Predicting Negative Mood State and Personal Growth in African American and White Long-Term Breast Cancer Survivors Laura S. Porter, Ph.D. Duke University Medical Center Margaret F. Clayton, R.N., Ph.D., Michael Belyea, Ph.D., Merle Mishel, R.N., Ph.D., Karen M. Gil, Ph.D., and Barbara B. Germino, R.N., Ph.D. University of North Carolina at Chapel Hill ABSTRACT Background: Relatively little research has examined cog- nitive processes that may impact psychological adaptation in older long-term breast cancer survivors (BCS). Purpose: This study investigated the strength of a conceptual model based on the literature and Uncertainty in Illness Theories which pro- poses that negative mood state and personal growth in older long-term White and African American BCS would be predicted by the combined influences of demographic and disease vari- ables, social support, religious participation, and cognitive pro- cesses (uncertainty, catastrophizing, troublesome thoughts, and cognitive reframing). Methods: Baseline data were gathered from 524 BCS (369 Whites and 155 African Americans, 5–9 years postdiagnosis) prior to their participating in an uncer- tainty management intervention program. The conceptual model was tested using structural equation modeling. Results: The multigroup model showed good fit to the data and explained substantial variance in negative mood state and personal growth. Cognitive processes showed both direct and indirect ef- fects on outcomes in the expected directions. Several ethnic dif- ferences were found: African Americans were more negative- ly affected by comorbidities and Whites by symptom distress, whereas cognitive reframing was a stronger predictor of per- sonal growth for African Americans than Whites. Conclusions: This is one of the first studies to explore predictors of both nega- tive mood and personal growth in a multiethnic sample of BCS. These findings suggest that cognitive processes play an im- portant role in psychological adaptation to breast cancer sur- vivorship. These processes are amenable to change, suggesting a logical target for intervention with this population. (Ann Behav Med 2006, 31(3):195–204) INTRODUCTION As of 2002, there were over 2 million breast cancer survi- vors in the United States, making women with breast cancer one of the largest groups of cancer survivors (1). Because the inci- dence of breast cancer increases with age and the 5-year survival rate is so high, long-term breast cancer survivors (BCS) are pre- dominantly women over 60 years of age. Yet there has been sur- prisingly little research on the psychosocial adjustment of older BCS after the initial diagnosis and treatment phases (2), and even less research focused on minority survivors. Although older long-term BCS generally report good quality of life and psychological functioning (3,4), many survivors experience continued symptoms and treatment-induced functional limita- tions (5,6) as well as concerns about recurrence well after being considered “cured” (7,8). Concerns about recurrence are trig- gered by a variety of events including new physical symptoms, medical checkups, and hearing of someone else’s cancer (7,8), and they can result in levels of uncertainty and fear equal to that experienced at the time of diagnosis (9). According to uncertainty in illness theories, experiences that are random, unpredictable, and uncontrollable in nature generate uncertainty (10,11), which in turn is associated with psychological distress (12). For older BCS, the experience of symptoms such as arm stiffness, fatigue, and pain can be a con- siderable source of uncertainty. These symptoms can occur fre- quently yet unpredictably, and women are often unsure how long they will last, how best to manage them, and how to distin- guish between treatment side effects and signs of aging (13). Thus, for older BCS, uncertainty regarding symptoms as well as concerns about recurrence may have a significant negative im- pact on psychological functioning. Conversely, as time since treatment passes, some women learn to reframe the uncertainty of survivorship into an opportu- nity for personal growth (11), reporting benefits or positive out- comes such as an enhanced sense of purpose and improvements in relationships and personal resources (8,14). Recent reviews have noted the need to examine these positive aspects of cancer survivorship quantitatively (15), yet only a few studies have done so. Two recent studies, for example, reported that younger women and African American women perceive higher levels of 195 Dr. Margaret Clayton is now at the University of Utah School of Nursing. Dr. Michael Belyea is now at Arizona State University School of Nursing. This research was in part supported by grants from the National In- stitute of Health, National Cancer Institute 1R01 CA78955-02, M. Mishel, Principal Investigator, and 1RO1 CA107477-01, D. Baucom, Principal Investigator. We thank Chanetta Washington, Project Manager; Susan Campbell and Betsy Clarke, Data Managers; and Guosheng Yin for assistance with data analyses; and all study participants for their time and effort. Reprint Address: L. Porter, Ph.D., Box 90399, Duke University Medi- cal Center, Durham, NC, 27708. E-mail: [email protected]; or M. Mishel, P.O. Box 7460, School of Nursing, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599. E-mail: Mishel@ unc.edu © 2006 by The Society of Behavioral Medicine.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Predicting Negative Mood State and Personal Growth in African Americanand White Long-Term Breast Cancer Survivors
Laura S. Porter, Ph.D.Duke University Medical Center
Margaret F. Clayton, R.N., Ph.D., Michael Belyea, Ph.D., Merle Mishel, R.N., Ph.D., Karen M. Gil, Ph.D.,and Barbara B. Germino, R.N., Ph.D.University of North Carolina at Chapel Hill
ABSTRACT
Background: Relatively little research has examined cog-nitive processes that may impact psychological adaptation inolder long-term breast cancer survivors (BCS). Purpose: Thisstudy investigated the strength of a conceptual model based onthe literature and Uncertainty in Illness Theories which pro-poses that negative mood state and personal growth in olderlong-term White and African American BCS would be predictedby the combined influences of demographic and disease vari-ables, social support, religious participation, and cognitive pro-cesses (uncertainty, catastrophizing, troublesome thoughts, andcognitive reframing). Methods: Baseline data were gatheredfrom 524 BCS (369 Whites and 155 African Americans, 5–9years postdiagnosis) prior to their participating in an uncer-tainty management intervention program. The conceptualmodel was tested using structural equation modeling. Results:The multigroup model showed good fit to the data and explainedsubstantial variance in negative mood state and personalgrowth. Cognitive processes showed both direct and indirect ef-fects on outcomes in the expected directions. Several ethnic dif-ferences were found: African Americans were more negative-ly affected by comorbidities and Whites by symptom distress,whereas cognitive reframing was a stronger predictor of per-sonal growth for African Americans than Whites. Conclusions:This is one of the first studies to explore predictors of both nega-tive mood and personal growth in a multiethnic sample of BCS.These findings suggest that cognitive processes play an im-portant role in psychological adaptation to breast cancer sur-
vivorship. These processes are amenable to change, suggestinga logical target for intervention with this population.
(Ann Behav Med 2006, 31(3):195–204)
INTRODUCTION
As of 2002, there were over 2 million breast cancer survi-vors in the United States, making women with breast cancer oneof the largest groups of cancer survivors (1). Because the inci-dence of breast cancer increases with age and the 5-year survivalrate is so high, long-term breast cancer survivors (BCS) are pre-dominantly women over 60 years of age. Yet there has been sur-prisingly little research on the psychosocial adjustment of olderBCS after the initial diagnosis and treatment phases (2), andeven less research focused on minority survivors. Althougholder long-term BCS generally report good quality of life andpsychological functioning (3,4), many survivors experiencecontinued symptoms and treatment-induced functional limita-tions (5,6) as well as concerns about recurrence well after beingconsidered “cured” (7,8). Concerns about recurrence are trig-gered by a variety of events including new physical symptoms,medical checkups, and hearing of someone else’s cancer (7,8),and they can result in levels of uncertainty and fear equal to thatexperienced at the time of diagnosis (9).
According to uncertainty in illness theories, experiencesthat are random, unpredictable, and uncontrollable in naturegenerate uncertainty (10,11), which in turn is associated withpsychological distress (12). For older BCS, the experience ofsymptoms such as arm stiffness, fatigue, and pain can be a con-siderable source of uncertainty. These symptoms can occur fre-quently yet unpredictably, and women are often unsure howlong they will last, how best to manage them, and how to distin-guish between treatment side effects and signs of aging (13).Thus, for older BCS, uncertainty regarding symptoms as well asconcerns about recurrence may have a significant negative im-pact on psychological functioning.
Conversely, as time since treatment passes, some womenlearn to reframe the uncertainty of survivorship into an opportu-nity for personal growth (11), reporting benefits or positive out-comes such as an enhanced sense of purpose and improvementsin relationships and personal resources (8,14). Recent reviewshave noted the need to examine these positive aspects of cancersurvivorship quantitatively (15), yet only a few studies havedone so. Two recent studies, for example, reported that youngerwomen and African American women perceive higher levels of
195
Dr. Margaret Clayton is now at the University of Utah School ofNursing. Dr. Michael Belyea is now at Arizona State University Schoolof Nursing.
This research was in part supported by grants from the National In-stitute of Health, National Cancer Institute 1R01 CA78955-02, M.Mishel, Principal Investigator, and 1RO1 CA107477-01, D. Baucom,Principal Investigator.
We thank Chanetta Washington, Project Manager; Susan Campbell andBetsy Clarke, Data Managers; and Guosheng Yin for assistance withdata analyses; and all study participants for their time and effort.
Reprint Address: L. Porter, Ph.D., Box 90399, Duke University Medi-cal Center, Durham, NC, 27708. E-mail: [email protected]; orM. Mishel, P.O. Box 7460, School of Nursing, University of NorthCarolina at Chapel Hill, Chapel Hill, NC 27599. E-mail: [email protected]
© 2006 by The Society of Behavioral Medicine.

positive meaning as a result of breast cancer (5,8). However,there has been little empirical study of personal growth inlong-term cancer survivors.
This study tested the strength of a conceptual model ex-plaining negative mood state and personal growth in a sample ofolder long-term White and African American BCS. The modelwas drawn from the uncertainty in illness theories (10,11) aswell as prior research on BCS pointing to the importance of dis-ease and demographic variables, social or contextual factors,and cognitive processes—such as uncertainty, catastrophizing,troublesome thoughts, and cognitive reframing—in overall ad-aptation to survivorship.
Demographic and Disease Factors
Age may potentially impact the psychological adjustmentof BCS. Although younger BCS report more psychological dif-ficulties (4,16), older BCS often have multiple other healthproblems that contribute to greater burden and uncertainty (17).Among long-term BCS, advanced age is associated with morecomorbidities and limitations in activities (3), which in turn pre-dict psychological distress (18). For older women in particular,enduring symptoms from treatment and declines in physicalfunction can affect activities of daily living and women’s abilityto live independently (2,16).
Social Context
Breast cancer patients who perceive more social supporttend to have less uncertainty, lower levels of psychological dis-tress, and enhanced role functioning (19,20). Social supportalso functions to provide meaning to illness-related events andto help cancer patients manage uncertainty (21). One compo-nent of the social context that may be particularly importantamong older women is religious participation, which has beenfound to shield women from psychological distress (20) anduncertainty (22).
Cognitive Processes
For BCS faced with frequent and repeated experiences thattrigger thoughts of cancer recurrence, negative cognitive pro-cesses, including uncertainty, catastrophic thinking, and trou-blesome thoughts about recurrence, are likely to result in higherlevels of negative mood state. Uncertainty has been linked withpsychological distress and symptom distress among cancersurvivors (12). Catastrophic thinking (ruminating on negativethoughts, believing the worst may happen, and feelings of help-lessness) has been consistently linked to poorer outcomes in-cluding depression, increased pain, and poorer adjustment to ill-ness (23,24). Conversely, cognitive reframing (the ability toreinterpret problems as manageable and as sources of opportu-nity rather than threat) may lead to more positive mood statesand the potential for personal growth (11,25). Understandingthe role of cognitive strategies in the psychological adaptationof BCS is important given that these processes are amenableto change (e.g., 26,27) and are thus potential targets of psy-chosocial interventions.
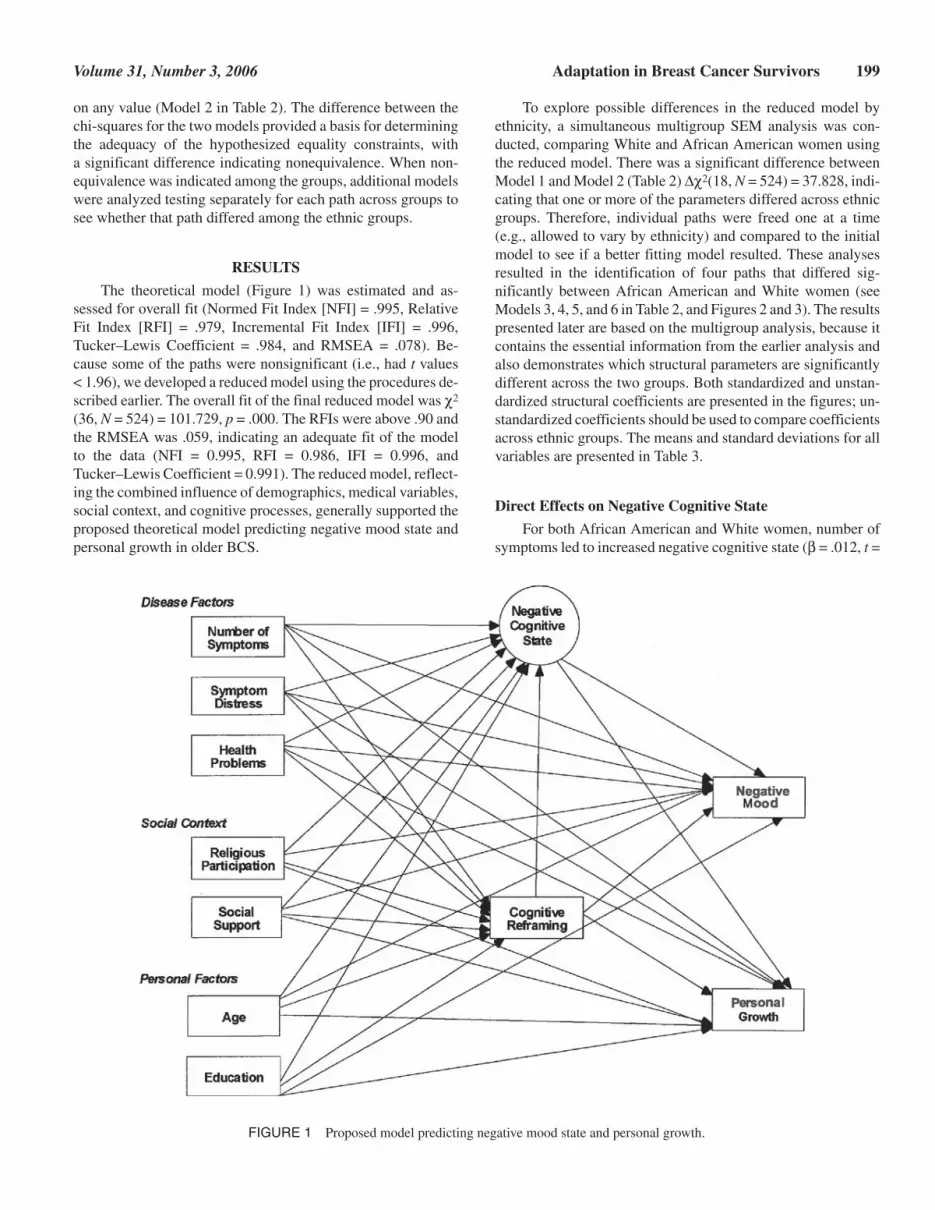
Thus, in this study, we adapted and tested a conceptualmodel of psychological adaptation in long-term BCS based onthe Uncertainty in Illness Theories that integrated the aforemen-tioned findings (10,11; see Figure 1). We hypothesized that neg-ative cognitive processes would be associated with higher levelsof negative mood and less personal growth, whereas cognitivereframing would be associated with better adjustment. We alsohypothesized that the cognitive variables would partially medi-ate the effects of disease, demographic, and social context vari-ables on adjustment. We tested this model using structural equa-tion modeling (SEM), a comprehensive approach to testinghypotheses about relations among observed (or manifest) andlatent (or unmeasured) variables. A major strength of SEM is itsability to deal with intervening or mediating variables, which al-lows for the statistical testing of the cognitive variables. Unliketraditional regression procedures (e.g., 28), SEM tests all rela-tionships simultaneously and gives an overall test of model fit.
A second aim of this study was to examine differences be-tween African American women and White women in predic-tors of adjustment. Although ethnicity influences numerous fac-tors that have been linked to adjustment in cancer survivors,including socioeconomic variables (e.g., income, education),cultural factors (e.g., religiosity, social support), and otherhealth problems (29,30), the potential role of ethnicity in psy-chological processes in cancer survivorship has been understud-ied (31). Thus, we tested the model shown in Figure 1 for ethnicdifferences in each of the paths to elucidate how patterns of as-sociation between the variables may be influenced by ethnicity.
METHOD
Participants
This study reports on baseline data of 524 women (369White women and 155 African American women) enrolled in alarger program of research evaluating an uncertainty manage-ment intervention for long-term BCS (32). Table 1 reports thedemographic and medical information of the participants byethnic group. There were significant ethnic differences for levelof education with White women having a higher level, t(522) =5.14, p < .001; for marital status with White women more likelyto be married, t(522) = –4.01, p < .001; and for months from di-agnosis with African American women significantly fartherfrom diagnosis than White women, t(517) = –2.82, p < .01.
Procedure
The entry criteria for the larger study included (a) age 50years or older, (b) 5 to 9 years post breast cancer diagnosis, (c)no other cancers or breast cancer recurrence, (d) African Ameri-can or White, (e) English speaking, and (f) access to a telephoneand willingness to be randomized to a psychoeducational inter-vention. Women were excluded if they scored 13 or lower on theshort form (33) of the Mini-Mental Status Examination (34).
Potential participants were identified using the tumor regis-tries associated with participating health care institutions inNorth Carolina. The tumor registries identified women whomay be eligible for the study and sent them introductory lettersasking for permission to release their contact information to the
196 Porter et al. Annals of Behavioral Medicine

research team. A trained recruiter then called those women whoagreed to be contacted to explain the study, answer questions,evaluate inclusion criteria, assess willingness to participate, andobtain permission for data collectors to set up an initial homevisit. Informed consent was obtained at the first home visit, andbaseline questionnaires were administered prior to randomiza-tion and the start of the intervention.
There were 1,055 eligible women contacted as potentialparticipants. Of these, 575, or 55%, agreed to participate Wom-en who chose not to participate cited lack of interest (50%), notenough time (26%), other health problems (10%), not wantingto be reminded of their breast cancer experience (5%), other rea-sons (3%), or no reason (6%). Fifty-three women were lost tocontact between recruitment and baseline or did not finish base-line assessments, resulting in 524 women who provided com-plete baseline data. This participation rate is comparable toother studies using cancer registries for recruitment, where ratesof 48% and 32% have been reported (35,36).
Measures
Number of symptoms and symptom distress were measuredby a modified version of the Symptom Distress Scale (37,38).The original scale was modified by the addition of some com-mon long-term side effects of breast cancer treatment. The re-vised version had 15 items and retained the format of the origi-nal scale with patients indicating whether they experienced eachsymptom, and for endorsed symptoms rating their degree ofsymptom distress on a scale from 1 (none) to 4 (a great deal).Symptom number was scored by summing the number of itemsendorsed, and symptom distress was scored as the sum of dis-
tress ratings divided by the number of items endorsed. Alphacoefficients for symptom number were .89 for African Ameri-cans and .88 for Whites; alpha coefficients for symptom distresswere .90 for African Americans and .89 for Whites. The mostcommon symptoms reported by women in this sample werenumbness in the treatment area (63%), fatigue (53%), skin ten-derness and sensitivity (44%), and weight gain since treatment(41%). A substantial number of women (> 25%) also reportedsymptoms of arm weakness, stiffness in the arm and shoulder,pain, arm and hand swelling, trouble thinking, and change inappearance.
Health problems were measured by the Co-Morbidity In-dex, a list of 25 conditions adapted by Satariano, Ragheb, andDupuis (39) from those used by the Human Population Labora-tory in the Alameda County (CA) Survey. A sum of the numberof conditions was tallied. This self-report health assessment hasbeen found to be both reliable and valid in several studies (38).The most common health problems reported by the women inthis sample were arthritis or rheumatism (59%), high or lowblood pressure (48%), other diagnosed health problems (31%),constipation and bowel problems (27%), and cataracts and eyeproblems (26%).
Social support satisfaction was measured by the six-itemSatisfaction subscale of the short form of the Social SupportQuestionnaire (40). Cronbach’s alphas were .90 for Whites and.89 for African Americans.
Religious participation was measured by the 11-item Par-ticipation in Religious Activities Scale which indexes the fre-quency of participation in religion-oriented social activities(41). Alpha coefficients were .92 for Whites and .88 for AfricanAmericans.
Volume 31, Number 3, 2006 Adaptation in Breast Cancer Survivors 197
TABLE 1Participant Characteristics
Whitea African Americanb Total Samplec
Mean age (SD) 64.4 (8.6) 65.0 (9.5) 64.5 (8.9)Mean years education (SD)d 14.06 (2.7) 12.7 (3.1) 13.6 (2.9)% married or partneredd,e 64 44 58Employment status (%)
Retired 42 41 42Working 31 28 30Homemaker 12 6 10
Mean months since diagnosis (SD)d,f 79.8 (12.9) 83.6 (16.2) 81.0 (14.0)Treatment (%)
Mastectomy 79.6 76.5 78.7Lumpectomy 18.7 22.8 19.9Chemotherapy 22 21.3 23Radiation 29.3 21.9 27Adjuvant hormonal 28.7 27.7 28
Stage at diagnosisg (%)0 6.3 9.0 7.11 55.9 53.1 55.52 30.4 28.3 29.23 7.4 9.7 8.2
an = 369. bn = 155. cN = 524. dSignificant differences between White and African American participants (see text for details). eInformation available for 490participants. fInformation available for 519 participants. gInformation available for 510 participants.

Negative Cognitive State, a latent variable, was constructedfrom the manifest variables of uncertainty, troublesomethoughts, and catastrophizing. Uncertainty was measured usingthe 22-item Mishel Uncertainty in Illness Scale–Survivor Ver-sion (MUIS–S). For the Survivor version used in this study,items relevant to the survival experience were selected from thecore Mishel Uncertainty in Illness scale and revised (10). Alphacoefficients on the MUIS–S were .78 for African Americans and.84 for Whites. Troublesome thoughts were measured with a13-item modified version of the Inventory of Negative Thoughtsin Response to Pain (INTRP) (42). The original scale consists ofa list of troublesome thoughts that are often reported in responseto pain. For this study, the stem and the wording of the itemswere modified to assess troublesome thoughts about possible re-currence. Alphas were .87 for African Americans and .85 forWhites. Catastrophizing was measured using a six-item modi-fied version of the Catastrophizing subscale of the CognitiveCoping Strategies Questionnaire (CSQ) (43). Items from theoriginal version of the instrument were modified in minor waysto better fit them to the revised stem, “when I feel anxiety or dis-tress about the possibility of my breast cancer coming back.”Cronbach’s alphas were .71 for African Americans and .74 forWhites.
Cognitive reframing, defined as the ability to address con-cerns from a positive point of view, was measured using the10-item Cognitive-Reframing subscale of the Self ControlSchedule (44). Cronbach’s alphas were .86 for Whites and .84for African Americans.
Negative mood state was measured using the total mooddisturbance score of the 37-item Profile of Mood States–ShortForm (POMS–SF) (45). Cronbach’s alphas were .95 for Whitesand .94 for African Americans.
Personal growth was measured using the 39-item GrowthThrough Uncertainty Scale (GTUS) (46). The GTUS measureswhether a new view of life has been constructed as a result of se-rious illness. Alpha coefficients were .95 for both Whites andAfrican Americans.
Statistical Analyses
SEM was used to test proposed linkages between variables.SEM has increasingly been used in behavioral oncology re-
search to look at mediational factors and multiple outcomes(47). Its use here is to evaluate theoretical predictions of nega-tive mood state and personal growth and potential ethnic differ-ences in these predictions.
AMOS software was used to calculate maximum likelihoodestimators for the model parameters using the covariance matri-ces for the total sample, and White and African American sam-ples. Multiple measures were used to assess the fit of data to themodel including R2, the root mean square error of approxima-tion (RMSEA), Bollen’s non-normed fit index (NNFI), andBentler’s comparative fit index (CFI); the chi-square test wasnot used for model evaluation due to its sensitivity to samplesize (48). An adequate fit of the data to the model is indicated bya RMSEA value between .05 and .08, and the NNFI and CFIabove 0.90 (48,49). If these criteria were not met, or if the abso-lute values of the t statistics for the path coefficient were lessthan 1.96, the Wald test and Lagrange Multipler test were usedto develop a better fitting model. Any modification was exam-ined for theoretical meaningfulness before proceeding.1
Once we obtained a model with adequate fit, we testedwhether it was equivalent across ethnic groups by applying amultigroup SEM model that models data from multiple groupssimultaneously. A series of nested models that differed in thenumber of cross-group equality constraints were tested. Thefirst model (Model 1 in Table 2) was constrained such that allpaths between the exogenous variables and endogenous vari-ables and all paths between the endogenous variables wereequal across the groups. This model was compared with a lessrestrictive model in which the same parameters were free to take
198 Porter et al. Annals of Behavioral Medicine
1Prior to model testing, data were evaluated for normality and out-liers. There were two variables that were nonnormal: social support andcatastrophizing. When we reran the models with asymptomatically dis-tribution free (ADF) estimators that are designed for nonnormal data,there was only one difference: The path between symptom distress andnegative cognitive state for African Americans went from being mar-ginally significant (.056) to being significant. However, given that ADFrequires a very large sample size, we felt that the original maximumlikelihood estimators were the most appropriate. In addition, there werea few outliers that had unusually large Mahalanobis d squared values.When these subjects were omitted from the analysis, the same resultswere obtained.
TABLE 2Model Fit Statistics for Simultaneous Multigroup Analysis Comparing African American and White Women
df χ2 Change df Change χ2 p(d) NFI RFI IFI TLC RMSEA
Model 1: All parameters fixed 90 171.636 .991 .982 .996 .991 .042Model 2: All parameters freed 72 133.808 18 38.75 .993 .982 .997 .992 .041Model 3: Health problems to negative mood state 89 166.052 1 5.584 0.018 .991 .982 .996 .992 .041Model 4: Symptom distress to negative
cognitive state88 159.859 1 6.193 0.012 .992 .982 .996 .992 .040
Model 5: Cognitive reframing to negativecognitive state
87 155.782 1 4.077 0.043 .992 .983 .996 .992 .039
Model 6: Cognitive reframing to personal growth 86 147.308 1 8.474 0.003 .992 .983 .997 .993 .037
Note. NFI = normed fit index; RFI = relative fit index; IFI = incremental fit index; TLC = Tucker–Lewis coefficient; RMSEA = root mean square error ofapproximation; p(d) = probability of the difference. All models were compared to the previous model.
on any value (Model 2 in Table 2). The difference between thechi-squares for the two models provided a basis for determiningthe adequacy of the hypothesized equality constraints, witha significant difference indicating nonequivalence. When non-equivalence was indicated among the groups, additional modelswere analyzed testing separately for each path across groups tosee whether that path differed among the ethnic groups.
RESULTS
The theoretical model (Figure 1) was estimated and as-sessed for overall fit (Normed Fit Index [NFI] = .995, RelativeFit Index [RFI] = .979, Incremental Fit Index [IFI] = .996,Tucker–Lewis Coefficient = .984, and RMSEA = .078). Be-cause some of the paths were nonsignificant (i.e., had t values< 1.96), we developed a reduced model using the procedures de-scribed earlier. The overall fit of the final reduced model was χ2
(36, N = 524) = 101.729, p = .000. The RFIs were above .90 andthe RMSEA was .059, indicating an adequate fit of the modelto the data (NFI = 0.995, RFI = 0.986, IFI = 0.996, andTucker–Lewis Coefficient = 0.991). The reduced model, reflect-ing the combined influence of demographics, medical variables,social context, and cognitive processes, generally supported theproposed theoretical model predicting negative mood state andpersonal growth in older BCS.
To explore possible differences in the reduced model byethnicity, a simultaneous multigroup SEM analysis was con-ducted, comparing White and African American women usingthe reduced model. There was a significant difference betweenModel 1 and Model 2 (Table 2) ∆χ2(18, N = 524) = 37.828, indi-cating that one or more of the parameters differed across ethnicgroups. Therefore, individual paths were freed one at a time(e.g., allowed to vary by ethnicity) and compared to the initialmodel to see if a better fitting model resulted. These analysesresulted in the identification of four paths that differed sig-nificantly between African American and White women (seeModels 3, 4, 5, and 6 in Table 2, and Figures 2 and 3). The resultspresented later are based on the multigroup analysis, because itcontains the essential information from the earlier analysis andalso demonstrates which structural parameters are significantlydifferent across the two groups. Both standardized and unstan-dardized structural coefficients are presented in the figures; un-standardized coefficients should be used to compare coefficientsacross ethnic groups. The means and standard deviations for allvariables are presented in Table 3.
Direct Effects on Negative Cognitive State
For both African American and White women, number ofsymptoms led to increased negative cognitive state (β = .012, t =
Volume 31, Number 3, 2006 Adaptation in Breast Cancer Survivors 199
FIGURE 1 Proposed model predicting negative mood state and personal growth.

2.048), whereas satisfaction with social support led to decreasednegative cognitive state (β = –.112, t = –3.950). For Whitewomen only, symptom distress (β = .213, t = 4.757) led to in-creased negative cognitive state, whereas cognitive reframing (β= –.032, t = –2.519) led to a less negative cognitive state. Thus,women with more symptoms and less satisfaction with their so-cial support reported more uncertainty, troublesome thoughts,and catastrophizing. White women who had more symptom dis-tress and used less cognitive reframing reported higher levels ofthese negative cognitive processes.
Direct Effects on Cognitive Reframing
Cognitive reframing is the ability to positively address con-cerns. For both White and African American women, religiousparticipation directly strengthened cognitive reframing (β =.452, t = 6.305), as did satisfaction with social support (β = .339,t = 2.990).
Direct and Indirect Effectson Negative Mood State
For both African American and White women, as symptomdistress (β = .145, t = 3.570) and negative cognitive state (β= .623, t = 5.616) increased, women reported more negativemood state. However, as religious participation (β = –.028, t =–1.091), cognitive reframing (β = –.037, t = –2.487), and satis-faction with social support (β = –.087, t = –2.041) increased,women reported less negative mood state. For African Ameri-can women only, more health problems also led to more nega-tive mood state (β = .052, t = 4.712).
As hypothesized, social support satisfaction, number ofsymptoms, symptom distress, and religious participation had in-direct effects on negative mood state through their relationshipswith either cognitive reframing or negative cognitive state (seeFigures 2 and 3). For White women, cognitive reframing alsohad an indirect effect on negative mood state via its relationshipwith negative cognitive state (see Figure 3).
200 Porter et al. Annals of Behavioral Medicine
FIGURE 2 Reduced model predicting negative mood state and personal growth in African American women. Unstandardized coefficients are pre-sented at the left of the line or above the line and standardized coefficients are presented to the right or below the line in parentheses. Bold paths differbetween African American and White women. All paths shown are statistically significant unless indicated otherwise.

201
TABLE 3Means and Standard Deviations for Variables Included in the Model
White African American Total Sample
M SD M SD M SD
Number of symptoms 5.18 3.84 5.27 4.19 5.21 3.95Symptom distress .53 .61 .543 .660 .53 .622Health problems 3.73 2.53 4.25 2.74 3.89 2.60Social support satisfaction 5.67 .60 5.89 .308 5.73 0.540Religious participation 3.64 0.91 3.64 .607 3.82 0.878Uncertainty 2.58 .50 2.62 .461 2.59 0.491Troublesome thoughts 1.82 .59 1.63 .611 1.77 0.603Catastrophizing .34 .63 .401 .738 0.37 0.663Cognitive reframing 7.61 1.46 8.42 1.22 7.86 1.44Negative mood state 0.98 0.58 .752 .453 0.91 0.554Personal growth 4.42 0.65 4.56 .672 4.46 0.661
FIGURE 3 Reduced model predicting negative mood state and personal growth in White women. Unstandardized coefficients are presented at theleft of the line or above the line and standardized coefficients are presented to the right or below the line in parentheses. Bold paths differ between Afri-can American and White women. All paths shown are statistically significant unless indicated otherwise.

Direct and Indirect Effects on Personal Growth
For both African American and White women, more symp-toms (β = .023, t = 2.981), greater religious participation (β =.184, t = 5.761), higher levels of education (β = .032, t = 3.514),and younger age (β = –.013, t = –4.329) were directly associatedwith higher levels of personal growth. Cognitive reframing wasalso highly significant in explaining personal growth for bothAfrican American and White women. However, there were sig-nificant ethnic differences in the magnitude of the effect with alarger effect among African American women (β = .219, t =4.221) than White women (β = .093, t = 5.898). In addition, cog-nitive reframing mediated the effects of social support and par-tially mediated the effects of religious participation on personalgrowth.
For both African American and White women, negativecognitive state (β = –.525, t = –2.487) was directly associatedwith less personal growth. Negative cognitive state also medi-ated the effects of symptom distress and social support satisfac-tion on personal growth.
DISCUSSION
This is one of the first studies to examine predictors of bothnegative mood and personal growth in a sample of older Whiteand African American long-term BCS. Of importance, the sam-ple included enough African American women to enable mean-ingful analyses of ethnic differences. In addition, participants inthis study were an average of 65 years old; thus the findingsfrom this study contribute to the literature on adjustment ofolder women who make up the majority of BCS. Overall, the re-sults supported the theoretical model which proposed that cog-nitive process variables would be important predictors of adjust-ment and would partially mediate the effects of demographic,disease, and social context factors on adjustment. Consistentwith other studies (31,50), there were several ethnic differencesin the patterns of results, suggesting that although BCS of differ-ent ethnic groups are similar in their overall levels of adjust-ment, there are also meaningful differences between groups thatwould preclude generalization from studies with homogeneoussamples.
Both cognitive reframing and negative cognitive state weresignificant predictors of adjustment. Negative cognitive state,which consisted of uncertainty, catastrophizing, and trouble-some thoughts of recurrence, accounted for the highest amountof variance in the model, explaining 35% of the variance in neg-ative mood state and 25% of the variance in personal growth forboth White and African American women. These findings areconsistent with uncertainty theories and with previous studies ofpatients with a variety of chronic and acute illnesses. For in-stance, uncertainty has been associated with psychological dis-tress among patients receiving treatment for cancer (23) andwith increased symptom distress in BCS (12). Among patientswith chronic pain conditions, catastrophizing and troublesomethoughts are strongly predictive of increased levels of painand psychological distress and decreased levels of functioning(23,42). However, to our knowledge, this is the first study to ex-amine catastrophizing and troublesome thoughts as a negative
appraisal of uncertainty in a sample of long-term BCS. The find-ings from this study underline the importance of understandinghow women respond to the specific and unique sources of emo-tional distress for BCS rather than how they cope with stress ingeneral.
Cognitive reframing, defined as the tendency to addressconcerns from a positive point of view, was also a significantpredictor of adjustment, accounting for 12% of the variance innegative mood state in all women, 21% of the variance in per-sonal growth for White women, and 40% of the variance in per-sonal growth for African American women. These findings sup-port the theoretical model described by Mishel (11), in whichcognitive reappraisal is used to reinterpret uncertain situationsas manageable rather than catastrophic, enabling the individualto gain control over emotional distress and perceive new oppor-tunities. Several prior studies have also found evidence of theimportance of cognitive appraisals in women with breast cancer.For instance, stress appraisals have been found to mediate the ef-fects of stress and symptom distress on quality of life (51), andpositive reappraisals have been associated with psychologicalgrowth (52).
Taken together, these findings suggest that cognitive pro-cesses may be quite important in understanding how long-termBCS from different ethnic groups adapt psychologically in theyears following treatment. Of importance, these processes aremodifiable and can be targeted with proven intervention strate-gies such as cognitive–behavioral coping skills (27) and stressmanagement training (26). Consistent with uncertainty theoriesand the literature on older BCS, the findings also support therole of social context and disease factors in both negative andpositive cognitive processes: Negative cognitive state was influ-enced by number of symptoms, symptom distress, and socialsupport satisfaction, whereas cognitive reframing was affectedby religious participation and social support satisfaction. Futurestudies could examine whether health care interventions aimedat more effective symptom management as well as psychosocialinterventions supporting religious and social involvement resultin more adaptive cognitive processes.
In addition, findings from this study indicated some aspectsof survivorship that may be uniquely important for women fromdifferent racial groups. For instance, among African Americanwomen only, those with more health problems also reportedmore negative mood state. This may reflect the increased burdenof health problems experienced by African American women,compounded by the difficulties they often report in dealing withthe health care system (53). Attention to comorbid conditions byhealth care providers, and referral for treatment of these condi-tions, may be helpful in reducing negative mood state for Afri-can American BCS. In contrast, among White women only, highlevels of symptom distress predicted a more negative cognitivestate. It is interesting that there were no ethnic differences in theeffects of religious participation or social support, areas thatare commonly identified as being of particular importance toAfrican American cancer survivors (54). However, the strongimpact of cognitive reframing on personal growth among Afri-can American women supports prior findings on the ability of
202 Porter et al. Annals of Behavioral Medicine
these women to find meaning in life as a result of having breastcancer (8,31,55). In general, findings from this and previousstudies suggest the importance of developing and implementinginterventions for breast cancer patients and survivors that aresensitive to factors influenced by ethnicity, including both so-cioeconomic and cultural issues.
This study has several limitations. First, the study designwas cross-sectional, and thus it is not possible to draw firm con-clusions regarding the direction of causality, for example,whether negative cognitive processes lead to more negativemood state or vice versa. However, the results of the SEM analy-sis indicated that the data were consistent with the proposed the-oretical model which specified the direction of causality be-tween variables. Additional studies confirming this model withother samples of BCS, as well as longitudinal studies assessingthese variables over time, would enable one to make more defin-itive statements regarding the causal relationships between vari-ables. In addition, the final reduced models that were presentedwere revised from those originally proposed based on the data;these models should be validated in independent samples. Fu-ture studies would also benefit from presenting all of the mea-sured variables in the model as latent variables and measuringeach with at least three indicators to take full advantage of SEMmethodology. Finally, all the study participants were from thesoutheastern region of the United States. This may have led tomore homogeneity between the African American and Whitewomen in the sample and may limit the generalizability of theresults concerning variables such as religiosity, which tend todiffer by geographic region.
Others have noted the importance of identifying cancer sur-vivors who are at risk for poor adjustment to target interventionsto their specific needs. The results of this study point to impor-tant modifiable variables that can be targeted with proven inter-vention strategies. Interventions targeted at reducing negativecognitive processes such as uncertainty, catastrophizing, andtroublesome thoughts, and increasing positive cognitive copingstrategies such as cognitive reframing, may lessen the psycho-logical distress of cancer survivors and increase their capacityfor personal growth in response to this life-changing event.
REFERENCES(1) Ries LAG, Eisner MP, Kosary CL, et al. (eds): SEER Cancer
Statistics Review, 1975–2002. Retrieved October 22, 2004 fromhttp://seer.cancer.gov/csr/1975_2002
(2) Mandelblatt J, Figueiredo M, Cullen J: Outcomes and quality oflife following breast cancer treatment in older women: When,why, how much, and what do women want? Health and Qualityof Life Outcomes. 2003, 1:45.
(3) Ganz PA, Desmond KA, Leedham B, et al.: Quality of lifein long-term, disease-free survivors of breast cancer: A fol-low-up study. Journal of the National Cancer Institute. 2002,94:39–49.
(4) Kroenke CH, Rosner B, Chen WY, et al.: Functional impact ofbreast cancer by age of diagnosis. Journal of Clinical Oncology.2004, 22:1849–1856.
(5) Tomich VS, Helgeson HL: Surviving cancer: A comparisonof 5-year disease-free breast cancer survivors with healthywomen. Psycho-Oncology. 2005, 14:307–317.
(6) Deimling GT, Kahana B, Bowman KF, Schaefer ML: Cancersurvivorship and psychological distress in later life. Psy-cho-Oncology. 2002, 11:479–494.
(7) Gil KM, Mishel MH, Belyea M, et al.: Triggers of uncertaintyabout recurrence and treatment side effects in long term olderbreast cancer survivors. Oncology Nursing Forum. 2004,31:1–7.
(8) Bower JE, Meyerowitz BE, Desmond KA, et al.: Percep-tions of positive meaning and vulnerability following breastcancer: Predictors and outcomes among long-term breastcancer survivors. Annals of Behavioral Medicine. 2005,29:236–245.
(9) Nelson JP: Struggling to gain meaning: Living with the uncer-tainty of breast cancer. Advances in Nursing Science. 1996,18:59–76.
(10) Mishel MH: Uncertainty in illness. Image: Journal of NursingScholarship. 1988, 20:225–232.
(11) Mishel MH: Reconceptualization of the uncertainty in ill-ness theory. Image: Journal of Nursing Scholarship. 1990,22:256–262.
(12) Mast ME: Survivors of breast cancer: Illness uncertainty, posi-tive reappraisal, and emotional distress. Oncology Nursing Fo-rum. 1998, 25:555–562.
(13) Baum A, Friedman AL, Zakowski SG: Stress and genetic test-ing for disease risk. Health Psychology. 1997, 16:8–19.
(14) Thornton A: Perceiving benefits in the cancer experience.Journal of Clinical Psychology in Medical Settings. 2002,9:153–165.
(15) Bloom JR: Surviving or thriving? Psycho-Oncology. 2002,11:89–99.
(16) Wenzel LB, Fairclough DL, Brady MJ, et al.: Age-related dif-ferences in the quality of life of breast carcinoma patients aftertreatment. Cancer. 1999, 86:1768–1774.
(17) Sammarco A: Psychosocial stages and quality of life of womenwith breast cancer. Cancer Nursing. 2001, 24:272–277.
(18) Bleiker EMA, Pouwer F, van der Ploeg HM, Leer JH, Ader HJ:Psychological distress two years after diagnosis of breast can-cer: Frequency and prediction. Patient Education and Coun-seling. 2000, 40:209–217.
(19) Maly RC, Umezawa Y, Leake B, Silliman RA: Mental healthoutcomes in older women with breast cancer: Impact of per-ceived family support and adjustment. Psycho-Oncology. 2005,14:535–545.
(20) Silliman RA, Dukes KA, Sullivan LM, Kaplan SH: Breastcancer care in older women: Sources of information, socialsupport, and emotional health outcomes. Cancer. 1998,83:706–711.
(21) Mishel MH, Braden CJ: Uncertainty: A mediator between sup-port and adjustment. Western Journal of Nursing Research.1987, 9:43–57.
(22) Mishel M, Belyea M, Germino B, et al.: Helping patients withlocalized prostate cancer manage uncertainty and treatmentside effects: Nurse delivered psycho-educational interventionvia telephone. Cancer. 2002, 94:1854–1866.
(23) Gaston–Johansson F, Ohly KV, Fall–Dickson JM, NandaJP, Kennedy MJ: Pain, psychological distress, health stat-us, and coping in patients with breast cancer scheduledfor autotransplantation. Oncology Nursing Forum. 1999,26:1337–1345.
(24) Sullivan MJL, Thorn B, Haythornthwaite JA, et al.: Theoreticalperspectives on the relation between catastrophizing and pain.Clinical Journal of Pain. 2001, 17:52–64.
Volume 31, Number 3, 2006 Adaptation in Breast Cancer Survivors 203

(25) Lazarus RS, Folkman S: Stress, Appraisal, and Coping. NewYork: Springer, 1984.
(26) Antoni MH, Lehman JM, Klibourn KM, et al.: Cognitive–Be-havioral stress management intervention decreases the preva-lence of depression and enhances benefit among women undertreatment for early-stage breast cancer. Health Psychology.2001, 20:20–32.
(27) Gil KM, Wilson JJ, Edens JL, et al.: Effects of cognitive copingskills training on coping strategies and experimental pain sen-sitivity in African American adults with sickle cell disease.Health Psychology. 1996, 15:3–10.
(28) Baron RM, Kenny DA: The moderator–mediator variable dis-tinction in social psychological research: Conceptual, strategic,and statistical considerations. Journal of Personality and SocialPsychology. 1986, 151:1173–1182.
(29) Ashing–Giwa KT, Padilla GV, Tejero JS, Kim J: Breast cancersurvivorship in a multiethnic sample: Challenges in recruitmentand measurement. Cancer. 2004, 101:450–465.
(30) Giedzinski AS, Meyerowitz BE, Ganz PA, Rowland JH:Health-related quality of life in a multiethnic sample of breastcancer survivors. Annals of Behavioral Medicine. 2004,28:39–51.
(31) Meyerowitz BE, Richardson J, Hudson S, Leedham B: Ethnic-ity and cancer outcomes: Behavioral and psychosocial consid-erations. Psychological Bulletin. 1998, 123:47–70.
(32) Mishel M, Germino B, Gil K, et al.: Benefits from an uncer-tainty management intervention for older long-term breast can-cer. Psycho-oncology (in press, 2005).
(33) Koenig HG: An abbreviated Mini-Mental State Examinationfor medically ill older adults. Journal of the American Geriat-rics Society. 1996, 44:215–216.
(34) Folstein MF, Folstein SE, McHugh PR: Mini-Mental State:A practical method for grading the cognitive state of patientsfor the clinician. Journal of Psychiatric Research. 1975,12:189–198.
(35) Boon H, Stewart M, Kennard MA, et al.: Use of complemen-tary/alternative medicine by breast cancer survivors in Ontario:Prevalence and perceptions. Journal of Clinical Oncology.2000, 18:2515–2521.
(36) Morris KT, Johnson N, Homer L, Walts D: A comparison ofcomplementary therapy use between breast cancer patients andother primary tumor sites. The American Journal of Surgery.2000, 179:407–411.
(37) McCorkle R, Young K: Development of a symptom distressscale. Cancer Nursing.1978, 1:373–378.
(38) McCorkle R, Quint–Benoliel J: Symptom distress, current con-cerns and mood disturbance after diagnosis of life-threateningdisease. Social Science and Medicine. 1983, 17:431–438.
(39) Satariano WA, Ragheb NE, Dupuis MH: Comorbidity in olderwomen with breast cancer: An epidemiologic approach. InYancik R, Yates J (eds), Cancer in the Elderly: Approaches to
Early Detection and Treatment. New York: Springer, 1989,71–107.
(40) Sarason IG, Levine HM, Basham RB, Sarason BR: Assessingsocial support: The social support questionnaire. Journal ofPersonality and Social Psychology. 1983, 44:127–139.
(41) Brown DR, Gary LE: Stressful life events, social support net-works, and the physical and mental health of urban black adults.Journal of Human Stress. 1987, Winter:165–173.
(42) Gil KM, Williams DA, Keefe FJ, Beckman JC: The relationshipof negative thoughts to pain and psychological distress. Behav-ior Therapy. 1990, 21:349–362.
(43) Rosenstiel AK, Keefe FJ: The use of coping strategies in lowback pain patients: Relationship to patient characteristics andcurrent adjustment. Pain. 1983, 17:33–40.
(44) Rosenbaum M: Learned resourcefulness as a behavioral reper-toire for the self-regulation of internal events: Issues and specu-lations. In Rosenbaum M, Franks CM, Jaffe Y (eds), Perspec-tives on Behavior Therapy in the Eighties. New York: Springer,1983, 54–73.
(45) Shacham S: A shortened version of the Profile of Mood States.Journal of Personality Assessment. 1983, 47:305–306.
(46) Mishel MH, Fleury J: The growth through uncertainty scale.Unpublished manuscript.
(47) Schnoll RA, Fang CY, Manne SL: The application of SEMto behavioral research in oncology: Past accomplishmentsand future opportunities. Structural Equation Modeling. 2004,11:583–614.
(48) Norris AE: Structural Equation Modeling. In Munro BH (ed),Statistical Methods for Health Care Research, 4th Edition.Philadelphia: Lippincott, 2001, 379–404.
(49) Byrne BM: Structural Equation Modeling With AMOS: BasicConcepts, Applications, and Programming. Mahwah, NJ: Law-rence Erlbaum Associates, Inc., 2001.
(50) Ashing–Giwa K, Ganz PA, Petersen L: Quality of life of Afri-can–American and White long term breast carcinoma survi-vors. Cancer. 1999, 85:418–426.
(51) Northouse LL, Caffey M, Deichelbohrer L, et al.: The quality oflife of African American women with breast cancer. Researchin Nursing & Health. 1999, 22:449–460.
(52) Bower JE, Low C, Ganz PA, et al.: Predictors and outcomes ofgrowth among women confronting breast cancer. Annals of Be-havioral Medicine. 2004, 27:103.
(53) Cooper–Patrick L, Gallo JJ, Gonzales JJ, et al.: Race, gender,and partnership in the patient–physician relationship. Journalof the American Medical Association. 1999, 282:583–589.
(54) Henderson PD, Gore SV, Davis BL, Condon EH: AfricanAmerican women coping with breast cancer: A qualitative anal-ysis. Oncology Nursing Forum. 2003, 30:641–647.
(55) Tomich PL, Helgeson VS: Is finding something good in the badalways good? Benefit finding among women with breast can-cer. Health Psychology. 2004, 23:16–23.
204 Porter et al. Annals of Behavioral Medicine
Related Documents











