Quality of Life Predictors of distress and poorer quality of life in High Grade Glioma patients Georgia K.B. Halkett a, *, Elizabeth A. Lobb b,c , Michelle M. Rogers a , The ´re ` se Shaw d , Anne P. Long e , Helen R. Wheeler f , Anna K. Nowak e,g a School of Nursing and Midwifery, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australia b Calvary Health Care Kogarah and Cunningham Centre for Palliative Care, Sydney, New South Wales, Australia c School of Medicine, The University of Notre Dame, Sydney, New South Wales, Australia d Telethon Kids Institute, University of Western Australia, Perth, Western Australia, Australia e Department of Medical Oncology, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia f Medical Oncology, Royal North Shore Hospital, Sydney, New South Wales, Australia g School of Medicine and Pharmacology, University of Western Australia, Perth, Western Australia, Australia 1. Introduction The median survival from High Grade Glioma (HGG) ranges from less than 1 year to 3 years from diagnosis [1]. In facing this life- limiting illness, patients must manage emotions, make treatment decisions, and adjust to lifestyle changes. These adjustments are needed to cope with actual and potential functional, emotional or cognitive decline. Additionally, this diagnosis is often associated with an inability to work, drive, or participate in previously productive activities [2,3]. Most patients face gradual cognitive decline, with some suffering impairment after initial surgery. This diagnosis has a profound impact on patients’ quality of life (QOL), and practical, emotional, and information related needs [4]. An Australian study in self-selected glioma patients participating at varied time points post-diagnosis reported significantly lower QOL than general population norms [5,6]. There is limited research describing QOL during active treatment outside the context of therapeutic clinical trials. A recent study found that 48% of patients newly diagnosed with brain tumours experienced high levels of distress, significantly Patient Education and Counseling 98 (2015) 525–532 A R T I C L E I N F O Article history: Received 26 August 2014 Received in revised form 5 December 2014 Accepted 6 January 2015 Keywords: High Grade Glioma Distress Quality of life Supportive care needs Questionnaire A B S T R A C T Objective: To determine High Grade Glioma (HGG) patients’ levels of distress and QOL during combined chemoradiotherapy, explore predictors of distress and QOL and prioritize patients’ supportive care needs. Methods: Patients diagnosed with HGG who were referred for combined chemoradiotherapy were recruited. Participants completed demographics and questionnaires assessing distress, function, and supportive care needs. Descriptive statistics, correlation coefficients, t-tests and linear and logistic regression analyses were performed. Results: 116 participants completed the questionnaire. Participants scored lower for QOL in physical, functional and emotional domains than the general Australian population. Poor physical function, lower education levels, loss of employment and financial impact associated with diagnosis were consistently linked with multiple domains of distress, poor QOL and high unmet needs. Having a carer who was their partner predicted lower emotional well-being. Conclusion: Patients with HGG experience a poor QOL, increased levels of distress and high unmet needs when commencing chemoradiotherapy. Patients who experience a financial impact and those with lower education levels may report higher levels of distress and increased unmet needs. Practice implications: Poor function, lower education and limited financial resources may help identify those who require additional screening and may benefit from additional information and psychological support at this time. ß 2015 Elsevier Ireland Ltd. All rights reserved. * Corresponding author at: School of Nursing and Midwifery, Faculty of Health Sciences, Curtin University, GPO Box U1987, Perth, WA 6845, Australia. Tel.: +61 418838914; fax: +61 8 9266 2508. E-mail address: [email protected] (Georgia K.B. Halkett). Contents lists available at ScienceDirect Patient Education and Counseling jo ur n al h o mep ag e: w ww .elsevier .co m /loc ate/p ated u co u http://dx.doi.org/10.1016/j.pec.2015.01.002 0738-3991/ß 2015 Elsevier Ireland Ltd. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Patient Education and Counseling 98 (2015) 525–532
Quality of Life
Predictors of distress and poorer quality of life in High Grade Gliomapatients
Georgia K.B. Halkett a,*, Elizabeth A. Lobb b,c, Michelle M. Rogers a, Therese Shaw d,Anne P. Long e, Helen R. Wheeler f, Anna K. Nowak e,g
a School of Nursing and Midwifery, Faculty of Health Sciences, Curtin University, Perth, Western Australia, Australiab Calvary Health Care Kogarah and Cunningham Centre for Palliative Care, Sydney, New South Wales, Australiac School of Medicine, The University of Notre Dame, Sydney, New South Wales, Australiad Telethon Kids Institute, University of Western Australia, Perth, Western Australia, Australiae Department of Medical Oncology, Sir Charles Gairdner Hospital, Perth, Western Australia, Australiaf Medical Oncology, Royal North Shore Hospital, Sydney, New South Wales, Australiag School of Medicine and Pharmacology, University of Western Australia, Perth, Western Australia, Australia
A R T I C L E I N F O
Article history:
Received 26 August 2014
Received in revised form 5 December 2014
Accepted 6 January 2015
Keywords:
High Grade Glioma
Distress
Quality of life
Supportive care needs
Questionnaire
A B S T R A C T
Objective: To determine High Grade Glioma (HGG) patients’ levels of distress and QOL during combined
chemoradiotherapy, explore predictors of distress and QOL and prioritize patients’ supportive care
needs.
Methods: Patients diagnosed with HGG who were referred for combined chemoradiotherapy were
recruited. Participants completed demographics and questionnaires assessing distress, function, and
supportive care needs. Descriptive statistics, correlation coefficients, t-tests and linear and logistic
regression analyses were performed.
Results: 116 participants completed the questionnaire. Participants scored lower for QOL in physical,
functional and emotional domains than the general Australian population. Poor physical function, lower
education levels, loss of employment and financial impact associated with diagnosis were consistently
linked with multiple domains of distress, poor QOL and high unmet needs. Having a carer who was their
partner predicted lower emotional well-being.
Conclusion: Patients with HGG experience a poor QOL, increased levels of distress and high unmet needs
when commencing chemoradiotherapy. Patients who experience a financial impact and those with
lower education levels may report higher levels of distress and increased unmet needs.
Practice implications: Poor function, lower education and limited financial resources may help identify
those who require additional screening and may benefit from additional information and psychological
support at this time.
� 2015 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Patient Education and Counseling
jo ur n al h o mep ag e: w ww .e lsev ier . co m / loc ate /p ated u co u
1. Introduction
The median survival from High Grade Glioma (HGG) ranges fromless than 1 year to 3 years from diagnosis [1]. In facing this life-limiting illness, patients must manage emotions, make treatmentdecisions, and adjust to lifestyle changes. These adjustments areneeded to cope with actual and potential functional, emotional or
* Corresponding author at: School of Nursing and Midwifery, Faculty of Health
Sciences, Curtin University, GPO Box U1987, Perth, WA 6845, Australia.
Tel.: +61 418838914; fax: +61 8 9266 2508.
E-mail address: [email protected] (Georgia K.B. Halkett).
http://dx.doi.org/10.1016/j.pec.2015.01.002
0738-3991/� 2015 Elsevier Ireland Ltd. All rights reserved.
cognitive decline. Additionally, this diagnosis is often associatedwith an inability to work, drive, or participate in previouslyproductive activities [2,3]. Most patients face gradual cognitivedecline, with some suffering impairment after initial surgery.
This diagnosis has a profound impact on patients’ quality of life(QOL), and practical, emotional, and information related needs [4].An Australian study in self-selected glioma patients participatingat varied time points post-diagnosis reported significantly lowerQOL than general population norms [5,6]. There is limited researchdescribing QOL during active treatment outside the context oftherapeutic clinical trials.
A recent study found that 48% of patients newly diagnosed withbrain tumours experienced high levels of distress, significantly

G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532526
more than following other cancer diagnoses [7]. Furthermore, theincidence of depression and anxiety in patients with brain cancer ishigh (48%) [8]. Thirty percent of patients with brain cancer reportanxiety and 17% report depression [5,6]. Anxiety and depressionwere correlated with QOL [5,6]. Depression is important not onlyfor its impact on QOL, but also as a predictor of poor adherence tooral chemotherapy [9] and lower satisfaction with cancer care [10].
Coinciding with high levels of distress, anxiety, depression andpoor QOL, patients with brain cancer report many unmet needsand dissatisfaction with information from healthcare providers[8]. A review on the needs of patients with malignant glioma andtheir carers demonstrated needs for information about diseaseprogression, treatment, psychological and social support, commu-nication with health professionals, and a key professional tocoordinate care [11]. Additional unmet needs included dealingwith fatigue, uncertainty about the future, difficulty with activitiesof daily living, and access to support services [5,6,12].
Our previous qualitative research highlighted patient dependen-cy on their carers to support them in every aspect of their lives [13–15]. Comprehending the patients’ prognosis was a major barrier forboth [15]. Four major themes were identified: (1) feelings ofuncertainty around prognosis and QOL; (2) the need for tailoredinformation on their individual clinical situation, needs andpreferences; (3) dependence on carers due to cognitive deficits,loss of balance and inability to drive; and (4) the importance ofskilled communication with health professionals around prognosticuncertainty and disease progression with communication barriersdue to complex language deficits [13]. Patients required informationand support during combined chemoradiotherapy.
This paper focuses on the needs of HGG patients during initialactive treatment. At this time, patients are newly engaged with thehealthcare system and providers have an opportunity to identifyand address unmet needs. Specifically, we aimed to determineHGG patients’ levels of distress and QOL during combinedchemoradiotherapy, explore predictors of distress and QOL andprioritize patients’ supportive care needs to direct and informservice provision. The strength of this paper is that it focusesexclusively on a homogenous population diagnosed with HGG at auniform time point (during combined chemoradiotherapy).
2. Materials and methods
Institutional human research ethics committee ethics approvalwas obtained from all sites. Participants gave written informedconsent. Eligible participants were people diagnosed with GradeIII-IV HGG, aged 18 years or older, and planned to start combinedchemoradiotherapy. Potential participants were excluded if theywere unable to complete questionnaires for language, literacy orphysical reasons. Participants were recruited from neurosurgical,radiation or medical oncology outpatient departments at fourtertiary neuro-oncology sites in two Australian states. Each siteserviced the majority of patients in their geographic area.Participants were recruited by the research assistant after theirinitial appointment with their medical oncologist and prior tocompleting combined chemoradiotherapy. The research assistantobtained informed consent and provided the initial questionnairein person. She was available to assist with understanding orclarifying questions if necessary. Subsequent questionnaires weremailed to participants. If patients required they could also seekhelp from their carers to physically complete the questionnaires.
Participants completed questionnaires at 3 time points: duringchemoradiotherapy, and 3 and 6 months later respectively. Carerswere also invited to participate in the study. However, patientswere still eligible for the study if carers declined participation. Thismanuscript describes the baseline patient data prior to completingchemoradiotherapy.
2.1. Study tools
The participant questionnaire comprised: demographics, theDistress Thermometer [16], the Functional Assessment of CancerTherapy-General Index (FACT-G), Functional Assessment of CancerTherapy-Brain Index (FACT-Br; the FACT-G with the addition of abrain cancer specific sub scale) [17,18], the Supportive Care NeedsScale (SCNS-34) [19], Brain Tumour Specific Supportive Care NeedsScale (BrTSCNS) [5,6] and information needs.
Demographic information included: gender, age, level ofeducation, employment status prior to and after diagnosis, thefinancial impact of the diagnosis, whether the patient was caringfor anyone else, whether the patient currently had a carer, andtheir current level of physical dependency as measured by a self-report description of Eastern Co-operative Oncology Group (ECOG)performance status (PS) [20] ranging from 0 (fully independent) to4 (completely disabled – cannot carry on any self-care). Financialimpact of the diagnosis was assessed by asking participants whateffect their diagnosis had on them financially with the followingpossible responses: (a) Had no effect on my financial situation; (b)Had a slight effect on me financially; (c) Had a significant effect onme financially and (d) other. These responses were dichotomisedto ‘no or slight effect’ and ‘significant effect’ during data analysis.
The Distress Thermometer is a validated self-report visualanalogue scale quantifying how distressed participants have feltover the past week. The scale ranges from 0 (no distress) to 10(extreme distress). Scores of 5 and 6 indicate moderate distress,while scores of 7 or greater indicate high distress [16].
The FACT tools are reliable and valid surveys that measurehealth related QOL in the past seven days [17,18]. The FACT-G is ageneral cancer QOL scale with subscales addressing physical well-being (PWB), social/family well-being (SWB), emotional well-being (EWB) and functional well-being (FWB). The FACT-Brconsists of the FACT-G with an additional brain cancer specificsubscale (BrCS). Summary scores can be calculated for thesubscales as well as an overall score, with higher scores indicatingbetter quality of life.
The SCNS-34 is a reliable and valid tool containing 34 itemsassessing the impact of cancer on participants’ lives [19]. Partici-pants indicate whether each listed need applies to them and if so,how well they feel these needs are being addressed. Participants’needs are assessed across the following areas: psychological,health system and information, physical and daily living, patientcare and support, and sexuality. Participants can select thefollowing categories – ‘‘not applicable’’, ‘‘satisfied’’, ‘‘low need’’,‘‘moderate need’’ and ‘‘high need’’. Responses were dichotomizedinto moderate or high need vs low or no need and items rankedbased on the percentage of participants with a moderate/high levelof need.
Participants’ level of needs to access services were also assessedusing the access to services supplement to the SCNS-34 comprising16 items relating to services available to cancer patients (e.g.financial, parking, transport, respite, etc.).
The BrTSCNS is a validated 16-item tool developed specificallyfor brain cancer patients [5]. It has a similar structure to the SCNS-34 and is designed to be co-administered with this scale.
Participants also answered questions about which informationsources they preferred (written, verbal, web based, group education,DVD or other) and accessing additional information sources (e.g.internet, library/books, relatives/friends, support group/otherpatients).
2.2. Data analysis
Based on initial power calculations, the study aimed to recruit200 patients; however, due to slow recruitment the study closed

G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532 527
early with 116 patients. A sample of 116 has 80% power to detect amean difference between two independent groups in the order of.5 (i.e. a moderate effect size (alpha = .05, two-sided test)).
Descriptive statistics, correlation coefficients, t-tests and linearand logistic regression analyses were performed using IBM SPSS(Version 22). The strongest correlates of each of the dependentvariables (namely the scores on the Distress Thermometer, thecombined scores for the FACT-G quality of life scales and subscales,the top ten ranked supportive care needs (SCNS-34) and topten ranked brain tumour specific needs (BrTSCNS)) were identifiedusing a two-phase variable selection process using an alphalevel of .05 for each stage. In the first phase, variables significantlyassociated with the relevant dependent variable were identifiedin univariable analyses. In the second, these were entered intomultivariable models and backwards elimination applied toidentify the most parsimonious models. Analyses were conductedto ensure the final models were not sensitive to the order in whichthe variables were eliminated. Results from the final models withthe strongest correlates are presented. This process was also usedto assess if patients’ information needs, understanding andpreference differed by level of education.
3. Results
Here we report results from patient participants duringcombined chemoradiotherapy (we report elsewhere on carers’
Table 1Patient baseline characteristics (n = 116).
Variable Category
Gender Male
Female
Tumour grade IV
III
Marital statusa Married/partner
Never married
Divorced/separated
Widowed
Level of Educationa High school or less
Tertiary education
Employment status changes Stayed the same
Dropped hours or stopped
Financial effect of diagnosisa No or slight effect
Significant effect
Caring for anyone else in homea Yes
No
Currently has a carera Yes
Carer is their partner
Carer is not their partner
No
Patient self-reported ECOG
status (level of physical
dependency)a
0: Fully independent
1: Restricted in physically strenuous
light work tasks
2: Able to move freely, capable of se
Up and about more than 50% of time
3: Limited in self-care ability, confin
4: Completely disabled, cannot carry
Employment
Full-time
Part-time
Unemployed
Retired
Self employed
Homemaker
Disability pension/stress leave/unable to work
a Missing data has resulted in this variable not summing to 100%.
data). 165 patient participants were assessed as eligible,127 consented and 116 completed baseline questionnaires (91%response rate). Reasons given for not participating includedphysical and emotional stress, lack of interest, patient admittedto hospital, patients’ cognitive health poor and would havedifficulty completing questionnaires.
All participants were diagnosed with HGG (glioblastoma,gliosarcoma, anaplastic astrocytoma, anaplastic oligodendro-glioma or anaplastic oligoastrocytoma). However, as chemora-diotherapy is standard care for glioblastoma/gliosarcoma only,this comprised the majority of diagnoses. A small proportion ofparticipants had grade III glioma (6%) because they wereundergoing combined chemoradiotherapy on a clinical trialprotocol or for other reasons. The mean age was 56 (SD = 13.3,range = 18–86 years). Table 1 summarizes baseline demographics.
3.1. Quality of life
Participants’ QOL was assessed using the FACT-G, FACT-Br andsubscales (Fig. 1). Participants scored higher on social and physicalwell-being than on emotional and functional well-being. Asexpected, they reported lower scores for the physical, functionaland emotional domains than the general Australian population [20].However, perceptions of social well-being were more positive thanthe available population norms (M = 23.2, SD = 4.7; M = 19.2,SD = 6.6). On the FACT-G, the HGG participants scored 10 points
n (%)
82 (70.7%)
34 (29.3%)
109 (93.9%)
7 (6.0%)
95 (82.9%)
5 (4.3%)
12 (10.3%)
3 (2.6%)
54 (46.6%)
60 (51.7%)
71 (61.2%)
45 (38.8%)
64 (55.2%)
49 (42.2%)
21 (18.1%)
94 (81.0%)
109 (94.0%)
91 (78.4%)
18 (15.5%)
6 (5.2%)
37 (31.9%)
activity but able to move freely and can carry out 41 (35.3%)
lf-care tasks, but unable to carry out work activities.
.
27 (23.3%)
ed to bed or chair 50% of waking hours. 8 (6.9%)
out most self-care tasks, confined to bed or chair. 2 (1.7%)
Pre-diagnosis Post-diagnosis
58 (50.0%) 24 (20.7%)
7 (6.0%) 2 (1.7%)
6 (5.2%) 23 (19.8%)
34 (29.3%) 37 (31.9%)
8 (6.9%) 10 (8.6%)
3 (2.6%) 1 (.9%)
– 19 (16.4%)
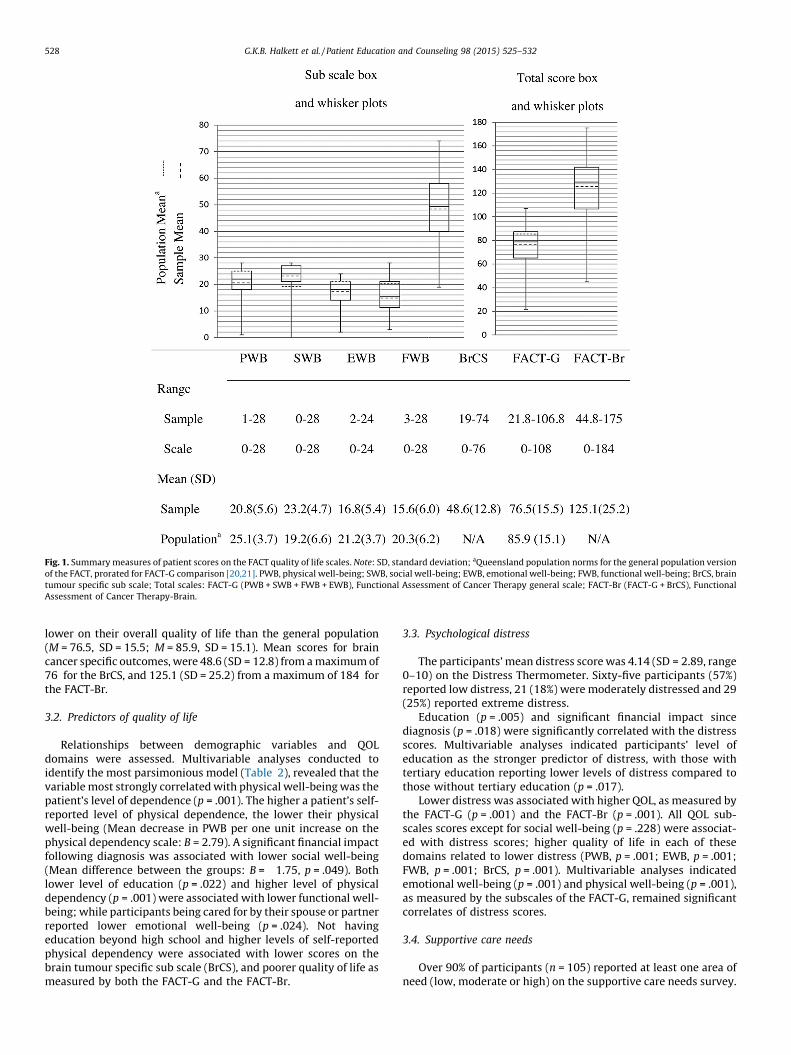
Fig. 1. Summary measures of patient scores on the FACT quality of life scales. Note: SD, standard deviation; aQueensland population norms for the general population version
of the FACT, prorated for FACT-G comparison [20,21]. PWB, physical well-being; SWB, social well-being; EWB, emotional well-being; FWB, functional well-being; BrCS, brain
tumour specific sub scale; Total scales: FACT-G (PWB + SWB + FWB + EWB), Functional Assessment of Cancer Therapy general scale; FACT-Br (FACT-G + BrCS), Functional
Assessment of Cancer Therapy-Brain.
G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532528
lower on their overall quality of life than the general population(M = 76.5, SD = 15.5; M = 85.9, SD = 15.1). Mean scores for braincancer specific outcomes, were 48.6 (SD = 12.8) from a maximum of76 for the BrCS, and 125.1 (SD = 25.2) from a maximum of 184 forthe FACT-Br.
3.2. Predictors of quality of life
Relationships between demographic variables and QOLdomains were assessed. Multivariable analyses conducted toidentify the most parsimonious model (Table 2), revealed that thevariable most strongly correlated with physical well-being was thepatient’s level of dependence (p = .001). The higher a patient’s self-reported level of physical dependence, the lower their physicalwell-being (Mean decrease in PWB per one unit increase on thephysical dependency scale: B = 2.79). A significant financial impactfollowing diagnosis was associated with lower social well-being(Mean difference between the groups: B = �1.75, p = .049). Bothlower level of education (p = .022) and higher level of physicaldependency (p = .001) were associated with lower functional well-being; while participants being cared for by their spouse or partnerreported lower emotional well-being (p = .024). Not havingeducation beyond high school and higher levels of self-reportedphysical dependency were associated with lower scores on thebrain tumour specific sub scale (BrCS), and poorer quality of life asmeasured by both the FACT-G and the FACT-Br.
3.3. Psychological distress
The participants’ mean distress score was 4.14 (SD = 2.89, range0–10) on the Distress Thermometer. Sixty-five participants (57%)reported low distress, 21 (18%) were moderately distressed and 29(25%) reported extreme distress.
Education (p = .005) and significant financial impact sincediagnosis (p = .018) were significantly correlated with the distressscores. Multivariable analyses indicated participants’ level ofeducation as the stronger predictor of distress, with those withtertiary education reporting lower levels of distress compared tothose without tertiary education (p = .017).
Lower distress was associated with higher QOL, as measured bythe FACT-G (p = .001) and the FACT-Br (p = .001). All QOL sub-scales scores except for social well-being (p = .228) were associat-ed with distress scores; higher quality of life in each of thesedomains related to lower distress (PWB, p = .001; EWB, p = .001;FWB, p = .001; BrCS, p = .001). Multivariable analyses indicatedemotional well-being (p = .001) and physical well-being (p = .001),as measured by the subscales of the FACT-G, remained significantcorrelates of distress scores.
3.4. Supportive care needs
Over 90% of participants (n = 105) reported at least one area ofneed (low, moderate or high) on the supportive care needs survey.

Table 2Final general linear models for FACT-G, FACT-Br and sub scales.
Total score Sub scale Predictor F B [95% CI] p
PWB ECOG 36.76 �2.79 [�3.70, �1.88] <.001
SWB Finance 3.97 �1.75 [�.01, �3.50] .049
FWB Education 5.41 2.27 [.34, 4.21] .022
ECOG 31.73 �2.77 [�3.75, �1.80] <.001
EWB Partner carer 5.22 �2.80 [�5.22, �.37] .024
FACT-G Education 6.53 6.71 [1.50, 11.91] .012ECOG 19.13 �5.80 [�8.42, �3.17] <.001
BrCS Education 5.50 4.40 [.68, 8.12] .021
ECOG 67.10 �7.75 [�9.62, �5.87] <.001
FACT-Br Education 8.10 11.02 [3.35, 18.69] .005ECOG 47.67 �13.49 [�17.36, �9.62] <.001
Note: CI, confidence interval. Subscales: PWB, physical well-being; SWB, social well-being; FWB, functional well-being; EWB, emotional well-being; BrCS, brain tumour
specific sub scale. Total scales: FACT-G (PWB + SWB + FWB + EWB), Functional Assessment of Cancer Therapy general scale; FACT-Br (FACT-G + BrCS), Functional Assessment of
Cancer Therapy-Brain. Total scale models are in boldface. Predictors: ECOG, self-reported ECOG status or level of dependency; Finance, significant/non-significant financial
impact of diagnosis (1: Significant); Education, tertiary education or not (1: Tertiary); Partner carer, carer is spouse/partner or not (1: Spouse/partner).
G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532 529
On average, participants reported 11 areas of need (M = 11.1,SD = 8.71, range 0–32) from a maximum possible of 34. The meannumber of items for which patients expressed a moderate to highneed was 6 (range 0–22). Participants reporting greater than 11unmet needs (11 = the average; N = 50 of 116) were significantlymore distressed than those with average or below average unmetneeds (DT M = 5.38 (2.64) vs M = 3.18 (2.72), p = .001).
A decrease in employment (p = .017), the financial impact ofdiagnosis (p = .017), and the reported level of physical dependency(p = .013) predicted more unmet needs. Those who experienced adecrease in the level of employment since diagnosis reported moreunmet needs (M = 13.5 (9.0)) than those who had not experienceda decrease (M = 9.6 (8.2)). Similarly, those for whom their diagnosishad a significant financial impact also reported significantly moreunmet needs (M = 13.2 (8.9)) than those who reported ‘‘no’’ to‘‘slight’’ financial effect (M = 9.3 (8.3)). As the level of physicaldependence increased, so did the number of unmet needs(p = .013). Additionally, it was found that if participants did notfeel adequately involved in decisions, they reported significantlymore unmet needs compared to those who felt they were involved(M = 17.4 (9.7) vs M = 9.8 (7.9), p < .001).
Predictors of the top 10 needs (based on percentage ofparticipants expressing a moderate to high need) were deter-mined (Table 3). The only significant predictor of the top need (i.e.the need for help due to the participant’s ‘Concerns about the
worries of those close to them’) was whether their illness had a
Table 3Patients’ ten most commonly reported areas for moderate to high levels of need and fi
Rank Reported need %
1 Concerns about the worries of those close to them 39.5
2 Not being able to do the things they used to 36.0
3 Uncertainty about the future 30.4
4 Feeling down or depressed 28.4
5 Anxiety 28.3
6 Being informed about their test results as soon as feasible 27.4
7 Lack of energy/tiredness 25.9
8 Being informed about things they can do to help
themselves get well
24.3
9 Feelings of sadness 23.9
10 Being informed about cancer that is under control or
diminishing (that is, remission)
23.0
Note: OR, odds ratio; CI, confidence interval; Predictors: ECOG, self-reported ECOG stat
diagnosis (1: Significant); Education, tertiary education or not (1: Tertiary); Married/w
significant financial impact. Participants for whom this was thecase had 2.7 greater odds of expressing this need compared tothose for whom the financial impact had been slight or less. Notunexpectedly, participants’ self-reported level of physical depen-dency predicted whether they needed help as a result of not beingable to function as before, with the odds of the participant having amoderate to high need due to ‘Not being able to do the things they
used to’ increasing by 2.6 for every one unit increase in level ofphysical dependency score. Participants with a tertiary educationexpressed fewer needs resulting from ‘Uncertainty about the
future’ (OR = .39), ‘lack of energy and tiredness’ (OR = .30), and‘feelings of sadness’ (OR = .34) than those without a tertiaryeducation. In addition to their concerns about those close to them,participants whose financial situation had been significantlyimpacted had increased odds of expressing needs related topsychological outcomes (i.e. depression, anxiety and sadness), aswell as an almost five-fold higher odds of needing support as aresult of a lack of energy and fatigue. Older participants expressedneeds related to anxiety and sadness more so than youngerpatients, with the odds of reporting a need due to anxietyincreasing by 7% per year of patient age.
3.5. Access to services needs
Participants’ level of needs to access services was also assessed.The highest level of need reported was for easy car parking at the
nal predictor models of these needs.
Predictor OR [95% CI] p
Finance 2.69 [1.23, 5.90] .013
ECOG 2.60 [1.63, 4.15] <.001
Education .39 [.17, .89] .025
Finance 2.49 [1.08, 5.74] .033
Finance 3.97 [1.50, 10.55] .006
Age 1.07 [1.02, 1.12] .006
–
Education .30 [.11, .85] .024
Finance 4.91 [1.66, 14.5] .004
ECOG 2.54 [1.47, 4.40] .001
Married/with partner .31 [.11, .85] .023
Education .34 [.13, .94] .038
Finance 3.50 [1.18, 10.4] .024
Age 1.07 [1.02, 1.12] .010
Married/with partner .21 [.08, .59] .003
us or level of dependency; Finance, significant/non-significant financial impact of
ith partner, patient is either married or has a partner (1: married/partner).

Table 4Patients’ ten most commonly reported areas for moderate to high levels of brain cancer specific needs and final predictor models of these needs.
Rank Reported need % Predictor OR [95% CI] p
1 Information on the latest developments in the research and treatment of brain tumours 28.1 (None)
2 Feeling like you are not the same person you were before the brain tumour 27.0 Finance 4.16 [1.63, 10.61] .003
ECOG 1.94 [1.22, 3.08] .005
3 Physical side effects from the tumour and/or treatment 23.5 Partner carer .35 [.13, .96] .041
ECOG 1.64 [1.06, 2.55] .028
4 Financial assistance/advice 21.4 Finance 14.87 [3.74, 59.10] <.001
ECOG 2.81 [1.52, 5.21] .001
5 Special testing and advice about mental thinking abilities 16.8 ECOG 2.67 [1.54, 4.65] .001
6 Rehabilitation services such as occupational therapists,
speech pathologists or physiotherapists.
16.2 ECOG 3.02 [1.66, 5.47] <.001
7 Internet or email to receive information and/or emotional
support
15.8 Education 3.61 [1.10, 11.88] .035
8 Legal assistance/advice 14.4 ECOG 1.84 [1.09, 3.12] .022
9 Change in your mental or thinking ability 13.9 Employ drop 3.71 [1.1, [12.06] .030
ECOG 1.84 [1.05, 3.20] .032
10 Talking to other people with a similar experience 12.3 Employ drop 4.64 [1.36, 15.89] .014
Note: OR, odds ratio; CI, confidence interval; Predictors: ECOG, self-reported ECOG status or level of physical dependency; Finance, significant/non-significant financial impact
of diagnosis (1: Significant); Education, tertiary education or not (1: Tertiary); Partner carer, carer is spouse/partner or not (1: Spouse/partner); Employ drop, patients
employment has stayed the same or dropped since diagnosis (1: Dropped).
G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532530
hospital or clinic (36%), followed by access to monetary allowancefor travel, treatment and equipment expenses (22%). The thirdhighest need was access to transport service to and from thehospital or clinic (10%).
3.6. Brain tumour specific needs
The most commonly reported moderate to high levels of braincancer specific needs are reported in Table 4. The top rankedneed, ‘information on the latest developments in the research and
treatment of brain tumours’ was not significantly correlated withany demographic or other variables assessed, indicating thisneed did not occur differentially for some groups vs others. Thesecond highest reported need of ‘Feeling like you are not the same
person you were before the brain tumor’ was four times more likely(OR = 4.16) to be reported for those who experienced significantfinancial impact. Not surprisingly, those who reported asignificant financial impact of diagnosis were also around 15times more likely to report a moderate to high need for ‘Financial
assistance/advice’ (OR = 14.87). Participants who had a carerwho was their partner, were less likely (OR = .35) to reportthat ‘Physical side effects from the tumour and/or treatment’ werea concern. For every one point increase in level of dependence,reporting a range of needs related to ‘Physical side effects from
the tumour and/or treatment’ (OR = 1.64), ‘Feeling like you are
not the same person you were before the brain tumor’ (OR = 1.94),‘Legal assistance/advice’ (OR = 1.84), ‘Change in your mental or
thinking ability’ (OR = 1.84), and ‘Special testing and advice about
mental thinking abilities’(OR = 2.67), ‘Financial assistance/advice’(OR = 2.81), and ‘Rehabilitation services such as occupational
Table 5Percentages of patients with and without tertiary education, who reported seeking
additional information about their illness and what source they used.
Source % of patients
Non-tertiary
education
Tertiary
education
Any source 42% 56%
The cancer council 9% 20%
Internet 22% 30%
Library/books 1% 4%
Relatives/friends 8% 13%
Support group/other patients 2% 20%
Note: These differences were not statistically significant assessed at a = .05.
therapists, speech pathologists or physiotherapists’ (OR = 3.02),also increased.
Tertiary education was the only correlate with the need for‘Internet or email to receive information and/or emotional support’,those with tertiary education being just over 3.5 times more likelyto report a need in this area compared to those without tertiaryeducation. Participants who experienced a decrease in employ-ment since diagnosis were 3.7 times more likely to report needs inrelation to ‘Change in your mental or thinking ability’ and 4.6 timesmore likely to report needs associated with ‘Talking to other people
with a similar experience’ than those who did not experience adecrease in employment.
3.7. Information needs
Those with higher education were more likely to report apreference for written material (p = .04) and were less likely toreport being adequately involved in treatment decisions(p = .012), than those without tertiary education. Those withhigher education were more likely to reported seeking informa-tion from other sources; however, these differences were notstatistically significant (Table 5). There were no other statisticallysignificant relationships between level of education and informa-tion variables.
4. Discussion and conclusion
4.1. Discussion
This is the first study to specifically explore the QOL, distresslevels and unmet needs of people with HGG during initial activetreatment. We have also identified correlates to help clinicianspredict those patients who are more likely to experience worseQOL and higher needs, and target more intensive screening andsupport to these groups. Poor physical function, lower educationlevels, loss of employment and a financial impact of the diagnosiswere consistently linked with multiple domains of distress, poorquality of life and high unmet needs.
Participants in this study scored lower for QOL in physical,functional and emotional domains than the general Australianpopulation [21,22], a finding which was not unexpected.However, the importance of financial strain as a predictor ofpoor social well-being, more distress, and greater levels of unmet

G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532 531
needs is clear in our results. Previous studies have identified thatpatients with brain cancer may experience financial difficultiesafter diagnosis [23–25]. This study highlights the impact of HGGon the patient’s immediate financial situation due to the suddenloss of employment in the context of immediate physical andcognitive impact of the newly diagnosed cancer, often with noprospect for return, and the downstream effects on patientwellbeing and unmet needs. Furthermore, if the carer is also thepartner of the patient, the patient diagnosis may also impact onthe carer’s ability to work to capacity, compounding the financialcrisis. Healthcare professionals should be aware of the impact ofchange of employment status, enquire regarding financial strain,and advocate for early outpatient involvement of financialcounselling, social workers, and financial assistance for thosewho have had a change of employment status.
Similar to previous findings perceptions of social well-beingin participants in this study were more positive than thepopulation norm [6,21,22], possibly due to the impact of aserious diagnosis on the provision of emotional support byfamily and friends. Surprisingly, we found that having a carerwho was also a partner predicted lower emotional well-being.This observation has not been made previously in other cancerdiagnoses. This may suggest that patients are aware of theimpact on the partner and suffer distress around this knowledge.Further analysis was conducted to explore this counterintuitivefinding. The items which loaded strongest in a factor analysis ofthe emotional well-being subscale, and are thus most indicativeof the construct being measured, were: ‘I worry about dying’ and‘I worry my condition will get worse’. We hypothesize that thescores for this subscale are lower for those with a spouse caringfor them because they have someone close who is also impactedby their health and will experience distress in the event of theirdeath or deterioration. It is also possible that support servicesare preferentially targeted at those without close partner orfamily support and perhaps may not address the needs of thosewith partners due to an assumption that partnered people arebetter supported. Provision of information and support to carersmay also improve patient well-being; this question is open tofuture research.
Age, cancer type and gender predict distress and poor QOL inthe general cancer population [26–28]. In this study we found thatpatient’s level of education was the best demographic predictor ofdistress, with those who had tertiary education reporting lowerdistress than those without tertiary education. Tertiary educatedparticipants also scored higher in general and brain-tumourspecific QOL domains, and had lower unmet needs for a number ofitems which were otherwise highly rated. Those with highereducation were more likely to prefer written educational material.They were also more likely than those without tertiary educationto report a need for access to electronic information. Overall, thosewith higher education were more likely to be looking for additionalinformation sources. Those with higher education were also lesslikely to report adequate involvement in decision-making.Comparatively, those without tertiary education did not recordsignificant preferences for different information sources and feltadequately involved in decision-making. We hypothesize thathigher education levels empower patients to seek and understandinformation regarding their diagnosis, and that empowerment andinformation may assist in relieving or preventing distress. Ourfindings support additional screening for distress and unmet needsin those with less than tertiary education, and additional researchinto provision of information tailored to patient education leveland understanding.
The supportive care needs of the general cancer populationhave been reported elsewhere [29,30]. Participants diagnosedwith HGG reported a number of high unmet needs, some of which
would not be routinely addressed in a medical consultation. Thehighest needs related to ‘worry about those closest to them’ (39%),‘not being able to do the things you used to’ (36%), and ‘uncertaintyabout the future’ (30%), suggesting that sensitive enquiry aroundthese issues would be helpful. In comparison, six months afterdiagnosis in a population with different cancers, 15% had worriesabout those close to them and 13% felt uncertainty about the future[30]. In our study psychological needs were particularlyprominent, comprising five of the top ten needs on this scale,and highlighting the importance of the routine provision of, or atleast accessibility of counselling and clinical psychology servicesfor this population.
A change in employment status, financial impact of diagnosis,and level of physical dependency predicted unmet needs. Wherespecific needs related to brain cancer were examined, participantsreported high needs related to cognitive function and personalitychanges. Cognitive, behavioural and personality changes occurfrequently in people with HGG, often in the context of tumour site(i.e. frontal lobe tumours) and treatment such as surgery andradiotherapy. However, they are difficult to diagnose and manage,and often offer limited prospect of future improvement. Those withhigher levels of physical dependency and a higher financial impactof diagnosis were more likely to identify cognitive function needs,although cognitive function decline may have been a precursor tochange in employment status, indicating this may be a spuriousassociation.
A key strength of our study is the consecutive recruitment atthe main study site (n = 90), which services a population of around2 million as a centralized neuro-oncology service. Patients whowere not fit for chemoradiotherapy were not included; however,data from our institution shows that nearly 80% of patients withHGG have combined chemoradiotherapy [31]. It is likely thatthose who were unfit for combination treatment would reportworse function and QOL. We also included a relatively homoge-nous population with HGG at a uniform time point. Furtheranalysis of collected data will allow us to understand how patientdistress, quality of life and needs change over time, but is beyondthe scope of this paper.
4.2. Conclusion
This study provides an understanding of the QOL, distress andneeds of patients diagnosed with HGG during active treatment, agroup with specific needs that are much higher than for peoplewith other cancers. These patients are likely to benefit fromadditional information and psychological support to alleviatedistress and reduce their needs. High distress and increased needsmay occur in patients who experience a financial impact and thosewith lower education levels.
4.3. Practice implications
Patients diagnosed with HGG are likely to benefit fromreceiving additional information and substantial psychologicalsupport at this time point to alleviate distress and reduce theirneeds. Screening for distress and additional support resources maybe of particular benefit for patients who experience a financialimpact and those with lower education levels. Further research isrequired with these groups.
Funding
This project was funded by the Western Australian Cancer andPalliative Care Network, Department of Health, Western Australiaand a HOTTAH grant provided by the Clinical Oncology Society ofAustralia.
G.K.B. Halkett et al. / Patient Education and Counseling 98 (2015) 525–532532
Acknowledgements
The authors thank Celine Fournier and Jenny Clarke for theirassistance in data collection. We also thank Liz Hovey for herassistance with recruitment for the study and staff working at ourcollaborating sites in NSW for their assistance with data collection.
References
[1] Osoba D, Brada M, Prados M, Yung W. Effect of disease burden on health-related quality of life in patients with malignant gliomas. Neuro Oncol2000;2:221–8.
[2] Keir S, Calhoun-Eagan R, Swartz U, Friedman H. Screening for distress inpatients with brain cancer using the NCCN’s rapid screening measure. Psy-chooncology 2008;17:621–5.
[3] Gofton GJT, Carver A. Identifying the palliative care needs of patients livingwith cerebral tumors and metastases: a retrospective analysis. J Neurooncol2012;108:527–34.
[4] Australian Cancer Network Adult Brain Tumour Guidelines Working Party.Clinical practice guidelines for the management of adult gliomas. Sydney:Cancer Council Australia; 2009.
[5] Janda M, Steginga S, Dunn J, Langbecker D, Walker D, Eakin E. Unmet support-ive care needs and interest in services among patients with a brain tumour andtheir carers. Patient Educ Couns 2008;71:251–8.
[6] Janda M, Steginga S, Langbecker D, Dunn J, Walker D, Eakin E. Quality of lifeamong patients with a brain tumor and their carers. J Psychosom Res 2007;63:617–23.
[7] Goebel S, Stark AM, Kaup L, von Harscher M, Mehdorn HM. Distress in patientswith newly diagnosed brain tumours. Psychooncology 2011;20:623–30.
[8] Ford E, Catt S, Chalmers A, Fallowfield L. Systematic review of supportive careneeds in patients with primary malignant brain tumors. Neuro-oncol 2012;14:392–404.
[9] Mathes T, Antoine SL, Pieper D, Eikermann M. Adherence enhancing inter-ventions for oral anticancer agents: a systematic review. Cancer Treat Rev2014;40:102–8.
[10] Bui QU, Ostir GV, Kuo YF, Freeman J, Goodwin JS. Relationship of depression topatient satisfaction: findings from the barriers to breast cancer study. BreastCancer Res Treat 2005;89:23–8.
[11] Moore G, Collins A, Brand C, Gold M, Lethborg C, Murphy M, et al. Palliative andsupportive care needs of patients with high-grade glioma and their carers: asystematic review of qualitative literature. Patient Educ Couns 2013;91:141–53.
[12] Parvataneni PMR, Freeman T, Lamborn K, Prados M, Butowski N, Liu R, et al.Identifying the needs of brain tumor patients and their caregivers. J Neuroon-col 2011;104:737–44.
[13] Halkett GK, Lobb EA, Oldham L, Nowak AK. The information and support needsof patients diagnosed with High Grade Glioma. Patient Educ Couns 2010;79:112–9.
[14] McConigley R, Halkett G, Lobb E, Nowak A. Caring for someone with high-gradeglioma: a time of rapid change for caregivers. Palliat Med 2010;24:473–9.
[15] Lobb E, Halkett G, Nowak A. Patient and caregiver perceptions of commu-nication of prognosis in high grade glioma. J Neurooncol 2011;104:315–22.
[16] Gessler S, Low J, Daniells E, Williams R, Brough V, Tookman A, et al. Screeningfor distress in cancer patients: is the distress thermometer a valid measure inthe UK and does it measure change over time? A prospective validation study.Psychooncology 2007;17:538–47.
[17] Brucker P, Yost K, Cashy J, Webster K, Cella DF. General population and cancerpatient norms for the Functional Assessment of Cancer Therapy-General(FACT-G). Eval Health Prof 2005;28:192–211.
[18] Pelleteir G, Veroef M, Khatri N, Hagen N. Quality of life in brain tumourpatients: the relative contributions of depression, fatigue, emotional distress,and existential issues. J Neurooncol 2002;57:41–9.
[19] Bonevski B, Sanson-Fisher R, Girgis A, Burton L, Cook P, Boyes A. Evaluation ofan instrument to assess the needs of patients with cancer. Cancer 2000;88:217–25.
[20] Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al.Toxicity and response criteria of the Eastern Cooperative Oncology Group. AmJ Clin Oncol 1982;5:649–55.
[21] Janda M, DiSipio T, Hurst C, Cella D, Newman B. The Queensland Cancer RiskStudy: general population norms for the Functional Assessment of CancerTherapy-General (FACT-G). Psychooncology 2009;18:606–14.
[22] Psycho-Oncology Co-operative Research Group. Calculating norm-based T-scores from your FACT-G data; 2014, Available from: http://www.pocog.org.au/pod/factgscores.aspx.
[23] Bradley C, Yabroff R, Dahman B, Feuer E, Mariotto A, Brown M. Productivitycosts of cancer mortality in the United States: 2000–2020. J Natl Cancer Inst2008;100:1763–70.
[24] Access economics: cost of cancer in NSW. Sydney: Cancer Council NSW; 2006.[25] Patterson H. Nobody can afford a brain tumor. . .The financial impact of brain
tumors on patients and families. San Francisco: National Brain Tumor Foun-dation; 2007. p. 1–8.
[26] Hack TF, Pickles T, Ruether JD, Weir L, Bultz BD, Mackey J, et al. Predictors ofdistress and quality of life in patients undergoing cancer therapy: impact oftreatment type and decisional role. Psychooncology 2010;19:606–16.
[27] Gao W, Bennett MI, Stark D, Murray S, Higginson IJ. Psychological distress incancer from survivorship to end of life care: prevalence, associated factors andclinical implications. Eur J Cancer 2010;46:2036–44.
[28] Ernstmann N, Neumann M, Ommen O, Galushko M, Wirtz M, Voltz R, et al.Determinants and implications of cancer patients’ psychosocial needs. Sup-port Care Cancer 2009;17:1417–23.
[29] Sanson-Fisher R, Girgis A, Boyes A, Bonevski B, Burton L, Cook P. The unmetsupportive care needs of patients with cancer. Cancer 2000;88:226–37.
[30] Boyes AW, Girgis A, D’Este C, Zucca AC. Prevalence and correlates of cancersurvivors’ supportive care needs 6 months after diagnosis: a population-basedcross-sectional study. BMC Cancer 2012;12:150.
[31] Jackson M, Bydder S, Maujean E, Taylor M, Nowak A. Radiotherapy in themanagement of high-grade gliomas diagnosed in Western Australia: a pat-terns of care study. J Med Imaging Radiat Oncol 2012;56:109–15.
Related Documents











