PRE-OP and POST-OP SURGICAL CONSIDERATIONS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PRE-OP and POST-OP SURGICAL
CONSIDERATIONS
Darlene Sorrell, DMD, is not an oral surgeon.
AIDC is an out-patient facility.
29 years of experience in IHS.
Advanced General Practice Residency.
No access to hospital medical information so may need to defer treatment until more information is available.
Is good for a planned extraction
Describes what to expect (how long to expect to take off from work or school)
Take 600-800mg Ibuprofen 1 hour prior to procedure if not allergic to medication or no GI ulcers

Layman’s terms
IHS Form
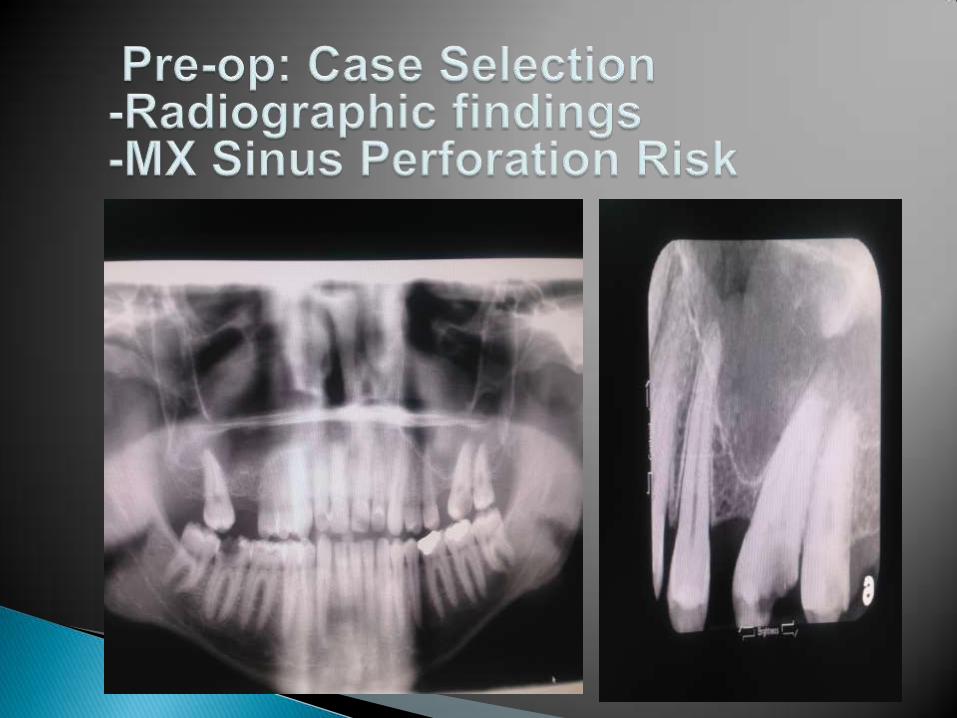
Lists potential Pre-op and Post-op Oral Surgery Considerations
Maxillary Sinus
Inferior Alveolar Location
Mandible Size: Elderly may have a thin mandible
Temporomandibular Joint: The pressure used during an extraction can increase or cause joint pain.

Take your time to review MH. Don’t feel pressured to extract. Refer for History/Physical or Medical
Clearance prior to dental treatment, if indicated.
Know when to refer to an oral surgeon, taking into consideration your training, experience, and credential level.
Consider emotional status of the patient.

Actonel, Boniva, Fosamax, Skelid, Didronel
IV has higher osteonecrosis rates compared to oral.
Some recommend an informed consent specific for patients taking Bisphosphonates.
Co-morbidities: chronic steroid therapy, diabetes, smoking, advanced age.
Refer for medical clearance if uncomfortable with status after research.
(I have Therapy Protocol if anyone wants copy.)
Should be taken prior to surgical procedure
Should have written clinic guidelines regarding when to seek a medical consult prior to invasive procedures

Patients on blood thinners (warfarin/coumadin); work with patient’s primary medical provider
Bleeding disorders (red blood cells, white blood cells and platelets); may need to be treated in a hospital environment by an oral surgeon.
Aspirin; may need to have patient bite longer on gauze
Temperature: Febrile
Lethargic/Malaise
Trismus
Compromised Airway: raised tongue, uvula deviated, sublingual swelling
**Depending on the severity of the above, should consider OMFS or ER referral and antibiotics.

Defer surgery until after delivery if possible.
If cannot defer, may want to consult with patient’s physician.
Avoid keeping the patient in the supine position for long periods of time to prevent vena cava compression.
Do not prescribe medication with teratogenic potential.


Must be verbal and written.
Language must be clear and simple enough to be followed by all patients.
Outlines care instructions for surgery day and a few days afterwards.
Explains what to do in an emergency when the clinic is closed.
Pressure: Clinically, pressure may need to be applied from 20 secs to 10 minutes
Epinephrine=vasoconstrictor
Procoagulants: Gelfoam, Surgicel, ActCel, Avitene
Sutures

Test: Gently pinch the patient’s nostrils and have her/him blow through nose and watch for air bubbles at extraction site.
Treatment determined by size: primary closure with vicryl sutures if larger than 2 mm, antibiotics, decongestant, follow-up
Refer to oral surgeon if membrane repair required.

Limited opening usually due to inflammation involving the muscles of mastication.
Can be caused by injection of anesthetic into muscles, most likely pterygoid muscle.
Complicated mandibular third molar extractions frequently results in trismus due to the inflammatory response near muscles.
Use of bite block can help to prevent trismus.
Inform patient in advance on consent form.

Ecchymosis=blood in the subcutaneous tissues (bruise)
Ecchymosis occurs more in older patients, is not dangerous and does not increase pain or infection but can be scary for patient.
Edema (Swelling)happens in most surgical procedures. Usually reaches max 48-72 hours after procedure. Should resolve in 1 week.
Increased swelling after 72 hours may indicate infection.
Swelling where mucoperiosteal flap surgery was performed.
Usually appears two weeks post-surgery and does not respond to antibiotics alone.
Often caused by foreign body or invasion of infectious organism between bone and periosteum.
Requires exploratory surgery: access, curettage, debride, irrigate and reapproximate.
Importance of “copious sterile irrigation”.

Most common is tearing of the mucosal flap during surgical extractions. PREVENTION: Create an adequate sized flap to prevent excess tension on flap and pay attention to retraction force on flap.
Second most common is inadvertent puncturing of soft tissue with an instrument. (Patient moves, friable tissue, instrument slips)
Treatment: Reapproximate and suture but may have to allow healing by secondary intention. And this may result in delayed healing.
Inform patient

Condyle slips past the Articular Eminence/disc
Patients are often able to reposition TMJ themselves
Inferior and posterior pressure (multiple tongue blades over posterior occlusion)
Muscle relaxer or get patient to relax muscles (massage)
Pain develops 3-4 days post-op.
Causes delayed healing but not associated with an infection.
Etiology unclear but it appears to be result of high levels of fibrinolytic activity around tooth extraction socket.
Smokers have increase risk
1-5% routine extractions; 20-30% impacted molars

Repeat post-op instructions i.e. no smoking
Minimize trauma and bacterial contamination during surgery.
Thoroughly debride extraction site and irrigate with copious amounts of saline.
Use surgical handpiece
Pre-rinse with peridex??

Treatment of pain with analgesics; treatment does not speed up healing.
Irrigation of socket with sterile saline and placement of medicated dressing on iodoform gauze.
Dressing is changed 24-48 hours for 3-6 days.
Result of excessive force with forceps which fractures large portions of cortical plate.
PREVENTION: ST Flap and controlled amounts of bone removal so tooth can be delivered easily.
PREVENTION: Perform a preoperative clinical and radiographic examination of the alveolar process.
Age of patient: Bones of elderly patients are less elastic and may fracture rather than expand with elevation.
If not excessively mobile, dissect tooth away from bone segment.
If excessively mobile, can splint tooth to adjacent tooth and allow to heal 6-8 weeks then extract with open surgical technique.
If excessively mobile, cut crown from root, allow to heal 6-8 weeks, then remove roots.
If tuberosity is completely separated from soft tissue then smooth bone, check for oroantral communication, and suture.
Also, can provide antibiotics and refer to OMFS.

Altered sensation due to nerve trauma or damage.
Greatest risk: mandibular and lingual nerves Risk factors: surgical technique, age of
patient (over age 0f 35), location of tooth. Most recovery without treatment within 6
months. Can refer for surgical repair if paresthesia is
persistent after 6 months. Follow patient and clearly document changes
at each visit.
Review done annually.
7210, 7220, 7230, and 7240 (Do not include routine extractions)
We do not include patient in pain but healing WNL.
Are we making the correct case selections?
15% and less complications
Dr. Tim Ricks
Dr. Jeff Stuart
On-line Sources (i.e. Medline)
The American Dental Association
The American Academy of Oral Medicine
The American Association of Oral and Maxillofacial Surgeons

Related Documents











