher proportion of womenin the BD group presented with vomitingthan the TDS group—4/18 (22.2%) versus3/24 (12.5%)—but this was not statistical-ly significant. On day 1, vomiting was re-corded in more BD patients; 7/18 (38.9%)versus 4/24 (16.7%) but this was not sta-tistically significant (P > 0.05). On day 2,significantly fewer patients in the BD thanthe TDS suffered from vomiting; 29/18(50.0%) versus 9/24 (79.2%) (P < 0.05).
Tinnitus was reported slightly less fre-quently by patients who received quinineBD, than in those who received it TDS; 12/18 (66.7%) versus 19/24 (79.2%) (P >0.05). Significantly fewer patients reportedabdominal pain in the BD group than in the
11 Low-dose quinine.pmd 8/17/2005, 11:07 AM556

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 557
TDS group, 1/18 (5.6%) versus 7/24(29.2%) (P = 0.05). Some of the TDSgroup developed hypoglycaemia; 4/24(16.7%), but this was not recorded in anypatient in the BD group (0/18); this differ-ence was not significant (P > 0.05).
While none of the patients in the BD de-livered prematurely (< 37 weeks), 2/24(8.3%) patients in the TDS group deliveredprematurely at 29 and 30 weeks gestationalage and their babies died immediately (P >0.05).
True recrudescence was confirmed byparasite genotyping on days 21 and 28 in 2/18 (11.1%) patients among the BD group.They were successfully treated withsulfadoxine–pyrimethamine. There was nodetectable parasitaemia during follow-up inthe TDS group, but this difference was notsignificant (P > 0.5).
The mean (SD) parasite clearance timewas lower in the BD than in the TDSgroup, but this did not reach the level ofsignificance: 27.2 (12.9) versus 33.7(12.7) hours.
Discussion
This is the first study of the efficacy oflow-dose quinine in the treatment of chlo-roquine-resistant falciparum malaria duringpregnancy in an area of high chloroquineresistance in eastern Sudan [8].
The study showed that significantlymore patients chose to continue the quininetreatment at home in the BD than in theTDS group and this may reflect the sim-plicity of this regimen. Moreover, quinineside-effects were reported more frequently
Table 1 Characteristics on admission and outcomes of treatment for pregnantwomen treated with quinine 10 mg/kg 2 times/day (BD) or 10 mg/kg 3 times/day(TDS)
Variable BD regimen TDS regimen P-value(n = 18) (n = 24)
Mean SD Mean SD
On admissionAge (years) 25.2 6.0 25.5 6.9 0.4Parity (No.) 2.6 1.9 2.6 2.2 0.3Weight (kg) 59.3 15.9 52.2 9.3 0.09Gestational age (weeks) 26.1 9.9 26.1 8.9 0.4Axillary temperature (°C) 38.1 0.9 37.8 1.0 0.8Haemoglobin level (g/L) 89.0 5.6 86.0 9.0 0.08Parasite count (rings/µL) 5837 8361 4207 12325 0.6Random blood sugar level (mg/dL) 117.6 30.1 106.5 25.7 0.9
Treatment outcomesFever remission timea (hours) 25.5 12.1 21.0 16.9 0.13Parasite clearance timeb (hours) 27.7 12.9 33.7 12.7 0.63
aFever remission time was defined as the time between admission and achievement ofnormal body temperature (37.5 °C). bTime from admission and start of treatment until 2 consecutive negative blood smearswere obtained.SD = standard deviation.
11 Low-dose quinine.pmd 8/17/2005, 11:07 AM557

558 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
in the TDS group than in the BD group; sig-nificantly more patients suffered fromvomiting and abdominal pain in the TDSgroup than in the BD group. Although theseside-effects were more frequent in theTDS than in the BD group, they might beconsidered a subjective assessment ofthese 2 regimens of quinine. Nevertheless,even objective side-effects were more fre-quent in the TDS than in the BD group. Forexample, hypoglycaemia was seen in moreof the patients in the TDS group than theBD group (16.7% versus 0%) although thedifferent not significant. However, hy-poglycaemia was reported in around 50%of pregnant women at one stage or anotherof severe falciparum malaria treated withquinine 3 times/day for 7 days [16], there-fore, hypoglycaemia may be dose related.In a recent study, a low dose of quininewas used in children in a community-basedstudy but hypoglycaemia was not assessed[13].
Two patients in the TDS group deliv-ered prematurely and their babies died im-mediately, but there was no prematuredelivery in the BD group. In a previousstudy where we were testing the efficacyof quinine 3 times/day in the treatment ofsevere falciparum malaria during pregnan-cy in central Sudan, 3/33 (9%) patients de-livered prematurely, and only 1 patientdelivered during quinine therapy [4]. Thiscomparison should be viewed with cautionbecause in the previous study we used qui-nine for severe illness, while such patientswere excluded in the present study. How-ever, no preterm labour was reported byMcGready et al. in 1998 [17]. Malaria cancause abortion and preterm labour as well,
and in central Sudan it was found to be theleading cause of low birth weight as a resultof preterm labour [3]. However, the oxyto-cic effect of quinine on the pregnant uteruscannot be excluded totally. Previously, qui-nine was used as a labour-inducing agentbut in high doses [18].
The parasite clearance time was shorterbut not significantly so in the BD groupthan in the TDS group. However, 2 patients(11.1%) in the BD group showed true para-site recrudescence during the follow-up,compared with none of the patient in theTDS group. This difference was not statis-tically significant and it should be viewedwith caution as it might be due to quinineresistance in this area of Sudan. Previously,we have observed quinine resistance by invivo testing and it has been confirmed by invitro testing in a nearby area [8,19]. Wehave previously shown 6% quinine resis-tance or re-infection during pregnancy incentral Sudan [4].
In conclusion, quinine in a low-doseregimen of 2 times/day causes fewer sub-jective side-effects and therefore is likely toimprove patient compliance than the stan-dard 3 times/day regimen. It also has alower risk of hypoglycaemia (which is im-portant in the outpatient setting) and of pre-term labour. Its disadvantage is the higherprobability of recrudescence, which is im-portant in the light of emerging resistancein Africa, where the drug is still the first linefor the treatment of severe falciparum ma-laria. However, there is an urgent need totest and apply other alternative drugs, espe-cially sulfadoxine–pyrimethamine combi-nation, which is free of side-effects suchas hypoglycaemia and preterm labour.
References
1. Ahmed SM et al. Malaria parasitemiaduring delivery. Saudi medical journal,2001, 23:684–8.
2. Taha TE et al. Levels and determinants ofperinatal mortality in Central Sudan. In-
11 Low-dose quinine.pmd 8/17/2005, 11:07 AM558

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 559
ternational journal of gynaecology andobstetrics, 1994, 45:109–15.
3. Taha TE et al. Malaria and low birthweight in central Sudan. American jour-nal of epidemiology, 1993, 138:318–25.
4. Adam et al. Quinine therapy in severePlasmodium falciparum malaria duringpregnancy in Sudan. Eastern Medi-terranean health journal, 2004, 10(1/2):159–66.
5. Maternal mortality in Sudan. Inter-re-gional meeting on the prevention ofmaternal mortality, Geneva 11–15 No-vember, 1985. Geneva, World HealthOrganization, 1985 (Unpublished docu-ment FHE/PMM/85.95).
6. Dafallah SE, El-Agib FH, Bushra GO.Maternal mortality in a teaching hospitalin Sudan. Saudi medical journal, 2003,24:369–73.
7. Dolan G et al. Bed nets for the preventionof malaria and anaemia in pregnancy.Transactions of the Royal Society ofTropical Medicine and Hygiene, 1993;87:620–6.
8. Adam I et al. In the Sudan: chloroquineresistance is worsening and quinine re-sistance is emerging. Sudan medicaljournal, 2001, 39:1–5.
9. Elkheir HK et al. Efficacy of sulphadoxineand pyrimethamine, doxycycline andtheir combination in the treatment ofchloroquine resistant falciparum ma-laria. Saudi medical journal, 2001, 228:690–3.
10. Adam I et al. Efficacy of sulfadoxine-py-rimethamine in the treatment of uncom-plicated Plasmodium falciparum malariain a small sample of Sudanese children.Eastern Mediterranean health journal,2004, 10(3):309–14.
11. Yousif MA, Adeel AA. Antimalarial pre-scribing pattern in Gezira State: precepts
and practice. Eastern Mediterraneanhealth journal, 2000, 6:939–47.
12. World Health Organization, Division ofControl of Tropical Diseases. Severe andcomplicated malaria. Transactions of theRoyal Society of Tropical Medicine andHygiene, 1990, 84(suppl.2):1–65.
13. Kofoed PE et al. Treatment of Plasmo-dium falciparum malaria with quinine inGuinea-Bissau: one daily dose is suffi-cient. Transactions of the Royal Societyof Tropical Medicine and Hygiene, 2002,96:185–8.
14. World Health Organization, Comm-unicable Diseases Cluster. Severefalciparum malaria. Transactions of theRoyal Society of Tropical Medicine andHygiene, 2000, 94(suppl.1):S1–90.
15. Brockman A et al. Application of geneticsmarker to the identification of recrudes-cent P. falciparum infection on the North-Western border of Thailand. Americanjournal of tropical medicine and hy-giene, 1999, 60:14–21.
16. Looareesuwan S et al. Quinine and se-vere falciparum malaria in late preg-nancy. Lancet, 1985, 2:4–8.
17. McGready R et al. Quinine and meflo-quine in the treatment of multidrug-resis-tant Plasmodium falciparum malaria inpregnancy. Annals of tropical medicineand parasitology, 1998, 92:643–53.
18. Mukherjee S, Bhose LN. Induction oflabour and abortion with quinine infu-sion in intrauterine fetal deaths. Ameri-can journal of obstetrics and gyneco-logy, 1968, 101:853–4.
19. Khalil IF. Sensitivity of chloroquine resis-tant Plasmodium falciparum to fansimef,mefloquine and halofantrine in Gadaref,eastern Sudan [MSc thesis]. Khartoum,Sudan, University of Khartoum, 1995.
11 Low-dose quinine.pmd 8/17/2005, 11:07 AM559

560 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Quinine for chloroquine-resistantfalciparum malaria in pregnantSudanese women in the first trimesterI. Adam1, H.M. Idris1 and M.I. Elbashir 2
1New Halfa Hospital, New Halfa, Sudan.2Faculty of Medicine, University of Khartoum, Khartoum, Sudan.Received: 14/07/03; accepted: 28/10/03
ABSTRACT A prospective clinical study in eastern Sudan described the efficacy and toxicity of quinine inearly pregnancy in mothers with chloroquine-resistant falciparum malaria. Twenty-six pregnant Sudanesewomen in their first trimester (mean gestational age 8.5 weeks) were given quinine 10 mg/kg 3 times per dayfor 7 days and followed up every 2 weeks until delivery. One patient aborted (3.8%) and 2 patients (7.7%)experienced threatened abortion but delivered term babies. Recrudescence or re-infection was observed onday 21 in 1 patient. One baby died aged 6 months. There were no detectable congenital malformations, noauditory or visual defects or any other neurological deficits in the remaining infants at birth or 1 year later.Quinine may be safe in the first trimester of pregnancy.
La quinine pour le paludisme à falciparum chloroquino-résistant chez des femmes enceintessoudanaises durant le premier trimestre de la grossesseRÉSUMÉ Une étude clinique prospective au Soudan oriental a décrit l’efficacité et la toxicité de la quinine audébut de la grossesse chez des mères atteintes de paludisme à falciparum résistant à la chloroquine. On aadministré de la quinine à raison de 10 mg/kg trois fois par jour pendant 7 jours à vingt-six femmes enceintessoudanaises durant le premier trimestre de la grossesse (âge gestationnel moyen de 8,5 semaines) etcelles-ci ont été suivies toutes les 2 semaines jusqu’à l’accouchement. Une patiente a avorté (3,8 %) et2 patientes (7,7 %) ont débuté une menace d’avortement mais ont mis au monde leur bébé à terme. Unerecrudescence ou une réinfection a été observée au 21e jour chez une patiente. Un bébé est décédé à l’âgede six mois. Il n’y avait aucune malformation congénitale décelable, aucun handicap visuel ou auditif ou autredéficit neurologique chez les autres enfants à la naissance ou un an plus tard. La quinine peut être con-sidérée comme sans danger durant le premier trimestre de la grossesse.
12 Quinine for chloroquine.pmd 8/17/2005, 11:07 AM560

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 561
Introduction
Malaria is a major health problem in tropicalcountries especially sub-Saharan Africa,where about 90% of clinical cases occur.There are nearly 500 million clinical casesof malaria worldwide each year and 1.1 to2.7 million people die annually [1]. In areaswhere malaria transmission is seasonal, asin eastern Sudan, there is low transmissionand hence low immunity. In Sudan, preg-nant women are particularly vulnerable tofalciparum malaria; the disease has adverseeffects on pregnancy, affecting all parities[2,3], and all manifestations are seen in-cluding cerebral malaria and haemoglobin-uria [4]. In central Sudan, falciparummalaria was found to be the leading causeof low birth weight, maternal anaemia andmaternal and perinatal mortality [5–7].
Plasmodium falciparum isolates fromeastern Sudan show the highest levels ofantimalarial drug resistance in the countrywith a rate of chloroquine resistanceamong isolates of 76% [8,9]. This situationnecessitates the use of alternative antima-larial drugs for the treatment of falciparummalaria. Quinine the drug of choice for se-vere falciparum malaria in Sudan.
Worldwide, very few studies have beenmade on the safety of quinine therapy dur-ing early pregnancy [10,11]. Quinine haslong been believed to induce abortion andlabour [12]; however, malaria itself canalso lead to abortion, while quinine, by low-ering fever, may in fact be helpful [13].This is important as the treatment ofchloroquine-resistant falciparum malaria inpregnancy is complicated by the poor safe-ty of other drugs, as both artemether andsulphadoxine-pyrimethamine are reportedto cause fetal resorption when given in ear-ly pregnancy [14,15].
In the light of the emerging multi-drugresistance in malaria-endemic areas, we de-scribe here the efficacy and toxic effects of
quinine on a small group of women withchloroquine-resistant malaria in early preg-nancy and its outcome on the infants at 1-year follow-up.
Methods
PatientsThe study was carried in New Halfa Hospi-tal, eastern Sudan, between October 2000and November 2002. The study groupwere all pregnant women in their first tri-mester of pregnancy with symptoms offalciparum malaria and failure to respond tochloroquine. Patients presenting with vagi-nal bleeding were excluded. The womenwere asked specifically about symptomssuggestive of malaria (fever, headache,sweating, joint pain and vomiting). Physicalexamination was performed and all infor-mation was kept in case report format.
InvestigationsPeripheral capillary blood smears were pre-pared, stained with Giemsa and examinedunder oil immersion for parasites. Parasitesand leukocytes were counted in the samefields until 200 leukocytes were counted;parasites densities were estimated using anassumed leukocyte count of 6000 leuko-cytes/µL blood. Baseline investigations(haemoglobin, urea, creatinine, albuminand bilirubin levels) were also performed.
Ultrasound was performed initially toconfirm the pregnancy, gestational age andviability of the fetus, and repeated every 4–6 weeks for placental localization and toexclude congenital malformations.
Treatment and follow-upThe women were treated with quinine(Laboratoires Renaudin, France) at a doseof 30 mg salt/kg/day for 7 days. It was giv-en at first by intravenous infusion in 5%dextrose solution over 2–4 hours, and
12 Quinine for chloroquine.pmd 8/17/2005, 11:07 AM561

562 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
when the patient could tolerate it, therapywas continued orally in the form of tablets.
The patients were discharged aftercompleting the full dose of quinine on day8, then seen on days 14, 21, 28, and every2 weeks in the antenatal clinic until deliv-ery. In the clinic they were examined by theobstetrician for weight, pallor, temperature,pulse, blood pressure, fundal level, fetalheart sounds and oedema. At every visit thepatient’s haemoglobin was estimated andblood films for malaria were taken. Theobstetrician supervised all hospital deliver-ies and kept close links with those who de-cided to deliver at home.
A paediatrician examined all the infantsat birth for congenital malformations andmade all necessary anthropometric mea-surements. Infants, both hospital- andhome-delivered, were followed up to 1 yearof age by the same paediatrician.
DefinitionsChloroquine-resistance was defined as thedetection of P. falciparum malaria parasitesin peripheral blood after a complete courseof chloroquine. Abortion was defined asexpulsion of a dead fetus before 28 weeksof gestation. Premature labour was deliveryafter 28 weeks and before 37 weeks ofgestation. Perinatal death was death of thebaby from 28 weeks in utero until the ageof 1 week post-delivery.
AnalysisData were analysed using SPSS/PC. Simplefrequency distributions, percentages,means and standard deviations were calcu-lated.
EthicsThe study received ethical clearance fromthe Faculty Research Board at the Facultyof Medicine, University of Khartoum andthe Federal Ministry of Health. Written con-
sent for participation in the study was ob-tained from the patients and their husbands.
Results
Out of 28 patients, 26 pregnant Sudanesewomen in their first trimester were givenquinine to treat falciparum malaria afterfailure of chloroquine treatment. Two pa-tients were excluded because they present-ed with vaginal bleeding. Fever, nausea,vomiting, headache, giddiness and insom-nia were the major presenting symptoms.Table 1 shows the main clinical and bio-chemical data at the time of presentation.
During quinine treatment, 1 patient(2.8%) developed vaginal bleeding and ab-dominal pain. After the third dose of qui-nine, the cervix was found to be open,implying inevitable abortion, and evacua-tion was carried out. Two more patients(7.7%) developed slight vaginal bleeding,i.e. threatened abortion, during quinine
Table 1 Major clinical and laboratory findingson admission in 26 pregnant women withchloroquine-resistant malaria
Parameter Mean SD
Age (years) 26.2 3.5
Parity (No.) 2.8 2.6
Gestational age (weeks) 8.5 0.9
Weight (kg) 65.8 4.6
Temperature (°C) 38.2 0.6
Haemoglobin (g/dL) 9.2 1.3
Parasite count (rings/µL)a 5856 1652
Blood glucose (mg/dL) 123.6 12.9
Blood urea (mg/dL) 27.3 3.6
Serum bilirubin (mg/dL) 1.09 0.12
aGeometric mean.SD = standard deviation.
12 Quinine for chloroquine.pmd 8/17/2005, 11:07 AM562

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 563
therapy on day 2 and 3 respectively, buttheir pregnancies continued until the deliv-ery of term babies.
All patients had negative blood films onday 7. However, 1 patient presented on day21 with recurrence of malaria symptomsand the blood film was positive for falci-parum malaria parasites. She was readmit-ted at the 10th week of gestation and givenartemether intramuscularly, 80 mg initiallyfollowed by 80 mg after 12 hours and thendaily for 4 days. She was discharged aftercompleting the treatment with full recoveryand was followed up closely until delivery.
Just under half the patients (12/26,46.2%) delivered in the hospital, the rest(14/26, 53.8%) delivered at home. Themean (SD) birth weight of babies whosemothers delivered at hospital was 2.9(0.4) kg.
One of the babies died at home at theage of 6 months due to unexplained febrileillness. There were no detectable congenitalmalformations and no auditory, visual orother neurological deficits in the remaininginfants at birth or 1 year later.
Discussion
Pregnant women are more susceptible tomalaria infection which can lead to manyadverse effects on the pregnancy such asabortion, premature labour and maternalanaemia [3]. The World Health Organiza-tion recommends that pregnant womenwith demonstrable malaria illness shouldreceive prompt treatment with effectiveand safe antimalarial drugs [16]. This situa-tion is limited by the safety profile of anti-malarial drugs themselves [14,15] and thespread of chloroquine-resistant strains ofP. falciparum.
In this study, 1 patient showed reap-pearance of the parasite on day 21, whichmight due to re-infection or parasite resis-
tance to quinine therapy. In Sudan, resis-tance to chloroquine has been recorded inalmost every region of the country andeven quinine resistance has been shown byin vivo and in vitro tests in the area of thestudy and in a nearby area [8,17]. We havepreviously observed that quinine failed totreat 2/33 (6%) of pregnant women in cen-tral Sudan [4]. This phenomenon warrantsmore investigations since quinine is still thefirst line of treatment for severe falciparummalaria in Africa.
One patient aborted and 2 patientsthreatened to abort but their pregnanciescontinued until term. This agrees withMcGready and colleagues’ report of qui-nine in early pregnancy [11], where the rateof abortion was not different from the pop-ulation in our community. In a recent com-munity-based study of risk factors foranaemia in our area, around 50% of womengave a history of previous abortion [18].We have previously observed that no pa-tient aborted among 33 patients treatedwith quinine for severe falciparum malariain central Sudan [4]. However, in that study3 patients delivered prematurely, 1 of themduring the quinine therapy. In another 2studies there was no effect of quinine onthe rate of abortion or preterm labour[19,20]. In the latter studies the patientspresented later in pregnancy (the gestation-al age was > 20 weeks) and this might ex-plain the rate of abortion (1/26, 3.8%) inthe present study where quinine was usedin early pregnancy. There are difficulties ininterpreting the findings of abortion, be-cause malaria itself is a known cause ofabortion especially during epidemics [21].Certainly in our study, 2 out of 28 malariapatients presented with vaginal bleedingand their pregnancies aborted before qui-nine was started (these women were ex-cluded from the study). Quinine has longago been reported to induce abortion and
12 Quinine for chloroquine.pmd 8/17/2005, 11:07 AM563

564 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
labour [12] and we believe that this hasbeen influential in limiting the use of quinineduring pregnancy. The situation remainedso until in 1985 it was declared that malariaand its fever were responsible for abortion,while quinine, by lowering temperature,may in fact decrease the amplitude of uter-ine contractions as confirmed by fetalmonitoring [13].
In our study, we found no hearing orvisual defects and no congenital or devel-opmental abnormalities in the infants after 1year. This confirms another recent study[11]. However, deafness and hypoplasia ofthe optic nerve have been described in chil-dren born after unsuccessful attempts toinduce abortion in women taking quinine
overdoses [22]. These were retrospectivereports and the exact numbers of patientswere not known.
In conclusion, our study and that ofMcGready and colleagues [11] suggeststhat quinine could be used safely as a cost-effective therapy during the first trimesterof pregnancy.
Acknowledgements
The authors thank the women who partici-pated in the study, Mrs Asma Abd Elwakeil,Mr Abdalla Ahmed Hafazalla for technicalassistance, and the staff of New Halfa Hos-pital for support and cooperation.
References
1. WHO expert committee on malaria: twen-tieth report. Geneva, World Health Orga-nization, 2000 (WHO Technical ReportSeries No. 892).
2. Brabin BJ et al. A study of the conse-quences of malaria infection in pregnantwomen and their infants Parassitologia,1993, 35(suppl.):9–11.
3. Nosten F et al. Malaria during pregnancyin an area of unstable endemicity. Trans-actions of the Royal Society of TropicalMedicine and Hygiene, 1991, 85:424–9.
4. Adam I al. Quinine therapy in severePlasmodium falciparum malaria duringpregnancy in Sudan. Eastern Mediterra-nean health journal, 2004, 10(1/2):159–66.
5. Taha Tel T, Gray RH, Mohamedani AA.Malaria and low birth weight in centralSudan. American journal of epidemiol-ogy, 1993, 138:318–25.
6. Ahmed SM et al. Malaria parasitemiaduring delivery. Saudi medical journal.2001, 23:684–8.
7. Taha TE et al. Levels and determinants ofperinatal mortality in central Sudan. In-ternational journal of gyneacology andobstetrics, 1994, 45:109–15.
8. Adam I et al. In the Sudan: chloroquineresistance is worsening and quinine re-sistance is emerging. Sudan medicaljournal, 2001, 39:5–11.
9. Babiker HA et al. Genetic diversity ofPlasmodium falciparum in a village inEastern Sudan. 2. Drug resistance, mo-lecular karyotypes and the mdr1 geno-type of recent isolates. Transactions ofthe Royal Society of Tropical Medicineand Hygiene, 1991, 85:578–83.
10. Heinonen OP, Slone D, Shapiro S. Birthdefects and drugs in pregnancy. Little-ton, Massachusetts, Publishing Sci-ences Group, 1977.
11. McGready R et al. The effects of quinineand chloroquine antimalarial treatmentin the first trimester of pregnancy. Trans-actions of the Royal Society of TropicalMedicine and Hygiene, 2002, 96:180–4.
12 Quinine for chloroquine.pmd 8/17/2005, 11:07 AM564

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 565
12. Mukherjee S, Bhose LN. Induction oflabour and abortion with quinine infu-sion in intrauterine fetal deaths. Ameri-can journal of obstetrics and gyneco-logy, 1968, 101:853–4.
13. Looareesuwan S et al. Quinine and se-vere falciparum malaria in late preg-nancy. Lancet, 1985, 2:4–8.
14. Briggs GC, Freeman RK, Yaffe SJ, eds.Drugs in pregnancy and lactation, 2nded. Baltimore, William and Wilkins, 1986:537–53.
15. Uche-Nwachi EO, Caxton-Martins AE.Sulfadoxine–pyrimethamine embryopa-thy in Wistar rats. Kaibogaku zasshi,1998, 73:135–9.
16. WHO expert committee on malaria: eigh-teenth report. Geneva, World Health Or-ganization, 1986:57–78 (WHO TechnicalReport Series, No. 735).
17. Khalil IF. Sensitivity of chloroquine resis-tant Plasmodium falciparum to fansimef,mefloquine and halofantrine in Gadaref,eastern Sudan [MSc thesis]. Khartoum,Sudan, University of Khartoum, 1995.
18. Adam I et al. Anemia in pregnant Suda-nese women: community based study.Saudi medical journal, 2004, 25:447–8.
19. McGready R et al. Quinine and meflo-quine in the treatment of multidrug-re-sistant Plasmodium falciparum malariain pregnancy. Annals of tropical medi-cine and parasitology, 1998, 92:643–53.
20. McGready R et al. Randomized compari-son of mefloquine–artesunate versusquinine in the treatment of multidrug-re-sistant falciparum malaria in pregnancy.Transactions of the Royal Society ofTropical Medicine and Hygiene, 2000,94:689–93.
21. Menon R. Pregnancy and malaria. Medi-cal journal of Malaysia, 1972, 27:115–9.
22. Studies on the toxicity of qinghaosu andits derivatives. China Cooperative Re-search Group on qinghaosu and its de-rivatives as antimalarials. Journal oftraditional Chinese medicine, 1982, 2:31–8.
12 Quinine for chloroquine.pmd 8/17/2005, 11:07 AM565

566 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Impact of the national protocol formalaria treatment on prescribingpatterns in Gezira state, Sudan M.E. Ahmed1 and M.A. Yousif 2
1Department of Community Medicine, Faculty of Medicine; 2Faculty of Pharmacy, University of Gezira,Gezira, Sudan.Received: 08/08/02; accepted: 18/08/03
ABSTRACT A cross-sectional study to assess the impact of the national protocol for malaria treatment wasconducted in a town in Gezira state, central Sudan, in 2001. Most of the 165 doctors and medical assistantsinterviewed (80.0%) had not been trained in the protocol and many (57.5%) were still using their ownprotocols. Analysis of 410 prescriptions showed chloroquine was the most common antimalarial drug used(69.5% of prescriptions). Compared with a study before implementation of the protocol, more prescriptionsmet the protocol standards for correct chloroquine dose, whereas regimens for administration of intrave-nous quinine were still inadequate. The study showed a lack of continuous supervision, training and follow-up in the protocol guidelines and negative attitudes of hospital specialists towards the protocol.
Impact du protocole national de traitement du paludisme sur les modes de prescription dans l’Étatde Gezira (Soudan)RÉSUMÉ Une étude transversale a été réalisée dans une ville de l’État de Gezira (Soudan central) en 2001afin d’évaluer l’impact du protocole national pour le traitement du paludisme. La plupart des 165 médecins etauxiliaires médicaux interrogés (80,0 %) n’avaient pas été formés à l’utilisation du protocole et beaucoup(57,5 %) utilisaient toujours leur propre protocole. L’analyse de 410 ordonnances a montré que la chloroquineétait l’antipaludique le plus couramment utilisé (69,5 % des ordonnances). Par rapport à une étude effectuéeavant l’application du protocole, un plus grand nombre d’ordonnances se conformaient aux normes duprotocole concernant la dose correcte de chloroquine, alors que les schémas d’administration de quinine parvoie intraveineuse demeuraient inappropriés. L’étude a montré un manque de supervision continue, deformation et de suivi pour les directives du protocole et des attitudes négatives des spécialistes hospitaliersvis-à-vis du protocole.
13 Impact of the national.pmd 8/17/2005, 11:07 AM566

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 567
Introduction
Sudan has contributed to and endorsed theWorld Health Organization (WHO) globalstrategy for malaria control and ‘Roll backmalaria’. It has been observed that, unlessdiagnosed and treated promptly, patientswith malaria deteriorate rapidly and the out-come is grave; hence plans to formulate anational protocol for the treatment of ma-laria were a priority in Sudan [1]. The na-tional protocol is a set of recommendationsand regulations concerning antimalarialdrugs and their utilization in a country. Itdefines the national malaria control policyand forms part of the national drug policy,which expresses and prioritizes themedium- to long-term goals set by the gov-ernment for the pharmaceutical sector. Thenational drug policy is both a commitmentto a goal and a guide for action, identifyingthe main strategies for attaining them, andproviding a framework within which theactivities of the pharmaceutical sector canbe coordinated [2].
The idea of formulating an antimalarialdrug policy was encouraged in Sudanthrough a coordinated effort between theDirectorate of Malaria, the Federal Ministryof Health and WHO. A preliminary work-shop of consultants was held in the Facultyof Medicine, University of Gezira, in April1998, followed by a national committee inJune 1998, which finalized the policy underevaluation [1].
A study of antimalarial drug prescribingpatterns was carried out in Wad Medanitown in Gezira state before the implementa-tion of the protocol in 1999 [3]. The studyshowed poor standards of prescribing ofantimalarial drugs, in terms of over-prescribing of chloroquine tablets and in-correct regimens for intravenous adminis-tration of quinine. The same study revealedthat most of the medical practitioners tend-
ed to follow their own regimens to treatmalaria infection.
The present study is the first attempt tomeasure the influence of the national proto-col on prescribing patterns in the samearea. It is important to make an evaluationof knowledge, attitudes and practices ofhealth providers towards the national pro-tocol, so that unintended consequences orconstraints can be identified and successfulinterventions and strategies reinforced.
Methods
This cross-sectional study was carried outin Wad Medani, a town situated in Gezirastate in central Sudan. The study was con-ducted in October, the month in which anormal rise of malaria infection is annuallyobserved.
The research process consisted of 3steps. The first step was an interview withthe state director of the malaria control pro-gramme. In the second step, we contactedall 181 doctors and medical assistants(from both public and private sectors) whowere providing medical services in thetown; 165 were available for interview.Questions were asked to assess theirknowledge, attitudes and practices relatingto the national protocol. In the third step, asample of 6 pharmacies was selected usingstratified random sampling from 3 strata.Over 3 consecutive days, 410 prescriptionsfrom both general practitioners and hospitaloutpatients departments were collected anda pre-tested checklist was filled in to assesstheir conformity to the protocol standardsof drug dosage, frequency of administra-tion, etc.
Standard treatment regimens at thattime according to the Malaria Administra-tion Department of the Federal Ministry ofHealth were as follows.
13 Impact of the national.pmd 8/17/2005, 11:07 AM567

568 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
• First line treament for simple malaria:chloroquine oral 25 mg/kg over 3 days.For chloroquine injection of adults: 1ampoule (200 mg base) followed by 1ampoule after 6 hours then 2 times perday (12 hours apart) for a total of 7 in-jections. For chloroquine injection ofchildren: 2.5–3.5 mg/kg.
• Second line treatment: pyrimethamine-sulfadoxine, 25/500 mg. For adults: 3tablets at once. For children: accordingto weight.
• Third line treatment: mefloquine or qui-nine.
The data were tabulated and analysed usingSPSS.
Results
Interview with state directorThe interview with the state director of themalaria control programme revealed that 6training courses had been conducted for145 doctors and medical assistants over a2-year period. The 3-day training sessions,which were run at 2 different centres, cov-ered the epidemiology, clinical picture andtreatment of malaria according to the na-tional protocol guidelines. The protocolguidelines had been distributed to all healthworkers after training, but neither continu-ous supervision nor surveys to assess theimplementation of the protocol had beencarried out by the malaria control pro-gramme.
Interviews with health workersOverall, the majority of the 165 healthworkers interviewed (132, 80.0%) report-ed that they had not received training aboutthe national protocol guidelines. None ofthe 58 house officers or 25 consultants hadbeen trained. No training had been receivedby 88.8% of hospital registrars, 64.0% of
medical assistants or 52.0% of generalpractitioners. A significant difference wasobserved in the training status among dif-ferent categories of health worker (Table1).
With regard to the level of awareness ofthe protocol, around two-thirds of thehealth workers (107, 64.8%) were awareof the guidelines. Hospital house officershad the lowest level of awareness (37.9%).The difference was significant across dif-ferent categories of health worker (Table1). Regarding the availability of the guide-lines, only 5 health workers (3.0%) report-ed having it in their clinic at the time of thestudy.
Adherence to the protocol was checkedby asking the health workers what regi-mens they used for the treatment of simplemalaria and complicated malaria comparedto the standard regimens recommended bythe Malaria Administration at the Ministryof Health. Despite the relatively high rate ofawareness, just over half of the interviewedhealth workers (95, 57.5%) showed no ad-herence to the protocol, with a significantdifference between the different categories(Table 1). When asked about reasons fornot adhering to the protocol guidelines,one-third of health workers mentioned lackof awareness of them (Table 2). Among thesenior hospital staff, however, it was due tonegative attitudes towards the protocol,since 72.0% of consultants and 100% ofregistrars claimed that the protocol was in-effective. Some health workers (11.5%)said that they did not adhere to the guide-lines in order to satisfy patients.
When evaluating the impact of the train-ing on the adherence to the protocol guide-lines a significant difference was observed.The 33 trained staff were more likely toadhere to the protocol (60.6% adhering)than the 132 untrained staff (only 37.9%adhering) (χ2 = 4.691, P < 0.05).
13 Impact of the national.pmd 8/17/2005, 11:07 AM568

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 569
Table 1 Training in, awareness of and adherence to the guidelines of the Sudan nationalprotocol of malaria treatment according to type of health worker
Variable Medical GPs House Registrars Consultants Totalassistants (n = 48) officers (n = 9) (n = 25) (n = 165)
(n = 25) (n = 58)No. % No. % No. % No. % No. % No. %
Trained aboutguidelines 9 36.0 23 48.0 0 0 1 11.2 0 0 33 20.0
Not trained aboutguidelines 16 64.0 25 52.0 58 100.0 8 88.8 25 100.0 132 80.0
χ2 = 48.58, P < 0.01
Aware ofprotocol 18 72.0 36 75.0 22 37.9 9 100.0 22 88.0 107 64.8
Not awareof protocol 7 28.0 12 25.0 36 62.1 0 0 3 12.0 58 35.2
χ2 = 31.92, P < 0.01
Adhering toprotocol 10 40.0 30 62.5 19 32.8 4 44.4 7 28.0 70 42.4
Not adheringto protocol 15 60.0 18 37.5 39 67.2 5 55.6 18 72.0 95 57.5
χ2 = 12.34, P = 0.015
n = total number of respondents.GPs = general practitioners.
Table 2 Reasons given by the health workers for not adhering to the guidelines of thenational protocol of malaria treatment (those adhering gave hypothetical answers)
Variable Medical GPs House Registrars Consultants Totalassistants (n = 48) officers (n = 9) (n = 25) (n = 165)
(n = 25) (n = 58)No. % No. % No. % No. % No. % No. %
Lack of awarenessof protocol 10 40.0 16 33.3 30 51.7 0 0 0 0 56 33.9
Believe protocol ineffective 5 20.0 24 50.0 19 32.8 9 100.0 18 72.0 75 45.5
Better patientsatisfaction 4 16.0 8 16.7 7 12.1 0 0 0 0 19 11.5
Others 6 24.0 0 0 2 3.4 0 0 7 28.0 15 9.1
n = total number of respondents.GPs = general practitioners.
13 Impact of the national.pmd 8/17/2005, 11:07 AM569

570 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Prescription analysisOut of 410 prescriptions, 128 were for an-timalarial drugs (31.2%). Most (91) werewritten by general practitioners, 11 bymedical assistants, and 26 by consultants.Overall, 102 (79.7%) of antimalarial drugprescriptions were judged to be adequate interms of correct dosage according to theprotocol. No significant difference wasobserved between different specialtiesregarding correct dosage; 80.2% of pre-scriptions from GPs followed the protocol,72.2% from medical assistants and 80.8%from consultants.
Chloroquine was the most commonlyprescribed antimalarial drug (89 prescrip-tions, 69.5%), followed by quinine (22,17.2%), pyrimethamine-sulfadoxine (13,10.2%), artemether (2, 1.6%), halofantrine(1, 0.8%) and primaquine (1, 0.8%).
The proportion of antimalarial drug pre-scriptions that correctly complied with theprotocol recommendations showed that in-tramuscular quinine was the formulationmost often prescribed incorrectly (4 out of9 prescriptions, 30.8%). One-fifth of pre-scriptions (5 out of 25, 19.2%) for chloro-quine oral tablets were incorrect, generallyfor more than the recommended 10 tablets.Conversely, many prescriptions for intra-venous chloroquine prescribed too fewampoules (15 out of 56 prescriptions,26.8%), as many doctors were still follow-ing the former recommendations for 5 am-poules instead of 7 ampoules in the 1999protocol guidelines. The poor compliancewith protocol guidelines for quinine oraltablets (2 out 8 prescriptions incorrect,25.0%) was mostly due to dispensing toofew tablets.
Discussion
The implementation of a national drug poli-cy faces several constraints, such as the
logistics of distribution, the large numberand variety of people and institutions in-volved and the rising cost of treatment [4].Appropriate planning is therefore essentialfor successful implementation. In thisstudy, some constraints and problems werehighlighted which reflect on the implemen-tation of the protocol for national malariacontrol in Sudan.
The study has revealed the impact oftraining on adherence to the protocol guide-lines, which highlights the importance ofcontinuous in-service training. Althoughthe house officers constituted the majorityof health providers, they were not targetedin the training process. This was obviousfrom the level of non-adherence to the pro-tocol. It might be necessary to introducethe protocol in the pre-service training.
The great majority of health workersdid not have the protocol guidelines in theirclinic at the time of the study, reflecting alack of continuous supervision and follow-up of the protocol.
Lack of awareness was an importantreason for the non-adherence in the major-ity of the health workers and this can bemostly attributed to the rapid turnover ofhealth workers. Patient satisfaction wasanother reason for non-adherence to theprotocol by some categories of healthworker, suggesting that education of thecommunity about the malaria treatmentprotocol would also be of value.
Although awareness of the protocolwas high among consultants, they were notadhering well to the protocol. Poor atti-tudes of senior staff are a concern as theymay be an influence on junior staff, espe-cially house officers being trained. Theconsultants justified their non-compliancein the belief that the protocol was not ef-fective due to the appearance of chloro-quine-resistant malaria in the area. Theresistance to chloroquine has been studied
13 Impact of the national.pmd 8/17/2005, 11:07 AM570

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 571
in Sudan by Abdel-Hamid et al., who con-cluded that chloroquine-resistant malariawas more than 25% in 4 sentinel posts [5].Another recent study in the same area in theyear 2000 revealed that 38% of Plasmodi-um falciparum were resistant to chloro-quine [S.A. Faragalla, unpublished report,2002]. Thus, monitoring and updating ofthe protocol is highly necessary.
The study revealed that the majority ofprescriptions (70.0%) were written bygeneral practitioners, thus highlighting theimportance of targeting them in future in-terventions. This is the routine practice inthe Sudan malaria control programme, ac-cording to the director of the programme;however the continuous turnover of gener-al practitioners has had a negative impacton the effectiveness of training.
The rate of prescriptions for antimalari-al drugs as a proportion of all prescriptionsin this study (31.2%) was similar to the na-tional figure (30.0%) [6]. Chloroquine wasthe most commonly prescribed antimalarialdrug (69.5%), as in the previous study(52.2%) [3]. Warrel observed that despitethe extensive spread of P. falciparum resis-tant strains, chloroquine is still the mostwidely used antimalarial drug in the world[7] as it is readily available and compara-tively cheap [8]. Two antimalarial drugs re-
cently launched in Sudan, artemether andhalofantrine, appeared on prescriptions inthis study although they should be reservedfor complicated malaria cases (which aretreated as hospital inpatients) as recom-mended by the protocol.
The proportion of antimalarial drug pre-scriptions that were compliant with theprotocol (79.7%) reflects a marked im-provement compared with the study beforethe implementation of the protocol (33.3%)[3]. However, regimens for administrationof intravenous quinine were still inadequatein 30% of cases and this should be stressedin future interventions.
We recommend the following: monitor-ing and updating of the protocol; introduc-ing the protocol guidelines in pre-servicetraining; and thorough distribution of theprotocol guidelines to health workers, withclose follow-up and supervision.
Acknowledgements
Thanks are due to Professor Ali Ahmed Idris,Department of Community, Faculty ofMedicine, University of Gezira for hisinvaluable assistance. We also thank theBatch 18 pharmacy students at the Universityof Gezira who contributed to data collection.
References
1. Department of Quality Assurance of Di-agnosis and Treatment. National pro-tocol for the treatment of malaria.Khartoum, Sudan, National Malaria Ad-ministration, 2001.
2. WHO policy perspectives on medicines.How to develop and implement a na-tional drug policy. Geneva, World HealthOrganization, 2003 (WHO/EDM/2002.5).
3. Yousif MA, Adeel AA. Antimalarial pre-scribing patterns in Gezira State: pre-
cepts and practices. Eastern Medi-terranean health journal, 2000, 6(5):939–47.
4. Antimalarial drug polices: data require-ments, treatment of uncomplicated ma-laria and management of malaria inpregnancy. Report of an informal consul-tation. Geneva, 14–18 March 1994.Geneva, World Health Organization,1994 (WHO/MAL/94.1070).
13 Impact of the national.pmd 8/17/2005, 11:07 AM571

572 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
5. Abdel-Hameed AA, El-Jak IE, FaragallaIA. Sentinel posts for monitoring thera-peutic efficacy of antimalarial drugsagainst Plasmodium falciparum infec-tions in the Sudan. African journal ofmedical sciences, 2001, 30(suppl.):1–5.
6. Malaria Administration Unit. Report onmalaria therapy. Khartoum, Sudan, Fed-eral Ministry of Health, 1998.
7. Warrel DA. Treatment and prevention ofmalaria. In: Gilles HM, Warrel DA, eds.Bruce-Chwatt’s essential malariology,3rd ed. London, Arnold, 1993:164–95.
8. Adome RO, Whyte SR. Hardon A. Popu-lar pills: community drug use in Uganda.Amsterdam, Het Spinhuis, 1996.
Funds and technical support are available: however, malaria is stilla serious challenge in the Region
Dr Hussein Gezairy, WHO Regional Director for the Eastern Mediterra-nean, called upon governments and the private sector in the mostcountries affected by malaria to ensure that safe and effectivedrugs are made affordable and accessible to patients, and that theimplementation of available vector control tools is throughintersectoral action for health – including community-based initia-tives and outreach health services.
The Regional Director pointed out that malaria is still a serious prob-lem in the Eastern Mediterranean Region, with more than 15 millionestimated cases every year and five of the worst-affected countriesin the world, namely Afghanistan, Djibouti, Somalia, Sudan andYemen. The Region still faces a serious malaria challenge to whichthe Regional Office is responding in many ways.
Source: WHO/EMRO Press release No. 722 May 2004
13 Impact of the national.pmd 8/17/2005, 11:07 AM572

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 573
Larvicidal activity of a neem treeextract (Neemarin) against mosquitolarvae in the Islamic Republic of IranH. Vatandoost1 and V.M. Vaziri1
1School of Public Health and Institute of Health Research, Tehran University of Medical Science, Tehran,Islamic Republic of Iran.Received: 22/10/02; accepted: 18/08/03
ABSTRACT An insecticide containing azadirachtin, a neem tree (Azadirachta indica) extract, was testedagainst mosquito larvae in the Islamic Republic of Iran under laboratory and field conditions. LC50 and LC90
values for Neemarin were 0.35 and 1.81 mg/L for Anopheles stephensi, the main local malaria vector, and0.69 and 3.18 mg/L for Culex quinquefasciatus. The mortality in the pupal stage was significantly higher thanthe other stages. In field trials, using recommended dosages of 1 and 2 L/hectare, mortality of Anopheles spp.larvae was also higher than Culex spp. Prevention of adult emerged and pupal mortality was the main activityof this compound. The maximum time of efficacy was 7 days at the highest concentration (2 L/hectare).
Activité larvicide d’un extrait du margousier (Neemarin) contre les larves de moustiques en Répu-blique islamique d’IranRÉSUMÉ Un insecticide contenant de l’azadirachtine, un extrait du margousier (Azadirachta indica), a ététesté en laboratoire et sur le terrain pour la lutte contre les larves de moustiques en République islamiqued’Iran. Les valeurs CL50 et CL90 pour le Neemarin étaient de 0,35 et 1,81 mg/L pour Anopheles stephensi, leprincipal vecteur local du paludisme, et 0,69 et 3,18 mg/L pour Culex quinquefasciatus. La mortalité au stadenymphe était significativement plus élevée qu’aux autres stades. Dans les essais sur le terrain, en utilisantles dosages recommandés de 1 et 2 L/hectare, la mortalité des larves d’Anopheles spp. était également plusélevée que pour Culex spp. La prévention de l’éclosion imaginale et la mortalité des nymphes constituaient laprincipale activité de ce composé. Le temps d’efficacité maximum était de sept jours à la concentration la plusélevée (2 L/hectare).
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:07 AM573

574 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Introduction
Malaria is the most important problem ofdeveloping countries. According to the lat-est report, it kills between 1.5–2.7 millionpeople every year [1]. Malaria has alwaysbeen considered as the most important vec-tor-borne disease in the Islamic Republic ofIran due to its socioeconomic effects onthe population [2].
Since the discovery of the insecticidedichloro-diphenyl-trichloroethane (DDT)before the Second World War, the wide-spread use of synthetic insecticides for thecontrol of pests as well as human diseasevectors has led to concerns about their tox-icity and environmental impact [3]. Be-cause of this, the search for newenvironmentally safe, target-specific insec-ticides is active throughout the world. Tofind new modes of action and to developactive agents based on natural plant prod-ucts, efforts are being made to isolate,screen and develop phytochemicals pos-sessing pesticidal activity. These categoriesof pesticides are known as biopesticides[3].
The neem tree (Azadirachta indica) is amember of the mahogany family (Melia-cea) that is native to India and Burma, but itwas introduced to other countries in thelate 19th century [4]. Six species in thefamily Meliacea have been studied for pes-ticidal properties in different parts of theworld. They are Azadirachta indica Juss,A. excelsa Jack, A. siamens Valeton, Meliaazadirachta L., M. toosendan Sieb. andZucc. and M. volkensii Gurke [3]. Howev-er, the most promising phytochemical pes-ticides studied in recent years are thosebased on extracts of Az. indica [3].
Various neem products have been re-searched extensively for their phytochem-istry and exploitation in pest control
programmes [3]. A number of bioactivecomponents have been isolated from vari-ous parts of the neem tree. These chemicalcompounds have different designations,among which azadirachtin A is the majorcomponent. In addition to azadirachtin, anumber of other active ingredients havealso been isolated and identified from dif-ferent parts of the neem tree, such as salan-nin, meliantriol and nimbin [3,4]. Two newtriterpenoids (22,23-dihydronimocinol anddes-furano-6-alpha-hydroxyazadiradione)were isolated from a methanolic extract ofthe fresh leaves of Az. indica along with aknown meliacin, 7-alpha-senecioyl-(7-deacetyl)-23-O-methylnimocinolide [5].
Neem components show multiple ef-fects against different insects such asmosquitoes, flies, triatomine bugs, cock-roaches, fleas, lice and ticks [3,4]. The ef-fect of neem on the activity of insects hasbeen neglected up to now, possibly becauseit does not rapidly lead to mortality. Howev-er, affected insects cannot survive adverseenvironmental conditions in the same wayas normal, healthy individuals; for exampleinsects with reduced activity (reducedsight, jumping, crawling and flying ability)may be caught more easily by natural pred-ators. Because of the variety of compo-nents and different mechanisms of action,insect resistance to neem compoundsseems likely to be low [8–10].
The repellent activity of neem oil solu-tions in coconut oil against populations ofmosquitoes consisting mainly of Mansoniaspp. in Gambella, western Ethiopia, wasdemonstrated by Hadis et al. [6]. The aimof the present study was to evaluate the ef-ficacy and durability of a neem extractagainst the main mosquito species in thesouthern part of the Islamic Republic ofIran.
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:07 AM574

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 575
Methods
Laboratory and field trials were carriedout using an azadirachtin-rich product,Neemarin 0.15% (Biotech InternationalLimited, New Delhi, India). The formula-tion consists of active ingredient (0.15%w/w), inert material (1.35% w/w) and pro-pylene glycol (98.5% w/w).
Laboratory testsLarvae of laboratory-reared strains ofAnopheles stephensi and Culex quinquefas-ciatus (originally from the Bandar-e-Abasscity area) were tested with different con-centrations of Neemarin at the late 3rd in-star and early 4th instar stages in a room at25 °C ± 1 °C in autumn and winter 1999,according to WHO methods [11]. Thestrains are susceptible to different insecti-cides such as DDT, organophosphates,carbamates and pyrethroids. Preliminarytesting was carried out to establish suitableconcentrations. Selected stock solutions ofNeemarin after preliminary tests were asfollows: 0.0586, 0.117, 0.234, 0.469,0.938, 1.875, and 3.750 mg/L. Lower loga-rithmic concentrations of Neemarin werediluted by adding the required volume of al-cohol solvent to the main stock of Neemar-in.
At each concentration, 200 mosquitoesrepresenting individuals of 25 larvae weretested on 4 occasions. Each test run con-sisted of 74 mL water, 1 mL of Neemarinstock solution (by use of sampler) and then25 larvae in 25 mL water were added, sothat the final volume was 100 mL. In con-trol runs, 1 mL alcohol was added insteadof Neemarin.
Mortality counts were made every 24hours after exposure until the test was ter-minated (when all the adults had emerged).In the analysis, both dead and moribundlarvae were considered as dead, and the
numbers alive at different stages (larvae,pupae, adults) were scored separately. Thepercentage mortality in the treated larvaewas corrected relative to the controls usingAbbotts formula [11]. The data were sub-jected to probit regression analysis accord-ing to Finney [12]. Goodness of fit of thepoints to a straight line was tested by chi-squared analysis.
Field trialsField trials were carried out in artificialponds (100 × 30 × 50 cm) in Jadas, Kazer-oun, in the south-eastern part of the IslamicRepublic of Iran in summer 2000, accord-ing to the method of Mulla and WHO rec-ommendations [11,13]. The ponds wereconstructed separately, without vegetationand were exposed to sunlight.
Replicate ponds were created for eachtreatment: 2 control ponds and 4 treatmentponds. In the treatment ponds, Neemarinwas sprayed on the water surface using amanual sprayer at 2 different concentra-tions (1 L/hectare and 2 L/hectare), as rec-ommended by other researchers [9,14].
The number of larvae in the artificialponds before and after the application ofNeemarin (up to 10 days) were countedusing a standard dipper. The frequency ofAnopheles and Culex spp. larvae werecounted using the method of Mulla with acubic metal frame incorporated into the netfor keeping and counting larvae in artificialponds [13].
The larvae were identified according tothe national identification key described byShahgudian [15].
Results
Laboratory testsUsing probit regression analysis software,regression lines were plotted for the dose–
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:07 AM575

576 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
response to Neemarin treatment of labora-tory strains of An. stephensi and Cx. quin-quefasciatus larvae (Figures 1 and 2). ForAn. stephensi the LC50 (lethal concentrationto cause 50% mortality in the population)was measured as 0.35 mg/L and the LC90(lethal concentration to cause 90% mortali-ty in the population) was 1.81 mg/L. ForCx. quinquefasciatus the LC50 was 0.69mg/L and LC90 was 3.18 mg/L respectively(Table 1). Thus, An. stephensi larvae need-ed a significantly lower concentration ofNeemarin than Cx. quinquefasciatus tocause the same mortality (P < 0.05).
The mortality among the pupal stageswas greater than other stages (P < 0.05).For example, among 400 larvae of Anophe-les species tested at the highest concentra-tion, the mortality rate of larvae, pupae andadults were 15.8%, 79.8% and 40.3% re-spectively. Similar data were obtained forother concentrations and for Culex species.Inhibition of adult emerged larvae throughmortality of pupae was the main action ofNeemarin.
Field trialsIn the field trials in artificial ponds, the dis-tribution of species identified during thefirst run of the test were An. stephensi(29%), An. fluviatilis (27%), An. dthali(13%), An. superpictus (6%) and Culexspp. (25%) for 500 mosquito larvae. Dur-ing the second run of the test the specieswere as follows: An. stephensi (26%), An.dthali (22%), An. superpictus (13%) andCulex spp. (38%) for 450 mosquito larvae.
Tables 2 and 3 show the mortality ratesof Anopheles and Culex spp. at differentstages (larvae, pupae, adult), comparingcontrols with 2 different concentrations ofNeemarin treatment (combining the 2 repli-cate runs). The main indicator of treatmentresponse was the percentage inhibition ofemerged adults. The inhibitory effect ofNeemarin declined over the 3 days of treat-ment. For Anopheles species, inhibition ofemerged adults fell from 33% and 56% at 1L/hectare and 2 L/hectare after 1 day to 5%and 20% respectively after 3 days. ForCulex species, inhibition of emerged adultsfell from 30% and 46% at 1 L/hectare and 2
Figure 1 Probit regression line for responseof Anopheles stephensi larvae to Neemarintreatment in laboratory tests
Figure 2 Probit regression line for response ofCulex quinquefasciatus larvae to Neemarintreatment in laboratory tests
50% mortality
50% mortality
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:08 AM576

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 577
L/hectare after 1 day to 1% and 21% re-spectively after 3 days. The frequency oflarvae in the artificial ponds were differentbefore and after application and increasedafter 7 days in all replicates, that showsmaximum time of efficacy and inhibition ofemerged adults at 7 days after applicationdid not show a significant difference (P <0.05).The maximum time of efficacy was7 days at the 2 L/hectare concentration
(P < 0.05). The durability of the productdepended on the dosage applied (P < 0.05).
As in the laboratory tests, pupal mortal-ity was higher than the other stages forAnopheles (Table 2) and Culex spp. (Table3). A lower concentration of Neemarin wasneeded for Anopheles spp. larvae than forCulex spp. to cause the same mortality (P <0.05).
Table 1 Probit regression line parameters of response of Anopheles stephensi and Culexquinquefasciatus to Neemarin treatment in laboratory tests
Mosquito Intercept Slope (SE) LC50 95% CI LC90 95% CI χχχχχ2 (df) P-valuespecies (mg/L) (mg/L)
An. stephensi 1.31 1.78 (0.07) 0.35 0.18–0.37 1.81 0.96–2.05 26.70 (4) < 0.0001
Cx. quinquefasciatus 0.85 1.91 (0.06) 0.69 0.36–0.74 3.18 1.68–3.38 29.08 (5) < 0.0001
SE = standard error.LC
50 = lethal concentration to cause 50% mortality in population.
LC90 = lethal concentration to cause 90% mortality in population.CI = confidence interval.χ2 (df) = heterogeneity about the regression line (degrees of freedom).
Table 2 Mortality of Anopheles spp. at different stages in artificial ponds,comparing controls with 2 different concentrations of Neemarin
Time after Larvae Mortality rate Survival Inhibitiona
treatment tested Larvae Pupae Adults Total rate (SE)No. % % % % % %
1 dayControls 93 7 8 3 18 821 L/hectare 130 18 22 5 45 55 33 (4.1)2 L/hectare 272 24 29 11 64 36 56 (2.9)
2 daysControls 90 9 6 3 18 821 L/hectare 160 10 18 3 31 69 16 (3.6)2 L/hectare 337 14 27 10 51 49 40 (2.7)
3 daysControls 105 12 14 5 18 821 L/hectare 200 6 9 2 17 78 5 (2.6)2 L/hectare 310 11 18 5 34 66 20 (2.6)
aPercentage inhibition of adult emerged larvae comparing treatment with controls.SE = standard error.
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:08 AM577

578 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
The findings of the present study werecompared with other researchers’ resultsusing different neem extract formulations(Neemazal, ANSKE, AZT-VR-K-E andMTB) on Aedes aegypti mosquitoes. TheEC50 for above formulations (molar con-centration of product which produces 50%of the maximum possible response) were8.4, 78.2, 18.1 and 5.9 ppm respectively(Table 4).
Discussion
Neem products are capable of producingmultiple effects on a number of insect spe-cies, such as anti-feeding effects, growthregulation, fecundity suppression and ster-ilization, oviposition repellency or attracta-ncy and changes in biological fitness [3].
In some cases, neem has repellent ef-fects. For example, the percentage protec-tion against sand fly bites provided by neem
oil was significantly higher than N,N-diet-hyphenylacetamide (DEPA) when appliedat 1% and 2% concentrations [16,17].Neem extracts have been shown to haverepellent activity against Mansonia spp.mosquitoes in Gambella, western Ethiopia[5].
Studies on the anti-feeding activity ofthe neem extracts showed that crops treat-ed with an aqueous suspension of neemseeds were protected from attack by lo-custs. Host plant selection is mainly gov-erned by the responses of the insect’sgustatory and olfactory sensilla. Since aza-dirachtin is non-volatile, the specificity andresponsiveness of receptors on the insect’staste neurons are likely to be critically im-portant in this process.
The effects of neem products on thereproduction of insects have been knownsince 1975 and reproduction reduction ef-fects have been found in Caelifera,
Table 3 Mortality of Culex spp. at different stages in artificial ponds, comparingcontrols with 2 different concentrations of Neemarin
Time after Larvae Mortality rate Survival Inhibitiona
treatment tested Larvae Pupae Adults Total rate (SE)No. % % % % % %
1 dayControls 61 7 4 2 13 871 L/hectare 50 14 22 3 39 61 30 (4.2)2 L/hectare 75 16 26 11 53 47 46 (5.3)
2 daysControls 45 5 5 7 17 831 L/hectare 60 5 15 1 21 79 5 (4.3)2 L/hectare 90 8 20 6 34 66 20 (4.2)
3 daysControls 54 6 7 0.4 13 871 L/hectare 51 5 8 1 14 86 1 (3.6)2 L/hectare 110 8 18 5 31 69 21 (3.8)
aPercentage inhibition of adult emerged larvae comparing treatment with controls.SE = standard error.
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:08 AM578

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 579
Table 4 Comparison of effectiveness of different neemformulations in laboratory tests on mosquito species
Mosquito species Neem EC50 Referenceformulation (ppm)
Aedes aegypti Neemazal 8.4 [11]
Ae. aegypti ANSKE 78.2 [11]
Ae. aegypti AZT-VR-K-E 18.1 [11]
Ae. aegypti MTB 5.9 [11]
Anopheles stephensi Neemark 0.05 [6]
Culex quinquefasciatus Neemark 0.22 [6]
An. stephensi Neemarin 0.18 Present study
Cx. quinquefasciatus Neemarin 0.36 Present study
Neemazal (Trifolio-M GmbH, Lahnau, Germany) 10 g/L azadirachtin.ANSKE = aqueous neem seed kernel extract.AZT-VR-K-E = enriched and formulated neem seed kernel extract.MTB = neem seed extract.Neemarin (Biotech International Limited, New Delhi, India) 0.15%azadirachtin.EC50 = molar concentration of product which produces 50% of themaximum possible response.
Heteroptera, Homoptera, Hymenoptera,Lepidoptera and Diptera [3,9]. A large num-ber of abortions (dead-born larvae) in thetsetse flies Glossina morsitans morsitansand Glossina pallidipes after treatment ofpregnant females with neem oil and the aza-dirachtin-enriched neem seed kernel ex-tract AZT-VR-K were found.
In mosquitoes, compounds extractedfrom Az. indica showed mortality forfourth instar larvae of An. stephensi, withLC50 values of 60 and 43 ppm, respectively[4]. This compares with the LC50 and LC90in our study of 0.36 and 1.81 ppm for An.stephensi and 0.69 and 3.18 ppm for Cx.quinquefasciatus respectively using a com-mercial preparation of neem extract,Neemarin. Our results were comparablewith findings from other researchers asshown in Table 4. The variation in LC50 isdue to mosquito species, formulation, cli-mate and method of application.
In order to compare the larvicidal effectof Neemarin with WHO-recommended lar-vicides (malathion, fenitrothion, temephos,chlorpyrifos), the regression lines werecompared. This showed that the toxicity ofNeemarin is less than other chemicals andthe LC50 and LC90 of Neemarin on laborato-ry strains of An. stephensi were to someextent similar to temephos [1].
Neem extracts act like insect growthregulators, so the mortality at differentstages were considered. Mortality of thepupae stage was significantly higher thanthe larvae and adult stages. In addition, themortality of Cx. quinquefasciatus was sig-nificantly lower than An. stephensi.
We conclude that Neemarin, at the rec-ommended concentrations in field studiesof 1 and 2 L/hectare, significantly reducesthe frequency of larvae and the estimatedresidual effect is 7 days.
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:08 AM579

580 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Acknowledgements
We would like to thank all of the staff mem-bers of the Medical Entomology Depart-
ment and Giahpezeshk Limited for theirkind collaboration.
References
1. Report of the fourth meeting of the globalcollaboration for development of pesti-cides for public health. Geneva 24–25June, 2004. Geneva, World Health Orga-nization, 2004 (WHO/CDS/WHOPES /GCDPP/2004.8).
2. Zaim M. Malaria control in Iran, presentand future. Journal of the American Mos-quito Control Association, 1987, 3:392–6.
3. Mulla MS, Su T. Activity and biologicaleffects of Neem products againstarthropods of medical and veterinary im-portance. Journal of the American Mos-quito Control Association, 1999, 15(2):133–52.
4. Ruskin FR. Neem: a tree for solving glo-bal problems. Washington DC, NationalAcademy Press, 1992.
5. Siddiqui BS et al. Two new triterpenoidsfrom Azadirachta indica and their insec-ticidal activity. Journal of natural prod-ucts, 2002, 65(8):1216–8.
6. Hadis M et al. Field trials on the repellentactivity of four plant product againstmainly Mansonia population in westernEthiopia. Phytotherapy research, 2003,17(3):202–5.
7. Sharma SK, Sharma VP. Field studies onthe mosquito repellent action of neemoil. Southeast Asian journal of tropicalmedicine and public health, 1995, 26(1):180–2.
8. Sharma VP, Dhiman RC. Neem oil as asandfly (Diptera: Psycodidae) repellent.Journal of the American Mosquito Con-trol Association, 1993, 9:364–6.
9. Dhar R et al. Effect of volatiles from neemand other natural products on gono-trophic cycle and oviposition of Anoph-eles stephensi and An. culicifacies(Diptera:Culicidae). Journal of medicalentomology, 1996, 33:195–201.
10. Rao DR, Reuben R. Evaluation of neemcake power and neem cake coated ureaas mosquito larvicides in rice fields. In:Uren MF, Block J, Manderson LH, eds.Arbovirus research in Australia. Pro-ceedings of the Fifth Symposium 28 Au-gust to 1 September 1989. Brisbane,Australia, CSIRO Tropical Animal Sci-ence, 1989:138–42.
11. Instructions for determining the suscepti-bility or resistance of mosquito larvae toinsect development inhibitors. Geneva,World Health Organization, 1981 (WHO/VBC/81.812).
12. Finney DJ. Probit analysis, 3rd ed. NewYork, Cambridge University Press, 1971.
13. Mulla M.S. Insect growth regulators forthe control of mosquito pests and dis-ease vectors. Chinese journal of ento-mology, 1991, 6:81–91.
14. Boschitz C, Grunewald J. The effect ofNeemAzal on Aedes aegypti (Diptera:Culicidae). Applied parasitology, 1994,35(4):251–6.
15. Shahgudian ER. A key to the Anophe-lines of Iran. Acta medica Iranica, 1960,3(3):38–48.
16. Srinivasan R, Kalyanasundaram M. Re-lative efficacy of DEPA and neem oil forrepellent activity against Phlebotomuspapatasi, the vector of leishmaniasis.
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:08 AM580

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 581
Journal of communicable diseases,2001, 33(3):180–4.
17. Parida MM et al. Inhibitory potential ofneem (Azadirachta indica Juss) leaves
on dengue virus type-2 replication. Jour-nal of ethnopharmacology, 2002, 79(2):273–8.
Malaria control in the Eastern Mediterranean Region
Significant progress was made in 2003 with the development ofappropriate technical guidelines for the improvement of key strate-gies for the control of malaria and other vector-borne diseases.These included the regional strategic framework for integrated vec-tor management, guidelines on monitoring insecticide resistance,regional guidelines on the management of public health pesticides,including country profiles, and guidelines on malaria microscopyand quality assurance. The WHO publications Instructions for treat-ment and use of insecticide-treated mosquito nets and Basic ma-laria microscopy were translated into Arabic. National strategic planson use of insecticide-treated nets were finalized for Afghanistan,Djibouti, Saudi Arabia, Sudan and Yemen. A regional network formonitoring vector resistance was initiated and country-level part-nership was fostered at the annual meeting of national malaria pro-gramme managers held in Lahore, Pakistan in June 2003.
Source: The Work of WHO in the Eastern Mediterranean Region. AnnualReport of the Regional Director 1 January–31 December 2003
Available at: http://www.emro.who.int/rd/AnnualReports/2003/index.htm
14 Larvicidal activity of a neem.pmd 8/17/2005, 11:08 AM581

582 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Characteristics of districts in Pakistanwith persistent transmission of wildpoliovirus, 2000–2001S.A. Lowther,1 T. Mir,2 M.K. Bile,2 R. Abdul Hafiz3 and A.W. Mounts2
1World Health Organization, Polio Eradication Initiative, Islamabad, Pakistan (Consultant, 2001).2World Health Organization, Islamabad, Pakistan.3National Institutes of Health, Expanded Programme on Immunization, Islamabad, Pakistan,Received: 31/03/03; accepted: 14/01/04
ABSTRACT We sought to identify factors associated with being a reservoir district for wild poliovirus in Pakistan.Differences between reservoir and non-reservoir districts were identified using acute flaccid paralysis surveillancedata, population census statistics and data from a survey of district health officials (DHOs). Of the 11 poliovirusreservoir districts identified, population density was significantly higher (median 550 persons/km2) than the non-reservoirs (median 175 persons/km2). DHOs from reservoir districts more often reported that planning was affectedby refugees and they had more frequent DHO transfers compared with non-reservoir districts. Multivariate analysisconfirmed that reservoirs more often had high population density and frequent DHO transfers. Assessment of district-level and management characteristics can supplement surveillance methods to further improve health programmes.
Caractéristiques des districts où la transmission du poliovirus sauvage continue au Pakistan, 2000-2001RÉSUMÉ Nous avons cherché à identifier les facteurs qui font qu’un district est une zone de réservoir du poliovirussauvage au Pakistan. Les différences entre les districts qui sont ou non une zone de réservoir ont été identifiées enutilisant les données de la surveillance de la paralysie flasque aiguë, les statistiques du recensement de la populationet des données tirées d’une enquête des responsables sanitaires de district. Dans les 11 districts identifiés commeétant une zone de réservoir du poliovirus, la densité de population était significativement plus élevée (médiane de 550personnes/km2) que dans les districts qui ne sont pas des zones de réservoir (médiane de 175 personnes/km2). Lesresponsables sanitaires des districts qui sont des zones de réservoir signalaient plus souvent que la planification étaitaffectée par les réfugiés et étaient plus fréquemment transférés par rapport aux districts qui ne sont pas une zone deréservoir. L’analyse multivariée a confirmé que les zones de réservoir avaient plus souvent une forte densité depopulation et dans ces zones, les transferts de responsables sanitaires de district étaient plus fréquents. L’évaluationdes caractéristiques de la gestion et au niveau du district peut compléter les méthodes de surveillance traditionnellespour améliorer davantage les programmes de santé.
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM582

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 583
Introduction
Global poliomyelitis incidence has de-creased 99% since the World Health As-sembly agreed to instigate the PoliomyelitisEradication Initiative in 1988 [1]. Pakistanbegan poliomyelitis eradication activities in1994 and has had considerable success [2].These activities are conducted with the on-going World Health Organization (WHO)Expanded Programme on Immunization(EPI), which seeks to vaccinate childrenagainst poliomyelitis, measles, diphtheria,pertussis, tuberculosis, tetanus, and hepati-tis B.
Numerous national immunization days(NIDs) have resulted in a considerable de-cline and localization of cases in Pakistan[2]. However, despite these efforts, severalareas in Pakistan appear to be reservoirswhere wild poliovirus circulation persiststhroughout the year, repeatedly reintroduc-ing infection to nearby susceptible popula-tions during the higher transmissionseason. Presumably a certain threshold ofsusceptible population would be required tosustain virus circulation in these districts;however, other factors such as effectivemanagement of health resources may alsobe important.
In Pakistan, the administrative tiers ofthe health system include the federal, pro-vincial and district levels. The federal of-fice is responsible for national health policydecisions, vaccine procurement and distri-bution of resources to provinces. Provin-cial health offices are responsible for theadministration of health programmesthroughout the province, distribution ofvaccines and supplies to districts, and su-pervision and monitoring of district-levelactivities. Programme implementation, dai-ly management and control of resourcesare performed at the district level by dis-trict health officers (DHOs) (or by agency
surgeons in the case of federally adminis-tered tribal agencies). In 2000 there were122 districts-level administrative areas (in-cluding 7 tribal agencies).
Areas with continued transmission ofwild poliovirus have been examined andidentified through ongoing active surveil-lance [1]. However, no published studieshave taken an ecologic approach to exam-ining district-level management character-istics that may affect the success of theadministrative area in poliomyelitis eradica-tion. Using acute flaccid paralysis (AFP)surveillance data, we sought to describe thecharacteristics of districts where there ap-peared to be persistent wild poliovirustransmission in Pakistan. This study exam-ines the relationship between several char-acteristics of districts, district healthmanagement and the presence of a poliovi-rus reservoir to identify specific factorsthat might be modified to improve the ef-fectiveness of poliomyelitis eradication inPakistan.
Methods
On February 28, 2001 a national confer-ence on poliomyelitis eradication was heldin Islamabad, Pakistan. All 122 DHOs andagency surgeons were asked to attend.(For this study, the designation “DHO” willinclude both district health officers andagency surgeons.) DHOs were asked tocomplete a self-administered survey to col-lect demographic information such as age,sex, educational achievements, training andyears of experience. Information on theirdistrict health system that might affecthealth programme planning, such as dataon population migration (e.g. refugees ordrought-related movement) was collected.The survey was also used as a forum toexpress opinions (e.g. describe specific
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM583

584 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
weaknesses or gaps in their district in per-sonnel or supplies). Surveys were latermailed to those DHOs that either did not at-tend the conference or did not complete thesurvey at the time of the conference. Be-cause of its nature as a feedback mecha-nism, the survey was neither anonymousnor confidential, and respondents were in-formed that the information they providedwould be examined to give feedback andassess programme planning with specificregard to their district.
AFP surveillance data reported from2000 through 2001 were analysed to identi-fy districts with persistent and low trans-mission season wild poliovirus circulation.Adequacy of surveillance data was as-sessed using standard surveillance indica-tors, i.e. rates of non-poliomyelitis AFP (1case per 100 000 population expected), 60-day case follow-up (expected to be done onall cases), and adequate stool collection(greater than 80% of all stool specimenscollected met the requirements of 2 stoolspecimens per case collected at least 24hours apart, within 14 days of the onset ofparalysis, and arriving in the laboratorywith intact reverse cold chain and suffi-cient quantity for analysis). Data on popu-lation size, area size and population densitywere obtained from the Population CensusBureau [3].
AnalysisReservoir districts were defined as thosedistricts with wild poliovirus isolated dur-ing 5 out of 8 quarters of the years 2000and 2001 and with virus isolated during lowtransmission season (December throughMarch) at least one of the years 2000 and2001.
Several continuous variables were re-coded for assessment. For example, be-cause of its broad range among districts,
population density was transformed to alogarithmic scale [i.e. ln (population densi-ty)] and was categorized into 2 levels: highdensity, defined as ln (population density) >7.0 and low density, defined as ln (popula-tion density) ≤ 7.0. The number of DHOstransferred in the past 5 years was also cat-egorized into 2 levels: frequent transfers(more than 4 per 5 years) and less frequenttransfers (4 or fewer per 5 years). Univari-ate analysis was performed using Epi-Infosoftware where differences were examinedbetween poliovirus reservoir districts andnon-reservoir districts. The Kruskal–Wallistest was used to compare district-levelcharacteristics whose values were codedas continuous with exact P-values report-ed. Odds ratios (OR) and exact 95% confi-dence intervals (95% CI) were used tocompare characteristics coded as categori-cal. Any factors found to be significantlyassociated with being a reservoir districtfrom univariate analysis were included inmultivariate analysis using SAS (Cary,North Carolina, United States of America)statistical software. For all statistical tests aP-level of 0.05 was used as significant.
Results
Reservoirs for wild poliovirusFifty-nine districts had poliovirus isolatedin 2000 and 34 in 2001; 11 administrativedistricts met our definition of reservoir dis-trict. These included Quetta district inBalochistan province; Bannu and Peshawardistricts in North-west Frontier Province,Faisalabad district in Punjab province; andHyderabad, Jacobabad, and Karachi dis-tricts in Sindh province (Figure 1). Karachiincluded 5 administrative districts of Kara-chi Central, Karachi South, Karachi East,Karachi West and Karachi Malir. As can be
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM584

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 585
seen from Figure 1, the districts were notclustered together geographically which ar-gues against a single large poliovirus reser-voir. Surveillance indicators for 2000 fromreservoir districts (rates of non-polio AFP,60-day follow-up and adequate stool col-lection) were not significantly differentfrom non-reservoir districts, and met theworldwide standards for such indicators ofadequate surveillance (Table 1). Populationdensity was higher among reservoir dis-tricts compared with non-reservoir dis-tricts (median = 550.7 versus 175.9persons per square km, P = 0.001).
Characteristics of DHOs
In all, 101 DHOs responded to the survey(21 never responded) from all provinces ofPakistan. There were no differences in theDHO response rate by reservoir districtstatus, AFP surveillance characteristics,
geographic location/province, or popula-tion density. The median age of respon-dents was 50 years (range 40–60 years)and all DHOs were male. All DHOs werephysicians (MBBS) and 46% had a publichealth degree or diploma; 10% reported re-ceiving management training in the past 3years. In addition, 97% reported having as-signed a specific person to be responsiblefor EPI. As regards the complications ofhealth programme planning, 90% of DHOsreported seasonal migration as a complica-tion, 51% cited refugees 36% citeddrought-related migration, 11% cited no-mads or gypsies, 4% cited other complica-tions including tribal clashes, border orline-of-control conflict, or smugglingroutes. About 16% reported having a pri-vate practice. Prior experience as a DHOwas reported by 49% of respondents witha median of 6 years of experience (range 0–27 years). In the past 5 years, 59% of
Figure 1 Districts identified from acute flaccid paralysis surveillance to have persistent wildpoliovirus transmission in Pakistan during 2000–2001 (defined as districts with wild poliovirusisolated during 5 out of 8 quarters of the years 2000 and 2001 and with the virus isolatedduring low transmission season (December–March) in at least 1 of the years)
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM585

586 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Table 1 Characteristics among districts and district health officials comparing wild poliovirusreservoir districts to non-reservoir districts, Pakistan, 2000–2001
Characteristics Reservoir Non-reservoir Statistical analysisdistrict district
Continuous variables Median Median Kruskal– P-valuea
WallisSurveillance indicators
No. poliomyelitis cases 2001 3.5 0.0 32.70 0.000Non-poliomyelitis AFP rate (1.00 expected) 1.95 1.42 2.75 0.097Non-poliomyelitis enterovirus rate(0.10 expected) 0.15 0.17 0.16 0.690Percentage with 60-day follow-up 100 100 0.25 0.617Percentage with adequate stoolcollection 74 71 0.02 0.892
District-level characteristicsPopulation density (persons per km2) 550.7 175.9 13.1 0.001Area size (km2) 2268 5286 6.80 0.009Population size 1 724 915 805 235 6.99 0.008Total district health officers in last5 years 5 3 7.73 0.005
Categorical variables No. % No. % Odds 95% CIa
ratio
District-level characteristicsLog (population density) > 7.0 3 33 1 1 45.5 4.1–506.2Log (population density) ≤ 7.0 6 67 91 99 1 –5 to 8 district health officers per 5years 6 67 20 22 7.2 1.7–31.4≤ 5 district health officers per 5years 3 33 72 88 1 –
District health officer characteristicsRespondents 9/11 82 101/111 91 0.98 0.2–9.5Previous experience as districthealth officer 6/9 67 42/93 45 2.38 0.6–10.1Has private practice 0/9 0 16/96 17 Undef –Has public health degree 2/9 22 44/94 47 0.3 0.1–1.6Specific person assigned to manageEPI 9/9 100 89/92 97 Undef –Had management training in last 5years 0/9 0 10/91 11 Undef –Reports drought affects district 3/9 33 31/89 35 0.92 0.2–3.9Reports refugees affect district 8/9 89 43/91 47 8.74 1.1–72.8Reports seasonal migration affectsdistrict 8/9 89 89/92 97 0.88 0.10–7.8
aExact P-value and 95% confidence intervals (CI) are given. A P-level of 0.05 and 95% CI excluding 1.0 wasconsidered statistically significant.AFP = acute flaccid paralysis. EPI = Expanded Programme on Immunization.
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM586

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 587
DHOs reported 2 or 3 transfers, with 20%reporting zero or 1 transfer and 21% re-porting 4 to 7 transfers.
In univariate analysis, several differenc-es were identified between reservoir andnon-reservoir districts (Table 1) amongcharacteristics of DHOs and districts.There was no difference in DHO responserate between reservoir and non-reservoirdistricts (82% versus 92% respectively, P= 0.97). DHOs from reservoir districtswere more likely to report that problems inhealth programme planning were affectedby refugees (OR = 8.74, P = 0.02) butwere equally likely as non-reservoir DHOsto report that problems in planning wereaffected by factors such as drought or sea-sonal movement. DHOs from reservoir andnon-reservoir districts did not differ by ed-ucational status, additional public healthtraining, or years of experience. DHOs re-ported that reservoir districts had signifi-cantly more DHOs in the last 5 yearscompared with non-reservoir districts (me-dian = 5 versus 3 DHOs, P = 0.005).
Multivariate analysis included 2 district-level characteristics (population densityand frequency of DHO transfers) and 1DHO characteristic (reporting that refu-gees affected health programme planning).This analysis indicated that reservoir dis-tricts were more likely to be those amongdistricts of high population density[ln(population density) > 7.0] (adjustedaOR = 28.1, 95% CI: 2.2–361.0) and dis-tricts with frequent DHO transfers (> 4DHO transfers in the last 5 years) (aOR =5.1, 95% CI: 1.03–25.5). However, aftercontrolling for population density and fre-quency of DHO transfers, DHOs reportingthat refugees affected programme planningwas no longer significantly associated withreservoir district status.
Discussion
This analysis describes characteristics ofdistricts and their DHOs in Pakistan withpersistent transmission of wild poliovirus,and considers the effect of managementand administration on the outcomes of adisease eradication programme. Our datashowed that districts with less frequentchange of managers were less likely to bepoliovirus reservoirs than those with fre-quent turnover, indicating that consistencyof management may improve the outcomeof poliomyelitis eradication activities in agiven district. Other characteristics of theDHO, such as previous experience as aDHO, management training or total yearsof experience, were not associated withpoliovirus reservoir status. DHOs in thePakistan health care system are the primarymanagers of all national public health pro-grammes and are key individuals responsi-ble for a programme’s success. Someexamples of the responsibilities of DHOs inregard to poliomyelitis eradication planninginclude: supervising and monitoring of dis-trict logistical and personnel planning, dis-bursement of financial resources andcommunication with local authorities forinvolvement.
Our analysis also demonstrated that res-ervoir districts were more likely to beamong districts with the highest populationdensity. This finding is consistent with evi-dence that urban areas with increased pop-ulation density are high-risk poliovirusreservoirs [4]. In addition, our analysis il-lustrates the process of identifying reser-voir districts based on natural seasonalityof the virus in Pakistan. We believe thismethod helped improve the effectivenessof immunization campaigns by allowing theconcentration of resources in areas needing
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM587

588 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
additional support; it continues to be an im-portant step in the final stages of poliomy-elitis eradication.
Our data also suggest that the presenceof a substantial refugee population may af-fect the success of poliomyelitis eradica-tion at the district level. This is consistentwith supplementary individual-level epide-miological data collected during 2001which indicated that Afghan refugees wereat higher risk of poliomyelitis in Pakistan[2]. The additional population may burden ahealth programmes’ allocation of resourcesas well as increase virus transmission be-cause of a raised population density. Con-tinued attention to identifying high-riskgroups will be invaluable as has been illus-trated in outbreak situations [5,6].
Previous studies have shown why indi-vidual children were under-vaccinatedthereby creating reservoirs for wild poliovi-rus [7,8]. However our study is the first toexamine risk factors for district and man-agement characteristics of these reser-voirs. In Pakistan during 1994, childrenmissed during NIDs were also those morelikely to have been unvaccinated or partial-ly-immunized through routine immuniza-tion services [9]. Elsewhere, risk factorsfor children missed during NIDs includedfailure to be reached by methods of socialmobilization, increased distance to NID site[10], lower parental literacy or educationalstatus [2], and age 0–6 months [11]. Allpolio vaccination campaigns in Pakistanhave been house-to-house since 1998 [12]because they have been found to be morecomplete in coverage and cost-effective.While the house-to-house strategy isshown consistently to improve coverage,published studies to describe reasons whychildren are missed during house-to-housecoverage are lacking. House-to-house im-munization campaigns are a massive under-taking which involve considerable planning
and more complex logistics on multiple ad-ministrative levels. It is therefore conceiv-able that quality and consistency ofprogramme administration and manage-ment may play a greater role in the suc-cessful outcomes of eradication activities.
Our assessment makes no attempt toexplain all the reasons for the continuedtransmission of poliovirus in Pakistan. Inthe recent past, poliomyelitis cases in Paki-stan have been un- or under-vaccinatedthrough routine immunization [8]. Routineimmunization coverage data could not bevalidated for the time period of study forevery district, and complete, validatedcountrywide district-specific NID cover-age estimations were not available.
The relationship between populationdensity, management turnover rate and po-liovirus reservoir may be complex. While acertain population density is necessary tosustain poliovirus circulation, it may alsobe that densely populated areas, particularlyurban areas, may be more desirable postsresulting in more frequent transfer of staff.Alternatively, DHOs in densely populatedurban areas may have more difficulties inmeeting expected performance standards.Other factors, such as a district literacyrates, socioeconomic status, or per capitahealth programme funding, may help to de-scribe areas having barriers to successfulhealth programme outcomes. Because ofits exploratory nature, our questionnaire didnot capture specific reasons for DHOtransfer. However, our analysis did identifyDHO transfer to be associated with districtreservoir status with no association foundamong factors such as total years of expe-rience, previous experience as a DHO, andtraining or certification in management.Further assessment of district managementmay be warranted, both in performanceexpectations and achievements.
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM588

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 589
This analysis identifies a managementfactor that may have an impact on the suc-cess of a high-priority disease eradicationprogramme. Our data suggest that decreas-ing the frequency of transfers in districtmanagement may improve the quality ofprogramme implementation. As a result ofthis study, the United Nations Children’sFund (UNICEF) and WHO have nowplaced district support teams, comprised ofindividuals with varying skills, to work di-rectly under the district managers and sup-port all poliomyelitis- and EPI-relatedactivities. These teams receive technicalsupervision from international and nationalconsultants from the 2 United Nationsagencies who are assigned to high-risk dis-tricts for periods of up to 1 year and pro-vide additional programme support andcontinuity.
During both 2002 and 2003 Pakistanconducted 4 rounds of NIDs and 4 roundsof sub-NIDs, which are targeted at areaswith factors (such as those described inour analysis) that indicate a high risk forcontinuing virus transmission [13]. In addi-
tion, Pakistan introduced wide- scale inde-pendent monitoring of coverage throughthird-party survey companies to improvethe quality of supplementary immunizationactivities by immediately identifying andvaccinating children initially missed duringNIDs.
In conclusion, our analysis has identi-fied DHO transfer rate and populationdensity as important determinants of polio-myelitis eradication success. These aspectsare now being addressed along with othercritical factors to improve efforts to stoptransmission of wild poliovirus. We beleivethat the findings described in our paperhave implications beyond poliomyelitiseradication and should be considered inother disease control programmes.
Acknowledgements
We would like to thank Mr Abid Sheik forhis administrative assistance in survey col-lection, and Alex and Samantha Rowe fortheir critical review of the manuscript.
References
1. Progress toward global eradication ofpoliomyelitis, 2001. Morbidity and mor-tality weekly report, 2002, 51:253–6.
2. Progress toward poliomyelitis eradica-tion—Pakistan and Afghanistan, Janu-ary 2000–April 2002. Morbidity and mor-tality weekly report, 51(24):523–4.
3. 1998 census report of Pakistan.Islamabad, Population Census Organi-zation, Statistics Division, Governmentof Pakistan, 1999.
4. Hull HF et al. Paralytic poliomyelitis: sea-soned strategies, disappearing disease.Lancet, 1994, 343:1331–7.
5. Aylward RB et al. Unimmunized gypsypopulations and implications for eradi-cation of poliomyelitis in Europe. Journalof infectious diseases, 1997, 175 (suppl.1):S86–8.
6. Reichler MR et al. Outbreak of paralyticpoliomyelitis in a highly immunizedpopulation in Jordan. Journal of infec-tious diseases, 1997, 175(suppl. 1):S62–70.
7. Hennessey KA et al. Widespread para-lytic poliomyelitis in Pakistan: a case-control study to determine risk factorsand implications for poliomyelitis eradi-
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM589

590 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
cation. Journal of infectious diseases,2000, 182(1):6–11.
8. Hennessey KA et al. Widespread para-lytic poliomyelitis in Pakistan: a case–control study to determine risk factorsand implications for poliomyelitis eradi-cation. Journal of infectious diseases,2000, 182(1):6–11.
9. Reichler MR et al. Evaluation of oral po-liovirus vaccine delivery during the 1994national immunization days in Pakistan.Journal of infectious diseases, 1997,175(suppl. 1):S205–9.
10. Reichler MR et al. Cluster survey evalua-tion of coverage and risk factors for fail-ure to be immunized during the 1995national immunization days in Egypt. In-
ternational journal of epidemiology,1998, 27(6):1083–9.
11. Singh B et al. Pulse polio immunizationin Delhi—1995–96: a survey. Indianjournal of pediatrics, 1997, 64(1):57–64.
12. Linkins RW et al. Evaluation of house-to-house versus fixed-site oral poliovirusvaccine delivery strategies in a mass im-munization campaign in Egypt. Bulletinof the World Health Organization, 1995,73(5):589–95.
13. Progress toward poliomyelitis eradica-tion—Afghanistan and Pakistan, Janu-ary 2002–May 2003. Morbidity andmortality weekly report, 2003, 52(29):683–5.
Poliomyelitis eradication in the Eastern Mediterranean Region
Rapid and significant progress towards the eradication of poliomy-elitis is continuing in all countries of the Eastern Mediterranean Re-gion. Poliovirus transmission has been interrupted in 17 countriesof the Region for more than 3 years. Comprehensive informationabout the poliomyelitis eradication programme in the Eastern Medi-terranean Region can be found at: http://www.emro.who.int/polio/
15 Characteristics of districts.pmd 8/17/2005, 11:08 AM590

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 591
Characterization of Leishmaniainfection in rodents from endemicareas of the Islamic Republic of IranM. Mohebali,1 E. Javadian,1 M.R. Yaghoobi-Ershadi,1 A.A. Akhavan,1 H. Hajjaran1 andM.R. Abaei1
1School of Public Health and Institute of Public Health Research, Tehran University of Medical Sciences,Tehran, Islamic Republic of Iran.Received: 14/04/03; accepted: 26/10/03
ABSTRACT Between 1991–2000, Leishmania species were isolated and characterized by isoenzyme andmolecular analysis from rodents caught in various parts of the Islamic Republic of Iran. In areas endemic forcutaneous leishmaniasis, parasites were observed by direct microscopy in smears from 18.6% of 566specimens. L. major was isolated from 4 species: Rhombomys opimus, Meriones libycus, Tatera indica andMer. hurrianae. L. turanica was isolated from R. opimus for the first time in this country. In endemic areas ofvisceral leishmaniasis, parasites were observed in liver and spleen from 13.7% of 504 rodents. Two specieswere positive on culture; promastigotes isolated from Mer. persicus were characterized as L. donovanizymodeme LON50 and from Mesocricetus auratus as L. infantum LON49.
Caractérisation de l’infection à Leishmania chez des rongeurs des zones endémiques de la Répu-blique islamique d’Iran.RÉSUMÉ Entre 1991 et 2000, des espèces de Leishmania ont été isolées et caractérisées par isoenzymeset analyse moléculaire chez des rongeurs capturés dans diverses parties de la République islamique d’Iran.Dans les zones d’endémie de la leishmaniose cutanée, des parasites ont été observés par microscopiedirecte dans des frottis provenant de 18,6 % des 566 échantillons. L. major a été isolé chez quatre espèces :Rhombomys opimus, Meriones libycus, Tatera indica et Mer. hurrianae. L. turanica a été isolé chez R. opimuspour la première fois dans ce pays. Dans les zones d’endémie de la leishmaniose viscérale, des parasitesont été observés dans le foie et la rate de 13,7 % des 504 rongeurs. Deux espèces ont donné des culturespositives ; les promastigotes isolés chez Mer. persicus ont été caractérisés comme zymodème LON50 deL. donovani et ceux isolés chez Mesocricetus auratus comme LON49 de L. infantum.
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM591

592 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Introduction
Leishmaniasis is an important health problemin the Islamic Republic of Iran. There are sev-eral foci of zoonotic cutaneous leishmaniasis(CL) in the north, east and south of the coun-try [1–6]. Zoonotic CL is essentially a diseaseof gerbils, transmitted by Phlebotomus pap-atasi and P. cocausicus and other species ofsand fly that breed in gerbil burrows [7]. Thehuman disease is secondary to the infectionof gerbils and is seen only in places where theinfected gerbils live [8]. Three different epi-demiological types of zoonotic CL have beenobserved in this country and 4 species of ro-dents (Gerbillidae) are the principal animalreservoir hosts in all foci [9].
Visceral leishmaniasis (VL), or kala-azar,is also seen sporadically all over the IslamicRepublic of Iran and is of the Mediterraneantype. Wild and domestic carnivores are themain animal reservoirs [10–12], but rodentshave been reported as reservoirs in the Mesh-kin-Shar district [13]. Sand flies of the genusPhlebotomus are the most likely vector of VLin the endemic areas [10].
The study of Leishmania infection inrodents in the Islamic Republic of Iranstarted in 1953 in the north-east of thecountry [8] but, while it was extended toother parts of the country, the isolation andcharacterization of the parasites has notbeen investigated in these areas. In thisstudy, we report the isolation and charac-terization of Leishmania species infectionfrom a number of species of rodents thatwere trapped alive in different parts of theIslamic Republic of Iran in the last decade.
Methods
Study areaThe investigation was conducted over aperiod of 10 years from 1991 to 2000 in
endemic foci of zoonotic CL and VL in theIslamic Republic of Iran (Figure 1).
Collection and examination ofrodentsThe study sites were determined by reportsfrom local health authorities of outbreaksof human CL and VL infection. The activecolonies of rodents were identified and therodents were trapped alive in various partsof these areas. Specimens were collectedfrom the colonies of gerbils located about1–1.5 km around villages where CL or VLwere endemic. Around 20–30 live trapswere used each week and rodents werecaught in all seasons. The genus and spe-cies of the rodents were determined byexternal characteristics: colour, body mea-surements, ears, tail, feet, teeth and crani-um [14,15].
Isolation of parasites from thecaught rodentsFor detecting CL infection, 2 impressionsmears were taken from the ears of eachrodent [13,16]. For detecting VL parasites,2 impression smears from the spleen andliver of each rodent were prepared. Thesmears were fixed in methanol, stained bystandard Giemsa methods and examinedfor parasites by light microscope at highmagnification (× 1000).
The samples from infected rodentswere cultured in Novy–MacNeal–Nicolle(NNN) culture and liver infusion brothtryptose (LIT) and RPMI 1640 medium(Gibco Life Technologies, New York,USA) containing 10% heat-inactivated fetalcalf serum. The cultures were checked forpromastigotes twice a week for a period of6 weeks.
Leishmania species were characterizedby random amplified polymorphic DNA–polymerase chain reaction (RAPD–PCR)
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM592

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 593
analysis [17,18] at the Medical Faculty,Shiraz University of Medical Sciences andthe School of Pubic Health, Tehran Univer-sity of Medical Sciences and by isoenzymeanalysis at the London School of Hygieneand Tropical Medicine, United Kingdom,and the Faculty of Medicine, University ofMontpellier, France.
Characterization of isolatedparasitesFor the RAPD–PCR analysis, DNA wasextracted from the promastigotes, culturedat 20 °C in RPMI1640 medium (10 000parasites per 10 mL) and washed withLocke’s solution. The pellet was resus-pended in 100 µL lysis buffer. The lysatewas extracted once with equal volumes of1:1 (v/v) phenol:chloroform and once with
24:1 (v/v) chloroform isoamylalcohol andprecipitated by ethanol. The DNA was re-suspended in the specified materials andamplification were done in a mixture con-taining 20 mmol/L (NH4)2(SO4), 75 mmol/LTris-HCl, pH.9, 0.01% (w/v) Tween 20, 2mmol/L MgCl2, 200 µmol/L deoxynulcleo-tide triposphate, 1 mmol/L primer and 1unit of Taq polymerase. Then 1 µL of DNA(20 ng/µL) was added by centrifugationthrough the mineral oil overlay and the re-action was carried out in a thermocycler(Genius, Techne Ltd, United Kingdom)programmed for 1 cycle of 2 min at 94 °C,followed by 30 cycles of 30 s at tempera-tures of 94 °C, 1 min at 36 °C and 2 min at72 °C. Aliquots from each reaction (12 µL)were run on 1.5% agarose gel and visual-ized under ultraviolet light with ethidium
Figure 1 Areas endemic for zoonotic cutaneous leishmaniasis (ZCL) and visceralleishmaniasis (VL) where rodents were collected for the study
aaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa
aaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa
aaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa
aaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa
aaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa
aaaaaaaaaaaaaaaa
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM593

594 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
bromide. The primers used in this studywere as follows:• AB1-07 GGT GAC GCA G• 327. ATA CGG CGT C• 329. GCG AAC CTC C• 333. GAA TGC GAC G• 335. TGG ACC ACC C
For the isoenzyme characterization, af-ter mass production of promastigotes,samples were cultured in monophasic me-dia with 10% to 20% fetal calf serum,washed with phosphate-buffered saline at4 °C with centrifugation at 2500–3000 × gfor 20 min 3 times and freeze-thawed in liq-uid nitrogen several times, followed byelectrophoresis on polyacrylamide gel. Inthis technique 12 enzymes were used:pyruvate kinase (PK), superoxide dismu-tase (SOD), phosphoglucomutase (PGM),peptidase D (PEPD), alanine aminotrans-ferase (ALT), aspartate aminotransferase(AST), nucleoside hydrolase (NH), glu-cose-6-phosphate dehydrogenase (G6PD),glucose-6-phosphate isomerase (GPI),esterase (ES), methanol dehydrogenase(MDH) and mannose-6-phosphate iso-merase (MPI) [19].
Results
Areas endemic for cutaneousleishmaniasisAltogether, 566 rodents (Gerbillidae) weretrapped alive in several CL-endemic areasthroughout the Islamic Republic of Iranfrom 1991 to 2000. Leishmania parasiteswere observed in cutaneous smears from105 (18.6%) of the rodents by direct highmagnification microscopy examination(Table 1).
L. major was isolated from Rhombomysopimus, Meriones libycus, Tatera indicaand Mer. hurrianae and characterized by
isoenzyme analysis and molecular proce-dures (RAPD–PCR). All of the Leishmaniaspecies and strains were similar to Leish-mania species that had been isolated fromhuman infection in the same areas. L. tu-ranica was isolated from an infected R.opimus for the first time in this country.
R. opimus was the principal reservoirhost of zoonotic CL in the north-eastern(Minoo Dasht) district where 85.2% of iso-lates tested positive (Table 1). It was alsoprominent in the central parts of the coun-try (Badrood, Ardakan and Sabzevar dis-tricts). Mer. libycus was found in 35.1% ofisolates in the south-west (Fars province)and 25.0% in the central area. T. indicawas the main reservoir host in foci of thesouth-west (14.3%) and south (Dashti andDashtestan districts) of the country (4.5%of isolates tested positive). In the south-east of the country (including southernparts of Baluchistan, Dashtyari, Konarakand Chabahar areas) the main animal reser-voir was Mer. hurrianae (17.9% of iso-lates).
Areas endemic for visceralleishmaniasisA further 504 rodents (Gerbillidae, Crice-tidae) were caught during 1994 to 2000 in 2areas endemic for VL: Meshkin-Shahr dis-trict (north-west) and Dashti and Dash-testan districts (south). Leishmania para-sites were seen in livers and spleens of 69(13.7%) of these rodents by microscopy(Table 2).
Leishmania spp. were isolated from 2specimens of Mer. persicus and 1 specimenof Mesocricetus auratus in culture media(Table 2). Although parasites were ob-served in a few specimens of Cricetulusmigratorius, none were positive on culture.Using isoenzyme techniques the promastig-otes isolated from Mer. persicus were char-acterized as L. donovani zymodeme
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM594

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 595
Table 1 Leishmania species isolates from rodents caught inareas of the Islamic Republic of Iran endemic for cutaneuosleishmaniasis (1991–2000)
Location of capture/ No. Positive on Leishmaniarodent species tested microscopy species
No. % identified
North-east (Minoo Dashtdistrict)
Rhombomys opimus 27 23 85.2 L. majorMeriones libycus 1 0 0 –
South (Dashti andDashtestan district)
Tatera indica 133 6 4.5 L. majorMeriones crassus 48 0 0 –Rattus rattus 3 0 0 –Nesokia indica 3 0 0 –Mus musculus 5 0 0 –
South-east (Baluchestan)Meriones hurrianae 28 5 17.9 L. majorTatera indica 27 1 3.7 –Rattus rattus 3 0 0 –Rattus norvegicus 4 0 0 –Mus musculus 5 0 0 –Nesokia indica 2 0 0 –Funambulus pennanti 1 0 0 –
West (Mehran district)Tatera indica 22 2 9.1 L. majorNesokia indica 8 0 0 _
Central (Badrood district)Meriones libycus 36 9 25.0 L. majorRhombomys opimus 25 8 32.0 L. major
South-west (Fars province)Meriones libycus 97 34 35.1 L. majorTatera indica 21 3 14.3 –
Central (Ardakan district)Rhombomys opimus 26 3 11.5 L. majorMeriones libycus 19 3 15.8 –
Central (Sabzevar district)Rhombomys opimus 22 8 36.4 L. major and
L. turanica
Total 566 105 18.6
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM595

596 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
LON50 and those from Mes. auratus wereidentified as L. infantum LON49.
Discussion
Both CL and VL are endemic in the IslamicRepublic of Iran. Mucosal leishmaniasis isusually an extension of the cutaneous form,except for 3 cases of lesions of the palatefor which the causative organisms are un-known [20].
The cutaneous form of leishmaniasis isseen in 2 forms: anthroponotic and zoonot-ic. Anthroponotic CL is endemic in manylarge- and medium-size cities, as well asvillages in the suburbs of these foci. Themain reservoir host of CL is man, althoughthe lesions have been observed on dogs inTehran, Mashad, Shiraz and Kerman [9].Zoonotic CL is endemic in many foci in thenorth, east and south of the country [9].This is essentially a disease of gerbils,transmitted by sand flies that live and breedin the gerbil burrows. The human disease issecondary to the infection of gerbils and is
seen only in places where the infected ger-bils live.
Our results show that R. opimus (greatgerbil) is the principal reservoir host ofzoonotic CL in the central and north-eastparts of the country. Mer. libycus (Libyanjird) was also found to be infected and canact as a secondary reservoir host in the ab-sence of R. opimus. Of course, in someareas from the centre and south of thecountry, gerbils have become the primaryreservoir of zoonotic CL due to ecologicalchanges [21]. Other foci are in Turkemen-Sahara, Lotfabad and Sarakhs, that is theborder with Turkemenistan Republic, Es-farayen in Khorasan, Bakran in Semnan,Abarkuh in Yazd, Neiriz and Estahban inFars provinces. Natural Leishmania spp.infection of R. opimus is found in Abardejof Varamin near Tehran but far from humanresidences and Leishmania species havenot yet been determined [9,22].
T. indica (Indian jird) is the main reser-voir host of zoonotic CL in foci of thesouth-west and south of the country.
Table 2 Leishmania species isolates from rodents caught in areas of the IslamicRepublic of Iran endemic for visceral leishmaniasis (1994–2000)
Location of capture/ No. Positive on Positive on Leishmania speciesrodent species tested microscopy culture media and zymodemes
identifiedNo. % No. %
Meshkin-ShahrCricetulus migratorius 15 2 13.3 0 0 –Mesocricetus auratus 2 1 50.0 1 50.0 L. infantum LON49Meriones persicus 394 66 16.8 2 0.5 L. donovani LON50Mus musculus 7 0 0 0 0 –Allactaga spp. 1 0 0 0 0 –
Dashti and Dashtestandistrict
Tatera indica 85 0 0 0 0 –
Total 504 69 13.7 3 0.6
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM596

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 597
These areas include the Iran–Iraq bordersfrom Sumar to the Gulf, all the provincesof Khuzestan and some parts of Ilam,Bushehr and Hormozegan [1,11,23].
In foci of the south-east of the country,the main animal reservoir is Mer. hurrianae(Indian desert jird). These areas include thesouthern parts of Baluchistan, Dashtyari,Konarak and Chabahar areas. This type ofzoonotic CL is similar to the foci of the dis-ease reported from Rajasthan in India[4,7,9].
The visceral form of leishmaniasis isseen in sporadic form all over the IslamicRepublic of Iran and is endemic in Ardebiland east Azerbaijan provinces in the north-west, and in Fars and Bushehr in the south.Wild and domestic dogs are the main reser-voir hosts of VL [12]. In this study,amastigotes were observed in 13.7% of therodents on microscopic examination of thesmears prepared from internal organs.
L. donovani LON-50 was isolated from2 specimens of Mer. persicus (Persian jird).It seems to transmit from infected rodentsto humans in these endemic areas. L. in-fantum LON-49 was isolated from 1 spec-imen of Mes. auratus (golden hamster).This species of Leishmania is zoonotic andhad been previously isolated from humans[10] and dogs in the Meshkin-Shahr area[12], and also from dogs and foxes in theDashti district of Bushehr province [11]. L.infantum had been isolated from Rattus rat-tus (black rat) in Italy and Iraq [24]. In onestudy, Mer. persicus was reported to be nat-urally infected with Leishmania spp. in eastAzerbaijan, in the north-west of the IslamicRepublic of Iran. In the smears preparedfrom the cutaneous lesion of this gerbil,considerable numbers of amastigotes wereseen. However, microscopic examination
of the smears prepared from the internalorgans and blood of this rodent did notshow any amastigotes [25]. In the otherstudy that was carried out in the Semes-kandeh area of Mazanderan province in thenorth of the Islamic Republic of Iran,Leishmania spp. infection was reported ininternal organs of R. rattus but Leishmaniaparasites were not isolated from them(Gholami, personal communication).
In conclusion, this study has shownthat rodents harbour Leishmania spp. in-fection and may therefore have a role intransmission of leishmaniasis to humans,particularly to children. Further ecologicaland biological studies of rodents and sandflies are necessary in endemic foci ofzoonotic VL from the Islamic Republic ofIran until the exact role of the rodents asanimal reservoirs is clarified completely.
Acknowledgements
We are very grateful to the field staff of theprovincial health department of Isfahan,Golestan, Bushehr, Baluchistan, Ilam, Farsand Yazd provinces. The authors would liketo thank Dr D. Evans and Dr S. Mazlumifrom the London School of Hygiene andTropical Medicine; Dr J.P. Dedet fromMontpellier, France, for isoenzyme charac-terization of the Leishmania isolates; andDr K.P. Chang from Chicago University,USA, and student Kayako for performingPCR-RFLP. Thanks are also due to Dr Y.Hamzavi and Dr H. Kathiri for field activi-ties. This investigation was supported bythe School of Public Health and Institute ofPublic Health Research, Tehran Universityof Medical Sciences.
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM597

598 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
References
1. Javadian E et al. Reservoir host of cuta-neous leishmaniasis in Iran [Abstract].Proceedings of the XIIth InternationalCongress of Tropical Medicine and Ma-laria. Amsterdam, The Netherlands, 18–23 September, 1988.
2. Nadim A, Seyedi-Rashti MA, Mesghali A.Epidemiology of cutaneous leishmania-sis in Turkemen Sahara, Iran. Journal oftropical medicine and hygiene, 1968,71:238–9.
3. Nadim A, Seyedi-Rashti MA. A brief re-view of the epidemiology of varioustypes of leishmaniasis in Iran. Actamedica iranica, 1971, XIV:99–106.
4. Seyedi-Rashti MA et al. Cutaneousleishmaniasis in Baluchistan, Iran [Ab-stract and Poster]. Proceedings of the XIInternational Congress of Tropical Medi-cine and Malaria. Calgary, Canada, 16–22 September, 1984.
5. Yaghoobi-Ershadi MR et al. Epidemiol-ogy study in a new focus of cutaneousleishmaniasis due to Leishmania majorin Ardestan town, Central Iran. Actatropica, 2002, 79:115–21.
6. Hamzavi Y et al. Epidemiological studiesof cutaneous leishmaniasis (human in-fection, animal reservoirs) in Dashti andDashtestan districts, Bushehr province.Iranian public health, 2000, 29(1–4):177–91.
7. Control of the leishmaniases. Report ofa WHO Expert Committee. Geneva,World Health Organization, 1990:1–158(WHO Technical Report Series, No. 793).
8. Nadim A, Faghih M. The epidemiology ofcutaneous leishmaniasis in the Isfahanprovince of Iran. I. The reservoir. II. Thehuman disease. Transactions of theRoyal Society of Tropical Medicine andHygiene, 1968, 62:534–42.
9. Nadim A. Leishmaniases. In: Azizi F etal., eds. Epidemiology and control ofprevalent diseases in Iran, 2nd ed.Isfahan, Iran, Endocrine and MetabolismResearch Centre, 2000:524–34 [inFarsi].
10. Edrissian GhH et al. Visceral leishmania-sis: the Iranian experience. Archives ofIranian medicine, 1998, 1(1):22–6.
11. Mohebali M et al. Seroepidemiologicalstudy of visceral leishmaniasis amonghumans and animal reservoirs inBushehr province, Islamic Republic ofIran. Eastern Mediterranean health jour-nal, 2001, 7:912–7.
12. Mohebali M et al. Study on canine vis-ceral leishmaniasis in the various partsof Iran. Veterinary journal of Tehran Uni-versity, 2001, 56(3):55–9.
13. Mohebali M et al. Rodents: anothergroup of animal reservoir hosts of vis-ceral leishmaniasis in Meshkin-Shahrdistrict, the Islamic Republic of Iran. East-ern Mediterranean health journal, 1998,4(2):376–8.
14. Ziaei H. A field guide for identifying of Ira-nian desert mammalians, 1st ed.Tehran, Iran, Iranian Environment Orga-nization, 1996:129–87.
15. Boitani L, Bartoli S. Macdonald encyclo-pedia of mammals. London, Macdonald& Co., 1980.
16. Edrissian GH, Zovein Z, Nadim A. Asimple technique for preparation ofsmears from the ear of Rhombomysopimus for the detection of leishmanialinfection. Transactions of the Royal Soci-ety of Tropical Medicine and Hygiene,1982, 76:706–7.
17. Noyes HA, Belli AA, Maingon R. Ap-praisal of various RAPD–PCR primers
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM598

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 599
for Leishmania identification. Americanjournal of tropical medicine and hy-giene, 1996, 55(1):98–105.
18. Motazedian H, Noyes H, Maingon R.Leishmania and sauroleishmania: theuse of random amplified polymorphicDNA for identification of parasites fromvertebrates and invertebrates. Experi-mental parasitology, 1996, 83:150–4.
19. Evans DB. Handbook on isolation, char-acterization and cryopreservation ofLeishmania. UNDP/World Bank/WHOSpecial Programme for Research andTraining in Tropical Diseases. Geneva,World Health Organization, 1989:14–32.
20. Yaghoobi MR et al. Mucosal leishmania-sis: report of three cases. Archives of Ira-nian medicine, 2001, 4(3):138–40.
21. Yaghoobi-Ershadi MR, Akhavan AA,Mohebali M. Meriones libycus andRhombomys opimus (Rodentia: Ger-billidae) are the main reservoir hosts in anew focus of zoontic cutaneous leishma-niasis in Iran. Transactions of the RoyalSociety of Tropical Medicine and Hy-giene, 1996, 90(5):503–4.
22. Seyedi-Rashti MA et al. A new focus ofzoonotic cutaneous leishmaniasis nearTehran, Iran. Proceedings of the VIIth In-ternational Congress of Parasitology,Paris, France, 20–24 August. Bulletin dela Societe Francaise de Parasitology,1990, (suppl.)2:1145.
23. Javadian E et al. Confirmation of Tateraindica (Rodentia:Gerbillidae) as themain reservoir host of zoonotic cutane-ous leishmaniasis in the west of Iran. Ira-nian journal of public health, 1998,27(1–2):55–60.
24. Desjeux P. Information of epidemio-logy and control of the leishmaniasesby country or territory. Geneva, WorldHealth Organization, 1991 (WHO/LEISH/91.30).
25. Edrissian GH, Ghorbani M, Tahvildar-Bidruni G. Meriones persicus, anotherprobable reservoir of zoonotic cutane-ous leishmaniasis in Iran. Transactionsof the Royal Society of Tropical Medicineand Hygiene, 1975, 69(5–6):517–9.
16 Characterization of Leishmania.pmd 8/17/2005, 11:08 AM599

600 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Smoking in Oman: prevalence andcharacteristics of smokersA.A. Al Riyami1 and M. Afifi1
1Department of Research and Studies, Ministry of Health, Muscat, Oman.Received: 07/01/03; accepted: 20/10/03
ABSTRACT We carried out a cross-sectional survey to study the prevalence and the characteristics ofcurrent and former smoking among Omani adults. Crude prevalence of current smoking was 7.0% (males13.4%, females 0.5%); 2.3% were former smokers. The overall highest prevalence of current smoking(11.1%) was observed in those 40–49 years (18.7% of males, 0.9% of females). Older age (≥ 40 years),higher educational level and larger family size were protective against smoking. Mean age for startingsmoking was 18.7 years for males and 24.3 years for females. Although smoking prevalence is low in Oman,prevention should be addressed in health education programmes, with the emphasis on heightening aware-ness in adolescents. Government action, e.g. tobacco taxation, clean air laws and bans on advertising, isalso recommended.
Le tabagisme à Oman : prévalence et caractéristiques des fumeursRÉSUMÉ Nous avons réalisé une enquête transversale pour étudier la prévalence et les caractéristiquesdes fumeurs actuels et des anciens fumeurs parmi les Omanais adultes. La prévalence brute du tabagismeactuel était de 7,0 % (hommes : 13,4 %, femmes : 0,5 %) ; 2,3 % étaient des anciens fumeurs. La préva-lence globale du tabagisme actuel la plus élevée (11,1 %) était observée chez les personnes de 40 à 49 ans(18,7 % d’hommes, 0,9 % de femmes). Un âge plus avancé (≥ 40 ans), un niveau d’études plus élevé et unefamille de plus grande taille représentaient une protection contre le tabagisme. L’entrée dans le tabagismeavait lieu à un âge moyen de 18,7 ans chez les hommes et 24,3 ans chez les femmes. Bien que la prévalencedu tabagisme soit faible à Oman, la prévention devrait être envisagée dans le cadre des programmesd’éducation sanitaire, en mettant l’accent sur la sensibilisation chez les adolescents. Une action des pou-voirs publics, par exemple par les taxes sur le tabac, les lois sur la pureté de l’air et l’interdiction de lapublicité, est également recommandée.
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM600

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 601
Introduction
Worldwide, it is estimated that tobaccocauses about 8.8% of deaths (4.9 million)and 4.1% of disability adjusted life years(59.1 million). Attributable mortality isgreater in males (13.3%) than in females(3.8%) [1]. Tobacco use is a growinghealth concern in the developing world,particularly in places where disposable in-come is increasing [2]. Smoking preva-lence has increased in adolescents since1991 even though there has been a declinein the overall prevalence of smoking inmany industrialized countries [3].
According to the most recent estimateby the World Health Organization, 4.9 mil-lion people worldwide died in 2000 as a re-sult of their addiction to nicotine, about halfof them prematurely [1]. Developing coun-tries already account for half of all deathsattributable to tobacco. The proportion willrise to 7 out of 10 by 2025 because smok-ing prevalence has been increasing in manylow-income and middle-income countrieswhile it is falling in richer countries, espe-cially among men [4]. Lam et al. concludedthat among middle aged men the proportionof deaths caused by smoking was morethan twice as great in Hong Kong in 1998as in mainland China 10 years earlier [5].Another study on smoking and mortalityfrom tuberculosis and other diseases in In-dia showed that the death rates from medi-cal causes of ever-smokers were doublethose of never smokers [6]. In Saudi Ara-bia, Al Khadra found that smoking was themain risk factor for having acute myocar-dial infarction at a young age (< 45 years),followed by low high-density lipoproteincholesterol, high low-density lipoproteincholesterol and diabetes [7].
Oman and other oil-producing countriesin the Middle East have experienced rapideconomic, sociodemographic and epidemi-
ological transitions over the past 3 decades.The sociocultural and economic patterns ofthe Omani population do not typically cor-respond to either the Western communityor to the developing countries in Asia. Thisis why data on smoking in Oman would bevaluable and therefore why we conductedour study.
The aim of the study was to estimateprevalence of smoking among adults ofboth sexes aged 20 years and above, tostudy the characteristics of current smok-ers, to identify the age of starting smoking,reasons for smoking and factors related tosmoking cessation in a community-basedsurvey as a part of the Omani NationalHealth Survey, 2000.
Methods
SampleThe sample for the survey was selected tobe representative of the nation as a whole.The survey adopted a multi-stage, stratifiedprobability-sampling design. In the firststage, all 10 regions of Oman were selectedand the sample was distributed accordingto proportional allocation of the populationin each. In each region, 1 or more wilayat(districts) were randomly chosen accord-ing to the size of the population. The num-ber of wilayat selected was 16 out of a totalof 59 (27%). Then, each wilayat was strat-ified into 2 strata; the first stratum was thewilayat centre, covering the urban area andthe second stratum was the villages or re-mote areas, the rural areas. The urban:ruralratio was 2:1, which is similar to the ratio inthe 1993 national census [8].
The second stage was the random se-lection of the population sampling units ineach stratum. These population samplingunits were the census units which wereused during the 1993 population census.
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM601

602 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
The third stage was the selection of house-holds from these population sampling units.Maps of the selected population samplingunits were updated and a complete listingof all Omani households in each unit wasmade to obtain the sampling frame, thenhouseholds were systematically randomlyselected. All individuals aged 20 years andabove in the selected household were invit-ed to participate in the survey. The totalnumber of households selected was 1968with a total of 7011 people fulfilling the se-lection criteria. The prevalence of the leastexpected disorder of the lifestyle risk fac-tors studied (smoking rate among femaleadults, 0.2%) was used to calculate thesample size of the survey. The responserate varied, according to the type of mea-surement or completed laboratory investi-gation, from 83% (for fasting blood sugar)to 91.5% (for blood pressure measure-ment).
Questionnaire and measurementsThe questionnaire covered demographicand socioeconomic data (age, sex, maritalstatus, educational status, work status,family size and place of residence) and in-cluded questions related to current smok-ing, age of starting smoking, number ofcigarettes smoked per day, type of tobaccoproduct smoked, reasons for smoking, his-tory of temporarily quitting smoking for ayear or more, being a former smoker andthe number of years of smoking cessationand reasons for smoking cessation. Mea-surements of blood pressure, weight,height, waist circumference and hip cir-cumference were registered in the ques-tionnaire. World Health Organization proce-dures were used for taking the measure-ments [9]. The questionnaire also includeditems for the laboratory investigations forfasting blood sugar and serum cholesterol.
Specimen collection and analysisThe survey was carried out by 25 teams.Each consisted of a nurse to take the mea-surements, a laboratory technician to drawthe blood samples, a health educator to in-terview the subjects, a health inspector totransport the samples to the laboratory anda field supervisor (statistician) to superviseand review the questionnaires during fieldoperations. They were all trained on themethodology of the survey for 2 weeks.
The eligible members of the selectedhouseholds were asked to start fasting 1–2hours before midnight the night before theywere due a visit by the survey team. Thefollowing morning at 07.00 the participantswere interviewed, measurements were tak-en, and venous fasting blood samples werecollected. Fasting blood samples for glu-cose were collected in sodium fluoride po-tassium oxalate tubes, labelled andtransferred immediately with laboratoryforms to the laboratory in the wilayat hos-pital in coldboxes. Samples were then im-mediately centrifuged, the plasma wasseparated and fasting plasma glucose wasdetermined by a glucose oxidase method onthe same day using the Hitachi 911 auto-mated clinical chemistry analyser (Boe-hringer Mannheim, Germany) [10]. Thesame manufacturer supplied the reagents.The samples for estimation of cholesterolwere collected in tubes containing lithiumheparin anticoagulants and transferred tothe laboratory in the same way. Estimationof serum cholesterol was done by enzy-matic colorimetric method using the Hita-chi 911 automated clinical chemistry ana-lyser [11].
Diagnostic criteriaThe World Health Organization criteria(1999) for diagnosis of hypertension, hy-percholesterolaemia, anthropometric mea-
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM602

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 603
surement and glucose intolerance wereused [12].
Prevalence of hypertension was esti-mated by adding the number of people self-reporting systolic or diastolic hypertension(whether their blood pressure was normalor not at the screening time) and the num-ber of people with mean of 2 readings≥ 140 mmHg systolic blood pressure or≥ 90 mmHg diastolic phase 5 blood pres-sure i.e. either isolated systolic or diastolichypertension. Blood pressure was taken ina sitting position at 5-minute intervals; theaverage of these readings was calculated tothe nearest 5 mmHg.
High total cholesterol was defined as≥ 5.2 mmol/L or ≥ 200 mg/dL.
Participants were considered under-weight if their body mass index (BMI) was< 18.5 kg/m2, normal if their BMI was18.5–24.9 kg/m2, overweight if their BMIwas 25.0–29.9 kg/m2, obese if their BMIwas 30.0–39.9 kg/m2, morbid obese if theirBMI was ≥ 40.0 kg/m2.
Abnormal waist:hip ratio [waist circum-ference (m)/hip circumference (m)] (cen-tral obesity) was defined as ≥ 0.85 forfemales and ≥ 0.95 for males.
Impaired fasting glucose (IFG) wasdefined as fasting blood glucose 6.1–6.9mmol/L. Diabetes prevalence was estimatedby adding the number of people selfreportingdiabetes and the number of people with fast-ing blood glucose ≥ 7.0 mmol/L. The totalnumber of participants with IFG was thesum of those with IFG and those with dia-betes.
Pilot studyA pretest was carried out to test the house-holds and the individual questionnaires andforms to obtain information about opera-tional and organizational procedures and toget an indication of the general response tophysical examination and specimen collec-
tion. A total of 120 households were se-lected from different areas in Muscat gov-ernorate. All the survey questionnaires andforms were interpolated and were revisedby experts. Measurements and specimenswere also taken. The questionnaires andforms and some organizational procedureswere adjusted after the debriefing sessionfor interviewers and supervisors. Theproblems, performance rates and generalreceptivity to the survey were analysed anddiscussed.
Data processing and analysisData entry was done using Epi-Info, ver-sion 6. The preparation of the data file wascompleted by July 2000. Respondentswere defined as current smokers if theywere smoking at the time of the survey andhad smoked more than 100 cigarettes intheir lifetime; they were defined as formersmokers if they had smoked more than 100cigarettes in their lifetime but no longersmoked; and they were defined as neversmokers if they had never smoked or hadsmoked less than 100 cigarettes in theirlifetime.
Analysis of the data was done usingSPSS, version 5.0. Data were given ascounts, means and percentages. Likelihoodchi-squared test examined the distributionof data while group means were comparedusing analysis of variance. Logistic regres-sion was conducted to test the most impor-tant independent associated factors (age,level of education, marital status, familysize, residence, work status, hypertension,total IFG, hypercholesterolaemia, obesityor central obesity) with the dependent orthe outcome variable (current smoking)with and the adjusted odds ratio (OR) wascalculated for these factors. Logistic re-gression determines the independence ofthe associations observed in bivariate anal-ysis by controlling for potential confound-
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM603

604 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
ing variables. The OR shows the change inthe odds of the dependent variable whenthe independent changes from 0 to 1. P <0.05 was considered statistically signifi-cant.
Results
A total of 7011 respondents aged 20 yearsand over [mean age 38 years, standard de-viation (SD) 15.2] participated in the study,3506 of them males (50% of the sample,mean age 38.4 years, SD = 16.7) and 3505females (mean age 37.6 years, SD = 15.6).Overall, 7.0% of the respondents wereclassified as current smokers, 2.3% asformer smokers and 90.7% as never smok-ers.
The majority of current smokerssmoked cigarettes (82.9%), 6.4% smokedshisha (water pipe), 7.9% smoked gadou(gouza, a differently shaped pipe that usesdifferent tobacco and a more direct burningmethod), 7.7% smoked a pipe, and 4.5%used other tobacco products e.g. chewingtobacco.
Current smokers constituted 13.4% ofmales; 4.6% were former smokers and82.1% were never smokers. Only 0.5% offemales were current smokers, 0.1% wereformer smokers and 90.4% were neversmokers. Of current smokers, 16.7% had ahistory of smoking cessation for 1 year ormore then returned to smoking; 41.8% ofthem stopped smoking for only 1 year.
Table 1 shows the number of currentsmokers according to age group, maritalstatus, education level, etc. In males and inthe overall sample, smoking prevalencewas highest in the age group 40–49 years,with 18.7% of males, 1.0% of females, and11.1% overall in this age group (χ2 test sig-nificant at P < 0.05).
For the whole sample, the prevalence ofsmoking was also significantly associated
with marital status, education level, workstatus and family size. For males, the samepattern was shown except for work status(χ2 test significant at P < 0.05). For fe-males, smoking was only associated withage and education level (Fisher exact testsignificant at P < 0.05). Smoking was notsignificantly associated with total IFG forthe overall sample, males or females,whereas it was significantly associatedwith hypertension for all 3 groups. Wefound no association between smoking andhypercholesterolaemia, obesity or centralobesity in the overall sample or the malesub-sample.
Using multiple logistic regression, age,level of education, marital status and familysize were the strongest determinants ofcurrent smoking for males (Table 2). Thetest was not done for the female group dueto the very low prevalence.
The majority of male smokers (58.7%)started smoking before the age of 20 years,while among females the highest percent-age (31.6%) started smoking at a later age(20–29 years) (Table 3). The mean age ofstarting smoking was 18.7 years for malesand 24.3 years for females and the differ-ence was significant at P < 0.05 by analysisof variance test (data not shown).
Of the current male smokers, 49.7%smoked 10 cigarettes or fewer per day,38.0% smoked 11–20 cigarettes per day(Table 4), while former smokers smokedfewer cigarettes: 62.3% smoked 1–10 cig-arettes per day. The same pattern was no-ticed for the overall sample.
Of the current smokers, 46.0% saidthat the reason for smoking was out ofhabit, while 21.5% of them said smokinghelped them to relax. In addition, 13.4% ofthe sample smoked because their friendssmoked and 11.5% looked on smoking asleisure (data not shown in tables).
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM604

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 605
Table 1 Prevalence of smoking in males and females for some demographic andhealth characteristics
Characteristic Males (n = 3506) Females (n = 3505) Total (n = 7011)n No. % n No. % n No. %
Age group (years)20–29 1454 167 11.5 1431 2 0.1 2885 169 5.930–39 674 118 17.5 789 5 0.6 1463 123 8.440–49 465 87 18.7 344 3 0.9 809 90 11.150–59 391 57 14.6 552 4 0.7 943 61 6.560–64 189 14 7.4 136 3 2.2 325 17 5.2≥ 65 329 26 7.9 249 2 0.8 578 28 4.8
Marital statusMarried 2327 337 14.5 2336 14 0.6 4663 351 7.5Single, divorced,widowed 1168 131 11.2 1156 5 0.4 2324 136 5.9
Education levelIlliterate/preparatoryschool 2492 413 16.6 2658 19 0.7 5150 432 8.4Secondary and above 964 52 5.4 789 0 0.0 1753 52 3.0
Work statusWorking 2348 327 13.9 429 0 0.0 2777 327 11.8Not working 1141 140 12.3 3044 18 0.6 4185 158 3.8
ResidenceUrban 2592 343 13.2 2548 17 0.7 5140 360 7.0Rural 910 126 13.8 953 2 0.2 1863 128 6.9
Family size≤ 10 members 1818 286 15.7 1870 12 0.6 3688 298 8.1> 10 members 1684 183 10.9 1631 7 0.4 3315 190 5.7
Total IFGNormal 2340 317 13.5 2441 13 0.5 4781 330 6.9TIFG 531 76 14.3 471 6 1.3 1002 82 8.2
Blood pressureNormal 1975 252 12.8 2312 7 0.3 4287 259 6.0Hypertension 1079 168 15.6 1042 12 1.2 2121 180 8.5
CholesterolNormal 1747 240 13.7 1726 10 0.6 3473 250 7.2Hypercholesterolaemia 1171 157 13.4 1201 9 0.8 2372 166 7.0
ObesityNo 1654 253 15.3 1694 10 0.6 3348 263 7.9Yes 1417 171 12.1 1659 9 0.5 3076 180 5.9
Central obesityNo 1947 258 13.3 1179 8 0.7 3126 266 8.5Yes 896 122 13.6 2145 11 0.5 3041 133 4.4
Some categories do not sum to the total sample due to missing data.TIFG = total impaired fasting glucose.
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM605

606 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Of the current smokers, 17.12% had ahistory of temporarily stopping smokingfor 1 year or more. Of these, 40.7% hadstopped for 1 year, 45.1% for 2–5 yearsand 14.2% for more than 5 years then re-turned to smoking. As regards former
smokers, 21.1% stopped smoking for cur-ative reasons, 33.6% because in the nega-tive effects of smoking and 27.5% realizedthat there was no benefit in smoking. About7% of the former smokers had ceasedsmoking for 1 year, 31.5% for 2–5 years,24.2% for 6–10 years and the rest for morethan 10 years. There was no significant as-sociation between the reason for smokingcessation and the number of years ofsmoking cessation. (χ2 = 0.01, P = 0.9)(data not shown in tables).
Discussion
There are few published data on the epide-miology of smoking in Gulf countries, in-cluding Oman. Comparable data on theprevalence of smoking are not widely avail-able and are often inaccurate, especiallywhen age-specific data are required. Moreimportantly, current prevalence of smokingis a poor proxy for the cumulative hazardsof smoking, which depend on several fac-tors, including the age at which smokingbegan, duration of smoking, number ofcigarettes smoked per day, degree of inha-lation, and cigarette characteristics such astar and nicotine content or type of filter [1].Smoking is related to substantially in-creased risk of mortality from lung cancer,upper aerodigestive cancer, several othercancers, heart disease, stroke, chronic res-piratory disease and a range of other medi-cal conditions. As a result, in populationswhere smoking has been common formany decades, tobacco use accounts for aconsiderable proportion of mortality, as il-lustrated by estimates of smoking-attributable deaths in industrialized coun-tries [5,13].
In 1995, the Oman Family Health Sur-vey revealed that an estimated 6.7% ofthose aged 15 years or over were current
Table 2 Multiple logistic regression forvariables significantly associated withcurrent smoking among males
Variable OR 95% CI P
Age group (years)20–39a
≥ 40 0.61 0.47–0.79 < 0.01
Education levelIlliterate/preparatoryschoola
Secondary andabove 0.26 0.18–0.38 < 0.01
Family size< 10 membersa
≥ 10 members 0.6 0.48–0.77 < 0.01
Marital statusMarrieda
Single, divorced,widowed 0.73 0.55–0.97 0.03
OR = odds ratio.CI = confidence interval.aReference category.
Table 3 Age when started smoking forcurrent and former smokers among males,females and overall sample
Age at starting Males Females Totalsmoking No. % No. % No. %(years)
≤ 10 32 5.6 1 5.3 33 5.6
11–14 81 14.3 3 15.8 84 14.3
15–19 221 38.8 4 21.1 225 38.3
20–29 195 34.3 6 31.6 201 34.2
30–39 31 5.4 3 15.8 34 5.8
≥ 40 9 1.6 2 10.5 11 1.9
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM606

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 607
smokers, 13.2% for males and 0.2% forthe female respondents (A.J.M. Sulaiman,A. Al Riyami, S. Farid, unpublished data,1995). The results of the 1995 survey wereonly descriptive in nature and there was,therefore, a need to study the epidemiologyand correlates of smoking. The smokingrate in our study did not show any signifi-cant rise compared to 1995. The preva-lence of smoking in Oman is lower thanthat in other Gulf or Asian countries. InKuwait, smoking rate was 38.1% amongphysicians [14], 30% among male students[15], 37% among married men and 0.5%among married women [16]. In Saudi Ara-bia, the 1994 smoking rate was 40.0% formales and 8.2% for females [17]. In Bahr-ain, in a study conducted in the year 2000,the prevalence of smoking was high forboth sexes: 32.1% among men and 20.7%among women aged 30–79 years [18]. InChina, the rate was much higher for males,66.6%, whereas it was low, 1.7%, amongfemales [19].
Women in Oman as well as other devel-oping countries tend to have lower rates ofsmoking than men [20, A.J.M. Sulaiman,A. Al Riyami, S. Farid, unpublished data,
1995]. They also start smoking later thanmen and smoke fewer cigarettes. This ismainly the result of sociocultural, religiousor economic factors. In some societies, itmay be considered improper or indecentfor females to be seen smoking in public; inaddition there may be religious or economicarguments against it.
Smoking rates were significantly lowerin people having a higher educational level(secondary and above) using bivariate andmultivariate analysis. The same resultswere found by Memon et al. in Kuwait[20]. In contrast, Saeed, Khoja and Khan inSaudi Arabia found that smoking rates weresignificantly higher among literate than illit-erate people, which could be explained bysmoking being popular in higher socialclasses as it could denote prestige [17].Older age was a protective factor againstsmoking; the majority of the current andformer smokers in our study, almost 55%,began smoking in adolescence. For thisreason, a major effort should be directedtowards implementing health education forchildren and adolescents. Anti-tobacco ed-ucation should be included as an integralpart of the curriculum in schools.
Table 4 Number of cigarettes smoked per day for former and current smokers
No. Males Females Totalcigarettes Current Former Current Former Current Formerper day smokers smokers smokers smokers smokers smokers
No. % No. % No. % No. % No. % No. %
≤ 10 217 49.7 94 62.3 10 62.5 2 66.7 227 50.1 96 62.3
11–20 166 38.0 44 29.1 5 31.3 1 33.3 171 37.8 45 29.2
21–30 33 7.6 6 4.0 1 6.3 0 0.0 34 7.5 6 3.9
31–40 21 4.8 4 2.6 0 0.0 0 0.0 21 4.6 4 2.6
> 40 0 0.0 3 2.0 0 0.0 0 0.0 0 0.0 3 1.9
Mean (SD) 13.8 (9.3) 11.8 (10.3) 10.2 (8.5) 9.7 (9.1) 13.7 (9.3) 11.8 (10.3)
SD = standard deviation.
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM607

608 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Conclusion andrecommendations
Although the study revealed lower rates ofsmoking in Oman in comparison with otherGulf countries, anti-tobacco programmesshould be vigorously implemented to pre-vent the health consequences of smoking.Tobacco is not cultivated or produced inOman. A pack of 20 imported cigarettescosts around US$ 1, and the war againsttobacco is not easy. Children and adoles-cents should be targeted, and reasons forsmoking cessation and the diseases associ-ated with smoking should be taken intoconsideration in planning a health educationprogramme.
Because some of the issues concerningtobacco control may be beyond the domainof national policies and legislation, tobaccocontrol policies are not being implementedworldwide at a rate that current scientificknowledge about the dangers of toba-
cco warrants. International collaborationshould be aimed for in order to share policyand programme information and implementtobacco control strategies. Governmentaction in the form of tobacco taxation;clean indoor air laws in public placesthrough legislation and enforcement; com-prehensive bans on advertising of tobaccothrough legislation; dissemination of infor-mation through health warning labels,counter-advertising and various consumerinformation packages; and nicotine re-placement therapy targeting current smok-ers aged 20–60 years are recommended.The benefits of reduction in tobacco usenow, although taking longer to materializethan those resulting from reduction ofsome other risks, are great and long lasting.This is seen in the estimated tens of mil-lions of healthy life years to be saved by2010 and 2020 as a result of preventing andreducing tobacco use [1].
References
1. The world health report 2002: reducingrisks, promoting healthy life. Geneva,World Health Organization, 2002.
2. World Bank. World development report1993: investing in health. New York, Ox-ford University Press, 1993.
3. Wechsler H et al. Increased levels ofcigarette use among college students:a cause for national concern. Journalof the American Medical Association,1998, 280(19):1673–8.
4. de Beyer J, Brigden LW, eds. Tobaccocontrol policy: strategies, success, andsetbacks. Washington, World Bank andResearch for International Tobacco Con-trol, 2003:1.
5. Lam TH et al. Mortality and smoking inHong Kong: a case–control study of all
adult deaths in 1998. British medicaljournal, 2001, 323(7309):361–7.
6. Gajalakshmi V et al. Smoking and mor-tality from tuberculosis and other dis-eases in India: retrospective study of43 000 adult male deaths and 35 000controls. Lancet, 2003, 362(9383):507–15.
7. Al Khadra AH. Clinical profile of youngpatients with acute myocardial infarctionin Saudi Arabia. International journal ofcardiology, 2003, 91(1):9–13.
8. Facts and figures: Special issue on devel-opment efforts 1970–2000. Muscat, Oman,Ministry of National Economy, Informationand Publication Centre, 2000: 4.
9. King H, Minjoot-Pereira G. Diabetes andnoncommunicable disease risk factor
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM608

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 609
surveys: a field guide. Geneva, WorldHealth Organization, 1999.
10. Kadish AH, Hall DA. A new method forthe continuous monitoring of bloodglucose by measurement of dissolvedoxygen. Clinical chemistry, 1965, 11(9):869–75.
11. Allain CC et al. Enzymatic determinationof total serum cholesterol. Clinical chem-istry, 1974, 20(4):470–5.
12. Definition, diagnosis and classificationof diabetes mellitus and its complica-tions. Report of a WHO consultation. Part1: Diagnosis and classification of diabe-tes mellitus. Geneva, World Health Orga-nization, 1999 (WHO/NCD/NCS/99.2).
13. Boyle P. Cancer, cigarette smoking andpremature death in Europe: a reviewincluding the Recommendations of Eu-ropean Cancer Experts ConsensusMeeting, Helsinki, October 1996. Lungcancer, 1997, 17(1):1–60.
14. Bener A, Gomes J, Anderson JA. Smok-ing habits among physicians in two Gulfcountries. Journal of the Royal Society ofHealth, 1993, 113(6):298–301.
15. Moody PM, Al Bustan A, Al Shatti A.Cigarette smoking habits among Kuwait
University male students pre- and post-invasion periods. Journal of the KuwaitMedical Association, 1996, 28(3):274–8.
16. Radovanovic Z, Shah N, Behbehani J.Prevalence of smoking among currentlymarried Kuwaiti males and females. Eu-ropean journal of epidemiology, 1999,15(4):349–54.
17. Saeed AA, Khoja TA, Khan SB. Smokingbehaviour and attitude among adultSaudi nationals in Riyadh City, SaudiArabia. Tobacco control, 1996, 5(3):215–9.
18. Hamadeh RR, Musaiger AO. Life stylepatterns in smokers and non-smokers inthe state of Bahrain. Nicotine and to-bacco research, 2000, 2(1):65–9.
19. Gong YL et al. Cigarette smoking inChina. Prevalence, characteristics andattitudes in Minhang district. Journalof the American Medical Association,1995, 274(15):1232–4.
20. Memon A et al. Epidemiology of smokingamong Kuwaiti adults: prevalence, char-acteristics, and attitudes. Bulletin ofthe World Health Organization, 2000,78(11):1306–15.
17 Smoking in Oman.pmd 8/17/2005, 11:08 AM609

610 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Some risk factors for hypertension inthe United Arab EmiratesS. Sabri,1 A. Bener,2 V. Eapen,1 M.S.O. Abu Zeid,3 A.M. Al-Mazrouei 4 and J. Singh5
1Department of Psychiatry, Faculty of Medicine and Health Science, UAE University, United Arab Emirates.2Department of Medical Statistics and Epidemiology, Hamad Medical Corporation and School of Epidemiologyand Health Sciences, University of Manchester, United Kingdom.3Primary Health Care Clinic, Oud Al Thoba, Ministry of Health, Al-Ain, United Arab Emirates.4Khalifa Hospital, Abu Dhabi Health Authority, Abu Dhabi, United Arab Emirates.5Department of Biological Sciences, University of Central Lancashire, United Kingdom.Received: 22/06/03; accepted: 23/12/03
ABSTRACT A case–control study evaluated the relationship between hypertension and socioeconomic andlifestyle factors in Al-Ain city. The survey included 426 hypertensive adults aged 20–65 years attending urbanand semi-urban clinics and a randomly selected sample of 436 normotensive controls. Hypertension amongcases was higher for men, age 40–49 years, non-UAE nationals, urban living, currently married, havingchildren, illiterate, administrative/professional job, living in traditional house and low income. There weresignificant differences between cases and controls with regard to obesity, raised cholesterol level, lowphysical activity and family history of heart disease, kidney disease or diabetes. Multivariate logistic regres-sion analysis revealed that obesity, medium/high income, history of diabetes, low physical activity and having3+ children were significantly associated with hypertension.
Certains facteurs de risque d’hypertension aux Émirats arabes unisRÉSUMÉ Une étude cas-témoins a évalué la relation entre l’hypertension et des facteurs socio-économiques et liés au mode de vie dans la ville d’Al-Ain. L’étude comprenait 426 adultes hypertendus âgésde 20 à 65 ans qui consultaient dans des dispensaires urbains et semi-urbains et un échantillon, sélectionnéde manière aléatoire, de 436 témoins normotendus. L’hypertension parmi les cas était plus élevée chez leshommes, âgés de 40 à 49 ans, non ressortissants des Émirats arabes unis, vivant en milieu urbain, mariésau moment de l’étude, ayant des enfants, analphabètes, occupant un emploi administratif/professionnel,vivant en maison traditionnelle et ayant un faible revenu. Il y avait des différences significatives entre les caset les témoins concernant l’obésité, un taux de cholestérol élevé, une activité physique faible et des antécé-dents familiaux de maladie cardiaque, de maladie rénale ou de diabète. L’analyse de régression logistiquemultivariée a révélé que l’obésité, un revenu moyen/élevé, des antécédents de diabète, une activité phy-sique faible et le fait d’avoir plus de trois enfants étaient significativement associés à l’hypertension.
18 Some risk factors.pmd 8/17/2005, 11:08 AM610

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 611
Introduction
The United Arab Emirates (UAE), like otherdeveloping countries, has undergone rapidchanges during the past 2 decades [1]. Thediscovery of oil in the middle of the lastcentury has contributed to significant so-cial change, and UAE, along with otherGulf Arab states, have experienced a rapidtransition in its socioeconomic status. Peo-ple in UAE now enjoy a high standard ofliving and substantial improvements in theirliving conditions. There has been a dramat-ic rise in the national economy, expressedin terms of per capita income. In 2001, thegross domestic product (GDP) per capitawere estimated as US$ 22 800. The infantmortality rate has decreased from 10.5 per1000 live births in 1981 to 6.6 in 2000 andlife expectancy has increased from 68years in 1977 to 75 years in 2000 (Ministryof Health, Annual Report, 1980–2000) [2].
Rapid economic growth in UAE has,however, brought about marked changesboth in lifestyle and in patterns of healthand disease. With the greater availability ofhousekeepers, cars, televisions and sophis-ticated household appliances, the lifestyleof the people of UAE has become moresedentary, and watching television and eat-ing snack foods are the main leisure-timeactivities. Hypertension has become one ofthe leading public health problems.
Hypertension is a major contributor toatherosclerosis-induced cardiovasculardisease [3,4]. The prevalence is higher inmen than in women below the age of 35years but by the age of 65 years the preva-lence is higher in women [5]. In elderlywomen, it is the single most important riskfactor for cardiovascular disease [6].
Data available from several EasternMediterranean countries indicate that hy-pertension is emerging as an importantcause of morbidity and mortality. Epidemi-
ological surveys on hypertension report aprevalence of 20% to 26% in the adult pop-ulation [7]. In some urban areas high bloodpressure may affect up to 30% of the adultpopulation [8]. The prevalence of hyper-tension appears to be lower in rural than inurban areas [9–11]. Other risk factors,such as obesity, dyslipidaemia, diabetes andsmoking, are also higher among hyperten-sive than normotensive people [12]. Thereis also a significant association betweenhypertension and diabetes mellitus in theUAE [3,4,13].
There have been no systematic studiesin the UAE population of the relationshipbetween health and socioeconomic factorssuch as income or demographic factors in-cluding education and occupation. Sinceeach community has its own common andunique socioeconomic determinants forcardiovascular diseases, particularly hyper-tension, it is important to study these vari-ables in different populations. In the UAE itis believed that the effect of education andoccupation on health are much weaker thanin the Western European countries due todifferences in the educational system andthe influence of the industrial economy inEurope.
The present study in the city of Al-Ain,UAE, compared hypertensive patients at-tending primary health care clinics withnon-hypertensive controls. The aim was toinvestigate the importance of socioeco-nomic status and lifestyle habits in relationto hypertension.
Methods
This was a matched case–control study todetermine the relationship between hyper-tension and demographic, socioeconomicand lifestyle factors. The survey was con-ducted from October 2001 to July 2002.
18 Some risk factors.pmd 8/17/2005, 11:08 AM611

612 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Sampling procedureA multi-stage stratified cluster sampling de-sign was developed using the administra-tive divisions of the Al-Ain city medicalhealth district which have approximatelyequal numbers of inhabitants. In order tosecure a representative sample of the studypopulation, sampling was stratified withproportional allocation according to stra-tum size from urban and semi-urban areas.The sample size was determined on the apriori assumption that the prevalence ofhypertension in the UAE would be more orless similar to the 20% rate observed in thepilot study. Assuming the prevalence of hy-pertension to be 20% and allowing for anerror of 5% at the 1% level of significance(Type 1 error) a sample size of 500 casesand 500 matched controls would be re-quired. Of the total 22 primary health careclinics in Al-Ain medical health district, 8clinics were selected randomly (7 from ur-ban and 1 from semi-urban areas).
Selection of participantsThe study population was identified by re-cruiting consecutive hypertensive patientsaged 20–65 years attending any of the clin-ics for follow-up examination or any othercause during a specified period of time.The researcher visited each clinic in a rota-tion of 2–3 weeks and reviewed the medi-cal records of the first 20 hypertensivepatients attending any of the specified pri-mary health centres until the target samplewas reached. The exclusion criteria werenon-Arab national, any severe chronic dis-ease, age less than 20 and more than 65years.
To select the control group, for everyhypertensive case a matching pair who wasnon-hypertensive and met the same inclu-sion criteria were recruited from the sameclinic. The control group subjects wereidentified from the visitors escorting the
patients to the health care centre or thoseattending for any other reason. Cases andcontrols were matched for age, sex andnationality. Before conducting the inter-view, the investigator reviewed the medicalfile of the controls (history and examina-tion) to ensure they were suitable for theinclusion criteria of the research, in partic-ular to check that they were free of any se-vere chronic diseases.
Data collectionPatients were checked by the general prac-titioner to see whether they met the inclu-sion criteria of the study and whether theyhad any family history of severe chronicdiseases. The recruited patients were givena brief explanation about the study andwere instructed to give their consent toparticipate in the study. They were askedby either the principal investigator or thenurse to fill out the questionnaire. Qualifiednurses measured the blood pressure,height, and weight of the participants.
The survey was based on standardizedinterviews performed by trained health pro-fessionals and nurses. Informed consentwas obtained from each person whoagreed to enter the study. The participantswere interviewed about their age, sex, na-tionality, educational level, occupation,place of living (urban or semi-urban), life-style habits, previous family history of hy-pertension, diabetes or kidney problemsand current use of medication for hyper-tension and diabetes. Blood pressure wasmeasured and height and weight were mea-sured using standardized methods withparticipants wearing light clothes withoutshoes. Information on cholesterol level wascollected from the patient’s medical record.
Blood pressure measurement was car-ried out by practising nurses who weretrained for 1 week on the use of the sphyg-momanometer and how to measure blood
18 Some risk factors.pmd 8/17/2005, 11:08 AM612

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 613
pressure with patients in the sitting posi-tion. It was measured from the right upperarm, with a random zero sphygmomanom-eter with a 14 cm cuff, after the partici-pants had rested for 10 minutes and wasrecorded to the nearest mmHg. Systolicpressure was recorded at the appearance ofsounds (first Korotkoff sounds) and dias-tolic pressure was recorded at the disap-pearance of sounds (fifth Korotkoffsounds). The mean value obtained from 3readings was used in the analysis.
QuestionnaireThe questionnaire and criteria for hyperten-sion were designed to meet the objectivesof this study. A translated Arabic version ofthe questionnaire was revised by the bilin-gual physician (M.S.O.A-Z) and translatedback by a bilingual co-investigator, unac-quainted with the original English version.Both translators met and made the neces-sary corrections, modifications and re-wording after considering the minordifferences and discrepancies that had oc-curred.
In a pilot study as a part of the processof validation, the first 20 patients wereasked about the clarity and appropriatenessof items on the questionnaire. Minorchanges were made in the questionnairetaking into account their feedback.
In addition to the questionnaire, a re-view was made of the medical files of allparticipants recruited.
DefinitionsHypertension was defined according toWorld Health Organization (WHO) stan-dardized criteria [14] as systolic BP ≥ 140mmHg and/or diastolic BP ≥ 90 mmHg and/or the use of antihypertensive medication[14]. Control participants were those withsystolic blood pressure < 140 mmHg or di-
astolic < 90 mmHg and not currently takingantihypertensive medication.
BMI was calculated as the weight in ki-lograms (1 kg subtracted to allow forclothing) divided by height squared inmeters. Subjects were classified into 3 cat-egories: acceptable weight (BMI < 25 kg/m2); overweight (BMI 25–29.9 kg/m2); andobese (BMI 30+ kg/m2) [15].
Smoking behaviour was classified as:current smoker (regularly smoked at least 1cigarette per day), ex-smoker (given upsmoking for at least 6 months) and non-smoker (never smoked regularly).
High cholesterol was a total cholesterollevel > 230 mg/dL, low-density lipoprotein(LDL) cholesterol level > 130 mg/dL ortriglyceride level 200–400 mg/dL.
Alcohol consumption was defined as:never drank, current drinker or ex-drinker.No data were obtained on alcohol con-sumption among women because it is un-common among females and due to thedifficulty in gathering information on thissubject in this conservative Muslim com-munity.
Physical activity was classified as fol-lows: sedentary and relatively inactive (notpractising sports or practising < 1 hour/week); relatively active (practising sportsfor 1–3 hours a week); or highly active(practising sports for > 3 hours a week).
Healthy eating was assessed by record-ing the number of times per week that fruitand vegetables were consumed.
AnalysisThe data were analysed using SPSS, ver-sion 11. Student t-test was used to find thedifference between means of systolic anddiastolic blood pressure among hyperten-sive and non-hypertensive patients. Mann–Whitney test was used for non-parametricdistribution. The chi-squared test was used
18 Some risk factors.pmd 8/17/2005, 11:09 AM613

614 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
for comparison of frequencies between hy-pertensive and non-hypertensive peopleand the frequency of other associated so-cioeconomic and lifestyle factors. Logisticregression analysis was used to adjust forpotential confounders and to order the im-portance of risk factors (determinants) forhypertension. Logistic regression resultswere expressed as odds ratios (OR) and95% confidence interval (CI) along with Pvalues (derived from likelihood ratios sta-tistics which have a chi-squared distribu-tion). The level P < 0.05 was the cut-offvalue for significance.
Results
Of the 500 patients with hypertension re-cruited, 64 did not participate in the studyand thus 436 cases and 436 matched non-hypertensive controls were included in thefinal analysis (87.2% response rate forcompletion of the study).
Among hypertensive patients, the meanand standard deviation (SD) of blood pres-sure [systolic 141.9 (17.1) mmHg/diastolic92.7 (9.8) mmHg] was significantly higherthan for controls [systolic 116.8 (8.7)mmHg/ diastolic 75.7 (6.2) mmHg] (P <0.0001).
Among the hypertensive patients, thecategories with the highest rates of hyper-tension were: men (55.3%), age group 40–49 years (39.7%), non-UAE nationals(52%), urban living (93.3%), currentlymarried (86.7%), having children (93.6%),illiterate (33.7%), administrative/profes-sional job (40.7%), living in mud-brick ortraditional house (56.9%) and low income(< 5000 dirhams per month) (34.1%) (Ta-ble 1).
Table 1 compares the sociodemograph-ic characteristics of hypertensive patientsand normotensive controls. There werestatistically significant differences between
cases and controls in the percentage ofparticipants having 3 or more children (P =0.034), administrative/professional occu-pation (P < 0.037), (low/medium income(5000–9999 dh) (P < 0.001) and obesity(BMI > 30 kg/m2) (P < 0.001).
Table 2 compares the lifestyle habits ofcases and controls. Significantly more pa-tients with hypertension than controls werecurrent smokers (P = 0.047), consumedalcohol (P < 0.03) and had a low level ofphysical activity (P = 0.007).
Table 3 shows a comparison of themedical conditions of hypertensive patientsand non-hypertensive control participants.Significantly more patients with hyperten-sion than controls had raised cholesterollevels (P < 0.001) or a family history ofheart disease (P < 0.001), kidney disease(P < 0.033) or diabetes (P < 0.001).
A stepwise logistic regression analysiswas used to adjust for potential confound-ers and order the importance of risk factors(determinants) for hypertension status (0for non-hypertensive and 1 hypertensive)(Table 4). The logistic regression modelwas adjusted for age, sex, nationality andmarital status. As can be seen from this ta-ble, factors associated with hypertensionwere: obesity (BMI > 30 kg/m2) (P <0.0001), medium/high income (5000+ dh)(P < 0.001), family history of diabetes (P <0.001), no physical activity (P = 0.003)and a high number of children (3+) (P =0.026).
Discussion
Hypertension is the most common of thecardiovascular diseases and is one of themost powerful contributors to cardiovas-cular morbidity and mortality especiallyfrom strokes and congestive heart failure[16–18]. In the present study, hypertensionwas found to be associated with poor
18 Some risk factors.pmd 8/17/2005, 11:09 AM614

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 615
Table 1 Socioeconomic characteristics of clinic attenders with hypertension and non-hypertensive controls in Al-Ain city, United Arab Emirates (UAE)
Variable Cases Controls Odds 95% CI P-value(n = 436) (n = 436) ratioNo. % No. %
SexFemale 195 44.7 217 50.2 1.00Male 241 55.3 219 49.8 0.903 0.79–1.03 0.154
Age (years)< 40 98 22.4 134 31.1 1.0040–49 173 39.7 172 39.9 0.73 0.51–1.03 0.06250–59 93 21.3 74 17.2 0.80 0.54–1.18 0.23960+ 72 16.5 51 11.8 0.89 0.54–1.47 0.628
NationalityUAE 209 48.0 207 47.7 1.00Other Arab 226 52.0 227 52.3 1.014 0.77–1.32 0.946
AreaUrban 402 93.3 375 86.4 1.00Semi-urban 29 6.7 59 13.6 1.30 0.87–1.87 0.242
Marital status (current)Married 372 86.7 359 83.9 1.00Single 57 13.3 69 16.1 1.25 0.84–1.87 0.242
No. of children< 3 101 23.3 123 29.1 1.003+ 304 70.2 265 62.8 0.72 0.52–0.99 0.034Not married 28 6.5 34 8.1 1.39 0.80–2.44 0.216
Educational levelIlliterate 145 33.7 126 29.2 1.00Elementary/preparatory 103 24.0 86 20.0 0.96 0.65–1.42 0.833Secondary 44 10.2 40 9.3 1.09 0.63–1.88 0.746College/university 138 32.1 179 41.5 1.43 0.86–2.38 0.148
Occupation typeNot working 50 11.6 45 10.3 1.00Unskilled/semi-skilledlabourer 62 14.3 46 10.6 0.82 0.46–1.49 0.495Administrative/professional 176 40.7 206 47.5 1.58 1.00–2.48 0.037Housewife 144 33.3 137 31.6 0.81 0.59–1.12 0.188
Type of residenceVilla 92 21.3 94 21.8 1.00Traditional mud-brick/prefabricated 245 56.9 244 56.3 0.97 0.69–1.39 0.882Apartment 94 21.8 95 21.9 1.01 0.72–1.44 0.931
18 Some risk factors.pmd 8/17/2005, 11:09 AM615

616 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Table 2 Comparison lifestyle habits of clinic attenders with hypertension and non-hypertensive controls in Al-Ain city, United Arab Emirates
Variable Cases Controls Odds 95% CI P-value(n = 436) (n = 436) ratioNo. % No. %
Tobacco smokingNever 292 68.4 344 79.8 1.00Current smoker 55 12.9 42 9.7 0.65 0.41–1.02 0.047Ex-smoker 80 18.7 45 10.4 0.74 0.41–1.31 0.270
Alcohol consumptionNever 402 94.1 413 97.2 1.00Current/ex-drinker 25 5.9 12 2.8 0.47 0.22–0.99 0.030
Physical activityYesa 188 43.1 229 52.5 1.00No 248 56.9 207 47.5 0.72 0.52–0.89 0.007
Vegetable consumption3+ times /week 366 87.4 359 85.4 1.00< 3 times /week 53 12.6 61 14.6 1.17 0.78–1.78 0.428
Fruit consumption3+ times /week 341 81.6 342 81.8 1.00< 3 times /week 77 18.4 76 18.2 0.98 0.68–1.42 0.928
n = total number of participants (data were missing in some categories).CI = confidence interval.aIf subject practised sport more than 1 hour per week.
Table 1 Socioeconomic characteristics of clinic attenders with hypertension andnon-hypertensive controls in Al-Ain city, United Arab Emirates (UAE) (concluded)
Variable Cases Controls Odds 95% CI P-value(n = 436) (n = 436) ratioNo. % No. %
Monthly income (dh)a
< 5000 138 34.1 98 25.1 1.005000–9999 140 34.6 176 45.1 1.77 1.24–2.53 < 0.00110 000–14 999 57 14.1 60 15.4 0.84 0.54–1.31 0.41315 000+ 80 17.3 56 14.4 0.66 0.39–1.13 0.108
BMI (kg/m2)Acceptable (< 25) 99 25.1 163 40.9 1.00Overweight (25–29.9) 132 33.5 150 37.6 0.69 0.48–0.99 0.035Obese (30+) 163 41.4 86 21.6 0.46 0.32–0.67 < 0.001
aUS$ 1 = 3.68 dirhams.n = total number of participants (data were missing in some categories).CI = confidence interval.BMI = body mass index.
18 Some risk factors.pmd 8/17/2005, 11:09 AM616

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 617
Table 4 Stepwise logistic regression analysis for hypertensionand associated socioeconomic and family historycharacteristics of clinic attenders with hypertension and non-hypertensive controls in Al-Ain city, United Arab Emirates
Independent variable Odds ratio 95% CI P-value
BMI(< 30 kg/m2 = 0, 30+ kg/m2 = 1) 4.29 2.76–6.66 0.0001
Incomea
(< 5000 dh = 0, 5000+ dh = 1) 2.69 1.76–4.10 0.001
Family history of diabetes(no = 0, yes = 1) 2.58 1.69–3.74 0.001
Physical activity(yes = 0, no = 1) 1.80 1.20–3.69 0.003
No. of children(< 3 = 0, 3+ = 1) 1.67 1.23–2.11 0.026
aUS$ 1 = 3.68 dirhams.CI = confidence interval.BMI = body mass index.
Table 3 Comparison of medical condition of clinic attenders with hypertension andnon-hypertensive controls in Al-Ain city, United Arab Emirates
Variable Cases Controls Odds 95% CI P-value(n = 436) (n = 436) ratio
No. % No. %
Cholesterol levelNormal 149 34.6 128 29.5 1.00Higher than normal 140 32.5 12 2.8 0.10 0.05–0.19 < 0.001Not measured 142 32.9 294 67.7 – –
Family history ofdiabetes
No 345 80.4 399 93.7 1.00Yes 84 19.6 27 6.3 0.28 0.17–0.45 < 0.001
Family history of heartdisease
No 352 82.1 415 98.1 1.00Yes 77 17.9 8 1.9 0.09 0.04–0.19 < 0.001
Family history of kidneyproblems
No 404 94.8 411 97.6 1.00Yes 22 5.2 10 2.4 0.45 0.19–1.00 0.033
n = total number of participants (data were missing in some categories).CI = confidence interval.
18 Some risk factors.pmd 8/17/2005, 11:09 AM617

618 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
health status as indicated by raised choles-terol levels and a family history of heart dis-ease, renal disease or diabetes.
The present study confirms the hypoth-esis of an association between hyperten-sion and poorer socioeconomic factors andmore sedentary lifestyle. We found a posi-tive association between hypertension andphysical inactivity, smoking and obesity.These finding are similar to those of Jo-hansson and colleagues in a study carriedout in Sweden [19]. This has implicationsfor preventive strategies, because smokingbehaviour, body fatness and physical activ-ity have been shown to be major candidatesfor possible early interventions [20].
Perhaps the common link to hyperten-sion for all these sociodemographic factorsis physical inactivity. If this were the case,it would suggest a number of potentiallymodifiable factors that could be targetedfor intervention. A study in Finland hasshown that the mean intensity of leisuretime physical activity had a positive dose–
response relationship with level of educa-tion and income [21]. It was also shownthat married or engaged men, those lesseducated, on lower incomes and unem-ployed or retired had a shorter duration ofconditioning physical activity especially inurban areas than others [21]. The authorsof the study concluded that physical activi-ty protects against poor health irrespectiveof high BMI and smoking.
Our finding that more expatriates thanUAE nationals had hypertension is in keep-ing with previous findings of a Swedishstudy [22], which found that foreign-bornindividuals had a higher risk for poor healththan Swedes after adjustment for sociode-mographic and lifestyle factors.
In conclusion, the present study sup-ports the importance of socioeconomicfactors, lifestyle habits and family historyin shaping risk for hypertension in UAE andindicates a need for more effective preven-tion programmes for control of hyperten-sion in this fast developing Arab country.
References
1. Bener A, Gomes J, Hamouda MFB. Hy-pertension among workers occupation-ally exposed to hydrocarbons andorganic solvents. Journal of environ-mental science and health, Part-A, 1996,31:291–303.
2. Annual report. Preventive medicine in 20years. Abu Dhabi, United Arab Emirates,Ministry of Health, 2000:1–270.
3. Bener A et al. Acanthosis nigricans,hyperinsulinaemia and risk factors forcardiovascular disease. Eastern Medi-terranean health journal, 2000, 6:416–24.
4. Corrao JM et al. Coronary heart diseaserisk factors in women. Cardiology, 1990,77(suppl. 2):8–24.
5. Rowland M, Roberts J. Blood pressurelevels and hypertension in personsaged 6–74 years: United States, 1976–1980. National Health and NutritionExamination Survey 1. Hyattsville, Mary-land, US Department of Health and Hu-man Services, 1982.
6. Sarraf-Zadegan N et al. Prevalence ofhypertension and associated risk factorsin Isfahan, Islamic Republic of Iran. East-ern Mediterranean health journal, 1999,5:992–1001.
7. Alwan A. Prevention and managementof hypertension. Alexandria, WorldHealth Organization, Regional Office forthe Eastern Mediterranean, 1996 (WHOEMRO Technical Publication, No. 23).
18 Some risk factors.pmd 8/17/2005, 11:09 AM618

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 619
8. Alwan A. Prevention and control of car-diovascular diseases. Alexandria, WorldHealth Organization, Regional Office forthe Eastern Mediterranean, 1995 (WHOEMRO Technical Publication, No. 22).
9. Sarraf-Zadegan N, Amini-Nik S. Bloodpressure pattern in urban and rural ar-eas in Isfahan, Iran. Journal of humanhypertension, 1997,11:425–8.
10. Sayeed MA et al. Prevalence of hyper-tension in Bangladesh: effect of socio-economic risk factor on differencebetween rural and urban community.Bangladesh Medical Research Councilbulletin, 2002, 28:7–18.
11. Faruqui A. Heart disease in South Asia:experiences in Pakistan. In: Hurst JW, ed.Clinical essays on the heart. Volume 2.New York, McGraw–Hill, 1983.
12. Laurenzi M et al. Multiple risk factors inhypertension: results from the Gubbiostudy. Journal of hypertension, supple-ment, 1990, 8:S7–12.
13. Bener A et al. Association betweenblood levels of lead blood pressure andrisk of diabetes and heart disease inworkers. International archives of occu-pational and environmental health,2001, 74(5):375–8.
14. World Health Organization/InternationalSociety of Hypertension. Guidelines forthe management of hypertension. Jour-nal of hypertension, 1999, 17:151–82.
15. Bray GA. Definition, measurement andclassification of the syndrome of obesity.International journal of obesity, 1978,2:99–112.
16. Kannel WB, Thom TJ. Declining cardio-vascular mortality. Circulation, 1984,70:331–6.
17. MacMahon S et al. Blood pressure,stroke and coronary heart disease. Part1, Prolonged differences in blood pres-sure: prospective observational studiescorrected for the regression dilution bias.Lancet, 1990, 335:765–74.
18. National Center for Health Statistics. An-nual summary of births, marriages, di-vorces and deaths, United States, 1989.Monthly vital statistics report,1990:38(13).
19. Johansson SE, Sundquist J. Change inlifestyle factors and their influence onhealth status and all-cause mortality. In-ternational journal of epidemiology,1999, 28(6):1073–80.
20. Twisk JW, Kemper HC, van Mechelen W.Tracking of activity and fitness and therelationship with cardiovascular diseaserisk factors. Medicine and science insports and exercise, 2000, 32(8):1455–61.
21. Lakka TA, Kauhanen J, Salonen JT. Con-ditioning leisure time physical activityand cardiorespiratory fitness in socio-demographic groups of middle-agesmen in eastern Finland. Internationaljournal of epidemiology, 1996, 25(1):86–93.
22. Sundquist J. Living conditions andhealth. A population-based study of la-bour migrants and Latin American refu-gees in Sweden and those who wererepatriated. Scandinavian journal of pri-mary health care, supplement, 1995,13(2):128–34.
18 Some risk factors.pmd 8/17/2005, 11:09 AM619

620 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Diabetic nephropathy as a cause ofend-stage renal disease in Egypt: asix-year studyA. Afifi,1 M. El Setouhy,2 M. El Sharkawy,1 M. Ali,1 H. Ahmed,1 O. El-Menshawy3 andW. Masoud4
1Department of Internal Medicine and Nephrology; 2Department of Public Health and OccupationalMedicine, Ain Shams University, Cairo, Egypt.3Department of Internal Medicine and Nephrology, Al Minya University, Egypt.4Department of Nephrology, Ahmed Maher Teaching Hospital, Cairo, Egypt.Received: 09/06/03; accepted: 26/10/03
ABSTRACT The prevalence of diabetic nephropathy as a cause of end-stage renal disease (ESRD) in Egypthas been examined in small cross-sectional studies, with conflicting results. The need for a large-scale studyprompted us to perform this 6-year multiple cross-sectional study. A sample of ESRD patients enrolled in theEgyptian renal data system was evaluated during the period 1996–2001 for the prevalence of diabeticnephropathy. Prevalence gradually increased from 8.9% in 1996, to 14.5% in 2001. The mean age of patientswith diabetic nephropathy was significantly higher than that of patients with ESRD from other causes.Mortality was also significantly higher in diabetic patients with ESRD.
La néphropathie diabétique comme cause de l’insuffisance rénale terminale en Égypte : étude sursix ansRÉSUMÉ La prévalence de la néphropathie diabétique comme cause de l’insuffisance rénale terminale enÉgypte a été examinée dans de petites études transversales, donnant des résultats contradictoires. Lebesoin d’une étude à grande échelle nous a incités à réaliser une étude transversale multiple sur six ans. Unéchantillon de patients souffrant d’insuffisance rénale terminale enregistrés dans le système égyptien dedonnées rénales a fait l’objet d’une évaluation pendant la période 1996-2001 pour la prévalence des né-phropathies diabétiques. La prévalence a augmenté progressivement, passant de 8,9 % en 1996 à 14,5 %en 2001. L’âge moyen des patients souffrant de néphropathie diabétique était significativement plus élevé quecelui des patients souffrant d’insuffisance rénale terminale due à d’autres causes. La mortalité était aussisignificativement plus élevée chez les diabétiques ayant une insuffisance rénale terminale.
19 Diabetic nephropathy.pmd 8/18/2005, 11:12 AM620

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 621
Introduction
Egypt, a developing country in North Afri-ca, had a population of approximately 68million in 2001. The estimated number ofdialysis patients in Egypt in that year was25 518 [1]
Diabetic nephropathy is rapidly becom-ing the leading cause of end-stage renaldisease (ESRD), particularly in the industri-alized countries of the world [2]. Ethnicand racial origin play an important role,resulting in increased prevalence rates ofdiabetic nephropathy in certain regions [3].
In many studies from Western Europ-ean countries as well as many other regionsof the world, diabetic nephropathy hasbeen reported as the main cause of ESRD.Variable incidence and prevalence rateshave been reported in Eastern Europe. Ta-ble 1 gives a summary of reported preva-lence of this condition in a number ofcountries. Data from 12 countries in theAsian Pacific region, including Australiaand New Zealand, showed an increase inboth incidence and prevalence between1998 and 2000 [4].
The prevalence of diabetic nephropathyas a cause of ESRD in Egypt has previouslybeen examined in 2 small cross-sectionalstudies with conflicting results [22,23].Other reports on prevalence of diabeticnephropathy also produced the followingwidely divergent figures: 8.4% [11], 13.7%[24], 20.1% [12] and 8.9% [25]. Thesemarked differences in the reported preva-lence rates may reflect the effect of urban-ization.
The need for a large-scale study hasprompted us to carry out this 6-year, multi-ple, cross-sectional study. The aim of ourstudy was to critically evaluate the preva-lence of diabetic nephropathy as a cause ofESRD in Egypt.
Methods
A sample of patients with ESRD enrolled inthe Egyptian renal data system was evaluat-ed during the period 1996–2001 for the
Table 1 Reported prevalence of diabeticnephropathy as a cause of renal diseasefor various parts of the world
Location End-stage renal diseasePrevalence of diabetic Reference
nephropathy (%) No.
United Statesof America ~ 50 5
WesternEurope Leading cause 6
Japan Leading cause 7
France Leading cause 8
Germany 21 9
Norway 10% of the incidentRRT population 10
Egypt 8.4 11
Egypt 20.1 12
Primary renal disease
Yugoslavia 7 13
Czech Republic 25.0 14
Slovakia 17.9 14
Poland 10.3 15
South America 16.0 16
Puerto Rico 51.2 16
Asian Pacific regionincluding Australiaand New Zealand 17.3 4
China 4.7 17
Taiwan 24.8 18
Saudi Arabia 27.9 19
Tunisia 11.4 20
Kuwait 21.2 21
RRT = renal replacement therapy.
19 Diabetic nephropathy.pmd 8/18/2005, 11:12 AM621

622 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
prevalence of diabetic nephropathy. Centreand patient questionnaires were sent to allidentified dialysis centres (370 centres). Allresponding centres and all patients reportedfrom these centres were included in thestudy. The number of patients evaluatedwas 4905 in 1996, 3013 in 1997, 1754 in1998, 1616 in 1999, 2150 in 2000 and 3172in 2001. Requested data included numberof patients, age, sex, renal biopsy results,cause of ESRD, and cause of death.
Criteria used for diagnosing diabeticnephropathy included:• long duration of diabetes before onset
of chronic renal failure (usually morethan 10 years)
• normal sized kidneys by ultrasound• presence of diabetic retinopathy by fun-
dus examination• absence of haematuria or red blood cell
casts in urine• proteinuria still present when the patient
has already started dialysis.The data collected were processed us-
ing an IBM-compatible PC and SPSS, ver-sion 6.1 for statistical analysis.
Results
The prevalence of diabetic nephropathyamong ESRD patients in Egypt increasedfrom 8.9% in 1996 to 14.5% in 2001 (Fig-ure 1).
The main causes of ESRD in Egypt oth-er than diabetic nephropathy includedhypertensive kidney disease, chronic glom-erulonephritis, undetermined etiology,reflux and chronic pyelonephritis, schisto-somal obstructive uropathy and schistoso-mal nephritis (Table 2).
The mean age of patients with diabeticnephropathy was higher than that of pa-tients having other causes of ESRD in theyears we studied (Table 3). Mortality
among diabetic patients with ESRD washigher than in patients with ESRD fromother causes (Figure 2).
Discussion
The prevalence of diabetes in adults world-wide was estimated to be 4.0% in 1995 andis predicted to rise to 5.4% by the year2025. It is higher in industrialized than indeveloping countries. The number of adultswith diabetes in the world is forecast to risefrom 135 million in 1995 to 300 million inthe year 2025. Most of this increase willoccur in developing countries [26].
A series of surveys of diabetes mellitushave been performed in Egypt using WorldHealth Organization criteria for diagnosisand classification. Average prevalence forpeople above the age of 10 years was4.3%, with distinct geographical differen-ces: 5.7% in urban areas, 4.1% in rural ag-ricultural areas, and 1.5% in rural desertareas. In some remote villages, diabeteswas almost completely absent [22]. A morerecent study in Egypt revealed that theprevalence of diabetes in rural areas was
Figure 1 Prevalence of diabetic nephropathyamong Egyptian patients with end-stagerenal disease, 1996–2001
19 Diabetic nephropathy.pmd 8/18/2005, 11:12 AM622

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 623
4.9%, increasing to 13.5% in lower socio-economic urban areas and 20% in highersocioeconomic urban areas [23].
Diabetic nephropathy is the commonestcause of ESRD in industrialized countries[26]. All countries with registries have re-ported a massive increase in the incidenceand prevalence in their dialysis population.
Table 3 Mean age of diabetic nephropathy patients andpatients with end-stage renal disease (ESRD) fromother causes
Year Diabetic Other causes P-valuenephropathy of ESRD
Mean age SD Mean age SD(years) (years)
1996 55.7 9.9 44.6 14.1 > 0.001
1997 54.9 11.4 44.9 16.8 > 0.001
1998 54.2 15.1 45.2 15.3 > 0.001
1999 56.6 11.6 45.4 15.3 > 0.001
2000 56.1 10.9 45.2 15.5 > 0.001
2001 56.5 29.2 46.1 16.1 > 0.001
SD = standard deviation.
Figure 2 Cause of mortality among diabetic and non-diabetic Egyptian patients with end-stagerenal disease
This increase is caused by an actual in-crease in prevalence of diabetes, increasingage of the dialysis population and bettersurvival rates for patients with diabetes,thus allowing more time for diabetic nephr-opathy to develop [2].
In Egypt, the estimated prevalence ofESRD increased from 225 per million pop-
19 Diabetic nephropathy.pmd 8/18/2005, 11:12 AM623

624 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Tabl
e 3
Mai
n c
ause
s o
f en
d-s
tag
e re
nal
dis
ease
in E
gyp
t oth
er th
an d
iab
etic
nep
hro
pat
hy
Year
Mai
n c
ause
s o
f en
d-s
tag
e re
nal
dis
ease
1996
Hyp
erte
nsio
n:C
hron
icU
ndet
erm
ined
Chr
onic
Obs
truc
tive
Dia
betic
Sch
isto
som
al28
.0%
glom
erul
onep
hriti
s:16
.2%
pyel
onep
hriti
s:ur
opat
hy:
neph
ropa
thy:
obst
ruct
ive
16.6
%14
.6%
9.3%
8.9%
urop
athy
: 6.0
%
1997
Hyp
erte
nsio
n:C
hron
icU
ndet
erm
ined
:C
hron
icD
iabe
ticS
chis
toso
mal
Obs
truc
tive
19.6
%gl
omer
ulon
ephr
itis:
12.5
%py
elon
ephr
itis:
neph
ropa
thy:
obst
ruct
ive
urop
athy
:13
.2%
10.4
%8.
5%ur
opat
hy: 7
.6%
7.5%
1998
Und
eter
min
ed:
Hyp
erte
nsio
n:C
hron
icO
bstr
uctiv
eD
iabe
ticS
chis
toso
mal
Chr
onic
22.1
%21
.0%
glom
erul
onep
hriti
s:ur
opat
hy:
neph
ropa
thy:
obst
ruct
ive
pyel
onep
hriti
s:11
.0%
9.5%
9.1%
urop
athy
: 6.7
%5.
5%
1999
Hyp
erte
nsio
n:U
ndet
erm
ined
:C
hron
icO
bstr
uctiv
eC
hron
icD
iabe
ticA
dult
23.6
%18
.4%
glom
erul
onep
hriti
s:ur
opat
hy:
pyel
onep
hriti
s:ne
phro
path
y:po
lycy
stic
:13
.9%
9.2%
7.8%
7.1%
4.3%
2000
Hyp
erte
nsio
n:U
ndet
erm
ined
:C
hron
icD
iabe
ticC
hron
icO
bstr
uctiv
eS
chis
toso
mal
23.5
%21
.8%
glom
erul
onep
hriti
s:ne
phro
path
y:py
elon
ephr
itis:
urop
athy
:ob
stru
ctiv
e12
.4%
10.5
%7.
4%6.
0%ur
opat
hy: 4
.0%
2001
Hyp
erte
nsio
n:D
iabe
ticC
hron
icU
ndet
erm
ined
:C
hron
icO
bstr
uctiv
eS
chis
toso
mal
22.1
%ne
phro
path
y:gl
omer
ulon
ephr
itis:
12.1
%py
elon
ephr
itis:
urop
athy
:ob
stru
ctiv
e14
.5%
12.4
%5.
6%5.
1%ur
opat
hy: 4
.4%
19 Diabetic nephropathy.pmd 8/18/2005, 11:12 AM624

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 625
ulation in 1996 [25] to 375 per million in2001 [1]. We found that the prevalence ofdiabetic nephropathy as a cause of ESRDincreased from 8.9% of patients in 1996 to14.5% in 2001. The mean age of diabeticnephropathy patients was higher than thatof patients with ESRD due to other causesfor the years studied.
Mortality among diabetic patients withESRD in Egypt is higher than mortality forall other causes of ESRD which is probablyrelated to the well known cardiovascularcomplications of diabetes (Figure 2).
Conclusions
Diabetic nephropathy is the commonestcause of ESRD in the industrialized coun-tries. In Egypt, there is a slower increase inthe prevalence of ESRD due to diabeticnephropathy, probably because of the high-er incidence of infections causing glo-merulonephritis, delayed referral to neph-rologists and increased mortality among di-abetic patients due to cardiovasculardisease and strokes before ESRD can de-velop.
References
1. Afifi A. Sixth annual report of the Egyp-tian Society of Nephrology. Paper pre-sented at the 22nd Congress of theEgyptian Society of Nephrology, 4–8February 2003, Sharm El Sheikh, Egypt.
2. Ritz E et al. End-stage renal failure intype 2 diabetes: A medical catastropheof worldwide dimensions. Americanjournal of kidney disease, 1999, 34(5):795–808.
3. Earle KK et al. Variation in the progres-sion of diabetic nephropathy accordingto racial origin. Nephrology, dialysis,transplantation, 2001, 16(2):286–290.
4. Lee G. End-stage renal disease in theAsian-Pacific region. Seminars in neph-rology, 2003, 23(1):107–14
5. US Renal Data System. USRDS 2002annual data report. Bethesda, Maryland,National Institutes of Health, National In-stitute of Diabetes and Digestive andKidney Diseases, 2002.
6. Jager K, Van Dijk P. 2002 ERA-EDTA reg-istry annual report, XXXIX ERA-EDTAcongress. Copenhagen, Denmark, Euro-pean Renal Association, 2002.
7. Hollenberg NK. Higher incidence of dia-betic nephropathy in type 2 than in type 1diabetes in early-onset diabetes in Ja-
pan. Current hypertension reports, 2001,3(3):177.
8. Halimi S et al. Huge progression of dia-betes prevalence and incidence amongdialysed patients in mainland Franceand overseas French territories. A sec-ond national survey six years apart.(UREMIDIAB 2 study). Diabetes and me-tabolism, 1999, 25(6):507–12.
9. Frei U, Schober-Halstenberg HJ. Annualreport of the German renal registry 1998.QuaSi-Niere task group for quality assur-ance in renal replacement therapy.Nephrology, dialysis, transplantation,1999, 14(5):1085–90.
10. Bergrem H, Leivestad T. Diabetic nephr-opathy and end-stage renal failure: theNorwegian story. Advances in renal re-placement therapy, 2001, 8(1):4–12.
11. El-Sharkawi M. Changing pattern of eti-ology of chronic renal failure amongdialysis patients [thesis]. Cairo, AinShams University, 1996.
12. Ahmed T. Clinical and laboratory fea-tures of patients with chronic renal failureat the start of dialysis [thesis]. Cairo, AinShams University, 1991.
13. Djukanovic L et al. Epidemiology of end-stage renal disease and current status of
19 Diabetic nephropathy.pmd 8/18/2005, 11:13 AM625

626 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
hemodialysis in Yugoslavia. Interna-tional journal of artificial organs, 2002,25(9):852–9.
14. Rutkowski B et al. Evolution of renal re-placement therapy in Central and East-ern Europe 7 years after political andeconomical liberation. Nephrology, di-alysis, transplantation, 1998, 13(4):860–4.
15. Rutkowski B et al. Renal replacementtherapy in an era of socioeconomicchanges–report from the Polish Registry.Nephrology, dialysis, transplantation,1997, 12(6):1105–8.
16. Mazzuchi N et al. Latin American registryof dialysis and renal transplantation:1993 Annual dialysis data report. Neph-rology, dialysis, transplantation, 1997,12(12):2521–7.
17. Li L. End-stage renal disease in China.Kidney international, 1996, 49(1):287–301.
18. Yang WC et al. The impact of diabetes oneconomic costs in dialysis patients: ex-periences in Taiwan. Diabetes researchand clinical practice, 2001, 54(suppl.1):S47–54.
19. Al-Khader AA. Impact of diabetes in re-nal diseases in Saudi Arabia. Nephrol-ogy, dialysis, transplantation, 2001,16(11):2132–5.
20. Ben Abdallah. Report of dialysis registryin Tunisia. Paper presented at the 21stCongress of the Egyptian Society ofNephrology, 15–20 February 2002,Cairo, Egypt.
21. El-Reshaid K et al. End-stage renal dis-ease and renal replacement therapy inKuwait–epidemiological profile over thepast 4½ years. Nephrology, dialysis,transplantation, 1994, 9(5):532–8.
22. Arab M. Diabetes mellitus in Egypt. Worldhealth statistics quarterly, 1992, 45(4):334–7.
23. Harman WH et al. Diabetes mellitus inEgypt: risk factors and prevalence. Dia-betic medicine, 1995, 12(12):1126–31.
24. Ibrahim T. Etiology of chronic renalfailure among a sample of Egyptianpopulation [thesis]. Cairo, Ain ShamsUniversity, 1998.
25. Afifi A, Karim MA. Renal replacementtherapy in Egypt: first annual report of theEgyptian Society of Nephrology, 1996.Eastern Mediterranean health journal,1999, 5(5):1023–9.
26. King H, Aubert RE, Herman WH. Globalburden of diabetes, 1995–2025: preva-lence, numerical estimates, and pro-jections. Diabetes care, 1998, 21(9):1414–31.
19 Diabetic nephropathy.pmd 8/18/2005, 11:13 AM626

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 627
Antiphospholipid syndrome andretinal vein occlusion in adultsR.M. Maaroufi,1,3 R. Hamdi,2 N. Jmili,3 M. Ghorbal,2 F. Bel Hadj Hamida 2 and T. Mahjoub3
1Higher Institute of Biotechnology, Monastir, Tunisia.2Department of Ophthalmology, Farhat Hached University Hospital, Sousse, Tunisia.3Haematology and Autoimmune Diseases Unit, Faculty of Pharmacy, University of Monastir, Tunisia.Received: 29/04/03; accepted: 23/12/03
ABSTRACT Antiphospholipid antibodies may play an important role in the pathogenesis of retinal vascularocclusions; therefore, we investigated the prevalence among 33 patients with retinal vein and artery occlu-sions and 80 controls. Prevalence was 33% and 5% respectively. Ophthalmic examination and fluoresceinangiography showed that occlusions were due to ischaemic events. The 11 patients were diagnosed withantiphospholipid syndrome: 9 patients were treated successfully with laser photocoagulation and anticoag-ulant and anti-aggregant therapy. Two patients with antiphospholipid antibodies associated with resistance toactivated protein C had unfavourable outcomes. Our results suggest a correlation between antiphospholipidsyndrome and retinal vein occlusions; we recommend a systematic search for antiphospholipid antibodies inocclusions of unexplained origin and laser photocoagulation treatment and long-term oral anticoagulant andanti-aggregant therapy.
Le syndrome des antiphospholipides et l’occlusion veineuse rétinienne chez l’adulteRÉSUMÉ Les antiphospholipides peuvent jouer un rôle important dans la pathogenèse des occlusionsvasculaires rétiniennes ; nous avons donc étudié la prévalence chez 33 patients atteints d’occlusionsveineuses et artérielles rétiniennes et 80 témoins. La prévalence s’élevait à 33 % et 5 % respectivement.L’examen ophtalmologique et l’angiographie fluorescéinique ont montré que les occlusions étaient dues à desévénements ischémiques. Le syndrome des antiphospholipides a été diagnostiqué chez 11 patients : neufpatients ont été traités avec succès par photocoagulation au laser associant un traitement anticoagulant etantiagrégant. Deux patients présentant des anticorps antiphospholipides associés à une résistance à laprotéine C activée ont eu une issue défavorable. Nos résultats semblent indiquer une corrélation entre lesyndrome des antiphospholipides et les occlusions veineuses rétiniennes ; nous recommandons une re-cherche systématique des anticorps antiphospholipides dans les occlusions d’origine inexpliquée et untraitement par photocoagulation au laser et un traitement anticoagulant et antiagrégant de longue durée.
20 Antiphospholipid syndrome.pmd 8/17/2005, 11:09 AM627

628 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Introduction
Antiphospholipid antibodies are a heteroge-neous family of antibodies directed to plas-ma protein co-factors bound to anionicphospholipids. The clinical relevance of an-tiphospholipid antibodies derives from theassociation with venous and arterial throm-bosis, recurrent abortions and thrombocy-topenia [1]. Antiphospholipid antibodiesinclude lupus anticoagulant and anticardio-lipin antibodies [2,3]. This association hasbeen termed the antiphospholipid syndrome(APS), which may occur alone (primaryAPS) or in the setting of an underlying dis-ease, mainly systemic lupus erythematosus(SLE) [4–7].
Hypercoagulable states, including a va-riety of disorders such as reduced levels ofantithrombin, protein C, protein S or pres-ence of antiphospholipid antibodies, arecommon in patients with retinal vein occlu-sions and may contribute to the etiology ofthe disease [8].
In particular, retinal vascular occlusionsin patients with primary APS, i.e. with an-tiphospholipid antibodies but with no otherconventional risk factors, result fromthrombus formation in either the retinalvein, artery or both [9–12].
We investigated the prevalence of an-tiphospholipid antibodies in a group of 33patients with retinal vein occlusion and in80 normal controls. Whether antiphospho-lipid antibodies included lupus anticoagu-lant, anticardiolipin antibodies or both wasalso investigated. This study aimed toassess the relationship between the occur-rence of antiphospholipid antibodies in pri-mary APS and occlusive retinal vascularevents.
Methods
From January–December 2002, 33 patients(14 men and 19 women, mean age 37 years
and age range 22–63 years) with retinalvein (29) or artery (4) occlusions were se-lected from the Department of Ophthalmol-ogy of the Farhat Hached Hospital, Sousse,Tunisia. Exclusion criteria were diabetes,hypertension, hypercholesterolaemia andhypertriglyceridaemia. We used 80 normalcontrols from among healthy blood donorsat the Centre Régional de Transfusion San-guine of Farhat Hached Hospital. Informedconsent was obtained from patients andcontrols prior to their participation in ourstudy.
Patients were examined clinically. Aquestionnaire was administered before pa-tients underwent ophthalmologic examina-tion and retinal flourescein angiography.
Biological assays for cholesterol andtriglycerides were performed. Antinuclearantibodies were investigated with standard-ized enzyme-linked immunosorbent assay(ELISA).
Screening studies for APS included as-says for anticardiolipin antibodies and lupusanticoagulant. Anticardiolipin antibodies(IgG and IgM isotypes) were also deter-mined by ELISA assay (Diagnostica Stago,Asnières, France). Lupus anticoagulantwas assayed with clotting techniques. Anti-cardiolipin antibodies and lupus anticoagu-lant were measured 8 weeks later.
We also screened for abnormalities inthe coagulation process. Activated partialthromboplastin time and kaolin clottingtime tests were performed. The levels ofprotein C and protein S were determined byELISA assay (Diagnostica Stago, Asnières,France). Antithrombin III level was evalu-ated by colorimetric assay (Asserachrom,Diagnostica Stago, Asnières, France) andlevels of factors VIIIc and XI were deter-mined with clotting assays (DiagnosticaStago, Asnières, France). Factor V Leidenwas investigated through the evaluation ofthe activated protein C–sensitivity ratio
20 Antiphospholipid syndrome.pmd 8/17/2005, 11:09 AM628

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 629
(Accelerimat, bioMérieux, Marcy l’Etoile,France). Genetic analysis of factor VLeiden mutation was performed as previ-ously described [13].
Chi-squared test was used to comparethe patient and control groups.
Results
All patients underwent fundus fluoresceinangiography and ophthalmologic examina-tion. Almost all suffered from retinal veinocclusions (29 of 33 patients); the occlu-sive events primarily involved the central (9patients) and the temporal (8 patients)veins. Only 4 patients had artery occlusions(Table 1). The prevalence of antiphospho-lipid antibodies in the study group was 33%(11 of 33 patients) while in the controlgroup it was 5% (4 of 80). This differencewas statistically significant (χ2 = 16.29, P< 0.001) .
All patients with antiphospholipid anti-bodies had retinal vein occlusions, particu-larly temporal vein occlusions (5 of 11patients). Only 1 patient with antiphospho-lipid antibodies had a central vein occlu-sion. None of the patients with arteryocclusions tested positive for any of theassays.
In the study group 2 patients were pos-itive for IgG-anticardiolipin antibodies, 3patients for IgM-anticardiolipin antibodiesand 1 patient for both isotypes IgG andIgM-anticardiolipin antibodies. The 5 re-maining patients were negative for anticar-diolipin antibodies but showed positivity forlupus anticoagulant (Table 1). Two patientshad associated protein C resistance. All pa-tients were negative for antinuclear anti-bodies. No deficiency in antithrombin III,protein C or protein S was found. FactorsVIII and XI levels were within normal.
Discussion
The etiology of retinal vein occlusion is stillnot well understood although thrombosisdoes occur histologically. Hypercoagulablestates seem to be common in patients withretinal vein occlusions [8]. The presence ofantiphospholipid antibodies in APS is likelyto generate a hypercoagulable state such asto cause thrombosis to occur [1]. It isknown that antiphospholipid antibodies im-pair the metabolism of arachidonic acid inendothelial cells and platelets causing theinhibition of prostaglandin I2 (PGI2) pro-duction by endothelial cells and activationof platelets through stimulating thrombox-ane A2 generation [14,15]. Furthermore,antiphospholipid antibodies inhibit protein Cand protein S, preventing coagulation fac-tors Va and VIIa from inactivation [16,17].Among other implications of the antiphos-pholipid antibodies syndrome is an increasein tissular factor release and in plasminogenactivator inhibitor level. These implicationscould make it possible for thrombosis tooccur even in veins or arteries, although
Table 1 Presence of anticardiolipinantibodies, lupus anticoagulant and factor VLeiden among the 11 retinal vein occlusionpatients testing positive forantiphospholipid antibodies
Measurand No.
Anticardiolipin antibodies 6a
IgG 2IgM 3IgG and IgM 1
Lupus anticoagulant 5
Associated factor V Leiden 2
Antinuclear antibodies 0
20 Antiphospholipid syndrome.pmd 8/17/2005, 11:09 AM629

630 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
most vascular occlusions (81%) werefound to affect venous vessels in a recentstudy [11].
Elevated levels of anticardiolipin anti-bodies have recently been associated withacute vascular occlusions of the eye al-though their role remains unclear [12,18–21]. Of 33 patients with retinal vascularocclusions, 11 (33%) were diagnosed withAPS. They possibly had primary APSwithout any underlying immune disorderlike lupus erythematosus because each wasnegative for antinuclear antibodies. None ofour patients, however, was investigated forother possible immune disorders. It is note-worthy that 9 of the 11 patients had no oth-er conventional risk for thrombosis,whereas the presence of antiphospholipidantibodies was associated with resistanceto activated protein C for the 2 others.
The high prevalence of antiphospholipidantibodies in our study indicates that an-tiphospholipid antibodies may play an im-portant role in the pathogenesis of retinalvein occlusions and thus may represent arisk factor of importance in the etiology ofthe disease. This may also suggest the ne-cessity of screening for antiphospholipidantibodies in such patients. Furthermore, inour study group, the prevalence of an-tiphospholipid antibodies seemed to be re-lated to retinal vein occlusions mainlyinvolving the temporal vein and not to ar-tery vein occlusions. This warrants furtherinvestigation. It should be noted that therole of antiphospholipid antibodies in retinalvein occlusion is still controversial. Our re-sults provide more support for such a roleof antiphospholipid antibodies in the patho-genesis of this disease.
Our results (33% prevalence of an-tiphospholipid antibodies in patients withretinal vascular occlusions) were dissimilarfrom studies that identified lower preva-
lences of 5%, 7.5% and 9% respectivelyamong patients with primary APS[18,9,12]; however, in the two latter stud-ies, these levels could have been 22.5% and22% if antiphospholipid antibodies were as-sociated with lupus erythematosus, the ele-vation of circulating immune complexes orcomplement deficiencies respectively[9,12]. Our results nevertheless indicatehigher prevalence of antiphospholipid anti-bodies in retinal vein occlusions than theresults of these authors. It should be notedthat our study is the first of its kind in Tuni-sia and that a cohort study among the Tuni-sian population is needed.
In our study, all patients with antiphos-pholipid antibodies except 2 were treatedsuccessfully with laser photocoagulationand anticoagulant and anti-aggregant thera-py (acenocoumarol, to get the patient’s in-ternational normalized ratio to 2–4, andlysine acetylsalicylate, 250 mg per day)[22]. The 2 exceptions had associated re-sistance to activated protein C with thepresence of antiphospholipid antibodies andexperienced unfavourable developments.One had an occlusive event in the secondeye and the other became blind even thoughtherapy was provided.
In retinal vascular occlusions of unex-plained origin, antiphospholipid antibodiesmay play an important role in pathogenesis.Detecting these antibodies in the serum ofpatients with retinal vascular occlusionsmay help to determine the appropriate treat-ment. The high prevalence of anticardio-lipin antibodies in these patients who arefree of conventional risk factors leads us torecommend a systematic search for specif-ic antiphospholipid antibodies for them.This should be part of a treatment combin-ing laser photocoagulation, and long-termanti-aggregant and oral anticoagulant thera-py [19].
20 Antiphospholipid syndrome.pmd 8/17/2005, 11:09 AM630

Eastern Mediterranean Health Journal, Vol. 10, Nos. 4/5, 2004 631
References
1. De Groot PG, Oosting JD, Derksen RH.Antiphospholipid antibodies: specificityand pathophysiology. Balliere’s clinicalhaematology, 1993, 6:691–709.
2. Exner T, Triplett DA. Lupus anticoagu-lants: characteristics, methods of la-boratory detection and some clinicalassociations. In: Harris EN et al., eds.Phospholipid binding antibodies. BocaRaton, Florida, CRC Press, 1991:141–58.
3. Loizou S et al. Measurement ofanticardiolipin antibodies by an en-zyme-linked immunosorbent assay(ELISA): standardization and quanti-tation of results. Clinical and experimen-tal immunology, 1985, 62:738–45.
4. Harris EN et al. Clinical and serologicalfeatures of the antiphospholipid syn-drome (APS). British journal of rheuma-tology, 1987, 26:19.
5. Alarcon-Segovia D, Sanchez-GuerreroJ. Primary antiphospholipid syndrome.Journal of rheumatology, 1989, 16:482–8.
6. Italian registry of antiphospholipid anti-bodies (IR–APA). Thrombosis and throm-bocytopenia in antiphospholipid syn-drome (idiopathic and secondary toSLE): first report from the Italian registry.Haematologica, 1993, 78:313–8.
7. Khamashta MA. Management of throm-bosis in the antiphospholipid syndrome.Lupus, 1996, 5(5):463–6.
8. Abu El-Asrar AM et al. Hypercoagulablestates in patients with retinal vein occlu-sion. Documenta ophthalmologica,1998, 95(2):133–43.
9. Cobo-Soriano R et al. Antiphospholipidantibodies and retinal thrombosis in pa-tients without risk factors: a prospectivecase–control study. American journal ofophthalmology, 1999, 128(6):725–32.
10. Coniglio M et al. Antiphospholipid anti-bodies are not an uncommon feature inretinal venous occlusions. Thrombosisresearch, 1996, 83(2):183–8.
11. Demirci FY et al. Ocular involvement inprimary antiphospholipid syndrome.Ocular involvement in primary APS.International ophthalmology, 1998,22(6):323–9.
12. Cobo Soriano R et al. Trombosisretiniana en pacientes jóvenes. Aspec-tos inmunológicos y clínicos. [Retinalthrombosis in young patients. Immuno-logical and clinical aspects.] Archivos dela Sociedad Española de Oftalmología,2001, 76(11):641.
13. Ridker PM et al. Mutation in the genecoding for coagulation factor V and therisk of myocardial infarction, stroke andvenous thrombosis in apparentlyhealthy men. New England journal ofmedicine, 1995, 332:912–7.
14. Lellouche F et al. Influence of thrombox-ane/prostacyclin biosynthesis in pa-tients with lupus anticoagulant. Blood,1991, 78:2894–9.
15. Karmochkine M et al. The effect of serawith antiphospholipid antibodies on en-dothelial cell procoagulant activity is de-pendent upon the charge of thephospholipids against which they are di-rected. Thrombosis research, 1994,74:435–40.
16. Cariou R et al. Effect of lupus anticoagu-lant on antithrombogenic properties ofendothelial cells. Inhibition of thrombo-modulin-dependent protein C activation.Thrombosis and haemostasis, 1988,60:54–8.
17. Smirnov MD et al. On the role of phos-phatidylethanolamine in the inhibition ofprotein C activity by antiphospholipidantibodies. Journal of clinical investiga-tion, 1995, 95:309–18.
20 Antiphospholipid syndrome.pmd 8/17/2005, 11:09 AM631

632 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
18. Glacet–Bernard A et al. Antiphospho-lipid antibodies in retinal vascular occlu-sions. A prospective study of 75 patients.Archives of ophthalmology, 1994,112(6):790–5.
19. Wiechens B et al. Primary antiphos-pholipid antibody syndrome and retinalocclusive vasculopathy. Americanjournal of ophthalmology, 1997, 123(6):848–50.
20. Ermakova NA et al. Rol’ antifosfo-lipidnykh antitel v okkliuzii sosudovsetchatki pri razlichnykh sosudistykh
zabolevaniiakh glaza. [Role of anti-phospholipid antibodies in occlusion ofretinal vessels in various vascular eyediseases.] Vestnik oftalmologii, 2002,118(2):29–32.
21. Carbone J et al. Antiphospholipid anti-bodies: a risk factor for occlusive retinalvascular disorders. Comparison withocular inflammatory diseases. Journal ofrheumatology, 2001, 28(11):2437–41.
22. Dunn JP et al. Antiphospholipid antibod-ies and retinal vascular disease. Lupus,1996, 5(4):313–22.
CorrectionScreening for congenital hypothyroidism in the Islamic Republic of Iran: strategies, obstacles andfuture perspectives A. Ordookhani, P. Mirmiran, R. Hajipour, M. Hedayati and F. Azizi. EasternMediterranean Health Journal, 2002, Vol. 8 Nos 4/5, pages 480–9.The title of the French abstract should read:Dépistage de l’hypothyroïdie congénitale en République islamique d’Iran : stratégies, obstacles etperspectives futures and hypothyroïdie should replace hyperthyroïdie throughout the text of the abstract.
20 Antiphospholipid syndrome.pmd 8/17/2005, 11:09 AM632

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 633
Hyperhomocysteinaemia: risk ofretinal vascular occlusionG.H. Yaghoubi,1 F. Madarshahian 2 and M. Mosavi 3
1Department of Ophthalmology, Valiaser Hospital; 2Nursing College, Birjand Medical University, Birjand,Islamic Republic of Iran.3Department of Ophthalmology, Mashhad University of Medical Science, Mashhad, Islamic Republic ofIran.Received: 09/05/03; accepted: 20/10/03
ABSTRACT To investigate the possible relationship between hyperhomocysteinaemia and retinal vascularocclusion, we measured plasma homocysteine levels in 25 patients with a history of retinal vascular occlu-sion in the previous 2 years and in a control group of 24. The difference in mean plasma homocysteine levelswas not statistically significant. All except 5 of the cases had hypertension, diabetes mellitus or hyperlipi-daemia. Most of the patients had branch retinal vein occlusion associated with recent onset of occlusion.Factors such as emotional status and associated systemic disease may play a role in predisposition ofretinal vascular occlusion, so more-precise studies are needed to determine the possible risk factors ofhyperhomocysteinaemia in retinal vascular occlusion.
Hyperhomocystéinémie : risque d’occlusion vasculaire rétinienneRÉSUMÉ Afin d’examiner le lien possible entre l’hyperhomocystéinémie et l’occlusion vasculaire rétinienne,nous avons mesuré les taux d’homocystéine plasmatique chez 25 patients ayant fait une occlusion vascu-laire rétinienne dans les deux années précédentes et dans un groupe témoin de 24 sujets. La différence destaux moyens d’homocystéine plasmatique n’était pas statistiquement significative. Tous les cas sauf cinqavaient une hypertension, un diabète sucré ou une hyperlipidémie. La plupart des patients avaient uneocclusion de branche veineuse rétinienne associée à la survenue récente de l’occlusion. Des facteurs telsque l’état émotionnel et une maladie systémique associée peuvent jouer un rôle dans la prédisposition àl’occlusion vasculaire rétinienne. Des études plus précises sont donc nécessaires pour déterminer lesfacteurs de risque possibles de l’hyperhomocystéinémie dans l’occlusion vasculaire rétinienne.
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM633

634 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Introduction
Thrombophilia is an increased tendency tothrombosis which is sustained by an ongo-ing stimulus to thrombogenesis or by adefect in the normal anticoagulant or fibrin-olytic mechanism. Genetic factors are im-portant in thrombophilia since thrombosiscan be familial and may be associated withcongenital deficiencies of the protein C an-ticoagulant pathway, antithrombin III, hep-arin cofactor II or plasminogen. Althoughthe relationship between hyperhomocys-teinaemia and vascular occlusion is still un-certain, it is of increasing interest that lesssevere abnormalities of methionine metabo-lism may predispose to the development ofpremature vascular disease. Endothelialdysfunction is also a factor in the complexchanges that occur in vessel walls in hyper-homocysteinaemia [1,2]. Retinal vein oc-clusion is a major cause of retinal vasculardisease, second only to diabetic retinopathy[3]. Branch retinal vein occlusion (BRVO)and central retinal vein occlusion (CRVO)are the 2 major categories, both having asimilar potential for loss of vision owing tocomplications causing macular oedema andneovascularization [4].
Considering the various uncertaintiesregarding the many possible risk factorsfor retinal vascular occlusion, this studywas carried out to measure plasma ho-mocysteine levels in patients diagnosedwith retinal vascular occlusion and to com-pare the results with those of a controlgroup to determine whether elevated ho-mocysteine level is a risk factor in retinalvascular occlusion.
Methods
We carried out a retrospective study of 25out of 31 patients with retinal vein occlu-sion who consecutively attended the eye
clinic of Valiasr Hospital, a teaching hospi-tal of Birjand Medical University, from May2002 to December 2002. Diagnosis of reti-nal vascular occlusion was based on clini-cal findings of ophthalmoscopic exami-nation (well-demarcated haemorrhage andoedema along obstructed retinal vein). Inuncertain cases fluorescein angiographywas also done. A matched control group of24 individuals was selected from people at-tending the clinic but who had no signs ofretinal vascular occlusion, glaucoma, uvei-tis or intraocular surgery/trauma.
All participants completed a checklistconsisting of questions covering demo-graphic data, current disease, disease histo-ry, eye trauma and consumption of drugs.Then the fasting plasma homocysteine lev-els of the patients who had agreed to partic-ipate and had given informed consent wasmeasured. Patients were classified into 3major categories of retinal vascular occlu-sion based on their first episode: CRVO,BRVO (macular or main branch) or centralretinal artery occlusion. The cases andcontrols were matched for age and sex.
Fasting blood samples were collected inheparinized tubes from all participants. Af-ter immediate centrifugation, the resultantplasma samples were packed in an iceboxand sent to the Pars Laboratory, Tehran tomeasure plasma homocysteine levels.
Analysis of data was done with respectto presence/absence of a systemic condi-tion, sex, age group and mean plasma ho-mocysteine as independent variables andretinal vein occlusion as the dependent vari-able.
Results
Of the 25 patients with retinal vascular oc-clusion, 14 had BRVO and 10 had CRVO.Central retinal artery occlusion was diag-nosed in a single case.
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM634

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 635
The onset of occlusion in 6 patients oc-curred within the previous 6 months (1–6months); in the rest, occlusion had oc-curred more than 6 months previously (7–30 months).
The characteristics of all participants,both cases and controls, are shown in Ta-bles 1 and 2. A more detailed comparison ofrelated disease in both cases and controls isshown in Table 3. The mean total plasma ho-mocysteine level was 15.0 (SD, 5.7) µmol/Lfor patients with retinal vascular occlusion and13.4 (SD 4.1) µmol/L for the control group(Table 4). The mean level was 13.8 µmol/Lin patients with BRVO and 16.5 µmol/L inpatients with CRVO. Of the 25 patients, 20had at least 1 associated disease (diabetesmellitus, hypertension, hyperlipidaemia,asthma) for which they were under treat-ment by their primary care doctor and weretaking medication. In the control group,these conditions were present in only 4 ofthe 24. The independent t-test showed nosignificant difference between plasma ho-mocysteine levels for cases and controls (P= 0.24).
The Mann–Whitney test showed no sig-nificant difference between homocysteinelevels in patients with BRVO and those withCRVO (P = 0.33). The Fisher test showedthat there was also no significant differencein homocysteine level between hyperten-sive patients with BRVO and those withCRVO (P = 0.67).
Visual acuity in all BRVO cases was 1.1or better in comparison to hand motion per-ception, and 0.1 in CRVO patients.
Discussion
In this study, we found no significant clini-cal association between hyperhomocys-teinaemia and retinal vascular occlusion,although mean plasma homocysteine levelswere higher in patients than in the control
group. Most of these patients had at least 1associated systemic disease.
The sample size in our study was smalland both the patients and those in the con-trol group were hospital-based subjects.This was a single blind study, in which theresults may have been affected by the typeof retinal vascular occlusion (most of thecases had BRVO). Our findings are similarto those of Larsson et al., who also report-ed that hyperhomocysteinaemia was not animportant factor in the etiology of CRVO[5].
There may be different pathogenesesfor the different kinds of retinal vascularocclusion. If there is an association withthe location of the vascular obstruction,this finding may be related to increasingplasma homocysteine levels, or more prob-ably to homodynamic change or local vas-cular insult. This was discussed by Cahill etal., who considered CRVO to be associatedwith similar risk factors to retinal arterialocclusive disease. Local factors such asatherosclerotic retinal arteries compressingthe retinal vein at arteriovenous crossingsmay be more important in the etiology ofBRVO [6].
Hyreh et al. recommended that, apartfrom routine medical evaluation, an exten-sive and expensive workup for systemicdisease is unwarranted in the vast majorityof patients with retinal vein occlusion [7].This raises 2 points. First, is vascular oc-clusion pathophysiologically different indifferent organs? If so, we can considerthat the attributing factors must be pro-duced in greater amounts or elevated inlarger vessels of the affected organ. Sec-ond, how much time has passed betweenthe occurrence of vascular occlusion andthe measurement of the plasma homocys-teine level, because homocysteine levels areaffected by many factors (diet, emotionalstate, etc.).
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM635

636 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Table 1 Characteristics of patients with retinal vascular occlusion
Patient Age Sex Eye Type of Associated Addiction Plasma(years) occlusion disease homocysteine
(µµµµµmol/L)
1 42 Female L BRVO HY None 6.6
2 76 Male R CRVO HY None 25.0
3 68 Male R CRVO HY None 11.9
4 60 Male L CRVO HY None 16.8
5 71 Female L BRVOMB None None 17.9
6 48 Female R CRAO None None 17.4
7 60 Female R BRVO HY, DI None 25.0
8 66 Female L BRVO HY None 18.0
9 56 Female L BRVO HY None 12.4
10 68 Female R CRVO DI None 12.5
11 45 Male L BRVO None None 14.2
12 48 Male L CRVO DI, HCH None 13.0
13 40 Male L BRVOMB HY, HCH None 12.7
14 38 Female R BRVO HY, DI None 14.6
15 56 Female R BRVO HCH None 11.0
16 60 Female R BRVO HY None 15.5
17 60 Female L BRVO HY None 11.5
18 63 Female R BRVO HY, HCH None 12.6
19 63 Male L CRVO AS None 18.0
20 61 Female R BRVO HCH None 10.3
21 65 Female L CRVO None None 9.2
22 70 Male R BRVO HY None 10.5
23 70 Male R CRVO HCH None 27.0
24 80 Male L CRVO None None 10.5
25 80 Male L CRVO HY None 21.0
CRVO = central retinal vein occlusion.BRVO = branch retinal vein occlusion.CRAO = central retinal artery occlusion.MB = macular branch.HY = hypertension.HCH = hypercholesterolaemia.DI = diabetes.AS = asthma.
Although our study did not find a signif-icant difference in hyperhomocysteinaemialevels between the case and the control
groups, Lahey et al. have reported that hy-percoagulability plays a role in thrombusformation in patients with CRVO who are
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM636

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 637
under 56 years old [8]. They concludedthat hypercoagulability may play a part inthe pathogenesis of CRVO, but the causeremains multifactorial, and laboratory testsalone cannot determine the cause in mostpatients. They recommended examiningblood pressure, intraocular pressure, com-plete blood count, glucose level and a lipid
Table2 Characteristics of participants in the control group
Participant Age Sex Associated Addiction Plasma(years) disease homocysteine
(µµµµµmol/L)
1 79 Male None None 7.0
2 77 Female None None 16.9
3 75 Female None None 11.7
4 25 Female None None 7.1
5 53 Female HY None 13.0
6 61 Female DI None 15.4
7 52 Male None None 21.0
8 57 Male HY None 19.4
9 47 Male None None 9.0
10 65 Female None Smoking 10.2
11 67 Female None None 11.8
12 47 Male None None 17.6
13 47 Female None None 7.3
14 47 Male None None 14.0
15 50 Female None None 11.8
16 51 Female HY None 13.8
17 60 Male None None 17.3
18 65 Female None None 9.9
19 70 Male None None 11.5
20 70 Male None None 12.5
21 74 Male None None 11.5
22 76 Male None None 22.0
23 80 Female None None 16.2
24 85 Male None None 13.8
HY = hypertension.DI = diabetes.
panel in all patients with CRVO. When testsfor these common risk factors for CRVOare negative, they would consider orderingselected tests in young patients with CRVOto rule out thrombophilia. Furthermore, in 2other studies the authors describe scleroticthickening of the central retinal artery thatcould easily compress the adjacent central
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM637

638 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Table 3 Characteristic of cases with retinal vascularocclusion and participants in the control group
Variable Cases (n = 25) Controls (n = 24)% Mean % Mean
homocysteine homocysteine(µµµµµmol/L) (µµµµµmol/L)
Male sex 44.0 – 50.0 –
Hypertension 56.0 15.3 12.5 15.4
Hyperlipidaemia 24.0 14.4 0.0 –
Diabetes mellitus 16.0 16.2 4.2 15.4
Without disease 16.0 13.8 83.3 12.4
Mean age of cases and controls was 60.5 and 61.7 yearsrespectively (P = 0.77).Mean homocysteine level in cases and controls was 15.0 and13.4 µmol/L respectively (P = 0.24).
retinal vein and begin the sequence thatleads to thrombus formation. Therefore,hyperhomocysteinaemia may represent a“double hit” in the multifactorial pathogene-sis of CRVO [9,10].
Although many reports suggest hyper-homocysteinaemia is a risk factor for vas-cular occlusion, our study shows that itplays a less important role than systemicrisk factors for retinal vascular occlusion.
Systemic hypertension was more commonin cases than in control subjects. Also,most of the cases had at least 1 systemicdisease (e.g. hypertension, diabetes, hyper-lipidaemia). Therefore, hyperhomocystein-aemia may represent a coincidentalassociation in the pathogenesis of retinalvascular occlusion. These paradoxical re-sults not only demand repeating cohortstudies with a larger sample size, they also
Table 4 Distribution of cases according to type of retinalvascular occlusion
Type of No. Diabetes Hyper- Hyper- Meanocclusion mellitus tension lipidaemia homocysteine
No. No. No. (µµµµµmol/L)
CRAO 1 0 0 0 17.4
CRVO 10 2 4 2 16.5
BRVO 14 2 10 4 13.8
Total 25 4 14 6 15.5
CRAO = central retinal artery occlusion.CRVO = central retinal vein occlusion.BRVO = branch retinal vein occlusion.
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM638

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 639
highlight the need to assess the preventiveeffects of lowering homocysteine levels onthe recurrence of retinal vascular occlusionin cases compared to future attacks in con-trol subjects.
Acknowledgement
We wish to thank our colleague Hydari Be-hroze for his valuable assistance.
References
1. Fermo I et al. Prevalence of moderatehyperhomocysteinaemia in a patientswith early-onset venous and arterial oc-clusive disease. Annals of internal medi-cine, 1995, 123(10):747–53.
2. Faraci FM. Hyperhomocysteinemia: amillion ways to lose control. Arterioscle-rosis, thrombosis, and vascular biology,2003, 23(3):371–3.
3. Blice JP, Brown GC. Retinal vascular oc-clusive disease. In: Spaide RF ed. Dis-eases of the retina and vitreous.Philadelphia, W.B. Saunders Company,1999:116.
4. Clarkson JG. Central retinal vein occlu-sion. In: Ryan SJ. Retina. Singapore, CVMosby, 2001:1368.
5. Larsson J, Hultberg B, Hillarp A. Hyper-homocysteinemia and the MTHFRC677T mutation in central retinal veinocclusion. Acta ophthalmologica scandi-navica, 2000, 78(3):340–3.
6. Cahill M et al. Raised plasma homocys-teine as a risk factor for retinal vasculardisease. British journal of ophthalmol-ogy, 2000, 84(2):154–7.
7. Hayreh SS et al. Systemic diseases as-sociated with various types of retinalvein occlusion. American journal of oph-thalmology, 2001, 131(1):61–77.
8. Lahey JM et al. Laboratory evaluation ofhypercoagulable states in patients withcentral retinal vein occlusion who areless than 56 years of age. Ophthalmol-ogy, 2002, 109(1):126–31.
9. Vine AK. Hyperhomocysteinemia: a newrisk factor for central retinal vein occlu-sion. American journal of ophthalmol-ogy, 2000, 129(5):640–4.
10. Brown BA et al. Homocysteine: a risk fac-tor for retinal venous occlusive disease.Ophthalmology, 2002, 109(2):287–90.
21 Hyperhomocysteinaemia.pmd 8/17/2005, 11:09 AM639

640 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Aspects cytologiques des leucémiesaiguës : à propos de 193 cas colligésdans la région centrale de la TunisieN. Braham Jmili,1 A. Ben Abdelaziz,2 M. Nagara,1 T. Mahjoub,1 H. Ghannem2 etM. Kortas1
1Laboratoire d’Hématologie; 2Service d’Epidémiologie, C.H.U. Farhat Hached, Sousse (Tunisie).Reçu : 13/08/03 ; accepté : 22/01/04
RÉSUMÉ En Tunisie, peu de données concernant les leucémies aiguës sont disponibles en l’absence d’unregistre de population. Nous avons étudié les caractéristiques épidémiologiques et cytologiques de193 patients atteints de leucémie aiguë. Des hémogrammes ont été réalisés et des frottis de sang et demoelle ont été examinés pour chaque patient. L’âge des patients variait de 10 mois à 83 ans avec uneprédominance masculine (rapport : 1,27). Concernant le type de leucémie aiguë, 40,4 % avaient uneleucémie aiguë lymphoblastique, 51,8 % une leucémie aiguë myéloblastique et 7,8 % étaient des cas difficilesà classer. Dans notre série, 31,6 % des cas de leucémie aiguë s’observaient à un âge de moins de 10 anset 72 % de ces cas étaient de type lymphoblastique. Une anémie (hémoglobine <11 g/dL) a été observéedans 88,5 % des cas, une thrombopénie (plaquettes <100 000/mm3) dans 80,5 %, une hyperleuco-cytose > 100 000/mm3 dans 14,5 % avec une blastose sanguine dans 92 % des cas.
Cytological features of acute leukaemia in the central region of TunisiaABSTRACT In Tunisia, because of an absence of population registry, data on acute leukaemia are scarce.We studied the epidemiological and cytological characteristic of 193 patients with acute leukaemia. Haemo-grams were carried out and slides for peripheral blood and bone marrow were prepared for each patient. Theage range of the patients was 10 months to 83 years with a predominance of males (ratio: 1.27). As regardstype of leukaemia, 40.4% had acute lymphoblastic leukaemia, 51.8% had acute myeloblastic leukemia and7.8% were unclassified. Diagnosis was made at less than 10 years in 31.6% of cases and 72% of these werethe lymphoblastic type. Anaemia (Hb < 11 g/dL was found in 85% of cases, thrombocytopenia (plate-lets < 100 000/mm3) in 80.5% and hyperleukocytosis (WBC > 100 000/mm3) in 14.5% of cases with blastsin peripheral blood in 92% of cases.
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM640

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 641
Introduction
Les leucémies aiguës (LA) constituent ungroupe hétérogène d’affections héma-tologiques clonales caractérisées par uneprolifération maligne dans la moelle osseused’un clone cellulaire anormal du tissuhématopoïétique et bloqué à un stade précisde différenciation avec expansion decellules immatures (blastes) qui peuventêtre présentes dans le sang périphérique[1,2].
En Europe et aux États-Unis, les LAreprésentent 80 % des leucémies et environ35 % des cancers de l’enfant [2,3]. EnTunisie, les leucémies représentent lapremière hémopathie maligne diagnostiquéeet traitée [4].
Dès les premières descriptions, la sous-classification des LA en une série devariétés distinctes s’est imposée du simplefait de leur diversité morphologique. Cessubdivisions ont montré par la suite unintérêt pronostique du fait de leur sensibilitédifférente aux chimiothérapies [1,5].Malgré le développement de nouvelles tech-nologies pour la caractérisation desdifférentes entités de leucémies aiguës dansles applications cliniques [6-8], on continueà utiliser dans beaucoup de pays en déve-loppement les recommandations anciennesde la classification FAB (French-American-British), mise au point en 1976 et basée surdes caractéristiques morphologiques et cy-tochimiques [9].
En Tunisie, en l’absence d’un registrede population, les laboratoires d’anatomo-pathologie et les dossiers hospitaliersconstituent les principales sources d’infor-mation sur l’épidémiologie des cancers[10]. Toutefois, peu de données nationalesconcernant le profil épidémiologique etcytologique des leucémies aiguës sontdisponibles.
L’objectif de ce travail est de décrire, àtravers une série de 193 cas, les caractéris-tiques épidémiologiques et cytologiques dusang périphérique et de la moelle chez lespatients atteints de leucémie aiguë dans larégion du centre de la Tunisie.
Méthodes
Il s’agit d’une étude descriptive réalisée auLaboratoire d’Hématologie de l’Hôpital Far-hat Hached de Sousse. Cette étude a con-cerné tous les patients chez lesquels uneleucémie aiguë a été diagnostiquée entre le1er janvier 1998 et le 30 juin 2002.
Les échantillons de sang ont étéprélevés par ponction veineuse sur destubes avec EDTA K3 (acide éthylènediamine tétracétique tripotassique). Laponction de la moelle osseuse a été pra-tiquée chez l’adulte au sternum et en épineiliaque postérieure chez l’enfant.
L’hémogramme a été déterminé sur« Coulter MAXM ». Les frottis de sang etde moelle ont été colorés au MGG (May-Grünwald-Giemsa) par la méthode automa-tique (HEMATEK-AMES). Pour chaquepatient, trois lectures indépendantes desfrottis de sang et de moelle ont été assuréeset validées par des cytologistes.
Le diagnostic de LA a été porté dès qu’ily avait plus de 30 % de blastes dans lamoelle osseuse. L’examen de sang a permisd’établir la formule leucocytaire sanguine eta contribué à la classification des LA selonle groupe FAB. La séparation entre lessous-groupes des LA a été basée surl’appréciation du pourcentage des blastesdans la moelle, le type de blastes et lecompte absolu des monocytes sanguins[11].
La sous-classification morphologiquedes leucémies aiguës lymphoblastiques
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM641

642 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
a été basée sur un système de score uti-lisant les caractères cellulaires suivants : lerapport nucléocytoplasmique, la présencede nucléoles, l’irrégularité du profil nu-cléaire et la présence de grandes cellules[12]. La recherche de l’activité myélope-roxydasique par la technique à la pyronine aété la réaction cytochimique appliquée surun frottis de moelle dans le cas où l’aspectmyéloïde n’était pas évident et elle a étéconsidérée négative si on notait une propor-tion de moins de 3 % de blastes peroxydasepositive.
Les données répertoriées ont été ensuiteinformatisées sur le logiciel de traite-ment statistique (SPSS.10) au Serviced’Epidémiologie du C.H.U. Farhat Hachedde Sousse. Les statistiques descriptives(moyennes, fréquences) ont été utiliséespour résumer les données.
Résultats
La répartition de 193 cas de LA selon lesmois a montré une variation saisonnièreavec deux pics : printemps et automne.L’âge des patients variait de 10 mois à83 ans. Le rapport était de 1,27 en faveurdu sexe masculin. Les leucémies aiguëstouchaient tous les âges avec unefréquence plus élevée chez l’enfant (Figure1).
L’examen cytologique des frottis desang et de moelle ont permis d’affirmer lediagnostic des 193 cas de LA et d’en pré-ciser le type cellulaire (Tableau 1) : 40,4 %des cas étudiés étaient de type lymphoblas-tique dont 56,4 % étaient de type L1 et32,1 % étaient de type L2. La réaction demyéloperoxydase était indispensable dans36 % des cas, vu l’absence de signe de dif-férenciation cytologique, et il était impossi-ble de classer 7,8 % des frottis examinés.Les leucémies aiguës de type myéloïde
Figure 1 Répartition par âge et par sexe de193 cas de leucémie aiguë colligés dans larégion centrale de la Tunisie
A : LAL (Leucémie aiguë lymphoblastique)
B : LAM (Leucémie aiguë myéloïde)
Hommes
Femmes
Hommes
Femmes
Âge
(an
s)Â
ge (
ans)
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM642

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 643
représentaient 51,8 % des cas avec une dis-tribution homogène des différents sous-types 1, 2, 3, 4 et 5. Les LAM 6 et 7 étaientplus rares. Le sous-typage était impossibledans 17 % des LAM et 6,6 % des LAL.
L’étude de la numération et formulesanguine de ces 193 patients atteints de LAa conclu aux différentes anomalies illus-trées par la figure 2. Elle a montré une blas-tose sanguine dans 92 % des cas. L’anémiea été observée dans 88,5 % des cas avecune thrombopénie dans 80,5 % des cas.
Discussion
Depuis une vingtaine d’années, la classifi-cation des LA fait appel aux recommanda-tions du groupe FAB. L’intérêt longtempsporté à cette classification tient à sa relativesimplicité basée sur une descriptionmorphologique simplifiée, après colorationdes frottis de sang et de moelle par la mé-thode de May-Grünwald-Giemsa com-plétée par des examens cytochimiques[11], accessible à tous les laboratoires ettenant compte des anomalies cytologiquesdu sang et de la moelle. Cette approchereste toujours la base du diagnostic des LAen application clinique malgré ses limites.
En effet, dans notre étude, le plussouvent le diagnostic des LA est évident.Cependant, des difficultés de classement sesont posées en cas de frottis pauvres oumal étalés. La ponction est difficile à réali-ser en cas de myélofibrose pouvant gênerl’aspiration de moelle. D’où la nécessité decaractériser la population blastique pard’autres marqueurs immunologiques etcytogénétiques pour affirmer ou mêmemodifier le diagnostic et aussi mieux ciblerles indications thérapeutiques initiées [2].C’est la confrontation de l’examen desfrottis sanguins et l’étude des moléculesmembranaires de surface qui permettra undiagnostic dans les cas difficiles [13,14].En effet, l’immunophénotypage est indis-pensable pour confirmer le diagnostic desLAL, rechercher une LA biphénotypique etéliminer une LAM indifférenciée (LAM0)[15]. L’intérêt du caryotype dans les leucé-mies aiguës est bien établi. Les anomaliesdécelées représentent l’un des critères declassement d’une LA [6,16]. De même, labiologie moléculaire a fait aujourd’hui sonentrée dans l’évaluation des LA, notam-ment pour la mise en évidence des translo-cations cryptiques et l’analyse des échecsdu caryotype et surtout son intérêt majeur
Tableau 1 Classification cytologique des193 cas de leucémie aiguë colligés dans larégion centrale de la Tunisie
Cas Nbre %
LAM 1 100 51, 8
LAM1 12 12,0
LAM2 17 17,0
LAM3 15 15,0
LAM4 16 16,0
LAM5 15 15,0
LAM6 7 7,0
LAM7 1 1,0
LAMDAC2 17 17
LAL3 78 40,4
LAL1 44 56,4
LAL2 25 32,1
LAL3 4 5,1
LALDAC4 5 6,4
LADAC5 15 7,8
Total 193 100
1LAM : leucémie aiguë myéloïde.2LAMDAC : leucémie aiguë myéloïde difficile àclasser.3LAL : leucémie aiguë lymphoïde.4LALDAC : leucémie aiguë lymphoïde difficile àclasser.5LADAC : leucémie aiguë difficile à classer.
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM643

644 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
pour l’évaluation de la maladie résiduelle[7]. Ainsi, la classification des LA proposéepar l’OMS intègre les données mor-phologiques, immunophénotypiques, géné-tiques et cliniques dans le but de définir desentités biologiquement homogènes et cli-niquement pertinentes [17]. Le classementdes leucémies aiguës est basé surl’appartenance des blastes à une lignéelymphoïde ou myéloïde.
Les leucémies aiguës lymphoïdes (LAL)sont divisées en LAL à précurseurs B etLAL à précurseurs T.
Les leucémies aiguës myéloïdes (LAM)comprennent 4 grandes catégories [8,17] :• LAM avec anomalies génétiques récur-
rentes ;• LAM avec signes de dysplasie touchant
plusieurs lignées ;
• LAM secondaires à des thérapeu-tiques ;
• LAM autres, n’entrant pas dans lescatégories précédentes.Toutefois, il faut noter que ces nou-
velles techniques sont longues à mettre enœuvre et nécessitent une certaine pratique,ce qui les réserve à des laboratoires spécia-lisés, et devant l’extrême urgence de lamaladie, l’examen cytologique du sang etde la moelle reste un moyen rapide qui per-met, dans l’heure qui suit le prélèvement, lediagnostic de la majorité des LA.
Les deux variétés L1 et L2 des LAL nesont pas réellement distinctes par unecatégorie particulière de cellules blastiquesmais plutôt par des proportions différentesd’éléments cellulaires qu’elles peuvent
Figure 2 Anomalies de l’hémogramme chez 193 cas de leucémie aiguë colligés dans la régioncentrale de la Tunisie.Anémie (hémoglobine < 11 g/dL), thrombopénie (plaquettes < 100 000/mm3), neutropénie(polynucléaires neutrophiles < 1500/mm3) hyperleucocytose (globules blancs > 10 000/mm3),neutropénie sévère (polynucléaires neutrophiles < 1000/mm3), thrombopénie sévère(plaquettes < 20 000/mm3), pancytopénie (anémie, thrombopénie et leucopénie : globulesblancs < 4000/mm3)
100
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM644

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 645
avoir en commun [4]. La valeur pronos-tique des formes L2 par rapport aux formesL1 n’a jamais pu être mise en évidence[11].
Cinq pour cent (5 %) des LAL étaient detype L3. Cette forme, distinguée par uncritère cytoplasmique très particulier descellules de Burkitt, doit être considérée àpart des LAL classiques. Le type L3 est peufréquent en France, tant chez l’adulte(9,7 %) que chez l’enfant (4,6 %) [18]. LesLAL de type Burkitt étaient classiquementde pronostic très péjoratif mais l’instau-ration de protocoles de chimiothérapie in-tensive et brève a entraîné un changementde pronostic et une amélioration des chan-ces de guérison.
La présence de granulations dans lesblastes fait suspecter une origine myélo-blastique. Le diagnostic peut être portéavec certitude sur un très faible pourcen-tage de blastes s’ils renferment un ou descorps d’Auer, témoignant de leur caractèremalin [15]. Les caractères cytologiques desLAM ont une valeur pronostique discutée ;des études ont montré que le taux de rémis-sion complète a été plus élevé dans lescatégories M1, M2 et M3 que dans lesformes M4, M5 et M6, mais ces constata-tions n’ont pas été partagées par d’autresauteurs [19].
La littérature médicale rapporte que lesLA de l’enfant, bien que rares en soi,représentent la première cause de cancerpédiatrique (30 %) et surviennent surtoutavant 9 ans. En Europe et aux États-Unis,les LAL représentent 75 % à 80 % desleucémies et environ 20 % des cancers del’enfant de moins de 15 ans [3]. En effet,les LAL touchent de préférence les âgesextrêmes avec une distribution bimodale del’incidence et de la mortalité (<15 ans et> 80 ans). Chez l’adulte, elles sont au con-traire quatre fois plus rares que les LAM(environ 5 % des leucémies) [18].
Dans notre série, 31,6 % des cas de LAs’observent à un âge de moins de 10 ans, et72 % des cas sont de type lymphoblastique.Cependant, notre série comportait seule-ment 2 cas de LAL chez les patients âgés deplus de 50 ans et nous pensons que cettefréquence pourrait être sous-estimée et quela pathologie serait sous-diagnostiquée danscette tranche d’âge. En revanche, nos ré-sultats corroborent ce qui est rapporté dansles différentes séries concernant la fré-quence des LAM chez l’adulte. Les LAMétaient quatre fois plus importantes que lesLAL dans la tranche 20 à 60 ans, puis lafréquence restait stable jusqu’à un âgesupérieur à 80 ans.
L’âge est le facteur de pronostic le plusimportant pour la réussite du traitementd’induction des LAM [20]. Concernant lesLAL, chez l’adulte, le risque de rechute oud’échec primaire s’accroît au-dessus de35 ans ; la maladie est souvent hyperleuco-cytaire avec une atteinte méningée initiale,et le traitement est plus toxique à cet âge.Chez l’enfant plus grand, le pronostic sedégrade à partir de 10-11 ans pour rejoindrecelui de l’adulte à partir de 15 ans. Lepronostic est très défavorable si l’âge estinférieur à 12 mois, et surtout inférieur à6 mois [2].
Le genre humain a une moindre valeurpronostique. Dans notre série, le rapport aété de 1,27 en faveur du sexe masculinavec une nette prédominance du sexe mas-culin à l’âge adulte. La prédominance mas-culine a été manifeste pour les leucémiesaiguës de type lymphoblastique (Figure 1).Le pronostic est plus défavorable pour lesexe masculin dans ce cas (rechute testicu-laire dans 5 % des cas). Contrairement auxLAL, le sexe ne semble pas être un facteurde pronostic dans les LAM.
Les leucémies aiguës associent à desdegrés variables des signes de proliférationet d’insuffisance médullaire. L’étude de
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM645

646 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
l’hémogramme a montré des cellules blas-tiques dans 92 % des cas mais cela n’a pasété suffisant pour poser le diagnostic [2].La détermination de la numération etformule sanguine a permis par ailleursd’apprécier :• le degré de l’anémie : un chiffre normal
d’hémoglobine (11,5 % des cas) traduitsouvent une forme rapidement évolutiveet de plus mauvais pronostic ;
• l’intensité de la thrombopénie et lerisque hémorragique : on notait unethrombopénie sévère avec un risqued’hémorragie cérébrale dans 35,1 %des cas ;
• la leucocytose qui constitue un facteurpronostique majeur. Le pronostic estplus favorable quand la leucocytose estinférieure à 100 000/mm3 [2]. Dansnotre série, les LA se présentaientfréquemment sous une forme hyper-leucocytaire (64,5 % des cas). Le chif-fre de globules blancs a été supérieur à100 000/mm3 dans 14,5 % des cas avecune pancytopénie uniquement dans10,5 % des 193 cas.
• Le degré de la neutropénie absolueprédit le risque infectieux. Nos résultats
ont montré une neutropénie dans78,3 % des cas ; elle a été sévère dans55,5 % des cas. Des résultats similairesont été déjà décrits et ont trouvé notam-ment une leucocytose supérieure à100 000/mm3 dans 5 à 10 % [2].
Conclusion
Un hémogramme complet avec une lectureminutieuse des frottis de sang et de moellecomplétée par des réactions cytochimiquespermettent encore le classement de laplupart des LA. Cependant l’étude d’autresmarqueurs cytogénétiques, immunolo-giques et moléculaires est devenue néces-saire pour confirmer le diagnostic des LALet pour identifier des LA d’aspect atypique.La classification OMS nouvellementproposée utilise une combinaison del’ensemble de ces approches, prenant enconsidération leur capacité à définir des en-tités biologiques qui, avec l’âge et lesanomalies de l’hémogramme, permettentde définir le schéma thérapeutique etreprésentent les éléments utiles au pronos-tic [9,17].
Références1. Hollard D. Les leucémies aiguës. EMC
(Paris-France). Sang, 1983, 13015 A20 :5-1983, 5–13.
2. Hunault-Berger M, Pellier I, NorbertI. Leucémie aiguë lymphoblastique(adulte et enfant). La Revue du Praticien,1999, 49:441–5.
3. Chan KW. Acute myeloid leukaemia.Acute lymphoblastic leukaemia. Currentproblems in pediatric and adolescenthealth care, 2002, 32(2):40–9.
4. Laatiri M, Ennabli S. Lymphomes nonhodgkiniens. In : Maalej M, ed. Cancé-
rologie pratique. Tunis, Centre de Publi-cation universitaire, 1999: 447–55
5. Flandrin G et al. Classification desleucémies aiguës. EMC (Paris-France),Sang, 13015 A10, 7-1988, 5–10.
6. Charrin C, Mugneret F. Cytogénétiquedes leucémies aiguës de novo. La Re-vue du Praticien, 1996, 46:37–41.
7. Gabert J. Utilité de la biologie molécu-laire dans le diagnostic des leucémiesaiguës et l’évaluation de la maladierésiduelle. La Revue du Praticien, 1996,46:42–7.
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM646

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 647
8. Paredes-Aguilera R et al. Flowcyto-met-ric analysis of cell-surface and intra cel-lular antigens in the diagnosis of acuteleukaemia. American journal of hematol-ogy, 2001, 68(2):69–74.
9. Flandrin G. La nouvelle classificationOMS des hémopathies malignes. Hémo-pathies myéloïdes. Hématologie, 2001,7(2):136–41.
10. Ben abdallah M. Epidémiologie des can-cers en Tunisie. In : Maalej M, ed.Cancérologie pratique. Tunis, Centre dePublication universitaire, 1999:33–7.
11. Imbert M, Jouault H, Tulliez M. Cytologiedes leucémies aiguës. La Revue duPraticien, 1996, 46:23–9.
12. Bennet JM et al. The morphological clas-sification of acute lymphoblastic leu-kaemia: concordance among observersand clinical correlation. British journal ofhaematology, 1981, 47(4):553–61.
13. Feki S et al. Contribution of flow cyto-metry to acute leukaemia classificationin Tunisia. Disease markers, 2000, 16:131–3.
14. Cabrera E et al. Acute myeloid leu-kaemia: clinical and laboratory charac-
teristics. Revista modica de Chile, 1999,125(4):433–7.
15. Imbert M. Place du biologiste dans lediagnostic et le suivi des leucémiesaiguës. Revue Française des Labora-toires, 2002, 344:67–70.
16. Bennett JM et al. Hypergranular promy-elocytic leukaemia: correlation betweenmorphology and chromosomal translo-cations including t(15;17) and t(11;17).Leukaemia, 2000, 14(7):1197–200.
17. Valensi F. Classification des leucémiesaiguës : nouvelles propositions del’OMS. Revue Française des Labora-toires, 2002, 344:19–24.
18. Roy P, Coleman MP. Epidémiologie desleucémies aiguës lymphoïdes. Revued’épidémiologie et de santé publique,1992, 40:323–34.
19. Reiffers J, Perel Y, David B. Traitementdes leucémies aiguës. In : Breton-GoriusJ et al., eds. L’hématologie de BernardDreyfus. Paris, Flammarion, 1992 :805–25.
20. Xavier T, Belharbi A. Leucémies aiguësmyéloïdes du sujet âgé : Mise au point.Bulletin du cancer, 2002, 2(2):143–54.
22 Aspects cytologiques 1.pmd 8/17/2005, 11:09 AM647

648 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Physicians’ knowledge, attitude andpractice towards erectile dysfunctionin Saudi ArabiaM.F. Abdulmohsen,1 I.S. Abdulrahman,1 A.H. Al-Khadra,1 A.A. Bahnassy,2 S.A. Taha,3
B.A. Kamal3, A.M. Al-Rubaish1 and A.H. Al-Elq1
1Department of Internal Medicine; 2Department of Family and Community Medicine; 3Department ofUrology, College of Medicine, King Faisal University, Dammam, Saudi Arabia.Received: 06/05/03; accepted: 19/11/03
ABSTRACT We aimed to test the knowledge, attitude and practice (KAP) of physicians towards erectiledysfunction in the Eastern province of Saudi Arabia. At a scientific meeting about erectile dysfunction, 159physicians from both government and private sectors answered a 34-item questionnaire in private. Themean total KAP score for the group was below the expected standard of 60%. Male physicians scoredsignificantly higher than females. Urologists scored the highest, followed by andrologists. Surprisingly, phy-sicians with higher qualifications scored lower than those with intermediate qualifications and even less thangeneral practitioners. Those who had practised for ≥ 10 years scored better than those with < 10 yearspractice. The role of cardiologists in the diagnosis and management of erectile dysfunction is discussed.
Connaissances, attitudes et pratiques des médecins concernant le dysfonctionnement érectile enArabie saouditeRÉSUMÉ Cette étude visait à tester les connaissances, attitudes et pratiques (CAP) des médecins concer-nant le dysfonctionnement érectile dans la province orientale d’Arabie saoudite. Lors d’une réunion scienti-fique sur le dysfonctionnement érectile, 159 médecins du secteur gouvernemental et du secteur privé ontrépondu en privé à un questionnaire de 34 items. Le score CAP total moyen pour le groupe était en deçà duniveau escompté de 60 %. Les médecins hommes ont obtenu un score significativement plus élevé que lesmédecins femmes. Les urologues ont eu les scores les plus élevés, suivis par les andrologues. De manièresurprenante, les médecins ayant les qualifications les plus élevées ont eu des scores inférieurs à ceux quiavaient des qualifications intermédiaires et même à ceux des généralistes. Les médecins qui pratiquaientdepuis 10 ans ou plus ont eu de meilleurs scores que ceux qui pratiquaient depuis moins de 10 ans. Le rôlejoué par les cardiologues dans le diagnostic et la prise en charge du dysfonctionnement érectile est examiné.
23 Physicians knowledge.pmd 8/17/2005, 11:09 AM648

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 649
Introduction
Erectile dysfunction is one of the morecommonly under-diagnosed medical disor-ders in the world [1]. It is defined as thepersistent inability to maintain or to achievean erection of sufficient rigidity to have sat-isfying sexual activity [2]. Recent estimatesfrom the National Institutes of Health(NIH) in the United States suggest thatabout 30 million Americans have partial orcomplete erectile dysfunction [1].
The problem of erectile dysfunction ismainly linked to age, as shown in the Mas-sachusetts Male Aging Study, where 52%of the male study population aged 40–70years had some degree of erectile dysfunc-tion [3]. Surprisingly, only about 1 in 10men with erectile dysfunction between 18and 59 years of age seek medical adviceabout their problem [4]. In another study,44% of 500 patients who were consultingtheir urologists for reasons other than erec-tile dysfunction were found to have a histo-ry of erectile dysfunction but failed toinform their physicians about their prob-lem. The reason given by 74% of them wasembarrassment [5].
It is believed that there are 2 major rea-sons for overlooking erectile dysfunctionas a major health disorder. First, the major-ity of men with erectile dysfunction do notseek medical advice despite the growingawareness of the available treatment op-tions. The main causes for that are: socialas well as religious; concerns about embar-rassment and shame; indifference; andfears about side-effects of treatment. Sec-ondly, the majority of physicians do not askenough questions to identify men witherectile dysfunction or encourage them toseek treatment [6].
The prevalence of erectile dysfunctionin non-insulin dependent Saudi diabeticmen from the Mecca region was 81.1%
[7]. The risk factors for erectile dysfunc-tion were: age, history of long standing dia-betes for more than 10 years, and poormetabolic control. In another study includ-ing 388 patients with different degrees oferectile dysfunction from Jeddah, SaudiArabia, the severity of erectile dysfunctionwas mainly age-related, and physical inac-tivity, alcohol consumption and drug addic-tion were the only independent risk factorsafter adjusting for age. It has also beenfound that severe erectile dysfunction wasa strong predictor of poor quality of life[8]. Therefore, physicians in general, andcardiologists in particular, should take theinitiative to open the discussion about sexu-al activity with their male patients for sev-eral important reasons. First, erectiledysfunction and coronary artery diseaseshare many risk factors such as diabetesmellitus, hypertension, smoking, dyslipi-daemia and ageing. Secondly, it is possiblethat the same vascular and endothelialchanges that take place in the coronary ar-teries are likely to occur in the cavernosalarteries that supply the penile erectile tissue[2,3,9]. The evaluation of erectile functionof a male patient may thus open a clinicalwindow to a silent, yet growing coronary,peripheral or cerebrovascular disease andto other undiagnosed medical problemssuch as hypertension, diabetes mellitus anddyslipidaemia [10–16]. One more aspect ofthe problem of overlooking erectile dys-function in our opinion is the inappropriateknowledge, attitude and practice (KAP) ofphysicians towards erectile dysfunction,which may alter their ability to provide theirpatients with proper advice about the treat-ment options.
The objective of this study was to as-sess the KAP of practising physicians to-wards erectile dysfunction in one region ofSaudi Arabia.
23 Physicians knowledge.pmd 8/17/2005, 11:09 AM649

650 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Methods
SampleThis was a cross-sectional study carriedout in the Eastern province of Saudi Arabia.The estimated sample size was 200 physi-cians, selected from both the governmentand private medical sectors in Dammamregion (Dammam, Al-Qatif and Al-Khobar).A multistage random sample was used,where physicians were classified into 2main strata: government and private. Usingproportional allocation, a systematic ran-dom sample was used to select the requirednumber of physicians from each stratum.
QuestionnaireA questionnaire with 36 questions was de-signed to collect information on: demo-graphic and professional data of therecruited physicians (8 items), currentknowledge (13 items), attitudes towardserectile dysfunction (8 items) and practiceswhen dealing with a patient suffering fromerectile dysfunction (7 items).
The questionnaire was designed by theauthors and validated by a panel of expertsin the field. A pilot study was undertaken on20 physicians from the university hospitalwho were excluded from the study popula-tion before choosing the sample. Based onthe results of the pilot study, the question-naire was modified. The weighting of eachquestion relating to knowledge, attitude andpractice was determined by the researchteam and experts in epidemiological stud-ies. The total score was 100 marks and themaximum scores for knowledge, attitudeand practice questions were 42, 28 and 30marks respectively.
Data collection and analysisThe targeted physicians were invited to at-tend a scientific meeting on erectile dys-function at 2 different locations, one for the
private and the other for the governmenthospital doctors.
The questionnaires were distributed andanswered in a 45-minute private session atthe beginning of the scientific meeting. Thesecond part of that scientific meeting was acomprehensive lecture about erectile dys-function including anatomy and patho-physiology, delivered by the principalinvestigator.
The data were entered into the personalcomputer using SPSS, version 10. Descrip-tive statistics for all variables wereperformed after scrutinizing the data. Sta-tistical analysis was made using t-test,Mann–Whitney test, analysis of varianceand Kruskal–Wallis as appropriate.
Results
Two hundred (200) physicians were invit-ed to attend the 2 scientific meetings. A to-tal of 192 physicians were able to attend(96%) and out of that number, 159 an-swered the questionnaire, giving a responserate of 82.8%. The number of male physi-cians was much higher than female physi-cians: 151 (95.6%) and 7 (4.4%) respec-tively. One physician failed to mention his/her sex.
The mean and standard deviation (SD)overall KAP score for all the respondentswas 55.6 (14.9) (maximum 100), theknowledge score was 19.0 (8.2) (maxi-mum 42), the attitude score was 19.0(4.5) (maximum 28) and the practicescore was 17.3 (5.3) (maximum 30).
Table 1 shows the mean total KAP scoreby sex. The mean overall KAP score forfemales was significantly lower than that ofmale physicians (P < 0.001). This was re-flected in significantly lower mean knowl-edge and practice scores for females (P =0.021 and P = 0.011 respectively). The
23 Physicians knowledge.pmd 8/17/2005, 11:09 AM650

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 651
mean attitude score was also lower for fe-males than males but this difference wasnot statistically significant.
The mean overall KAP score of physi-cians was significantly different by special-ity (Table 1). Urologists scored the highestmarks followed by andrologists, psychia-trists, general surgeons, cardiologists, gy-naecologists and other specialties includinggeneral practitioners (P < 0.001). Theknowledge score of the urologists was the
highest, followed by andrologists, thengeneral surgeons, cardiologists, psychia-trists, gynaecologists, and other specialities(P < 0.001). The highest score for attitudewas obtained by gynaecologists and thelowest by other specialities, but the differ-ence was not significant (P = 0.087). Thescore for practice was significantly differ-ent among different specialities (P <0.001). Urologists scored the highestmarks, followed by andrologists, psychia-
Table 1 Knowledge, attitude and practice scores for physicians by sex,specialty, qualifications and years of practice
Variable No. Mean (SD)Knowledge Attitude Practice Total(max. 42) (max. 28) (max.30) (max. 100)
SexMale 151 19.4 (8.1) 19.0 (4.5) 17.6 (5.2) 58.2 (14.9)Female 7 11.4 (5.6) 17.4 (3.4) 12.5 (3.9) 42.9 (9.6)
P = 0.011 P = 0.353 P = 0.013 P = 0.021
SpecialtyUrologist 14 29.0 (6.2) 19.7 (4.5) 23.6 (2.9) 73.0 (8.9)Andrologist 11 24.3 (10.6) 21.1 (4.0) 21.6 (3.8) 67.0 (14.9)Psychiatrist 7 20.0 (7.3) 20.9 (6.6) 19.3 (3.5) 60.1 (14.1)General surgeon 16 20.7 (8.2) 20.8 (3.4) 16.9 (5.6) 58.9 (15.9)Cardiologist 10 20.4 (8.9) 18.6 (4.9) 18.3 (6.1) 57.3 (18.1)Gynaecologist 6 19.7 (9.9) 21.5 (3.6) 13.2 (6.7) 54.4 (19.2)Other specialty 84 16.9 (6.5) 18.3 (4.2) 16.3 (4.6) 51.8 (11.8)
P < 0.001 P = 0.087 P < 0.001 P < 0.001
QualificationsMD or equivalent 31 14.5 (6.3) 17.1 (4.6) 15.0 (4.3) 47.4 (11.7)MSc or equivalent 55 21.0 (8.9) 20.1 (3.9) 18.3 (5.2) 59.5 (15.3)GP with MB BS 66 19.9 (7.7) 19.4 (4.4) 18.1 (5.3) 57.5 (14.2)
P < 0.001 P = 0.007 P = 0.008 P < 0.001
Years of practice< 10 52 17.3 (6.8) 18.3 (4.0) 15.9 (4.6) 51.6 (13.0)≥ 10 97 20.5 (8.6) 19.5 (4.7) 18.4 (5.3) 58.7 (15.1)
P = 0.021 P = 0.112 P = 0.005 P = 0.005
GP = general practitioner.SD = standard deviation.aNumber of respondents; responses missing for some categories.
23 Physicians knowledge.pmd 8/17/2005, 11:10 AM651

652 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
trists, cardiologists, general surgeons, oth-er specialities, and the lowest score by gy-naecologists.
Table 1 also shows physicians’ KAP to-wards erectile dysfunction in relation totheir qualifications. Surprisingly, the physi-cians with highest qualifications, e.g. med-ical doctorate or equivalent, scored thelowest marks [mean knowledge score 14.5(SD 6.3)] compared with physicians withintermediate qualifications, e.g. master’sdegree or equivalent, (21.0, SD = 8.9) orgeneral practitioners (19.9, SD = 7.7) (P <0.001). There was a similar trend on theattitude and practice sections, with signifi-cant differences among the physicians ac-cording to level of qualifications (P = 0.007and P = 0.008 respectively).
The mean overall KAP score was signif-icantly higher for physicians with 10 ormore years practice than those with lessthan 10 years practice (P = 0.005) (Table1). The difference between the 2 groupswas significant for knowledge and practice(P = 0.021 and P = 0.005 respectively) butnot for attitude (P = 0.112).
Some examples of responses to individ-ual questions are as follows. Question no.10 (knowledge question) asked for theproper definition of erectile dysfunction;this was correctly answered by 66.5% ofphysicians. Question no.12 (attitude ques-tion) inquired about the most common eti-ology of erectile dysfunction; surprisingly,52.5% of the physicians believe that it ismainly a psychogenic problem. Questionno. 23 (practice question) inquired aboutthe actions to be considered in dealing witha patient reporting a new onset of erectiledysfunction; 46.2% believed that such pa-tients should be referred to the urologist,whereas 14.0% did not know the correctanswer to this question. Question no. 26(practice question) dealt with the therapeu-tic modality of choice for treating the ma-
jority of cases of erectile dysfunction, and83.9% of the physicians were able to givethe correct answer.
Discussion
Erectile dysfunction is a major public healthproblem worldwide, but is commonly un-der-diagnosed [1,2,7,13]. In this study, weaimed to answer the main question: “Dophysicians know enough about erectiledysfunction and do they have the right atti-tude and practice towards it?”
The study results revealed a high re-sponse rate, with 159 out of 192 meetingattendees (83%) answering the question-naire. The mean overall KAP score for allphysicians was below 60% of the total, theknown accepted standard for the evalua-tion of both undergraduate and postgradu-ate medical students. The performance offemale physicians was significantly lowerthan the performance of male physicians,despite the assurance of the highest degreeof confidentiality. Social and cultural fac-tors may account for the significant gap inboth knowledge and interest of the femalephysicians in this part of the world.
Approximately 80% of cases of erectiledysfunction are due to an organic cause,especially atherosclerosis of the cavernosalarteries of the penile tissue, and only 20%of the cases are due to psychiatric and psy-chogenic disorders [1–3]. Therefore, theclinical evaluation and treatment of erectiledysfunction should have a multidisciplinaryapproach. Fifty per cent (50%) of themembers of NIH Consensus DevelopmentPanel on Impotence held in 1992 were urol-ogists, 14% were psychiatrists and 35%were representatives of other medical spe-cialities [1]. This misconception that erec-tile dysfunction is under the domain ofurologists agrees with our results. Urolo-
23 Physicians knowledge.pmd 8/17/2005, 11:10 AM652

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 653
gists had the highest marks in the total KAPscore (73%), followed by andrologists andpsychiatrists, as compared with the rest ofthe specialities who scored lower. Despitethe fact that 66.5% of the studied physi-cians were able to define erectile dysfunc-tion correctly, 52.5% still believed that theetiology of this problem is mainly psy-chogenic. Furthermore, 46% of the studiedphysicians preferred to refer patients pre-senting with new onset erectile dysfunctiondirectly to the urologist, and 60% of themignored the importance of obtaining a de-tailed medical history, performing a properphysical examination or requesting the nec-essary investigations (such as fasting bloodsugar, lipid profile, testosterone, prolactin,luteinizing hormone and follicle-stimulatinghormone) [2,9].
The total KAP score of the study popu-lation was strongly affected by the level ofqualifications. Unexpectedly, physicianswith higher qualifications scored muchlower than physicians with intermediatequalifications, and even less than generalpractitioners. The poor performance ofhighly qualified physicians may be relatedto an inappropriate attitude towards erectiledysfunction, whose diagnosis and manage-ment was thought to be mainly under thedomain of urologists and/or psychiatrists.Physicians with higher qualifications andwho are highly specialized may have littleinterest in updating their general medicalknowledge. However, the duration of phy-sicians’ practice in years was a positivepredictor of better performance. Physi-cians who had more than 10 years practicescored significantly higher than those withless than 10 years practice.
The increased understanding of thepathogenesis, proper evaluation and accu-rate diagnosis, and the available treatment
options of erectile dysfunction, shouldstimulate health care planners to find waysof improving public awareness and physi-cians’ up-to-date knowledge about this ma-jor medical problem.
Conclusion andrecommendations
The role of physicians, especially cardiolo-gists, is pivotal in the process of evaluationand management of erectile dysfunction. Inthis study of physicians who have a scien-tific and clinical interest in erectile dysfunc-tion, the overall KAP scores for allphysicians were below the expected stan-dard. We recommend that:• Undergraduate curricula and postgradu-
ate training programmes should bemodified to accommodate and empha-size up-to-date knowledge about earlydetection, evaluation and managementof erectile dysfunction.
• The Ministry of Health, through healthpolicy planners, universities and othermedical sectors should find the properapproach and plans to improve the gen-eral public awareness regarding theimportance of early diagnosis and treat-ment of erectile dysfunction.
Acknowledgements
We are grateful to Dr Emmanuel Larbi,Consultant Internist/Clinical Pharmacologyand Professor of the Department of Inter-nal Medicine, King Faisal University, andKing Fahd Hospital of the University for hisinvaluable effort in reviewing this manu-script, and Mr Ramesh Kumar for his sec-retarial support.
23 Physicians knowledge.pmd 8/17/2005, 11:10 AM653

654 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
1. NIH Consensus Development Panel onImpotence. Journal of the AmericanMedical Association, 1993, 270:83–90.
2. Miller TA. Diagnostic evaluation of erec-tile dysfunction. American family physi-cian, 2000, 61(1):95–104, 109–10.
3. Feldman HA et al. Impotence and itsmedical and psychological correlates,results of the Massachusetts Male AgingStudy. Journal of urology, 1994, 151:54–61.
4. Laumann EO, Paik A, Rosen RC. Sexualdysfunction in the United States: preva-lence and predictors. Journal of theAmerican Medical Association, 1999,281:537–44.
5. Baldwin KC, Ginsberg PC, HarkawayRC. Underreporting of erectile dysfunc-tion among men with unrelated urologicconditions. Abstract presented at the An-nual Meeting of the American UrologicalAssociation, April 29–May 4, 2000, At-lanta, Georgia.
6. Levine LA, Kloner RA. Importance of ask-ing questions about erectile dysfunction.American journal of cardiology, 2000,86:1210–3.
7. El-Sakka AI, Tayeb KA. Erectile dysfunc-tion risk factors in noninsulin dependentdiabetic Saudi patients. Journal of urol-ogy, 2003, 169(3):1043–7.
8. Abolfotouh MA, Al-Helali NS. Effect oferectile dysfunction on quality of life.Eastern Mediterranean health journal,2001, 7(3):510–8.
9. DeWire DM. Evaluation and treatment oferectile dysfunction. American familyphysician, 1996, 53:2101–8.
10. Pritzker MR. The penile stress test: a win-dow to the hearts of man. Abstract pre-sented at the 72nd Scientific Session ofthe American Heart Association, Novem-ber 7–10, 1999, Atlanta, Georgia.
11. Billups K, Friedrich S. Assessment of fast-ing lipid panels and Doppler ultrasoundtesting in men presenting with erectiledysfunction and no other medical prob-lems. Abstract presented at the Ame-rican Urological Association, April 29–May 4, 2000, Atlanta, Georgia.
12. Cheitlin MD et al. ACC/AHA expert con-sensus document. Use of sildenafilcitrate (Viagra) in patients with cardio-vascular disease. Journal of the Ameri-can College of Cardiology, 1999, 33:273–82.
13. Jackson G. Erectile dysfunction and car-diovascular disease. International jour-nal of clinical practice, 1999, 53:363–8.
14. Jackson G et al. A systematic approachto erectile dysfunction in the cardiovas-cular patient: a consensus statement. In-ternational journal of clinical practice,1999, 53:445–51.
15. Jackson G. Sexual intercourse and an-gina pectoris. International rehabilitationmedicine, 1979, 3:35–7.
16. O’Kane PD, Jackson G. Erectile dysfunc-tion: is there silent obstructive coronaryartery disease? International journal ofclinical practice, 2001, 55:219–20.
References
23 Physicians knowledge.pmd 8/17/2005, 11:10 AM654

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 655
Report
SARS: the new challenge tointernational health and travelmedicineS. Venkatesh1 and Z.A. Memish2
1Medical Affairs Division; 2Infection Prevention and Control Program and Infectious Diseases Division,Department of Medicine, King Abdulaziz Medical City, Riyadh, Saudi Arabia.Received: 24/08/03; accepted: 25/01/04
SUMMARY Severe acute respiratory syndrome (SARS), the first severe new infectious disease of thismillennium, caused widespread public disruption. By July 2003, 8427 probable SARS cases had beenreported from 29 countries with a case fatality rate of 9.6%. The new febrile respiratory illness spread aroundthe world along the routes of international air travel, with outbreaks concentrated in transportation hubs ordensely populated areas. The etiologic agent was identified as a novel coronavirus, SARS-CoV. The diseaseis transmissible person-to-person through direct contact, large droplet contact and indirect contact fromfomites and unwashed hands. Saudi Arabia successfully prevented the entry of the disease by imposingtravel restrictions, special entry requirements, screening procedures at airports, including temperaturechecks, and quarantine. Ongoing efforts are aimed at developing case investigation, case management andsurveillance protocols for SARS.
Introduction
In the first half of 2003, the global commu-nity saw the emergence and impact of se-vere acute respiratory syndrome (SARS),the first severe and easily transmissiblenew infectious disease of the new millenni-um. From Guangdong province of China,the SARS virus spread along internationaltravel routes to 30 countries and becamedeeply embedded in 6 of them. By 11 July2003, 8427 probable SARS cases had beenreported from 29 countries with 813 deaths[1]. There was widespread public panic,and social stability was jeopardized in someof the hardest hit areas. Economists esti-mated the costs in the Far East alone at US$30 billion. The containment of SARS, how-ever, was achieved through the diligent ap-plication of centuries’ old control
measures. The most pressing questionsnow are whether SARS is seasonal andcould return in winter, and whether theSARS virus could hide in some animal orenvironmental reservoir and resurfacewhen conditions again become favourablefor spread to humans.
Development of the SARSpandemic
The first cases of a life-threatening respira-tory disease of unknown cause are nowknown to have appeared in Guangdongprovince in China in mid-November 2002[2]. But it was only on 11 February 2003,that the World Health Organization (WHO)received the first official report of an out-break of atypical pneumonia in the prov-
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM655

656 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
ince, said to have affected 305 persons andcaused 5 deaths. An infected medical doc-tor, who had treated patients in his home-town in Guangdong province, carried theSARS infection out of China on 21 Febru-ary 2003 to Hong Kong. Guests and visi-tors to the hotel’s ninth floor where hestayed seeded outbreaks in the hospital sys-tems of Hong Kong, Viet Nam and Sin-gapore days later [2].
Dr Carlo Urbani, a WHO epidemiologistwho investigated the Hanoi outbreak, wasthe first to recognize the condition as a dis-tinct entity. The WHO designated the illnessas severe acute respiratory syndrome(SARS) in late February 2003. Consider-able progress was achieved in the followingmonths in understanding its epidemiologyand clinical features. A collaborative net-work of scientists from 11 laboratoriesaround the world worked hard and suc-cessfully identified the etiologic agent as anew species of coronavirus, now calledSARS-CoV [3–5]. WHO confirmed theGuangdong cases to be consistent with thedefinition of SARS after its team was per-mitted on 2 April 2003 to visit the province.
SARS began spreading along air travelroutes, as persons who came in contactwith the earliest cases travelled internation-ally. Hanoi, Hong Kong, Singapore and Tor-onto were the initial “hot zones” for SARS,with rapid increases in the number of cas-es, especially in health care workers (whoexposed themselves without barrier protec-tion) and their close contacts. Subsequentchains of secondary transmission occurredoutside the health care environment.
The new disease showed a clear capac-ity to spread around the world along theroutes of international air travel. The maxi-mum incubation period, estimated at 10days, allows spread via air travel betweenany 2 cities in the world. Mounting evi-dence now points to certain source cases
making a special contribution to the rapidspread of SARS infection. An importedhospitalized SARS case infected health careworkers and other patients; they infectedtheir close contacts and then the diseasemoved into the larger community. Epidemi-ological analyses revealed that the out-breaks of greatest concern wereconcentrated in transportation hubs ordensely populated areas.
Clinical features andmanagement
The Centers for Disease Control and Pre-vention (CDC) defines a “suspected case”of SARS as a person with onset of feverand lower respiratory tract symptoms(temperature > 38 ºC or 100.4 ºF) within 10days of either travel to an area with docu-mented transmission of SARS or closecontact with a person believed to haveSARS [6,7]. If a suspected case developschest radiographic findings of pneumonia,acute respiratory distress syndrome(ARDS) or an unexplained respiratory ill-ness resulting in death, with autopsy find-ings of ARDS without identifiable causethen he/she is reclassified as a “probablecase” of SARS. Laboratory findings fur-ther reclassify suspected and probable cas-es into “laboratory positive”, “laboratorynegative” or “indeterminate”. Householdmembers or persons caring for or sharingpersonal items with a SARS patient areconsidered a “close contact” [6].
The incubation period for the diseasevaried from 2 to 10 days with a mean andmedian of 5 and 6 days respectively [8–12].The classical presentation was of a febrileillness followed in 48–72 hours by drycough, which progressed rapidly to causerespiratory compromise and hypoxaemia.This necessitated ventilator support in one-
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM656

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 657
quarter of the patients and led to mortalityin 20%–45% of cases. The mortality washighest among elderly patients who hadother co-morbid conditions [9]. Exposureto a high viral load was another factor sug-gested to explain the mortality from SARSamong previously healthy young healthcare workers. Interestingly, SARS affectedrelatively few children and appeared milderin this age group [13]. Serological studieshave shown that a symptomatic or sub-clinical infection is uncommon.
None of the therapeutic modalities triedin different parts of the world (broad-spec-trum antibiotics, steroids, ribavirin, inter-feron, and retinovir/lopinavir) have shownconclusive evidence of curative effect onthe disease and no standard regimen hasbeen developed [14]. Current managementof the disease therefore is purely supportiveand efforts should be focused on appropri-ate infection control measures to preventits spread.
Infection control
The epidemiological features of the diseasesuggest that it is transmissible from per-son-to-person through direct contact, largedroplet contact, and through indirect con-tact from fomites and unwashed hands [8].The virus is present in the respiratory se-cretions of infected patients and has alsobeen found in the urine and faeces, raisingthe possibility of faecal–oral spread in somesituations.
It is critical that patients with suspectedSARS be identified promptly to institute theisolation precautions needed to prevent thespread of the disease. Triage screening hasbeen recommended, with a questionnaire toidentify SARS symptoms and history ofpossible exposure. Patients suspected ofhaving SARS need to be immediately sepa-
rated from other patients, given a mask andevaluated carefully by a health care workerwearing a gown, gloves, and N-95 respira-tor, ideally in a negative pressure room.One way of avoiding the spread of diseasein hospitals is to set up a fever triage clinicoutside the hospital emergency room,equipped with all necessary contact pre-caution supplies. These clinics were devel-oped in Taiwan and Toronto during thepeak of the SARS epidemic.
Patients who need to be admitted shouldbe isolated in a negative pressure room in aspecial isolation ward, with restrictions onvisitors and the number of health careworkers involved in the patient care. Medi-cal procedures such as bronchoscopy orrespiratory nebulization of medicationsshould be avoided. If the number of pa-tients exceeds the hospital’s capacity fornegative pressure rooms, then the priorityshould be to keep patients with SARSpneumonia in isolation negative pressurerooms while maintaining other SARS pa-tients in private rooms.
Restricting employees’ access to hospi-tals with SARS patients and identifying theemployees who are taking care of SARSpatients are critical steps to ensuring thathealth care workers do not suffer unpro-tected exposure to SARS patients. Staffshould be actively monitored for any signsand symptoms of SARS, i.e. new onsetupper respiratory tract illness and high tem-perature, for early detection of cases.Health care workers with symptomsshould be immediately confined to theirhomes with daily reporting of symptoms tothe employee health department or infec-tion control personnel at the hospital. Allpersonnel involved in aerosol-generatingprocedures on patients with confirmedSARS should be quarantined for 10 days if
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM657

658 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
adequate precautionary measures were nottaken during the procedure.
Intensive education of health careworkers and family is mandatory. This in-cludes proper infection control precau-tions, which should stress the 2 most likelymodes of transmission of SARS: contactand respiratory droplets. Health care work-ers need personal protective equipment ap-propriate for standard, contact andairborne precautions (i.e. hand hygiene,gown, gloves and N-95 respirator) in addi-tion to eye protection, and use of theseshould be enforced. Household membersshould be educated about the mode ofspread of the disease and proper precau-tions when in contact with the infected per-son by wearing gloves and mask andwashing and disinfecting the hands fre-quently. If they develop symptoms, theyshould call the public health department andarrange to be examined by a qualified per-son. This coordination is crucial to pre-venting the spread of the disease frominfected family members to health careworkers who may be unaware of the riskof SARS contact.
Suspect or possible cases that do notrequire admission to hospital should bemanaged as outpatients. These patientsshould be given clear instructions abouthand hygiene practices with frequent handwashing and wearing a surgical mask tocover the mouth for coughing and sneez-ing. In addition, they should not share eat-ing utensils, towels and bedding withfamily members until washed. These pa-tients should remain at home until 10 daysafter the resolution of fever, if cough andother respiratory symptoms have resolvedor improved. When no respiratory symp-toms or fever are present, family membersneed not be restricted from going out andcarrying out their usual activities includingwork or school.
Global action
WHO issued a global alert on 12 March2003 about cases of severe atypical pneu-monia with unknown etiology that ap-peared to place health workers at high risk.On 15 March 2003, WHO increased thelevel of the global alert to a rare emergencytravel advisory for international travellers,health care professionals, and health au-thorities to the perceived worldwide threatto health from SARS. The Global OutbreakAlert and Response Network (GOARN)teams from WHO provided support at allthe main outbreak sites.
WHO regarded every country with aninternational airport, or bordering an areahaving recent local transmission, as beingat potential risk of an outbreak. The lack ofvaccine and effective treatment forcedhealth authorities to resort to control toolsdating back to the earliest days of empiricalmicrobiology: isolation and quarantine.Countries around the world, guided byWHO, adopted aggressive and unprece-dented measures including travel restric-tions, special entry requirements, screeningprocedures at airports including tempera-ture checks and quarantine. Other controlmeasures included public information andeducation to encourage prompt reportingof symptoms, early identification and isola-tion of patients, vigorous contact tracing,and management of close contacts. Thesesucceeded to a large extent in containingthe disease.
Hospitals, schools, and borders wereclosed, and several governments advisedtheir citizens not to travel to hard-hit areas.Some airlines decided not to carry passen-ger with a fever of 37.5 °C or above on anyof their flights regardless of local govern-ment regulations. Hong Kong adapted anelectronic tracking system used in criminalinvestigations for contact tracing and mon-
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM658

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 659
itoring of compliance with quarantine. Sin-gapore deployed its military forces to assistin contact tracing and to enforce quaran-tines that halted the normal lives of thou-sands of people [7]. The country alsobanned visitors at public hospitals.
On being notified by Singapore, throughWHO, Germany removed a physician fromSingapore (returning from New York afterattending a medical conference who hadsymptoms suggestive of SARS) along withhis 2 accompanying family members fromtheir flight at a stopover in Frankfurt, im-mediately isolated them and placed themunder hospital care. This prompt actionsaved Germany from any further spread.
The WHO announced in late June thatHong Kong and Beijing, the 2 most severelyaffected areas, had interrupted transmis-sion. Toronto and Taiwan followed shortlyafterwards. On 5 July 2003, the WHO de-cided [15], on the basis of country surveil-lance reports, that all known person-to-person transmission of SARS-CoV hadceased and the global SARS outbreak wascontained as it removed Taiwan from its listof areas with recent local transmission ofthe disease. The human chains of SARS vi-rus transmission appeared to have beenbroken everywhere. While the containmentwas a milestone, nations were cautionedagainst becoming complacent, and to main-tain vigilance against the re-emergence ofthe illness that resulted in over 800 deathsworldwide, mostly in China and HongKong, and for which there is no simpletreatment. Some experts say it could beseasonal.
Saudi Arabia
Saudi Arabia had a special reason for con-cern. It has a large expatriate working pop-ulation of 5.3 million persons coming from
various regions of the world. Around 2 mil-lion international pilgrims from over 140countries visit Mecca, the focal point of Is-lam, for the annual hajj pilgrimage; a small-er number visit the country throughout theyear for the individual and shorter umra pil-grimage. The country also receives a largenumber of business travellers the yearround. Were measures not taken immedi-ately to prevent the entry of SARS, it wouldspread quickly and wreak havoc.
Acting promptly, the Saudi Ministry ofHealth, on 10 April 2003, banned the entryof people who had visited any of the 5SARS-stricken South East Asian coun-tries—China, Hong Kong, Taiwan, Sin-gapore and Viet Nam. The ban wasenforced to protect both citizens and expa-triates in the country. Saudi Arabian citizenswere advised against travelling to SARS af-fected countries. The Saudi missions inChina, Singapore, Hong Kong and the Phil-ippines were instructed to stop issuingumra visas indefinitely. Isolation wardswere designated in major hospitals in all re-gions to quarantine all suspected cases ofSARS and admit confirmed SARS cases.The Sahari hospital, a new tuberculosishospital in Riyadh, was the designated hos-pital for the Central region. Mass mediawas used extensively to increase aware-ness of SARS among the population.
Customs, passport and health employ-ees at international airports were ordered toput on masks while dealing with flights ar-riving from countries with cases of SARS.All arriving passengers were required to fillin a mandatory health declaration form forimmigration clearance. At the same time,the health officers at the airport distributeda health alert card with information aboutSARS. The card advised persons to con-tact doctors or designated hospitals if theylater developed symptoms suggestive of
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM659

660 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
SARS, such as high fever (> 38 °C, >100.4 °F), dry cough, shortness of breathor breathing difficulties.
Health personnel checked all incomingpassengers for fever. Within weeks, ther-mal scanners were installed before immi-gration clearance at the 3 internationalairports at Riyadh, Jeddah and Dammam inSaudi Arabia to identify persons with raisedbody temperature. This non-intrusivecheck did not affect passengers, as it didnot delay them. Passengers with tempera-ture below 38 °C were allowed to proceedfor immigration clearance as normal.Those with body temperature above 38 °Cwere taken for a secondary temperaturecheck. Where fever was confirmed, thestaff asked the passenger a series of health-related questions recommended by theWHO: if they have other symptoms ofSARS, such as cough, breathing difficultyor shortness of breath; if they or their fam-ily members have had close contact withany person/s who have been diagnosedwith SARS; and if, in the last 10 days, theyhad travelled to any SARS-affected areas.When SARS was suspected, the passengerwas to be referred to the airport health de-partment for follow-up to be kept underobservation for 10 days. Saudi Arabian cit-izens and expatriate workers returningfrom or transiting through SARS-affectedcountries within the incubation period ofSARS, when cleared by checking for feverand symptoms in the airport, were quaran-tined in their homes; staff from the Minis-try of Health visited them daily to checktheir temperature until the 10th day.
The measures were further stepped upon 28 April 2003. The Saudi Ministry ofHealth set up a special committee in Riyadhwith branches throughout the country tocoordinate efforts to fight the disease. TheMinistry barred entry to nationals of SARS-affected countries as a precautionary mea-
sure. All international airlines were notifiednot to transport any passenger coming tothe Kingdom from the SARS-hit countriesvia a third country unless that passengerhad stayed at least 10 days in that thirdcountry after departing from the lastSARS-stricken station.
The Saudi Arabia and 6 other Gulfcountries met in Qatar in the first week ofMay to coordinate their efforts againstSARS. The countries agreed to informeach other about SARS cases registeredamong their citizens or expatriates.
The ban on passengers coming to SaudiArabia from countries affected by SARSwas lifted on 8 July 2003 following positivereports from WHO that no new cases hadbeen reported for the past 20 days, includ-ing Canada and China. The Saudi Arabianhealth authorities, however, continued tomonitor the country’s entry points in orderto prevent the incursion of any potentialSARS-carrier. For the subsequent hajj (atthe end of January/beginning of February2004), plans were made that all pilgrimscoming from the earlier SARS endemiccountries would not be allowed to enter thecountry unless there was evidence on his/her passport that he/she had been outsideof the country for a minimum of 10 daysimmediately prior to arrival in Saudi Arabia.
Perspective
SARS is a particularly serious threat forpublic health internationally. It also had far-reaching economic and social consequenc-es. Alerted by WHO, all countries withimported cases, with the exception ofprovinces in China, were able through rapidcase detection, immediate isolation, strictinfection control, and vigorous contacttracing to successfully prevent furthertransmission.
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM660

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 661
The high level of mass media attentionfocused on SARS and the concerted workof medical professionals, together withWHO’s pragmatic leadership role, helpedcreate widespread awareness of the severi-ty of the infectious disease threat, and unit-ed the global community. Scientists andclinicians in various countries collaboratedand pooled expertise and resources to com-bat the shared threat. This helped healthauthorities to identify imported SARS casesquickly, prevent a SARS outbreak, and thusavoid the devastating consequences seenelsewhere. The SARS experience in coun-tries like Viet Nam and Singapore showedthat immediate political commitment at thehighest level can prove decisive in combat-ing the spread of the disease.
SARS has posed important challengesfor medical professionals. There are con-cerns over the future evolution of out-breaks as the virus belongs to a familynotorious for its frequent mutations. Ge-nomic studies have shown a remarkablegenetic conservation of the virus; there ap-pears little likelihood of mutation to a be-nign infection with attenuated symptoms.With neither herd immunity nor attenuationof the virus, the next epidemic when it oc-curs will have large-scale outbreaks withsevere symptoms. Efforts are on to devel-
op case investigation, case managementand surveillance protocols for SARS in thepost-outbreak environment.
The major challenges of the disease areits poorly understood epidemiology andpathogenesis, its non-specific and commoninitial symptoms, the limitations in the avail-able diagnostic tests and the vulnerability ofhospital staff, the human resource vital forSARS control [8]. The requirement for in-tensive care for SARS cases is a strain onhospital resources. A rapid diagnostic testneeds to be developed urgently for diagnos-ing SARS within days of onset for differen-tiating it from other atypical pneumonias.Research should be intensified to identifythe possible animal reservoir. A global data-base on SARS has to be developed and anevidence-based approach used for thera-peutic approaches for SARS treatment [2].
The efforts at combating the threat ofSARS have revealed the strengths andweaknesses of national, regional and globalcapacities to respond to infectious diseasethreats. Areas for urgent improvement havenow been highlighted in the health surveil-lance systems of various countries. Theseneed to be addressed so that countries areadequately prepared when the world is nextconfronted with SARS or another infec-tious disease pandemic.
References
1. Cumulative number of reported cases ofsevere acute respiratory syndrome(SARS). Geneva, World Health Organi-zation, 2003 (http://www.who.int/csr/sars/country/2003_07_11/en, accessed12 January 2005).
2. Severe acute respiratory syndrome(SARS): status of the outbreak and les-sons for the immediate future. Geneva,World Health Organization, 2003.
3. Peiris JSM et al. Coronavirus as a pos-sible cause of severe acute respiratorysyndrome. Lancet, 2003, 361:1319–25.
4. Ksiazek TG et al. A novel coronavirusassociated with severe acute respiratorysyndrome. New England journal of medi-cine, 2003, 348:1953–66.
5. Drosten C et al. Identification of a novelcoronavirus in patients with severe
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM661

662 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
acute respiratory syndrome. New En-gland journal of medicine, 2003, 348:1967–76.
6. Centers for Disease Control and Pre-vention. Updated interim surveillancecase definition for severe acute respira-tory syndrome (SARS)—United States,April 29, 2003. Morbidity and mortalityweekly report, 2003, 52(17):391–3.
7. Centers for Disease Control and Pre-vention. Severe acute respiratory syn-drome—Singapore, 2003. Morbidity andmortality weekly report, 2003, 52:405–11.
8. Conly JM, Johnston BL. SARS: a tale oftwo epidemics. Adult infectious diseasenotes, 2003, 14(3) (http://www.pulsus.com/Infdis/14_03/conl_ed.htm, acces-sed 12 January 2005).
9. Peiris JS et al. Clinical progression andviral load in a community outbreak ofcoronavirus-associated SARS pneumo-nia: a prospective study. Lancet, 2003,361:1767–72.
10. Poutanen SM et al. Identification of se-vere acute respiratory syndrome in
Canada. New England journal of medi-cine, 2003, 348:1995–2005.
11. Hsu LY et al. Severe acute respiratorysyndrome (SARS) in Singapore: clinicalfeatures of index patient and initial con-tacts. Emerging infectious diseases,2003, 9(6):713–7.
12. Booth CM et al. Clinical features andshort-term outcomes of 144 patients withSARS in the greater Toronto area. Jour-nal of the American Medical Association,2003, 289:2801–9.
13. Hon KLE et al. Clinical presentationsand outcome of severe acute respiratorysyndrome in children. Lancet, 2003,361:1701–13.
14. So LK et al. Development of a standardtreatment protocol for severe acute res-piratory syndrome. Lancet, 2003, 361:1615–7.
15. SARS outbreak contained worldwide.Press release. Geneva, World Health Or-ganization, 2003 (http://www.who.int/mediacentre/releases/2003/pr56/en ac-cessed 12 January 2005).
24 SARS the new challenge.pmd 8/17/2005, 11:10 AM662

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 663
Review
Prevalence of physical inactivity inSaudi Arabia: a brief reviewH.M. Al-Hazzaa1
1Exercise Physiology Laboratory, King Saud University, Riyadh, Saudi Arabia.Received: 06/06/03; accepted: 23/12/03
SUMMARY Major lifestyle changes in recent years in Saudi Arabia may be leading to physical inactivity anda low level of physical fitness. This paper reviews the current literature about physical inactivity in the SaudiArabian population and discusses its implications for health. Available data from a small number of studiessuggests a high prevalence (43.3%–99.5%) of physical inactivity among Saudi children and adults alike.Furthermore, the proportion of Saudi children and adults who are at risk due to inactivity is much higher thanfor any other coronary heart disease risk factor. It is recommended that a national policy encouraging activityin daily life be established and more studies are carried out to address physical activity patterns withrepresentative samples of the Saudi Arabian population.
Introduction
Until recent times, the physical demands ofdaily life and work in Saudi Arabia weresufficient to maintain a lean body mass andan appropriate level of physical fitnessamong the population. However, during thepast 25 years, rapid developments in stan-dards of living in the Kingdom of SaudiArabia and increased mechanization havetouched all aspects of people’s lives. As aresult, great changes in physical activityand eating habits have occurred in our soci-ety and low levels of physical activity andsedentary living are becoming increasinglyprevalent among the Saudi population [1–9]. Moreover, with massive urbanizationand increased reliance on computer andtelecommunication technology, further re-ductions in physical activity are projectedfor the coming years.
These lifestyle changes that are rapidlyoccurring in Saudi Arabia (as well as in the
rest of the Gulf Cooperation Council coun-tries) have a considerable impact on thehealth of society. In fact, such lifestyletransformation is thought to be responsiblefor the epidemic of non-communicable dis-eases, and their complications, in this partof the world [1,10–16]. In addition, theWorld Health Organization (WHO) has rec-ognized physical inactivity as a major threatto worldwide population health [17]. WHOrecommended some possible goals and pri-ority actions aimed at promoting active liv-ing. Included in these actions is the need toassess the level of physical activity amongvarious segments of the population.
This paper aims to provide a brief over-view of the published data about the level ofphysical activity in the Saudi Arabian popu-lation and discuss the implications of phys-ical inactivity on the health of Saudisociety.
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM663

664 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Prevalence of physicalinactivity among the SaudiArabian population
A MEDLINE search was made for studiespublished from 1990 onwards, using thewords “physical activity and Saudi Arabia”and “physical inactivity and Saudi Arabia”.Seven papers were found, 3 of which wererelevant and were included in the review. Amanual search of the local medical journalswas conducted, which revealed 5 addition-al papers related to physical inactivity inSaudi Arabia.
That little research has been publishedon this important public health issue showsthat research into the epidemiology ofphysical activity in Saudi Arabia and neigh-bouring countries is still in its infancy. Nonationally representative population studyhas been made to describe the patterns ofphysical activity and energy expenditure ofthe Saudi people. The available publisheddata on the physical activity profile of Sau-di people come from studies largely con-ducted in urbanized areas and few of thesehave used large and randomized samples[2–9]. In addition, in some cases, assess-ment of physical activity was not the pri-mary focus of the study [6,8].
Table 1 presents a summary of physicalinactivity prevalence among various seg-ments of the Saudi population [1–9]. Sevenout of the 8 reported studies used question-naires [3–9], while 1 study involving pre-adolescent boys utilized continuous heartrate monitoring [2]. Across all of the stud-ies shown in Table 1, the total rate of inac-tivity ranged from 43.3% to 99.5%. Only 2studies included data for both males andfemales and their findings indicated that fe-males were much less active than males[6,9].
Based on the results of 1 recent studyinvolving adult men living in Riyadh city
and using a fairly large and random sample,there appears to be a curvilinear relation-ship between inactivity prevalence and age[5]. As shown in Figure 1, the proportionof inactive men was highest during themiddle-age years (30–49 years). In thesame study, physical inactivity was shownto be higher among the less educated Saudimales [5]. Furthermore, the most importantreasons for being physically inactiveamong Saudi males were time constraintsand lack of facilities, as reported by morethan 70% of the respondents [5]. In anoth-er study [9], the prevalence of physical in-activity in males increased from earlyadulthood (16–30 years) to reach its peakat a later age (46–60 years).
Overall, what is striking from the find-ings of these studies is that the prevalenceof inactivity among the Saudi populationseems to be higher than rates reported inmany industrialized countries of Europeand America [18–22]. However, accordingto the WHO report, 60% of the world pop-ulation is sedentary or not active enough togain health benefits [17].
As shown also in Table 1, the percent-age of Saudi boys who do not take moder-ate daily physical activity, i.e activity thatraises the heart rate to above 139 beats perminute (bpm), for 30 minutes or more wasreported to be 57.1% [1,2]. Such a level ofmoderate intensity physical activity hasbeen recommended as a minimum level ofphysical activity for children and adoles-cents [18,23–26]. In addition, Saudi boysspend, on average, limited time on activitiesthat raise the heart rate above 159 bpm.This level of vigorous activity is considerednecessary for optimal cardiovascular healthand fitness in children and adolescents [24–26]. In addition, according to a recent sur-vey conducted on a sample of adolescentboys in Riyadh city, the rate of inactive ad-olescents (exercising for 1 day or less per
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM664

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 665
Tabl
e 1
Ph
ysic
al a
ctiv
ity
rate
s in
the
Sau
di A
rab
ian
po
pu
lati
on
Po
pu
lati
on
Reg
ion
[ref
eren
ce]
Ass
essm
ent
No
. of
Ag
e (y
ears
)L
evel
of p
hys
ical
act
ivit
ym
eth
od
sub
ject
sM
ean
(SD
)R
ang
eN
ever
Irre
gu
lar
Tota
lac
tive
acti
vity
inac
tive
a
%%
%
Chi
ldre
nP
re-a
dole
scen
tR
iyad
h ci
ty [1
,2]
Con
tinuo
us h
eart
929.
6 (1
.5)
7–12
––
57.1
b
boys
rate
mon
itorin
g
Ado
lesc
ents
Ado
lesc
ent b
oys
Riy
adh
city
[3]
Que
stio
nnai
rec
894
15.7
(1.8
)12
–20
––
48.4
Adu
ltsC
olle
ge m
enR
iyad
h ci
ty [4
]Q
uest
ionn
aire
362
21.9
(2.1
)17
–30
45.8
32.4
78.2
Adu
lt m
enR
iyad
h ci
ty [5
]Q
uest
ionn
aire
1333
41.1
(9.7
)19
–68
53.4
27.5
80.9
Prim
ary
care
patie
nts
Eas
tern
pro
vinc
e [6
]Q
uest
ionn
aire
227
Mal
e41
.5 (1
1.2)
43.3
––
Fem
ale
32.5
(11.
4)84
.7–
–P
rimar
y ca
reph
ysic
ians
Riy
adh
city
[7]
9842
.0 (6
.5)
26–6
021
.555
.076
.5A
ndro
logy
and
urol
ogy
patie
nts
Jedd
ah c
ity [8
]Q
uest
ionn
aire
388
43.2
(12.
5)20
–86
82.0
––
Low
land
ers
and
high
land
ers
Asi
r pro
vinc
e [9
]Q
uest
ionn
aire
d90
5M
ale
16–6
027
.531
.959
.4Fe
mal
e16
–60
88.6
11.3
99.5
a Tot
al r
epre
sent
s bo
th n
ever
exe
rcis
e an
d irr
egul
ar p
hysi
cal
activ
ity.
b Per
cent
age
of b
oys
not
taki
ng e
xerc
ise
suffi
cien
t to
rai
se h
eart
rat
e >
139
bpm
for
at
leas
t 30
min
utes
per
day
.c F
requ
ency
of
phys
ical
act
ivity
≤ 1
tim
e/w
eek.
d Usi
ng L
ipid
Res
earc
h C
linic
Que
stio
nnai
re (
inac
tive
mea
ns t
hose
rep
ortin
g no
str
enuo
us e
xerc
ise
for
≥ 3
times
per
wee
k).
SD
= s
tand
ard
devi
atio
n.
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM665

666 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
week) was approximate 50% [3]. The ma-jor determinants of physical activity in Sau-di children and adolescents appear to becardiorespiratory fitness, obesity, the quali-ty of the physical education programmes,TV viewing and parental influence [27].From a comparative point of view, it seemsthat both levels of moderate (heart rate >139 bpm) and vigorous (> 159 bpm) phys-ical activity of Saudi boys are considerablylower than those levels reported for chil-dren from other countries [19,28,29].
Health implications of physicalinactivity in Saudi Arabiansociety
It is now well recognized that physical in-activity and increased sedentary habits rep-resent a risk factor for a number of chronicdiseases including coronary heart disease(CHD) and obesity [30,31]. On the otherhand, regular physical activity has beenshown to reduce the risk of both cardio-vascular disease and all-cause mortality[18,23,30,32]. Furthermore, research onphysical activity epidemiology indicatesthat inactivity appears to be far more im-
portant risk factor than was previously es-timated [33,34]. The reason is that thereare higher proportions of the populationwho are inactive and at risk for CHD thanthose who are at risk for any of the otherCHD risk factors [33,34]. Figure 2 illus-trates this point using data from a recentphysical activity study conducted on Saudimales [5]. The proportion of Saudi adultswho are at risk due to inactivity is muchhigher than those at risk due to any of theother CHD risk factors, including hyper-tension [13], hypercholesterolaemia [14],obesity [15] and cigarette smoking [35].Therefore, health promotion strategies aim-ing at decreasing the proportion of inactiveSaudi adults should be a priority publichealth concern.
The proportion of Saudi boys who areat risk of CHD due to inactivity relative toother risk factors is similar to that of Saudiadults. Figure 3 clearly shows that the per-centage of Saudi boys who are physicallyinactive is twice the rate of those with hy-perlipidaemia. Diseases such as CHD andobesity, for which inactivity is a likely riskfactor, have their origin in childhood[36,37]. Moreover, CHD risk factors wereshown to track from childhood to adult-
Figure 1 Prevalence of physical inactivity among Saudi Arabian males by age [5]
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM666

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 667
Figure 2 Risk factors for coronary heart disease among Saudi Arabian males: proportions withphysical inactivity [5], high systolic (SBP) and high diastolic (DBP) blood pressure [13], hightotal cholesterol level (TC) [14], obesity [15] and cigarette smoking [35]
Figure 3 Risk factors for coronary heart disease among Saudi Arabian boys: proportions withphysical inactivity [1,2], low high-density lipoprotein cholesterol level (HDL-C), high bloodpressure (BP), low cardiorespiratory fitness (unfit), obesity (fat > 25% body mass), high low-density lipoprotein cholesterol level (LDL-C), high total cholesterol level (TC) and hightriglycerides level (TG) [10]
Inactivity
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM667

668 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
hood [38]. Thus, prevention of lifestyle-re-lated disease at an early age is an importantpublic health priority, especially consider-ing the fact that children and adolescentsaccount for more than 50% of the Saudipopulation. Indeed, a recent statementfrom the American Heart Association’sCouncil on Cardiovascular Disease in theYoung has recommended that physiciansshould incorporate physical activity coun-selling into medical practice as a way ofpromoting physical activity among childrenand adolescents [39].
Conclusion andRecommendations
From this brief review of the current levelof physical activity in Saudi Arabia, it canbe concluded that the prevalence of physi-
cal inactivity among Saudi children, adoles-cents and adults is high. This may be large-ly the result of the recent dramatic changesin the people’s lifestyle. Moreover, the pro-portion of Saudi children and adults whoare at-risk due to inactivity is much higherthan for any of the other CHD risk factors.It is recommended, therefore, that a nation-al policy encouraging active living and dis-couraging inactivity be established. Suchan approach has been recommended previ-ously [12,27]. Health care providers havean important role in promoting physical ac-tivity and fitness among all Saudi people.Finally, national studies addressing physicalactivity patterns with representative sam-ples of the Saudi population are urgentlyneeded. Such surveillance will provide in-valuable information for public health au-thorities and policy-makers.
References
1. Al-Hazzaa HM. Physical activity, fitnessand fatness among Saudi children andadolescents: implications for cardiovas-cular health. Saudi medical journal,2002, 23:144–50.
2. Al-Hazzaa HM, Sulaiman MA. Maximaloxygen uptake and daily physical activ-ity in 7-to-12 year-old boys. Pediatric ex-ercise science, 1993, 5:357–66.
3. Al-Rukban MO. Obesity among Saudimale adolescents in Riyadh, SaudiArabia. Saudi medical journal, 2003,24:27–33.
4. Al-Hazzaa HM. Physical activity profile ofcollege male subjects. King Saud Uni-versity journal, 1990, 2:383–96 [in Ara-bic].
5. Al-Refaee S, Al-Hazzaa HM. Physicalactivity profile of Saudi males: implica-tions for health. Saudi medical journal,2001, 22:784–9.
6. Taha AZ, Bella H. Heart disease risk fac-tors: prevalence and knowledge in a pri-mary care setting, Saudi Arabia. EastMediterranean health journal, 1998,4:293–300.
7. Al-Shahri M, Al-Almaei S. Promotion ofphysical exercise by primary health carephysicians in Riyadh city. Saudi medicaljournal, 1998, 19:67–9.
8. Al-Helali NS, Abolfotouh MA, GhanemHM. Pattern of erectile dysfunction inJeddah city. Saudi medical journal,2001, 22:34–8.
9. Khalid M. The association betweenstrenuous physical activity and obesityin high and low altitude populations insouthern Saudi Arabia. Internationaljournal of obesity and related metabolicdisorders, 1995, 19:776–80.
10. Al-Hazzaa H et al. Prevalence of coro-nary artery disease risk factors in Saudi
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM668

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 669
children. Journal of the Saudi Heart As-sociation, 1993, 5:126–33.
11. Al-Hazzaa H et al. Cardiorespiratory fit-ness, physical activity patterns, and se-lected coronary artery disease riskfactors in preadolescent boys. Interna-tional journal of sports medicine, 1994,15:267–72.
12. Alwan A. Noncommunicable diseases: amajor challenge to public health in theRegion. Eastern Mediterranean healthjournal, 1997, 3:6–16.
13. Al-Nozha M, Ali M, Osman A. Arterial hy-pertension in Saudi Arabia. Annals ofSaudi medicine, 1997, 17:170–4.
14. Al-Nuaim A et al. Prevalence of hyperc-holesterolemia in Saudi Arabia, epide-miological study. International journal ofcardiology, 1996, 19:41–9.
15. Al-Nuaim AR et al. High prevalence ofoverweight and obesity in Saudi Arabia.International journal of obesity andrelated metabolic disorders, 1996, 20:547–52.
16. El-Hazmi M et al. Diabetes mellitus andimpaired glucose tolerance in SaudiArabia. Annals of Saudi medicine, 1996,4:381–5.
17. Annual global Move for Health initiative:a concept paper. Geneva, World HealthOrganization, 2003 (WHO/NMH/PAH/03.1)
18. US Department of Health and HumanServices. Physical activity and health: areport of the Surgeon General. Atlanta,Georgia, Centers for Disease Controland Prevention (CDC), National Cen-ters for Chronic Disease Preventionand Health Promotion, 1996 (http://www.cdc.gov/nccdphp/sgr/sgr.htm, ac-cessed 26 December 2004).
19. US Department of Health and HumanServices. Healthy people 2010: under-standing and improving health, 2nd
ed. Washington, DC, US GovernmentPrinting Office, 2000 (http://www.h e a l t h y p e o p l e . g o v / D o c u m e n t /tableofcontents.htm, accessed 26 De-cember 2004).
20. Crespo CJ et al. Prevalence of physicalinactivity and its relation to social class inUS adults: results from the Third NationalHealth and Nutrition Examination Sur-vey, 1988–1994. Medicine and sciencein sports and exercise, 1999, 31:1821–7.
21. Caspersen CJ, Merritt RK. Physical ac-tivity trends among 26 states, 1986–1990. Medicine and science in sportsand exercise, 1995, 27:713–20.
22. Caspersen C, Merritt R, Stephens T. In-ternational physical activity patterns:a methodological perspective. In: Dish-man R, ed. Advances in exercise ad-herence. Champaign, Illinois, HumanKinetics, 1994:73–110.
23. National Institutes of Health. NIH con-sensus development panel on physicalactivity and cardiovascular health. Jour-nal of the American Medical Association,1996, 276:241–6.
24. American College of Sports Medicine.ACSM’s guidelines for exercise testingand prescription. Baltimore, Williamsand Wilkins, 2000.
25. Cavill N, Biddle S, Sallis J. Health en-hancing physical activity for youngpeople: statement of the United Kingdomexpert consensus conference. Pediatricexercise science, 2001, 13:12–25.
26. Sallis J, Patrick K. Physical activityguidelines for adolescents: consensusstatement. Pediatric exercise science,1994, 6:302–14.
27. Al-Hazzaa H. Patterns of physical activityamong Saudi children, adolescents andadults with special reference to health.In: Musaiger A, Miladi S, eds. Nutrition
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM669

670 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
and physical activity in the Arab coun-tries of the Near East. Manama, BahrainCentre for Studies and Research, 2000:109–27.
28. Armstrong N, Bray S. Physical activitypatterns defined by continuous heartrate monitoring. Archives of disease inchildhood, 1991, 66:245–7.
29. Sallo M, Silla R. Physical activity withmoderate to vigorous intensity in pre-school and first grade schoolchildren.Pediatric exercise science, 1997, 9:44–54.
30. Leon A, ed. Physical activity and cardio-vascular health. A national consensus.Champaign, Illinois, Human Kinetics,1997.
31. Bijnen FC, Caspersen CJ, Mostard WL.Physical inactivity as a risk factor forcoronary heart disease: a WHO and In-ternational Society and Federation ofCardiology position statement. Bulletinof the World Health Organization, 1994,72(1):1–4.
32. Blair SN et al. Physical fitness and all-cause mortality: a prospective study ofhealthy men and women. Journal of theAmerican Medical Association, 1989,262:2395–401.
33. Caspersen CJ. Physical activity epide-miology: concepts, methods and appli-cations to exercise science. Exerciseand sport sciences reviews, 1989, 17:423–73.
34. Powell K. Population attributable risk ofphysical inactivity. In: Leon A, ed. Physi-cal activity and cardiovascular health. Anational consensus. Champaign, Illinois:Human Kinetics, 1997:40–7.
35. Jarallah JS et al. Prevalence and deter-minants of smoking in three regions ofSaudi Arabia. Tobacco control, 1999,8:53–6.
36. Berenson G et al. Association betweenmultiple cardiovascular risk factors andatherosclerosis in children and youngadults. The Bogalusa Heart Study. NewEngland journal of medicine, 1998,338(23):1650–6.
37. McGill HC Jr et al. Association of coro-nary heart disease risk factors withmicroscopic qualities of coronary ath-erosclerosis in youth. Circulation, 2000,102:374–9.
38. Webber LS et al. Tracking of serum lipidsand lipoproteins from childhood to adult-hood. The Bogalusa Heart Study. Ameri-can journal of epidemiology, 1991, 133:884–99.
39. Williams C et al. Cardiovascular healthin childhood. A statement for health pro-fessionals from the committee on athero-sclerosis, hypertension, and obesity inthe young (AHOY) of the council on car-diovascular disease in the young, Ameri-can Heart Association. Circulation,2002, 106:143–60.
25 Prevalence of physical.pmd 8/17/2005, 11:10 AM670

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 671
Report
Frequency of the CCR5-delta 32chemokine receptor gene mutation inthe Lebanese populationW. Karam,1 R. Jurjus,2 N. Khoury,3 H. Khansa,3 C. Assad,4 P. Zalloua5 and A. Jurjus2
1Faculty of Public Health, Balamand University, Beirut, Lebanon.2Faculty of Medicine, American University of Beirut, Beirut, Lebanon.3Faculty of Public Health, Lebanese University, Beirut, Lebanon.4Division of Medical Sciences and Public Health, Lebanese Council for Scientific Research, Beirut,Lebanon.5Chronic Care Centre, Hazmieh, Lebanon.Received: 14/05/03; accepted: 14/09/03
SUMMARY A direct correlation between HIV infection and mutation in the chemokine receptor (CCR5) genehas been established. However, such correlation has never been investigated in Lebanon. We report thefrequency of the CCR5-delta 32 mutation in a random sample of 209 healthy, HIV-1 seronegative Lebaneseaged 19–68. Overall, 4.8% were heterozygous for the mutation. Homozygosity was absent from our sample.The frequency for the CCR5-delta 32 allele was 2.5%. Distribution of the mutation was unaffected by sex,age, religion or educational level. The frequency in the Lebanese population is consistent with that in the originof the mutation in northern Europe. This could be attributed to a gene flow into the Middle East from northernEurope.
Introduction
According to a World Health Organizationreport, 42 million people were living withHIV/AIDS worldwide in 2002; 92% wereadults, 46% women, and 8% children un-der the age of 15. This resulted in 3.1 mil-lion deaths in 2002. In North Africa and theMiddle East alone, 550 000 people are cur-rently living with HIV/AIDS [1]. In Leba-non, the cumulative number of reportedHIV/AIDS cases reached 987 by the end of2002, while the estimated number could beas much as 3000 [2].
It has been established that infection byHIV-1 is influenced by a mutation in thechemokine receptor (CCR5) gene [3,4].The product of the CCR5 gene encodes a
CC-type seven-transmembrane G-protein-coupled chemokine receptor that bindsRANTES, MIP-1alpha and MIP-1beta, andhas been shown to mediate entry of M-tropic HIV-1 strains into target cells [5–7].CCR5 also serves as an entry co-receptorfor primary human immunodeficiency vi-rus strains that infect monocytes and mac-rophages [7–9]. The CCR5 gene is locatedon chromosome 3p21.3. Individuals resis-tant to repeated exposure to the virus havebeen shown to be homozygous for a 32 bpdeletion in the CCR5 gene [5,6]. Heterozy-gosity for the mutation is associated with aslower progression to AIDS following HIV-1 infection with a typical delay of 2–4 years[4,6,10]. The 32 bp deletion in the genecauses a frame shift at amino acid 185,
26 Frequency of the CCR5-delta.pmd 8/17/2005, 11:10 AM671

672 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
which results in a stop codon and prema-ture truncation within the third extracellulardomain. Analysis of the infectability of cellsof 3 different genotypes by Liu et al. dem-onstrated that HIV-1 replicated in wild-typehomozygous cells but failed to replicate inhomozygous delta-32 cells, whereas repli-cation of the virus in cells heterozygous forthe mutation proceeded at an intermediaterate [5].
In this study we report the frequency ofthe CCR5-delta 32 mutation in the Lebanesepopulation.
Methods
The participants were selected from Leba-nese adults attending the blood bank of amajor teaching hospital in Beirut, Lebanonover a 6-month period between July andDecember 2001. Sample size was 220.Participants were healthy, HIV-1 seronega-tive, of both sexes, and ages ranged from19 to 68 years. Palestinian, Syrian, and Ar-menian donors were not included in thestudy. None of the blood samples collectedtested positive for HIV. In addition, the do-nated blood was further screened for anti-body titres and potential pathogens beforebeing considered suitable for donation. Ev-ery third qualified donor was included inthe study; people who donated blood atnight or on Sundays, however, were ex-cluded. The donors were not inconve-nienced in any way. An anonymousquestionnaire was completed for each par-ticipant. The questionnaire included ques-tions relating to marital status, number ofsex partners, practice of safe sex, druguse, history of blood or blood productstransfusion, and whether the participanthad previously been tested for HIV. Institu-tional ethical clearance and informed con-sent of the blood donors were obtained. Wefollowed the Helsinki Declaration (1964,
amended in 1975 and 1983) of the WorldMedical Association.
About 2 mL of donated peripheralvenous blood was collected from each par-ticipant. The GFX genomic blood DNA pu-rification kit (Amersham PharmaciaBiotech Europe GmbH, Freiburg, Germa-ny) was used to extract genomic DNAfrom white blood cells following the lysisof red blood cells. DNA was eluted in100 µL molecular biology grade water andstored at –20 °C. DNA concentrationswere determined spectrophotometrically.
Polymerase chain reaction was per-formed following the methods of Martin-son et al. [11]. Briefly, 100 ng of genomicDNA was denatured at 94 °C for 10 min-utes, following which it was subjected to30 cycles of denaturation, annealing andextension. The last cycle was followed byan incubation at 72 °C for 10 minutes. Thereaction mixture of 50 µL contained,50 mmol KCl, 10 mmol Tris-HCl, pH 8.3,800 µmol dNTPs, 100 µg/mL gelatin, 10pmoles of each of the CCR5-specific for-ward and reverse primers, and 1.5 units ofTaq polymerase enzyme (GibcoBRL LifeTechnologies GmbH, Karlsruhe, Germa-ny). Electrophoresis was performed inTris-Borate EDTA running buffer and poly-merase chain reaction products were de-tected in 2% agarose containing 1 µg/mLethidium bromide, and visualized by transil-lumination with ultraviolet light [11].
Cross contamination was avoided byusing pipette-tips fitted with aerosol barrierfilters, and frequent decontamination ofwork surfaces with short ultra-violet lightirradiation and diluted bleach. Carry-overcontamination was prevented by physicallyseparating the extraction, amplification anddetection areas.
Both deleted and normal PCR productswere extracted from agarose gels using thePCR product clean-up kit from (Roche
26 Frequency of the CCR5-delta.pmd 8/17/2005, 11:10 AM672

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 673
Molecular Biochemicals GmbH, Man-nheim, Germany) and dideoxyterminationcycle sequencing (Applied Biosystems,Foster City, California,) of normal and de-leted polymerase chain reaction productswas performed to confirm the identities ofamplicons and to determine the exact na-ture and location of the deletion along theCCR5 gene.
Eleven samples did not yield amplifiableDNA, consequently, the effective numberof donors included in the study was 209.
Statistical analysis was performed andindividual parameters were tested for sig-nificance by analysis of variance.
Results
Overall, 4.8% of the people we studiedwere heterozygous for the mutation; ho-mozygosity was not found. The frequencyfor the CCR5-delta 32 allele was 2.5%.Distribution of the mutation was unaffect-ed by sex (P = 0.21), age (P = 0.41), oreducation level (P = 0.62), and was similaramong the religious groups that we exa-mined (P = 0.43) (Table 1). The sequen-cing of the polymerase chain reactionproducts purified from agarose gels con-firmed their identity with that of the CCR5gene (GenBank X91492). Also, the natureand location of the deletion identified by se-quencing of the deleted polymerase chainreaction products were identical to that re-ported by Liu et al. [5].
Discussion
A north to south gradient in the delta 32 al-lele frequency has been reported acrossEurope, with the highest allele frequenciesin the Finnish and other populations livingaround the Baltic Sea (10%–20% heterozy-gous; 1% homozygous), and the lowest in
Sardinia and Greece, where the frequencydrops to almost zero [11–13]. The mutationis also seen at very low frequencies in pop-ulations from Saudi Arabia, Syrian ArabRepublic, Islamic Republic of Iran, Tuni-sia, Morocco, Cyprus (Greek), India, Paki-stan and Asia. It is virtually absent in nativepopulations from sub-Saharan Africa andOceania [11–15]. Based on the demograph-ic distribution, it is believed that the muta-tion arose in northern Europe in response toselective pressures such an infection epi-demic. Our results are consistent with re-ports in the medical literature: we detectedthe mutated allele in our study population at
Table 1 Distribution of CCR5 genotype inhealthy HIV-1 seronegative Lebanese adults(n = 209)
Variable No. with No. with P-CCR5/CCR5 CCR5/CCR5- valuea
delta 32
Total 199 (95.2%) 10 (4.8%)
SexM 112 6 0.21F 87 4
Age (years)Range 19–68 20–60 0.41≤ 40 125 5> 40 32 3Unknown 42 2
EthnicityChristian 119 8 0.43Muslim 40 2Unknown 40 0
EducationUniversity 84 5 0.62High school 63 3Technical 31 2Other 21 0
aAll P-values were > 0.05, indicating no significanteffect of age, sex, education or ethinicity in thiscase on the mutation frequency.
26 Frequency of the CCR5-delta.pmd 8/17/2005, 11:10 AM673

674 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
a frequency of 2.5%, which is close towhat is being reported in the Syrian ArabRepublic (1.4%), Islamic Republic of Iran(2.4%), Tunisia (1%), Morocco (1.5%)and Cyprus (2.8%) [15].
The frequency in the Lebanese popula-tion is consistent with the location of theorigin of the mutation in northern Europe.This could be attributed to a gene flow intothe Middle East from northern Europe. Inaddition, frequencies of the deletion gradu-ally decrease as the distance from Europebecomes greater and it is virtually absent inAsia, the Far East, Oceania and South Afri-ca. We therefore propose that, in addition
to the gradient seen in Europe, a gradientoutside Europe also exists for the mutationacross the Middle East region and into Asia,the Far East and Oceania and across Eu-rope into Africa. This is in accord with asingle point of origin for the mutation locat-ed in northern Europe, where the highestfrequencies for the deletion have been re-ported.
Acknowledgement
The authors would like to acknowledge thesupport of the Lebanese Scientific Re-search Council for funding the study.
References
1. AIDS epidemic update. Geneva, WorldHealth Organization, 2002.
2. National AIDS program annual report2002. Beirut, Lebanon, Ministry of PublicHealth, 2002.
3. Huang Y et al. The role of a mutant CCR5allele in HIV-1 transmission and diseaseprogression. Nature medicine, 1996,2(11):1240–3.
4. Fowke KR et al. Resistance to HIV-1 in-fection among persistently seronegativeprostitutes in Nairobi, Kenya. Lancet,1996, 348(9038):1347–51.
5. Liu R et al. Homozygous defect in HIV-1coreceptor accounts for resistance ofsome multiply-exposed individuals toHIV-1 infection. Cell, 1996, 86(3):367–77.
6. Dean M et al. Genetic restriction of HIV-1infection and progression to AIDS bya deletion allele of the CKR5 structuralgene. Hemophilia growth and develop-ment study, Multicenter AIDS cohortstudy, Multicenter hemophilia cohortstudy, San Francisco City cohort, ALIVEstudy. Science, 1996, 274(5290):1856–62.
7. Dragic T et al. HIV-1 entry into CD4+ cellsis mediated by the chemokine receptorCC-CKR-5. Nature, 1996, 381(6584):667–73.
8. Alkhatib G et al. CC CKR5: a RANTES,MIP-1alpha, MIP-1beta receptor as a fu-sion cofactor for macrophage-tropic HIV-1. Science, 1996, 272(5270):1955–8.
9. Zhao SF et al. Chemokine receptors andthe molecular basis for human immuno-deficiency virus type 1 entry into periph-eral hematopoietic stem cells and theirprogeny. Journal of infectious diseases,1998, 178(6):1623–34.
10. Michael NL et al. The role of viral pheno-type and CCR-5 gene defects in HIV-1transmission and disease progression.Nature medicine, 1997, 3(3):338–40.
11. Martinson JJ et al. Global distribution ofthe CCR5 gene 32-basepair deletion.Nature genetics, 1997, 16(1):100–3.
12. Libert F et al. The deltaccr5 mutation con-ferring protection against HIV-1 in Cau-casian populations has a single andrecent origin in Northeastern Europe.Human molecular genetics, 1998, 7(3):399–406.
26 Frequency of the CCR5-delta.pmd 8/17/2005, 11:10 AM674

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 675
13. Magierowska M et al. Distribution of theCCR5 gene 32 base pair deletion andSDF1-3´ A variant in healthy individualsfrom different populations. Immunoge-netics, 1998, 48(6):417–9.
14. Szalai C et al. High frequency of theCCR5 deletion allele in Gypsies livingin Hungary. Immunology letters, 1998,63(1):57–8.
15. Lu Y et al. Genotype and allele frequencyof a 32-base pair deletion mutation in theCCR5 gene in various ethnic groups:absence of mutation among Asians andPacific Islanders. International journal ofinfectious diseases, 1999, 3(4):186–91.
Genetics in developing countries
Low- to middle-income countries vary in their capacities in medicalgenetics. Some may not have the resources to set up appropriategenetic services. Others provide genetic services but need assist-ance to improve equity of access to these services. The WorldHealth Organization is supporting country capacity building by con-structing educational modules and pilot studies to develop nationalcommunity genetics, including the ethical, legal and societal impli-cations (ELSI).
Source: WHO Fact sheet: genetics and healthAvailable at: http://www.who.int/genomics/en/E_hgn-_final.pdf
26 Frequency of the CCR5-delta.pmd 8/17/2005, 11:10 AM675

676 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Report
Evaluation of cervical smears at KingHussein Medical Centre, Jordan, overthree and a half yearsS.R. Malkawi,1 R.M. Abu Hazeem,1 B.M. Hajjat1 and F.K. Hajjiri1
1Princess Iman Research and Laboratory Sciences Centre, King Hussein Medical Centre, Amman,Jordan.Received: 21/05/03; accepted: 03/08/03
SUMMARY Cervical smears taken from women referred for a check-up or with vaginal itching/dischargeover a period of 3.5 years were reviewed at the King Hussein Medical Centre, Jordan. All smears were fixedwith 96% alcohol, stained with Papanicolaou stain and screened microscopically. Of the smears from 1176women aged 18–70 years, 4.5% were classified as inadequate, 7.7% were normal and 79.9% showed non-specific inflammation. Abnormal vaginal flora was found in 4.8% of cases, Candida albicans in 1.2%, Tri-chomonas vaginalis in 0.9% and actinomycosis in 1 case. Dysphasic changes were rare: 9 cases (0.8%)were classified as atypical squamous cells of undetermined significance (ASCUS) and 2 cases (0.2%) werelow-grade squamous intraepithelial lesion (LSIL). No cases of human papillomavirus infection (HPV) orcervical carcinoma were found.
Introduction
The cervical smear (Papanicolaou, Papsmear) is a routine screening test used forthe detection of early cervical abnormali-ties, namely precancerous dysplasticchanges of the uterine cervix [1], togetherwith viral, bacterial, and fungal infectionsof the cervix and vagina. Cervical screen-ing is a relatively simple, low cost and non-invasive method. Regular screening forcervical cancer reduces both the mortalityand incidence of cervical carcinoma. Cer-vical neoplasia typically develops into inva-sive cancer over a 10-year period [3–6] andapparent cases of rapidly progressive cer-vical cancer are likely to be among womenwho have escaped screening and properfollow-up. Annual screening reduces theprobability of developing invasive carcino-ma by over 95% [2].
There is also epidemiological and exper-imental evidence that Pap smears are bene-ficial in detecting infections that are riskfactors associated with cervical cancer,such as human papillomavirus (HPV) [7,8].Societies where sexual activity starts at ayoung age and where multiple partners arecommon are at a higher risk of exposure toHPV than in conservative societies such asJordan. HPV is a virus that infects repro-ducing cells, thus enhancing proliferationof the cell population; this increases therisk of transformation to high-grade lesionsor carcinomas [9–11]. A cervical smearalso detects vaginal infections such as Can-dida albicans, where patients present withphysical discomfort, excess vaginal dis-charge, itching and other complaints.
In the absence of a national cervicalscreening programme in Jordan, the aim of
27 Evaluation of cervical smears.pmd 8/17/2005, 11:10 AM676

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 677
this study was to evaluate the prevalence ofcervical lesions in cervical smears analysedat the Princess Iman Research and Labora-tory Sciences Centre, Jordan.
Methods
Over a period of 3.5 years from August1999 to February 2003, a retrospective re-view was made of records of 1176 cervicalsmears analysed at the Princess Iman Re-search and Laboratory Sciences Centre atKing Hussein Medical Centre in Jordan. Pa-tients were those who had been referredfrom all military hospitals in Jordan to thegynaecology clinic at the Centre with com-plaints of vaginal itching or discharge, andthose who came for a first-time or follow-up cervical smear.
Cervical smears were taken by gynae-cologists at the clinics using a specu-lum and brush; endocervical cells weresmeared onto slides with direct fixation by96% ethanol.
Smears were sent to the laboratoryfixed in 96% ethyl alcohol. All smears werestained with Papanicolaou stain and stainedslides were screened microscopically bytrained staff comprising 2 cytotechnolo-gists and 1 pathologist. The adequacy ofsmears was determined by the presence ofa good number of ecto- and endocervicalcomponents, no air dryness and no arte-facts. All smears were routinely stained byPapanicolaou stain using a Leica Autostain-er programmed for the purpose.
Slides were classified into 5 main cate-gories: specific cervicitis, non-specific cer-vicitis, normal, cervical dysplasia, cervicalcarcinoma and inadequate.
Results
Of the cervical smears from 1176 womenaged from 18–70 years, 91 (7.7%) were
normal, while 53 (4.5%) smears were clas-sified as inadequate (Table 1).
Of the remaining smears, 940 (79.9%)showed non-specific inflammation, i.e. aninflammatory background with no evi-dence of viral changes or bacteria.
Specific inflammation was found in 81cases: 56 (4.8%) cases showed abnormalvaginal flora, including Gardnerella vagi-nalis, 14 cases had Candida albicans(1.2%), 10 cases (0.9%) had Trichomonasvaginalis and 1 case had actinomycosis(0.1%). No cases of HPV infection werefound.
Low-grade cervical abnormalities wereseen in 11 cases: 9 cases (0.8%) were clas-sified as atypical squamous cells of unde-termined significance (ASCUS) and 2cases (0.2%) were low-grade squamousintraepithelial lesion (LSIL). No malignantcases were reported within this study peri-
Table 1 Classification of 1176 cervical smears
Category No. of %smears
Inadequate 53 4.5
Normal 91 7.7
Non-specific cervicitis 940 79.9
Specific cervicitisAbnormal vaginal flora,including Gardnerella vaginalis 56 4.8Candida albicans 14 1.2Trichomonas vaginalis 10 0.9Actinomycosis 1 0.1
Cervical dysplasiaASCUS 9 0.8LSIL 2 0.2
Cervical carcinoma 0 0
Total 1176 100.0
ASCUS = atypical squamous cells of undeterminedsignificance.LSIL = low-grade squamous intraepithelial lesions.
27 Evaluation of cervical smears.pmd 8/17/2005, 11:10 AM677

678 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
od. None of the categories were clusteredin any specific age group.
Discussion
The cervical smear is a widely used routinetest with many benefits, especially in de-tecting early cervical changes that can betreated to limit dysplastic processes devel-oping into cancer. Of the cervical smeartests on 1176 women in our hospital,79.9% showed non-specific inflammation,namely unexplained inflammatory back-ground, thus showing no bacterial or viralfeatures. The remaining cases of inflamma-tion showed 4.8% cases of specific inflam-mation, 1.2% candida infections, 0.9%trichomonal infections and 1 case of acti-nomycosis.
The incidence of dysplastic changes inour study (1.0%) was low compared withother studies performed in industrializedcountries [1,13,14] and we found no casesof cervical carcinoma. This contrasts, for
example, with a study in New England inthe United States of America (USA) whichfound that 11.8% of women aged 20–29years and 8.4% of those over 30 years hadinfectious processes and 3.5% and 1.3%respectively showed squamous intraepithe-lial lesions (SIL) [15].
No cases of HPV infection were re-corded in our hospital during this studyperiod. Statistics from the Centers for Dis-ease Control and Prevention’s NationalCenter for HIV, STD, and TB Preventionshowed that 5.5 million people in the USAbecame infected with HPV each year, andinfection rates were highest in young wom-en [12]. In Jordan, sexual activity typicallystarts only after marriage where the maritalage is over 16 years, and the cultural andreligious traditions of our conservative so-ciety restrict the likelihood of multiple sex-ual partners. This may explain why nocases of sexually transmitted HPV, or cer-vical carcinoma, were found in our studygroup of women.
References
1. Greenlee RT et al. Cancer statistics,2000. CA: a cancer journal for clinicians,2000, 50(1):7–33.
2. McCrory DC et al. Evaluation of cervicalcytology. Evidence report/technologyassessment no.5. Rockville, Maryland,Agency for Health Care Policy andResearch, 1999 (AHCPR publicationno.99–E010).
3. Schwartz PE et al. Rapidly progressivecervical cancer: the Connecticut experi-ence. American journal of obstetrics andgynecology, 1996, 175:1105–9.
4. Frame PS, Frame JS. Determinantsof cancer screening frequency: the ex-ample of screening for cervical cancer.Journal of the American Board of FamilyPractice, 1998, 11:87–95.
5. Kenter GG et al. The cytological screen-ing history of 469 patients withsquamous cell carcinoma of the cervixuteri; does interval carcinoma exist?Acta obstetricia et gynecologica scandi-navica, 1996, 75:400–3.
6. IARC Working Group on Evaluationof Cervical Cancer Screening Pro-grammes. Screening for squamous cer-vical cancer: duration of low risk afternegative results of cervical cytology andits implications for screening policies.British medical journal, 1986, 293:659–64.
7. National Institutes of Health ConsensusDevelopment Conference statement oncervical cancer. April 1–3, 1996. Gyneco-logic oncology, 1997, 66:351–61.
27 Evaluation of cervical smears.pmd 8/17/2005, 11:10 AM678

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 679
8. Schiffman MH, Bauer HM, Hoover RN.Epidemiologic evidence that humanpapillomavirus infection causes mostcervical intraepithelial neoplasia. Jour-nal of the National Cancer Institute,1993, 85:958–64.
9. Stoler MH. A brief synopsis of the role ofhuman papillomavirus in cervical car-cinogenesis. American journal of obstet-rics and gynecology, 1996, 175:1091–8.
10. Richart RM et al. Human papillomavirus,IAC Task Force summary. Acta cytolo-gica, 1998, 42:50–8.
11. Stoler MH. Human papillomavirus andcervical neoplasia: a model for carcino-genesis. International journal of gyneco-logical pathology, 2000, 19:16–28.
12. A closer look at HPV infection. In: Track-ing the hidden epidemics 2000: trends in
STDs in the United States. Atlanta, Geor-gia, Centers for Disease Control andPrevention, 2000.
13. Johannesson G, Giersson G, Day N. Theeffect of mass screening in Iceland,1965–74, on the incidence and mortalityof cervical carcinoma. International jour-nal of cancer, 1978, 21:418–25.
14. Hakama M et al. Effect of organizedscreening on the risk of cervical cancerin the Nordic countries. In: Miller AB et al.,eds. Cancer screening. UICC project onevaluation of screening for cancer. Cam-bridge, United Kingdom, InternationalUnion Against Cancer, 1999:153–62.
15. Mount SL, Papillo JL. A study of 10,296pediatric and adolescent Papanicoleausmear diagnosis in northern New En-gland. Pediatrics, 1999, 103(3):539–45.
27 Evaluation of cervical smears.pmd 8/17/2005, 11:10 AM679

680 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
Case report
Glutaric aciduria type 1 in a KuwaitiinfantH.A. Elsori,1 K.K. Naguib2 and M.S. Hammoud3
1Department of Paediatrics, Adan Hospital, Kuwait.2Medical Genetics Centre, Maternity Hospital, Salmiyah, Kuwait (email: [email protected]).3Department of Paediatrics, Faculty of Medicine, University of Kuwait, Kuwait.Received: 25/03/03; accepted: 23/12/03
Introduction
Glutaryl-coenzyme A (CoA) dehydrogena-se deficiency (MIM 231670) is a recessive-ly inherited neurometabolic disorder asso-ciated with encephalopathic crises and se-vere extra-pyramidal symptoms [1]. Mac-rocephaly, frontotemporal brain atrophyand acute encephalopathic episodes char-acterize it, with striatal necrosis followedby dystonia [2]. However, some patientsdevelop motor disease without overt crisisand other biochemically affected individu-als remain asymptomatic [3–8].
This is the first report of a Kuwaiti maleinfant with glutaric aciduria type 1 (GA-1).The clinical picture, the course of the dis-ease, neuro-imaging findings and treatmentare discussed.
Case report
F.A. is a Kuwaiti child, aged 3.5 years, whowas admitted to hospital at the age of 10months because of fever, cough and re-peated vomiting of 1-week duration. Afteradmission, he developed a series of shortleft-sided seizures followed a few days lat-er by right-sided seizures. Phenobarbitaltherapy was started. The seizures contin-ued for 5 days. Shortly after, he developed
a left hemiplegia, and he was no longer ableto sit or crawl and lost his words.
He is the sixth and youngest child tofirst-cousin phenotypically normal parentsand has 5 healthy sisters. Pregnancy anddelivery were normal. Birth weight was 3.6kg. Macrocephaly was noted at birth, andhis head circumference continued to growparallel to the 98th centile. His developmentwas said to be entirely normal until the ageof 10 months. He sat alone at 7.5 months,was crawling and pulling to stand at 8months and by 10 months he had 1 or 2words. He was admitted to hospital at theage of 5 months with suspected meningitisexcluded by cerebrospinal fluid (CSF) ex-amination.
Examination after the acute episode at10 months revealed a relatively healthy,mentally normal child, with weight 10 kgand head circumference 51.5 cm. His cra-nial nerves were normal on examination. Hehad a dystonia of the left side and left hemi-paresis with increased muscle tone and ex-aggerated tendon reflexes on the same side.There were no abnormal neurological signsin the right limb. Examination of chest,heart, abdomen, skin and genitalia showedthat all signs were within normal values.Fundus examination revealed no haemor-rhage or other abnormalities. The following
28 Glutaric aciduria type 1.pmd 8/17/2005, 11:10 AM680

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 681
investigations were normal: plasma sodi-um, potassium, urea, creatinine, liver en-zymes and glucose, haemoglobin, whiteblood cells and platelets, blood pH (7.36)and serum bicarbonate (21.2 nmol/L), pro-thrombin time, thrombin time and fibrino-gen, and serum ammonia, lactic acid andamino acids. Activated partial thromboplas-tin time (APTT) was slightly increased at42 seconds. Plasma ceruloplasmin wasslightly elevated. CSF investigations werenormal. However, urinary glutaric acid was67 µmol/mol creatinine (normal < 14) and3-hydroxy glutaric acid was 85 µmol/molcreatinine (normal range: traces). Glutaryl-carnitine levels in urine were elevated andglutaryl-CoA dehydrogenase activity in cul-tured fibroblasts was low.
Computerized tomography (CT) andmagnetic resonance imaging (MRI) scansof the head revealed severe frontotemporalatrophy and bilateral subdural haemorrhage(Figures 1 and 2).
His current therapy consists of carnitine500 mg 6 hourly, with a low protein dietand carbohydrate drinks to be given during
infections and sick days. He is also receiv-ing regular physiotherapy. Phenobarbitalwas gradually discontinued 5 months afterthe acute episode. He is generally stable,fit-free, and showing mild improvementwith left sided hemiparesis. The child is stillalive at the time of writing this report.
Discussion
Since the first description of GA-1 byGoodman et al. in 1975 [9], several reportshave been added to the literature describingone of the more frequent inherited metabol-ic disorders [10–12]. GA-1 is an autosomalrecessive disorder caused by deficiency ofglutaryl-CoA dehydrogenase, a mitochon-drial enzyme involved in the metabolism oflysine, hydroxylysine and tryptophan. Theclinical picture typically shows varying de-grees of muscular hypotonia, motor delay,dystonia, dysarthria and dyskinesia begin-ning acutely or gradually in the first fewyears of life, often in macrocephalic chil-dren [7,13].
Figure 1 Computerized tomography scansof the head shows severe fronto-temporalatrophy
Figure 2 Magnetic resonance imaging scansof the head shows fronto-temporal atrophyand bilateral subdural haemorrhage
28 Glutaric aciduria type 1.pmd 8/17/2005, 11:10 AM681

682 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
It is difficult to estimate the incidence ofGA-1, as the clinical presentation is vari-able. But the figure of 1:40 000 in Cauca-sians seems a reasonable approximation[14–16]. An incidence as high as 1:30 000has been suggested [16,17]. The disease isparticularly frequent in certain communi-ties such as the Amish people in Pennsyl-vania (1:4000) and Saulteaux/OjibwayIndians in Canada [1,13–15,18]. Few pa-tients have been recorded among Arab pop-ulations [19]. In Kuwait, its incidence hasnot been estimated so far. However, thefrequency of metabolic disorders is com-mon in Kuwait [20].
In the present report, the clinical pic-ture, the course of the disease and thebiochemical and radiological findings rep-resent the classic presentation of GA-1.Both the onset and the clinical picture ofthe patient, who had a viral illness followedby encephalopathic crisis, have been con-sidered common features. However,among 100 cases described worldwide,only 4 asymptomatic homozygotes for thedisease have been described [3,11,15].This variability in presentation sometimesnecessitates a high index of suspicion fordiagnosis. Page et al. [21] reported a casethat presented in the neonatal period withseizures, while Superti-Furga and Hoff-mann [2] emphasized that presentation maystart between the early weeks and the 4thto 5th year of life when intercurrent illness-es, viral infections or gastroenteritis maytrigger acute encephalopathy. The bio-chemical findings of the present case werehighly diagnostic. The diagnosis of GA-1 issuggested by the findings of excess 3-hy-droxyglutaric acid in the urine and thisshould be found on a urinary organic acidscreen. Blood acylcarnitine profile has alsobeen used as a more sensitive test. Howev-er, both tests may show negative resultsand a strong clinical suspicion is needed
[22]. Recognition of the biochemicalchanges before the brain has been injured isessential for a satisfactory outcome. Diag-nosis depends on the recognition of rela-tively non-specific physical findings suchas hypotonia, irritability, macrocephaly andurine organic acid quantification [13]. Thelow activity of glutaryl-CoA dehydrogenasein cultured fibroblasts confirms the diagno-sis of GA-1. In addition, the radiologicalfinding of fronto-temporal atrophy is typi-cally described in patients with GA-1 [23].It has been suggested that the combinationof wide CSF spaces anterior to the tempo-ral lobe and low-density lesions in the basalganglia are almost diagnostic of this condi-tion [24]. In addition, the presence of sub-dural haemorrhage has been reported [25].
Glutaryl-CoA dehydrogenase is a multi-functional enzyme, which exists in the mi-tochondrial matrix as a homotetramer of45-kD subunits. The human gene for glu-taryl-CoA dehydrogenase has been clonedand mapped to the short arm of chromo-some 19p13 [26]. More than 63 mutationshave been identified so far in GA-1 families,but no one prevalent mutation was detectedand little if any relationship between geno-type and clinical phenotype could be re-cognized. The mutations were widelydistributed through the gene, with the larg-est number in exon 10 [27]. Recessive in-heritance of this disorder is confirmed.
In conclusion, this report is the first ofGA-1 from Kuwait. The clinical, biochemi-cal and radiological findings confirm the di-agnosis. Our patient is now stable but hasonly minor improvement, which agreeswith most of the reported cases in the liter-ature. We hope that continued therapy withcarnitine and low protein diet together withemergency regimen with carbohydratedrinks will at least prevent further deterio-ration and encephalopathic crisis. Coordi-nated research is needed to understand the
28 Glutaric aciduria type 1.pmd 8/17/2005, 11:10 AM682

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 683
pathogenesis of the brain pathology, to de-fine the role of dietary therapy and to ex-plore the possibility of neonatal screening.
Multi-centre studies are needed to establishthe best method for diagnosis and the opti-mal therapy of this disorder.
References
1. Hoffmann GF et al. Clinical course, earlydiagnosis, treatment and prevention ofdisease in glutaryl-CoA dehydrogenasedeficiency. Neuropediatrics, 1996,27:115–23.
2. Superti-Furga A, Hoffman G. Glutaric aci-duria type 1 (glutaryl-CoA-dehydroge-nase deficiency): advances and un-answered questions. European journalof paediatrics, 1997, 156:821–8.
3. Amir N et al. Glutaric aciduria type 1: en-zymatic and neuroradiologic investi-gations of two kindred. Journal ofpediatrics, 1989, 114:983–9.
4. Lipkin PH et al. A case of glutaric aci-demia type I: effect of riboflavin and car-nitine. Journal of pediatrics, 1988, 112:62–5.
5. Hoffman GF et al. Early signs and courseof disease of glutaryl-CoA dehydroge-nase deficiency. Journal of inheritedmetabolic disease, 1995, 18:173–6.
6. Woelfle J et al. Subdural hemorrhage asan initial sign of glutaric aciduria type 1: adiagnostic pitfall. Pediatric radiology,1996, 26:779–81.
7. Renner C et al. Clinically asymptomaticglutaric aciduria type I in a 4 5/12-year-old girl with bilateral temporal arachnoidcysts. Journal of inherited metabolic dis-ease, 1997, 20:840–1.
8. Pineda M et al. Glutaric aciduria type Iwith high residual glutaryl-CoA dehydro-genase activity. Developmental medi-cine and child neurology, 1998, 40:840–2.
9. Goodman S et al. Glutaric aciduria: a“new” disorder of amino acid metabo-
lism. Biochemical medicine, 1975, 12:12–21.
10. Gregersen N et al. Glutaric aciduria: clini-cal and laboratory findings in two broth-ers. Journal of pediatrics, 1977, 90:740–5.
11. Kyllerman M et al. Dystonia and dyskine-sia in glutaric aciduria type I: clinicalheterogeneity and therapeutic consider-ations. Movement disorders, 1994, 9:22–30.
12. Hgberg B, Kyllerman M, Steen G. Dyski-nesia and dystonia in neurometabolicdisorders. Neuropediatrics, 1979, 10:305–20.
13. Baric I et al. Diagnosis and managementof glutaric aciduria type I. Journal of in-herited metabolic disease, 1998, 21:326–40.
14. Haworth J et al. Phenotypic variabilitiesin glutaric aciduria type I: report of four-teen cases in five Canadian kindred.Journal of pediatrics, 1991, 118:52–8.
15. Morton DH et al. Glutaric aciduria type I: acommon cause of episodic encephal-opathy and spastic paralysis in theAmish of Lancaster county, Pennsylva-nia. American journal of medical genet-ics, 1991, 41:89–95.
16. Ziadeh R, Naylor E, Ginegold D. Identifi-cation of two cases of glutaric aciduriatype I through routine neonatal screen-ing using liquid secondary ionizationtandem mass spectrometry. Abstracts ofthe 6th International Congress on InbornErrors of Metabolism, Milan, Italy, May27–31, 1994: WS–2.
28 Glutaric aciduria type 1.pmd 8/17/2005, 11:10 AM683

684 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
17. Kyllerman M, Steen G. Glutaric aciduria.A “common” metabolic disorder? Ar-chives francaises de pediatrie, 1980,37:279.
18. Goodman S, Freeman F. Organic aci-demias due to defects in lysine oxida-tion: 2-ketoadipic academia and glutaricacademia. In: Scriver CR et al., eds. Themetabolic and molecular bases of in-herited disease, 7th ed. New York,McGraw–Hill, 1995:1451–60.
19. Al-Essa M et al. Glutaric aciduria type 11:observations in seven patients with neo-natal- and late-onset disease. Journal ofperinatology, 2000, 20(2):120–8.
20. Teebi AS et al. Phenylketonuria in Ku-wait and Arab countries. European jour-nal of pediatrics, 1987, 146:59–60.
21. Page A et al. Early clinical manifestationof glutaric aciduria type I and nephriticsyndrome during the first months of life.Acta paediatrica, 1997, 86(10):1144–7.
22. Hauser S, Peters H. Glutaric aciduriatype I: an undiagnosed cause of en-cephalopathy and dystonia-dyskinesiasyndrome in children. Journal of pediat-rics and child health, 1998, 34(3):302–4.
23. Martinez-Lage J et al. Macrocephalydystonia and bilateral temporal arach-noid cysts: glutaric aciduria type 1.Child’s nervous system, 1994, 10:198–203.
24. Brisman J, Ozand P. CT and MRI of thebrain in glutaric aciduria type I. A reviewof 59 published cases and a report of5 new patients. American journal ofneuroradiology, 1995, 16:675–83.
25. Greenberg C et al. Assignment of hu-man glutaryl-CoA-dehydrogenase gene(GCDH) to the short arm of chromosome19, 19p13.2, by in situ hybridization andsomatic cell hybrid analysis. Genomics,1994, 21:289–90.
26. Biery BJ et al. Gene structure and muta-tion of glutaryl-coenzyme A dehydro-genase: impaired association of enzymesubunits that is due to an A421V substi-tution causes glutaric acidemia type 1 inthe Amish. American journal of humangenetics, 1996, 59(5):1006–11.
27. Goodman S et al. Glutaryl-coA dehydro-genase mutations in glutaric acidemia(type 1): review and report of thirty novelmutations. Human mutation, 1998, 12:141–4.
28 Glutaric aciduria type 1.pmd 8/17/2005, 11:11 AM684

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 685
Case report
Maternal death due to severepulmonary oedema caused byfalciparum malaria: a case reportI. Adam1 and M.I. Elbashir 2
1New Halfa Teaching Hospital, New Halfa, Sudan.2Faculty of Medicine, University of Khartoum, Khartoum, Sudan.Received: 12/10/03; accepted: 23/12/03
Introduction
Pregnancy increases susceptibility to falci-parum malaria, and the level of diseasetransmission in an area influences the man-ifestations of the disease during pregnancy.In areas of low and unstable transmission,malaria during pregnancy is usually symp-tomatic, unlike the situation in areas of highendemicity, where patients are usually as-ymptomatic or present with severe anaemia[1,2]. There is some degree of immunesuppression during pregnancy, with se-questration of infected red blood cells inthe placenta through binding to chondroitinsulfate [3,4].
Malaria constitutes 40% of the infec-tious disease burden and approximately50%–70% of all outpatient visits to hospi-tals in Sudan [5]. In eastern Sudan, malariais mesoendemic and the predominant ma-laria species is Plasmodium falciparum[6,7]. We have previously observed differ-ent forms of clinical presentations of se-vere malaria among pregnant Sudanesewomen, including cerebral malaria, andthat all parities were infected [8]. Antima-larial drug resistance is also a growingthreat in Sudan [6].
We report a young pregnant womanwith severe chloroquine-resistant falci-
parum malaria and pulmonary oedema whodied of respiratory failure in spite of ade-quate treatment with quinine in hospital.
Case report
A 24-year-old primigravida presented toNew Halfa Teaching Hospital (easternSudan) on 28 December 2002 with amen-orrhoea for 34 weeks, fever, headache,productive cough and vomiting for 5 days.Two days before admission she had re-ceived 5 injections of chloroquine afterconfirmation of P. falciparum infectionwithout improvement.
The following findings were recordedon presentation: weight 73 kg, temperature39.2 °C, pulse 95 beats/minute, blood pres-sure 110/70 mmHg, respiratory rate 30breaths/minute, haemoglobin 9 g/dL, totalwhite blood cells 8500 cells/µL, blood glu-cose 110 mg/dL, blood urea 25 mg/dL, se-rum creatinine 0.9 mg/dL. Her chest wasclear clinically, with no crepitations orrhonchi. Examination of the baby showed afundal height that correlated with the moth-er’s dates, cephalic presentation and audi-ble heartbeat.
The diagnosis of chloroquine-resistantfalciparum malaria with or without chest
29 Maternal death due.pmd 8/17/2005, 11:11 AM685

686 La Revue de Santé de la Méditerranée orientale, Vol. 10, No 4/5, 2004
infection was suspected initially. Thickblood films confirmed parasitaemia and thepatient was put on quinine hydrochlorideinfusion in 5% dextrose 600 mg 3 timesdaily and also given benzyl penicillin 1 mil-lion IU intravenously every 4 hours.
After 24 hours the woman’s axillarytemperature was slightly lower at 38.8 °C,respiratory rate had risen to 50 breaths/minute and the blood film was still positive,but she was cyanosed. Pulmonary oedemawas suspected and the diagnosis was con-firmed by chest X-ray. The patient was puton intermittent oxygen, furosemide 40 mg/kg twice daily and 15 mg of morphine wasgiven intramuscularly. Quinine and penicil-lin were continued but there was no im-provement.
On the third day the patient’s bloodfilms were negative but she was deeply cy-anosed, respiratory rate was 54 breaths/minute, temperature was 38.4 °C and shehad chest crepitations. She died on the thirdday from respiratory failure.
Discussion
This report draws the attention to the threatcaused by falciparum malaria in pregnantwomen in areas of low and unstable malariatransmission such as that in eastern Sudan.However, complications of falciparum ma-laria in adults, especially lung injury and re-nal failure, can occur after several days oftreatment when the parasites have de-
creased from baseline or even when para-sites disappear from the peripheral blood[9]. This patient presented with manifesta-tions of malaria after 5 days of treatmentwith chloroquine, a drug that is showingincreasingly high failure rates in Sudan [6].
In many Asian and African countries,malaria is reported as one of the main caus-es of maternal mortality [10–14], and incentral Sudan it was the leading cause ofmaternal mortality over the 15 years 1985–99, accounting for 37% of maternal deaths[12]. Therefore, the utmost care andprompt early treatment with effectivedrugs is recommended in pregnant women,due to high susceptibility to severe compli-cations in areas of low and unstable trans-mission, and the rising rate of multi-drugresistance in all malaria-endemic areas. TheWorld Health Organization recommendsquinine as the drug of choice for severe fal-ciparum malaria [15]. However, it shouldnot be relied upon as the sole treatment, butattention should be also directed to goodmonitoring of blood pH and gases (serviceslacking in our centre) and of venous pres-sure to avoid over-hydration that maycause or exacerbate pulmonary oedema.Likewise, intensive care units with a venti-lator are of paramount importance for pa-tients with pulmonary oedema. As inover-hydration, heart failure, renal failureand pulmonary irritants, falciparum malariashould be remembered as a cause of pul-monary oedema.
References
1. Brabin BJ et al. A study of the conse-quences of malaria infection in pregnantwomen and their infants. Parassitologia,1993, 35(suppl.):9–11.
2. Nosten F et al. Malaria during pregnancyin an area of unstable endemicity. Trans-actions of the Royal Society of TropicalMedicine and Hygiene, 1991, 85:424–9.
3. Fievet N et al. Immune response to Plas-modium falciparum antigens in Came-roonian primigravidae: evolution afterdelivery and during second preg-nancy. Clinical experimental immunol-ogy, 1997, 107:462–7.
4. Fried M, Duffy PE. Adherence of plasmo-dium falciparum to chondroitin sulfate A
29 Maternal death due.pmd 8/17/2005, 11:11 AM686

Eastern Mediterranean Health Journal, Vol. 10, Nos 4/5, 2004 687
in human placenta. Science, 1996, 272:1502–4.
5. El Gaddal AA. The experience of theBlue Nile Health Project in the control ofmalaria and other water associated dis-eases. In: American Association for Ad-vancement of Science. Malaria anddevelopment in Africa. A cross-sectoralapproach. Washington DC, AAAS, 1991.
6. Adam I et al. In the Sudan: chloroquineresistance is worsening and quinine re-sistance is emerging. Sudan medicaljournal, 2001, 39:5–11.
7. El Gadal AA. Malaria in the Sudan. In:Buck AA, ed. Proceedings of the confer-ence on malaria in Africa. Washington,DC, American Institute of Biological Sci-ences/USAID, 1986:156–9.
8. Adam I et al. Quinine therapy in severePlasmodium falciparum malaria duringpregnancy in Sudan. Eastern Mediterra-nean health journal, 2004, 10(1/2):159–66.
9. World Health Organization, Communi-cable Diseases Cluster. Severe falci-parum malaria. Transactions of the RoyalSociety of Tropical Medicine and Hy-giene, 2000, 94(suppl. 1):S1–90.
10. Wickramasuriya GAW. Malaria and anky-lostomiasis in the pregnant woman.Their more serious complications andsequelae. Oxford, Oxford UniversityPress, 1937.
11. Menon R. Pregnancy and malaria. Medi-cal journal of Malaysia, 1972, 27:115–9.
12. Dafallah SE, El Agib FH, Bushra GO. Ma-ternal mortality in a teaching hospital inSudan. Saudi medical journal, 2003,24:369–73.
13. Fawcus S et al. Community based studycause of maternal mortality in rural andurban Zimbabwe. Central African journalof medicine, 1995, 41:105–13.
14. Urassa E et al. Female mortality in thereproductive ages in Dar es Salam, Tan-zania. East African medical journal,1994, 71:226–31.
15. World Health Organization, Division ofControl of Tropical Diseases. Severe andcomplicated malaria. Transactions of theRoyal Society of Tropical Medicine andHygiene, 1990, 84(suppl. 2):1–65.
29 Maternal death due.pmd 8/17/2005, 11:11 AM687









Related Documents