Vol. 2, 1801-1808, October 1996 Clinical Cancer Research 1801 Prediction of Occult Neck Metastases in Laryngeal Carcinoma: Role of Proliferating Cell Nuclear Antigen, MIB-1, and E-Cadherin Immunohistochemical Determination Alessandro Franchi, Oreste Gallo, Vieri Boddi, and Marco Santuccit Institute of Anatomic Pathology [A. F., M. S.]. Otolaryngology Clinic [0. 0.], and Institute of General Pathology [V. B.], University of Florence, Viale 0. B. Morgagni 85, 50134 Florence, Italy ABSTRACT The aim of this study is to investigate the predictive value of proliferative activity assessment and E-cadherin expression by means of immunohistochemistry in identify- ing patients with laryngeal squamous cell carcinoma at a high risk for occult node metastasis. Thirty consecutive patients treated for laryngeal carcinoma with false clinically negative nodes (occult metastases, pN+) between the years 1980 and 1990 were selected for this study. A group of 30 cases with negative cervical lymph nodes (pN-) having a similar anatomic site and tumor size distribution was used as control. In each case, several histological parameters, including grade, pattern of invasion, number of mitosis (X 10 high-power field), tumor inflammatory infiltrate, and tumor sclerosis, were assessed. Proliferative activity was deter- mined using immunohistochemical staining for proliferating cell nuclear antigen (PCNA) and MIB-1. Other putative prognostic factors investigated at the immunohistochemical level were the cell adhesion molecule E-cadherin and two oncoproteins, p53 and c-erbB-2. In pN+ cases, the expres- sion of PCNA and MIB-l was significantly higher than in the pN- group. Moreover, a significant loss of E-cadherin expression was observed in carcinomas with occult metas- tases. No differences in p53 and c-erbB-2 oncoproteins were found between pN+ and pN- cases. Among the other path- ological parameters examined, only histological grade was significantly associated with the presence of occult metasta- ses, but on mubtivariate analysis, this relationship was lost. We conclude that PCNA, MIB-1, and E-cadherin are inde- pendent predictors of occult nodal disease in laryngeal squamous cell carcinoma, and their immunohistochemical determination could be useful in identifying patients with clinically negative lymph nodes who are at considerable risk for occult metastases and who may benefit from elective neck dissection. Received 3/26/96: revised 7/3/96; accepted 7/3/96. I To whom requests for reprints should be addressed. Phone: 39 55 416951; Fax: 39 55 4379868. INTRODUCTION Preoperative identification of occult lymph node metastasis represents a crucial point in the clinical management of patients with laryngeal cancer for its prognostic and therapeutic impli- cations (I). Data from literature indicate that 4-40% of patients with laryngeal carcinoma and clinically negative neck lymph nodes have indeed occult metastases on subsequent histological examination (2-6). As a consequence, treatment of N0 patients is a matter of great controversy between those who are in favor of a “wait and see” attitude and those who prefer elective neck dissection. Indeed, prophylactic neck dissection eliminates the risk of late metastases in N0 cases, but exposes the patient to a higher morbidity and higher hospital costs, which are in most cases unnecessary (I , 3). Another possible disadvantage of bymphadenectomy may be the local reduction of the immuno- logical host defense, which may facilitate the spread of residual tumor cells. Therefore, the identification of biological tumor factors indicative of high or low risk of occult lymph node metastases would be extremely helpful in deciding on elective or delayed therapeutic strategy in the treatment of the neck in N0 laryngeal cancer. Previous clinicopathobogical studies have shown that the presence of locoregional metastases in patients with laryngeal carcinoma is significantly associated with some histological features of the primary tumor, such as the degree of differenti- ation, tumor growth pattern, presence of peritumoral desmopla- sia, and inflammation (7-9). Additional studies confirmed that histological grade and host immune response correlate signifi- cantly with occult lymph node metastasis (1 , 10). However, because of the absence of established criteria, the evaluation of this group of histological parameters is very subjective, and reproducibility is poor. In recent years, the efforts of several research groups have bed to a dramatic improvement in the understanding of the neoplastic growth process and have furnished novel molecular tools that may help in identifying tumors more likely to metas- tasize, being therefore potentially useful for management and prognostic purposes. In particular, several lines of evidence suggest that the evaluation of tumor cell proliferative activity, cell adhesion markers, and oncoprotein expression could allow an estimate of the biological behavior of head and neck squa- mous cell carcinoma. When proliferative activity was evaluated by tumor labeling index in a series of head and neck squamous cell carcinomas, the results indicated that lesions with a high proliferative activity have a poorer survival (1 1). Recently, Benazzo et a!. observed a significant correlation between pro- liferative indices measured after in vivo bromodeoxyuridine incorporation and tumor dimension, histological differentation, and lymph node involvement in a group of patients with carci- nomas of the head and neck ( 1 2). Similar results were obtained Research. on June 12, 2020. © 1996 American Association for Cancer clincancerres.aacrjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Vol. 2, 1801-1808, October 1996 Clinical Cancer Research 1801
Prediction of Occult Neck Metastases in Laryngeal Carcinoma: Role
of Proliferating Cell Nuclear Antigen, MIB-1, and E-Cadherin
Immunohistochemical Determination
Alessandro Franchi, Oreste Gallo, Vieri Boddi,
and Marco Santuccit
Institute of Anatomic Pathology [A. F., M. S.]. Otolaryngology Clinic[0. 0.], and Institute of General Pathology [V. B.], University of
Florence, Viale 0. B. Morgagni 85, 50134 Florence, Italy
ABSTRACT
The aim of this study is to investigate the predictive
value of proliferative activity assessment and E-cadherin
expression by means of immunohistochemistry in identify-
ing patients with laryngeal squamous cell carcinoma at a
high risk for occult node metastasis. Thirty consecutive
patients treated for laryngeal carcinoma with false clinically
negative nodes (occult metastases, pN+) between the years
1980 and 1990 were selected for this study. A group of 30
cases with negative cervical lymph nodes (pN-) having a
similar anatomic site and tumor size distribution was used
as control. In each case, several histological parameters,
including grade, pattern of invasion, number of mitosis (X 10
high-power field), tumor inflammatory infiltrate, and tumor
sclerosis, were assessed. Proliferative activity was deter-
mined using immunohistochemical staining for proliferating
cell nuclear antigen (PCNA) and MIB-1. Other putative
prognostic factors investigated at the immunohistochemical
level were the cell adhesion molecule E-cadherin and two
oncoproteins, p53 and c-erbB-2. In pN+ cases, the expres-
sion of PCNA and MIB-l was significantly higher than in
the pN- group. Moreover, a significant loss of E-cadherin
expression was observed in carcinomas with occult metas-
tases. No differences in p53 and c-erbB-2 oncoproteins were
found between pN+ and pN- cases. Among the other path-
ological parameters examined, only histological grade was
significantly associated with the presence of occult metasta-
ses, but on mubtivariate analysis, this relationship was lost.
We conclude that PCNA, MIB-1, and E-cadherin are inde-
pendent predictors of occult nodal disease in laryngeal
squamous cell carcinoma, and their immunohistochemical
determination could be useful in identifying patients with
clinically negative lymph nodes who are at considerable risk
for occult metastases and who may benefit from elective
neck dissection.
Received 3/26/96: revised 7/3/96; accepted 7/3/96.I To whom requests for reprints should be addressed. Phone: 39 55416951; Fax: 39 55 4379868.
INTRODUCTION
Preoperative identification of occult lymph node metastasis
represents a crucial point in the clinical management of patients
with laryngeal cancer for its prognostic and therapeutic impli-
cations (I). Data from literature indicate that 4-40% of patients
with laryngeal carcinoma and clinically negative neck lymph
nodes have indeed occult metastases on subsequent histological
examination (2-6). As a consequence, treatment of N0 patients
is a matter of great controversy between those who are in favor
of a “wait and see” attitude and those who prefer elective neck
dissection. Indeed, prophylactic neck dissection eliminates the
risk of late metastases in N0 cases, but exposes the patient to a
higher morbidity and higher hospital costs, which are in most
cases unnecessary ( I , 3). Another possible disadvantage of
bymphadenectomy may be the local reduction of the immuno-
logical host defense, which may facilitate the spread of residual
tumor cells. Therefore, the identification of biological tumor
factors indicative of high or low risk of occult lymph node
metastases would be extremely helpful in deciding on elective
or delayed therapeutic strategy in the treatment of the neck in N0
laryngeal cancer.
Previous clinicopathobogical studies have shown that the
presence of locoregional metastases in patients with laryngeal
carcinoma is significantly associated with some histological
features of the primary tumor, such as the degree of differenti-
ation, tumor growth pattern, presence of peritumoral desmopla-
sia, and inflammation (7-9). Additional studies confirmed that
histological grade and host immune response correlate signifi-
cantly with occult lymph node metastasis (1 , 10). However,
because of the absence of established criteria, the evaluation of
this group of histological parameters is very subjective, and
reproducibility is poor.
In recent years, the efforts of several research groups have
bed to a dramatic improvement in the understanding of the
neoplastic growth process and have furnished novel molecular
tools that may help in identifying tumors more likely to metas-
tasize, being therefore potentially useful for management and
prognostic purposes. In particular, several lines of evidence
suggest that the evaluation of tumor cell proliferative activity,
cell adhesion markers, and oncoprotein expression could allow
an estimate of the biological behavior of head and neck squa-
mous cell carcinoma. When proliferative activity was evaluated
by tumor labeling index in a series of head and neck squamous
cell carcinomas, the results indicated that lesions with a high
proliferative activity have a poorer survival (1 1). Recently,
Benazzo et a!. observed a significant correlation between pro-
liferative indices measured after in vivo bromodeoxyuridine
incorporation and tumor dimension, histological differentation,
and lymph node involvement in a group of patients with carci-
nomas of the head and neck ( 1 2). Similar results were obtained
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1802 Predictors of Occult Metastases in Laryngeal Carcinoma
2 The abbreviations used are: PCNA, proliferating cell nuclear antigen;
OR, odds ratio; Cl, confidence interval.
Table 1 C linicab features of 60 pa tients with 1arynge al squam ous cell carcinoma, the obj ect of this study
Site T” Treatment
Partial Total Age (Mean) Sex M:FSupraglottic Glottic 1 2 3 4
pN+ 20 10 7 8 10 5 13 17 58.5 29:1
pN- 20 10 8 9 8 5 16 14 59.3 29:1
a TNM staging.
when proliferation was measured by flow cytometric analysis of
DNA content (13).
Loss of intercellular adhesion might be an important event
in the early phases of the metastatic process. The potential
relationship between the expression of the adhesion molecule
E-cadherin, a member of a family of calcium-dependent cell-cell
adhesion molecules also including P- and N-cadherin, and thepresence of lymph node metastasis in laryngeal carcinoma has
been the object of studies by different groups. Schipper ci’ a!.
observed that E-cadherin expression decreased with loss of
differentintion in primary cnrcinomns, and thnt lymph node
metastases expressed a lower bevel of the protein. suggesting an
important role of cadhenn loss in the metastatie process ( 14). In
a subsequent study, Mattijssen e� a!, were unable to find anysignificant relationship between the level of li-eadherin expres2sion and the presence of lymph node metastasis in a group of 50
head and neck squamous cell carcinomas ( I 5) However. these
studies only examined patients with clinical evidence of mela-
static disease. and no information is available in the literature
about the relationship between E-cadherin expression and the
presence of occult lymph node metastases,Indeed, most of the studies concerning predictors of the
behavior of carcinomas of the head and neck have consideredheterogeneous groups of lesions concerning both the site of
primarylesion and the clinical node status, The present study is
focused on a homogeneous population of patients with laryngealsquamous cell carcinoma and clinically negative neck lymph
nodes with the aim of defining prognostic parameters that per�mit the identification of patients at risk for occult metastases,We evaluated several histopathological features of primary le-
sions, and determined immunohistochemically tumor cell pro-
liferative activity and E-cadherin expressionS Moreover, westudied the expression of e-erbB-2 and p53 oneoproteins. the
products of two genes known to be involved in the development
of head and neck squamous cell carcinomas (16-18),
PATIENTS AND METHODS
Cases Studied. Thirty consecutive patients treated at the
Institute of Otorhinolaryngology of the University of Florence
between 1980 and 1990 for laryngeal squamous cell carcinomawith occult baterocervical metastases were selected for thisstudy, All patients had clinically negative laterocervical lymphnodes and underwent elective neck dissection, with subsequenthistological recognition of one or more occult metastases
(pN + )‘ A group of 30 patients treated in the same period for
laryngeal squamous cell carcinoma with clinically and histobog-
ically negative laterocervical lymph nodes (pN-) was used as
control, Clinical data of the two groups of patients are summa-ri�ed in Table 1.
Formalin-fixed, paraffin-embedded tissue samples from re-
section specimens were retrieved in each case, and serial see-
tions were stained with H&E or used for the immunohistochem-
ical studies. In each case, the following histological parameters
were assessed: histological degree of differentiation (well, mod-
erately, or poorly differentiated), pattern of invasion (pushing or
infiltrating), number of mitoses (X 10 high-power field), peritu-
moral inflammatory infiltrate (present or absent), and peritu-
moral sclerosis (present or absent).
Immunohlstochemlstry. lmmunohistochemical studies
were performed by the uvidin-biotin complex technique (Duko-
putts. High Wycombe. UK)� Proliferative activity was investi-
gated using monocbonul antibodies against Ki-67 (MIB-l. lm-
munotech, Marseille, France) and PCNA2 (PC-lO, DAKO
Corp,, Carpinteria, CA). For E-cudherin detection, the mono-
clonal antibody HECD- 1 (Nuclear Laser Medicine, Milan, Italy)was employed, For p53 and c-erhB-2 detection, the monoclonal
antibodies D07 (DAKO Corp.) and mAhI (Triton Diagnostics.
Alameda, CA) were used, MIB-1, E-cadherin, and p53 immu-
nostuining required microwave pretreatment of dewuxed and
rehydrated sections, Negative controls were performed by sub-stitution of the primary antibody with nonimmune rabbit ormouse serum,
Scoring of the immunostaining was performed by oneobserver (A, F.). who had no knowledge of patients’ clinical
status, using a standard light microscope equipped with an
eyepiece grid of 10 X 10 squares and a X40 objective, In each
case, at beast 1000 tumor cells were counted from areas withhigh and low expression of the antigen. All stained cells were
considered positive regardless of the intensity of the staining.
and the results were expressed in percentage of’ positive cells.
An arbitrary cutoff value of 20% positive cells was chosen to
separate cases with high and low expression of the antigens.
Statistical Analysis. Statistical tests were performed us-ing EGRET (Statistics and Epidemiology Research Corporation.Seattle, WA) and Stata (Stata Corporation. College Station,
TX) The relationship between clinical and pathological van-
ables was assayed by Fisher’s exact test, The correlation be-
tween the different immunohistochemical indices was evaluated
using Spearman’s correlation coefficient. The role of each pos-sible prognostic factor (univaniate analysis) and the joint effect
of all these factors (multivaniate analysis) was explored using
the multivaniate logistic regression analysis, The final results of
these analysis are the ORs and their 95% CIs, The likelihood
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 1803
The distribution of percentages of positively stained cells
Table 2 Evaluation of prognostic parameters in 30 pN+ and 30
pN- squamous cell carcinomas of the larynx
Prognostic factors Score pN+ pN-
PCNA >20% 24 6MIB-l >20% 17 5E-cadherin �20% 15 4
C-erbB-2 Negative
�50%
>50%
21
3
6
226
2
p53 Negative
1-10%
11-60%60-100%
11
3
88
10
4
II5
Histological grade I
IIIII
S
178
1 1
181
Pattern of invasion
Number of mitoses
PushingInfiltrating
� 10
14I 619
191 118
Peritumoral inflammation AbsentPresent
1911
1812
Peritumoral sclerosis Absent
Present
18
12
12
18
ratio statistic was used to test the following hypothesis: OR =
1.0. P values <0.05 were considered significant.
RESULTS
Table 2 synoptically summarizes the results of the immu-
nohistochemical and histopathological analysis of the pN+ and
pN- groups.
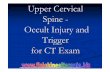
All 60 tumors stained positively for PCNA, which local-ized in the nucleus, with different degrees of intensity (Fig. 1).
Some of the mitotic figures were associated with weak anddiffuse cytoplasmic staining. The PCNA score for the whole
series ranged between 6.4 and 7 1 .7% (25.6 ± 15.9, mean ±
SD). Twenty-four patients in the pN+ group had a tumor with
PCNA score greater than 20%, whereas only six patients of thepN- group had carcinomas with more than 20% of positive
cells (P < 0.001; Fisher’s exact test).
Positivity for MIB-l was observed in all cases. Only nu-
clear staining having a finely granular pattern was observed
(Fig. 2). Almost all mitotic figures were stained. The percentage
of positive cells ranged between 2 and 49. 1% (mean, I 8.9 ±
10.3). In the pN+ group, 18 cases showed more than 20% of
positive cells, whereas in the pN- group, only 5 cases had a
MIB-l score >20% (P < 0.001 ; Fisher’s exact test).
Considering the whole series of 60 cases, the percentage of
labeled cells tended to be higher using the PCNA antibody.
However, a significant correlation between PCNA and MIB-limmunoreactivity in each case was found (r�� 0.61 ; P <
0.001). Both PCNA and MIB-l scores increased as tumorsbecame less differentiated (P = 0.03 and 0.2, respectively;
Fisher’s exact test). No relationship was found between PCNA
and MIB-l indices and mitosis count.E-cadherin expression varied greatly from case to case, and
in most tumor cells, immunoreactivity was associated with the
cell membrane (Fig. 3). Cytoplasmic staining was observed in
seven cases, and four of these were poorly differentiated card-
nomas. The percentage of E-cadherin-positive cells decreased
‘ ‘ �-.I �
� � *�a’�$ � , b�’ � ) -
. #{149}*s��r#{149}O?�1r�, ‘0#{149}.
� :� � ‘� ‘-“
�. � �� �-4 &� � ‘ �
� �: � � . �
� ‘ �-. a:
#{149}‘#{248}’U#{216}? � “ �
‘. ,4H,#{149}!* %� �
� 4� � ‘a #{149}�*�
t� � � , � -
. � � !�_-�..�,‘s’ � ‘-
# V A � � ‘- at#{149}%4#{149} S : ,� � � � -
-� . . #{163}. -‘-
4’ . . a � S � ..�
-.- #{149}�-‘,d��’.. 1�b. S*� Q!.p� *�
, �. .� . � J
� .4, � . -
Fig. I Diffuse nuclear immunostaining for PCNA in a poorly differ-
entiated squamous cell carcinoma.
significantly in the less-differentiated tumors (P = 0.00 1 ; Fish-
er’s exact test). Moreover, a significant association was found
between bow levels of cadherin expression (�20% of positive
cells) and the presence of occult lymph node metastasis (P =
0.006; Fisher’s exact test). When the expression of proliferation
markers (PCNA and MIB-b) was compared with E-cadherin
expression in each single case of the whole series, no significant
relationship was found. However, when groups with high and
low expression of the antigens (>20% and �20%) were com-
pared, it became evident that cases with high proliferative ac-
tivity tended to have a low expression of E-cadherin. In partic-
ular, a significant relationship was found between high
expression of PCNA and low expression of E-cadherin (P =
0.004; Fisher’s exact test).
Regarding p53 expression, 39 cases (65%) showed positive
nuclear staining for the oncoprotein (Fig. 4). No significant
differences were found in p53 levels between the pN+ and pN-
group using either a four-point scale scoring system ( - , nega-
tive; +, 1-10%; ++, 11-50%; and +++, >50%: Ref. 19) or
a single cutoff point (�20% or >20% positive cells). No rela-
tionship was evidenced between p53 expression and prolifera-
tion indices. c-erbB-2 oncoprotein was detected in 17 cases
(28.3%). In 14 instances, the immunostaining localized at the
cytoplasmic membrane bevel (Fig. 5), and in 3 there was diffusecytoplasmic staining. Six cases from the pN+ group and two
cases from the pN- group showed a number of positive cells
greater than 20%, but this difference was not significant. Sim-
ilarly, no significant differences were found using a three-point
scale scoring system (- , negative; +, �50%; and + +, >50%:
Ref. 20).
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1804 Predictors of Occult Metastases in Laryngeal Carcinoma
p �, , . , I :‘..�
.t 1�1�� � #{149} � .
., ‘ v#,0, . # .
,.I � - . ‘ ‘.
,�,1 .�‘
t�’.t’�, ,: . ‘, _, � a. ,‘;‘3t�,�ms. .,. -� ‘ ‘.‘!
... ‘ I � .�-, , � ., ..f,-#{149}:’� ‘ ‘ “ .,� p . ,
�:/. #{149} � ;dI..!.� .;�..‘� .c-. #{149}
.. #{182}.t�, .# -,
)4. � ‘ 4 ‘‘“S ‘ � ,,�-. -. . . ,.-,-.
.:i’� �#{149}s�’. � . � ;‘�‘.
‘,.. ,. I ‘%��‘�
2 a-,. , #{149}�,, . , : #{149} ‘�‘ �“--:- � #{149}‘�, ,, ‘I
. : _� . . . � I. ,,� , #{149}, #{149}�#{149}�, . ‘. . .,, ‘.� #{149}
‘a ;�‘r’�i:’ � . � � .% . I ‘ #{149}_4._ ‘.. ‘: #{149}.. . , �. .1g.
..-.�-I’ � � , � “- -. . ‘ � .
� /0 “ ‘“s � .
-.st. � ‘ � .“,. �_‘.; 4
pI.,,,* #{149}.::!r, � #{149}
. ‘ . #{149}�-‘�.;‘ -j.: �
- �
� ‘ , M� ‘ :� - -.�. � -. . , � �- .
. .‘ ‘Si,,’ . � ‘..‘
. # ‘�. . ‘. .
Fig. 2 MIB-l nuclear immunoreactivity in a well-differentiated squa-
mous cell carcinoma. The staining is distributed predominantly at theperiphery of tumor nests.
using the antibodies against PCNA, MIB-l, E-cadherin, p53,
and c-erbB-2 in each individual tumor of pN- and pN+ groups
is reported in Fig. 6.
Among the several histopathological features analyzed,
only the histological grade had a significant relationship with
the presence of occult metastases (P 0.02; Fisher’s exact test),
as patients with poorly differentiated carcinomas had a higher
risk of occult metastatic disease.
Univariate logistic regression analysis of the different pa-
rameters showed that high levels of PCNA and MIB-l, low
levels of E-cadherin, and poor histological differentiation were
significantly associated with the presence of occult lymph node
metastases. On multivariate analysis, only PCNA, MIB-l, and
E-cadhenn expression maintained an independent status for the
prediction of occult lymph node metastases (Table 3).
Comparison of the immunohistochemical findings in
T3-T4 tumors versus T1-T2 tumors showed that the advanced
lesions had a higher proliferative activity as assessed with both
PCNA and MIB-l stainings (P = 0.009 and P = 0.07, respec-
tively; Fisher’ s exact test) and decreased E-cadherin expression
(P = 0.07; Fisher’s exact test). Levels of p53 and c-erbB-2
expression were comparable in the two groups. No significant
difference for any of the markers tested was evidenced between
gbottic and supragbottic carcinomas.
DISCUSSIONThe metastatic process is the result of the progressive
acquisition of an aggressive tumor cell behavior, characterized
by increased cell proliferation rates, modification of cell adhe-
sive properties, and genetic alterations. Accordingly, in the
present study, we observed that in laryngeal squamous cell
carcinoma, a high proliferative activity assessed by MIB-l and
PCNA immunostaining, and low expression of the adhesion
molecule E-cadherin, significantly correlated with the presence
of occult nodal metastases.
Until recently, a major limitation in evaluating the prog-
nostic significance of these markers by means of immunohisto-
chemistry, which allows the in situ identification of the antigen,
was the necessity of employing fresh tissue, in which morphol-
ogy preservation is often suboptimal, thus precluding the use of
archive material. This problem has been overcome partially by
the introduction of methods of antigen retrieval, such as micro-
wave oven pretreatment of paraffin sections, which have greatly
facilitated the study of putative prognostic markers in surgical
pathology of tumors (2 1 ). The reliability of this technique in
studying cell proliferation and cell adhesion processes has been
demonstrated clearly by several groups (21-23). A double as-
sessment of proliferative activity using both PCNA and MIB-l
immunostainings was performed in this study, because it has
been pointed out that PCNA immunostaining may suffer from
some limitations, the major one being a reduction of positivity
when fixation time exceeds 48 h (24). On the other hand, MIB-l
determination seems not to be affected by fixation time (25), but
experimental data suggest that reduction of blood supply, which
is a common event in central areas of a tumor, may determine a
modification of the expression of the antigen (26). In the present
series, PCNA index tended to be higher than MIB-l index.
Nevertheless, a significant relationship was found between the
expression of the two antigens as already observed in other
malignancies (27-29). On the other hand, no relationship was
found between the expression of PCNA and MIB-l indices and
mitosis count, possibly because these parameters evaluate dif-
ferent phases of the proliferating cell cycle.
The results of the present study indicate that tumor cell
proliferation indices assessed by immunohistochemistry corre-
late strongly with the presence of occult metastases in laryngeal
squamous cell carcinoma. A similar relationship has been found
previously in carcinomas from different sites (28, 30). Several
studies have now confirmed the adverse prognosis of laryngeal
carcinomas with high proliferative activity as well as the asso-
ciation of other prognostic parameters, such as the degree of
differentiation and pboidy status, with enhanced proliferation
(1 1, 31). Therefore, enhanced proliferative activity may not only
be important in the early phases of malignant transformation of
the squamous epithelium of the larynx (32, 33) during the
transition from dysplasia to invasive carcinoma but could also
be a feature of lesions with a higher tendency to spread and
metastasize. Our findings are discordant with those of a recent
study, in which no association was found between PCNA and
Ki-67 indices and the presence of lymph node metastasis in a
series of laryngeal carcinomas (34). A comparison of the results
is difficult, because the distribution of PCNA and Ki-67 indices
in the node-negative and node-positive groups is not indicated in
this article. In addition, the carcinomas examined belonged to
different histotypes (squamous cell, spindle cell, large cell un-
differentiated, and neuroendocrine), and patients had different
clinical N status, whereas we considered only squamous cell
carcinomas in patients with clinically negative neck lymph
nodes.
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

siveness (35, 36). Our results confirm that there is a significant
loss of E-cadherin expression in poorly differentiated squamous
cell carcinomas of the larynx ( 14, 15). Moreover, we observed
that loss of tumor differentiation was also accompanied by
Fig. 3 E-cadherin expression in
a well-differentiated squamous
cell carcinoma. The immuno-staining is localized at the cell
membrane of most tumor cells(A). In a moderately differenti-ated carcinoma, only a few tu-
mor cells express the antigen (B).
Clinical Cancer Research 1805
‘. � � � ‘#{149},�.J � , . �
. . t,,#{149},., . ‘�;“% #{149}... ,
‘ - . \�, . � . ,‘ � �
‘ ‘ S � �
�. : ‘� � ‘ � i’, . ..
‘ . , . ‘ , d� � �
� ‘‘..,: � --,“ #{149}� . �1#{149}� :‘�.
. ‘,�%#{234}� #e ‘
.‘ ..... . ‘#{149}.,� . �l . �
‘ . #{149}4’ “‘ �w . � ‘
? ‘,‘ . � #� ..# . . ‘.,bv..� :: t�1;
. ...�?‘ � )#{149}�� �
‘$. . � . �‘..... �‘;.. .. . .-. ,,.:‘�,, . ‘ .� � .
. ,.,.-,,‘. ..,.....- ‘#{149}#{149}__., �:. . ,. .#{149} ‘ . . . �‘�:�‘ � :�‘. �
. . (� � ..�.‘- �: ‘� �
#{149}‘�‘�;, ‘ \r,.�‘ �. I � ,. . � � ‘ �‘‘. ‘ ,�,..
,� � ‘a � , � ‘;� ‘
. . ‘‘::: � � ‘ .� � ‘ .. � . .‘�;-�.‘_ ‘.
. . �c”�” �‘�‘,: ‘�‘ � “ � . . .. ::‘ � ,..‘� ,:�, a. ,“‘.‘� .. ;,. . :‘. �. - . � ‘ .� ‘ ,d S,., ,
.. . � .,.,t � �. , ., ‘:� #{149}q�’ (. ‘ J%’’-.’ % � ‘ . ..‘ .,:‘� � t$.�%,:.??�:I, � � ., ‘. .‘
. . #{149}‘�b � g,’ � �‘. a: I ‘: S... ‘� � �#{149}:.‘‘ �: � : � � :� -
Fig. 4 pS3 oncoprotein expression in a moderately differentiated squa-
mous cell carcinoma.
Several recent studies have shown that E-cadherin expres-
sion is reduced in epithebial tumors from different sites when
compared with the epithelia of origin; these modifications have
been correlated with tumor degree of differentiation and aggres-
, -. ..z�_d#{248}, ,,
� �-... . . ‘, --...--.#{149}�-..- ..‘. t ‘
_\ . I:’ : .‘ � 4i1 #{149} .‘ �l.’ ‘� �. . �1’��” � ‘ �“ ‘, t#{149}
“V’p.�.1#f”‘ ._I ! ‘� � , � :? � ,�
. ‘ ‘�Jl”w “fY!f’ji’�#{149}�� a
,. I- � ,# ‘ ,.jt ,#{149}� a” F
� :
,.. a; � � � ,#{149},� � .�: � ;�1:. !7.Z.I: ‘
..� .� -�.-“ �� ,.* ., � �
� a
� � � . I
. . . w.� �. , � � � . � I
.. � ‘;.r.���__�i:Ic:7.! .:‘�
‘ , I-. #{149}‘‘“.. y‘. .. � . a ,�
;P�#{149}, ‘� , ., . :� ,TT �
Fig. 5 c-erbB-2 immunostaining in a well-differentiated squamous cell
carcinoma.
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

0
0
‘CzUQ. a-a
x
100
Vm
w
0
0
0
0
100
mIn
pN- pN+
S 100
0
B0
50C.w
0
0
0
0
0
0
a0pN- pN+
0
60
006
pN- pN+
1806 Predictors of Occult Metastases in Laryngeal Carcinoma
§0
0
Fig. 6 Distribution of percent-age of cells positive for PCNA,MIB-l, E-cadherin, p53, and c-erbB-2 in a group of 30 pN-and 30 pN+ squamous cell car-
cinomas of the larynx with cut-
off line at 20%.
Table 3 Univariate and multivariate logistic regression analysis of 60 laryngeal cane er patients according to presence (pN + ) or absence (pN -)
of occult neck metastases
Prognostic parameter Categories
Univariate analysis Multivariate stepwise analysis
OR (95% CI) LRS (dfl” P value OR!� (95% CI) LRS (df)� P value
PCNA �20%C>20%
1.0016.00 (4.52-56.70) 23.13 (1) <0.001
1.006.16 (1.61-23.58) 1 1.56 (1) <0.001
MIB-1 �20%C
>20%1.00
8.64 (2.57-29.01) 14.30 (1) <0.0011.00
4.76 (1.01-22.58) 3.89 (1) 0.048E-cadherin
c-erbB-2
s20%’�>20%
Negativec�50%>50%
1.00
0.15 (0.04-0.55) 9.77 (1)
1.00 3.14(3)
0.52 (0.12-2.37)
3.14 (0.57-17.35)
0.0080.371
1.00
0.13 (0.04-0.40) 15.61 (1) <0.001
p53 Negativec1-10%
1 1-50%<50%
1.00 1.36 (4)0.68 (0.12-3.82)0.66 (0.19-2.31)1.45 (0.36-5.94)
0.850
Histological grade ICII
ifi
1.00 8.53 (3)
2.08 (0.60-7.24)17.60 (1.71-181.3)
0.036
Pattern of invasion PushingcInfiltrating
1.001.97 (0.70-5.54) 1.69 (1) 0.429
Number of mitoses �l0’
>101.00
0.58 (0.21-1.62) 1.07 (1) 0.584
Peritumoral inflammation AbsentcPresent
1.00
0.87 (0.31-2.46) 0.07 (1) 0.965Pentumoral sclerosis Absentc
Present1.000.44 (0.16-1.25) 2.42 (1) 0.299
a Computed by likelihood ratio statistic; df, degrees of freedom.b Adjusted OR of metastasis.C Reference category.
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 1807
cytoplasmic localization of the antigen in a number of cases,
thus confirming the findings obtained in other carcinomas and
adenocarcinomas (37-39). These data taken together suggest
that deregulated E-cadherin expression is related to the acqui-
sition of a dedifferentiated and more aggressive phenotype by
the neoplastic cells, resulting in a higher tendency to spread to
locoregional lymph nodes (36). In contrast to our data, Mattijs-
sen et a!. found no relationship between the levels of E-cadherin
expression and the presence of lymph node metastases in a
group of 50 head and neck squamous cell carcinomas (15).
However, these authors included in their series squamous cell
carcinomas from different sites, thus limiting a direct compari-
son of the results.
In vitro studies have shown that cell-cell adhesion is related
strictly to proliferation and differentiation processes. Decreased
proliferative activity has been noted when stratification is in-
duced in cultures of normal human urothelial cells, a process
that is associated with desmosome formation and increased
expression of E-cadherin (40). Similarly, cyclic AMP and re-
baxin induce differentiation, growth inhibition, and increased
expression of E-cadherin in cultured human breast cancer cells
(41, 42). We observed that loss of cadherin expression was
accompanied by an increased PCNA and MIB-1 expression in
our series of laryngeal squamous cell carcinomas. It is therefore
possible that decreased cell-cell adhesion activity in tumor tis-
sue may be rebated not only to the invasive and metastatic
properties, but also to the growth rate of tumor cells.
Our study confirms the high frequency of p53 oncopro-
tein expression in laryngeal carcinomas, indicating that p53
gene alterations may be a common genetic event in the
development ofthese neoplasms (17, 18, 43, 44). Differently
from Field et a!. (16), we found a limited expression of
c-erbB-2 in our series. Moreover, we prevalently obtained
membrane immunostaining, whereas the above-mentioned
authors observed only cytoplasmic staining. As observed
previously, the study of the expression of p53 and c-erbB-2
oncoproteins failed to reveal any significant relationship with
the presence of lymph node metastases in laryngeal squa-
mous cell carcinoma (17, 34, 45).
The evaluation of several traditional histopathological pa-
rameters showed that only the degree of differentiation was
correlated significantly with the presence of occult lymph node
metastases in our series. However, in multivariate analysis, this
parameter failed to add independent information to identify
patients at risk for occult disease. The absence of prognostic
significance of parameters such as tumor growth pattern, peri-
tumoral sclerosis, and inflammatory reaction, which has been
correlated previously with lymph node status in laryngeal car-
cinoma by other authors (1, 7, 10), points out the difficulty in
obtaining an objective and reproducible evaluation of these
histopathobogical features.
In conclusion, our study indicates that the use of an immu-
nohistochemical determination of tumor cell proliferation and
E-cadherin expression in specimens of laryngeal squamous cell
carcinoma may help in the identification of those patients with
clinically negative lymph nodes who are at considerable risk for
occult metastases. Although the sensitivity and specificity of
these markers may still be insufficient to allow a decision of
elective neck dissection, they may supplement the results ob-
tamed by sophisticated imaging techniques (46) and may be
incorporated in a multidisciplinary approach to the definition of
the appropriate therapeutic strategy in the treatment of the neck
in these patients.
REFERENCES
I. Bocca, E., Calearo, C., De Vincentiis, I., Marullo. T., Mona, 0., andOttaviani, A. Occult metastases in cancer of the larynx and their rela-
tionship to clinical and histological aspects of the primary tumor: a
four-year multicentric research. Laryngoscope, 94: 1086-1090, 1984.
2. Van den Brekel, M. W. M, Casteljins, J. A., Croll, 0. A., Stel, H. V.,Valk, J., Van der Waal, I., Golding, R. P., Meyer, C. J. L. M., and Snow,0. B. Magnetic resonance imaging vs palpation of cervical lymph node
metastases. Arch. Otolaryngol. Head & Neck Surg., 117: 666-673,1991.
3. Gallo, 0., Boddi, V., Bottai, 0. V., Parrella, F., and Fini Storchi, 0.
The treatment of the clinically negative neck in laryngeal cancer pa-tients. Head Neck, in press, 1996.
4. Shah, J. T., Medina, J. E., Shaha, A. R., Schantz, S. T., and Marti,
J. R. Cervical lymph node metastasis. Curr. Probl. Surg., 30: 273-344,1993.
5. Friedman, M., Mafee, M. F., Pacella, B. L. Strorigl, T. L., Dew, L. L.,
and Toriumi, D. M. Rationale for elective neck dissection in 1990.
Laryngoscope, 100: 54-59, 1990.
6. Au, S., Tiwan, R. M., and Snow, 0. B. False positive and falsenegative neck nodes. Head Neck Surg., 8: 78-82, 1985.
7. McGavran, M. H., Bauer, W. C., and Ogura, J. K. The incidence ofcervical lymph node metastases from epidermoid carcinoma of the
larynx and their relationship to certain characteristics of the primarytumor. Cancer (Phiba.), 14: 55-66, 1960.
8. Geelen, 0. P., Hordijck, 0. J., Ravasz, L. A., and Terhaard, C. H.Degree of tumor differentiation as a prognostic factor in advancedlaryngeal cancer. Acta Otorhinolaryngol. BeIg., 49: 1-4, 1995.
9. Kowalski, L. P., Franco, E. L., and De Andrade Sobrinho, J. Factorsinfluencing regional lymph node metastasis from laryngeal carcinoma.
Ann. Otol. Rhinol. & Laryngol., 104: 442-447, 1995.
10. Ghouri, A., Zamora, R. L., Session, D. 0., Spitznagel, E. L., and
Harvey, J. E. Prediction of occult neck disease in laryngeal cancer by
means of a logistic regression statistical model. Laryngoscope, 104.
1280-1284, 1994.
1 1 . Chauvel, P., Courdi, A., Gioanni, J., Vallicioni, J., Santini, J., andDemard, F. The labelling index: a prognostic factor in head and neckcarcinoma. Radiother. Oncol., 14: 231-237, 1989.
12. Benazzo, M., Mevio, E., Occhini, A., Franchini, 0., and Danova,
M. Proliferative characteristics of head and neck tumors: in t’ivo eval-uation by bromodeoxyuridine incorporation and flow cytometry. ORL J.
Otorhinolaryngol. Relat. Spec., 57: 39-43, 1995.
13. Wolf, 0. T., Fisher, S. 0., Truelson, J. M., and Beals, T. F. DNA
content and regional metastases in patients with advanced laryngeal
squamous cell carcinoma. Laryngoscope, 104: 479-483, 1994.
14. Schipper, J. H., Frixen, U. H., Behrens, J., Unger, A., Jahnke, K.,
and Birchmeier, W. E-cadherin expression in squamous cell carcinomas
of head and neck: inverse correlation with tumor differentiation and
lymph node metastasis. Cancer Res., 51: 6328-6337, 1991.
15. Mattijssen. V., Peters, H. M., Schalkwijk, L., Manni, J. J.,
Van’t Hof-Grootenboer, B., De Mulder P. H. M., and Ruiter, D. J.E-cadherin expression in head and neck squamous-cell carcinoma is
associated with clinical outcome. Int. J. Cancer, 55: 580-585, 1993.
16. Field, J. K., Spandidos, D. A., Yiagnisis, M., Gosney, J. R.,
Papadimitriou, K., and Stell, P. M. C-erbB-2 expression in squamous
cell carcinoma of the head and neck. Anticancer Res., 12: 613-620,
1992.
17. Field, J. K., Pavelic, Z. P., Spandidos, D. A.. Stambrook, P. J.,Jones, A. S., and Gluckman, J. L. The role of the p53 tumor suppressor
gene in squamous cell carcinoma of the head and neck. Arch. Otolar-
yngol. Head Neck Surg., 119: 1118-1122, 1993.
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1808 Predictors of Occult Metastases in Laryngeal Carcinoma
18. Maestro, R., Dolcetti, D., Gasparotto, D., Doglioni, C., Pelucchi, S.,
Barzan, L., Grandi, E., and Boiocchi, M. High frequency of p53 genealterations associated with protein over-expression in human squamouscell carcinoma of the larynx. Oncogene, 7: 1 159-1 166, 1992.
19. Ebina, M., Steinberg, S. M., Muishine, J. L., and Linnoila, R. I.Relationship of p53 overexpression and up-regulation of proliferatingcell nuclear antigen with the clinical course of non-small cell lungcancer. Cancer Res., 54: 2496-2503, 1994.
20. Kay, E. W., Barry Walsh, C. J., Cassidy, M., Curran, B., andLeader, M. C-erbB-2 immunostaining: problems with interpretation.
J. Clin. Pathol., 47: 816-822, 1994.
21. Cuevas, E. C., Bateman, A. C., Wilkins, B. S., Johnson, P. A.,
Williams, J. H., Lee, A. H. S., Jones, D. B., and Wright, B. H.Microwave antigen retrieval in immunocytochemistry: a study of 80antibodies. J. Clin. Pathob., 47: 448-452, 1994.
22. Moll, R., Mitze, M., Frixen, U. H., and Birchmeier, W. Differentialboss of E-cadherin expression in infiltrating ductal and lobular breastcarcinomas. Am. J. Pathol., 143: 1731-1742, 1993.
23. Pignatelli, M., Ansari, T. Q., Gunter, P., Liu, D., Hirano, S.,Takeichi, M., Kloppel, 0., and Lemoine, N. Loss of membranousE-cadherin expression in pancreatic cancer: correlation with lymph nodemetastasis, high grade, and advanced stage. J. Pathol., 174: 243-248,
1994.
24. Golick, M. L., and Rice, M. Optimum staining of PCNA in paraffin
sections is dependent on fixation, drying, and intensification. J. Histo-
technol., 15: 39-41, 1992.
25. Rose, D. S. C., Maddox, P. H., and Brown, D. C. Which prolifer-
ation markers for routine immunohistology? A comparison of fiveantibodies. J. Clin. Pathol., 47: 1010-1014, 1994.
26. Baisch, H., and Gerdes, J. Simultaneous staining of exponentiallygrowing versus plateau phase cells with the proliferation-associated
antibody 1067 and propidium iodide: analysis by flow cytometry. Cell
Tissue Kinet., 20: 387-391, 1987.
27. Kamel, 0. W., LeBrun, D. P., Davis, R. E., Berry, 0. J., andWarnke, R. A. Growth fraction estimation of malignant bymphomas informalin-fixed paraffin-embedded tissue using anti-PCNA/cyclin l9A2.Correlation with Ki67 labelling. Am. J. Pathol., 138: 1471-1477, 1991.
28. Oya, M., Yao, 1., Nagai, E.. and Tsuneyoshi, M. Metastasizing
intramucosal gastric carcinomas. Well differentiated type and prolifer-ative activity using proliferative cell nuclear antigen and Ki-67. Cancer(Phila.), 75: 926-935, 1995.
29. Czader, M., Porwit, A., Tani, E., Ost, A., Mazur, J., and Auer, 0.DNA image cytometry and the expression of proliferative markers(proliferating cell nuclear antigen and Ki-67) in non-Hodgkin’s lym-
phomas. Mod. Pathol., 8: 5 1-58, 1995.
30. Albers, P., Miller, 0. A., Orazi, A., Ulbright, T. M., Abbers, J.,Donohue, J. P., and Foster, R. S. Immunohistochemical assessment oftumor proliferation and volume of embryonal carcinoma identify pa-tients with clinical stage A nonseminomatous testicular germ cell tumorat low risk for occult metastasis. Cancer (Phila.), 75: 844-850, 1995.
31. Tomasino, R. M., Daniele, E., Bazan, V., Morello, V., Tralongo, V.,
Nuara, R., Nagar, C., Salvato, M., Ingria, F., Restico, S., Dardanoni, 0.,Vecchione, A., and Russo, A. Prognostic significance of cell kinetics inlaryngeal squamous cell carcinoma: clinicopathological associations.
Cancer Res., 55: 6103-6108, 1995.
32. Munck-Wikland, E., Edstrdm, S., Jungmark, E., Kuylesteerna, R.,
Lindholm, J., and Auer, 0. Nuclear DNA content, proliferating-cell
nuclear antigen (PCNA), and p53 immunostaining in predicting pro-gression of laryngeal cancer in situ lesions. mt. J. Cancer, 56: 95-99,1994.
33. Shin, D. M., Voravud, N., Ro, J. Y., Lee, J. S., Hong, W. K., and
Hittelman, W. N. Sequential increases in proliferating cell nuclearantigen expression in head and neck tumorigenesis: a potential bio-marker. J. Natl. Cancer Inst., 85: 971-978, 1993.
34. Resnick, J. M.. Uhlman, D., Niehans, 0. A., Gapany. M., Adams.
0., Knapp, D., and Jaszcz, W. Cervical lymph node status and survivalin laryngeal carcinoma: prognostic factors. Ann. Otol. Rhinol. &
Laryngol., 104: 685-694, 1995.
35. Shimoyama, Y., Hirohashi, S., Hirano, S., Noguchi, M., Shimosato,
Y., Takeichi, M., and Abe, 0. Cadherin cell-adhesion molecules inhuman epithelial tissues and carcinomas. Cancer Res., 49: 2128-2133,
1989.
36. Pignatelli, M. E-cadherin: a biological marker of tumour differen-tiation. J. Pathol., 171: 81-82, 1993.
37. Pignatelli, M., Ansari, T. Q., Gunter, P., Liu. D., Shinji, H.,Takeichi, M., Kloppeb, 0., and Lemoine, N. R. Loss of membranousE-cadherin expression in pancreatic cancer: correlation with lymph node
metastasis, high grade, and advanced stage. J. Pathol., 174: 243-248,
1994.
38. Rasbridge, S. A., Gillett, C. E., Sampson, S. A., Walsh, F. S., and
Millis, R. R. Epithelial (E-) and placental (P-) cadherin cell adhesion
molecule expression in breast carcinoma. J. Pathol., 169: 245-250,
1993.
39. Gagliardi, 0., Kandemir, 0., Liu, D., Guida, M., Benvestito, S.,Ruers, T. 0. M., Benjamin, I. S., Northover, J. M. A., Stamp, 0. W. H.,Talbot, I. C., and Pignatelli, M. Changes in E-cadherin immunoreactiv-ity in the adenoma-carcinoma sequence of the large bowel. Virchows
Archiv., 426: 149-154, 1995.
40. Southgate, J., Hutton, K. A. R., Thomas, D. F. M., and
Trejdosiewicz, L. K. Normal human urothelial cells in vitro: prolifera-tion and induction of stratification. Lab. Invest., 71: 583-594, 1994.
41. Revillion, F., Vandewalle, B., Hornez, L., and Lefebvre, J. Influ-
ence of cAMP on E-cadhenn expression and cell surface heparan sulfateproteoglycan synthesis in human breast cancer cells. Anticancer Res.,13: 1625-1630, 1993.
42. Sacchi, T., Bani, D., Brandi, M. L., Falchetti, A., and Bigazzi, M.
Relaxin influences growth, differentiation, and cell-cell adhesion ofhuman breast-cancer cells in culture. mt.j. Cancer, 57: 129-134, 1994.
43. Dolcetti, R., Doglioni, C., Maestro, R., Gasparotto, D., Barzan, L.,
Pastore, A., Romanelli, M., and Boiocchi, M. p53 over-expression is anearly event in the development of human squamous-cell carcinoma ofthe larynx: genetic and prognostic implications. mt. J. Cancer, 52:
178-182, 1992.
44. Anwar, K., Nakakuki, K., Imai, H., Naiki, H., and Inuzuka, M.
Overexpression of p53 protein in human laryngeal carcinoma. Int. J.
Cancer, 53: 952-956, 1993.
45. Nadal, A., Campo, E., Pinto, J., Mallofr#{232}, C., PalacIn, A., Arias, C.,
Traserra, J., and Cardesa, A. p53 expression in normal, dysplastic, and
neoplastic laryngeal epithelium: absence of a correlation with prognostic
factors. J. Pathol., 175: 181-188, 1995.
46. Baatenburg de Jong, R. J., Knegt, P., and Verwoerd, C. D. A.
Reduction of the number of neck treatments in patients with head and
neck cancer. Cancer (Phila.), 71: 2312-2318, 1993.
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1996;2:1801-1808. Clin Cancer Res A Franchi, O Gallo, V Boddi, et al. immunohistochemical determination.role of proliferating cell nuclear antigen, MIB-1, and E-cadherin Prediction of occult neck metastases in laryngeal carcinoma:
Updated version
http://clincancerres.aacrjournals.org/content/2/10/1801
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/2/10/1801To request permission to re-use all or part of this article, use this link
Research. on June 12, 2020. © 1996 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Related Documents