Predictive Role of Daily Coping and Affective Reactivity in Cognitive Therapy Outcome: Application of a Daily Process Design to Psychotherapy Research Kathleen C. Gunthert, American University Lawrence H. Cohen, University of Delaware Andrew C. Butler, Judith S. Beck Beck Institute for CognitiveTherapy and Research We hypothesized that patients' initial ability to cope with daily stress would predict their rates of improvement in cognitive therapy (CT). For I week at the beginning of CT, 43 adult outpatients with depression and/or anxiety diag- noses completed daily assessments of stressors and associ- ated appraisals, negative cognitions, coping strategies, and negative mood. Depression was assessed at intake and at every treatment session. Even after the statistical control of intake depression level, treatment length, and concurrent medication status, many of the stress and coping variables were associated with rates of depression-reduction in the expected direction. We discuss the findings' implications for CT theory and practice as well as the heuristic value of a daily process design to evaluate the predictive role of pa- tient factors in psychotherapy outcome. COGNITIVE THERAPY (CT) is an efficacious and effective treatment for depression and anxiety (Barlow, Raffa, & Cohen, 2002; DeRubeis & Crits- Cristoph, 1998). However, a significant percentage (as many as 50%) of patients do not achieve com- plete recovery in CT (e.g., Elkin et al., 1989). De- spite the large CT outcome literature, we know very little about the patient factors that predict the effectiveness of this treatment (Kuyken, Kurzer, DeRubeis, Beck, & Brown, 2001; Whisman, 1993). Identification of patient characteristics that predict CT outcome could point to patient factors that are malleable and can be addressed clinically, either through revision of CT interventions or augment- ing CT with additional interventions. Address correspondence to Kathleen C. Gunthert, Department of Psychology, American University, Washington, DC 20016; e-mail: [email protected]. BEHAVIOR THERAPY 36, 77--88, 2005 005-7894105/0077-008851.00/0 Copyright 2005 by Associationfor Advancementof BehaviorTherapy All rights for reproduction in any form reserved. In the present study we evaluated the predictive role of daily stress responses in CT outcome. We were interested in how patients' initial appraisals, cognitions, coping, and affective reactivity in re- sponse to daily stressors were related to changes in depressive symptomatology over the course of treatment. Therefore, our focus was on assessing typical patterns of daily functioning to learn if these patterns interfere with or promote CT's effective- ness. We predicted that, independent of their initial depression severity, patients who show the greatest improvement would be those who initially: (a) ap- praise daily stressors as less undesirable and them- selves as more capable of coping; (b) respond to daily stressors with fewer negative automatic thoughts; (c) cope with daily stressors by using more adaptive strategies such as direct action and positive reinter- pretation; and (d) evidence lower affective reactiv- ity to negative appraisals and cognitions associated with daily stressors. Cognitive and Transactional Models of Stress and Coping A fundamental component of Beck's cognitive the- ory and therapy of depression concerns how indi- viduals evaluate and react to their daily stressful situations. Beck proposes that depression is at least in part maintained by negatively biased thinking in response to everyday stress. Beck's cognitive ther- apy (CT) of depression teaches patients to reduce their negative affect by using adaptive cognitive and behavioral strategies to deal with stressful sit- uations, modify negative thoughts, and increase their engagement in positive activities (Alford & Beck, 1997). This cognitive theory of depression is consistent with Lazarus and Folkman's (1984) transactional model of stress and coping. Lazarus and Folkman propose that when faced with a stressful situation, the individual first assesses the features of the event, such as controllability and undesirability (primary

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Predictive Role of Daily Coping and Affective Reactivity in Cognitive Therapy Outcome: Application of a Daily
Process Design to Psychotherapy Research
Kathleen C. Gunthert, American University Lawrence H. Cohen, University of Delaware
Andrew C. Butler, Judith S. Beck Beck Institute for CognitiveTherapy and Research
We hypothesized that patients ' initial ability to cope with
daily stress would predict their rates of improvement in
cognitive therapy (CT). For I week at the beginning of CT,
43 adult outpatients with depression and/or anxiety diag- noses completed daily assessments of stressors and associ- ated appraisals, negative cognitions, coping strategies, and negative mood. Depression was assessed at intake and at every treatment session. Even after the statistical control of
intake depression level, treatment length, and concurrent medication status, many of the stress and coping variables were associated with rates of depression-reduction in the expected direction. We discuss the findings' implications for
CT theory and practice as well as the heuristic value of a
daily process design to evaluate the predictive role of pa- tient factors in psychotherapy outcome.
COGNITIVE THERAPY (CT) is an efficacious and effective treatment for depression and anxiety (Barlow, Raffa, & Cohen, 2002; DeRubeis & Crits- Cristoph, 1998). However, a significant percentage (as many as 50%) of patients do not achieve com- plete recovery in CT (e.g., Elkin et al., 1989). De- spite the large CT outcome literature, we know very little about the patient factors that predict the effectiveness of this treatment (Kuyken, Kurzer, DeRubeis, Beck, & Brown, 2001; Whisman, 1993). Identification of patient characteristics that predict CT outcome could point to patient factors that are malleable and can be addressed clinically, either through revision of CT interventions or augment- ing CT with additional interventions.
Address correspondence to Kathleen C. Gunthert, Department of Psychology, American University, Washington, DC 20016; e-mail: [email protected].
BEHAVIOR THERAPY 36, 77--88, 2005 005-7894105/0077-008851.00/0 Copyright 2005 by Association for Advancement of Behavior Therapy All rights for reproduction in any form reserved.
In the present study we evaluated the predictive role of daily stress responses in CT outcome. We were interested in how patients' initial appraisals, cognitions, coping, and affective reactivity in re- sponse to daily stressors were related to changes in depressive symptomatology over the course of treatment. Therefore, our focus was on assessing typical patterns of daily functioning to learn if these patterns interfere with or promote CT's effective- ness. We predicted that, independent of their initial depression severity, patients who show the greatest improvement would be those who initially: (a) ap- praise daily stressors as less undesirable and them- selves as more capable of coping; (b) respond to daily stressors with fewer negative automatic thoughts; (c) cope with daily stressors by using more adaptive strategies such as direct action and positive reinter- pretation; and (d) evidence lower affective reactiv- ity to negative appraisals and cognitions associated with daily stressors.
Cognitive and Transactional Models of Stress and Coping A fundamental component of Beck's cognitive the- ory and therapy of depression concerns how indi- viduals evaluate and react to their daily stressful situations. Beck proposes that depression is at least in part maintained by negatively biased thinking in response to everyday stress. Beck's cognitive ther- apy (CT) of depression teaches patients to reduce their negative affect by using adaptive cognitive and behavioral strategies to deal with stressful sit- uations, modify negative thoughts, and increase their engagement in positive activities (Alford & Beck, 1997).
This cognitive theory of depression is consistent with Lazarus and Folkman's (1984) transactional model of stress and coping. Lazarus and Folkman propose that when faced with a stressful situation, the individual first assesses the features of the event, such as controllability and undesirability (primary

78 G U N T H E R T E T A L .
appraisals), and then evaluates his or her resources for coping (secondary appraisal). The individual then chooses and implements specific coping strat- egies to deal with the event. This process results in some outcome, such as a change in mood. Cogni- tive mediation is a central focus of this model, be- cause it proposes that the impact of an event on individual outcomes (e.g., change in mood) is deter- mined by its meaning to the individual, rather than the event's objective characteristics. Given CT's em- phasis on stress appraisals, coping, and stress-based affective reactivity, it is important to examine how these factors, along with negative automatic think- ing, influence a patient's ability to benefit from CT.
Patient Predictors of CT Outcome Rude and Rehm (1991) reviewed the literature on the predictive role of specific pretreatment cogni- tive and behavioral deficits that are targeted for change in CT. They concluded that there is some evidence that patients who score in the more adap- tive direction on pretreatment measures of relevant cognitive and behavioral variables fare better in CT than those who score in the less adaptive range. In other words, it appears that CT works best with patients who can capitalize on preexisting skills and resources (Whisman, 1993). Cronbach and Snow (1977) referred to this general pattern as the "capitalization model" of treatment response.
However, with respect to the stress and coping process, we know yery little about how day-to-day attempts to deal with stressors and to regulate daily negative affect influence the course of CT. This gap in the literature is striking, given CT's em- phasis on changing perceptions of, and reactions to, daily stressors. If it were shown that patients with poor initial coping skills had worse outcomes in CT, then treatment could be adapted to meet their particular needs. For instance, such patients might require a refined treatment protocol, per- haps one that includes more intensive and/or ex- tended initial training on coping skills and affect regulation.
D A I L Y C O G N I T I O N S A N D A P P R A I S A L S
Although few studies have examined the impact of daily cognitions and appraisals on change in cogni- tive therapy, a number of researchers have evalu- ated the predictive role of patients' pretreatment "cognitive styles," such as dysfunctional attitudes and a pessimistic explanatory style. Dysfunctional attitudes refer to maladaptive underlying assump- tions, such as "I should be able to please every- body" (Weissman & Beck, 1978). Explanatory style refers to attributions that individuals make about the causes of life events (Abramson, Selig-
man, & Teasdale, 1978). Research has shown that individuals who have greater dysfunctional atti- tudes and a pessimistic explanatory style at intake are less responsive to CT (Kuyken et al., 2001; Si- mons, Gordon, Monroe, & Thase, 1995; Sotsky et al., 1991; Zuroff, Blatt, Sanislow, Bondi, & Pilkonis, 1999). Whisman (1993) suggested that depressed patients with greater "cognitive dysfunction" will have more difficulty benefiting from CT techniques because they lack the skills and learning histories to successfully implement these techniques.
When researchers assess dysfunctional attitudes as a measure of cognitive vulnerability, the assump- tion is that these maladaptive beliefs affect how people perceive and react emotionally to stressful circumstances. However, given that dysfunctional attitudes presumably exert their influence through reactions to everyday stressors, one could argue that these dispositional measures are several steps re- moved from the thoughts and appraisals that occur when an individual confronts his or her daily stress. A more direct strategy would be to assess parti- cipants' actual thoughts in response to naturally oc- curring stress, rather than to request their more general reports of underlying dysfunctional attitudes.
C O P I N G
Evidence for the influence of patients' pretreatment coping resources on CT outcome is equivocal. Si- mons, Lustman, Wetzel, and Murphy (1985) eval- uated the predictive role of pretreatment "learned resourcefulness," a construct that is comprised of a set of self-control skills including cognitive strate- gies, problem solving, delay of gratification, and self-efficacy expectations. They found that indi- viduals with high initial learned resourcefulness responded more positively to CT. On the other hand, Burns and Nolen-Hoeksema (1991) found that initial active coping style was not related to homework compliance or improvement in CT (although willingness to learn new coping strate- gies was associated with greater improvement), and Bryant, Simons, and Thase (1999) found that learned resourcefulness did not predict compli- ance in CT.
Benefits of a Daily Assessment Approach To date, CT research findings on the predictive role of patients' stress and coping factors have been in- conclusive and difficult to interpret. We believe that some of the inconsistencies are attributable to methodological problems in the assessment of stress and coping variables. To assess coping, most re- searchers have used either dispositional measures, which assess how respondents "typically" cope with life events, retrospective reports of coping with a

D A I L Y C O P I N G A N D C O G N I T I V E T H E R A P Y O U T C O M E 79
specific past stressor, or measures of projected coping in hypothetical situations. Recent research suggests that findings obtained from these types of studies bear little resemblance to those obtained from daily studies that assess coping with concur- rent life events (Stone et al., 1998). Therefore, we assessed coping using repeated assessments over a number of days to reduce retrospective bias and biased trait-like reporting (Porter & Stone, 1996), and to obtain a closer approximation of what indi- viduals actually do and think on a day-to-day basis as they confront specific stressors.
Another important benefit of repeated daily as- sessments is the added information that can be ob- tained through the use of within-person statistics. Until recently, most studies of the relationships be- tween stress, cognitions, coping, and mood relied on a cross-sectional, between-person analytic strat- egy. However, the inferences that can be made from these studies are limited. For example, we can infer that people who have more negative appraisals of stress also tend to have negative mood, but we do not know how these factors are related on any given day; that is, when perceptions of stress in- crease, to what degree does negative mood also increase? By using a within-person analytic ap- proach, we can evaluate how depressed an individ- ual feels on days when he or she is reporting an in- crease in perceived stress, as compared to days that are less stressful (Affleck, Zautra, Tennen, & Armeli, 1999). Clinical researchers are increasingly using these within-person analyses to assess stress reac- tivity (Zuroff & Blatt, 2002). In our study, we used this approach to assess affective reactivity in re- sponse to daily stressors.
Affective Reactivity It has been well established in the cognitive therapy literature that depressed people have a negative bias in their thinking and have more negative thoughts than nondepressed people (Clark, Beck, & Alford, 1999). However, it is also important to consider that depressed individuals might experi- ence not only a greater frequency of negative cog- nitions, but also greater increases in negative mood when their negative thoughts occur. In other words, depressed individuals might be more affectively re- active to the negative thoughts they have (Gunt- hert, Cohen, & Armeli, 2002), perhaps because they believe their negative thoughts more than nonde- pressed persons, or they may attach more negative personal meaning to these thoughts (J. Beck, 1995).
Bolger and Zuckerman (1995) defined affective reactivity with respect to the within-person rela- tionship between stressful events and mood. They
proposed that each person has a unique relation- ship between number of daily negative events and negative mood. If one computed within-person re- gression statistics to capture that relationship, a highly reactive individual would evidence a strong positive within-person relationship between these two variables. Compared to a less reactive person, a highly reactive person's negative mood would in- crease more drastically given the same increase in number of daily stressful events. Affective reactiv- ity is therefore defined as a within-person index of the relationship between stress and mood.
In principle, CT attempts to reduce depressed patients' affective reactivity to daily stressors by encouraging them to challenge and modify their negative appraisals and cognitions associated with these daily events. A capitalization model (Cron- bach & Snow, 1977) would suggest that patients who enter CT with relative strengths in their ability to regulate daily negative affect in response to stress appraisals and cognitions will have superior outcomes in CT. In the present study, we used a daily process design to assess CT patients' initial affective reactivity to stress appraisals and negative cognitions, and we used these affective reactivity indices as predictors of CT outcome.
Method P A R T I C I P A N T S
The participants were 43 adult outpatients at the Beck Institute for Cognitive Therapy and Research. Only patients who met Diagnostic and Statistical Manual (DSM-IV; American Psychiatric Associa- tion, 1994) criteria for a depressive and/or anxiety disorder were recruited for the study. We included both depressive and anxiety disorders because of their high rate of comorbidity (Rieger, Rae, Nar- row, Kaelber, & Schatzberg, 1998). We were inter- ested in investigating change in depressive symp- toms, and although anxiety patients might not have diagnosable clinical depression, many of them manifest significant depressive symptomatology. In our final sample, for example, the mean Beck De- pression Inventory-II (BDI-II; A. T. Beck, Steer, & Brown, 1996) score of anxious patients was 16, which reflects at least mild depressive symptoma- tology. Exclusionary criteria were coexisting active substance abuse or dependence and coexisting psy- chotic disorder. Ninety-three eligible patients were informed of the study, and 50 (54%) agreed to participate. One patient only completed 2 days of questionnaires, which left 49 patients who completed 3 or more days of the week-long daily stress and coping assessments. Because our study focused on longitudinal decreases in depressive symptoms, we only included individuals with an

8 0 G U N T H E R T E T A L .
intake depression score of 10 or higher on the BDI- II. For patients with a BDI-II score of 9 or lower, there is little room for improvement in their de- pression scores (a floor effect). Three patients were excluded due to this criterion. Three participants participated in only two sessions of therapy, and thus were excluded from analyses.
Diagnoses were made at intake by one of three doctoral-level clinicians based on the Structured Clinical Interview for DSM-IV (SCID; First, Spitzer, Gibbon, & Williams, 1995). Diagnosticians had received comprehensive training for the SCID and had an average of 7.3 years experience administer- ing the interview in a research setting. The diagnos- tic composition of the sample was: major depres- sive disorder (51%; n -- 22); generalized anxiety disorder (12%; n = 5); adjustment disorder with mixed features (9%; n = 4); dysthymic disorder (7%; n -- 3); adjustment disorder with depressed mood (5%; n = 2); social phobia (5%; n = 2); spe- cific phobia (5%; n =2); panic disorder (2%; n = 1); bipolar II disorder, depressive episode (2%; n -- 1); and obsessive-compulsive disorder (2%; n = 1). These categories represent the primary Axis I diag- noses, but many patients had secondary diagnoses as well; thus, many patients were categorized as having both a depressive and anxiety disorder. More generally, 51% (n = 22) were diagnosed with a depressive disorder only, 16% (n = 7) were diagnosed with an anxiety disorder only, and 33% (n = 14) were diagnosed with both an anxiety dis- order and a mood disorder.
The sample included 28 women (65%) and 15 men (35%), and was predominantly Caucasian (95%). The average age was 40 years (SD = 11.00; range = 21 to 70). Approximately half of the sam- ple was married (54%; n = 23), 35% (n = 15) were single and had never been married, 7% (n = 3) were divorced or separated, one individual (2%) was widowed, and one (2%) did not report her marital status. In general, the participants were very well-educated: 58% (n = 25) had an ad- vanced or professional degree, and 26% (n = 11) had a college degree.
The mean treatment length for the 43 partici- pants was 12.30 sessions, with a range from 3 to 34 sessions (SD = 6.66). (Due to this large range, we controlled for number of sessions in all analyses of rates of change in treatment). Twenty (39%) participants received concurrent pharmacotherapy during the course of the study. Only 3 (7%) of the 43 participants terminated treatment prematurely, that is, without the therapist's agreement. 1
l There were missing data on 8 patients regarding conditions of termination.
M E A S U R E S
Initial and weekly depression. Participants' ini- tial and weekly level of depression was assessed using the 21-item BDI-II (A. T. Beck et al., 1996). Depressive symptoms are rated for severity on a 4- point scale, and item ratings are summed to obtain a total score. A number of studies document the re- liability and validity of the BDI-II (Dozois, Dob- son, & Ahnberg, 1998).
Daily stress, appraisal, and coping. After their first treatment session, participants completed a modified version of the Daily Coping Inventory (DCI; Stone & Neale, 1984) at the end of the day for 7 consecutive days. The DCI assesses partici- pants' most stressful daily event by requesting a written description of "the worst or most bother- some problem of the day." Assessment of primary and secondary appraisals and use of specific coping strategies require a single event reference, and the day's most stressful event serves as that reference. To code these event descriptions, we generated a list of event categories by reading and recording a large sample of event responses. We categorized the events as interpersonal, work-related, somatic (illness or physical complaints), emotional-cognitive (e.g., "I could not stop crying"), and other stressors. After generating categories, the first and second au- thors independently coded all of the daily event re- sponses (kappa -- .88).
Participants then rated the day's most stressful event on two primary appraisal dimensions: con- trollability (0 -- no control to 4 -- complete con- trol) and undesirability (0 = not undesirable to 4 = extremely undesirable). Participants also rated a secondary appraisal item, perceived coping effi- cacy, which assessed whether they believe they had the resources to cope with the stressor (0 = defi- nitely not to 4 = definitely).
The DCI then assesses how the individual coped with the day's most stressful event. The measure consists of a list of eight broad coping categories: distraction, positive reinterpretation (originally called situation redefinition), direct action, cathar- sis, acceptance, seeking social support, relaxation, and religion. To decrease the length of the ques- tionnaire, we omitted the religion category. Addi- tionally, because we were interested in the use of coping strategies that are relevant to CT, we added the category "checked negative thoughts." All of these categories were followed by a brief defini- tion to ensure that participants understood the strategies. Participants were instructed to check all of the coping strategies that they used to deal with the day's most stressful event. This strategy to assess daily appraisals and coping has been used

D A I L Y C O P I N G A N D C O G N I T I V E T H E R A P Y O U T C O M E 81
successfully in several daily stress studies (David & Suls, 1999; Gunthert, Cohen, & Armeli, 1999).
Negative cognitions. We assessed negative au- tomatic thoughts in response to the day's most stressful event using five items from the Cognition Checklist (CCL; Beck, Brown, Steer, Eidelson, & Riskind, 1987). The CCL was developed to assess the frequency of automatic thoughts related to de- pression and anxiety. We condensed this scale by selecting five items from the depressive cognition subscale (CCL-D). We chose the five highest load- ing items on the CCL-D scale which were appli- cable to any situation (and not linked to a specific situation such as pain or a social interaction). Items include, for example, "I 'm worthless, .... I will never overcome my problem." The participants were in- structed to rate how often these thoughts occurred to them "today" in response to the problem (the day's most stressful event) they described (0 = not at all to 4 = very often). Items were averaged to obtain daily negative cognition scores. Steer, Beck, Clark, and Beck (1994) reported extensive reliability and validity data on the CCL. For the present study, Cronbach's alpha for the five CCL items was .88.
End-of-day mood. State depressed and anxious mood at the end of each day was assessed using Watson and Clark's (1994) Positive and Negative Affect Schedule-Expanded Form (PANAS-X). This measure assesses general positive and negative af- fect, along with other specific mood states (e.g., fear and sadness). The PANAS-X lists adjectives describing the mood states, and participants rate the items according to the extent to which they feel each item "at this moment" (1 = very slightly or not all to 5 = extremely). We administered the 6- item fear/anxiety subscale and the 5-item sadness/ depressed mood subscale. In our sample, the aver- age correlation between these two subscales was r = .48, p < .001. To form an overall measure of "negative affect," we summed the two scales. Cronbach's alpha for this composite scale was .92.
S E T T I N G A N D P R O C E D U R E
The Beck Institute for Cognitive Therapy and Re- search is located in Bala Cynwyd, Pennsylvania (just outside of Philadelphia). The Institute special- izes in CT, primarily for depressed and anxious adults. Virtually all patients are seen once per week. Although not explicitly manualized, CT at the Institute is provided by highly trained and ex- perienced cognitive therapists who receive regu- lar in-service supervision and consultation from Aaron T. Beck, M.D., and Judith S. Beck, Ph.D. In the present study, seven (four women) licensed doctoral-level psychologists provided psychother- apy. Their experience with CT ranged from 7 to 20
years (median = 10 years). The distribution of patients to therapists was unequal; 2 therapists treated 29 (67%) of the patients, and the remaining therapists treated between 1 and 5 patients each. This distribution reflected the respective therapists' workload and job description at the Institute.
The initial measures of demographic informa- tion and depression (BDI-II) were completed at in- take. At the first session of therapy, therapists used a standardized set of instructions to introduce the study to each patient. If a patient agreed to partic- ipate at the first therapy session, he or she was given an envelope containing seven packets, one for each night until the next therapy session. The partici- pants were instructed to complete one packet at the end of each day, close to when they went to bed. The order of the daily packet was: PANAS-X, a self- esteem inventory relevant to another project, DCI event description, CCL-D, and the DCI appraisal and coping sections. We ordered the measures such that mood ratings would not be influenced by re- flecting on and reporting the daily stressful events, thoughts, appraisals, and coping. To maximize com- pliance, we called each participant on days 3 and 5 to remind him or her to complete the daily mea- sures. The completed measures were returned at the second session. Before all therapy sessions, pa- tients completed the BDI-II, which was used to as- sess change in depressive symptomatology over time.
Results D E S C R I P T I V E A N A L Y S E S
Participants versus nonparticipants. The 43 par- ticipants were compared to the 44 nonparticipants on age, gender, diagnostic category (depression, anxiety, or mixed), and intake score on the BDI-II. The only difference was that a higher proportion of men refused to participate.
Weekly depression scores. On average, patients completed the depression measure for 81% of their weekly sessions (SD -- .25). To handle missing data in our analyses, we used a listwise deletion strategy for all multilevel models (Bryk & Raudenbush, 1992). It is noteworthy that the listwise deletion strategy primarily affects level-1 observations and thus did not affect the total N for the sample. In the case of a missing data point at level-l, the program will delete the full observation for that session, not the entire record for that individual. 2
2We examined whether predictor variables (daily stress and coping measures) were related to rates of missing depression scores. All variables were unrelated to rates of missing data with the exception of direct action (p < .05), such that patients who fre- quently used direct action coping were more likely to have missing data. There were also trends for catharsis and checking negative thoughts, such that greater reliance on these coping strategies was predictive of more missing data.
82 G U N T H E R T E T A L .
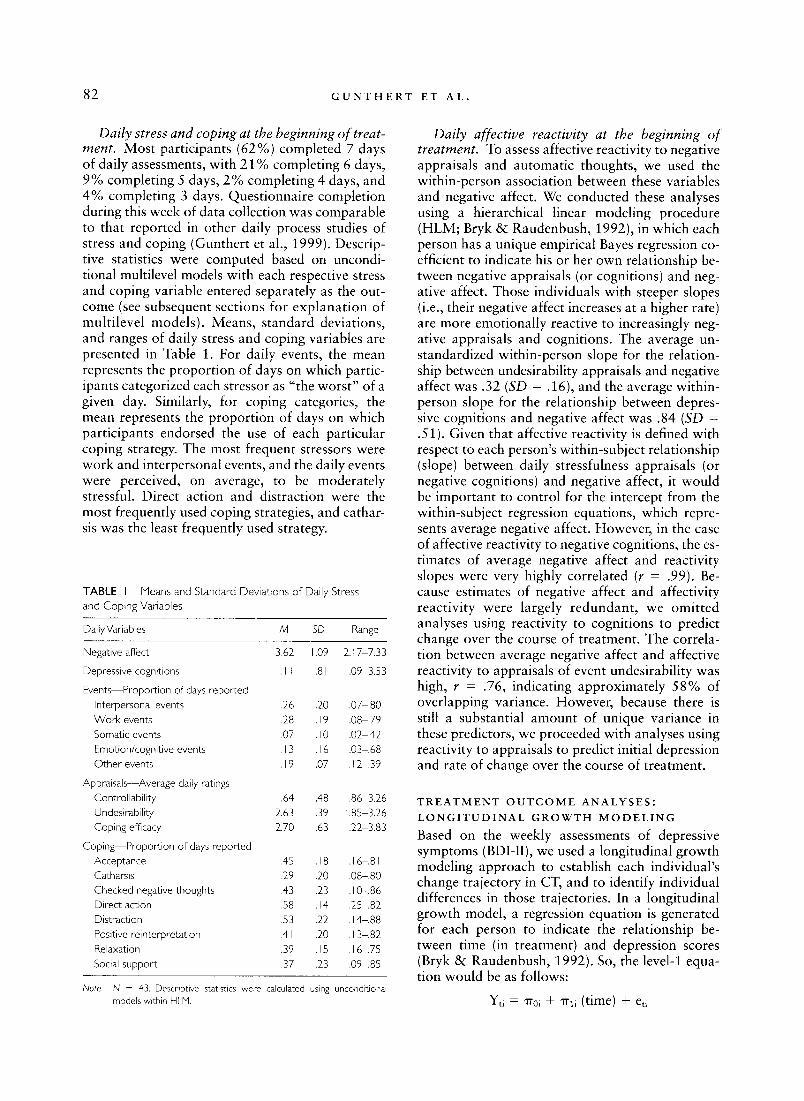
Daily stress and coping at the beginning of treat- ment. Most participants (62%) completed 7 days of daily assessments, with 21% completing 6 days, 9% completing 5 days, 2% completing 4 days, and 4% completing 3 days. Questionnaire completion during this week of data collection was comparable to that reported in other daily process studies of stress and coping (Gunthert et al., 1999). Descrip- tive statistics were computed based on uncondi- tional multilevel models with each respective stress and coping variable entered separately as the out- come (see subsequent sections for explanat ion of multilevel models). Means, standard deviations, and ranges of daily stress and coping variables are presented in Table 1. For daily events, the mean represents the proport ion of days on which partic- ipants categorized each stressor as "the worst" of a given day. Similarly, for coping categories, the mean represents the proport ion of days on which participants endorsed the use of each particular coping strategy. The most frequent stressors were work and interpersonal events, and the daily events were perceived, on average, to be moderately stressful. Direct action and distraction were the most frequently used coping strategies, and cathar- sis was the least frequently used strategy.
TABLE I Means and Standard Deviations of Daily Stress and Coping Variables
Daily Variables M SD Range
Negative affect
Depressive cognitions
Events Proportion of days reported Interpersonal events Work events Somatic events Emotion/cognitive events Other events
Appraisals--Average daily ratings Controllability Undesirability Coping efficacy
Coping--Proportion of days reported Acceptance Catharsis Checked negative thoughts Direct action Distraction Positive reinterpretation Relaxation Social support
3,62 1,09 2.17 7.33
I.I1 .81 .09 3.53
.26 .20 .07 ,80
.28 .19 .08 .79
.07 .10 .02 ,42
.13 .16 .03-.68 ,19 ,07 ,12 .39
1.64 ,48 ,86 3.26 2.63 .39 1.85 3.26 2.70 ,63 1.22 3.83
.45 .18 .16-.81
.29 .20 .08-.80
.43 .23 .10-.86
.58 .14 .25-.82
.53 .22 .14-.88
.41 .20 .13-.82
.39 .15 .16 .75
.37 .23 .09-.85
Note. N = 43. Descriptive statistics were calculated using unconditional models within HLM.
Daily affective reactivity at the beginning of treatment. To assess affective reactivity to negative appraisals and automatic thoughts, we used the within-person association between these variables and negative affect. We conducted these analyses using a hierarchical linear modeling procedure (HLM; Bryk & Raudenbush, 1992), in which each person has a unique empirical Bayes regression co- efficient to indicate his or her own relationship be- tween negative appraisals (or cognitions) and neg- ative affect. Those individuals with steeper slopes (i.e., their negative affect increases at a higher rate) are more emotionally reactive to increasingly neg- ative appraisals and cognitions. The average un- standardized within-person slope for the relation- ship between undesirability appraisals and negative affect was .32 (SD -- .16), and the average within- person slope for the relationship between depres- sive cognitions and negative affect was .84 (SD = .51). Given that affective reactivity is defined with respect to each person's within-subject relationship (slope) between daily stressfulness appraisals (or negative cognitions) and negative affect, it would be important to control for the intercept from the within-subject regression equations, which repre- sents average negative affect. However, in the case of affective reactivity to negative cognitions, the es- timates of average negative affect and reactivity slopes were very highly correlated (r = .99). Be- cause estimates of negative affect and affectivity reactivity were largely redundant , we omit ted analyses using reactivity to cognitions to predict change over the course of treatment. The correla- tion between average negative affect and affective reactivity to appraisals of event undesirability was high, r = .76, indicating approximately 58% of overlapping variance. However, because there is still a substantial amount of unique variance in these predictors, we proceeded with analyses using reactivity to appraisals to predict initial depression and rate of change over the course of treatment.
T R E A T M E N T O U T C O M E A N A L Y S E S :
L O N G I T U D I N A L G R O W T H M O D E L I N G
Based on the weekly assessments of depressive symptoms (BDI-II), we used a longitudinal growth modeling approach to establish each individual's change trajectory in CT, and to identify individual differences in those trajectories. In a longitudinal growth model, a regression equation is generated for each person to indicate the relationship be- tween time (in treatment) and depression scores (Bryk & Raudenbush, 1992). So, the level-1 equa- tion would be as follows:
Yti = rr0~ + "rhi (time) + eti
D A I L Y C O P I N G A N D C O G N I T I V E T H E R A P Y O U T C O M E 83
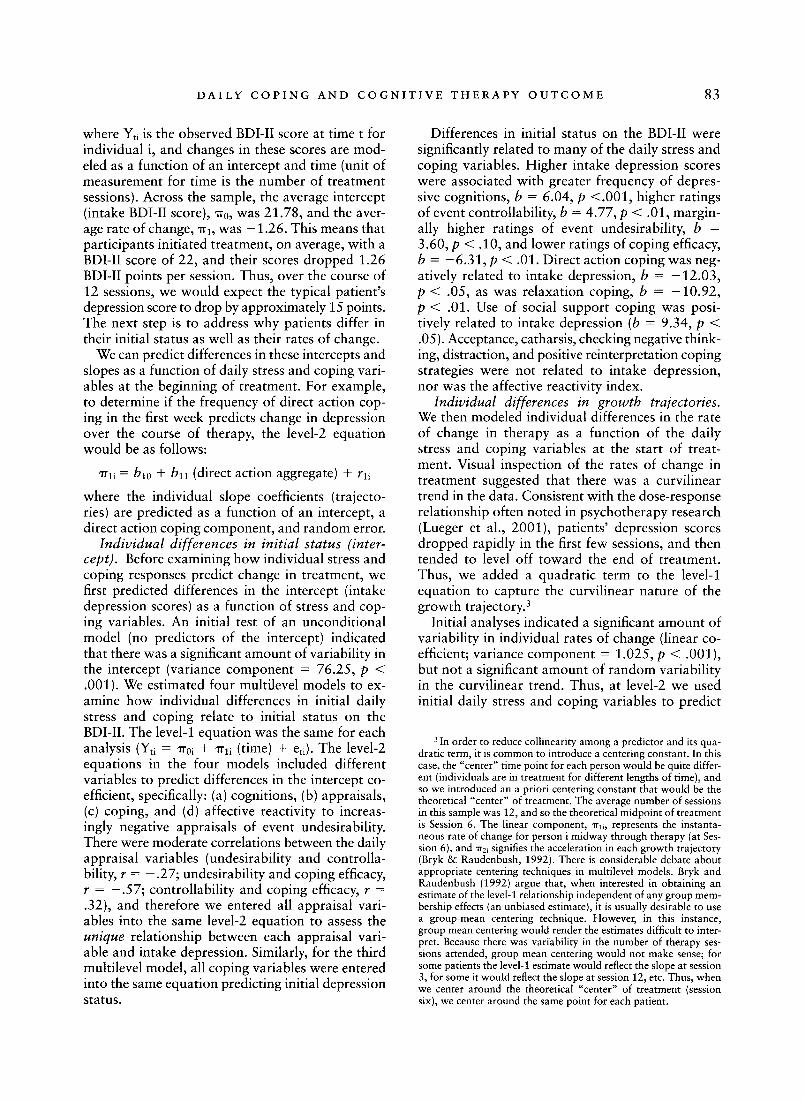
where Yti is the observed BDI-II score at time t for individual i, and changes in these scores are mod- eled as a function of an intercept and time (unit of measurement for time is the number of treatment sessions). Across the sample, the average intercept (intake BDI-II score), "rr0, was 21.78, and the aver- age rate of change, 7rl, was - 1.26. This means that participants initiated treatment, on average, with a BDI-II score of 22, and their scores dropped 1.26 BDI-II points per session. Thus, over the course of 12 sessions, we would expect the typical patient's depression score to drop by approximately 15 points. The next step is to address why patients differ in their initial status as well as their rates of change.
We can predict differences in these intercepts and slopes as a function of daily stress and coping vari- ables at the beginning of treatment. For example, to determine if the frequency of direct action cop- ing in the first week predicts change in depression over the course of therapy, the level-2 equation would be as follows:
~rli = hi0 + bll (direct action aggregate) + rli
where the individual slope coefficients (trajecto- ries) are predicted as a function of an intercept, a direct action coping component, and random error.
Individual differences in initial status (inter- cept). Before examining how individual stress and coping responses predict change in treatment, we first predicted differences in the intercept (intake depression scores) as a function of stress and cop- ing variables. An initial test of an unconditional model (no predictors of the intercept) indicated that there was a significant amount of variability in the intercept (variance component = 76.25, p < .001). We estimated four multilevel models to ex- amine how individual differences in initial daily stress and coping relate to initial status on the BDI-II. The level-1 equation was the same for each analysis (Yti = ' r r0i q- ' r r l i (time) + eti). The level-2 equations in the four models included different variables to predict differences in the intercept co- efficient, specifically: (a) cognitions, (b) appraisals, (c) coping, and (d) affective reactivity to increas- ingly negative appraisals of event undesirability. There were moderate correlations between the daily appraisal variables (undesirability and controlla- bility, r = - .27; undesirability and coping efficacy, r = - .57; controllability and coping efficacy, r = .32), and therefore we entered all appraisal vari- ables into the same level-2 equation to assess the unique relationship between each appraisal vari- able and intake depression. Similarly, for the third multilevel model, all coping variables were entered into the same equation predicting initial depression status.
Differences in initial status on the BDI-II were significantly related to many of the daily stress and coping variables. Higher intake depression scores were associated with greater frequency of depres- sive cognitions, b = 6.04, p <.001, higher ratings of event controllability, b = 4.77, p < .01, margin- ally higher ratings of event undesirability, b = 3.60, p < .10, and lower ratings of coping efficacy, b = -6 .31 , p < .01. Direct action coping was neg- atively related to intake depression, b = -12 .03 , p < .05, as was relaxation coping, b = -10 .92 , p < .01. Use of social support coping was posi- tively related to intake depression (b = 9.34, p < .05). Acceptance, catharsis, checking negative think- ing, distraction, and positive reinterpretation coping strategies were not related to intake depression, nor was the affective reactivity index.
Individual differences in growth trajectories. We then modeled individual differences in the rate of change in therapy as a function of the daily stress and coping variables at the start of treat- ment. Visual inspection of the rates of change in treatment suggested that there was a curvilinear trend in the data. Consistent with the dose-response relationship often noted in psychotherapy research (Lueger et al., 2001), patients' depression scores dropped rapidly in the first few sessions, and then tended to level off toward the end of treatment. Thus, we added a quadratic term to the level-1 equation to capture the curvilinear nature of the growth trajectory. 3
Initial analyses indicated a significant amount of variability in individual rates of change (linear co- efficient; variance component = 1.025, p < .001), but not a significant amount of random variability in the curvilinear trend. Thus, at level-2 we used initial daily stress and coping variables to predict
3 In order to reduce collinearity among a predictor and its qua- dratic term, it is common to introduce a centering constant. In this case, the "center" time point for each person would be quite differ- ent (individuals are in treatment for different lengths of time), and so we introduced an a priori centering constant that would be the theoretical "center" of treatment. The average number of sessions in this sample was 12, and so the theoretical midpoint of treatment is Session 6. The linear component, ~rli, represents the instanta- neous rate of change for person i midway through therapy (at Ses- sion 6), and ~r2i signifies the acceleration in each growth trajectory (Bryk & Raudenbush, 1992). There is considerable debate about appropriate centering techniques in multilevel models. Bryk and Raudenbush (1992) argue that, when interested in obtaining an estimate of the level-1 relationship independent of any group mem- bership effects (an unbiased estimate), it is usually desirable to use a group-mean centering technique. However, in this instance, group mean centering would render the estimates difficult to inter- pret. Because there was variability in the number of therapy ses- sions attended, group mean centering would not make sense; for some patients the level-1 estimate would reflect the slope at session 3, for some it would reflect the slope at session 12, etc. Thus, when we center around the theoretical "center" of treatment (session six), we center around the same point for each patient.
84 G U N T H E R T E T A L .
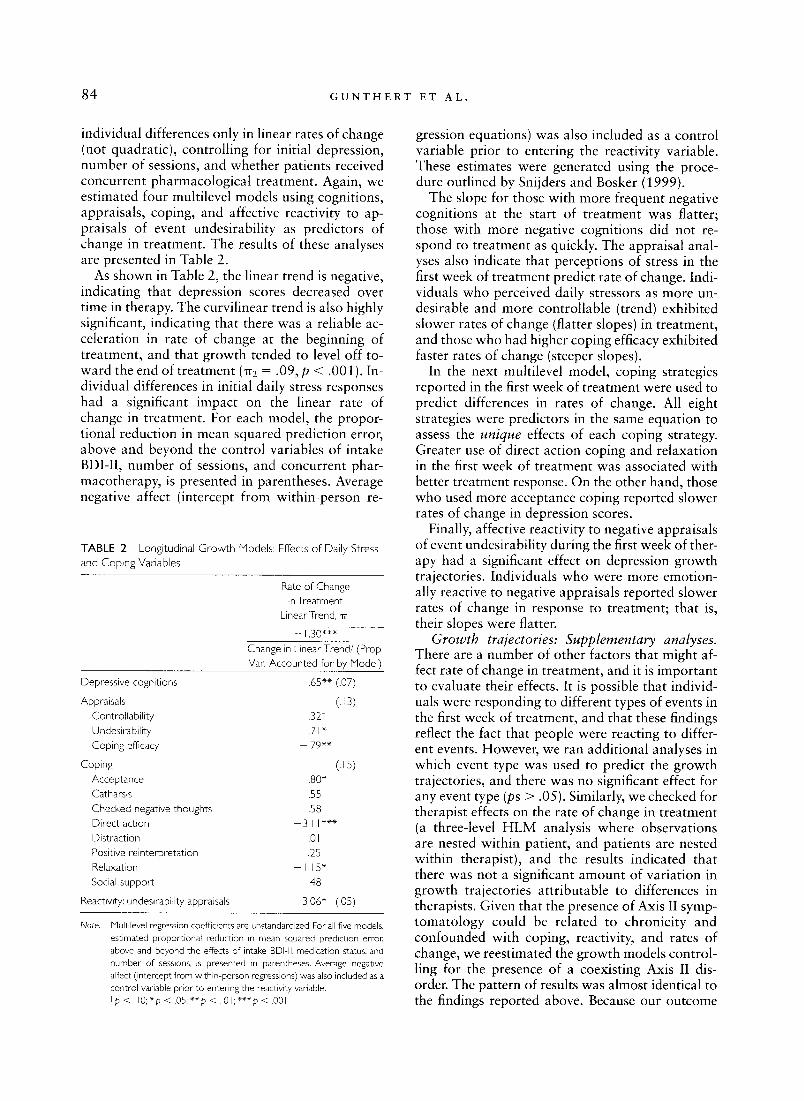
individual differences only in linear rates of change (not quadratic), controlling for initial depression, number of sessions, and whether patients received concurrent pharmacological treatment. Again, we estimated four multilevel models using cognitions, appraisals, coping, and affective reactivity to ap- praisals of event undesirability as predictors of change in treatment. The results of these analyses are presented in Table 2.
As shown in Table 2, the linear trend is negative, indicating that depression scores decreased over time in therapy. The curvilinear trend is also highly significant, indicating that there was a reliable ac- celeration in rate of change at the beginning of treatment, and that growth tended to level off to- ward the end of treatment (zr2 = .09, p < .001). In- dividual differences in initial daily stress responses had a significant impact on the linear rate of change in treatment. For each model, the propor- tional reduction in mean squared prediction error, above and beyond the control variables of intake BDI-II, number of sessions, and concurrent phar- macotherapy, is presented in parentheses. Average negative affect (intercept from within-person re-
TABLE 2 Longitudinal G row th Models: Effects o f Daily Stress and Coping Variables
Rate of Change in Treatment
Linear Trend, ITI
-1,30"** Change in Linear Trend/(Prop Van Accounted for by Model)
Depressive cognitions .65"* (.07)
Appraisals (. 13) Controllabil i ty .32t
Undesirability .71" Coping efficacy - , 7 9 " *
Coping (. 15) Acceptance ,80" Catharsis .55 Checked negative thoughts .58 Direct action 3, I I * * * Distraction .0 I Positive reinterpretation - . 25 Relaxation - I, 15* Social support ,48
Reactivity: undesirability appraisals 3.06* (.05)
Note, Multilevel regression coefficients are unstandardized. For all five models, estimated proportional reduction in mean squared prediction error, above and beyond the effects of intake BDI-II, medication status, and number of sessions, is presented in parentheses. Average negative affect (intercept from within-person regressions) was also included as a control variable prior to entering the reactivity variable. I p < . 1 0 ; * p < . 0 5 ; * * p < . 0 1 ; * * * p < . 0 0 1
gression equations) was also included as a control variable prior to entering the reactivity variable. These estimates were generated using the proce- dure outlined by Snijders and Bosker (1999).
The slope for those with more frequent negative cognitions at the start of treatment was flatter; those with more negative cognitions did not re- spond to treatment as quickly. The appraisal anal- yses also indicate that perceptions of stress in the first week of treatment predict rate of change. Indi- viduals who perceived daily stressors as more un- desirable and more controllable (trend) exhibited slower rates of change (flatter slopes) in treatment, and those who had higher coping efficacy exhibited faster rates of change (steeper slopes).
In the next multilevel model, coping strategies reported in the first week of treatment were used to predict differences in rates of change. All eight strategies were predictors in the same equation to assess the unique effects of each coping strategy. Greater use of direct action coping and relaxation in the first week of treatment was associated with better treatment response. On the other hand, those who used more acceptance coping reported slower rates of change in depression scores.
Finally, affective reactivity to negative appraisals of event undesirability during the first week of ther- apy had a significant effect on depression growth trajectories. Individuals who were more emotion- ally reactive to negative appraisals reported slower rates of change in response to treatment; that is, their slopes were flatter.
Growth trajectories: Supplementary analyses. There are a number of other factors that might af- fect rate of change in treatment, and it is important to evaluate their effects. It is possible that individ- uals were responding to different types of events in the first week of treatment, and that these findings reflect the fact that people were reacting to differ- ent events. However, we ran additional analyses in which event type was used to predict the growth trajectories, and there was no significant effect for any event type (ps > .05). Similarly, we checked for therapist effects on the rate of change in treatment (a three-level HLM analysis where observations are nested within patient, and patients are nested within therapist), and the results indicated that there was not a significant amount of variation in growth trajectories attributable to differences in therapists. Given that the presence of Axis II symp- tomatology could be related to chronicity and confounded with coping, reactivity, and rates of change, we reestimated the growth models control- ling for the presence of a coexisting Axis II dis- order. The pattern of results was almost identical to the findings reported above. Because our outcome

D A L L Y C O P I N G A N D C O G N I T I V E T H E R A P Y O U T C O M E 8 5
measure (BDI-II) pertains to depressive symptoms, we reestimated the longitudinal growth models ex- cluding patients with anxiety disorders only (no comorbid depression). Despite the decrease in sample size, all of the predictive effects of daily negative cognitions, appraisals, and coping re- mained significant or marginally significant, with the exception of two predictors which did not reach significance: acceptance coping (p = .14) and affective reactivity to undesirability appraisals (p = • 11 ). Finally, although we controlled for number of sessions in all analyses, we were concerned that the large variability in treatment length could have an impact on our findings. For this reason, we reesti- mated the growth models using only the first 12 sessions for all participants, and we excluded 5 pa- tients who had less than 5 sessions. Again, most of the significant effects remained the same, with the exceptions of undesirability appraisals (p = .36) and acceptance coping (p = .14).
Discussion Previous attempts to evaluate the predictive role of stress and coping variables in CT outcome have yielded inconsistent results, which could be due to limitations in the assessment of coping and affect regulation and reliance on less powerful pretest- posttest comparisons of symptom level. The daily assessment paradigm and longitudinal growth modeling approach should enhance our ability to model the effects of patient characteristics on treat- ment response.
We hypothesized that patients who began treat- ment with fewer negative daily cognitions and ap- praisals, more frequent use of coping strategies that are presumably more adaptive, and lower emotional reactivity would be better equipped to capitalize on CT, and therefore would evidence superior t reatment response. Overall, our major hypotheses were supported.
D A I L Y S T R E S S V A R I A B L E S A N D
I N I T I A L D E P R E S S I O N
Intake depression level was significantly associated with more negative daily cognitions and appraisals of event undesirability and coping efficacy in re- sponse to stress, as well as with the use of less ac- tive coping and more social support coping. These findings are consistent with previous research show- ing that depression is associated with more severe primary appraisals (Gunthert et al., 2002; Lyubomir- sky, Tucker, Caldwell, & Berg, 1999) and with Beck's cognitive theory that depressed patients have information processing biases, such as over- generalization of the meaning of negative events (e.g., Haaga & Beck, 1992). However, our finding
that perceived controllability of events was posi- tively related to intake depression was unexpected, because numerous studies have shown that depres- sion is associated with perceptions of event uncon- trollability (Mineka, Pury, & Luten, 1995). On the other hand, research suggests that depressed pa- tients are more likely to blame themselves for their problems, as compared to nondepressed patients (Wall & Hayes, 2000). Thus, we might infer that patients who attribute negative events to internal causes believe that the events were in their control, and therefore their fault. Consistent with previous findings, our results indicated that those higher in depression used less active coping strategies (e.g., Kuyken & Brewin, 1994; Whatley, Foreman, & Richards, 1998), which could be partly attribut- able to their lower confidence in their coping abili- ties. Instead, patients higher in depression relied comparatively more on social support. Because our measure of social support was only one item, we do not know the nature or effectiveness of this elic- ited support. Those higher in depression might en- gage in social support coping through spending positive time with others, or through less healthy coping such as relying on others to solve problems or excessive reassurance seeking (Joiner, Metalsky, Gencoz, & Gencoz, 2001).
D A I L Y S T R E S S V A R I A B L E S A N D
T R E A T M E N T R E S P O N S E
The treatment response findings generally support a capitalization perspective. Overall, faster rates of change were found among those who: (a) perceived events to be less undesirable and less controllable; (b) perceived themselves to be more capable of coping; (c) relied more frequently on direct action and relaxation coping; (d) relied less frequently on acceptance coping; and (e) were less emotionally reactive to increases in the perceived undesirability of daily events. It may be that patients with rela- tively lower initial daily stress were better able to use the therapy and thus improved more rapidly• Alternatively, these patients may have started out with relatively more skills at problem solving and relaxation which, in turn, allowed them to both handle daily stress better and to respond to treat- ment more rapidly. In contrast , pat ients who began treatment with relatively more daily stress and/or relatively less coping ability had more to contend with and more to learn in therapy, which translated into slower remission of depressive symp- toms. Unfortunately, we have no way of knowing whether patients' stress appraisals reflect typical styles of responding to daily stress or simply reflect the objective circumstances of the patients at that time.

86 G U N T H E R T E T A L .
Our findings are consistent with previous re- search (Simons et at., 1985) showing that patients who are better able to address and resolve their daily stressors at the start of therapy might be bet- ter equipped to learn from and implement cogni- tive strategies. Although patients who more fre- quently used direct action and relaxation coping reported faster rates of change in treatment, those who initially responded to daily stress with more acceptance coping showed a diminished treatment response. Of course, acceptance coping is not inherently positive or negative, but according to a goodness-of-fit model (Lazarus & Folkman, 1984), would be most helpful in the face of uncon- trollable stressors. Perhaps patients who use more acceptance tend to do so even in the face of con- trollable daily stress. If patients too often simply accept that stressors happen and believe that they cannot do anything to change them or related out- comes, it is not likely that they will act on their en- vironments to improve their circumstances.
Finally, patients who were more emotionally re- active to increases in the severity of their undesir- ability appraisals showed a weaker treatment re- sponse across time. Teasdale (1999) has suggested that CT does not alter the occurrence of negative thoughts, but instead improves the ability to objec- tively view them as just thoughts, and not reality. Recast in this way, negative thoughts are less likely to provoke strong emotional responses. Perhaps patients who are less reactive to their negative ap- praisals are more prepared to notice and objec- tively evaluate their negative appraisals. If this is the case, the skills taught in CT, such as challenging negative appraisals, would be easier to learn and implement in daily life.
Our finding regarding the predictive role of af- fective reactivity to appraisals is particularly note- worthy, because the within-subject index of daily affect regulation represents a more process-oriented approach to understanding stress responses. Rather than simply using average levels of negative ap- praisals, for example, to predict outcomes, we are able to capture how mood shifts in response to negative appraisals and use this index to predict success in treatment.
L I M I T A T I O N S
Our findings should be considered in light of some methodological limitations. First, this sample is rel- atively small, which certainly has an impact on generalizability and our ability to detect significant effects. However, it is noteworthy that we found a number of theoretically consistent effects despite the relatively low power. It is also important to note that there was no control group in our study.
Thus, it is unclear whether we would have ob- tained the same pattern of results for patients in any kind of treatment, including pharmacotherapy and other types of psychotherapy. In addition, a number of patients (46%) received a combination of CT and pharmacotherapy. Although we con- trolled for patients' psychotropic medication status (yes/no), this classification is simplistic and does not take into account the various types of medica- tion, when patients first began pharmacotherapy, and changes in their medication over the course of treatment. Most of our patients were Caucasian and well-educated, and it is unknown if our results would generalize to minority patients or patients with lower education levels.
Although the repeated daily assessments are an improvement over past attempts to measure pa- tients' initial stress and coping, there are a few limitations of our approach. Because the patients completed the daily assessment questionnaires for up to 7 days and returned them to their therapist just once (at the end of the week), we have no way to verify that measures were actually completed on a daily basis (Stone, Shiffman, Schwartz, Bro- derick, & Hufford, 2003). For the sake of brevity, we used a measure of the worst event of the day to measure stress and relevant appraisals. This strategy should be augmented by a checklist of potential stressors, in order to get a more accurate picture of all stressors a patient experiences on a given day. Due to our concern with keeping the daily assessment brief, we omitted some impor- tant appraisal dimensions, such as event predict- ability, and coping strategies, such as religious coping. Also, although all of the targeted coping strategies were actual ways of responding to stress, sometimes the strategies themselves, such as ca- tharsis, overlap with depressive symptoms. Ten- hen and Affleck (2002) argue that the unclear boundaries between coping responses, cognitions, and symptoms plague the coping literature as a whole. A similar problem involves our event cat- egories. Often, patients reported a cognitive or emotional "event" as their worst problem of the day. Thus, the symptoms themselves became stress- ful situations with which patients had to learn to cope. Because the DCI asks for the worst "prob- lem" of the day, instead of prompting for a spe- cific event, patients might have been more in- clined to report cognitive or emotional symptoms as stressors.
An underlying assumption of our reactivity mea- sure was that negative appraisals or cognitions led to an increase in negative mood. However, because we assessed these variables only once per day, cau- sality is ambiguous, and it is possible that on some

D A I L Y C O P I N G A N D C O G N I T I V E T H E R A P Y O U T C O M E 87
days negative mood preceded more negative ap- praisals and thoughts.
Another concern is that higher levels of depres- sion are associated with a more negative reporting bias (Summerfeldt & Endler, 1996). We controlled for initial depression level in an attempt to mitigate this concern. In addition, the use of within-person statistics addresses this issue to some degree. The affective reactivity index is less affected by negative reporting bias, because it captures how distressed an individual is when he or she perceive stress to be very undesirable, relative to how distressed he or she "typically" is (i.e., on other days during the week of data collection).
Other limitations of the study relate to the chal- lenges of evaluating change in psychotherapy. First, because research shows that a substantial portion of the gains made in therapy are attained in the first few weeks of treatment (Ilardi & Craighead, 1994), assessing daily stress and coping variables after the first week of treatment is not ideal. It would be de- sirable to assess these variables immediately after intake. Second, we did not assess potential media- tors of treatment outcome, such as compliance with homework assignments or in-session process variables (Barber & DeRubeis, 1989; Burns & Nolen-Hoeksema, 1991 ), or the occurrence of stress- ful life events during the course of treatment. For this reason, we are unable to evaluate why daily stress and coping variables had their expected ef- fects on CT outcome. Finally, we had no measure of treatment integrity, which is important to any analysis of treatment outcomes.
Conclusions We predicted that patients with better initial ability to handle daily stressors would have better out- comes in CT. Although previous CT studies evalu- ated the predictive role of coping variables, broadly defined, none examined coping with real-life daily stressors. Our findings generally support the capi- talization model and suggest the need for further clinical investigation and empirical research to bet- ter help patients with poor ability to cope with daily stress. Additional research with alternative treatments is required, to evaluate the specificity of our findings. More generally, our findings illustrate the powerful potential of a daily process design, and within-subjects analyses, to study patient pre- dictors of psychotherapy outcome.
References Abramson, L., Seligman, M., & Teasdale, J. (1978). Learned
helplessness in humans: Critique and reformulation. Jour- nal of Abnormal Psychology, 87, 49-74.
Affleck, G., Zautra, A., Tennen, H., & Armeli, S. (1999).
Multilevel daily process designs for consulting and clinical psychology: A preface for the perplexed. Journal of Con- sulting and Clinical Psychology, 67, 746-754.
Alford, B., & Beck, A. T. (1997). The integrative power of cog- nitive therapy. New York: The Guilford Press.
American Psychiatric Association. (1994). Diagnostic and sta- tistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Association.
Barber, J. P., & DeRubeis, R. J. (1989). On second thought: Where the action is in cognitive therapy for depression. Cognitive Therapy and Research, 13,441-457.
Barlow, D. H., Raffa, S., & Cohen, E. M. (2002). Psychosocial treatments for panic disorders, phobias, and generalized anxiety disorder. In P. C. Nathan & J. M. Gorman (Eds.), A guide to treatments that work (pp. 301-335). London: Oxford University Press.
Beck, A. T., Brown, G., Steer, R., Eidelson, J., & Riskind, J. (1987). Differentiating anxiety and depression: A test of the cognitive content-specificity hypothesis. Journal of Abnor- mal Psychology, 96, 179-183.
Beck, A. T., Steer, R., & Brown, G. (1996). Beck Depression Inventory manual (2nd ed.). San Antonio, TX: Psychologi- cal Corporation.
Beck, J. (1995). Cognitive therapy: Basics and beyond. N e w York: The Guilford Press.
Bolger, N., & Zuckerman, A. (1995). A framework for study- ing personality in the stress process. Journal of Personality and Social Psychology, 69, 890-902.
Bryant, M. J., Simons, A. D., & Thase, M. E. (1999). Therapist skill and patient variables in homework compliance: Con- trolling an uncontrolled variable in cognitive therapy out- come research. Cognitive Therapy and Research, 23, 381- 399.
Bryk, A., & Raudenbush, S. (1992). Hierarchical linear mod- els. Newbury Park, CA: Sage Publications.
Burns, D. D., & Nolen-Hoeksema, S. (1991). Coping styles, homework compliance, and the effectiveness of cognitive- behavioral therapy. Journal of Consulting and Clinical Psy- chology, 59, 305-311.
Clark, D., Beck, A. T., & Alford, B. A. (1999). Scientific foun- dations of cognitive theory and therapy of depression. N e w York: John Wiley & Sons.
Coyne, J. C. (1976). Toward an interactional description of depression. Psychiatry, 39, 28-40.
Cronbach, L., & Snow, R. (1977). Aptitudes and instructional methods. New York: Irvington.
David, J., & Suls, J. (1999). Coping efforts in daily life: Role of big five traits and problem appraisals. Journal of Personal- ity, 67, 265-294.
DeRubeis, R., & Crits-Christoph, P. (1998). Empirically sup- ported individual and group psychological treatments for adult mental disorders. Journal of Consulting and Clinical Psychology, 66, 37-52.
Dozois, D., Dobson, K., & Ahnberg, J. (1998). A psychometric evaluation of the Beck Depression Inventory-II. Psycholog- ical Assessment, 10, 83-89.
Elkin, I., Shea, M., Watkins, J., Imber, S., Sotsky, S., Collins, J., Glass, D., Pilkonis, P., Leber, W., Dockerty, J., Fiester, S., & Parloff, M. (1989). NIMH Treatment of Depression Col- laborative Research Program: General effectiveness of treatments. Archives of General Psychiatry, 46, 971-983.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1995). User's guide for the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I/P), (Version 2.0). Unpublished manuscript, Biometrics Research Department, N e w York State Psychiatric Institute.
Gunthert, K., Cohen, L. H., & Armeli, S. (1999). The role of

88 G U N T H E R T ET A L .
neuroticism in daily stress and coping. Journal of Personal- ity and Social Psychology, 77, 1087-1100.
Gunthert, K., Cohen, L., H., & Armeli, S. (2002). Unique effects of depressive and anxious symptomatology on daily stress and coping. Journal of Social and Clinical Psychol- ogy, 583-609.
Haaga, D., & Beck, A. T. (1992). Cognitive therapy. In E. S. Paykel (Ed.), Handbook ofaffective disorders (2nd ed., pp. 511-523). New York: The Guilford Press.
Ilardi, S., & Craighead, W. E. (1994). The role of nonspecific factors in cognitive-behavior therapy for depression. Clini- cal Psychology: Science and Practice, 1,138-156.
Joiner, T. E., Metalsky, G. I., Gencoz, E, & Gencoz, T. (2001). The relative specificity of excessive reassurance-seeking to depressive symptoms and diagnoses among clinical samples of adults and youth. Journal of Psychopathology and Behav- ioral Assessment, 23, 35-41.
Kuyken, W., & Brewin, C. (1994). Stress and coping in depressed women. Cognitive Therapy and Research, 18, 403-412.
Kuyken, W., Kurzer, N., DeRubeis, R. J., Beck, A. T., & Brown, G. K. (2001). Response to cognitive therapy in depression: The role of maladaptive beliefs and personality disorders. Journal of Consulting and Clinical Psychology, 69, 560- 566.
Lazarus, R., & Folkman, S. (1984). Stress, appraisal, and cop- ing. New York: Springer.
Lueger, R. J., Howard, K. I., Martinovich, Z., Lutz, W., Ander- son, E. E., & Grissom, G. (2001). Assessing treatment progress of individual patients using expected treatment response models. Journal of Consulting and Clinical Psy- chology, 69, 150-158.
Lyubomirsky, S., Tucker, K. L., Caldwell, N. D., & Berg, K. (1999). Why ruminators are poor problem solvers: Clues from the phenomenology of dysphoric rumination. Journal of Personality and Social Psychology, 77, 1041-1060.
Mineka, S., Pury, C., & Luten, A. (1995). Explanatory style in anxiety and depression. In G. Buchanan & M. Seligman (Eds.), Explanatory style (pp. 135-158). Hillsdale, NJ: Erlbaum.
Porter, L. S., & Stone, A. A. (1996). An approach to assessing daily coping. In M. Zeidner & N. S. Endler (Eds.), Hand- book of coping: Theory, research, applications (pp. 133- 150). New York: John Wiley & Sons.
Regier, D. A., Rae, D. S., Narrow, W. E., Kaelber, C. T., & Schatzberg, A. E (1998). Prevalence of anxiety disorders and their comorbidity with mood and addictive disorders. British Journal of Psychiatry, 173, 24-28.
Rude, S., & Rehm, L. (1991). Response to treatments for depression: The role of initial status on targeted cognitive and behavioral skills. Clinical Psychology Review, 11,494- 514.
Simons, A., Gordon, J., Monroe, S., & Thase, P. (1995). Toward an integration of psychologic, social, and biologic factors in depression. Effects on outcome and course of cog- nitive therapy. Journal of Consulting and Clinical Psychol- ogy, 63,369-377.
Simons, A. D., Lustman, P. J., Wetzel, R. D., & Murphy, G. E. (1985). Predicting response to cognitive therapy of depres- sion: The role of learned resourcefulness. Cognitive Ther- apy and Research, 9, 79-89.
Snijders, T. A., & Bosker, R. J. (1999). Multilevel analysis: An
introduction to basic and advanced multilevel modeling. London: Sage Publications.
Sotsky, S., Glass, D., Shea, M., Pilkonis, P., Collins, J., Elkin, I., Watkins, J., Imber, S., Leber, W., Moyer, J., & Oliveri, M. (1991). Patient predictors of response to psychotherapy and pharmacotherapy: Findings in the NIMH Treatment of Depression Collaborative Research Program. American Journal of Psychiatry, 148, 997-1008.
Steer, R., Beck, A. T., Clark, D., & Beck, J. (1994). Psychomet- ric properties of the Cognition Checklist with psychiatric outpatients and university students. Psychological Assess- ment, 6, 67-70.
Stone, A., & Neale, J. (1984). New measure of daily coping: Development and preliminary results. Journal of Personal- ity and Social Psychology, 46, 892-906.
Stone, A., Schwartz, J., Neale, J., Shiffman, S., Marco, C., Hickcox, M., Paty, J., Porter, L., & Cruise, L. (1998). A comparison of coping assessed by ecological momentary assessment and retrospective recall. Journal of Personality and Social Psychology, 74, 1670-1680.
Stone, A., Shiffman, S., Schwartz, J. E., Broderick, J. E., & Hufford, M. R. (2003). Patient compliance with paper and electronic diaries. Controlled Clinical Trials, 24, 182-199.
Summerfeldt, L. J., & Endler, N. S. (1996). Coping with emo- tion and psychopathology. In M. Zeidner & N. S. Endler (Eds.), Handbook of coping: Theory, research, applications (pp. 602-639). New York: John Wiley & Sons.
Teasdale, J. D. (1999). Emotional processing, three modes of mind and the prevention of relapse in depression. Behavior Research and Therapy, 37(Suppl. 1), $53-77.
Tennen, H., & Affleck, G. (2002). The challenge of capturing daily processes at the interface of social and clinical psy- chology. Journal of Social and Clinical Psychology, 21, 610-627.
Wall, T. N., & Hayes, J. A. (2000). Depressed clients' attribu- tions of responsibility for the causes of and solutions to their problems. Journal of Counseling and Development, 78, 81-86.
Watson, D., & Clark, L. A. (1994). The PANAS-X: Manual for the Positive and Negative Affect Schedule--Expanded Form. Iowa City: University of Iowa.
Weissman, A., & Beck, A. T. (1978). Development and valida- tion of the Dysfunctional Attitude Scale: A preliminary investigation. Paper presented at the annual meeting of the Education Research Association, Toronto, Ontario, Canada.
Whatley, S. L., Foreman, A. C., & Richards, S. (1998). The relationship of coping style to dysphoria, anxiety, and anger. Psychological Reports, 83,783-791.
Whisman, M. (1993). Mediators and moderators of change in cognitive therapy of depression. Psychological Bulletin, 114, 248-265.
Zuroff, D., & Blatt, S. (2002). Vicissitudes of life after short- term treatment of depression: Roles of stress, social sup- port, and personality. Journal of Social and Clinical Psy- chology, 21,473-496.
Zuroff, D., Blatt, S., Sanislow, C., Bondi, C., & Pilkonis, P. (1999). Vulnerability to depression: Reexamining state dependence and relative stability. Journal of Abnormal Psy- chology, 108, 76-89.
RECEIVED: March 13, 2003 ACCEPTED: March 22, 2004
Related Documents