Archives of the Balkan Medical Union Copyright © 2017 Balkan Medical Union vol. 52, no. 1, pp. 117-121 March 2017 RÉSUMÉ Difficultés diagnostiques préopératives de l’adenocar- cinome de la valvule ileo-caecale – rapport de cas Introduction. L’adénocarcinome valvulaire iléo-cae- cale est une cause rare d’obstruction intestinale et peut être très difficile à diagnostiquer avant l’intervention chirurgicale en cas d’indication d’urgence. La plupart des patients deviennent symptomatiques seulement lorsque des complications et la croissance tumorale se produisent, donc un bon diagnostic avant l’inter- vention chirurgicale en cas d’indication d’urgence est échappé. Rapport de cas. Dans cet article, nous présentons un cas exceptionnellement rare d’adénocarcinome impliquant seulement la valvule iléo-cæcale, qui a été diagnostiqué en intra-opératoire lors d’une inter- vention chirurgicale d’urgence pour une obstruction intestinale aiguë. La présentation clinique consistait en symptômes d’occlusion intestinale aiguë. La radiog- raphie abdominale simple a révélé de multiples images hydroaériques suggestives pour l’obstruction de l’intes- tin grêle. L’aggravation des symptômes a déterminé la décision d’effectuer une chirurgie d’urgence pour une obstruction intestinale aiguë. La palpation du caecum ABSTRACT Introduction. Ileocecal valve adenocarcinoma is a very rare cause of bowel obstruction, very difficult to diagnose prior to surgical intervention for emergency indication. Most of the patients are symptomatic only when complications occur. Case report . We present an exceptionally rare case of adenocarcinoma involving only the ileocecal valve, which was diagnosed intraoperatively during emergen- cy surgery for acute bowel obstruction. The patient presented with acute bowel obstruction symptoms. Plain abdominal X-ray revealed multiple hydro-ae- ric images suggestive for small bowel obstruction. Worsening of the symptoms leads to the decision to perform emergency surgery for acute bowel obstruc- tion. Intraoperative palpation of cecum revealed a small tumor of the ileocecal junction, with no expres- sion to serosa, and determining a complete stenosis at this level. Discussion. The structures of the ileocecum may be involved in many pathological processes, many of them being common in clinical practice. The disease may involve only one of the structures, several of them simultaneously or may be part of a general process. In this case, there was no expression on the serosa, no CASE REPORT PREOPERATIVE DIAGNOSTIC DIFFICULTIES OF ILEOCECAL VALVE ADENOCARCINOMA – A CASE REPORT Cristian Bălălău 1,2 , Nicolae Bacalbașa 2 , Ion Motofei 1,2 , Petrișor Banu 1,2 , Răzvan Scăunașu 2 , Ștefan Voiculescu 2 , Oana-Denisa Bălălău 1 , Vlad-Denis Constantin 1,2 1 Department of General Surgery „Sf. Pantelimon“ Clinical Hospital, Bucharest, Romania 2 University of Medicine and Pharmacy „Carol Davila“, Bucharest, Romania Corresponding author: Bălălău Cristian, MD., PhD phone (+4)0727841827 email: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Archives of the Balkan Medical UnionCopyright © 2017 Balkan Medical Union
vol. 52, no. 1, pp. 117-121March 2017
RÉSUMÉ
Difficultés diagnostiques préopératives de l’adenocar-cinome de la valvule ileo-caecale – rapport de cas
Introduction. L’adénocarcinome valvulaire iléo-cae-cale est une cause rare d’obstruction intestinale et peut être très difficile à diagnostiquer avant l’intervention chirurgicale en cas d’indication d’urgence. La plupart des patients deviennent symptomatiques seulement lorsque des complications et la croissance tumorale se produisent, donc un bon diagnostic avant l’inter-vention chirurgicale en cas d’indication d’urgence est échappé. Rapport de cas. Dans cet article, nous présentons un cas exceptionnellement rare d’adénocarcinome impliquant seulement la valvule iléo-cæcale, qui a été diagnostiqué en intra-opératoire lors d’une inter-vention chirurgicale d’urgence pour une obstruction intestinale aiguë. La présentation clinique consistait en symptômes d’occlusion intestinale aiguë. La radiog-raphie abdominale simple a révélé de multiples images hydroaériques suggestives pour l’obstruction de l’intes-tin grêle. L’aggravation des symptômes a déterminé la décision d’effectuer une chirurgie d’urgence pour une obstruction intestinale aiguë. La palpation du caecum
ABSTRACT
Introduction. Ileocecal valve adenocarcinoma is a very rare cause of bowel obstruction, very difficult to diagnose prior to surgical intervention for emergency indication. Most of the patients are symptomatic only when complications occur. Case report. We present an exceptionally rare case of adenocarcinoma involving only the ileocecal valve, which was diagnosed intraoperatively during emergen-cy surgery for acute bowel obstruction. The patient presented with acute bowel obstruction symptoms. Plain abdominal X-ray revealed multiple hydro-ae-ric images suggestive for small bowel obstruction. Worsening of the symptoms leads to the decision to perform emergency surgery for acute bowel obstruc-tion. Intraoperative palpation of cecum revealed a small tumor of the ileocecal junction, with no expres-sion to serosa, and determining a complete stenosis at this level. Discussion. The structures of the ileocecum may be involved in many pathological processes, many of them being common in clinical practice. The disease may involve only one of the structures, several of them simultaneously or may be part of a general process. In this case, there was no expression on the serosa, no
CASE REPORT
PREOPERATIVE DIAGNOSTIC DIFFICULTIES OF ILEOCECAL VALVE ADENOCARCINOMA – A CASE REPORT
Cristian Bălălău1,2, Nicolae Bacalbașa2, Ion Motofei1,2, Petrișor Banu1,2, Răzvan Scăunașu2, Ștefan Voiculescu2, Oana-Denisa Bălălău1, Vlad-Denis Constantin1,2
1 Department of General Surgery „Sf. Pantelimon“ Clinical Hospital, Bucharest, Romania 2University of Medicine and Pharmacy „Carol Davila“, Bucharest, Romania
Corresponding author: Bălălău Cristian, MD., PhD
phone (+4)0727841827
email: [email protected]

Preoperative diagnostic diffi culties of ileocecal valve adenocarcinoma… – BĂLĂLĂU et al
118 / vol. 52, no. 1
INTRODUCTION
Ileocecal valve adenocarcinoma is very rare, only few cases being reported in the literature1,5. While ad-enocarcinomas developed from the ampulla of Vater and the periampullary region are typically included in the category of small bowel adenocarcinomas, those arising from the ileocecal valve, appendix, and Meckel’s diverticulum are excluded6. An increased risk of developing small bowel adenocarcinoma has been described in patients with inflammatory bowel disease, familial adenomatous polyposis and heredi-tary nonpolyposis colorectal cancer7–9.
The clinical manifestations are non-specif-ic, varying from right lower abdominal discomfort to intestinal obstruction. Although there are some X-Ray findings suggestive of malignant tumors of the valve10, pre operative diagnosis is extremely difficult. Particularly, the infiltrative type of carcinoma of the ileocecal valve may be easily misdiagnosed by X-Ray imaging and clinical symptoms of inflammatory bow-el disease11.
Most of the patients become symptomatic only when complications and tumor growth occur,
therefore diagnosis prior to emergency surgical inter-vention is rare.
In this article, we present an exceptionally rare case of adenocarcinoma involving only the ileocecal valve, which was diagnosed intraoperatively during emergency surgery for acute bowel obstruction.
CASE PRESENTATION
We present the case of a 77 year old man, ad-mitted 10 days before for signs of acute bowel ob-struction. He was diagnosed with post-appendectomy adherent bowel obstruction, before surgery. The past medical history included signs of recurrent bowel obstruction, starting two months ago, with abdom-inal pain and intermittent abdominal distention followed by diarrhea. The patient presented with symptoms and signs of acute bowel obstruction: ab-dominal pain, lack of intestinal transit for both gases and stools, and vomiting. The physical exa mination showed abdominal distention and tenderness. Plain abdominal X-ray revealed multiple hydro-aeric images suggestive for small bowel obstruction. Because the symptoms improved and the intestinal transit re star-ted, the patient was referred for colonoscopy, which
a révélé une petite tumeur située à la jonction iléo-cae-cale, sans expression de la séreuse, et la détermination d’une sténose complète à ce niveau. Discussion. Les structures de la région iléo-caecale peuvent être affectées dans de nombreux processus pathologiques, dont beaucoup sont fréquents dans la pratique clinique et la maladie peut impliquer une seule des structures, plusieurs d’entre elles simultané-ment ou faire partie d’un processus général. Dans ce cas, il n’y avait pas d’expression sur la séreuse, pas de rétraction mésentérique ou d’adénopathie macro-scopique pour signaler l’endroit de la tumeur. Seule la transition abrupte des boucles dilatées de l’intestin grêle et du côlon droit vide, ainsi que la détection pal-pable de la tumeur ont révélé le diagnostic. Conclusion. L’évolution de la tumeur valvulaire iléo-caecale est rapide vers l’obstruction intestinale ai-guë due au petit calibre de la valve. Le diagnostic est souvent retardé en raison du manque de symptômes spécifiques et de méthodes de dépistage efficaces, et le début est souvent par complication (obstruction). La néoplasie valvulaire iléo-caecale est une localisation très rare également prouvée par la rareté de la littéra-ture des cas, et presque impossible d’être un bon diag-nostic avant la complication.
Mots-clés: valvule iléo-caecale, néoplasie colique, hémicolectomie droite.
mesenteric retraction or macroscopic adenopathy to signalize the place of the tumor. Only the abrupt tran-sition from dilated small bowel loops to empty right colon, along with palpatory detection of the tumor revealed the diagnosis. Conclusion. Ileocecal valve tumor evolution leads to acute bowel obstruction due to small caliber of the valve. Diagnosis is often delayed due to lack of spe-cific symptoms and effective screening methods, and the onset is often due to complication (obstruction). Neoplasms of ileocecal valve are very rare, in the med-ical literature being reported only a small number of cases.
Keywords: ileocecal valve, colonic neoplasia, right hemicolectomy.
Archives of the Balkan Medical Union
March 2017 / 119
was followed by barium enema due to technical diffi-culties to overpass the right angle of the colon. Both investigations did not detect any pathological chang-es. The patient refused the exploratory laparoscopy, and therefore he was discharged with diagnosis of post-appendectomy adherent syndrome.
On the current admission, laboratory tests were done, with normal results, excepting increased pro-thrombin time and INR values, due to chronic an-ticoagulant treatment for an old acute myocardial
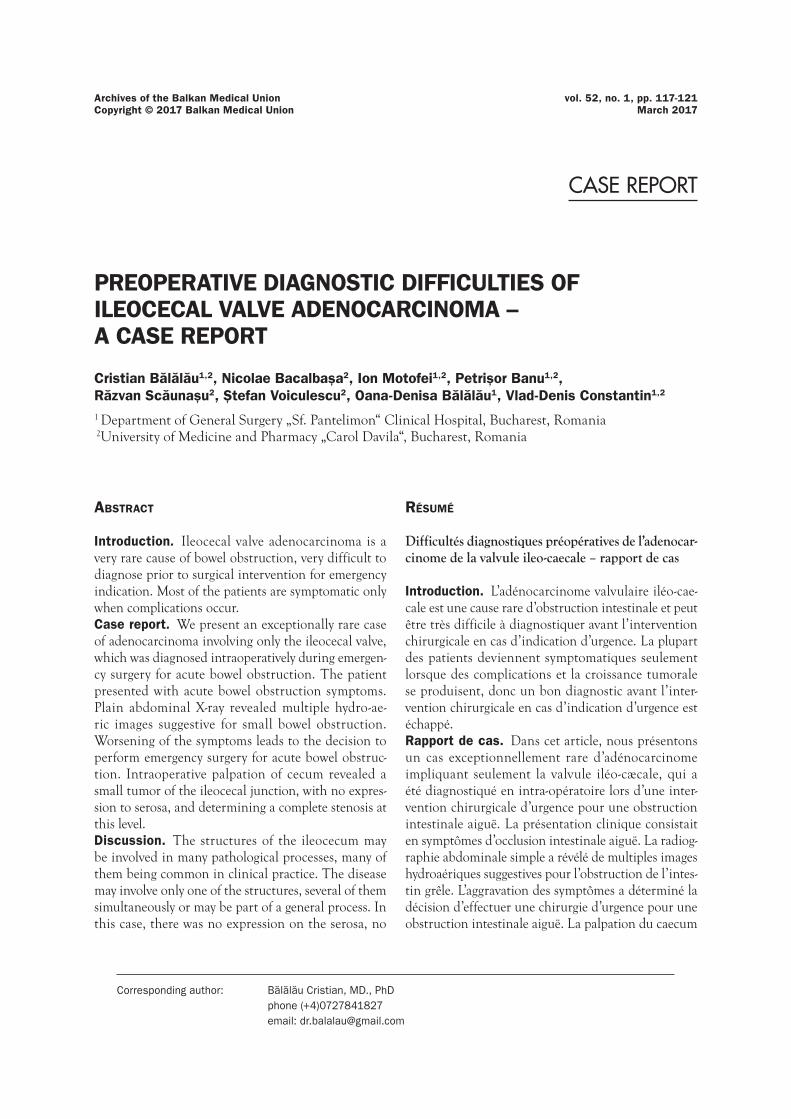
infarction. The plain abdominal X-ray revealed the same multiple hydroaeric images suggestive for small bowel obstruction as in the previous hospitalization, but worsening in dynamics (Fig. 1 and Fig. 2).
The emergency abdominal ultrasonography showed dilated small bowel segments and a mini-mal amount of free fluid in Morrison space (Fig. 3). Pulmonary X-ray result was normal.
Emergency surgery was performed, for acute bowel obstruction. The preoperative diagnosis was
Figure 1. Abdominal X-ray – hydroaeric images on admission
Figure 3. Ultrasound revealing free fluid in Morrison space
Figure 4. Macroscopic aspect of ileocecal valve neoplasia
Figure 2. Abdominal X-ray - hydroaeric images 5 hours after admission

Preoperative diagnostic diffi culties of ileocecal valve adenocarcinoma… – BĂLĂLĂU et al
120 / vol. 52, no. 1
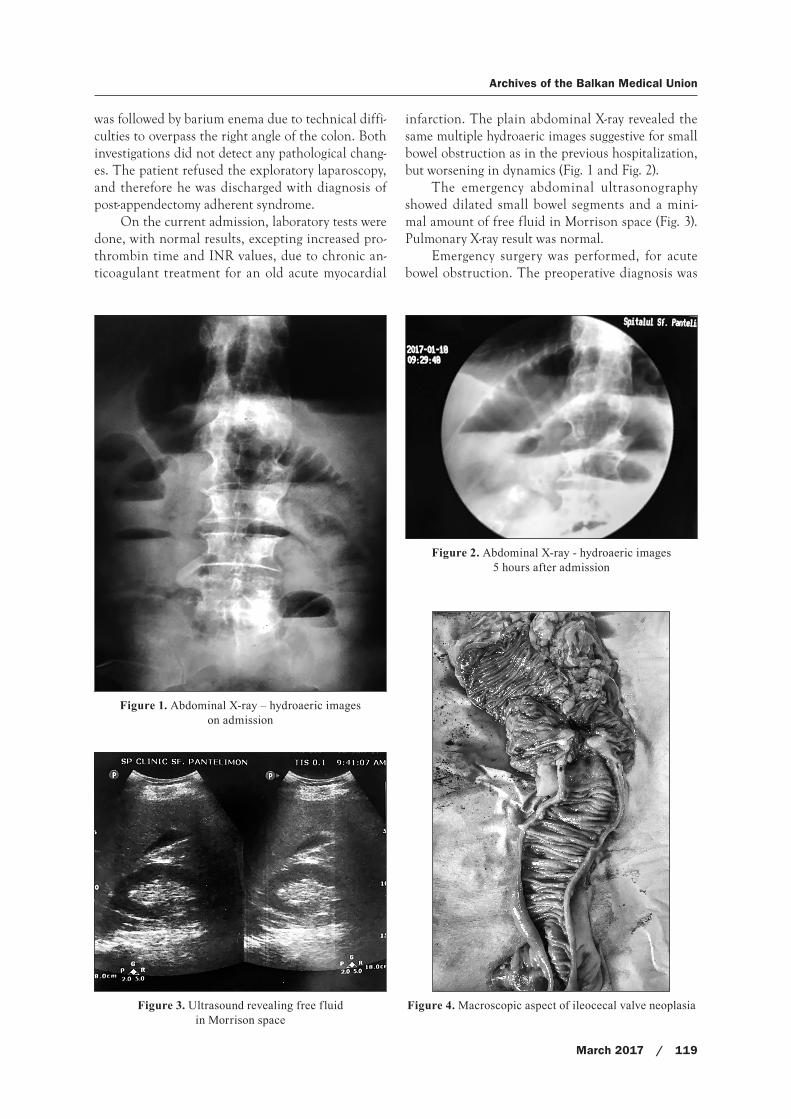
small bowel obstruction due to post-appendectomy adhesions. We did a median abdominal incision. Minimal free serous fluid has been found by explora-tion of the peritoneal cavity, with dilated small bowel segments, from angle of Treitz to cecum, and a nor-mal colic loop, without any post-operative adhesions. Palpation of cecum revealed a small tumor situated at the ileocecal junction, with no expression to sero-sa, and determining a complete stenosis at this level. Right hemicolectomy and peritoneal drainage were performed. The macroscopic aspect of the resection specimen is shown in figure 4.
The postoperative evolution was without com-plications, with early mobilization, oral food intake starting 24 hours after surgery and bowel transit rees-tablished in the first 72 h after surgery. The peritoneal drainage was suppressed on day 5. The patient was dis-charged on the 6th day, with complete surgical healing.
The histopathological examination of the resec-tion specimen revealed a moderately differentiated, ulcerative adenocarcinoma of the ileocecal valve, with invasion of the muscular layer (Fig.5).
DISCUSSION
Acute pain in the right iliac fossa is one of the most common symptoms in patients admitted in sur-gical wards. Many pathologies may present with acute pain in the right iliac fossa, with diverse therapeutic approaches (surgical/non-surgical). The exact etiolog-ical diagnosis in most of the cases is possible due to imaging techniques12. In the case presented, pre vious imaging investigation could not detect the presence of the tumor, before complications occurred. The di-agnosis was established only intraoperatively.
The structures of the ileocecum may be involved in many pathological processes, many of them be-ing common in clinical practice. The disease may involve only one of the structures, several of them
simultaneously or may be part of a general process. In this case, there was no expression on the serosa, no mesenteric retraction or macroscopic adenopathy to signalize the place of tumor. Only the abrupt tran-sition from dilated small bowel loops to empty right colon, along with palpable detection of the tumor, revealed the diagnosis.
The clinical presentations are variable, from as-ymptomatic patients to severe cases of acute abdo-men. In these situations, the role of imaging is cru-cial. In our patient, imaging investigations could only detect the acute bowel obstruction by revealing hy-droaeric images (plain abdominal X-ray) and free peri-toneal fluid, along with dilated small bowel loops (ul-trasound abdominal examination). The clinical onset by an acute complication (bowel obstruction) and the short time from admission to surgical intervention left no time for an accurate preoperative diagnosis.
Although imaging findings suggestive of ma-lignant tumors of the ileocecal valve have been de-scribed, these lesions are often difficult to detect, especially in the presence of obstruction (10). Lack of general neoplastic symptoms and failure to detect the ileocecal valve tumor in the prior admission misled to the diagnosis of adherent syndrome, sustained by appendectomy in the past medical history and recent recurrent symptoms of acute bowel obstruction. Due to the small calibre of ileocecal valve, a shorter evo-lution than in other colonic localization led to early acute bowel obstruction by tumor, with lack of gener-al signs and symptoms of neoplasia.
CONCLUSIONS
Ileocecal valve tumor evolution is fast toward acute bowel obstruction due to small calibre of the valve. Diagnosis is often delayed due to lack of specific symptoms and effective screening methods, and the clinical onset is often by complication (obstruction).
The overall staging and pattern of spread is simi-lar to that of colorectal cancer, but on a stage-for-stage basis, prognosis is worse for small bowel adenocar-cinoma. Resectability of the primary tumor is a key prognostic factor, along with age, performance status and presence of distant metastasis.
Surgery is the mainstay of treatment for both localized and locally advanced disease. Careful in-traoperative assessment, including evaluation of the tract of the bowel involved, inspection and palpation of the liver, resection and examination of the spec-imen are essential to identify malignancy13. If neo-plastic lesion of ileocecal valve is suspected, the right hemicolectomy is the procedure of choice14.
Despite the actual diagnosis and the onset by an acute complication, the long term vital prognosis for
Figure 5. Microscopic aspect of ileocecal valve adenocarcinoma

Archives of the Balkan Medical Union
March 2017 / 121
patients with ileocecal valve tumor seems to be better than for other bowel localization. This is due to the short evolution and, consecutively, to a smaller win-dow of opportunity for metastatic process to develop.
Differential diagnosis includes cecal carcinoids that generally arise near the ileocecal valve and share histopathologic and clinical features with ileal carci-noids. Adenomatous polyp or benign ulceration of the ileocecal valve are also two very rare and distinct entities, with symptoms similar with ileocecal valve tumors15,16.
Neoplasms of ileocecal valve are very rare, in the medical literature being reported only a small num-ber of cases.
ACKNOWLEDGEMENT
We thank each member of the medical team and the patient.
Conflict of interest: nothing to declare
REFERENCES
1. Upadhyay R, McKinlay AW, Danesh BJ, et al. An unusual case of ileocecal carcinoma presenting with steatorrhea. Am J Gastroenterology 1989; 84(11):1467-8.
2. Glasser ST, Mersheimer W. Carcinoma of the ileocecal valve. Am J Surg. 1942;56(3):650–4.
3. Gallego MS, Pulpeiro JR, Arenas A, Colina F. Primary ade-nocarcinoma of the terminal ileum simulating Crohn’s dis-ease. Gastrointest Radiol. 1986;11(4):355–6.
4. Horton KM, Jones B, Baylesss TM, et al. Mucinous adeno carcinoma at the ileocecal valve mimicking Crohn’s disease. Dig Dis SCI 1994; 39(10): 2276-81.
5. Dickstein AM, Shinagare S, Guelrud M. An unusual ileoce-cal valve mass. Gastroenterology. 2015;148(7):1292–3.
6. Shivaani Kummar, MBBS, Thomas E. Ciesielski, MD, and Miklos C. Fogarasi. Management of small bowel adenocar-cinoma. Oncol J, Colorectal Cancer, Gastrointest Cancer 2002. www.cancernetwork.com (accessed January 2017).
7. Greenstein AJ, Sachar DB, Smith H, et al. A comparison of cancer risk in Crohn’s disease and ulcerative colitis. Cancer 1981;48:2742-2745.
8. Offerhaus GJ, Giardiello FM, Krush AJ, et al. The risk of upper gastrointestinal cancer in familial adenomatous pol-yposis. Gastroenterology 1992;102:1980-1982.
9. Rodriguez -Bigas MA, Vasen HF, Lynch HT, et al. Characteristics of small bowel carcinoma in hereditary non-polyposis colorectal carcinoma. International Collaborative Group on HNPCC. Cancer 1998;83:240-244.
10. El-Amin LC, Levine MS, Rubesin SE, et al. Ileocecal valve: spectrum of normal findings at double-contrast barium en-ema examination. Radiology 2003; 227: 52-8.
11. Park YS, Lee JD, Seo YS, et al. A case of adenocarcinoma in ileocecal valve mimicking inflammatory bowel disease. Korean J Gastrointest Endosc 2002; 25(4):232-6.
12. H. Vidal Trueba, S. Marques Llano, F. Gonzalez, Crespo Del Pozo. Mysteries to be solved in the ileocecal area: tricks to reach a correct diagnosis. Radiological Society of North America 2013 Scientific Assembly and Annual Meeting, December 1-December 6, 2013, Chicago, Il. http://archive.rsna.org/2013/13018357.html (accessed February 19, 2017).
13. Peck JJ. Management of carcinoma discovered unex-pectedly at operation for acute appendicitis. Am J Surg. 1988;155(5):683–5.
14. Fiume I, Napolitano V, Del Genio G, Allaria A, Del Genio A. Cecum cancer underlying appendicular abscess. Case report and review of literature. World J Emerg Surg. 2006;1(1):11.
15. Hildreth DH, Bishop RP, Johnson TR. Adenomatous pol-yps of the ileocecal valve: report of three cases. Dis Colon Rectum. 1975;18(1):52–8.
16. C Papanikolaou, G Anthimidis, I Tsadila, et al. Benign ul-ceration of ileocecal valve: a new cause of low gastrointesti-nal bleeding? The Internet Journal of Surgery. 2009; 22 (1).
Related Documents











