Predictors of outcome in Internet-based cognitive behavior therapy for severe health anxiety Erik Hedman a, b, c, * , Nils Lindefors a , Gerhard Andersson a, d , Erik Andersson a , Mats Lekander b, e , Christian Rück a , Brjánn Ljótsson a, c a Department of Clinical Neuroscience, Division of Psychiatry, Karolinska Institutet, Retzius väg 8, SE-171 77 Stockholm, Sweden b Department of Clinical Neuroscience, Osher Center for Integrative Medicine, Karolinska Institutet, Stockholm, Sweden c Department of Clinical Neuroscience, Division of Psychology, Karolinska Institutet, Stockholm, Sweden d Department of Behavioural Sciences and Learning, Swedish Institute for Disability Research, Linköping University, Linköping, Sweden e Stress Research Institute, Stockholm University, Stockholm, Sweden article info Article history: Received 17 April 2013 Received in revised form 30 July 2013 Accepted 30 July 2013 Keywords: Severe health anxiety Predictors Cognitive behavior therapy Internet abstract Internet-based cognitive behavior therapy (CBT) for severe health anxiety can be effective, but not all patients achieve full remission. Under these circumstances, knowledge about predictors is essential for the clinician in order to make reliable treatment recommendations. The primary aim of this study was to investigate clinical, demographic, and therapy process-related predictors of Internet-based CBT for se- vere health anxiety. We performed three types of analyses on data from a sample comprising partici- pants (N ¼ 81) who had received Internet-based CBT in a randomized controlled trial. Outcomes were a) end state health anxiety, b) improvement in health anxiety (continuous change scores), and c) clinically significant improvement. Outcomes were assessed at six-month follow-up. The results showed that the most stable predictors of both end state health anxiety and improvement were baseline health anxiety and depressive symptoms. Treatment adherence, i.e. the number of completed treatment modules, also significantly predicted outcome. Notably, health anxiety at baseline was positively associated with symptom improvement while depressive symptoms was negatively related to improvement. De- mographic factors were largely without significant impact on end state symptoms or improvement. We conclude that baseline symptom burden and adherence to treatment have strong predictive effects in Internet-based CBT for severe health anxiety. Ó 2013 Elsevier Ltd. All rights reserved. Introduction The main feature of severe health anxiety, or hypochondriasis according to DSM-IV, is a persistent fear of serious illness based on misinterpretation of bodily symptoms (American Psychiatric Association, 2000). Although severe health anxiety was not long ago considered a disorder highly difficult to treat, cognitive behavior therapy (CBT) has been found to be effective in reducing health anxiety (Clark et al., 1998; Greeven et al., 2007; Seivewright et al., 2008; Sorensen, Birket-Smith, Wattar, Buemann, & Sal- kovskis, 2011; Speckens et al., 1995; Thomson & Page, 2007; Warwick, Clark, Cobb, & Salkovskis, 1996). In a recently published study of CBT delivered via the Internet for severe health anxiety, we showed that this could be an effective treatment yielding effect sizes at par with conventional CBT (Hedman et al., 2011). Internet- based CBT has several advantages, one of the most important being that it can be used to increase availability to psychological treatments. Although generally effective, there is considerable inter- individual variance in outcome and at least one-third of patients with severe health anxiety do no respond sufficiently well to CBT regardless if delivered in a conventional format or via the Internet (Buwalda, Bouman, & van Duijn, 2007; Hedman et al., 2011). Under these circumstances investigation of predictors of treatment outcome is important as the information obtained could be used to lessen the proportion of treatment failures, and to inform the clinician about which treatment to recommend for whom (Keijsers, Hoogduin, & Schaap, 1994; Kraemer, Wilson, Fairburn, & Agras, * Corresponding author. Department of Clinical Neuroscience, Karolinska Insti- tutet, Retzius väg 8, SE-17177 Stockholm, Sweden. Tel.: þ46 484 26 29; fax: þ46 8 779 54 16. E-mail address: [email protected] (E. Hedman). Contents lists available at ScienceDirect Behaviour Research and Therapy journal homepage: www.elsevier.com/locate/brat 0005-7967/$ e see front matter Ó 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.brat.2013.07.009 Behaviour Research and Therapy 51 (2013) 711e717

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

lable at ScienceDirect
Behaviour Research and Therapy 51 (2013) 711e717
Contents lists avai
Behaviour Research and Therapy
journal homepage wwwelsevier comlocatebrat
Predictors of outcome in Internet-based cognitive behavior therapyfor severe health anxiety
Erik Hedman abc Nils Lindefors a Gerhard Andersson ad Erik Andersson aMats Lekander be Christian Ruumlck a Brjaacutenn Ljoacutetsson ac
aDepartment of Clinical Neuroscience Division of Psychiatry Karolinska Institutet Retzius vaumlg 8 SE-171 77 Stockholm SwedenbDepartment of Clinical Neuroscience Osher Center for Integrative Medicine Karolinska Institutet Stockholm SwedencDepartment of Clinical Neuroscience Division of Psychology Karolinska Institutet Stockholm SwedendDepartment of Behavioural Sciences and Learning Swedish Institute for Disability Research Linkoumlping University Linkoumlping Swedene Stress Research Institute Stockholm University Stockholm Sweden
a r t i c l e i n f o
Article historyReceived 17 April 2013Received in revised form30 July 2013Accepted 30 July 2013
KeywordsSevere health anxietyPredictorsCognitive behavior therapyInternet
Corresponding author Department of Clinical Netutet Retzius vaumlg 8 SE-171 77 Stockholm Sweden Te779 54 16
E-mail address kirehedmankise (E Hedman)
0005-7967$ e see front matter 2013 Elsevier Ltdhttpdxdoiorg101016jbrat201307009
a b s t r a c t
Internet-based cognitive behavior therapy (CBT) for severe health anxiety can be effective but not allpatients achieve full remission Under these circumstances knowledge about predictors is essential forthe clinician in order to make reliable treatment recommendations The primary aim of this study was toinvestigate clinical demographic and therapy process-related predictors of Internet-based CBT for se-vere health anxiety We performed three types of analyses on data from a sample comprising partici-pants (N frac14 81) who had received Internet-based CBT in a randomized controlled trial Outcomes were a)end state health anxiety b) improvement in health anxiety (continuous change scores) and c) clinicallysignificant improvement Outcomes were assessed at six-month follow-up The results showed that themost stable predictors of both end state health anxiety and improvement were baseline health anxietyand depressive symptoms Treatment adherence ie the number of completed treatment modules alsosignificantly predicted outcome Notably health anxiety at baseline was positively associated withsymptom improvement while depressive symptoms was negatively related to improvement De-mographic factors were largely without significant impact on end state symptoms or improvement Weconclude that baseline symptom burden and adherence to treatment have strong predictive effects inInternet-based CBT for severe health anxiety
2013 Elsevier Ltd All rights reserved
Introduction
The main feature of severe health anxiety or hypochondriasisaccording to DSM-IV is a persistent fear of serious illness based onmisinterpretation of bodily symptoms (American PsychiatricAssociation 2000) Although severe health anxiety was not longago considered a disorder highly difficult to treat cognitivebehavior therapy (CBT) has been found to be effective in reducinghealth anxiety (Clark et al 1998 Greeven et al 2007 Seivewrightet al 2008 Sorensen Birket-Smith Wattar Buemann amp Sal-kovskis 2011 Speckens et al 1995 Thomson amp Page 2007
uroscience Karolinska Insti-l thorn46 484 26 29 fax thorn46 8
All rights reserved
Warwick Clark Cobb amp Salkovskis 1996) In a recently publishedstudy of CBT delivered via the Internet for severe health anxiety weshowed that this could be an effective treatment yielding effectsizes at par with conventional CBT (Hedman et al 2011) Internet-based CBT has several advantages one of the most important beingthat it can be used to increase availability to psychologicaltreatments
Although generally effective there is considerable inter-individual variance in outcome and at least one-third of patientswith severe health anxiety do no respond sufficiently well to CBTregardless if delivered in a conventional format or via the Internet(Buwalda Bouman amp van Duijn 2007 Hedman et al 2011) Underthese circumstances investigation of predictors of treatmentoutcome is important as the information obtained could be used tolessen the proportion of treatment failures and to inform theclinician about which treatment to recommend for whom (KeijsersHoogduin amp Schaap 1994 Kraemer Wilson Fairburn amp Agras
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717712
2002) Predictor variables can broadly be classified into three cat-egories a) clinical characteristics ie variables related to the clin-ical disorder such as symptom levels b) demographic variables egage and gender and c) therapy process-related variables eg ex-pectancy of treatment outcome
Previous studies investigating predictors on conventional face-to-face CBT for severe health anxiety have demonstrated thatclinical characteristics associated with outcome are severity ofhealth anxiety general anxiety and negative cognitions regardingbodily symptoms (Buwalda amp Bouman 2008 Hiller Leibbrand Riefamp Fichter 2002 Nakao Shinozaki Ahern amp Barsky 2011) It seemshowever that these predictive clinical factors are mainly related tolevels of health anxiety after treatment ie persons with higherlevels of these symptoms at baseline tend to have more healthanxiety at post-treatment When it comes to predictors ofimprovement one fairly robust result seems to be that baselinehealth anxiety predicts larger improvement from baseline to post-treatment (Buwalda amp Bouman 2008 Nakao et al 2011) Thiscould be interpreted as higher initial symptom severity gives roomfor more improvement
As for demographic predictors no previous studies on CBT forhealth anxiety have demonstrated clear predictive effects In onestudy higher age was associated with less pre-to-post-treatmentgains (Buwalda amp Bouman 2008) but in two other reports nopredictive effect of age was found (Hiller et al 2002 Nakao et al2011) Following the same pattern of mixed results Nakao et al(2011) found that marital status predicted better outcome ie be-ing married was associated with larger improvements while therewas no such association in the study by Hiller et al (2002)
When it comes to therapy process-related factors publisheddata are scarce Buwalda and Bouman investigated the prognosticeffect of expectancy of treatment outcome but found no significantassociation with health anxiety reduction (Buwalda amp Bouman2008) In research on other anxiety disorders higher expectancyof treatment outcome has been shown to predict larger improve-ments (Chambless Tran amp Glass 1997 Hedman et al 2012Mausbach Moore Roesch Cardenas amp Patterson 2010) InInternet-based CBT for social anxiety disorder treatment adher-ence ie number of completed modules has been shown to predictbetter treatment outcomes (Hedman et al 2012 Nordgreen et al2012)
In sum based on the previous literature baseline health anxietyemerges as the only stable predictor of both end state health anx-iety and improvement in CBT for severe health anxiety To date nostudy has investigated predictors of Internet-based CBT for thispatient group Although the hypothesized therapeutic mechanismsare the same in Internet-based and conventional CBT there areimportant differences potentially influencing what factors thatpredict outcome These differences include that patients haveminimal therapist guidance and thus must take a larger re-sponsibility for learning how the treatment works and how toapply general therapeutic principles on their own idiosyncratichealth anxiety behaviors Other differences are that the Internet-based CBT requires basic computer skills and that the patientmust read lengthy fairly complex texts It could therefore be thatdemographic factors such as age computer skills and educationalbackground have a larger impact on outcome in Internet-basedCBT As treatment delivered via the Internet requires a highlyactive patient despite limited therapist guidance it could also bethat clinical factors related to passive coping such as comorbiddepressive symptoms have a larger negative predictive value inthis form of therapy compared to conventional CBT Prior researchon social anxiety disorder has shown that delivery format ieInternet or face-to-face can moderate the effect of predictors(Hedman et al 2012) Against this background it is highly
important to examine which factors that predict treatmentoutcome in Internet-based CBT for severe health anxiety
The main aim of this study was to investigate clinical de-mographic and therapy process-related predictors of treatmentoutcome both regarding end state and improvement in Internet-based CBT for severe health anxiety We hypothesized that morehealth anxiety at baseline would predict larger improvements butalso more health anxiety at six-month follow-up Due to the mixedresults in the literature in terms of demographic and therapy pro-cess factors the analyses in these domains were consideredexploratory The second aim of the study was to investigate pat-terns of change in health anxiety between end of treatment andlonger-term follow-up and predictors of this change
Methods
Study design
This was a study with a repeated measurements design inves-tigating predictors of outcome in a sample of participants (N frac14 81)who received treatment within the context of a previously pub-lished randomized controlled trial (RCT) (Hedman et al 2011) Inthe trial participants were randomized to ICBT (n frac14 40) or thecontrol condition (n frac14 41) As participants in the control conditionhad stable symptom levels during the initial 12 weeks and werecrossed over to treatment directly after the 12 weeks all random-ized participants were included in this study and no waiting listdata were used This meant that all predictor analyses were con-ducted using data from a sample that had received treatment andthat the distinction between the treatment condition and thecontrol condition in the original RCT is not relevant for the presentstudy All dependent variables were assessed at six-month follow-up and in the main analyses potential predictors were assessed atbaseline
Participants
The study was conducted at an Internet psychiatry unit(Hedman et al 2013) located in a university hospital in StockholmSweden Table 1 presents the characteristics of the participants Themain inclusion criteria were that participants had to (a) have aprincipal diagnosis of severe health anxiety ie hypochondriasisaccording to DSM-IV (American Psychiatric Association 2000) (b)agree not to undergo any other psychological treatment during thestudy (c) have a constant dosage two months prior to treatment ifon prescribed medication for anxiety or depression (d) have nohistory of psychosis or bipolar disorder and (e) not score gt20 onthe Montgomery Aringsberg Depression Rating Scale-Self-report(MADRS-S Svanborg amp Aringsberg1994) if diagnostic criteria for majordepression were met (f) have no serious somatic disease (g) haveno history of CBT in the past four years and (h) not meet criteria forany personality disorder within cluster A or B according to theDSM-IV In the inclusion process all participants underwent adiagnostic interview with a psychologist
Treatment e Internet-based CBT
The treatment used in this study can essentially be described asInternet-delivered CBT-bibliotherapy with web-based therapistcontact The treatment consisted of a self-help text provided in 12modules completed over 12 weeks through an Internet-basedtreatment platform with access to a therapist via a secure onlinecontact system The treatment platform was used as a mean ofproviding the tools and knowledge necessary for conducting thein vivo behavior change prescribed by the treatment
Table 1Description of the participants
Variable Internet-basedCBT participants(N frac14 81)
Age Mean age yrs (SD) 39 (97)Range yrs 25e69
Gender Women 60 (74)Men 21 (26)
Marital status Married or de facto 70 (86)Not married 11 (14)
Parental status Parent 54 (67)Not parent 27 (33)
Educational level Secondary school or shorter 23 (28)University started but did not finish 14 (17)University finished 44 (54)
Computer skill Mean self-rated skill (SD) 43Range 2e5
Occupationalstatus
Working full time 63 (78)Not working full time 18 (22)
Health Anxiety Mean duration of symptoms yrs (SD) 210 (132)SHAI score at baseline (SD) 325 (72)
Comorbidpsychiatricdisorder atbaseline
Any anxiety disorder () 41 (51)Median no of anxiety disorders (range) 1 (0e3)Depression or dysthymia 14 (18)
Depressivesymptoms
MADRS-S score at baseline (SD) 130 (67)
Abbreviations CBT Cognitive behavior therapy SHAI Short Health Anxiety In-ventory MADRS-S Montgomery Aringsberg Depression Rating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 713
The treatment was based on a CBT model for health anxietyemphasizing the role of avoidance and safety behaviors as main-taining factors of health anxiety (Furer Walker amp Stein 2007Taylor amp Asmundson 2004) The main component of the treat-ment was exposure and response prevention In brief modules 1and 2 comprised psychoeducation about CBT and health anxietyand introduced mindfulness training module 3 focused on cogni-tive processes in health anxiety the main component of modules4e10 was exposure to health anxiety stimuli and response pre-vention and modules 11e12 were focused on relapse preventionThe treatment protocol was developed by our research group and ithas been validated in a trial investigating the effects of group CBTfor severe health anxiety (Hedman Ljoacutetsson Andersson et al2010)
Dependent variables
Primary outcome measure and types of end pointsThe primary outcome measure was the Health Anxiety In-
ventory (HAI Salkovskis Rimes Warwick amp Clark 2002) The HAI(scale range 0e192) has excellent psychometric propertiesincluding high internal consistency (Cronbachrsquos a frac14 95) good test-retest reliability (r frac14 90) and good convergent validity (Salkovskiset al 2002)
Three types of outcomes based on the HAI were used in thepresent study They were a) HAI score at six-month follow-up b)change score of the HAI from baseline to six-month follow-up andc) clinically significant improvement at six-month follow-up usingthe Jacobson and Truax criteria (Jacobson amp Truax 1991) The latteroutcome meant that participants had to experience an improve-ment beyond fluctuations due to measurement error ie reliablechange (an improvement by at least 17 HAI points) and also becloser to the healthy population than to the clinical population interms of health anxiety ie absolute improvement criterion (have ascore of 60 or lower on the HAI) That is to be classified as clinicallysignificant improved both the reliable change criterion and theabsolute improvement criterion had to be met
Potential predictors
Clinical characteristicsDuring the clinical interview diagnostic assessments were
conducted using the Health Anxiety Interview (Taylor ampAsmundson 2004) and the Mini International Diagnostic Inter-view (MINI Sheehan et al 1998) Continuous measures ofdepressive symptoms general anxiety and anxiety sensitivity werethe MADRS-S (Svanborg amp Aringsberg 1994) the Beck Anxiety In-ventory (BAI Beck Epstein Brown amp Steer 1988) and the AnxietySensitivity Inventory (ASI Reiss Peterson Gursky amp McNally1986) respectively During the clinical interviews information onyears with severe health anxiety and concurrent psychotropicmedication (SSRISNRI) was also collected Self-report measureswere conducted over the Internet which has been shown to be avalid administration format (Hedman Ljoacutetsson Ruumlck et al 2010)The investigated potential clinical predictors were comorbid majordepression comorbid anxiety disorder (any type) baseline scoreson the MADRS-S BAI and the ASI years with severe health anxietyand concurrent stable psychotropic medication with SSRISNRI
Demographic characteristicsDemographic data were collected during the clinical interviews
The following demographic characteristics were investigated aspotential predictors age gender marital status educational levelworking full time (yesno) and having children or not
Therapy process-related variablesTo investigate whether participantsrsquo view of the treatment in
terms of credibility ie how believable and convincing the treat-ment is and expectancy ie how improved participants believethey will be the Credibility Scale was used (C-scale Borkovec ampNau 1972) The C-scale consists of five items that are scored on a10-point Likert scale and the measure has demonstrated high in-ternal consistency (Cronbachrsquos a frac14 84) and high test-retest reli-ability (r frac14 75e83) (Devilly amp Borkovec 2000) As the treatmentwas Internet-delivered we also assessed if computer skills pre-dicted outcome which was done through self-assessment using asingle 5-point Likert scale item (1 frac14 very lowly skilled to 5 veryhighly skilled) Investigated potential therapy process-related pre-dictors were C-scale scores number of completed modules andcomputer skills
Statistical analysis
Statistical analyses were conducted using SPSS version 200(SPSS inc Chicago) and the ROC4 (Stanford University) We con-ducted three types of analyses when investigating potential pre-dictors First linear regression analyses were performed adoptingthe two-step approach proposed by de Graaf Hollon and Huibers(2010) by identifying significant single predictors and subse-quently adding those into a final multiple regression model Foreach potential predictor variable a regressionmodel was built usingHAI scores (six-month follow-up scores and baseline to six-monthfollow-up change scores in separate analyses) as dependent vari-able and forced entry as regression method All significant pre-dictors were then analysed within a multiple regression modelusing backward deletion The second type of analysis performedwas logistic regression using fulfilment of criteria for clinicallysignificant improvement ie at least 17 HAI points improvementand a score below 61 on the same scale as dependent variableapplying the same model building approach as in the first series ofanalyses
Finally signal detection analysis based on recursive partitioningwas performed yielding receiver operator characteristics (ROC) of
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717714
subgroups with high and low chance of achieving clinically sig-nificant improvement using the same criteria as above (Andreescuet al 2008 Kraemer Lowe amp Kupfer 2005) Signal detection is aniterative process of splitting the sample in two groups based on theoptimal predictor cut-offs and is suitable when entering manypredictors due to its robustness concerning multicollinearity andoutliers (Kiernan Kraemer Winkleby King amp Taylor 2001) Foreach node in the tree odds ratios were calculated
Analyses of missing data were conducted using Littlersquos Missing-Completely-At-Random test (MCAR Little amp Rubin 1987) Missingdatawere replaced using linear regression imputation based on theavailable covariates When analysing patterns of change aftertreatment we used reliable change (ie an HAI score change of atleast 17 points) as an indicator of whether participants wereimproved or deteriorated between post-treatment and six-monthfollow-up
Results
Attrition and adherence
According to Littlersquos MCAR test data were missing completely atrandom (c(232)2 frac14 22693 plt 58) Therewas no data loss at baselinewhile 79 of 81 (98) participants completed assessments at post-treatment At six-month follow-up 74 of 81 participants (91)completed assessments Participants completed 81 modules(SD frac14 39) on average of a total possible of 12
Brief description of the efficacy of Internet-based CBT
The results of the outcome study showed that the within-groupeffect sizes were large on the primary outcome measure HAI atpost-treatment (d frac14 169 95CI frac14 132e204) and six-monthfollow-up (d frac14 190 95CI frac14 152e227) compared to baselineMixed effects models analysis showed that there was a significanteffect of time on the HAI from baseline to six-month follow-up(F frac14 131 df frac14 145 p lt 001) Of the 81 participants 42 (52) metthe criteria for clinically significant improvement at six-monthfollow-up
Predictors of end state health anxiety and improvement
Significant predictors of end state health anxiety (HAI) at six-month follow-up from the final multiple linear regression modelexplained 40 of the outcome variance (R2 frac14 40 p lt 001) Thecorresponding estimate of explained variance when using baselineto six-month follow-up change on the HAI as outcome was 33(R2 frac14 33 p lt 001) In the final multiple regression models thesignificant predictors were the same irrespective of using end statehealth anxiety or change in health anxiety as dependent variablesBelow results from each predictor domain are presented
Clinical characteristicsBoth when using end state health anxiety at six-month follow-
up and baseline to six-month follow-up change in health anxiety asdependent variable univariate linear regression analyses showedthat baseline health anxiety (HAI) depressive symptoms (MADRS-S) general anxiety (BAI) and anxiety sensitivity (ASI) were signifi-cant predictors The association was negative when using end statehealth anxiety as outcome meaning that higher symptom levels atbaseline predictedmore health anxiety at six-month follow-up Theassociation was positive when using change in health anxiety asdependent variable suggesting that more baseline symptoms inthese areas predicted larger improvements One exception wasdepressive symptoms where higher baseline scores on the MADRS-
S predicted less improvement in health anxiety In addition to thesepredictors results from the univariate analyses showed that havinga comorbid anxiety disorder predicted more health anxiety at six-month follow-up but this factor did not predict change in healthanxiety Years with severe health anxiety concurrent stable psy-chotropic medication with SSRISNRI and comorbid majordepression were not significantly related to outcome
In the final multiple regression model where all significantpredictors above was included in the model baseline health anxi-ety and depressive symptoms remained significant predictorsThus higher levels of health anxiety at baseline predicted morehealth anxiety at six-month follow-up (B frac14 45 SE frac14 13 p lt 001)and larger improvements in health anxiety (B frac14 55 SE frac14 13p lt 001) More depressive symptoms at baseline predicted morehealth anxiety at follow-up (B frac14 153 SE frac14 37 p lt 001) and lessimprovement in health anxiety (B frac14 152 SE frac14 37 p lt 001)
Demographic characteristicsThe only significant predictor from the initial univariate linear
regression was employment status Working full time predictedless symptoms at six-month follow-up but was unrelated tochange in health anxiety None of the other investigated de-mographic variables ie age gender marital status educationallevel and having children or not significantly predicted healthanxiety at six-month follow-up nor change in health anxietyEmployment status did not remain significant in the final multipleregression model
Therapy process-related variablesUnivariate regression analysis showed that more completed
modules predicted both less health anxiety at six-month follow-upand larger improvement in health anxiety Treatment credibilityand computer skills were unrelated to outcome In the final mul-tiple regression analysis number of completedmodules remained asignificant predictor of end state health anxiety (B frac14 154SE frac14 63 p lt 02) and of improvement in health anxiety (B frac14 154SE frac14 64 p lt 02)
Predictors of clinically significant improvement
Clinical characteristicsUnivariate logistic regression showed that more baseline health
anxiety depressive symptoms and general anxiety were associ-ated with a lower chance of being clinically significant improveddefined as an HAI score reduction by at least 17 points and a totalscore below 61 at six-month follow-up Years with severe healthanxiety concurrent stable psychotropic medicationwith SSRISNRIcomorbid depression comorbid anxiety disorder and anxietysensitivity were not significantly related to outcome In the finalmultiple regression model baseline health anxiety (B frac14 06SE frac14 02 p lt 001) and depressive symptoms (B frac14 12 SE frac14 05p lt 02) remained significant predictors of clinical significantimprovement
Demographic variablesThe only significant predictor in this domain was parental sta-
tus ie having children predicted higher probability of being clin-ically significant improved Age gender marital status educationallevel and employment status were unrelated to outcome The finalmultiple regression model retained parental status as a significantpredictor of clinically significant improvement
Therapy process-related factorsNone of the investigated therapy process-related factors ie C-
scale scores number of completed modules and computer skills
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 715
significantly predicted outcome in terms of clinically significantimprovement
Signal detection analysis and decision tree
Fig 1 displays the clinical decision tree including optimal cutoffpoints and receiver operator characteristics using clinically signif-icant improvement as outcome As shown in Fig 1 the analysisyielded a model with two significant interacting predictors in formof baseline health anxiety (HAI) and depressive symptoms(MADRS-S) (c2 frac14 87e134 ps lt 01) The odds ratios ranged from55 to 124 indicating a moderate to large effect of the predictors
Patterns of change from post-treatment to six-month follow-upUsing the criterion for reliable change ie a change score of at
least 17 HAI points 15 (19) of 81 participants made further im-provements in health anxiety between post-treatment and six-month follow-up Univariate logistic regression analyses showedthat less health anxiety change during the treatment and morehealth anxiety at post-treatment was related to a larger chance ofimprovement between post-treatment and six-month follow-up Inthe final logistic regression model health anxiety at post-treatmentremained a significant predictor (B frac14 03 SE frac14 01 p lt 03)
We also investigated patterns of deterioration after the end ofthe treatment period From post-treatment to six-month follow-up8 (10) of the participants reliably increased in their health anxietyHigher levels of health anxiety at post-treatment were associatedwith a reduced risk of making a reliable deterioration to six-monthfollow-up (B frac14 05 SE frac14 02 p lt 02)
Discussion
To the best of our knowledge this study is the first to investigatepredictors of outcome in Internet-based CBT for severe healthanxiety The results showed that the most stable predictors were
Clinical significant impn=42
52 of total sam
Health anxiety at
HAI score ge 108n=11
(29 clinically significant improved)Lowest probability of improvement
MADRS-S score ge 1n=5
(38 clinically significant i
Fig 1 Decision tree of predictors from signal detection analysis Receiver operator character70 (b) Negative predictive value 71 ROC for predictor depressive symptoms at baseliAbbreviations HAI Health anxiety inventory MADRS-S Montgomery Aringsberg Depression R
baseline health anxiety and depressive symptoms As hypothe-sized more health anxiety at baseline predicted more health anx-iety at six-month follow-up but also larger improvements in healthanxiety Signal detection analyses yielded a clinical decision treedemonstrating that a cutoff oflt108 on the HAI (health anxiety) andlt15 on the MADRS-S (depressive symptoms) was optimal toidentify the subgroup participants with the highest probability ofachieving clinically significant improvement The final model usingend state health anxiety as dependent variable showed that theincluded predictors explained 40 of the outcome variance Theexplained variance was slightly lower 33 when baseline to six-month follow-up change in health anxiety was used as outcomeOverall this suggests that it is possible to predict both symptomlevels at longer-term follow-up as well as improvement whichcould be of high value to the clinician when making treatmentrecommendations
When comparing the most powerful predictors baseline healthanxiety and depressive symptoms an interesting different in pre-dictive patterns emerged Persons with more health anxiety beforetreatment made larger improvements in health anxiety while thosewith more depressive symptoms made less improvements inhealth anxiety In our view this indicates that patients with themost severe forms of health anxiety are suitable candidates forInternet-based CBT but it is likely that they will still be having mildto moderate health anxiety after treatment
As for patients with high levels of depressive symptoms atbaseline the picture is slightly more complicated This patientgroup is not only more likely to have more residuals symptoms ofhealth anxiety at follow-up it also has a lower chance of beingimproved We do not generally discourage from using Internet-based CBT if the patient has comorbid depression However thesepersons would benefit from careful monitoring during the treat-ment and the clinician should take additional actions fairly early ifthe patient does not respond to the treatment Although one of theexclusion criteria in the original RCT was scoring higher than 20 on
rovement
ple
baseline
HAI score lt 108n=31
(69 clinically significant improved)
Depressive symptoms at baseline
5
mproved)
MADRS-S score lt 15n=26
(83 clinically significant improved)Highest probability of improvement
istics (ROC) for predictor health anxiety at baseline (HAI) (a) Positive predictive valuene (MADRS-S) (a) Positive predictive value 83 (b) Negative predictive value 62ating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717716
the MADRS-S if being diagnosed with depression it should benoted that no participant was excluded because of it In additionthe mean MADRS-S score of the sample at baseline was above thecutoff indicating depression (Svanborg amp Ekselius 2003) whichmeans that it is probably fair to assume that this sample was notbiased in terms of having too low levels of depressive symptoms Inan analysis of meditators we also found that improvements inhealth anxiety at a given time T during the 12-week treatmentmediated improvement in depressive symptoms at T thorn 1 week(unpublished data)
Demographic variables were largely unrelated to treatmentoutcome with the one exception that having children was associ-ated with a higher chance of achieving clinically significantimprovement (but not with continuous measures of health anxi-ety) Thus it seems that Internet-based CBT suits equally well ifyoung or old man or woman married or unmarried and regardlessif highly educated or not
As for therapy process-related measures the only significantpredictor was number of completedmodules which predicted bothend state symptom levels and change in health anxiety This sug-gests that adherence is important which has been shown also inprevious predictor research on Internet-based CBT for social anxi-ety disorder (Hedman et al 2012) Interestingly computer skillsdid not predict outcome thus replicating findings from priorstudies of Internet-based CBT (Hedman et al 2012) It shouldhowever be noted that participants on average rated their com-putes skill to be high which could reduce the power to detect adifference due to range restriction Taken together with the factthat age was unrelated to outcome this nevertheless suggests thatthe common conception that Internet-based treatments are pri-marily for young persons highly skilled in computer use is likely tobe incorrect
A common question in relatively brief psychological treatmentsis what the chances are of being further improved after the finalsession The analyses of this study showed that as many as 19 ofthe participants made reliable improvements from post-treatmentto six-month follow-up and that health anxiety at post-treatmentsignificantly predicted subsequent improvement This is clinicallyinformative as it means that patients with more post-treatmentresidual symptoms could expect to be further improved
In comparison to prior research on of predictors of conventionalCBT for severe health anxiety the results of this study are similar tothe findings of the study of Nakao et al (2011) which showed thatmore baseline health anxiety predicted larger improvements As inthis study Buwalda and Bouman (2008) found that more baselinehealth anxiety predicted more symptoms at follow-up in groupCBT and Hiller et al (2002) showed that responders had lowerlevels of health anxiety before treatment when investigating pre-dictors of individual CBT Similar to the findings of the study byBuwalda and Bouman (2008) age did not predict outcome at six-month follow-up in the present study although their study founda small negative association between age and health anxiety atpost-treatment Taken together this suggests that prognostic fac-tors are the same in Internet-based CBT for severe health anxiety asin conventional CBT That is for those patients with severe healthanxiety for which face-to-face CBT works Internet-based CBT isalso likely to be effective
This study has some limitations First as participants receivedtreatment within the context of an RCT the use of inclusion criteriaimposed a restriction of range of the predictors This meant that thepersons with the lowest chance of responding to the treatmentwere likely to be excluded eg children or persons with comorbidpsychotic disorders However our general aim when choosing theinclusion criteria was to apply largely the same as we would use inclinical routine care A second limitation was power to detect
predictive factors with less impact However the sample size wassufficient to detect predictors of moderate effect thus representingfactors to be considered useful in a clinical perspective
Considering the strengths of this study ie the high quality ofassessments the standardized treatment format and low attritionrates the findings are important as they show that end state healthanxiety as well as improvement can be predicted in Internet-basedCBT
Financial disclosure
None reported
Funding
This study was funded by Karolinska Institutet and by researchgrants from Stockholm County Council
Role of the sponsor
The main funding organizations (Karolinska Institutet andStockholm County Council) are public institutions and neither ofthe funding organizations had any role in the design and conduct ofthe study in the collection or interpretation of the data nor in thewriting of the report or in the decision to submit it
Conflict of interest
All authors report that they have no competing interests
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mentaldisorders DSM-IV-TR (4th ed) Washington DC American PsychiatricAssociation
Andreescu C Mulsant B H Houck P R Whyte E M Mazumdar SDombrovski A Y et al (2008) Empirically derived decision trees for thetreatment of late-life depression American Journal of Psychiatry 165(7) 855e862 httpdxdoiorg101176appiajp200807081340
Beck A T Epstein N Brown G amp Steer R A (1988) An inventory for measuringclinical anxiety psychometric properties Journal of Consulting and ClinicalPsychology 56(6) 893e897
Borkovec T D amp Nau S D (1972) Credibility of analogue therapy rationalesJournal of Behavior Therapy and Experimental Psychiatry 3(4) 257e260
Buwalda F M amp Bouman T K (2008) Predicting the effect of psychoeducationalgroup treatment for hypochondriasis Journal of Psychology amp Psychotherapy15(6) 396e403 httpdxdoiorg101002cpp602
Buwalda F M Bouman T K amp van Duijn M A (2007) Psychoeducation for hy-pochondriasis a comparison of a cognitive-behavioural approach and aproblem-solving approach Behaviour Research and Therapy 45(5) 887e899httpdxdoiorg101016jbrat200608004
Chambless D L Tran G Q amp Glass C R (1997) Predictors of response tocognitive-behavioral group therapy for social phobia Journal of Anxiety Disor-ders 11(3) 221e240 S0887-6185(97)00008-X
Clark D Salkovskis P Hackmann A Wells A Fennell M Ludgate J et al (1998)Two psychological treatments for hypochondriasis A randomised controlledtrial British Journal of Psychiatry 173(3) 218e225 httpdxdoiorg101192bjp1733218
Devilly G J amp Borkovec T D (2000) Psychometric properties of the credibilityexpectancy questionnaire Journal of Behavior Therapy and Experimental Psy-chiatry 31(2) 73e86
Furer P Walker J R amp Stein M B (2007) Treating health anxiety and fear of deathA practitionerrsquos guide New York NY Springer
de Graaf L E Hollon S D amp Huibers M J (2010) Predicting outcome incomputerized cognitive behavioral therapy for depression in primary care arandomized trial Journal of Consulting and Clinical Psychology 78(2) 184e189doi 2010-05835-005 [pii] 101037a0018324 [doi]
Greeven A van Balkom A J Visser S Merkelbach J W van Rood Y R vanDyck R et al (2007) Cognitive behavior therapy and paroxetine in the treat-ment of hypochondriasis a randomized controlled trial American Journal ofPsychiatry 164(1) 91e99 doi 164191 [pii] 101176appiajp164191
Hedman E Ljoacutetsson B Andersson E Ruumlck C Andersson G amp Lindefors N(2010) Effectiveness and cost offset analysis of group CBT for hypochondriasisdelivered in a psychiatric setting an open trial Cognitive Behaviour Therapy39(4) 239e250 httpdxdoiorg101080165060732010496460
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189

E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717712
2002) Predictor variables can broadly be classified into three cat-egories a) clinical characteristics ie variables related to the clin-ical disorder such as symptom levels b) demographic variables egage and gender and c) therapy process-related variables eg ex-pectancy of treatment outcome
Previous studies investigating predictors on conventional face-to-face CBT for severe health anxiety have demonstrated thatclinical characteristics associated with outcome are severity ofhealth anxiety general anxiety and negative cognitions regardingbodily symptoms (Buwalda amp Bouman 2008 Hiller Leibbrand Riefamp Fichter 2002 Nakao Shinozaki Ahern amp Barsky 2011) It seemshowever that these predictive clinical factors are mainly related tolevels of health anxiety after treatment ie persons with higherlevels of these symptoms at baseline tend to have more healthanxiety at post-treatment When it comes to predictors ofimprovement one fairly robust result seems to be that baselinehealth anxiety predicts larger improvement from baseline to post-treatment (Buwalda amp Bouman 2008 Nakao et al 2011) Thiscould be interpreted as higher initial symptom severity gives roomfor more improvement
As for demographic predictors no previous studies on CBT forhealth anxiety have demonstrated clear predictive effects In onestudy higher age was associated with less pre-to-post-treatmentgains (Buwalda amp Bouman 2008) but in two other reports nopredictive effect of age was found (Hiller et al 2002 Nakao et al2011) Following the same pattern of mixed results Nakao et al(2011) found that marital status predicted better outcome ie be-ing married was associated with larger improvements while therewas no such association in the study by Hiller et al (2002)
When it comes to therapy process-related factors publisheddata are scarce Buwalda and Bouman investigated the prognosticeffect of expectancy of treatment outcome but found no significantassociation with health anxiety reduction (Buwalda amp Bouman2008) In research on other anxiety disorders higher expectancyof treatment outcome has been shown to predict larger improve-ments (Chambless Tran amp Glass 1997 Hedman et al 2012Mausbach Moore Roesch Cardenas amp Patterson 2010) InInternet-based CBT for social anxiety disorder treatment adher-ence ie number of completed modules has been shown to predictbetter treatment outcomes (Hedman et al 2012 Nordgreen et al2012)
In sum based on the previous literature baseline health anxietyemerges as the only stable predictor of both end state health anx-iety and improvement in CBT for severe health anxiety To date nostudy has investigated predictors of Internet-based CBT for thispatient group Although the hypothesized therapeutic mechanismsare the same in Internet-based and conventional CBT there areimportant differences potentially influencing what factors thatpredict outcome These differences include that patients haveminimal therapist guidance and thus must take a larger re-sponsibility for learning how the treatment works and how toapply general therapeutic principles on their own idiosyncratichealth anxiety behaviors Other differences are that the Internet-based CBT requires basic computer skills and that the patientmust read lengthy fairly complex texts It could therefore be thatdemographic factors such as age computer skills and educationalbackground have a larger impact on outcome in Internet-basedCBT As treatment delivered via the Internet requires a highlyactive patient despite limited therapist guidance it could also bethat clinical factors related to passive coping such as comorbiddepressive symptoms have a larger negative predictive value inthis form of therapy compared to conventional CBT Prior researchon social anxiety disorder has shown that delivery format ieInternet or face-to-face can moderate the effect of predictors(Hedman et al 2012) Against this background it is highly
important to examine which factors that predict treatmentoutcome in Internet-based CBT for severe health anxiety
The main aim of this study was to investigate clinical de-mographic and therapy process-related predictors of treatmentoutcome both regarding end state and improvement in Internet-based CBT for severe health anxiety We hypothesized that morehealth anxiety at baseline would predict larger improvements butalso more health anxiety at six-month follow-up Due to the mixedresults in the literature in terms of demographic and therapy pro-cess factors the analyses in these domains were consideredexploratory The second aim of the study was to investigate pat-terns of change in health anxiety between end of treatment andlonger-term follow-up and predictors of this change
Methods
Study design
This was a study with a repeated measurements design inves-tigating predictors of outcome in a sample of participants (N frac14 81)who received treatment within the context of a previously pub-lished randomized controlled trial (RCT) (Hedman et al 2011) Inthe trial participants were randomized to ICBT (n frac14 40) or thecontrol condition (n frac14 41) As participants in the control conditionhad stable symptom levels during the initial 12 weeks and werecrossed over to treatment directly after the 12 weeks all random-ized participants were included in this study and no waiting listdata were used This meant that all predictor analyses were con-ducted using data from a sample that had received treatment andthat the distinction between the treatment condition and thecontrol condition in the original RCT is not relevant for the presentstudy All dependent variables were assessed at six-month follow-up and in the main analyses potential predictors were assessed atbaseline
Participants
The study was conducted at an Internet psychiatry unit(Hedman et al 2013) located in a university hospital in StockholmSweden Table 1 presents the characteristics of the participants Themain inclusion criteria were that participants had to (a) have aprincipal diagnosis of severe health anxiety ie hypochondriasisaccording to DSM-IV (American Psychiatric Association 2000) (b)agree not to undergo any other psychological treatment during thestudy (c) have a constant dosage two months prior to treatment ifon prescribed medication for anxiety or depression (d) have nohistory of psychosis or bipolar disorder and (e) not score gt20 onthe Montgomery Aringsberg Depression Rating Scale-Self-report(MADRS-S Svanborg amp Aringsberg1994) if diagnostic criteria for majordepression were met (f) have no serious somatic disease (g) haveno history of CBT in the past four years and (h) not meet criteria forany personality disorder within cluster A or B according to theDSM-IV In the inclusion process all participants underwent adiagnostic interview with a psychologist
Treatment e Internet-based CBT
The treatment used in this study can essentially be described asInternet-delivered CBT-bibliotherapy with web-based therapistcontact The treatment consisted of a self-help text provided in 12modules completed over 12 weeks through an Internet-basedtreatment platform with access to a therapist via a secure onlinecontact system The treatment platform was used as a mean ofproviding the tools and knowledge necessary for conducting thein vivo behavior change prescribed by the treatment
Table 1Description of the participants
Variable Internet-basedCBT participants(N frac14 81)
Age Mean age yrs (SD) 39 (97)Range yrs 25e69
Gender Women 60 (74)Men 21 (26)
Marital status Married or de facto 70 (86)Not married 11 (14)
Parental status Parent 54 (67)Not parent 27 (33)
Educational level Secondary school or shorter 23 (28)University started but did not finish 14 (17)University finished 44 (54)
Computer skill Mean self-rated skill (SD) 43Range 2e5
Occupationalstatus
Working full time 63 (78)Not working full time 18 (22)
Health Anxiety Mean duration of symptoms yrs (SD) 210 (132)SHAI score at baseline (SD) 325 (72)
Comorbidpsychiatricdisorder atbaseline
Any anxiety disorder () 41 (51)Median no of anxiety disorders (range) 1 (0e3)Depression or dysthymia 14 (18)
Depressivesymptoms
MADRS-S score at baseline (SD) 130 (67)
Abbreviations CBT Cognitive behavior therapy SHAI Short Health Anxiety In-ventory MADRS-S Montgomery Aringsberg Depression Rating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 713
The treatment was based on a CBT model for health anxietyemphasizing the role of avoidance and safety behaviors as main-taining factors of health anxiety (Furer Walker amp Stein 2007Taylor amp Asmundson 2004) The main component of the treat-ment was exposure and response prevention In brief modules 1and 2 comprised psychoeducation about CBT and health anxietyand introduced mindfulness training module 3 focused on cogni-tive processes in health anxiety the main component of modules4e10 was exposure to health anxiety stimuli and response pre-vention and modules 11e12 were focused on relapse preventionThe treatment protocol was developed by our research group and ithas been validated in a trial investigating the effects of group CBTfor severe health anxiety (Hedman Ljoacutetsson Andersson et al2010)
Dependent variables
Primary outcome measure and types of end pointsThe primary outcome measure was the Health Anxiety In-
ventory (HAI Salkovskis Rimes Warwick amp Clark 2002) The HAI(scale range 0e192) has excellent psychometric propertiesincluding high internal consistency (Cronbachrsquos a frac14 95) good test-retest reliability (r frac14 90) and good convergent validity (Salkovskiset al 2002)
Three types of outcomes based on the HAI were used in thepresent study They were a) HAI score at six-month follow-up b)change score of the HAI from baseline to six-month follow-up andc) clinically significant improvement at six-month follow-up usingthe Jacobson and Truax criteria (Jacobson amp Truax 1991) The latteroutcome meant that participants had to experience an improve-ment beyond fluctuations due to measurement error ie reliablechange (an improvement by at least 17 HAI points) and also becloser to the healthy population than to the clinical population interms of health anxiety ie absolute improvement criterion (have ascore of 60 or lower on the HAI) That is to be classified as clinicallysignificant improved both the reliable change criterion and theabsolute improvement criterion had to be met
Potential predictors
Clinical characteristicsDuring the clinical interview diagnostic assessments were
conducted using the Health Anxiety Interview (Taylor ampAsmundson 2004) and the Mini International Diagnostic Inter-view (MINI Sheehan et al 1998) Continuous measures ofdepressive symptoms general anxiety and anxiety sensitivity werethe MADRS-S (Svanborg amp Aringsberg 1994) the Beck Anxiety In-ventory (BAI Beck Epstein Brown amp Steer 1988) and the AnxietySensitivity Inventory (ASI Reiss Peterson Gursky amp McNally1986) respectively During the clinical interviews information onyears with severe health anxiety and concurrent psychotropicmedication (SSRISNRI) was also collected Self-report measureswere conducted over the Internet which has been shown to be avalid administration format (Hedman Ljoacutetsson Ruumlck et al 2010)The investigated potential clinical predictors were comorbid majordepression comorbid anxiety disorder (any type) baseline scoreson the MADRS-S BAI and the ASI years with severe health anxietyand concurrent stable psychotropic medication with SSRISNRI
Demographic characteristicsDemographic data were collected during the clinical interviews
The following demographic characteristics were investigated aspotential predictors age gender marital status educational levelworking full time (yesno) and having children or not
Therapy process-related variablesTo investigate whether participantsrsquo view of the treatment in
terms of credibility ie how believable and convincing the treat-ment is and expectancy ie how improved participants believethey will be the Credibility Scale was used (C-scale Borkovec ampNau 1972) The C-scale consists of five items that are scored on a10-point Likert scale and the measure has demonstrated high in-ternal consistency (Cronbachrsquos a frac14 84) and high test-retest reli-ability (r frac14 75e83) (Devilly amp Borkovec 2000) As the treatmentwas Internet-delivered we also assessed if computer skills pre-dicted outcome which was done through self-assessment using asingle 5-point Likert scale item (1 frac14 very lowly skilled to 5 veryhighly skilled) Investigated potential therapy process-related pre-dictors were C-scale scores number of completed modules andcomputer skills
Statistical analysis
Statistical analyses were conducted using SPSS version 200(SPSS inc Chicago) and the ROC4 (Stanford University) We con-ducted three types of analyses when investigating potential pre-dictors First linear regression analyses were performed adoptingthe two-step approach proposed by de Graaf Hollon and Huibers(2010) by identifying significant single predictors and subse-quently adding those into a final multiple regression model Foreach potential predictor variable a regressionmodel was built usingHAI scores (six-month follow-up scores and baseline to six-monthfollow-up change scores in separate analyses) as dependent vari-able and forced entry as regression method All significant pre-dictors were then analysed within a multiple regression modelusing backward deletion The second type of analysis performedwas logistic regression using fulfilment of criteria for clinicallysignificant improvement ie at least 17 HAI points improvementand a score below 61 on the same scale as dependent variableapplying the same model building approach as in the first series ofanalyses
Finally signal detection analysis based on recursive partitioningwas performed yielding receiver operator characteristics (ROC) of
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717714
subgroups with high and low chance of achieving clinically sig-nificant improvement using the same criteria as above (Andreescuet al 2008 Kraemer Lowe amp Kupfer 2005) Signal detection is aniterative process of splitting the sample in two groups based on theoptimal predictor cut-offs and is suitable when entering manypredictors due to its robustness concerning multicollinearity andoutliers (Kiernan Kraemer Winkleby King amp Taylor 2001) Foreach node in the tree odds ratios were calculated
Analyses of missing data were conducted using Littlersquos Missing-Completely-At-Random test (MCAR Little amp Rubin 1987) Missingdatawere replaced using linear regression imputation based on theavailable covariates When analysing patterns of change aftertreatment we used reliable change (ie an HAI score change of atleast 17 points) as an indicator of whether participants wereimproved or deteriorated between post-treatment and six-monthfollow-up
Results
Attrition and adherence
According to Littlersquos MCAR test data were missing completely atrandom (c(232)2 frac14 22693 plt 58) Therewas no data loss at baselinewhile 79 of 81 (98) participants completed assessments at post-treatment At six-month follow-up 74 of 81 participants (91)completed assessments Participants completed 81 modules(SD frac14 39) on average of a total possible of 12
Brief description of the efficacy of Internet-based CBT
The results of the outcome study showed that the within-groupeffect sizes were large on the primary outcome measure HAI atpost-treatment (d frac14 169 95CI frac14 132e204) and six-monthfollow-up (d frac14 190 95CI frac14 152e227) compared to baselineMixed effects models analysis showed that there was a significanteffect of time on the HAI from baseline to six-month follow-up(F frac14 131 df frac14 145 p lt 001) Of the 81 participants 42 (52) metthe criteria for clinically significant improvement at six-monthfollow-up
Predictors of end state health anxiety and improvement
Significant predictors of end state health anxiety (HAI) at six-month follow-up from the final multiple linear regression modelexplained 40 of the outcome variance (R2 frac14 40 p lt 001) Thecorresponding estimate of explained variance when using baselineto six-month follow-up change on the HAI as outcome was 33(R2 frac14 33 p lt 001) In the final multiple regression models thesignificant predictors were the same irrespective of using end statehealth anxiety or change in health anxiety as dependent variablesBelow results from each predictor domain are presented
Clinical characteristicsBoth when using end state health anxiety at six-month follow-
up and baseline to six-month follow-up change in health anxiety asdependent variable univariate linear regression analyses showedthat baseline health anxiety (HAI) depressive symptoms (MADRS-S) general anxiety (BAI) and anxiety sensitivity (ASI) were signifi-cant predictors The association was negative when using end statehealth anxiety as outcome meaning that higher symptom levels atbaseline predictedmore health anxiety at six-month follow-up Theassociation was positive when using change in health anxiety asdependent variable suggesting that more baseline symptoms inthese areas predicted larger improvements One exception wasdepressive symptoms where higher baseline scores on the MADRS-
S predicted less improvement in health anxiety In addition to thesepredictors results from the univariate analyses showed that havinga comorbid anxiety disorder predicted more health anxiety at six-month follow-up but this factor did not predict change in healthanxiety Years with severe health anxiety concurrent stable psy-chotropic medication with SSRISNRI and comorbid majordepression were not significantly related to outcome
In the final multiple regression model where all significantpredictors above was included in the model baseline health anxi-ety and depressive symptoms remained significant predictorsThus higher levels of health anxiety at baseline predicted morehealth anxiety at six-month follow-up (B frac14 45 SE frac14 13 p lt 001)and larger improvements in health anxiety (B frac14 55 SE frac14 13p lt 001) More depressive symptoms at baseline predicted morehealth anxiety at follow-up (B frac14 153 SE frac14 37 p lt 001) and lessimprovement in health anxiety (B frac14 152 SE frac14 37 p lt 001)
Demographic characteristicsThe only significant predictor from the initial univariate linear
regression was employment status Working full time predictedless symptoms at six-month follow-up but was unrelated tochange in health anxiety None of the other investigated de-mographic variables ie age gender marital status educationallevel and having children or not significantly predicted healthanxiety at six-month follow-up nor change in health anxietyEmployment status did not remain significant in the final multipleregression model
Therapy process-related variablesUnivariate regression analysis showed that more completed
modules predicted both less health anxiety at six-month follow-upand larger improvement in health anxiety Treatment credibilityand computer skills were unrelated to outcome In the final mul-tiple regression analysis number of completedmodules remained asignificant predictor of end state health anxiety (B frac14 154SE frac14 63 p lt 02) and of improvement in health anxiety (B frac14 154SE frac14 64 p lt 02)
Predictors of clinically significant improvement
Clinical characteristicsUnivariate logistic regression showed that more baseline health
anxiety depressive symptoms and general anxiety were associ-ated with a lower chance of being clinically significant improveddefined as an HAI score reduction by at least 17 points and a totalscore below 61 at six-month follow-up Years with severe healthanxiety concurrent stable psychotropic medicationwith SSRISNRIcomorbid depression comorbid anxiety disorder and anxietysensitivity were not significantly related to outcome In the finalmultiple regression model baseline health anxiety (B frac14 06SE frac14 02 p lt 001) and depressive symptoms (B frac14 12 SE frac14 05p lt 02) remained significant predictors of clinical significantimprovement
Demographic variablesThe only significant predictor in this domain was parental sta-
tus ie having children predicted higher probability of being clin-ically significant improved Age gender marital status educationallevel and employment status were unrelated to outcome The finalmultiple regression model retained parental status as a significantpredictor of clinically significant improvement
Therapy process-related factorsNone of the investigated therapy process-related factors ie C-
scale scores number of completed modules and computer skills
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 715
significantly predicted outcome in terms of clinically significantimprovement
Signal detection analysis and decision tree
Fig 1 displays the clinical decision tree including optimal cutoffpoints and receiver operator characteristics using clinically signif-icant improvement as outcome As shown in Fig 1 the analysisyielded a model with two significant interacting predictors in formof baseline health anxiety (HAI) and depressive symptoms(MADRS-S) (c2 frac14 87e134 ps lt 01) The odds ratios ranged from55 to 124 indicating a moderate to large effect of the predictors
Patterns of change from post-treatment to six-month follow-upUsing the criterion for reliable change ie a change score of at
least 17 HAI points 15 (19) of 81 participants made further im-provements in health anxiety between post-treatment and six-month follow-up Univariate logistic regression analyses showedthat less health anxiety change during the treatment and morehealth anxiety at post-treatment was related to a larger chance ofimprovement between post-treatment and six-month follow-up Inthe final logistic regression model health anxiety at post-treatmentremained a significant predictor (B frac14 03 SE frac14 01 p lt 03)
We also investigated patterns of deterioration after the end ofthe treatment period From post-treatment to six-month follow-up8 (10) of the participants reliably increased in their health anxietyHigher levels of health anxiety at post-treatment were associatedwith a reduced risk of making a reliable deterioration to six-monthfollow-up (B frac14 05 SE frac14 02 p lt 02)
Discussion
To the best of our knowledge this study is the first to investigatepredictors of outcome in Internet-based CBT for severe healthanxiety The results showed that the most stable predictors were
Clinical significant impn=42
52 of total sam
Health anxiety at
HAI score ge 108n=11
(29 clinically significant improved)Lowest probability of improvement
MADRS-S score ge 1n=5
(38 clinically significant i
Fig 1 Decision tree of predictors from signal detection analysis Receiver operator character70 (b) Negative predictive value 71 ROC for predictor depressive symptoms at baseliAbbreviations HAI Health anxiety inventory MADRS-S Montgomery Aringsberg Depression R
baseline health anxiety and depressive symptoms As hypothe-sized more health anxiety at baseline predicted more health anx-iety at six-month follow-up but also larger improvements in healthanxiety Signal detection analyses yielded a clinical decision treedemonstrating that a cutoff oflt108 on the HAI (health anxiety) andlt15 on the MADRS-S (depressive symptoms) was optimal toidentify the subgroup participants with the highest probability ofachieving clinically significant improvement The final model usingend state health anxiety as dependent variable showed that theincluded predictors explained 40 of the outcome variance Theexplained variance was slightly lower 33 when baseline to six-month follow-up change in health anxiety was used as outcomeOverall this suggests that it is possible to predict both symptomlevels at longer-term follow-up as well as improvement whichcould be of high value to the clinician when making treatmentrecommendations
When comparing the most powerful predictors baseline healthanxiety and depressive symptoms an interesting different in pre-dictive patterns emerged Persons with more health anxiety beforetreatment made larger improvements in health anxiety while thosewith more depressive symptoms made less improvements inhealth anxiety In our view this indicates that patients with themost severe forms of health anxiety are suitable candidates forInternet-based CBT but it is likely that they will still be having mildto moderate health anxiety after treatment
As for patients with high levels of depressive symptoms atbaseline the picture is slightly more complicated This patientgroup is not only more likely to have more residuals symptoms ofhealth anxiety at follow-up it also has a lower chance of beingimproved We do not generally discourage from using Internet-based CBT if the patient has comorbid depression However thesepersons would benefit from careful monitoring during the treat-ment and the clinician should take additional actions fairly early ifthe patient does not respond to the treatment Although one of theexclusion criteria in the original RCT was scoring higher than 20 on
rovement
ple
baseline
HAI score lt 108n=31
(69 clinically significant improved)
Depressive symptoms at baseline
5
mproved)
MADRS-S score lt 15n=26
(83 clinically significant improved)Highest probability of improvement
istics (ROC) for predictor health anxiety at baseline (HAI) (a) Positive predictive valuene (MADRS-S) (a) Positive predictive value 83 (b) Negative predictive value 62ating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717716
the MADRS-S if being diagnosed with depression it should benoted that no participant was excluded because of it In additionthe mean MADRS-S score of the sample at baseline was above thecutoff indicating depression (Svanborg amp Ekselius 2003) whichmeans that it is probably fair to assume that this sample was notbiased in terms of having too low levels of depressive symptoms Inan analysis of meditators we also found that improvements inhealth anxiety at a given time T during the 12-week treatmentmediated improvement in depressive symptoms at T thorn 1 week(unpublished data)
Demographic variables were largely unrelated to treatmentoutcome with the one exception that having children was associ-ated with a higher chance of achieving clinically significantimprovement (but not with continuous measures of health anxi-ety) Thus it seems that Internet-based CBT suits equally well ifyoung or old man or woman married or unmarried and regardlessif highly educated or not
As for therapy process-related measures the only significantpredictor was number of completedmodules which predicted bothend state symptom levels and change in health anxiety This sug-gests that adherence is important which has been shown also inprevious predictor research on Internet-based CBT for social anxi-ety disorder (Hedman et al 2012) Interestingly computer skillsdid not predict outcome thus replicating findings from priorstudies of Internet-based CBT (Hedman et al 2012) It shouldhowever be noted that participants on average rated their com-putes skill to be high which could reduce the power to detect adifference due to range restriction Taken together with the factthat age was unrelated to outcome this nevertheless suggests thatthe common conception that Internet-based treatments are pri-marily for young persons highly skilled in computer use is likely tobe incorrect
A common question in relatively brief psychological treatmentsis what the chances are of being further improved after the finalsession The analyses of this study showed that as many as 19 ofthe participants made reliable improvements from post-treatmentto six-month follow-up and that health anxiety at post-treatmentsignificantly predicted subsequent improvement This is clinicallyinformative as it means that patients with more post-treatmentresidual symptoms could expect to be further improved
In comparison to prior research on of predictors of conventionalCBT for severe health anxiety the results of this study are similar tothe findings of the study of Nakao et al (2011) which showed thatmore baseline health anxiety predicted larger improvements As inthis study Buwalda and Bouman (2008) found that more baselinehealth anxiety predicted more symptoms at follow-up in groupCBT and Hiller et al (2002) showed that responders had lowerlevels of health anxiety before treatment when investigating pre-dictors of individual CBT Similar to the findings of the study byBuwalda and Bouman (2008) age did not predict outcome at six-month follow-up in the present study although their study founda small negative association between age and health anxiety atpost-treatment Taken together this suggests that prognostic fac-tors are the same in Internet-based CBT for severe health anxiety asin conventional CBT That is for those patients with severe healthanxiety for which face-to-face CBT works Internet-based CBT isalso likely to be effective
This study has some limitations First as participants receivedtreatment within the context of an RCT the use of inclusion criteriaimposed a restriction of range of the predictors This meant that thepersons with the lowest chance of responding to the treatmentwere likely to be excluded eg children or persons with comorbidpsychotic disorders However our general aim when choosing theinclusion criteria was to apply largely the same as we would use inclinical routine care A second limitation was power to detect
predictive factors with less impact However the sample size wassufficient to detect predictors of moderate effect thus representingfactors to be considered useful in a clinical perspective
Considering the strengths of this study ie the high quality ofassessments the standardized treatment format and low attritionrates the findings are important as they show that end state healthanxiety as well as improvement can be predicted in Internet-basedCBT
Financial disclosure
None reported
Funding
This study was funded by Karolinska Institutet and by researchgrants from Stockholm County Council
Role of the sponsor
The main funding organizations (Karolinska Institutet andStockholm County Council) are public institutions and neither ofthe funding organizations had any role in the design and conduct ofthe study in the collection or interpretation of the data nor in thewriting of the report or in the decision to submit it
Conflict of interest
All authors report that they have no competing interests
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mentaldisorders DSM-IV-TR (4th ed) Washington DC American PsychiatricAssociation
Andreescu C Mulsant B H Houck P R Whyte E M Mazumdar SDombrovski A Y et al (2008) Empirically derived decision trees for thetreatment of late-life depression American Journal of Psychiatry 165(7) 855e862 httpdxdoiorg101176appiajp200807081340
Beck A T Epstein N Brown G amp Steer R A (1988) An inventory for measuringclinical anxiety psychometric properties Journal of Consulting and ClinicalPsychology 56(6) 893e897
Borkovec T D amp Nau S D (1972) Credibility of analogue therapy rationalesJournal of Behavior Therapy and Experimental Psychiatry 3(4) 257e260
Buwalda F M amp Bouman T K (2008) Predicting the effect of psychoeducationalgroup treatment for hypochondriasis Journal of Psychology amp Psychotherapy15(6) 396e403 httpdxdoiorg101002cpp602
Buwalda F M Bouman T K amp van Duijn M A (2007) Psychoeducation for hy-pochondriasis a comparison of a cognitive-behavioural approach and aproblem-solving approach Behaviour Research and Therapy 45(5) 887e899httpdxdoiorg101016jbrat200608004
Chambless D L Tran G Q amp Glass C R (1997) Predictors of response tocognitive-behavioral group therapy for social phobia Journal of Anxiety Disor-ders 11(3) 221e240 S0887-6185(97)00008-X
Clark D Salkovskis P Hackmann A Wells A Fennell M Ludgate J et al (1998)Two psychological treatments for hypochondriasis A randomised controlledtrial British Journal of Psychiatry 173(3) 218e225 httpdxdoiorg101192bjp1733218
Devilly G J amp Borkovec T D (2000) Psychometric properties of the credibilityexpectancy questionnaire Journal of Behavior Therapy and Experimental Psy-chiatry 31(2) 73e86
Furer P Walker J R amp Stein M B (2007) Treating health anxiety and fear of deathA practitionerrsquos guide New York NY Springer
de Graaf L E Hollon S D amp Huibers M J (2010) Predicting outcome incomputerized cognitive behavioral therapy for depression in primary care arandomized trial Journal of Consulting and Clinical Psychology 78(2) 184e189doi 2010-05835-005 [pii] 101037a0018324 [doi]
Greeven A van Balkom A J Visser S Merkelbach J W van Rood Y R vanDyck R et al (2007) Cognitive behavior therapy and paroxetine in the treat-ment of hypochondriasis a randomized controlled trial American Journal ofPsychiatry 164(1) 91e99 doi 164191 [pii] 101176appiajp164191
Hedman E Ljoacutetsson B Andersson E Ruumlck C Andersson G amp Lindefors N(2010) Effectiveness and cost offset analysis of group CBT for hypochondriasisdelivered in a psychiatric setting an open trial Cognitive Behaviour Therapy39(4) 239e250 httpdxdoiorg101080165060732010496460
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189

Table 1Description of the participants
Variable Internet-basedCBT participants(N frac14 81)
Age Mean age yrs (SD) 39 (97)Range yrs 25e69
Gender Women 60 (74)Men 21 (26)
Marital status Married or de facto 70 (86)Not married 11 (14)
Parental status Parent 54 (67)Not parent 27 (33)
Educational level Secondary school or shorter 23 (28)University started but did not finish 14 (17)University finished 44 (54)
Computer skill Mean self-rated skill (SD) 43Range 2e5
Occupationalstatus
Working full time 63 (78)Not working full time 18 (22)
Health Anxiety Mean duration of symptoms yrs (SD) 210 (132)SHAI score at baseline (SD) 325 (72)
Comorbidpsychiatricdisorder atbaseline
Any anxiety disorder () 41 (51)Median no of anxiety disorders (range) 1 (0e3)Depression or dysthymia 14 (18)
Depressivesymptoms
MADRS-S score at baseline (SD) 130 (67)
Abbreviations CBT Cognitive behavior therapy SHAI Short Health Anxiety In-ventory MADRS-S Montgomery Aringsberg Depression Rating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 713
The treatment was based on a CBT model for health anxietyemphasizing the role of avoidance and safety behaviors as main-taining factors of health anxiety (Furer Walker amp Stein 2007Taylor amp Asmundson 2004) The main component of the treat-ment was exposure and response prevention In brief modules 1and 2 comprised psychoeducation about CBT and health anxietyand introduced mindfulness training module 3 focused on cogni-tive processes in health anxiety the main component of modules4e10 was exposure to health anxiety stimuli and response pre-vention and modules 11e12 were focused on relapse preventionThe treatment protocol was developed by our research group and ithas been validated in a trial investigating the effects of group CBTfor severe health anxiety (Hedman Ljoacutetsson Andersson et al2010)
Dependent variables
Primary outcome measure and types of end pointsThe primary outcome measure was the Health Anxiety In-
ventory (HAI Salkovskis Rimes Warwick amp Clark 2002) The HAI(scale range 0e192) has excellent psychometric propertiesincluding high internal consistency (Cronbachrsquos a frac14 95) good test-retest reliability (r frac14 90) and good convergent validity (Salkovskiset al 2002)
Three types of outcomes based on the HAI were used in thepresent study They were a) HAI score at six-month follow-up b)change score of the HAI from baseline to six-month follow-up andc) clinically significant improvement at six-month follow-up usingthe Jacobson and Truax criteria (Jacobson amp Truax 1991) The latteroutcome meant that participants had to experience an improve-ment beyond fluctuations due to measurement error ie reliablechange (an improvement by at least 17 HAI points) and also becloser to the healthy population than to the clinical population interms of health anxiety ie absolute improvement criterion (have ascore of 60 or lower on the HAI) That is to be classified as clinicallysignificant improved both the reliable change criterion and theabsolute improvement criterion had to be met
Potential predictors
Clinical characteristicsDuring the clinical interview diagnostic assessments were
conducted using the Health Anxiety Interview (Taylor ampAsmundson 2004) and the Mini International Diagnostic Inter-view (MINI Sheehan et al 1998) Continuous measures ofdepressive symptoms general anxiety and anxiety sensitivity werethe MADRS-S (Svanborg amp Aringsberg 1994) the Beck Anxiety In-ventory (BAI Beck Epstein Brown amp Steer 1988) and the AnxietySensitivity Inventory (ASI Reiss Peterson Gursky amp McNally1986) respectively During the clinical interviews information onyears with severe health anxiety and concurrent psychotropicmedication (SSRISNRI) was also collected Self-report measureswere conducted over the Internet which has been shown to be avalid administration format (Hedman Ljoacutetsson Ruumlck et al 2010)The investigated potential clinical predictors were comorbid majordepression comorbid anxiety disorder (any type) baseline scoreson the MADRS-S BAI and the ASI years with severe health anxietyand concurrent stable psychotropic medication with SSRISNRI
Demographic characteristicsDemographic data were collected during the clinical interviews
The following demographic characteristics were investigated aspotential predictors age gender marital status educational levelworking full time (yesno) and having children or not
Therapy process-related variablesTo investigate whether participantsrsquo view of the treatment in
terms of credibility ie how believable and convincing the treat-ment is and expectancy ie how improved participants believethey will be the Credibility Scale was used (C-scale Borkovec ampNau 1972) The C-scale consists of five items that are scored on a10-point Likert scale and the measure has demonstrated high in-ternal consistency (Cronbachrsquos a frac14 84) and high test-retest reli-ability (r frac14 75e83) (Devilly amp Borkovec 2000) As the treatmentwas Internet-delivered we also assessed if computer skills pre-dicted outcome which was done through self-assessment using asingle 5-point Likert scale item (1 frac14 very lowly skilled to 5 veryhighly skilled) Investigated potential therapy process-related pre-dictors were C-scale scores number of completed modules andcomputer skills
Statistical analysis
Statistical analyses were conducted using SPSS version 200(SPSS inc Chicago) and the ROC4 (Stanford University) We con-ducted three types of analyses when investigating potential pre-dictors First linear regression analyses were performed adoptingthe two-step approach proposed by de Graaf Hollon and Huibers(2010) by identifying significant single predictors and subse-quently adding those into a final multiple regression model Foreach potential predictor variable a regressionmodel was built usingHAI scores (six-month follow-up scores and baseline to six-monthfollow-up change scores in separate analyses) as dependent vari-able and forced entry as regression method All significant pre-dictors were then analysed within a multiple regression modelusing backward deletion The second type of analysis performedwas logistic regression using fulfilment of criteria for clinicallysignificant improvement ie at least 17 HAI points improvementand a score below 61 on the same scale as dependent variableapplying the same model building approach as in the first series ofanalyses
Finally signal detection analysis based on recursive partitioningwas performed yielding receiver operator characteristics (ROC) of
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717714
subgroups with high and low chance of achieving clinically sig-nificant improvement using the same criteria as above (Andreescuet al 2008 Kraemer Lowe amp Kupfer 2005) Signal detection is aniterative process of splitting the sample in two groups based on theoptimal predictor cut-offs and is suitable when entering manypredictors due to its robustness concerning multicollinearity andoutliers (Kiernan Kraemer Winkleby King amp Taylor 2001) Foreach node in the tree odds ratios were calculated
Analyses of missing data were conducted using Littlersquos Missing-Completely-At-Random test (MCAR Little amp Rubin 1987) Missingdatawere replaced using linear regression imputation based on theavailable covariates When analysing patterns of change aftertreatment we used reliable change (ie an HAI score change of atleast 17 points) as an indicator of whether participants wereimproved or deteriorated between post-treatment and six-monthfollow-up
Results
Attrition and adherence
According to Littlersquos MCAR test data were missing completely atrandom (c(232)2 frac14 22693 plt 58) Therewas no data loss at baselinewhile 79 of 81 (98) participants completed assessments at post-treatment At six-month follow-up 74 of 81 participants (91)completed assessments Participants completed 81 modules(SD frac14 39) on average of a total possible of 12
Brief description of the efficacy of Internet-based CBT
The results of the outcome study showed that the within-groupeffect sizes were large on the primary outcome measure HAI atpost-treatment (d frac14 169 95CI frac14 132e204) and six-monthfollow-up (d frac14 190 95CI frac14 152e227) compared to baselineMixed effects models analysis showed that there was a significanteffect of time on the HAI from baseline to six-month follow-up(F frac14 131 df frac14 145 p lt 001) Of the 81 participants 42 (52) metthe criteria for clinically significant improvement at six-monthfollow-up
Predictors of end state health anxiety and improvement
Significant predictors of end state health anxiety (HAI) at six-month follow-up from the final multiple linear regression modelexplained 40 of the outcome variance (R2 frac14 40 p lt 001) Thecorresponding estimate of explained variance when using baselineto six-month follow-up change on the HAI as outcome was 33(R2 frac14 33 p lt 001) In the final multiple regression models thesignificant predictors were the same irrespective of using end statehealth anxiety or change in health anxiety as dependent variablesBelow results from each predictor domain are presented
Clinical characteristicsBoth when using end state health anxiety at six-month follow-
up and baseline to six-month follow-up change in health anxiety asdependent variable univariate linear regression analyses showedthat baseline health anxiety (HAI) depressive symptoms (MADRS-S) general anxiety (BAI) and anxiety sensitivity (ASI) were signifi-cant predictors The association was negative when using end statehealth anxiety as outcome meaning that higher symptom levels atbaseline predictedmore health anxiety at six-month follow-up Theassociation was positive when using change in health anxiety asdependent variable suggesting that more baseline symptoms inthese areas predicted larger improvements One exception wasdepressive symptoms where higher baseline scores on the MADRS-
S predicted less improvement in health anxiety In addition to thesepredictors results from the univariate analyses showed that havinga comorbid anxiety disorder predicted more health anxiety at six-month follow-up but this factor did not predict change in healthanxiety Years with severe health anxiety concurrent stable psy-chotropic medication with SSRISNRI and comorbid majordepression were not significantly related to outcome
In the final multiple regression model where all significantpredictors above was included in the model baseline health anxi-ety and depressive symptoms remained significant predictorsThus higher levels of health anxiety at baseline predicted morehealth anxiety at six-month follow-up (B frac14 45 SE frac14 13 p lt 001)and larger improvements in health anxiety (B frac14 55 SE frac14 13p lt 001) More depressive symptoms at baseline predicted morehealth anxiety at follow-up (B frac14 153 SE frac14 37 p lt 001) and lessimprovement in health anxiety (B frac14 152 SE frac14 37 p lt 001)
Demographic characteristicsThe only significant predictor from the initial univariate linear
regression was employment status Working full time predictedless symptoms at six-month follow-up but was unrelated tochange in health anxiety None of the other investigated de-mographic variables ie age gender marital status educationallevel and having children or not significantly predicted healthanxiety at six-month follow-up nor change in health anxietyEmployment status did not remain significant in the final multipleregression model
Therapy process-related variablesUnivariate regression analysis showed that more completed
modules predicted both less health anxiety at six-month follow-upand larger improvement in health anxiety Treatment credibilityand computer skills were unrelated to outcome In the final mul-tiple regression analysis number of completedmodules remained asignificant predictor of end state health anxiety (B frac14 154SE frac14 63 p lt 02) and of improvement in health anxiety (B frac14 154SE frac14 64 p lt 02)
Predictors of clinically significant improvement
Clinical characteristicsUnivariate logistic regression showed that more baseline health
anxiety depressive symptoms and general anxiety were associ-ated with a lower chance of being clinically significant improveddefined as an HAI score reduction by at least 17 points and a totalscore below 61 at six-month follow-up Years with severe healthanxiety concurrent stable psychotropic medicationwith SSRISNRIcomorbid depression comorbid anxiety disorder and anxietysensitivity were not significantly related to outcome In the finalmultiple regression model baseline health anxiety (B frac14 06SE frac14 02 p lt 001) and depressive symptoms (B frac14 12 SE frac14 05p lt 02) remained significant predictors of clinical significantimprovement
Demographic variablesThe only significant predictor in this domain was parental sta-
tus ie having children predicted higher probability of being clin-ically significant improved Age gender marital status educationallevel and employment status were unrelated to outcome The finalmultiple regression model retained parental status as a significantpredictor of clinically significant improvement
Therapy process-related factorsNone of the investigated therapy process-related factors ie C-
scale scores number of completed modules and computer skills
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 715
significantly predicted outcome in terms of clinically significantimprovement
Signal detection analysis and decision tree
Fig 1 displays the clinical decision tree including optimal cutoffpoints and receiver operator characteristics using clinically signif-icant improvement as outcome As shown in Fig 1 the analysisyielded a model with two significant interacting predictors in formof baseline health anxiety (HAI) and depressive symptoms(MADRS-S) (c2 frac14 87e134 ps lt 01) The odds ratios ranged from55 to 124 indicating a moderate to large effect of the predictors
Patterns of change from post-treatment to six-month follow-upUsing the criterion for reliable change ie a change score of at
least 17 HAI points 15 (19) of 81 participants made further im-provements in health anxiety between post-treatment and six-month follow-up Univariate logistic regression analyses showedthat less health anxiety change during the treatment and morehealth anxiety at post-treatment was related to a larger chance ofimprovement between post-treatment and six-month follow-up Inthe final logistic regression model health anxiety at post-treatmentremained a significant predictor (B frac14 03 SE frac14 01 p lt 03)
We also investigated patterns of deterioration after the end ofthe treatment period From post-treatment to six-month follow-up8 (10) of the participants reliably increased in their health anxietyHigher levels of health anxiety at post-treatment were associatedwith a reduced risk of making a reliable deterioration to six-monthfollow-up (B frac14 05 SE frac14 02 p lt 02)
Discussion
To the best of our knowledge this study is the first to investigatepredictors of outcome in Internet-based CBT for severe healthanxiety The results showed that the most stable predictors were
Clinical significant impn=42
52 of total sam
Health anxiety at
HAI score ge 108n=11
(29 clinically significant improved)Lowest probability of improvement
MADRS-S score ge 1n=5
(38 clinically significant i
Fig 1 Decision tree of predictors from signal detection analysis Receiver operator character70 (b) Negative predictive value 71 ROC for predictor depressive symptoms at baseliAbbreviations HAI Health anxiety inventory MADRS-S Montgomery Aringsberg Depression R
baseline health anxiety and depressive symptoms As hypothe-sized more health anxiety at baseline predicted more health anx-iety at six-month follow-up but also larger improvements in healthanxiety Signal detection analyses yielded a clinical decision treedemonstrating that a cutoff oflt108 on the HAI (health anxiety) andlt15 on the MADRS-S (depressive symptoms) was optimal toidentify the subgroup participants with the highest probability ofachieving clinically significant improvement The final model usingend state health anxiety as dependent variable showed that theincluded predictors explained 40 of the outcome variance Theexplained variance was slightly lower 33 when baseline to six-month follow-up change in health anxiety was used as outcomeOverall this suggests that it is possible to predict both symptomlevels at longer-term follow-up as well as improvement whichcould be of high value to the clinician when making treatmentrecommendations
When comparing the most powerful predictors baseline healthanxiety and depressive symptoms an interesting different in pre-dictive patterns emerged Persons with more health anxiety beforetreatment made larger improvements in health anxiety while thosewith more depressive symptoms made less improvements inhealth anxiety In our view this indicates that patients with themost severe forms of health anxiety are suitable candidates forInternet-based CBT but it is likely that they will still be having mildto moderate health anxiety after treatment
As for patients with high levels of depressive symptoms atbaseline the picture is slightly more complicated This patientgroup is not only more likely to have more residuals symptoms ofhealth anxiety at follow-up it also has a lower chance of beingimproved We do not generally discourage from using Internet-based CBT if the patient has comorbid depression However thesepersons would benefit from careful monitoring during the treat-ment and the clinician should take additional actions fairly early ifthe patient does not respond to the treatment Although one of theexclusion criteria in the original RCT was scoring higher than 20 on
rovement
ple
baseline
HAI score lt 108n=31
(69 clinically significant improved)
Depressive symptoms at baseline
5
mproved)
MADRS-S score lt 15n=26
(83 clinically significant improved)Highest probability of improvement
istics (ROC) for predictor health anxiety at baseline (HAI) (a) Positive predictive valuene (MADRS-S) (a) Positive predictive value 83 (b) Negative predictive value 62ating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717716
the MADRS-S if being diagnosed with depression it should benoted that no participant was excluded because of it In additionthe mean MADRS-S score of the sample at baseline was above thecutoff indicating depression (Svanborg amp Ekselius 2003) whichmeans that it is probably fair to assume that this sample was notbiased in terms of having too low levels of depressive symptoms Inan analysis of meditators we also found that improvements inhealth anxiety at a given time T during the 12-week treatmentmediated improvement in depressive symptoms at T thorn 1 week(unpublished data)
Demographic variables were largely unrelated to treatmentoutcome with the one exception that having children was associ-ated with a higher chance of achieving clinically significantimprovement (but not with continuous measures of health anxi-ety) Thus it seems that Internet-based CBT suits equally well ifyoung or old man or woman married or unmarried and regardlessif highly educated or not
As for therapy process-related measures the only significantpredictor was number of completedmodules which predicted bothend state symptom levels and change in health anxiety This sug-gests that adherence is important which has been shown also inprevious predictor research on Internet-based CBT for social anxi-ety disorder (Hedman et al 2012) Interestingly computer skillsdid not predict outcome thus replicating findings from priorstudies of Internet-based CBT (Hedman et al 2012) It shouldhowever be noted that participants on average rated their com-putes skill to be high which could reduce the power to detect adifference due to range restriction Taken together with the factthat age was unrelated to outcome this nevertheless suggests thatthe common conception that Internet-based treatments are pri-marily for young persons highly skilled in computer use is likely tobe incorrect
A common question in relatively brief psychological treatmentsis what the chances are of being further improved after the finalsession The analyses of this study showed that as many as 19 ofthe participants made reliable improvements from post-treatmentto six-month follow-up and that health anxiety at post-treatmentsignificantly predicted subsequent improvement This is clinicallyinformative as it means that patients with more post-treatmentresidual symptoms could expect to be further improved
In comparison to prior research on of predictors of conventionalCBT for severe health anxiety the results of this study are similar tothe findings of the study of Nakao et al (2011) which showed thatmore baseline health anxiety predicted larger improvements As inthis study Buwalda and Bouman (2008) found that more baselinehealth anxiety predicted more symptoms at follow-up in groupCBT and Hiller et al (2002) showed that responders had lowerlevels of health anxiety before treatment when investigating pre-dictors of individual CBT Similar to the findings of the study byBuwalda and Bouman (2008) age did not predict outcome at six-month follow-up in the present study although their study founda small negative association between age and health anxiety atpost-treatment Taken together this suggests that prognostic fac-tors are the same in Internet-based CBT for severe health anxiety asin conventional CBT That is for those patients with severe healthanxiety for which face-to-face CBT works Internet-based CBT isalso likely to be effective
This study has some limitations First as participants receivedtreatment within the context of an RCT the use of inclusion criteriaimposed a restriction of range of the predictors This meant that thepersons with the lowest chance of responding to the treatmentwere likely to be excluded eg children or persons with comorbidpsychotic disorders However our general aim when choosing theinclusion criteria was to apply largely the same as we would use inclinical routine care A second limitation was power to detect
predictive factors with less impact However the sample size wassufficient to detect predictors of moderate effect thus representingfactors to be considered useful in a clinical perspective
Considering the strengths of this study ie the high quality ofassessments the standardized treatment format and low attritionrates the findings are important as they show that end state healthanxiety as well as improvement can be predicted in Internet-basedCBT
Financial disclosure
None reported
Funding
This study was funded by Karolinska Institutet and by researchgrants from Stockholm County Council
Role of the sponsor
The main funding organizations (Karolinska Institutet andStockholm County Council) are public institutions and neither ofthe funding organizations had any role in the design and conduct ofthe study in the collection or interpretation of the data nor in thewriting of the report or in the decision to submit it
Conflict of interest
All authors report that they have no competing interests
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mentaldisorders DSM-IV-TR (4th ed) Washington DC American PsychiatricAssociation
Andreescu C Mulsant B H Houck P R Whyte E M Mazumdar SDombrovski A Y et al (2008) Empirically derived decision trees for thetreatment of late-life depression American Journal of Psychiatry 165(7) 855e862 httpdxdoiorg101176appiajp200807081340
Beck A T Epstein N Brown G amp Steer R A (1988) An inventory for measuringclinical anxiety psychometric properties Journal of Consulting and ClinicalPsychology 56(6) 893e897
Borkovec T D amp Nau S D (1972) Credibility of analogue therapy rationalesJournal of Behavior Therapy and Experimental Psychiatry 3(4) 257e260
Buwalda F M amp Bouman T K (2008) Predicting the effect of psychoeducationalgroup treatment for hypochondriasis Journal of Psychology amp Psychotherapy15(6) 396e403 httpdxdoiorg101002cpp602
Buwalda F M Bouman T K amp van Duijn M A (2007) Psychoeducation for hy-pochondriasis a comparison of a cognitive-behavioural approach and aproblem-solving approach Behaviour Research and Therapy 45(5) 887e899httpdxdoiorg101016jbrat200608004
Chambless D L Tran G Q amp Glass C R (1997) Predictors of response tocognitive-behavioral group therapy for social phobia Journal of Anxiety Disor-ders 11(3) 221e240 S0887-6185(97)00008-X
Clark D Salkovskis P Hackmann A Wells A Fennell M Ludgate J et al (1998)Two psychological treatments for hypochondriasis A randomised controlledtrial British Journal of Psychiatry 173(3) 218e225 httpdxdoiorg101192bjp1733218
Devilly G J amp Borkovec T D (2000) Psychometric properties of the credibilityexpectancy questionnaire Journal of Behavior Therapy and Experimental Psy-chiatry 31(2) 73e86
Furer P Walker J R amp Stein M B (2007) Treating health anxiety and fear of deathA practitionerrsquos guide New York NY Springer
de Graaf L E Hollon S D amp Huibers M J (2010) Predicting outcome incomputerized cognitive behavioral therapy for depression in primary care arandomized trial Journal of Consulting and Clinical Psychology 78(2) 184e189doi 2010-05835-005 [pii] 101037a0018324 [doi]
Greeven A van Balkom A J Visser S Merkelbach J W van Rood Y R vanDyck R et al (2007) Cognitive behavior therapy and paroxetine in the treat-ment of hypochondriasis a randomized controlled trial American Journal ofPsychiatry 164(1) 91e99 doi 164191 [pii] 101176appiajp164191
Hedman E Ljoacutetsson B Andersson E Ruumlck C Andersson G amp Lindefors N(2010) Effectiveness and cost offset analysis of group CBT for hypochondriasisdelivered in a psychiatric setting an open trial Cognitive Behaviour Therapy39(4) 239e250 httpdxdoiorg101080165060732010496460
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189

E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717714
subgroups with high and low chance of achieving clinically sig-nificant improvement using the same criteria as above (Andreescuet al 2008 Kraemer Lowe amp Kupfer 2005) Signal detection is aniterative process of splitting the sample in two groups based on theoptimal predictor cut-offs and is suitable when entering manypredictors due to its robustness concerning multicollinearity andoutliers (Kiernan Kraemer Winkleby King amp Taylor 2001) Foreach node in the tree odds ratios were calculated
Analyses of missing data were conducted using Littlersquos Missing-Completely-At-Random test (MCAR Little amp Rubin 1987) Missingdatawere replaced using linear regression imputation based on theavailable covariates When analysing patterns of change aftertreatment we used reliable change (ie an HAI score change of atleast 17 points) as an indicator of whether participants wereimproved or deteriorated between post-treatment and six-monthfollow-up
Results
Attrition and adherence
According to Littlersquos MCAR test data were missing completely atrandom (c(232)2 frac14 22693 plt 58) Therewas no data loss at baselinewhile 79 of 81 (98) participants completed assessments at post-treatment At six-month follow-up 74 of 81 participants (91)completed assessments Participants completed 81 modules(SD frac14 39) on average of a total possible of 12
Brief description of the efficacy of Internet-based CBT
The results of the outcome study showed that the within-groupeffect sizes were large on the primary outcome measure HAI atpost-treatment (d frac14 169 95CI frac14 132e204) and six-monthfollow-up (d frac14 190 95CI frac14 152e227) compared to baselineMixed effects models analysis showed that there was a significanteffect of time on the HAI from baseline to six-month follow-up(F frac14 131 df frac14 145 p lt 001) Of the 81 participants 42 (52) metthe criteria for clinically significant improvement at six-monthfollow-up
Predictors of end state health anxiety and improvement
Significant predictors of end state health anxiety (HAI) at six-month follow-up from the final multiple linear regression modelexplained 40 of the outcome variance (R2 frac14 40 p lt 001) Thecorresponding estimate of explained variance when using baselineto six-month follow-up change on the HAI as outcome was 33(R2 frac14 33 p lt 001) In the final multiple regression models thesignificant predictors were the same irrespective of using end statehealth anxiety or change in health anxiety as dependent variablesBelow results from each predictor domain are presented
Clinical characteristicsBoth when using end state health anxiety at six-month follow-
up and baseline to six-month follow-up change in health anxiety asdependent variable univariate linear regression analyses showedthat baseline health anxiety (HAI) depressive symptoms (MADRS-S) general anxiety (BAI) and anxiety sensitivity (ASI) were signifi-cant predictors The association was negative when using end statehealth anxiety as outcome meaning that higher symptom levels atbaseline predictedmore health anxiety at six-month follow-up Theassociation was positive when using change in health anxiety asdependent variable suggesting that more baseline symptoms inthese areas predicted larger improvements One exception wasdepressive symptoms where higher baseline scores on the MADRS-
S predicted less improvement in health anxiety In addition to thesepredictors results from the univariate analyses showed that havinga comorbid anxiety disorder predicted more health anxiety at six-month follow-up but this factor did not predict change in healthanxiety Years with severe health anxiety concurrent stable psy-chotropic medication with SSRISNRI and comorbid majordepression were not significantly related to outcome
In the final multiple regression model where all significantpredictors above was included in the model baseline health anxi-ety and depressive symptoms remained significant predictorsThus higher levels of health anxiety at baseline predicted morehealth anxiety at six-month follow-up (B frac14 45 SE frac14 13 p lt 001)and larger improvements in health anxiety (B frac14 55 SE frac14 13p lt 001) More depressive symptoms at baseline predicted morehealth anxiety at follow-up (B frac14 153 SE frac14 37 p lt 001) and lessimprovement in health anxiety (B frac14 152 SE frac14 37 p lt 001)
Demographic characteristicsThe only significant predictor from the initial univariate linear
regression was employment status Working full time predictedless symptoms at six-month follow-up but was unrelated tochange in health anxiety None of the other investigated de-mographic variables ie age gender marital status educationallevel and having children or not significantly predicted healthanxiety at six-month follow-up nor change in health anxietyEmployment status did not remain significant in the final multipleregression model
Therapy process-related variablesUnivariate regression analysis showed that more completed
modules predicted both less health anxiety at six-month follow-upand larger improvement in health anxiety Treatment credibilityand computer skills were unrelated to outcome In the final mul-tiple regression analysis number of completedmodules remained asignificant predictor of end state health anxiety (B frac14 154SE frac14 63 p lt 02) and of improvement in health anxiety (B frac14 154SE frac14 64 p lt 02)
Predictors of clinically significant improvement
Clinical characteristicsUnivariate logistic regression showed that more baseline health
anxiety depressive symptoms and general anxiety were associ-ated with a lower chance of being clinically significant improveddefined as an HAI score reduction by at least 17 points and a totalscore below 61 at six-month follow-up Years with severe healthanxiety concurrent stable psychotropic medicationwith SSRISNRIcomorbid depression comorbid anxiety disorder and anxietysensitivity were not significantly related to outcome In the finalmultiple regression model baseline health anxiety (B frac14 06SE frac14 02 p lt 001) and depressive symptoms (B frac14 12 SE frac14 05p lt 02) remained significant predictors of clinical significantimprovement
Demographic variablesThe only significant predictor in this domain was parental sta-
tus ie having children predicted higher probability of being clin-ically significant improved Age gender marital status educationallevel and employment status were unrelated to outcome The finalmultiple regression model retained parental status as a significantpredictor of clinically significant improvement
Therapy process-related factorsNone of the investigated therapy process-related factors ie C-
scale scores number of completed modules and computer skills
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 715
significantly predicted outcome in terms of clinically significantimprovement
Signal detection analysis and decision tree
Fig 1 displays the clinical decision tree including optimal cutoffpoints and receiver operator characteristics using clinically signif-icant improvement as outcome As shown in Fig 1 the analysisyielded a model with two significant interacting predictors in formof baseline health anxiety (HAI) and depressive symptoms(MADRS-S) (c2 frac14 87e134 ps lt 01) The odds ratios ranged from55 to 124 indicating a moderate to large effect of the predictors
Patterns of change from post-treatment to six-month follow-upUsing the criterion for reliable change ie a change score of at
least 17 HAI points 15 (19) of 81 participants made further im-provements in health anxiety between post-treatment and six-month follow-up Univariate logistic regression analyses showedthat less health anxiety change during the treatment and morehealth anxiety at post-treatment was related to a larger chance ofimprovement between post-treatment and six-month follow-up Inthe final logistic regression model health anxiety at post-treatmentremained a significant predictor (B frac14 03 SE frac14 01 p lt 03)
We also investigated patterns of deterioration after the end ofthe treatment period From post-treatment to six-month follow-up8 (10) of the participants reliably increased in their health anxietyHigher levels of health anxiety at post-treatment were associatedwith a reduced risk of making a reliable deterioration to six-monthfollow-up (B frac14 05 SE frac14 02 p lt 02)
Discussion
To the best of our knowledge this study is the first to investigatepredictors of outcome in Internet-based CBT for severe healthanxiety The results showed that the most stable predictors were
Clinical significant impn=42
52 of total sam
Health anxiety at
HAI score ge 108n=11
(29 clinically significant improved)Lowest probability of improvement
MADRS-S score ge 1n=5
(38 clinically significant i
Fig 1 Decision tree of predictors from signal detection analysis Receiver operator character70 (b) Negative predictive value 71 ROC for predictor depressive symptoms at baseliAbbreviations HAI Health anxiety inventory MADRS-S Montgomery Aringsberg Depression R
baseline health anxiety and depressive symptoms As hypothe-sized more health anxiety at baseline predicted more health anx-iety at six-month follow-up but also larger improvements in healthanxiety Signal detection analyses yielded a clinical decision treedemonstrating that a cutoff oflt108 on the HAI (health anxiety) andlt15 on the MADRS-S (depressive symptoms) was optimal toidentify the subgroup participants with the highest probability ofachieving clinically significant improvement The final model usingend state health anxiety as dependent variable showed that theincluded predictors explained 40 of the outcome variance Theexplained variance was slightly lower 33 when baseline to six-month follow-up change in health anxiety was used as outcomeOverall this suggests that it is possible to predict both symptomlevels at longer-term follow-up as well as improvement whichcould be of high value to the clinician when making treatmentrecommendations
When comparing the most powerful predictors baseline healthanxiety and depressive symptoms an interesting different in pre-dictive patterns emerged Persons with more health anxiety beforetreatment made larger improvements in health anxiety while thosewith more depressive symptoms made less improvements inhealth anxiety In our view this indicates that patients with themost severe forms of health anxiety are suitable candidates forInternet-based CBT but it is likely that they will still be having mildto moderate health anxiety after treatment
As for patients with high levels of depressive symptoms atbaseline the picture is slightly more complicated This patientgroup is not only more likely to have more residuals symptoms ofhealth anxiety at follow-up it also has a lower chance of beingimproved We do not generally discourage from using Internet-based CBT if the patient has comorbid depression However thesepersons would benefit from careful monitoring during the treat-ment and the clinician should take additional actions fairly early ifthe patient does not respond to the treatment Although one of theexclusion criteria in the original RCT was scoring higher than 20 on
rovement
ple
baseline
HAI score lt 108n=31
(69 clinically significant improved)
Depressive symptoms at baseline
5
mproved)
MADRS-S score lt 15n=26
(83 clinically significant improved)Highest probability of improvement
istics (ROC) for predictor health anxiety at baseline (HAI) (a) Positive predictive valuene (MADRS-S) (a) Positive predictive value 83 (b) Negative predictive value 62ating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717716
the MADRS-S if being diagnosed with depression it should benoted that no participant was excluded because of it In additionthe mean MADRS-S score of the sample at baseline was above thecutoff indicating depression (Svanborg amp Ekselius 2003) whichmeans that it is probably fair to assume that this sample was notbiased in terms of having too low levels of depressive symptoms Inan analysis of meditators we also found that improvements inhealth anxiety at a given time T during the 12-week treatmentmediated improvement in depressive symptoms at T thorn 1 week(unpublished data)
Demographic variables were largely unrelated to treatmentoutcome with the one exception that having children was associ-ated with a higher chance of achieving clinically significantimprovement (but not with continuous measures of health anxi-ety) Thus it seems that Internet-based CBT suits equally well ifyoung or old man or woman married or unmarried and regardlessif highly educated or not
As for therapy process-related measures the only significantpredictor was number of completedmodules which predicted bothend state symptom levels and change in health anxiety This sug-gests that adherence is important which has been shown also inprevious predictor research on Internet-based CBT for social anxi-ety disorder (Hedman et al 2012) Interestingly computer skillsdid not predict outcome thus replicating findings from priorstudies of Internet-based CBT (Hedman et al 2012) It shouldhowever be noted that participants on average rated their com-putes skill to be high which could reduce the power to detect adifference due to range restriction Taken together with the factthat age was unrelated to outcome this nevertheless suggests thatthe common conception that Internet-based treatments are pri-marily for young persons highly skilled in computer use is likely tobe incorrect
A common question in relatively brief psychological treatmentsis what the chances are of being further improved after the finalsession The analyses of this study showed that as many as 19 ofthe participants made reliable improvements from post-treatmentto six-month follow-up and that health anxiety at post-treatmentsignificantly predicted subsequent improvement This is clinicallyinformative as it means that patients with more post-treatmentresidual symptoms could expect to be further improved
In comparison to prior research on of predictors of conventionalCBT for severe health anxiety the results of this study are similar tothe findings of the study of Nakao et al (2011) which showed thatmore baseline health anxiety predicted larger improvements As inthis study Buwalda and Bouman (2008) found that more baselinehealth anxiety predicted more symptoms at follow-up in groupCBT and Hiller et al (2002) showed that responders had lowerlevels of health anxiety before treatment when investigating pre-dictors of individual CBT Similar to the findings of the study byBuwalda and Bouman (2008) age did not predict outcome at six-month follow-up in the present study although their study founda small negative association between age and health anxiety atpost-treatment Taken together this suggests that prognostic fac-tors are the same in Internet-based CBT for severe health anxiety asin conventional CBT That is for those patients with severe healthanxiety for which face-to-face CBT works Internet-based CBT isalso likely to be effective
This study has some limitations First as participants receivedtreatment within the context of an RCT the use of inclusion criteriaimposed a restriction of range of the predictors This meant that thepersons with the lowest chance of responding to the treatmentwere likely to be excluded eg children or persons with comorbidpsychotic disorders However our general aim when choosing theinclusion criteria was to apply largely the same as we would use inclinical routine care A second limitation was power to detect
predictive factors with less impact However the sample size wassufficient to detect predictors of moderate effect thus representingfactors to be considered useful in a clinical perspective
Considering the strengths of this study ie the high quality ofassessments the standardized treatment format and low attritionrates the findings are important as they show that end state healthanxiety as well as improvement can be predicted in Internet-basedCBT
Financial disclosure
None reported
Funding
This study was funded by Karolinska Institutet and by researchgrants from Stockholm County Council
Role of the sponsor
The main funding organizations (Karolinska Institutet andStockholm County Council) are public institutions and neither ofthe funding organizations had any role in the design and conduct ofthe study in the collection or interpretation of the data nor in thewriting of the report or in the decision to submit it
Conflict of interest
All authors report that they have no competing interests
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mentaldisorders DSM-IV-TR (4th ed) Washington DC American PsychiatricAssociation
Andreescu C Mulsant B H Houck P R Whyte E M Mazumdar SDombrovski A Y et al (2008) Empirically derived decision trees for thetreatment of late-life depression American Journal of Psychiatry 165(7) 855e862 httpdxdoiorg101176appiajp200807081340
Beck A T Epstein N Brown G amp Steer R A (1988) An inventory for measuringclinical anxiety psychometric properties Journal of Consulting and ClinicalPsychology 56(6) 893e897
Borkovec T D amp Nau S D (1972) Credibility of analogue therapy rationalesJournal of Behavior Therapy and Experimental Psychiatry 3(4) 257e260
Buwalda F M amp Bouman T K (2008) Predicting the effect of psychoeducationalgroup treatment for hypochondriasis Journal of Psychology amp Psychotherapy15(6) 396e403 httpdxdoiorg101002cpp602
Buwalda F M Bouman T K amp van Duijn M A (2007) Psychoeducation for hy-pochondriasis a comparison of a cognitive-behavioural approach and aproblem-solving approach Behaviour Research and Therapy 45(5) 887e899httpdxdoiorg101016jbrat200608004
Chambless D L Tran G Q amp Glass C R (1997) Predictors of response tocognitive-behavioral group therapy for social phobia Journal of Anxiety Disor-ders 11(3) 221e240 S0887-6185(97)00008-X
Clark D Salkovskis P Hackmann A Wells A Fennell M Ludgate J et al (1998)Two psychological treatments for hypochondriasis A randomised controlledtrial British Journal of Psychiatry 173(3) 218e225 httpdxdoiorg101192bjp1733218
Devilly G J amp Borkovec T D (2000) Psychometric properties of the credibilityexpectancy questionnaire Journal of Behavior Therapy and Experimental Psy-chiatry 31(2) 73e86
Furer P Walker J R amp Stein M B (2007) Treating health anxiety and fear of deathA practitionerrsquos guide New York NY Springer
de Graaf L E Hollon S D amp Huibers M J (2010) Predicting outcome incomputerized cognitive behavioral therapy for depression in primary care arandomized trial Journal of Consulting and Clinical Psychology 78(2) 184e189doi 2010-05835-005 [pii] 101037a0018324 [doi]
Greeven A van Balkom A J Visser S Merkelbach J W van Rood Y R vanDyck R et al (2007) Cognitive behavior therapy and paroxetine in the treat-ment of hypochondriasis a randomized controlled trial American Journal ofPsychiatry 164(1) 91e99 doi 164191 [pii] 101176appiajp164191
Hedman E Ljoacutetsson B Andersson E Ruumlck C Andersson G amp Lindefors N(2010) Effectiveness and cost offset analysis of group CBT for hypochondriasisdelivered in a psychiatric setting an open trial Cognitive Behaviour Therapy39(4) 239e250 httpdxdoiorg101080165060732010496460
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189
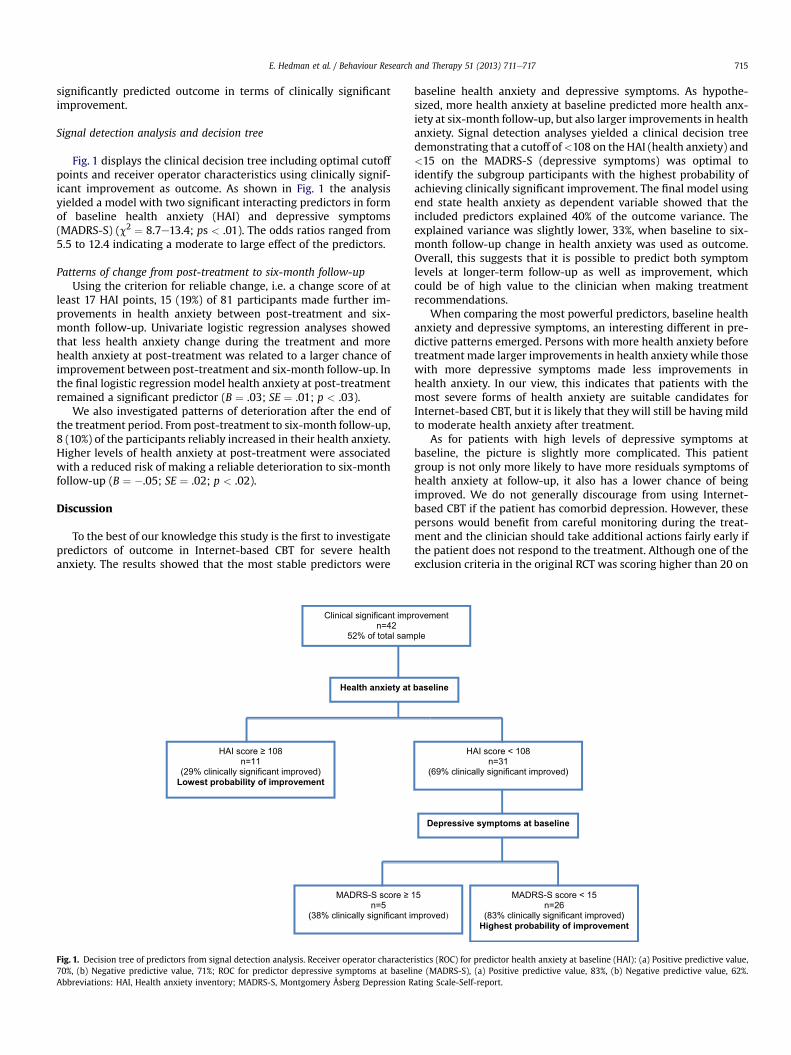
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 715
significantly predicted outcome in terms of clinically significantimprovement
Signal detection analysis and decision tree
Fig 1 displays the clinical decision tree including optimal cutoffpoints and receiver operator characteristics using clinically signif-icant improvement as outcome As shown in Fig 1 the analysisyielded a model with two significant interacting predictors in formof baseline health anxiety (HAI) and depressive symptoms(MADRS-S) (c2 frac14 87e134 ps lt 01) The odds ratios ranged from55 to 124 indicating a moderate to large effect of the predictors
Patterns of change from post-treatment to six-month follow-upUsing the criterion for reliable change ie a change score of at
least 17 HAI points 15 (19) of 81 participants made further im-provements in health anxiety between post-treatment and six-month follow-up Univariate logistic regression analyses showedthat less health anxiety change during the treatment and morehealth anxiety at post-treatment was related to a larger chance ofimprovement between post-treatment and six-month follow-up Inthe final logistic regression model health anxiety at post-treatmentremained a significant predictor (B frac14 03 SE frac14 01 p lt 03)
We also investigated patterns of deterioration after the end ofthe treatment period From post-treatment to six-month follow-up8 (10) of the participants reliably increased in their health anxietyHigher levels of health anxiety at post-treatment were associatedwith a reduced risk of making a reliable deterioration to six-monthfollow-up (B frac14 05 SE frac14 02 p lt 02)
Discussion
To the best of our knowledge this study is the first to investigatepredictors of outcome in Internet-based CBT for severe healthanxiety The results showed that the most stable predictors were
Clinical significant impn=42
52 of total sam
Health anxiety at
HAI score ge 108n=11
(29 clinically significant improved)Lowest probability of improvement
MADRS-S score ge 1n=5
(38 clinically significant i
Fig 1 Decision tree of predictors from signal detection analysis Receiver operator character70 (b) Negative predictive value 71 ROC for predictor depressive symptoms at baseliAbbreviations HAI Health anxiety inventory MADRS-S Montgomery Aringsberg Depression R
baseline health anxiety and depressive symptoms As hypothe-sized more health anxiety at baseline predicted more health anx-iety at six-month follow-up but also larger improvements in healthanxiety Signal detection analyses yielded a clinical decision treedemonstrating that a cutoff oflt108 on the HAI (health anxiety) andlt15 on the MADRS-S (depressive symptoms) was optimal toidentify the subgroup participants with the highest probability ofachieving clinically significant improvement The final model usingend state health anxiety as dependent variable showed that theincluded predictors explained 40 of the outcome variance Theexplained variance was slightly lower 33 when baseline to six-month follow-up change in health anxiety was used as outcomeOverall this suggests that it is possible to predict both symptomlevels at longer-term follow-up as well as improvement whichcould be of high value to the clinician when making treatmentrecommendations
When comparing the most powerful predictors baseline healthanxiety and depressive symptoms an interesting different in pre-dictive patterns emerged Persons with more health anxiety beforetreatment made larger improvements in health anxiety while thosewith more depressive symptoms made less improvements inhealth anxiety In our view this indicates that patients with themost severe forms of health anxiety are suitable candidates forInternet-based CBT but it is likely that they will still be having mildto moderate health anxiety after treatment
As for patients with high levels of depressive symptoms atbaseline the picture is slightly more complicated This patientgroup is not only more likely to have more residuals symptoms ofhealth anxiety at follow-up it also has a lower chance of beingimproved We do not generally discourage from using Internet-based CBT if the patient has comorbid depression However thesepersons would benefit from careful monitoring during the treat-ment and the clinician should take additional actions fairly early ifthe patient does not respond to the treatment Although one of theexclusion criteria in the original RCT was scoring higher than 20 on
rovement
ple
baseline
HAI score lt 108n=31
(69 clinically significant improved)
Depressive symptoms at baseline
5
mproved)
MADRS-S score lt 15n=26
(83 clinically significant improved)Highest probability of improvement
istics (ROC) for predictor health anxiety at baseline (HAI) (a) Positive predictive valuene (MADRS-S) (a) Positive predictive value 83 (b) Negative predictive value 62ating Scale-Self-report
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717716
the MADRS-S if being diagnosed with depression it should benoted that no participant was excluded because of it In additionthe mean MADRS-S score of the sample at baseline was above thecutoff indicating depression (Svanborg amp Ekselius 2003) whichmeans that it is probably fair to assume that this sample was notbiased in terms of having too low levels of depressive symptoms Inan analysis of meditators we also found that improvements inhealth anxiety at a given time T during the 12-week treatmentmediated improvement in depressive symptoms at T thorn 1 week(unpublished data)
Demographic variables were largely unrelated to treatmentoutcome with the one exception that having children was associ-ated with a higher chance of achieving clinically significantimprovement (but not with continuous measures of health anxi-ety) Thus it seems that Internet-based CBT suits equally well ifyoung or old man or woman married or unmarried and regardlessif highly educated or not
As for therapy process-related measures the only significantpredictor was number of completedmodules which predicted bothend state symptom levels and change in health anxiety This sug-gests that adherence is important which has been shown also inprevious predictor research on Internet-based CBT for social anxi-ety disorder (Hedman et al 2012) Interestingly computer skillsdid not predict outcome thus replicating findings from priorstudies of Internet-based CBT (Hedman et al 2012) It shouldhowever be noted that participants on average rated their com-putes skill to be high which could reduce the power to detect adifference due to range restriction Taken together with the factthat age was unrelated to outcome this nevertheless suggests thatthe common conception that Internet-based treatments are pri-marily for young persons highly skilled in computer use is likely tobe incorrect
A common question in relatively brief psychological treatmentsis what the chances are of being further improved after the finalsession The analyses of this study showed that as many as 19 ofthe participants made reliable improvements from post-treatmentto six-month follow-up and that health anxiety at post-treatmentsignificantly predicted subsequent improvement This is clinicallyinformative as it means that patients with more post-treatmentresidual symptoms could expect to be further improved
In comparison to prior research on of predictors of conventionalCBT for severe health anxiety the results of this study are similar tothe findings of the study of Nakao et al (2011) which showed thatmore baseline health anxiety predicted larger improvements As inthis study Buwalda and Bouman (2008) found that more baselinehealth anxiety predicted more symptoms at follow-up in groupCBT and Hiller et al (2002) showed that responders had lowerlevels of health anxiety before treatment when investigating pre-dictors of individual CBT Similar to the findings of the study byBuwalda and Bouman (2008) age did not predict outcome at six-month follow-up in the present study although their study founda small negative association between age and health anxiety atpost-treatment Taken together this suggests that prognostic fac-tors are the same in Internet-based CBT for severe health anxiety asin conventional CBT That is for those patients with severe healthanxiety for which face-to-face CBT works Internet-based CBT isalso likely to be effective
This study has some limitations First as participants receivedtreatment within the context of an RCT the use of inclusion criteriaimposed a restriction of range of the predictors This meant that thepersons with the lowest chance of responding to the treatmentwere likely to be excluded eg children or persons with comorbidpsychotic disorders However our general aim when choosing theinclusion criteria was to apply largely the same as we would use inclinical routine care A second limitation was power to detect
predictive factors with less impact However the sample size wassufficient to detect predictors of moderate effect thus representingfactors to be considered useful in a clinical perspective
Considering the strengths of this study ie the high quality ofassessments the standardized treatment format and low attritionrates the findings are important as they show that end state healthanxiety as well as improvement can be predicted in Internet-basedCBT
Financial disclosure
None reported
Funding
This study was funded by Karolinska Institutet and by researchgrants from Stockholm County Council
Role of the sponsor
The main funding organizations (Karolinska Institutet andStockholm County Council) are public institutions and neither ofthe funding organizations had any role in the design and conduct ofthe study in the collection or interpretation of the data nor in thewriting of the report or in the decision to submit it
Conflict of interest
All authors report that they have no competing interests
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mentaldisorders DSM-IV-TR (4th ed) Washington DC American PsychiatricAssociation
Andreescu C Mulsant B H Houck P R Whyte E M Mazumdar SDombrovski A Y et al (2008) Empirically derived decision trees for thetreatment of late-life depression American Journal of Psychiatry 165(7) 855e862 httpdxdoiorg101176appiajp200807081340
Beck A T Epstein N Brown G amp Steer R A (1988) An inventory for measuringclinical anxiety psychometric properties Journal of Consulting and ClinicalPsychology 56(6) 893e897
Borkovec T D amp Nau S D (1972) Credibility of analogue therapy rationalesJournal of Behavior Therapy and Experimental Psychiatry 3(4) 257e260
Buwalda F M amp Bouman T K (2008) Predicting the effect of psychoeducationalgroup treatment for hypochondriasis Journal of Psychology amp Psychotherapy15(6) 396e403 httpdxdoiorg101002cpp602
Buwalda F M Bouman T K amp van Duijn M A (2007) Psychoeducation for hy-pochondriasis a comparison of a cognitive-behavioural approach and aproblem-solving approach Behaviour Research and Therapy 45(5) 887e899httpdxdoiorg101016jbrat200608004
Chambless D L Tran G Q amp Glass C R (1997) Predictors of response tocognitive-behavioral group therapy for social phobia Journal of Anxiety Disor-ders 11(3) 221e240 S0887-6185(97)00008-X
Clark D Salkovskis P Hackmann A Wells A Fennell M Ludgate J et al (1998)Two psychological treatments for hypochondriasis A randomised controlledtrial British Journal of Psychiatry 173(3) 218e225 httpdxdoiorg101192bjp1733218
Devilly G J amp Borkovec T D (2000) Psychometric properties of the credibilityexpectancy questionnaire Journal of Behavior Therapy and Experimental Psy-chiatry 31(2) 73e86
Furer P Walker J R amp Stein M B (2007) Treating health anxiety and fear of deathA practitionerrsquos guide New York NY Springer
de Graaf L E Hollon S D amp Huibers M J (2010) Predicting outcome incomputerized cognitive behavioral therapy for depression in primary care arandomized trial Journal of Consulting and Clinical Psychology 78(2) 184e189doi 2010-05835-005 [pii] 101037a0018324 [doi]
Greeven A van Balkom A J Visser S Merkelbach J W van Rood Y R vanDyck R et al (2007) Cognitive behavior therapy and paroxetine in the treat-ment of hypochondriasis a randomized controlled trial American Journal ofPsychiatry 164(1) 91e99 doi 164191 [pii] 101176appiajp164191
Hedman E Ljoacutetsson B Andersson E Ruumlck C Andersson G amp Lindefors N(2010) Effectiveness and cost offset analysis of group CBT for hypochondriasisdelivered in a psychiatric setting an open trial Cognitive Behaviour Therapy39(4) 239e250 httpdxdoiorg101080165060732010496460
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189

E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717716
the MADRS-S if being diagnosed with depression it should benoted that no participant was excluded because of it In additionthe mean MADRS-S score of the sample at baseline was above thecutoff indicating depression (Svanborg amp Ekselius 2003) whichmeans that it is probably fair to assume that this sample was notbiased in terms of having too low levels of depressive symptoms Inan analysis of meditators we also found that improvements inhealth anxiety at a given time T during the 12-week treatmentmediated improvement in depressive symptoms at T thorn 1 week(unpublished data)
Demographic variables were largely unrelated to treatmentoutcome with the one exception that having children was associ-ated with a higher chance of achieving clinically significantimprovement (but not with continuous measures of health anxi-ety) Thus it seems that Internet-based CBT suits equally well ifyoung or old man or woman married or unmarried and regardlessif highly educated or not
As for therapy process-related measures the only significantpredictor was number of completedmodules which predicted bothend state symptom levels and change in health anxiety This sug-gests that adherence is important which has been shown also inprevious predictor research on Internet-based CBT for social anxi-ety disorder (Hedman et al 2012) Interestingly computer skillsdid not predict outcome thus replicating findings from priorstudies of Internet-based CBT (Hedman et al 2012) It shouldhowever be noted that participants on average rated their com-putes skill to be high which could reduce the power to detect adifference due to range restriction Taken together with the factthat age was unrelated to outcome this nevertheless suggests thatthe common conception that Internet-based treatments are pri-marily for young persons highly skilled in computer use is likely tobe incorrect
A common question in relatively brief psychological treatmentsis what the chances are of being further improved after the finalsession The analyses of this study showed that as many as 19 ofthe participants made reliable improvements from post-treatmentto six-month follow-up and that health anxiety at post-treatmentsignificantly predicted subsequent improvement This is clinicallyinformative as it means that patients with more post-treatmentresidual symptoms could expect to be further improved
In comparison to prior research on of predictors of conventionalCBT for severe health anxiety the results of this study are similar tothe findings of the study of Nakao et al (2011) which showed thatmore baseline health anxiety predicted larger improvements As inthis study Buwalda and Bouman (2008) found that more baselinehealth anxiety predicted more symptoms at follow-up in groupCBT and Hiller et al (2002) showed that responders had lowerlevels of health anxiety before treatment when investigating pre-dictors of individual CBT Similar to the findings of the study byBuwalda and Bouman (2008) age did not predict outcome at six-month follow-up in the present study although their study founda small negative association between age and health anxiety atpost-treatment Taken together this suggests that prognostic fac-tors are the same in Internet-based CBT for severe health anxiety asin conventional CBT That is for those patients with severe healthanxiety for which face-to-face CBT works Internet-based CBT isalso likely to be effective
This study has some limitations First as participants receivedtreatment within the context of an RCT the use of inclusion criteriaimposed a restriction of range of the predictors This meant that thepersons with the lowest chance of responding to the treatmentwere likely to be excluded eg children or persons with comorbidpsychotic disorders However our general aim when choosing theinclusion criteria was to apply largely the same as we would use inclinical routine care A second limitation was power to detect
predictive factors with less impact However the sample size wassufficient to detect predictors of moderate effect thus representingfactors to be considered useful in a clinical perspective
Considering the strengths of this study ie the high quality ofassessments the standardized treatment format and low attritionrates the findings are important as they show that end state healthanxiety as well as improvement can be predicted in Internet-basedCBT
Financial disclosure
None reported
Funding
This study was funded by Karolinska Institutet and by researchgrants from Stockholm County Council
Role of the sponsor
The main funding organizations (Karolinska Institutet andStockholm County Council) are public institutions and neither ofthe funding organizations had any role in the design and conduct ofthe study in the collection or interpretation of the data nor in thewriting of the report or in the decision to submit it
Conflict of interest
All authors report that they have no competing interests
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mentaldisorders DSM-IV-TR (4th ed) Washington DC American PsychiatricAssociation
Andreescu C Mulsant B H Houck P R Whyte E M Mazumdar SDombrovski A Y et al (2008) Empirically derived decision trees for thetreatment of late-life depression American Journal of Psychiatry 165(7) 855e862 httpdxdoiorg101176appiajp200807081340
Beck A T Epstein N Brown G amp Steer R A (1988) An inventory for measuringclinical anxiety psychometric properties Journal of Consulting and ClinicalPsychology 56(6) 893e897
Borkovec T D amp Nau S D (1972) Credibility of analogue therapy rationalesJournal of Behavior Therapy and Experimental Psychiatry 3(4) 257e260
Buwalda F M amp Bouman T K (2008) Predicting the effect of psychoeducationalgroup treatment for hypochondriasis Journal of Psychology amp Psychotherapy15(6) 396e403 httpdxdoiorg101002cpp602
Buwalda F M Bouman T K amp van Duijn M A (2007) Psychoeducation for hy-pochondriasis a comparison of a cognitive-behavioural approach and aproblem-solving approach Behaviour Research and Therapy 45(5) 887e899httpdxdoiorg101016jbrat200608004
Chambless D L Tran G Q amp Glass C R (1997) Predictors of response tocognitive-behavioral group therapy for social phobia Journal of Anxiety Disor-ders 11(3) 221e240 S0887-6185(97)00008-X
Clark D Salkovskis P Hackmann A Wells A Fennell M Ludgate J et al (1998)Two psychological treatments for hypochondriasis A randomised controlledtrial British Journal of Psychiatry 173(3) 218e225 httpdxdoiorg101192bjp1733218
Devilly G J amp Borkovec T D (2000) Psychometric properties of the credibilityexpectancy questionnaire Journal of Behavior Therapy and Experimental Psy-chiatry 31(2) 73e86
Furer P Walker J R amp Stein M B (2007) Treating health anxiety and fear of deathA practitionerrsquos guide New York NY Springer
de Graaf L E Hollon S D amp Huibers M J (2010) Predicting outcome incomputerized cognitive behavioral therapy for depression in primary care arandomized trial Journal of Consulting and Clinical Psychology 78(2) 184e189doi 2010-05835-005 [pii] 101037a0018324 [doi]
Greeven A van Balkom A J Visser S Merkelbach J W van Rood Y R vanDyck R et al (2007) Cognitive behavior therapy and paroxetine in the treat-ment of hypochondriasis a randomized controlled trial American Journal ofPsychiatry 164(1) 91e99 doi 164191 [pii] 101176appiajp164191
Hedman E Ljoacutetsson B Andersson E Ruumlck C Andersson G amp Lindefors N(2010) Effectiveness and cost offset analysis of group CBT for hypochondriasisdelivered in a psychiatric setting an open trial Cognitive Behaviour Therapy39(4) 239e250 httpdxdoiorg101080165060732010496460
E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189

E Hedman et al Behaviour Research and Therapy 51 (2013) 711e717 717
Hedman E Ljoacutetsson B Ruumlck C Furmark T Carlbring P Lindefors N et al(2010) Internet administration of self-report measures commonly used inresearch on social anxiety disorder a psychometric evaluation Computers inHuman Behavior 26 736e740
Hedman E Andersson G Andersson E Ljotsson B Ruck C Asmundson G Jet al (2011) Internet-based cognitive-behavioural therapy for severe healthanxiety randomised controlled trial British Journal of Psychiatry 198 230e236doi 1983230 [pii] 101192bjpbp110086843 [doi]
Hedman E Andersson E Ljotsson B Andersson G Andersson E Schalling Met al (2012) Clinical and genetic outcome determinants of Internet- and group-based cognitive behavior therapy for social anxiety disorder Acta PsychiatricaScandinavica 126(2) 126e136 httpdxdoiorg101111j1600-0447201201834x
Hedman E Ljotsson B Ruck C Bergstrom J Andersson G Kaldo V et al(2013) Effectiveness of Internet-based cognitive behaviour therapy for panicdisorder in routine psychiatric care Acta Psychiatrica Scandinavica httpdxdoiorg101111acps12079
Hiller W Leibbrand R Rief W amp Fichter M M (2002) Predictors of course andoutcome in hypochondriasis after cognitive-behavioral treatment Psychother-apy and Psychosomatics 71(6) 318e325 doi 65990
Jacobson N S amp Truax P (1991) Clinical significance a statistical approach todefining meaningful change in psychotherapy research Journal of Consultingand Clinical Psychology 59(1) 12e19
Keijsers G P Hoogduin C A amp Schaap C P (1994) Predictors of treatmentoutcome in the behavioural treatment of obsessive-compulsive disorder BritishJournal of Psychiatry 165(6) 781e786
Kiernan M Kraemer H C Winkleby M A King A C amp Taylor C B (2001) Dologistic regression and signal detection identify different subgroups at riskImplications for the design of tailored interventions Psychological Methods6(1) 35e48
Kraemer H C Wilson G T Fairburn C G amp Agras W S (2002) Mediators andmoderators of treatment effects in randomized clinical trials Archives of GeneralPsychiatry 59(10) 877e883 doi ynv10179 [pii]
Kraemer H C Lowe K K amp Kupfer D J (2005) To your health New York OxfordUniversity Press
Little R J A amp Rubin D B (1987) Statistical analysis with missing data New YorkWiley
Mausbach B T Moore R Roesch S Cardenas V amp Patterson T L (2010) Therelationship between homework compliance and therapy outcomes an upda-ted meta-analysis Cognitive Therapy and Research 34(5) 429e438 httpdxdoiorg101007s10608-010-9297-z
Nakao M Shinozaki Y Ahern D K amp Barsky A J (2011) Anxiety as a predictor ofimprovements in somatic symptoms and health anxiety associated with
cognitive-behavioral intervention in hypochondriasis Psychotherapy and Psy-chosomatics 80(3) 151e158 httpdxdoiorg101159000320122
Nordgreen T Havik O E Ost L G Furmark T Carlbring P amp Andersson G(2012) Outcome predictors in guided and unguided self-help for social anxietydisorder Behaviour Research and Therapy 50(1) 13e21 httpdxdoiorg101016jbrat201110009
Reiss S Peterson R A Gursky D M amp McNally R J (1986) Anxiety sensitivityanxiety frequency and the prediction of fearfulness Behaviour Research andTherapy 24(1) 1e8 doi 0005-7967(86)90143-9 [pii]
Salkovskis P M Rimes K A Warwick H M amp Clark D M (2002) The healthanxiety Inventory development and validation of scales for the measurementof health anxiety and hypochondriasis Psychological Medicine 32(5) 843e853
Seivewright H Green J Salkovskis P Barrett B Nur U amp Tyrer P (2008)Cognitive-behavioural therapy for health anxiety in a genitourinary medicineclinic randomised controlled trial British Journal of Psychiatry 193(4) 332e337doi 1934332 [pii] 101192bjpbp108052936 [doi]
Sheehan D V Lecrubier Y Sheehan K H Amorim P Janavs J Weiller E et al(1998) The Mini-International Neuropsychiatric Interview (MINI) thedevelopment and validation of a structured diagnostic psychiatric interview forDSM-IV and ICD-10 Journal of Clinical Psychiatry 59(Suppl 20)
Sorensen P Birket-Smith M Wattar U Buemann I amp Salkovskis P (2011)A randomized clinical trial of cognitive behavioural therapy versus short-termpsychodynamic psychotherapy versus no intervention for patients with hypo-chondriasis Psychological Medicine 41(2) 431e441 httpdxdoiorg101017s0033291710000292
Speckens A E M van Hemert A M Spinhoven P Hawton K E Bolk J H ampRooijmans H G M (1995) Cognitive behavioural therapy for medically un-explained physical symptoms a randomised controlled trial British MedicalJournal (Clinical Research Edition) 311(7016) 1328e1332
Svanborg P amp Aringsberg M (1994) A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale Acta Psy-chiatrica Scandinavica 89(1) 21e28
Svanborg P amp Ekselius L (2003) Self-assessment of DSM-IV criteria for majordepression in psychiatric out- and inpatients Nordic Journal of Psychiatry 57(4)291e296
Taylor S amp Asmundson G J G (2004) Treating health anxiety A cognitiveebehavioral approach New York Guilford Press
Thomson A B amp Page L A (2007) Psychotherapies for hypochondriasis CochraneDatabase of Systematic Reviews httpdxdoiorg10100214651858CD006520pub2 (4) CD006520
Warwick H Clark D Cobb A amp Salkovskis P (1996) A controlled trial ofcognitive-behavioural treatment of hypochondriasis British Journal of Psychia-try 169(2) 189e195 httpdxdoiorg101192bjp1692189
Related Documents











