Prediction of Potential Metastatic Sites in Cutaneous Head and Neck Melanoma Using Lymphoscintigraphy Christopher J. O'Brien, FRACS, Roger F. Uren, FRACP, John F. Thompson, FRACS, Robert B. Howman-Giles, FRACP, Karin Petersen-Schaefer, RN, Helen M. Shaw, PHD, Michael J. Quinn, FRACS, William H. McCarthy, FRACS, Sydney, Australia BACKGROUND:The technique of lymphoscintigra- phy may allow a more selective approach to the management of clinically negative neck nodes among patients with cutaneous head and neck melanoma. PATIENTSAND METHODS:A group of 97 patients with cutaneous head and neck melanoma had preoperative lymphoscintigraphy using intrader- mal injections of technetium 99m antimony tri- sulfide colloid to identify sentinel nodes. Fifty-one patients were eligible for clinical analysis after initial definitive treatment by wide excision only (n = 11), wide excision and elective dissection of the neck (n = 19) or axilla (n = 1), or wide excision and a sentinel node biopsy procedure (n = 20). RESULTS: Sentinel nodes were identified in 95 of 97 lymphoscintigrams, and 85% of patients had multiple sentinel nodes. In 21 patients (22%), sentinel nodes were identified outside the parotid region and the 5 main neck levels, mostly in postauricular nodes (n = 13). Lympho- scintigrams were discordant with clinical predic- tions in 33 patients (34%). Lymph nodes were positive in 4 elective dissections and 4 sentinel node biopsies. Among 16 patients evaluable af- ter wide excision and a negative sentinel node biopsy, 4 patients subsequently developed metastatic nodes; however, confident identifica- tion of all nodes marked as sentinel nodes on lymphoscintigraphy was not achieved at the original biopsy procedure in 3 of these patients. CONCLUSIONS: Lymphoscintigraphy and sentinel node biopsy are more difficult to perform in the head and neck than in other parts of the body. The reliability of sentinel node biopsy based on lymphoscintigraphy may be improved by identi- From The SydneyMelanomaUnit (C JOB, JFT, KPS, HMS, MJQ, WMC), RoyalPrinceAlfred Hospital,Sydney;and NuclearMedicine and Diagnostic Ultrasound (RFU, RBHG), Camperdown, Australia. Requestsfor reprintsshould be addressedto AssociateProfessor C.J. O'Brien, The Sydney Melanoma Unit, Royal Prince Alfred Hospital, Missenden Road, Camperdown NSW 2050 Australia. Presented at the 41st Annual Meetingof the Societyof Head and Neck Surgeons, Boston, Massachussetts,May 1-3, 1995. fying and marking all nodes that are considered to receive direct lymphatic drainage from the primary melanoma, and by use of a gamma probe intraoperatively. Am J Surg. 1995;170: 461--466. T here is still no definite evidence that elective re- gional node dissection improves survival among pa- tients with cutaneous melanoma. ~4 Elective lym- phadenectomy increases the morbidity and cost of treatment, and many patients are found not to have pathologically in- w~lved nodes) Consequently, the manageraent of regional lymph nodes among patients with cutaneous melanoma needs to be more selective. This is especially true in the head and neck, where elective lymphadenectomy may be associ- ated with unwanted cosmetic and functional problems. 5 The use of modified and selective neck dissections reflects an effort to achieve a more individualized approach among patients with head and neck melanoma, since only certain lymph node groups are removed, and important anatomic structures are preserved. These operations are based on clin- ical prediction of likely metastatic sites in the parotid gland and neck, depending upon the anatomic site of the primary melanoma. 6s In a recently reported experience from the Sydney Melanoma Unit, a high rate of disease control was achieved using this approach, and false-negative results were rare2 A total of 106 patients had elective modified or se- lective neck dissections over a 6-year period by one surgeon, and there were only 3 recurrences outside the dissected fields. In contrast to these results, other recent publications 9-'~ have suggested that such clinical predictions of metastatic sites are unreliable and, because lymphatic pathways in the head and neck can be highly variable, lymphoscintigraphy should be used to identify at-risk lymph nodes. In one study, Wells et al 1~reported that lymphoscintigraphy demonstrated lymphatic drainage to sites not predicted clinically in 2l of a group of 25 patients (84%). These findings deserve close scrutiny, since their validity is clearly dependent upon the accuracy of clinical forecasting. For example, it was stated in that study that the most likely site of lymphatic drainage for 3 of 4 patients with melanoma of the ear was to the pos- terior triangle. We would not agree with that clinical pre- diction. There were also unusual lymphoscintigraphic find- ings of uncertain clinical significance. For example, all 4 patients with melanoma of the cheek in that study demon- strated drainage to the posterior triangle. Clearly, further investigation is needed to evaluate the ef- THE AMERICAN JOURNAL OF SURGERY '~ VOLUME 170 NOVEMBER 1995 461

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Prediction of Potential Metastatic Sites in Cutaneous Head and Neck Melanoma
Using Lymphoscintigraphy Christopher J. O'Brien, FRACS, Roger F. Uren, FRACP, John F. Thompson, FRACS,
Robert B. Howman-Giles, FRACP, Karin Petersen-Schaefer, RN, Helen M. Shaw, PHD, Michael J. Quinn, FRACS, William H. McCarthy, FRACS, Sydney, Australia
BACKGROUND: The technique of lymphoscintigra- phy may allow a more selective approach to the management of clinically negative neck nodes among patients with cutaneous head and neck melanoma.
PATIENTS AND METHODS: A group of 97 patients with cutaneous head and neck melanoma had preoperative lymphoscintigraphy using intrader- mal injections of technetium 99m antimony tri- sulfide colloid to identify sentinel nodes. Fifty-one patients were eligible for clinical analysis after initial definitive treatment by wide excision only (n = 11), wide excision and elective dissection of the neck (n = 19) or axilla (n = 1), or wide excision and a sentinel node biopsy procedure (n = 20).
RESULTS: Sentinel nodes were identified in 95 of 97 lymphoscintigrams, and 85% of patients had multiple sentinel nodes. In 21 patients (22%), sentinel nodes were identified outside the parotid region and the 5 main neck levels, mostly in postauricular nodes (n = 13). Lympho- scintigrams were discordant with clinical predic- tions in 33 patients (34%). Lymph nodes were positive in 4 elective dissections and 4 sentinel node biopsies. Among 16 patients evaluable af- ter wide excision and a negative sentinel node biopsy, 4 patients subsequently developed metastatic nodes; however, confident identifica- tion of all nodes marked as sentinel nodes on lymphoscintigraphy was not achieved at the original biopsy procedure in 3 of these patients.
CONCLUSIONS: Lymphoscintigraphy and sentinel node biopsy are more difficult to perform in the head and neck than in other parts of the body. The reliability of sentinel node biopsy based on lymphoscintigraphy may be improved by identi-
From The Sydney Melanoma Unit (C JOB, JFT, KPS, HMS, MJQ, WMC), Royal Prince Alfred Hospital, Sydney; and Nuclear Medicine and Diagnostic Ultrasound (RFU, RBHG), Camperdown, Australia.
Requests for reprints should be addressed to Associate Professor C.J. O'Brien, The Sydney Melanoma Unit, Royal Prince Alfred Hospital, Missenden Road, Camperdown NSW 2050 Australia.
Presented at the 41 st Annual Meeting of the Society of Head and Neck Surgeons, Boston, Massachussetts, May 1-3, 1995.
fying and marking all nodes that are considered to receive direct lymphatic drainage from the primary melanoma, and by use of a gamma probe intraoperatively. Am J Surg. 1995;170: 461--466.
T here is still no definite evidence that elective re- gional node dissection improves survival among pa- tients with cutaneous melanoma. ~4 Elective lym-
phadenectomy increases the morbidity and cost of treatment, and many patients are found not to have pathologically in- w~lved nodes) Consequently, the manageraent of regional lymph nodes among patients with cutaneous melanoma needs to be more selective. This is especially true in the head and neck, where elective lymphadenectomy may be associ- ated with unwanted cosmetic and functional problems. 5
The use of modified and selective neck dissections reflects an effort to achieve a more individualized approach among patients with head and neck melanoma, since only certain lymph node groups are removed, and important anatomic structures are preserved. These operations are based on clin- ical prediction of likely metastatic sites in the parotid gland and neck, depending upon the anatomic site of the primary melanoma. 6s In a recently reported experience from the Sydney Melanoma Unit, a high rate of disease control was achieved using this approach, and false-negative results were rare2 A total of 106 patients had elective modified or se- lective neck dissections over a 6-year period by one surgeon, and there were only 3 recurrences outside the dissected fields.
In contrast to these results, other recent publications 9-'~ have suggested that such clinical predictions of metastatic sites are unreliable and, because lymphatic pathways in the head and neck can be highly variable, lymphoscintigraphy should be used to identify at-risk lymph nodes. In one study, Wells et al 1~ reported that lymphoscintigraphy demonstrated lymphatic drainage to sites not predicted clinically in 2l of a group of 25 patients (84%). These findings deserve close scrutiny, since their validity is clearly dependent upon the accuracy of clinical forecasting. For example, it was stated in that study that the most likely site of lymphatic drainage for 3 of 4 patients with melanoma of the ear was to the pos- terior triangle. We would not agree with that clinical pre- diction. There were also unusual lymphoscintigraphic find- ings of uncertain clinical significance. For example, all 4 patients with melanoma of the cheek in that study demon- strated drainage to the posterior triangle.
Clearly, further investigation is needed to evaluate the ef-
THE AMERICAN JOURNAL OF SURGERY '~ VOLUME 170 NOVEMBER 1995 461
LYMPHOSCINTIGRAPHY TO PREDICT MELANOMA METASTATIC SITES/O'BRIEN ET AL I
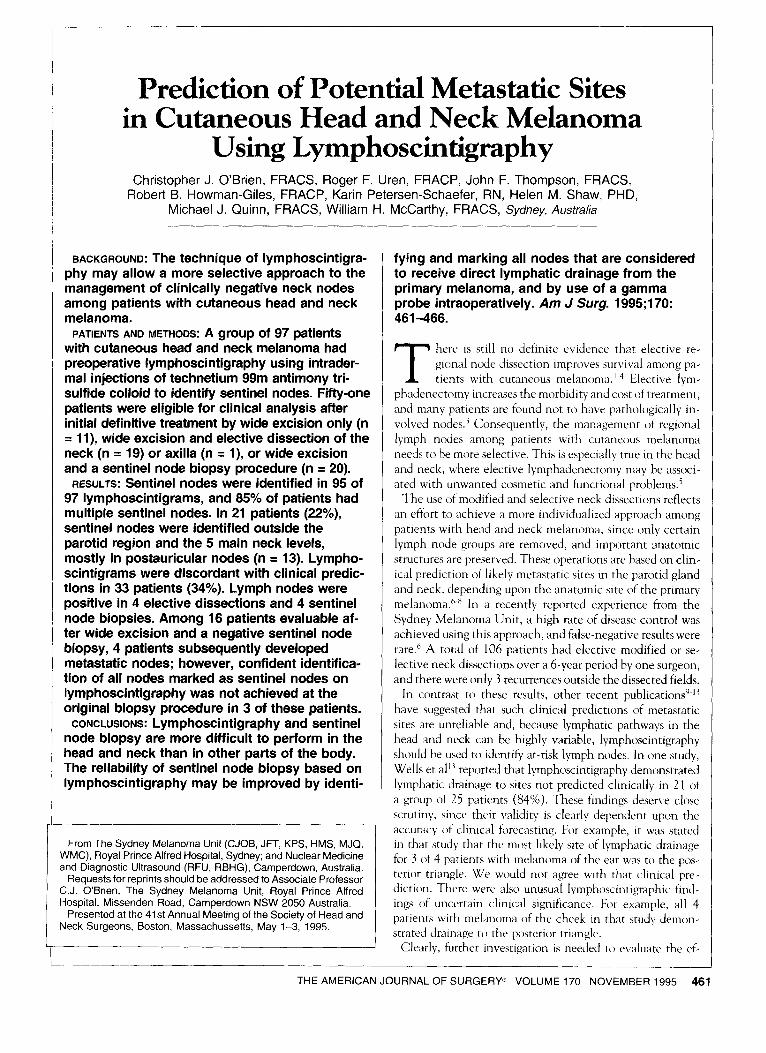
Figure 1. The numbers of primary melanomas at each of the 10 cutaneous head and neck subsites are shown for 97 pa- tients with cutaneous head and neck melanoma.
ficacy and accuracy of lymphoscmtigraphy in the head and neck, especially since this technique is playing an increas- ing role in clinical decision making and is an integral part of the technique of lymphatic mapping and sentinel node biopsy. 14 Lymphoscintigraphy has been shown to be accu- rate in identifying sites of potential nodal metastases in melanoma patients with widespread primary sites, mainly of the trunk and limbs. 15"17 We believe, however, that there are potential problems with the techniques of lymphoscintigra- phy and sentinel node biopsy in the head and neck that do not occur elsewhere.
The present study has three aims: first, to document the lymphoscintigraphic findings in a group of patients with cu- taneous malignant melanoma of the head and neck; second, to correlate these results with clinically predicted metasta- tic sites that would be encompassed by modified and selec- tive neck dissections previously recommended6; and third, to correlate the clinical outcome of patients after definitive surgery with lymphoscintigraphic findings to determine their clinical relevance.
P A T I E N T S A N D M E T H O D S Between January 1986 and March 1995, two of the authors
(RU and RH-G) performed a total of 800 lymphoscintigrams on patients with melanomas at all sites who subsequently had treatment at the Sydney Melanoma Unit. Patients were included in the present analysis only if they had a previously untreated malignant melanoma arising on the skin of the
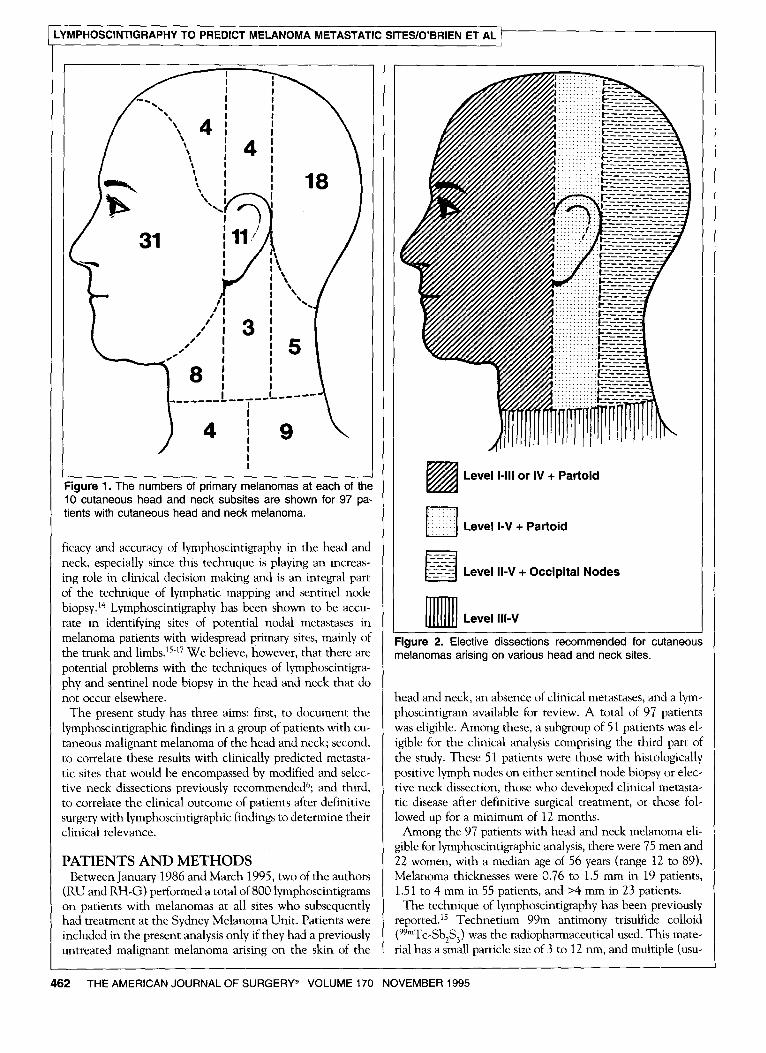
~ Level I-III or IV + Partoid
~ Level I-V + Partoid
~ Level II-V + Occipital Nodes
~ Level UI-V
Figure 2, Elective dissections recommended for cutaneous melanomas arising on various head and neck sites.
head and neck, an absence of clinical metastases, and a lym- phoscintigram available for review. A total of 97 patients was eligible. Among these, a subgroup of 51 patients was el- igible for the clinical analysis comprising the third part of the study. These 51 patients were those with histologically positive lymph nodes on either sentinel node biopsy or elec- tive neck dissection, those who developed clinical metasta- tic disease after definitive surgical treatment, or those fol- lowed up for a minimum of 12 months.
Among the 97 patients with head and neck melanoma eli- gible for lymphoscintigraphic analysis, there were 75 men and 22 women, with a median age of 56 years (range 12 to 89). Melanoma thicknesses were 0.76 to 1.5 mm in 19 patients, 1.51 to 4 mm in 55 patients, and >4 mm in 23 patients.
The technique of lymphoscintigraphy has been previously reported. 15 Technetium 99m antimony trisulfide colloid (99mTc-Sb283) was the radiopharmaceutical used. This mate- rial has a small particle size of 3 to 12 nm, and multiple (usu-
462 THE AMERICAN JOURNAL OF SURGERY ~ VOLUME 170 NOVEMBER 1995

LYMPHOSCINTIGRAPHY TO PREDICT MELANOMA METASTATIC SITES/O'BRIEN ET AL
TABLE I
Distribution of Sentinel Nodes Detected by Lymphoscintigraphy in Patients With Cutaneous Head and Neck Melanoma
Level
ally 4 to 6) small-w~lume intradennal injections of approximately 0.05 to 0.1 mL were placed around the melanoma biopsy site of the primary lesion. All studies were performed prior to wide excision of the melanoma. Scanning was carried out using a rectangular field-~)f-view digital gamma camera with a low-energy, high-resolution col- limator. Scanning was carried out im- mediately and the major lymph chan- nels were defined at this stage. Delayed scans were then performed approxi- mately 2.5 hours later. Antero- posterior and lateral views were ob- tained as necessary. A sentinel node was defined as any draining node that was seen to receive direct lymph drainage from the biopsy site. On the delayed images, these were also the most intense nodes on the scan. The
Primary Site N I II III IV V Parotid Other*
Anterior scalp 4 3 2 4 1 Coronal scalp 4 3 2 1 1 2 3 Posterior scalp 18 9 2 1 2 2 6 Face 31 10 17 3 1 1 21 2 Ear 11 11 1 2 5 3 Anterior upper neck 8 3 2 2 2 1 1 Coronal neck 3 3 2 1 Posterior upper neck 5 3 1 4 2 Anterior lower neck 4 t 2 4 1 1 Posterior lower neck 9 2 4 4 3 Total 97 21
Table values are numbers of patients with, in the N column, a primary lesion at the ~ndicated site; or, for the region/levels columns, a sentinel node at the indicated level. "Pahents listed in this column had sentinel nodes seen on lymphoscintlgraphy that were outside the parotid region or the five major neck levels
skin overlying the sentinel node or nodes was marked with indelible pen fi)r later clinical correlation. We defined 10 anatomic subsites of the head and neck, and the number of primary melanomas at each subsite is shown in Figure 1.
Clinical predictions of metastatic pathways were based on the anatomic site of the primary melanoma. Recommended clectivc dissections have been previously described and are summarized in Figure 2. For the purposes of correlation with the lymphoscmtigraphic results, selective neck dissection of levels 1 to II1 with parotidectomy was used as the recom- mended operation for primary lesions in the face and ante- rior scalp. The lymph node levels, which reflect the stan- dard terminology used in head and neck oncology, were: level l--submandibular and submental triangles; level I I - - upper jugular; level llI--mid-jugular; level IV~lower jugu- lar; and level V--posterior triangle groups, respectively. In Figure~ 1 and 2 the width of the band through the coronal plane was 5 cm. This was arbitrary, as was the horizontal border between the upper and lower neck, which was the l¢~wer border of the thyroid cartilage.
The surgical management of the patients in this study was not part of a single prospective protocol, although many pa- tients had been registered in separate trials of sentinel node biopsy and elective neck dissection. Some patients had wide excision of the primary melanoma alone, some had wide ex- cision and a sentinel node biopsy procedure, while others had wide excision and selective or modified lymph node dissection. Therefi ~re, n~t all sentinel nodes were biopsied and not: all op- erations were based on the results of lymphoscintigraphy.
Our technique of lymphatic mapping and sentinel node biopsy has been previously described. 16 Patients were given tour tc, six intradermal injections of Patent Blue V dye (Guerbert, Aulnay-Sous-Bois, France) around the primary melanoma or biopsy site, up to a volume of 0.5 to 1 mL. lnjecti~ns were given 10 to l 5 minutes prior to commence- ment of surgery and exploration of the sentinel node was performed at the sites marked on the skin at the time of lym- phoscintigraphy. Successful sentinel node biopsy depended upon the operating surgeon's finding an afferent blue/green
lymphatic leading to a similarly stained lymph node. All sen- tinel nodes were examined histologically by permanent hematoxylin and eosin-stained paraffin sections, and more recently, immunohistochemical stains were used to improve the accuracy of diagnosis of metastatic melanoma.
RESULTS Lymphoscintigraphic Findings
Sentinel lymph nodes were identified by preoperative lym- phoscintigraphy in 95 of 97 patients. In 2 patients there was no flow after injection of tracer. In 13 patients only 1 sen- tinel node was demonstrated; 33 patients had 2 nodes, 28 pa- tients had 3 nodes, 15 patients had 4 nodes, and 6 patients had 5 sentinel nodes. The mean number was 2.7 nodes. The distribution of sentinel nodes is documented in Table I. Nodes were identified as lying in the parotid gland or the five major neck levels, while nodes identified at other sites were placed in the "other" colunm. The numbers in the columns, therefore, refer to the number of patients who had a sentinel node identified at a particular neck level. For example, among 4 patients with anterior scalp primary lesions, 3 patients had sentinel nodes demonstrated at level I1, 2 patients had sen- tinel nodes at level IV, and all 4 had lymphoscintigraphic ev- idence of sentinel nodes in the parotid gland. In 1 of the pa- tients, a sentinel node was identified outside these sites, and in this case, it was a postauricular node.
Sentinel nodes found in level I were associated with pri- mary sites of the face and anterior upper neck only. Sentinel nodes at level ii were demonstrated for melanomas in every anatomic site, even the lower neck. Similarly, virtually all anatomic sites demonstrated the ability to drain to levels 1V and V, although sentinel nodes in level V were very un- common when the primary site was the anterior scalp, the face, or the anterior upper neck. More than one third of pa- tients demonstrated drainage to the parotid region, princi- pally from the expected primary sites of coronal scalp, ante- rior scalp, face, and anterior upper neck.
Finally, a total of 21 of 97 patients (22%) demonstrated sentinel nodes in sites other than the parotid glands and the
THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 NOVEMBER 1995 463
1 LYMPHOSCINTIGRAPHY TO PREDICT MELANOMA METASTATIC SITES/O'BRIEN ET AL /
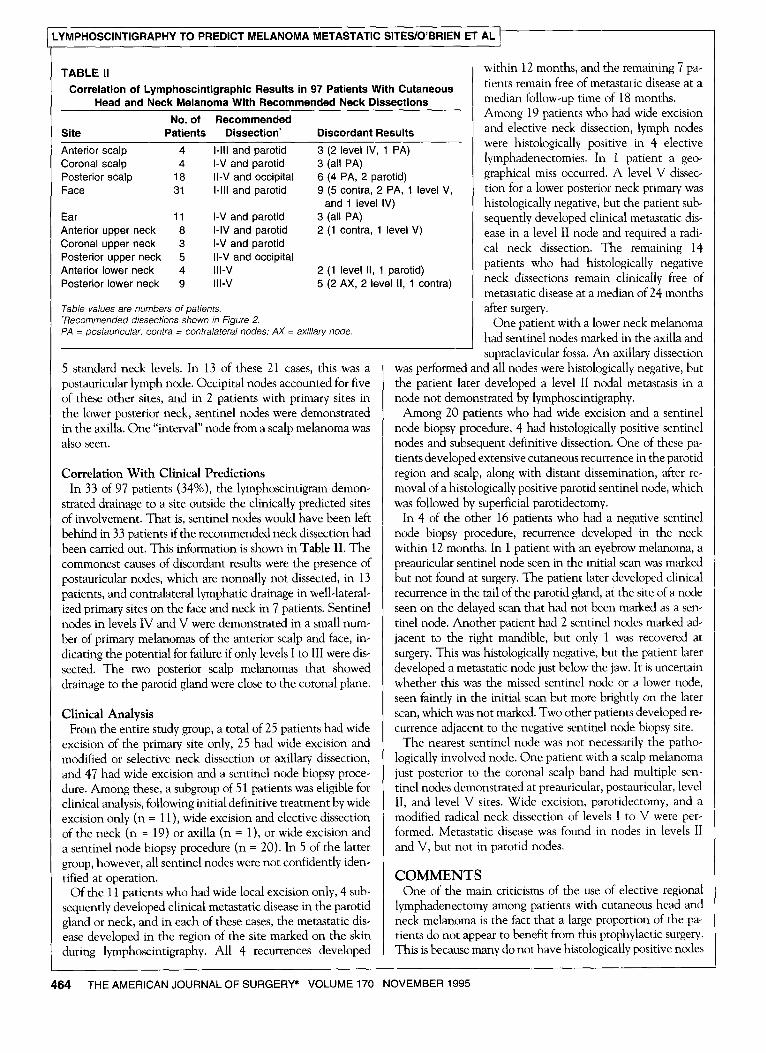
TABLE II Correlation of Lymphoscintigraphic Results in 97 Patients With Cutaneous
Head and Neck Melanoma With Recommended Neck Dissections
No. of Recommended Site Patients Dissection" Discordant Results
Anterior scalp 4 I-III and parotid Coronal scalp 4 I-V and parotid Posterior scalp 18 I I-V and occipital Face 31 I-III and parotid
Ear 11 I-V and parotid Anterior upper neck 8 I-IV and parotid Coronal upper neck 3 I-V and parotid Posterior upper neck 5 II-V and occipital Anterior lower neck 4 III-V Posterior lower neck 9 III-V
3 (2 level IV, 1 PA) 3 (all PA) 6 (4 PA, 2 parotid) 9 (5 contra, 2 PA, 1 level V,
and 1 level IV) 3 (all PA) 2 (1 contra, 1 level V)
2 (1 level II, 1 parotid) 5 (2 AX, 2 level II, 1 contra)
Table values are numbers of patients. "Recommended dissections shown in Figure 2. PA = postauricular; contra = contralateral nodes; AX = axillary node.
5 standard neck levels. In 13 of these 21 cases, this was a postauricular lymph node. Occipital nodes accounted for five of these other sites, and in 2 patients with primary sites in the lower posterior neck, sentinel nodes were demonstrated in the axilla. One "interval" node from a scalp melanoma was also seen.
Correlation With Clinical Predictions In 33 of 97 patients (34%), the lymphoscintigram demon-
strated drainage to a site outside the clinically predicted sites of involvement. That is, sentinel nodes would have been left behind in 33 patients if the recommended neck dissection had been carried out. This information is shown in Table II. The commonest causes of discordant results were the presence of postauricular nodes, which are normally not dissected, in 13 patients, and contralateral lymphatic drainage in well-lateral- ized primary sites on the face and neck in 7 patients. Sentinel nodes in levels IV and V were demonstrated in a small num- ber of primary melanomas of the anterior scalp and face, in- dicating the potential for failure if only levels I to III were dis- sected. The two posterior scalp melanomas that showed drainage to the parotid gland were close to the coronal plane.
Clinical Analysis From the entire study group, a total of 25 patients had wide
excision of the primary site only, 25 had wide excision and modified or selective neck dissection or axillary dissection, and 47 had wide excision and a sentinel node biopsy proce- dure. Among these, a subgroup of 51 patients was eligible for clinical analysis, following initial definitive treatment by wide excision only (n = 11), wide excision and elective dissection of the neck (n = 19) or axilla (n --- 1), or wide excision and a sentinel node biopsy procedure (n = 20). In 5 of the latter group, however, all sentinel nodes were not confidently iden- tified at operation.
Of the 11 patients who had wide local excision only, 4 sub- sequently developed clinical metastatic disease in the parotid gland or neck, and in each of these cases, the metastatic dis- ease developed in the region of the site marked on the skin during lymphoscintigraphy. All 4 recurrences developed
within 12 months, and the remaining 7 pa- tients remain free of metastatic disease at a median follow-up time of 18 months. Among 19 patients who had wide excision and elective neck dissection, lymph nodes were histologically positive in 4 elective lymphadenectomies. In 1 patient a geo- graphical miss occurred. A level V dissec- tion for a lower posterior neck primary was histologically negative, but the patient sub- sequently developed clinical metastatic dis- ease in a level II node and required a radi- cal neck dissection. The remaining 14 patients who had histologically negative neck dissections remain clinically free of metastatic disease at a median of 24 months after surgery.
One patient with a lower neck melanoma had sentinel nodes marked in the axilla and supraclavicular fossa. An axillary dissection
was performed and all nodes were histologically negative, but the patient later developed a level II nodal metastasis in a node not demonstrated by lymphoscintigraphy.
Among 20 patients who had wide excision and a sentinel node biopsy procedure, 4 had histologically positive sentinel nodes and subsequent definitive dissection. One of these pa- tients developed extensive cutaneous recurrence in the parotid region and scalp, along with distant dissemination, after re- moval of a histologically positive parotid sentinel node, which was followed by superficial parotidectomy.
In 4 of the other 16 patients who had a negative sentinel node biopsy procedure, recurrence developed in the neck within 12 months. In 1 patient with an eyebrow melanoma, a preauricular sentinel node seen in the initial scan was marked but not found at surgery. The patient later developed clinical recurrence in the tail of the parotid gland, at the site of a node seen on the delayed scan that had not been marked as a sen- tinel node. Another patient had 2 sentinel nodes marked ad- jacent to the right mandible, but only 1 was recovered at surgery. This was histologically negative, but the patient later developed a metastatic node just below the jaw. It is uncertain whether this was the missed sentinel node or a lower node, seen faintly in the initial scan but more brightly on the later scan, which was not marked. Two other patients developed re- currence adjacent to the negative sentinel node biopsy site.
The nearest sentinel node was not necessarily the patho- logically involved node. One patient with a scalp melanoma just posterior to the coronal scalp band had multiple sen- tinel nodes demonstrated at preauricular, postauricular, level II, and level V sites. Wide excision, parotidectomy, and a modified radical neck dissection of levels I to V were per- formed. Metastatic disease was found in nodes in levels II and V, but not in parotid nodes.
C O M M E N T S One of the main criticisms of the use of elective regional
lymphadenectomy among patients with cutaneous head and neck melanoma is the fact that a large proportion of the pa- tients do not appear to benefit from this prophylactic surgery. This is because many do not have histologically positive nodes
4.64 THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 NOVEMBER 1995

LYMPHOSCINTIGRAPHY TO PREDICT MELANOMA METASTATIC SITES/O'BRIEN ET AL
found in the neck dissection specimen, and a considerable number die of disseminated disease despite negative node pathology? Even modified radical and selective neck dissec- tions can be criticized on these grounds, despite the fact that they allow for a significant reduction in morbidity when com- pared with elective radical neck dissection. The concept of performing definitive lymphadenectomy only on those pa- tients with histologically positive nodes is an attractive one, and the techniques of lymphoscintigraphy and sentinel lymph node biopsy are aimed at identifying this patient group.[ 4'I6
Our prewous experience shows that lymphoscinligraphy, combined with sentinel node biopsy using blue dye, is accu- rate in identifying the sites of potential nodal meta:stases in p'atie~ts with melanoma of the trunk and extremities./517 Clearly, a large, prospective, randomized clinical trial is nec- essary to establish the efficacy of the sentinel node biopsy tech- nique, and such a trial is currently being carried out. Therefore, a thorough evaluation of that technique is beyond the scope ~f the present report. In the present study, we have aimed to evaluate the usefidness of lymphoscintigraphy among patients with cutaneous melanoma of the head and neck, and we have fi~und this t¢~ be the most difficult area of the body in which to apply these techniques. Other recent publications have re- ported very small patient numbers, usually combining head and neck and upper-trunk melanomas, 9'1 l.lz or have described ~nty limited use of lymphoscintigraphy among patients hav- ing sentinel node biopsy. >
The primary melanomas examined in this study were dis- tributed widely over the various subsites of the head and neck. Lymphatic drainage patterns from these sites were imaged in 05 ~f the 97 patients, and in only 2 patients was there a flail- ure to demonstrate flow of tracer from the primary site. The results of the present study show that for head and neck melanomas, the majority of patients have multiple nodes demonstrated by the radiopharmaceutical tracer and, further- more, the nodes nearest to the primary melanoma are not necessarily the ones affected by metastatic spread. This is be- cause any node receiving direct drainage from the primary site is a potential site fbr metastases. A channel can traverse node groups in the upper neck and pass directly to a ~,entinel node in the lower neck
It is important to appreciate that not all nodes showing tracer uptake on delayed scans are sentinel nodes. Sentinel nodes are nodes that can be demonstrated to have direct drainage from the primary melanoma site. In the head and neck, a potential problem arises where both false-negative and fialse-positive results can occur. Failure to demonstrate sentinel nodes was rare, but an inability to find all sentinel nodes ~t surgery was a definite problem. We believe that this latter deficiency was a reflection of the fact that sentinel nodes in the neck are often small and difficult to isolate, rather d~an suggesting that the lymphoscintigram incorrectly demonstrated activity in tissue other than lymph nodes.
Of 97 patients, 21 had sentinel nodes demonstrated in sites outside the parotid gland and the 5 main levels of the neck. Nearly all ~f these nodes were in the postauricular or occipi- tal regions. Differentiating between postauricular and occipi- tal nodes was sometimes difficult for the nuclear medicine physicians, but it is recommended that these nodal groups sh~uld be marked and named as accurately as possible at the
time of lymphoscintigraphy. Metastatic disease in occipital nodes did not occur in the present study, but is regularly seen. The need to remove occipital nodes in selective neck dissec- tion of levels II to V for posterior scalp melanomas has been raised in a previous study. 6 In contrast, postauricular nodal in- volvement is very rare, and so the clinical relevance of lym- phatic drainage to these nodes on lymphoscintigraphy is un- clear. In our series of 183 neck dissections performed in 179 patients, ~ no patient presented with postauricular nodal in- volvement, no patient had dissection of the postauricular nodes, and no patient has developed recurrent disease in postauricular nodes. No incidence of postauricular nodal in- volvement has yet occurred in the present study.
Two melanomas that demonstrated drainage to the axilla were located on the posterior lower neck, and this must be regarded as a watershed area from which unpredictable drainage can occur.
When the lymphoscintigraphic findings were compared with clinical predictions by matching them with the rec- ommended modified and selective operations used at the Sidney Melanoma Unit, e one third of patients demonstrated sentinel nodes at a site that would have been missed by the recommended dissection. This does not necessarily mean, however, that metastatic disease would inevitably develop in these nodes. These discordant results include the group of 13 patients with tracer activity in postauricular lymph nodes, but other findings were also of interest. Of 4 patients with primary sites in the anterior scalp, 2 had sentinel lymph nodes at level IV, suggesting that simply dissecting the parotid gland and levels I to III may lead to subsequent t:ail- ure in the lower neck. Shah et al r recommended level I to IV dissection for this site. Similarly, 2 of 31 patients with melanomas of the face showed sentinel nodes at levels IV and V. Of 18 patients with posterior scalp melanomas, 2 demonstrated sentinel nodes in the preauricular region, but these patients both had primary lesions just posterior to the coronal band, arbitrarily set at a 5-cm width. Some vari- ability in lymphatic drainage clearly exists in this region, and the coronal line through the external auditory meatus can- not be regarded as a guaranteed line of demarcation between anterior and posterior lymphatic drainage. Melanomas of the lower neck, both anterior and posteric~r, also demonstrated variance from the predicted sites.
Despite these findings, the majority of sentinel lymph nodes identified were within the predicted regions of the parotid gland and neck. The relevance of discordant results in the remaining 34% of patients is the important issue, and this can only be established by adequate follow-up. The clinical outcome of a group of patients who had modified and selec- tive neck dissections based on these clinical predictions has already been reported ~
The clinical follow-up of the 51 patients in this study for whom we have outcome data demonstrates a number of im- portant points. First, nearly all the metastatic nodes that de- veloped after wide excision alone or that were identified at sen- tinel node biopsy or elective neck dissection were found in the region of sentinel nodes demonstrated by preoperative lym- phoscintigraphy. Second, the technique of sentinel node biopsy in the head and neck region is not straightforward. Difficulties arose in some patients regarding the designation of
THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 NOVEMBER 1995 465

LYMPHOSCINTIGRAPHY TO PREDICT MELANOMA METASTATIC SITES/O'BRIEN ET AL l
which of the nodes demonstrated on lymphoscintigraphy were sentinel nodes, and in 5 of 20 patients in whom sentinel node biopsy was attempted, not all the marked sentinel nodes could be found. In 4 patients, regional metastatic disease developed after a negative sentinel node biopsy procedure. In 3 of them, confident sentinel node identification had not been achieved at operation, and metastatic disease subsequently developed in nodes adjacent to the site. Another patient failed in the neck after an axillary dissection performed on the basis of lympho- scintigraphy. We do not believe that any of these examples represent "skip metastases." Rather, they reflect the presence of direct lymphatic channels to the involved nodes from the primary melanoma site.
Biopsy of sentinel nodes in the parotid region may present special problems. Sentinel nodes in the parotid gland are of- ten very small, may be difficult to find, and their removal may put the facial nerve at risk. These concerns were raised in a previous report, 5 which suggested that formal parotidectomy with dissection of the facial nerve may be the safest approach to sentinel nodes at this site. Since one third of the 97 patients in the present study had lymphatic drainage to the parotid gland, the management of lymph nodes at this site is a signif- icant issue among patients with head and neck melanomas.
Although this study has demonstrated some of the limita- tions of lymphoscintigraphy and sentinel node biopsy in the head and neck, this combination of techniques has consid- erable potential. It may allow the management of the clini- cally negative neck to be more selective for melanoma pa- tients and help to minimize the cost and possible morbidity of elective regional node surgery by avoiding operation in pa- tients who do not have metastatic disease. It is possible that the use of the gamma probe 19 during surgery will allow the identification of all sentinel nodes seen on lymphoscintigra- phy if the blue dye method does not readily identify them. On the other hand, the merits of removing multiple sentinel nodes must be carefully considered, as it will be preferable to perform a selective neck dissection that may encompass all the nodes in a particular level or region. Further follow-up is still required to determine whether removing clinically neg- ative nodes containing microscopic disease by using this tech- nique will confer a survival benefit.
REFERENCES 1. Veronesi U, Adamus J, Bandiera DC, et al. Inefficacy of immedi- ate node dissection in stage I melanoma of the limbs. NEJM. 1977;297: 627-63O. 2. Sire FH, Taylor WF, Pritchard DJ, Soule Eli. Lymphadenectomy in the management of stage I malignant melanoma: a prospective ran- domized study. Mayo Clin Proc. 1986;61:697-705.
3. O'Brien CJ, Coates AS, Petersen-Schaefer K, et al. Experience with 998 cutaneous melanomas of the head and neck over 30 years. Am J Surg. 1991;162:310-314. 4. Coates AS, Ingvar CI, Petersen-Schaefer K, et al. Elective lymph node dissection in patients with primary melanoma of the trunk and limbs treated at the Sydney Melanoma Unit from 1960 to 1991. J Am CoU Surg. 1995;80:402-409. 5. O'Brien CJ, Petersen-Schaefer K, Papadopoulos T, Malka V. Evaluation of 107 therapeutic and elective parotidectomies for cuta- neous melanoma. Am J Surg. 1994;168:400-403. 6. O'Brien CJ, Petersen-Schaefer K, Ruark D, et al. Radical, modified and selective neck dissection for cutaneous malignant melanoma. Head Neck. 1995;17:232-241. 7. Shah JP, Kraus DH, Dubner S, Sarkar S. Patterns of regional lymph node metastases from cutaneous melanomas of the head and neck. Am J Surg. 1991;162:320-323. 8. Balm AJM, Kroon BBR, Gregor RT, Hilgers FJM. Value of elec- tive lymph node dissection in head and neck melanoma. D/agn Oncd. 1993;3:263-267. 9. Wanebo HJ, Harpole D, Teates D. Radionudide lymphoscintigra- phy with technetium 99m antimony sulfide colloid to identify lym- phatic drainage of cutaneous melanoma at ambiguous sites in the head and neck and trunk. Cancer. 1985;55:1403-1413. 10. Wanebo HJ, Chung M. Radionuclide lymphoscintigraphy to iden- tify lymphatic drainage patterns of cutaneous head and neck melanoma. Diagn Oncol. 1993;3:258-262. 11. Norman J, Cruse W, Espinosa C, et al. Redefinition of cutaneous lymphatic drainage with the use of lymphoscintigraphy for malignant melanoma. Am J Surg. 1991;162:432-437. 12. Eberbach MA, Wahl RI, Argenta LC, et al. Utility of lympho- scintigmphy in directing surgical therapy for melanomas of the head, neck and upper thorax. Surgery. 1987;102:433-442. 13. Wells KE, Cruse CW¢, Daniels S, eta[. The use of lymphoscintig- raphy in melanoma of the head and neck. Plast Reconstr Surg. 1994;93: 757-761. 14. Morton DL, Wen D-R, Wong JH, et al. Technical details of intra- operative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127:392-399. 15. Uren RF, Howman-Giles RB, Shaw HM, et al. Lympho- scintigraphy in high-risk melanoma of the trunk: predicting draining node groups, defining lymphatic channels and locating the sentinel node. J Nucl Med. 1993;34:1435-1440. 16. Thompson JF, McCarthy WH, Bosch CMJ, et al. Sentinel lymph node status as an indicator of the presence of metastatic melanoma in regional lymph nodes. Melanoma Res. 1995;5:255-260. 17. Uren RF, Howman-Giles R, Thompson JF, et al. Lymphoscin- tigraphy to identify sentinel lymph nodes in patients with melanoma. Melanoma Res. 1994;4:395-399. 18. Morton DL, Wen D-R, Foshag LJ, et al. Intraoperative lymphatic mapping and selective cervical lymphadenectomy for early-stage melanomas of the head and neck. J Clin Oncol. 1993;11:1751-1756. 19. Alex JC, Weaver DL, Fairbank JT, et al. Gammma-probe-guided lymph node localization in malignant melanoma. Surg Oncol. 1993;2: 303-308.
466 THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 NOVEMBER 1995
Related Documents











