Page 1/23 Preoperative dose-dense docetaxel and cyclophosphamide alternating with epirubicin and cisplatin(ddDCEP): an effective, novel way of incorporating platinum in the treatment of early TNBC Ashish Singh Christian Medical College and Hospital: Christian Medical College Vellore Josh Thomas Georgy ( [email protected] ) Christian Medical College and Hospital: Christian Medical College Vellore https://orcid.org/0000-0002- 7119-9710 Ajoy Oommen John Christian Medical College and Hospital: Christian Medical College Vellore Divya Bala Thumaty Christian Medical College and Hospital: Christian Medical College Vellore Anjana Joel Christian Medical College and Hospital: Christian Medical College Vellore Parth Sharma Christian Medical College and Hospital: Christian Medical College Vellore Anand George Andrews Christian Medical College and Hospital: Christian Medical College Vellore Shalom Patole Johns Hopkins University School of Medicine Grace Rebekah Christian Medical College and Hospital: Christian Medical College Vellore Elanthenral Sigamani Christian Medical College and Hospital: Christian Medical College Vellore Marie Therese Manipadam Christian Medical College and Hospital: Christian Medical College Vellore Anish Jacob Cherian Christian Medical College and Hospital: Christian Medical College Vellore Deepak Thomas Abraham Christian Medical College and Hospital: Christian Medical College Vellore Mazhuvanchary Jacob Paul

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Page 1/23
Preoperative dose-dense docetaxel andcyclophosphamide alternating with epirubicin andcisplatin(ddDCEP): an effective, novel way ofincorporating platinum in the treatment of earlyTNBCAshish Singh
Christian Medical College and Hospital: Christian Medical College VelloreJosh Thomas Georgy ( [email protected] )
Christian Medical College and Hospital: Christian Medical College Vellore https://orcid.org/0000-0002-7119-9710Ajoy Oommen John
Christian Medical College and Hospital: Christian Medical College VelloreDivya Bala Thumaty
Christian Medical College and Hospital: Christian Medical College VelloreAnjana Joel
Christian Medical College and Hospital: Christian Medical College VelloreParth Sharma
Christian Medical College and Hospital: Christian Medical College VelloreAnand George Andrews
Christian Medical College and Hospital: Christian Medical College VelloreShalom Patole
Johns Hopkins University School of MedicineGrace Rebekah
Christian Medical College and Hospital: Christian Medical College VelloreElanthenral Sigamani
Christian Medical College and Hospital: Christian Medical College VelloreMarie Therese Manipadam
Christian Medical College and Hospital: Christian Medical College VelloreAnish Jacob Cherian
Christian Medical College and Hospital: Christian Medical College VelloreDeepak Thomas Abraham
Christian Medical College and Hospital: Christian Medical College VelloreMazhuvanchary Jacob Paul
Page 2/23
Christian Medical College and Hospital: Christian Medical College VelloreRajesh Balakrishnan
Christian Medical College and Hospital: Christian Medical College VellorePatricia Sebastian
Christian Medical College and Hospital: Christian Medical College VelloreSelvamani Backianathan
Christian Medical College and Hospital: Christian Medical College VelloreRaju Titus Chacko
Christian Medical College and Hospital: Christian Medical College Vellore
Research Article
Keywords: Triple-Negative Breast Cancers, Breast Cancer, cis-Platinum, cis-Diamminedichloroplatinum(II),Neoadjuvant Chemotherapy, Pathological Complete Response, ddDCEP, alternating chemotherapy
Posted Date: April 18th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1519744/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 3/23
Abstract
PurposeCarboplatin-containing treatment regimens in early TNBC have shown improved pCR(pathologicalcomplete response) and better EFS(event-free survival) but at the expense of increased toxicity, oftenleading to compromised delivery of planned treatment. We aimed to evaluate a novel alternating regimento incorporate platinum in early TNBC.
MethodsWe analyzed the data of women with early TNBC who were treated with four cycles each ofdocetaxel(D;75 mg/m2) and cyclophosphamide(C;600 mg/m2) alternating with cisplatin(P;60 mg/m2)and epirubicin(E;90 mg/m2) (ddDCEP) given every two weeks over a duration of 16 weeks. Pathologicalcomplete response was the primary endpoint assessed, along with treatment delivery, adverse events, andsurvival.
ResultsA total of 116 women with stage I-III TNBC received neoadjuvant ddDCEP. Pathological completeresponse(pCR) de�ned as no residual invasive cancer in both breast(T0/Tis) and axilla(N0), wasobserved in 55.2% of all evaluable patients. The proportion of pCR in stage I/II disease was 62.2%, andstage III was 49.5%. 37.9% of patients developed grade 3 anaemia. Grade 3/4 neutropenia occurred in16.3%, and febrile neutropenia in 4.3% of patients. 86% of patients completed all 8 cycles ofchemotherapy, and 98% at least 6 out of 8 cycles. 12% of patients required a dose reduction of taxane,13% for epirubicin, and 19% for platinum. The proportion of patients requiring dose reduction and theaverage total dose reduction was signi�cantly higher in the pCR compared to the no pCR group forcisplatin and epirubicin. At 2 years of median follow-up, the recurrence-free survival was 91.2%, andoverall survival was 97%.
ConclusionIn non-metastatic TNBC, treatment with ddDCEP as neoadjuvant therapy resulted in a high pCR(55.2%)proportion allowing good delivery of all planned therapy with manageable toxicity.
HighlightsPathological complete response(pCR) is associated with better survival in triple-negative breastcancer (TNBC)

Page 4/23
A new regimen administering four cycles each of docetaxel and cyclophosphamide alternating withcisplatin and epirubicin every two weeks over 16 weeks (ddDCEP), resulted in pCR of 55.2% in stageI-III TNBC
This regimen was well tolerated with good treatment completion rates and low incidence of grade3/4 adverse events, especially febrile neutropenia
ddDCEP could be an optimal method of platinum delivery and could serve as an effectivechemotherapy backbone for checkpoint inhibitors preoperatively to maximize pathological response
IntroductionTriple-negative breast cancer (TNBC) comprises up to 17% of all breast cancers worldwide.(1) The �ve-year net survival for breast cancer in India stands at 60%, in stark contrast to the 85–90% survivalreported in the developed world.(2–5) Although the treatment landscape of early TNBC is rapidly evolvingwith the addition of checkpoint inhibitors(6) and poly(ADP-ribose) polymerase(PARP) inhibitors(7), thesingle-agent activity of platinum salts(8) and the implication of the homologous recombination repairpathway de�ciency(HRD) in the pathogenesis of TNBC(9, 10), have led to a growing interest in evaluatingthese drugs in early-stage disease.(9)
Carboplatin has improved pCR in multiple randomised trials and EFS in two of them.(7) At the same time,it has increased toxicity, resulting in reduced delivery of all planned chemotherapy doses.(11) A recentlyupdated meta-analysis, which included 6 RCTs, has con�rmed the EFS gain from the addition of platinumfor early-stage TNBC.(12)
The pCR rates with cisplatin, when used as a single agent or in combination therapy, range from 18–62%.(13–17) However, data supporting the use of cisplatin-based combination chemotherapy, especially inpatients with locally advanced TNBC, is limited.
We chose cisplatin over carboplatin, considering the lower incidence of myelotoxicity with it, which could,in turn, maintain dose density, intensity and complete delivery of planned doses. We studied the e�cacyand safety of a novel schedule of alternating dose-dense neoadjuvant chemotherapy incorporatingcisplatin in TNBC and report our outcomes.
Materials And MethodsDesign and patient selection
This was a single-arm retrospective cohort study done at a tertiary teaching hospital in South India. FromJan 2017 to Jan 2020, 116 consecutive patients with early or locally advanced triple-negative breastcancer who had good performance status consented to receive the novel ddDCEP regimen asneoadjuvant therapy.
Page 5/23
Inclusion criteria were histologically con�rmed invasive triple-negative breast cancer(< 1% tumour cellspositive for oestrogen and progesterone receptors and Her2 neu immunohistochemistry(IHC) score of 0 or1 + or ISH(in-situ hybridisation) negative if 2+/equivocal by IHC) and performance status of ECOG 0–2.
All data for the retrospective analysis were collected from the hospital’s electronic medical recordssystem and paper records. Patients were staged according to the 7th edition of the AJCC/UICC stagingmanuals. Patients were prospectively followed up to assess relapse and survival events. The study wasapproved by the ethics committee(Institutional Review Board) of the Christian Medical College, Vellore(CMC IRB Min. No. 13960 [Retro]). All participants in this study had given written informed consent toundergo treatment with the ddDCEP regimen. As this was a retrospective analysis, consent for publicationwas waived by the institutional review board.
Treatment
Patients received docetaxel(D;75 mg/m2) and cyclophosphamide(C;600 mg/m2) given in cycles 1, 3, 5and 7 alternating with cisplatin(P;60 mg/m2) and epirubicin(E;90 mg/m2) given in cycles 2, 4, 6 and 8.The cycles were administered every two weeks with peg�lgrasitim support over a total duration of 16weeks. Patients underwent mastectomy or breast conservation surgery depending on patient preferenceand feasibility as assessed by the surgeon. Following surgery, patients received adjuvant radiationtherapy, if indicated. Patients with residual disease in the resection specimen were offered adjuvantcapecitabine for 6–8 cycles.
Outcomes and follow-up
The primary outcome of interest was the proportion of patients who had pathological complete responsefollowing neoadjuvant chemotherapy with the ddDCEP regimen. Secondary outcomes assessed includedadherence to planned chemotherapy cycles, dose reduction, dose omissions, disease-free survival (DFS),and overall survival (OS). Adverse events were graded in accordance with the Common TerminologyCriteria for Adverse Events (CTCAE) v4.0.
Response to chemotherapy, as seen in the surgical specimen, was graded by the pathologist based on theMiller-Payne and TNM systems. Pathological complete response was de�ned as no residual invasivecancer in the breast or axilla(ypT0/Tis, N0).(18) Miller Payne response grades of 3 and 4 were classi�edas “good pathological response” to therapy. The pCR in breast alone and axilla alone were analysedseparately.
Patients were followed up for DFS and OS events by a telephonic interview. In those who could not becontacted over the telephone, the most recent out-patient visit was taken as the last point of follow-up.The data cut-off was in November 2021.
Statistical analysis
Page 6/23
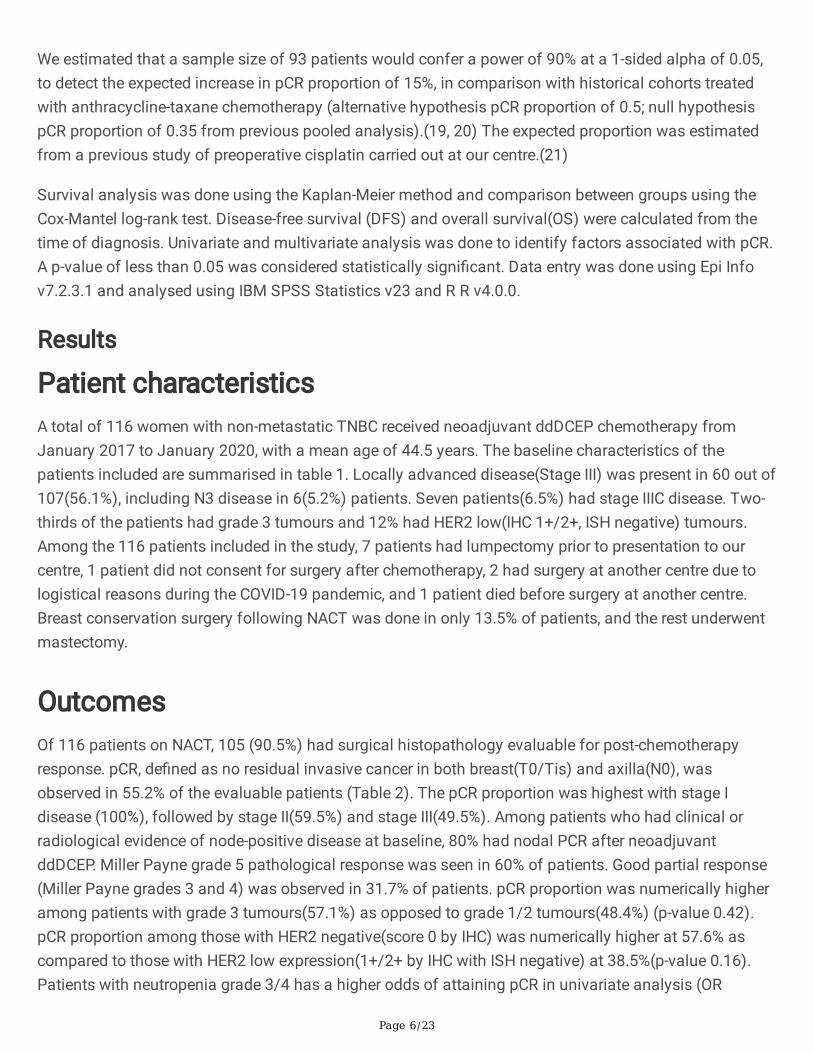
We estimated that a sample size of 93 patients would confer a power of 90% at a 1-sided alpha of 0.05,to detect the expected increase in pCR proportion of 15%, in comparison with historical cohorts treatedwith anthracycline-taxane chemotherapy (alternative hypothesis pCR proportion of 0.5; null hypothesispCR proportion of 0.35 from previous pooled analysis).(19, 20) The expected proportion was estimatedfrom a previous study of preoperative cisplatin carried out at our centre.(21)
Survival analysis was done using the Kaplan-Meier method and comparison between groups using theCox-Mantel log-rank test. Disease-free survival (DFS) and overall survival(OS) were calculated from thetime of diagnosis. Univariate and multivariate analysis was done to identify factors associated with pCR.A p-value of less than 0.05 was considered statistically signi�cant. Data entry was done using Epi Infov7.2.3.1 and analysed using IBM SPSS Statistics v23 and R R v4.0.0.
Results
Patient characteristicsA total of 116 women with non-metastatic TNBC received neoadjuvant ddDCEP chemotherapy fromJanuary 2017 to January 2020, with a mean age of 44.5 years. The baseline characteristics of thepatients included are summarised in table 1. Locally advanced disease(Stage III) was present in 60 out of107(56.1%), including N3 disease in 6(5.2%) patients. Seven patients(6.5%) had stage IIIC disease. Two-thirds of the patients had grade 3 tumours and 12% had HER2 low(IHC 1+/2+, ISH negative) tumours.Among the 116 patients included in the study, 7 patients had lumpectomy prior to presentation to ourcentre, 1 patient did not consent for surgery after chemotherapy, 2 had surgery at another centre due tologistical reasons during the COVID-19 pandemic, and 1 patient died before surgery at another centre.Breast conservation surgery following NACT was done in only 13.5% of patients, and the rest underwentmastectomy.
OutcomesOf 116 patients on NACT, 105 (90.5%) had surgical histopathology evaluable for post-chemotherapyresponse. pCR, de�ned as no residual invasive cancer in both breast(T0/Tis) and axilla(N0), wasobserved in 55.2% of the evaluable patients (Table 2). The pCR proportion was highest with stage Idisease (100%), followed by stage II(59.5%) and stage III(49.5%). Among patients who had clinical orradiological evidence of node-positive disease at baseline, 80% had nodal PCR after neoadjuvantddDCEP. Miller Payne grade 5 pathological response was seen in 60% of patients. Good partial response(Miller Payne grades 3 and 4) was observed in 31.7% of patients. pCR proportion was numerically higheramong patients with grade 3 tumours(57.1%) as opposed to grade 1/2 tumours(48.4%) (p-value 0.42).pCR proportion among those with HER2 negative(score 0 by IHC) was numerically higher at 57.6% ascompared to those with HER2 low expression(1+/2+ by IHC with ISH negative) at 38.5%(p-value 0.16).Patients with neutropenia grade 3/4 has a higher odds of attaining pCR in univariate analysis (OR

Page 7/23
2.93[0.98-8.78], p-value 0.04). In a multivariate logistic regression model incorporating 5 independentvariables, higher grade of neutropenia remained signi�cantly associated with a higher chance of pCR inthis cohort(p-value 0.047)(Table 3).
The median duration of follow-up was 24.03 months(IQR 14.25- 29.46). At 24 months of follow-up, thedisease-free survival was 91.2%(95% C.I 0.86-0.97), and overall survival was 97% (95% C.I 0.93-1.00). Thedisease-free survival for those with and without pCR was 90.5%(95% C.I 0.82- 0.99) and 84.2%(95% C.I0.72-0.98) respectively, at 36 months(log-rank p-value 0.665).(Figure 1A) The At data cutoff, amongpatients evaluable for pCR, with a total of 9 RFS events(4 in the PCR group and 5 in the no PCR), thisdifference did not reach statistical signi�cance. Median survival has not been reached for either group.
Adverse events Anaemia was the predominant haematological toxicity.(Table 4) At baseline, 47.4% had anaemia (WHOde�nition)(22), highlighting the high prevalence of anaemia in this population of Indian breast cancerpatients. During chemotherapy, 37.9% of patients developed CTCAE v4.0 grade 3 anaemia.
The median baseline hemoglobin was 12.1 g/dL(IQR 10.9-12.7 g/dL), median lowest hemoglobin was 8.3g/dL(IQR 7.6-9.3 g/dL) and median post-chemotherapy hemoglobin was 9.3 g/dL(IQR 8.5-10.1 g/dL).(Figure 2A) 37.9% of patients required transfusion of at least one unit of packed red cells(indicationswere Hb<8g/dL or anemia in heart failure). The incidence of thrombocytopenia was 63% overall, withgrade 3/4 being 8.6%. Grade 3/4 neutropenia was seen in 16.3% of patients, with febrile neutropeniaoccurring in 4.3%. Nine patients developed grade 1/2 acute kidney injury (AKI) attributable to cisplatinadministration which resolved with hydration, and none required dose omissions of cisplatin or delay inchemotherapy. There were no patients with grade 3/4 renal toxicity, hearing loss or tinnitus.
Nausea and vomiting were documented in 25.9% of patients, and clinically signi�cant peripheralneuropathy was reported in 7 patients (all grade 1/2). The neuropathy did not warrant dose omission.
Treatment delivery
Delivery of 6 out of 8 planned cycles (75% of all agents) was achieved in 98% of patients, and all 8 cyclesin 85%. (Figure 2B) This translates to 91% dose completion for DC(docetaxel- cyclophosphamide) and86% dose completion for EP(epirubicin- cisplatin). Twelve per cent of patients required a dose reductionin docetaxel, 13% required dose reductions in cyclophosphamide and epirubicin and 19% required dosereductions in cisplatin. Among the patients who required a dose reduction, the median dose reductionwas 25%(IQR 6-25) for docetaxel, 12.5%(IQR 1-25) for cyclophosphamide, 25%(IQR 6-28) for epirubicinand 20%(IQR 6-25) for cisplatin. The average total dose reduction was signi�cantly higher in the pCR vs.no pCR group for cisplatin(5.2% vs. 1.4%; p-value 0.01) and epirubicin(3.7% vs. 1.2%; p-value 0.03)(Figure3A). The difference in the proportion of patients who had dose reduction in epirubicin and cisplatinbetween the pCR and no pCR groups was also statistically signi�cant (Figure 3B).

Page 8/23
DiscussionPathological complete response(pCR) following neoadjuvant chemotherapy is a strong surrogate end-point, predicting better survival outcomes in TNBC.(23) The CTNeoBC pooled analysis, as well as anothermeta-analysis of 27,895 patients both, found a strong association between pCR and OS.(24, 25) A morerecent meta-analysis, however, which took into account 54 randomised trials comprising data of 32,611patients has cast doubt on the surrogacy of pCR at the trial level for disease-free survival and overallsurvival, even in the TNBC subgroup.(26) Notwithstanding the controversy, with the current standard ofcare of dose-dense anthracycline and taxane-based NACT in most centres worldwide, the expected pCRranges from 31 to 33.6%, as reported in pooled analysis.(23) This low pCR proportion is probably due to alarge proportion of patients presenting with node-positive or locally advanced disease in regions lackingscreening and early detection facilities.(2, 27, 28)
The necessity for higher pathological response rates and better survival outcomes in these patients led tothe current study evaluating the e�cacy and safety of the neoadjuvant ddDCEP chemotherapy regimendesigned to enable safe, dose-dense delivery of a platinum salt along with the other active agents in earlyTNBC.
The addition of neoadjuvant carboplatin to anthracycline, taxane and cyclophosphamide has improvedpCR rates to 46–59% in the GeparSixto, CALGB 40603, ADAPT-TN, GeparOcto and BrighTNess trials.(7,11, 29–31) However, improvements in event-free survival have been inconsistent, seen only with theGeparSixto and BrighTNess trials. No trial has demonstrated an overall survival bene�t thus far, probablydue to inadequate sample size to detect an effect. Hence, the debate on the use of carboplatinpreoperatively in early TNBC continues and is optional across guidelines proposed by variousprofessional societies.(32, 33) This apparent lack of survival bene�t in the carboplatin trials could beattributed to the signi�cantly higher grade 3/4 haematological toxicity leading to dose omissions,especially of the other drugs in the regimen.(7) Thus, the bene�t of increased pCR might be offset by theinability to deliver all the planned doses of active agents.
Cisplatin being less myelotoxic than carboplatin could mitigate the hematologic toxicity attributable tothe addition of carboplatin to weekly paclitaxel, thus increasing treatment compliance and maintainingdose-density.(34) There are no randomised trials comparing carboplatin with cisplatin in early breastcancer. However, a retrospective study of 144 patients by Hurley et al. comparing carboplatin andcisplatin in locally advanced TNBC showed a possible survival advantage with the use of the latter.(15)The safety of cisplatin in early TNBC has been explored previously. The INFORM phase II randomisedtrial(TBCRC 031) compared cisplatin with doxorubicin-cyclophosphamide(AC) NACT in HER2 negativebreast cancer patients. Cisplatin given at 75mg/m2(3 weekly) was well-tolerated with a good safetypro�le. In the ddDCEP regimen, we used cisplatin 60mg/m2 of at an interval of 4 weeks. The TBCRC 030phase II randomised trial compared preoperative cisplatin vs paclitaxel monotherapy in 139 TNBCpatients with HRD and found similar PCR rates(26.4% and 22.3%, respectively) with an acceptable safetypro�le.
Page 9/23
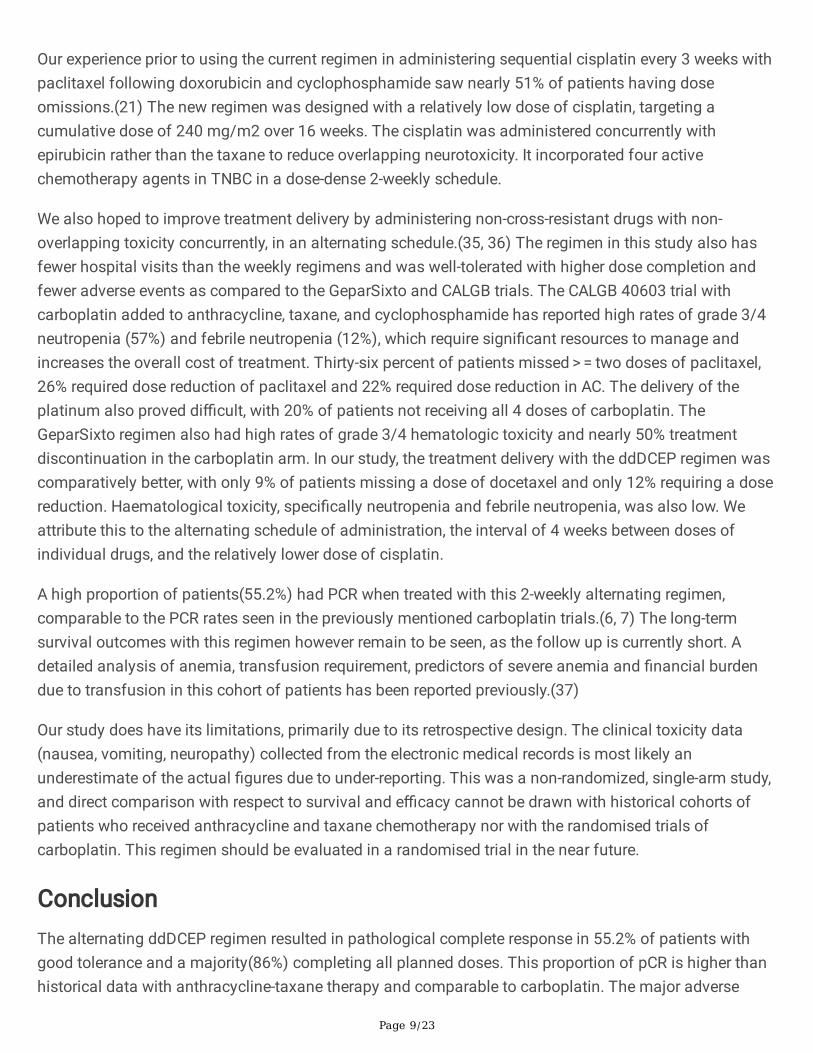
Our experience prior to using the current regimen in administering sequential cisplatin every 3 weeks withpaclitaxel following doxorubicin and cyclophosphamide saw nearly 51% of patients having doseomissions.(21) The new regimen was designed with a relatively low dose of cisplatin, targeting acumulative dose of 240 mg/m2 over 16 weeks. The cisplatin was administered concurrently withepirubicin rather than the taxane to reduce overlapping neurotoxicity. It incorporated four activechemotherapy agents in TNBC in a dose-dense 2-weekly schedule.
We also hoped to improve treatment delivery by administering non-cross-resistant drugs with non-overlapping toxicity concurrently, in an alternating schedule.(35, 36) The regimen in this study also hasfewer hospital visits than the weekly regimens and was well-tolerated with higher dose completion andfewer adverse events as compared to the GeparSixto and CALGB trials. The CALGB 40603 trial withcarboplatin added to anthracycline, taxane, and cyclophosphamide has reported high rates of grade 3/4neutropenia (57%) and febrile neutropenia (12%), which require signi�cant resources to manage andincreases the overall cost of treatment. Thirty-six percent of patients missed > = two doses of paclitaxel,26% required dose reduction of paclitaxel and 22% required dose reduction in AC. The delivery of theplatinum also proved di�cult, with 20% of patients not receiving all 4 doses of carboplatin. TheGeparSixto regimen also had high rates of grade 3/4 hematologic toxicity and nearly 50% treatmentdiscontinuation in the carboplatin arm. In our study, the treatment delivery with the ddDCEP regimen wascomparatively better, with only 9% of patients missing a dose of docetaxel and only 12% requiring a dosereduction. Haematological toxicity, speci�cally neutropenia and febrile neutropenia, was also low. Weattribute this to the alternating schedule of administration, the interval of 4 weeks between doses ofindividual drugs, and the relatively lower dose of cisplatin.
A high proportion of patients(55.2%) had PCR when treated with this 2-weekly alternating regimen,comparable to the PCR rates seen in the previously mentioned carboplatin trials.(6, 7) The long-termsurvival outcomes with this regimen however remain to be seen, as the follow up is currently short. Adetailed analysis of anemia, transfusion requirement, predictors of severe anemia and �nancial burdendue to transfusion in this cohort of patients has been reported previously.(37)
Our study does have its limitations, primarily due to its retrospective design. The clinical toxicity data(nausea, vomiting, neuropathy) collected from the electronic medical records is most likely anunderestimate of the actual �gures due to under-reporting. This was a non-randomized, single-arm study,and direct comparison with respect to survival and e�cacy cannot be drawn with historical cohorts ofpatients who received anthracycline and taxane chemotherapy nor with the randomised trials ofcarboplatin. This regimen should be evaluated in a randomised trial in the near future.
ConclusionThe alternating ddDCEP regimen resulted in pathological complete response in 55.2% of patients withgood tolerance and a majority(86%) completing all planned doses. This proportion of pCR is higher thanhistorical data with anthracycline-taxane therapy and comparable to carboplatin. The major adverse

Page 10/23
effects were haematological, predominantly anemia, with febrile neutropenia occurring in 4% of patients.Further follow-up is required to determine the long-term survival of these patients, especially those withresidual disease. The e�cacy results of this study are reassuring and merit further evaluation of thischemotherapy backbone alone or in combination with checkpoint inhibitors in future randomised trials.
Declarations
Competing Interests
The authors have no relevant �nancial or non-�nancialinterests to disclose.
Data AvailabilityThe datasets generated during and/or analysed during the current study are not publicly available due toinstitutional policy, but are available from the corresponding author on reasonable request
FundingThe authors declare that no funds, grants, or other support were received during the preparation of thismanuscript.
Ethics approvalThe study was approved by the ethics committee (Institutional Review Board) of the Christian MedicalCollege, Vellore (CMC IRB Min. No. 13960 [Retro]).
Consent to participateInformed consent was obtained from all individual participants included in the study to receive theddDCEP chemotherapy regimen.
Consent to publishAs this was a retrospective analysis, consent for publication was waived by the institutional ethicscommittee/review board.
Page 11/23
Author ContributionsCRediT author statement
Ashish Singh: Conceptualization, Methodology, Formal analysis, Investigation, Writing - Review & Editing,Visualization, Supervision, Project administration, Funding acquisition
Josh Thomas Georgy: Conceptualization, Methodology, Formal analysis, Investigation, Writing -
Original Draft, Visualization
Ajoy Oommen John: Conceptualization, Methodology, Formal analysis, Writing - Review & Editing,Visualization
Divya Bala Thumaty: Conceptualization, Methodology, Formal analysis, Investigation, Writing -
Review & Editing, Visualization
Anjana Joel: Conceptualization, Methodology, Formal analysis, Investigation, Writing- Review & Editing,Visualization, Supervision
Parth Sharma: Methodology, Formal analysis, Investigation, Writing – Original Draft
Anand Andrews: Methodology, Formal analysis, Investigation, Writing – Original Draft
Shalom Patole: Methodology, Formal analysis, Investigation, Writing - Review & Editing, Visualization
Grace Rebekah: Formal analysis, Software
Elanthenral Sigamani: Methodology, Formal analysis, Investigation, Writing - Review & Editing,Visualization
Marie Therese Manipadam: Methodology, Formal analysis, Investigation, Writing - Review & Editing
Anish Jacob Cherian: Methodology, Formal analysis, Investigation, Writing - Review & Editing,Visualization
Deepak Thomas Abraham: Methodology, Formal analysis, Investigation, Writing - Review & Editing,Visualization
Paul M J: Methodology, Formal analysis, Investigation, Writing - Review & Editing, Visualization
Rajesh Balakrishnan: Methodology, Formal analysis, Investigation, Writing - Review & Editing,Visualization
Patricia Sebastian: Methodology, Formal analysis, Investigation, Writing - Review & Editing, Visualization

Page 12/23
Selvamani Backianathan: Methodology, Formal analysis, Investigation, Writing - Review & Editing,Visualization
Raju Titus Chacko: Writing - Review & Editing, Supervision, Project administration, Funding
acquisition, Resources
References1. Reis-Filho JS, Tutt ANJ (2008) Triple negative tumours: A critical review. Histopathology 52(1):108–
118
2. Suhani S, Kazi M, Parshad R, Seenu V, Verma E, Mathur S et al (2020) An audit of over 1000 breastcancer patients from a tertiary care center of Northern India. Breast Dis. Jan 1;39(2):91–9
3. Cancer of the Breast (Female) - Cancer Stat Facts [Internet]. SEER. [cited 2021 Aug 29]. Availablefrom: https://seer.cancer.gov/statfacts/html/breast.html
4. Breast cancer survival statistics [Internet], Cancer Research UK (2015) [cited 2021 Aug 29]. Availablefrom: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/survival
5. Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang X-S et al (2015 Mar) Global surveillanceof cancer survival 1995–2009: analysis of individual data for 25 676 887 patients from 279population-based registries in 67 countries (CONCORD-2). The Lancet 385(9972):977–1010
�. Schmid P, Cortes J, Pusztai L, McArthur H, Kümmel S, Bergh J et al Pembrolizumab for Early Triple-Negative Breast Cancer.New England Journal of Medicine. 2020 Feb27;382(9):810–21
7. Loibl S, O’Shaughnessy J, Untch M, Sikov WM, Rugo HS, McKee MD et al (2018 Apr) Addition of thePARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapyin triple-negative breast cancer (BrighTNess): a randomised, phase 3 trial. Lancet Oncol 19(4):497–509
�. Tutt A, Tovey H, Cheang MCU, Kernaghan S, Kilburn L, Gazinska P et al (2018 May) A randomisedphase III trial of carboplatin compared with docetaxel in BRCA1/2 mutated and pre-speci�ed triplenegative breast cancer “BRCAness” subgroups: the TNT Trial. Nat Med 24(5):628–637
9. Telli ML, Timms KM, Reid J, Hennessy B, Mills GB, Jensen KC et al Homologous RecombinationDe�ciency (HRD) Score Predicts Response to Platinum-Containing Neoadjuvant Chemotherapy inPatients with Triple-Negative Breast Cancer. Clin Cancer Res. 2016 Aug 1;22(15):3764–73
10. Belli C, Duso BA, Ferraro E, Curigliano G (2019 Jun) Homologous recombination de�ciency in triplenegative breast cancer. Breast 45:15–21
11. Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM et al (2015) Impact of theAddition of Carboplatin and/or Bevacizumab to Neoadjuvant Once-per-Week Paclitaxel Followed byDose-Dense Doxorubicin and Cyclophosphamide on Pathologic Complete Response Rates in Stage IIto III Triple-Negative Breast Cancer: CALGB 40603 (Alliance). JCO. Jan 1;33(1):13–21
Page 13/23
12. Poggio F, Tagliamento M, Ceppi M, Bruzzone M, Conte B, Fregatti P et al (2021) Adding a platinumagent to neoadjuvant chemotherapy for triple negative breast cancer: the end of the debate.Annals ofOncology. Nov;S0923753421048316.
13. Tung N, Arun B, Hacker MR, Hofstatter E, Toppmeyer DL, Isakoff SJ et al (2020 May) TBCRC 031:Randomized Phase II Study of Neoadjuvant Cisplatin Versus Doxorubicin-Cyclophosphamide inGermline BRCA Carriers With HER2-Negative Breast Cancer (the INFORM trial). J Clin Oncol10(14):1539–1548
14. Mayer EL, Abramson V, Jankowitz R, Falkson C, Marcom PK, Traina T et al (2020) TBCRC 030: aphase II study of preoperative cisplatin versus paclitaxel in triple-negative breast cancer: evaluatingthe homologous recombination de�ciency (HRD) biomarker. Annals of Oncology. 31:1518–15251
15. Hurley J, Reis IM, Rodgers SE, Gomez-Fernandez C, Wright J, Leone JP et al (2013) The use ofneoadjuvant platinum-based chemotherapy in locally advanced breast cancer that is triple negative:retrospective analysis of 144 patients. Breast Cancer Res Treat. Apr 1;138(3):783–94
1�. Jovanović B, Mayer IA, Mayer EL, Abramson VG, Bardia A, Sanders ME et al A Randomized Phase IINeoadjuvant Study of Cisplatin, Paclitaxel With or Without Everolimus in Patients with Stage II/IIITriple-Negative Breast Cancer (TNBC): Responses and Long-term Outcome Correlated with IncreasedFrequency of DNA Damage Response Gene Mutations, TNBC Subtype, AR Status, and Ki67. ClinCancer Res. 2017 Aug 1;23(15):4035–45
17. Frasci G, Comella P, Rinaldo M, Iodice G, Di Bonito M, D’Aiuto M et al (2009) Preoperative weeklycisplatin–epirubicin–paclitaxel with G-CSF support in triple-negative large operable breast cancer.Ann Oncol. Jul 1;20(7):1185–92
1�. Kuroi K, Toi M, Ohno S, Nakamura S, Iwata H, Masuda N et al (2015) Comparison of differentde�nitions of pathologic complete response in operable breast cancer: a pooled analysis of threeprospective neoadjuvant studies of JBCRG. Breast Cancer 22(6):586–595
19. CRAB SWOG Statistical Tools Calculators (https://stattools.crab.org)
20. Fleiss JL (2003) An Introduction to Applied Probability. In: Statistical Methods for Rates andProportions [Internet]. John Wiley & Sons, Ltd; [cited 2022 Mar 1]. p. 1–16. Available from:https://onlinelibrary.wiley.com/doi/abs/10.1002/0471445428.ch1
21. Georgy JT, Singh A, John AO, Joel A, Andrews AG, Thumaty DB et al (2021) Pathological responseand clinical outcomes in operable triple-negative breast cancer with cisplatin added to standardneoadjuvant chemotherapy. Klinicka onkologie: casopis Ceske a Slovenske onkologicke spolecnosti.34:49–551
22. WHO Scienti�c Group on Nutritional Anaemias. Nutritional anaemias: report of a WHO scienti�cgroup [meeting held in Geneva from 13 to 17 March 1967]. World Health Organization (1968) ; p.Russian version of nos. 404–438 bound together (barcode no. 00073779). (World HealthOrganization technical report series ; no. 405)
23. von Minckwitz G, Untch M, Blohmer J-U, Costa SD, Eidtmann H, Fasching PA et al (2012 May)De�nition and impact of pathologic complete response on prognosis after neoadjuvant
Page 14/23
chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 20(15):1796–1804
24. Spring LM, Fell G, Arfe A, Sharma C, Greenup R, Reynolds KL et al Pathological complete responseafter neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: acomprehensive meta-analysis.Clin Cancer Res. 2020 Jun15;26(12):2838–48
25. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N et al (2014 Jul) Pathologicalcomplete response and long-term clinical bene�t in breast cancer: the CTNeoBC pooled analysis. TheLancet 384(9938):164–172
2�. Conforti F, Pala L, Sala I, Oriecuia C, Pas TD, Specchia C et al (2021) Evaluation of pathologicalcomplete response as surrogate endpoint in neoadjuvant randomised clinical trials of early stagebreast cancer: systematic review and meta-analysis. BMJ. Dec 21;375:e066381
27. Sharma M, Sharma JD, Sarma A, Ahmed S, Kataki AC, Saxena R et al (2014) Triple negative breastcancer in people of North East India: critical insights gained at a regional cancer centre. Asian Pac JCancer Prev 15(11):4507–4511
2�. Li C-Y, Zhang S, Zhang X-B, Wang P, Hou G-F, Zhang J (2013) Clinicopathological and prognosticcharacteristics of triple- negative breast cancer (TNBC) in chinese patients: A retrospective study.Asian Pac J Cancer Prev 14(6):3779–3784
29. von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M et al (2014 Jun) Neoadjuvantcarboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG66): a randomised phase 2 trial. Lancet Oncol 15(7):747–756
30. Gluz O, Nitz U, Liedtke C, Christgen M, Grischke E-M, Forstbauer H et al (2017) Comparison ofNeoadjuvant Nab-Paclitaxel1Carboplatin vs Nab-Paclitaxel1Gemcitabine in Triple-Negative BreastCancer: Randomized WSG-ADAPT-TN Trial Results. ; Available from:https://academic.oup.com/jnci/article/110/6/628/4698155
31. Schneeweiss A, Moebus V, Tesch H, Hanusch C, Denkert C, Luebbe K et al (2017 May) A randomisedphase III trial comparing two dose-dense, dose-intensi�ed approaches (EPC and PM(Cb)) forneoadjuvant treatment of patients with high-risk early breast cancer (GeparOcto). J Clin Oncol35(15suppl):518
32. NCCN. Breast Cancer v7.2021- August 23 2021 [Internet]. NCCN.org. [cited 2021 Aug 29]. Availablefrom: https://www.nccn.org/guidelines/guidelines-detail
33. Cardoso F, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rubio IT et al (2019) Early breastcancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals ofOncology. Oct 1;30(10):1674
34. Lück H-J, Roché H Weekly paclitaxel: an effective and well-tolerated treatment in patients withadvanced breast cancer.Critical Reviews in Oncology/Hematology. 2002 Dec27;44:15–30
35. Pritchard JR, Lauffenburger DA, Hemann MT (2012 Oct) Understanding Resistance to CombinationChemotherapy. Drug Resist Updat 15(0):249–257
3�. Evans WK, Feld R, Murray N, Willan A, Coy P, Osoba D et al (1987 Oct) Superiority of alternating non-cross-resistant chemotherapy in extensive small cell lung cancer. A multicenter, randomized clinical

Page 15/23
trial by the National Cancer Institute of Canada. Ann Intern Med 107(4):451–458
37. Sharma P, Georgy JT, Andrews AG, John AO, Joel A, Chacko RT et al (2022) Anemia requiringtransfusion in breast cancer patients on dose-dense chemotherapy: Prevalence, risk factors, cost andeffect on disease outcome. Support Care Cancer. Mar 21
TablesTable 1 Baseline characteristics

Page 16/23
Characteristic Number %
Female 116 100
Age in years (Median, range) 44.5, 22-67 -
Menopausal status
Premenopausal 76 66.4
Postmenopausal 40 33.6
Performance status*
ECOG 0 82 70.7
ECOG 1 33 28.4
ECOG 2 1 0.9
T stage(clinical) *
Tx 9 7.8
T0 1 0.9
T1 4 3.4
T2 44 37.9
T3 27 23.3
T4a 1 0.9
T4b 28 24.1
T4c 1 0.9
T4d 1 0.9
N stage(clinical) *
N0 27 23.3
N1 65 56.0
N2a 18 15.5
N3a 2 1.7
N3b 1 0.9
N3c 3 2.6
AJCC stage*
IA 3 2.8

Page 17/23
IIA 13 12.1
IIB 31 29.0
IIIA 24 22.4
IIIB 29 27.1
IIIC 7 6.5
Grade of tumour
Grade 1 1 0.9
Grade 2 34 29.3
Grade 3 77 66.4
Unclear/unknown 4 3.4
HER2 expression*
HER2 negative(IHC score 0) 92 87.6
HER2 low(IHC score 1/2, ISH neg) 13 12.4
Histopathology of tumour
Ductal carcinoma 108 93.1
Metaplastic carcinoma 2 1.7
Apocrine carcinoma 1 0.9
Papillary carcinoma 1 0.9
Unclear/unknown 4 3.4
Type of surgery*
Breast conservation 15 13.4
Mastectomy 97 86.6
Received adjuvant RT 105 90.5
Received adjuvant capecitabine*
Overall(N=116) 40 34.5
Without pCR(N=47) 34 72.3
*N varies with missing data for each characteristic

Page 18/23
Table 2 Pathological response
Patient subroup N %
pCR(ypT0/is N0) overall(N=105) 58 55.2
pCR(ypT0/is, N0) by clinical stage
Stage I/II(N=45) 28 62.2
Stage III (N=57) 27 47.4
Breast pCR(ypT0/is N0/+) (N=104) 63 60.5
Nodal pCR(ypN0) (N=81) 65 80.2
Miller Payne response(N=104)
Miller Payne grade 1 2 1.9
Miller Payne grade 2 6 5.8
Miller Payne grade 3 17 16.3
Miller Payne grade 4 16 15.4
Miller Payne grade 5 63 60.6
Pathological response by grade(N=101)
Grade 1/2(N=31) 15 48.4
Grade 3(N=70) 40 57.1
Pathological response by HER2 expression(N=105)
HER2 negative(IHC score 0) (N=92) 53 57.6
HER2 low(IHC score 1/2, ISH neg) (N=13) 5 38.5
Table 3 Factors associated with pCR (univariate and multivariate)

Page 19/23
Characteristic pCR No pCR OR (95% C.I) P-value
Multivariate p-value*
Age
48 or less
49 or more
40(53.3%)
18(60%)
35(46.7%)
12(40%)
1.31(0.56-3.10)
0.535 -
Menopause
Pre
Post
36(52.9%)
22(59.5%)
32(47.1%)
15(40.5%)
1.30(.58-2.93)
0.521
-
Histology
Others
Ductal carcinoma
4(66.7%)
53(54.6%)
2(33.3%)
44(45.4%)
1.66(0.29-9.49)
0.689
-
Grade of tumor
Grade 3
Grade 1/2
40(57.1%)
15(48.4%)
30(42.9%)
16(51.6%)
1.42(0.61-3.32)
0.415
-
HER2 expression
Negative
Low (1+/2+ ISH neg)
53(57.6%)
5(38.5%)
39(42.4%)
8(61.5%)
0.46(0.14-1.51)
0.158 0.203
T clinical
T3/T4
T2 and below
26(48.1%)
29(60.4%)
28(51.9%)
19(39.6%)
0.61(0.28-0.34)
0.215
-
N stage clinical
N2/3
N0/1
9(42.9%)
49(58.3%)
12(57.1%)
35(41.7%)
0.54(0.20-1.41)
0.202 -
AJCC Stage
Locally advanced (III)
Early(I/II)
27(47.4%)
28(62.2%)
30(52.6%)
17(37.8%)
0.55(0.25-1.21)
0.135 0.144
Neutropenia grade 3/4
Yes
No
15(75%)
43(50.6%)
5(25%)
42(49.4%)
2.93(0.98-8.78)
0.040 0.047

Page 20/23
Thrombocytopenia grade3/4
Yes
No
7(70%)
50(52.6%)
3(30%)
45(47.4%)
2.01(0.49-8.26)
0.260 0.514
Anemia grade 3/4
Yes
No
23(54.8%)
35(55.6%)
19(45.2%)
28(44.4%)
0.97(0.44-2.12)
0.936 0.617
Blood transfusion
Yes
No
25(59.5%)
33(52.4%)
17(40.5%)
30(47.6%)
1.34(0.61-2.95)
0.471 -
*Multivariate binary logistic regression model
Table 4. Adverse events
Adverse event Grade 1/2
N(%)
Grade 3
N(%)
Grade 4
N(%)
Anemia 72(62.1%) 44(37.9%) -
Thrombocytopenia 64(55.2%) 8(6.9%) 2(1.7%)
Neutropenia 22(18.9%) 7(6%) 12(10.3%)
Febrile neutropenia - 4(3.4%) 1(0.9%)
Acute kidney injury 9(7.8%) - -
Nausea and vomiting 27(23.3%) 3(2.6%) -
Myalgia 9(7.7%) 1(0.9%) -
Peripheral neuropathy 7(6%) 1(0.9%) -
Figures

Page 21/23
Figure 1
Disease-free survival A. Strati�ed by pathological response (pCR vs. no pCR) B. Strati�ed by stage (I/II vs.III)

Page 22/23
Figure 2
A. Trend in Hemoglobin during treatment B. Number of doses completed out of eight planned forindividual patient

Page 23/23
Figure 3
A. Proportion of total dose reduced for each drug strati�ed by pCR(red dots show average dose reductionin *pCR vs. ~no pCR group) B. Proportion of patients requiring dose reduction for each drug strati�ed bypCR
Related Documents