THE JOURNAL OF THE EGYPTIAN PUBLIC HEALTH ASSOCIATION Vol. 85 No. 1&2 2010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

THE JOURNAL OFTHE EGYPTIAN PUBLICHEALTH ASSOCIATION
Vol. 85 No. 1&2 2010
J Egypt Public Health Assoc Vo/. 85 N°. 1 & 2,2010
Prevalence of Latent TB among Health CareWorkers in Four Major Tertiary Care Hospitals
in Riyadh, Saudi Arabia
Moustafa A.F. Abbas *'**, Nasser AE. AIHamdan *, Lamiaa A.Fiala **,*** Awwad K. AIEnezy ****, Mohamed S. AIQahtani ****
* Community Medicine Dept., Faculty oJ Medicine, KFMC, KSA U-HS,Riyadh, Saudi Arabia
** Community Medicine Dept., Faculty oJ Medicine, Suez Canal University,Ismailia, Egypt
*** Community Health Sciences Dept., King Saud University, Riyadh, SaudiArabia
****Employee Health Clinics, KFMC, MOH, Riyadh, Saudi Arabia
ABSTRACT
Background: Tuberculosis (TB) infection represents a global health
problem and a great risk to Health Ca~'e Workers (HCWs). Identifyingindividuals, particularly HCWs with latent tuberculosis infection (LTBI)will support TB control through chemoprophylaxis and prevent crossinfection. Objectives: This study aimed to identify prevalence of Latent
TB among a two-year new hires of HCWs in 4 major tertiary carehospitals in Riyadh, Saudi Arabia. Material and Methods: 2650 recently(2-years) hired HCWs were surveyed for latent TB using TuberculinSkin Test (TST). Data was collected from January 2008 to December
2009. Induration due to TST equal to or more than 10 mm. within 48-72hours was considered positive. The results of TST were correlated withother variables such as age group, gender, job category, country of
origin. Results: as an overall rate, 291(11%) out of 2650 were positive forTST, with the highest significant positive rates among physicians(14.9%) and nurses (12.9%) compared to students as a reference group.
Corresponding Author:Dr. Moustafa A. F. Abbas
Community Medicine Dept.Faculty of Medicine, King Fahad Medical CityRiyadh, Saudi Arabia.Faculty of Medicine, Suez Canal University.Ismailia, Egypt.Email: [email protected]
J Egypt Public Health Assoc Vol. 85 N°. 1 & 2,2010
No statistically significant difference was detected between both sexes.The highest significant positive TST rates were found among HCWs inthe age group of 50 years and older (32.6%) compared to 10-19years agegroup as a reference group, and among HCWs coming from subSaharan countries (61.1%) compared to Saudi HCWs with the lowestpositive rates (5%) as a reference group. Conclusion andrecommendations: LTB is prevalent among newly hired HCWs inRiyadh tertiary hospitals. Stcndard programs for detection andtreatment of LTBshould be encouraged.
Keywords: Health Care Workers (HCWs), Latent Tuberculosis (LTB),occupational health.
INTRODUCTION
Tuberculosis is a global health problem and World Health
Organization (WHO) in 2010 reported that someone in the world
is newly infected with TB bacilli every second. One-third of the
world's population is currently infected with the TB bacillus.
Also, 5-10% of people who are infected with TB bacilli (but whoare not infected with HIV) become sick or infectious at some time
during their life.(l)
TB is on the list of biologic health hazards to HCWs, and
remains a very important occupational risk for HCWs in Low andMedium Income Countries and for workers in some institutions
in High Income Countries. Risk appears particularly high whenthere is increased exposure like working at infectious diseases
hospitals, emergency rooms and laboratory settings, combined
with inadequate infection control measures.(2-4)
De Vries et aI., (2006) (5) confirmed the importance of
vigilance in TB control and emphasized that a high suspicion of
tuberculosis by the clinician, adequate infection control
78
J Egypt Public Health Assoc Vol. 85 N°. 1 & 2,2010
measures by hospital authorities, and early identification of
latent tuberculosis infection by occupational and public-healthspecialists are necessary to prevent tuberculosis amonghealthcare workers.
Many studies pointed to the high prevalence of Latent TB
among health care workers that reached up to 69% in some
studies. (6,7) On the other hand, molecular-epidemiologicalstudies and a comprehensive review of the existing evidence
concerning the infection risk for HCWs lead to the conclusion
that TB in HCWs is often caused by infection at the workplace. (8)
TST testing has been accepted universally as the main
method for detecting LTB, in spite of its limitations and theeffectiveness of recent BCG vaccinations. (9,10)
Identifying positive Latent TB among HCWs helps m
reducing the risk of later development of open TB among them.
The aim of this study was the identification of the prevalence of
Latent TB among recently hired HCWs in 4 major tertiary carehospitals in Riyadh, Saudi Arabia.
MATERIAL AND METHODS
This study included 2650 recently hired HCWs in 4 major
tertiary care hospitals in Riyadh, Saudi Arabia, starting from
January 2008 to December 2009. Data were collected from eachHCW including; age, gender, job category, and country of
citizenship. They were examined for Latent TB using TST byinjection of 0.1 ml (5 units) of Purified Protein Derivative (PPD)
intracutaneously, usually in the volar aspect of the forearm. Thereaction was read 48-72 hours later, the size of the reaction was
determined by measurement of the induration not the erythema.
79
J Egypt Public Health Assoc Vol. 85 N°. 1 & 2,2010
A measurement equal to or more than 10 mm was considered
positive. (11- 13) The results of the TST testing were correlated withother variables.
Statistical analysis:Statistical analysis was done using the Epi Info Software
program, version 6.04 (14) and the SPSS program version 16. (15)
Odds ratios were calculated and p values less than 0.05 were
considered significant.
RESULTS
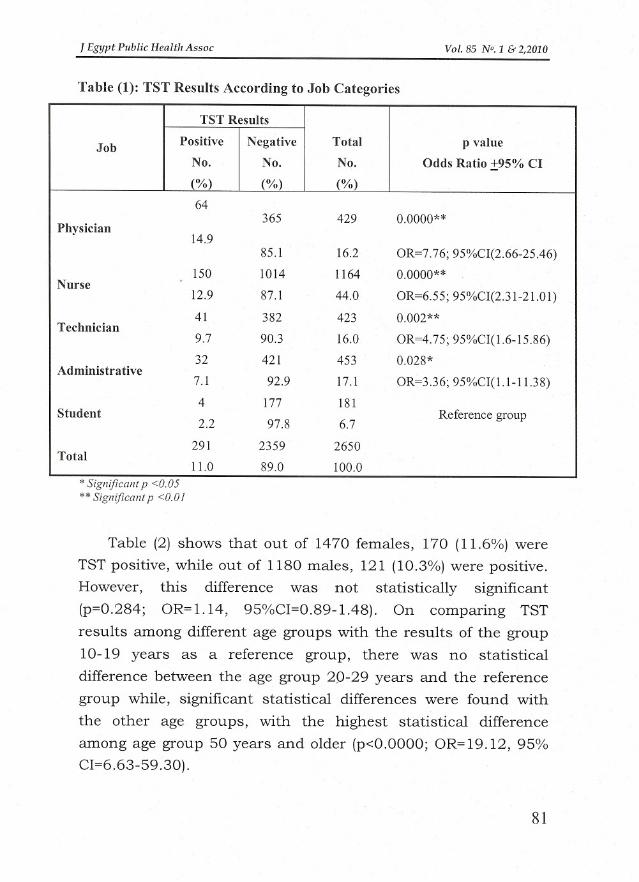
Table (1) shows that the 2650 HCWs who participated in the
study included 429 (16.2%) physicians, 1164 (44%) nurses, 423
(16%) technicians, 453 (17.1%) administrative employees and
181 (6.7 %) medical students. Out of the 2650 HCWs, 291 (11%)
were positive for TST, of them 64 (14.9%) were physicians, 150
(12.9%) were nurses, 41 (9.7%) were technicians, 32(7.1%) were
administrative employees and 4 (2.2%) were medical students.There were statistically significant differences between rates of
positive TST among different job categories of HCWs compared tostudents as a reference group. The highest odds of infection was
among physicians (7.76, 95%CI (2.66-25.46)).
80
1Egypt Public Health Assoc
Table (1): TST Results According to Job Categories
Vol. 85 N°. 1 & 2,2010
TST Results
Job
PositiveNegativeTotal p value
No.
No.No.Odds Ratio ±95% Cl(%)
(%)(%)
64365
4290.0000**Physician 14.985.1
16.2OR=7.76; 95%CI(2.66-25.46)
150
101411640.0000**Nurse 12.9
87.144.0OR=6.55; 95%CI(2.31-21.01)
41
3824230.002**Technician 9.7
90.316.0OR=4.75; 95%CI(1.6-15.86)32
4214530.028*Administrative 7.1
92.917.1OR=3.36; 95%CI(1.l-11.38)
4
177181Student Reference group2.2
97.86.7
291
23592650Total 11.0
89.0100.0
* Significant p <0.05** Significant p <0.0 I
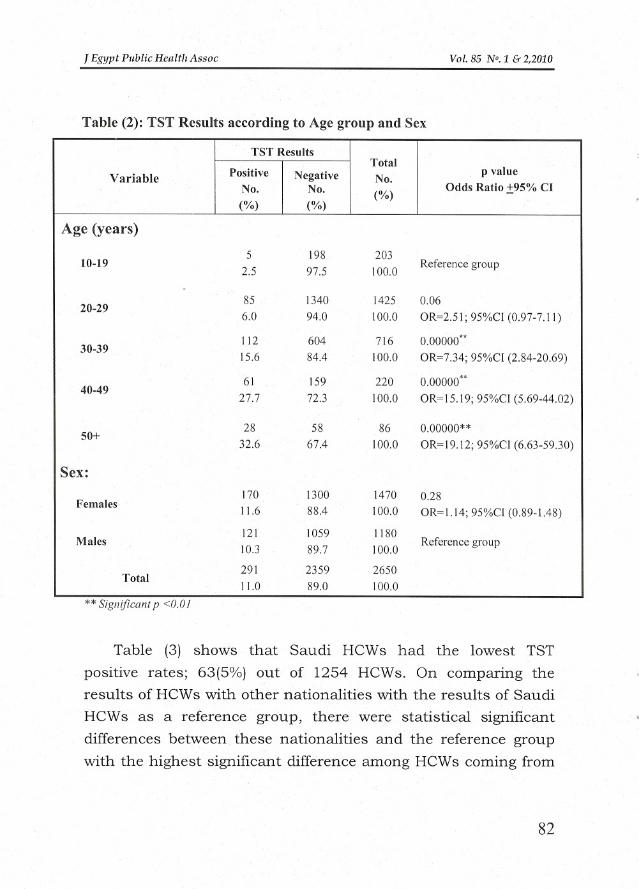
Table (2) shows that out of 1470 females, 170 (11.6%) wereTST positive, while out of 1180 males, 121 (10.3%) were positive.
However, this difference was not statistically significant
(p=0.284; OR=1.14, 95%CI=0.89-1.48). On comparing TST
results among different age groups with the results of the group
10-19 years as a reference group, there was no statisticaldifference between the age group 20-29 years and the referencegroup while, significant statistical differences were found with
the other age groups, with the highest statistical difference
among age group 50 years and older (p<O.OOOO;OR=19.12, 95%CI=6.63-59.30).
81
J Egypt Public Health Assoc
Table (2): TST Rcsults according to Age group and Sex
Vo!. 85 N°. 1 & 2,2010
TST ResultsTotalVariable
PositiveNegativeNo.
p value
No.
No.(%)Odds Ratio ±95% Cl
(%)
(%)
Age (years) 5
19820310-19 2.5
97.5100.0Reference group
85
134014250.0620-29 6.0
94.0100.0OR=2.51; 95%CI (0.97-7.11)
112
6047160.00000*'30-39 15.6
84.4100.0OR=7.34; 95%CI (2.84-20.69)
61
1592200.00000**40-49 27.7
72.3100.0OR=15.19; 95%CI (5.69-44.02)
28
58860.00000**50+ 32.6
67.4]00.0OR=] 9.12; 95%C] (6.63-59.30)
Sex: 170
130014700.28Females 11.6
88.4100.0OR=1.14; 95%CI (0.89-1.48)
121
10591180Males 10.3
89.7100.0Reference group
291
23592650Total 11.0
89.0100.0
** Significant p <0.01
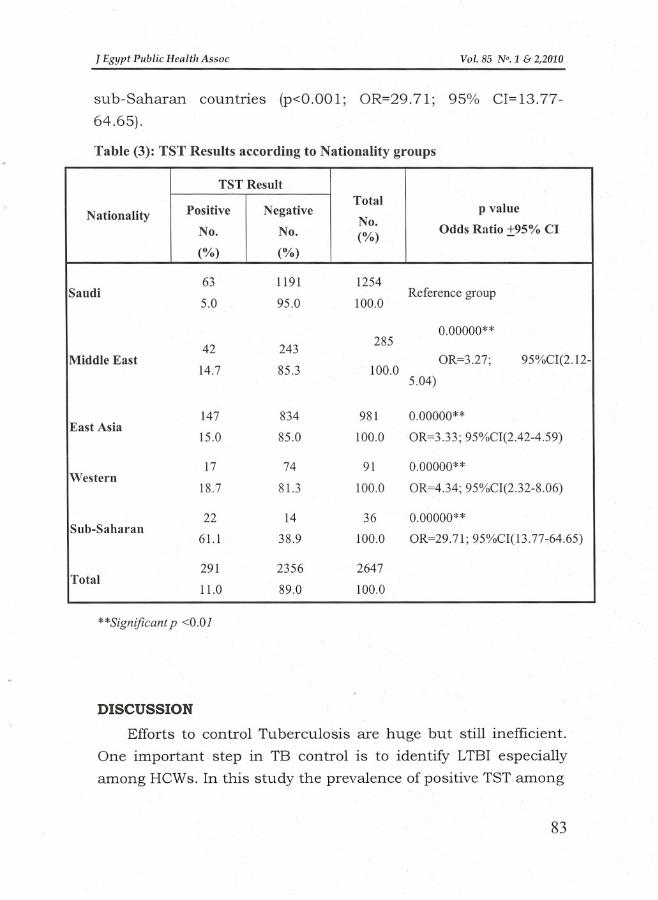
Table (3) shows that Saudi HCWs had the lowest TST
positive rates; 63(5%) out of 1254 HCWs. On comparing theresults of HCWs with other nationalities with the results of Saudi
HCWs as a reference group, there were statistical significant
differences between these nationalities and the reference group
with the highest significant difference among HCWs coming from
82
J Egypt Public Health Assoc Vol. 85 N°. 1 & 2,2010
sub-Saharan countries (p<O.OOl; OR=29.71; 95% CI=13.77
64.65).
Table (3): TST Results according to Nationality groups
TST ResultTotalp valueNationalityPositive
NegativeNo.No.
No.(%)Odds Ratio ±95% Cl
(%)
(%)
63
11911254Saudi
Reference group5.0
95.0100.0
0.00000**42
243285
Middle East
OR=3.27;95%CI(2.12-14.7
85.3100.05.04)
147
8349810.00000**East Asia 15.0
85.0100.0OR=3.33; 95%CI(2.42-4.59)
17
74910.00000**Western 18.7
81.3100.0OR=4.34; 95%CI(2.32-8.06)
22
14360.00000**Sub-Saharan 61.1
38.9100.0OR=29.71; 95%CI(13.77-64.65)
291
23562647Total 11.0
89.0100.0
**Significant p <0.01
DISCUSSION
Efforts to control Tuberculosis are huge but still inefficient.
One important step in TB control is to identify LTBI especiallyamong HCWs. In this study the prevalence of positive TST among
83
J Egypt Public Health Assoc Vo/. 85 N°. 1 & 2,2010
HCWs was found to be 11% with the highest prevalence (32.6%)alIlOng age group 50 years or older. These results were
comparable to the findings of Nienhaus et al., (2007) (6) whofound a positive TST prevalence of 12.8%. In their study, therewas also strong relationship between age and TST results, with
the highest prevalence of positive TST (69.2%) among age group
60 years or more. On the other hand, lower rates were reportedby other studies. For example, among health care workers in a
hospital for pulmonary diseases in Germany, Schablon et al.,(2009) (7) found the prevalence of LTBI to be 7.2%. In HCWs
younger than 30 years LTBI prevalence was 3.5% and in thoseolder than 50 years it was found to be 22% which is less than
our findings probably due to the use of Quantiferon blood ELISA
testing which has much less false positive results than standardTST used in our study.
By using the interferon-gamma release assay (IGRA) inanother study by Nienhaus, (2009) (8) LTBI prevalence in HCWs
was 10 %, and this study recommended that preventionstrategies in Germany should be reconsidered.
On studying 1755 Italian HCWs, Franchi et al., in 2009 (9)
found the overall Positive TST to be 6% which is much less than
our findings, but agreed with our results in that older age andbeing physicians were high risk factors for TST positivity.
While Demkow et al., (2008) (16) on studying 155 HCWs m
Poland, using interferon-gamma whole blood and tuberculin skin
tests, found that the prevalence of LTBI was, on average, 27.1%,a higher risk of acquiring LTBI was associated with certain work
locations (TB lab workers--prevalence 50%, TB ward clinicians-
34%, nurses--30%, analytical lab technician-- 20%, and in
84
J Egypt Public Health Assoc Vo!. 85 N°. 1 & 2,2010
administration staff-- 15%). Drobniewski et al., (2007) (17)
mentioned that Russia is one of 22 high burden tuberculosis
countries. LTBI was seen in 40.8% (107/262) of staff and was
significantly higher in doctors and nurses (39.1%) than in
students (8.7%). In their systematic review, Joshi et aI., (2006) (18)
reported high rates of LTB among HCWs in many countries; our
findings agreed with their results in that physicians had higherTST positive rates among all HCWs job categories.
CONCLUSIONS AND RECOMMENDATIONS
LTB was prevalent among HCWs (11%) who are newly hired
m major hospitals in Saudi Arabia. Higher TST positive rates
were associated with older age and certain job categories as
physicians and nurses. Testing of HCWs at hire and periodicallycan help in the detection of LTBI and using prophylaxistreatment for positive TST cases can reduce the number of HCWs
who may develop TB later on. There is a need for using the newly
introduced method of ELISA techniques in performing more
studies for detection of LTB, hopefully to increase true positive
results and reducing false negative results encountered on usingTST.
REFERENCES
1. World Health Organization. Tuberculosis. Fact sheet N°104, March,2010.
2. Menzies D, Joshi R, Pai M. Risk of tuberculosis infection and disease
associated with work in health care settings. Int J Tuberc Lung Dis.2007; 11(6):593-605.
85
J Egypt Public Helllth Assoc Vo!. 85 N°. 1 & 2,2010
3. Garber E, San Gabriel P, Lambert L, Saiman 1. A survey of latent
tuberculosis infection among laboratory healthcare workers in New
York City. Infect Control Hosp Epidemiol.2003; 24(11):801-6.
4. Driver CRI Stricof RL, Granville K, Munsiff SS, Savranskaya G,
Kearns C et al. Tuberculosis in health care workers during declining
tuberculosis incidence in New York State. Am J Infect Control. 2005;
33(9):519-26.
5. De Vries G, Sebek MM, Lambregts-van Weezenbeek CS. Healthcare
workers with tuberculosis infected during work. Eur Respir J. 2006;
28(6):1216-21.
6. Nienhaus A Schablon A Loddenkemper K Hauer B, Wolf N, DielR. Prevalence of latent tuberculosis infection in healthcare workers
in geriatric care. Pneumologie. 2007; 61(9):613-6.
7. Schablon A Beckmann G, Harling M, Diel R, Nienhaus A.
Prevalence of latent tuberculosis infection among health care
workers in a hospital for pulmonary diseases. Journal of
Occupational Medicine and Toxicology. 2009. [cited 2009 January
9]. Available from: http://www.occup-med.com/content/ 4/1/1
8. Nienhaus A. Tuberculosis in healthcare workers. Pneumologie.
2009; 63(1):23-30.
9. Franchi A, Diana 0, Franco G. Job-related risk of latent tuberculosis
infection in a homogeneous population of hospital workers in a low
incidence area. Am J Ind Med. 2009; 52(4):297-303.
10. Brodie D, Schluger NW. The diagnosis of Tuberculosis. Clin Chest
Med. 2005; 26: 247-71.
11. Centers for Diseases Control (CDC). Notice to readers: revised
technical instructions for tuberculosis screening and treatment for
panel physicians. MMWR. 2008; 57:292-3.
86
J Egypt Public Health Assoc Vol. 85 N°. 1 & 2,2010
12. American Thoracic Society. Diagnostic standards and classification
of tuberculosis in adults and children. Am J Respir Crit Care Med.2000; 161: 1376-95.
13. Jasmer RM, Nahid P, Hopewell Pc. Latent tuberculosis infection. N
Engl J Med. 2002; 347(23): 1860-6.
14. Epi Info ver 6.04: Centers for Diseases Control, USA, Statistical
Package for Epidemiologists. Release 6.04, Augustl, 2001.
15. SPSS Ver 16: Statistical Package for Social Studies. SPSS Inc. USA,
Release 16.0.0, September 17, 2007.
16. Demkow U, Broniarek-Samson B, Filewska M, Lewandowska K,
Maciejewski J, Zycinska K, et (11. Prevalence of latent tuberculosis
infection in health care workers in Poland assessed by interferon
gamma whole blood and tuberculin skin tests. J Physiol Pharmacol;
2008; 59(6): 209-17.
17. Drobniewski F, Balabanova Y, Zakamova E, Nikolayevskyy V,Fedorin 1. Rates of latent tuberculosis in health care staff in Russia.
PLoS Med., 2007; 4(2): e55.
18. Joshi R, Reingold AL, Menzies D, Pai M. Tuberculosis among health
care workers in low- and middle-income countries: a systematic
review. PLoS Med. 2006; 3 (12):e494.
87
Related Documents











