Check the question -- never copy completely :/ and see if you can find the answer to some (: Share with as many people IN THE CLASS as you want to. 1. Name 5 sympt oms of diabete s Fatigue, unexplained weight loss, excessive thirst (polydipsia), excessive urination (polyuria), excessive eating/increase hunger (polyphagia), poor wound healing, infections , blurry vision 2. Insu lin is th e first l ine of t hera py fo r Type I I diab ete s Not true. Usually metformin 3. Desc ribe 2 phys iolo gica l etiolo gies (ca use s) of type I diab etes? Autoimmune disorder 4. Name 4 test used to determine the le vel of glu cose i n the body Urine analysis Fasting blood glucose level test / FPG (≥ 7.0 mmol/L (126 mg/dL) Haemoglobin A1c test (≥ 6.5%) Oral glucose tolerance test / OGTT ( Plasma glucose ≥ 11.1 mmol/L (200 mg/dL) two hours after a 75 g oral glucose load) http://diabetes.niddk.nih.gov/dm/pubs/diagnosis/ 5. Apart from monitorin g glucose level and b lood press ure, name 2 othe r annual t est that should be carried out for diabetic patients. Why should these 2 test be done? Dilated eye exam: An eye care professional uses eye drops to temporarily widen, or dilate, the black part of the patient's eyes (pupils) to see inside the eyes. Uncontrolled diabetes can damage the eyes, harming vision and possibly leading to blindness. Foot exam: A check of the foot's nerves and blood circulation. Uncontrolled diabetes can lead to foot problems that may eventually require amputation. 6. Explain the rationale behind the mode of administration o f insulin an d the disadvantage of such administration method Treatment of diabetes always involves injection of insulin (IV) because if taken orally, insulin would be destroyed in the stomach before it could get into the blood where it is needed. Insulin therapy requires close monitoring and great deal of patient education as improper administration is quite dangerous. E.g. food intake reduced, less insulin required or may cause hypoglycaemic reaction, may promote small blood vessels disease. Creates risk because of the inability to continuously know a person’s blood glucose level and adjust the insulin infusion appropriately. http://en.wikipedia.org/wiki/Diabetes_management 7. Name 2 c lasses of T ype II ora l anti-diabe tic medica tion. Give 1 examp le for each class. Sulfonylureas (Glucovance is a combination medicine that contains glyburide and metformin, Metaglip is a combination medicine that contains glipizide and metformin.) - Inc rease amount of ins uli n pr oduce d by pancr eas Thiazolidinediones Brand name: Actos (generic name: pioglitazone), Brand name: Avandia (generic name: rosiglitazone).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/3/2019 Pre Lesson Notes
http://slidepdf.com/reader/full/pre-lesson-notes 1/5
Check the question -- never copy completely :/ and see if you can find the answer tosome (: Share with as many people IN THE CLASS as you want to.
1. Name 5 symptoms of diabetesFatigue, unexplained weight loss, excessive thirst (polydipsia), excessive urination(polyuria), excessive eating/increase hunger (polyphagia), poor wound healing,
infections, blurry vision
2. Insulin is the first line of therapy for Type II diabetesNot true. Usually metformin
3. Describe 2 physiological etiologies (causes) of type I diabetes?Autoimmune disorder
4. Name 4 test used to determine the level of glucose in the bodyUrine analysis
Fasting blood glucose level test / FPG (≥ 7.0 mmol/L (126 mg/dL)Haemoglobin A1c test (≥ 6.5%)
Oral glucose tolerance test / OGTT (Plasma glucose ≥ 11.1 mmol/L (200 mg/dL) twohours after a 75 g oral glucose load)
http://diabetes.niddk.nih.gov/dm/pubs/diagnosis/
5. Apart from monitoring glucose level and blood pressure, name 2 other annual test thatshould be carried out for diabetic patients. Why should these 2 test be done?
Dilated eye exam: An eye care professional uses eye drops to temporarily widen, or dilate, the black part of the patient's eyes (pupils) to see inside the eyes. Uncontrolleddiabetes can damage the eyes, harming vision and possibly leading to blindness.
Foot exam: A check of the foot's nerves and blood circulation. Uncontrolled diabetes
can lead to foot problems that may eventually require amputation.
6. Explain the rationale behind the mode of administration of insulin and the disadvantageof such administration methodTreatment of diabetes always involves injection of insulin (IV) because if taken orally,insulin would be destroyed in the stomach before it could get into the blood where it isneeded. Insulin therapy requires close monitoring and great deal of patient education as improper administration is quite dangerous. E.g. food intake reduced, less insulin required or maycause hypoglycaemic reaction, may promote small blood vessels disease. Creates riskbecause of the inability to continuously know a person’s blood glucose level and adjustthe insulin infusion appropriately.
http://en.wikipedia.org/wiki/Diabetes_management
7. Name 2 classes of Type II oral anti-diabetic medication. Give 1 example for each class.
Sulfonylureas (Glucovance is a combination medicine that contains glyburide andmetformin, Metaglip is a combination medicine that contains glipizide and metformin.)- Increase amount of insulin produced by pancreasThiazolidinediones Brand name: Actos (generic name: pioglitazone), Brand name:Avandia (generic name: rosiglitazone).
8/3/2019 Pre Lesson Notes
http://slidepdf.com/reader/full/pre-lesson-notes 2/5
- Helps to lower insulin resistance in cells, improving the way that body responds to insulin
8. Name primary site of action for the following classes of OHGA (oral hypoglycemicagents)
a. Alpha-glucosides inhibitor(acarbose) (saccharides that act as competitiveinhibitors of enzymes needed to digest carbohydrates), reduce impact of
carbohydrates on blood sugar by preventing digestion of carbohydratesb. Biguanides(metformin) (reduce gluconeogenesis in the liver, and, as a result,
reduce the level of glucose in the blood)c. Sulfonylureas (ATP-dependent K+(KATP) channel on the cell membrane of
pancreatic beta cells)d. Thiazolidinedones (activating PPARs (peroxisome proliferator-activated
receptors), a group of receptor molecules inside the cell nucleus, specifically
PPARγ (gamma). The ligands for these receptors are free fatty acids (FFAs) and
eicosanoids. When activated, the receptor migrates to the DNA, activating
transcription of a number of specific genes.)
9. What is the rationale behind combination drug therapyMonotherapy often fails after a period of time, thus multiple drugs is needed to achieveglycemic control
10. Describe the mechanism of action of Type II oral anti-diabetic drugs
11. Apart from medication dispensed how would you counsel a diabetic patient on self-care‘Have a healthy diet (if patient obese, recommend dietitian), eat consistent, well-balanceddiet consist of high in fiber, low in saturated fat, low in concentrated sweets, advise toexercise regularly, moderate alcohol consumption, quit smoking, self-monitored bloodglucose
12. Name 3 complication in diabetes and describe how high level of plasma glucose couldlead to these complication
Diabetic hyperglycemic hyperosmolar coma - extremely high blood glucose levelswithout presence of ketones, condition of dehydration
- Kidney make up for high glucose levels in blood by allowing extra glucose to leave the
body through urine.
- Not enough fluid/fluid with sugar > kidney cannot get rid of extra glucose > glucose level
in blood increase > blood more concentrated than normal (hyperosmolarity)
- Hyperosmolarity: blood has high conc of salt(sodium), glucose and other substances
that normally cause water to move into the bloodstream > draws water out of body’s
organ(brain) > cycle of increasing blood glucose level & dehydration
Diabetic ketoacidosis - occurs when the body cannot use sugar (glucose) as a fuelsource because there is no insulin or not enough insulin. Fat is used for fuelinstead. Byproducts of fat breakdown called ketones build up in body.
- Glucose not available, fat is broken down (normally in type 1 diabetes)- Acids(ketones) build up in blood and urine when fat breaks down, high level of ketones
is poisonous (ketoacidosis)- BGL rise (>300mg/dL) because liver makes glucose to combat problem
8/3/2019 Pre Lesson Notes
http://slidepdf.com/reader/full/pre-lesson-notes 3/5
13. If a person is hyperglycaemic is he/she considered in diabetic? No
http://www.emedicinehealth.com/diabetes/article_em.htm
Diabetes mellitus (DM): body cannot regulate the amount of sugar (glucose) in the blood.
Process
• Liver converts food into glucose
• Glucose release into bloodstream
• Healthy person – blood glucose regulated by several hormones (primarily insulin).
• Insulin produced in pancreas (organ between stomach & liver)
• Insulin allows glucose to move out of blood to cells throughout body where it is needed
for fuel
•
Diabetic person – do not produce enough insulin (type 1 diabetes) / cannot use insulinproperly (type 2 diabetes) or both
• Diabetes – glucose in blood cannot move efficiently to cells, therefore blood glucose
remains high. Starves cells that need glucose for fuel and harm organs/tissues exposed
to high glucose levels
8/3/2019 Pre Lesson Notes
http://slidepdf.com/reader/full/pre-lesson-notes 4/5
Type 1 diabetes (T1D/IDDM): The body stops producing insulin or produces too little insulin to
regulate blood glucose level.
- Usually diagnosed during childhood or adolescence. Referred as juvenile-onset diabetes
or insulin-dependent DM
- Can occur in older individual due to destruction of pancreas by alcohol/disease/removal
in surgery or progressive failure of pancreatic beta cells (cell that produce insulin)- Requires insulin treatment daily to sustain life
- Cause by body’s immune system that attacks the cell in pancreas that produces insulin
(autoimmune disorder)
Type 2 diabetes (T2D/NIDDM): Although the pancreas still secretes insulin, the body of
someone with type 2 diabetes is partially or completely unable to use this insulin. This is
sometimes referred to as insulin resistance. The pancreas tries to overcome this resistance by
secreting more and more insulin. People with insulin resistance develop type 2 diabetes when
they fail to secrete enough insulin to cope with their higher demands.
- Usually diagnosed in adulthood after age 45. Referred as adult-onset diabetes or non-
insulin dependent DM but names no longer use as it occurs in younger people and some
people requires insulin therapy
- Controlled with diet, weight loss, exercise and oral medications (metformin; first line
treatment as it decreases mortality, acarbose, sulfonylureas, thiazolidinediones)
- Cause by strong genetics link (tends to run in the families), lifestyle, medical conditions
Gestational diabetes (GDM) is a form of diabetes that occurs during the second half of
pregnancy.
Both type 1 and type 2 diabetes ultimately lead to high blood sugar levels, a condition called
hyperglycemia. Over a long period of time, hyperglycemia damages the retina of the eye, theblood vessels of the kidneys, the nerves, and other blood vessels.
8/3/2019 Pre Lesson Notes
http://slidepdf.com/reader/full/pre-lesson-notes 5/5
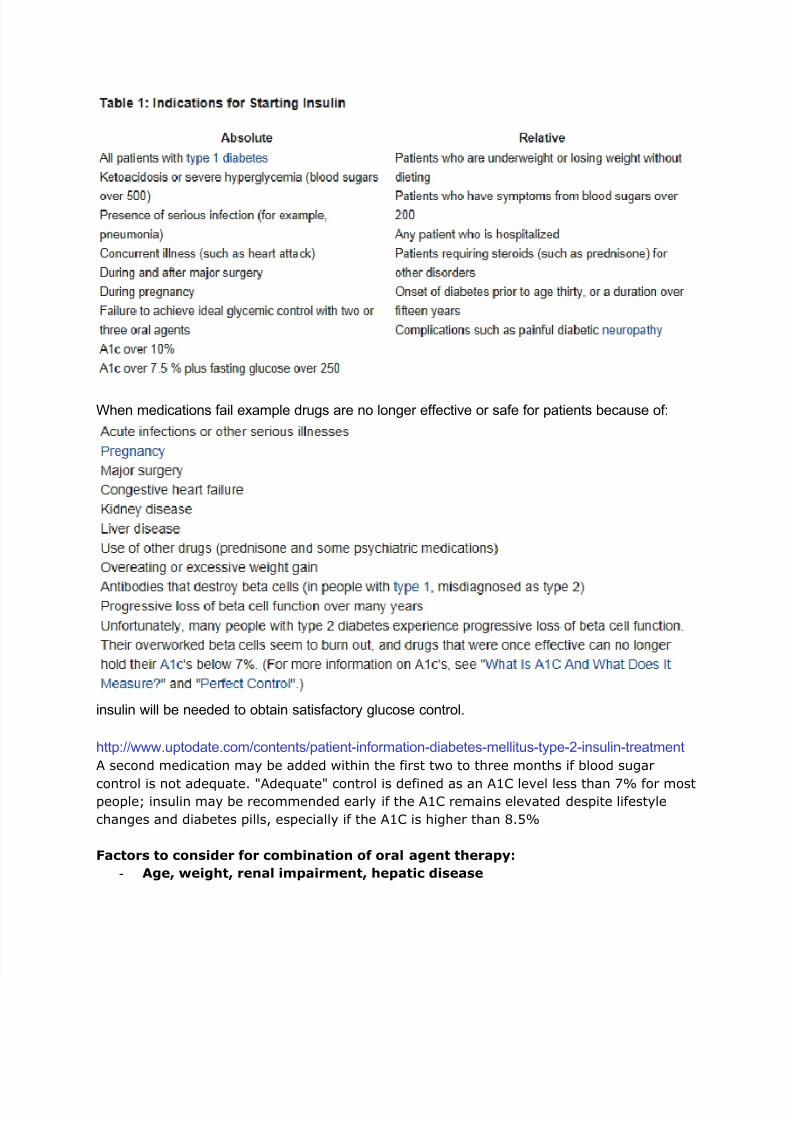
When medications fail example drugs are no longer effective or safe for patients because of:
insulin will be needed to obtain satisfactory glucose control.
http://www.uptodate.com/contents/patient-information-diabetes-mellitus-type-2-insulin-treatment
A second medication may be added within the first two to three months if blood sugar
control is not adequate. "Adequate" control is defined as an A1C level less than 7% for mostpeople; insulin may be recommended early if the A1C remains elevated despite lifestyle
changes and diabetes pills, especially if the A1C is higher than 8.5%
Factors to consider for combination of oral agent therapy:
- Age, weight, renal impairment, hepatic disease
Related Documents