Predictors of Heart Failure in Patients with Stable Coronary Artery Disease: A PEACE Study Eldrin F. Lewis, M.D., M.P.H. 1 , Scott D. Solomon, M.D. 1 , Kathleen A. Jablonski, Ph.D. 2 , Madeline Murguia Rice, Ph.D. 2 , Francesco Clemenza, M.D. 3 , Judith Hsia, M.D. 4 , Aldo P. Maggioni, M.D. 5 , Miguel Zabalgoitia, M.D. 6 , Thao Huynh, M.D. 7 , Thomas E. Cuddy, M.D. 8 , Bernard J. Gersh, M.B.,ChB,D.Phil 9 , Jean Rouleau, M.D. 10 , Eugene Braunwald, M.D. 1 , and Marc A. Pfeffer, M.D., Ph.D. 1 the PEACE Investigators 1 Cardiovascular Division, Brigham and Women’s Hospital, Boston, MA 2 Biostatistics Center, George Washington University, Washington, D.C. and Rockville, MD 3 Mediterranean Institute for Transplantation and Advanced Specialized Therapies, Palermo, Italy 4 Astra Zeneca, Wilmington, DE 5 AMNCO Foundation, Florence, Italy 6 Department of Medicine, University of Texas Health Science Center, San Antonio, Texas 7 Montreal General Hospital, McGill University Health Center, Montreal, Quebec, Canada 8 University of Manitoba, Winnipeg, Manitoba, Canada Address correspondence to: Eldrin F. Lewis, MD, MPH, Cardiovascular Division, Brigham and Women’s Hospital,75 Francis Street, Boston, MA 02115, Phone: 617-525-7057; Fax: 617-264-5265, [email protected]. Conflict of Interest Disclosures Dr Lewis has received research grants from Novartis, and has received research grants and honoraria for Amgen. Drs Jablonski and Rice have received research grants from Knoll Pharmaceuticals and Abbott Laboratories. Dr Gersh has served on scientific advisory boards for AstraZeneca, Abbott Laboratories, Bristol-Myers Squibb, Boston Scientific, and Novartis. Dr. Hsia is currently employed by and owns stock in AstraZeneca. Dr. Rouleau served as a consultant for Novartis, received research funds from Scios, and has received honoraria and has served as a consultant for Bristol Myer Squibb. Dr Pfeffer has received research grant support from Amgen, Baxter, Bristol-Myers Squibb, Celladon, Novartis, and Sanofi-Aventis; has served on scientific advisory boards for Amgen, AstraZeneca, Biogen, BMS, CV Therapeutics, Genentech, Medtronic, Merck, Novartis, Sanofi; and is the coinventor on patent held by Brigham and Women’s Hospital for the use of inhibitors of the renin-angiotensin system in survivors of MI. Dr Braunwald has received research grant support from AstraZeneca, Johnson & Johnson, Beckman Coulter, Bristol Myers Squibb, CV Therapeutics, Eli Lilly, Genentech, Integrated Therapeutics Group, Merck, Novartis, Pfizer, Roche Diagnostics, Sanofi Aventis, Schering Plough Research Institute, Daiichi Sankyo, and Eisai Medical Research; honoraria from Eli Lilly, Merck, Schering-Plough, and Sanofi Aventis; he has served as a consultant or is on the advisory board for Bayer, CV Therapeutics, Daiichi Sankyo, Merck, Momenta, Pfizer, Schering-Plough, Sanofi Aventis, Cytokinetics, Genzyme, and GlaxoSmithKline. Dr. Maggioni has received research support from AstraZeneca, Novartis, Takeda, and Pfizer and has been a consultant for Novartis. Drs. Solomon, Zabalgoitia, Clemenza, Cuddy, and Huynh have nothing to disclose. Short Commentary: Identifying patients at risk for heart failure among a healthier cohort with coronary artery disease may enable better strategies to manage these patients as prevention of heart failure has major implications given the excess mortality in these patients and the large economic burden for the treatment of the disease. We identified several traditional and easily available factors associated with a greater risk of heart failure development, even among a low-risk coronary artery disease population. ACE-inhibition reduces the risk of heart failure among this low risk population irrespective of these factors. Clinicians should discuss the risk of heart failure and its subsequent mortality and decreased quality of life as a way of motivating patients to lose weight. Moreover, adherence to guidelines should be emphasized among those patients at particular high risk for heart failure development, including ongoing smokers and those with a lower glomerular filtration rate, a readily calculated measure which is increasingly being reported. Although the risk of heart failure is not as great as survivors of myocardial infarction, the prevalence of “low risk” coronary artery disease is much greater and these patients may have a misperception that they remain at low risk and thus are not as adherent to preventive efforts. As the prevalence of coronary artery disease continues to increase, newer therapies can target those patients among this low risk group who may derive the greatest benefit from more aggressive interventions and the risk score may be used to stratify patients for future clinical trials. NIH Public Access Author Manuscript Circ Heart Fail. Author manuscript; available in PMC 2010 December 23. Published in final edited form as: Circ Heart Fail. 2009 May ; 2(3): 209–216. doi:10.1161/CIRCHEARTFAILURE.108.820696. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Predictors of Heart Failure in Patients with Stable CoronaryArtery Disease: A PEACE Study
Eldrin F. Lewis, M.D., M.P.H.1, Scott D. Solomon, M.D.1, Kathleen A. Jablonski, Ph.D.2,Madeline Murguia Rice, Ph.D.2, Francesco Clemenza, M.D.3, Judith Hsia, M.D.4, Aldo P.Maggioni, M.D.5, Miguel Zabalgoitia, M.D.6, Thao Huynh, M.D.7, Thomas E. Cuddy, M.D.8,Bernard J. Gersh, M.B.,ChB,D.Phil9, Jean Rouleau, M.D.10, Eugene Braunwald, M.D.1, andMarc A. Pfeffer, M.D., Ph.D.1 the PEACE Investigators1Cardiovascular Division, Brigham and Women’s Hospital, Boston, MA2Biostatistics Center, George Washington University, Washington, D.C. and Rockville, MD3Mediterranean Institute for Transplantation and Advanced Specialized Therapies, Palermo, Italy4Astra Zeneca, Wilmington, DE5AMNCO Foundation, Florence, Italy6Department of Medicine, University of Texas Health Science Center, San Antonio, Texas7Montreal General Hospital, McGill University Health Center, Montreal, Quebec, Canada8University of Manitoba, Winnipeg, Manitoba, Canada
Address correspondence to: Eldrin F. Lewis, MD, MPH, Cardiovascular Division, Brigham and Women’s Hospital,75 FrancisStreet, Boston, MA 02115, Phone: 617-525-7057; Fax: 617-264-5265, [email protected] of Interest DisclosuresDr Lewis has received research grants from Novartis, and has received research grants and honoraria for Amgen. Drs Jablonski andRice have received research grants from Knoll Pharmaceuticals and Abbott Laboratories. Dr Gersh has served on scientific advisoryboards for AstraZeneca, Abbott Laboratories, Bristol-Myers Squibb, Boston Scientific, and Novartis. Dr. Hsia is currently employedby and owns stock in AstraZeneca. Dr. Rouleau served as a consultant for Novartis, received research funds from Scios, and hasreceived honoraria and has served as a consultant for Bristol Myer Squibb. Dr Pfeffer has received research grant support fromAmgen, Baxter, Bristol-Myers Squibb, Celladon, Novartis, and Sanofi-Aventis; has served on scientific advisory boards for Amgen,AstraZeneca, Biogen, BMS, CV Therapeutics, Genentech, Medtronic, Merck, Novartis, Sanofi; and is the coinventor on patent heldby Brigham and Women’s Hospital for the use of inhibitors of the renin-angiotensin system in survivors of MI. Dr Braunwald hasreceived research grant support from AstraZeneca, Johnson & Johnson, Beckman Coulter, Bristol Myers Squibb, CV Therapeutics, EliLilly, Genentech, Integrated Therapeutics Group, Merck, Novartis, Pfizer, Roche Diagnostics, Sanofi Aventis, Schering PloughResearch Institute, Daiichi Sankyo, and Eisai Medical Research; honoraria from Eli Lilly, Merck, Schering-Plough, and SanofiAventis; he has served as a consultant or is on the advisory board for Bayer, CV Therapeutics, Daiichi Sankyo, Merck, Momenta,Pfizer, Schering-Plough, Sanofi Aventis, Cytokinetics, Genzyme, and GlaxoSmithKline. Dr. Maggioni has received research supportfrom AstraZeneca, Novartis, Takeda, and Pfizer and has been a consultant for Novartis. Drs. Solomon, Zabalgoitia, Clemenza, Cuddy,and Huynh have nothing to disclose.Short Commentary:Identifying patients at risk for heart failure among a healthier cohort with coronary artery disease may enable better strategies tomanage these patients as prevention of heart failure has major implications given the excess mortality in these patients and the largeeconomic burden for the treatment of the disease. We identified several traditional and easily available factors associated with agreater risk of heart failure development, even among a low-risk coronary artery disease population. ACE-inhibition reduces the riskof heart failure among this low risk population irrespective of these factors. Clinicians should discuss the risk of heart failure and itssubsequent mortality and decreased quality of life as a way of motivating patients to lose weight. Moreover, adherence to guidelinesshould be emphasized among those patients at particular high risk for heart failure development, including ongoing smokers and thosewith a lower glomerular filtration rate, a readily calculated measure which is increasingly being reported. Although the risk of heartfailure is not as great as survivors of myocardial infarction, the prevalence of “low risk” coronary artery disease is much greater andthese patients may have a misperception that they remain at low risk and thus are not as adherent to preventive efforts. As theprevalence of coronary artery disease continues to increase, newer therapies can target those patients among this low risk group whomay derive the greatest benefit from more aggressive interventions and the risk score may be used to stratify patients for futureclinical trials.
NIH Public AccessAuthor ManuscriptCirc Heart Fail. Author manuscript; available in PMC 2010 December 23.
Published in final edited form as:Circ Heart Fail. 2009 May ; 2(3): 209–216. doi:10.1161/CIRCHEARTFAILURE.108.820696.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

9Division of Cardiovascular Disease and Internal Medicine, Mayo Clinic, Rochester, Minnesota10Université de Montreal, Montreal, Canada
AbstractBackground—Heart failure (HF) is a disease commonly associated with coronary artery disease(CAD). Most risk models for HF development have focused on acute myocardial infarction (MI)patients. The prevention of events with angiotensin-converting enzyme inhibition (PEACE)population enabled the development of a risk model to predict HF in patients with stable CAD andpreserved ejection fraction.
Methods and Results—In the 8290 PEACE patients without pre-existing HF, new-onset HFhospitalizations and fatal HF were assessed over a median follow-up of 4.8 years. Covariates wereevaluated and maintained in the Cox regression multivariable model using backward selection ifp<0.05. A risk score was developed and converted to an integer-based scoring system. Among thePEACE population (age 64±8, female 18%, prior MI 55%), there were 268 cases of fatal and non-fatal HF. Twelve characteristics were associated with increased risk of HF along with severalbaseline medications, including older age, history of hypertension, and diabetes. Randomization totrandolapril independently reduced risk of HF. There was no interaction between trandolapriltreatment and other risk factors for HF. The risk score (range 0–21) demonstrated excellentdiscriminatory power (c-statistic 0.80). Risk of HF ranged from 1.75% in patients with a risk scoreof 0 to 33% in patients with risk score≥16.
Conclusion—Among patients with stable CAD and preserved EF, traditional and newer factorswere independently associated with increased risk of HF. Trandolopril decreased the risk of HF inthese patients with preserved EF.
Keywordsheart failure; coronary artery disease; ACE-inhibitors; predictors
INTRODUCTIONThe prevalence of coronary artery disease (CAD) is expected to increase over the next fewdecades given the increase in the prevalence of risk factors such as obesity and diabetes andthe improved survival after the diagnosis(1,2). These patients living with CAD are at higherrisk for death and a range of additional cardiovascular outcomes, including recurrentmyocardial infarction (MI), arrhythmia, stroke, and heart failure(3–6). The risk ofexperiencing these important cardiovascular events also varies considerably across thespectrum of CAD survivors. The development of heart failure (HF) is particularly serioussince patients manifesting HF have a several fold increase in the risk of death whencompared with other CAD patients and MI survivors(3,7). Among a MI population with lowleft ventricular ejection fraction (LVEF), those who developed HF had increased mortality(8). Thus, efforts to prevent development of HF have major implications for individualpatients as well as the health care and public health community given the economic andsocietal impact of the syndrome(9).
Many of the prediction models of HF development have focused on patients withhypertension(10,11) and MI survivors in the acute and sub-acute phase(12,13). A fewinvestigators have characterized risk factors for HF in patients with higher-risk, stableCAD(14). Moreover, angiotensin-converting enzyme (ACE) inhibitors have beendemonstrated to reduce mortality and morbidity in patients with HF, MI complicated by HF,and high-risk CAD(8,15–17). Less is known about predictors associated with HF in lower-risk patients with CAD. A better understanding of the factors involved in the eventual
Lewis et al. Page 2
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

development of HF among these lower risk patients may enable new strategies to preventprogression of disease, preserve quality of life, and improve overall survival. The Preventionof Events with an ACE Inhibitor (PEACE) cohort of patients was a low-risk CADpopulation that was the focus of this study. The aims were a) to identify predictors of HF ina low-risk CAD population, b) to determine the impact of trandolapril on subsequent HFevents, and c) to develop a risk score to predict HF.
METHODSThe design and results of the PEACE trial have been previously published(18). Briefly, 8290patients ≥50 years with documented CAD and documented left ventricular ejection fraction≥40% were randomized to trandolapril or placebo and followed for a median of 4.8 years.The primary endpoint was cardiovascular death, non-fatal MI, or coronary revascularization.Patients with a serum creatinine >2.0 mg/dL or who had hospitalization for unstable anginawithin 2 months or revascularization within 3 months were excluded. In addition, patientswith a condition that required the use of an ACE-inhibitor, including HF, were excluded.
Baseline characteristics were obtained by site investigators and staff and included medicalhistory, prior MI and/or coronary revascularization, vital signs, and left ventricular ejectionfraction. Serum creatinine was obtained at baseline. Glomerular filtration rate (GFR) wasestimated using the 4-component Modification of Diet in renal Disease (MDRD) equationwhich includes serum creatinine, sex, age, and race(19). New HF was determined by theinvestigators and required hospitalization for the treatment of HF or was adjudicated as theprimary cause of death by a clinical endpoints committee. In addition, all deaths were sub-classified and those deaths attributed to HF were noted. The primary outcome for this studyfocused on HF hospitalization or fatal HF.
Statistical analysisWe computed descriptive statistics for all potential covariates. For each continuous variable,we tested for linearity in the log hazard using cubic splines(20). We then used thecollinearity index to check for intercorrelations among the variables. All covariates wereentered into a Cox proportional hazard model and the final model was chosen using abackward selection procedure. Of note, a forward selection procedure resulted in the sameindependent predictors of HF events. All two-way interactions with treatment were testedand a p-value of 0.01 was considered significant. We tested model fit using residual analysisand the proportional hazards assumptions using the log-log survival function(21). Tovalidate the final Cox model, we used the methods of Assman, Cullen, and Schulte(22). Werandomly divided the sample into five equal parts and generated models using everypossible combination of four of the five sets. A c-score was computed to assess the model’spredictive ability(23). Hazard ratios with 95% confidence intervals are reported for the finalmodel.
To develop a risk stratification algorithm, we assigned a point score to baselinecharacteristics that independently predicted CHF. A risk score was developed using themethods of Rassi et al(24). Each coefficient was divided by the smallest coefficient androunded to the nearest integer. Kaplan-Meier survival curves were generated for each riskscore. The scores were grouped into 3 categories of risk; low (<9 points) , medium (10–14points), and high (≥15 points). We used the log-rank test to test for differences in survivalbetween the groups.
Several supportive analyses were conducted. The variables that were determined to bepredictive of HF in a stable MI cohort in Cholesterol and Recurrent Events (CARE) werecompared with PEACE population using Cox Proportional Hazards Model. Patients in the
Lewis et al. Page 3
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

PEACE trial who suffered a MI post-randomization were evaluated to determine theproportion of patients who had a MI prior to HF event. The SAS analysis system version 9.1was used for all analyses (SAS Institute, Inc., Cary, NC).
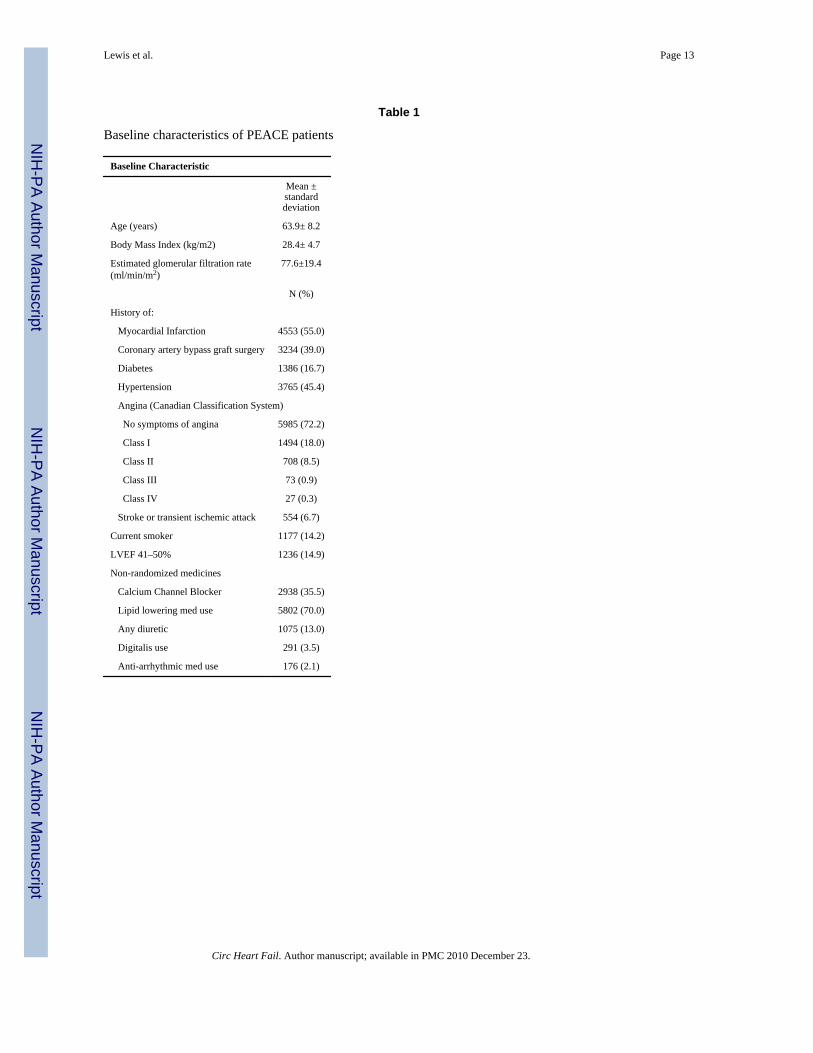
RESULTSThe baseline characteristics of the PEACE population have been previously reported(18).Briefly, the mean age was 64±8 with 18% female and 31.0% having a body mass index >30kg/m2. The mean left ventricular ejection fraction was 58±9% with only 14.9% of patientshaving a LVEF between 40–50%, the lowest eligible range of left ventricular function. Themean estimated glomerular filtration rate was 78±19 ml/kg/min/1.73 m2, and 16.4% ofpatients had Stage 3 chronic kidney disease based upon an eGFR<60 ml/kg/min/1.73 m2. Ahistory of hypertension was present in 45% of patients and 55% had a prior MI. A total of412 patients (5%) had missing quantitative values of LVEF, but systolic function wasreported by echocardiography as being qualitatively preserved, and 405 patients (5%) weremissing cholesterol values. The remainder of the data required for the multivariable modelwas available in 99% of patients. Mean arterial pressure and serum creatinine were not inthe multivariable model as they were highly correlated with systolic/diastolic blood pressureand eGFR respectively.
Fatal and Nonfatal Heart Failure EventsDuring a median follow-up of 4.8 years, there were 268 patients (3.3%) of 8211 PEACEpatients who had a HF event which averages to 0.7%/year. The majority of patients with aHF event (n=239) were hospitalized and 29 patients (0.35%) died of HF without ever beinghospitalized. After adjudication by a blinded endpoints committee, patients who were felt tohave died predominantly as a result of pump failure were classified as “fatal HF”. Of these268 patients, 47 (17.5%) had an acute MI between randomization and the HF event, but themajority developed HF without an interim MI. Baseline characteristics of patients are listedin Table 1.
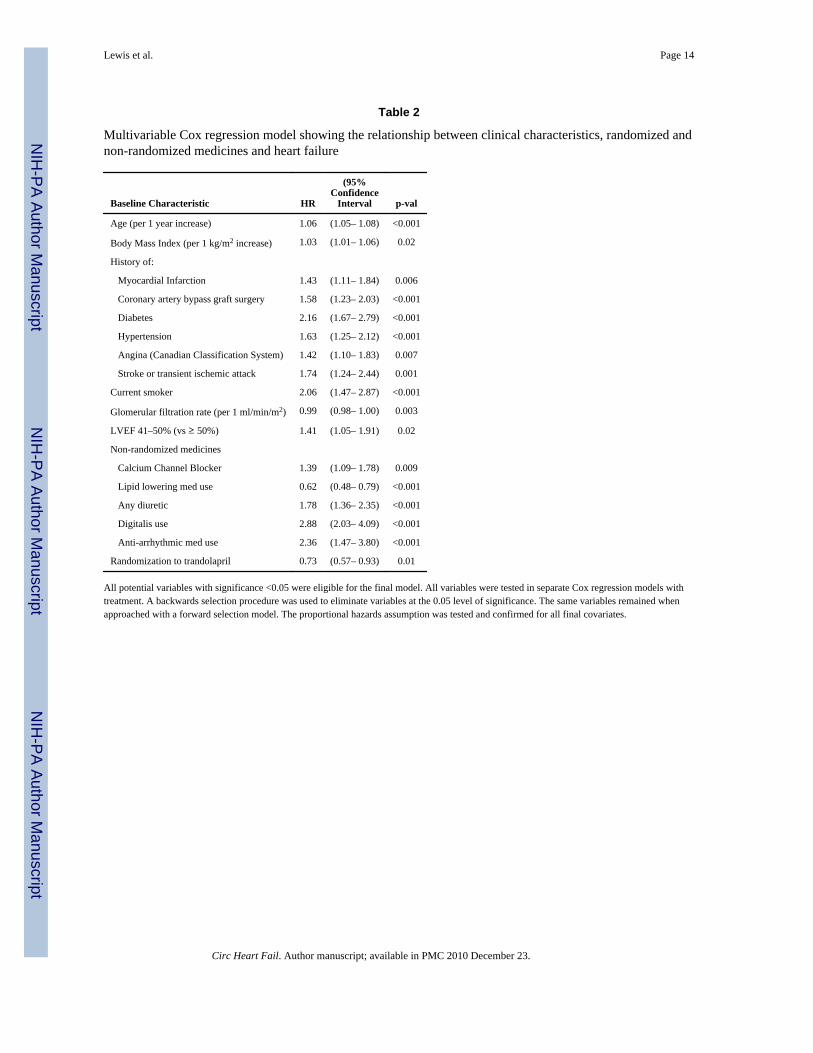
Multivariable analyses identified increasing age, diabetes, prior revascularization,hypertension, and current smoking as the most robust predictors of HF (Table 2). Patientswith a prior MI had a 43% increased risk of HF and patients with lower LVEF (LVEF 41–50%) had a 41% increased risk. Higher body mass index and lower eGFR were alsoassociated with increased risk. Several baseline medications that were used at the discretionof the treating physician were also associated with HF development, including use ofdiuretic, digitalis, calcium channel blocker, or anti-arrhythmic drugs. Use of lipid loweringmedicines was associated with a lower risk of HF.
Randomization to trandolapril significantly reduced the risk of HF compared with placeboafter adjusting for all other predictors of HF (HR 0.73, 95% CI 0.57–0.93, p=0.01). Therewere no significant interactions between trandolapril and each variable in the final model.The same variables were identified using forward selection as well as backward selection.Cross-validation resulted in several variables that changed significance levels in one or morevalidity data sets. This included the presence of angina, LVEF stratification (40–50% vs.≥50%), non-randomized use of calcium channel blockers, and history of MI. Amultivariable model developed with an endpoint of “HF or all-cause mortality resulted insimilar predictors.
Risk ScoreFor the purpose of risk score development, continuous variables were categorized (i.e.,eGFR, age, and BMI). There was no difference in the Cox regression model when using
Lewis et al. Page 4
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
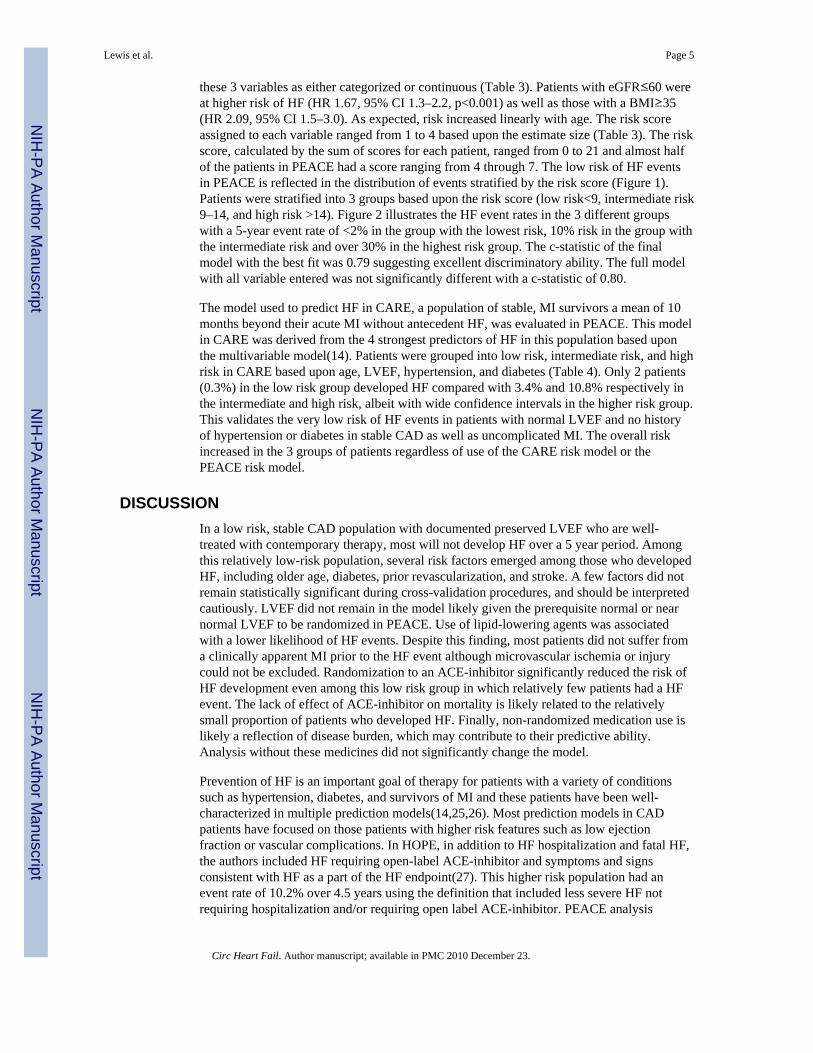
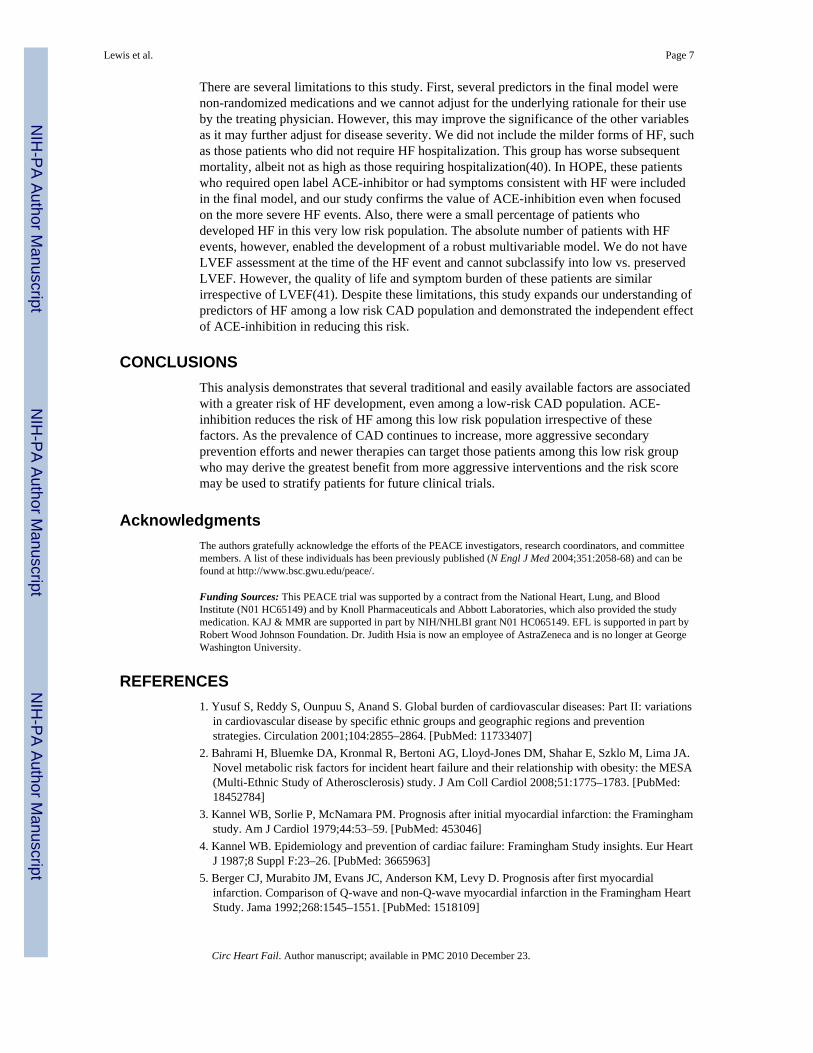
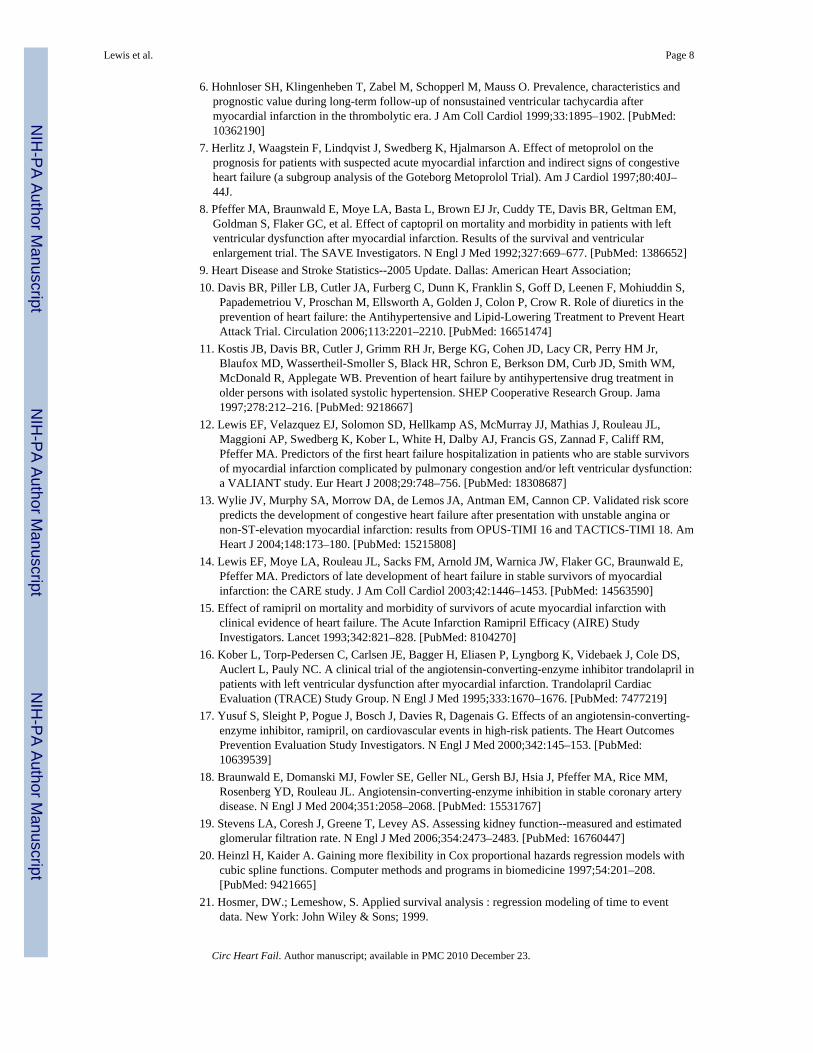
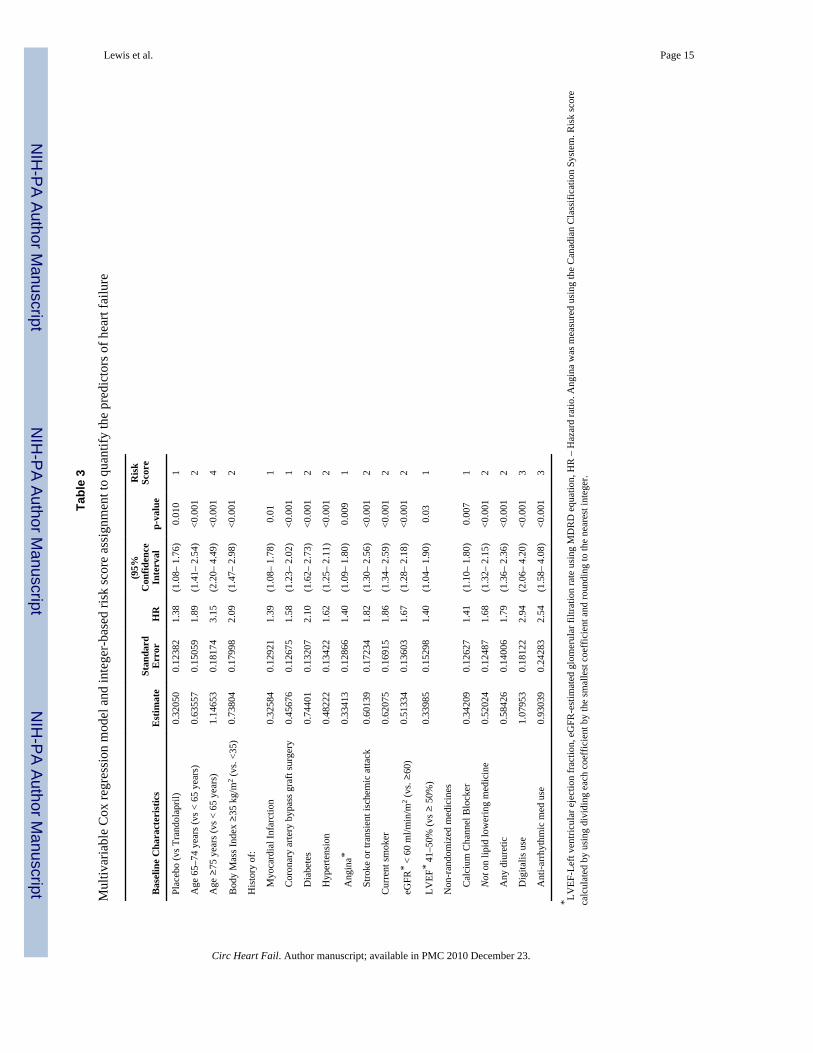
these 3 variables as either categorized or continuous (Table 3). Patients with eGFR≤60 wereat higher risk of HF (HR 1.67, 95% CI 1.3–2.2, p<0.001) as well as those with a BMI≥35(HR 2.09, 95% CI 1.5–3.0). As expected, risk increased linearly with age. The risk scoreassigned to each variable ranged from 1 to 4 based upon the estimate size (Table 3). The riskscore, calculated by the sum of scores for each patient, ranged from 0 to 21 and almost halfof the patients in PEACE had a score ranging from 4 through 7. The low risk of HF eventsin PEACE is reflected in the distribution of events stratified by the risk score (Figure 1).Patients were stratified into 3 groups based upon the risk score (low risk<9, intermediate risk9–14, and high risk >14). Figure 2 illustrates the HF event rates in the 3 different groupswith a 5-year event rate of <2% in the group with the lowest risk, 10% risk in the group withthe intermediate risk and over 30% in the highest risk group. The c-statistic of the finalmodel with the best fit was 0.79 suggesting excellent discriminatory ability. The full modelwith all variable entered was not significantly different with a c-statistic of 0.80.
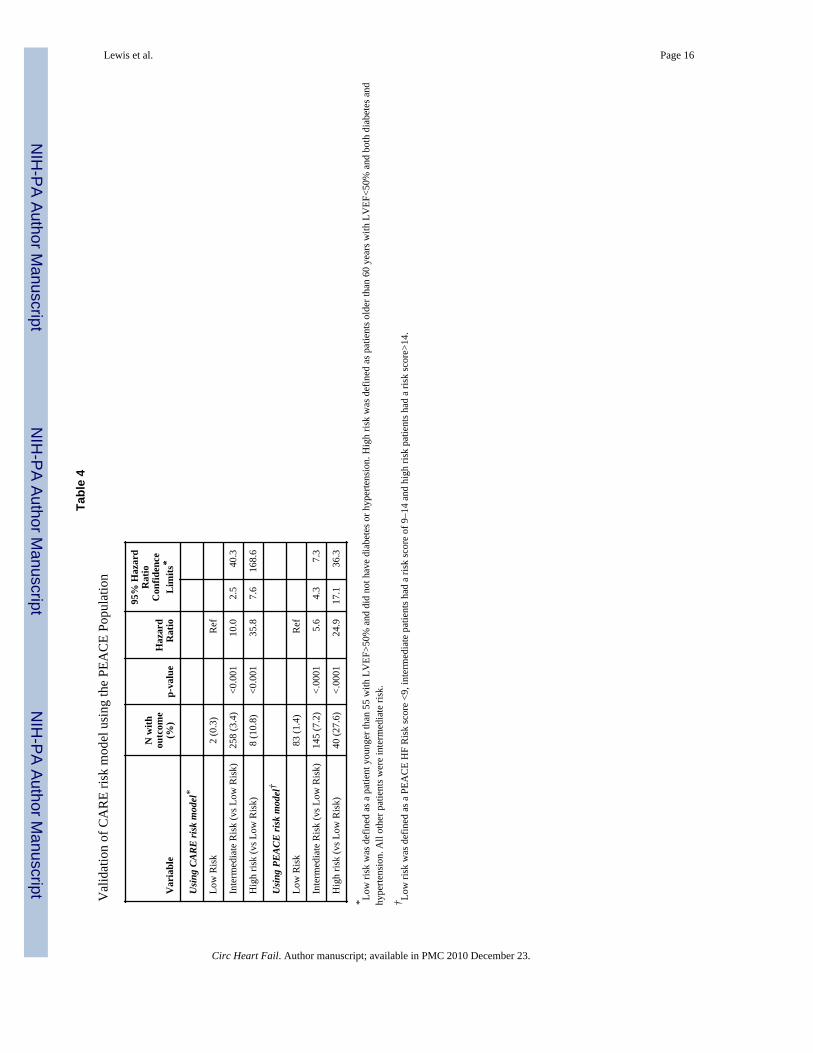
The model used to predict HF in CARE, a population of stable, MI survivors a mean of 10months beyond their acute MI without antecedent HF, was evaluated in PEACE. This modelin CARE was derived from the 4 strongest predictors of HF in this population based uponthe multivariable model(14). Patients were grouped into low risk, intermediate risk, and highrisk in CARE based upon age, LVEF, hypertension, and diabetes (Table 4). Only 2 patients(0.3%) in the low risk group developed HF compared with 3.4% and 10.8% respectively inthe intermediate and high risk, albeit with wide confidence intervals in the higher risk group.This validates the very low risk of HF events in patients with normal LVEF and no historyof hypertension or diabetes in stable CAD as well as uncomplicated MI. The overall riskincreased in the 3 groups of patients regardless of use of the CARE risk model or thePEACE risk model.
DISCUSSIONIn a low risk, stable CAD population with documented preserved LVEF who are well-treated with contemporary therapy, most will not develop HF over a 5 year period. Amongthis relatively low-risk population, several risk factors emerged among those who developedHF, including older age, diabetes, prior revascularization, and stroke. A few factors did notremain statistically significant during cross-validation procedures, and should be interpretedcautiously. LVEF did not remain in the model likely given the prerequisite normal or nearnormal LVEF to be randomized in PEACE. Use of lipid-lowering agents was associatedwith a lower likelihood of HF events. Despite this finding, most patients did not suffer froma clinically apparent MI prior to the HF event although microvascular ischemia or injurycould not be excluded. Randomization to an ACE-inhibitor significantly reduced the risk ofHF development even among this low risk group in which relatively few patients had a HFevent. The lack of effect of ACE-inhibitor on mortality is likely related to the relativelysmall proportion of patients who developed HF. Finally, non-randomized medication use islikely a reflection of disease burden, which may contribute to their predictive ability.Analysis without these medicines did not significantly change the model.
Prevention of HF is an important goal of therapy for patients with a variety of conditionssuch as hypertension, diabetes, and survivors of MI and these patients have been well-characterized in multiple prediction models(14,25,26). Most prediction models in CADpatients have focused on those patients with higher risk features such as low ejectionfraction or vascular complications. In HOPE, in addition to HF hospitalization and fatal HF,the authors included HF requiring open-label ACE-inhibitor and symptoms and signsconsistent with HF as a part of the HF endpoint(27). This higher risk population had anevent rate of 10.2% over 4.5 years using the definition that included less severe HF notrequiring hospitalization and/or requiring open label ACE-inhibitor. PEACE analysis
Lewis et al. Page 5
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

confirmed several predictors of HF that were identified in the HOPE population, includingolder age, higher body mass index, prior CABG, diabetes, stroke, and lack of lipid loweringtherapy. Approximately 80% of the HOPE patients had CAD and less patients were treatedwith beta-blockers, lipid-lowering agents, and anti-platelet therapy(28). In addition,impaired renal function was also associated with increased risk of HF in PEACE. LowerGFR has previously been shown to be predictive of adverse events in patients withmyocardial infarction(29) and chronic HF(30,31) and has identified patients who may bemore likely to benefit from medical interventions(32). Among women with CAD, only aGFR<40 cc/min/m2 was predictive of subsequent HF(33). This increasingly recognized riskfactor may be associated with HF development due to left ventricular remodeling andworsening anemia. Additional predictors identified in PEACE include presence of angina,current smoking, and history of MI.
Risk scores have been commonly developed in the prediction of a variety of outcomes inpatients with cardiovascular disease. The clinical utility has been relatively low for a varietyof factors, including the cumbersome use in medical decision making. This risk scoreemploys an integer-based scoring system, which could facilitate its clinical applicability.Although it has excellent discriminatory characteristics, the very low event rate in this lowrisk population attenuates the overall impact of the score. Patients with intermediate andhigh risk scores are at much greater risk of HF development. However, the majority ofpatients had a score < 9 and was at low risk. Improving the ability to stratify these lowestrisk patients may impact a larger population with CAD. The addition of biomarkers mayincrease the precision of prediction models using clinical characteristics. Brain natriureticpeptide (BNP) and pro-BNP have been predictive of HF events in PEACE and increased thec-statistic from 0.82 using several baseline characteristics and CRP to 0.84 with BNP addedand 0.85 with pro-BNP added to the model(34). In the Heart and Soul study, pro-BNP wasan independent predictor of new-onset HF in patients with stable CAD, but the number ofclinical characteristics adjusted in the multivariable model was limited by the small numberof events(33). Other possible biomarkers include anemia, C-reactive protein, and cystatinC(35). Most of the publications regarding predictors of HF in low risk CAD populationshave focused on biomarkers or in patients with imaging evidence of ischemia(36).
The use of ACE-inhibitors has been established as clearly beneficial in a variety of patientpopulations, including those with chronic HF across the spectrum of disease severity,myocardial infarction patients with low LVEF and/or signs of HF, diabetes mellitus withproteinuria, and complicated CAD patients with high risk features. The current guidelinesrecommend ACE-inhibitors as a Class IIa indication for patients with CAD and normal tomildly reduced LVEF(37). In HOPE and EUROPA, ACE-inhibition decreased CV risk andmortality(17,38).
In a lower risk population in PEACE with documented preserved LVEF, randomization totrandolapril reduced HF development, but not the primary endpoint or mortality. Thisefficacy was seen after adjusting for factors associated with HF development. Based uponother studies, HF development was associated with a 4 to 9 fold increased mortality, andprevention of this complication of CAD may attenuate this mortality (14,27). Longer follow-up in patients at less risk of mortality may enable realization of benefit of ACE-inhibition.Also, HF management costs an estimated 29 billion dollars annually in the United Statesalone and prevention of HF development in patients with CAD would decrease theeconomic burden of CV disease. Patients who develop HF have a distinctly different lifetrajectory with decreased survival, increased anxiety and depression, and worse quality oflife. Finally, a meta-analysis of HOPE, EUROPA, and PEACE demonstrated consistentreduction in CV events and HF(39).
Lewis et al. Page 6
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
There are several limitations to this study. First, several predictors in the final model werenon-randomized medications and we cannot adjust for the underlying rationale for their useby the treating physician. However, this may improve the significance of the other variablesas it may further adjust for disease severity. We did not include the milder forms of HF, suchas those patients who did not require HF hospitalization. This group has worse subsequentmortality, albeit not as high as those requiring hospitalization(40). In HOPE, these patientswho required open label ACE-inhibitor or had symptoms consistent with HF were includedin the final model, and our study confirms the value of ACE-inhibition even when focusedon the more severe HF events. Also, there were a small percentage of patients whodeveloped HF in this very low risk population. The absolute number of patients with HFevents, however, enabled the development of a robust multivariable model. We do not haveLVEF assessment at the time of the HF event and cannot subclassify into low vs. preservedLVEF. However, the quality of life and symptom burden of these patients are similarirrespective of LVEF(41). Despite these limitations, this study expands our understanding ofpredictors of HF among a low risk CAD population and demonstrated the independent effectof ACE-inhibition in reducing this risk.
CONCLUSIONSThis analysis demonstrates that several traditional and easily available factors are associatedwith a greater risk of HF development, even among a low-risk CAD population. ACE-inhibition reduces the risk of HF among this low risk population irrespective of thesefactors. As the prevalence of CAD continues to increase, more aggressive secondaryprevention efforts and newer therapies can target those patients among this low risk groupwho may derive the greatest benefit from more aggressive interventions and the risk scoremay be used to stratify patients for future clinical trials.
AcknowledgmentsThe authors gratefully acknowledge the efforts of the PEACE investigators, research coordinators, and committeemembers. A list of these individuals has been previously published (N Engl J Med 2004;351:2058-68) and can befound at http://www.bsc.gwu.edu/peace/.
Funding Sources: This PEACE trial was supported by a contract from the National Heart, Lung, and BloodInstitute (N01 HC65149) and by Knoll Pharmaceuticals and Abbott Laboratories, which also provided the studymedication. KAJ & MMR are supported in part by NIH/NHLBI grant N01 HC065149. EFL is supported in part byRobert Wood Johnson Foundation. Dr. Judith Hsia is now an employee of AstraZeneca and is no longer at GeorgeWashington University.
REFERENCES1. Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: Part II: variations
in cardiovascular disease by specific ethnic groups and geographic regions and preventionstrategies. Circulation 2001;104:2855–2864. [PubMed: 11733407]
2. Bahrami H, Bluemke DA, Kronmal R, Bertoni AG, Lloyd-Jones DM, Shahar E, Szklo M, Lima JA.Novel metabolic risk factors for incident heart failure and their relationship with obesity: the MESA(Multi-Ethnic Study of Atherosclerosis) study. J Am Coll Cardiol 2008;51:1775–1783. [PubMed:18452784]
3. Kannel WB, Sorlie P, McNamara PM. Prognosis after initial myocardial infarction: the Framinghamstudy. Am J Cardiol 1979;44:53–59. [PubMed: 453046]
4. Kannel WB. Epidemiology and prevention of cardiac failure: Framingham Study insights. Eur HeartJ 1987;8 Suppl F:23–26. [PubMed: 3665963]
5. Berger CJ, Murabito JM, Evans JC, Anderson KM, Levy D. Prognosis after first myocardialinfarction. Comparison of Q-wave and non-Q-wave myocardial infarction in the Framingham HeartStudy. Jama 1992;268:1545–1551. [PubMed: 1518109]
Lewis et al. Page 7
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
6. Hohnloser SH, Klingenheben T, Zabel M, Schopperl M, Mauss O. Prevalence, characteristics andprognostic value during long-term follow-up of nonsustained ventricular tachycardia aftermyocardial infarction in the thrombolytic era. J Am Coll Cardiol 1999;33:1895–1902. [PubMed:10362190]
7. Herlitz J, Waagstein F, Lindqvist J, Swedberg K, Hjalmarson A. Effect of metoprolol on theprognosis for patients with suspected acute myocardial infarction and indirect signs of congestiveheart failure (a subgroup analysis of the Goteborg Metoprolol Trial). Am J Cardiol 1997;80:40J–44J.
8. Pfeffer MA, Braunwald E, Moye LA, Basta L, Brown EJ Jr, Cuddy TE, Davis BR, Geltman EM,Goldman S, Flaker GC, et al. Effect of captopril on mortality and morbidity in patients with leftventricular dysfunction after myocardial infarction. Results of the survival and ventricularenlargement trial. The SAVE Investigators. N Engl J Med 1992;327:669–677. [PubMed: 1386652]
9. Heart Disease and Stroke Statistics--2005 Update. Dallas: American Heart Association;10. Davis BR, Piller LB, Cutler JA, Furberg C, Dunn K, Franklin S, Goff D, Leenen F, Mohiuddin S,
Papademetriou V, Proschan M, Ellsworth A, Golden J, Colon P, Crow R. Role of diuretics in theprevention of heart failure: the Antihypertensive and Lipid-Lowering Treatment to Prevent HeartAttack Trial. Circulation 2006;113:2201–2210. [PubMed: 16651474]
11. Kostis JB, Davis BR, Cutler J, Grimm RH Jr, Berge KG, Cohen JD, Lacy CR, Perry HM Jr,Blaufox MD, Wassertheil-Smoller S, Black HR, Schron E, Berkson DM, Curb JD, Smith WM,McDonald R, Applegate WB. Prevention of heart failure by antihypertensive drug treatment inolder persons with isolated systolic hypertension. SHEP Cooperative Research Group. Jama1997;278:212–216. [PubMed: 9218667]
12. Lewis EF, Velazquez EJ, Solomon SD, Hellkamp AS, McMurray JJ, Mathias J, Rouleau JL,Maggioni AP, Swedberg K, Kober L, White H, Dalby AJ, Francis GS, Zannad F, Califf RM,Pfeffer MA. Predictors of the first heart failure hospitalization in patients who are stable survivorsof myocardial infarction complicated by pulmonary congestion and/or left ventricular dysfunction:a VALIANT study. Eur Heart J 2008;29:748–756. [PubMed: 18308687]
13. Wylie JV, Murphy SA, Morrow DA, de Lemos JA, Antman EM, Cannon CP. Validated risk scorepredicts the development of congestive heart failure after presentation with unstable angina ornon-ST-elevation myocardial infarction: results from OPUS-TIMI 16 and TACTICS-TIMI 18. AmHeart J 2004;148:173–180. [PubMed: 15215808]
14. Lewis EF, Moye LA, Rouleau JL, Sacks FM, Arnold JM, Warnica JW, Flaker GC, Braunwald E,Pfeffer MA. Predictors of late development of heart failure in stable survivors of myocardialinfarction: the CARE study. J Am Coll Cardiol 2003;42:1446–1453. [PubMed: 14563590]
15. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction withclinical evidence of heart failure. The Acute Infarction Ramipril Efficacy (AIRE) StudyInvestigators. Lancet 1993;342:821–828. [PubMed: 8104270]
16. Kober L, Torp-Pedersen C, Carlsen JE, Bagger H, Eliasen P, Lyngborg K, Videbaek J, Cole DS,Auclert L, Pauly NC. A clinical trial of the angiotensin-converting-enzyme inhibitor trandolapril inpatients with left ventricular dysfunction after myocardial infarction. Trandolapril CardiacEvaluation (TRACE) Study Group. N Engl J Med 1995;333:1670–1676. [PubMed: 7477219]
17. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart OutcomesPrevention Evaluation Study Investigators. N Engl J Med 2000;342:145–153. [PubMed:10639539]
18. Braunwald E, Domanski MJ, Fowler SE, Geller NL, Gersh BJ, Hsia J, Pfeffer MA, Rice MM,Rosenberg YD, Rouleau JL. Angiotensin-converting-enzyme inhibition in stable coronary arterydisease. N Engl J Med 2004;351:2058–2068. [PubMed: 15531767]
19. Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function--measured and estimatedglomerular filtration rate. N Engl J Med 2006;354:2473–2483. [PubMed: 16760447]
20. Heinzl H, Kaider A. Gaining more flexibility in Cox proportional hazards regression models withcubic spline functions. Computer methods and programs in biomedicine 1997;54:201–208.[PubMed: 9421665]
21. Hosmer, DW.; Lemeshow, S. Applied survival analysis : regression modeling of time to eventdata. New York: John Wiley & Sons; 1999.
Lewis et al. Page 8
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
22. Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronaryevents based on the 10-year follow-up of the prospective cardiovascular Munster (PROCAM)study. Circulation 2002;105:310–315. [PubMed: 11804985]
23. Pencina MJ, D'Agostino RB. Overall C as a measure of discrimination in survival analysis: modelspecific population value and confidence interval estimation. Stat Med 2004;23:2109–2123.[PubMed: 15211606]
24. Rassi A Jr, Rassi A, Little WC, Xavier SS, Rassi SG, Rassi AG, Rassi GG, Hasslocher-Moreno A,Sousa AS, Scanavacca MI. Development and validation of a risk score for predicting death inChagas' heart disease. N Engl J Med 2006;355:799–808. [PubMed: 16928995]
25. Carr AA, Kowey PR, Devereux RB, Brenner BM, Dahlof B, Ibsen H, Lindholm LH, Lyle PA,Snapinn SM, Zhang Z, Edelman JM, Shahinfar S. Hospitalizations for new heart failure amongsubjects with diabetes mellitus in the RENAAL and LIFE studies. Am J Cardiol 2005;96:1530–1536. [PubMed: 16310435]
26. Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression from hypertension tocongestive heart failure. Jama 1996;275:1557–1562. [PubMed: 8622246]
27. Arnold JM, Yusuf S, Young J, Mathew J, Johnstone D, Avezum A, Lonn E, Pogue J, Bosch J.Prevention of Heart Failure in Patients in the Heart Outcomes Prevention Evaluation (HOPE)Study. Circulation 2003;107:1284–1290. [PubMed: 12628949]
28. Fox K, Ferrari R, Yusuf S, Borer JS. Should angiotensin-converting enzyme-inhibitors be used toimprove outcome in patients with coronary artery disease and 'preserved' left ventricular function?Eur Heart J 2006;27:2154–2157. [PubMed: 16905555]
29. Anavekar NS, McMurray JJ, Velazquez EJ, Solomon SD, Kober L, Rouleau JL, White HD,Nordlander R, Maggioni A, Dickstein K, Zelenkofske S, Leimberger JD, Califf RM, Pfeffer MA.Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. NEngl J Med 2004;351:1285–1295. [PubMed: 15385655]
30. Hillege HL, Nitsch D, Pfeffer MA, Swedberg K, McMurray JJ, Yusuf S, Granger CB, MichelsonEL, Ostergren J, Cornel JH, de Zeeuw D, Pocock S, van Veldhuisen DJ. Renal function as apredictor of outcome in a broad spectrum of patients with heart failure. Circulation 2006;113:671–678. [PubMed: 16461840]
31. Dries DL, Exner DV, Domanski MJ, Greenberg B, Stevenson LW. The prognostic implications ofrenal insufficiency in asymptomatic and symptomatic patients with left ventricular systolicdysfunction. J Am Coll Cardiol 2000;35:681–689. [PubMed: 10716471]
32. Solomon SD, Rice MM, K AJ, Jose P, Domanski M, Sabatine M, Gersh BJ, Rouleau J, PfefferMA, Braunwald E. Renal function and effectiveness of angiotensin-converting enzyme inhibitortherapy in patients with chronic stable coronary disease in the Prevention of Events with ACEinhibition (PEACE) trial. Circulation 2006;114:26–31. [PubMed: 16801465]
33. Bibbins-Domingo K, Lin F, Vittinghoff E, Barrett-Connor E, Hulley SB, Grady D, Shlipak MG.Predictors of heart failure among women with coronary disease. Circulation 2004;110:1424–1430.[PubMed: 15353499]
34. Omland T, Sabatine MS, Jablonski KA, Rice MM, Hsia J, Wergeland R, Landaas S, Rouleau JL,Domanski MJ, Hall C, Pfeffer MA, Braunwald E. Prognostic value of B-Type natriuretic peptidesin patients with stable coronary artery disease: the PEACE Trial. J Am Coll Cardiol 2007;50:205–214. [PubMed: 17631211]
35. Sarnak MJ, Katz R, Stehman-Breen CO, Fried LF, Jenny NS, Psaty BM, Newman AB, SiscovickD, Shlipak MG. Cystatin C concentration as a risk factor for heart failure in older adults. AnnIntern Med 2005;142:497–505. [PubMed: 15809461]
36. Elhendy A, Schinkel AF, van Domburg RT, Bax JJ, Poldermans D. Incidence and predictors ofheart failure during long-term follow-up after stress Tc-99m sestamibi tomography in patients withsuspected coronary artery disease. J Nucl Cardiol 2004;11:527–533. [PubMed: 15472637]
37. Fraker TD Jr, Fihn SD, Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS,Ferguson TB Jr, Fihn SD, Fraker TD Jr, Gardin JM, O'Rourke RA, Pasternak RC, Williams SV,Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM,Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Page RL, Riegel B,Tarkington LG, Yancy CW. 2007 chronic angina focused update of the ACC/AHA 2002Guidelines for the management of patients with chronic stable angina: a report of the American
Lewis et al. Page 9
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
College of Cardiology/American Heart Association Task Force on Practice Guidelines WritingGroup to develop the focused update of the 2002 Guidelines for the management of patients withchronic stable angina. Circulation 2007;116:2762–2772. [PubMed: 17998462]
38. Fox KM. Efficacy of perindopril in reduction of cardiovascular events among patients with stablecoronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (theEUROPA study). Lancet 2003;362:782–788. [PubMed: 13678872]
39. Dagenais GR, Pogue J, Fox K, Simoons ML, Yusuf S. Angiotensin-converting-enzyme inhibitorsin stable vascular disease without left ventricular systolic dysfunction or heart failure: a combinedanalysis of three trials. Lancet 2006;368:581–588. [PubMed: 16905022]
40. Lewis EF, Hellkamp AS, Pfeffer MA, Greenspon AJ, Machado C, Singh S, Schron E, Lee KL,Lamas GA. The association of the heart failure score with mortality and heart failurehospitalizations in elderly patients: insights from the Mode Selection Trial (MOST). Am Heart J2006;151:699–705. [PubMed: 16504635]
41. Lewis EF, Lamas GA, O'Meara E, Granger CB, Dunlap ME, McKelvie RS, Probstfield JL, YoungJB, Michelson EL, Halling K, Carlsson J, Olofsson B, McMurray JJ, Yusuf S, Swedberg K,Pfeffer MA. Characterization of health-related quality of life in heart failure patients withpreserved versus low ejection fraction in CHARM. Eur J Heart Fail 2007;9:83–91. [PubMed:17188020]
Lewis et al. Page 10
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
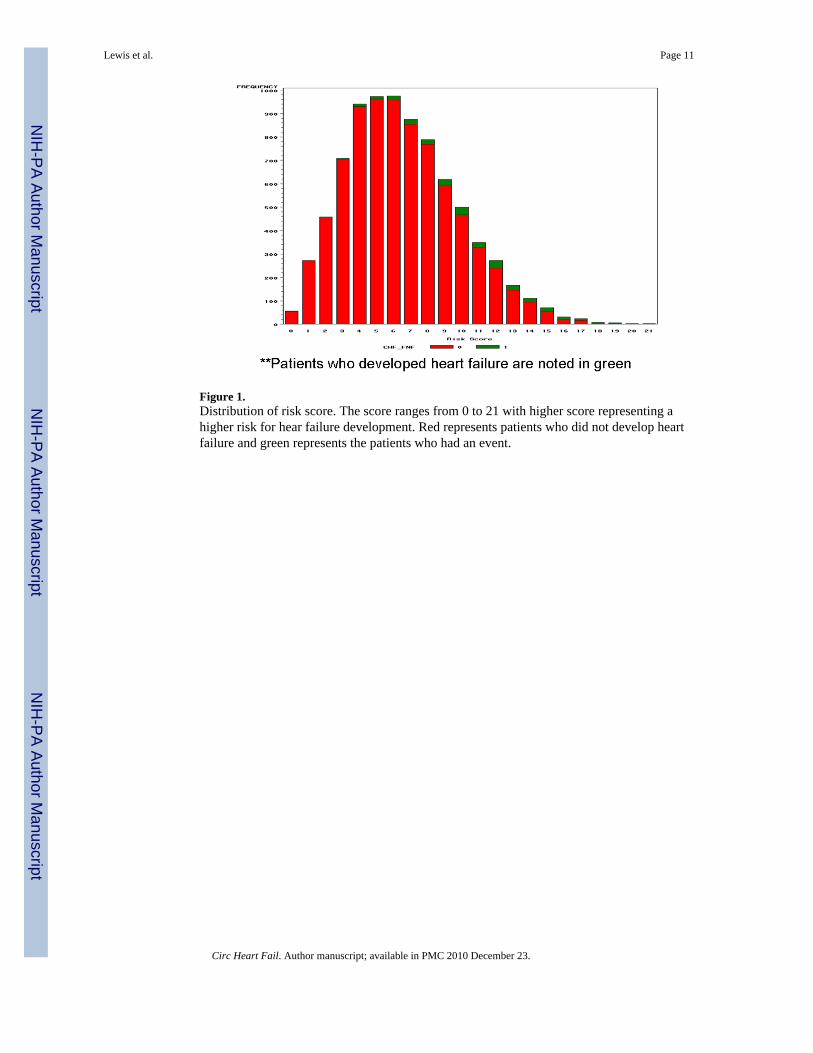
Figure 1.Distribution of risk score. The score ranges from 0 to 21 with higher score representing ahigher risk for hear failure development. Red represents patients who did not develop heartfailure and green represents the patients who had an event.
Lewis et al. Page 11
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
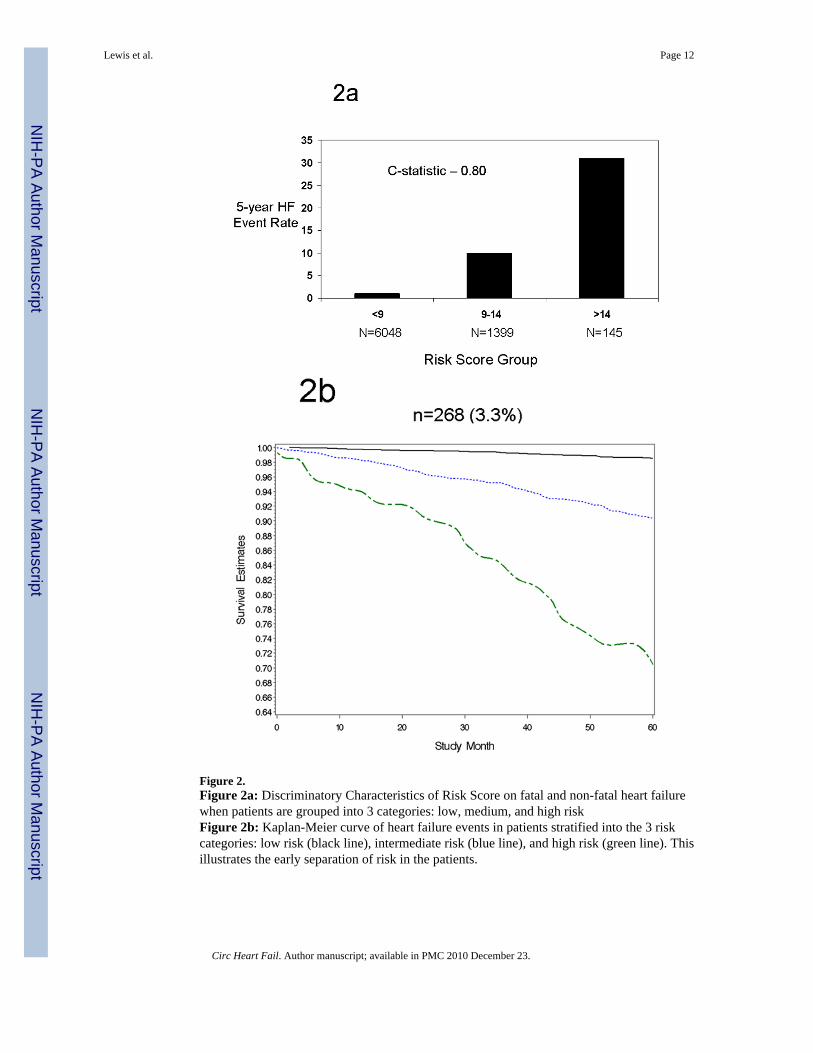
Figure 2.Figure 2a: Discriminatory Characteristics of Risk Score on fatal and non-fatal heart failurewhen patients are grouped into 3 categories: low, medium, and high riskFigure 2b: Kaplan-Meier curve of heart failure events in patients stratified into the 3 riskcategories: low risk (black line), intermediate risk (blue line), and high risk (green line). Thisillustrates the early separation of risk in the patients.
Lewis et al. Page 12
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Lewis et al. Page 13
Table 1
Baseline characteristics of PEACE patients
Baseline Characteristic
Mean ±standarddeviation
Age (years) 63.9± 8.2
Body Mass Index (kg/m2) 28.4± 4.7
Estimated glomerular filtration rate(ml/min/m2)
77.6±19.4
N (%)
History of:
Myocardial Infarction 4553 (55.0)
Coronary artery bypass graft surgery 3234 (39.0)
Diabetes 1386 (16.7)
Hypertension 3765 (45.4)
Angina (Canadian Classification System)
No symptoms of angina 5985 (72.2)
Class I 1494 (18.0)
Class II 708 (8.5)
Class III 73 (0.9)
Class IV 27 (0.3)
Stroke or transient ischemic attack 554 (6.7)
Current smoker 1177 (14.2)
LVEF 41–50% 1236 (14.9)
Non-randomized medicines
Calcium Channel Blocker 2938 (35.5)
Lipid lowering med use 5802 (70.0)
Any diuretic 1075 (13.0)
Digitalis use 291 (3.5)
Anti-arrhythmic med use 176 (2.1)
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Lewis et al. Page 14
Table 2
Multivariable Cox regression model showing the relationship between clinical characteristics, randomized andnon-randomized medicines and heart failure
Baseline Characteristic HR
(95%Confidence
Interval p-val
Age (per 1 year increase) 1.06 (1.05– 1.08) <0.001
Body Mass Index (per 1 kg/m2 increase) 1.03 (1.01– 1.06) 0.02
History of:
Myocardial Infarction 1.43 (1.11– 1.84) 0.006
Coronary artery bypass graft surgery 1.58 (1.23– 2.03) <0.001
Diabetes 2.16 (1.67– 2.79) <0.001
Hypertension 1.63 (1.25– 2.12) <0.001
Angina (Canadian Classification System) 1.42 (1.10– 1.83) 0.007
Stroke or transient ischemic attack 1.74 (1.24– 2.44) 0.001
Current smoker 2.06 (1.47– 2.87) <0.001
Glomerular filtration rate (per 1 ml/min/m2) 0.99 (0.98– 1.00) 0.003
LVEF 41–50% (vs ≥ 50%) 1.41 (1.05– 1.91) 0.02
Non-randomized medicines
Calcium Channel Blocker 1.39 (1.09– 1.78) 0.009
Lipid lowering med use 0.62 (0.48– 0.79) <0.001
Any diuretic 1.78 (1.36– 2.35) <0.001
Digitalis use 2.88 (2.03– 4.09) <0.001
Anti-arrhythmic med use 2.36 (1.47– 3.80) <0.001
Randomization to trandolapril 0.73 (0.57– 0.93) 0.01
All potential variables with significance <0.05 were eligible for the final model. All variables were tested in separate Cox regression models withtreatment. A backwards selection procedure was used to eliminate variables at the 0.05 level of significance. The same variables remained whenapproached with a forward selection model. The proportional hazards assumption was tested and confirmed for all final covariates.
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Lewis et al. Page 15
Tabl
e 3
Mul
tivar
iabl
e C
ox re
gres
sion
mod
el a
nd in
tege
r-ba
sed
risk
scor
e as
sign
men
t to
quan
tify
the
pred
icto
rs o
f hea
rt fa
ilure
Bas
elin
e C
hara
cter
istic
sE
stim
ate
Stan
dard
Err
orH
R
(95%
Con
fiden
ceIn
terv
alp-
valu
e
Ris
kSc
ore
Plac
ebo
(vs T
rand
olap
ril)
0.32
050
0.12
382
1.38
(1.0
8– 1
.76)
0.01
01
Age
65–
74 y
ears
(vs <
65
year
s)0.
6355
70.
1505
91.
89(1
.41–
2.5
4)<0
.001
2
Age
≥75
yea
rs (v
s < 6
5 ye
ars)
1.14
653
0.18
174
3.15
(2.2
0– 4
.49)
<0.0
014
Bod
y M
ass I
ndex
≥35
kg/
m2 (
vs. <
35)
0.73
804
0.17
998
2.09
(1.4
7– 2
.98)
<0.0
012
His
tory
of:
M
yoca
rdia
l Inf
arct
ion
0.32
584
0.12
921
1.39
(1.0
8– 1
.78)
0.01
1
C
oron
ary
arte
ry b
ypas
s gra
ft su
rger
y0.
4567
60.
1267
51.
58(1
.23–
2.0
2)<0
.001
1
D
iabe
tes
0.74
401
0.13
207
2.10
(1.6
2– 2
.73)
<0.0
012
H
yper
tens
ion
0.48
222
0.13
422
1.62
(1.2
5– 2
.11)
<0.0
012
A
ngin
a*0.
3341
30.
1286
61.
40(1
.09–
1.8
0)0.
009
1
St
roke
or t
rans
ient
isch
emic
atta
ck0.
6013
90.
1723
41.
82(1
.30–
2.5
6)<0
.001
2
Cur
rent
smok
er0.
6207
50.
1691
51.
86(1
.34–
2.5
9)<0
.001
2
eGFR
* <
60 m
l/min
/m2 (
vs. ≥
60)
0.51
334
0.13
603
1.67
(1.2
8– 2
.18)
<0.0
012
LVEF
* 41
–50%
(vs ≥
50%
)0.
3398
50.
1529
81.
40(1
.04–
1.9
0)0.
031
Non
-ran
dom
ized
med
icin
es
C
alci
um C
hann
el B
lock
er0.
3420
90.
1262
71.
41(1
.10–
1.8
0)0.
007
1
N
ot o
n lip
id lo
wer
ing
med
icin
e0.
5202
40.
1248
71.
68(1
.32–
2.1
5)<0
.001
2
A
ny d
iure
tic0.
5842
60.
1400
61.
79(1
.36–
2.3
6)<0
.001
2
D
igita
lis u
se1.
0795
30.
1812
22.
94(2
.06–
4.2
0)<0
.001
3
A
nti-a
rrhy
thm
ic m
ed u
se0.
9303
90.
2428
32.
54(1
.58–
4.0
8)<0
.001
3
* LVEF
-Lef
t ven
tricu
lar e
ject
ion
frac
tion,
eG
FR-e
stim
ated
glo
mer
ular
filtr
atio
n ra
te u
sing
MD
RD
equ
atio
n, H
R –
Haz
ard
ratio
. Ang
ina
was
mea
sure
d us
ing
the
Can
adia
n C
lass
ifica
tion
Syst
em. R
isk
scor
eca
lcul
ated
by
usin
g di
vidi
ng e
ach
coef
ficie
nt b
y th
e sm
alle
st c
oeff
icie
nt a
nd ro
undi
ng to
the
near
est i
nteg
er.
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Lewis et al. Page 16
Tabl
e 4
Val
idat
ion
of C
AR
E ris
k m
odel
usi
ng th
e PE
AC
E Po
pula
tion
Var
iabl
e
N w
ithou
tcom
e(%
)p-
valu
eH
azar
dR
atio
95%
Haz
ard
Rat
ioC
onfid
ence
Lim
its*
Usin
g CA
RE ri
sk m
odel
*
Low
Ris
k2
(0.3
)R
ef
Inte
rmed
iate
Ris
k (v
s Low
Ris
k)25
8 (3
.4)
<0.0
0110
.02.
540
.3
Hig
h ris
k (v
s Low
Ris
k)8
(10.
8)<0
.001
35.8
7.6
168.
6
Usin
g PE
ACE
risk
mod
el†
Low
Ris
k83
(1.4
)R
ef
Inte
rmed
iate
Ris
k (v
s Low
Ris
k)14
5 (7
.2)
<.00
015.
64.
37.
3
Hig
h ris
k (v
s Low
Ris
k)40
(27.
6)<.
0001
24.9
17.1
36.3
* Low
risk
was
def
ined
as a
pat
ient
you
nger
than
55
with
LV
EF>5
0% a
nd d
id n
ot h
ave
diab
etes
or h
yper
tens
ion.
Hig
h ris
k w
as d
efin
ed a
s pat
ient
s old
er th
an 6
0 ye
ars w
ith L
VEF
<50%
and
bot
h di
abet
es a
ndhy
perte
nsio
n. A
ll ot
her p
atie
nts w
ere
inte
rmed
iate
risk
.
† Low
risk
was
def
ined
as a
PEA
CE
HF
Ris
k sc
ore
<9, i
nter
med
iate
pat
ient
s had
a ri
sk sc
ore
of 9
–14
and
high
risk
pat
ient
s had
a ri
sk sc
ore>
14.
Circ Heart Fail. Author manuscript; available in PMC 2010 December 23.
Related Documents