-
8/6/2019 PRADEEP'S_ Brain Tumor
1/32
-
8/6/2019 PRADEEP'S_ Brain Tumor
2/32
DEFINITION A brain tumor is a localized intracraniallesion that occupies space within theskull. Tumors usually grow as a spherical mass, but they can grow
diffusely and infiltrate tissue. The effects of neoplasms occur from the compression and infiltration of tissue. A variety of
physiologic changes result, causing any or all of the following pathophysiologic events:
Increased intracranial pressure (ICP) and cerebral edemaSeizure activity and focal neurologic signsHydrocephalusAltered pituitary function
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
3/32
Primary brain tumors originate fromcells and structures within the brain.
Secondary, or metastatic, braintumors develop from structures outside
the brain and occur in 20% to 40% of allpatients with cancer. Brain tumors rarelymetastasize outside the CNS, butmetastatic lesions to the brain occur
commonly from the lung, breast, lowergastrointestinal tract, pancreas, kidney,and skin
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
4/32
CLASS IFI CA TION B rain tumors may be classified into several groups:
those arising from the coverings of the brain (e.g. Duralmeningioma),
those developing in or on the cranial nerves (eg, acousticneuroma),
those originating within brain tissue (e.g. gliomas), and
Metastatic lesions originating elsewhere in the body.
Tumors of the pituitary and pineal glands and of cerebralblood vessels are also types of\ brain tumors.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
5/32
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
6/32
IN C IDEN C E
It is estimated that there are about 17,000 new cases of primary brain tumors per year, 9,600 in men and 7,400 inwomen (American Cancer Society, 2002).Secondary tumors or metastases to the brain from a
systemic primary cancer are more common.The highest incidence of brain tumors in adults occurs in thefifth, sixth, and seventh decades, with a slightly higher incidence in men.In adults, most brain tumors originate from glial cells (glialcells make up the structure and support system of the brainand spinal cord) and are supra,tentorial (located above thecovering of the cerebellum).
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
7/32
ETIO L OGY
1. The cause of primary brain tumors is unknown.2. The only known risk factor is exposure to ionizing
radiation.3. Both glial and meningeal neoplasms have been linked to
irradiation of the cranium, with a latency period of 10 to 20years after exposure.
4. Additional possible causes have been investigated,& resultsof studies are conflicting and unconvincing; suggestedcauses have included use of cellular telephones, exposureto high-tension wires, use of hair dyes, head trauma,dietary exposure to such factors as nitrates (found in some
processed and barbecued foods), and other sources.12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
8/32
P A THO P HY S IO L OGY
D ue to etiological factors
Growth of intracranial tumors (accompanied by edema)
Compress normal tissue and impair function
Produce neurologic manifestations.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
9/32
-
8/6/2019 PRADEEP'S_ Brain Tumor
10/32
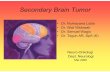
Figure 65-1 indicates common tumor sites in the brain.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
11/32
CL INI CAL M A NIFE S T A TION S I ncreased ICPH eadacheVomitingVisual Disturbances
LOCALIZED SYMPTOMS T he most common focal or localized symptomsare -
H emiparesis,Seizures, andMental status changes.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
12/32
WHENSP ECIFIC R EGION S OF T HE BRA IN AR E AFFECTED, ADDITIONAL L OCAL S IGN S A NDSYMP TO MS
OCCUR , SUCHAS :Sensory and motor abnormalities,Visual alterations,
Alterations in cognition, andLanguage disturbances such asaphasia.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
13/32
correlating the signs and symptoms toknown areas of the brain-
Although some tumors are not easily localized because they lie in so-called silent areas of the brain (i.e.areas in which functions are not definitely determined),many tumors can be localized by correlating the signs andsymptoms to known areas of the brain, as follows:Amotor cortex tumor produces seizure-like movements
localized on one side of the body, called Jacksonian
seizures .An occipital lobe tumor produces visual manifestations:
contra-lateral homonymous hemianopsia (visual loss inhalf of the visual field on the opposite side of the tumor)
and visual hallucinations .12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
14/32
Acerebellar tumor causes dizziness , an ataxic orstaggering gait with a tendency to fall toward the side of the lesion, marked muscle in-coordination , andnystagmus (involuntary rhythmic eye movements), usuallyin the horizontal direction.
A frontal lobe tumor frequently produces personalitydisorders, changes in emotional state and behavior, and anuninterested mental attitude. The patient often becomesextremely untidy and careless and may use obscenelanguage.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
15/32
Acerebello-pontine angle tumor usually originates in thesheath of the acoustic nerve and gives rise to a characteristicsequence of symptoms. T innitus and vertigo appear first ,soon followed by progressive nerve deafness (eighthcranial nerve dysfunction). Numbness and tingling of theface and the tongue occur (due to involvement of the fifthcranial nerve). Later, weakness or paralysis of the facedevelops (seventh cranial nerve involvement). Finally,
because the enlarging tumor presses on the cerebellum ,abnormalities in motor function may be present.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
16/32
DI A GNO S TI C FINDING S A neurologic examination indicates the areas of the CNS
involved.
Computed tomography (CT) scans, enhanced by a contrast agent-gives specific information concerning the number, size, anddensity of the lesions and the extent of secondary cerebral edema.
CT scans can provide information about the ventricular system.
Magnetic resonance imaging (MRI) is the most helpful diagnostictool for detecting brain tumors, particularly smaller lesions, andtumors in the brain stem and pituitary regions, where bone
interferes with CT.
Positron emission tomography (PET) - Is used to supplement MRI.On PET scans, low-grade tumors are associated with hypo-metabolism and high-grade tumors show hyper-metabolism. This
information can be useful in treatment decisions.12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
17/32
C omputer-assisted stereotactic (three-dimensional)biopsy is being used to diagnose deep-seated brain tumors
and to provide a basis for treatment and prognosis.
C erebral angiography provides visualization of cerebral blood vessels and can localize most cerebral tumors.
An electroencephalogram (EEG) to detect an abnormal brain wave in regions occupied by a tumor and is used to
evaluate temporal lobe seizures and assist in ruling out other disorders.C ytologic studies of the C SF may be performed to detectmalignant cells because CNS tumors can shed cells into theCSF.12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
18/32
MEDI CAL M A N A GEMENT 1. C hemotherapy and external-beam radiation therapy2. Autologous bone marrow transplantation
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
19/32
SUR GI CAL M A N A GEMENT The objective of surgical management is -
to remove or destroy the entire tumor without
increasing the neurologic deficit (paralysis, blindness) or
to relieve symptoms by partial removal(decompression).
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
20/32
Trans-sphenoidal microsurgerySUR GI CAL M A N A GEMENT
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
21/32
C raniotomy
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
22/32
R adioisotopes -iodine 131 (131I)
131 I
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
23/32
G amma knife
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
24/32
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
25/32
N URS ING M A N A GEMENT Preoperative Medical and Nursing Management.1. Instruct patient and family about the necessity and
importance of diagnostic tests to determine the exactlocation of the tumor.
2. Monitor and record vital signs and neurological statusaccurately q2-4h, or as ordered. Report changes to
professional nurse immediately.3. Institute measures to prevent inadvertent increases in
intracranial pressure.1. Elevate head of bed 30.2. Stool softeners to prevent straining at stool (which increases
intracranial pressure).
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
26/32
4. Institute seizure precautions at patient's bedside. (Tongue blade airway.)
5. Supportive nursing care is given depending upon the patient's symptoms and ability to perform activities of
daily living.
6. Administer all doses of steroids and antiepileptic agentson time.
Withholding steroids can result in adrenal crisis.Withholding of antiepileptic agents frequently
precipitates seizure.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
27/32
Post Operative Nursing C areC onsiderations.a.Meticulous nursing management and care aimed at
prevention of postoperative complications are imperativefor the patient's survival.
b.Accurately monitor and record all vital signs andneurological signs.i. Postoperative cerebral edema peaks between 48 and 60 hours
following surgery.
ii.Patient may be lucid during first 24 hours, then experience adecrease in level of consciousness during this time.
c.Administer artificial tears (eye drops) as ordered, to prevent corneal ulceration in the comatose patient.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
28/32
d. Maintain skin integrity.e. Bone flap may not have been replaced over surgical site;
turning patient to the affected side, if the flap has beenremoved, can cause irreversible damage in the first 72hours.
f. Maintain head of bed at 30elevation.g. Perform passive range of motion exercises to all
extremities every 2-4 hours.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
29/32
-
8/6/2019 PRADEEP'S_ Brain Tumor
30/32
L. Continuously talk to the patient while providing care,reorienting him to person, place, and time.
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
31/32
12/22/2010 Prinz
-
8/6/2019 PRADEEP'S_ Brain Tumor
32/32
12/22/2010 Prinz