MICROBIAL DRUG RESISTANCE Volume 4, Number 3, 1998 Mary Ann Liebert, Inc. Predominance of the Multiresistant 23F International Clone of Streptococcus pneumoniae among Isolates from Mexico GABRIELA ECHANIZ-AVILES,* MARIA ELENA VELAZQUEZ-MEZA,* MARIA NOEMÍ CARNALLA-BARAJAS,* ARACELI SOTO-NOGUERÓN,* JOSÉ LUIS DI FABIO,| FORTINO SOLÓRZANO-SANTOS,$ YOLANDA JIMÉNEZ-TAPIA,§ and ALEXANDER TOMASA ABSTRACT During a surveillance study to determine the relative prevalence of capsular types of Streptococcus pneumo- niae and antimicrobial susceptibility of invasive isolates in children <5 years old in Mexico City, 220 isolates were collected. The serotype 23F was the most common found, followed by types 6A + B, 14, 19F, and 19A. Diminished susceptibility to penicillin was detected in 106 isolates (48.2%), and high penicillin resistance was found in 49 strains (22.2%), 31 belonging to type 23F. Resistance was also observed to erythromycin (13.1%), to chloramphenicol (43.1%), and to cefotaxime (10.9%). No strains were resistant to ofloxacin or vancomycin. Forty-four of the highly penicillin resistant isolates (penicillin MIC &2.0 /ng/ml) were examined with molec- ular fingerprinting techniques; 29 (65.9%) of these isolates (all except two strains) were serotype 23F and shared subtype variants of PFGE type A characteristic of the internationally spread Spanish/USA clone of S. pneumoniae. These strains were also resistant to trimethoprim/sulfametoxasole (TMP/SMX), chlorampheni- col, and tetracycline, and most of them were susceptible to erythromycin. Another 6 of the highly penicillin- resistant strains (serogroups 9 and 14) showed PFGE fingerprints and antimicrobial susceptibility pattern characteristic of a second internationally spread clone (French/Spanish clone) and carried resistance to peni- cillin and TMP/SMX. The rest of the 9 penicillin-resistant isolates were represented by 7 distinct additional PFGE types. The findings suggest that almost 80% of all highly penicillin resistant strains may have been "imported" into Mexico. INTRODUCTION Streptococcus pneumoniae is a common microorganism of the normal human respiratory flora and a major cause of human morbidity and mortality worldwide, causing more than 1 million deaths each year in children <5 years of age in the developing world.3 The emergence of pneumococcal strains re- sistant to penicillin and other antibiotics and the spread of re- sistant strains over the world have become a major concern for antimicrobial therapy of such infections and has required in- creased epidemiologic surveillance.8 Recently, several Latin American countries reported diminished penicillin susceptibil- ity of invasive pneumococcal strains, from 12% in Colombia to 40% in Uruguay.1,2,9 In Mexico we reported 48.2% of pneu- mococcal strains with diminished susceptibility to penicillin from children <5 years of age.7 Resistance to penicillin in S. pneumoniae is due to the ex- pression of altered high molecular-weight penicillin-binding proteins (PBPs) that have reduced antibiotic affinity.22 Among resistant strains, alterations in four (1 A, 2X, 2A, and 2B) of the five high molecular-weight PBPs expressed by isolates of the species have been identified in resistant patient isolates.4,11,22 Research has shown that two processes have contributed to the rise of these organisms. First, many distinct susceptible strains *Instituto Nacional de Salud Pública, Cuernavaca, Mor., México. tPan American Health Organization, Washington, DC. ^Hospital de Pediatría, Centro Médico Nacional Siglo XXI, México. §Hospital Infantil de Mexico, SS, México. IlThe Rockefeller University, New York, NY 10021. 241

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MICROBIAL DRUG RESISTANCEVolume 4, Number 3, 1998Mary Ann Liebert, Inc.
Predominance of the Multiresistant 23F International Clone ofStreptococcus pneumoniae among Isolates from Mexico
GABRIELA ECHANIZ-AVILES,* MARIA ELENA VELAZQUEZ-MEZA,*MARIA NOEMÍ CARNALLA-BARAJAS,* ARACELI SOTO-NOGUERÓN,* JOSÉ LUIS DI FABIO,|FORTINO SOLÓRZANO-SANTOS,$ YOLANDA JIMÉNEZ-TAPIA,§ and ALEXANDER TOMASA
ABSTRACT
During a surveillance study to determine the relative prevalence of capsular types of Streptococcus pneumo-niae and antimicrobial susceptibility of invasive isolates in children <5 years old in Mexico City, 220 isolateswere collected. The serotype 23F was the most common found, followed by types 6A + B, 14, 19F, and 19A.Diminished susceptibility to penicillin was detected in 106 isolates (48.2%), and high penicillin resistance was
found in 49 strains (22.2%), 31 belonging to type 23F. Resistance was also observed to erythromycin (13.1%),to chloramphenicol (43.1%), and to cefotaxime (10.9%). No strains were resistant to ofloxacin or vancomycin.Forty-four of the highly penicillin resistant isolates (penicillin MIC &2.0 /ng/ml) were examined with molec-ular fingerprinting techniques; 29 (65.9%) of these isolates (all except two strains) were serotype 23F andshared subtype variants of PFGE type A characteristic of the internationally spread Spanish/USA clone of S.pneumoniae. These strains were also resistant to trimethoprim/sulfametoxasole (TMP/SMX), chlorampheni-col, and tetracycline, and most of them were susceptible to erythromycin. Another 6 of the highly penicillin-resistant strains (serogroups 9 and 14) showed PFGE fingerprints and antimicrobial susceptibility patterncharacteristic of a second internationally spread clone (French/Spanish clone) and carried resistance to peni-cillin and TMP/SMX. The rest of the 9 penicillin-resistant isolates were represented by 7 distinct additionalPFGE types. The findings suggest that almost 80% of all highly penicillin resistant strains may have been"imported" into Mexico.
INTRODUCTION
Streptococcus pneumoniae is a common microorganism ofthe normal human respiratory flora and a major cause of
human morbidity and mortality worldwide, causing more than1 million deaths each year in children <5 years of age in thedeveloping world.3 The emergence of pneumococcal strains re-
sistant to penicillin and other antibiotics and the spread of re-sistant strains over the world have become a major concern forantimicrobial therapy of such infections and has required in-creased epidemiologic surveillance.8 Recently, several LatinAmerican countries reported diminished penicillin susceptibil-
ity of invasive pneumococcal strains, from 12% in Colombiato 40% in Uruguay.1,2,9 In Mexico we reported 48.2% of pneu-mococcal strains with diminished susceptibility to penicillinfrom children <5 years of age.7
Resistance to penicillin in S. pneumoniae is due to the ex-
pression of altered high molecular-weight penicillin-bindingproteins (PBPs) that have reduced antibiotic affinity.22 Amongresistant strains, alterations in four (1A, 2X, 2A, and 2B) of thefive high molecular-weight PBPs expressed by isolates of thespecies have been identified in resistant patient isolates.4,11,22Research has shown that two processes have contributed to therise of these organisms. First, many distinct susceptible strains
*Instituto Nacional de Salud Pública, Cuernavaca, Mor., México.tPan American Health Organization, Washington, DC.^Hospital de Pediatría, Centro Médico Nacional Siglo XXI, México.§Hospital Infantil de Mexico, SS, México.IlThe Rockefeller University, New York, NY 10021.
241

242 ECHÁNIZ-AVILES ET AL.
are independently evolving to the resistance phenotype. The ac-
quisition of PBP gene segments from foreign donors, such as
oral streptococci, is apparently a primary driving force.6 At themolecular level, the result is generation of mosaic genes andremodeled PBP proteins with decreased affinity for penicillin.5The importance of rapid local clonal spread of antibiotic-resis-tant S. pneumoniae is illustrated by events in Iceland, wherenow more than 20% of their isolates are resistant to penicillin.18Investigations of the molecular population genetics of pneu-mococci has led to the realization that horizontal transfer andrecombination processes are also serving to generate variationsin capsule type, which can have serious consequences with re-
gard to the outcome of the current vaccines strategy, which fo-cuses entirely on the use of capsular polysaccharides repre-senting a restricted number of capsular types.8,!7
Considering the scarcity of information regarding the mole-cular population genetics of pneumococci in our country, weutilized PFGE following Smal restriction digestion of chromo-somal DNA to conduct a molecular analysis of penicillin-re-sistant invasive S. pneumoniae strains. These strains were iso-lated between 1993 and 1995 from children attending two
pédiatrie hospitals in Mexico City, during a surveillance studyto determine the relative prevalence of pneumococcal capsulartypes within the Regional Vaccine System (SIREVA). We alsocompared the strains to S. pneumoniae international clones fromdifferent parts of the world to determine their genetic relation-ships.
MATERIALS AND METHODS
Bacterial strains
We studied a sample of 44 highly penicillin-resistant pneu-mococcal strains (minimal inhibitory concentration MIC >2pglml) recovered from 1993 to 1995 from normally sterile sitesof children <5 years of age from two pédiatrie hospitals inMexico City. Typing was done by the capsular reaction withpooled, type, or group antisera from Statens Seruminstitut,Copenhagen, Denmark. Susceptibility testing was done inMueller-Hinton broth supplemented with 3% lysed horse bloodby the broth microdilution method recommended by the Na-tional Committee for Clinical Laboratory Standards (NCCLS)15for penicillin, cefotaxime, chloramphenicol, erythromycin, van-comycin, and trimethoprim-sulfamethoxazole (TMP/SMX).Disc diffusion was used for tetracycline, clindamycin, andofloxacin.
Clinical isolates of penicillin-resistant S. pneumoniae fromdifferent parts of the world were from the strain collection atThe Rockefeller University, USA, and from C. Brandileone, In-stituto Adolfo Lutz, Brazil. A penicillin-susceptible S. pneu-moniae laboratory strain X was used in this study as reference.Quality control for typing and antimicrobial susceptibility ofthe broth microdilution method was performed at the CanadianNational Centre for Streptococcus, Edmonton, Alberta.
Preparation of chromosomal DNA for pulsed-field gelelectrophoresis (PFGE)
The method used was modified from a previously publishedprocedure19 and was done in the Laboratory of Microbiology
at The Rockefeller University in New York. Strains were grownin a synthetic medium, supplemented with yeast extract (0.1%w/v final concentration; Difco, Detroit, MI) without aeration at37°C. Growth was monitored by determination of optical den-sity (OD62o). A 6-ml overnight culture of pneumococci was pel-leted, washed with 1 ml of buffer (10 mM Tris, pH 8.0, IMNaCl, or 50 mM potassium phosphate, pH 8.0), and resus-
pended into 200 pi of the same buffer. Cell concentrations were
adjusted to an A62o of 5.0. This cell suspension was then di-luted 1:1 with 100 pi of 1.5% low-gelling-temperature agarose(Sea Plaque, FMC Bioproducts, Rockland, ME) in buffer; disksof 20 ¿d were allowed to solidify for 5 min at
—
20°C. The cellswere lysed by incubation of the disks at 37°C for 3 h with 50pg of RNase I in 1 ml of buffer (6 mM Tris, pH 8.0, 1 M NaCl,0.1 M EDTA, pH 8.0) and a mixture of 0.2% sodium deoxy-cholate, 0.5% Sarkosyl, 0.5% Brij 58. The disks were next in-cubated in a solution of proteinase K ( 1 mg/ml) in ES buffer(0.5 M EDTA, pH 9, and 1% Sarkosyl) at 50°C for 17 h. Theagarose disks were washed three times in 13 ml of TE buffer(10 mM Tris and 1 mM EDTA, pH 7.5) for 1 h with gentle ag-itation. The DNA fixed in the agarose disk was preincubatedin 1 ml of restriction buffer (6 mM Tris, pH 8.0, 20 mM KC1,6 mM MgCl2, and 6 mM 2-mercaptoethanol) at 25°C for 30min. Restriction continued for 18 h in 40 pi of restriction buffercontaining bovine serum albumin (250 pglml) and Smal (12units). The reaction was stopped with 10 pi of ES buffer and5 (A of loading buffer.
Pulsed-field gel electrophoresisThe gels were prepared following the methods described in
previous publications.18 A CHEF-DRII apparatus (Bio-Rad)was used to run the gels. The running conditions were as fol-lows: 23 h at 14°C in 0.5 X TBE buffer; the voltage was set at200 V, ramped with initial forward time 1 s, final forward time30 s. The gels were stained with ethidium bromide.
Analysis of DNA relatedness
Similarity of the strains was determined by visual compari-son of macrorestriction patterns as a means of quantifying therelatedness or lack thereof among the isolates. Because a sin-gle base mutation in the chromosomal DNA is sufficient to in-troduce a difference of three fragments in its restriction pattern,isolates with restriction patterns showing a one-to-six fragmentdifference were considered to belong to a common major re-striction type.21
RESULTS
Serotypes and antimicrobial susceptibilitiesOf the 44 pneumococcal penicillin-resistant isolates studied
from two pédiatrie hospitals in Mexico City, the great major-ity of strains, 30 (68.1%), belonged to serotype 23F, 4 (9%) toserotype 19F, 4 (9%) to serotype 9A, 3 (6.8%) to type 14, andone each to types 6A, 6B, and 9V. Thirty-three (75%) strainsshowed a decreased susceptibility also for the third-generationcephalosporin cefotaxime with strains in the intermediate andresistant category. Thirty-eight (86.4%) strains were resistant

RESISTANT PNEUMOCOCCI IN MEXICO 243
Table 1. Properties of Streptococcus pneumoniae Isolates from Mexico
Strain SerotypeMIC fig/mlPenicillin
MIC pig/mlCefotaxime
Smalpattern
Suscep., Interm. or Resist.CM Ery Cli TMP/SMX Tet Ofl Van
23 C9 H109 H122 H35 C36 C67 H76 H107 H43 C44C63 C66 C35 H46 H132 H11 C13 H85 H102 H68 CI H31 HII H22 C58 H61 C60 C13 C
23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F23F146B
444444222222284484442488S4448
2112440.0311110.030.0322220.03120.0312221121
AlA2A2A2A2A2A2A2A2A2A2A2A2A3A3A4A5A5A5A5A6A7A8A9A9A9A10A12A13
RRRRRRRRRRRRRRRRRRRRRRRRRRRRR
SSsssssRSSssssSssSssS1ssssRRs
RR
RRRRRRRRRRRRRRRRRRRRRRRRRRRRR
RRRRRRRRRRRRRRRRRRRRRRRRRRRRR
82 H24 H108 H38 C15 H58 C
9A9A9A9A9A14
422244
0.0321211
BlBlBlBlBllB12
SSSsss
sssssR
RRRRRR
21 H18 H
23F23F
0.030.0015
CC
RR
12 C
99 H
65 C
23F
14
6A
2
2
2
1
1
0.03
D
E
F
S
S
R
S
S
s
s
R
s
62 H20 C
19F19F
0.51
GG
RI
80 H
22 H
19F
19F
0.25
2
H
I
S
s
12 3 4 5 6 7 8 9 10 1112 131415161718 19 20212223
97.0 —
48.5 —
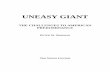
FIG. 1. Predominance of the multiresistant 23F clone of S. pneumoniae among isolates from Mexico. Chromosomal DNA re-
stricted by Smal was separated by PFGE. Lanes 1, 23: lambda ladder marker. Lane 14: low molecular weight marker. Lane 2:penicillin-susceptible laboratory strain X. Lanes 3, 6: strain Clev-2 (reference strain for International Clone A). Lane 4: strainH67. Lane 5: strain H76. Lane 7: strain H85. Lane 8: strain H102. Lane 9: strain H107. Lane 10: strain H109. Lane 11: strainHI. Lane 12: strain H9. Lane 13: strain H13. Lane 15: strain H122. Lane 16: strain H132. Lane 17: strain Cll. Lane 18: strainC22. Lane 19: strain C35. Lane 20: strain C36. Lane 21: strain C63. Lane 22: strain C66.
12 3 4 5 6 7 8 9 10111213141516171819 20212223
388.0_339.5—
292.0 —
242.5 —
194.0 —
145.5 —
97.0 —
48.5 —
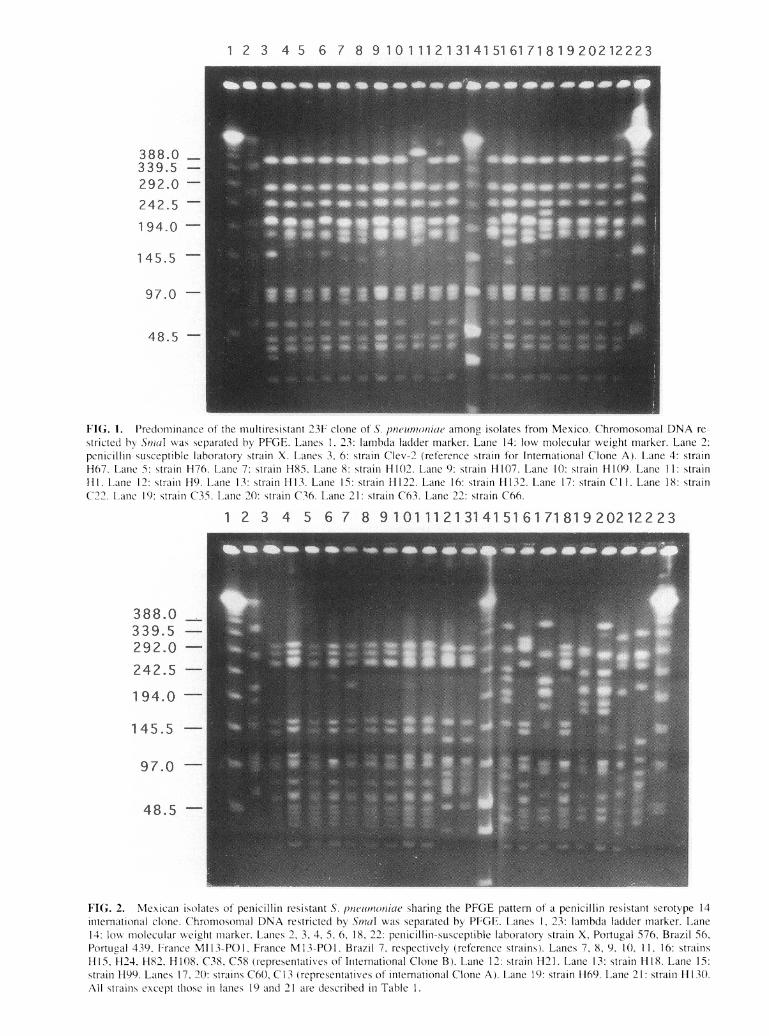
FIG. 2. Mexican isolates of penicillin resistant S. pneumoniae sharing the PFGE pattern of a penicillin resistant serotype 14international clone. Chromosomal DNA restricted by Smal was separated by PFGE. Lanes 1, 23: lambda ladder marker. Lane14: low molecular weight marker. Lanes 2, 3, 4, 5, 6, 18, 22: penicillin-susceptible laboratory strain X, Portugal 576, Brazil 56,Portugal 439, France MI13-P01, France M13-P01, Brazil 7, respectively (reference strains). Lanes 7, 8, 9, 10, 11, 16: strainsH15, H24, H82, H108, C38, C58 (representatives of International Clone B). Lane 12: strain H21. Lane 13: strain H18. Lane 15:strain H99. Lanes 17, 20: strains C60, C13 (representatives of international Clone A). Lane 19: strain H69. Lane 21: strain H130.All strains except those in lanes 19 and 21 are described in Table 1.

RESISTANT PNEUMOCOCCI IN MEXICO 245
to TMP/SMX, and 29 (65.9%) were resistant to chlorampheni-col. Most 23F strains showed multiresistance. Table 1 summa-
rizes the relevant properties of the clinical isolates examined,including serotypes, antibiotic resistance MICs and resistance,levels and the assignment for PFGE patterns as determined af-ter Smal digestion of chromosomal DNA preparations followedby separation in contour-clamped electrophoresis.
PFGE patternsFigure 1 shows PFGE profiles of chromosomal DNA iso-
lated from a group of 23F strains, all sharing variants of PFGEtype A, comparing them with strain Cleveland-2 (Clev-2),which is the reference strain for international Spanish/USAClone A. Figure 2 shows 6 of the highly penicillin resistantstrains (serogroups 9 and 14) showing PFGE type B character-istic of a second internationally spread clone (French/Spanishclone), which carried resistance to penicillin, cefotaxime (allexcept one strain) and TMP/SMX and are compared with a
strain from Brazil and another one from Portugal, both ofserotype 14 and the same clonal type (PFGE pattern B). Twoisolates, 60C and 13C, shared the PFGE pattern of internationalclone A but belonged to serotypes 14 and 6B, respectively. Therest of the penicillin resistant isolates were represented by 7 dis-tinct additional PFGE types.
DISCUSSION
The most interesting feature of the collection of highly peni-cillin-resistant S. pneumoniae isolates studied from two pédi-atrie hospitals in Mexico City is the predominance of the mul-tiresistant capsular type 23F clone. These isolates not onlyshared the common capsular type but also shared similar MICvalues for penicillin, cefotaxime, chloramphenicol, tetracycline,and TMP/SMX. All except 6 were susceptible to erythromycin,and 3 showed resistance to clindamycin. All were susceptibleto vancomycin and ofloxacin. Several examples of the interna-tional spread of this resistant pneumococcal clone have beenreported. In 1991, Muñoz et al. first reported evidence for theintercontinental spread of the multiresistant clone of S. pneu-moniae type 23F from Spain to the United States.14 This clonesubsequently disseminated throughout the United States13 andhas been reported in many countries.10,12,19,20 It has been pre-sent in Mexico since 1992 (Brian Spratt, personal communica-tion), and considering our results, at least in these two hospi-tals, it still represents the majority of pneumococcal strainscausing invasive disease in small children. Two strains shownin Fig. 2, 60C and 13C, lanes 17 and 20 respectively, share a
very similar multiresistance pattern and PFGE type (PFGE typeA) but have different serotypes 14 and 6B, respectively. An-other 6 of the highly penicillin-resistant strains (serogroups 9and 14) showed PFGE fingerprints and resistant phenotypecharacteristic of a second internationally spread clone(French/Spanish clone B) and carried resistance to penicillinand TMP/SMX. They were very similar compared with strainBr 56 from Brazil (serotype 14) and strains 576 and 439 fromPortugal. Identification of the DNA fingerprints of the PBPgenes in these bacteria through PCR amplification and deter-mination of restriction fragmentation length polymorphism
should help clarify the nature of these isolates and possibletransformation of capsules.16
An overall 79.5% of highly penicillin-resistant pneumococ-cal isolates recovered from two pédiatrie hospitals in MexicoCity shared PFGE with two internationally spread clones thathave become established in parts of Europe, the U.S., the U.K.,South Africa, and now Mexico. This clearly suggests that thespread of unique highly resistant clones is contributing to theemergence of resistant in most parts of the world.
The detection and the reduction of transmission of drug-re-sistant pneumococci that are currently spreading rapidly all overthe world will be a major task for pneumococcal control strate-gies. In this respect, the restrictive use of antibiotics remainsthe major defense against the epidemic dissemination of suchstrains, particularly in countries like Mexico, where antibioticsare easily sold over the counter. In addition, the emergence ofmultidrug-resistant penumococci increases the need for vacci-nation of patients at risk for pneumococcal disease, such as theelderly, and the need to improve conjugate vaccines to effi-ciently protect young children.
ACKNOWLEDGMENTS
We are grateful to Elena Severina, Laboratory of Microbi-ology, The Rockefeller University, New York, for help with thePFGE technique, and the staffs of the Bacteriology Laboratoryat the Hospital Infantil de México and Hospital de Pediatría,Centro Médico Nacional, for participating in the surveillanceprogram. These studies received partial support from a grant ofthe U.S. Public Health Service, ROI AI37275, and from theCEM/NET Initiative.
REFERENCES
1. Casteñeda, E., A.L. Leal, O. Castillo, F. De La Hoz, M.C. Vela,M. Arango, H. Trujillo, A. Levy, M.E. Gama, M. Calle,M.L. Valencia, W. Parra, N. Agudelo, G.I. Mejía, S. Jaramillo,F. Montoya, I.L. Porras, A. Sánchez, D. Saa, J.L. Di Fabio,A. Homma, and the Pneumococcal Study Group in Colombia.1997. Distribution of capsular types and antimicrobial susceptibil-ity of invasive isolates of Streptococcus pneumoniae in Colombianchildren. Microb. Drug Resist. 3:147-152.
2. De Cunto-Brandileone, M.C, V.S. Dias Vieira, S. TadeuCasagrande, R. Cobo Zanella, M. Leopoldo Silva Guerra,S. Bokermann, J. Cássio De Moraes, E.R. Baldacci, C.B. Cha-mone, M.A.A. Oliveira, D.G. Cavalcanti De Matos, T.M. CatâoArruda, M. Ferreira Da Costa Coelho, S. MachadoD'Avila, A.R. Dos Santos, J.L. Di Fabio, and the Pneumococ-cal Study Group in Brazil for the SIREVA Project. 1997. Preva-lence of serotypes and antimicrobial resistance of Streptococcuspneumoniae strains isolated from Brazilian children with invasiveinfections. Microb. Drug Resist. 3:141-146.
3. Di Fabio, J.L., A. Homma, and C. De Quadros. 1997. Pan Amer-ican Health Organization Epidemiological Surveillance Networkfor Streptococcus pneumoniae. Microb. Drug Resist. 3:131-133.
4. Dowson, CG., A. Hutchison, and B.G. Spratt. 1989. Extensiveremodelling of the transpeptidase domain of penicillin-binding pro-tein 2B of a penicillin-resistant South African isolate of Strepto-coccus pneumoniae. Mol. Microbiol. 3:95-102.
5. Dowson, CG., T.J. Coffey, and B.G. Spratt. 1994. Origin and

246 ECHANIZ-AVILES ET AL.
molecular epidemiology of penicillin-binding protein mediated re-
sistance to /3-lactam antibiotics. Trends Microbiol. 2:361-366.6. Dowson, CG., T.J. Coffey, C. Kell, and R.A. Whiley. 1993. Evo-
lution of penicillin resistance in Streptococcus pneumoniae: Therole of Streptococcus mitis in the formation of a low affinity PBP2Bin S. pneumoniae. Mol. Microbiol. 9:635-643.
7. Echániz-Aviles, G. M.E. Velazquez, M.N. Carnalla, A. Soto, F.Solórzano, A. Pérez, R. Gatica, and J.L. Di Fabio. 1997. An-timicrobial susceptibilities and capsular types of invasive Strepto-coccus pneumoniae isolated in children in Mexico City. Microb.Drug Resist. 3:153-157.
8. Hermans, P.W.M., M. Sluijter, S. Dejsirilert, N. Lemmens, K.Elzenaar, A. Van Veen, W.H.F. Goessens, and R. De Groot.1997. Molecular epidemiology of drug-resistant pneumococci: To-ward and international approach. Microb. Drug Resist. 3:243-251.
9. Hortal, M., and the Pneumococcus Study Group. 1997. Capsu-lar type distribution and susceptibility to antibiotics of Streptococ-cus pneumoniae clinical strains isolated from Uruguayan childrenwith systemic infections. Microb. Drug Resist. 3:159-163.
10. Klugman, K.P., T.J. Coffey, A. Smith, A. Wasas, M. Myers,and B.G. Spratt. 1994. Cluster of an erythromycin-resistant vari-ant of the Spanish multiply resistant 23F clone of Streptococcuspneumoniae in South Africa. Eur. J. Clin. Microbiol. 13:171-174.
11. Laible, G., B.G. Spratt, and R. Hakenbeck. 1991. Interspeciesrecombinational events during the evolution of altered PBP 2Xgenes in penicillin-resistant clinical isolates of Streptococcus pneu-moniae. Mol. Microbiol. 5:1993-2002.
12. Lefevre, J.C., M.A. Bertrand, and G. Faucon. 1995. Molecularanalysis by pulsed-field gel electrophoresis of penicillin-resistantStreptococcuspneumoniae from Toulouse, France. Eur. J. Clin. Mi-crobiol. Infect. Dis. 14:491^*97.
13. McDougal, L.K., R. Facklam, M. Reeves, S. Hunter, J.M. Swen-son, B.C. Hill, and F.C. Tenover. 1992. Analysis of multiply an-
timicrobial-resistance isolates of Streptococcus pneumoniae fromthe United States. Antimicrob. Agents Chemother. 36:2176-2184.
14. Muñoz, R., T.J. Coffey, M. Daniels, CG. Dowson, G. Laible,J. Casai, R. Hakenbeck, M. Jacobs, J.M. Musser, B.G. Spratt,and A. Tomasz. 1991. Intercontinental spread of a multiresistantclone of serotype 23F Streptococcus pneumoniae. I. Infect. Dis.164:302-306.
15. National Committee for Clinical Laboratory Standards. 1995.Methods for dilution antimicrobial susceptibility tests for bacteria
that grow aerobically: Approved Standard M7-A3, 3rd The Na-tional Committee for Clinical Laboratory Standards, Villanova, PA.
16. Nesin, M., M. Ramirez, and A. Tomasz. 1988. Capsular trans-formation ofmultidrug resistant Streptococcus pneumoniae in vivo.I. Infect. Dis. 177:707-713.
17. Sniadack, D.H., B. Schwartz, H. Lipman, J. Bogaerts, J.C.Butler, R. Dagan, G. Echaniz-Aviles, N. Lloyd-Evans, A.Fenoll, N.I. Girgis, J. Henrichsen, K. Klugman, D. Lehmann,A.K. Takala, J. Vanderpitte, S. Gove, and R.F. Breiman. 1995.Potential interventions for the prevention of childhood pneumo-nia: Geographic and temporal differences in serotype andserogroup distribution of sterile site pneumococcal isolates fromchildren—implications for vaccine strategies. Pediatr. Infect. Dis.I. 14:503-510.
18. Soares, S., K.G. Kristinsson, J.M. Musser, and A. Tomasz.1993. Evidence for the introduction of a multiresistant clone ofserotype 6B Streptococcus pneumoniae from Spain to Iceland inthe late 1980s. I. Infect. Dis. 168:158-163.
19. Tarasi, A., N. Sterk-Kuzmanovic, K. Sieradzki, S. Schoenwald,R. Austrian, and A. Tomasz. 1995. Penicillin-resistant and mul-tidrug-resistant Streptococcus pneumoniae in a pédiatrie hospitalin Zagreb, Croatia. Microb. Drug Resist. 1:169-176.
20. Tarasi, A., Y. Chong, K. Lee, and A. Tomasz. 1997. Spread ofthe serotype 23F multidrug-resistant Streptococcus pneumoniaeclone to South Korea. Microb. Drug Resist. 3:105-109.
21. Tenover, F.C, R.D. Arbeit, R.V. Goering, P.A. Mickelsen, B.E.Murray, D.H. Persing, and B. Swaminathan. 1995. Interpretingchromosomal DNA restriction patterns produced by pulsed-fieldgel electrophoresis: criteria for bacterial strain typing. I. Clin. Mi-crobiol. 33:2233-2239.
22. Zighelboim, S., and A. Tomasz. 1980. Penicillin-binding proteinsof the multiply antibiotic-resistant South African strains of Strep-tococcus pneumoniae. Antimicrob. Agents Chemother. 17:434—442.
Address reprint requests to:Gabriela Echániz-Aviles
Instituto Nacional de Salud PúblicaAv. Universidad 655
Colonia Sta. María AhuacatitlánCuernavaca, Morelos, México 62508

This article has been cited by:
1. Gabriela Echaniz-Aviles, Araceli Soto-Nogueron, Guadalupe Miranda-Novales, Maria N. Carnalla-Barajas, Maria ElenaVelazquez-Meza, Fortino Solórzano-Santos. 2015. Streptococcus pneumoniae Serotypes Identified in Mexican Childrenwith Invasive Disease before and After the Introduction of PCV7 (1993–2012). Archives of Medical Research . [CrossRef]
2. Christopher Gerard Dowson, Krzysztof TrzcinskiEvolution and Epidemiology of Antibiotic-Resistant Pneumococci229-254. [CrossRef]
3. F Quiñones-Falconi. 2004. Antimicrobial susceptibility patterns of Streptococcus pneumoniae in Mexico. DiagnosticMicrobiology and Infectious Disease 49, 53-58. [CrossRef]
4. Mariana Castanheira, Ronald N. Jones, Suzane Silbert, Maria C.C. Brandileone, Hélio S. Sader. 2003. Typing andMolecular Characterization of Streptococcus pneumoniae with Reduced Susceptibility to Cefotaxime Isolated in LatinAmerica. Microbial Drug Resistance 9:4, 345-351. [Abstract] [Full Text PDF] [Full Text PDF with Links]
5. Anna Skoczyńska, Waleria Hryniewicz. 2003. Genetic Relatedness, Antibiotic Susceptibility, and Serotype Distributionof Streptococcus pneumoniae Responsible for Meningitis in Poland, 1997-2001. Microbial Drug Resistance 9:2, 175-182.[Abstract] [Full Text PDF] [Full Text PDF with Links]
6. M. Hortal, M. Lovgren, F. de la Hoz, C.I. Agudelo, M.C. Brandileone, T. Camou, S. Casagrande, E. Castañeda, A. Corso,G. Echaniz, J.C. Hormazabal, J. Pace, R. Palacio, G. Perez-Giffoni, R. Ruvinsky, J.L. Di Fabio. 2001. Antibiotic Resistancein Streptococcus pneumoniae in Six Latin American Countries: 1993-1999 Surveillance. Microbial Drug Resistance 7:4,391-401. [Abstract] [Full Text PDF] [Full Text PDF with Links]
7. José LUIS Di Fabio, Elizabeth Castañeda, Clara Inés Agudelo, Fernando De La Hoz, María Hortal, Teresa Camou,Gabriela Echániz-Avilés, María Noemi Carnalla Barajas, Ingrid Heitmann, Juan Carlos Hormazabal, Maria Cristina C.Brandileone, Vera Simonsen Dias Vieira, Mabel Regueira, Raúl Ruvinski, Alejandra Corso, Marguerite Lovgren, JamesA. Talbot, Ciro De Quadros. 2001. Evolution of S treptococcus pneumoniae serotypes and penicillin susceptibility inLatin America, Sireva-Vigía Group, 1993 to 1999. The Pediatric Infectious Disease Journal 20, 959-967. [CrossRef]
8. María Claudia Vela, Nacxiry Fonseca, José Luis Di Fabio, Elizabeth Castañeda. 2001. Presence of InternationalMultiresistant Clones of Streptococcus pneumoniae in Colombia. Microbial Drug Resistance 7:2, 153-164. [Abstract][Full Text PDF] [Full Text PDF with Links]
9. G. H. McCracken. 2000. Pharmacodynamics of Gatifloxacin in Experimental Models of Pneumococcal Meningitis.Clinical Infectious Diseases 31, S45-S50. [CrossRef]
10. Anders Håkansson, Malin Svensson, Ann-Kristin Mossberg, Hemant Sabharwal, Sara Linse, Irene Lazou, Bo Lönnerdal,Catharina Svanborg. 2000. A folding variant of α-lactalbumin with bactericidal activity against Streptococcus pneumoniae.Molecular Microbiology 35, 589-600. [CrossRef]
11. Alberto Villaseñor-Sierra, José Ignacio, Santos Preciado. 1999. Otitis media today: a challenge for physicians and thecommunity. Current Opinion in Infectious Diseases 12, 205-212. [CrossRef]
12. 1999. Acquisition of New Capsular Genes Among Clinical Isolates of Antibiotic-Resistant Streptococcus pneumoniae.Microbial Drug Resistance 5:4, 241-246. [Abstract] [Full Text PDF] [Full Text PDF with Links]
13. 1998. Molecular Characterization of Penicillin-Resistant Streptococcus pneumoniae Isolates Causing Respiratory Diseasein the United States. Microbial Drug Resistance 4:4, 325-337. [Abstract] [Full Text PDF] [Full Text PDF with Links]
Related Documents