ASSESSMENT: Resources: "Pressure Ulcers/Injuries - Introduction and Assessment" (a) History and physical exam: see Table 1 and Table 2 (b) Risk factors: b1. For development of PU/PI: neurological conditions impeding movement, lower extremity trauma (e.g. hip fractures), older age, prolonged surgical procedures, critically ill patients, incontinence, malnutrition. See Structured Risk Assessment and validated tools (Braden, Norton, Waterlow) b2. For infection: onset > 4 weeks, location near frequently contaminated areas (e.g, near anus), cardiovascular and endocrine conditions, malnutrition (c) Blood supply: If PU/PI on lower extremity, conduct non- invasive arterial tests to rule out peripheral arterial disease. See table with values and interpretations in topic "How to Select Adequate Compression Therapy Pressure Levels and Products". (d) Differential diagnoses: see Table 3 (e) Determine healability: see Table 4 (f) PU/PI classification/stages: see topic "Pressure Ulcers/Injuries - Classification/Staging". Stage drawings NPUAP copyright & used with permission ALGORITHM: ASSESSMENT Pressure Ulcer / Injury (PU/PI) ©2019 Wound reference Inc. All rights reserved. Not intended to replace healthcare professional judgment with respect to individual needs. Revised 02/17/2019 Determine: Differential diagnoses (d) Healability: potential for ulcer to heal with conservative treatment (e) PU/PI classification/stages (f) History and physical exam consistent with PU/PI? (a) Which risk factors led to development of PU/PI? (b1) Are there risk factors for infection? (b2) If ulcer on lower extremity, is there adequate blood supply to the ulcer? (c) Patient's and caregiver's concerns? Other Diagnosis Manage according to likely differential diagnosis NEW ULCER Quality Measures See Algorithm for Treatment of PU/PI (coming soon) Stage 1 Non-blanchable erythema of intact skin Stage 2 Partial-thickness skin loss with exposed dermis Stage 3 Full-thickness skin loss (no exposed bones, cartilage, tendon Stage 4 Full-thickness skin and tissue loss (exposed bones, cartilage, tendon) Unstageable PU/PI Obscured full- thickness skin and tissue loss (covered with slough, eschar) Deep Tissue Injury (DTI) Persistent non- blanchable deep red, maroon or purple discoloration PU/PI Stages drawings by NPUAP copyright & used with permission

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

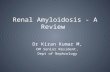
ASSESSMENT:
Resources: "Pressure Ulcers/Injuries - Introduction andAssessment"
(a) History and physical exam: see Table 1 and Table 2
(b) Risk factors:
b1. For development of PU/PI: neurological conditionsimpeding movement, lower extremity trauma (e.g. hipfractures), older age, prolonged surgical procedures, criticallyill patients, incontinence, malnutrition. See Structured RiskAssessment and validated tools (Braden, Norton, Waterlow)b2. For infection: onset > 4 weeks, location near frequentlycontaminated areas (e.g, near anus), cardiovascular andendocrine conditions, malnutrition
(c) Blood supply: If PU/PI on lower extremity, conduct non-invasive arterial tests to rule out peripheral arterial disease. Seetable with values and interpretations in topic"How to SelectAdequate Compression Therapy Pressure Levels and Products".
(d) Differential diagnoses: see Table 3 (e) Determine healability: see Table 4(f) PU/PI classification/stages: see topic "PressureUlcers/Injuries - Classification/Staging". Stage drawings NPUAPcopyright & used with permission
ALGORITHM: ASSESSMENT
Pressure Ulcer / Injury (PU/PI)
©2019 Wound reference Inc. All rights reserved. Not intended to replacehealthcare professional judgment with respect to individual needs. Revised 02/17/2019
Determine:
Differential diagnoses (d)Healability: potential for ulcer to heal with conservative treatment (e)PU/PI classification/stages (f)
History and physical exam consistent with PU/PI? (a)Which risk factors led to development of PU/PI? (b1)
Are there risk factors for infection? (b2)If ulcer on lower extremity, is there adequate blood supply to the ulcer? (c)
Patient's and caregiver's concerns?
Other Diagnosis
Manageaccording to
likelydifferentialdiagnosis
NEW ULCER
Quality Measures
See Algorithm for Treatment of PU/PI (coming soon)
Stage 1 Non-blanchable
erythema of intactskin
Stage 2 Partial-thickness
skin loss withexposed dermis
Stage 3 Full-thicknessskin loss (no
exposed bones,cartilage, tendon
Stage 4 Full-thickness skin
and tissue loss(exposed bones,cartilage, tendon)
UnstageablePU/PI
Obscured full-thickness skin and
tissue loss(covered with
slough, eschar)
Deep TissueInjury (DTI)
Persistent non-blanchable deepred, maroon or
purple discoloration
PU/PI Stages drawings by NPUAP copyright & used with permission

Table 1. History and Physical Examination
History focused on identification of risk factors for development of PU/PI and infection
See detailed framework for chief complaint and history of present illness, medications, social history,review of systems. Conduct a structured risk assessment with validated tools (e.g.“Braden Scale for Predicting PressureSore Risk”) and clinical judgement
Patient's and caregiver's concerns
Pain, depression, social and financial support, ability/willingness to adhere to care plan. Resources: Wound-Quality of Life (QoL) and patient-reported Wound Outcome, validated painmeasurement tools (CRIES, FLACC, FACES, Braden Scale)
Nutritional Assessment
Complete food log covering 2-3 days, BMIMalnutrition (2 out of the following 6 parameters): Insufficient energy intake, Weight loss, Loss ofmuscle mass, Loss of subcutaneous fat, Localized or generalized fluid accumulation that may maskweight loss, Decreased functional status measured by hand grip Labs: albumin, pre-albumin, HbA1c, blood glucose, complete blood count, C‐reactive protein, ESRStandardized tools: "Nestlé MNA" and "Self-MNA®" It is important that a registered dietitian be involved in the evaluation if possible
Functional, Equipment, and Seating Evaluation
Assess level of activity in the last 24h, mobility (with/ without assistance), posture, neurological function,bowel and bladder control, pressure redistribution devices, sleeping surface, wheelchair, cushion, etcConsider ordering a Physical Therapy or Occupational Therapy Evaluation
Focused Physical Examination:
Rectum/Genitalia/Pelvic: incontinence associated dermatitis (consultation with nurse specialized incontinence recommended) Neurologic: mental status, motor, sensation, cerebellar function, bladder and bowel controlSkin: local edema, lymphedema, scars, erythema, ecchymosis, dermatitis, skin tears, signs of abuse orneglectIf PU/PI on lower extremity, perform non-invasive arterial tests. See table with values andinterpretations in topic "How to Select Adequate Compression Therapy Pressure Levels and Products".
Validated wound assessment tools:
Pressure Ulcer Scale for Healing (PUSH) Tool Bates-Jensen Wound Assessment Tool
Ulcer location, category/stage. See topic "Pressure Ulcers/Injuries - Classification/Staging"
Complications: Local/ spreading/ systemic infection, fistulas, amyloidosis, heterotopic calcification, malignancy
Table 3. PU/PI Differential Diagnoses
Diabetic foot ulcer, arterial ulcer, venous ulcer, inflammatory ulcer (e.g.pyoderma gangrenosum), erythema that blanches on compression, moisture-associated dermatitis, skin tears, tape burns, excoriationsPatient may also have PU/PI with mixed etiology
Table 4. Determining Healability of PU/PI
Healable wound: the cause is corrected, there is enough blood supply to heal;moist interactive healing Maintenance wound: the wound could heal, but the cause is not correcteddue to patient unwillingness to adhere to treatment or a lack of required systemresources Non-healable wound: the patient is ill or may have negative protein balance orinadequate blood supply that is not bypassable or dilatable
National Pressure Ulcer Advisory Panel (NPUAP), European Pressure Ulcer Advisory Panel (EPUAP), and Pan Pacific Pressure Injury Alliance (PPPIA) et al. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guidelines and Quick ReferenceGuide. 2014Wound, Ostomy and Continence Nurses Society-Wound Guidelines Task Force. et al. WOCN 2016 Guideline for Prevention and Management of Pressure Injuries (Ulcers): An Executive Summary. Journal of wound, ostomy, and continence nursing.2017;volume 44(3):241-246.Gould L, Stuntz M, Giovannelli M, Ahmad A, Aslam R, Mullen-Fortino M, Whitney JD, Calhoun J, Kirsner RS, Gordillo GM et al. Wound Healing Society 2015 update on guidelines for pressure ulcers. Wound repair and regeneration. 2016;volume24(1):145-62.Sibbald RG, Elliott JA, Ayello EA et al. Optimizing the Moisture Management Tightrope with Wound Bed Preparation 2015©. Advances in skin & wound care. 2015;28(10):466-76; quiz 477-8.Rubayi S. Reconstructive Plastic Surgery of Pressure Ulcers 2015th Edition, 2015
©2019 Wound reference Inc. All rights reserved. Not intended to replace healthcare professional judgment with respect to individual needs. Revised on 02/17/2019
Table 2. Workup
For all patients with PU/PI
Labs: White blood cells and differential (WBC), C-reactive protein anderythrocyte sedimentation rate (ESR), Complete metabolic panel, Coagulationpanel, Urinalysis and culture/sensitivity Radiographs: If indicated (e.g. PU/PI located on sacrum or trochanters) plain X-rays of the pelvis in the antero-posterior (AP) position, and bilateral hip X-ray inthe lateral position
For suspected soft tissue infection or non-healing ulcer:
Tissue biopsy or quantitative validated swab technique (e.g., Levine) forculture, obtained after debridement, ORChronic wound fluid protein analysis
For suspected osteomyelitis:
Bone biopsy for culture and histology: gold standard but invasive Imaging modalities: magnetic resonance imaging has the greatest sensitivity
Related Documents