Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript






Prehospital resuscitative thoracotomy is a
prehospital autopsy

Prehospital = a location
Re (back) suscitare (raise). PATIENT IS DEAD
Thoracotomy = surgical procedure
LOCATION dictates access to life-saving intervention
PROCEDURE is speciality specific

SURGEON 1
SURGEON 3SURGEON 2

Cardiac Theatre 2 Tuesdays 8am to 6pm
No teleporters
NO TIME
TIME
Penetrating traumatic cardiac arrest
LOSS OF OUTPUT to THORACOTOMY <10min
Pericardiotomy in 2-3min AFTER KNIFE to SKIN

Option 1: Don’t do thoracotomy, send to morgue
Option 2: Do thoracotomy, may live.


ProcedureSimple Equipment
Simple to train
Simplified steps
Clear indications + contraindications
Targeted Rx:
specific purpose of relieving clotted CT
controlling a cardiac wound(s)
if necessary providing internal cardiac massage.
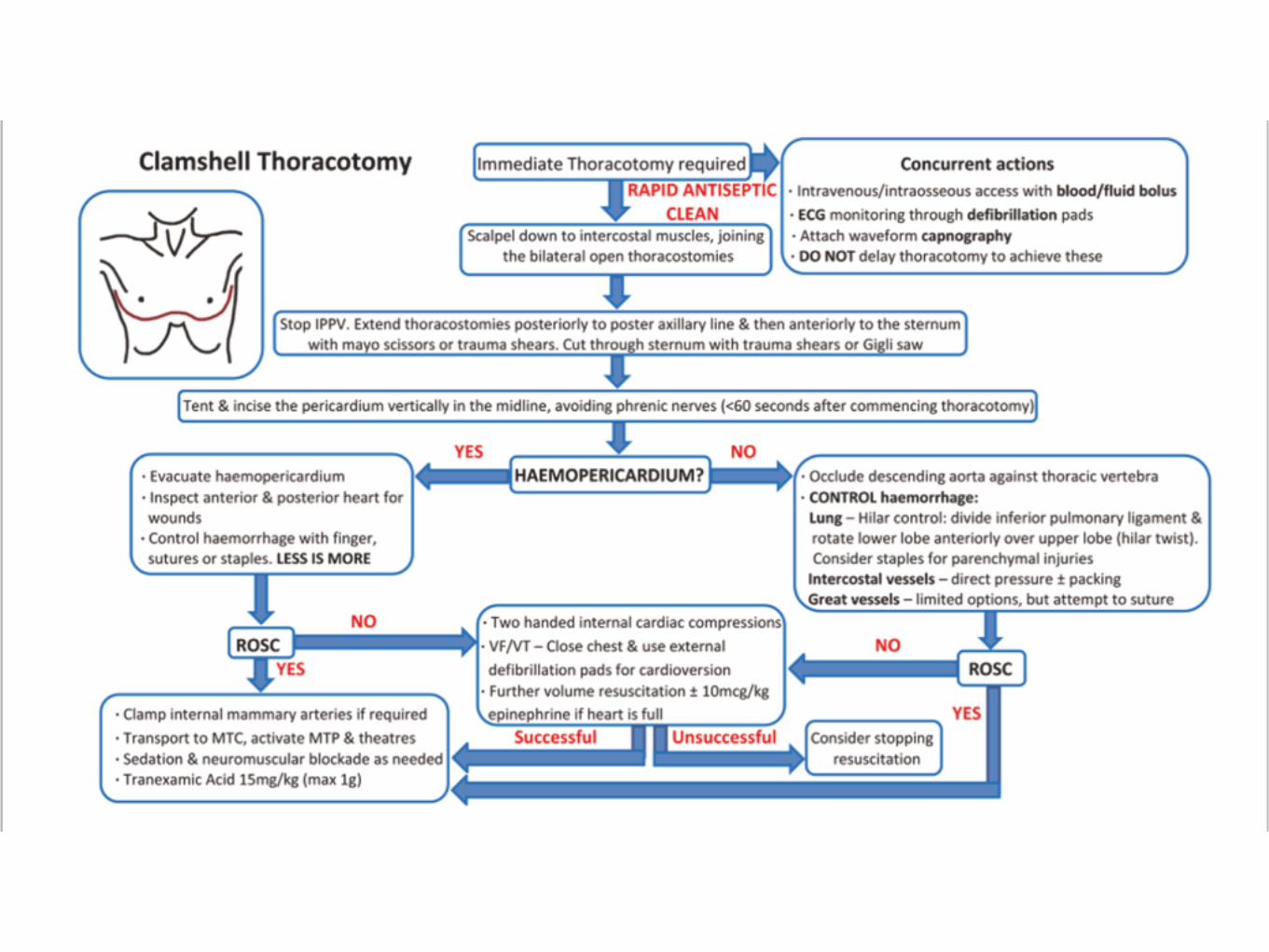

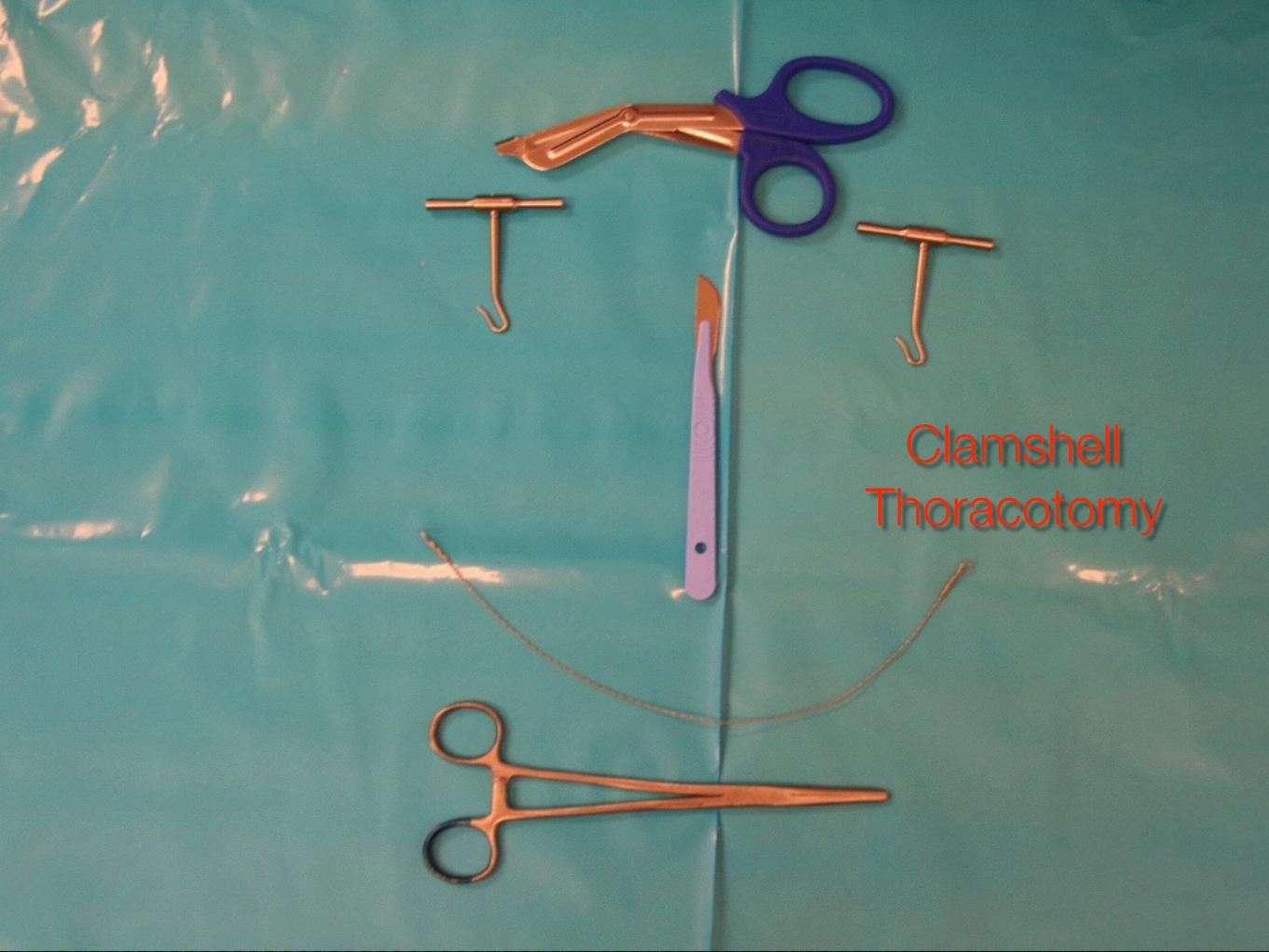
Clamshell thoracotomy
Indications
Contraindications
Clamshell Thoracotomy

NSW AE RO ME DI CAL & ME DICAL RETRIE V AL SE RV ICE
Authorised by: Director Aeromedical and Medical Retrieval Services Page 1 of 5
HELICOPTER OPERATING PROCEDURE
Traumatic Cardiac Arrest
HOP No: C/06 Issued: April 2013
Page: 1 of 5 Revision No: 2
TRIM No: 09/300 Document No: D13/5679
Distribution: Sydney Illawarra Orange !!! Helicopter Road Fixed Wing
1. Introduction
1.1. Cardiac arrest refers to the combination of pulselessness and the absence of signs of life 1.2. Survival rates from traumatic cardiac arrest are poor but comparable with published
survival rates for out-of-hospital cardiac arrest of any cause. Patients who arrest after hypoxic insults and those who undergo out-of-hospital thoracotomy after penetrating trauma have a higher chance of survival. Patients with hypovolemia as the primary cause of arrest rarely survive1.
2. Objectives
2.1. To optimise the approach to the management of pre-hospital traumatic cardiac arrest by pre-hospital critical care teams.
3. Scope
3.1. Clinical crew
4. Process 4.1. Airway Management 4.1.1 All cardiac arrest patients should be intubated without anaesthetic drugs, however if ROSC occurs anticipate the need for IV sedation and analgesia. 4.1.2 Quantitative capnometry should be used to confirm tracheal tube placement, to assess the effectiveness of resuscitation, and to inform prognosis2. 4.2 Respiratory Management 4.2.1 Unless the possibility of tension pneumothorax can be reliably excluded, bilateral open thoracostomies should be made3. Needle thoracocentesis may be performed initially for reasons of access or expediency but these should not be considered to provide definitive pleural decompression.
X X X
X X

VLE -life and limb saving procedures
Thoracotomy workshop
Pig lab procedural skills
Simulation assessment + training
Governance


100% mortality if not performed
Meaningful survivors if performed

WTF?
WTF?
WTF?
The Skeptics
competency in the face of rarity
competency of non-surgeons

Surgeons: RT, craniotomy competency for non-surgeons
Radiology- FAST, REBOA
Anaesthesia: RSI
“Not survivable”. literature doesn’t support the nihilism
Ethics: beneficence/non-maleficence are met.
benefit:harm approaches infinity

RT
@pulmcrit

Cowboys/adrenaline junkies
Patients not dead- pseudoPEA

FAILURE to build a system that can access the central circulation and control it in the next 10
years is a trauma system that needs resuscitation
Related Documents