Preseptal cellulitis Authors Christopher Gappy, MD Steven M Archer, MD Michael Barza, MD Section Editors Stephen B Calderwood, MD Jonathan Trobe, MD Morven S Edwards, MD Deputy Editor Allyson Bloom, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Sep 2015. | This topic last updated: Jun 24, 2015. INTRODUCTION — Preseptal cellulitis (sometimes called periorbital cellulitis) is an infection of the anterior portion of the eyelid, not involving the orbit or other ocular structures. In contrast, orbital cellulitis is an infection involving the contents of the orbit (fat and ocular muscles) but not the globe. Although preseptal and orbital cellulitis may be confused with one another because both can cause ocular pain and eyelid swelling and erythema, they have very different clinical implications. Preseptal cellulitis is generally a mild condition that rarely leads to serious complications, whereas orbital cellulitis may cause loss of vision and even loss of life. Orbital cellulitis can usually be distinguished from preseptal cellulitis by its clinical features (ophthalmoplegia, pain with eye movements, and proptosis) and by imaging studies. In cases in which the distinction is not clear, clinicians should treat patients as though they have orbital cellulitis. Both conditions are more common in children than in adults, and preseptal cellulitis is much more common than orbital cellulitis. The pathogenesis, microbiology, clinical manifestations, diagnosis, and treatment of preseptal cellulitis will be reviewed here. Orbital cellulitis and its complications, such as subperiosteal abscess and orbital abscess, are discussed separately. Orbital infections caused by fungi, mainly the Mucorales (which cause mucormycosis) andAspergillus spp and, much more rarely, Mycobacterium tuberculosis, are also presented elsewhere. (See "Orbital cellulitis" and "Mucormycosis (zygomycosis)" and"Epidemiology and clinical manifestations of invasive aspergillosis" and "Tuberculosis and the eye" .) TERMINOLOGY — Preseptal cellulitis and orbital cellulitis involve different anatomic sites, with preseptal cellulitis referring to infections of the soft tissues anterior to the orbital septum and orbital cellulitis referring to infections posterior to it (figure 1 ). Neither infection involves the globe. (See 'Anatomy' below.) There is some debate regarding the appropriate terminology for these infections. Some clinicians use the term "periorbital cellulitis" rather than "preseptal cellulitis" or use the terms interchangeably. We prefer the term "preseptal cellulitis" to make a clear distinction between this infection and the more serious infection, "orbital cellulitis." Orbital cellulitis is sometimes referred to as "postseptal cellulitis"; we favor the term "orbital cellulitis," and will use it throughout this topic. ANATOMY — Basic familiarity with the anatomy of the eye is fundamental to understanding the pathogenesis, clinical manifestations, and complications of preseptal and orbital cellulitis. The orbit is a cone-shaped structure, lying horizontally, with its apex in the skull. It is surrounded by paranasal sinuses, namely, the frontal (lying superior), ethmoid (medial) and maxillary (inferior) sinuses (figure 2 ). The orbit is lined by periosteum. The ethmoid sinuses are separated from the orbit by a paper-thin layer called the lamina papyracea, which contains many perforations for nerves and blood vessels as well as some natural fenestrations termed Zuckerkandl’s dehiscences. Th e most common route of infection of the orbit is by extension from the ethmoid sinuses, presumably through these perforations. The orbital septum is a membranous sheet that extends from the periosteum of the orbit to the tarsal plate and forms the anterior boundary of the orbital compartment (figure 1 ). As noted above, preseptal cellulitis involves the soft tissues anterior to the orbital septum. The superior and inferior ophthalmic veins drain blood directly into the cavernous sinus (figure 3 ). Because of this communication and because the inferior orbital veins are valveless, infection can pass readily from the orbit to intracranial structures [ 1 ]. EPIDEMIOLOGY — Preseptal cellulitis is much more common than orbital cellulitis. In two pediatric case series, 94 percent and 87 percent of cases, respectively, were diagnosed as preseptal cellulitis [ 2,3 ]; the remainder of cases were diagnosed as orbital cellulitis. Both infections are much more common in children than in adults; accordingly, most of the data regarding these infections comes from studies in children.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Preseptal cellulitis Authors
Christopher Gappy, MD Steven M Archer, MD Michael Barza, MD Section Editors
Stephen B Calderwood, MD Jonathan Trobe, MD Morven S Edwards, MD Deputy Editor
Allyson Bloom, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Sep 2015. | This topic last updated: Jun 24, 2015.
INTRODUCTION — Preseptal cellulitis (sometimes called periorbital cellulitis) is an infection of the anterior portion of the
eyelid, not involving the orbit or other ocular structures. In contrast, orbital cellulitis is an infection involving the contents of
the orbit (fat and ocular muscles) but not the globe. Although preseptal and orbital cellulitis may be confused with one
another because both can cause ocular pain and eyelid swelling and erythema, they have very different clinical
implications. Preseptal cellulitis is generally a mild condition that rarely leads to serious complications, whereas orbital
cellulitis may cause loss of vision and even loss of life. Orbital cellulitis can usually be distinguished from preseptal
cellulitis by its clinical features (ophthalmoplegia, pain with eye movements, and proptosis) and by imaging studies. In
cases in which the distinction is not clear, clinicians should treat patients as though they have orbital cellulitis. Both
conditions are more common in children than in adults, and preseptal cellulitis is much more common than orbital
cellulitis.
The pathogenesis, microbiology, clinical manifestations, diagnosis, and treatment of preseptal cellulitis will be reviewed
here. Orbital cellulitis and its complications, such as subperiosteal abscess and orbital abscess, are discussed separately.
Orbital infections caused by fungi, mainly the Mucorales (which cause mucormycosis) andAspergillus spp and, much
more rarely, Mycobacterium tuberculosis, are also presented elsewhere. (See "Orbital cellulitis" and "Mucormycosis
(zygomycosis)" and"Epidemiology and clinical manifestations of invasive aspergillosis" and "Tuberculosis and the eye".)
TERMINOLOGY — Preseptal cellulitis and orbital cellulitis involve different anatomic sites, with preseptal cellulitis
referring to infections of the soft tissues anterior to the orbital septum and orbital cellulitis referring to infections posterior
to it (figure 1). Neither infection involves the globe. (See 'Anatomy' below.)
There is some debate regarding the appropriate terminology for these infections. Some clinicians use the term "periorbital
cellulitis" rather than "preseptal cellulitis" or use the terms interchangeably. We prefer the term "preseptal cellulitis" to
make a clear distinction between this infection and the more serious infection, "orbital cellulitis." Orbital cellulitis is
sometimes referred to as "postseptal cellulitis"; we favor the term "orbital cellulitis," and will use it throughout this topic.
ANATOMY — Basic familiarity with the anatomy of the eye is fundamental to understanding the pathogenesis, clinical
manifestations, and complications of preseptal and orbital cellulitis. The orbit is a cone-shaped structure, lying
horizontally, with its apex in the skull. It is surrounded by paranasal sinuses, namely, the frontal (lying superior), ethmoid
(medial) and maxillary (inferior) sinuses (figure 2). The orbit is lined by periosteum. The ethmoid sinuses are separated
from the orbit by a paper-thin layer called the lamina papyracea, which contains many perforations for nerves and blood
vessels as well as some natural fenestrations termed Zuckerkandl’s dehiscences. The most common route of infection of
the orbit is by extension from the ethmoid sinuses, presumably through these perforations.
The orbital septum is a membranous sheet that extends from the periosteum of the orbit to the tarsal plate and forms the
anterior boundary of the orbital compartment (figure 1). As noted above, preseptal cellulitis involves the soft tissues
anterior to the orbital septum. The superior and inferior ophthalmic veins drain blood directly into the cavernous sinus
(figure 3). Because of this communication and because the inferior orbital veins are valveless, infection can pass readily
from the orbit to intracranial structures [1].
EPIDEMIOLOGY — Preseptal cellulitis is much more common than orbital cellulitis. In two pediatric case series, 94
percent and 87 percent of cases, respectively, were diagnosed as preseptal cellulitis [2,3]; the remainder of cases were
diagnosed as orbital cellulitis. Both infections are much more common in children than in adults; accordingly, most of the
data regarding these infections comes from studies in children.

It is important to distinguish between preseptal and orbital cellulitis because the complications, treatments, and outcomes
of the two entities are very different. (See'Clinical manifestations' below.)
PATHOGENESIS — Whereas the paranasal sinuses are the main source of infection in orbital cellulitis, many cases of
preseptal cellulitis (the proportion varying from study to study) arise from external sources. In one retrospective series of
315 children admitted to the hospital with preseptal or orbital cellulitis, sinusitis was the underlying condition in all 18
children with orbital cellulitis but in only 15 percent of those with preseptal cellulitis [2]. However, other studies have found
sinusitis to be the most common cause of preseptal cellulitis [4,5].
Other sites from which preseptal cellulitis may arise are the surrounding tissues of the face and eyelids following local
trauma [6,7], insect bites [7], animal bites [8], or foreign bodies. In one retrospective series of 104 patients with preseptal
cellulitis admitted to a tertiary care center, roughly 30 percent were thought to originate from each of the following causes:
acute dacryocystitis, sinusitis or upper respiratory tract infection, or trauma (including recent eyelid or strabismus surgery)
[9]. In another retrospective study that included 262 children with preseptal or orbital cellulitis, trauma (including insect
bites) was much more common in patients with preseptal cellulitis than in those with orbital cellulitis (40 versus 11
percent) [3]. Bacteremic seeding of the preseptal space is rare. It is occasionally seen in infants with bacteremia due
toStreptococcus pneumoniae, Streptococcus pyogenes, or Haemophilus influenzae.
MICROBIOLOGY — Data concerning the causes of preseptal cellulitis are limited. Blood cultures are almost always
negative, and it is usually difficult to obtain cultures from the infected site. Based on the available data, the most common
causes of preseptal cellulitis are Staphylococcus aureus, Streptococcus pneumoniae, other streptococci, and anaerobes
(table 1) [3,9], presumably depending on the site of origin of the infection.
Of S. aureus strains, community-acquired methicillin-resistant S. aureus (CA-MRSA) is thought to be an increasingly
common cause of infection. Although most cases of preseptal cellulitis caused by CA-MRSA have been published only as
case reports or retrospective series [10,11], the proportion of other skin and soft tissue infections caused by CA-MRSA
has increased dramatically. In a report of 422 adults presenting to emergency departments in 11 United States cities in
2004 with skin and soft tissue infections, 59 percent were caused by MRSA and 97 percent of cases of MRSA were
caused by CA-MRSA [12]. (See "Methicillin-resistant Staphylococcus aureus infection in adults: Epidemiology", section on
'Community-associated methicillin-resistant Staphylococcus aureus'.)
Although Haemophilus influenzae was previously a common cause of preseptal cellulitis, routine immunization of children
with the H. influenzae type b vaccine has caused a sharp decline in the incidence of this species as a cause of preseptal
cellulitis [2]. (See "Microbiology, epidemiology and treatment of Haemophilus influenzae".)
Infrequent causes of preseptal cellulitis include Acinetobacter species [13,14], Nocardia brasiliensis [15], Bacillus
anthracis [16], Pseudomonas aeruginosa [17],Neisseria gonorrhoeae [18], Proteus spp [19], Pasteurella
multocida [8], Mycobacterium tuberculosis [20], and Trichophyton spp (the cause of "ringworm") [21]. These pathogens
can usually be linked to specific exposures.
CLINICAL MANIFESTATIONS — Patients with preseptal cellulitis typically present with ocular pain, eyelid swelling, and
erythema (picture 1); importantly, preseptal and orbital cellulitis may be confused with one another because both
infections can cause these manifestations, but they have very different clinical implications [3,22-25]. In contrast to
preseptal cellulitis, orbital cellulitis causes swelling and inflammation of the extraocular muscles and fatty tissues within
the orbit, leading to pain with eye movements, proptosis, and ophthalmoplegia with diplopia. Chemosis (conjunctival
swelling) may occasionally occur in severe cases of preseptal cellulitis but is more common with orbital cellulitis. Orbital
cellulitis, but not preseptal cellulitis, may cause visual impairment. In a retrospective study that included 262 children,
fever occurred more commonly in those with orbital cellulitis than in those with preseptal cellulitis (94 versus 47 percent)
[3]. Leukocytosis may be present in patients with preseptal cellulitis but is not a sensitive indicator of this infection. The
clinical manifestations of orbital cellulitis are discussed in greater detail separately. (See "Orbital cellulitis", section on
'Clinical manifestations'.)
Serious complications are very rare in preseptal cellulitis. It is rare for untreated preseptal cellulitis to give rise to orbital
cellulitis and very rare for either infection to invade the globe (to produce endophthalmitis). However, some cases that are
initially diagnosed as preseptal cellulitis may, in fact, be orbital cellulitis. Therefore, clinicians must be vigilant for features
suggesting possible misdiagnosis. (See 'Diagnosis' below and "Orbital cellulitis", section on 'Diagnosis'.)

The tables indicate the clinical signs and symptoms associated with the two conditions (table 2 and table 3). Combined
with imaging studies, when indicated, these features usually allow for a reasonable degree of confidence in distinguishing
between the two entities. However, the clinical evaluation can be challenging in young children, who may not be able to
cooperate with a full examination.
DIFFERENTIAL DIAGNOSIS — The differential diagnosis of preseptal cellulitis includes:
●Orbital cellulitis (see "Orbital cellulitis")
●Insect bite
●Allergic response
●Hordeolum (stye)
●Conjunctivitis
It is critical to distinguish preseptal cellulitis from the more serious orbital cellulitis. (See "Orbital cellulitis", section on
'Diagnosis'.)
DIAGNOSIS — The diagnosis of preseptal cellulitis is based upon the history (eg, insect bite, local face and/or eyelid
trauma) and physical examination, but, in cases in which there is doubt, computed tomography (CT) scanning of the
orbits and sinuses is used to distinguish preseptal cellulitis from orbital cellulitis. The approach to diagnosis when a case
of preseptal cellulitis is difficult to distinguish from orbital cellulitis is discussed separately. (See "Orbital cellulitis", section
on 'Diagnosis'.)
Despite the low yield, we recommend obtaining blood cultures from patients with suspected preseptal cellulitis before the
administration of antibiotics.
Imaging studies — Contrast-enhanced CT scanning of the orbits and sinuses is helpful for distinguishing between
preseptal and orbital cellulitis. In preseptal cellulitis, there is swelling of the eyelid(s) but no proptosis, no fat strand ing of
the orbital contents, and no edema of the extraocular muscles. Sinusitis may be present in preseptal cellulitis but is
almost always present in orbital cellulitis. It is important to note that in some cases of orbital cellulitis, the CT scan
abnormalities may be subtle.
Imaging studies are indicated if any of the clinical signs or symptoms point to orbital cellulitis rather than preseptal
cellulitis. They are also indicated in patients with presumed preseptal cellulitis who exhibit marked eyelid swelling, fever,
and leukocytosis, or whose infection fails to show improvement after 24 to 48 hours of appropriate antibiotics. Imaging
studies in patients with suspected orbital cellulitis are discussed in detail separately. (See "Orbital cellulitis", section on
'Imaging studies'.)
TREATMENT — There are no randomized trials of antibiotic regimens for the treatment of preseptal cellulitis. Blood
cultures are rarely positive and cultures from the site of infection are difficult to obtain. Therefore, treatment is almost
always empiric and based upon knowledge of the common infecting organisms (Staphylococcus aureus,Streptococcus
pneumoniae, other streptococci and anaerobes) and their usual susceptibility patterns.
Adults and children older than one year of age with mild preseptal cellulitis and no signs of systemic toxicity can generally
be treated as outpatients with oral antibiotics provided that close follow-up can be ensured. Children younger than one
year of age, children who cannot cooperate fully for an examination, and patients who are severely ill should generally be
admitted to the hospital and managed according to the recommendations for orbital cellulitis. This is discussed in greater
detail separately. (See "Orbital cellulitis", section on 'Treatment'.)
It is important to note that patients with subtle clinical and/or radiographic findings suggesting that the orbit is involved
should be treated as though they have orbital cellulitis given the serious complications of this entity. Young children who
are not able to cooperate for a thorough examination should also be treated as though they have orbital cellulitis.
(See "Orbital cellulitis", section on 'Treatment'.)
Antibiotic regimens — The choice of antibiotics for empiric treatment has been made much more difficult by the
emergence of community-acquired methicillin-resistantS. aureus (CA-MRSA), which now constitute a substantial
proportion of community-acquired strains of S. aureus. Previously, amoxicillin-clavulanic acid, cefpodoxime,
and cefdinir were excellent choices. However, these agents do not have activity against CA-MRSA. Orally administered
drugs that have good activity against most strains of CA-MRSA include trimethoprim-sulfamethoxazole, clindamycin, and
tetracyclines (eg, doxycycline). However, trimethoprim-sulfamethoxazole and doxycycline are not reliably effective for

group A streptococcal infections, and doxycycline is not approved for use in children under the age of eight years, and
should be used with caution in such patients.
Therefore, we suggest one of the following regimens for empiric oral treatment of preseptal cellulitis:
●Clindamycin:
•In children: 30 to 40 mg/kg per day in three to four equally divided doses, not to exceed 1.8 grams per day
[26]
•In adults: 300 mg every eight hours) monotherapy or
●Trimethoprim-sulfamethoxazole (TMP-SMX; in children: 8 to 12 mg/kg per day of the trimethoprim component
divided every 12 hours; in adults: 8 mg/kg per day of the trimethoprim component divided every 8 or 12 hours [one
double strength tablet contains 160 mg of trimethoprim; as examples, TMP-SMX can be given as one double
strength tablet every 8 hours or two double strength tablets every 12 hours depending on the patient's
weight]) plus one of the following:
•Amoxicillin
-In children: usual dosing is 45 mg/kg per day divided every 12 hours; dosing for severe infections or
when penicillin-resistant Streptococcus pneumoniaeis a concern is 80 to 100 mg/kg per day in divided
doses every eight hours
-In adults: 875 mg orally every 12 hours or
•Amoxicillin-clavulanic acid
-In children: usual dosing is 45 mg/kg per day divided every 12 hours; dosing for severe infections or
when penicillin-resistant S. pneumoniae is a concern (using the 600 mg/5 mL suspension) is
90 mg/kg per day divided every 12 hours
-In adults: 875 mg every 12 hours or
•Cefpodoxime
-In children <12 years of age: 10 mg/kg per day divided every 12 hours, usual maximum dose 200 mg; in
children ≥12 years and adolescents: 400 mg every 12 hours
-In adults: 400 mg every 12 hours or
•Cefdinir
-In children: 7 mg/kg twice daily, maximum daily dose 600 mg
-In adults: 300 mg twice daily
The recommendation to use clindamycin alone is based primarily on published susceptibility data rather than on clinical
efficacy data for patients with preseptal cellulitis. However, the drug has shown good efficacy for skin and soft tissue
infections caused by staphylococci and streptococci [26]. (See "Treatment of skin and soft tissue infections due to
methicillin-resistant Staphylococcus aureus in adults", section on 'Clindamycin' and "Evaluation and management of
suspected methicillin-resistant Staphylococcus aureus skin and soft tissue infections in children".)
If the patient has not been immunized against Haemophilus influenzae, one of the combination regimens should be used
in order to insure coverage for this organism.
Topical antibiotics have no role in the treatment of this infection.
Response to therapy — Preseptal cellulitis typically responds rapidly and completely to appropriate antibiotics.
Outpatients whose infections fail to show signs of improvement in 24 hours should generally be hospitalized, treated with
broad-spectrum intravenous antibiotics, and undergo a computed tomography (CT) scan to evaluate for orbital cellulitis
and its complications. (See "Orbital cellulitis", section on 'Treatment'.)
Duration — There are no controlled trials evaluating the duration of antimicrobial therapy in preseptal cellulitis. Treatment
recommendations are based on small case series. We generally recommend a duration of 7 to 10 days [27,28], but if
signs of cellulitis persist at the end of this period, treatment should be continued until the eyelid erythema and swelling
have resolved or nearly resolved.
Recurrent preseptal cellulitis — Preseptal cellulitis rarely recurs. When it does, it is usually due to an underlying cause
that has not been diagnosed [29,30]. A case series of six patients with recurrent preseptal cellulitis, defined as three or
more episodes within a one year period with complete resolution between episodes, identified the underlying cause in two

patients as environmental allergies, and in one patient each as recurrent sinusitis, herpes simplex infection, contact
dermatitis to cosmetics, and Munchausen’s syndrome [29]. An anatomic abnormality of the sinuses may also predispose
to recurrent preseptal cellulitis [30].
SUMMARY AND RECOMMENDATIONS — Preseptal cellulitis and orbital cellulitis involve different anatomic sites, with
preseptal cellulitis referring to infections of the soft tissues anterior to the orbital septum and orbital cellulitis referring to
infections posterior to it (figure 1). Orbital cellulitis involves the muscles and fat located within the orbit. Although preseptal
and orbital cellulitis may be confused with one another because both can cause ocular pain and eyelid swelling and
erythema, they have very different clinical implications. Preseptal cellulitis is generally a mild condition that rarely leads to
serious complications, whereas orbital cellulitis may cause loss of vision and even loss of life. Orbital cellulitis can usually
be distinguished from preseptal cellulitis by its clinical features (ophthalmoplegia, pain with eye movements, and
proptosis) and by imaging studies; in cases in which the distinction is not clear, clinicians should treat patients as though
they have orbital cellulitis. Both conditions are more common in children than in adults. (See 'Introduction' above
and 'Terminology' above.)
●Preseptal cellulitis arises most commonly from sinusitis or a contiguous infection of the soft tissues of the face and
eyelids secondary to local trauma, insect or animal bites, or foreign bodies. (See 'Pathogenesis' above.)
●The most common causes of preseptal cellulitis are Streptococcus pneumoniae and other
streptococci, Staphylococcus aureus (including community-acquired methicillin-resistant S. aureus [CA-MRSA]), and
anaerobes (table 1). (See 'Microbiology' above.)
●The diagnosis of preseptal cellulitis is based upon the history (eg, insect bite, local face and/or eyelid trauma) and
physical examination. However, in cases in which there is doubt, computed tomography (CT) scanning of the orbits
and sinuses can usually distinguish preseptal cellulitis from orbital cellulitis. (See 'Diagnosis'above.)
●During the initial evaluation, it is critical to distinguish preseptal cellulitis from the more serious orbital cellulitis
(table 2 and table 3). Although both preseptal cellulitis and orbital cellulitis typically cause eyelid swelling and
erythema, the presence of ophthalmoplegia, pain with eye movements, chemosis, and/or proptosis occur only with
orbital cellulitis. (See 'Clinical manifestations' above.)
●Adults and children older than one year of age with mild preseptal cellulitis can be managed on an outpatient
basis, provided that the patient has no signs of systemic toxicity and close follow-up is ensured. In these cases, we
recommend treatment with oral antibiotics with activity against S. aureus (including MRSA) and streptococci, such
as clindamycin monotherapy or combination therapy with trimethoprim-sulfamethoxazole plus one of the following
agents: amoxicillin, amoxicillin-clavulanic acid, cefpodoxime, or cefdinir (Grade 2B). If the patient has not been
immunized against Haemophilus influenzae, one of the combination regimens should be used. (See 'Antibiotic
regimens' above.)
●We generally recommend a treatment duration of 7 to 10 days, but if signs of cellulitis persist at the end of this
period, treatment should be continued until the erythema and swelling have resolved or nearly resolved.
(See 'Duration' above.)
●Patients younger than one year of age and those who are severely ill should be admitted to the hospital and
managed according to the recommendations for orbital cellulitis. Patients with subtle clinical and/or radiographic
findings suggesting that the orbit is involved, as well as young children who are not able to cooperate for a thorough
examination, should also be treated as though they have orbital cellulitis given the serious complications of this
entity. (See "Orbital cellulitis", section on 'Treatment'.)
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Zhang J, Stringer MD. Ophthalmic and facial veins are not valveless. Clin Experiment Ophthalmol 2010; 38:502. 2. Ambati BK, Ambati J, Azar N, et al. Periorbital and orbital cellulitis before and after the advent of Haemophilus
influenzae type B vaccination. Ophthalmology 2000; 107:1450. 3. Botting AM, McIntosh D, Mahadevan M. Paediatric pre- and post-septal peri-orbital infections are different
diseases. A retrospective review of 262 cases. Int J Pediatr Otorhinolaryngol 2008; 72:377. 4. Mills RP, Kartush JM. Orbital wall thickness and the spread of infection from the paranasal sinuses. Clin
Otolaryngol Allied Sci 1985; 10:209. 5. Jackson K, Baker SR. Periorbital cellulitis. Head Neck Surg 1987; 9:227. 6. Ganesh A, Venugopalan P. Preseptal orbital cellulitis following oral trauma. J Pediatr Ophthalmol Strabismus
2000; 37:315.

7. Smith TF, O'Day D, Wright PF. Clinical implications of preseptal (periorbital) cellulitis in childhood. Pediatrics 1978; 62:1006.
8. Hutcheson KA, Magbalon M. Periocular abscess and cellulitis from Pasteurella multocida in a healthy child. Am J Ophthalmol 1999; 128:514.
9. Chaudhry IA, Shamsi FA, Elzaridi E, et al. Inpatient preseptal cellulitis: experience from a tertiary eye care centre. Br J Ophthalmol 2008; 92:1337.
10. Charalampidou S, Connell P, Fennell J, et al. Preseptal cellulitis caused by community acquired methicillin resistant Staphylococcus aureus (CAMRSA). Br J Ophthalmol 2007; 91:1723.
11. Blomquist PH. Methicillin-resistant Staphylococcus aureus infections of the eye and orbit (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc 2006; 104:322.
12. Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med 2006; 355:666.
13. Miller J. Acinetobacter as a causative agent in preseptal cellulitis. Optometry 2005; 76:176. 14. Mathews D, Mathews JP, Kwartz J, Inkster C. Preseptal cellulitis caused by Acinetobacter lwoffi. Indian J
Ophthalmol 2005; 53:213. 15. Brannan PA, Kersten RC, Hudak DT, et al. Primary Nocardia brasiliensis of the eyelid. Am J Ophthalmol 2004;
138:498. 16. Caça I, Cakmak SS, Unlü K, et al. Cutaneous anthrax on eyelids. Jpn J Ophthalmol 2004; 48:268. 17. Milstone AM, Ruff AJ, Yeamans C, Higman MA. Pseudomonas aeruginosa pre-septal cellulitis and bacteremia in
a pediatric oncology patient. Pediatr Blood Cancer 2005; 45:353; discussion 354. 18. Raja NS, Singh NN. Bilateral orbital cellulitis due to Neisseria gonorrhoeae and Staphylococcus aureus: a
previously unreported case. J Med Microbiol 2005; 54:609. 19. Sears JM, Gabriel HM, Veith J. Preseptal cellulitis secondary to Proteus species: a case report and review. J Am
Optom Assoc 1999; 70:661. 20. Raina UK, Jain S, Monga S, et al. Tubercular preseptal cellulitis in children: a presenting feature of underlying
systemic tuberculosis. Ophthalmology 2004; 111:291. 21. Velazquez AJ, Goldstein MH, Driebe WT. Preseptal cellulitis caused by trichophyton (ringworm). Cornea 2002;
21:312. 22. Seltz LB, Smith J, Durairaj VD, et al. Microbiology and antibiotic management of orbital cellulitis. Pediatrics 2011;
127:e566. 23. Nageswaran S, Woods CR, Benjamin DK Jr, et al. Orbital cellulitis in children. Pediatr Infect Dis J 2006; 25:695. 24. Durand, ML. Periocular infections. In: Principles and Practice of Infectious Diseases, 7th ed, Mandell, GL,
Bennett, et al. (Eds), Churchill Livingstone Elsevier, Philadelphia 2010. p.1569. 25. Sobol SE, Marchand J, Tewfik TL, et al. Orbital complications of sinusitis in children. J Otolaryngol 2002; 31:131. 26. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for
the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 2011; 52:e18. 27. Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol Allied Sci
2004; 29:725. 28. Uzcátegui N, Warman R, Smith A, Howard CW. Clinical practice guidelines for the management of orbital
cellulitis. J Pediatr Ophthalmol Strabismus 1998; 35:73. 29. Sorin A, April MM, Ward RF. Recurrent periorbital cellulitis: an unusual clinical entity. Otolaryngol Head Neck
Surg 2006; 134:153. 30. Karkos PD, Karagama Y, Karkanevatos A, Srinivasan V. Recurrent periorbital cellulitis in a child. A random event
or an underlying anatomical abnormality? Int J Pediatr Otorhinolaryngol 2004; 68:1529.
Topic 16650 Version 13.0

The orbital septum
Diagram showing the proximity of the periosteum in relation to the orbital septum. Orbital cellulitis arises
posterior to the orbital septum
Medial wall of the left orbit (lateral wall removed)
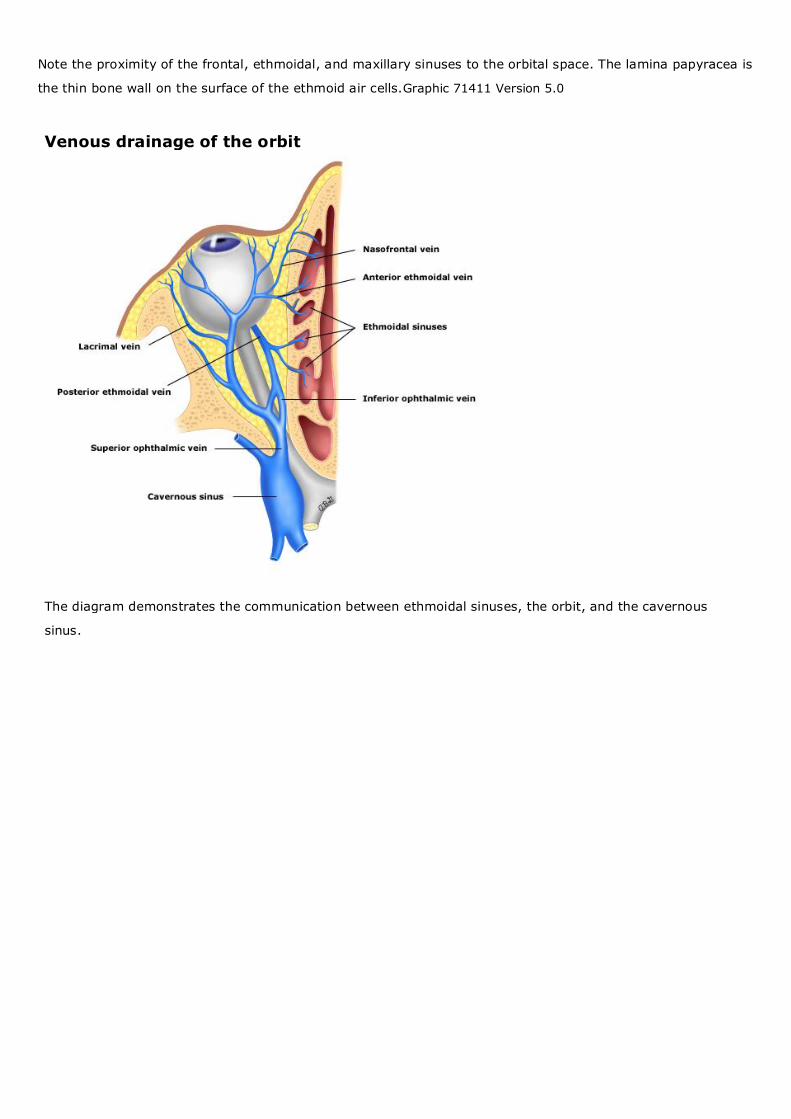
Note the proximity of the frontal, ethmoidal, and maxillary sinuses to the orbital space. The lamina papyracea is
the thin bone wall on the surface of the ethmoid air cells.Graphic 71411 Version 5.0
Venous drainage of the orbit
The diagram demonstrates the communication between ethmoidal sinuses, the orbit, and the cavernous
sinus.

Microbiology of preseptal and orbital cellulitis*
Preseptal cellulitis Orbital cellulitis
Chaudhry,
et al[1]
Botting, et
al[2]
McKinley,
et al[3] Seltz, et al[4]
Nageswaran, et
al[5]
Botting,
et al[2] Goytia, et al[6]
Number of patients 104 227 38 94 41 35 85
Number of patients with
a positive culture
(except¶)
36 53¶ 24 29 20 11¶ 29¶
Staphylococcus aureus Δ 32 11 8 3 7 14
MSSA NR NR 3 7 NR NR 7
MRSA NR NR 8 1 NR NR 7
Alpha-hemolytic
streptococci (includingS.
pneumoniae) or non-
hemolytic streptococci
Δ 4 7 15
Beta-hemolytic
streptococci (includingS.
pyogenes)
Δ 7 13 6 5 3 10
Streptococcus
anginosus (formerly S.
milleri)
2 14 2
Rothia mucilaginosa 1
Haemophilus influenzae 8 5 3 3 3 5
Haemophilus
parainfluenzae
1
Klebsiella pneumoniae 3 1
Moraxella catarrhalis 1
Arcanobacterium spp 1 1
Eikenella corrodens 1 2
Anaerobes 2 2 8 4
Skin flora/contaminant 5 11◊ 12◊
Possible pathogen§ 10

Sites of culture Blood,
wound,
abscess
NR Blood,
orbital
abscess,
eye, sinus,
epidural
abscess,
nose
Blood,
sinus/orbit,
subdural
space
Orbital abscess,
subperiostial
abscess, sinus
NR Blood, endoscopic
sinus,
subperiosteal,
intraorbital
MSSA: methicillin-susceptible Staphylococcus aureus; MRSA: methicillin-resistant Staphylococcus aureus; NR: not
reported.* Results are reported as the number of cultures that grew a given organism. Some cultures grew >1
organism and some patients had >1 positive culture.¶ Results are reported as number of positive cultures (rather than
number of patients with a positive culture); some patients may have had >1 positive culture.Δ Staphylococcus spp
and Streptococcus spp were recovered from 26 (72 percent) of cultures, but the authors did not report the number of
positive cultures for individual species.◊ In McKinley, et al[3], coagulase-negative Staphylococcus spp was reported as
a recovered organism, but in Seltz, et al[4], this organism was classified as a contaminant. We have classified it as a
contaminant for both studies.§ The authors of this study classifed some (but not all) sinus/orbit cultures as possible
pathogens rather than true pathogens.
Orbital cellulitis
This young girl has erythema and edema in the preseptal area, which could be caused by either orbital
or preseptal infection.

Clinical features of preseptal and orbital cellulitis
Clinical feature Preseptal cellulitis Orbital cellulitis
Eyelid swelling with or without erythema Yes Yes
Eye pain/tenderness May be present Yes; may cause deep eye pain
Pain with eye movements No Yes
Proptosis No Usually, but may be subtle
Ophthalmoplegia +/- diplopia No Yes
Vision impairment No May be present*
Chemosis Rarely present May be present
Fever May be present Usually present

Clinical manifestations of preseptal and orbital cellulitis studies on admission
Study: Study design, patient population
Nageswaran, et
al[1]
:Retrospective,
children
Botting, et
al[2]
:Retrospective,
children
Chaudhry, et
al[3]
:Retrospective¶,
children and adults
Sobol, et al[4]
:Retrospective,
children
Seltz, et
al[5]
:Retrospective,
children
Type of cellulitis Type of cellulitis Type of cellulitis Type of cellulitis Type of cellulitis
Preseptal Orbital
(n = 41)
Preseptal
(n =
227)
Orbital
(n =
35)
Preseptal (n = 104) Orbital Preseptal
(n =
101)
Orbital
(n =
26)Δ
Preseptal Orbital
(n = 94)
Age (yrs)◊ 7.5
(range 0-
16)
3.9 7.5 19 (range 0-75) 3.8
(range 0-
16)
6.4
(range
0-13)
6 (range
0-18)
History of
trauma*
Excluded 89 (39) 4 (11) 28 Excluded
Eye pain and/or
tenderness
64 (62)
Eyelid swelling
+/– erythema
104 (100)
Proptosis 25 (61) 2 (0.9) 33
(94)
1 (1) 20
(77)
36 (38)
Ophthalmoplegia 19 (46) 1 (0.4) 4 (11) 1 (1) 20
(77)
45 (48)
Diplopia 2 (0.9) 19
(54)
Vision impaired 0 1 (3) 3 (3) 3 (11) 11 (12)
No
ophthalmologic
signs (proptosis,
ophthalmoplegia,
visual loss)
11 (27)
Chemosis 10 (11)
Fever 27 (66) 106 (47) 33
(94)
Children 52 percent;
adults 10 percent
59 (59) 18
(69)
63 (67)
White blood cell 19 (46)

count >15,000
Sinusitis§ 21 (9) 32
(91)
Ethmoid
sinusitis
40
(98)
30
(86)
22
(86)
87
(93)
Maxillary
sinusitis
29
(71)
21
(60)
22
(86)
84
(89)
Subperiosteal
abscess
24 (59) 12
(34)
Δ 44 (47)
Orbital abscess 10 (24) 2 (6) 0 8 (8)
>Surgical
procedure
29 (71) 11 (5) 8 (23) 52 (50)¶ 0 6 (23)
Δ
Results are reported as number of patients with a given finding (percent). * Eg, insect bites, scratches. ¶ This study
involved patients referred to a tertiary care hospital in Saudi Arabia. 38.5 percent of patients were >16 years of age.
Many had acute dacryocystitis, trauma, or recent surgery, which is probably why such a large proportion of patients
underwent surgical procedures. Δ In this study, 12 cases of children with subperiosteal abscess were evaluated
separately; these cases are not shown in the table, but the findings were similar to those with simple orbital cellulitis. Of
patients with orbital cellulitis or subperiosteal abscess, 12 of 38 (32 percent) had a subperiosteal abscess; 66 percent of
patients with subperiosteal abscess underwent surgery. ◊ The mean age is reported for all studies except for Seltz et
al[5]; this study reported the median age. § The ethmoid and maxillary sinuses were involved most commonly, but some
patients had frontal sinusitis and/or sphenoid sinusitis; many patients had involvement of multiple sinuses.

Orbital cellulitis Authors
Christopher Gappy, MD Steven M Archer, MD Michael Barza, MD Section Editors
Stephen B Calderwood, MD Morven S Edwards, MD Jonathan Trobe, MD Deputy Editor
Allyson Bloom, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Sep 2015. | This topic last updated: Jun 24, 2015.
INTRODUCTION — Orbital cellulitis is an infection involving the contents of the orbit (fat and ocular muscles). I t must be
distinguished from preseptal cellulitis (sometimes called periorbital cellulitis), which is an infection of the anterior port ion of
the eyelid. Neither infection involves the globe itself.
Although preseptal and orbital cellulitis may be confused with one another because both can cause ocular pain and eyelid
swelling and erythema, they have very different clinical implications. Preseptal cellulitis is generally a mild condition that
rarely leads to serious complications, whereas orbital cellulitis may cause loss of vision and even loss of life. Orbital
cellulitis can usually be distinguished from preseptal cellulitis by its clinical features (ophthalmoplegia, pain with eye
movements, and proptosis) and by imaging studies; in cases in which the distinction is not clear, clinicians should treat
patients as though they have orbital cellulitis. Both conditions are more common in children than in adults, and preseptal
cellulitis is much more common than orbital cellulitis.
The pathogenesis, microbiology, clinical manifestations, complications, diagnosis, and treatment of orbital cellulitis will be
reviewed here. Preseptal cellulitis is discussed separately. Orbital infections caused by fungi, mainly the Mucorales
(which cause mucormycosis) and Aspergillus spp, and, much more rarely, Mycobacterium tuberculosis are also
presented separately. (See "Preseptal cellulitis" and "Mucormycosis (zygomycosis)" and "Epidemiology and clinical
manifestations of invasive aspergillosis" and "Tuberculosis and the eye".)
TERMINOLOGY — Preseptal cellulitis and orbital cellulitis involve different anatomic sites, with preseptal cellulitis
referring to infections of the soft tissues anterior to the orbital septum, and orbital cellulitis referring to infections posterior
to it (figure 1). Orbital cellulitis involves the muscle and fat located within the orbit. Orbital cellulitis does not involve the
globe. (See 'Anatomy' below and "Preseptal cellulitis", section on 'Anatomy'.)
There is some debate regarding the appropriate terminology for these infections. Some clinicians use the term "periorbital
cellulitis" rather than "preseptal cellulitis" or use the terms interchangeably. We prefer the term "preseptal cellulitis" to
make a clear distinction between this infection and the more serious infection, "orbital cellulitis." Orbital cellulitis is
sometimes referred to as "postseptal cellulitis"; we favor the term "orbital cellulitis," and will use it throughout this topic.
ANATOMY — Basic familiarity with the anatomy of the eye is fundamental to understanding the pathogenesis, clinical
manifestations, and complications of orbital cellulitis. The orbit is a cone-shaped structure, lying horizontally, with its apex
in the skull. It is surrounded by paranasal sinuses, namely, the frontal (lying superior), ethmoid (medial) and maxillary
(inferior) sinuses (figure 2). The orbit is lined by periosteum. The ethmoid sinuses are separated from the orbit by a paper-
thin layer called the lamina papyracea, which contains many perforations for nerves and blood vessels as well as some
natural fenestrations termed Zuckerkandl's dehiscences. The most common route of infection of the orbit is by extension
from the ethmoid sinuses, presumably through these perforations.
The orbital septum is a membranous sheet that extends from the periosteum of the orbit to the tarsal plate and forms the
anterior boundary of the orbital compartment (figure 1). The superior and inferior orbital veins drain blood directly into the
cavernous sinus (figure 3). Because of this communication and because the inferior orbital veins are valveless, infection
can pass readily from the orbit to intracranial structures [1].
EPIDEMIOLOGY AND PATHOGENESIS — Orbital cellulitis is much more common in young children than in older
children or adults. Orbital cellulitis is an uncommon complication of bacterial rhinosinusitis, but rhinosinusitis is the source
of most cases of orbital cellulitis; coexisting rhinosinusitis is present in 86 to 98 percent of cases of orbital cellulitis [2-5].
Ethmoid sinusitis and pansinusitis are the forms of rhinosinusitis most likely to lead to orbital cellulitis. (See "Acute

sinusitis and rhinosinusitis in adults: Clinical manifestations and diagnosis" and "Acute bacterial rhinosinusitis in children:
Clinical features and diagnosis", section on 'Complications'.)
As has been noted above, the ethmoid sinuses are separated from the orbit by the lamina papyracea, a thin structure with
many fenestrations. Computed tomography (CT) scanning often shows the predominant site of inflammation to be the
medial aspect of the orbit, adjacent to the ethmoid sinuses, and subperiosteal abscesses most often occur in the same
location (figure 2). (See 'Anatomy' above and "Preseptal cellulitis", section on 'Anatomy'.)
Although bacterial rhinosinusitis is the most common cause of orbital cellulitis, other potential causes are:
●Ophthalmic surgery, including strabismus surgery [6], blepharoplasty [7], radial keratotomy [8], and retinal surgery.
●Peribulbar anesthesia [9,10].
●Orbital trauma with fracture or foreign body [11,12].
●Dacryocystitis [13,14]. (see "Congenital nasolacrimal duct obstruction (dacryostenosis) and dacryocystocele",
section on 'Acute dacryocystitis')
●Infection of the teeth [15], middle ear [16], or face.
●An infected mucocele that erodes into the orbit [17].
Fungal rhinosinusitis can also lead to orbital cellulitis. (See 'Fungi and mycobacteria' below and "Fungal rhinosinusitis".)
MICROBIOLOGY — The causative organisms of orbital cellulitis are often difficult to identify. Cultures from the orbit are
only obtained if surgical intervention is needed, usually to drain an abscess. Sinus cultures obtained during surgery can
be used to guide antimicrobial therapy [18], but may not accurately reflect the pathogen(s) in the orbit. Blood cultures are
sometimes positive in children, the percentages ranging from 0 to 33 percent in various retrospective series [19-23]. They
are rarely positive in adults. In one series of patients with orbital cellulitis, blood cultures were positive in 33 percent of
children younger than four years of age but in only 5 percent of adults [20].
Bacteria — The most commonly identified pathogens in orbital cellulitis are Staphylococcus aureus and streptococci
(table 1) [2-4,24]. In one series of 94 children admitted to a tertiary care children's hospital with orbital cellulitis between
2004 and 2009, members of the Streptococcus anginosus (milleri) group were the most commonly identified pathogens
(15 percent) followed by S. aureus (9 percent), group A beta-hemolytic streptococci (Streptococcus pyogenes, 6 percent),
and Streptococcus pneumoniae (4 percent) [3]. Only one patient had methicillin-resistant S. aureus (MRSA) infection but
one would expect an increasing proportion of MRSA infections given the rising prevalence of community-acquired MRSA
(CA-MRSA) among strains of S. aureus. Cases of neonatal and infantile orbital cellulitis caused by CA-MRSA have been
reported [25].
Uncommon causes of orbital cellulitis include Haemophilus influenzae and nonspore-forming anaerobes [24,26],
Aeromonas hydrophila [27], Pseudomonas aeruginosa [28] and Eikenella corrodens [29]. H. influenzae type b, formerly
an important cause of orbital cellulitis in children, has become rare with the widespread use of the vaccine [24,30,31].
Some cases of orbital cellulitis are polymicrobial, often with a combination of aerobic and anaerobic bacteria. As an
example, in a study of 20 children with orbital cellulitis who had positive cultures from specimens obtained during surgery
(from an orbital or subperiosteal abscess and/or a paranasal sinus), seven (35 percent) had more than one organism
isolated [4]. Two small studies have observed polymicrobial infections in all patients [32,33].
Fungi and mycobacteria — Although most cases of orbital cellulitis are caused by bacteria, fungi, especially Mucorales
(which causes mucormycosis) and Aspergillus spp can cause life-threatening, invasive orbital infections. Mucormycosis
and invasive aspergillosis should be considered in patients with defects in host defenses. Mucormycosis primarily affects
patients with diabetic ketoacidosis and sometimes in patients with renal acidosis. Aspergillus infection of the orbit occurs
in patients with severe neutropenia or other immune deficiencies, including HIV infection. These infections are discussed
briefly below and more fully elsewhere. (See 'Diagnosis' below and "Mucormycosis (zygomycosis)" and "Fungal
rhinosinusitis" and "Epidemiology and clinical manifestations of invasive aspergillosis".)
Fungal causes of orbital cellulitis have been reported rarely in apparently immunocompetent infants [34].
Rarely, fungal pathogens other than the Mucorales or Aspergillus spp [35] or mycobacteria (especially Mycobacterium
tuberculosis) cause orbital infections. (See"Tuberculosis and the eye".)

CLINICAL MANIFESTATIONS — It is important to distinguish preseptal from orbital cellulitis because the two conditions
have very different clinical implications (table 2and table 3) [2-5,36]. Both orbital cellulitis and preseptal cellulitis cause
ocular pain and eyelid swelling with erythema (picture 1); in some cases of orbital cellulitis, eyelid erythema is absent.
Only orbital cellulitis causes swelling and inflammation of the extraocular muscles and fatty tissues within the orbit,
leading to pain with eye movements, proptosis, and ophthalmoplegia with diplopia. Chemosis (conjunctival swelling) may
occasionally occur in severe cases of preseptal cellulitis, but is more common with orbital cellulitis. In both conditions, but
especially in orbital cellulitis, there may be fever and peripheral leukocytosis with a predominance of neutrophils [2,37]. In
a retrospective study that included 262 children, fever occurred more commonly in those with orbital cellulitis than in those
with preseptal cellulitis (94 versus 47 percent) [2]. Rarely in orbital cellulitis, there may be visual impairment, and even
blindness, arising from inflammation or ischemia of the optic nerve [38].
The frequencies with which the signs and symptoms of orbital and preseptal cellulitis have been reported in different
studies are summarized in the table (table 2).
COMPLICATIONS — Although it is much less common than preseptal cellulitis, orbital cellulitis is a far more
consequential infection because it can be sight- or even life-threatening [36,39]. It can be complicated by subperiosteal
abscess, orbital abscess, vision loss, cavernous sinus thrombophlebitis, and/or brain abscess [18,36]. The most common
complications of orbital cellulitis are subperiosteal abscess and orbital abscess. These complications may develop rapidly;
therefore, close monitoring is indicated, with daily checks of visual acuity and assessment of the pupillary light reflex. A
sluggish or absent pupillary light reflex or a relative afferent pupillary defect indicates optic nerve involvement. Any
worsening of the patient's symptoms or signs should lead to a contrast-enhanced computed tomography (CT) scan of the
orbits and sinuses (or repeat CT if one was done earlier) to detect an abscess. (See 'Imaging studies' below.)
Orbital cellulitis results in loss of vision in 3 to 11 percent of patients and in death in 1 to 2 percent of patients [39].
Rare complications include cavernous sinus thrombosis and central retinal artery occlusion [40,41]. These complications
are discussed separately. (See "Septic dural sinus thrombosis", section on 'Septic cavernous sinus
thrombosis' and "Central and branch retinal artery occlusion".)
Subperiosteal abscess — Subperiosteal abscess is a fairly common complication of orbital cellulitis, occurring in 15 to
59 percent of cases in various retrospective series (table 2) [2-4,42]. It is difficult to distinguish subperiosteal abscess
from simple orbital cellulitis on clinical grounds, although marked displacement of the globe is suggestive of abscess.
Orbital imaging or surgery is necessary to make the diagnosis (image 1).
In some patients, a subperiosteal abscess, arising by extension from a sinus infection, precedes orbital cellulitis [43] or
occurs without orbital cellulitis. The abscess can present with minimal symptoms [44] until it ruptures into the orbit.
Subperiosteal abscesses in younger children tend to lie medially in the orbit [45], to be amenable to antibiotic treatment
without surgery (when small or in the form of poorly organized phlegmons) [18,32,45], and to contain a single aerobic
species [32]. Nonmedial abscesses in older children, and abscesses located superiorly (near the frontal sinus) appear to
be at highest risk for intracranial abscess. Abscesses in older patients usually contain mixtures of aerobic and anaerobic
microbes [33,46] and are more likely to require drainage than those in children.
Orbital abscess — Like subperiosteal abscess, orbital abscess is difficult to distinguish from uncomplicated orbital
cellulitis. It has been reported in up to 24 percent of cases of orbital cellulitis (table 2) [2-5,37]. Patients with orbital
abscess typically have more severe signs (proptosis, ophthalmoplegia) and symptoms (pain with eye movements) than
those with uncomplicated orbital cellulitis [37].
In a retrospective cohort study that included 298 otherwise healthy children admitted to a pediatric emergency department
who underwent CT scanning for suspected acute periorbital (preseptal) or orbital cellulitis, six (2 percent) were found to
have an orbital abscess [37]. Proptosis, pain with external ocular movement, and ophthalmoplegia were associated with
the presence of an orbital abscess, although 51 percent of patients with abscess did not have these findings. On
multivariate analysis, other factors associated with orbital abscess were a peripheral absolute neutrophil count (ANC)
>10,000 per microL, absence of conjunctivitis, periorbital edema, age >3 years, and previous antibiotic therapy.
(See 'Imaging studies' below.)
Extraorbital extension — Infection may rarely extend to the orbital apex, causing visual loss, or intracranially, causing
epidural or subdural empyema, brain abscess, meningitis, cavernous sinus thrombosis, or dural sinus thrombosis [18].
The visual loss associated with orbital cellulitis is thought to result from any of the following processes [38]:

●Optic neuritis as a result of inflammation from nearby infection
●Ischemia resulting from thrombophlebitis along the orbital veins
●Pressure resulting in central retinal artery occlusion
Intracranial complications may be heralded by severe headache, protracted vomiting, mental status changes and, in
patients with cavernous sinus thrombosis, cranial nerve palsies. Bilateral cranial nerve palsies can be a sign of bilateral
cavernous sinus thrombosis.
Intracranial extension may be more common in patients with frontal sinus involvement [18,47]; of note, frontal sinusitis
does not occur in young children since the frontal sinuses do not develop until at least six years of age, and do not
develop fully until mid-adolescence. (See "Acute bacterial rhinosinusitis in children: Clinical features and diagnosis",
section on 'Anatomy'.)
DIFFERENTIAL DIAGNOSIS — The differential diagnosis of orbital cellulitis includes a range of infectious and
noninfectious diseases. Although orbital cellulitis is most commonly caused by bacteria, in patients with certain risk
factors, fungal pathogens (and occasionally tuberculosis) should be considered. As noted below, it is critical to distinguish
preseptal cellulitis from the more serious orbital cellulitis. (See 'Diagnosis' below.)
Diseases that should be considered in the differential diagnosis of orbital cellulitis include:
●Preseptal cellulitis (See "Preseptal cellulitis".)
●Mucormycosis or aspergillosis involving the orbit (See "Mucormycosis (zygomycosis)" and "Epidemiology and
clinical manifestations of invasive aspergillosis".)
●Cavernous sinus thrombosis (See "Septic dural sinus thrombosis", section on 'Septic cavernous sinus
thrombosis'.)
●Herpes simplex or varicella zoster virus infections involving the eye (See "Herpes simplex keratitis" and "Clinical
manifestations of varicella-zoster virus infection: Herpes zoster", section on 'Herpes zoster ophthalmicus'.)
●Tuberculosis involving the orbit (See "Tuberculosis and the eye".)
●Endophthalmitis (See "Bacterial endophthalmitis" and "Treatment of endogenous endophthalmitis due to Candida
species" and "Treatment of exogenous endophthalmitis due to Candida species" and "Treatment of endophthalmitis
due to molds".)
●Tumors (eg, neuroblastoma [48], rhabdomyosarcoma [49])
●Orbital pseudotumor (idiopathic orbital inflammation) and Tolosa-Hunt syndrome [50,51] (See "Tolosa-Hunt
syndrome".)
●Posterior scleritis [52]
●Periocular dermoid cyst [53]
●Granulomatosis with polyangiitis (Wegener's disease) of the orbit [54]
●Trauma, including insect bites
●Allergic response [55,56]
●Hordeolum (stye)
●Severe conjunctivitis [57,58]
●Mucocele
●Thrombosed orbital varix
●Graves' disease
Certain findings are suggestive of the following serious conditions:
●Cavernous sinus thrombosis should be suspected if signs of orbital inflammation (redness and swelling of the
eyelids, ophthalmoplegia, decreased visual acuity) also occur in the contralateral eye. The second eye may become
involved a day or two after the first eye. The cranial nerves III, IV, V1, V
2, and VI pass through the cavernous sinus
and account for many of the manifestations. In addition, there may be decreased visual acuity due to edema of the
optic disc and there may be numbness over the upper face due to involvement of V1 and
V
2. These patients often
have sphenoid and posterior ethmoid sinusitis. This topic is discussed in greater detail elsewhere. (See "Septic dural
sinus thrombosis".)

●Mucormycosis and aspergillosis arise by spread from the upper airway, especially the posterior ethmoid or
sphenoid sinuses. Accordingly, they sometimes present as the "orbital apex syndrome" with ophthalmoplegia and
progressive visual loss, but otherwise minimal signs of inflammation (eg, mild eyelid swelling, little or no fever). They
may begin in indolent fashion, but may progress quickly to involve critical structures in the eye, nose, and brain.
(See "Mucormycosis (zygomycosis)", section on 'Rhino-orbital-cerebral mucormycosis' and "Epidemiology and
clinical manifestations of invasive aspergillosis", section on 'Rhinosinusitis'.)
●Endophthalmitis should be considered if visual acuity is reduced and the red reflex cannot be seen due to vitreous
haze.
DIAGNOSIS — The diagnosis of orbital cellulitis is suspected clinically and can be confirmed by computed tomography
(CT) scanning. During the initial evaluation, it is critical to distinguish preseptal cellulitis from the more serious orbital
cellulitis. It is also important to look for complications of orbital cellulitis, such as subperiosteal abscess, orbital abscess,
visual loss, and intracranial extension. Although both preseptal cellulitis and orbital cellulitis typically cause eyelid swelling
with or without erythema, the presence of ophthalmoplegia, pain with eye movement, and/or proptosis occur only with
orbital cellulitis. Another finding that is more common with orbital cellulitis, and rare or absent with preseptal cellulitis, is
chemosis. Fever is more common with orbital cellulitis than with preseptal cellulitis [2,4].
It is important for an ophthalmologist to evaluate patients with suspected orbital cellulitis in order to evaluate the
extraocular movements and visual acuity, and to assess for proptosis. In patients with extensive rhinosinusitis, an
otolaryngologist should generally be consulted as well. (See 'Surgery' below.)
Imaging studies — The goals of imaging studies are to support the diagnosis of orbital cellulitis and to search for an
abscess or other complications requiring surgical drainage. (See 'Surgery' below.)
Imaging modalities — CT scanning and magnetic resonance imaging (MRI) are useful for the diagnosis of orbital
cellulitis and its complications. There are no controlled trials comparing these modalities and the choice is usually based
on the availability of the test and on the clinical experience of the physicians involved. CT scanning of the orbits and
sinuses is used most commonly to evaluate for possible orbital cellulitis and its complications. MRI is superior to CT scan
in following the progression of soft tissue disease [59], but may not be readily available and may require sedation in
young children.
When cavernous sinus thrombosis is suspected, an imaging study that includes venography should be performed, such
as magnetic resonance (MR) venography or CT venography. These modalities are discussed in detail separately. MR
venography is used most commonly, and would show nonfilling of the cavernous sinus in patients with cavernous sinus
thrombosis. (See "Etiology, clinical features, and diagnosis of cerebral venous thrombosis", section on 'Diagnosis'.)
Imaging findings — In preseptal cellulitis, inflammation is confined to the eyelids. In orbital cellulitis, inflammation of
extraocular muscles, fat stranding, and anterior displacement of the globe are common findings. It is important to note
that some cases of orbital cellulitis will have subtle abnormalities by CT scan. There is almost always evidence of
rhinosinusitis, most commonly ethmoid sinusitis, and the most intense inflammatory response in the orbit is often seen
adjacent to the ethmoid sinus.
Subperiosteal abscesses and orbital abscesses appear as low-density collections on CT scan. Subperiosteal abscesses
lie between the periosteum and the wall of the bony sinus (image 1). Both types of abscesses, but especially
subperiosteal abscesses, are often found adjacent to the ethmoid sinus (figure 2).
Indications for imaging — Whether every patient with suspected orbital cellulitis should have a CT scan is controversial
[19,26,60,61]. Clinicians may be reluctant to obtain a CT scan due to concern about exposure of the pediatric patient to
radiation. Guidelines for the management of orbital cellulitis from the United Kingdom offer the following indications for CT
scanning: inability to assess vision; proptosis, ophthalmoplegia, bilateral edema, or deteriorating visual acuity; lack of
improvement after 24 hours of administration of intravenous antibiotics; "swinging" fevers not resolving within 36 hours; or
signs or symptoms of central nervous system (CNS) involvement [60].
In the study of CT scanning in children with suspected acute preseptal or orbital cellulitis described above, the presence
of edema beyond the eyelid margin or an absolute neutrophil count (ANC) >10,000 cell/microL were independent risk
factors for an orbital abscess; the authors concluded that the presence of either of these findings should necessitate an
expedited evaluation, including emergent CT scanning [37]. (See 'Orbital abscess' above.)
In addition, CT scanning should be done in all patients in whom surgical drainage is being considered [5].

Based on the studies and guidelines described above, we recommend that patients with suspected orbital cellulitis with
any of the following features undergo a contrast-enhanced CT scan of the orbits and sinuses:
●Proptosis
●Limitation of eye movements
●Pain with eye movements
●Double vision
●Vision loss
●Edema extending beyond the eyelid margin
●ANC >10,000 cell/microL
●Signs or symptoms of CNS involvement
●Inability to examine the patient fully (usually patients less than one year of age)
●Patients who do not begin to show improvement within 24 to 48 hours of initiating appropriate therapy
Microbiologic studies — Despite the low yield, we recommend obtaining blood cultures from patients with suspected
orbital cellulitis before the administration of antibiotics. If surgery is performed, the material obtained should be examined
by Gram stain and, in patients with risk factors for a fungal and/or mycobacterial etiology, by special stains for fungi and
mycobacteria. Cultures should be done for ordinary bacterial pathogens and, depending on the circumstances, fungi and
mycobacteria.
TREATMENT
Antibiotic regimens — Most patients with uncomplicated orbital cellulitis can be treated with antibiotics alone [4,5,62].
Even in patients who are initially treated with antibiotics alone, an ophthalmologist and an otolaryngologist should be
consulted because the physical examination requires ophthalmologic and/or otolaryngologic expertise and surgery is
sometimes required. (See 'Surgery' below.)
There are no randomized controlled trials evaluating empiric antibiotic regimens for the treatment of orbital cellulitis.
Treatment regimens are usually empiric and designed to address the most common pathogens because, in the absence
of surgical intervention, reliable culture results are difficult to obtain.
The usual choices are a parenterally administered broad-spectrum regimen aimed at S. aureus (including methicillin-
resistant S. aureus [MRSA]), S. pneumoniae and other streptococci, as well as gram-negative bacilli. When intracranial
extension is suspected, the regimen should also include coverage for anaerobes. Prompt treatment is important because
delayed intervention can lead to loss of vision and/or other serious complications [12,18,38].
Appropriate antibiotic regimens for empiric treatment in patients with normal renal function include a combination of:
●Vancomycin (in children: 40 to 60 mg/kg IV per day in three or four divided doses, maximum daily dose 4 g; in
adults: 30 to 60 mg/kg IV per day in two or three divided doses; the appropriate dose in adults requires
measurement of a trough concentration of vancomycin) plus one of the following:
•Ceftriaxone (in children: 50 mg/kg per dose IV once or twice per day [the higher dose should be used if
intracranial extension is suspected], maximum daily dose 4 g/day; in adults: 2 g IV every 24 hours [2 g IV every
12 hours if intracranial extension is suspected]) or
•Cefotaxime (in children: 150 to 200 mg/kg IV per day in three doses, maximum daily dose 12 g; in adults: 2 g
IV every four hours) or
•Ampicillin-sulbactam (in children: 300 mg/kg IV per day in four divided doses in children, maximum daily dose
12 g ampicillin-sulbactam [8 g ampicillin component]; in adults: 3 g IV every six hours) or
•Piperacillin-tazobactam (in children: 240 mg/kg per day in three divided doses, maximum daily dose 16 g
of piperacillin component; in adults: 4.5 g IV every six hours)
In patients with suspected intracranial extension who are being treated with ceftriaxone or cefotaxime, metronidazole (in
children: 30 mg/kg IV or orally per day in divided doses every 6 hours; in adults: 500 mg IV or orally every 8 hours) should
be added to include coverage for anaerobes. (See "Treatment and prognosis of bacterial brain abscess".)
Like vancomycin, daptomycin, linezolid and telavancin also are active against MRSA, but there is little experience using
them for orbital or intracranial infections. Moreover, linezolid concentrations in the central nervous system (CNS) have

been inconsistent in children and, accordingly, linezolid is not recommended for children with CNS infections [63].
Therefore, unless there is a contraindication to its use (eg, allergy), vancomycin is the preferred agent for MRSA
coverage of orbital cellulitis.
Adults and children with a serious allergy to penicillins and/or cephalosporins can be treated with a combination
of vancomycin and either ciprofloxacin or levofloxacin. In adults, ciprofloxacin is given at a dose of 400 mg IV twice daily
(or 500 to 750 mg orally twice daily) and levofloxacin is given at a dose of 500 to 750 mg IV or orally once daily. In
children, ciprofloxacin is given at a dose of 20 to 30 mg/kg per day divided every 12 hours with a maximum dose of 1.5
grams orally daily or 800 mg IV daily. Limited information regarding levofloxacin use in pediatric patients is available.
Some centers recommend a dose for infants ≥6 months and children <5 years of 10 mg/kgper dose every 12 hours, and
for children ≥5 years of 10 mg/kg per dose every 24 hours (maximum daily dose 500 mg).
Desensitization to a penicillin or cephalosporin may be considered in patients with a history of an IgE-mediated
(anaphylactic) reaction to these agents. (See "Penicillin allergy: Immediate reactions", section on 'Desensitization'.)
If a pathogen is retrieved on cultures of blood or orbital or subperiosteal aspirates, or from sinuses from cultures obtained
by endoscopic sinus surgery, treatment should be modified accordingly. For example, if a methicillin-susceptible strain of
S. aureus (MSSA) is recovered, treatment should be changed from vancomycin to oxacillin ornafcillin (in children: 100 to
200 mg/kg/day in divided doses every six hours, maximum daily dose 12 g; in adults: 2 g IV every four hours) because
these agents are more rapidly bactericidal for MSSA than vancomycin. Because these infections are often polymicrobial,
broad-spectrum therapy is usually continued until anaerobic culture data are available, usually for approximately five days
after collection.
Response to therapy — Patients should begin to show improvement within 24 to 48 hours of initiating appropriate
therapy; if this does not occur, repeat imaging should be performed to search for an abscess or another indication for
surgery. (See 'Surgery' below.)
Duration and switch to oral therapy — There have been no controlled trials to define the optimal duration of
antimicrobial therapy in orbital cellulitis or when to switch from intravenous to oral treatment. For patients with
uncomplicated orbital cellulitis (ie, without abscess or other complications) whose infection responds well, it is reasonable
to switch to oral therapy. We generally switch to oral therapy after the patient is afebrile and the eyelid and orbital findings
have begun to resolve substantially, which usually takes three to five days. When a range of doses can be used for an
oral antibiotic, we favor the higher end of the dose range if penicillin-resistantStreptococcus pneumoniae is a concern.
If there are no definitive culture data, appropriate empiric oral regimens include:
●Clindamycin (for adults: 300 mg every eight hours; for children: 30 to 40 mg/kg per day in three to four equally
divided doses, not to exceed 1.8 grams per day) alone [64].
●Either clindamycin or trimethoprim-sulfamethoxazole (for adults: 1 to 2 double strength tablets every 12 hours; for
children: 10 to 12 mg/kg per day of thetrimethoprim component divided every 12 hours) PLUS one of the following:
•Amoxicillin
-For adults: 875 mg orally every 12 hours
-For children: the dose range is 45 mg/kg per day (in divided doses every 12 hours) to 80 to
100 mg/kg per day in divided doses every eight hours (maximum dose 500 mg/dose) or
•Amoxicillin-clavulanic acid
-For adults: 875 mg every 12 hours
-For children: the dose range is 40 to 45 mg/kg per day (in divided does every 8 to 12 hours) to
90 mg/kg per day divided every 12 hours (using the 600mg/5 mL suspension) or
•Cefpodoxime
-For adults: 400 mg every 12 hours
-For children: 10 mg/kg per day divided every 12 hours, not to exceed 200 mg per dose or
•Cefdinir
-For adults: 300 mg twice daily
-For children: 7 mg/kg twice daily, not to exceed 600 mg/day
If definitive culture data are available, oral therapy should be directed against the infecting organism(s).

The recommendation to use clindamycin alone is based primarily on published susceptibility data rather than on clinical
efficacy data for patients with orbital cellulitis. However, the drug has shown good efficacy for skin and soft tissue
infections caused by staphylococci and streptococci [64]. (See "Treatment of skin and soft tissue infections due to
methicillin-resistant Staphylococcus aureus in adults", section on 'Clindamycin' and "Evaluation and management of
suspected methicillin-resistant Staphylococcus aureus skin and soft tissue infections in children".)
In adults and children who have serious allergies to penicillins and cephalosporins, appropriate alternatives to the agents
listed above are ciprofloxacin or levofloxacin. In adults, ciprofloxacin is given at a dose of 500 to 750 mg orally twice daily
and levofloxacin is given at a dose of 500 to 750 mg orally once daily. In children, ciprofloxacin is given at a dose of 20 to
30 mg/kg per day divided every 12 hours with a maximum dose of 1.5 grams orally daily. Limited information regarding
levofloxacin use in pediatric patients is available. Some centers recommend a levofloxacin dose for infants ≥6 months and
children <5 years of 10 mg/kg per dose every 12 hours, and for children ≥5 years of 10 mg/kg per dose every 24 hours
(maximum daily dose 500 mg). When a fluoroquinolone is used, it should be combined with clindamycin or trimethoprim-
sulfamethoxazole to cover MRSA. Desensitization to a penicillin or cephalosporin may be considered in patients with a
history of an IgE-mediated (anaphylactic) reaction to these agents. (See "Penicillin allergy: Immediate reactions", section
on 'Desensitization'.)
For patients with uncomplicated orbital cellulitis, we suggest that antibiotics be continued until all signs of orbital cellulitis
have resolved, and for a total of at least two to three weeks. A longer period (at least four weeks), is recommended for
patients with severe ethmoid sinusitis and bony destruction of the sinus [26,65]. The management of the complications of
orbital cellulitis is discussed separately. (See "Septic dural sinus thrombosis" and "Treatment and prognosis of bacterial
brain abscess" and"Epidural abscess".)
Surgery — The main indications for surgery are a poor response to antibiotic treatment, worsening visual acuity or
pupillary changes, or evidence of an abscess, especially a large abscess (>10 mm in diameter) or one that fails to
respond promptly to antibiotic treatment [66,67]. In some cases, drainage of affected sinuses is also required to control
the infection. The results of cultures and susceptibility testing from samples obtained during surgery can be used to tailor
therapy.
Medial subperiosteal abscesses in children often respond to medical therapy without surgery [32,45]. In one series of 68
children with subperiosteal abscess, only 21 (31 percent) underwent surgery [42]. Those undergoing surgery had, on
average, larger abscesses (>10 mm in diameter). Another study also found the volume of the abscess to be an important
criterion for surgery, with volumes <1250 mm3 not requiring surgery [68]. In another study in children, the degree of
proptosis was the only significant predictor of the need for surgical intervention [69].
We suggest that patients with large abscesses (>10 mm in diameter) be strongly considered for surgery. Patients with
smaller abscesses can generally be followed clinically and with repeat imaging unless impairment of vision is a concern. If
either the clinical findings or CT scan show no improvement within 24 to 48 hours, surgical drainage is generally
indicated. Surgery is almost always indicated in patients with intracranial extension of the infection. Surgery may also be
indicated to obtain culture material (eg, in patients with suspected fungal or mycobacterial infection of the orbit).
External approaches (through the orbit) and endoscopic transcaruncular surgery have been employed [70-73]. The
transcaruncular approach involves a lower eyelid transconjunctival incision extended medially around the lacrimal
caruncle [71].
Sinus surgery is indicated for debridement in patients with severe, destructive rhinosinusitis.
OUTCOMES — The outcomes of orbital cellulitis depend on whether complications are present. The majority of patients
with orbital cellulitis respond rapidly and completely to appropriate therapy. The most serious complications are
cavernous sinus thrombosis, intracranial extension, and vision loss, which can lead to permanent sequelae and, in the
case of complications in the former two, death. These complications are rare. (See 'Complications' above.)
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics" and "Beyond
the Basics." The Basics patient education pieces are written in plain language, at the 5th to 6
th grade reading level, and
they answer the four or five key questions a patient might have about a given condition. These articles are best for
patients who want a general overview and who prefer short, easy-to-read materials. Beyond the Basics patient education
pieces are longer, more sophisticated, and more detailed. These articles are written at the 10th to 12
th grade reading level
and are best for patients who want in-depth information and are comfortable with some medical jargon.

Here are the patient education articles that are relevant to this topic. We encourage you to print or e-mail these topics to
your patients. (You can also locate patient education articles on a variety of subjects by searching on "patient info" and
the keyword(s) of interest.)
●Basics topics (see "Patient information: Orbital cellulitis (The Basics)")
SUMMARY AND RECOMMENDATIONS — Orbital cellulitis is an infection involving the contents of the orbit (fat and
ocular muscles). Preseptal cellulitis and orbital cellulitis involve different anatomic sites, with preseptal cellulitis referring to
infections of the soft tissues anterior to the orbital septum and orbital cellulitis referring to infections posterior to it (figure
1). Although the two entities may initially be confused with one another, it is important to distinguish between them
because they have very different clinical implications. Preseptal cellulitis is generally a mild condition that rarely leads to
serious complications, whereas orbital cellulitis may cause loss of vision and even loss of life. Orbital cellulitis can usually
be distinguished from preseptal cellulitis by its clinical features (ophthalmoplegia, pain with eye movements, and
proptosis) and by imaging studies; in cases in which the distinction is not clear, clinicians should treat patients as though
they have orbital cellulitis. Both conditions are more common in children than in adults. (See 'Introduction' above
and 'Terminology' above.)
●The most common underlying factor that leads to orbital cellulitis is acute sinusitis, particularly ethmoid sinusitis;
less common causes are ophthalmic surgery and orbital trauma. (See 'Epidemiology and pathogenesis' above.)
●Orbital cellulitis is often a polymicrobial infection. The most commonly identified pathogens in orbital cellulitis are
Staphylococcus aureus and streptococci (table 1). (See 'Microbiology' above.)
●The diagnosis of orbital cellulitis is suspected clinically and can be confirmed by contrast-enhanced computed
tomography (CT) scanning of the orbits and sinuses. During the initial evaluation, it is critical to distinguish preseptal
cellulitis from the more serious orbital cellulitis (table 3 and table 2). It is also important to evaluate for complications
of orbital cellulitis, such as subperiosteal abscess, orbital abscess, visual loss, and intracranial extension. Although
both preseptal cellulitis and orbital cellulitis typically cause eyelid swelling with or without erythema, features such as
ophthalmoplegia, pain with eye movements, and/or proptosis occur only with orbital cellulitis. (See 'Clinical
manifestations' above and 'Diagnosis' above.)
●The diagnosis of orbital cellulitis is made by a combination of physical examination findings (including formal
assessments of extraocular movements, visual acuity, and proptosis), and radiologic assessment with CT scanning.
(See 'Diagnosis' above.)
●We recommend that patients with suspected orbital cellulitis with any of the following features undergo a contrast-
enhanced CT scan of the orbits and sinuses to confirm the diagnosis of orbital cellulitis and detect potential
complications:
•Proptosis
•Limitation of eye movements
•Pain with eye movements
•Double vision
•Vision loss
•Edema extending beyond the eyelid margin
•Absolute neutrophil count (ANC) >10,000 cell/microL
•Signs or symptoms of central nervous system (CNS) involvement
•Inability to examine the patient fully (usually patients less than one year of age)
•Patients who do not begin to show improvement within 24 to 48 hours of initiating appropriate therapy
(see 'Indications for imaging' above)
●Complications of orbital cellulitis may develop rapidly and include subperiosteal and orbital abscesses, extension
to the orbital apex causing vision loss, or intracranial extension causing epidural abscess or subdural empyema,
intracranial abscess, meningitis, or cavernous sinus thrombosis. (See 'Complications' above.)
●For patients with orbital cellulitis, we suggest initial empiric antibiotic treatment with parenteral broad-spectrum
therapy with activity against S. aureus (including methicillin-resistant S. aureus [MRSA]), streptococci, and gram-
negative bacilli; this should include vancomycin plus one of the following: ampicillin-sulbactam,piperacillin-
tazobactam, ceftriaxone, or cefotaxime (Grade 2B). If ceftriaxone or cefotaxime is employed and there is concern
for intracranial extension, we suggest that metronidazole be added to the regimen to cover anaerobes (Grade 2B).
(See 'Antibiotic regimens' above.)
http://www.uptodate.com/contents/piperacillin-and-tazobactam-sodium-drug-information?source=see_link

●Signs and symptoms should begin to show improvement within 24 to 48 hours following the initiation of appropriate
therapy; if this does not occur, repeat imaging should be performed and surgery should be considered.
(See 'Response to therapy' above.)
●For patients with uncomplicated orbital cellulitis, we suggest that antibiotics be continued until all signs of orbital
cellulitis have resolved, and for a total of at least two to three weeks (including both intravenous and oral therapy). A
longer period (at least four weeks) is recommended for patients with severe ethmoid sinusitis and bony destruction
of the sinus. The management of the complications of orbital cellulitis is discussed separately. (See 'Duration and
switch to oral therapy' above.)
●Although initial treatment may consist of intravenous antibiotics alone, management should be in consultation with
an ophthalmologist and an otolaryngologist because the physical examination requires
ophthalmic and/or otolaryngologic expertise and surgery is sometimes required. The main indications for surgery are
a poor response of the infection to antibiotic treatment, worsening visual acuity or pupillary changes, or evidence of
an abscess, especially a large abscess (>10 mm in diameter) or one that fails to respond promptly to antibiotic
treatment. (See 'Surgery' above.)
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Zhang J, Stringer MD. Ophthalmic and facial veins are not valveless. Clin Experiment Ophthalmol 2010; 38:502. 2. Botting AM, McIntosh D, Mahadevan M. Paediatric pre- and post-septal peri-orbital infections are different
diseases. A retrospective review of 262 cases. Int J Pediatr Otorhinolaryngol 2008; 72:377. 3. Seltz LB, Smith J, Durairaj VD, et al. Microbiology and antibiotic management of orbital cellulitis. Pediatrics 2011;
127:e566. 4. Nageswaran S, Woods CR, Benjamin DK Jr, et al. Orbital cellulitis in children. Pediatr Infect Dis J 2006; 25:695. 5. Sobol SE, Marchand J, Tewfik TL, et al. Orbital complications of sinusitis in children. J Otolaryngol 2002; 31:131. 6. Weakley DR. Orbital cellulitis complicating strabismus surgery: a case report and review of the literature. Ann
Ophthalmol 1991; 23:454. 7. Allen MV, Cohen KL, Grimson BS. Orbital cellulitis secondary to dacryocystitis following blepharoplasty. Ann
Ophthalmol 1985; 17:498. 8. McLeod SD, Flowers CW, Lopez PF, et al. Endophthalmitis and orbital cellulitis after radial keratotomy.
Ophthalmology 1995; 102:1902. 9. Varma D, Metcalfe TW. Orbital cellulitis after peribulbar anaesthesia for cataract surgery. Eye (Lond) 2003;
17:105. 10. Hofbauer JD, Gordon LK, Palmer J. Acute orbital cellulitis after peribulbar injection. Am J Ophthalmol 1994;
118:391. 11. Malik NN, Goh D, McLean C, Huchzermeyer P. Orbital cellulitis caused by Peptostreptococcus. Eye (Lond) 2004;
18:643. 12. Chaudhry IA, Shamsi FA, Elzaridi E, et al. Outcome of treated orbital cellulitis in a tertiary eye care center in the
middle East. Ophthalmology 2007; 114:345. 13. Schmitt NJ, Beatty RL, Kennerdell JS. Superior ophthalmic vein thrombosis in a patient with dacryocystitis-
induced orbital cellulitis. Ophthal Plast Reconstr Surg 2005; 21:387. 14. Ataullah S, Sloan B. Acute dacryocystitis presenting as an orbital abscess. Clin Experiment Ophthalmol 2002;
30:44. 15. Allan BP, Egbert MA, Myall RW. Orbital abscess of odontogenic origin. Case report and review of the literature.
Int J Oral Maxillofac Surg 1991; 20:268. 16. Rubinstein JB, Handler SD. Orbital and periorbital cellulitis in children. Head Neck Surg 1982; 5:15. 17. Weber AL, Mikulis DK. Inflammatory disorders of the paraorbital sinuses and their complications. Radiol Clin
North Am 1987; 25:615. 18. Goytia VK, Giannoni CM, Edwards MS. Intraorbital and intracranial extension of sinusitis: comparative morbidity.
J Pediatr 2011; 158:486. 19. Uzcátegui N, Warman R, Smith A, Howard CW. Clinical practice guidelines for the management of orbital
cellulitis. J Pediatr Ophthalmol Strabismus 1998; 35:73. 20. Schramm VL Jr, Curtin HD, Kennerdell JS. Evaluation of orbital cellulitis and results of treatment. Laryngoscope
1982; 92:732. 21. Swift AC, Charlton G. Sinusitis and the acute orbit in children. J Laryngol Otol 1990; 104:213. 22. Mills R. Orbital and periorbital sepsis. J Laryngol Otol 1987; 101:1242. 23. Dudin A, Othman A. Acute periorbital swelling: evaluation of management protocol. Pediatr Emerg Care 1996;
12:16. 24. McKinley SH, Yen MT, Miller AM, Yen KG. Microbiology of pediatric orbital cellulitis. Am J Ophthalmol 2007;
144:497. 25. Kobayashi D, Givner LB, Yeatts RP, et al. Infantile orbital cellulitis secondary to community-associated methicillin-
resistant Staphylococcus aureus. J AAPOS 2011; 15:208. 26. Starkey CR, Steele RW. Medical management of orbital cellulitis. Pediatr Infect Dis J 2001; 20:1002.

27. Chou SY, Tsai CC, Kau SC, et al. Aeromonas hydrophila orbital cellulitis in a patient with myelodysplastic syndrome. J Chin Med Assoc 2004; 67:51.
28. Maccheron LJ, Groeneveld ER, Ohlrich SJ, et al. Orbital cellulitis, panophthalmitis, and ecthyma gangrenosum in an immunocompromised host with pseudomonas septicemia. Am J Ophthalmol 2004; 137:176.
29. Hemady R, Zimmerman A, Katzen BW, Karesh JW. Orbital cellulitis caused by Eikenella corrodens. Am J Ophthalmol 1992; 114:584.
30. Ambati BK, Ambati J, Azar N, et al. Periorbital and orbital cellulitis before and after the advent of Haemophilus influenzae type B vaccination. Ophthalmology 2000; 107:1450.
31. Barone SR, Aiuto LT. Periorbital and orbital cellulitis in the Haemophilus influenzae vaccine era. J Pediatr Ophthalmol Strabismus 1997; 34:293.
32. Harris GJ. Subperiosteal abscess of the orbit. Age as a factor in the bacteriology and response to treatment. Ophthalmology 1994; 101:585.
33. Brook I, Frazier EH. Microbiology of subperiosteal orbital abscess and associated maxillary sinusitis. Laryngoscope 1996; 106:1010.
34. Chawla B, Sharma S, Kashyap S, et al. Primary orbital mycosis in immunocompetent infants. J AAPOS 2011; 15:211.
35. Jones J, Katz SE, Lubow M. Scedosporium apiospermum of the orbit. Arch Ophthalmol 1999; 117:272. 36. Durand, ML. Periocular infections. In: Principles and Practice of Infectious Diseases, 7th ed, Mandell, GL,
Bennett, et al. (Eds), Churchill Livingstone Elsevier, Philadelphia 2010. p.1569. 37. Rudloe TF, Harper MB, Prabhu SP, et al. Acute periorbital infections: who needs emergent imaging? Pediatrics
2010; 125:e719. 38. Patt BS, Manning SC. Blindness resulting from orbital complications of sinusitis. Otolaryngol Head Neck Surg
1991; 104:789. 39. Osguthorpe JD, Hochman M. Inflammatory sinus diseases affecting the orbit. Otolaryngol Clin North Am 1993;
26:657. 40. Okamoto Y, Hiraoka T, Okamoto F, Oshika T. A case of subperiosteal abscess of the orbit with central retinal
artery occlusion. Eur J Ophthalmol 2009; 19:288. 41. Komolafe OO, Ashaye AO. Combined central retinal artery and vein occlusion complicating orbital cellulitis. Niger
J Clin Pract 2008; 11:74. 42. Ryan JT, Preciado DA, Bauman N, et al. Management of pediatric orbital cellulitis in patients with radiographic
findings of subperiosteal abscess. Otolaryngol Head Neck Surg 2009; 140:907. 43. Harris GJ. Age as a factor in the bacteriology and response to treatment of subperiosteal abscess of the orbit.
Trans Am Ophthalmol Soc 1993; 91:441. 44. Filips RF, Liudahl JJ. Asymptomatic posterior orbital cellulitis resulting from ethmoid/maxillary sinusitis. J Am
Optom Assoc 1997; 68:55. 45. Greenberg MF, Pollard ZF. Medical treatment of pediatric subperiosteal orbital abscess secondary to sinusitis. J
AAPOS 1998; 2:351. 46. Bergin DJ, Wright JE. Orbital cellulitis. Br J Ophthalmol 1986; 70:174. 47. Reynolds DJ, Kodsi SR, Rubin SE, Rodgers IR. Intracranial infection associated with preseptal and orbital
cellulitis in the pediatric patient. J AAPOS 2003; 7:413. 48. Russo G, Di Pietro M, La Spina M. Ocular involvement in neuroblastoma: not always metastasis. Lancet Oncol
2004; 5:324. 49. Shields CL, Shields JA, Honavar SG, Demirci H. Primary ophthalmic rhabdomyosarcoma in 33 patients. Trans
Am Ophthalmol Soc 2001; 99:133. 50. Jacobs D, Galetta S. Diagnosis and management of orbital pseudotumor. Curr Opin Ophthalmol 2002; 13:347. 51. Sirbaugh PE. A case of orbital pseudotumor masquerading as orbital cellulitis in a patient with proptosis and
fever. Pediatr Emerg Care 1997; 13:337. 52. Rubinstein A, Riddell CE. Posterior scleritis mimicking orbital cellulitis. Eye (Lond) 2005; 19:1232. 53. Abou-Rayyah Y, Rose GE, Konrad H, et al. Clinical, radiological and pathological examination of periocular
dermoid cysts: evidence of inflammation from an early age. Eye (Lond) 2002; 16:507. 54. Ziakas NG, Boboridis K, Gratsonidis A, et al. Wegener's granulomatosis of the orbit in a 5-year-old child. Eye
(Lond) 2004; 18:658. 55. Youssef Z, Pennefather PM, Watts MT. Orbital cellulitis vs allergic reaction to hyaluronidase as the cause of
periorbital oedema. Eye (Lond) 2005; 19:691. 56. Patil B, Agius-Fernandez A, Worstmann T. Hyaluronidase allergy after peribulbar anesthesia with orbital
inflammation. J Cataract Refract Surg 2005; 31:1480. 57. Hegde V, Smith G, Choi J, Pagliarini S. A case of gonococcal kerato-conjunctivitis mimicking orbital cellulitis. Acta
Ophthalmol Scand 2005; 83:511. 58. Ruttum MS, Ogawa G. Adenovirus conjunctivitis mimics preseptal and orbital cellulitis in young children. Pediatr
Infect Dis J 1996; 15:266. 59. Eustis HS, Mafee MF, Walton C, Mondonca J. MR imaging and CT of orbital infections and complications in acute
rhinosinusitis. Radiol Clin North Am 1998; 36:1165. 60. Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol Allied Sci
2004; 29:725. 61. Mair MH, Geley T, Judmaier W, Gassner I. Using orbital sonography to diagnose and monitor treatment of acute
swelling of the eyelids in pediatric patients. AJR Am J Roentgenol 2002; 179:1529.

62. Mahalingam-Dhingra A, Lander L, Preciado DA, et al. Orbital and periorbital infections: a national perspective. Arch Otolaryngol Head Neck Surg 2011; 137:769.
63. Zyvox (linezolid) prescribing information. Pharmacia & Upjohn Company. Revised June 2010. http://www.pfizer.com/files/products/uspi_zyvox.pdf (Accessed on August 19, 2011).
64. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 2011; 52:e18.
65. Givner LB. Periorbital versus orbital cellulitis. Pediatr Infect Dis J 2002; 21:1157. 66. Nelson LB, Olitsky SE. Disorders of the orbit. In: Harley's Pediatric Ophthalmology, Lippincott Williams and
Wilkins, Philadelphia 2005. p.389. 67. Youssef OH, Stefanyszyn MA, Bilyk JR. Odontogenic orbital cellulitis. Ophthal Plast Reconstr Surg 2008; 24:29. 68. Todman MS, Enzer YR. Medical management versus surgical intervention of pediatric orbital cellulitis: the
importance of subperiosteal abscess volume as a new criterion. Ophthal Plast Reconstr Surg 2011; 27:255. 69. Rahbar R, Robson CD, Petersen RA, et al. Management of orbital subperiosteal abscess in children. Arch
Otolaryngol Head Neck Surg 2001; 127:281. 70. Arjmand EM, Lusk RP, Muntz HR. Pediatric sinusitis and subperiosteal orbital abscess formation: diagnosis and
treatment. Otolaryngol Head Neck Surg 1993; 109:886. 71. Pelton RW, Smith ME, Patel BC, Kelly SM. Cosmetic considerations in surgery for orbital subperiosteal abscess
in children: experience with a combined transcaruncular and transnasal endoscopic approach. Arch Otolaryngol Head Neck Surg 2003; 129:652.
72. Younis RT, Lazar RH, Bustillo A, Anand VK. Orbital infection as a complication of sinusitis: are diagnostic and treatment trends changing? Ear Nose Throat J 2002; 81:771.
73. Tanna N, Preciado DA, Clary MS, Choi SS. Surgical treatment of subperiosteal orbital abscess. Arch Otolaryngol Head Neck Surg 2008; 134:764.
Topic 3414 Version 17.0

The orbital septum
Diagram showing the proximity of the periosteum in relation to the orbital septum. Orbital cellulitis arises
posterior to the orbital septum
Medial wall of the left orbit (lateral wall removed)
Note the proximity of the frontal, ethmoidal,
and maxillary sinuses to the orbital space. The lamina papyracea is the thin bone wall on the surface of the
ethmoid air cells

Venous drainage of the orbit
The diagram demonstrates the communication between ethmoidal sinuses, the orbit, and the cavernous sinus.
Subperiosteal abscess by CT scan
This CT scan with intravenous contrast shows a medial subperiosteal abscess associated with maxillary and
ethmoid sinusitis. The arrows indicate the location of the subperiosteal abscess.
Related Documents











