Entero- hepatic diseases

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Entero- hepatic diseases

Liver, acute viral hepatitis (hepatitis B virus)
• portal area
Low power

Liver, acute viral hepatitis (hepatitis B virus)
• bile pigment
• hepatocytes
• liver sinusoid
• regenerating hepatocytes
• inflammatory infiltrate
High power

Liver, acute viral hepatitis (hepatitis B virus)
• balloning of degenerating hepatocytes
• inflammation
• councilman/ acidophilic body

Liver, fulminant hepatitis
• necrotic area
Gross Low power

Liver, viral hepatitis, carrier state (hepatitis B virus)
• ground- glass hepatocyteimmunohistochemical stain for HbsAg
Medium power High power

Liver, chronic viral hepatitis (hepatitis B virus)
• portal area
Medium power
• portal area
• inflammation surrounding hepatocites
Patient 1 Patient 2

Liver, chronic viral hepatitis (hepatitis C virus) - Low power
• portal area
• lymphoid agregate
• steatosis

Liver, cirrhosis from chronic viral hepatitis -
• Regenerative liver nodul
GrossCut surface
Liver, alcoholic cirrhosis
contains numerous, fairly uniform, small
nodules of regenerative hepatocytes separated by
depressed areas of fibrous scar tissue

Liver, biliary cirrhosis Gross, cut surface
This is a section of liver from a child who died of biliary cirrhosis secondary to biliary atresia. The cut surface is dark green, due to marked cholestasis within the liver. Regenerative nodules of liver parenchyma are separated by tan bands of fibrous tissue
Biliary tree, biliary atresia
Biliary atresia, a common cause of neonatal cholestasis,
results from progressive destruction of the hepatic and
common bile ducts. In this image, the common bile duct is reduced to a thin band
of fibrous tissue extending from the hilum of the liver, which is green due to the presence of cholestasis, to the duodenal
area. This leads to the development of cirrhosis in the first year of life. It is the most common cause of referral for
liver transplantation in children

Ascites - Clinical presentation Skin, spider telangiectasia
-
Ascites
Esophagus, varices - Gross, mucosal surface
• esophagus
• stomach
• erosion due to sclerosing th

Liver, hepatocellular carcinoma
a. hepatocellular carsinoma
b. satellite tumor nodule
Gross
Cut surface
• Cord of malignant hepatocites
Medium power

Liver, alcoholic hepatic steatosis (fatty liver)
cut surfaceGross,
Enlarged, soft, and yellow. a greasy texture
Low power
Medium power
• mallory bodies
• hepatocites
• high power view
• intracytoplasmic fat
• mallory bodies

Liver, nonalcoholic steatohepatitis, trichrome stain - High power
Conditions associated with the development of NAFL and NASH are Obesity and diabetes
mellitus
• central vein
• perivenular (chicken wire) type fibrosis

Liver neoplasia
• central stellata fibrous scar
focal nodular hyperplasiacavernous hemangioma
• low power image
• normal liver
• hemangioma
• liver cell adenoma

cholangiocarcinoma
• outer surface
• cut surface
gross Low power
• fibrostic tissue and tumor
• cholangiosarcoma
• uninvolved liver

congenital and metabolic disease
Liver, Wilson disease
accumulation of copper in the hepatocytes
Liver, hemochromatosis
• hemosiderin in ductullar cell
• hemosiderin in hepatocites

Liver, metastatic adenocarcinoma
there are numerous tan, sometimes hemorrhagic and necrotic, nodules of metastatic tumor throughout the liver. Also, there is bile staining of the
remaining liver
Most tumors metastasize to the liver hematogenously through the portal vein or hepatic artery. Biliary tract tumors directly and
contiguously spread to the liver.

Liver,
localized, pale, and typically subcapsular,
are rare
congestive heart failure
hepatic infarct
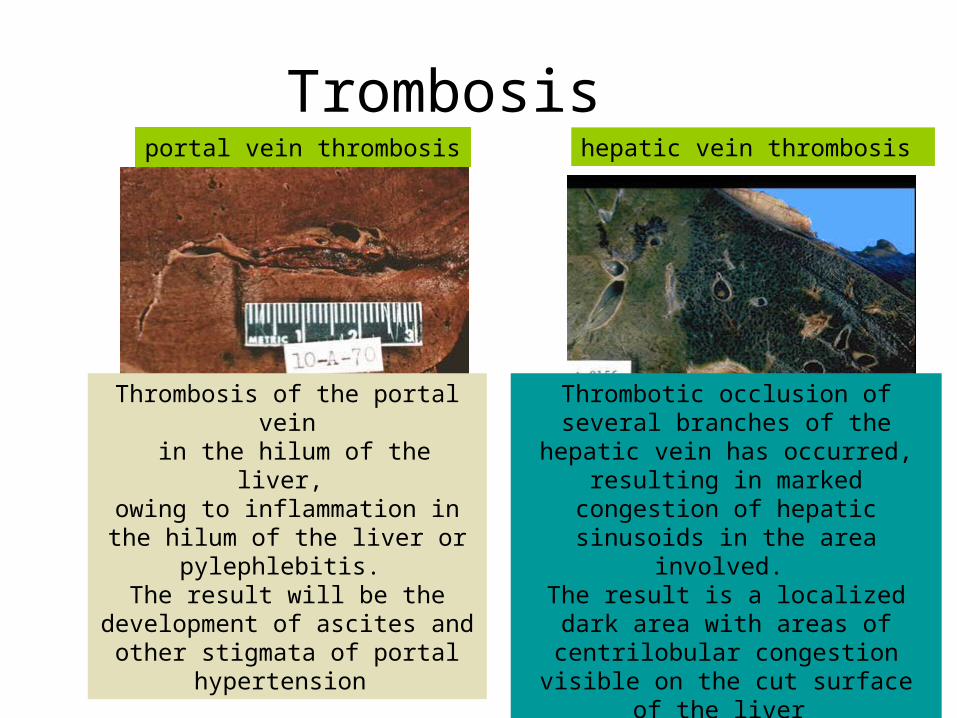
Trombosis
Thrombosis of the portal vein in the hilum of the liver,
owing to inflammation in the hilum of the liver or pylephlebitis.
The result will be the development of ascites and other stigmata of
portal hypertension
hepatic vein thrombosis portal vein thrombosis
Thrombotic occlusion of several branches of the hepatic vein has
occurred, resulting in marked congestion of hepatic sinusoids in the
area involved. The result is a localized dark area with
areas of centrilobular congestion visible on the cut surface of the liver

Gallbladder,
cholelithiasis and acute and chronic cholecystitis -
A section of a gallbladder from this case of acute and chronic cholecystitis shows marked fibrous thickening of the wall with areas of mucosal necrosis and ulceration. An inflammatory cellular infiltrate is present in the wall, especially in the areas of ulceration
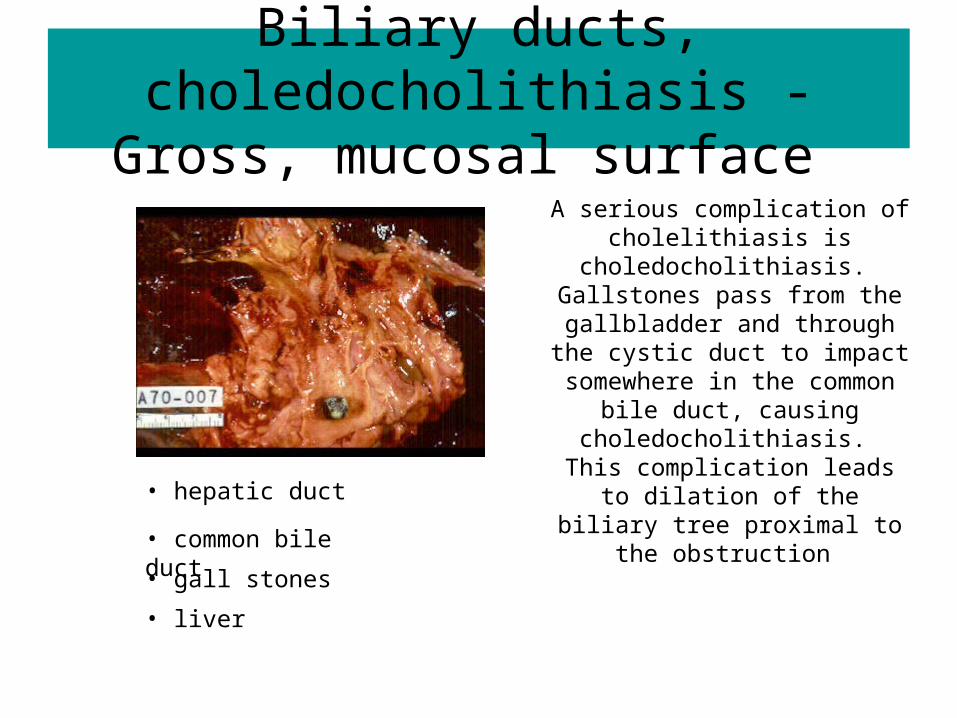
Biliary ducts, choledocholithiasis - Gross, mucosal surface
• hepatic duct
• common bile duct
• gall stones
• liver
A serious complication of cholelithiasis is
choledocholithiasis. Gallstones pass from the
gallbladder and through the cystic duct to impact somewhere in the
common bile duct, causing choledocholithiasis.
This complication leads to dilation of the biliary tree proximal to the
obstruction

Pancreas, acute pancreatitis
Etiology= Alcoholism, along with biliary tract disease (cholelithiasis)(80%); idiopathic( 10- 20%); there is increasing evidence of several genetic defects.
Patogenesis= the result of release of pancreatic enzymes from acinar cells, causing proteolysis, lipolysis, and hemorrhage. Released elastase degrades elastic tissue in
vessel walls. Pancreatic amylase is also released. Proposed mechanisms of pancreatic injury and subsequent enzyme release include:
(1) duct obstruction, (2) direct acinar cell injury, and (3) deranged intracellular transport of pancreatic enzymes.

Common bile duct, stricture ERCP image
Endoscopic Retrograde Cholangiopancreatography (ERCP) shows a stricture of the distal common bile duct
• dilated common bile and hepatic duct
• pancreatic duct
• stricture area, distal common bile duct

Pancreas, carcinoma and chronic pancreatitis
Chronic pancreatitis is associated with only a slightly increased risk of cancer, so the finding is most likely coincidental.
Chronic pancreatitis results in destruction of the exocrine and, eventually, endocrine portions of the pancreas.
It usually follows repeated bouts of acute pancreatitis that are due to alcohol ingestion or obstruction of the pancreatic duct. Other causes include tropical pancreatitis, hereditary pancreatitis, and idiopathic
cases.
• etiology
• location • sign & symptoms
Related Documents











