NUR HAZIERAH MUHAMMAD SYAZWAN SUPERVISOR: MR. KUMAR DR CHE AHMAD MUTTAQIN

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NUR HAZIERAH
MUHAMMAD SYAZWAN
SUPERVISOR: MR. KUMAR
DR CHE AHMAD MUTTAQIN

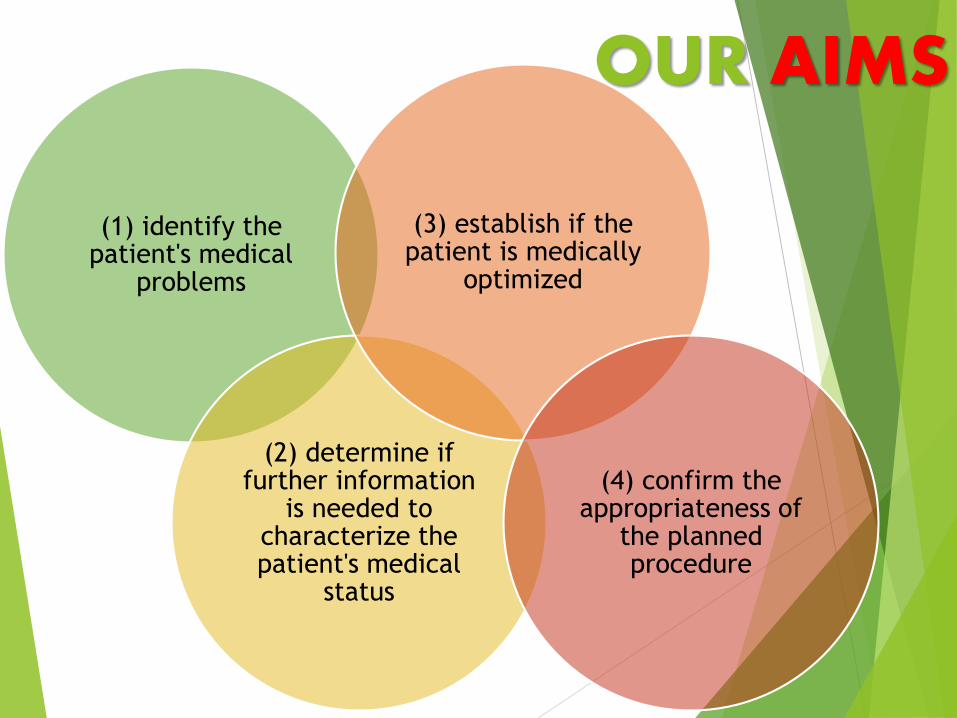
OUR AIMS
(1) identify the patient's medical
problems
(2) determine if further information
is needed to characterize the patient's medical
status
(3) establish if the patient is medically
optimized
(4) confirm the appropriateness of
the planned procedure

Correct abnormalities
Informed consent
Details of Preparations
Lab Investigations
Cross-match blood
Physiotherapy
Breathing Exercise
DVT Prophylaxis
Anaesthetic Premedications
Principles of
Preoperative
Preparation

The Assessments
Full History
Examination
Lab Test
Radiographs
ECG
Appropriate Procedure
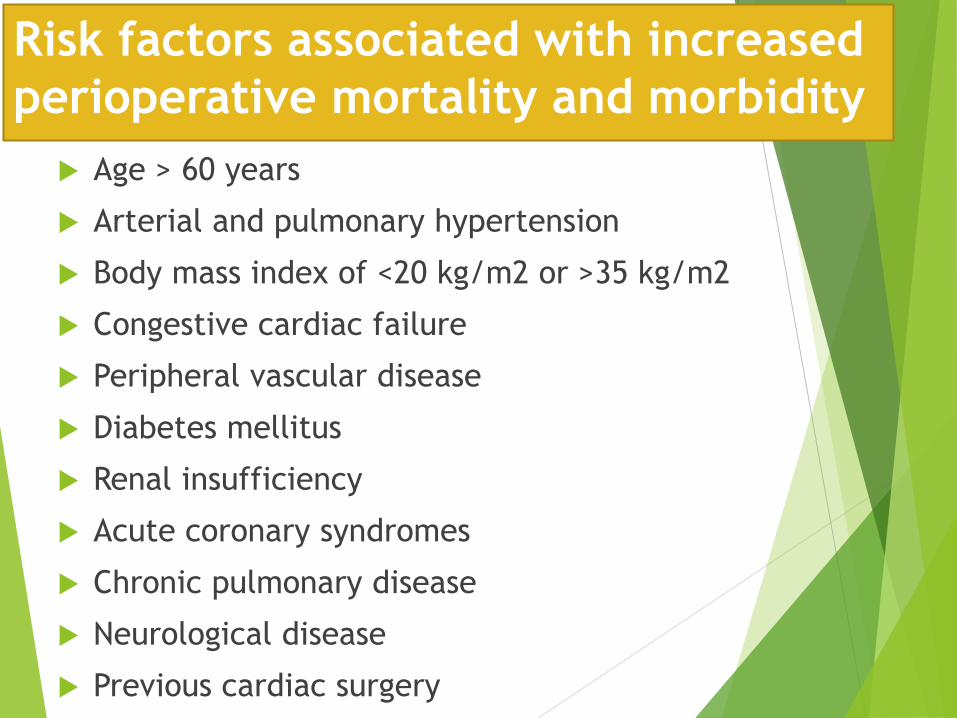
Risk factors associated with increased
perioperative mortality and morbidity
Age > 60 years
Arterial and pulmonary hypertension
Body mass index of <20 kg/m2 or >35 kg/m2
Congestive cardiac failure
Peripheral vascular disease
Diabetes mellitus
Renal insufficiency
Acute coronary syndromes
Chronic pulmonary disease
Neurological disease
Previous cardiac surgery

General Problems in Surgical Patients
• Extreme age
• Limits: cardiac, repiratory, renal reserve
• Smaller doses of narcotics, sedatives & analgesics
Age
• Affects wound healing
• High incidence of respiratory problems
• DVT & Pulmonary embolism are common
• Bedsores
Obesity
• Reduced response to trauma & infection
• Causes: Immunosuppressive drugs, uremia. Malnutrition or liver disease
Compromised Host

General Problems (cont.)
• Sensitivity to sedatives, anaesthetic, antibiotic drugs or dressing
• Unexpected reaction might occur
• Severe cases -> Anaphylactic shock
Allergies
• Diabetics might need to change to sliding scale
• Patient on steroids may need additional cover during major surgery
• Adjustment anticoagulant therapy
• Warfarin -> Heparin (perioperatively)
• Clopidogrel contraindicated in regional anaesthesia (causing epidural hematoma)
• Acetylcholine & ATH Inhibitor (Antithrombin + Heparin inhibitor) should stop 24hours before surgery to prevent severe & refractory hypotension
Drugs

CO
MO
RB
ID D
ISE
ASE
CARDIOVASCULAR DISEASE
RESPIRATORY DISEASE & SMOKING
MALNUTRITION, ADHESION AND JAUNDICE
RENAL DISEASE
HEMATOLOGICAL DISEASE
OBESITY
DIABETES MELLITUS

ASA Physical Status Classification System
1• A normal healthy patient
2• A patient with mild/moderate systemic disease
3
• A patient with severe systemic disease which limits activities
4
• A patient with severe systemic disease that is a constant threat to life
5
• A moribund patient who is not expected to survive without the operation
6
• A declared brain-dead patient whose organs are being removed for donor purposes
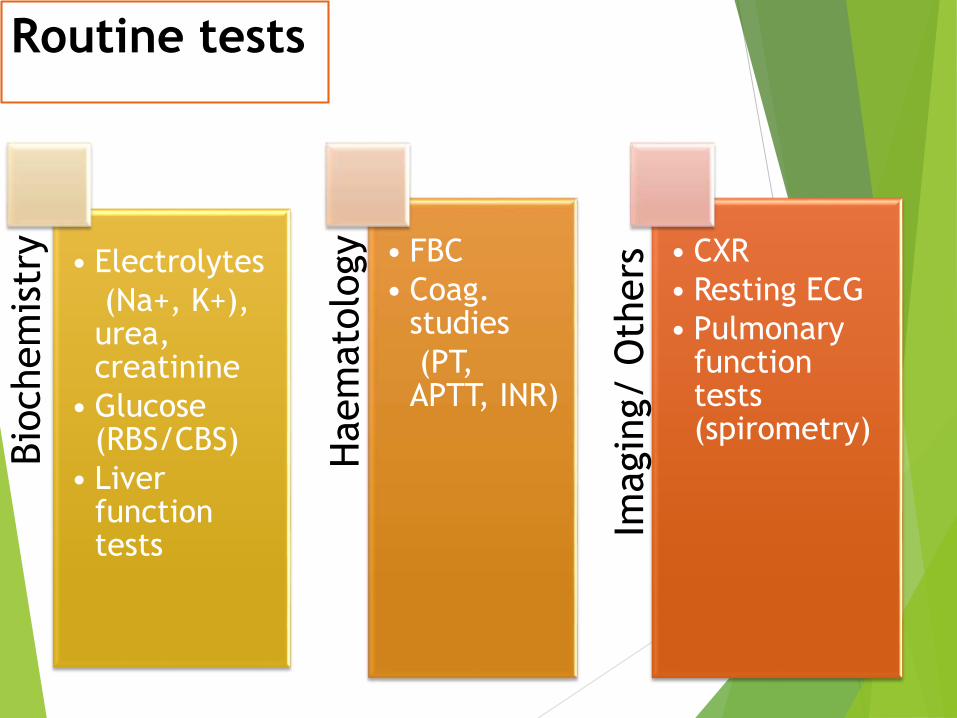
Routine testsBio
chem
istr
y
• Electrolytes
(Na+, K+), urea, creatinine
• Glucose (RBS/CBS)
• Liver function tests
Haem
ato
logy • FBC
• Coag. studies
(PT, APTT, INR)
Imagin
g/ O
thers • CXR
• Resting ECG
• Pulmonary function tests (spirometry)

PRE-OPERATIVE INVESTIGATIONSPatient status ECG CXR BUSE FBC RBS LFT COAG
<50years, ASA 1 No investigations needed
>50 years, ASA 1 X
>60 years, ASA 1 X X X X
Diabetes X X X X
HPT, IHD X X X
Anemia X
Renal disease X X X
Liver disease X X X X
Haematological disease X X
Respiratory disease X
Alcohol abuse X
On Chemotherapy X
On Anticoagulants X
Procedures with blood loss >15% X X

PROPHYLACTIC MEASURES AGAINST COMMON
POST OPERATIVE COMPLICATONS
• Antibiotics before op such as IV Rocephine and Flagyl
Surgical infections
• Chemical – Heparin
• Mechanical –compression stokings
DVT
• Adequate renal perfusion
• Adequate oxygenation
Renal failure

REASONS FOR ANESTHETIC REFERRAL
Allergy or intolerance to certain substances, drugs or classes of drugs
Documented allergy to anesthetic drugs, analgesics, localanesthetics or muscle relaxants
Instability or immobility of the cervical spine
Rheumatoid arthritis, Down’s syndrome, Ankylosing spondylitis
Previous instrumentation of the cervical spine
Known or potential difficult airway
Limited jaw opening (temperomandibular joint arthritis, trismusrelated to oral or submental sepsis, previously wired teeth, facialradiotherapy or burns, previous reconstructive surgery tomandible, tongue or mouth).
Small mandible
Large tongue (acromegaly, morbid obesity)

Difficult venous access
Previous chemotherapy
Abusers of intravenous drugs
Burns to upper limb
Severe and widespread skin disorders (psoriasis, epidermolysis
bullosa, pemphigus, pemphigoid)
Morbid obesity
Clotting disorders
Treatment with anticoagulant or anti-platelet drugs
Haemophilia and variants
Platelet disorders

ASSESSMENT OF THE LIKELY IMMEDIATE
POST-OP COURSE & THUS THE NEED FOR
HDU/ICU SUPPORT
Circumstance in which patients requiring ICU care
postoperatively:-
When an operation causes major physiological disturbances
requiring close monitoring and /or organ support (e.g. major
surgery)
When an unexpected major medical or surgical complication
occurs during surgery, threatening organ dysfunction (e.g.
intraoperative haemorrhage and myocardial infarction)
When previous intercurrent disease compromises physiological
reserve (e.g. patient with severe COPD undergoes major
abdominal surgery)

PART II: SURGICAL
CONSENT

Informed consent serves to identify and respect a
patient’s best interest by giving each patient the
opportunity to decide autonomously what his/her
best interest are in light of the planned
procedure.
SURGICAL CONSENT

CONSENT
Important because:
i) Rights of the patient
ii) Patient education
iii) Prevent misunderstanding
iv) Prevent medico-legal cases


INFORMED CONSENT

INFORMING THE PATIENT

IN GENERAL
Should presented clearly as possible
Include discussion of the diagnosis
Should include explanation of the procedure
Explanation of risks
Benefits
Potential consequences of the procedure
Treatment options
Alternatives to treatment (including nonsurgical management or non
intervention)
The consent process can technically be done
without satisfying any of the essential elements of
the “informed” component
Permissible for actual signature to be obtained by
resident, physician assistants after surgeon
properly informed the patients.
the actual informed consent documents need to
fullfill a number of criteria (table 2)
OBTAINING CONSENT FROM THE PATIENTS

Essential Components of
Documenting Consent

What is Legally Effective
Informed Consent
Under ordinary circumstances, legally effective
informed consent is obtained by reviewing the
approved informed consent with the subject,
answering any questions, and getting the subject’s
signature.
Subject Unable to Consent
• What if the subject
• Lacks capacity
• Has diminished decisional capacity
• Is a minor
• Is unconscious

Who is a Legally
Authorized Representative
• Legal Guardians
• Healthcare Surrogates
• Proxies
• Attorneys-in-fact

Other Considerations:
• Patient may refuse an operation because he/she unable to make decision
• Surgeon should explore with the patients the reason for refusing this gives some insight into patient’s thought process.
PATIENT REFUSAL
• Cognitive dysfunction, psychiatric illness
• Should consult with psychiatrists, lawyers, or other physicians goal is to improve the patient’s decision-making capacity. Not to simply obtain that the patient needs a proxy decision-maker.
DIMINISHED CAPACITY
• Korean americans, japanese americans, mexicanamericans
• Believe that terminal diagnosis relevant to treatment should be withheld from patient, and instead communicated only with the patient’s family.
CULTURAL AND FAMILIAL ISSUES

Related Documents











