ORIGINAL ARTICLE – HEPATOBILIARY AND PANCREATIC TUMORS Preoperative Serum CA19-9 and Dissected Peripancreatic Tissue Margin as Determiners of Long-Term Survival in Pancreatic Cancer Mina Waraya, MD, Keishi Yamashita, MD, PhD, Hiroyuki Katagiri, MD, PhD, Kenichiro Ishii, MD, PhD, Yoshihito Takahashi, MD, PhD, Kazunori Furuta, MD, PhD, and Masahiko Watanabe, MD, PhD, FACS Department of Surgery, Medical School, Kitasato University Hospital, Sagamihara, Kanagawa, Japan ABSTRACT Background. Pancreatic cancer, a particularly deadly form of malignancy, has increased in the last decade worldwide. The purpose of this study is to identify markers for determining and identifying possible long-term survi- vors in cases of advanced pancreatic cancer. Patients and methods. 117 patients with pancreatic ductal carcinoma, including 89 with invasive tubular adenocar- cinoma of the pancreas, Japan Pancreas Society (JPS) stage III–IVb patients, who underwent tumor resection between 1986 and 2006. Results. Univariate prognostic analyses of the 5-year disease-specific survival (DSS) revealed that JPS stage (P \ 0.0001), preoperative serum carbohydrate antigen 19-9 (CA19-9) level (preCA19-9; P \ 0.0001), dissected peripancreatic tissue margin (DPM; P \ 0.0001), residual tumor (R factor; P = 0.0007), lymph node metastasis den- sity over 10% (ND10; P = 0.006), volume of the stromal connective tissue (stroma factor; P = 0.008), growth pattern (P = 0.01), and histology (P = 0.03) were all significantly associated with poor outcome in advanced pancreatic can- cer. Multivariate logistic analysis confirmed that preCA19-9 [P = 0.0006, relative risk (RR) = 2.16] and DPM (P = 0.04, RR = 1.62) were prognostic factors that remained, independent of JPS stage (P = 0.001). The higher preCA19-9 was, the worse the prognosis was. Astonishingly, among JPS stage III cases, 76.9% of the patients with preCA19-9 below 37 U/ml survived more than 5 years. This, combined with an analysis of DPM, allowed us to identify those with the potentiality for long-term survival. Conclusion. Our results reveal for the first time that it is possible with JPS stage III–IVb invasive tubular adeno- carcinomas of the pancreas to differentiate prognostic groups and potential survival rates, like with other cancers. Pancreatic cancer is responsible for 34,000 deaths per year in the USA, and is the fourth most common cause of death from cancer, a position higher than its rate of incidence (tenth) because of its dismal prognosis. 1 In Japan, prevalence of pancreatic cancer has increased in the last decade to become the fifth leading cause of cancer death in men and the sixth in women. 2 Surgical resection has provided the only chance for cure or long-term survival, despite the develop- ment of multidisciplinary treatments. Resection rates have increased due to recent advances in surgical techniques and the application of extensive surgery. However, postoperative prognosis has still been dismal due to commonly occurring liver metastasis, local recurrence, and peritoneal dissemi- nation. It is important to be able to predict prognosis precisely after pancreatectomy for assessment of therapeutic effect, consideration of administering adjuvant therapy, and providing information to the patient. The most common staging system used for pancreatic cancer is the tumor–node–metastasis (TNM) classification. This system was developed by the International Union against Cancer (UICC) and is similar to that used by the Japan Pancreas Society (JPS). However, TNM staging does not offer an adequately broad picture of a patient’s prognosis. Previous studies proposed that the prognostic factors for pancreatic cancer were tumor size, differentia- tion, lymph node metastasis density (ND), large vessel involvement, resection margin status, and tumor markers Electronic supplementary material The online version of this article (doi:10.1245/s10434-009-0415-7) contains supplementary material, which is available to authorized users. Ó Society of Surgical Oncology 2009 First Received: 15 December 2008; Published Online: 5 March 2009 M. Watanabe, MD, PhD, FACS e-mail: [email protected] Ann Surg Oncol (2009) 16:1231–1240 DOI 10.1245/s10434-009-0415-7

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL ARTICLE – HEPATOBILIARY AND PANCREATIC TUMORS
Preoperative Serum CA19-9 and Dissected Peripancreatic TissueMargin as Determiners of Long-Term Survival in PancreaticCancer
Mina Waraya, MD, Keishi Yamashita, MD, PhD, Hiroyuki Katagiri, MD, PhD, Kenichiro Ishii, MD, PhD,
Yoshihito Takahashi, MD, PhD, Kazunori Furuta, MD, PhD, and Masahiko Watanabe, MD, PhD, FACS
Department of Surgery, Medical School, Kitasato University Hospital, Sagamihara, Kanagawa, Japan
ABSTRACT
Background. Pancreatic cancer, a particularly deadly
form of malignancy, has increased in the last decade
worldwide. The purpose of this study is to identify markers
for determining and identifying possible long-term survi-
vors in cases of advanced pancreatic cancer.
Patients and methods. 117 patients with pancreatic ductal
carcinoma, including 89 with invasive tubular adenocar-
cinoma of the pancreas, Japan Pancreas Society (JPS) stage
III–IVb patients, who underwent tumor resection between
1986 and 2006.
Results. Univariate prognostic analyses of the 5-year
disease-specific survival (DSS) revealed that JPS stage
(P \ 0.0001), preoperative serum carbohydrate antigen
19-9 (CA19-9) level (preCA19-9; P \ 0.0001), dissected
peripancreatic tissue margin (DPM; P \ 0.0001), residual
tumor (R factor; P = 0.0007), lymph node metastasis den-
sity over 10% (ND10; P = 0.006), volume of the stromal
connective tissue (stroma factor; P = 0.008), growth pattern
(P = 0.01), and histology (P = 0.03) were all significantly
associated with poor outcome in advanced pancreatic can-
cer. Multivariate logistic analysis confirmed that preCA19-9
[P = 0.0006, relative risk (RR) = 2.16] and DPM
(P = 0.04, RR = 1.62) were prognostic factors that
remained, independent of JPS stage (P = 0.001). The higher
preCA19-9 was, the worse the prognosis was. Astonishingly,
among JPS stage III cases, 76.9% of the patients with
preCA19-9 below 37 U/ml survived more than 5 years. This,
combined with an analysis of DPM, allowed us to identify
those with the potentiality for long-term survival.
Conclusion. Our results reveal for the first time that it is
possible with JPS stage III–IVb invasive tubular adeno-
carcinomas of the pancreas to differentiate prognostic
groups and potential survival rates, like with other cancers.
Pancreatic cancer is responsible for 34,000 deaths per
year in the USA, and is the fourth most common cause of
death from cancer, a position higher than its rate of incidence
(tenth) because of its dismal prognosis.1 In Japan, prevalence
of pancreatic cancer has increased in the last decade to
become the fifth leading cause of cancer death in men and the
sixth in women.2 Surgical resection has provided the only
chance for cure or long-term survival, despite the develop-
ment of multidisciplinary treatments. Resection rates have
increased due to recent advances in surgical techniques and
the application of extensive surgery. However, postoperative
prognosis has still been dismal due to commonly occurring
liver metastasis, local recurrence, and peritoneal dissemi-
nation. It is important to be able to predict prognosis
precisely after pancreatectomy for assessment of therapeutic
effect, consideration of administering adjuvant therapy, and
providing information to the patient.
The most common staging system used for pancreatic
cancer is the tumor–node–metastasis (TNM) classification.
This system was developed by the International Union
against Cancer (UICC) and is similar to that used by the
Japan Pancreas Society (JPS). However, TNM staging
does not offer an adequately broad picture of a patient’s
prognosis. Previous studies proposed that the prognostic
factors for pancreatic cancer were tumor size, differentia-
tion, lymph node metastasis density (ND), large vessel
involvement, resection margin status, and tumor markers
Electronic supplementary material The online version of thisarticle (doi:10.1245/s10434-009-0415-7) contains supplementarymaterial, which is available to authorized users.
� Society of Surgical Oncology 2009
First Received: 15 December 2008;
Published Online: 5 March 2009
M. Watanabe, MD, PhD, FACS
e-mail: [email protected]
Ann Surg Oncol (2009) 16:1231–1240
DOI 10.1245/s10434-009-0415-7
[CA19-9 and carcinoembryonic antigen (CEA)].3–6 More-
over, a number of molecular markers such as K-ras,
S100A6, and SMAD4 have also been shown to have
potential for prognostic value following resection.7–10 The
aim of this study was to determine which characteristics or
clinicopathological factors point to an increased possibility
of a long-term survival prognosis.
PATIENTS AND METHODS
Registration of Patients
Between January 1, 1986 and December 31, 2006, 117
patients with primary pancreatic carcinoma underwent
pancreatectomy with D0–D3 lymph node dissection at the
Surgical Department of Kitasato University Hospital.
Among the 117 cases, 106 patients had tubular adenocar-
cinoma; the other 11 patients had invasive mucinous
cystadenocarcinoma (n = 2), invasive carcinoma origi-
nating in an intraductal tumor (n = 3), papillary
adenocarcinoma (n = 4), mucinous carcinoma (n = 1),
and adenosquamous carcinoma (n = 1). Among the 106
tubular adenocarcinoma patients, 10 had double cancer
with life-threatening phenotype, and so we excluded them
from our analysis. Among the remaining 96 pancreatic
tubular adenocarcinoma patients, 6 were classified as JPS
stage 0–II (stage 0, n = 1; stage I, n = 2; stage II, n = 3);
the potential for analysis of survival rates was limited to the
small number of patients in this group, so analysis was
therefore performed to the largest group: those with JPS
stages III–IVb. Our patient distribution was consistent with
the nationwide registry, where most cases are classified as
JPS advanced stage (stages III–IVb), a classification
applicable to 96.2% of patients in our study.11 Of these
remaining 90 patients with invasive tubular adenocarci-
noma of the pancreas, clinicopathological characteristics
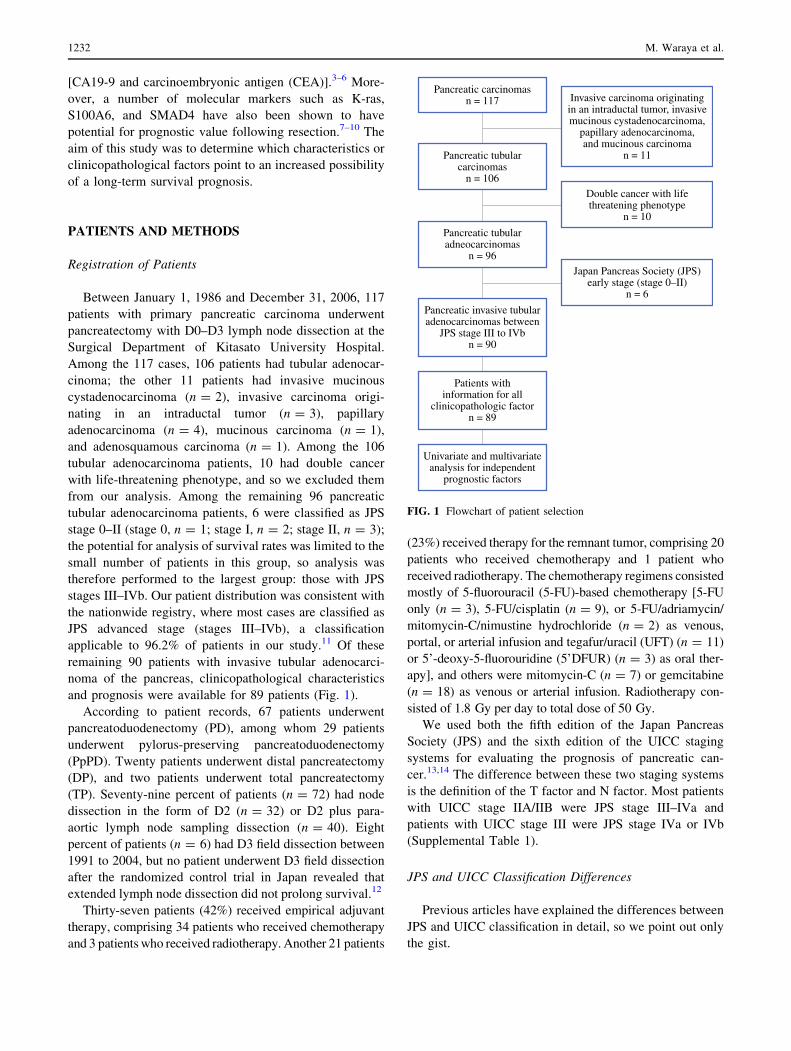
and prognosis were available for 89 patients (Fig. 1).
According to patient records, 67 patients underwent
pancreatoduodenectomy (PD), among whom 29 patients
underwent pylorus-preserving pancreatoduodenectomy
(PpPD). Twenty patients underwent distal pancreatectomy
(DP), and two patients underwent total pancreatectomy
(TP). Seventy-nine percent of patients (n = 72) had node
dissection in the form of D2 (n = 32) or D2 plus para-
aortic lymph node sampling dissection (n = 40). Eight
percent of patients (n = 6) had D3 field dissection between
1991 to 2004, but no patient underwent D3 field dissection
after the randomized control trial in Japan revealed that
extended lymph node dissection did not prolong survival.12
Thirty-seven patients (42%) received empirical adjuvant
therapy, comprising 34 patients who received chemotherapy
and 3 patients who received radiotherapy. Another 21 patients
(23%) received therapy for the remnant tumor, comprising 20
patients who received chemotherapy and 1 patient who
received radiotherapy. The chemotherapy regimens consisted
mostly of 5-fluorouracil (5-FU)-based chemotherapy [5-FU
only (n = 3), 5-FU/cisplatin (n = 9), or 5-FU/adriamycin/
mitomycin-C/nimustine hydrochloride (n = 2) as venous,
portal, or arterial infusion and tegafur/uracil (UFT) (n = 11)
or 5’-deoxy-5-fluorouridine (5’DFUR) (n = 3) as oral ther-
apy], and others were mitomycin-C (n = 7) or gemcitabine
(n = 18) as venous or arterial infusion. Radiotherapy con-
sisted of 1.8 Gy per day to total dose of 50 Gy.
We used both the fifth edition of the Japan Pancreas
Society (JPS) and the sixth edition of the UICC staging
systems for evaluating the prognosis of pancreatic can-
cer.13,14 The difference between these two staging systems
is the definition of the T factor and N factor. Most patients
with UICC stage IIA/IIB were JPS stage III–IVa and
patients with UICC stage III were JPS stage IVa or IVb
(Supplemental Table 1).
JPS and UICC Classification Differences
Previous articles have explained the differences between
JPS and UICC classification in detail, so we point out only
the gist.
Pancreatic carcinomasn = 117
Pancreatic tubularadneocarcinomas
n = 96
Pancreatic invasive tubularadenocarcinomas between
JPS stage III to IVbn = 90
Patients withinformation for all
clinicopathologic factorn = 89
Univariate and multivariateanalysis for independent
prognostic factors
Pancreatic tubularcarcinomas
n = 106
Invasive carcinoma originatingin an intraductal tumor, invasivemucinous cystadenocarcinoma,
papillary adenocarcinoma,and mucinous carcinoma
n = 11
Double cancer with lifethreatening phenotype
n = 10
Japan Pancreas Society (JPS)early stage (stage 0–II)
n = 6
FIG. 1 Flowchart of patient selection
1232 M. Waraya et al.

In the JPS edition, the T category is specified by
determining local invasion of the pancreas and adjacent
structures as absent or present for eight local extension
factors. The descriptions of JPS Tis, T1, and T2 are the
same as those of the UICC sixth edition. JPS T3 is a tumor
in which one or more of intrapancreatic common bile duct
(CH), duodenum (DU), serosa (S), and retropancreatic
tissue (RP) factors are positive, irrespective of tumor size.
JPS T4 is a tumor in which one or more of portal venous
system (PV), arterial system (A), extrapancreatic nerve
plexus (PL), and other organs (OO) factors are positive.
UICC T3 is a tumor that extends beyond the pancreas but
without involvement of the celiac axis or superior mesen-
teric artery. UICC T4 is a tumor that involves the celiac
axis or superior mesenteric artery.
In the JPS edition, the status of lymph node metastasis is
divided into four categories, N0–3, according to whether
metastasis is present in lymph node group 1–3, defined on
the basis of lymph flow. The presence of distant metastasis
is defined as metastasis to the distant organs, peritoneum or
distant lymph nodes in the JPS and UICC classification.
Clinicopathological Factors
All histological and other clinicopathological factors
were judged independently and blindly by histopatholo-
gists, and all histopathologic factors from the General
Rules for the Study of Pancreatic Cancer (JPS fifth edition)
were abstracted from the medical records. The volume of
the stromal connective tissue in cancer (stroma factor) is
classified into three categories: medullary type, small in
volume; scirrhous type, large in volume; intermediate type,
which is neither medullary nor scirrhous. Lymphatic per-
meation (ly) and vascular permeation (v) are defined as ly0,
1, 2, 3 and v0, 1, 2, 3 by infiltrative grade. However, this
classification is subjective; therefore, we classified ly and v
in terms of absence or presence.
The dissected peripancreatic tissue margin (DPM)
includes every surgical margin other than pancreatic cut
end margin (PCM) and bile duct cut end margin (BCM),
i.e., anterior and posterior pancreatic, especially along the
vessels, and can be judged intraoperatively by pathologists.
Currently, lymph node metastatic progression, as lymph
node metastasis density (ND), has been demonstrated to be
one of the most potent predictors of survival.6,15,16 In this
study, we determined optimal cutoff ratio value (6.6%) on
receiver–operating characteristic (ROC) curve analysis
based on prognosis (sensitivity 64%, specificity 78%) (data
not shown), and so defined ND cutoff level as 10% above
or below.
CA19-9 is a carbohydrate antigen with the sialylated
Lewis (sLe)a blood group, and individuals with an Lea-b-
genotype (lacking the Lewis antigen glycosyltransferase)
are unable to synthesize CA19-9 (about 5–7% of the gen-
eral population). CA19-9 expresses on a mucin, a high-
molecular-mass (200–1,000 kD) glycoprotein complex in
serum. The recommended upper limit of normal for CA19-
9 level is 37 U/ml, when CA19-9 levels were determined
and defined from the standard deviations of normal, healthy
people by using a chemiluminescent enzyme immunoassay
kit manufactured by Fujirebio Limited (Tokyo, Japan). In
this study, 89 patients had documented preoperative serum
CA19-9 levels, which were obtained just before operation,
avoiding the effects of obstructive jaundice and/or
inflammation of the hepatobiliary tree. Forty-four patients
had obstructive jaundice before surgery and 41 patients
were treated with biliary juice drainage. Among these 41
patients, 23 patients obtained a normal total bilirubin level,
but 18 patients, after draining of biliary juice, were still
above the upper limit of normal before surgery: the range
of total bilirubin (T.Bil.)/direct bilirubin (D.Bil.) was
reduced from 8.6/6.8–1.6/0.9 to 29.9/24.4–4.4/3.9 mg/dl.
The three other patients with obstructive jaundice had
operations without biliary juice drainage (range of T.Bil./
D.Bil.: 1.6/1.1- 4.3/4.2 mg/dl).
Statistical Analysis
Kaplan–Meier method was used for the 5-year disease-
specific survival (DSS) analysis, and the difference in
survival rate was assessed by log-rank test.17 DSS was
measured from date of operation to date of death or last
follow-up. Patients who died from causes other than pan-
creatic cancer (n = 16) and those with more than
60 months survival were regarded as censored or excluded
at the time of death or 60 months, respectively.
The variables that had prognostic potential suggested by
univariate analysis (P \ 0.05) were subjected to multi-
variate analysis with the logistic model.18 A value of
P \ 0.05 was considered to indicate statistical significance.
All statistical analyses were done with the SAS software
package StatView, version 5.0 (SAS Institute, Cary, NC).
RESULTS
Patient Characteristics and Univariate Prognostic
Analysis in Advanced Pancreatic Cancer (JPS stage
III–IVb)
The characteristics of 89 pancreatic cancer patients in
this study (44 men and 45 women) are summarized in
Table 1. Median age was 63 years (range 39–85 years).
Comparison of the 5-year DSS curves according to stage
revealed that stratification was more homogeneous in the
JPS classifications of stage III–IVb (UICC stage IIA–IV)
Determiners of Long-Term Survival in Pancreatic Cancer 1233
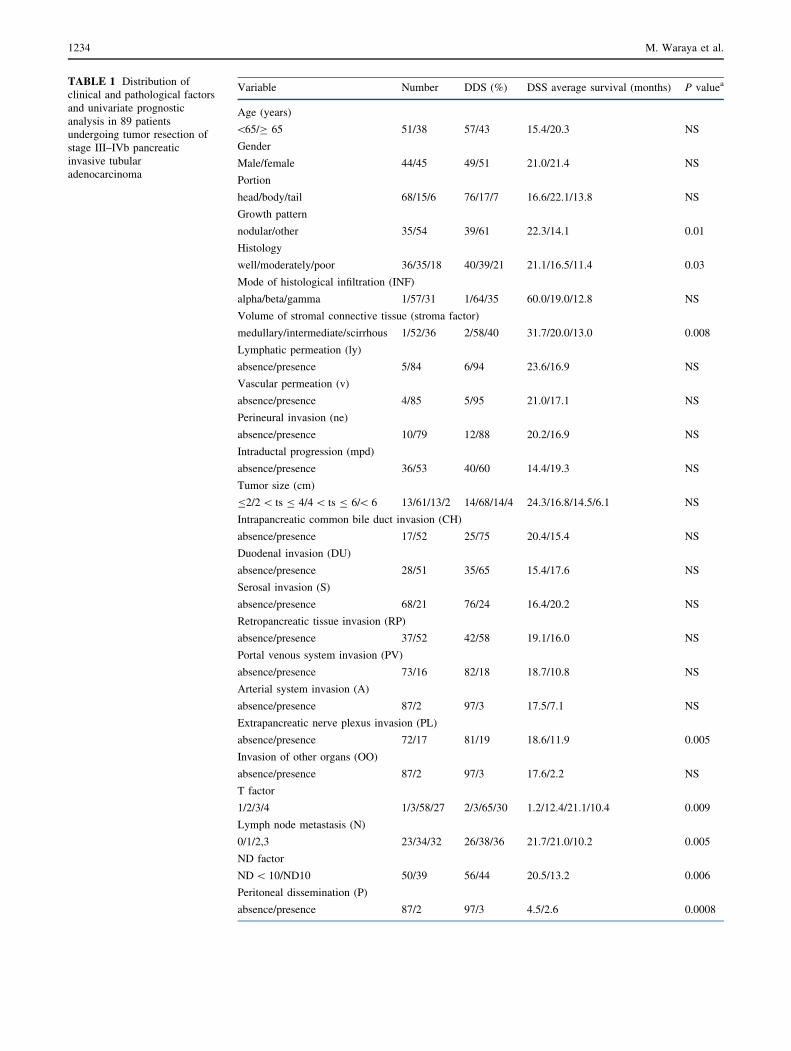
TABLE 1 Distribution of
clinical and pathological factors
and univariate prognostic
analysis in 89 patients
undergoing tumor resection of
stage III–IVb pancreatic
invasive tubular
adenocarcinoma
Variable Number DDS (%) DSS average survival (months) P valuea
Age (years)
\65/C 65 51/38 57/43 15.4/20.3 NS
Gender
Male/female 44/45 49/51 21.0/21.4 NS
Portion
head/body/tail 68/15/6 76/17/7 16.6/22.1/13.8 NS
Growth pattern
nodular/other 35/54 39/61 22.3/14.1 0.01
Histology
well/moderately/poor 36/35/18 40/39/21 21.1/16.5/11.4 0.03
Mode of histological infiltration (INF)
alpha/beta/gamma 1/57/31 1/64/35 60.0/19.0/12.8 NS
Volume of stromal connective tissue (stroma factor)
medullary/intermediate/scirrhous 1/52/36 2/58/40 31.7/20.0/13.0 0.008
Lymphatic permeation (ly)
absence/presence 5/84 6/94 23.6/16.9 NS
Vascular permeation (v)
absence/presence 4/85 5/95 21.0/17.1 NS
Perineural invasion (ne)
absence/presence 10/79 12/88 20.2/16.9 NS
Intraductal progression (mpd)
absence/presence 36/53 40/60 14.4/19.3 NS
Tumor size (cm)
B2/2 \ ts B 4/4 \ ts B 6/\ 6 13/61/13/2 14/68/14/4 24.3/16.8/14.5/6.1 NS
Intrapancreatic common bile duct invasion (CH)
absence/presence 17/52 25/75 20.4/15.4 NS
Duodenal invasion (DU)
absence/presence 28/51 35/65 15.4/17.6 NS
Serosal invasion (S)
absence/presence 68/21 76/24 16.4/20.2 NS
Retropancreatic tissue invasion (RP)
absence/presence 37/52 42/58 19.1/16.0 NS
Portal venous system invasion (PV)
absence/presence 73/16 82/18 18.7/10.8 NS
Arterial system invasion (A)
absence/presence 87/2 97/3 17.5/7.1 NS
Extrapancreatic nerve plexus invasion (PL)
absence/presence 72/17 81/19 18.6/11.9 0.005
Invasion of other organs (OO)
absence/presence 87/2 97/3 17.6/2.2 NS
T factor
1/2/3/4 1/3/58/27 2/3/65/30 1.2/12.4/21.1/10.4 0.009
Lymph node metastasis (N)
0/1/2,3 23/34/32 26/38/36 21.7/21.0/10.2 0.005
ND factor
ND \ 10/ND10 50/39 56/44 20.5/13.2 0.006
Peritoneal dissemination (P)
absence/presence 87/2 97/3 4.5/2.6 0.0008
1234 M. Waraya et al.
than in the UICC classifications (Supplemental Fig. 1).
Therefore, we adopted the JPS classification staging system
for patient prognosis in our study. Table 1 also presents the
univariate prognostic factors of the 89 JPS stage III–IVb
patients on 5-year DSS: JPS stage (P \ 0.0001), preoper-
ative serum CA19-9 level (preCA19-9; P \ 0.0001),
distant metastasis (M factor; P \ 0.0001), dissected peri-
pancreatic tissue margin (DPM; P \ 0.0001), residual
tumor (R factor; P = 0.0007), peritoneal dissemination (P
factor; P = 0.0008), hepatic metastasis (H factor;
P = 0.004), lymph node metastasis (N factor; P = 0.005),
extrapancreatic nerve plexus (PL factor; P = 0.005),
lymph node metastasis density over 10% (ND10;
P = 0.006), volume of the stromal connective tissue
(stroma factor; P = 0.008), T factor (P = 0.009), growth
pattern (P = 0.01), and histology (P = 0.03), which were
all significantly associated with poor outcome in advanced
pancreatic cancer.
Multivariate Prognostic Analysis in Advanced
Pancreatic Cancer (JPS Stage III–IVb)
The eight variables that had prognostic potential sug-
gested by the univariate analysis (P \ 0.05): JPS stage,
preCA19-9, DPM, R factor, ND10, stroma factor, growth
pattern, and histology, were subjected to multivariate
analysis, in which staging factors were excluded, i.e., M
factor, P factor, H factor, N factor, T factor, and PL factor.
This analysis revealed that preCA19-9 (P = 0.0006,
RR = 2.16) and DPM (P = 0.04, RR = 1.62) were the
only remaining prognostic factors independent of JPS stage
(P = 0.001) (Table 2). Kaplan–Meier curves of the two
independent prognostic factors are shown in Fig. 2. Mul-
tivariate analysis including staging factors could not be
performed by the SAS software package StatView, version
5.0, because too many relative factors would have to be
included for analysis.
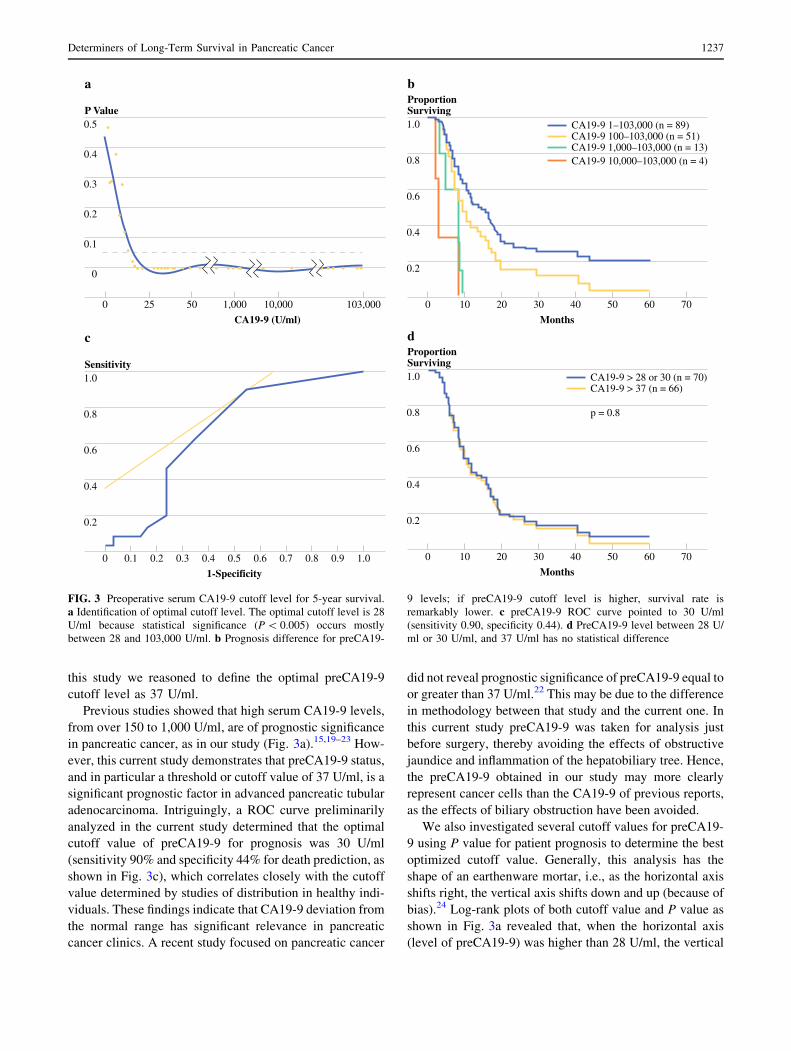
Prognostic Impact of preCA19-9
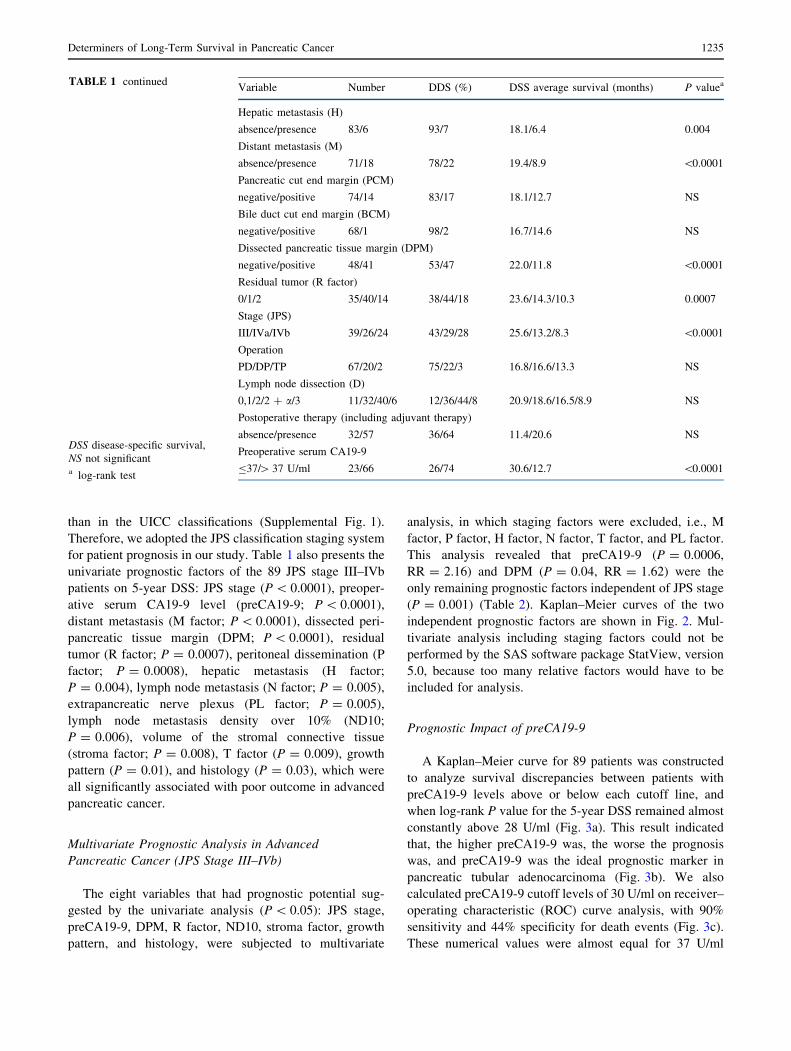
A Kaplan–Meier curve for 89 patients was constructed
to analyze survival discrepancies between patients with
preCA19-9 levels above or below each cutoff line, and
when log-rank P value for the 5-year DSS remained almost
constantly above 28 U/ml (Fig. 3a). This result indicated
that, the higher preCA19-9 was, the worse the prognosis
was, and preCA19-9 was the ideal prognostic marker in
pancreatic tubular adenocarcinoma (Fig. 3b). We also
calculated preCA19-9 cutoff levels of 30 U/ml on receiver–
operating characteristic (ROC) curve analysis, with 90%
sensitivity and 44% specificity for death events (Fig. 3c).
These numerical values were almost equal for 37 U/ml
TABLE 1 continued
DSS disease-specific survival,
NS not significanta log-rank test
Variable Number DDS (%) DSS average survival (months) P valuea
Hepatic metastasis (H)
absence/presence 83/6 93/7 18.1/6.4 0.004
Distant metastasis (M)
absence/presence 71/18 78/22 19.4/8.9 \0.0001
Pancreatic cut end margin (PCM)
negative/positive 74/14 83/17 18.1/12.7 NS
Bile duct cut end margin (BCM)
negative/positive 68/1 98/2 16.7/14.6 NS
Dissected pancreatic tissue margin (DPM)
negative/positive 48/41 53/47 22.0/11.8 \0.0001
Residual tumor (R factor)
0/1/2 35/40/14 38/44/18 23.6/14.3/10.3 0.0007
Stage (JPS)
III/IVa/IVb 39/26/24 43/29/28 25.6/13.2/8.3 \0.0001
Operation
PD/DP/TP 67/20/2 75/22/3 16.8/16.6/13.3 NS
Lymph node dissection (D)
0,1/2/2 ? a/3 11/32/40/6 12/36/44/8 20.9/18.6/16.5/8.9 NS
Postoperative therapy (including adjuvant therapy)
absence/presence 32/57 36/64 11.4/20.6 NS
Preoperative serum CA19-9
B37/[ 37 U/ml 23/66 26/74 30.6/12.7 \0.0001
Determiners of Long-Term Survival in Pancreatic Cancer 1235
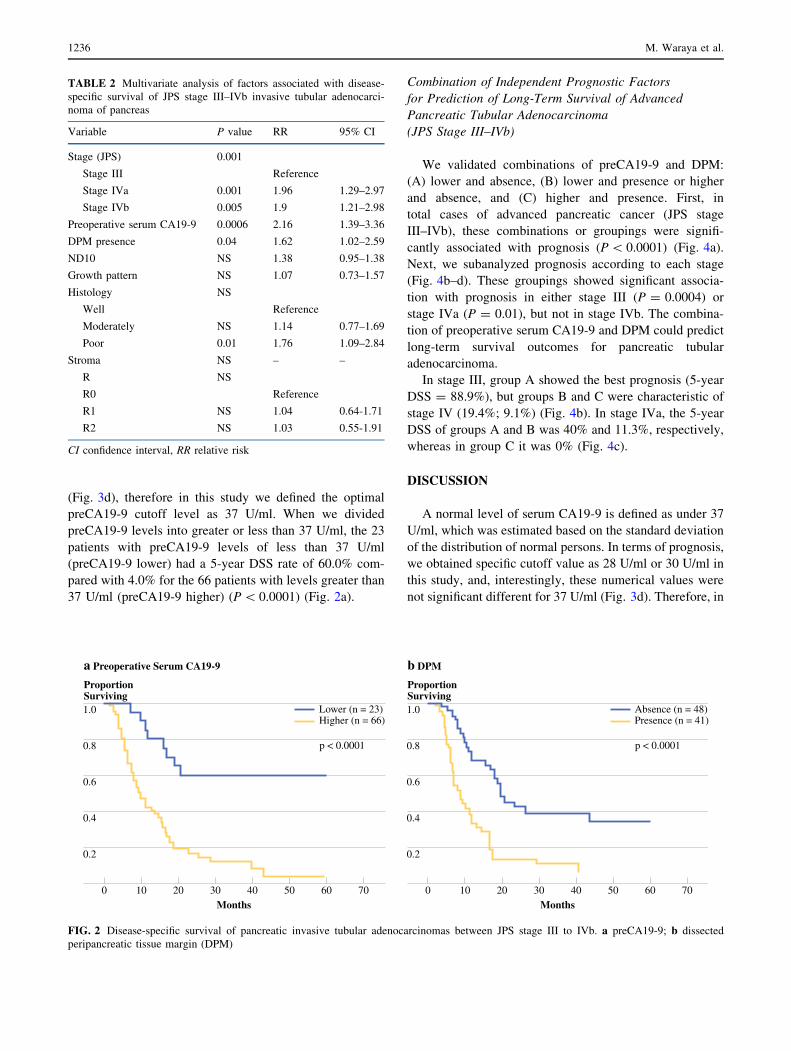
(Fig. 3d), therefore in this study we defined the optimal
preCA19-9 cutoff level as 37 U/ml. When we divided
preCA19-9 levels into greater or less than 37 U/ml, the 23
patients with preCA19-9 levels of less than 37 U/ml
(preCA19-9 lower) had a 5-year DSS rate of 60.0% com-
pared with 4.0% for the 66 patients with levels greater than
37 U/ml (preCA19-9 higher) (P \ 0.0001) (Fig. 2a).
Combination of Independent Prognostic Factors
for Prediction of Long-Term Survival of Advanced
Pancreatic Tubular Adenocarcinoma
(JPS Stage III–IVb)
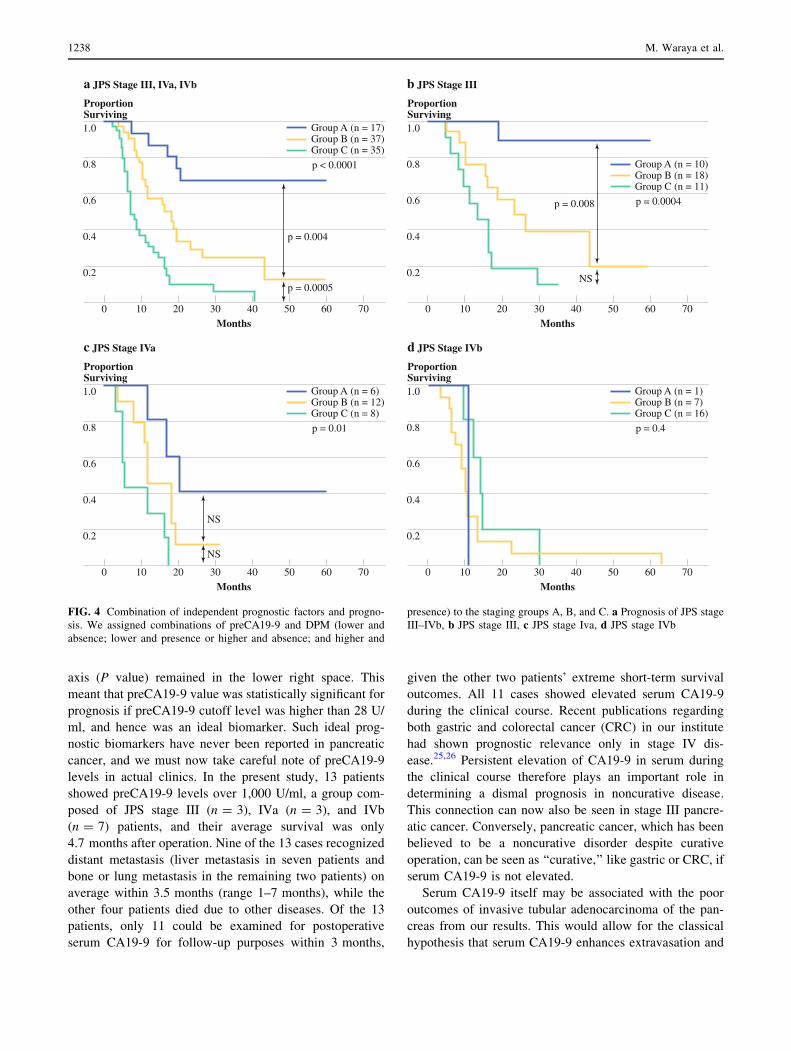
We validated combinations of preCA19-9 and DPM:
(A) lower and absence, (B) lower and presence or higher
and absence, and (C) higher and presence. First, in
total cases of advanced pancreatic cancer (JPS stage
III–IVb), these combinations or groupings were signifi-
cantly associated with prognosis (P \ 0.0001) (Fig. 4a).
Next, we subanalyzed prognosis according to each stage
(Fig. 4b–d). These groupings showed significant associa-
tion with prognosis in either stage III (P = 0.0004) or
stage IVa (P = 0.01), but not in stage IVb. The combina-
tion of preoperative serum CA19-9 and DPM could predict
long-term survival outcomes for pancreatic tubular
adenocarcinoma.
In stage III, group A showed the best prognosis (5-year
DSS = 88.9%), but groups B and C were characteristic of
stage IV (19.4%; 9.1%) (Fig. 4b). In stage IVa, the 5-year
DSS of groups A and B was 40% and 11.3%, respectively,
whereas in group C it was 0% (Fig. 4c).
DISCUSSION
A normal level of serum CA19-9 is defined as under 37
U/ml, which was estimated based on the standard deviation
of the distribution of normal persons. In terms of prognosis,
we obtained specific cutoff value as 28 U/ml or 30 U/ml in
this study, and, interestingly, these numerical values were
not significant different for 37 U/ml (Fig. 3d). Therefore, in
TABLE 2 Multivariate analysis of factors associated with disease-
specific survival of JPS stage III–IVb invasive tubular adenocarci-
noma of pancreas
Variable P value RR 95% CI
Stage (JPS) 0.001
Stage III Reference
Stage IVa 0.001 1.96 1.29–2.97
Stage IVb 0.005 1.9 1.21–2.98
Preoperative serum CA19-9 0.0006 2.16 1.39–3.36
DPM presence 0.04 1.62 1.02–2.59
ND10 NS 1.38 0.95–1.38
Growth pattern NS 1.07 0.73–1.57
Histology NS
Well Reference
Moderately NS 1.14 0.77–1.69
Poor 0.01 1.76 1.09–2.84
Stroma NS – –
R NS
R0 Reference
R1 NS 1.04 0.64-1.71
R2 NS 1.03 0.55-1.91
CI confidence interval, RR relative risk
1.0
0.8
0.6
0.4
0.2
0 70Months
4020 50 603010
ProportionSurviving
a Preoperative Serum CA19-9
Lower (n = 23)Higher (n = 66)
p < 0.0001
1.0
0.8
0.6
0.4
0.2
0 70Months
4020 50 603010
ProportionSurviving
b DPM
Absence (n = 48)Presence (n = 41)
p < 0.0001
FIG. 2 Disease-specific survival of pancreatic invasive tubular adenocarcinomas between JPS stage III to IVb. a preCA19-9; b dissected
peripancreatic tissue margin (DPM)
1236 M. Waraya et al.
this study we reasoned to define the optimal preCA19-9
cutoff level as 37 U/ml.
Previous studies showed that high serum CA19-9 levels,
from over 150 to 1,000 U/ml, are of prognostic significance
in pancreatic cancer, as in our study (Fig. 3a).15,19–23 How-
ever, this current study demonstrates that preCA19-9 status,
and in particular a threshold or cutoff value of 37 U/ml, is a
significant prognostic factor in advanced pancreatic tubular
adenocarcinoma. Intriguingly, a ROC curve preliminarily
analyzed in the current study determined that the optimal
cutoff value of preCA19-9 for prognosis was 30 U/ml
(sensitivity 90% and specificity 44% for death prediction, as
shown in Fig. 3c), which correlates closely with the cutoff
value determined by studies of distribution in healthy indi-
viduals. These findings indicate that CA19-9 deviation from
the normal range has significant relevance in pancreatic
cancer clinics. A recent study focused on pancreatic cancer
did not reveal prognostic significance of preCA19-9 equal to
or greater than 37 U/ml.22 This may be due to the difference
in methodology between that study and the current one. In
this current study preCA19-9 was taken for analysis just
before surgery, thereby avoiding the effects of obstructive
jaundice and inflammation of the hepatobiliary tree. Hence,
the preCA19-9 obtained in our study may more clearly
represent cancer cells than the CA19-9 of previous reports,
as the effects of biliary obstruction have been avoided.
We also investigated several cutoff values for preCA19-
9 using P value for patient prognosis to determine the best
optimized cutoff value. Generally, this analysis has the
shape of an earthenware mortar, i.e., as the horizontal axis
shifts right, the vertical axis shifts down and up (because of
bias).24 Log-rank plots of both cutoff value and P value as
shown in Fig. 3a revealed that, when the horizontal axis
(level of preCA19-9) was higher than 28 U/ml, the vertical
0.5
0.4
0.3
0.2
0
0.1
0 103,000
CA19-9 (U/ml)
10,00050 1,00025
P Value
a
1.0
0.8
0.6
0.4
0.2
0 70
Months
4020 50 603010
ProportionSurviving
b
CA19-9 1–103,000 (n = 89)CA19-9 100–103,000 (n = 51)CA19-9 1,000–103,000 (n = 13)CA19-9 10,000–103,000 (n = 4)
1.0
0.8
0.6
0.4
0.2
0 70
Months
4020 50 603010
ProportionSurviving
d
CA19-9 > 28 or 30 (n = 70)CA19-9 > 37 (n = 66)
p = 0.8
1.0
0.8
0.6
0.4
0.2
0 1.0
1-Specificity
0.40.2 0.8 0.90.3 0.6 0.70.50.1
Sensitivity
c
FIG. 3 Preoperative serum CA19-9 cutoff level for 5-year survival.
a Identification of optimal cutoff level. The optimal cutoff level is 28
U/ml because statistical significance (P \ 0.005) occurs mostly
between 28 and 103,000 U/ml. b Prognosis difference for preCA19-
9 levels; if preCA19-9 cutoff level is higher, survival rate is
remarkably lower. c preCA19-9 ROC curve pointed to 30 U/ml
(sensitivity 0.90, specificity 0.44). d PreCA19-9 level between 28 U/
ml or 30 U/ml, and 37 U/ml has no statistical difference
Determiners of Long-Term Survival in Pancreatic Cancer 1237
axis (P value) remained in the lower right space. This
meant that preCA19-9 value was statistically significant for
prognosis if preCA19-9 cutoff level was higher than 28 U/
ml, and hence was an ideal biomarker. Such ideal prog-
nostic biomarkers have never been reported in pancreatic
cancer, and we must now take careful note of preCA19-9
levels in actual clinics. In the present study, 13 patients
showed preCA19-9 levels over 1,000 U/ml, a group com-
posed of JPS stage III (n = 3), IVa (n = 3), and IVb
(n = 7) patients, and their average survival was only
4.7 months after operation. Nine of the 13 cases recognized
distant metastasis (liver metastasis in seven patients and
bone or lung metastasis in the remaining two patients) on
average within 3.5 months (range 1–7 months), while the
other four patients died due to other diseases. Of the 13
patients, only 11 could be examined for postoperative
serum CA19-9 for follow-up purposes within 3 months,
given the other two patients’ extreme short-term survival
outcomes. All 11 cases showed elevated serum CA19-9
during the clinical course. Recent publications regarding
both gastric and colorectal cancer (CRC) in our institute
had shown prognostic relevance only in stage IV dis-
ease.25,26 Persistent elevation of CA19-9 in serum during
the clinical course therefore plays an important role in
determining a dismal prognosis in noncurative disease.
This connection can now also be seen in stage III pancre-
atic cancer. Conversely, pancreatic cancer, which has been
believed to be a noncurative disorder despite curative
operation, can be seen as ‘‘curative,’’ like gastric or CRC, if
serum CA19-9 is not elevated.
Serum CA19-9 itself may be associated with the poor
outcomes of invasive tubular adenocarcinoma of the pan-
creas from our results. This would allow for the classical
hypothesis that serum CA19-9 enhances extravasation and
1.0
0.8
0.6
0.4
0.2
0 70Months
4020 50 603010
ProportionSurviving
a JPS Stage III, IVa, IVb
Group A (n = 17)Group B (n = 37)Group C (n = 35)
p < 0.0001
p = 0.004
p = 0.0005
1.0
0.8
0.6
0.4
0.2
0 70Months
4020 50 603010
ProportionSurviving
c JPS Stage IVa
Group A (n = 6)Group B (n = 12)Group C (n = 8)
p = 0.01
NS
NS
1.0
0.8
0.6
0.4
0.2
0 70Months
4020 50 603010
ProportionSurviving
b JPS Stage III
Group A (n = 10)Group B (n = 18)Group C (n = 11)
p = 0.0004p = 0.008
NS
1.0
0.8
0.6
0.4
0.2
0 70Months
4020 50 603010
ProportionSurviving
d JPS Stage IVb
Group A (n = 1)Group B (n = 7)Group C (n = 16)
p = 0.4
FIG. 4 Combination of independent prognostic factors and progno-
sis. We assigned combinations of preCA19-9 and DPM (lower and
absence; lower and presence or higher and absence; and higher and
presence) to the staging groups A, B, and C. a Prognosis of JPS stage
III–IVb, b JPS stage III, c JPS stage Iva, d JPS stage IVb
1238 M. Waraya et al.

metastasis by interaction with E-selectin expressed on
endothelium.27 Recent publications additionally propose
emerging mechanisms of serum CA19-9 involving
systemic dissemination of cancer cells. (1) Mucins
expressing CA19-9 were associated with the induction of
inflammatory molecules such as interleukin-6 (IL-6) and
prostaglandin (PGE2) in human cancer, and such inflam-
matory status is a prerequisite for systemic metastasis.28,29
(2) P-selectin, another specific ligand for serum CA19-9,
may be involved in promoting tumor aggregation with
platelets, leading to systemic cancer spread.30,31 Matsum-
oto et al. actually showed that blocking serum CA19-9 by
cimetidine is beneficial to CRC patients’ outcomes, and
therefore, antagonism with CA19-9 inhibitors might have
great potential to inhibit tumor metastasis.32,33
Resection status (R factor) has produced mixed results
as a prognostic factor.34–39 In this study, R factor was
eliminated as an independent prognostic factor, while
DPM, one part of R factor, was used. Of the 41 patients
with DPM present, 38 patients (93%) had positive retro-
pancreatic tissue margin, suggesting that DPM actually
represents retropancreatic tissue invasion. Previous studies
have emphasized the importance of tumor-free retroperi-
toneal tissue for patient survival after the resection of
ductal adenocarcinoma of the head of the pancreas.11,40,41
On the other hand, Luttges et al. and Westgaard et al. could
not demonstrate significant difference according to retro-
peritoneal tissue margin status, therefore it was necessary
to establish whether the retroperitoneal margin status was
significant for prognosis.42,43 Both preCA19-9 and DPM
can be informative during surgery (histopathologists can
diagnose DPM intraoperatively with a quick histopatholo-
gical diagnosis), and the information may influence
operative procedures during the operation.
Surgical margin status may, however, simply represent
an invasive phenotype of pancreatic cancer, rather than the
result of operative treatment. If so, we must identify the
oncogene involved in such malignancy for novel molecular
targeting. Reflecting this possibility, randomized trials
actually concluded that the addition of extended lym-
phadenectomy and retroperitoneal soft tissue clearance did
not significantly improve patient prognosis.12,44–47 Never-
theless, surgical resection has provided the only chance for
long-term survival in pancreatic cancer, and in consider-
ation of the present study, an attempt at complete clearance
of retroperitoneal tumor tissue (DPM absence) may be
worthwhile for those patients with putative pathological
stage III–IVa, when preCA19-9 levels are in the lower
range.
Finally, this is a retrospective study over 20 years with
89 patients included for analysis. So, this study might
suffer from bias, i.e., change in treatment strategy such
as range of lymph node dissection and application of
chemoradiotherapy, and learning curve. Prospective vali-
dation is further needed to clarify the relationship between
preCA19-9 and DPM, and prognosis in invasive tubular
adenocarcinoma of the pancreas.
REFERENCES
1. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CACancer J Clin. 2008;58(2):71-96. Epub 2008 Feb 20.
2. Matsuno S, Egawa S, Fukuyama S, et al. Pancreatic Cancer
Registry in Japan: 20 years of experience. Pancreas. 2004;28(3):
219-30.
3. Benassai G, Mastrorilli M, Quarto G, et al. Factors influencing
survival after resection for ductal adenocarcinoma of the head of
the pancreas. J Surg Oncol. 2000;73(4):212-8.
4. Ni XG, Bai XF, Mao YL, et al. The clinical value of serum CEA,
CA19-9, and CA242 in the diagnosis and prognosis of pancreatic
cancer. Eur J Surg Oncol. 2005;31(2):164-9.
5. Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreati-
coduodenectomies for pancreatic cancer: A single-institution
experience. J Gastrointest Surg. 2006;10(9):1199-210; discussion
1210-1.
6. Smith RA, Bosonnet L, Ghaneh P, et al. Preoperative CA19-9
levels and lymph node ratio are independent predictors of sur-
vival in patients with resected pancreatic ductal adenocarcinoma.
Dig Surg. 2008;25(3):226-232.
7. Kim J, Reber HA, Dry SM, et al. Unfavourable prognosis asso-
ciated with K-ras gene mutation in pancreatic cancer surgical
margins. Gut. 2006;55(11):1598-605. Epub 2006 May 8.
8. Vimalachandran D, Greenhalf W, Thompson C, et al. High
nuclear S100A6 (Calcyclin) is significantly associated with poor
survival in pancreatic cancer patients. Cancer Res. 2005;65(8):
3218-25.
9. Tascilar M, Skinner HG, Rosty C, et al. The SMAD4 protein and
prognosis of pancreatic ductal adenocarcinoma. Clin Cancer Res.2001;7(12):4115-21.
10. Kawesha A, Ghaneh P, Andren-Sandberg A, et al. K-ras onco-
gene subtype mutations are associated with survival but not
expression of p53, p16(INK4A), p21(WAF-1), cyclin D1, erbB-2
and erbB-3 in resected pancreatic ductal adenocarcinoma. Int JCancer. 2000;89(6):469-74.
11. Nakao A, Fujii T, Sugimoto H, et al. Oncological problems in
pancreatic cancer surgery. World J Gastroenterol. 2006;12(28):
4466-72.
12. Nimura Y, Nagino M, Kato H, et al. Regional versus extended
lymph node dissection in radical pancreatoduodenectomy for pan-
creatic cancer: a multicenter, randomized contorolled trial. OfficialJ Int Hepatopancreatobiliary Assoc. 2004;6:(supplement I)2.
13. Japan Pancreas Society, ed. General rules for study of pancreatic
cancer, April 2002 (5th ed). Tokyo: Kanahara; 2002.
14. Sobin LH, Wittekind CH, ed. International Union Againt Cancer
(UICC): TNM classification of malignant tumors, 6th ed. New
York: Wiley and Liss; 2002.
15. Slidell MB, Chang DC, Cameron JL, et al. Impact of total lymph
node count and lymph node ratio on staging and survival after
pancreatectomy for pancreatic adenocarcinoma: a large, popula-
tion-based analysis. Ann Surg Oncol. 2008;15(1):165-74. Epub
2007 Sep 26.
16. Schwarz RE, Smith DD. Extent of lymph node retrieval and
pancreatic cancer survival: information from a large US popu-
lation database. Ann Surg Oncol. 2006;13(9):1189-200. Epub
2006 Sep 6.
17. Kaplan EL, Meier P. Nonparametric estimation from incomplete
observations. J Am Stat Assoc. 1958;53(282):457-481.
Determiners of Long-Term Survival in Pancreatic Cancer 1239
18. Cox DR. Regression models and life-tables. J R Stat Soc B(Methdological). 1972;34(2):187-220.
19. Sperti C, Pasquali C, Catalini S, et al. CA 19-9 as a prognostic
index after resection for pancreatic cancer. J Surg Oncol. 1993;
52(3):137-41.
20. Lundin J, Roberts PJ, Kuusela P, Haglund C. The prognostic
value of preoperative serum levels of CA 19-9 and CEA in
patients with pancreatic cancer. Br J Cancer. 1994;69(3):515-9.
21. Berger AC, Meszoely IM, Ross EA, Watson JC, Hoffman JP.
Undetectable preoperative levels of serum CA 19-9 correlate
with improved survival for patients with resectable pancreatic
adenocarcinoma. Ann Surg Oncol. 2004;11(7):644-9. Epub 2004
Jun 14.
22. Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, Fer-
nandez-del Castillo C, Warshaw AL. Perioperative CA19-9 levels
can predict stage and survival in patients with resectable pan-
creatic adenocarcinoma. J Clin Oncol. 2006;24(18):2897-902.
23. Zhang S, Wang YM, Sun CD, Lu Y, Wu LQ. Clinical value of
serum CA19-9 levels in evaluating resectability of pancreatic
carcinoma. World J Gastroenterol. 2008;14(23):3750-3.
24. Mandelker DL, Yamashita K, Tokumaru Y, et al. PGP95 pro-
moter methylation is an independent prognostic factor for
esophageal squamous cell carcinoma. Cancer Res. 2005;65(11):
4963-8.
25. Yamashita K, Sakuramoto S, Kikuchi S, Katada N, Kobayashi N,
Watanabe M. Surgical resection of stage IV gastric cancer and
prognosis. Anticancer Res. 2007;27(6):4381-6.
26. Katoh H, Yamashita K, Kokuba Y, et al. Surgical resection of
stage IV colorectal cancer and prognosis. World J Surg. 2008;
32(6):1130-7.
27. Magnani JL. The discovery, biology, and drug development of
sialyl Lea and sialyl Lex. Arch Biochem Biophys. 2004;426(2):
122-31.
28. Yokoigawa N, Takeuchi N, Toda M, et al. Enhanced production
of interleukin 6 in peripheral blood monocytes stimulated with
mucins secreted into the bloodstream. Clin Cancer Res. 2005;
11(17):6127-32.
29. Yokoigawa N, Takeuchi N, Toda M, et al. Overproduction of
PGE2 in peripheral blood monocytes of gastrointestinal cancer
patients with mucins in their bloodstream. Cancer Lett. 2007;
245(1-2):149-55. Epub 2006 Feb 20.
30. Kannagi R, Izawa M, Koike T, Miyazaki K, Kimura N. Carbo-
hydrate-mediated cell adhesion in cancer metastasis and
angiogenesis. Cancer Sci. 2004;95(5):377-84.
31. Honn KV, Tang DG, Crissman JD. Platelets and cancer
metastasis: a causal relationship? Cancer Metastasis Rev. 1992;
11(3-4):325-51.
32. Matsumoto S. Cimetidine and survival with colorectal cancer.
Lancet. 1995;346(8967):115.
33. Matsumoto S, Imaeda Y, Umemoto S, Kobayashi K, Suzuki H,
Okamoto T. Cimetidine increases survival of colorectal cancer
patients with high levels of sialyl Lewis-X and sialyl Lewis-A
epitope expression on tumour cells. Br J Cancer. 2002;86(2):
161-7.
34. Takai S, Satoi S, Toyokawa H, et al. Clinicopathologic evaluation
after resection for ductal adenocarcinoma of the pancreas: a
retrospective, single-institution experience. Pancreas. 2003;26(3):
243-9.
35. Richter A, Niedergethmann M, Sturm JW, Lorenz D, Post S,
Trede M. Long-term results of partial pancreaticoduodenectomy
for ductal adenocarcinoma of the pancreatic head: 25-year
experience. World J Surg. 2003;27(3):324-9. Epub 2003 Feb 27.
36. Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Buchler
MW. Curative resection is the single most important factor
determining outcome in patients with pancreatic adenocarcinoma.
Br J Surg. 2004;91(5):586-94.
37. Verbeke CS. Resection margins and R1 rates in pancreatic can-
cer–are we there yet? Histopathology. 2008;52(7):787-96. Epub
2007 Dec 13.
38. Raut CP, Tseng JF, Sun CC, et al. Impact of resection status on
pattern of failure and survival after pancreaticoduodenectomy for
pancreatic adenocarcinoma. Ann Surg. 2007;246(1):52-60.
39. Esposito I, Kleeff J, Bergmann F, et al. Most pancreatic cancer
resections are R1 resections. Ann Surg Oncol. 2008;15(6):1651-
60. Epub 2008 Mar 20.
40. Takahashi S, Ogata Y, Tsuzuki T. Combined resection of the
pancreas and portal vein for pancreatic cancer. Br J Surg. 1994;
81(8):1190-3.
41. Nakao A, Takeda S, Sakai M, et al. Extended radical resection
versus standard resection for pancreatic cancer: the rationale for
extended radical resection. Pancreas. 2004;28(3):289-92.
42. Luttges J, Vogel I, Menke M, Henne-Bruns D, Kremer B,
Kloppel G. The retroperitoneal resection margin and vessel
involvement are important factors determining survival after
pancreaticoduodenectomy for ductal adenocarcinoma of the head
of the pancreas. Virchows Arch. 1998;433(3):237-42.
43. Westgaard A, Tafjord S, Farstad IN, et al. Resectable adenocar-
cinomas in the pancreatic head: the retroperitoneal resection
margin is an independent prognostic factor. BMC Cancer.2008;8:5.
44. Pedrazzoli S, DiCarlo V, Dionigi R, et al. Standard versus
extended lymphadenectomy associated with pancreatoduodenec-
tomy in the surgical treatment of adenocarcinoma of the head of
the pancreas: a multicenter, prospective, randomized study.
Lymphadenectomy Study Group. Ann Surg. 1998;228(4):508-17.
45. Yeo CJ, Cameron JL, Lillemoe KD, et al. Pancreaticoduoden-
ectomy with or without distal gastrectomy and extended
retroperitoneal lymphadenectomy for periampullary adenocarci-
noma, part 2: randomized controlled trial evaluating survival,
morbidity, and mortality. Ann Surg. 2002;236(3):355-66; dis-
cussion 366-8.
46. Capussotti L, Massucco P, Ribero D, Vigano L, Muratore A,
Calgaro M. Extended lymphadenectomy and vein resection for
pancreatic head cancer: outcomes and implications for therapy.
Arch Surg. 2003;138(12):1316-22.
47. Farnell MB, Pearson RK, Sarr MG, et al. A prospective
randomized trial comparing standard pancreatoduodenectomy
with pancreatoduodenectomy with extended lymphadenectomy in
resectable pancreatic head adenocarcinoma. Surgery. 2005;138(4):
618-28; discussion 628-30.
1240 M. Waraya et al.
Related Documents











