1 Ultrasound Imaging the Jaundiced dog ROBERT H. WRIGLEY ROBERT H. WRIGLEY Professor Professor Veterinary Diagnostic Imaging Veterinary Diagnostic Imaging University University of Sydney of Sydney Veterinary Teaching Hospital Veterinary Teaching Hospital Professor Emeritus Colorado State Professor Emeritus Colorado State University University Preparation Withhold food to allow stomach to empty

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
UltrasoundImaging the Jaundiced dog
ROBERT H. WRIGLEYROBERT H. WRIGLEY
Professor Professor Veterinary Diagnostic ImagingVeterinary Diagnostic ImagingUniversityUniversity of Sydneyof Sydney
Veterinary Teaching HospitalVeterinary Teaching HospitalProfessor Emeritus Colorado State Professor Emeritus Colorado State
UniversityUniversity
Preparation
Withhold food to allow stomach to empty

2
Normal GallbadderBiliary Sediment/Sludge
• Amount within the GB is variable• Seen in healthy, non fasting dogs.• Considered an incidental finding• Seen with biliary stasis from fasting or
illness• Usually does not shadow• Sludge balls
– Round, mobile, nonshadowing structures– Uncertain cause and significance
Courtesy Dr H Thode

3
Cystic Mucinous Hypertrophy or Hyperplasia of the Gall Bladder
• Not associated with obstruction of CD• Not associated with any clinical findings• Considered an incidental finding• Histologically
– No evidence of inflammation– Serosal, muscular, and vascular structures appear
intact and normal– Mucosal surface irregular; polypoid cystic lining
• Ultrasound– Thickened, irregular GB wall – Biliary sludge usually observed
CBC, SADP, U/A
PCV < 15Nucleated RBCs
Bilirubinuria
PCV > 20Abnormal liver enzymes
Hepatic disease Post Hepatic Biliary DiseaseHemolytic Disease
Clinical Icterus
Courtesy Dr H Thode, CSU
HepatitisHepatitisToxinsToxinsCirrhosisCirrhosisNeoplasiaNeoplasia
Normal Anatomy Echogenicity comparisons
Renal Medulla < Renal Cortex < Liver < Spleen < Renal PelvisMy Cat Loves Sunny Places
Blacker Whiter
Hypoechoic HyperechoicTissue Tissue
Least Echogenic Most EchogenicTissue Tissue
4
Biopsy - Cirrhosis
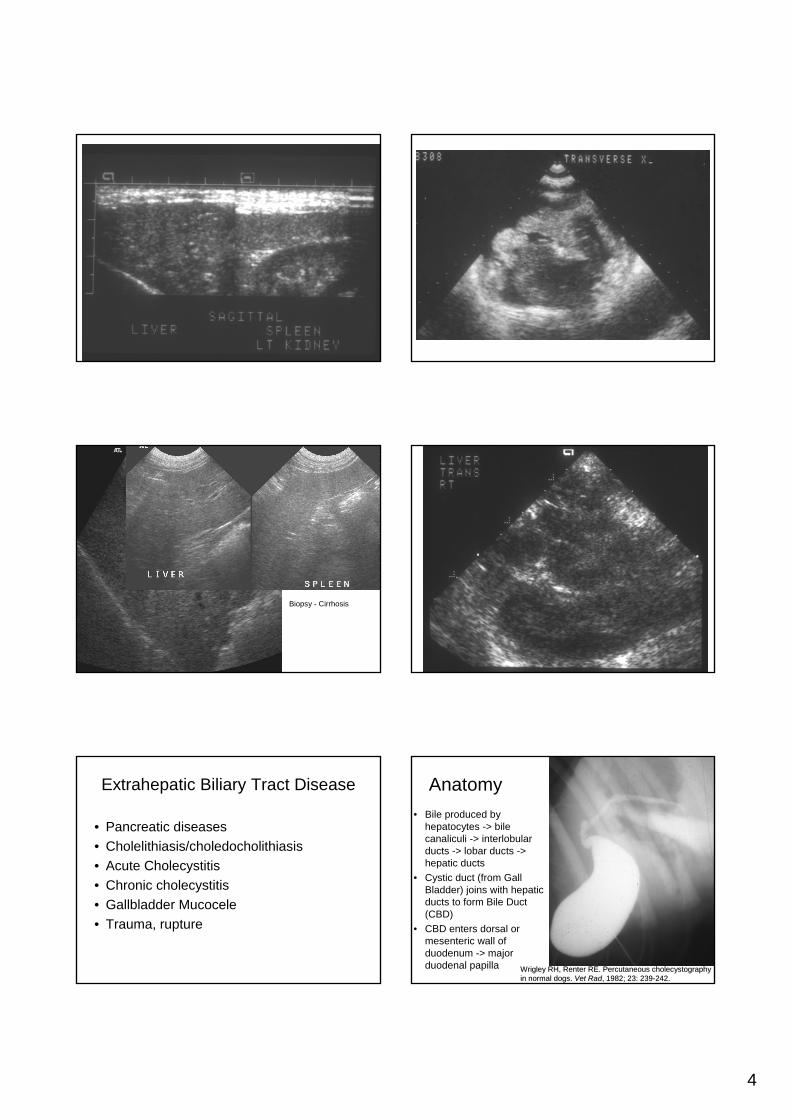
Extrahepatic Biliary Tract Disease
• Pancreatic diseases• Cholelithiasis/choledocholithiasis• Acute Cholecystitis• Chronic cholecystitis• Gallbladder Mucocele• Trauma, rupture
Anatomy• Bile produced by
hepatocytes -> bile canaliculi -> interlobular ducts -> lobar ducts -> hepatic ducts
• Cystic duct (from Gall Bladder) joins with hepatic ducts to form Bile Duct (CBD)
• CBD enters dorsal or mesenteric wall of duodenum -> major duodenal papilla Wrigley RH, Renter RE. Wrigley RH, Renter RE. PercutaneousPercutaneous cholecystographycholecystography
in normal dogs. in normal dogs. Vet Vet RadRad, 1982; 23: 239, 1982; 23: 239--242.242.

5
Clinical Signs of ExtrahepaticBiliary Tract Obstruction (EHBO)
• Nonspecific• Mimic other abdominal disorders• May wax/wane for several weeks prior to
presentation• Most patients not likely to be examined
until clinical signs of icterus develop• May see acholic feces
Diagnostic Evaluation• Animals may not demonstrate clinical
signs or hematologic abnls for weeks to months after the obstruction
• CBD obstruction– Increased total serum bilirubin (>90%
conjugated)– Bilirubinuria
• renal excretion becomes important for elimination of the pigment
• may precede the development of jaundice
Experimental Bile Duct Ligation in the Dog
• CBD surgically ligated in 5 nl adult dogs• US exams performed pre-op and at 24
hour intervals post-op• Sequence of biliary system dilation was
from CBD to peripheral intrahepatic ducts• GB, cystic duct, and CBD enlargement
evident in 24 – 48 hours• Peripheral bile duct dilation recognized by
5 – 7 days after obstruction••Nyland TG, Gillett NA. Nyland TG, Gillett NA. SonographicSonographic evaluation of experimental bile duct ligation evaluation of experimental bile duct ligation in the dog. in the dog. Vet Vet RadRad, 1982; 23: 252, 1982; 23: 252--260.260.
6
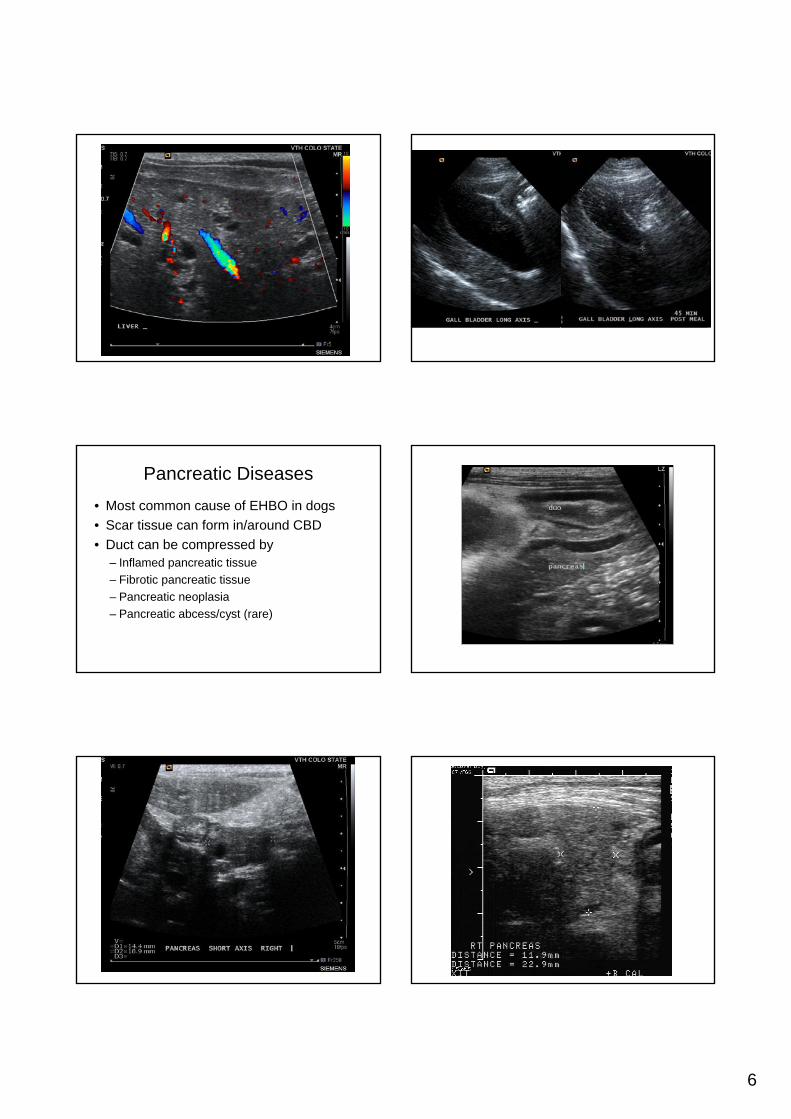
Pancreatic Diseases• Most common cause of EHBO in dogs• Scar tissue can form in/around CBD• Duct can be compressed by
– Inflamed pancreatic tissue– Fibrotic pancreatic tissue– Pancreatic neoplasia– Pancreatic abcess/cyst (rare)
7
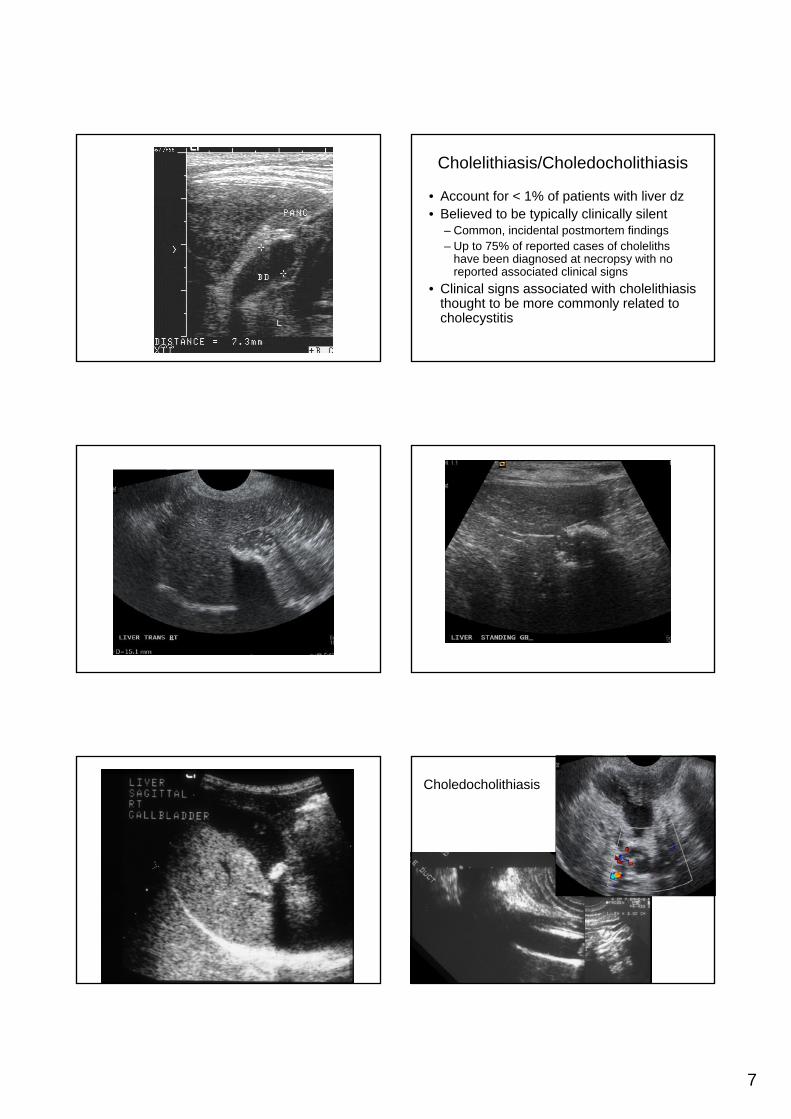
Cholelithiasis/Choledocholithiasis
• Account for < 1% of patients with liver dz• Believed to be typically clinically silent
– Common, incidental postmortem findings– Up to 75% of reported cases of choleliths
have been diagnosed at necropsy with no reported associated clinical signs
• Clinical signs associated with cholelithiasisthought to be more commonly related to cholecystitis
Choledocholithiasis

8
Acute Cholecystitis• May have a variety of sonographic
appearances• GB wall thickening usually a consistent
finding• Pain may be detected in region of the GB
during scanning • Emphysematous cholecystitis
– Gas formation in wall/lumen of GB– Usually combination of GB wall ischemia and
proliferation of gas-forming bacteria
Chronic Cholecystitis
• Usually presents in a less acute form than acute cholecystitis
• Can see GB wall thickening due to inflammation and fibrosis
• Fibrosis/inflammation may prevent even normal distention of the GB
• Mineralization of the GB wall may occur with chronic inflammation

9
• Liver disease is common in cats• Cholangitis/cholangiohepatitis: 20-30%• Ascending bacterial infection• Biopsy and culture needed for diagnosis• Specific long-term antibiotic therapyPercutaneous ultrasound-guided
cholecystocentesis - Considered routine in humans
Percutaneous Ultrasound-guided Cholecystocentesis in Healthy Cats
Savary- Bataille et al. JVIM 2003 17: 298-303
Courtsey Dr Quimby CSU
Methods - PUC• Ketamine/valium sedation• 22 gauge/1.5 inch with 12 ml syringe• Right transhepatic approach (1 cat)• Right ventral direct puncture (11 cats)
• Right transhepatic approach –immediate mild effusion, hemorrhagic bile (1 cat)
• Right ventral direct approach – no complications (11 cats)
• 1.8ml +/- 0.8ml (range 0.9 – 3ml)
Results - PUC
Results
• Right transhepatic approach – immediate mild effusion, hemorrhagic bile (1 cat)
• Right ventral direct approach – no complications (11 cats)
• 1.8ml +/- 0.8ml (range 0.9 – 3ml)
• Direct proportional relationship between weight and volume of bile.
Results
• 4 cats had mild transient hyporexia• 4 cats had mild abdominal discomfort• No U/S changes for direct approach
• Necropsy – no abnormalities noted• Cytology – 11 cats - just bile• Cultures
– No growth– One contaminant

10
•Wrigley RH, Renter RE. Percutaneous cholecystography in normal dogs. Vet Rad, 1982; 23: 239-242.
Finish by emptying the gallbladder
Fast for additional 12 hours
Choledocholithiasis
Gallbladder Mucocele
• An abnormal accumulation of mucus distending the gallbladder
• Etiology is uncertain– ? Bile stasis– ? Mucinous hyperplasia of GB mucosa– ? Inflammation– ? Biliary sludge a predisposing factor– ? Altered contractility of the GB wall– ? Combination of factors
• Gelatinous bile may extend into CD and/or CBD and cause obstruction
Gallbladder Mucocele• Tendency to affect smaller dogs• Cocker Spaniels may be predisposed• More common in older dogs• Clinical signs nonspecific• Usually have clinocopathologic evidence of
hepatobiliary disease• 50 – 60% incidence of GB rupture
– Poor prognosis– Cholecystectomy (emergency if GB wall rupture is
suspected)

11
Bile Patterns with Mucoceles• Besso JG, Wrigley RH, et al.
Ultrasonographic appearance and clinical findings in 14 dogs with gallbladder mucocele. Vet Rad & US, 2000; 41: 261-271.
•Pike FS, et al. Gallbladder mucocele in dogs: 30 cases (2000-2002). JAVMA, 2004; 224: 1615-1622.
Worley DR, et al. Surgical management of gallbladder mucoceles in dogs: 22 cases (1999-2003). JAVMA, 2004; 225: 1418-1422.
References• Besso JG, Wrigley RH, et al. Ultrasonographic appearance and clinical findings in 14 dogs with
gallbladder mucocele. Vet Rad & US, 2000; 41: 261-271.• Center SA. Diseases of the biliary tree. In: Guilford WG, et al, eds. Small Animal
Gastroenterology. Philadelphia: WB Saunders,1996: 860-861, 865.• Mehler SJ, Bennett RA. Canine extrahepatic biliary tract disease and surgery. Compendium,
2006; 28: 302-314.• Newell SM, et al. Gallbladder mucocele causing biliary obstruction in two dogs: ultrasonographic,
scintigraphic, and pathological findings. Jnl AAHA, 1995; 31: 467-472.• Nyland TG, Gillett NA. Sonographic evaluation of experimental bile duct ligation in the dog. Vet
Rad, 1982; 23: 252-260.• Nyland TG, Mattoon JS, et al. Liver. In: Nyland TG, Mattoon JS, eds. Small Animal Diagnostic
Ultrasound. Philadelphia: WB Saunders, 2002: 113-117.• Partington BP, Biller DS. Liver. In: Green RW, ed. Small Animal Ultrasound. Philadelphia:
Lippincott-Raven, 1996: 119-124.• Pike FS, et al. Gallbladder mucocele in dogs: 30 cases (2000-2002). JAVMA, 2004; 224: 1615-
1622.• Rivers BJ, et al. Acalculus cholecystitis in four canine cases: ultrasonographic findings and use of
ultrasonographic-guided percutaneous cholecystocentesis in diagnosis. Jnl AAHA, 1997; 33: 207-214.
• Worley DR, et al. Surgical management of gallbladder mucoceles in dogs: 22 cases (1999-2003). JAVMA, 2004; 225: 1418-1422.
• Wrigley RH, Renter RE. Percutaneous cholecystography in normal dogs. Vet Rad, 1982; 23: 239-242.
Related Documents











