PREGNANCY and PARTURITION Submitted To: Dr. Neeta Dave In the subject of- Physiology & Clinical Biochemistry Submitted By: Saloni P. Shroff Roll No.: 04 Semester - 2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PREGNANCYand
PARTURITION
Submitted To: Dr. Neeta Dave
In the subject of- Physiology & Clinical Biochemistry
Submitted By: Saloni P. ShroffRoll No.: 04 Semester - 2
PREGNANCYPregnancy is the development of one or more
offspring, known as embryo or fetus, in the uterus of a woman.
Fertilization• The process of fusion of
male gamete (sperm) with female gamete (Ovum) in the ampullary-isthmic junction of the fallopian tube.
Implantation• The process by which the
fertilized ovum implants (inserts or fixes itself) in the endometrial lining of uterus.
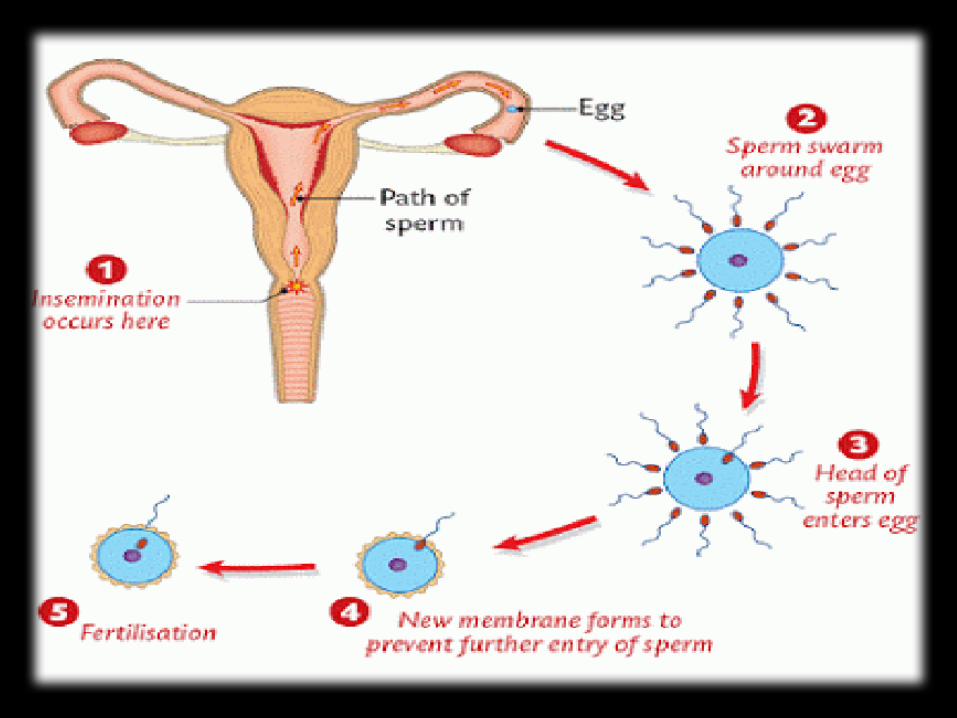
HOW fertilization
takes place??
During coitus semen is released by the
penis into the vagina (insemination)
The motile sperms swim rapidly through cervix,
enter the uterus & reach the ampullary-isthmus
junction
The ovum released by the ovary also reaches
the junction where fertilization takes
place.
A sperm comes in contact with the
ZONA PELLUCIDA layer of the ovum
This is facilitated by Hyaluronidase &
Proteolytic enzymes present in the
acrosome of sperm
These enzymes also abolish the activity of
additional sperms ensuring that only one sperm fertilizes the ova
As the sperm enters the cytoplasm of the ovum, it induces completion of the meiotic division of the secondary oocyte
Formation of a Second Polar Body
and a haploid ovum (ootid)
The haploid nucleus of the sperm and
ovum fuse together to form a diploid
ZYGOTE.
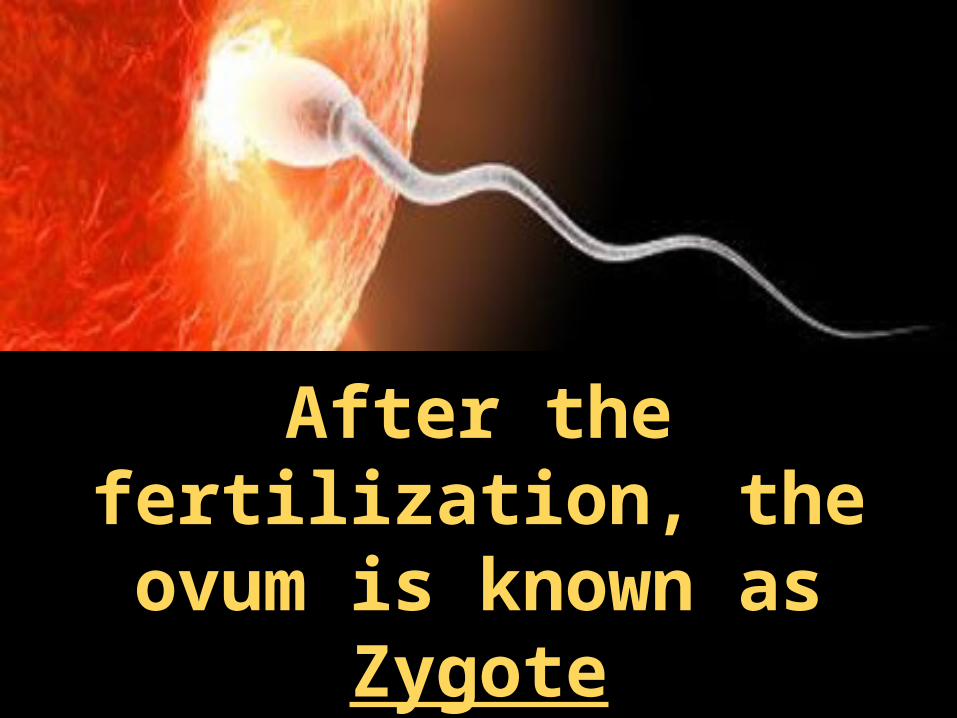
After the fertilization, the
ovum is known as Zygote
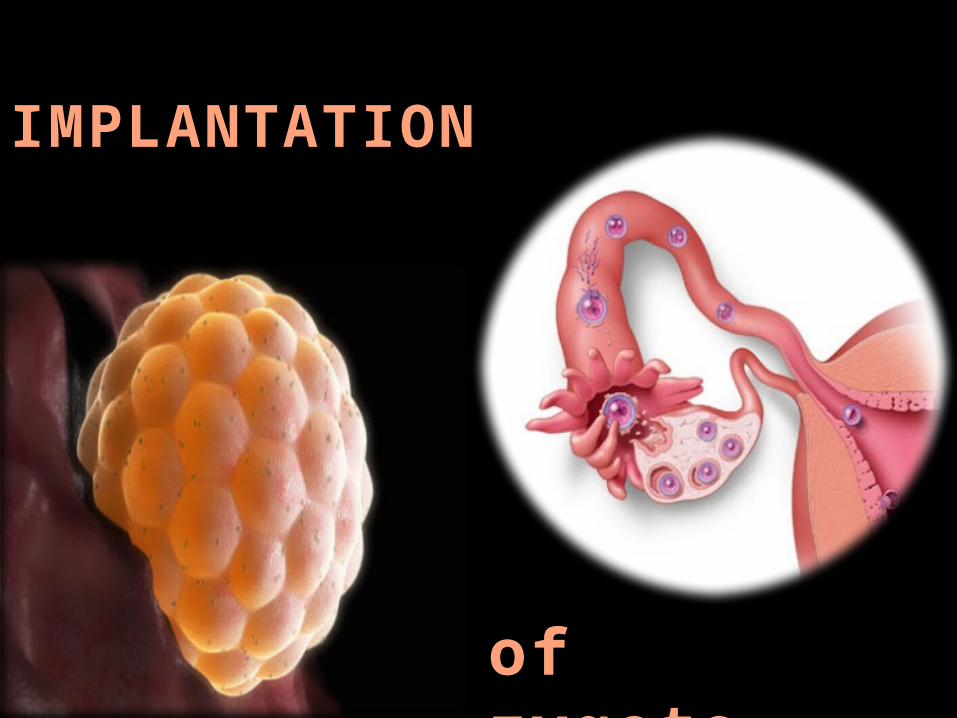
IMPLANTATION
of zygote..
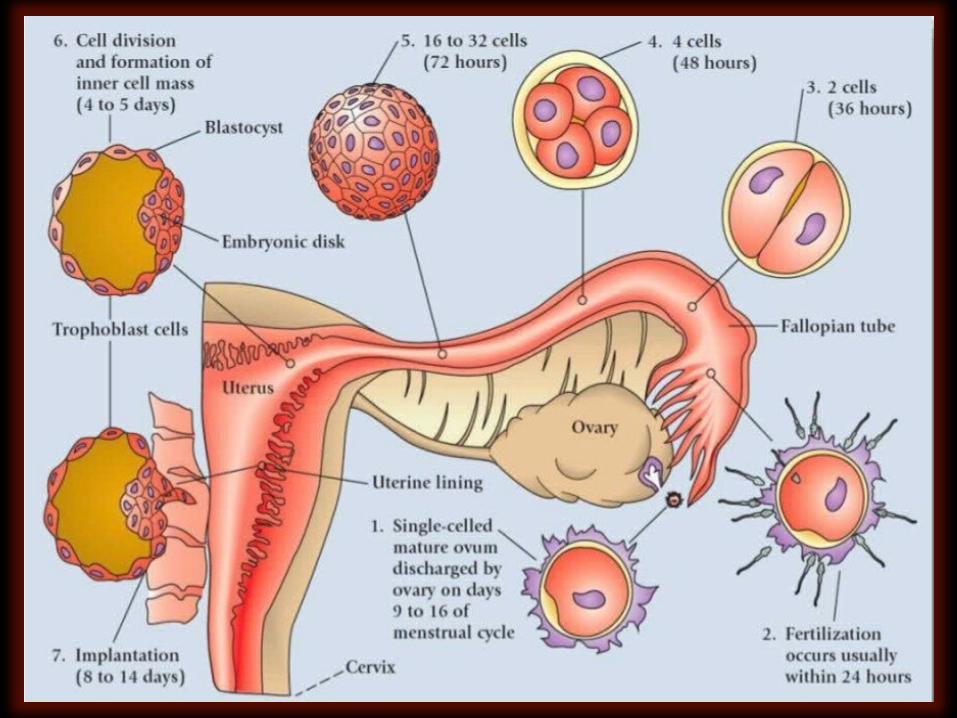
The mitotic division starts as the zygote moves through the isthmus of the oviduct towards the uterus & forms 2, 4, 8, 16 daughter cells called Blastomers.
The zygote takes 3-5 days to move to reach the uterine cavity from fallopian tube. After reaching the uterus, the developing zygote remains freely in the uterine cavity for 2-4 days before it is implanted.
Just before implantation, the zygote develops into Morula. The embryo with 8 to 16 blastomers is called a Morula.
The blastomers in the blastocyst are arranged into an outer layer called trophoblast and an inner group of cells attached to it called the Inner cell mass.
The trophoblast cells release proteolytic enzymes over the surface of the endometrium and digest the cells of the endometrium. The morula gets inside the endometrium and implants itself. The inner cell mass gets differentiated as Embryo.

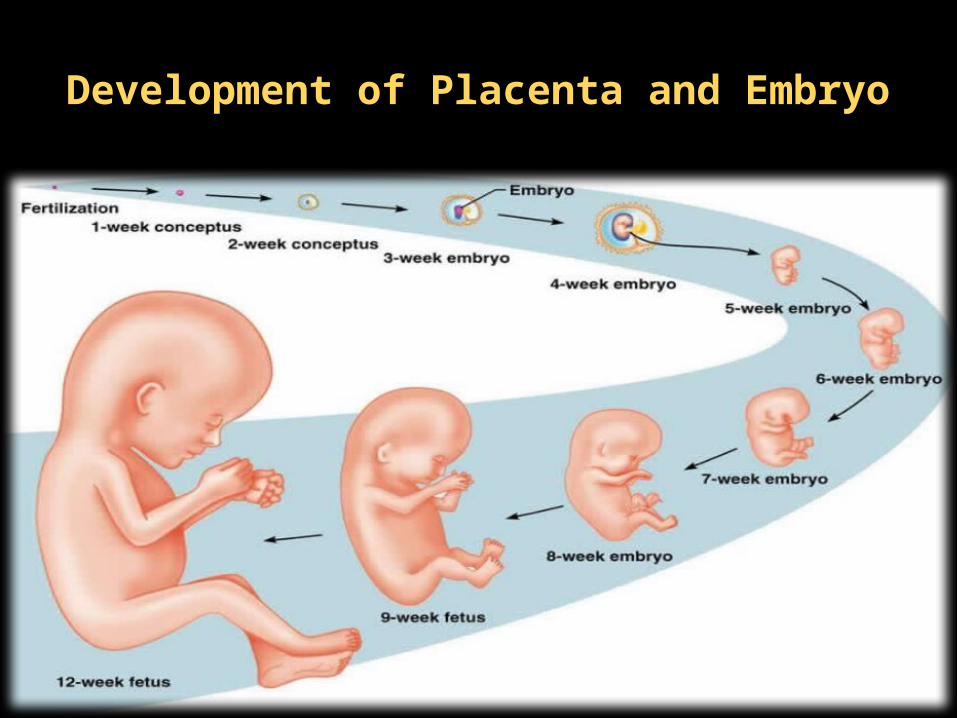
Development of Placenta and Embryo
After implantation, finger-like projections appear on the trophoblast called chorionic villi which are surrounded by the uterine tissue and maternal blood.
The chorionic villi and uterine tissue become interdigitated with each other and jointly form a structural and functional unit between developing embryo (fetus) and maternal body called placenta.
Placenta is a temporary organ present during pregnancy. It is considered as an anchor for the growing fetus.
Placenta is connected to the fetus by umbilical cord which contains blood vessels and connective tissue, helping in the transport of substances to and from the embryo.
Amniotic sac – a thin membrane arising from a cell mass within the blastocyst that completely surrounds the embryo/fetus and contains a protective fluid in which the embryo/fetus is immersed
Functions of Placenta!
NUTRITIVE FUNCTION
• The various nutritive substances, electrolytes and hormones necessary for the development of fetus diffuse from the mother’s blood into the fetal blood through placenta.
EXCRETORY FUNCTION
• The metabolic end products and other waste products from the fetal body are excreted into the mother’s blood through placenta.
RESPIRATORY FUNCTION
• Fetal lungs are nonfunctioning and placenta forms the respiratory organ for fetus.
• O2 necessary for fetus is received by diffusion from the maternal blood and CO2 from the fetal blood diffuses into the mother’s blood through placenta.
Exchange of respiratory gases between fetal blood and maternal blood:
ENDOCRINE FUNCTION
Placenta secretes 5 major hormones:
1) Human Chorionic Gonadotropin (HCG)2) Estrogen3) Progesterone4) Human Chorionic Somatomammotropin
(HCS)5) Relaxin
Human Chorionic Gonadotropin (HCG)
Its Action-
• On Corpus Luteum: HCG is responsible for the preservation and the secretory activity of corpus luteum. Progesterone and estrogen secreted by corpus luteum are essential for the maintenance of pregnancy.
• Deficiency or absence of HCG during the first two months of pregnancy leads to abortion, because of involution (shrinks or turns in) of corpus luteum.
• On fetal testes: Action of HCG on fetal testes is similar to that of LH in adults. It stimulates the interstitial cells of Leydig and causes secretion of testosterone. The testosterone is necessary for the development of sex organs in male fetus.
(Placental) Estrogen
Its Action-
• On Uterus: Causes enlargement of the uterus so that the uterus could be accommodated.
• On breasts: Responsible for the enlargement of the breasts and growth of the duct system in the breast.
• On external genitalia: Causes enlargement of the female external genitalia.
• On pelvis: Relaxes pelvic ligaments. It facilitates the passage of the fetus through the birth canal at the time of labor.
(Placental) Progesterone Its Action-
• On endometrium of uterus: Accelerates the proliferation and development of decidual cells in the endometrium of uterus. The decidual cells are responsible for the supply of nutrition to the embryo in the early stage.
• On the movement of the uterus: Inhibits the contraction of the muscles in the pregnant uterus. It is an important function of progesterone as it prevents expulsion of fetus during pregnancy.
• On breasts: Causes enlargement of breasts and growth of duct system of the breasts. Progesterone is responsible for further development and preparation of mammary glands for lactation.
Human Chorionic Somatomammotropin (HCS)
Also known as Placental Lactogen. Its Action-
• On protein metabolism: HCS acts like GH on protein metabolism. It causes anabolism of proteins and accumulation of proteins in the fetal tissues. Thus the growth of fetus is enhanced.
• On carbohydrate metabolism: It reduces the peripheral utilization of glucose in the mother leading to availability of large quantity of glucose to the growing fetus.
• On lipid metabolism: it mobilizes fat from the adipose tissue of the mother. A large amount of free fatty acid is made available as the source of energy in the mother’s body. It compensates the loss of glucose from the mother’s blood to fetus.
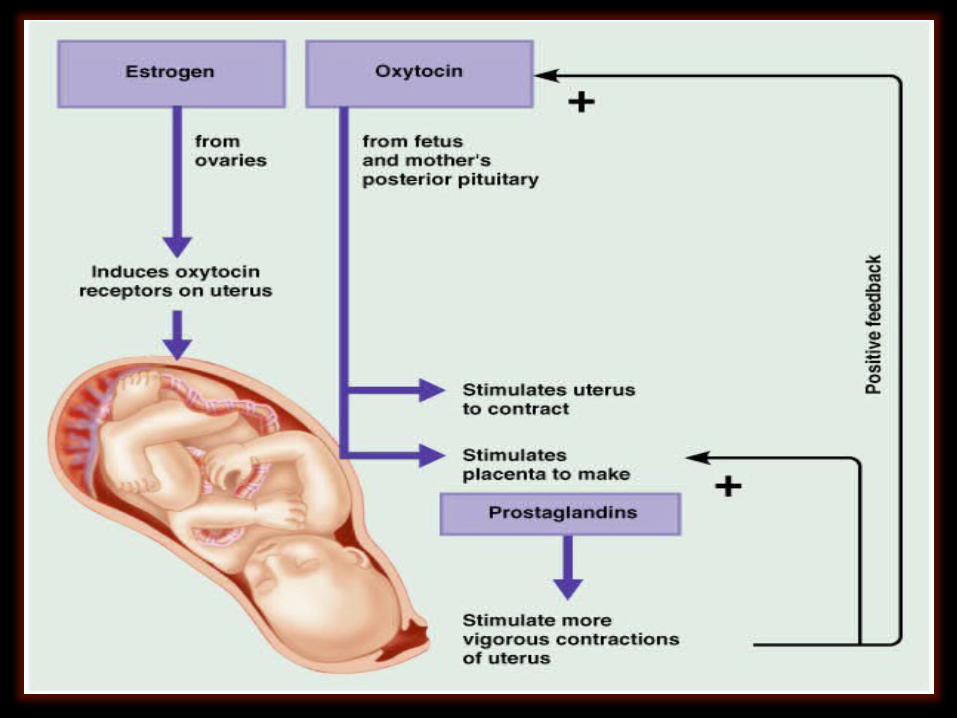
Relaxin
• Relaxin is a polypeptide which is secreted by corpus luteum, ovary and mammary glands.
• It is secreted in large quantities at the time of labor. It helps in labor.
The Fetoplacental
Unit
Fetus and placenta interact with each other to synthesize
some steroid hormones and due to this interaction
the fetus and placenta are
together called fetoplacental unit.
Some of the enzymes involved
in steroid synthesis present
in fetus are absent in
placenta and, those present in
placenta are absent in fetus.
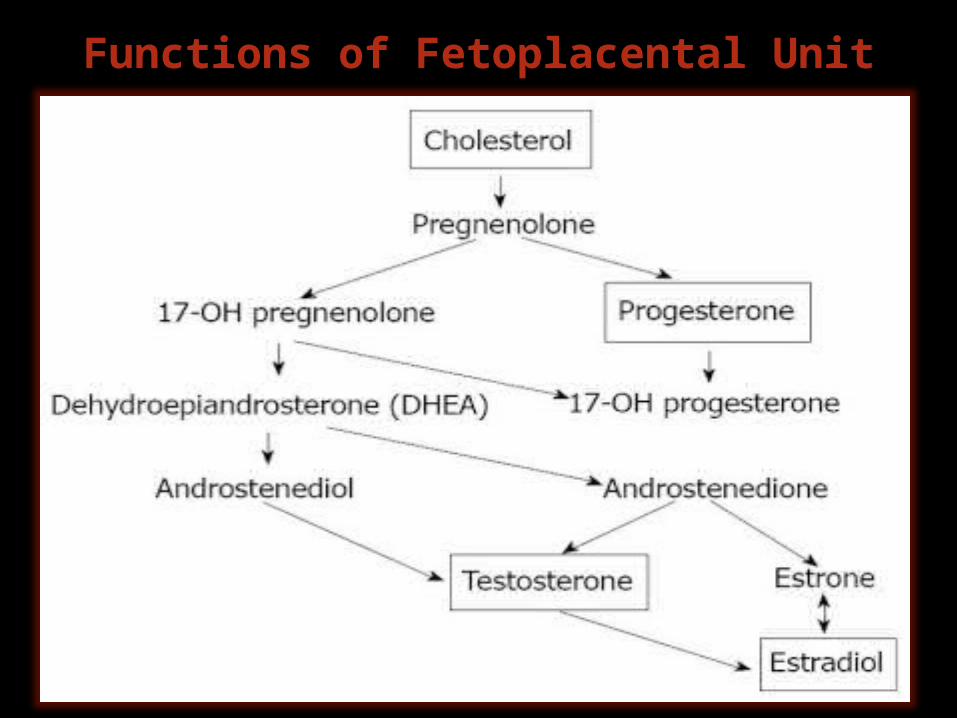
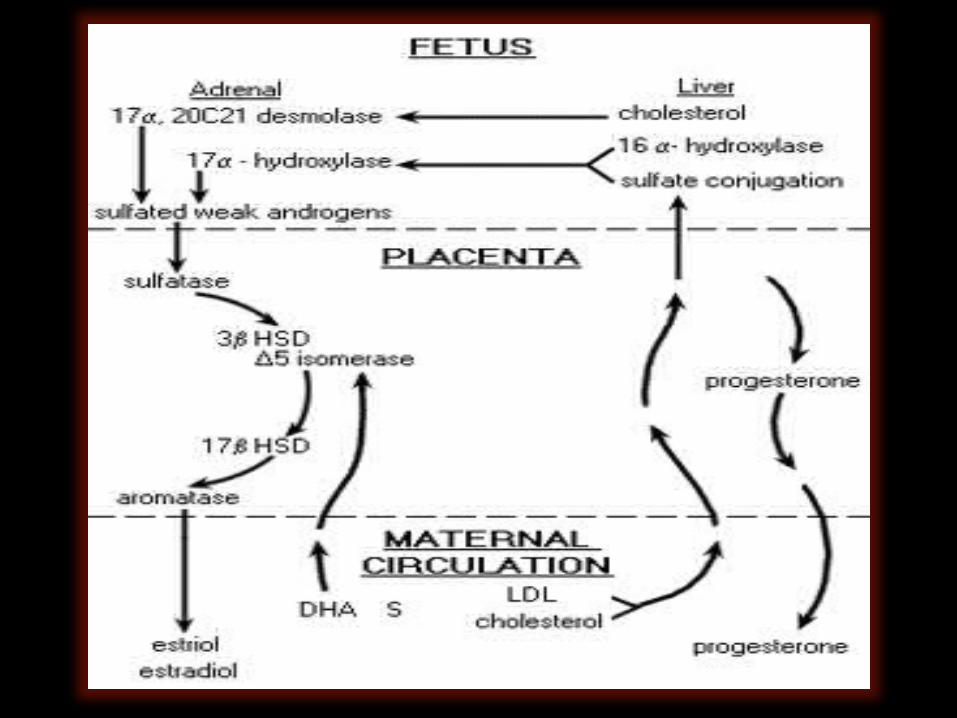
Functions of Fetoplacental Unit
EMBRYONIC OR GESTATION PERIOD..
Third week: The neural plate forms and becomes the brain and neural tube (spinal cord). Neurogenesis, the production of neurons begins. The heart chambers and
blood vessels develop.
Fourth week: The heart begins to beat, arm and leg buds are visible, eyes, ears, nerves, and muscular,
skeletal, and digestive systems begin to form. Vertebrae are present, major veins and arteries are
completed.
Fifth week: The brain has five components and the nose and lips begin to form.
Sixth week: Differentiation of external genitalia and internal reproductive organs begins. The head and brain are prominent; arms and legs are longer; and hands and feet have fingers and toes. The lungs begin to develop.
Seventh week: The face, eyelids, and neck begin to form. The stomach and other internal organs are in position. Muscles are forming, arms and legs are
apparent, and the embryo can move.
Eighth week: The embryo appears more human, the inner and middle ear develop, and the embryo is the size
of a grape.
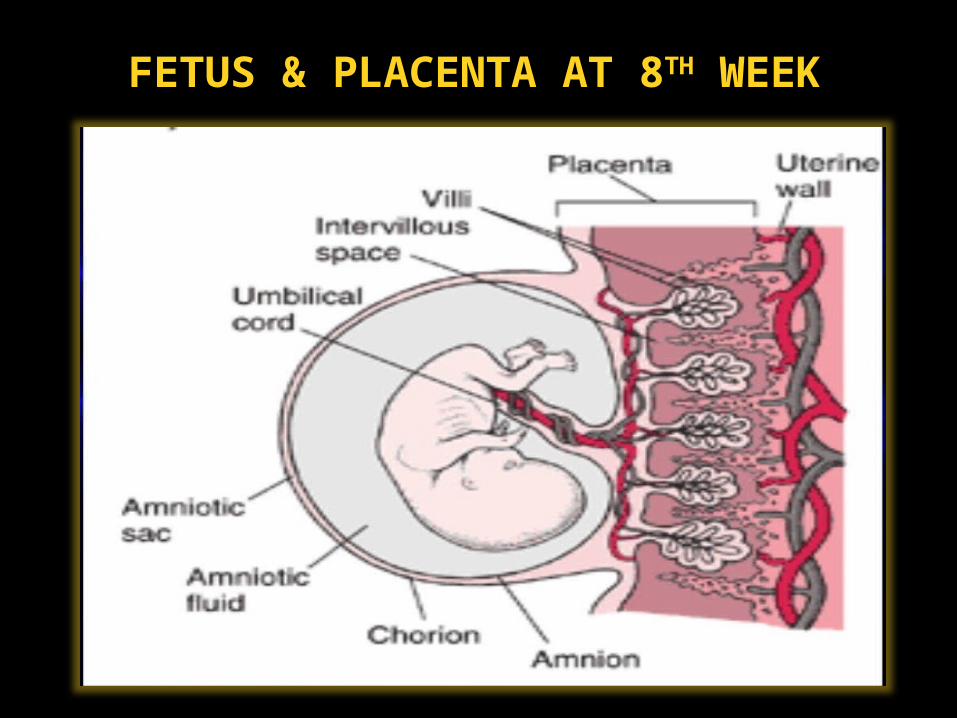
FETUS & PLACENTA AT 8TH WEEK
THE PERIOD OF THE FETUS: 9 WEEKS TO BIRTH
• The period of prenatal development that begins after organogenesis is 95% complete at about week 9 and continues until birth.
– 9 to 12 weeks: Intestines are in position, the spinal cord is visible, the eyes take final form and the eyelids can close, red blood cells form in the liver. Sex organs are now apparent. Tooth buds appear. The heartbeat is audible with the right equipment. The fetus is 2.4 to 3 inches long.
– 13 to 16 weeks: The skin is almost transparent, the bones and joints are distinct, the brain’s hemispheres are visible. Lanugo (fine hair) and vernix caseosa (oil) begin to appear on skin. The fetus is 4.7 inches long and weighs 3.5 oz. The mother may feel quickening (fetal movement).
– 17 – 20 weeks: Dental enamel forms . Myelination of nerves begin. The intestines and kidneys work. Ultrasound is typically done at around 20 weeks.
– By 24 weeks: Fat begins to accumulate. Bone marrow begins producing red blood cells. Eyes are fully formed. The fetus is 9 inches long and weighs 21.6 oz.
FETAL DEVELOPMENT FROM WEEK 25 TO WEEK 40
• Viability – The ability of the fetus to survive outside the womb; at about week 24 to 25.
– By 28 weeks: The brain continues to develop, fetal activity increases, fat forms, fingernails appear, the eyes open, close, and blink in response to light and sound. The fetus is 10.6 inches long and weighs 38 oz.
– By 32 weeks: The fetus responds to sound and external pressure, in males, the testes descend, the brain is 25% of adult weight. The fetus is 12.2 inches long and weighs 4 to 4.6 lbs.
–By 36 weeks: The lanugo begins to disappear, physical growth slows while the brain continues developing and becomes more convoluted, and the fetus has obvious sleep and wake cycles.
–By 40 weeks: The fetus gains 50% of its birth weight in the last month. The skin is smooth. The head has hair and lanugo only remains on the shoulders. Myelination increases. The fetus is the size of the average newborn: roughly 17 – 20 inches long and weighing about 7 lbs.
Maternal Changes During Pregnancy
The maternal system may produce a series of changes in order to adapt to the needs of fetal growth and development influenced by placental hormones and neuro-endocrine system. The changes observed are mainly-
1. Structural 2. Metabolic 3. Physiological
STRUCTURAL CHANGES
Observed in primary sex organs, accessory sex organs and mammary glands.
1. Ovaries: No follicular changes and no ovulation
because FSH and LH inhibited. Enlargement of Corpus Luteum- secretes
progesterone and little estrogen; degeneration after 3 months
2. Uterus: Increase in volume from almost zero to 5-7 liters at
the end of pregnancy. Increase in size due to hyperplasia, hypertrophy and
growth of fetus. Change in shape from pyriform to globular. Increase in weight from 30-50g to 1000-1200g Formation of Decidua- bed for the growing fetus.
3. Vagina: Increase in size. Violet coloration due to increased blood supply. Less cornification of superficial epithelial cells Decrease in pH – below 3.5 Increased deposition of glycogen in the epithelial
cells due to increased secretion of estrogen
4. Cervix: Increase in blood supply and mucus secretion Softening of tough muscles Formation of mucus plug which closes the cervical canal.
5. Fallopian tube: Increase in blood supply and hyperplasia of epithelial cells Upward movement of fallopian tube due to the large sized
uterus.
6. Mammary glands: Development of more new ducts and alveoli. Increase in size and deposition of fat. Increase in vascularization. Pigmentation of nipple and areola.
Increase in body weight The average weight gained during pregnancy is about 12
kg.
METABOLIC CHANGES
• Accelerated metabolic activities due to increased hormonal secretions of Thyroxine, Cortisol and Androgens.
1. Basal Metabolic rate- increases by about 15% in the later stages of pregnancy.
2. Protein metabolism- • Anabolism increases• Positive nitrogen balance• Deposition of proteins increases in uterus
3. Carbohydrate metabolism-• Blood glucose level increases. As a result, hyperplasia of
beta cells of islets of langerhans in pancreas takes place leading to increase in insulin secretion.
• Hepatic glycogen depletes leading to glycosuria.
4. Lipid metabolism- Deposition of about 3-4 kg of fat in the
maternal body. Increase in blood cholesterol level and
ketosis.
5. Water and Mineral metabolism- Estrogen and progesterone increase the
retention of sodium and water. Reabsorption of sodium from renal tubules
due to aldosterone. Retention of calcium and phosphorus which
are necessary for the growing fetus.

PHYSIOLOGICAL CHANGES1. Blood: Increase in volume to about 20% or 1 liter due to
increase in plasma volume; causing hemodilution. Anemia observed because of increased demand for
iron by the fetus.
2. Cardiovascular system: Cardiac output increases by about 30% in the first
trimester. Gradually decreases and then reaches to normal. Slight lowering of blood pressure during second
trimester. Hypertension observed if prenatal care is not taken
3. Respiratory system: Overall activity of respiratory system increases- higher
pulmonary ventilation and oxygen utilization.
4. Excretory system: Increased renal blood flow and GFR; increase in urine
formation.
5. Digestive system: Occurrence of morning sickness during initial stages. Nausea, vomiting and giddiness due to hormonal imbalance. G.I. tract motility suppresses due to progesterone leading to
constipation. Indigestion and hypochlorhydria occurs.
6. Nervous system: General excitement of nervous system. Psychological imbalance- mood swings, excitement or
depression in the early stages of the pregnancy.
7. Endocrine system:
Anterior pituitary- increased size, secretion of corticotropin, thyrotropin and prolactin increases. Decrease in LH and FSH due to negative feedback by estrogen and progesterone.
Adrenal cortex- moderate increase in secretion of cortisol; helps in mobilization of amino acids from mother’s tissue to fetus. Increased secretion of aldosterone; water and sodium retention.
Thyroid gland- increase in size and secretory activity. Thyroxine helps in mammary gland preparation for lactation. Increased BMR.
Parathyroid glands- increase in size and secretory activity. Parathormone responsible for maintenance of blood calcium levels in the mother.

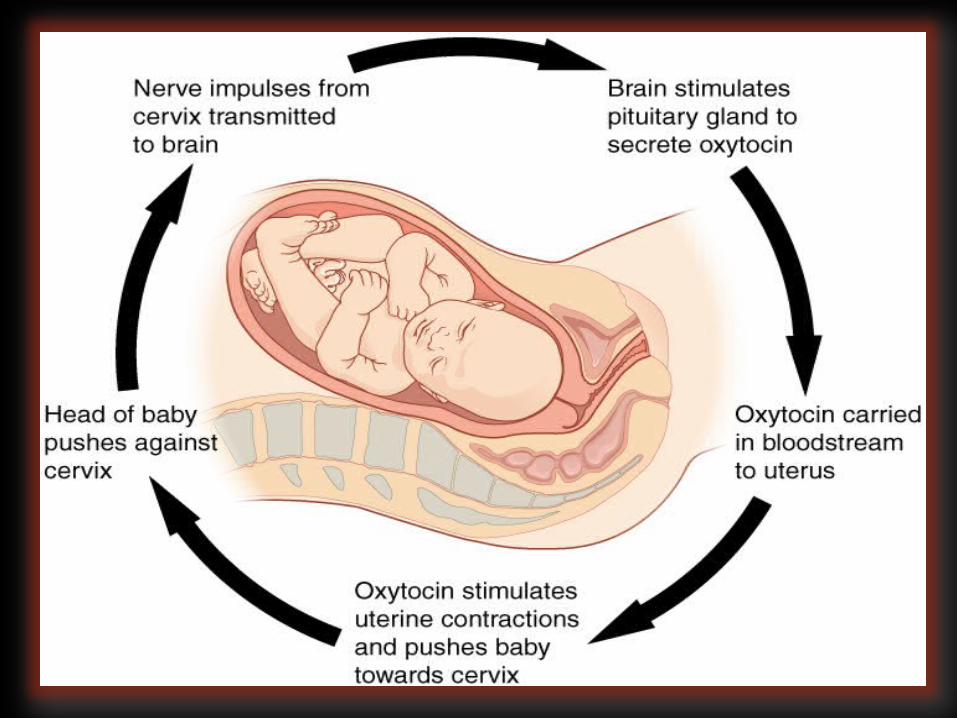
PARTURITION• Refers to the expulsion or delivery
of the fetus from the mother’s body.
• LABOR: Physiologic process by which a fetus is expelled from the uterus.
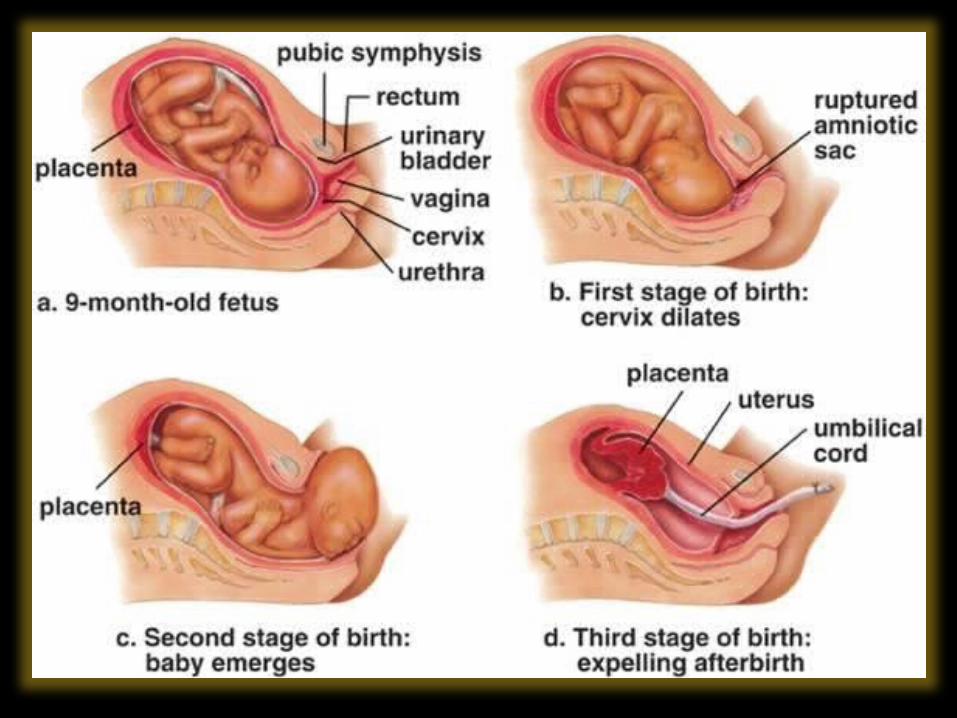
STAGES OF PARTURITION
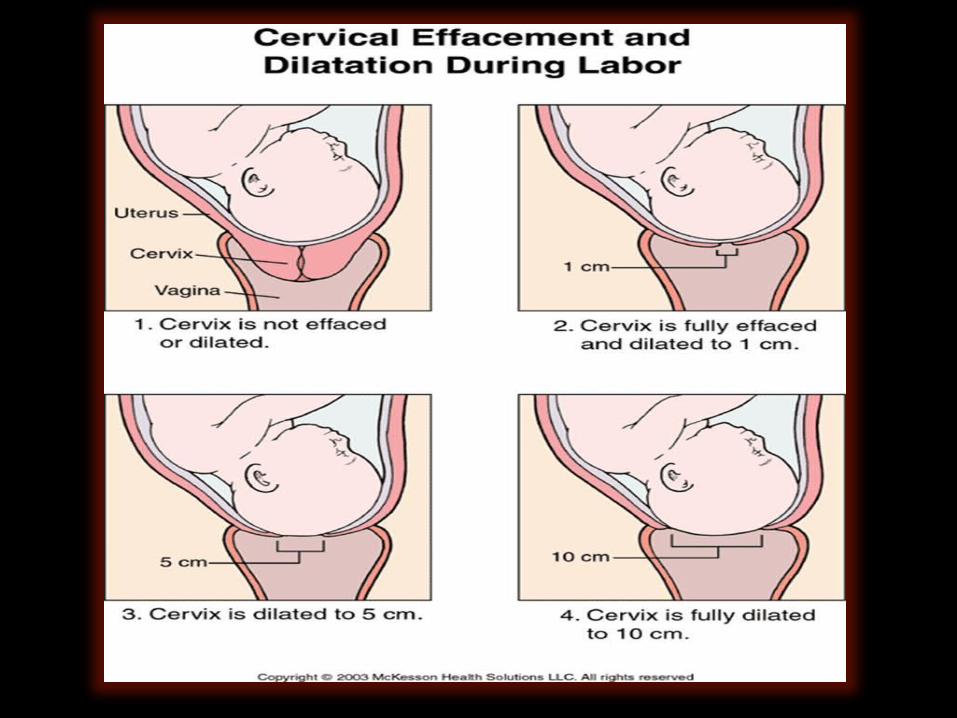
1st Stage •The strong uterine contractions called labor contractions commence. It arise from the fundus of uterus and move downwards so that the head of fetus is pushed against the cervix. It results in dilatation of cervix and vaginal canal.
2nd Stage •The fetus is delivered out from the uterus through cervix and vaginal canal. This stage lasts for about one hour.
3rd Stage •During this stage, placenta is detached from the decidua and is expelled out from uterus. It occurs within 10-15 minutes after the delivery of the child.

BIBLIOGRAPHY..• Textbook of Biology – for class XII (NCERT)
• Essentials of medical Physiology – 5th EditionK Sembulingam, Prema Sembulingam
Websites (links URL) :-• http://www.myoops.org/cocw/mit/NR/rdonlyres/Health-Sciences-
and-Technology/HST-071Human-Reproductive-BiologyFall2002/031165F7-DB57-4806-ADC4-0B3F3D4F2339/0/ln19ahms_1960_parturition.pdf
• http://hapmd.com/home/hapmdcom/public_html/wp-content/up-loads/2009/03/sub/articulos-e-imagenes/20110615_endocrinology_of_pregnancy_and_fetoplacental_unit.pdf
• http://cdn.intechopen.com/pdfs-wm/27781.pdf
THEEND
Related Documents











