Prague 2008 1 Plasma vs. tissue concentration to predict antibiotic efficacy PL Toutain UMR 181 Physiopathologie et Toxicologie Experimentales INRA/ENVT ECOLE NATIONALE VETERINAIRE T O U L O U S E Fourth International conference on AAVM Prague, Czech republic 24-28, 2008

Prague 2008 1 Plasma vs. tissue concentration to predict antibiotic efficacy PL Toutain UMR 181 Physiopathologie et Toxicologie Experimentales INRA/ENVT.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Prague 2008 1
Plasma vs. tissue concentration to predict antibiotic efficacy
PL ToutainUMR 181 Physiopathologie et Toxicologie Experimentales
INRA/ENVT
ECOLENATIONALEVETERINAIRET O U L O U S E
Fourth International conference on AAVM Prague, Czech republic 24-28, 2008

Prague 2008 2
In veterinary medicine, there are many publications on tissular concentrations to promote the idea that some antibiotics having a high tissular concentration accumulate in biophase (quinolones, macrolides) and are more efficacious as suggested by their low or undetectable plasma concentrations
The inadequate tissue penetration hypothesis

Prague 2008 3
• Two false assumptions1. tissue is homogenous2. bacteria are evenly distributed through
tissue
spurious interpretation of all important tissue/serum ratios in predicting the antibacterial effect of AB
The inadequate tissue penetration hypothesis: Schentag 1990
Schentag, 1990

Prague 2008 4
Statements such as ‘concentrations in tissue x h after dosing are much higher than the MICs for
common pathogens that cause disease’ are meaningless
Mouton & al JAC 2007
Prague 2008 5
Objectives of the presentation:To address some basic questions
1. Where are located the bugs ?
• Extracellular vs. intracellular
2. Where is the biophase?
• Interstitial space fluid vs. intracellular cytosol vs. intracellular organelles
3. What is a tissue and what is a tissue concentration
4. How to assess the biophase antibiotic concentration
• Total tissular concentration vs. ISF concentration.
5. The issue of lung penetration
1. Epithelial lining fluid (ELF):????
2. The hypothesis of targeted delivery of the active drug at the infection site by phagocytes
6. Plasma as the best surrogate of biophase concentration for PK/PD interpretation
Prague 2008 6
Q1: Where are located the pathogens
Prague 2008 7
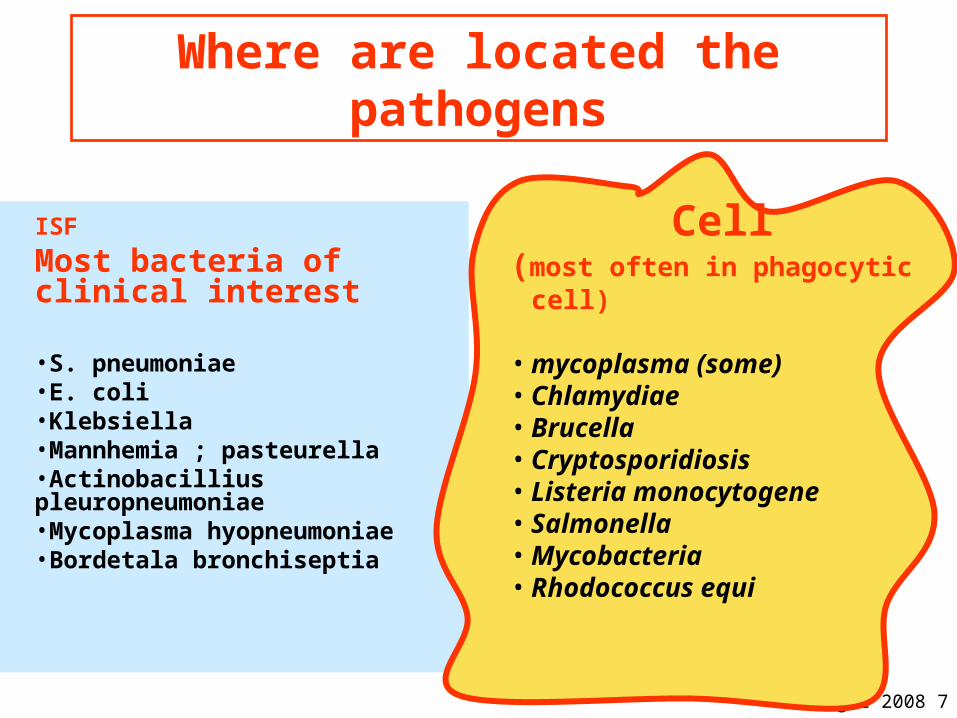
Where are located the pathogens
ISF
Most bacteria of clinical interest
•S. pneumoniae•E. coli•Klebsiella•Mannhemia ; pasteurella•Actinobacillius pleuropneumoniae•Mycoplasma hyopneumoniae•Bordetala bronchiseptia
Cell(most often in phagocytic cell)
• mycoplasma (some)• Chlamydiae• Brucella• Cryptosporidiosis• Listeria monocytogene• Salmonella• Mycobacteria• Rhodococcus equi

Prague 2008 8
Q2: Where is the biophase

Prague 2008 9
The interstitial space fluid is the biophase
1. Most bacterial infections are located in the extracellular compartment.
2. Except few cases, In acute infections in non-specialized tissues, where there is no abscess formation, interstitial space fluid (ISF) must be considered as the actual target space for anti-infective agents
3. ISF concentrations are of primary interest
Muller et al. AAC , 2004, 48: 1441-1453

Prague 2008 10
Q3: what is a tissue & what is a tissular concentration
Prague 2008 11
Historical definition of a tissue drug concentration
• In the past, it was used to characterize the total concentration in a homogenized biopsy sample– For vet medicine: a by-product of regulatory
residue studies
• It was assumed that:– tissue is homogenous– that antibiotics is evenly repartited in tissue – That bacteria are evenly repartited in tissue
– Each of these assumptions is false and can be very misleading

Prague 2008 12
Why a total drug tissue concentrations may be misleading?
1. Drug distributed mainly extracellularly• β-lactams and aminoglycosides,• grinding up the tissue means dilution of the drug by
mixing intracellular and extracellular fluids, resulting in underestimation of its concentrations at the site of infection.
2. Drug accumulated by cells • fluoroquinolones or macrolides• assay of total tissue levels will lead to gross
overestimation of the extracellular concentration.• The opposite is true for intracellular infections.

Prague 2008 13
Methods for studies of target site drug distribution in antimicrobial
chemotherapy

Prague 2008 14
“Tissue concentrations”
• Total tissue– homogenates– biopsies
• Extracellular fluids– implanted cages– implanted threads– wound fluid– blister fluid– ISF (Microdialysis, Ultrafiltration)

Prague 2008 15
The tissue cage model for in vivo and ex vivo investigations

Prague 2008 16
The tissue cage model
• Perforated hollow devices• Subcutaneous
implantation• development of a highly
vascularized tissue• fill up with a fluid with half
protein content of serum (delay 8 weeks)
•C.R. Clarke. J. Vet. Pharmacol. Ther. 1989, 12: 349-368

Prague 2008 17
The tissue cage model : PK limitations
• A foreign body– Not a physiological space
– Clinical counterparts?
• Ascitic fluid, effusions ( pericardial, pleural…)
• Interpretation may be difficult because PK
determined by:– diffusion capacity across the TC
– TC size and geometry
• surface area/volume ratio is the major determinant of peak and
trough drug level

Prague 2008 18
The tissue cage model
Drug administration
Slow equilibration
inoculation
Time
(C)
Time
(C)
T1/2 varies with the surface area / volume ratio of the tissue cage
Penicillin 5 to 20 hDanofloxacin 3 to 30 h
Greko, 2003, PhD Thesis

Prague 2008 19
Microdialysis & ultrafiltration Techniques

Prague 2008 20
What is microdialysis (MD)?
• Microdialysis, a tool to monitors free antibiotic concentrations in the fluid which directly surrounds the infective agent

Prague 2008 21
Microdialysis: The Principle
• The MD Probe mimics a "blood capillary".
•There is an exchange of substances via extracellular fluid
•Diffusion of drugs is across a semipermeable membrane at the tip of an MD probe implanted into the ISF of the tissue of interest.

Prague 2008 22
• the implanted MD probe is perfused with the perfusate, ie, a physiologic liquid at a very slow rate.
• Substances present in the interstitial space fluid of the investigated site can diffuse into the perfusate through a semipermeable membrane at the tip of the MD probe and appear in the dialysate.
• Afterward the concentration in the dialysate is chemically analyzed and the true concentration in the interstitial space fluid can be calculated.
Microdialysis: The Principle
Antibiotic

Prague 2008 23
Microdialysis materials
CMA60 MicrodialysisCMA60 Microdialysis CMA60 MicrodialysisCMA60 Microdialysis
1. Introducer with CMA 60 Microdialysis Catheter
2. Outlet tube
3. Vial holder
4. Microvial
5. Inlet tube
6. Luer lock connection
7. Puncture needle.

Prague 2008 24
Microdialysis : Limits
• MD need to be calibrated
• Retrodialysis method– Assumption: the diffusion process is quantitatively
equal in both directions through the semipermeable membrane.
– The study drugs are added to the perfusion medium and the rate of disappearance through the membrane equals in vivo recovery.
– The in vivo percent recovery is calculated (CV of about 10-20%)
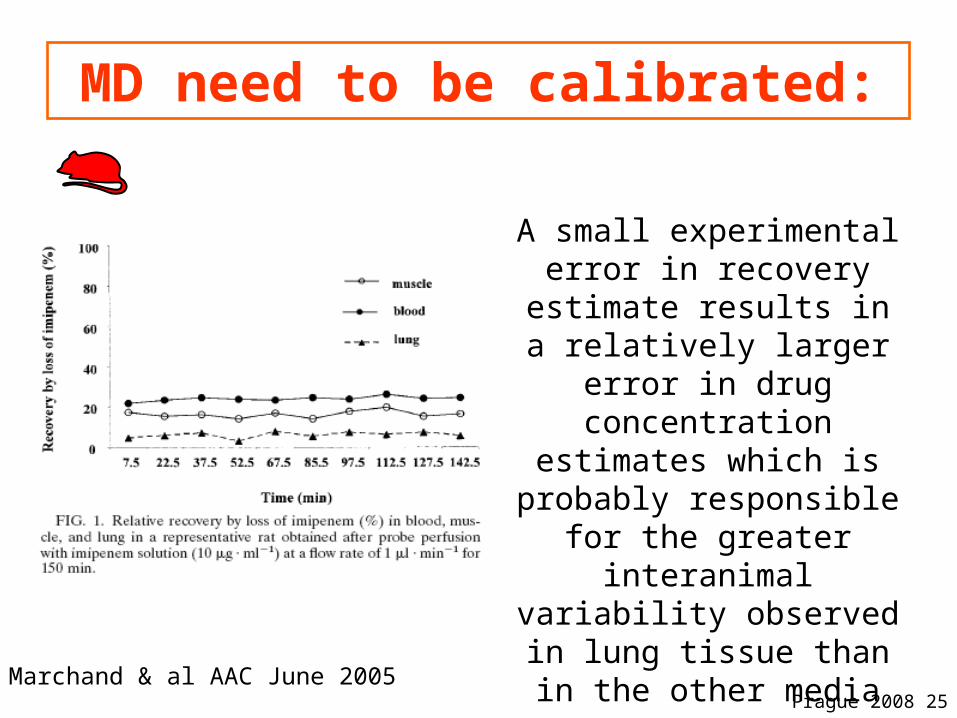
Prague 2008 25
A small experimental error in recovery estimate results in a relatively larger error in
drug concentration estimates which is probably responsible for the greater
interanimal variability observed in lung tissue than in the other media
Marchand & al AAC June 2005
MD need to be calibrated:

Prague 2008 26
Ultrafiltration
• Excessive (in vivo) calibration procedures are required for accurate monitoring
• Unlike MD, UF-
sample concentrations are independent on probe diffusion characteristics
Prague 2008 27
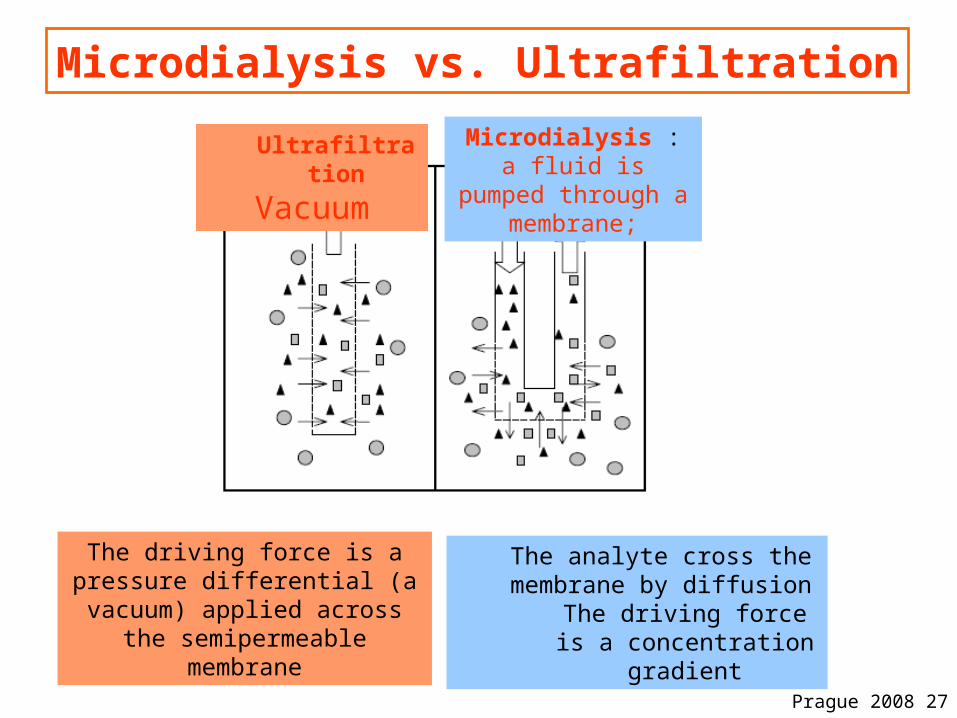
Microdialysis vs. Ultrafiltration
Ultrafiltration
Vacuum
Microdialysis :a fluid is pumped
through a membrane;
The driving force is a pressure differential (a vacuum) applied
across the semipermeable membrane
The analyte cross the membrane by diffusion
The driving force is a concentration gradient
Prague 2008 28
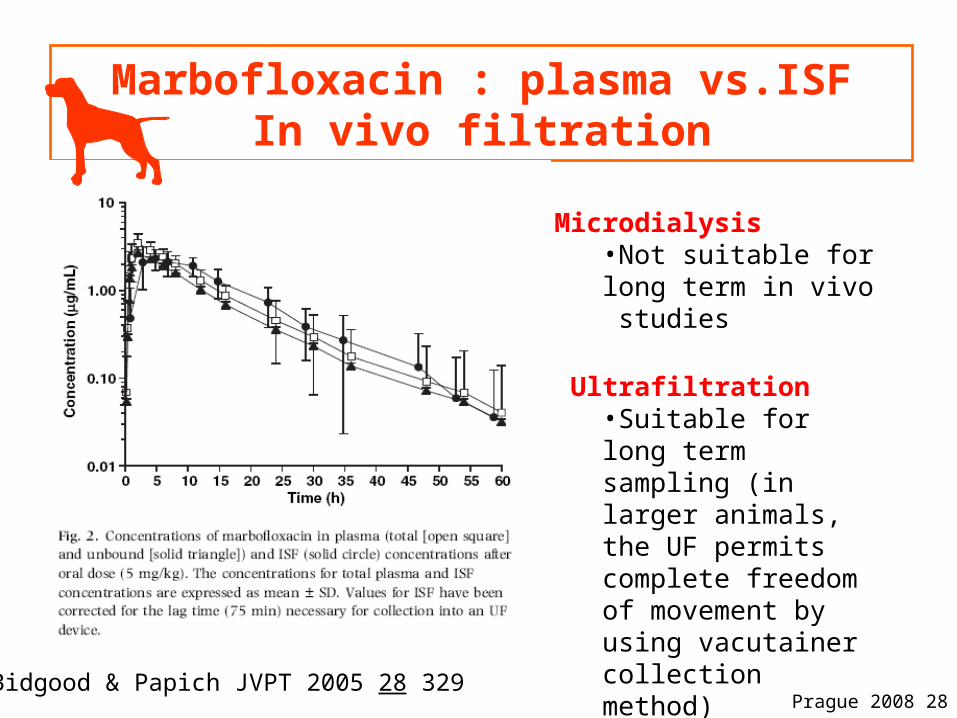
Marbofloxacin : plasma vs.ISFIn vivo filtration
Bidgood & Papich JVPT 2005 28 329
Microdialysis•Not suitable for long term in vivo studies
Ultrafiltration•Suitable for long term sampling (in larger animals, the UF permits complete freedom of movement by using vacutainer collection method)
Prague 2008 29
What we learnt with animal and human microdialysis studies

Prague 2008 30
Plasma (total, free) concentration vs interstitial concentration (muscle, adipose
tissue) (Moxifloxacin)
Muller AAC, 1999 Time (h)
Total (plasma, muscle)free (plasma)interstitial muscleinterstitial adipose tissue
2 6 10 12 30 4020
100
1000
Co
nce
ntr
ati
on
(n
g/m
L)

Prague 2008 31
Plasma (total, free) concentration vs muscle (free) concentration
Total (plasma)free (muscle)free (plasma)
Liu J.A.C. 2002
cefpodoxine
cefixime

Prague 2008 32
What we learnt with animal and human MD studies
• MD studies showed that:1. the concentrations in ISF of selected
antibiotics correspond to unbound concentrations in plasma
2. They are generally much lower than total concentrations reported from whole-tissue biopsy specimens especially for macrolides and quinolones

Prague 2008 33
What we learnt with MD studies: Inflammation

Prague 2008 34
Tissue concentrations of levofloxacin in inflamed and healthy subcutaneous adipose tissue
Methods: Free Concentrations measured in six patients by
microdialysis after administration of a single intravenous dose of 500 mg.
Results:The penetration of levofloxacin into tissue appears to be unaffected by local inflammation.Same results obtained with others quinolones
Hypothesis: Accumulation of fibrin and other proteins, oedema, changed pH and altered capillary permeability
may result in local penetration barriers for drugs
Bellmann & al Br J Clin Pharmacol 2004 57
Inflammation
No inflammation

Prague 2008 35
What we learnt with MD studies: Inflammation
• Acute inflammatory events seem to have little influence on tissue penetration.
• “These observations are in clear contrast to reports on the increase in the target site availability of antibiotics by macrophage drug uptake and the preferential release of antibiotics at the target site a concept which is also used as a marketing strategy by the drug industry” Muller & al AAC May 2004

Prague 2008 36
In acute infections in non-specialized tissues, where there is no abscess formation, free serum
levels of antibiotics are good predictors of free levels in tissue
fluid
Prague 2008 37
The issue of lung penetration

Prague 2008 38
Animal and human studies MD: The issue of lung penetration
•Lung MD require maintenance under anesthesia, thoracotomy (patient undergoing lung surgery)..
•Does the unbound concentrations in muscle that are relatively accessible constitute reasonable predictors of the unbound concentrations in lung tissue (and other tissues)?

Prague 2008 39
Free muscle concentrations of cepodoxime were similar to free lung concentration and therefore provided a surrogate measure
of cefpodoxime concentraion at the pulmonary target site
Liu et al., JAC, 2002 50 Suppl: 19-22.
Cefpodoxime at steady state: plasma vs. ISF (muscle & Lung)
Plasma
Free plasma
Muscle Lung

Prague 2008 40
The issue of lung penetration:Imipem
• The major finding of this study was the observation of virtually superimposed free IPM concentration-versus-time profiles in the three media investigated,
• This result not only is in agreement with theory but also is consistent with most of the data in the literature.
imipenem distribution in muscle and lung interstitial fluids
Marchand & al AAC June 2005

Prague 2008 41
The issue of lung penetration

Prague 2008 42
Lung infections
• Uncertainty of the relevant actual location of proliferating bacteria– Alveoli, pulmonary interstitium, bronchioles, blood??
• What is the biophase??– Epithelium lining fluid (ELF)– Lung IF, alveolar macrophages, tisue biopsies, blood,
bronchial secretion, sputum??
• ELF seems the most relevant specimen but potential sources of error: dilution, release of AB from alveolar macrophage in the sample
Prague 2008 43
Prague 2008 44
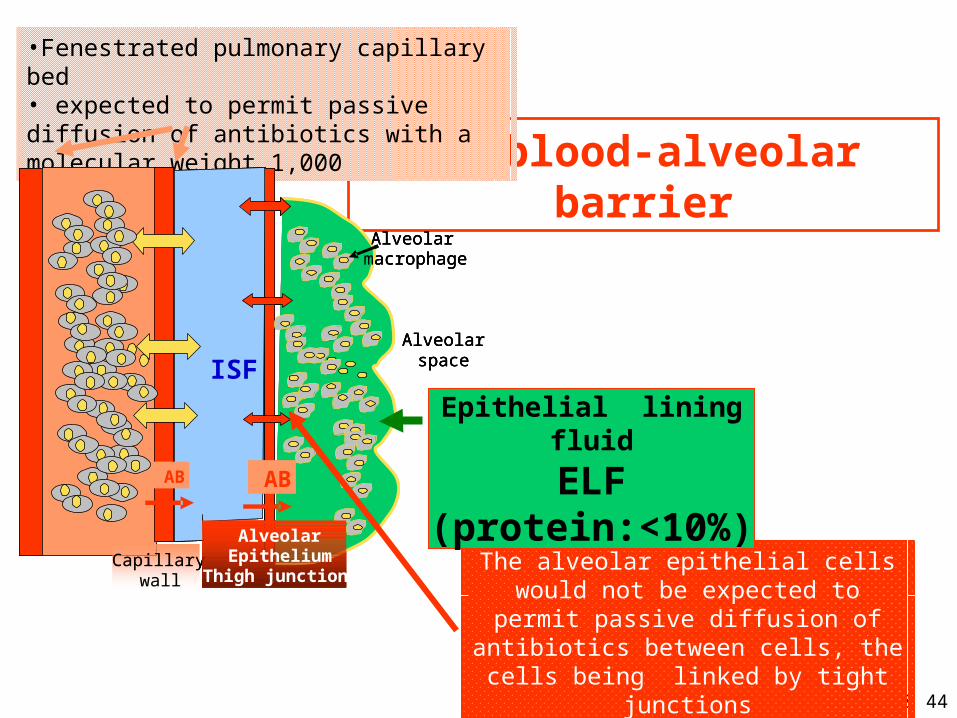
The blood-alveolar barrier
The alveolar epithelial cells would not be expected to permit passive diffusion of
antibiotics between cells, the cells being linked by tight junctions
•Fenestrated pulmonary capillary bed• expected to permit passive diffusion of antibiotics with a molecular weight 1,000
Epithelial lining fluid
ELF(protein:<10%)
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
space
Alveolarmacrophage
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
space
Alveolarmacrophage
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
space
Alveolarmacrophage
ABAB
AlveolarAlveolarAlveolar

Prague 2008 45
Drug passage in the lung
Drug passage through the alveolar epithelial cells will depend on the lipophilicity
and diffusibility of the antibiotics, similar to the
drug entry into the central nervous system.
Kiem & Schentag AAC 2008 Jan 24-36
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ELF

Prague 2008 46
ELF concentration: possible biais
• Measurement problems may confound the interpretation of the ELF concentrations of antibiotics.
• Cells, especially AM cells (that constitute 3.8 to 10.0% of ELF volume) are included in the composition of ELF
• The cells may be lysed during the measurement of antibiotic concentration in BAL-derived fluids.
Kiem & Schentag AAC 2008 Jan 24-36
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ELF
Prague 2008 47
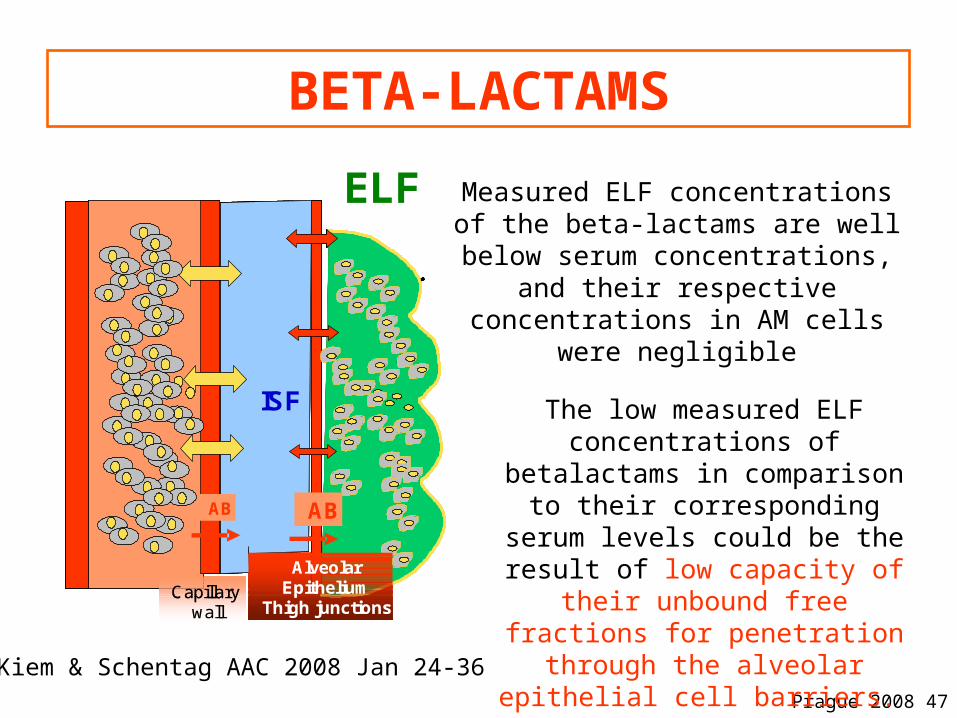
BETA-LACTAMS
Measured ELF concentrations of the beta-lactams are well below serum concentrations, and their respective
concentrations in AM cells were negligible
The low measured ELF concentrations of betalactams in
comparison to their corresponding serum levels could be the result of low capacity of their unbound free
fractions for penetration through the alveolar epithelial cell barriers.
Kiem & Schentag AAC 2008 Jan 24-36
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ELF
Prague 2008 48
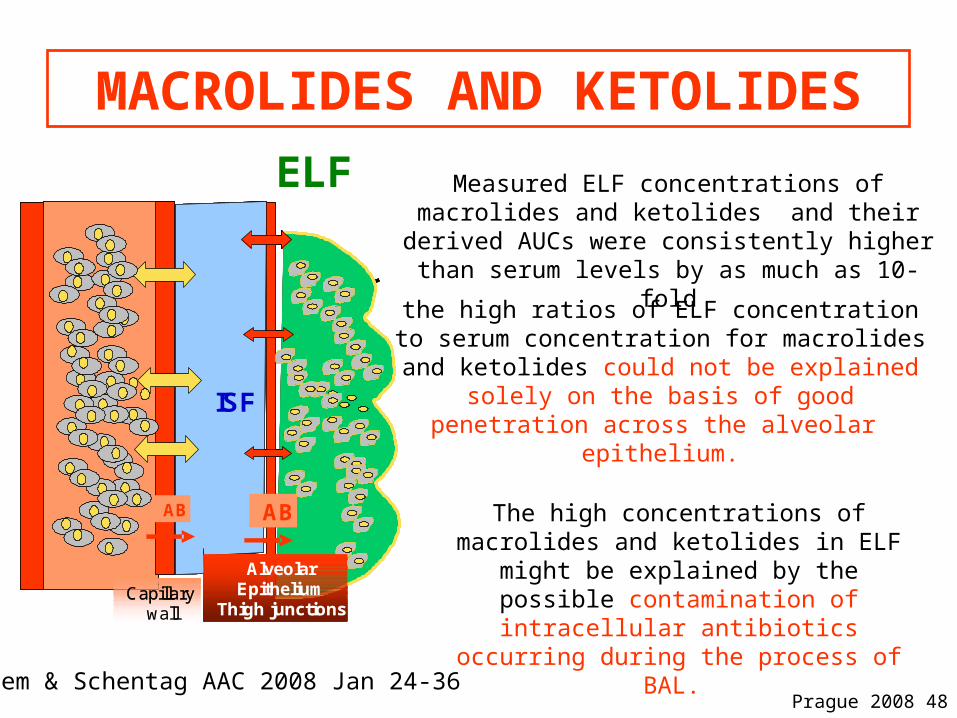
MACROLIDES AND KETOLIDES
Measured ELF concentrations of macrolides and ketolides and their derived AUCs were consistently
higher than serum levels by as much as 10-fold
the high ratios of ELF concentrationto serum concentration for macrolides and
ketolides could not be explained solely on the basis of good penetration across the alveolar
epithelium.
The high concentrations of macrolides and ketolides in ELF might be explained
by the possible contamination of intracellular antibiotics occurring during
the process of BAL.
Kiem & Schentag AAC 2008 Jan 24-36
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ELF
Prague 2008 49
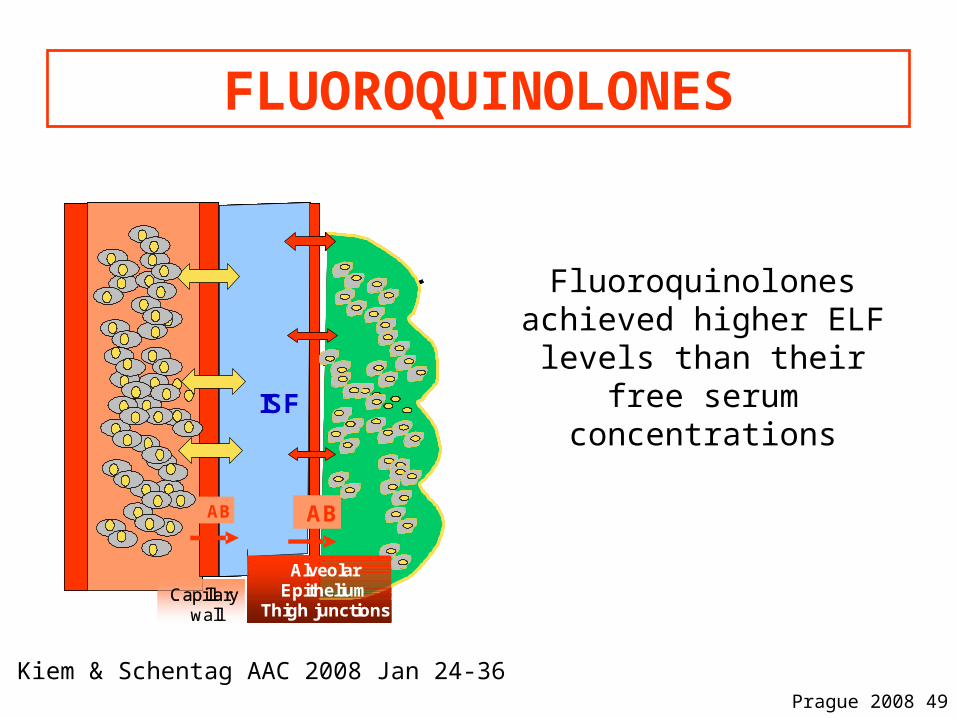
FLUOROQUINOLONES
Fluoroquinolones achieved higher ELF levels than their free
serum concentrations
Kiem & Schentag AAC 2008 Jan 24-36
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB
ISF
Capillarywall
AlveolarEpithelium
Thigh junctions
ABAB

Prague 2008 50
• The high ELF concentrations of some antibiotics, which were measured by the BAL technique, might be explained by possible contamination from high achieved intracellular concentrations and subsequent lysis of these cells during the measurement of ELF content.
• This effect is similar to the problem of measuring tissue content using homogenization
Kiem & Schentag’ Conclusions (1)

Prague 2008 51
• Fundamentally, ELF may not represent the lung site where antibiotics act against infection.
• In view of the technical and interpretive problems with conventional ELF and especially BAL, the lung microdialysis experiments may offer an overall better correlation with microbiological outcomes.
• We continue to express PK/PD parameters using serum concentration of total drug because these values do correlate with microbiological outcomes in patients.
Kiem & Schentag’ Conclusions (2)

Prague 2008 52
The site of infection: Intracellular pathogens
Prague 2008 53
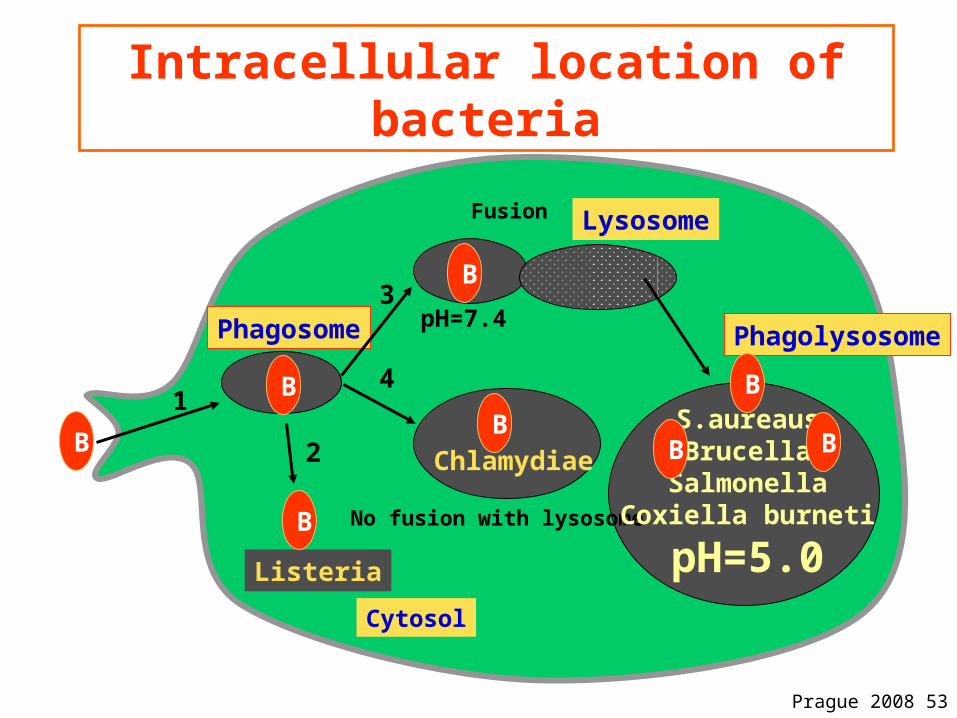
Intracellular location of bacteria
Phagosome
Lysosome
Chlamydiae
Listeria
No fusion with lysosome
Phagolysosome
S.aureausBrucella
SalmonellaCoxiella burneti
pH=5.0
3
4
2
1
Fusion
pH=7.4
BB
B
B
B
B
B B
Cytosol

Prague 2008 54
Intracellular location of antibiotics
Phagolysosomevolume 1 to 5% of cell volume
pH=5.0
Macrolides (x10-50)Aminoglycosides (x2-4)
CytosolpH=7.2
Fluoroquinolones(x2-8)beta-lactams (x0.2-0.6)
Rifampicin (x2)Aminoglycosides (slow)
Ion trapping for weak base with high pKa value

Prague 2008 55
What are the antibiotic intracellular expressions of activity
Phagolysosome
Macrolides Aminoglycosides
CytosolpH=7.2
Fluoroquinolonesbeta-lactamsRifampicin
Aminoglycosides
Good Low or nul

Prague 2008 56
The hypothesis of targeted delivery of active drug at the active site by the phagocytes

Prague 2008 57
Drug delivery by the phagocytes
• Transport by "non professional" phagocytes (e.g. azithromycin by fibroblast)
• Fibroblast acts as a reservoir for drug and macrophages
Prague 2008 58
Neutrophils as antibiotic delivery system
The ability of neutrophils to migrate preferentially to sites of infection makes them attractive as a delivery mechanism for antibiotics; theoretically , with the proper cellular PK, an antibiotic could be taken up by neutrophils, which would then transport the drug and later release it . This could provide a mechanism for achieving higher levels of antibiotic in tissues i.e. directly at the nidus of infection.
Scorneaux & Shryock tilmicosine in pigs; JVPT 1998, 21: 257-258 & tilmicosine in cattle in: J. Dairy Sci. 1999, 82: 1202-1212)

Prague 2008 59
Macrolides: how to explain efficacy of low plasma concentrations?
M
M1.PK hypothesis
2-PD hypothesis
M
PMN
Nucleus
High local M concentration in the vicinity of the bug
Sink or reservoir???
Prague 2008 60
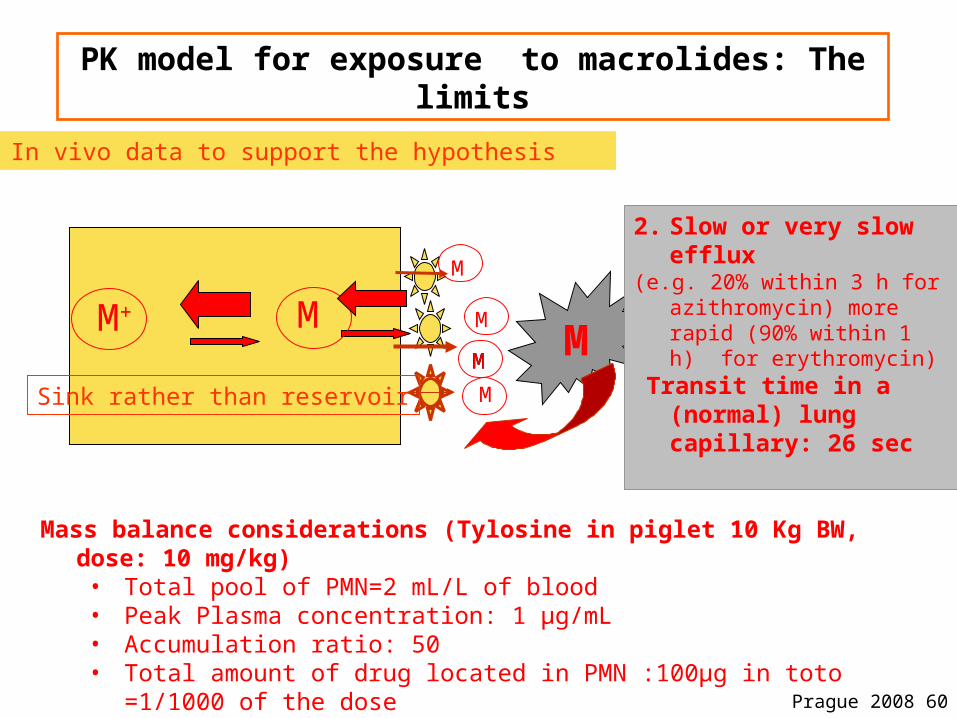
PK model for exposure to macrolides: The limits
M+ M
M
M
MMM
MM
2. Slow or very slow efflux(e.g. 20% within 3 h for
azithromycin) more rapid (90% within 1 h) for erythromycin)
Transit time in a (normal) lung capillary: 26 sec
No In vivo data to support the hypothesis
Mass balance considerations (Tylosine in piglet 10 Kg BW, dose: 10 mg/kg)• Total pool of PMN=2 mL/L of blood• Peak Plasma concentration: 1 µg/mL• Accumulation ratio: 50• Total amount of drug located in PMN :100µg in toto =1/1000 of the dose
Sink rather than reservoir
Prague 2008 61
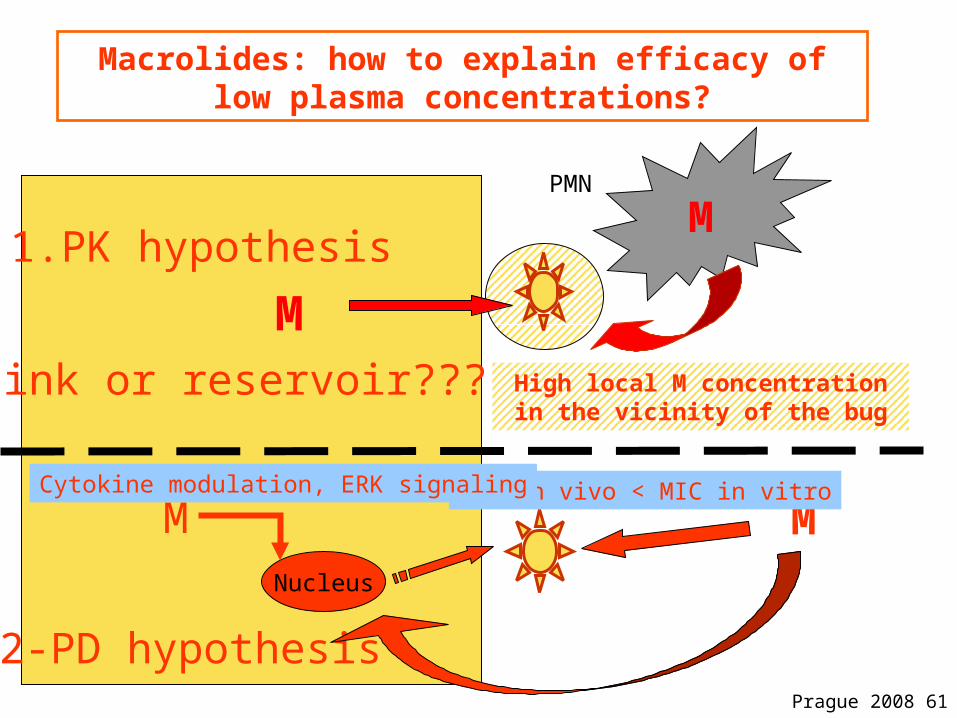
Macrolides: how to explain efficacy of low plasma concentrations?
M
M1.PK hypothesis
2-PD hypothesis
M
PMN
Nucleus
MIC in vivo < MIC in vitroCytokine modulation, ERK signaling
High local M concentration in the vicinity of the bug
M
Sink or reservoir???

Prague 2008 62
Conclusions:
1. In acute infections in non-specialized tissues, where there is no abscess formation, free plasma levels of antibiotics are good predictors of free levels in interstitial fluid
2. PK/PD indices predictive of antibiotic efficacy should be based on free plasma concentration
3. People who truly understand tissue concentration work in corporate marketing departments (Apley, 1999)
Related Documents











