Not for Distribution or Citation Draft 2, December 6, 2005 PRACTICE GUIDELINE FOR THE TREATMENT OF PATIENTS WITH OBSESSIVE-COMPULSIVE DISORDER WORK GROUP ON OBSESSIVE-COMPULSIVE DISORDER Lorrin M. Koran, M.D., Chair Gregory L. Hanna, M.D. Gerald Nestadt, M.D. Eric Hollander, M.D. Helen Blair Simpson, M.D., Ph.D. STEERING COMMITTEE ON PRACTICE GUIDELINES John S. McIntyre, M.D., Chair Sara C. Charles, M.D., Vice-Chair Daniel J. Anzia, M.D. James E. Nininger, M.D. Ian A. Cook, M.D. Paul Summergrad, M.D. Molly T. Finnerty, M.D. Sherwyn M. Woods, M.D., Ph.D. Bradley R. Johnson, M.D. Joel Yager, M.D. AREA AND COMPONENT LIAISONS Robert Pyles, M.D. (Area I) C. Deborah Cross, M.D. (Area II) Roger Peele, M.D. (Area III) Philip M. Margolis, M.D. (Area IV) John P.D. Shemo, M.D. (Area V) Lawrence Lurie, M.D. (Area VI) David L. Duncan, M.D. (Area VII) Mary Ann Barnovitz, M.D. Sheila Hafter Gray, M.D. Sunil Saxena, M.D. Tina Tonnu, M.D. STAFF Robert Kunkle, M.A., Senior Program Manager Amy B. Albert, B.A., Assistant Project Manager Laura J. Fochtmann, M.D., Medical Editor, Practice Guidelines Claudia Hart, Director, Dept. of Quality Improvement and Psychiatric Services Darrel Regier, M.D., M.P.H., Director, Division of Research Comments on this draft are due Wednesday, January 11, 2006, via: E-mail: [email protected] Mail: Amy Albert Dept. of Quality Improvement and Psychiatric Services American Psychiatric Association 1000 Wilson Blvd., Ste. 1825 Arlington, VA 22209-3901 Ph: 703.907.8605 Fax: 703.907.7823 (attn: Amy Albert)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Not for Distribution or Citation Draft 2, December 6, 2005
PRACTICE GUIDELINE FOR THE TREATMENT OF PATIENTS WITH OBSESSIVE-COMPULSIVE DISORDER
WORK GROUP ON OBSESSIVE-COMPULSIVE DISORDER
Lorrin M. Koran, M.D., Chair Gregory L. Hanna, M.D. Gerald Nestadt, M.D.
Eric Hollander, M.D. Helen Blair Simpson, M.D., Ph.D.
STEERING COMMITTEE ON PRACTICE GUIDELINES John S. McIntyre, M.D., Chair
Sara C. Charles, M.D., Vice-Chair Daniel J. Anzia, M.D. James E. Nininger, M.D.
Ian A. Cook, M.D. Paul Summergrad, M.D. Molly T. Finnerty, M.D. Sherwyn M. Woods, M.D., Ph.D.
Bradley R. Johnson, M.D. Joel Yager, M.D.
AREA AND COMPONENT LIAISONS Robert Pyles, M.D. (Area I)
C. Deborah Cross, M.D. (Area II) Roger Peele, M.D. (Area III)
Philip M. Margolis, M.D. (Area IV) John P.D. Shemo, M.D. (Area V) Lawrence Lurie, M.D. (Area VI)
David L. Duncan, M.D. (Area VII) Mary Ann Barnovitz, M.D. Sheila Hafter Gray, M.D.
Sunil Saxena, M.D. Tina Tonnu, M.D.
STAFF
Robert Kunkle, M.A., Senior Program Manager Amy B. Albert, B.A., Assistant Project Manager
Laura J. Fochtmann, M.D., Medical Editor, Practice Guidelines Claudia Hart, Director, Dept. of Quality Improvement and Psychiatric Services
Darrel Regier, M.D., M.P.H., Director, Division of Research
Comments on this draft are due Wednesday, January 11, 2006, via: E-mail: [email protected] Mail: Amy Albert
Dept. of Quality Improvement and Psychiatric Services American Psychiatric Association 1000 Wilson Blvd., Ste. 1825 Arlington, VA 22209-3901 Ph: 703.907.8605
Fax: 703.907.7823 (attn: Amy Albert)

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
2
CONTENTS Statement of Intent.............................................................................................................. 5 Guide to Using This Practice Guideline ............................................................................. 6 Overview of Guideline Development Process.................................................................... 7 PART A. TREATMENT RECOMMENDATIONS FOR PATIENTS WITH OBSESSIVE-COMPULSIVE DISORDER (OCD) ........................................................... 9 I. EXECUTIVE SUMMARY OF TREATMENT RECOMMENDATIONS ............... 9 II. FORMULATION AND IMPLEMENTATION OF A TREATMENT PLAN .......... 9
II.A. Psychiatric Management..................................................................................... 9 II.A.1. Establish a Therapeutic Alliance .............................................................. 10 II.A.2. Assess the Symptoms and Make a Diagnosis ........................................... 11 II.A.3. Consider Rating the Severity of OCD Symptoms and of Co-occurring Conditions and Their Effects on the Patient’s Functioning...................................... 15 II.A.4. Evaluate the Safety of Others ................................................................... 16 II.A.5. Complete the Psychiatric Assessment ...................................................... 17 II.A.6. Establish Goals for Treatment .................................................................. 21 II.A.7. Establish the Appropriate Setting for Treatment ...................................... 22 II.A.8. Enhance Treatment Adherence ................................................................. 23 II.A.9. Provide Education to the Patient and, When Appropriate, to the Family. 25 II.A.10. Coordinate the Patient’s Care With Other Providers of Care and Social Agencies 25
II.B. Acute Phase....................................................................................................... 26 II.B.1. Choice of Initial Treatment Modality ....................................................... 26 II.B.2. Choice of Specific Pharmacologic Treatment .......................................... 28
II.B.2.a. Implementation of Pharmacotherapy................................................ 29 II.B.2.b. Managing Medication Side Effects................................................... 35
II.B.3. Choice of a Specific Form of Psychotherapy ........................................... 37 II.B.4. Implementation of Cognitive-Behavioral Therapies ................................ 37 II.B.5. Monitor the Patient’s Psychiatric Status ................................................... 39 II.B.6. When and Whether to Change Treatments ............................................... 40 II.B.7. Pursuing Sequential Treatment Trials....................................................... 41
II.B.7.a. Adding Psychotherapy to an SRI...................................................... 44 II.B.7.b. Adding an SRI to Psychotherapy...................................................... 44 II.B.7.c. Switching to a Different SRI or to the SNRI Venlafaxine................ 45 II.B.7.d. Augmenting With an Antipsychotic Medication .............................. 45 II.B.7.e. Switching to Mirtazapine.................................................................. 47 II.B.7.f. Augmenting an SRI With Other Pharmacotherapies ........................ 47 II.B.7.g. Approaches Reported in Case Reports, Case Series, Uncontrolled Trials, or Small Controlled Trials ......................................................................... 48
II.C. Discontinuation of Active Treatment................................................................ 50 III. SPECIFIC CLINICAL FEATURES INFLUENCING THE TREATMENT PLAN . 51
III.A. Psychiatric Features ............................................................................................ 52 III.A.1. Chronic Motor Tics................................................................................... 53 III.A.2. Tourette’s Disorder ................................................................................... 53 III.A.3. Major Depression...................................................................................... 53 III.A.4. Bipolar Disorder........................................................................................ 54
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
3
III.A.5. Panic Disorder........................................................................................... 54 III.A.6. Social Phobia (Social Anxiety Disorder).................................................. 55 III.A.7. Schizophrenia............................................................................................ 55 III.A.8. Substance Use Disorders........................................................................... 56 III.A.9. Personality Disorders ................................................................................ 56 III.A.10. General Medical Conditions Inducing OCD......................................... 57
III.B. Demographic and Psychosocial Factors ....................................................... 58 III.B.1. Children and Adolescents ......................................................................... 58 III.B.2. Ethnicity.................................................................................................... 58 III.B.3. Pregnancy and Breast-Feeding ................................................................. 59
III.C. Treatment Implications of Concurrent General Medical Disorders ............. 61 PART B: BACKGROUND INFORMATION AND REVIEW OF AVAILABLE EVIDENCE....................................................................................................................... 62 IV. DISEASE DEFINITION, EPIDEMIOLOGY, NATURAL HISTORY, COURSE, AND GENETICS.............................................................................................................. 62
IV.A. Disease Definition......................................................................................... 62 IV.B. Epidemiology................................................................................................ 64 IV.C. Natural History and Course .......................................................................... 66 IV.D. Genetics......................................................................................................... 67
IV.D.1. Twin and Family Studies ...................................................................... 67 IV.D.2. Genetic Linkage and Candidate Gene Studies...................................... 68
V. REVIEW AND SYNTHESIS OF AVAILABLE EVIDENCE................................... 69 V.A. Medications....................................................................................................... 69
V.A.1. Clomipramine ........................................................................................... 70 V.A.1.a. Intravenous Clomipramine................................................................ 74 V.A.1.b. Clomipramine as an Augmentation Agent........................................ 74
V.A.2. SSRIs......................................................................................................... 75 V.A.2.a. Fluvoxamine ..................................................................................... 75 V.A.2.b. Fluoxetine ......................................................................................... 79 V.A.2.c. Paroxetine ......................................................................................... 82 V.A.2.d. Sertraline ........................................................................................... 83 V.A.2.e. Citalopram......................................................................................... 85 V.A.2.f. Venlafaxine ....................................................................................... 86
V.A.3. Other Antidepressants............................................................................... 88 V.A.3.a. Monoamine Oxidase Inhibitors......................................................... 88 V.A.3.b. Tricyclic Antidepressants.................................................................. 89 V.A.3.c. Trazodone ......................................................................................... 89
V.A.4. Antipsychotics........................................................................................... 90 V.A.4.a. Monotherapy ..................................................................................... 90 V.A.4.b. Augmentation.................................................................................... 91 V.A.4.c. Haloperidol ....................................................................................... 92 V.A.4.d. Risperidone ....................................................................................... 92 V.A.4.e. Olanzapine ........................................................................................ 93 V.A.4.f. Quetiapine ......................................................................................... 94 V.A.4.g. Other Antipsychotic Agents.............................................................. 96
V.A.5. Other Agents ............................................................................................. 96
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
4
V.A.5.a. Adrenergic Agents ............................................................................ 96 V.A.5.b. Benzodiazepines ............................................................................... 97 V.A.5.c. Buspirone .......................................................................................... 97 V.A.5.d. Inositol .............................................................................................. 98 V.A.5.e. Lithium.............................................................................................. 98 V.A.5.f. Mirtazapine ....................................................................................... 99 V.A.5.g. Other Medications............................................................................. 99
V.B. Other Somatic Therapies................................................................................. 101 V.B.1. Transcranial Magnetic Stimulation (TMS)............................................. 102 V.B.2. Electroconvulsive Therapy (ECT) .......................................................... 104 V.B.3. Deep Brain Stimulation........................................................................... 105 V.B.4. Neurosurgery........................................................................................... 107
V.C. Psychotherapies............................................................................................... 109 V.C.1. Exposure Therapy ................................................................................... 109
V.C.1.a. Randomized Controlled Trials Comparing Exposure Therapy to a Non-Active Treatment ........................................................................................ 110 V.C.1.b. Factors that Affect Outcome From Exposure Therapy................... 113 V.C.1.c. Long-Term Outcome From Exposure Therapy .............................. 114 V.C.1.d. Can Exposure Therapy Augment SRI Response? .......................... 115
V.C.2. Cognitive Therapy .................................................................................. 115 V.C.2.a. Is Cognitive Therapy (Without Exposure) Efficacious for OCD?.. 115 V.C.2.b. Is Cognitive Therapy as Efficacious as Exposure Therapy for OCD? 116 V.C.2.c. Does the Addition of Cognitive Therapy Make Exposure Therapy More Effective? .................................................................................................. 120
V.C.3. Group and Multifamily Behavioral Treatment ....................................... 121 V.C.4. Computer-Assisted Behavioral Therapy................................................. 123 V.C.5. Kundalini Yoga....................................................................................... 123
V.D. Combined Therapy.......................................................................................... 124 V.E. Discontinuation of Active Treatment.............................................................. 128
PART C. FUTURE RESEARCH NEEDS ..................................................................... 130 Acknowledgments........................................................................................................... 132 Individuals and organizations that submitted comments ................................................ 133 Appendix A..................................................................................................................... 133 Appendix B ..................................................................................................................... 139 References....................................................................................................................... 139

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
5
STATEMENT OF INTENT 1
This practice guideline is based on available evidence and clinical consensus and offers 2
recommendations to help psychiatrists in assessing and treating adult patients with 3
obsessive compulsive disorder (OCD). This report is not intended to be construed or to 4
serve as a standard of medical care. Standards of medical care are determined on the basis 5
of all clinical data available for an individual patient and are subject to change as 6
scientific knowledge and technology advance and practice patterns evolve. These 7
parameters of practice should be considered guidelines only. Adherence to them will not 8
ensure a successful outcome for every individual, nor should they be construed as 9
including all proper methods of care or excluding other acceptable methods of care aimed 10
at the same results. The ultimate judgment regarding a particular clinical procedure or 11
treatment plan must be made by the psychiatrist in light of the clinical data presented by 12
the patient and the diagnostic and treatment options available. 13
This practice guideline has been developed by psychiatrists who are in active 14
clinical practice. In addition, some contributors are primarily involved in research or 15
other academic endeavors. It is possible that through such activities some contributors 16
have received income related to treatments discussed in this guideline. A number of 17
mechanisms are in place to minimize the potential for producing biased recommendations 18
due to conflicts of interest. The guideline has been extensively reviewed by members of 19
APA as well as by representatives from related fields. Contributors and reviewers have 20
all been asked to base their recommendations on an objective evaluation of available 21
evidence. Any contributor or reviewer who has a potential conflict of interest that may 22
bias (or appear to bias) his or her work has been asked to notify the APA Department of 23
Quality Improvement and Psychiatric Services. This potential bias is then discussed with 24
the work group chair and the chair of the Steering Committee on Practice Guidelines. 25
Further action depends on the assessment of the potential bias. 26
This practice guideline was approved in MONTH YEAR and published in 27
MONTH YEAR. 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
6
GUIDE TO USING THIS PRACTICE GUIDELINE 1
The Practice Guideline for the Treatment of Patients With Obsessive-Compulsive 2
Disorder consists of three parts (Parts A, B, and C) and many sections, not all of which 3
will be equally useful for all readers. The following guide is designed to help readers find 4
the sections that will be most useful to them. 5
Part A, “Treatment Recommendations,” is published as a supplement to the 6
American Journal of Psychiatry and contains general and specific treatment 7
recommendations. Section I summarizes the key recommendations of the guideline and 8
codes each recommendation according to the degree of clinical confidence with which 9
the recommendation is made. Section II is a guide to the formulation and implementation 10
of a treatment plan for the individual patient. Section III, “Specific Clinical Features 11
Influencing the Treatment Plan,” discusses a range of clinical considerations that could 12
alter the general recommendations discussed in Section I. 13
Part B, “Background Information and Review of Available Evidence,” and Part C, 14
“Future Research Needs,” are not included in the American Journal of Psychiatry 15
supplement but are provided with Part A in the complete guideline, which is available in 16
print format from American Psychiatric Publishing, Inc., and online through the 17
American Psychiatric Association (http://www.psych.org). Part B provides an overview 18
of OCD, including general information on natural history, course, and epidemiology. It 19
also provides a structured review and synthesis of the evidence that underlies the 20
recommendations made in Part A. Part C draws from the previous sections and 21
summarizes areas for which more research data are needed to guide clinical decisions.22
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
7
OVERVIEW OF GUIDELINE DEVELOPMENT 1
PROCESS 2
This practice guideline was developed under the auspices of the Steering Committee on 3
Practice Guidelines. The development process is detailed in a document available from 4
the APA Department of Quality Improvement and Psychiatric Services: the “APA 5
Guideline Development Process.” Key features of this process include the following: 6
• A comprehensive literature review to identify all relevant randomized clinical trials as 7
well as less rigorously designed clinical trials and case series when evidence from 8
randomized trials was unavailable. 9
• Development of evidence tables that reviewed the key features of each identified 10
study, including funding source, study design, sample sizes, subject characteristics, 11
treatment characteristics and treatment outcomes. 12
• Initial drafting of the guideline by a work group that included psychiatrists with 13
clinical and research expertise in OCD. 14
• Production of multiple revised drafts with widespread review; XXXX organizations 15
and XXXX individuals submitted significant comments. 16
• Approval by the APA Assembly and Board of Trustees. 17
• Planned revisions at regular intervals. 18
Relevant literature was identified through a PubMed literature search for articles 19
published between 1966 and December 2004 using the key words “Obsessive-20
Compulsive Disorder”[MeSH] OR “Compulsive Behavior”[MeSH]) OR 21
(“obsession”[All Fields] OR “obsessional”[All Fields] OR “obsessions”[All Fields] OR 22
“obsessive”[All Fields]) OR (“compulsion”[All Fields] OR “compulsions”[All Fields] 23
OR “compulsive”[All Fields]. This yielded 13182 references of which 10756 were in 24
English. Additional, less formal, literature searches were conducted by APA staff and 25
individual work group members. 26
This document represents a synthesis of current scientific knowledge and rational 27
clinical practice. It strives to be as free as possible of bias toward any theoretical 28
approach to treatment. The recommendations are based on the best available data and 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
8
clinical consensus with regard to a particular clinical decision. The summary of treatment 1
recommendations <<not yet included in this draft>> is <<will be>> keyed according to 2
the level of confidence with which each recommendation is made. In addition, each 3
reference is followed by a letter code in brackets that indicates the nature of the 4
supporting evidence.5

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
9
PART A. TREATMENT RECOMMENDATIONS FOR 1
PATIENTS WITH OBSESSIVE-COMPULSIVE 2
DISORDER (OCD) 3
The physician should look upon the patient as a besieged city and try to rescue him with 4 every means that art and science place at his command. 5
Alexander of Tralles, AD 525–605 6
I. EXECUTIVE SUMMARY OF TREATMENT 7
RECOMMENDATIONS 8
<<Note to Reviewers: The Executive Summary will be written after draft 2 is 9
reviewed.>> 10
II. FORMULATION AND IMPLEMENTATION OF A 11
TREATMENT PLAN 12
II.A._PSYCHIATRIC MANAGEMENT 13
The patient should be managed the way the doctor or a member of his family would wish 14 to be treated if he were that patient in that bed at that time. 15
Robert F. Loeb, 1895–?, U.S. physician 16 Attributed 17
18 Obsessive-compulsive disorder (OCD) that motivates seeking care is usually a chronic 19
illness with a waxing and waning course. With appropriate treatment, OCD usually 20
improves over weeks or months. Offering treatment is indicated when symptoms interfere 21
with functioning and cause distress. Attaining complete symptom remission is 22
uncommon. As a result, treatment is usually ongoing, and treatment planning and 23
psychiatric management will be iterative processes adapted to the patient’s current status 24
and response to previous interventions. Psychiatric management consists of a broad 25
collection of professional actions and interventions designed to benefit the patient. These 26
actions and interventions include providing: 27

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
10
• pharmacotherapy and psychotherapy in the appropriate setting, as indicated by 1
patient preference and clinical judgment; 2
• guidance regarding educational materials in published form and on the Web 3
(Appendix A); and 4
• information about local support groups (Appendix A). 5
In the case of children, materials should be provided to the parents. 6
Psychiatric management should be offered to all patients with OCD throughout 7
the course of illness at an intensity consistent with the patient’s needs and desires. The 8
components of psychiatric management and the stages of illness are described in more 9
detail below. 10
II.A.1. ______Establish a Therapeutic Alliance 11
The essential unit of medical practice is the occasion when, in the intimacy of the 12 consulting room or sick room, a person who is ill, or believes himself to be ill, seeks the 13 advice of a doctor whom he trusts. 14
Sir James Calvert Spence, 1892–1954 15 The Purpose and Practice of Medicine, Ch. 18 16
17
As in all of medicine, the physician first attempts to establish and then to maintain a 18
therapeutic alliance, so that care is a mutual endeavor. The therapeutic alliance allows the 19
psychiatrist to obtain the information needed to plan effective treatment. The alliance 20
allows the patient to trust the clinician and helps motivate adherence to treatments 21
collaboratively planned. Tailoring one’s communication style to the patient’s needs, 22
along continua from detailed to broad brush, from biologically to psychosocially framed, 23
and from warm to neutral, is important, as is considering other aspects of both the 24
transference and the countertransference. The excessive doubting characteristic of OCD 25
may require special approaches to building the alliance. For example, the clinician may 26
need to allow the patient more time to consider treatment decisions and may need to 27
repeat explanations several times and at several visits. The psychiatrist should explore 28
why the patient has come to him or her specifically, and why now. What does the patient 29
want and expect? How are these desires and expectations affected by the patient’s 30
cultural background, beliefs about the illness (its cause, effects, and mechanisms) and 31
experience with past treatments? 32
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
11
II.A.2. ______Assess the Symptoms and Make a Diagnosis 1
He is a great physician, who, above other men, understands diagnosis. 2 Jacob Bigelow, 1786–1879 3
Nature in Disease, Ch. 2 4 5 The psychiatrist should establish the diagnosis according to the DSM-IV-TR criteria 6
(Table 1).7

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
12
TABLE 1. DSM-IV-TR Diagnostic Criteria for 300.3 Obsessive-Compulsive Disorder 1 A. Either obsessions or compulsions: 2
Obsessions as defined by (1), (2), (3), and (4): 3 1. recurrent and persistent thoughts, impulses, or images that are experienced, at some time during the 4
disturbance, as intrusive and inappropriate and that cause marked anxiety or distress 5 2. the thoughts, impulses, or images are not simply excessive worries about real-life problems 6 3. the person attempts to ignore or suppress such thoughts, impulses, or images, or to neutralize them 7
with some other thought or action 8 4. the person recognizes that the obsessional thoughts, impulses, or images are a product of his or her 9
own mind (not imposed from without as in thought insertion) 10 Compulsions as defined by (1) and (2): 11
1. repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, 12 repeating words silently) that the person feels driven to perform in response to an obsession, or 13 according to rules that must be applied rigidly 14
2. the behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded 15 event or situation; however, these behaviors or mental acts either are not connected in a realistic way 16 with what they are designed to neutralize or prevent or are clearly excessive 17
B. At some point during the course of the disorder, the person has recognized that the obsessions or compulsions 18 are excessive or unreasonable. Note: This does not apply to children. 19
C. The obsessions or compulsions cause marked distress, are time consuming (take more than 1 hour a day), or 20 significantly interfere with the person's normal routine, occupational (or academic) functioning, or usual social 21 activities or relationships. 22
D. If another Axis I disorder is present, the content of the obsessions or compulsions is not restricted to it (e.g., 23 preoccupation with food in the presence of an Eating Disorder; hair pulling in the presence of Trichotillomania; 24 concern with appearance in the presence of Body Dysmorphic Disorder; preoccupation with drugs in the presence 25 of a Substance Use Disorder; preoccupation with having a serious illness in the presence of Hypochondriasis; 26 preoccupation with sexual urges or fantasies in the presence of a Paraphilia; or guilty ruminations in the presence 27 of Major Depressive Disorder). 28
E. The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) 29 or a general medical condition. 30
31 Specify if: 32 With Poor Insight: if, for most of the time during the current episode, the person does not recognize that the obsessions 33 and compulsions are excessive or unreasonable. 34 35 <<AA to request permission from APPI to reprint DSM criteria; note to self: move table if citation is added to maintain ref order.>> 36
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
13
Screening questions might include some of the following: Are you are troubled by 1
unpleasant thoughts that you can’t get rid of? Do you worry that you might impulsively 2
harm someone? Do you have to wash your hands or check things over and over? Do you 3
worry about whether you performed religious rituals correctly or have been immoral? Do 4
you need things arranged symmetrically or in a very exact order? Do you have trouble 5
discarding things, so that your house is quite cluttered? In the absence of screening, OCD 6
is likely to be underdiagnosed (Fireman et al. 2001). 7
The psychiatrist must differentiate obsessions and compulsions from similar 8
symptoms found in other disorders. Unlike obsessions, depressive ruminations are not 9
experienced as inconsistent with one’s self-image or values. They often focus on past 10
events but may concern possible current or future negative events or anticipated failures. 11
Their subject matter usually concerns self-criticism, guilt, or regret. The worries of 12
generalized anxiety disorder focus on real life problems and do not lead to compulsive 13
rituals. The individual is troubled more by the possibility of the feared events occurring 14
than by the presence of the fears. Generalized anxiety disorder may also present as a 15
vague but troubling feeling of foreboding, whereas OCD obsessions always have clear 16
content. The intrusive thoughts and images of posttraumatic stress disorder are 17
replays of actual events not anticipations of future events. Persons with OCD may 18
partially or fully lose insight into the irrationality of their obsessions and occasionally 19
become delusional. Obsessions with delusional conviction can be distinguished from 20
schizophrenic and manic delusions by the absence of the signs and symptoms of these 21
disorders. Moreover, delusional obsessions will have typical OCD content rather than 22
content related to paranoia, grandiosity, ideas of reference, or to delusions of being 23
controlled. 24
OCD can be differentiated from hypochondriasis by noting that the 25
hypochondriac’s fear or belief regarding serious disease arises from misinterpretation of 26
ordinary bodily signs and symptoms. In OCD such fears arise from external stimuli, e.g., 27
a patient fearing he has contracted AIDS because he was served with a waiter wearing a 28
bandage, possibly exposing him to blood. In body dysmorphic disorder, the recurrent 29
and intrusive preoccupations are limited to the fear or belief that one is ugly or exhibits 30
some disturbing defect visible to others. In anorexia nervosa and bulimia nervosa, the 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
14
intrusive ideation and irrational behaviors center on weight and its effects on self-1
evaluation. In contrast to paraphilic thoughts and urges, OCD-related sexual obsessions 2
or images regarding a current or past partner are not accompanied by stalking behavior 3
and are ego-dystonic, as are OCD-generated thoughts or images of having sex with a 4
child. 5
Differentiating compulsive urges to harm an infant that occur as postpartum 6
symptoms of OCD from superficially similar symptoms of postpartum depression is 7
critical. The OCD urges are experienced as inconsistent with one’s self, are resisted, and 8
are not accompanied by depressed mood. The impulses that arise in postpartum 9
depression may be experienced as justified, may not be strongly resisted, and are 10
accompanied by depressed mood and other symptoms diagnostic of major depression. In 11
postpartum depression, steps to protect the infant may be necessary. 12
Differentiating compulsions from the complex vocal or motor tics sometimes 13
seen in Tourette’s Disorder can be difficult. Tics, however, are purposeless; unlike 14
compulsions, they are not aimed at relieving anxiety or at preventing or undoing an 15
undesired event. DSM-IV (American Psychiatric Association 1994) defines a tic as “a 16
sudden, rapid, recurrent, nonrhythmic, [and] stereotyped motor movement or 17
vocalization.” Tics are often preceded by premonitory sensations such as muscular 18
tension and may involve repeating an action until an unpleasant, localized physical 19
tension or a sense of incompleteness is relieved (Mansueto & Keuler 2005). Complex 20
motor tics can take the form of arranging, ordering, making symmetrical, or touching 21
(Mansueto & Keuler 2005). Repeating an action until “it feels right,” e.g., repeatedly 22
closing a door until the right sound or sensation of closure is achieved, may be a complex 23
tic or a compulsion, or reflect elements of both symptoms. Tics may be distinguished 24
from “tic-like” compulsions by whether the patient attaches a meaning or purpose to the 25
behavior (Holzer et al. 1994). The index of suspicion for complex tics should be raised in 26
individuals with a personal or family history of motor or phonic tics; a history of 27
hypersensitivity to sensations associated with scratchy fabrics, the touch of clothing 28
labels, or to uneven shoelaces or socks; and individuals with comorbid diagnoses of 29
attention deficit disorder or learning disorder (Mansueto & Keuler 2005). 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
15
Differentiating OCD from obsessive-compulsive personality disorder (OCPD) 1
may be difficult. Fundamentally, the person with OCPD experiences the concerns and 2
behaviors as part of the normal self and does not resist them, but, to the contrary, 3
considers them valued attributes. Despite the possibility that OCPD traits often irritate 4
those around the individual, the individual himself or herself has no desire to change 5
these traits. Hoarding, scrupulosity, perfectionism, and preoccupation with rules, order, 6
and lists may occur in both disorders. In OCD, anxiety about feared consequences of 7
foregoing compulsive behaviors is prominent; in OCPD, the focus is on “doing things my 8
way, the right way,” i.e., on the need for control. In OCD, perfectionism and 9
preoccupation with rules is focal, limited to feared events, whereas in OCPD these traits 10
globally color the individual’s attitudes and behavior. 11
II.A.3. ______Consider Rating the Severity of OCD Symptoms 12 and of Co-occurring Conditions and Their Effects 13 on the Patient’s Functioning 14
A physician is obligated to consider more than a diseased organ, more even than the 15 whole man—he must view the man in his world. 16
Harvey Cushing, 1869–1939 17 Man Adapting, Ch. 12 (René J. Dubois) 18
19 Use of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) Symptom Checklist 20
(Goodman et al. 1989c) (Appendix B), which allows the recording of current and past 21
symptoms, or the 18-item Obsessive-Compulsive Inventory (Foa et al. 2002) may be 22
helpful. The Y-BOCS Symptom Checklist lists 40 obsessions, 15 behavioral 23
compulsions, 5 mental compulsions, and 9 miscellaneous compulsions. The psychiatrist 24
should consider using a rating scale such as the 10-item Y-BOCS (Goodman et al. 1989b; 25
Goodman et al. 1989c) (Appendix B) to record baseline severity, since this provides a 26
way to measure response to treatment. The Y-BOCS rating can also be compared to the 27
patient’s and the family’s impressions of severity. The Y-BOCS measures separately for 28
obsessions and compulsions, time spent or taken, and the degrees of interference with 29
functioning, distress, resistance to the symptoms, and success in resistance. A simpler 30
measure is a visual analogue scale in the form of a thermometer with the bottom labeled 31
“no OCD symptoms” and the top labeled “incapacitating OCD symptoms.” Encouraging 32
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
16
the patient to use a rating scale will help him or her become a better self-observer. If a 1
rating scale is not used, the psychiatrist should document the patient’s estimate of the 2
number of hours per day spent in obsessing and in performing compulsive behaviors, and 3
the degree of effort applied to resisting the thoughts and behaviors. Recording items or 4
situations that the patient actively avoids because of OCD also provides a useful baseline 5
against which change can be measured. 6
For monitoring depression, the clinician might consider the Hamilton Depression 7
Rating Scale (HAM-D) (HAMILTON 1960), the 10-item Montgomery-Asberg 8
Depression Rating Scale (MADRS) (Montgomery & Asberg 1979), or the 30-item 9
Inventory of Depressive Symptoms–Clinician Version (IDS–C) or the shorter 16-item 10
version (QIDS–C) (Trivedi et al. 2004). Self-rated scales can be as simple as visual 11
analog scales or severity “1 to 10” scales measuring symptoms of interest. Self-rated 12
scales that may be useful for monitoring depression include the self-rated Beck 13
Depression Inventory (BDI) (BECK et al. 1961), Zung Depression Scale (Zung 1968), or 14
the patient-rated versions of the IDS or QIDS (Trivedi et al. 2004). 15
OCD symptoms may seriously impair interpersonal relationship, vocational 16
ability, marital and family relationships, and child-rearing capacities. Thus, including a 17
rating of disability may be useful, e.g., the self-rated, three-item Sheehan Disability Scale 18
(SDS) (Leon et al. 1992; Sheehan et al. 1996), which records disability in the domains of 19
work, family, and social relationships. Some patients, however, may not accurately 20
recognize the degree of their disability until after successful treatment. For most patients, 21
OCD seriously impairs quality of life (Koran 2000). A rating of the patient’s quality of 22
life, using a scale such as the Q-LES-Q (Endicott et al. 1993) or the more detailed 23
WHOQOL-100 (Skevington et al. 1999) can provide a broader measure of disease impact 24
and of the results of treatment. 25
II.A.4. ______Evaluate the Safety of Others 26
The psychiatrist should evaluate the safety of others. In addition to evaluating safety in 27
postpartum situations, this will entail inquiring about whether the patient has become 28
violent when others have interfered with the performance of compulsive rituals. Such 29
violence is rare. The patient may experience and fear ego-dystonic homicidal impulses or 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
17
thoughts, or urges or images related to sexually abusing a child. Although acting on 1
agressive impulses or thoughts has not been reported, the patient may fear loss of control 2
and engage in extensive avoidance rituals. The psychiatrist should recall, however, that 3
individuals with OCD are not immune to co-occurring antisocial personality disorder, 4
intermittent explosive disorder, substance abuse disorders, or other disorders that can 5
give rise to violent acts. 6
II.A.5. ______Complete the Psychiatric Assessment 7
More mistakes are made from want of a proper examination than for any other reason. 8 Russell John Howard, 1875–1942 9
Quoted by F.B. St. Clair, Strange in The Hip, Ch 9 10 11 The psychiatrist should evaluate all symptoms and their effects on the patient’s sense of 12
well-being, functioning (relationships with family and friends, work/school performance, 13
household management, self-care), and quality of life (relationships, living situation, use 14
of leisure time). The psychiatrist should assess the role of the family in precipitating, 15
maintaining, and exacerbating symptoms and in facilitating treatment. Assessing the 16
family’s understanding of the fact that the patient is ill and of the potential treatments is 17
also important for treatment planning. 18
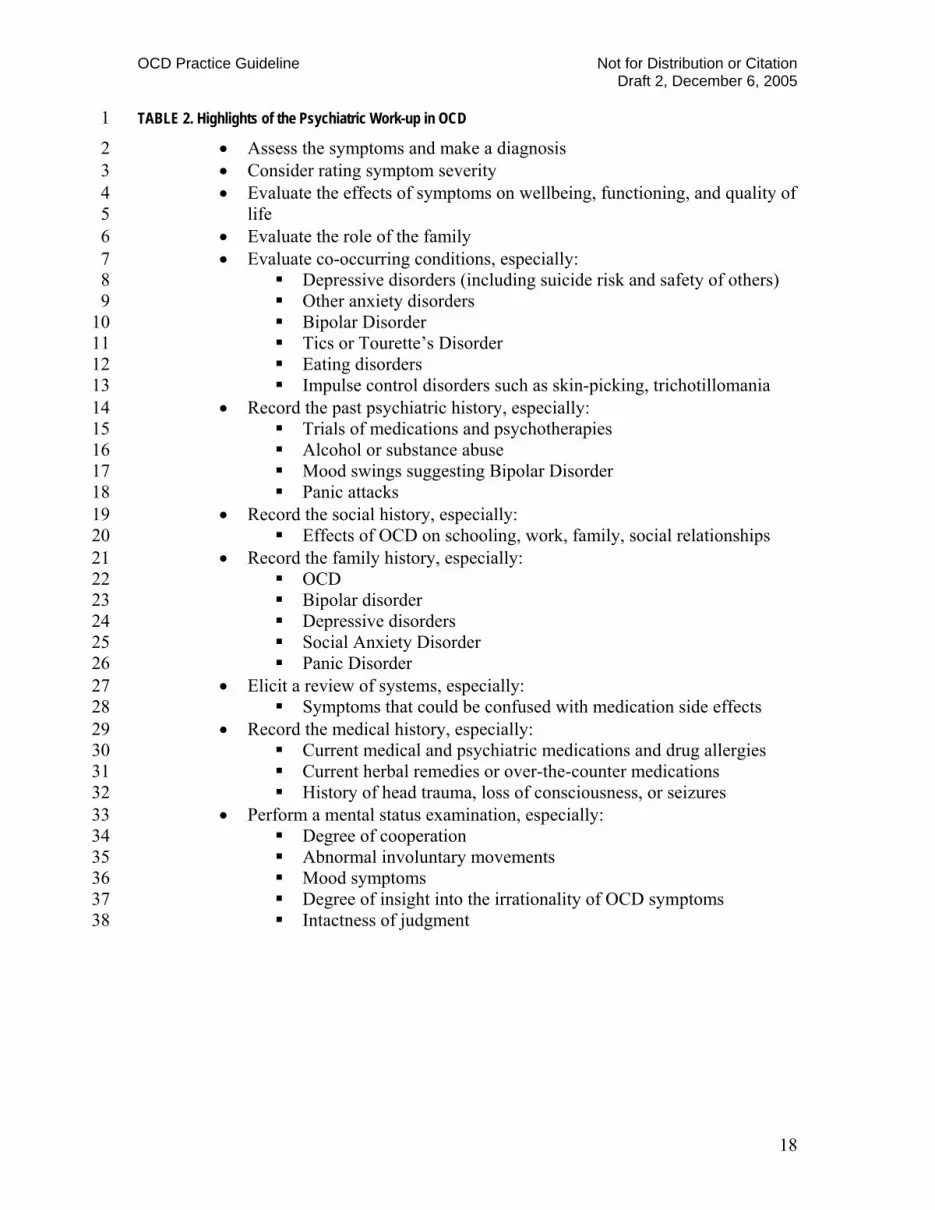
In completing the psychiatric assessment, the psychiatrist will usually visit all the 19
elements of the traditional medical work-up, including current co-occurring conditions, 20
past history, social history, family history, review of systems, current and past medical 21
problems, current medications and drug allergies, and the mental status evaluation (Table 22
2). 23
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
18
TABLE 2. Highlights of the Psychiatric Work-up in OCD 1
• Assess the symptoms and make a diagnosis 2 • Consider rating symptom severity 3 • Evaluate the effects of symptoms on wellbeing, functioning, and quality of 4
life 5 • Evaluate the role of the family 6 • Evaluate co-occurring conditions, especially: 7
Depressive disorders (including suicide risk and safety of others) 8 Other anxiety disorders 9 Bipolar Disorder 10 Tics or Tourette’s Disorder 11 Eating disorders 12 Impulse control disorders such as skin-picking, trichotillomania 13
• Record the past psychiatric history, especially: 14 Trials of medications and psychotherapies 15 Alcohol or substance abuse 16 Mood swings suggesting Bipolar Disorder 17 Panic attacks 18
• Record the social history, especially: 19 Effects of OCD on schooling, work, family, social relationships 20
• Record the family history, especially: 21 OCD 22 Bipolar disorder 23 Depressive disorders 24 Social Anxiety Disorder 25 Panic Disorder 26
• Elicit a review of systems, especially: 27 Symptoms that could be confused with medication side effects 28
• Record the medical history, especially: 29 Current medical and psychiatric medications and drug allergies 30 Current herbal remedies or over-the-counter medications 31 History of head trauma, loss of consciousness, or seizures 32
• Perform a mental status examination, especially: 33 Degree of cooperation 34 Abnormal involuntary movements 35 Mood symptoms 36 Degree of insight into the irrationality of OCD symptoms 37 Intactness of judgment 38
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
19
In assessing the presence and history of co-occurring conditions, the psychiatrist 1
should pay particular attention to mood disorders and suicidal ideation and behaviors, 2
since depressive disorders are common in OCD. Suicide attempt rates are elevated by 3
50% or more in individuals with OCD compared with individuals in the general 4
population (Hollander et al. 1996; Angst et al. 2004). In assessing potential for suicide, 5
the psychiatrist will usually evaluate current mood, ideation, plans, and intent; access to 6
related means of committing suicide; co-occurring substance abuse, psychosis, borderline 7
personality disorder, or other disorders associated with increased risk; the patient’s past 8
history of suicidal attempts including potential lethality; real or perceived lack of social 9
supports; recent losses, including impairments resulting from medical conditions; cultural 10
and ethnic factors; and collateral information from family members or others. Further 11
information is available in APA’s Practice Guideline for the Assessment and Treatment 12
of Patients With Suicidal Behaviors (American Psychiatric Association 2003). 13
Other anxiety disorders (panic disorder, generalized anxiety disorder, 14
generalized social anxiety) are common in OCD patients (Diniz et al. 2004; LaSalle et al. 15
2004) and may complicate treatment planning as described below (Sections III.A.5 and 16
III.A.6). 17
Bipolar disorder is more common in patients with OCD than in the general 18
population (Perugi et al. 2002). Careful exploration for co-occurring bipolar disorder is 19
important in view of the risk of precipitating hypomania or mania with anti-OCD 20
medications. Other disorders with elevated prevalence in OCD include alcohol 21
abuse/dependence and certain impulse control disorders such as skin picking. In children 22
and adolescents with OCD, the prevalence of attention deficit hyperactivity disorder 23
(ADHD) and of oppositional defiant disorder (ODD) is elevated. 24
Tics are common in individuals with OCD. Conversely, OCD has been diagnosed 25
in from 28% to 62% of individuals with Tourette’s Disorder (Koran 1999). In patients 26
with co-occurring OCD and Tourette’s Disorder it may be helpful to use a rating scale 27
such as the Yale Global Tic Severity Scale (YGTSS) (Leckman et al. 1989). This scale 28
provides anchor points for rating the number, frequency, intensity, complexity, 29
interference, and impairment associated with motor and phonic tics. 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
20
Anorexia nervosa and bulimia nervosa may be more common in men and 1
women with OCD (Rubinstein et al. 1992). The prevalence of OCD appears to be 2
elevated in patients with either anorexia nervosa or bulimia nervosa (Thiel et al. 1995; 3
Matsunaga et al. 1999). 4
In assessing the past psychiatric history, the psychiatrist should attempt to 5
document the patient’s past medication trials to be sure that drug doses and trial 6
durations have been adequate, to understand side effects and other factors influencing 7
adherence, and to evaluate the degree of response. The nature and extent of all trials of 8
psychotherapy including cognitive-behavioral therapy and the patient’s response 9
should be documented. Past histories of alcohol or substance abuse or dependence 10
(Section III.A.8), mood swings (Section III.A.4), or panic attacks (Section III.A.5) will 11
influence treatment planning. 12
In assessing the patient’s social history, the psychiatrist should evaluate how 13
OCD has interfered with academic and vocational achievement as well as familial and 14
social relationships. 15
In assessing the family history, a history of OCD is of interest particularly for its 16
psychological effects and the increased likelihood of OCD in family members. However, 17
one should not expect specific OCD symptoms to repeat among siblings or across 18
generations. Hoarding may be an exception (Winsberg et al. 1999). A family history of 19
bipolar disorder suggests a need for caution in prescribing SRIs. A family history of 20
major depression, generalized social anxiety disorder, or panic disorder puts the patient at 21
increased risk of having these disorders. 22
In performing the review of systems, it is important to record the presence and 23
severity of somatic or psychological symptoms that could be confused with medication 24
side effects. 25
In assessing the medical history, the psychiatrist should consider whether the 26
OCD is a manifestation of a general medical condition (e.g., brain trauma, stimulant 27
abuse, carbon monoxide poisoning, Parkinsonism), although this is rare and usually 28
obvious (Koran 1999). Current medical conditions and any history of head trauma or 29
seizures should be documented. In children, the psychiatrist should look for a sudden 30
onset of OCD and subsequent exacerbation of symptoms in relation to streptococcus or 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
21
other infections. Although the concept remains controversial, pediatric autoimmune 1
disorders associated with streptococcus Type A (PANDAS), in which OCD is 2
hypothesized to be due to autoimmune mechanisms, may account for a portion of acute 3
childhood-onset OCD (Mell et al. 2005; Dale et al. 2005). 4
Current medications and doses should be reviewed to prevent pharmacokinetic 5
and pharmacodynamic interactions with psychotropic drugs. Herbal or “natural” remedies 6
must also be inquired about, along with over-the-counter medications. Allergies to 7
medical and psychotropic medications should be recorded, although what the patient 8
describes as “allergies” will on careful exploration often turn out to be unpleasant but 9
manageable side effects. 10
The mental status examination provides a place to record the patient’s degree of 11
cooperativeness, whether any abnormal involuntary movements are present at baseline 12
(since this can influence the choice of medication augmentation strategies), 13
characteristics of speech such as circumstantiality (which is not rare in OCD), the 14
presence of mood symptoms that may interfere with cooperation with treatment, the 15
degree of insight into the irrationality of the OCD symptoms, and the degree to which 16
OCD is affecting judgment, as measured by its effects on the patient’s management of the 17
ordinary decisions of daily life. Recommendations for conducting a general psychiatric 18
evaluation are provided in APA’s Practice Guideline for the Psychiatric Evaluation of 19
Adults, 2nd edition (American Psychiatric Association 2006a). 20
II.A.6. ______Establish Goals for Treatment 21
Since OCD is not usually curable, in the sense of bringing about complete and permanent 22
symptom remission, the goals of treatment include the amelioration, if not the 23
elimination, of symptoms; improving the patient’s functioning; and helping the patient to 24
improve his or her quality of life (in family, social, work/school, home, parental, and 25
leisure domains). The goals of psychiatric care also include enhancing the patient’s 26
ability to cooperate with care in the face of the frightening cognitions that are typical of 27
OCD; anticipating stressors likely to exacerbate the condition and helping the patient 28
develop coping strategies; providing assistance and support in dealing with stresses; 29
monitoring the patient’s psychiatric status and intervening as indicated; minimizing the 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
22
adverse effects of treatment; and, educating the patient and family regarding the disorder 1
and its treatment. The clinician can take the following as reasonable targets for treatment 2
outcomes: reducing the time spent in obsessing and in compulsive behaviors to less than 3
one hour per day, reducing the degree of OCD anxiety to no more than mild, and 4
reducing the degree of interference with the tasks of ordinary living to little or none. 5
Some patients, despite the psychiatrist’s best efforts, will be unable to reach these targets. 6
II.A.7. ______Establish the Appropriate Setting for Treatment 7
The appropriate treatment setting will depend on a number of factors. 8
a. Hospital treatment (Drummond 1993) may be indicated by suicide risk, an 9
inability to provide adequate self care, danger to others, need for constant 10
supervision or support, an inability to tolerate outpatient medication trials because 11
of side effects, the presence of medical conditions that necessitate hospital 12
observation while anti-OCD medications are initiated, or by co-occurring 13
conditions that themselves require hospital treatment, such as severe or suicidal 14
depression, schizophrenia, or mania. 15
b. Residential treatment or partial hospitalization (Bystritsky et al. 1996; Stewart et 16
al. 2005) could be indicated by a need for intensive cognitive-behavioral therapy 17
(CBT), other adjunctive psychotherapeutic interventions, a supportive milieu, 18
daily monitoring of behavior or medications, or to stabilize and increase the gains 19
made during a period of full hospitalization. Goals of day treatment include 20
prevention of relapse and maintenance and improvement of social functioning. 21
c. Home-based treatment may be necessary for patients with hoarding or, initially, 22
for those with contamination fears or other symptoms so impairing that they 23
cannot come to the office or clinic. 24
d. Outpatient treatment is usually sufficient, but the intensity may vary from daily 25
psychotherapy such as intensive CBT to treatment less than once a week (after 26
achieving substantial symptom reduction and stabilization). 27
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
23
II.A.8. ______Enhance Treatment Adherence 1
The art has three factors, the disease, the patient, the physician. The physician is the 2 servant of the art. The patient must co-operate with the physician in combating the 3 disease. 4
Hippocrates, 460–357 BC 5 Epidemics, I.XI 6
7 The physician must not only be prepared to do what is right himself, but also to make the 8 patient, the attendants, and the externals co-operate. 9
Hippocrates, 460–357 BC 10 Aphorisms, I.I 11
12 Factors influencing adherence can be thought of as related to the illness, the patient, the 13
physician, the patient-physician relationship, the treatment, and the social or 14
environmental milieu (Leo et al. 2005). In the eloquent Hippocratic formulations: The 15
psychiatrist must consider the patient’s beliefs about the nature of the illness and its 16
treatments and the patient’s goals and priorities. In this context, the physician’s obligation 17
to provide patient and family education may facilitate adherence (Appendix A). For 18
example, it is important to inform patients about the usual delay of weeks after starting 19
medication before substantial symptom relief is expected, the need for extended periods 20
of medication taking, and likely side effects and strategies for managing them (Bourgeois 21
2005). Note that the patient’s culture may influence his or her willingness to report 22
medication side effects (e.g., sexual side effects) or to report how discomfiting the side 23
effects are. It is important to explain that all psychotherapy, including CBT, involves 24
confronting feared thoughts and situations, but at a rate that is tolerable. 25
The fears, doubting, and need for certainty that are characteristic of OCD can 26
influence the patient’s willingness and ability to cooperate in care and can challenge the 27
physician’s patience. The cognitive and motivational effects of co-occurring conditions 28
such as major depression must also be taken into account. What will treatment require of 29
the patient, and how does this match his or her skills, resources, and methods of coping? 30
Medication side effects and the need in CBT to confront feared situations can influence 31
adherence. Since effective medications differ both in side effect profiles and in their 32
adverse effects on a given patient, the psychiatrist has many options for responding to the 33
patient’s concerns and preferences. Being available to respond quickly to concerns about 34
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
24
side effects and scheduling follow-up appointments soon after starting or changing 1
medications will enhance adherence. In all psychotherapies, including CBT, interventions 2
must be paced at a rate that does not create anxiety so severe that it precludes 3
cooperation. A strong therapeutic alliance and good rapport are vital to maintaining 4
cooperation. The interventions must be well-tailored to the patient’s specific fears. The 5
therapist becomes a supportive coach, not a disciplinarian, and encourages behavior 6
change and praises successes while validating the difficulty of confronting the OCD 7
symptoms. 8
As with all psychotherapies, there is a potential for transference reactions which 9
can interfere with adherence and cooperation. These reactions can often be dealt with in 10
the course of CBT, and at other times may best yield to an adjunctive psychodynamic 11
psychotherapy. Similarly, potential countertransference issues in working with these 12
often difficult patients may interfere with adherence and therapeutic success. 13
The psychiatrist should also consider the role of the patient’s family and social 14
support system in maintaining the symptoms through misguided efforts to reduce the 15
patient’s discomfort. Family members, for example, may provide inappropriate 16
reassurance regarding the absence of dangers or inappropriately offer to do the patient’s 17
bedtime checking rituals so the patient can get more rest. The family or significant others 18
may not understand that OCD is an illness that gives rise to the patient’s compulsive 19
behaviors. They may accuse the patient of being weak or crazy or may react to 20
symptomatic behavior with inappropriate anger. Family therapy may be indicated to deal 21
with hostility, dependency, or other family system issues. The patient’s permission must 22
be obtained before initiating a family contact. 23
Finally, practical issues such as cost, insurance coverage, and transportation may 24
need to be addressed. Pharmaceutical companies will provide free medications for 25
patients with severe financial limitations, the exact criteria differing from company to 26
company. Information on patient assistance programs is available from the company Web 27
sites and from the Web site of the Pharmaceutical Research and Manufacturers of 28
America (http://www.helpingpatients.org). 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
25
II.A.9. ______Provide Education to the Patient and, When 1 Appropriate, to the Family 2
Patients often have little knowledge of the nature, biology, course, or treatment of their 3
disorders. Those with childhood onset of OCD may confuse symptoms with aspects of 4
their inner selves. Educated patients can be more effective allies in treatment. Education 5
will help destigmatize the illness and allow the patient to make more fully informed 6
decisions about treatments. Education may also increase the patient’s motivation and 7
ability to cooperate in care. All patients with OCD should be provided with information 8
and access to educational materials explaining the nature of the disorder and the range of 9
available treatments. When appropriate, access should also be offered to the involved 10
family members. Appendix A contains lists of self-help books for patients with OCD and 11
with co-occurring OCD spectrum disorders (McElroy et al. 1994; Hollander & Wong 12
1995; Koran 1999), patient advocacy group Web sites that provide scientifically reliable 13
information, Web sites that provide information on the use of medications in pregnancy 14
and during breast-feeding, and scientifically reliable, broader mental health Web sites. 15
All OCD patients should be made aware of the OC Foundation (www.ocfoundation.org), 16
which provides both educational materials and access to support groups. 17
II.A.10. _____Coordinate the Patient’s Care With Other Providers 18 of Care and Social Agencies 19
The psychiatrist should coordinate the patient’s care with physicians treating co-20
occurring medical conditions, with other clinicians, and with social agencies such as 21
schools and vocational rehabilitation programs. 22
OCD may result in functional impairments involving family, social, academic, or 23
occupational roles, and these impairments may bring financial problems. The possible 24
need for family therapy has been mentioned. For OCD of disabling severity, the 25
psychiatrist must be willing to write on the patient’s behalf to government agencies that 26
control access to disability income, publicly financed health care, or government-27
supported housing. The psychiatrist may have to write to the federal Internal Revenue 28
Service and state tax authorities to explain that a patient’s hoarding or procrastination has 29
prevented timely filing of income tax returns. Students may need letters explaining the 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
26
need for special dormitory living situations or extra time for taking tests. Employers may 1
need help in understanding what accommodations are appropriate in light of the 2
Americans With Disabilities Act (Americans With Disabilities Act 1990). The 3
psychiatrist may find it appropriate to refer the patient to a state vocational rehabilitation 4
agency or to an occupational therapist. 5
OCD patients who are parents of young children may want advice regarding the 6
genetic risk of OCD. The clinician may wish to refer these parents to a genetic counselor, 7
but should be aware of the available data (Section IV.D). The psychiatrist should help 8
patients concerned about the possibility of OCD in their children find clinicians who can 9
conduct an appropriate evaluation. (Educational materials for parents of children with 10
OCD are included in Appendix A.) 11
II.B._ACUTE PHASE 12
II.B.1. ______Choice of Initial Treatment Modality 13
At the beginning no one tries extreme remedies. 14 Seneca, c. 4 BC–65 AD, Roman writer and statesman 15
Agamemnon 153 16 17
As to diseases, make a habit of two things: to help or at least not to harm. 18 Hippocrates, 460–357 BC 19
Corpus Hippocraticum 20 21 On the basis of clinical trial data, cognitive-behavioral therapy (CBT) and serotonin 22
reuptake inhibitors (SRIs) are recommended as safe and effective first-line treatments for 23
OCD. Whether to recommend a form of CBT, a selective serotonin reuptake inhibitor 24
(SSRI), or combined treatment will depend on a number of factors. These include the 25
nature and severity of the patient’s symptoms, the nature of any co-occurring psychiatric 26
and medical conditions, and the patient’s past treatment history, current medications, and 27
preferences. Because most treatment studies have been of three or four months duration, 28
only limited data are available to guide long-term treatment decisions (see Section II.C.) 29
For OCD patients without co-occurring depression, data from one large (N>100) 30
randomized controlled trial suggest that CBT may be superior to clomipramine 31
monotherapy (Foa et al. 2005; Simpson et al. 2005b). The evidence base for the form of 32

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
27
CBT that relies primarily on behavioral techniques, such as exposure and response 1
prevention (Meyer 1966) is the strongest <<BS we need a meta-analysis reference here 2
LK>>. 3
Data also support the use of CBT that focuses on cognitive techniques whose 4
primary aim is to identify, challenge, and modify dysfunctional beliefs (Freeston et al. 5
1996; van Balkom et al. 1998; Cottraux et al. 2001; Whittal et al. 2005) if these 6
techniques are combined with behavioral experiments. However, some data suggest, and 7
many clinical experts believe, that the most effective form of CBT for OCD integrates 8
exposure, ritual prevention, discussion of feared consequences and dysfunctional beliefs, 9
and relapse prevention. There is little data from controlled trials to support cognitive 10
therapy without exposure or behavioral experiments. 11
CBT alone is commonly considered for a patient who is not too depressed, 12
anxious, or lacking in motivation to cooperate with this treatment modality, or who 13
prefers not to take medications. 14
An SSRI alone is commonly considered for a patient who is not currently able to 15
cooperate with CBT, has previously responded well to a given drug, or prefers treatment 16
with an SSRI alone. 17
Non-specific psychotherapeutic elements are ordinarily present in all physician-18
patient relationships. The available data suggest that combining an SRI and CBT is more 19
effective than monotherapy in some patients, but is not necessary for all. Combined 20
treatment should be considered in patients with an unsatisfactory response to 21
monotherapy, those with co-occurring psychiatric conditions for which SRIs are 22
effective, and those who wish to take medications for the shortest possible time. In the 23
latter instance, uncontrolled follow-up studies suggest that CBT may delay or mitigate 24
relapse when SRI treatment is discontinued (Hembree et al. 2003; Simpson et al. 2004; 25
Biondi & Picardi 2005). Combined treatment or starting with an SRI alone may also be 26
considered in patients with severe OCD, since the medication may diminish symptom 27
severity to a point where the patient can cooperate with the demands of CBT. 28

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
28
II.B.2. ______Choice of Specific Pharmacologic Treatment 1
Although meta-analyses of placebo-controlled trials suggest greater efficacy for 2
clomipramine than for the older SSRIs, the results of trials comparing clomipramine and 3
SSRIs directly do not support this impression (see Section V.A.1). Because SSRIs have a 4
less troublesome side effect profile (see below), an SSRI is preferred for a first 5
medication trial. Although all SSRIs appear to be equally effective, individual patients 6
may respond well to one and not to another. The reasons for this patient-specific response 7
are unknown. 8
In choosing among the SSRIs, the psychiatrist should consider the safety and 9
acceptability of particular side effects for the patient, potential drug interactions, past 10
treatment response, and the presence of co-occurring general medical conditions. For 11
example, paroxetine, the SSRI most associated with weight gain (Maina et al. 2004) and 12
the most anticholinergic SSRI, would not be the first choice for patients with obesity, 13
diabetes mellitus, constipation, or urinary hesitancy. 14
Citalopram, escitalopram, venlafaxine, and mirtazapine offer the advantage of not 15
meaningfully inhibiting the hepatic P450 enzyme system or displacing drugs tightly 16
bound to plasma proteins, e.g., warfarin and digoxin. Reviews are available of potential 17
drug interactions caused by liver CYP450 enzyme effects or by drug displacement from 18
serum protein binding sites (Richelson 1997; Greenblatt et al. 1998; Ciraulo 2005). Many 19
of these interactions, however, reflect only in vitro data, and their clinical importance is 20
not established. Web sites providing data on potential drug interactions include 21
http://medicine.iupui.edu/flockhart/clinlist.htm. For up-to-date clinical reports of 22
interactions between specific SRIs and other medications, psychiatrists can consult the 23
federal National Library of Medicine at 24
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?DB=pubmed, which is also accessible by 25
entering the term “pubmed” in a search engine. Since there are very few absolute 26
contraindications to treatment with SSRIs (e.g., the risk of serotonin syndrome from 27
adding an SSRI to an MAOI, tramadol, meperidine, dextromethorphan, or in rare cases 28
buspirone, mirtazapine, or lithium (Gillman 1999; Keck, Jr. & Arnold 2000)), the 29
psychiatrist will much more often have to consider the relative contraindications for 30
specific SSRIs in relation to interactions with the patient’s other medications. 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
29
Although no definitive data are available, the response of first-degree relatives to 1
particular medications may be predictive of the patient’s response because of genetic 2
similarity. This is a subject, however, for future research. 3
II.B.2.a. _____Implementation of Pharmacotherapy 4
The need to educate the patient about any medication recommended has been emphasized 5
earlier. Table 3 displays suggested starting doses, known effective doses, maximum 6
recommended doses, and maximum doses occasionally prescribed for each SRI. 7

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
30
TABLE 3. Dosing of Serotonin Reuptake Inhibitors in OCD 1 2
3 a Some patients may need to start at half this dose or less to minimize undesired side effects such as nausea or to 4
accommodate anxiety about taking medications. 5 b These doses are sometimes used for rapid metabolizers or for patients with no or mild side effects and 6
inadequate therapeutic response after 8 weeks or more at the usual maximum dose. 7 c Combined plasma levels of clomipramine plus desmethylclomipramine 12 hours after the dose should be kept 8
below 500 ng/ml to minimize risk of seizures and cardiac conduction delay. 9
SRI
Start Dose and Incremental Dose
(mg/day) a
Usual Target Dose
(mg/day) Usual Maximum Dose (mg/day)
Occasionally Prescribed
Maximum Dose (mg/day) b
Citalopram 20 40–60 80 120
Clomipramine 25 100–250 250 c
Escitalopram 10 20 40 60
Fluoxetine 20 40–60 80 120
Fluvoxamine 50 200 300 400
Paroxetine 20 40–60 60 100
Sertraline 50 200 200 400
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
31
Patients who are worried about side effects can be started at half these doses or less, since 1
many SSRIs (including citalopram, escitalopram, fluoxetine, paroxetine, and sertraline) 2
are available in liquid form. Most patients will not experience substantial improvement 3
earlier than 4 to 6 weeks after starting medication, and some who will ultimately respond 4
will experience little improvement for as many as 10 to 12 weeks. Available trial data 5
suggest that higher SSRI doses produce a somewhat higher response rate and somewhat 6
greater magnitude of symptom relief (Tollefson et al. 1994a; Greist et al. 1995a; Stein et 7
al. 2001; Hollander et al. 2003a) (Table 4). 8

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
32
TABLE 4. Effects of Higher SSRI Doses in Fixed Dose Trials on OCD 1 2
Drug/Study Response Definition When Dose 1 Dose 2 Dose 3
Fluoxetine Tollefson et al. 1994 (Tollefson et al. 1994b)
YBOCS ↓ ≥35%
(mean ↓)
Week 13 LOCF*
20 mg 32%
3.4 points
40 mg 32%
4.6 points
60 mg 35%
5.9 points
Citalopram Stein et al. 2001 <<LK: Which ref?>>
YBOCS ↓ ≥25%
(mean ↓)
Week 12 LOCF
20 mg 57%
8.4 points
40 mg 52%
8.9 points
60 mg 65%
10.4 points Sertraline Greist et al. 1995 (Greist et al. 1995b)
YBOCS ↓ in mean
score
Week 12 LOCF
50 mg ~6.8 points
100 mg ~5.7 points
200 mg ~7.5 points
Paroxetine Hollander et al. 2003 (Hollander et al. 2003a)
YBOCS ↓ in mean
score
Week 12 LOCF
20 mg 4.1 points
40 mg 6.4 points
60 mg 7.3 points
3 * LOCF = last observation carried forward 4

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
33
Moreover, patients who have not responded to 10 to 12 weeks of a known effective dose 1
may respond at higher doses (Tollefson et al. 1994b)<<Placeholder for Ninan, Koran, et 2
al. 2005 sertraline paper, submitted>> (Table 5). 3

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
34
TABLE 5. Response to Raising the SSRI Dose In Non-responders 1 2
Drug/Study Response Definition
Initial Dose & Duration
Higher Dose’s Duration
Higher Dose and Response
Rate
Higher Dose and Response
Rate Fluoxetine Tollefson et al. 1994 <<LK: Which ref?>>
YBOCS ↓ ≥25%
13 weeks 26 weeks LOCF*
20 mg 60 mg 80%
(8/10)
80 mg 46%
(15/33) 40 mg 20%
(1/5) 53%
(17/32) 60 mg 50%
(15/30) Sertraline Ninan et al. 2005 <<LK: Which ref?>>
YBOCS ↓ ≥25%
16 weeks 200 mg
12 weeks (completers)
200 mg 34%
(10/29)
377 mg 52%
(11/21)
3 *LOCF = last observation carried forward 4
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
35
For this reason, some clinicians prefer to titrate patients in weekly increments to the 1
maximum recommended dose if this is comfortably tolerated and then await the results 2
rather than waiting for one to two months at each dose to evaluate results. Sertraline, 3
alone among the SSRIs, is better absorbed with food. Paroxetine should be started at 10 4
mg/day in elderly patients (those aged 65 and older), for whom the maximum daily dose 5
should ordinarily not exceed 50 mg/day (Physicians Medical Economics 2005). 6
II.B.2.b. _____Managing Medication Side Effects 7
Unlike the SSRIs, clomipramine also blocks norepinephrine reuptake, muscarinic 8
cholinergic receptors, H1 histamine receptors and α1-adrenergic receptors, as well as 9
sodium channels in the heart and brain. As a result, clomipramine is more likely to induce 10
anticholinergic effects such as dry mouth, constipation, and blurred vision, although these 11
typically diminish over time. Clomipramine is also more likely to induce delayed 12
urination or, uncommonly, urinary retention. Histaminic blockade is associated with 13
weight gain and sedation. Adrenergic blockade may lead to orthostatic hypotension and 14
postural dizziness. Sodium channel blockade can induce seizures (estimated to occur in 15
0.7% of patients treated with up to 300 mg/day for up to 6 years (Trimble 1990) or 16
cardiac arrhythmias. In view of clomipramine’s less favorable side effect profile, expert 17
opinion favors one or more SSRI trials before trying clomipramine (Expert Consensus 18
Panel 1997). Starting with 25 mg/day or less will increase clomipramine’s early 19
tolerability (Flament & Bisserbe 1997). 20
The most common side effects of the SSRIs include gastrointestinal distress 21
(especially in the first weeks of treatment), agitation, insomnia or somnolence, increased 22
tendency to sweat, and sexual side effects, including diminished libido and difficulty with 23
erection and orgasm. Gastrointestinal distress can be minimized by starting with low 24
doses; if mild queasiness or nausea occurs, it will usually disappear within 1 to 2 weeks 25
at constant dose. Insomnia may necessitate addition of a sleep-promoting agent. Fatigue 26
or sleepiness may respond to the addition of modest doses of modafinil (Fava et al. 27
2005). Cases of successful treatment of sweating have been reported with low doses of 28
anticholinergic agents such as benztropine (Pierre & Guze 2000; Marcy & Britton 2005), 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
36
clonidine (Feder 1995), cyproheptadine (Ashton & Weinstein 2002) and mirtazapine 1
(Buecking et al. 2005). 2
Few controlled trials have been published regarding the management of sexual 3
side effects, which may affect one-third or more of patients (Clayton et al. 2002). 4
Management approaches include reducing the dose to the minimal effective dose, waiting 5
for the symptom to remit (which clinical impression suggests may occur within two 6
months in about 10% of patients), trying a once-weekly, one-day “drug holiday” before 7
engaging in sexual activity, switching to another SSRI (which may relieve the sexual 8
dysfunction but not contain the patient’s OCD), or adding a pharmacologic antidote. The 9
drug holiday approach may alleviate difficulties with erection or orgasm but not with 10
libido. It is not effective for fluoxetine because of its long half-life (Rothschild 1995) and 11
may induce withdrawal symptoms if attempted with paroxetine or venlafaxine. Taking 12
drug holidays more than once weekly risks a return of OCD symptoms. Case series and 13
primarily uncontrolled studies report modest success in restoring libido, erection, and 14
orgasm by adding amantadine, buproprion, buspirone, stimulants such as 15
methylphenidate or dexedrine, yohimbine, Ginkgo biloba extract (Zajecka 2001), and 16
ropinirole (Worthington, III et al. 2002). Adding bupropion has the best evidence base 17
(Clayton et al. 2004), but even this literature is mixed (Debattista et al. 2005). Case series 18
and uncontrolled studies report modest success in restoring erection or orgasm but not 19
libido with cyproheptadine or mirtazapine (Zajecka 2001). Controlled trials support the 20
use of sildenafil to restore erection and orgasmic ability (Nurnberg et al. 2001; Seidman 21
et al. 2003). 22
SSRIs may be associated with increased intra-operative blood loss in patients also 23
taking non-steroidal anti-inflammatory drugs (Weinrieb et al. 2005) and may interact 24
with anesthetics and opiate pain relievers. Thus, in patients anticipating elective surgery, 25
initiation of pharmacotherapy should be postponed. 26
A drug discontinuation syndrome consisting most often of dizziness, 27
nausea/vomiting, headache, and lethargy but also including agitation, insomnia, 28
myoclonic jerks, and paresthesias (Zajecka et al. 1997; Tamam & Ozpoyraz 2002) may 29
occur if medication is suddenly stopped. The syndrome occurs most often after rapid 30
discontinuation of paroxetine or the SNRI venlafaxine (Tamam & Ozpoyraz 2002) but 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
37
may occur after stopping any SSRI. A slow taper over several weeks or more will 1
minimize the likelihood of this syndrome. If symptoms do occur, raising the SSRI dose 2
and slowing the taper may bring relief. 3
II.B.3. ______Choice of a Specific Form of Psychotherapy 4
CBT is the only form of psychotherapy supported by controlled OCD treatment trials. 5
Although psychodynamic or interpersonal therapy may help the patient improve 6
relationships, resolve life issues, conquer resistance to undergoing treatment, or 7
overcome excessive dependency or entitlement, there are no studies to indicate whether 8
these therapies ameliorate OCD. As noted in Section II.B.1, the CBT variant that relies 9
primarily on behavioral techniques, such as exposure and response prevention (ERP), has 10
the strongest evidence base. <<BS: We need a meta-analysis reference here. LK>> Some 11
data suggest that ERP is more effective if it integrates habituation (McLean et al. 2001; 12
Whittal et al. 2005) with discussions of feared consequences and dysfunctional beliefs, 13
and with relapse prevention (Huppert & Franklin 2005)<<Placeholder for Rector study 14
from BS>>. <<BS: Do you mean this FREESTON 1997 ref?: Freeston, M. H., 15
Ladouceur, R., Gagnon, F., Thibodeau, N., Rheaume, J., Letarte, H. et al. (1997). 16
Cognitive-behavioral treatment of obsessive thoughts: a controlled study. J.Consult 17
Clin.Psychol., 65, 405-413>>(Vogel et al. 2004; Foa et al. 2005). 18
Data also support CBT that primarily utilizes cognitive techniques such as 19
identifying and modifying faulty beliefs (Freeston et al. 1996)<<BS: Would you like to 20
add refs re: use of cognitive techniques?>> if this therapeutic work is combined with 21
behavioral experiments. In direct comparisons, CBT utilizing cognitive techniques and 22
behavioral experiments had efficacy similar to ERP that focused only on habituation. 23
There is little data to support attempting to treat OCD with cognitive therapy alone, 24
without exposure or behavioral experiments. 25
II.B.4. ______Implementation of Cognitive-Behavioral Therapies 26
Cognitive-behavioral therapies have been delivered in individual, group (Fals-Stewart et 27
al. 1993; McLean et al. 2001), and family therapy sessions, with session length varying 28
from less than 1 hour to 2 hours (Mehta 1990; Van Noppen et al. 1997) (for a summary 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
38
of group and family therapy studies see (Van Noppen et al. 1997; Steketee & Van 1
Noppen 1998)). One group has explored a computer-based approach coupled with a 2
touch-tone telephone system accessible 24 hours a day (Marks et al. 1998; Greist et al. 3
2002). The literature and expert opinion suggest that ERP or CBT sessions should be 4
scheduled at least once weekly (March et al. 1997; Whittal et al. 2005). One study 5
suggests that five sessions per week may be more effective than once-weekly sessions but 6
are clearly not more effective than twice-weekly sessions (Abramowitz et al. 2003). The 7
number of treatment sessions, their length, and the duration of an adequate trial have not 8
been established, but expert consensus recommends 13 to 20 weekly sessions “for most 9
patients” (March et al. 1997). The majority of treatment trials have been only 8 to 16 10
weeks long. The long-term persistence of treatment effects and whether “booster 11
sessions” should be arranged periodically require further study. 12
The psychiatrist may elect to conduct the cognitive behavioral therapy, or refer 13
the patient for this or another adjunctive psychotherapy to an appropriately trained 14
therapist. Psychiatrists wishing to utilize various forms of ERP or CBT can consult a 15
number of treatment manuals (Steketee 1993; Kozak & Foa 1997; Steketee 1999; 16
Wilhelm & Steketee 2006) or other publications (Freeston & Ladouceur 1997; Koran 17
1999; Abramowitz 2005; Baer & Minichiello 2005). The psychiatrist initiating ERP or 18
CBT should explain to the patient the nature of the treatment, including its here and now 19
focus, the rationale underlying treatment procedures, and what the patient will be 20
required to do. When resources for CBT are not available, the psychiatrist can suggest 21
and supervise the use of self-help treatment guides (Appendix A) and support groups 22
accessible through the OC Foundation (Appendix A), although these interventions have 23
not been subjected to controlled study. 24
At the start of therapy, the psychiatrist can use the Y-BOCS symptom checklist 25
(Goodman et al. 1989c) (Appendix B) to help the patient create a list of target symptoms, 26
including obsessions, compulsions, and items or situations avoided because of OCD 27
concerns. The patient ranks the listed items from least to most anxiety-provoking. 28
In ERP patients are taught to confront feared situations and objects (i.e., 29
exposure) and to refrain from performing compulsions (i.e., ritual prevention). Exposures 30
may include in vivo confrontations (e.g., touching objects in public bathrooms) and 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
39
imaginal confrontations of feared consequences (e.g., imagining becoming ill from 1
“contamination”). Exposures that provoke moderate anxiety are prescribed first, followed 2
as quickly as tolerable by exposures of increasing difficulty. Moving at too slow a pace 3
can diminish faith in the treatment and motivation to continue. Patients must face their 4
fears for a prolonged period without ritualizing, allowing the anxiety or discomfort to 5
dissipate on its own (“habituation”). The goal is to weaken the connections between 6
feared stimuli and distress and between ritualizing and relief from distress. 7
As noted, ERP can be combined with formal cognitive techniques (Vogel et al. 8
2004)<<Placeholder for Rector study from BS>>. Modifications of ERP that include 9
formal cognitive techniques as well as other interventions have been suggested for OCD 10
patients with certain symptoms (e.g., hoarding (Steketee & Frost 2003)) and those 11
without overt rituals (e.g., (Freeston & Ladouceur 1997)). Dysfunctional beliefs in OCD 12
include magical thinking (e.g., contamination by proximity), an inflated sense of 13
responsibility for unwanted events, overestimations of the probability of feared events, 14
the assumption that thoughts are morally equivalent to actions or inevitably lead to action 15
(“thought-action fusion”), perfectionism, the belief that anxiety/discomfort will persist 16
forever, and the need for control. A number of techniques for changing dysfunctional 17
beliefs have been described but have not been subjected to controlled trials (Freeston et 18
al. 1996; Schwartz 1996; Freeston & Ladouceur 1997). These techniques include the 19
“brain lock technique” (Schwartz 1996), satiation (prolonged exposure to feared thoughts 20
via taped monologues or exposure in imagination), thought stopping, Socratic dialogue, 21
and encouraging experimental testing of beliefs. For example, a patient who believes that 22
wishing harm to others will bring harm can be asked to try killing a goldfish in a local pet 23
store with death wishes. Satiation is not advisable for patients with impaired reality 24
testing, e.g., those with schizotypal personality disorder. 25
II.B.5. ______Monitor the Patient’s Psychiatric Status 26
A great part, I believe, of the Art is to be able to observe. 27 Hippocrates 460–357 BC 28
Corpus Hippocraticum 29 30 Some psychiatrists believe that a patient should be seen within 1 to 2 weeks after starting 31
any new pharmacotherapy. The indicated frequency of visits will depend on the severity 32

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
40
of the patient’s symptoms, the complexities introduced by co-occurring conditions, 1
whether suicidal ideation is present, and the likelihood of troubling side effects. Patients 2
should be seen as often as necessary for good management. They should be encouraged 3
to telephone between visits if medication questions arise. If telephone calls become 4
reassurance rituals, the physician should work with the patient and the patient’s family to 5
limit the frequency of such calls, using exposure and response prevention just as in 6
treating any other ritual. 7
As noted earlier, symptom rating scales can be utilized for monitoring the 8
response of OCD, co-occurring depression or co-occurring anxiety disorders (see 9
Appendix B). Although using scales is not expected in routine practice, keeping an 10
objective record over time in those unresponsive to initial treatments may be helpful. 11
II.B.6. ______When and Whether to Change Treatments 12
Amid many possibilities of error, it would be strange indeed to be always in the right. 13 Peter Mere Latham, 1789–1875 14
General Remarks on the Practice of Medicine 15 The Heart and Its Affection, Ch. IV 16
17 The physician’s goals are always to reduce suffering and disability while minimizing the 18
adverse effects of treatment. Because first treatments rarely produce freedom from all 19
OCD symptoms, the psychiatrist must decide with the patient when, whether, and how to 20
alter the treatment approach. In the opinion of CBT experts, 13–20 sessions of weekly 21
outpatient CBT or 50 hours of daily CBT over 3 weeks is an adequate dose after which 22
next steps can be considered (March et al. 1997). With regard to SRIs, expert opinion 23
supports changing medication strategy (switching or augmenting) after a trial of 8 to 12 24
weeks of pharmacotherapy, with 4 to 6 weeks at the maximum comfortably tolerated 25
dose (March et al. 1997). Whether to alter the treatment approach will depend on the 26
degree of suffering and disability the patient wishes to accept. Because illness can bring 27
secondary gains (familial attention and caring and freedom from responsibilities) and 28
because depressed mood can diminish hopefulness, the psychiatrist may have to address 29
these issues when patients are not well motivated to pursue further treatments despite 30
limited improvement in their OCD. 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
41
In clinical trials, OCD “responders” are variously defined as those whose Y-1
BOCS scores decrease by at least 25% or 35% from baseline, or who are rated much 2
improved or very much improved on the Clinical Global Impressions-Improvement scale 3
(CGI-I) (Pallanti et al. 2002a). But even these degrees of improvement leave much room 4
for additional gains. 5
When the outcome of initial treatment has not been satisfactory, the psychiatrist 6
should first consider the possible contribution of several factors: interference by co-7
occurring conditions such as panic disorder, major depression, alcohol or substance 8
abuse, or severe personality disorder; inadequate patient adherence to treatment; the 9
presence of psychosocial stressors; and a failure to tolerate an adequate trial of 10
psychotherapy or maximum recommended drug doses. Note, studies indicate that there is 11
no relationship between OCD treatment outcome and plasma levels of clomipramine 12
(Koran et al. 2005b), fluoxetine (Koran et al. 1996a), fluvoxamine (Goodman et al. 13
1997), or sertraline (Greist et al. 1995a). However, these studies were not designed to 14
identify whether rapid or ultra-rapid metabolizers of these medications were more 15
common among the nonresponders. When the patient’s response to the initial treatment 16
regimen is insufficient, the psychiatrist should first consider extending or intensifying the 17
psychotherapeutic or pharmacotherapeutic intervention. Figure 1 displays a treatment 18
algorithm outlining potential next steps. <<Note to reviewers: an algorithm will be 19
developed after review of this draft.>> 20
II.B.7. ______Pursuing Sequential Treatment Trials 21
Anyone who believes that anything can be suited to everyone is a great fool, because 22 medicine is practiced not on mankind in general, but on every individual in particular. 23
Henri de Mondeville, 1260–1320, Chirurgie 24 25 When the patient has an inadequate response to the initial treatment and no interfering 26
factor can be identified, the psychiatrist and patient must decide upon next treatment 27
steps without the benefit of data from controlled trials comparing all the possibilities. The 28
sequence of treatment trials shown in Figure 1 is based only on expert opinion (e.g., 29
(March et al. 1997) and contributors to this Guideline). As reviewed below, augmentation 30
with antipsychotic medications is supported by strong evidence, augmentation of SRIs 31
with CBT or vice versa by modest evidence. As shown in Table 6, many patients respond 32
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
42
when switched to a different SRI or to venlafaxine. The available evidence does not 1
allow one to predict the chance of response. A trial of mirtazapine is supported by one 2
open pilot study and a double-blind discontinuation trial. Augmenting with 3
clomipramine, once-weekly oral morphine, or pindolol is supported only by small trials at 4
best. The remaining treatment strategies are supported only by case series and case 5
reports, literatures that are less likely to see the publication of negative experiences. 6

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
43
TABLE 6. Chance of Responding to the Next SRI After Failing to Benefit from the Previous SRI 1 2
Study Drug/Dose When Response Definition
Responders Drug Naïve
Responders Experienced
Rasmussen 1997 (Rasmussen et al. 1997b)
Sertraline 50–200 mg
week 12 GCI-I = 1,2 53% (N=293)
33% (N=172)
Goodman et al. 1997 (Goodman et al. 1997)
Fluvoxamine 50–300 mg
week 10 CGI-I = 1,2 50% (N=126)
19% (N=31)
Ackerman et al. 1998 (Ackerman et al. 1998)
Fluoxetine 20,40,60 mg
week 13 YBOCS ↓ ≥35%
42% (N=83)
11%–27%** (N=19,59)
Ravizza in Hollender et al. 2002 (Hollander et al. 2002)
Venlafaxine 225–350 mg
Clomipramine 150–225 mg Citalopram 40–60 mg
week 12 YBOCS ↓ ≥35%
– V8 38%*
CMI11 27%
Cit9 11%
Koran et al. 2005 (Koran et al. 2005b)
Clomipramine 100–250 mg
week 13 YBOCS ↓ ≥35%
– 34% (N=32)
Denys et al. 2004 (Denys et al. 2004b)
Paroxetine 60 mg Venlafaxine 300 mg
week 12 YBOCS ↓ ≥25%
– V27→P 56% P16→V 19%
3 * Subscripts indicate the number of patients treated. 4 ** 11% if previously treatment with SRIs alone, 27% if previously also treated with behavior therapy. 5

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
44
II.B.7.a. _____Adding Psychotherapy to an SRI 1
Data from open trials (Simpson et al. 1999; Tolin et al. 2004), a 6-month randomized trial 2
(Tenneij et al. 2005), and a randomized controlled trial nearing completion <<LK: 3
reference here?>> indicate that ERP can successfully augment a partial response to an 4
adequate SRI trial. An open trial also suggests that the addition of ERP combined with 5
cognitive therapy can help SRI nonresponders, although this trial lacked a control group 6
continuing on medication alone (Kampman et al. 2002). No data are available regarding 7
the effectiveness of adding cognitive therapy elements alone to augment medication 8
response. 9
II.B.7.b. _____Adding an SRI to Psychotherapy 10
The available data suggest that combination treatment (SRI + CBT) can produce a better 11
outcome than monotherapy in some OCD patients but is not necessary for all OCD 12
patients. A 9-week study suggested that combination treatment may be more helpful than 13
CBT alone when obsessions dominate the clinical picture or when secondary depression 14
is present (Hohagen et al. 1998). A 24-week study (Cottraux et al. 1990) found greater 15
effect for combined treatment (exposure plus fluvoxamine) but did not use standard 16
outcome measures or adequately describe the CBT intervention. On the other hand, two 17
studies found no greater effectiveness for combination therapy over CBT alone. In a 16-18
week study, CBT alone (delivered weekly and consisting of self-guided exposure only) 19
produced an outcome similar to 8 weeks of fluvoxamine followed by 8 weeks of 20
combination (CBT + fluvoxamine) treatment (van Balkom et al. 1998). However, neither 21
CBT nor fluvoxamine treatment was optimized. A 12-week study (Foa et al. 2005) 22
comparing combination treatment (clomipramine + CBT) to exposure therapy (delivered 23
in an intensive protocol by skilled therapists) found similar efficacy for the two 24
treatments. Combination treatment and CBT alone were each superior to clomipramine 25
alone in reducing OCD symptoms and in producing remission (i.e., no more than minimal 26
symptoms) (Simpson et al. 2005b). However, interpretation is limited by uncertainty as to 27
whether the treatment groups were equally treatment resistant at baseline. Preliminary 28
data suggest that combining an SRI and CBT can enhance adherence to CBT (Marks et 29
al. 1980) and can be used to minimize SRI exposure (Foa et al. 2005). 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
45
II.B.7.c. _____Switching to a Different SRI or to the SNRI Venlafaxine 1
Patients unresponsive to one SRI may respond well to another (Table 6). The literature 2
does not allow specification of the chance of response as a function of the number of 3
previously failed adequate SRI trials. Clinical experience suggests that response rates to a 4
second SRI trial are close to 50%. 5
II.B.7.d. _____Augmenting With an Antipsychotic Medication 6
The only augmentation strategy effective in multiple controlled trials is the addition of 7
antipsychotic medications, including haloperidol (McDougle et al. 1994), risperidone 8
(McDougle et al. 2000; Hollander et al. 2003b; Erzegovesi et al. 2005), quetiapine 9
(Denys et al. 2004a), and olanzapine (Bystritsky et al. 2004) (Table 7) <<Reviewers: 10
Should Table 7 be limited to double-blind studies? LK>>.11
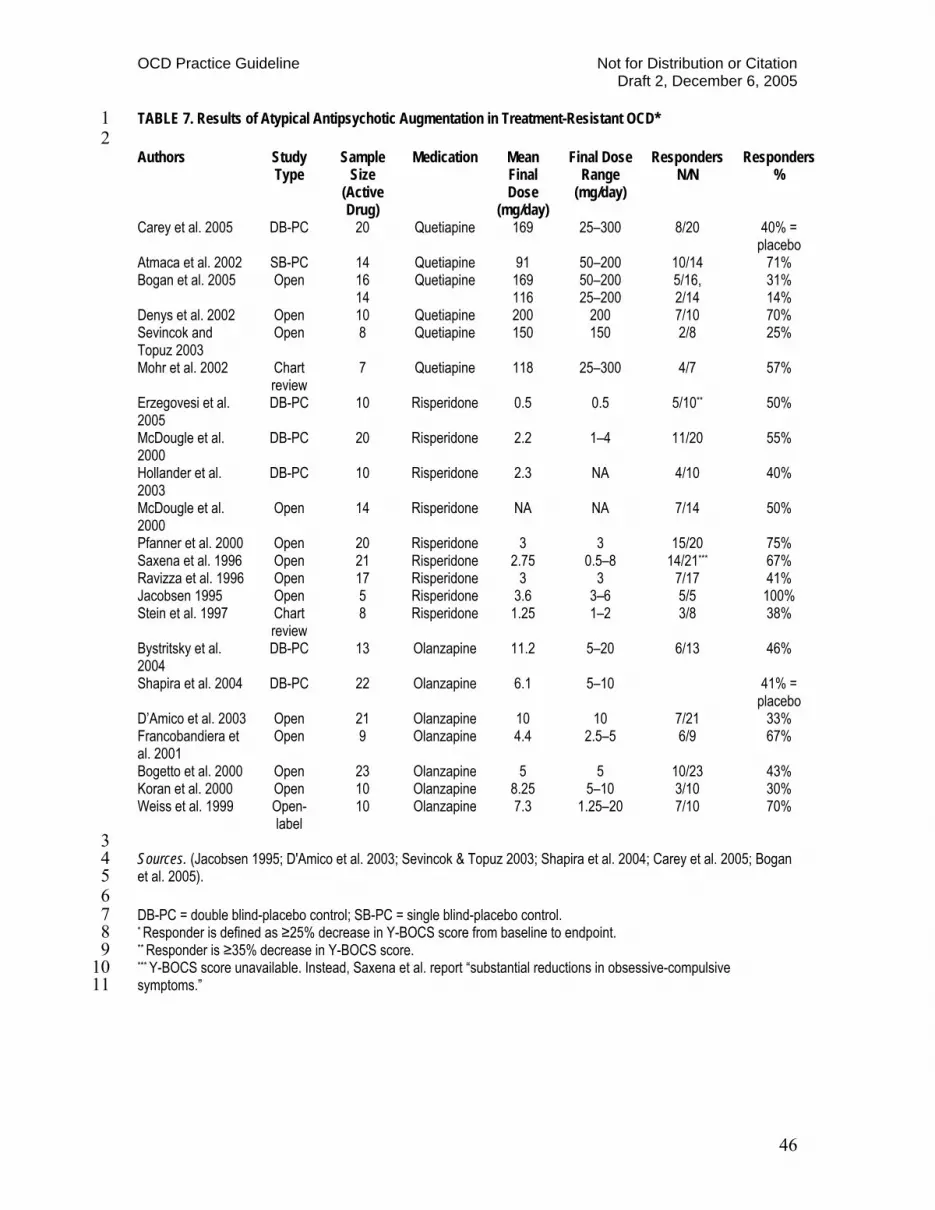
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
46
TABLE 7. Results of Atypical Antipsychotic Augmentation in Treatment-Resistant OCD* 1 2 Authors Study
Type Sample
Size (Active Drug)
Medication Mean Final Dose
(mg/day)
Final Dose Range
(mg/day)
Responders N/N
Responders %
Carey et al. 2005 DB-PC 20 Quetiapine 169 25–300 8/20 40% = placebo
Atmaca et al. 2002 SB-PC 14 Quetiapine 91 50–200 10/14 71% Bogan et al. 2005 Open 16
14 Quetiapine 169
116 50–200 25–200
5/16, 2/14
31% 14%
Denys et al. 2002 Open 10 Quetiapine 200 200 7/10 70% Sevincok and Topuz 2003
Open 8 Quetiapine 150 150 2/8 25%
Mohr et al. 2002 Chart review
7 Quetiapine 118 25–300 4/7 57%
Erzegovesi et al. 2005
DB-PC 10 Risperidone 0.5 0.5 5/10** 50%
McDougle et al. 2000
DB-PC 20 Risperidone 2.2 1–4 11/20 55%
Hollander et al. 2003
DB-PC 10 Risperidone 2.3 NA 4/10 40%
McDougle et al. 2000
Open 14 Risperidone NA NA 7/14 50%
Pfanner et al. 2000 Open 20 Risperidone 3 3 15/20 75% Saxena et al. 1996 Open 21 Risperidone 2.75 0.5–8 14/21*** 67% Ravizza et al. 1996 Open 17 Risperidone 3 3 7/17 41% Jacobsen 1995 Open 5 Risperidone 3.6 3–6 5/5 100% Stein et al. 1997 Chart
review 8 Risperidone 1.25 1–2 3/8 38%
Bystritsky et al. 2004
DB-PC 13 Olanzapine 11.2 5–20 6/13 46%
Shapira et al. 2004 DB-PC 22 Olanzapine 6.1 5–10 41% = placebo
D’Amico et al. 2003 Open 21 Olanzapine 10 10 7/21 33% Francobandiera et al. 2001
Open 9 Olanzapine 4.4 2.5–5 6/9 67%
Bogetto et al. 2000 Open 23 Olanzapine 5 5 10/23 43% Koran et al. 2000 Open 10 Olanzapine 8.25 5–10 3/10 30% Weiss et al. 1999 Open-
label 10 Olanzapine 7.3 1.25–20 7/10 70%
3 Sources. (Jacobsen 1995; D'Amico et al. 2003; Sevincok & Topuz 2003; Shapira et al. 2004; Carey et al. 2005; Bogan 4 et al. 2005). 5 6 DB-PC = double blind-placebo control; SB-PC = single blind-placebo control. 7 * Responder is defined as ≥25% decrease in Y-BOCS score from baseline to endpoint. 8 ** Responder is ≥35% decrease in Y-BOCS score. 9 *** Y-BOCS score unavailable. Instead, Saxena et al. report “substantial reductions in obsessive-compulsive 10 symptoms.”11

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
47
Significant differences between the antipsychotics and placebo were observed within 4–6 1
weeks. Although some controlled trials found no difference between antipsychotic and 2
placebo augmentation (e.g., (Shapira et al. 2004; Carey et al. 2005)), this was probably 3
due to design limitations, e.g., starting the augmentation before a full SRI effect was 4
obtained or using too small a dose of the antipsychotic drug. Double-blind placebo-5
controlled trials report response rates in the range of 40% to 55% (Table 7). A chart 6
review study found that discontinuing successful augmentation after one to twelve 7
months resulted in relapse for more than 80% (15/18) of patients, most within two 8
months of discontinuation (Maina et al. 2003). 9
Many questions about antipsychotic augmentation in OCD remain unanswered, 10
including the optimal dose for each drug, long-term tolerability, when and how to 11
discontinue treatment, and the reasons that only some patients benefit. In addition, the 12
drugs’ relative efficacy has not been examined. One study (McDougle et al. 1994) 13
suggests that haloperidol helps only OCD patients with co-occurring tic disorders. 14
II.B.7.e. _____Switching to Mirtazapine 15
A study combining an open-label first phase with a double-blind discontinuation phase 16
suggests that mirtazapine may be effective for OCD in patients who have not failed more 17
than one adequate SRI trial (Koran et al. 2005c). 18
II.B.7.f. _____Augmenting an SRI With Other Pharmacotherapies 19
Expert opinion (March et al. 1997; Figueroa et al. 1998) and two open-label studies 20
(Ravizza et al. 1996a; Pallanti et al. 1999) support clomipramine augmentation of 21
SSRIs. If clomipramine is added, plasma levels of clomipramine and 22
desmethylclomipramine should be assayed two to three weeks after reaching a dose of 50 23
mg/day, keeping the total plasma concentration below 500 ng/ml to avoid cardiac and 24
central nervous system toxicity. Fluvoxamine most increases plasma clomipramine levels 25
(Szegedi et al. 1996), but substantial increases may occur with fluoxetine and paroxetine. 26
A screening ECG may be advisable in patients suspected of having heart disease or over 27
the age of 40. Pulse rate and blood pressure should be monitored as the dose is increased. 28
Small, controlled augmentation trials with lithium, buspirone, L-29
Triiodothyronine, inositol, and desipramine have produced generally negative results, 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
48
but design limitations in the lithium and buspirone studies prevent a firm conclusion that 1
these drugs will not help any OCD patients. Positive case reports exist for both drugs. 2
Adding once-weekly oral morphine sulfate 30–45 mg to various SSRIs with or without 3
other augmenters was superior to placebo in a double-blind crossover study (Koran et al. 4
2005a); again, positive case reports exist, along with a postive case series for the weak 5
narcotic agonist, tramadol. Adding pindolol 2.5 mg thrice daily was effective in one 6
small double-blind placebo-controlled trial (Dannon et al. 2000) but not in another 7
(Mundo et al. 1998). 8
A small, 12-week, open-label study reported that augmentation of SSRIs and 9
other augmenting medications utilizing riluzole 50 mg twice daily was often helpful, but 10
severe methodological limitations prevent confidence that the benefit was due to riluzole 11
itself. 12
II.B.7.g. _____Approaches Reported in Case Reports, Case Series, 13
Uncontrolled Trials, or Small Controlled Trials 14
Few data are available regarding psychotherapeutic approaches other than those falling 15
within the umbrella concept of CBT. Kundalini yoga is supported by one small 16
controlled trial, but requires independent replication in a larger sample. Although well 17
tolerated, it cannot be recommended at this time. Additionally, there is no evidence to 18
support the use of hypnosis or acupuncture to treat OCD symptoms. 19
Positive case reports or case series exist for anticonvulsants, MAOIs, 20
ondansetron, L-tryptophan, hallucinogens, and St. John’s wort. A 12-week, flexible-21
dose placebo-controlled trial of St John’s wort, however, found it no better than placebo 22
(Kobak et al. 2005). These treatments should be considered only after first- and second-23
line treatments and well-supported augmentation strategies have been exhausted. One 24
should recall that negative cases are less likely to find their way to publication in the the 25
case report or case series literature. 26
A case series (n=5) reports modest decrease in OCD symptoms in four of five 27
patients treated with nicotine delivered via transdermal patch or chewing gum (Lundberg 28
et al. 2004). Further investigation seems to be indicated. 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
49
The literature on the use of electroconvulsive therapy (ECT) in treatment-1
resistant OCD includes a case series (Maletzky et al. 1994) and several individual cases. 2
However, these reports are marred by a lack of blinded raters and modern outcome 3
measures, non-standard ECT methods and variable administration of concomitant 4
medications. Moreover, ECT carries the risks of anesthesia and objectionable memory 5
impairment. As a result, ECT cannot be recommended for the treatment of OCD, but may 6
be considered for treating co-occurring conditions for which it may be indicated (e.g., 7
major depression, uncontrollable mania, and schizophrenia) (American Psychiatric 8
Association 2000b; American Psychiatric Association 2001; American Psychiatric 9
Association 2002; American Psychiatric Association 2004). 10
Transcutaneous magnetic stimulation (TMS) has been tested in OCD in one 11
double-blind and three open studies, all small. The trial designs differed in important 12
ways: site of stimulation, treatment parameters, and treatment duration. Therefore, 13
notwithstanding the promising findings reported in some trials, conclusions about the 14
efficacy of TMS in OCD cannot be drawn. Of note, TMS demonstrated good tolerability 15
with no drop-outs and only temporary mild side effects. 16
The efficacy of deep brain stimulation in severe, treatment-resistant, or 17
pharmacologically intractable OCD is supported by case reports and two double-blind 18
controlled single-subject studies. Stimulation frequency and amplitude parameters may 19
vary notably across patients; appropriate parameters should be clarified by additional 20
research. 21
The efficacy of neurosurgery (anterior capsulotomy, limbic leucotomy, 22
cingulotomy, and other approaches) in severe, treatment-refractory, or pharmacologically 23
intractable OCD has been evaluated in case reports and unblinded studies. Improvement 24
rates have been up to 35%. Adverse events range from personality changes to transient 25
mania and mild, transient side effects such as urinary dysfunction. The recent 26
development of less invasive (deep brain stimulation) and non-invasive (TMS) 27
procedures makes it harder to consider neurosurgery an alternative for highly treatment-28
resistant or intractable OCD. Although some studies report relatively high rates of 29
improvement, the unblinded nature of these studies and the ongoing treatment of many 30
patients limit one’s confidence in these results. 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
50
II.C._DISCONTINUATION OF ACTIVE TREATMENT 1
For, in disease of the mind, as well as in all other ailments, it is an art of no little 2 importance to administer medicines properly; but, it is an art of much greater and more 3 difficult acquisition to know when to suspend or altogether to omit them. 4
Philippe Pinel, 1745–1826 5 A Treatise on Insanity, Sect. I (tr. D. Davis) 6
7 Four double-blind SRI discontinuation studies have concerned different SRIs, used 8
different designs (e.g., length of observation and method of placebo substitution), and 9
different relapse definitions. These discontinuation studies reported rates of relapse or 10
discontinuation for insufficient clinical response of: 11
• 89% among 18 clomipramine responders during 7 weeks of a blinded switch to 12
placebo, after a minimum of 4 months of clomipramine treatment (Pato et al. 13
1988); 14
• 9% during 28 weeks on continued treatment with sertraline 50–200 mg/day versus 15
24% on placebo (significant), after responding during 52 weeks of sertraline 16
treatment (Koran et al. 2002); 17
• 21% during 52 weeks on continued treatment with fluoxetine 20, 40, or 60 18
mg/day versus 32% on placebo (not significant), after responding during 20 19
weeks of fluoxetine treatment (Romano et al. 2001); 20
• 38% during 6 months of continued treatent with paroxetine up to 60 mg/day 21
versus 59% on placebo (significant), after responding during 9 months of 22
paroxetine treatment (Hollander et al. 2003a). 23
An unblinded discontinuation study, after response to six months of open treatment, 24
reported significantly higher 6-month relapse rates for the patients whose medication was 25
discontinued: 8% (clomipramine 150 mg/day) versus 46% (no drug), 0% (fluoxetine 40 26
mg/day) versus 40% (no drug), and 8% (fluvoxamine 300 mg/day) versus 62% (no drug) 27
(Ravizza et al. 1996a). Equally large or larger disparities were present after one and two 28
years of treatment versus no treatment. 29
In a review of 16 ERP studies, Foa and Kozak (Foa & Kozak 1996) concluded 30
that about three-quarters of patients receiving ERP (with and without concomitant 31
medication) did well after a mean follow-up period of a little more than two years. While 32
suggestive, this finding is inconclusive because of: 1) design limitations in some studies; 33
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
51
2) methodological limitations in others; 3) differences in determining “response”; 4) 1
inconsistencies in whether treatment during follow-up was permitted (and reported); and 2
5) differences in length of follow-up. Because the relapse definition employed in this 3
review differs from those used in the SRI studies, the relapse rates cannot be compared. 4
A multi-site study that compared the effects of clomipramine and ERP after 12 5
weeks of treatment (Foa et al. 2005) and again 12 weeks after discontinuation of 6
treatment (Simpson et al. 2004) found that ERP responders (with or without concomitant 7
clomipramine) had a significantly lower relapse rate (12%) and longer time to relapse 8
than responders to clomipramine alone (45%). Post-hoc analyses using different relapse 9
criteria generally supported these findings, albeit with substantial variability in observed 10
relapse rates (Simpson et al. 2005a). 11
Together, these data suggest that ERP treatment response may be more durable, at 12
least in the short-run, than response to some SRIs once they are discontinued. However, 13
the observed differences could be explained by other factors, including differences in the 14
intensity of treatment before discontinuing it, the rate of medication taper, the subjects 15
studied, the length of follow-up, and the relapse criteria. Thus, no definitive conclusions 16
about the relative durability of SRI and ERP treatment effects can be drawn from the 17
available studies. 18
III. SPECIFIC CLINICAL FEATURES INFLUENCING 19
THE TREATMENT PLAN 20
It is as important to know what sort of person has the disease as to know what sort of 21 disease the person has. 22
Caleb Parry, 1755–1822, English physician and researcher 23 Attributed 24
25
Many of the clinical features that will influence the treatment plan have been mentioned 26
in describing the choice of a treatment setting and methods to enhance adherence. 27
Additional features are described below. 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
52
III.A. PSYCHIATRIC FEATURES 1
In suggesting treatments for adults, the clinician should consider the patient’s response to 2
past treatments, including the benefits and side effects, and the patient’s motivation and 3
ability to comply with pharmacotherapy and psychotherapy. As noted, educational efforts 4
may be needed to enhance treatment motivation. An unstable or stressful living situation 5
will diminish the chances of successful treatment and may require concomitant 6
interventions such as family therapy. 7
Patients whose predominant or only symptom is hoarding (the accumulation or 8
acquisition of items beyond reasonable need or items of little objective value) appear to 9
be less likely to benefit from medications or combined treatment than patients with other 10
symptom patterns, perhaps because they usually demonstrate less insight and less 11
motivation for change (Black et al. 1998; Mataix-Cols et al. 1999; Winsberg et al. 1999; 12
Leckman et al. 2001; Saxena et al. 2002; Bogan et al. 2005) <<Placeholder for Saxena et 13
al. paroxetine study reported at ADAA, 2005>>. Commonly saved items include 14
newspapers, magazines, books, packaging, old clothing, notes, and lists. A biological 15
basis for this poorer treatment outcome is suggested by differences in the pattern of 16
abnormal cerebral glucose metabolism in OCD hoarders compared with non-hoarder 17
OCD patients (Saxena et al. 2004). The hoarding phenotype of OCD has been linked to 18
genetic markers on chromosomes 4, 5, and 17 in families with Tourette’s Disorder 19
(Zhang et al. 2002). Specific treatment programs that achieve benefit have been described 20
(Koran 1999; Steketee & Frost 2003; Saxena & Maidment 2004) but not tested in 21
controlled trials. Appendix A includes a helpful Web site. 22
The degree of insight should be recorded because it may influence the patient’s 23
willingness to cooperate with treatment. The Brown Assessment of Beliefs Scale (Eisen 24
et al. 1998) provides a quantitative measure. Poor insight is associated with poorer 25
response to SRIs in most studies (Denys et al. 2003a; Ravi Kishore et al. 2004) but not all 26
(Eisen et al. 2001), as well as poorer response to cognitive-behavioral therapies in some 27
studies (Foa et al. 1999) but not others (Salkovskis & Warwick 1985; Lelliott & Marks 28
1987; Lelliott et al. 1988). 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
53
III.A.1.______Chronic Motor Tics 1
Co-occurring chronic motor tics, without Tourette’s Disorder, decrease the likelihood of 2
response to fluvoxamine (McDougle et al. 1993a; McDougle et al. 1994) but not to 3
clomipramine (Miguel et al. 2003). Patients with co-occurring tics and OCD 4
unresponsive to an SRI may benefit from the addition of an antipsychotic drug 5
(McDougle et al. 1994; Eapen & Robertson 2000). Although the onset or exacerbation of 6
tics during SSRI treatment is reported in isolated cases (Fennig et al. 1994; Kotler et al. 7
1994), these do not justify withholding SSRIs from OCD patients with co-occurring 8
motor tics. 9
III.A.2.______Tourette’s Disorder 10
OCD co-occurring with Tourette’s Disorder can be treated with SRIs without fear of 11
exacerbating the Tourette’s Disorder (Eapen & Robertson 2000). When OCD fails to 12
respond after one or two adequate SRI trials, adding a first-generation (typical) or 13
second-generation (atypical) antipsychotic drug in low to modest dose may relieve both 14
disorders (Eapen & Robertson 2000). Clinical experience suggests that tic severity may 15
decrease modestly along with OCD symptoms after SRI treatment alone. 16
III.A.3.______Major Depression 17
Co-occurring major depression does not adversely affect the OCD response to SRIs 18
(Den Boer 1997; Denys et al. 2003a). When the OCD responds well and the major 19
depression does not, the clinician has many choices, none of which have been subjected 20
to large double-blind trials. As a result, it is reasonable to apply the treatment strategies 21
outlined in APA’s Practice Guideline for the Treatment of Patients With Major 22
Depressive Disorder (American Psychiatric Association 2000b). These include 23
psychotherapies that are effective in treating depression (i.e., interpersonal 24
psychotherapy, cognitive-behavior therapy or short-term psychodynamic therapy), 25
increasing the SRI dose, adding an antidepressant from another class, adding an 26
augmenting agent, or in severe, refractory, or suicidal depression, utilizing 27
electroconvulsive therapy. In many (Foa et al. 1985; Keijsers et al. 1994; Abramowitz & 28
Foa 2000) but not all (Foa et al. 1992) trials of CBT, co-occurring major depression has 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
54
been associated with a poorer OCD outcome. Severe depression clearly interferes with 1
CBT (Abramowitz et al. 2000). Thus, it may be useful to utilize antidepressant 2
medication, and particularly SRIs, to treat co-occurring major depression before or during 3
a trial of CBT. 4
III.A.4.______Bipolar Disorder 5
In order to minimize the possibility of precipitating hypomania or mania, co-occurring 6
bipolar disorder must be successfully treated before initiating pharmacotherapy for 7
OCD. In bipolar OCD patients, SSRIs appear to be less likely than clomipramine to 8
precipitate hypomania or mania (Perugi et al. 2002). Stabilizing the bipolar disorder may 9
require a combination of medications including lithium, anti-epileptics and/or second-10
generation antipsychotic drugs (American Psychiatric Association 2002). Potential drug 11
interactions should be carefully considered when clomipramine, fluoxetine, fluvoxamine, 12
paroxetine, or sertraline are considered for use in combination with these agents. Episodic 13
OCD, characterized by periods of markedly different symptom severity independent of 14
OCD treatment, appears to be considerably more common in OCD patients with bipolar 15
disorder (Perugi et al. 2002). Thus, a history of episodic OCD should raise the 16
psychiatrist’s suspicion that co-occurring bipolar disorder may be present. Perhaps as a 17
result of co-occurring bipolar disorder, patients with episodic OCD appear to be more 18
likely to suffer from alcohol abuse or dependence (Perugi et al. 2002), which will also 19
require treatment. 20
III.A.5.______Panic Disorder 21
Co-occurring panic disorder may respond to the SSRI utilized to treat the patients’ OCD 22
(American Psychiatric Association 1998). When co-occurring panic disorder or a history 23
of panic attacks is present, SRI treatment should be initiated at low doses and slowly 24
titrated upward over a period of weeks in order to avoid initiating or exacerbating panic 25
attacks (American Psychiatric Association 1998). Alternatively, the clinician can start 26
usual doses of an SRI combined with anti-panic doses of a benzodiazepine for the first 27
month or so and then try to taper off the benzodiazepine over a period of weeks 28
(American Psychiatric Association 1998). If CBT alone is utilized for treating the OCD, 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
55
attention to anxiety management skills (Taylor 2000; Rayburn & Otto 2003) may be 1
needed to prevent exposure therapy from triggering panic attacks. 2
III.A.6.______Social Phobia (Social Anxiety Disorder) 3
Co-occurring generalized social anxiety disorder may respond to the SSRI utilized to 4
treat the patient’s OCD (Blanco et al. 2003). Large double-blind placebo-controlled 5
studies support the effectiveness of escitalopram (Stein et al. 2004), fluoxetine (Davidson 6
et al. 2004), fluvoxamine (Stein et al. 1999), paroxetine (Lepola et al. 2004) and 7
sertraline (van Ameringen et al. 2001), as well as venlafaxine (Liebowitz et al. 2005) and 8
clonazepam (Davidson et al. 1993). Phenelzine, while effective, cannot be combined with 9
SRIs because this combination will elicit the serotonin syndrome. Controlled trials 10
suggest that generalized social anxiety disorder also responds to cognitive and behavioral 11
therapies (Hambrick et al. 2003). In one small study, OCD patients with co-occurring 12
social anxiety disorder experienced a poorer response to SSRI treatment than did those 13
without this co-occurring condition (Carrasco et al. 1992). 14
III.A.7.______Schizophrenia 15
In patients with co-occurring schizophrenia, OCD or OC symptoms may be present 16
independently or may be precipitated or exacerbated by second-generation antipsychotic 17
medications (Lykouras et al. 2003). Some patients have insight into the irrationality of 18
their obsessions and compulsions while lacking insight into their schizophrenic delusions. 19
In other cases, the obsessions and delusions become illogically linked, as for example 20
when the patient believes that obsessions have been inserted into his mind by an external 21
force or that his compulsive rituals control world events. When clinically significant 22
OCD or OC symptoms are present independently, the psychiatrist must rely on clinical 23
judgment in formulating a treatment plan, since no large, controlled trials have been 24
conducted. The patient’s antipsychotic regimen should first be stabilized. A review of the 25
treatment literature (Poyurovsky et al. 2004) suggests that SRIs are usually well tolerated 26
and can be beneficial, but isolated reports of psychotic exacerbation exist. Olanzapine 27
monotherapy has been beneficial in two case series. Adding fluvoxamine has been 28
helpful in two open trials, and adding fluoxetine, paroxetine, or sertraline in individual 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
56
cases. Clozapine has been reported to both induce and relieve OC symptoms in patients 1
with schizophrenia. The case reports suggest that low doses (75–300 mg/day) and slow 2
upward titration are indicated (Poyurovsky et al. 2004). When a second-generation 3
antipsychotic drug induces OC symptoms, they may disappear within a few weeks. If not, 4
treatment options include adding an SRI, switching to another second-generation 5
antipsychotic, or attempting a trial of cognitive-behavioral therapy. No controlled trials 6
exist to guide treatment planning, but reviewing the results of published cases (Lykouras 7
et al. 2003; Poyurovsky et al. 2004) may be helpful. Potential drug interactions must be 8
borne in mind. 9
III.A.8.______Substance Use Disorders 10
Because co-occurring alcohol or substance abuse or dependence can interfere with 11
treatment adherence and response and bring risks of drug interactions, these disorders 12
must be treated either before or while treating the patient’s OCD. Several organizations 13
have published guidelines to aid in treatment planning (VA/DoD Evidence-Based 14
Clinical Practice Guideline Working Group 2001; Substance Abuse and Mental Health 15
Services Administration 2005; American Psychiatric Association 2006b). 16
III.A.9.______Personality Disorders 17
Although the majority of studies suggest that personality disorders are common in 18
patients with OCD (Steketee et al. 2000), the literature is mixed with regard to their 19
impact on treatment outcome, whether from pharmacotherapy or CBT. Attempts to draw 20
conclusions are hampered by methodological problems such as small sample sizes, 21
differing diagnostic criteria, difficulties in validly measuring the presence/absence of 22
these disorders (Perry 1992), retrospective study design, differing lengths of follow-up, 23
and poorly defined outcome criteria. Some personality traits (e.g., passive-aggressive) 24
and disorders (e.g., borderline personality disorder) have been reported to interfere with 25
adherence to treatment (Hermesh et al. 1987; Fricke et al. 2005). Other traits (e.g., the 26
odd thinking style in schizotypal personality disorder) or particular disorders (especially 27
schizotypal personality disorder (Baer et al. 1992; Ravizza et al. 1995)) have been 28
associated with poor outcome for unclear reasons in some but not all studies (Dreessen et 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
57
al. 1997; Fricke et al. 2005). Thus, the presence of a co-occurring personality disorder 1
should alert the clinician to consider whether treatments should be provided to target the 2
personality disorder. Obsessive-compulsive personality disorder, for example, has been 3
reported to be improved by psychodynamic psychotherapy or individual psychotherapy 4
with an expressive emphasis (Gunderson 1988; McCullough & Maltsberger 2001; 5
Gabbard & Newman 2005) as well as CBT (Beck 1997). Psychodynamic principles may 6
also help the psychiatrist understand and address resistances to treatment and transference 7
and countertransference issues (Gabbard 2005). For example, patients with obsessive-8
compulsive personality disorder (OCPD) may feel threatened by a lack of control in 9
therapy, deny negative and painful feelings, intellectualize feelings, or resist becoming 10
“dependent” on medications or therapy. Strategies to enhance the therapeutic alliance 11
with patients with co-occurring OCPD include respecting the patient’s defenses, helping 12
the patient embrace his or her humanness, enlisting the patient’s collaboration in 13
treatment planning, and empathizing with the patient’s feelings of shame and fear 14
(Gabbard 2005). 15
III.A.10._____General Medical Conditions Inducing OCD 16
OCD or obsessive-compulsive symptoms not meeting DSM-IV-TR diagnostic criteria 17
can be manifestations of a number of general medical conditions including brain 18
trauma, stroke, encephalitis, temporal lobe epilepsy, Prader-Willi syndrome, 19
Syndenham’s chorea, neurodegenerative diseases such as Parkinson’s disease and 20
Huntington’s disease, CO poisoning, and manganese poisoning (Koran 1999; Weiss & 21
Jenike 2000; Isaacs et al. 2004). Treatment is first directed to the underlying medical 22
condition when this is possible. When OCD symptoms persist after treatment or 23
stabilization of the underlying condition, isolated case reports suggest that treatment with 24
an SRI and/or cognitive-behavioral therapy may be of some benefit. No controlled 25
treatment trials have been conducted in patients with OCD induced by general medical 26
conditions. 27
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
58
III.B. DEMOGRAPHIC AND PSYCHOSOCIAL FACTORS 1
III.B.1.______Children and Adolescents 2
In children and adolescents, treatment should often start with psychotherapy or with a 3
combination of psychotherapy and an SSRI. Since there is controversy about a possible 4
increase in the risk of suicidal thinking in children and adolescents treated with 5
antidepressants, treating OCD with an SSRI alone in these groups with only infrequent 6
clinical contact early in treatment should be avoided. However, the use of SSRIs in 7
treating children and adolescents with both OCD and major depression may be necessary 8
and should not be avoided (Food and Drug Administration 2004; American Psychiatric 9
Association & American Academy of Child and Adolescent Psychiatry 2004a; American 10
Psychiatric Association & American Academy of Child and Adolescent Psychiatry 11
2004b; Cheung et al. 2005; Ryan 2005; Wanger 2005). 12
III.B.2.______Ethnicity 13
Pharmacogenetic influences on the probability of therapeutic outcomes and adverse 14
reactions to SRIs are beginning to be reported. Differences in neurotransmitter transporter 15
and receptor genotypes are beginning to be implicated in predicting therapeutic response. 16
Differences in the prevalence of CYP450 slow, normal, extensive, and ultra-rapid 17
metabolizers of psychotropic medications, and hence pharmacokinetic contributions to 18
rates of adverse events, are being associated with ethnicity (Kirchheiner et al. 2001). 19
Gene chips are being introduced to avoid both adverse responses and metabolism-related 20
treatment failures by identifying CYP450 genotypes. Data indicate that 13% to 23% of 21
Asians are CYP2C19 poor metabolizers compared to 2% to 5% of Caucasians, and thus 22
should receive about 60% of the average dose of clomipramine (Kirchheiner et al. 2004). 23
CYP2D6 poor metabolizers may require lower doses of paroxetine, which is both an 24
inhibitor and a substrate for this enzyme (Kirchheiner et al. 2004). The data are too sparse 25
to support guidelines at present, but psychiatrists should remain alert for helpful 26
information. 27
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
59
III.B.3.______Pregnancy and Breast-Feeding 1
Deciding whether to start or stop a psychotropic drug during pregnancy or breast-2
feeding requires making a risk-benefit calculation in the absence of complete 3
information. Risks to the well-being of the fetus, the infant and the mother occur whether 4
medications are started or stopped, since the mother’s health will influence the outcome 5
of pregnancy and post-partum infant care. A model to integrate and weigh the elements 6
of decision-making in this situation has been proposed (Wisner et al. 2000). In counseling 7
the female patient and her concerned others, the physician should provide clear 8
summaries of the available data and, if desired, aid in obtaining more detailed data. Two 9
helpful Web sites are listed in Appendix A. Consultation with the patient’s obstetrician-10
gynecologist should be offered. Because OCD patients are often quite anxious, 11
experience doubting, and can suffer from perfectionism or a need for certainty, helping 12
the patient and her significant other reach an informed decision may take several 13
sessions. Medico-legal considerations make it advisable to document the information 14
provided and the individual’s agreement to accept full responsibility for the decisions 15
made. CBT alone should be considered during pregnancy and while a patient is breast-16
feeding, and for patients wishing to become pregnant. 17
OCD symptom onset during pregnancy has been reported in 13% (Williams & 18
Koran 1997) to 39% (Neziroglu et al. 1992) of women with OCD who have been 19
pregnant. The severity of pre-existing OCD is usually unaffected by pregnancy but has 20
been reported to worsen in from 8% (Labad et al. 2005) to 17% (Williams & Koran 21
1997) and to improve in 14% (Williams & Koran 1997). (Premenstrual worsening of 22
OCD has been reported in from 20% (Labad et al. 2005) to 42% (Williams & Koran 23
1997) of women.) 24
The available data suggest that exposure to tricyclics, fluoxetine, fluvoxamine, 25
paroxetine, or sertraline does not increase rates of intrauterine death (Wisner et al. 2000). 26
The available data do not suggest increased rates of major malformations after in utero 27
exposure to citalopram or escitalopram (Einarson & Einarson 2005), fluoxetine, 28
paroxetine, sertraline, or tricyclics (Wisner et al. 2000; Simon et al. 2002) or fluvoxamine 29
(Kulin et al. 1998). The data are conflicting regarding whether SSRI exposure decreases 30
birth weight or increases rates of premature delivery (Nordeng & Spigset 2005). A 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
60
neonatal behavioral syndrome including central nervous system, motor, respiratory, and 1
gastrointestinal signs may occur but is usually mild, can usually be managed with 2
supportive care, and disappears by two weeks of age (Moses-Kolko et al. 2005). Thus, 3
monitoring a neonate exposed to SSRIs in the third trimester is warranted. Since the 4
severity of OCD symptoms may not rapidly increase when medication is tapered, 5
tapering the patient’s SRI dose during the last weeks of pregnancy may be considered to 6
further reduce the risk of the neonatal behavioral syndrome. The very limited data 7
regarding long-term effects of exposure to tricyclics or SSRIs throughout pregnancy do 8
not suggest an elevated risk of abnormalities in cognitive function, language, 9
temperament, or general behavior between ages 15 and 71 months (Nulman et al. 2002). 10
Another study found no evidence for developmental delay up to 2 years of age associated 11
with exposure in utero to tricyclics, fluoxetine, sertraline, or paroxetine at varying times 12
and for varying durations (Simon et al. 2002). Although there are no data specific to 13
OCD, increases in the SSRI dose in the early third trimester have been needed to 14
maintain remission in major depression. 15
The pharmacokinetic, pharmacodynamic, and safety considerations in 16
administering SRIs and other psychotropic drugs in pregnancy (and during breast-17
feeding) are reviewed elsewhere (Newport et al. 2004). This review also notes that a large 18
database supports the relative safety of administering first-generation antipsychotics, 19
especially trifluoprazine and perphenazine, during pregnancy. The data regarding second-20
generation antipsychotics consists only of case reports and case series totaling fewer than 21
100 children for any individual drug except clozapine, where the total approaches 150 22
children. The FDA classifies all second-generation antipsychotics in pregnancy as risk 23
Category C (“Risk cannot be ruled out”), except clozapine, which is in Category B (“No 24
evidence of risk in humans”). A literature review (Newport et al. 2004) concludes that 25
benzodiazepines are apparently not associated with a significant risk of somatic 26
teratogenesis, but the risk of neurobehavioral effects is unclear because of conflicting 27
reports. The reviewers recommend tapering these drugs before delivery when possible 28
and utilizing benzodiazepines in FDA Category C (clonazepam) or those with less 29
potential for fetal accumulation (lorazepam and oxazepam). 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
61
The available data concerning the effects on the infant of maternal SSRI ingestion 1
during breast-feeding are derived from only a few hundred infants. The data suggest that 2
the risk of contemporaneous, noticeable effects is quite low (Newport et al. 2004; 3
Weissman et al. 2004). Cases of respiratory depression, hypotonia, poor feeding, 4
irritability, and uncontrollable crying have been reported (Weissman et al. 2004). There 5
are no reports of long-term adverse effects of exposure, but in the absence of large, 6
controlled trials or observational studies, caution remains in order. The American 7
Academy of Pediatrics Committee on Drugs recommends that a nursing mother be 8
informed that the infant will be exposed to maternal medications (American Academy of 9
Pediatrics 2001). No consensus exists regarding how best to measure infant exposure 10
(Stowe et al. 2003), but sertraline and paroxetine appear least likely to produce detectable 11
or elevated infant plasma drug levels (Weissman et al. 2004). Monitoring maternal or 12
breast milk antidepressant levels is not recommended (Weissman et al. 2004). Discarding 13
the breast milk 8 to 9 hours after taking sertraline reduces infant exposure by a little more 14
than 15% (Stowe et al. 2003). Data helpful in evaluating the risks and benefits of taking 15
other psychotropic drugs during breast-feeding are reviewed elsewhere (Burt et al. 2001; 16
Newport et al. 2004). 17
III.C. TREATMENT IMPLICATIONS OF CONCURRENT GENERAL MEDICAL 18 DISORDERS 19
Co-occurring medical conditions and any medications being used to treat them must be 20
considered when choosing pharmacotherapies for OCD. In particular, the effects of 21
kidney and liver disease upon drug metabolism and the potentials for pharmacokinetic 22
and pharmacodynamic drug interactions must be reviewed. SSRIs would be preferred 23
over clomipramine in individuals a) with epilepsy because of lower seizure risk, b) with 24
cardiac arrythmias, congestive heart failure, or blood pressure abnormalities 25
because of relative cardiovascular safety, and c) who are overweight because of a lesser 26
likelihood of stimulating appetite. The psychiatrist should recall that SSRIs have been 27
associated with cases of bradycardia, hypertension, hyponatremia, bleeding, easy 28
bruising, nausea, diarrhea, constipation, changes in urination, extrapyramidal symptoms, 29
and other symptoms that can be confused with manifestations of co-occurring medical 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
62
conditions or treatments (Koran 1999). SSRIs are not contraindicated in migraine 1
headache patients taking triptans (Evans & Lipton 2001) nor in patients with Parkinson’s 2
disease, although there are isolated case reports of worsened motor functioning (Tesei et 3
al. 2000; Vajda & Solinas 2005). In individuals with diabetes mellitus, selecting second-4
generation antipsychotics with the least likely effect on glucose metabolism and appetite 5
is important (American Psychiatric Association 2004; American Diabetes Association 6
2004). In all cases, the potential for interactions between the patient’s medical and 7
psychiatric medications should be reviewed. <<additions?>> 8
PART B: BACKGROUND INFORMATION AND 9
REVIEW OF AVAILABLE EVIDENCE 10
IV. DISEASE DEFINITION, EPIDEMIOLOGY, 11
NATURAL HISTORY, COURSE, AND GENETICS 12
IV.A. DISEASE DEFINITION 13
The conceptualization of OCD has changed over the last two centuries (Berrios 1996). 14
Obsessions, marked by preserved insight, were gradually distinguished from delusions; 15
compulsions were distinguished from various paroxysmal, stereotyped, and impulsive 16
behaviors. DSM-IV-TR identifies the essential features of OCD as “recurrent obsessions 17
or compulsions (Criterion A) that are severe enough to be time consuming (i.e., they take 18
more than 1 hour a day) or cause marked distress or significant impairment (Criterion 19
C).” The full criteria set is shown in Table 1. DSM-IV-TR describes obsessions as 20
intrusive, persistent, unwanted thoughts, impulses, or images that give rise to marked 21
anxiety or distress. Compulsions are physical or mental acts that the patient feels driven 22
to perform in order to magically prevent some feared event, undo some thought, or 23
reduce anxiety or distress. Compulsive acts are carried out repetitively, excessively, and 24
usually according to rules or in a rigid manner. Compulsions are distinguished from 25
repetitive behaviors motivated by pleasure or gratification. 26
The psychiatrist should differentiate between obsessions and mental rituals or 27
compulsions, since the cognitive-behavioral therapy approaches to these symptoms 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
63
differ. Obsessions occur spontaneously or are evoked by a feared environmental stimulus 1
or event and generate anxiety or distress. Mental compulsions such as counting, praying, 2
or reviewing actions, conversations, or lists are initiated by the patient willfully, albeit 3
usually reluctantly, with the aim of reducing anxiety or distress. 4
The DSM-IV (and DSM-IV-TR) diagnostic criteria differ from those in DSM-III-5
R in allowing a diagnosis of OCD when insight into the irrationality or excessiveness of 6
obsessions or compulsions is severely compromised or absent. The field trial of the 7
DSM-IV criteria (Foa et al. 1995) reported that 8% of OCD patients currently lacked 8
insight and 5% had never had insight. Thus, DSM-IV and DSM-IV-TR incorporate a 9
specifier, “with poor insight,” and allow an additional diagnosis of delusional disorder 10
(297.1) or psychotic disorder not otherwise specified (289.9) when obsessions are of 11
delusional intensity. The DSM-IV and DSM-IV-TR criteria also clarify that the 12
“neutralizing thoughts” mentioned in DSM-III-R are mental compulsions, not obsessions. 13
The DSM-IV field trial revealed that most patients with OCD have both 14
obsessions and compulsions (Foa et al. 1995). The Y-BOCS symptom checklist indicated 15
that 96% of OCD patients had obsessions and compulsions, 2% predominantly 16
obsessions and 2% predominantly compulsions. Clinicians rated about 49% of patients as 17
troubled equally by obsessions and compulsions, nearly 30% as troubled predominantly 18
by obsessions and about 21% predominantly by compulsions. 19
The most common themes of obsessions are fears of contamination; of being a 20
victim (as in a burglary) or perpetrator of aggression (as in murder); of making a 21
significant mistake (e.g., leaving a stove on, a door unlocked, a bill incorrectly paid); of 22
committing a religious offense or moral infraction; of contracting a disease; and, of 23
committing pedophilic or homosexual acts or of being considered homosexual. Hoarding, 24
when a symptom of OCD, is not usually feared, though it may be regretted. In addition, 25
individuals with OCD may obsess about orderliness or symmetry, lucky or unlucky 26
numbers or colors, needing to know (e.g., everything in the news or every word in a 27
movie), heterosexual acts, or bodily health. Obsessions are often accompanied by a 28
feeling of doubt, uncertainty, or incompleteness that drives repetitive thought or action. 29
Obsessive thinking is often colored by an inflated estimate of danger, an increased sense 30
of responsibility, or a need for certainty or perfection. Re-investigating the nature and 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
64
extent of symptoms after a therapeutic alliance has been established may be helpful since 1
patients may not reveal embarrassing symptoms in a first visit. 2
Since compulsions are usually performed in response to obsessions, the common 3
themes are similar: cleaning, checking, harm avoidance, undoing, asking for reassurance 4
or confessing, accumulating (hoarding), arranging, repeating, praying, and counting. 5
IV.B. EPIDEMIOLOGY 6
Clinically significant OCD is not uncommon. For DSM-IV OCD, the 1-month prevalence 7
in adults is estimated to be 0.6% (Stein et al. 1997). Estimates of the 12-month 8
prevalence in adults range from 0.6% to 1.0% for DSM-IV OCD (Crino et al. 2005; 9
Kessler et al. 2005a)and 0.8% to 2.3% for DSM-III-R OCD (Karno et al. 1988). The 10
lifetime prevalence in adults is estimated to be 1.6% (Kessler et al. 2005b). The World 11
Health Organization places OCD among the ten most disabling medical conditions 12
worldwide (Murray & Lopez 1996) and the National Comorbidity Survey Replication 13
indicates that OCD is the anxiety disorder with the highest percentage (50.6%) of serious 14
cases (Kessler et al. 2005b). DSM-IV OCD is rare in young children, but its prevalence 15
rises exponentially with increasing age through adolescence (Heyman et al. 2001). 16
In contrast to the prevalence rates of DSM-IV OCD, the mean lifetime prevalence 17
of DSM-III OCD was 2.5% across five U.S. catchment areas (Karno et al. 1988). The 18
lifetime prevalence rates of DSM-III OCD in seven countries ranged from 0.7% (in 19
Taiwan) to 2.5% (in Puerto Rico) (Weissman et al. 1994). The differences in OCD 20
prevalence rates between studies using DSM-III and DSM-IV criteria have been 21
attributed to refinements in diagnostic interviews and to changes in DSM-III-R and 22
DSM-IV that better defined obsessions and compulsions while also emphasizing the 23
degree of distress and impairment required for diagnosis (Crino et al. 2005). In contrast to 24
the prevalence of clinical OCD, up to 80% of the general population may experience 25
intrusive, unpleasant, or unwanted thoughts (Salkovskis & Harrison 1984) and about 50% 26
may engage in ritualized behaviors (Muris et al. 1997). 27
The mean age of OCD onset ranges in epidemiological studies between 22 and 35 28
years, with at least one-third of cases beginning by 15 years (Burke et al. 1990; 29
Weissman et al. 1994). The National Comorbidity Survey Replication reported a median 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
65
age at onset of 19 years, with 21% of cases starting by age 10 (Kessler et al. 2005a). A 1
second incidence peak occurs in both males and females in middle to late age in some 2
studies (Nestadt et al. 1998). However, others report that onset of OCD after age 50 is 3
relatively unusual (Weiss & Jenike 2000). 4
Males generally have earlier onset than females, possibly contributing to a 5
preponderance of males in most clinical samples of children and adolescents with OCD 6
and of adults with early-onset OCD (Geller et al. 1998; Fontenelle et al. 2003; Tukel et 7
al. 2005). However, several epidemiological studies of children and adolescents reported 8
equal rates in boys and girls (Flament et al. 1988; Heyman et al. 2001). A slight female 9
predominance is reported in epidemiological studies by age 18 years (Douglass et al. 10
1995), a pattern found in most adult samples (Burke et al. 1990; Weissman et al. 1994; 11
Nestadt et al. 1998). The disorder is evenly distributed across socioeconomic strata in 12
most studies, although there tends to be a paucity of minority subjects in epidemiological 13
and clinical studies in the United States (Karno et al. 1988). 14
Although the symptoms of OCD are virtually identical in children and adults, 15
there appear to be important clinical differences between early- and late-onset OCD. 16
Early-onset OCD has been associated with higher symptom severity ratings (Rosario-17
Campos et al. 2001; Fontenelle et al. 2003), higher rates of compulsions without 18
obsessions (Geller et al. 1998), and higher rates of clinically significant obsessive-19
compulsive symptoms (Sobin et al. 2000; Fontenelle et al. 2003). It has also been 20
associated with higher rates of co-occurring tic disorders (Eichstedt & Arnold 21
2001)<<GH: Which MILLET 2004 ref here?>>, attention-deficit hyperactivity disorder 22
(ADHD), and multiple anxiety disorders (Geller et al. 2001). 23
There are no established environmental risk factors for OCD. However, 24
streptococcal infection may be associated with a form of early-onset OCD that involves 25
an abrupt onset of obsessive-compulsive symptoms and co-occurring tics, often 26
abbreviated PANDAS for pediatric autoimmune disorders associated with strep (Giulino 27
et al. 2002; Snider & Swedo 2003; Murphy et al. 2004). 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
66
IV.C. NATURAL HISTORY AND COURSE 1
In attempting to describe the natural history and course of OCD, one is handicapped by 2
the methodological limitations of available studies. These include differences in sampling 3
settings; criteria for diagnosis, inclusion, improvement, or deterioration; reliance on 4
subjects’ recall of distant histories; and varying intervening treatment histories. 5
Retrospective studies with a mean follow-up of at least 10 years and conducted before 6
effective pharmacotherapies became available reported improvement rates of 32% to 7
74% (cited in Skoog and Skoog, 1999 (Skoog & Skoog 1999)). In a unique study, one 8
psychiatrist twice evaluated 144 adult patients aged 19–52 years who had been admitted 9
for inpatient treatment of OCD symptoms in Göteborg, Sweden, between 1947 and 1953. 10
The first evaluations occurred between 1954 and 1956 and the second between 1989 and 11
1993, providing follow-ups after a mean of 47 years (Skoog & Skoog 1999). After 12
varying histories of treatment or no treatment, about two-thirds of the patients improved 13
within a decade of OCD onset, and 83% by the end of the study. Nearly half (48%) 14
experienced a “clinical recovery” (no clinically relevant symptoms for ≥5 years), but only 15
20% achieved a full remission (no symptoms in the previous five years). At the second 16
evaluation, 80% had clinical (52%) or subclinical (obvious symptoms without distress or 17
interference) (28%) symptoms; 9% showed no improvement; 8% had experienced a 18
deteriorative course. Of those who were ill at the first evaluation (n=125), 50% had a 19
chronic course (≥5 years of continuous symptoms of the same degree), 25% an 20
intermittent course (≥2 episodes with symptom-free intervals), 12% an episodic course 21
(one episode lasting <5 years), and 2% were unspecified. Relapses occurred after 20 22
years of remission (absence of clinical symptoms) in 17% of subjects. However, of those 23
in remission at the first evaluation, 46% remained in remission for at least 30 years. 24
Retrospective diagnostic evaluation indicated that 85% of the subjects met DSM-IV 25
diagnostic criteria. 26
Similar statistics regarding course were reported for a cohort admitted to the 27
University of Pisa, Italy, outpatient treatment program, meeting DSM-III-R diagnostic 28
criteria and followed up after at least 10 years of illness: 27% had an intermittent course 29
(≥6 months of full symptom remission) [termed “episodic” by the authors], and 73% had 30
a chronic course (stable or fluctuating symptoms or deterioration) (Perugi et al. 1998). A 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
67
U.S. study of 200 OCD outpatients meeting DSM-III-R criteria reported that 85% had a 1
continuous course with waxing and waning symptoms, 2% an episodic course with full 2
remissions of ≥6 months, and 10% a deteriorative course (Rasmussen & Eisen 1988). 3
Only one study has involved a long-term follow-up of a community sample of 4
OCD subjects (Angst et al. 2004). The number of OCD subjects is, unfortunately, small 5
(n=22). The investigators attempted six evaluations over a 20-year period of OCD cases 6
first diagnosed at ages 19 and 20 years in Zurich, Switzerland. The long-term outcomes 7
were favorable. After a mean follow-up period of 12.9 years, 86% had no symptoms, 9% 8
had symptoms and moderate distress, and only 5% met DSM-IV diagnostic criteria. Only 9
one-third had received treatment. 10
These studies suggest that individuals whose OCD leads them into treatment 11
experience a more chronic and troubling course than do all cases occurring before age 20 12
and ascertained through community survey. Only larger community studies can confirm 13
or refute this impression. 14
IV.D. GENETICS 15
IV.D.1. _____Twin and Family Studies 16
The genetic epidemiology of OCD has been examined in twin and family studies but not 17
in adoption studies (Hettema et al. 2001). Both twin and family studies provide evidence 18
that genetic factors are involved in the transmission and expression of OCD. In two of the 19
larger twin studies, concordance rates ranged from 80% to 87% for monozygotic twins 20
and from 47% to 50% for dizygotic twins (INOUYE 1965; Carey & Gottesman 1981). 21
Heritability is defined as the ratio of the genetic variance (i.e., that attributable to 22
genotypic differences among individuals) to the total phenotypic variance in the 23
population (Khoury et al. 1993). In a study with 419 twin pairs, the heritability estimate 24
for obsessive-compulsive symptoms was 47%, suggesting that just under half the 25
variation was due to genetic factors (Clifford et al. 1984). In a study with 527 female twin 26
pairs, the best-fit model suggested heritabilities of 33% and 26%, respectively, for factors 27
roughly corresponding to obsessions and compulsions (Jonnal et al. 2000). By way of 28
comparison, the heritability of panic disorder has been estimated to be in the range of 29
43% (Kendler & Diehl 1993; Cannon et al. 1998; Hettema et al. 2001). 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
68
Controlled family studies using adult probands have found that the lifetime 1
prevalence of OCD is significantly higher in cases compared with control relatives 2
(10.3% to 11.7% vs. 1.9% to 2.7%) (Pauls et al. 1995; Nestadt et al. 2000b). A meta-3
analysis of data from five family studies with adult probands found a summary odds ratio 4
of 4.0 for OCD in case and control first-degree relatives (Hettema et al. 2001). “Odds” 5
means the ratio of the probability of an event occurring to the probability of it not 6
occurring. The “odds ratio” in a case/control study is the ratio of the odds of the disease 7
occurring in case relatives to the odds of it occurring in control group relatives. 8
In family studies utilizing adult probands, an early age at onset of obsessive-9
compulsive symptoms has been strongly associated with a more familial form of OCD 10
(Bellodi et al. 1992; Pauls et al. 1995; Nestadt et al. 2000b). Although family studies 11
using pediatric probands have often lacked control groups and yielded divergent results, a 12
recent controlled family study utilizing pediatric probands found that the lifetime 13
prevalence of OCD was significantly higher in case compared with control relatives 14
(22.5% vs. 2.6%) (Hanna et al. 2005b). In addition, first-degree relatives of probands 15
with ordering compulsions had a significantly higher lifetime prevalence of definite and 16
subthreshold OCD than relatives of case probands without ordering compulsions (45.4% 17
vs. 18.8%) (Hanna et al. 2005b). A similar pattern with symmetry and ordering 18
symptoms was noted in a segregation analysis of family data (Alsobrook et al. 1999; 19
Pauls & Alsobrook 1999). These findings suggest that ordering compulsions may 20
characterize a more familial and possibly more etiologically homogeneous form of OCD. 21
IV.D.2. _____Genetic Linkage and Candidate Gene Studies 22
A genome scan has found suggestive evidence for linkage on chromosome 9p24 (Hanna 23
et al. 2002), which has been replicated by an independent research group (Willour et al. 24
2004). A genome scan of hoarding in affected sibling pairs with Tourette’s disorder 25
found significant allele sharing for hoarding phenotypes for markers at 4q34-35, 5q35.2-26
35.3, and 17q25 (Zhang et al. 2002). Association studies examining candidate genes in 27
the 9p24 region have produced mixed results, with one study finding modest association 28
at two microsatellite markers flanking SLC1A1 (Willour et al. 2004) and another finding 29
no evidence of association at two single nucleotide polymorphisms (SNPs) in SLC1A1 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
69
intron 3 (Veenstra-VanderWeele et al. 2001). SLC1A1, which codes for the glutamate 1
transporter EAAC1 (EAAT3), is the most promising candidate gene in the region shared 2
by the 9p24 linkage findings and the reported 9p monosomy. 3
Numerous other studies have examined genetic loci, mainly associated with 4
serotonergic, dopaminergic, or glutamatergic pathways or immunological processes, as 5
functional candidate genes for OCD (e.g., (Mundo et al. 2002; Hall et al. 2003; Millet et 6
al. 2003; Arnold et al. 2004; Chabane et al. 2004; Zai et al. 2004)). Results have been 7
mixed. A missense mutation has been described in the serotonin transporter gene that 8
appears to be associated with a complex neurobehavioral syndrome that includes OCD, 9
social phobia, and Asperger’s disorder (Ozaki et al. 2003). 10
V. REVIEW AND SYNTHESIS OF AVAILABLE 11
EVIDENCE 12
Let us remember always that whatever truth we may get by scientific study about 13 ourselves and our environment is always relative, tentative, subject to change and 14 correction, and that there are no final answers. 15
Chauncy D. Leake, 1896–1978 16 New York State Journal of Medicine 1960; 60:1496 17
V.A. MEDICATIONS 18
In the following summaries of pharmacological treatment outcome studies, outcomes are 19
given for the intent-to-treat (ITT) sample with the last-observation-carried-forward 20
(LOCF) method unless otherwise indicated. ITT results inform the clinician of what 21
outcome to expect when considering all patients exposed to a treatment. Results reported 22
for study completers, by contrast, indicate what to expect for those exposed to completed 23
durations of treatment. Finally, visit-wise outcome results indicate likely outcomes for 24
patients exposed to those particular durations of treatment. In considering “responder” 25
rates reported in OCD pharmacotherapy studies, it may be helpful to keep in mind the 26
responder rates reported in subjects in the placebo arms of such studies. As noted 27
previously in Section II.B.6, “responders” are variously defined as subjects who 28
experience a ≥25% or ≥35% decrease in Y-BOCS score or a CGI-I score 1 (very much 29
improved) or 2 (much improved), usually after 12 weeks of treatment. In one analysis of 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
70
studies published before the year 1997, responder rates in placebo subjects ranged from 1
0% to 35% (mean 15%), with later studies generally reporting higher placebo response 2
rates (Ackerman & Greenland 2002). In the interest of brevity, the above responder 3
criteria are symbolized in this section as follows: YBOCS-25%, YBOCS-35%, CGI-I:1,2. 4
No demographic or clinical variables are sufficiently accurate predictors of 5
treatment outcome to permit their use in selecting medications (Denys et al. 2003a). The 6
recent availability of gene chips that can be used to identify slow or rapid drug 7
metabolizers may allow more informed drug choice in the near future (Mrazek 2004). 8
V.A.1. ______Clomipramine 9
Clomipramine is a mixed serotonin and norepinephrine reuptake inhibitor (and 10
cholinergic and histaminic blocking agent) which was approved by the FDA in 1989 for 11
the treatment of OCD. It was introduced in Europe in 1966 for treating depression and 12
was subsequently used for OCD . 13
Randomized controlled studies have found clomipramine significantly superior to 14
placebo in the treatment of OCD. Trials directly comparing clomipramine with certain 15
SSRIs (e.g., fluoxetine, fluvoxamine, and paroxetine) report equal effectiveness. 16
However, in some studies the SSRIs appear to have better tolerability. Sample sizes limit 17
the power of most of these studies to detect differences, and most studies do not include a 18
placebo comparison group. 19
Clomipramine is recommended for treating OCD, but safety and tolerability 20
issues favor the SSRIs. No adequate studies have determined the minimally effective or 21
optimal clomipramine dosage. 22
The Clomipramine Collaborative Study (The Clomipramine Collaborative Study 23
Group 1991), the first large, double-blind placebo-controlled trial in the United States of 24
a pharmacotherapy for OCD, was a landmark for the treatment of OCD in general, and 25
clomipramine specifically. This 10-week double-blind placebo-controlled multi-center 26
study included 260 subjects in each group. Subjects who had not received prior 27
behavioral therapy or clomipramine and scored ≥16 on the Y-BOCS and ≥7 on the NIMH 28
OC Scale were included. Subjects took clomipramine at least 200 mg/day, with the 29
opportunity to increase to 300 mg/day. The mean Y-BOCS score decreased 40% 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
71
compared with 4% in the placebo group. The clomipramine YBOCS-35% responder rate 1
rate (55%) far exceeded that in the placebo group (7%). Many additional randomized 2
double-blind placebo-controlled or active comparator studies support the effectiveness of 3
clomipramine treatment of OCD (Piccinelli et al. 1995; Ackerman & Greenland 2002). 4
Katz et al. (Katz et al. 1990) conducted a 1-year extension in a subsample 5
(N=134) of participants in the prior study. OCD symptoms fell to the subclinical range in 6
50% of the clomipramine group, compared with 4% of the placebo group. Clomipramine 7
CGI-I:1,2 responder rates were 50% versus 7% for placebo. Adverse reactions, however, 8
led 17/129 (13%) clomipramine subjects to drop out of the study. 9
These studies suggest that clomipramine in doses of up to 250 mg/day is an 10
effective treatment for OCD. Adverse effects, especially anticholinergic and 11
cardiovascular effects and weight gain, are common; however, drop-out rates are not high 12
except as reported in one study (Zohar & Judge 1996). Clomipamine may elevate liver 13
transaminases, and a potential for seizures exists at doses exceeding 250 mg/day. 14
Several studies have compared clomipramine with other medications (see 15
summaries of SSRIs for additional studies). Pigott et al. (Pigott et al. 1990) compared 16
clomipramine 250 mg/day (n=5) to fluoxetine 40 mg/day (n=6) in a small cross-over trial 17
of 10 weeks on each drug with a 4-week washout period interposed. The Y-BOCS score 18
decreased significantly in both groups, with no between-group significant difference. 19
Lopez-Ibor et al. (Lopez-Ibor, Jr. et al. 1996) found no difference in Y-BOCS score 20
decrease in an 8-week double-blind comparison of clomipramine 150 mg/day (n=25) and 21
fluoxetine 40 mg/day (n=30). The YBOCS-25%, but not the YBOCS-35% responder rate 22
was significantly higher for clomipramine. The drugs did not differ in drop-out rates. 23
This was, however, a small study with no placebo control arm and which used low 24
dosages of both medications. 25
A meta-analysis of studies comparing clomipramine and fluoxetine reported a 26
greater effect size for clomipramine (1.84) than fluoxetine (1.34) (Jenike et al. 1990a), 27
but with fewer adverse events for fluoxetine. Drop-out rates did not differ. A later meta-28
analysis (Cox et al. 1993) found the effect size for fluoxetine (3.45) in 7 studies to be 29
greater than that for clomipramine (3.24) in 12 studies, with a lower drop-out rate for the 30
fluoxetine subjects. 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
72
A 10-week, multicenter randomized controlled trial (Freeman et al. 1994) 1
compared clomipramine (N= 34; maximum dose = 250 mg) and fluvoxamine (N=30; 2
maximum dose = 250 mg). All patients had Y-BOCS scores ≥16 at baseline and half had 3
had prior treatment. Improvement was equivalent (fluvoxamine mean Y-BOCS score 4
decrease = 8.6, clomipramine decrease = 7.8). Both medications were well tolerated, but 5
the clomipramine group experienced more sexual dysfunction. In a 10-week multicenter 6
randomized controlled trial, patients scoring ≥16 on the Y-BOCS were treated with 7
clomipramine (N=65; maximum dose = 300 mg, mean = 206 mg) or fluvoxamine (N=37; 8
maximum dose = 300 mg, mean = 212 mg). The drugs were equally effective (YBOCS-9
25% responder rates were 56% and 54%). Both medications were well tolerated, with no 10
difference in drop-out rates due to adverse events (Koran et al. 1996b). Another 10-week 11
multicenter randomized controlled trial enrolling patients scoring ≥16 on the Y-BOCS 12
compared clomipramine (N=42; maximum dose = 250 mg, mean = 255 mg) with 13
fluvoxamine (N=37; maximum dose = 300 mg, mean = 201 mg). The drugs were equally 14
effictive, but fluvoxamine was better tolerated; constipation and dry mouth were 15
problematic in the clomipramine group (Mundo et al. 2000). 16
Foa et al. (Foa et al. 2005) compared clomipramine (N=36), ERP (N=29), 17
clomipramine plus ERP (N=31), and placebo (N=26). In this 12-week randomized trial 18
enrolling subjects with Y-BOCS ≥16, no major depression and no prior adequate 19
treatment with clomipramine or ERP, clomipramine was more effective than placebo. 20
ERP combined with clomipramine was more effective than clomipramine alone, but not 21
ERP alone. 22
At least three meta-analyses have evaluated randomized double-blind controlled 23
studies comparing clomipramine to SSRIs. Using completer data, Abramowitz 24
(Abramowitz 1997) found a modestly greater effect size for clomipramine than for 25
certain SSRIs (effects sizes: clomipramine versus placebo, 1.31/0.66 [Clinician 26
rating/Patient rating] fluvoxamine versus placebo, 1.28/ 0.37; sertraline versus placebo, 27
0.37/ 1.09; fluoxetine versus placebo, 0.68/[no patient rating done]). When the difference 28
in side effect profiles between the clomipramine and the placebo groups was statistically 29
adjusted to zero, the superiority of clomipramine over the SSRIs disappeared. Eddy et al. 30
(Eddy et al. 2004) also found a greater effect size for clomipramine in analyzing 32 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
73
randomized controlled studies (18 involving clomipramine) published between 1980 and 1
2001, enrolling 3,500 subjects. The pre-post clomipramine effect size was 1.55; the 2
sertraline effect size (largest among the SSRIs) was 1.36. This result must be viewed with 3
caution because more subjects in the clomipramine trials were treatment naïve, one-third 4
of potential subjects were excluded from the studies, and only 80% completed the trials. 5
A meta-analysis using meta-regression (effect-size modeling) applied to 25 randomized 6
controlled trials published between 1989 and 1997 found that the superiority of 7
clomipramine over fluoxetine, fluvoxamine, and sertraline in placebo-controlled trials 8
persisted after controlling for heterogeneity effects (Ackerman & Greenland 2002). There 9
was no significant difference among the SSRIs when comparing placebo-controlled trial 10
results. 11
Several explanations have been proposed for this disparity in results between 12
placebo-controlled and clomipramine-SSRI direct comparison studies. The meta-analysis 13
using meta-regression (Ackerman & Greenland 2002) found that age at onset, pre-trial 14
OCD severity, date of publication, trial length, and length of single-blind pre-15
randomization each affected the magnitude of the treatment effect; but after controlling 16
for these predictive factors, clomipramine still appeared superior when comparing across 17
placebo-controlled trials. Abramowitz (Abramowitz 1997) suggested that the apparent 18
superiority of clomipramine may have resulted from its more obvious side effects, thus 19
diminishing the integrity of the blind in placebo-controlled studies. The larger effect size 20
of clomipramine compared with that of the SSRIs is further cast into doubt by the fact 21
that double-blind trials directly comparing clomipramine with fluvoxamine, fluoxetine, 22
and paroxetine show no difference (Ackerman & Greenland 2002) and a double-blind 23
comparison trial with sertraline found sertraline more effective (Bisserbe et al. 1997). 24
Inappropriately high starting doses of clomipramine (50 mg/day), producing a high drop-25
out rate, and low maximum clomipramine doses strongly influenced this result. 26
Clomipramine has been compared, albeit in methodlolically limited studies, with 27
the MAO inhibitors clorgyline and phenelzine. A small crossover study with 6-week drug 28
treatment periods found a significant effect for clomipramine but not for clorgyline (Insel 29
et al. 1983b). A 12-week randomized trial comparing clomipramine 225 mg/day (n=16) 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
74
with phenelzine 75 mg/day (n=14) found no difference, but used non-standard outcome 1
measures (Vallejo et al. 1992). 2
V.A.1.a._____Intravenous Clomipramine 3
A few investigators have studied the effects of intravenously administered clomipramine, 4
which offers the prospect of achieving higher immediate plasma levels by by-passing first 5
pass liver metabolism. However, this treatment is not available in the United States. In 6
controlled trials, intravenous clomipramine has been superior to placebo in treatment-7
resistant patients (Fallon et al. 1998). A double-blind pilot study found pulse-loaded 8
intravenous clomipramine more rapidly effective than identical oral doses (Koran et al. 9
1997), but a subsequent larger study did not confirm these results <<Placeholder for 10
Koran 2006, in press, J Clin Psychopharmacol>>. Both studies reported good results in 11
some very treatment-resistant patients, suggesting that rapid oral dose escalation may be 12
helpful in such patients. Pulse loaded intravenous clomipramine was more rapidly 13
effective and brought greater improvement than gradually increased intravenous dosing 14
when both were followed by oral maintenance treatment (Koran et al. 1998). 15
V.A.1.b._____Clomipramine as an Augmentation Agent 16
The strategy of adding clomipramine to an SSRI or vice versa is supported by expert 17
opinion (March et al. 1997; Figueroa et al. 1998) and several open-label trials. In a 18
randomized open-label 90-day trial that compared adding clomipramine or nothing to 19
citalopram in patients who had failed adequate 16-week trials of both clomipramine and 20
fluoxetine, nine of nine in the clomipramine augmentation group were YBOCS-35% 21
responders, versus only one of seven assigned to citalopram alone (Pallanti et al. 1999). 22
In patients with an inadequate response to six months of clomipramine 150 mg/day, 23
Ravizza et al. (Ravizza et al. 1996b) reported a better response and fewer side effects 24
when sertraline 50 mg/day was added to clomipramine 150 mg/day than when the 25
clomipramine dose was raised to 250 mg day. 26

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
75
V.A.2. ______SSRIs 1
V.A.2.a._____Fluvoxamine 2
The SSRI fluvoxamine was one of the first tested in the treatment of OCD and was the 3
first non-TCA compound to be approved by the FDA for treating OCD. 4
The efficacy of fluvoxamine has been investigated in placebo-controlled and 5
active-comparison studies, as well as in open-label trials. These studies indicate that 6
fluvoxamine is significantly more effective than placebo. In addition, double-blind active 7
comparison studies suggest fluvoxamine is equal in efficacy to clomipramine and other 8
SSRIs (citalopram, paroxetine), although the sample size for the latter comparison was 9
small. Compared with clomipramine, fluvoxamine showed fewer anticholinergic side 10
effects and better tolerability. None of the available studies have clearly demonstrated 11
that the combination of fluvoxamine with CBT (particularly ERP) is more effective than 12
CBT alone, especially after medication was discontinued. However, confidence in these 13
findings is limited by methodological shortcomings. 14
An early double-blind placebo-controlled parallel groups trial (Goodman et al. 15
1989a) reported positive findings when 42 OCD patients— half of whom also had 16
depressive symptoms—were randomized to fluvoxamine (up to 300 mg/day, mean final 17
dose 255 mg/day) or placebo for 6 to 8 weeks. Nine of 21 fluvoxamine patients were 18
CGI-I:1,2 responders (mean Y-BOCS score decrease from baseline = 42%) versus none 19
in the placebo group. The majority of week 6 partial responders became full responders at 20
week 8 of fluvoxamine treatment, suggesting that at least 8 weeks of treatment are 21
needed to detect a full clinical response. 22
In a double-blind trial Jenike et al. (Jenike et al. 1990b) randomly assigned 40 23
OCD subjects to fluvoxamine (up to 300 mg/day, mean maximum dose 294 mg/day) or 24
placebo for 10 weeks and reported a statistically significant greater improvement for 25
fluvoxamine on Y-BOCS and National Institute of Mental Health Obsessive-Compulsive 26
(NIMH-OC) but not CGI measures compared to placebo. 27
Two pivotal 10-week multicenter double-blind placebo-controlled parallel groups 28
studies (n=160 each) provide convincing evidence for the therapeutic efficacy of 29
fluvoxamine in OCD (Greist et al. 1995c; Goodman et al. 1996). The study protocols 30
were identical, thus allowing pooling of data. Fluvoxamine was flexibly titrated to 100–31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
76
300 mg/day. Subjects met DSM-III-R criteria for OCD of at least 12 months’ duration 1
and had an NIMH-OC scale score of ≥7 and a 17-item Hamilton Depression Scale 2
(HAM-D) score of ≤19. A total of 121 (76%) fluvoxamine-treated subjects and 139 3
(87%) placebo-treated subjects completed the studies. The mean fluvoxamine dose at 4
week 10 was 249 mg/day, at which time the mean Y-BOCS score had fallen 23% in the 5
fluvoxamine group compared with 7% in the placebo group (among patients who 6
received at least one post-baseline rating). A statistically significant difference between 7
the two groups was first observed at week 6. CGI-I:1,2 response was achieved in 33% 8
and 38% of fluvoxamine subjects compared with 9% and 15% of placebo subjects. 9
The largest double-blind placebo-controlled fluvoxamine trial (Hollander et al. 10
2003e) randomized 253 OCD subjects (efficacy analyses n = 237, 117 fluvoxamine 11
controlled release, 120 placebo). After 12 weeks, fluvoxamine was significantly more 12
effective than placebo on all efficacy measures, including the Y-BOCS and CGI scales. 13
YBOCS-25% and YBOCS-35% response rates were significantly higher in the 14
fluvoxamine group as were remission rates (44% vs. 31% and 18% vs. 8%, given Y-15
BOCS threshold values of ≤16 and ≤8, respectively). Therapeutic effects were evident at 16
week 2, which is earlier than reported in other fluvoxamine versus placebo studies, 17
perhaps due to the initiation of treatment at a higher starting dose (100 mg/day). 18
Fluvoxamine, although having more side effects (e.g., insomnia, nausea, somnolence) 19
than placebo, was safe and generally well tolerated. 20
In double-blind active-comparison studies, fluvoxamine was superior to 21
desipramine and as efficacious as other SRIs (clomipramine and some SSRIs); however, 22
the lack of placebo control groups prevents calculating the net drug effect. 23
An 8-week trial (Goodman et al. 1990) randomized OCD subjects to fluvoxamine 24
(up to 300 mg/day, mean final dose 214 mg/day) or desipramine (up to 300 mg/day, 25
mean final dose 223 mg/day). Forty subjects completed at least 2 weeks of treatment and 26
were included in the efficacy analysis. The mean Y-BOCS score decreased 29% from 27
baseline in the fluvoxamine group and was virtually unchanged in the placebo group. 28
A 12-week trial (Smeraldi et al. 1992) randomized 12 OCD subjects to 29
fluvoxamine or clomipramine (both up to 200 mg/day). For the 10 completers, the Y-30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
77
BOCS score decreases were similar in the treatment groups; however, the small number 1
of subjects limits the power to detect differences. 2
In a 10-week multicenter trial (Freeman et al. 1994), fluvoxamine (up to 250 3
mg/day, mean final dose 200 mg/day) was as effective as clomipramine (up to 250 4
mg/day, mean final dose 200 mg/day). Endpoint Y-BOCS scores among the 64 5
randomized subjects who had at least one post-baseline rating were not statistically 6
significantly different between the two treatment groups. Fluvoxamine produced fewer 7
anticholinergic side effects and less sexual dysfunction than clomipramine. These 8
findings were replicated in a subsequent 10-week study (Koran et al. 1996b) which 9
involved 79 OCD subjects randomly assigned to fluvoxamine (up to 300 mg/day, mean 10
final dose 225 mg/day) or clomipramine (up to 300 mg/day, mean final dose 201 11
mg/day). Among the 73 subjects who had at least one post-baseline rating, the percentage 12
of responders in the two groups showed no difference at any time. The mean Y-BOCS 13
score decrease was 30.2% in the fluvoxamine and 30% in the clomipramine group. The 14
fluvoxamine group experienced fewer anticholinergic side effects. 15
A large 10-week multicenter double-blind trial randomly assigned 227 OCD 16
subjects to fluvoxamine (up to 300 mg/day) or clomipramine (up to 300 mg/day) (Mundo 17
et al. 2001). Both groups experienced a marked improvement in OCD as evidenced by Y-18
BOCS, NIMH-OC, and CGI scores. Fluvoxamine was better tolerated because of 19
unwanted anticholinergic side effects in the clomipramine group. A small 10-week 20
single-blind trial randomized 30 OCD patients to fluvoxamine (up to 300 mg/day, mean 21
final dose 290 mg/day), paroxetine (up to 60 mg/day, mean final dose 53.3 mg/day) or 22
citalopram (up to 60 mg/day, mean final dose 50.9 mg/day); all patients completed the 23
study (Mundo et al. 1997). At endpoint the percentage of responders across the three 24
groups (response was defined as a YBOCS-35% and a CGI-I score ≤3 [minimally 25
improved]) showed no statistically significant differences, suggesting similar 26
effectiveness in the acute treatment of OCD. However, the small number of subjects in 27
each group severely limited the power to detect differences between the drugs. 28
Two double-blind studies compared the efficacy of fluvoxamine combined with 29
different forms of psychotherapy to psychotherapies alone or combined with placebo. 30
Cottraux and his group (Cottraux et al. 1990) in a combined single- and double-blind trial 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
78
randomized 60 patients to fluvoxamine and antiexposure therapy, fluvoxamine and 1
exposure therapy, or placebo and exposure therapy. Pharmacotherapy (fluvoxamine up to 2
300 mg/day, mean dose 282 mg/day) lasted for 24 weeks followed by a 4-week period to 3
taper off medication; after this, patients were left free to seek treatment as desired. 4
Evaluations were conducted after 2 months of active treatment (N=50), and at the end of 5
active treatment (6 months, N=44). Follow-up evaluations by a blinded rater were done at 6
1 year (N=37) and 18 months (N=33). Fluvoxamine with exposure therapy and 7
fluvoxamine with antiexposure therapy yielded greater reduction in rituals at week 8 and 8
in depression at week 24 than placebo with exposure therapy, but this superiority 9
disappeared at 1 year. At week 24 all treatments reduced OCD symptoms with no 10
significant between-group differences. Fluvoxamine plus antiexposure and fluvoxamine 11
plus exposure had more effect on depressive measures than exposure plus placebo. 12
However, the lack of a standard response measure (Y-BOCS), the small number of 13
subjects in each treatment group, and varying treatments subjects received during follow-14
up limit interpretation of the results. 15
Hohagen et al. (Hohagen et al. 1998) randomized 60 OCD inpatients to 10 weeks 16
of fluvoxamine (up to 300 mg/day, mean dose 288.1 mg/day) plus multi-modal 17
behavioral therapy or to placebo plus multi-modal behavioral therapy. In the 49 18
completers both treatments significantly reduced OCD symptoms. However, there were 19
significantly more YBOCS-35% responders in the fluvoxamine plus behavior therapy 20
group (87.5%) than in the placebo plus behavior therapy group (60%). Post-hoc analyses 21
suggested that patients with OCD and depression benefited more from fluvoxamine plus 22
behavioral therapy than from placebo plus behavioral therapy. 23
Van Balkom and his group (van Balkom et al. 1998) randomized 99 outpatients to 24
four treatment conditions: fluvoxamine plus cognitive therapy, fluvoxamine plus self-25
guided exposure and response prevention, cognitive therapy alone, and finally self-guided 26
exposure and response prevention alone. An 8-week wait list control (N=18; 117 subjects 27
in all) was also included. Fluvoxamine was titrated to 300 mg/day with a mean endpoint 28
dose of 197.1 mg/day. Pharmacotherapy lasted 16 weeks, and a naturalistic follow-up 29
measurement was made at 6 months. Completer and ITT analyses post-treatment revealed 30
no differences in effects (Y-BOCS, SCL-90, BDI) between the four treatment conditions; 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
79
however, this result may be due to inadequate power. Overall, 36% of completers were 1
responders (Y-BOCS score ≤12 and ≥6-point improvement). No evidence was found that 2
the combination of fluvoxamine with CBT was superior to the CBT variations alone. 3
However, because of the lack of a group treated with fluvoxamine alone and the absence 4
of a control arm for the duration of the study, the differential efficacy of fluvoxamine 5
alone and CBT alone cannot be determined at week 16. 6
A recent follow-up study (Hembree et al. 2003) assessed 62 OCD subjects who 7
completed controlled trials (23 with EX/RP alone, 24 with SRI alone [fluvoxamine or 8
clomipramine], 15 with EX/RP + medication) and found that most subjects showed long-9
term improvement following both EX/RP and medication treatment. The authors 10
concluded that the combination of serotonergic (fluvoxamine or clomipramine) 11
medication and EX/RP might be the optimal treatment for many OCD patients. The small 12
number of patients in each group, however, limits the power to detect differences 13
between the groups. 14
One fluvoxamine study supports the hypothesis that OCD patients with co-15
occurring chronic tic disorders may be a clinically meaningful subtype. An 8-week open-16
label trial (McDougle et al. 1993a) assessed the efficacy of fluvoxamine in 66 OCD 17
patients, of whom 33 had tic disorders. Of the OCD patients with co-occurring chronic tic 18
disorders, 21% were fluvoxamine YBOCS-35% and CGI-I:1,2 responders compared with 19
52% of those without co-occurring chronic tics. The authors concluded that fluvoxamine 20
monotherapy may be less efficacious in OCD patients with tics than in those free of this 21
condition. 22
V.A.2.b._____Fluoxetine 23
Fluoxetine was approved by the Food and Drug Administration (FDA) for the treatment 24
of OCD in adults in 1994 and in children and adolescents in 2003. Studies indicate that 25
fluoxetine is superior to placebo and is as effective as either clomipramine or sertraline in 26
treating OCD. 27
Two large double-blind random-assignment placebo-controlled studies 28
deomonstrated the effectiveness of fluoxetine in the treatment of adults with DSM-III-R 29
OCD. Montgomery et al. (Montgomery et al. 1993) randomized 214 subjects to 8 weeks 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
80
of double-blind fluoxetine 20, 40, or 60 mg/day or placebo. Fluoxetine response 1
(YBOCS-25% and CGI-I:1,2) rates (36%, 48%, 47%) were significantly higher in the 40 2
mg/day and 60 mg/day groups than in the placebo group (26%). In a 16-week extension, 3
nonresponders who took fluoxetine 60 mg daily had a highly significant decrease in Y-4
BOCS scores. Fluoxetine and placebo drop-out rates did not differ significantly. 5
Although the acute treatment phase was relatively brief, the results support the safety and 6
efficacy of fluoxetine treatment of OCD. 7
A 13-week randomized double-blind trial (Tollefson et al. 1994b) assessed the 8
effects of fluoxetine 20, 40, or 60 mg/day versus placebo in 355 outpatients with OCD. 9
Each fluoxetine dose was significantly superior to placebo on the Y-BOCS and other 10
efficacy measures, with statistical significance reached by week 5. The fluoxetine-treated 11
groups had YBOCS-35% response rates of 32%, 32%, and 35% respectively, compared 12
with 8.5% in the placebo group. A trend suggesting greater improvement at 60 mg daily 13
was observed. Fluoxetine response rates and overall improvement were greatest for 14
patients with a history of remissions, no previous drug treatment, or more severe OCD 15
(Ackerman et al. 1998). Fluoxetine response was not significantly correlated with current 16
age, age at OCD onset, gender, or race. None of the demographic or clinical factors 17
evaluated was related to improvement in the placebo group. The safety and efficacy of 18
fluoxetine in the acute treatment of OCD are further supported by open trials (Turner et 19
al. 1985; Fontaine & Chouinard 1986; Jenike et al. 1989; Liebowitz et al. 1989). 20
Two studies compared fluoxetine with clomipramine in the treatment of DSM-III-21
R OCD without using a placebo control group (Pigott et al. 1990; Lopez-Ibor, Jr. et al. 22
1996). In the first study, involving cross-over designs with 10 weeks of treatment, 4 23
weeks of drug washout, and samples of 6 and 20 subjects, fluoxetine up to 80 mg/day 24
was as effective as clomipramine up to 250 mg/day (Pigott et al. 1990). Both drugs 25
produced a significant decrease in the Y-BOCS score, although clomipramine was 26
associated with more adverse events. The second study, an 8-week double-blind 27
randomized trial compared fluoxetine 40 mg/day (n=30) with clomipramine 150 mg/day 28
(n=25) (Lopez-Ibor, Jr. et al. 1996). The two drugs appeared equally effective over this 29
short treatment period. The YBOCS-25% but not the YBOCS-35% responder rate was 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
81
higher with clomipramine. The discontinuation rate for adverse events was 3% for 1
fluoxetine and 4% for clomipramine. 2
A 24-week randomized double-blind trial compared the efficacy and tolerability 3
of fluoxetine (mean dose 57 ± 23 mg/day) and sertraline (mean dose 140 ± 59 mg/day) in 4
outpatients with DSM-IV OCD (Bergeron et al. 2002). Equivalent and significant 5
improvement was found at week 24 in Y-BOCS and NIMH-OC scale scores. Remission 6
rates (Y-BOCS score ≤11 and CGI-I:1,2) at weeks 12 and 24 were significantly higher 7
for sertraline (36% versus 22% at week 24). Both medications were well-tolerated; 8
discontinuation rates for adverse events were: fluoxetine 14%, sertraline 19%. Subjects 9
treated with sertraline showed an earlier improvement on some but not all efficacy 10
measures. 11
A 10-week randomized trial compared fluoxetine 80 mg/day, phenelzine 60 12
mg/day, and placebo in 64 adults with DMS-III-R OCD (Jenike et al. 1997). These doses 13
were achieved by the end of the third week of the trial. Fluoxetine was superior to 14
placebo at weeks 6 and 10 as well as to phenelzine at week 10. Symmetry obsessions and 15
lower baseline Y-BOCS scores were significantly more common in phenelzine 16
responders than in fluoxetine responders; however, this post-hoc analysis provides only 17
weak evidence for a phenelzine effect in this OCD subgroup. 18
The long-term treatment of OCD with fluoxetine has been examined to a limited 19
extent. In a continuation of the 13-week double-blind placebo-controlled fixed-dose 20
fluoxetine study (Tollefson et al. 1994b), treatment responders continued their blinded 21
treatment, whereas nonresponders began a 24-week open-label trial of maximally 22
tolerated doses up to 80 mg/day (Tollefson et al. 1994a). Among acute phase responders, 23
all three doses of fluoxetine (20, 40, and 60 mg/day) were associated with further Y-24
BOCS improvement. The acute phase non-responders benefited from upward dose 25
titration, with two-thirds achieving a YBOCS-35% response. 26
One study assessed the efficacy and safety of 52 weeks of fluoxetine or placebo 27
treatment in patients with DSM-IV OCD who had responded to single-blind fluoxetine 28
for 20 weeks (Romano et al. 2001). Patients who received fluoxetine had numerically 29
lower relapse rates compared with those who received placebo, although the difference 30
was not significant (see Section V.E for details). 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
82
V.A.2.c._____Paroxetine 1
Paroxetine’s safety and effectiveness are supported by three double-blind placebo-2
controlled trials and two double-blind active-comparator trials. One double-blind switch 3
study suggests that paroxetine may be more effective for venlafaxine non-responders than 4
vice versa. Paroxetine was more effective than placebo in a double-blind study in 5
maintaining acute response over a 6-month continuation treatment period (Hollander et 6
al. 2003a). Paroxetine’s tolerability is comparable to that of other SSRIs; some evidence 7
(Fava et al. 2000) but not all (Hollander et al. 2003a) suggests it is more likely to be 8
associated with significant weight gain. Paroxetine is more likely to induce 9
anticholinergic side effects than are other SSRIs (Zajecka et al. 1997; Black et al. 2000). 10
It also carries a greater risk than other SSRIs of an unpleasant withdrawal syndrome, 11
comparable to the risk associated with venlafaxine (Haddad 2001). Paroxetine is a strong 12
inhibitor as well as a substrate of hepatic enzyme P450/2D6 and may cause drug 13
interactions via this mechanism. 14
A 12-week double-blind trial (Hollander et al. 2003a) randomly assigned OCD 15
patients without co-occurring major depression, tics, or Tourette’s Disorder to paroxetine 16
20 mg/day (n=88), 40 mg/day (n=86), 60 mg/day (n=85), or placebo (n=89). A little more 17
than half of subjects had had a prior SRI trial. Endpoint response rates (YBOCS-25% or 18
GCI-Severity score decrease of ≥2 points) for paroxetine 40 mg/day (25%) and 60 19
mg/day (29%) but not 20 mg/day (16%) were significantly greater than for placebo 20
(13%). A 12-week double-blind flexible-dose study (Kamijima et al. 2004) randomly 21
assigned 191 subjects to placebo or paroxetine increasing from 20 mg/day to 40 mg/day 22
by week three and up to 50 mg/day from week 8. The CGI-I:1,2 response rate was 23
significantly greater in the paroxetine (50%) than in the placebo group (24%). A 24
significantly greater response rate was similarly observed in subjects randomly assigned 25
to 12 weeks of flexibly dosed paroxetine 20–60 mg/day (mean study dose 37 mg/day) 26
(n=201) or placebo (n=99) (Zohar & Judge 1996). More than half (55%) the paroxetine 27
subjects were YBOCS-25% responders compared with 35% of placebo subjects. The 28
active comparator, flexibly dosed clomipramine (150–250 mg/day, mean study dose 113 29
mg/day), produced the same responder rate as paroxetine. 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
83
Two 12-week randomized double-blind studies comparing paroxetine to 1
venlafaxine reached different conclusions. The larger, flexible dose study (Denys et al. 2
2003b) found no significant difference in YBOCS-35% responder rates for up to 60 3
mg/day of paroxetine (44%) (n=76), and up to 300 mg/day of venlafaxine (37%) (n=75). 4
The YBOCS-25% responder rate was higher for paroxetine (66%) than venlafaxine 5
(49%). When non-responders in this study were switched double-blind to the alternative 6
medication, a superior YBOCS-25% responder rate was observed for paroxetine (56% 7
[15/27]) than venlafaxine (19% [3/19]) (Denys et al. 2004b). 8
Long-term effectiveness of paroxetine has been observed in one study. Paroxetine 9
responders in a 12-week double-blind study and its 6-month open-label flexible dose 10
extension phase (n=105) were randomly assigned to six months of double-blind 11
paroxetine or placebo (Hollander et al. 2003a). Relapse was defined as a return to the 12
baseline Y-BOCS score or an increase of ≥1 point in the CGI-Severity score for more 13
than one visit. Subjects assigned to placebo had a significantly higher relapse rate (59%) 14
than those assigned to paroxetine (38%). The mean time to relapse was 29 days in the 15
placebo group and 63 days in the paroxetine group. 16
V.A.2.d._____Sertraline 17
The safety and efficacy of sertraline 50–200 mg/day is supported by two large double-18
blind placebo-controlled trials. The failure of the 100 mg/day dose to separate from 19
placebo in the only fixed-dose, double-blind trial probably reflects a chance finding 20
related to an increased drop-out rate in this dose group. Sertraline in flexible doses from 21
50–200 mg day is as effective as flexibly dosed clomipramine 50–200 mg/day and is 22
better tolerated. In patients with co-occurring major depression, sertraline is more 23
effective in relieving OCD symptoms and is better tolerated than desipramine. Extending 24
treatment to 2 years in responders to 1 year of treatment, brings about small but 25
noticeable continued decrease in symptoms (Rasmussen et al. 1997a). Sertraline is more 26
effective than placebo over a 6-month period in preventing acute exacerbations and 27
relapse in patients who have responded to one year of treatment (Koran et al. 2002) (see 28
Section V.E. for details). Rates of relapse without placebo or after periods greater than 6 29
months after discontinuing medication remain to be determined. 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
84
A 12-week randomized fixed dose trial (Greist et al. 1995a) assigned subjects to 1
sertraline 50 mg/day (n=80), 100 mg/day (n=81), 200 mg/day (n=80), or placebo (n=84). 2
Sertraline 50 mg/day and 200 mg/day were significantly superior to placebo with regard 3
to change in Y-BOCS, NIMH-OC, CGI-S, and CGI-I scores, but the 100 mg dose only 4
for the NIMH-OC, probably because of the high drop-out rate (33%) in this dose group. 5
A 12-week double-blind randomized study of flexibly-dosed sertraline 50–200 mg/day 6
(mean maximum dose at endpoint 165 ± 55 mg/day) found the drug (n=86) more 7
effective than placebo (n=81) with regard to change in Y-BOCS, NIMH-OC, and CGI-S 8
scores (Kronig et al. 1999). The CGI-I:1,2 responder rate was numerically but not 9
significantly higher for sertraline (41%) than for placebo (23%). 10
In a 16-week double-blind comparison of sertraline 50 mg/day for four weeks 11
then flexibly increased to 200 mg/day (mean final dose 132 mg/day) versus clomipramine 12
50 mg/day for four weeks then flexibly increased to 200 mg/day (mean final dose 101 13
mg/day), Bisserbe et al. (Bisserbe et al. 1997) observed significantly greater improvement 14
for the sertraline group as measured by the Y-BOCS, NIMH-OC, and CGI-S. 15
Inappropriately high starting doses of clomipramine (50 mg/day), producing a high drop-16
out rate, and low maximum clomipramine doses strongly influenced this result. Among 17
subjects treated for at least four weeks, the two drugs produced equal results, but the 18
mean final clomipramine dose can be regarded as on the low side. 19
In a 24-week double-blind randomized flexible dose comparison of sertraline 50 20
mg/day to 200 mg/day (mean endpoint dose 140 ± 59 mg/day) (n=77) versus fluoxetine 21
20 mg/day to 80 mg/day (mean endpoint dose 57 ± 23 mg/day), the differences in CGI-22
I:1,2 responder rates (60% and 60%) and remission (CGI-I:1,2 plus Y-BOCS <12) rates 23
(36% versus 22%) were not significant (Bergeron et al. 2002). 24
In OCD patients with co-occurring depression randomly assigned to double-blind, 25
flexibly-dosed sertraline 50 mg/day to 200 mg/day (mean endpoint dose 160 ± 50 26
mg/day) or desipramine 50 mg/day to 300 mg/day (mean endpoint dose 194 ± 90 27
mg/day), sertraline (n=79) was more effective than desipramine (n=85) in bringing about 28
“robust improvement in OCD symptoms” (Y-BOCS score decrease ≥40%) (Hoehn-Saric 29
et al. 2000). 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
85
A completed year of continued treatment with open-label sertraline flexibly dosed 1
from 50 mg/day to 200 mg/day was associated with a mean decrease in Y-BOCS scores 2
from about 12 to about 9 in 38 subjects (Rasmussen et al. 1997a) who had been CGI-I:1,2 3
responders in a one-year, fixed dose, double-blind study (Greist et al. 1995b). 4
Finally, Koran et al. (Koran et al. 2002) found that after one year of single-blind 5
treatment, sertraline responders rarely relapsed over 28 weeks whether they were 6
maintained on flexibly dosed sertraline (50 mg/day to 200 mg/day) (3/108=3%) or 7
switched over 2 weeks to placebo (5/113=4%) (see Section V.E. for details). 8
V.A.2.e._____Citalopram 9
The safety and efficacy of citalopram treatment for OCD is supported by a large double-10
blind placebo-controlled trial and small active comparator or open-label trials. The 11
minimum dose reported effective in controlled trials is 20 mg/day, and the maximum 12
dose is 60 mg/day. Some evidence exists for a dose-response relationship and a dose 13
versus time-to-response relationship, with faster response at higher doses. Citalopram 14
improved functioning in work, social, and family domains. Citalopram (and its active 15
enantiomer, escitalopram) are less likely to cause pharmacokinetic drug interactions than 16
other SRIs and do not displace drugs that are tightly bound to plasma proteins, e.g., 17
warfarin and digoxin. Intravenous citalopram 20 to 80 mg/day was well tolerated in one 18
study (Pallanti et al. 2002b). Bjerot (Bejerot & Bodlund 1998) reported a single case 19
unresponsive after 3 months of 80 mg/day but subsequently responsive to 160 mg/day, 20
which was well tolerated over a long term. 21
In the only double-blind, placebo-controlled randomized trial, 12 weeks of 22
citalopram in fixed doses of 20 mg/day (n=102), 40 mg/day (n=98), and 60 mg/day 23
(n=100) was associated with higher YBOCS-25% response rates (57%, 52%, and 65% 24
respectively) than was placebo (37%). There were trends for the highest dose to be 25
associated with more rapid response and a higher response rate. 26
Open-label trials suggest that citalopram (mean dose 51 mg/day) (n=11) and 27
paroxetine (mean dose 53 mg/day) (n=9) bring about similar YBOCS-35% responder 28
rates (40% and 45%) in inpatients (Mundo et al. 1997). The response rate to fluvoxamine 29
(mean dose 290 mg/day) (n=10) (60%) was numerically but not statistically significantly 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
86
higher. A random assignment flexible dose open-label study utilizing a blinded rater 1
observed no significant difference in the YBOCS-35% responder rates to two weeks of 2
citalopram 40 to 60 mg/day (n=23) (48%), fluvoxamine 200 to 300 mg/day (n=83) 3
(55%), clomipramine 150 to 250 mg/day (n=37) (48%) or paroxetine 40 to 60 mg/day 4
(n=16) (50%) (Erzegovesi et al. 2001). 5
Two small open-label studies suggest that patients who have failed to respond to 6
other SSRIs may respond to citalopram. An open-label trial of citalopram flexibly dosed 7
from 20 mg/day to 60 mg/day (mean final dose 46 mg/day) reported that 22/29 (76%) 8
patients who completed 24 weeks of treatment experienced a ≥50% decrease in Y-BOCS 9
score (Koponen et al. 1997). Among 18 patients who completed 16 weeks of citalopram 10
(20 mg/day for two weeks, then 40 mg/day) after having failed two to three adequate, 6-11
month SRI trials (Y-BOCS decrease <25% and score ≥21), 14 (78%) were CGI-I:1 12
responders (Marazziti et al. 2001). Pallanti et al. (Pallanti et al. 1999) in a shorter, 12-13
week trial reported a lower responder rate using the YBOCS-35% definition: only 1/7 14
(14%) subjects who had failed to benefit (Y-BOCS score decrease <35%) from fluoxetine 15
(≥20 mg/day for ≥12 weeks) and from clomipramine (≥150 mg/day for ≥12 weeks) 16
responded to citalopram (20 mg/day for two weeks and then 40 mg/day). 17
Intravenous citalopram (unavailable in the United States) may have a faster onset 18
of action than oral citalopram and appears to be well tolerated (Pallanti et al. 2002b). 19
V.A.2.f. _____Venlafaxine 20
Venlafaxine, a serotonin and norepinephrine reuptake inhibitor (SNRI), has been 21
investigated in one small (negative) placebo-controlled trial and several active 22
comparator and open-label trials. Venlafaxine does not have a specific indication from 23
the FDA for OCD. Most trials found venlafaxine in doses of at least 150 mg/day effective 24
in the treatment of OCD. Venlafaxine may be as effective as paroxetine and 25
clomipramine, and may be efficacious for treatment-naïve patients and those 26
unresponsive to prior SSRI trials. One study showed superiority of paroxetine in 27
venlafaxine nonresponders compared to the effectiveness of venlafaxine in paroxetine 28
nonresponders. Venlafaxine has been generally well tolerated. 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
87
The only double-blind placebo-controlled trial (Yaryura-Tobias & Neziroglu 1
1996) randomized 30 OCD patients to placebo or venlafaxine (up to 225 mg/day) for 8 2
weeks. At endpoint, there were no statistically significant differences in response, 3
although there was a positive trend for the venlafaxine group. The study’s small sample 4
size, short trial length, low venlafaxine dose, and lack of standard outcome measures 5
(CGI, ratings of avoidance) severely constrain interpretation. 6
A 12-week double-blind randomized active comparator study (Denys et al. 7
2003b) randomized 150 OCD patients to venlafaxine XR (up to 300 mg/day) or 8
paroxetine (up to 60 mg/day). Full response was defined as a decrease of 50% on the Y-9
BOCS and partial response as a decrease of 35%. An intent-to-treat (ITT) last observation 10
carried forward (LOCF) analysis demonstrated no significant differences in responder 11
rates (full response: 24% venlafaxine vs. 22% paroxetine and partial response 37% 12
venlafaxine vs. 44% paroxetine). Of note, the venlafaxine group had undergone more 13
prior unsuccessful medication trials. Only a small percentage of patients (5%) dropped 14
out due to adverse effects. Methodological limitations of the study are the lack of a 15
placebo control group, and dosages of venlafaxine not exceeding 300 mg/day. 16
Non-responders (Y-BOCS decrease <25%) in this study (n=43) were treated for 17
12 additional weeks with the alternate medication (Denys et al. 2004b). A significantly 18
higher proportion of those switched to paroxetine (56%, 15/27) were YBOCS-25% 19
responders than those switched to venlafaxine XR (19%, 3/16). However, the small 20
sample size, the lack of a placebo control group, and a less stringent response criterion 21
are methodological limitations in this second study phase. 22
In a 12-week double-blind trial (Albert et al. 2002), 73 OCD subjects were 23
randomized to venlafaxine (225 to 350 mg/day, mean dose 265 mg/day) or clomipramine 24
(150 to 225 mg/day, mean dose 168 mg/day). Visitwise and LOCF analyses at study end 25
revealed no statistically significant difference between the groups in YBOCS-35% and 26
CGI-I:1,2 responder rates (visitwise responder rates: venlafaxine 36% vs. clomipramine 27
50%; LOCF responder rates: venlafaxine 35% vs. clomipramine 43%). The investigators 28
concluded that venlafaxine at these doses may be as efficacious acutely as clomipramine, 29
with fewer side effects. However, confidence in these results is again limited by the lack 30
of a placebo control group and by the relatively low mean clomipramine dose. 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
88
An open-label study treated 39 OCD patients (29 resistant to prior SRI trials) for a 1
mean of 18 months with venlafaxine up to 450 mg/day (mean final dosage 230 mg/day) 2
(Hollander et al. 2003c). At study end, 69% of subject entering the study were CGI-I:1,2 3
responders. Of note, 76% of those unresponsive to one or more SRI trials, and 82% of 4
those unresponsive to two or more SRI trials were sustained responders. The high 5
venlafaxine dose was well tolerated. 6
An 8-week open-label trial treated 12 OCD patients with venlafaxine 150–300 7
mg/day and reported responder rates of 75% (YBOCS-35%) and 35% (CGI-I:1,2) 8
(Sevincok & Uygur 2002) without substantial side effects. A 12-week open-label trial of 9
venlafaxine 150 to 350 mg/day in 10 OCD patients reported responder rates of 30% 10
(YBOCS-35%) and 40 % (CGI–I:1,2), with a more robust response in treatment-naïve 11
patients (Rauch et al. 1996). Marazziti (Marazziti 2003) reported 5 OCD patients resistant 12
to SSRIs who improved (Y-BOCS, HAMD, and other clinical evaluations) for at least 13
one year with venlafaxine 150 to 225 mg/day. 14
V.A.3. ______Other Antidepressants 15
V.A.3.a._____Monoamine Oxidase Inhibitors 16
The data very weakly support the use of MAOIs in severely ill OCD patients who have 17
failed most or all first-line treatments and most second-line treatments. The presence of 18
severe anxiety or panic attacks, or of symmetry obsessions has been a positive predictor 19
in some case reports. The side effect burden of MAOIs, including cardiovascular side 20
effects and weight gain, argues against their use, except as just noted. Dietary restrictions 21
are necessary when non-selective MAOIs or high-dose selective MAOIs are utilized 22
(McCabe 1986; Sweet et al. 1995). 23
In a small double-blind placebo- and fluoxetine-controlled study, the Y-BOCS 24
score decrease for subjects completing 10 weeks of phenelzine 60 mg/day (n=17) was not 25
significantly greater than for those completing placebo treatment (n=18), whereas the 26
decrease produced by fluoxetine 80 mg/day (n= 19) was (Jenike et al. 1997). In a post-27
hoc analysis, the authors suggested that symmetry obsessions might be a strong predictor 28
of phenelzine “response” (undefined). A blinded 12-week random assignment open-label 29
comparison of phenelzine 75 mg/day (n=12 completers) and clomipramine 225 mg/day 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
89
(n=14), both doses reached by week 5, found no significant difference on either the 1
Maudsley Obsessive Compulsive Inventory or a non-standard scale (Vallejo et al. 1992). 2
The absence of a placebo group, use of non-standard rating scales, and small sample size 3
limit this study’s evidentiary weight. A case series (Jenike et al. 1983) and isolated case 4
reports add only minimal evidence of the effectiveness of MAOIs. 5
V.A.3.b._____Tricyclic Antidepressants 6
Limited investigations of tricyclic antidepressants other than clomipramine have found no 7
evidence for their efficacy in treating OCD. 8
A randomized controlled trial comparing nortriptyline, clomipramine, and 9
placebo, with eight subjects in each treatment group, found that clomipramine, but not 10
nortriptyline, was superior to placebo in reducing interview-based ratings of OCD 11
severity (Thoren et al. 1980). However, there was no significant difference in 12
effectiveness between clomipramine and nortriptyline. 13
In a placebo-controlled trial, imipramine (mean dose 233/mg/day) reduced 14
depression over 6 weeks in highly depressed OCD patients (n=37), but did not affect 15
obsessive-compulsive symptoms in these patients or in those less depressed (Foa et al. 16
1987). 17
In another study, 38 patients were divided into highly and mildly depressed 18
groups according to their Beck Depression Inventory scores (Foa et al. 1992). One half of 19
each group received imipramine and the other half received placebo for six weeks 20
followed by three weeks of daily behavioral treatment and then 12 weekly sessions of 21
supportive psychotherapy. Although imipramine improved depressive symptoms in 22
depressed patients, it did not affect obsessive-compulsive symptom severity. Behavioral 23
therapy reduced OCD symptom severity, but imipramine did not potentiate behavioral 24
therapy effects. No differences in OCD response to behavior therapy was seen in highly 25
depressed versus mildly depressed patients. 26
V.A.3.c._____Trazodone 27
Case reports and case series (Hermesh et al. 1990) suggest that trazodone in doses of at 28
least 250 mg/day may be worth trying in OCD patients who have failed first- and second-29
line treatments. However, a double-blind placebo-controlled 10-week trial with 11 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
90
trazodone completers (mean dose 235 mg/day) and 6 placebo completers found no 1
evidence of effectiveness (Pigott et al. 1992b). The trial was too short (≥250 mg/day for 2
six weeks) and too small to allow definitive conclusions. In a case series (n=5), 3
augmentation of an SSRI with trazodone 300–600 mg/day was helpful in alleviating 4
OCD and anxiety as well as sleep disturbance, gastrointestinal distress, and sexual 5
dysfunction (Marazziti et al. 1999). Sedation is likely to be a limiting side effect, and 6
males must be warned of the risk of priapism, which may occur in from 1/1000 to 7
1/10,000 men (Haria et al. 1994). Toursade de points is a rare side effect (Haria et al. 8
1994). 9
V.A.4. ______Antipsychotics 10
V.A.4.a._____Monotherapy 11
Few studies have examined the efficacy of antipsychotics as monotherapy for OCD and 12
the available evidence does not support their use as monotherapy. An early study 13
(TRETHOWAN & SCOTT 1955) examined chlorpromazine in a mixed population of 14
patients (“psychoneuroses or personality disorders with some symptoms of an obsessive 15
or compulsive type”) and did not use standardized assessment instruments. Case studies 16
using haloperidol were inconclusive (e.g., (O'Regan 1970; Hussain & Ahad 1970)). A 17
case report describes an OCD patient who responded well to loxapine (Rivers-Bulkeley 18
& Hollender 1982). 19
More recently, the possible efficacy of clozapine 300–600 mg/day was examined 20
in an open 10-week trial involving 12 OCD patients (McDougle et al. 1995). The patients 21
had previously not responded (Y-BOCS -35% with score <16 and a CGI-I:1,2) to prior 22
SRI trials. Two patients dropped out due to side effects (sedation and hypotension). In the 23
ten completers, none responded; the mean Y-BOCS reduction was 10%. The authors 24
concluded that clozapine is ineffective as monotherapy in patients resistant to prior SRI 25
treatment. 26
Most recently, Connor et al. (Connor et al. 2005) examined the efficacy of 27
aripiprazole in eight OCD patients over 8 weeks. Seven patients took 10–30 mg/day, but 28
two dropped out due to side effects (akathisia, nausea). Among the five completers, three 29
experienced a Y-BOCS decrease of ≥30%; two subjects were rated much or very much 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
91
improved. The authors concluded that some patients may benefit from aripiprazole 1
monotherapy. However, the small sample and open-label design preclude strong 2
conclusions. 3
V.A.4.b._____Augmentation 4
Many OCD patients have either no response or a partial response to SRI treatment. The 5
addition of antipsychotic medications has been used to augment SRI response. Evidence 6
for the different agents is presented below (see also Table 7). In sum, randomized 7
placebo-controlled trials support the use of both first-generation (haloperidol) and 8
second-generation (risperidone, olanzapine, quetiapine) antipsychotic medications to 9
augment SRI response in OCD patients (McDougle et al. 1994; McDougle et al. 2000; 10
Hollander et al. 2003b; Bystritsky et al. 2004; Denys et al. 2004a; Erzegovesi et al. 2005). 11
The addition of antipsychotics further reduced Y-BOCS scores in up to 50% of OCD 12
patients; significant differences between the antipsychotic medications and placebo were 13
observed within 4–6 weeks. Some controlled trials did not find significant differences 14
between antipsychotic and placebo augmentation (Shapira et al. 2004; Carey et al. 2005; 15
Fineberg et al. 2005); however, methodological limitations in some of these studies likely 16
contributed to the negative findings. 17
Only one (Fineberg et al. 2005) controlled trial lasted longer than 8 weeks, and it 18
was a negative study. Thus, the long-term effects of antipsychotic augmentation have not 19
been systematically studied. A retrospective chart review (Maina et al. 2003) found that 20
15 of 18 patients (83%) who responded to antipsychotic augmentation relapsed within 21
two months after the antipsychotic was discontinued. Thirteen of the 15 who relapsed did 22
so by the eighth week after discontinuation. 23
There are many unanswered questions about antipsychotic augmentation in OCD, 24
including the optimal dose for each of the agents, the long-term tolerability of the agents, 25
and the reasons some patients benefit but others do not. In addition, the relative efficacy 26
of the different agents has not been examined; one study (McDougle et al. 1994) suggests 27
that haloperidol helps only OCD patients with co-occurring tic disorders. 28

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
92
V.A.4.c._____Haloperidol 1
In the first double-blind placebo-controlled study of antipsychotic augmentation 2
(McDougle et al. 1994), 34 patients resistant to 8 weeks of fluvoxamine (defined as less 3
than YBOCS-35% or a score ≥16 and not CGI-I:1,2) were randomized to 4 weeks of 4
adjunctive haloperidol (n=17) or placebo (n=17). Adjunctive haloperidol (initiated at 2 5
mg and increased to a maximum of 10 mg/day) was significantly more effective than 6
placebo. Eleven of 17 haloperidol patients responded versus none on placebo, but 7
akathisia requiring propranol treatment was common. Response was defined as: 1) 8
YBOCS-35% and score <16; 2) GCI-I:1,2; and 3) consensus of the treating clinician and 9
two of the primary investigators. Of the 11 responders, 7 met all three criteria, and 4 met 10
two criteria. All 8 subjects with co-occurring tics were responders to haloperidol, versus 11
3 of 9 without tics. No subject with tics responded to placebo. The authors concluded that 12
OCD patients with a chronic tic disorder might benefit from adjunctive haloperidol, but it 13
should not be used indiscriminately because of the risk of tardive dyskinesia. 14
V.A.4.d._____Risperidone 15
Three double-blind placebo-controlled studies, albeit of modest size, and several open-16
label studies support the safety and effectiveness of risperidone augmentation of SRI 17
treatment of OCD. McDougle et al. (McDougle et al. 2000) examined the efficacy and 18
tolerability of adjunctive risperidone, a second-generation antipsychotic with a more 19
favorable side effect profile (Voruganti et al. 2000; Tamminga 2003). Thirty-six patients 20
resistant to 12 weeks of SRI treatment (< YBOCS-35% decrease or a score ≥16 and CGI-21
I:1,2) were randomized to 6 weeks of added risperidone (n=20) or placebo (n=16). 22
Risperidone was initiated at 1 mg/day and increased by 1 mg weekly. The mean 23
risperidone dose was only 2.2 mg/day (SD=0.7 mg/day; range 1–4). Among completers 24
(risperidone, n=18; placebo, n=15), risperidone was significantly superior to placebo (Y-25
BOCS reduction: 32% risperidone; 9% placebo). Nine (50%) of 18 risperidone 26
completers were responders compared to none of 15 placebo completers. Response was 27
defined as in McDougle et al. (McDougle et al. 1994) (see Section V.A.4.c above). 28
Risperidone was generally well tolerated. The most prominent adverse effect was mild 29
transient sedation; one risperidone patient dropped out in the first week because of 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
93
intolerable insomnia. There was no difference in outcome between OCD patients with 1
and without co-occurring tic disorder or schizotypal personality disorder. 2
A smaller controlled study (Hollander et al. 2003b) randomized 16 OCD patients 3
who had “failed” (i.e., no more than minimally improved) at least two 12-week SRI trials 4
to 8 weeks of adjunctive risperidone (n=10) or placebo (n=6). Risperidone was started at 5
0.5 mg/day and increased by 0.5 mg weekly to a maximum of 3 mg/day; the mean 6
risperidone dose was 2.25 mg/day (SD=0.86), with no difference between responders and 7
nonresponders. In the ITT sample, the risperidone group had a numerically larger mean 8
Y-BOCS score decrease (25%) than the placebo group (5%). Four of 10 (40%) 9
risperidone patients and none of six (0%) placebo patients were YBOCS-25% responders. 10
Three subjects discontinued (risperidone, n=1; placebo, n=2) all due to unsatisfactory 11
clinical response. Risperidone was generally well-tolerated; only four risperidone patients 12
experienced side effects (sedation, dizziness, dry mouth). 13
A randomized controlled trial (Erzegovesi et al. 2005) examined the efficacy of 14
0.5 mg/day of risperidone versus placebo in OCD patients who either responded or did 15
not respond to their first SRI trial. All patients received 12 weeks of fluvoxamine 16
(maximum dose 300 mg/day, but final doses not provided). Responders (YBOCS-35% 17
and CGI-I:1,2) and “nonresponders” were then randomized to risperidone 0.5 mg/day or 18
placebo for 6 weeks. In the 39 patients completing the trial, risperidone significantly 19
reduced OCD symptoms in the 10 fluvoxamine nonresponders but not the 9 fluvoxamine 20
responders (Y-BOCS reduction for fluvoxamine nonresponders: risperidone 26%, 21
placebo 7%; Y-BOCS reduction for the fluvoxamine responders: risperidone 4%, placebo 22
28%). Among the fluvoxamine nonresponders, 5/10 (50%) risperidone patients and 2/10 23
(20%) placebo patients had a YBOCS-35% response. The study’s limitations include the 24
small sample size, the potential for ceiling effects in the fluvoxamine responders, and the 25
lack of information about whether patients in the different treatment groups received a 26
similar dose and duration of fluvoxamine prior to augmentation. 27
V.A.4.e._____Olanzapine 28
The safety and effectiveness of adjunctive olanzapine in OCD has been examined in two 29
randomized placebo-controlled trials and several open-label trials. Bystritsky et al. 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
94
(Bystritsky et al. 2004) randomized 26 OCD patients, who had not “improved” 1
(undefined) after at least two 12-week SRI trials and at least one EX/RP trial, to 6 weeks 2
of adjunctive olanzapine (n=13) or placebo (n=13). OCD patients with current co-3
occurring Axis I disorders were excluded. The mean olanzapine dose was 11.2 mg/day 4
(SD=6.5; range, 5 to 20 mg/day). In the ITT sample, olanzapine was significantly 5
superior (Y-BOCS reduction: olanzapine 17%; Y-BOCS increase: placebo 2%). Six 6
(46%) of 13 olanzapine patients had a YBOCS-25% response compared with none in the 7
placebo group. Two of the 13 olanzapine patients (15%) discontinued because of side 8
effects: sedation (n=1) or weight gain (n=1). 9
Shapira et al. (Shapira et al. 2004) randomized OCD nonresponders (not YBOCS-10
25%) or partial responders (YBOCS-25% but score ≥16) to 8 weeks of fluoxetine (40 11
mg/day in 42 subjects, 20 mg/day in 1 subject), 6 weeks of adjunctive olanzapine (n=22), 12
or placebo (n=22). Olanzapine was started at 5 mg/day and increased to a maximum of 10 13
mg/day. Both treatment groups improved significantly with no significant difference 14
between them; both had a similar proportion of responders (YBOCS-25% = 41% for both 15
groups; YBOCS-35% = 23% for olanzapine, 18% for placebo). The authors concluded 16
that adding olanzapine was not superior to extending the 8-week SRI monotherapy trial. 17
However, as they noted, the patients were unlikely to have attained full benefit from the 18
SRI before the olanzapine trial began, thus obscuring any olanzapine effect. Olanazpine 19
patients gained a mean of 2.8 (±3.1) kg compared with 0.5 (±1.8) kg for placebo patients. 20
V.A.4.f. _____Quetiapine 21
The safety and effectiveness of quetiapine augmentation of SRI treatment in OCD has 22
been evaluated in three randomized double-blind placebo-ctonrolled trials, one 23
randomized single blind placebo-controlled trial, and several open-label studies. 24
Denys et al. (Denys et al. 2004a) randomized 40 OCD patients without co-25
occurring diagnoses who were unresponsive (Y-BOCS decrease <25%) to at least two 26
SRIs (at maximum tolerated dose for 8 weeks) to adjunctive quetiapine (n=20) or placebo 27
(n=20) for 8 weeks. Quetiapine was started at 50 mg/day and increased using a fixed 28
dosing schedule to a maximum of 300 mg/day. In the ITT sample, quetiapine was 29
significantly superior to placebo (Y-BOCS reduction: quetiapine 32%; placebo 7%). 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
95
Eight (40%) of the 20 quetiapine patients were responders (YBOCS-35% and CGI-I:1,2), 1
compared to only 2 (10%) of 20 placebo patients. The most common side effects of 2
quetiapine were somnolence (95%), dry mouth (55%), weight gain (30%), and dizziness 3
(30%). 4
Carey et al. (Carey et al. 2005) randomized 41 patients who had not responded 5
(not CGI-I:1,2 or not YBOCS-25%) to 12 weeks of SRI treatment to 6 weeks of flexibly 6
dosed quetiapine (n=20) or placebo (n=21). The mean final quetiapine dose was 169 7
(±121) mg/day. Both quetiapine and placebo led to a significant reduction in mean Y-8
BOCS scores (Y-BOCS reduction: quetiapine 27%; placebo 26%), with no significant 9
difference between them. Responder (CGI-I:1, 2 and YBOCS-25%) rates were quetiapine 10
40%, placebo 48%. Two quetiapine patients dropped out due to severe sedation, and 75% 11
complained of sedation (versus 33% of placebo patients). Quetiapine augmentation was 12
no more effective than placebo but several study limitations (e.g., patients had received 13
their maximum SRI dose for only 6 weeks before randomization) probably contributed to 14
the negative findings. 15
Fineberg et al. (Fineberg et al. 2005) randomized 21 adult OCD with minimal 16
response (<25% Y-BOCS decrease) to 12 weeks of an SRI at the maximum tolerated 17
dose to either quetiapine (N=11) or placebo (n=10). After 16 weeks of augmentation, 18
there was no difference between the two groups in the ITT sample (Y-BOCS reduction: 19
quetiapine 14%; placebo 6%). Three of 11 quetiapine-treated patients were YBOCS-25% 20
responders compared to one of 10 placebo patients. The authors suggested that their 21
exclusion of Axis I disorders and tic disorders may have led to their negative results. 22
A single-blind placebo-controlled study (Atmaca et al. 2002) randomized 27 OCD 23
patients unresponsive to at least one 12-week SRI trial (i.e., no more than minimal 24
improvement, a Y-BOCS score of ≥18, and agreement of three of the authors) to 25
adjunctive quetiapine (n=14) or placebo (n=13) for 8 weeks. Ten (71%) of 14 quetiapine 26
patients (on 50 to 200 mg/day) improved (defined as Y-BOCS decrease ≥30%), 27
compared to the placebo patients, who did not improve a significant difference. Nine 28
quetiapine patients reported side effects (nausea, n=6; sedation, n=3; dizziness, n=1). The 29
study’s main limitation was the single-blind design. 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
96
V.A.4.g._____Other Antipsychotic Agents 1
Data from double-blind placebo-controlled studies are not available for ziprasidone or 2
aripiprazole. Published case reports suggest the efficacy of ziprasidone augmentation of 3
SRI pharmacotherapy (Crane 2005). 4
V.A.5. ______Other Agents 5
V.A.5.a._____Adrenergic Agents 6
Pindolol, a beta-blocker and 5-HT1A presynaptic receptor antagonist, increases 7
serotonergic transmission through its effect on the presynaptic 5-HT1A receptor. Small 8
studies have produced mixed results regarding its possible effectiveness as an 9
augmentation agent. 10
An 8-week double-blind placebo-controlled trial examined pindolol augmentation 11
of fluvoxamine in 15 patients (Mundo et al. 1998). Neither quantitative nor qualitative 12
analysis revealed any differences between the two treatment groups. In particular, 13
pindolol did not shorten the latency of anti-obsessional response to fluvoxamine. 14
A double-blind placebo-controlled trial enrolled 14 patients with DSM-IV OCD 15
who had failed to respond to paroxetine and at least two other SRIs (Dannon et al. 2000). 16
Augmentation with pindolol 2.5 mg thrice daily was associated with significant decrease 17
in the Y-BOCS score after the fourth week of treatment. The greatest improvement was 18
noted in the ability to resist compulsions. No group differences were found in pulse or 19
blood pressure. 20
An open-label study found beneficial therapeutic effects from a combination of 21
pindolol and a serotonergic antidepressant for treatment-resistant OCD only after 22
tryptophan was added (Blier & Bergeron 1996). Another open-label study found that one 23
of eight patients with treatment-resistant OCD responded to pindolol augmentation 24
(Koran et al. 1996c). It has been suggested that pindolol can be given once or twice daily 25
for augmentation in psychiatric disorders (Koch et al. 2000). 26
A double-blind cross-over comparison trial with 6-week drug periods found 27
clonidine (maximum dose 1.0 mg/day) ineffective in 28 patients with DSM-III-R OCD 28
(Hewlett et al. 1992). 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
97
V.A.5.b._____Benzodiazepines 1
Benzodiazepines cannot be recommended as monotherapy for OCD, despite positive case 2
reports for clonazepam and alprazolam, except in those rare individuals unable or 3
unwilling to take standard anti-OCD medications. Case reports have noted onset of action 4
within one to three weeks. For clonazepam, negative results from a double-blind placebo-5
controlled trial (Hollander et al. 2003d) and an open trial (Stein et al. 1992) cast serious 6
doubt on the positive results of a double-blind multiple crossover trial (Hewlett et al. 7
1992). In the latter study, effectiveness seems to have necessitated doses that were poorly 8
tolerated and produced serious adverse events. Modest doses of benzodiazepines may 9
relieve anxiety and distress in OCD without directly diminishing the frequency or 10
duration of obsessions or compulsions. Among patients with histories of substance abuse 11
or dependence, benzodiazepine use may aggravate symptoms and should be prescribed 12
cautiously (American Psychiatric Association 1998; American Psychiatric Association 13
2006b). 14
V.A.5.c._____Buspirone 15
Small and methodologically limited studies provide inconsistent results regarding the 16
possible effectiveness of buspirone 60 mg/day as monotherapy and no substantial 17
evidence of its effectiveness as an augmenting agent. 18
A 6-week double-blind comparison of buspirone titrated to 60 mg/day (n=10) and 19
clomipramine titrated to 250 mg/day (n=10) suggested equal effectiveness (Pato et al. 20
1991). In a 4-week double-blind placebo-controlled crossover trial (n=13), however, 21
buspirone was no better than placebo (Grady et al. 1993). And an 8-week open trial with 22
a dose of 60 mg/day for the last five weeks reported virtually no decrease in the mean Y-23
BOCS score of the 10 study completers (Jenike & Baer 1988). 24
In a 10-week double-blind placebo-controlled trial of buspirone as an 25
augmentation strategy (n=14), the drug failed to separate from placebo, although 29% 26
(4/14) of buspirone subjects experienced a YBOCS-25% response (Pigott et al. 1992a). A 27
6-week double-blind placebo-controlled trial of buspirone 60 mg/day augmentation of 28
fluvoxamine was negative but enrolled treatment-resistant patients (<35% decrease in Y-29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
98
BOCS score and rated “unimproved” by the investigators) rather than partial responders 1
for whom augmentation was sought (McDougle et al. 1993b). 2
V.A.5.d._____Inositol 3
Inositol, an isomer of glucose and precursor in the phosphatidylinositol cycle, has been 4
studied in two double-blind placebo-controlled crossover studies (one alone and one as an 5
augmentor) and an open augmentation trial. The data weakly suggest that inositol may 6
benefit a minority of OCD patients, but do not support a recommendation that it be 7
routinely tried. Inositol appears to be well tolerated. 8
A double-blind cross-over study administered inositol (18 gm/day) and placebo 9
for 6 weeks in each condition in 13 subjects free of major depression and with variable 10
responses to SSRIs (Levine 1997). There was a small but significantly greater change in 11
the Y-BOCS score in the inositol condition (5.9 points) compared with the placebo 12
condtion (2.8 points). A double-blind placebo-controlled cross-over augmentation study 13
with 6 weeks in each condition and no washout between conditions found no difference 14
in Y-BOCS score decrease between inositol and placebo in the first drug condition, but 15
the study groups were small (6 inositol and 4 placebo) (Fux et al. 1999). Subjects had 16
been on a stable SRI dose for at least 8 weeks before randomization, but showed greater 17
improvement in the study’s first 6 weeks than in its second 6 weeks regardless of which 18
blinded drug was first administered. An open study (Seedat & Stein 1999) added inositol 19
(18 gm/day) for 6 weeks to an SSRI in 10 subjects who were rated minimally improved 20
on the CGI-I after 12 weeks or more of stable treatment. Mean Y-BOCS scores fell 21
significantly from 23.6 (±4.4) to 17.6 (±4.6), but only 3 subjects (30%) achieved CGI-I 22
scores of much improved. 23
V.A.5.e._____Lithium 24
Case reports suggest that lithium monotherapy may deserve further study in trials that 25
utilize an adequate serum level (≥0.6 mEq/l) and an adequate duration of treatment (≥10 26
weeks). However, an 8-week double-blind crossover augmentation study (n=16) with 27
mean serum levels of 0.54 mEq/l (Pigott et al. 1991) and a 4-week double-blind placebo-28
controlled augmentation trial (n=10) with a mean serum level of 0.77 mEq/l (McDougle 29
et al. 1991) were both negative. The 4-week lithium treatment period in these studies may 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
99
have been too short to fully evaluate lithium’s potential utility as an augmatation agent in 1
OCD. The utility of lithium in the treatment of co-occurring bipolar disorder is clearly 2
established (American Psychiatric Association 2002). 3
V.A.5.f. _____Mirtazapine 4
A study combining an open-label first phase with a double-blind discontinuation phase 5
suggests that mirtazapine may be effective for OCD in patients who have not failed more 6
than one adequate SRI trial (Koran et al. 2005c). However, the small sample size (15 7
treatment-naïve patients and 15 who had failed exactly one adequate SRI trial) makes 8
these results suggestive rather than indicate strong evidence for mirtazapine’s 9
effectiveness. Significant weight gain was observed in more than 30% of patients in the 10
first 12 weeks of treatment. A small pilot study provides slight additional support (Koran 11
et al. 2001). Additional double-blind placebo-controlled trials utilizing a parallel groups 12
design are indicated. 13
V.A.5.g._____Other Medications 14
A case series (Warneke 1997) and a double-blind placebo-controlled crossover study 15
(Koran et al. 2005a) suggest that once-weekly oral morphine sulphate, 30–45 mg, may 16
be useful as an augmentation strategy for resistant OCD. In the double-blind study, 7 of 17
23 subjects (30%) experienced a YBOCS-25% response to morphine versus none in the 18
placebo condition. In addition, a small (n=8) 6-week open-label study found evidence for 19
the effectiveness of tramadol monotherapy 254 ± 119 mg/day in the six patients who 20
completed at least 2 weeks of treatment (Shapira et al. 1997). The dose-limiting side 21
effect was sedation. The use of mu-receptor agonists deserves further study in both 22
intermittent and constant dose designs. Investigation of partial agonist/antagonists such as 23
buprenorphine as well as longer acting full agonists such as methadone should be 24
pursued. Whether tolerance to therapeutic effect develops will be important to determine. 25
Some anticonvulsants (valproate, oxcarbazapine, carbamazepine, gabapentin, 26
topiramate) have been reported to help individual patients either as monotherapy or as 27
augmentation agents. A small (n=9) 8-week open-label carbamazepine trial (Joffe & 28
Swinson 1987a) and a small case series (n=5) (Jenike & Brotman 1984) each reported 29
only one positive response. A 6-week open-label study of gabapentin augmentation 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
100
(mean dose 2520 mg/day) in five patients partially responsive to fluoxetine suggested 1
some benefit (Cora-Locatelli et al. 1998), but a 6-week double-blind placebo-controlled 2
crossover trial of gabapentin 3600 mg/day added to fluoxetine found none (Sporn et al. 3
2001). An open case series reviewing at least 14 weeks of topiramate augmentation, 4
mean daily dose 253 mg, in 16 patients partially responsive or nonresponive to SRI 5
treatment reported 11/16 (68.8%) CGI-I:1,2 responders. The mean time to response was 9 6
weeks (Van Ameringen et al. 2005). 7
L-tryptophan 3–9 gm/day with nicotinic acid 1 gm twice daily and pyridoxine 8
200 mg twice daily was reported beneficial in early case reports that predated modern 9
diagnostic criteria and measurement instruments (Yaryura-Tobias & Bhagavan 1977; 10
Yaryura-Tobias 1981). However, some patients became violent. Adding L-tryptophan at 11
doses exceeding 1–2 gm/day to an SRI can induce the serotonin syndrome. 12
D-amphetamine 30 mg, studied in a single-dose double-blind placebo-controlled 13
trial, was associated with a significant decrease in self-rated symptoms about 6 hours 14
after the dose, independent of effects on mood (Insel et al. 1983a). Two patients 15
continued 10–20 mg/day for “several weeks” with continued response. Open-label 16
methylphenidate, 40 mg once orally, produced no significant effect on OCD or mood 4 17
hours later in a small study (n=13), although four patients had a 50% decrease in an OCD 18
rating scale score (Joffe & Swinson 1987b). In a small (n=11) double-blind placebo-19
controlled crossover study of single doses of methylphenidate 40 mg and dextro-20
amphetamine 30 mg, both taken orally, the latter drug was associated with a significantly 21
greater reduction in OCD symptom rating than placebo (Joffe et al. 1991). Case reports 22
exist of OCD benefit after treating co-occurring attention deficit disorder with stimulants. 23
Further investigation of the possible role of stimulants in the treatment of OCD is 24
warranted, with trial lengths of a month or more. The presence of tics or Tourette’s 25
Disorder is not a contraindication to the use of stimulants to treat ADHD co-occurring 26
with OCD; methylphenidate appears to be better tolerated in this situation than 27
dextroamphetamine (Kurlan 2003). 28
Hallucinogens have been reported to alleviate OCD in individual cases (Leonard 29
& Rapoport 1987; Moreno & Delgado 1997). Since hallucinogens are not a practical 30
treatment modality, studies of safer 5-HT2a,c receptor agonists may be warranted. 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
101
Ondansetron 1 mg three times daily was associated with significant decrease in 1
Y-BOCS scores in a small (n=8) 8-week open-label study (Hewlett et al. 2003). The 2
results support the further study of 5-HT3 receptor antagonists such as mirtazapine. 3
St. John’s wort (450 mg of 0l.3% hypericum twice daily), a weak serotonin-4
reuptake inhibitor, was associated with CGI-I:1,2 response in 5 of 12 (42%) subjects in 5
an 12-week open-label trial (Taylor & Kobak 2000). However, a 12-week flexible-dose 6
placebo-controlled trial enrolling 60 subjects found St. John’s wort no better than placebo 7
(Kobak et al. 2005). Note, St. John’s wort interacts with anti-HIV medications (American 8
Psychiatric Association 2000a) and birth control pills (Murphy et al. 2005), among 9
others, and predisposes to sun sensensitivity. 10
Bupropion titrated from 150 mg/day to 300 mg/day after two weeks had no mean 11
effect on Y-BOCS scores in an open trial involving 12 patients (Vulink et al. 2005). 12
However, two patients were YBOCS-25% responders. Four patients “improved,” with a 13
mean Y-BOCS decrease of 31% and eight patients deteriorated, with a mean Y-BOCS 14
increase of 21%. The authors concluded that the bimodal distribution of results supports 15
the hypothesis that dopamine is involved in the pathophysiology of OCD. 16
A 12-week open-label study adding riluzole 50 mg twice daily to SSRIs and other 17
augmenting medications reported that 7/13 (54%) patients with treatment-resistant OCD 18
were YBOCS-35% responders (Coric et al. 2005). Since prior treatment regimens were 19
stable for only 4 weeks before riluzole was added and other augmenting medications 20
were present and ratings were not blinded, these results must be viewed cautiously. 21
Riluzole was well tolerated, although one patient experienced an asymptomatic increase 22
in liver enzyme ALT more than 9 times normal, which decreased despite continued 23
treatment. Further study of riluzole (with appropriate liver function monitoring) and of 24
other glutamate antagonists is warranted. 25
V.B. OTHER SOMATIC THERAPIES 26
Somatic therapies used in the treatment of OCD include deep brain stimulation (DBS), 27
transcranial magnetic stimulation (TMS), electroconvulsive therapy (ECT), and 28
neurosurgery. Plasmapheresis has been investigated only in childhood OCD. DBS and 29
TMS have been applied to OCD treatment primarily in the last decade. Neurosurgery and 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
102
ECT have long histories in the treatment of psychiatric disorders (e.g., depression, 1
schizophrenia), but there are relatively few reports regarding their use in OCD. None of 2
these therapies (DBS, TMS, ECT, and neurosurgery) are considered first-line treatments 3
for OCD, and their use is limited to treatment-resistant patients. 4
Specific descriptions of the criteria used to assess treatment resistance as well as 5
eligibility for surgical treatments (neurosurgery and DBS) in OCD patients have been 6
published elsewhere (Diering & Bell 1991; Pallanti et al. 2002a; Mashour et al. 2005). 7
Data regarding treatment of OCD with these somatic therapies are quite limited. 8
Relatively few patients have been treated, and there is an understandable absence or 9
paucity of double-blind trials; as a result, no certain conclusions can be drawn. The 10
majority of available reports are case series and open-label trials. Although neurosurgery 11
has a more abundant database in treatment-resistant or clinically intractable OCD than the 12
other somatic therapies, its cost, irreversibility, and the lack of a clear relationship 13
between specific anatomic lesions and successful outcomes have limited and continue to 14
limit its use. 15
V.B.1. ______Transcranial Magnetic Stimulation (TMS) 16
Findings of the four published trials of repetitive TMS (rTMS) are inconsistent, perhaps 17
in part because the studies differed in design, stimulation sites, duration, and stimulation 18
parameters. The promising results and the techinique’s non-invasiveness and good 19
tolerability should encourage future research 20
Greenberg et al. (Greenberg et al. 1997) randomized 12 OCD patients (mean Y-21
BOCS 19.8 ± 9.7; 6 patients with past or current major depression) to 1 session of active 22
right-side or left-side or sham (occipital) rTMS (freq.: 20 Hz; Int.: 80%; 2 sec per minute, 23
time: 20 min; 8-shaped coil). Evaluations by blinded raters were made during the 24
stimulation and 30 minutes and 8 hours after treatment. Compulsive urges decreased 25
significantly with right lateral prefrontal rTMS (during stimulation and 30 minutes and 8 26
hours after stimulation), but not after left rTMS or occipital rTMS. Obsessive thoughts 27
did not change significantly after any stimulation. There was a modest increase in 28
positive mood after right prefrontal rTMS but not left or occipital stimulation. Treatment 29
was well tolerated, with two patients reporting mild headache after stimulation. 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
103
Methodological limitations include the duration of the treatment, the lack of Y-BOCS 1
outcome measures, small sample size, and the lack of a control group. 2
Alonso et al. (Alonso et al. 2001) found no advantages for low-frequency right 3
rTMS (freq.: 1 Hz; Int.: 110%; time: 20 min; circular coil) (n=10) over sham stimulation 4
(n=8) in a 6-week trial (three sessions per week). No drop-outs were reported, and side 5
effects, consisting of headache and cognitive difficulties, were modest and transient. 6
Sachdev et al. (Sachdev et al. 2001) randomized 12 treatment-resistant OCD 7
patients (a mean of 5.2 antiobsessional treatments and 0.8 trials of behavioral therapy 8
previously tried) to a 10-session single-blind 2-week trial of active right-side or left-side 9
rTMS (freq.: 110 HZ; Int.: 110%; time: 15 min; 8-shaped coil). Ten subjects taking 10
medications (benzodiazepines, antidepressants, or antipsychotics) were maintained on a 11
constant dose for 8 weeks prior to and during the study. Evaluations after 2 weeks of 12
stimulation and 4 weeks later showed significant reduction in obsessions and 13
compulsions in both groups, with no significant difference in Y-BOCS score between 14
right and left stimulation. Four patients (2 receiving left rTMS and 2 receiving right 15
TMS) had a clinically significant improvement (Y-BOCS reduction >40%); one patient 16
relapsed but responded somewhat to repeat treatment. No drop-outs were reported, and 17
stimulation was generally well tolerated, with three patients reporting headache. The 18
study interpretaton is limited by the lack of a placebo control group and the presence of 19
concurrent pharmacotherapy. 20
In an open-label trial (Mantovani et al. 2005), 10 treatment-resistant patients (5 21
with OCD, 3 with Tourette’s Syndrome and 2 with both) received low-frequency rTMS 22
(freq: 1 Hz; Int. 100%; 1200 stimuli/day, pulse series of of 5 minutes duration with inter-23
pulse interval of 2 minutes) for two weeks. Medication doses were stable for at least 12 24
weeks before and throughout rTMS and the follow-up period. The coil was placed along 25
the sagittal midline to stimulate the supplementary motor area bilaterally. Eight patients 26
completed the study; no drop-outs due to side effects were reported. CGI scores 27
decreased significantly at the end of the first and second weeks of treatment, with benefit 28
maintained at 1-month (t=5.670;d.f.=9; p=0.000) and 3-month (t=5.582; d.f.=9; p=0.000) 29
follow-ups. Three of the five pure OCD patients had a clinically significant improvement, 30
with a >40% reduction in Y-BOCS scores, and two Tourette’s patients had a complete 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
104
remission at the second week. Sixty percent of the sample had sustained clinical 1
improvement that persisted at 3-month follow-up. The study was limited by the open 2
design and small sample size. 3
V.B.2. ______Electroconvulsive Therapy (ECT) 4
The literature on ECT in treatment-resistant OCD includes a case series and several 5
individual cases, with some degree of effectiveness. However, the frequent Axis I 6
comorbidity among subjects, lack of standard outcome measures, absence of blinded 7
trials, and the invasiveness of ECT prevent it from being considered a valid treatment 8
strategy for treatment-resistent OCD uncomplicated by co-occurring conditions. 9
Common side effects include mild and temporary confusion and headache. 10
The case series (Maletzky et al. 1994) is a retrospective study of 32 patients with 11
DSM-III-R treatment-resistant OCD who received ECT between 1979 and 1991 (19 not 12
depressed and 13 depressed; 14 primarily checkers, 13 primarily cleaners, 4 did both). 13
They were treated with bilateral frontotemporal ECT (average 3–5 seizures per session 14
over 2–3 weeks) and were evaluated 2 days before and at 5 days, and 6 and 12 months 15
after the end of treatment. Comparison of baseline scores (BHS, WT, M-OCI) with scores 16
5 days after treatment yielded highly significant pre-post paired t-test (p<0.001). At 6 17
months post-treatment, the differences were still significant. However, by 12 months only 18
the M-OCI scores remained significantly different from those prior to ECT. Five patients 19
reported post-treatment agitation, which was treated with benzodiazepines. This study 20
found ECT had an antiobsessional effect, with improvements occurring equally 21
frequently and to an equal extent in the depressed and nondepressed groups. However, 22
methodological limitations include the absence of blinded ratings and standard outcome 23
measures, the use of medications during the long-term follow-up, and the presence of co-24
occurring depression in a significant proportion of patients (13/32). Furthermore, the 25
electrode placement and number of seizures per session are not considered standard ECT 26
procedure. 27
In addition, several single case-reports (Mellman & Gorman 1984; Casey & Davis 28
1994; Lavin & Halligan 1996; Thomas & Kellner 2003; Strassnig et al. 2004) provide 29
further evidence of possible efficacy of ECT in treatment-resistant OCD. However, the 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
105
unblinded ratings, frequent Axis I comorbidity (schizophrenia, depression, Tourette’s 1
syndrome), and the differing ECT parameters limit the confidence that can be placed in 2
the findings. Moreover, negative case reports are unlikely to have been written or 3
published. 4
V.B.3. ______Deep Brain Stimulation 5
Two small-sample double-blind trials and several case reports investigate the efficacy of 6
deep brain stimulation (DBS) in OCD. Given the preliminary promising results in 7
treatment-resistant OCD, the procedure’s reversibility in comparison with neurosurgery, 8
and the absence to date of serious adverse events, DBS deserves investigation in severe, 9
treatment-resistant OCD. 10
The first report (Nuttin et al. 1999; Nuttin et al. 2003) concerns six subjects with 11
OCD refractory to various antiobsessional treatments, and CBT (Y-BOCS ≥30, GAF 12
≤45, both for a minimum of 5 years) who were treated with DBS. Quadripolar electrodes 13
were implanted bilaterally in the anterior limbs of the internal capsules (parameters: pulse 14
width 210 to 450 microsec, frequency of 100 Hz and amplitude range of 4 to 10.5 v), 15
with the stimulation-off condition representing the placebo condition throughout the 21 16
months of evaluation. During all evaluation sessions the patients and the evaluating 17
psychiatrists and psychologists were blinded to the stimulation condition. Four patients 18
completed a blinded crossover trial (i.e., stimulator on for 3 months and stimulator off for 19
3 months, or vice versa, in random order). Three were YBOCS-35% responders during 20
the stimulation-on condition, with CGI-I scores of much improved. The mean CGI-21
Severity score decreased from 5.0 in the stimulation-off condition to 3.3 with the 22
stimulator on. Side effects included fatigue and memory disturbances. This small case 23
series showed that bilateral electrical stimulation in the anterior limbs of the internal 24
capsules may induce a significant decrease in OCD symptoms assessed with double-blind 25
evaluations. Responders reported clinically meaningful improvement in the first week of 26
stimulation. The persistence of the effect for at least 21 months argues against a placebo 27
effect. 28
The other two patients were subsequently studied (Gabriels et al. 2003). Patient 5 29
received a different electrode placement, one in each dorsomedial thalamic nucleus (DM) 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
106
and one in each internal capsula. The patient was always stimulated bilaterally in either 1
the internal capsules or the DMs. These conditions were then compared to the 2
stimulation-off condition in a gradual exposure experiment lasting 15 minutes. Each 3
combination was tested twice in a randomized order. The DM did not seem a good target 4
for this patient who, moreover, was considered a nonresponder with longer-term internal 5
capsule stimulation. 6
Patient 6 experienced a major improvement (more than 50% decrease in 7
postoperative tests) in his aggressive, intrusive thoughts when stimulation was turned on. 8
His mood improved dramatically as well. However, since his obsessions returned with 9
the former intensity 1 week after the crossover to blinded stimulation-off condition, the 10
research team, blinded to the stimulation condition, decided to abort this condition. 11
A double-blind trial enrolled four subjects with DSM-IV OCD refractory to at 12
least four antiobsessional medications, and CBT (Y-BOCS ≥25; GAF ≤44) (Abelson et 13
al. 2005). The patients, who had been on stable medication regimens for at least 6 weeks 14
before surgery and during the blinded phase of the study, received DBS with quadripolar 15
electrodes, placed stereotaxically in the anterior limb of each internal capsule 16
(parameters: fixed frequency of 130 Hz, pulse width of 210 microsec, amplitude range of 17
3–10.5 volts); the stimulation-off condition was the control. The double-blind phase of 18
the study consisted of four consecutive 3-week periods (in an alternating on-off design), 19
followed by an open phase in which stimulation, medication and CBT were adjusted to 20
optimize response for up to one year. During the double-blind phase, patient 2 showed a 21
YBOCS-35% response with stimulators on for periods 2 and 3. Patient 3 showed a more 22
moderate Y-BOCS improvement but also a placebo response. Patient 1 showed more 23
improvement in OCD and depression scores with stimulators on than off, but these 24
effects were small and not clinically meaningful. Patient 4 showed no consistent and 25
meaningful effects of stimulation during the blinded phase. During the open phase, two 26
patients showed a YBOCS-35% response. One subject showed mood elevation in 27
response to stimulation. PET scans showed orbitofrontal deactivation in the two patients 28
who had a positive clinical response and not in those with no response. Side effects, 29
mostly transient and prominent only at high amplitudes and monopolar settings, included 30
tingling, nausea, and diarrhea. This combined double-blind/open-label case-report series 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
107
showed positive results for deep brain stimulation in some patients with refractory OCD. 1
Chronic stimulation produced impressive reductions in OCD symptom ratings and 2
depression, although in one patient the depression remission was not maintained. 3
Beneficial effects needed variable times to appear ranging from 3 weeks to some months. 4
In addition, three recent single case reports of open DBS (Anderson & Ahmed 5
2003; Aouizerate et al. 2004; Fontaine et al. 2004) suggested the efficacy of deep brain 6
stimulation in treatment-resistant patients with OCD. Generally, stimulation was 7
prolonged for several months after surgery, and positive results were maintained in the 8
subsequent follow-up visits for up to 15 months. No serious adverse events were 9
reported. 10
V.B.4. ______Neurosurgery 11
Neurosurgical treatment for psychiatric disorders has a long and controversial history. 12
Today this approach is a highly selective treatment performed for only a few patients 13
with severe, treatment-refractory, affective, anxiety, or obsessive-compulsive disorders. 14
Given the availability of less invasive and reversible surgical procedures (deep brain 15
stimulation) for the treatment of intractable and treatment-resistant OCD, use of 16
traditional, irreversible neurosurgery is likely to dwindle in the near future. However, it 17
still represents a potentially efficacious alternative for a few carefully selected patients 18
with very severe OCD. 19
In view of the changes in neurosurgical techniques in the last decade, only trials 20
using these advanced techniques with adequate numbers of patients and specified 21
inclusion criteria and outcome measures are reviewed. 22
Oliver et al. (Oliver et al. 2003) reported on a prospective unblinded study of 23
bilateral anterior capsulotomy in 15 subjects with treatment-refractory OCD (mean 24
duration 18.1 ± 5.6 years; mean total Y-BOCS score 29.7). They observed positive 25
results at 1 and 12 months post-surgery: mean decrease on the Y-BOCS of 33.2%; 52.9% 26
of the patients showed a 33% decrease, 29.4% of the cases showed a 50% decrease and 27
17% showed a 66% decrease. No cognitive deficit was evident in neuropsychological 28
screening tests. Complications were observed in three cases: one with transitory 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
108
hallucinations, one with a single epileptic seizure, and one who developed a progressive 1
behavior disorder (not further specified) that became permanent. 2
An unblinded study (Dougherty et al. 2002) (including previous reported cases 3
(Jenike et al. 1991; Baer et al. 1995)) treated 44 subjects with DSM-III-R OCD refractory 4
to at least three SRIs trials, at least one SRI augmentation trial, and a trial of CBT (Y-5
BOCS ≥25, GAF ≤60, both for ≥5 years) with one or more cingulotomies (electrodes 6
positioned in each cingulate gyrus with MRI stereotactic guidance). Follow-up 7
evaluations were performed a mean of 32 months after the neurosurgery. At the first 8
follow-up (mean of 6.7 months after the first cingulotomy), mean Y-BOCS score 9
decrease was 20.4%, 11% of patients met full responder criteria (YBOCS-35% and CGI-10
I:1,2) and 9% of patients for partial response (either YBOCS-35% or CGI-I:1,2 or this 11
improvement not attributed to cingulotomy). At 32 months follow-up, mean Y-BOCS 12
score decrease was 28.7%, with 32% of patients classified as responders and 14% as 13
partial responders. At the most recent follow-up for the 18 patients who received multiple 14
cingulotomies, five (28%) were responders and two (11%) were partial responders. These 15
results suggest that cingulotomy may benefit some patients with severe treatment-16
refractory OCD. Although 20% of patients reported at least one adverse effect after 17
cingulotomy (memory disturbances, apathy, urinary disturbances), only two patients (5%) 18
reported enduring sequelae (seizure disorder and hydrocephalus). 19
Kim et al. (Kim et al. 2003) assessed the efficacy of bilateral anterior cingulotomy 20
in 14 subjects with treatment refractory and medically intractable OCD and evaluated 21
them up to 12 months after surgery. At the 6- and 12-month follow-ups, the mean Y-22
BOCS score decreased 28.9% and 36%, respectively, with 4/14 and 6/14 responders 23
(YBOCS-35% and CGI-I:1,2). No significant changes in cognitive functions and memory 24
were reported at the 12-month evaluation compared with preoperative scores. Adverse 25
effects after cingulotomy (headache, insomnia, weight-gain/loss) did not last more than 3 26
months with conservative treatment. 27
A retrospective unblinded study assessed the efficacy of bilateral anterior 28
cingulotomy in 15 subjects with treatment-refractory and medically intractable OCD and 29
followed them up for approximately 1 year (Richter et al. 2004). Four of the 15 patients 30
were YBOCS-35% responders. However, only one had sustained benefit lasting more 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
109
than one year. Minor postoperative symptoms included headache, nausea/vomiting and 1
urinary incontinence, which resolved after several months. Postoperative MRIs revealed 2
no clear relationship between lesion location and significant clinical improvement. 3
A small unblinded study of 12 subjects with treatment-refractory and medically 4
intractable OCD assessed the efficacy of limbic leucotomy (Montoya et al. 2002). 5
Patients were evaluated after a mean of 26 months. Five of 12 patients (42%) were 6
classified as responders (physician-rated CGI-I:1,2), and 8 of 13 (62%) patients rated 7
themselves as responders (self-report CGI-I:1,2). YBOCS-35% responder criterion was 8
met by 36%. One patient with a history of a suicide attempt committed suicide after the 9
surgical procedure. Minor postoperative symptoms of headache, low-grade fever, and 10
nausea/vomiting were common but generally lasted less than 48 hours. Postoperative 11
somnolence and apathy were noted in 29% and 24% of patients, respectively. Results are 12
comparable to the limited previous experience with limbic leucotomy in intractable OCD 13
reported (Hay et al. 1993). 14
V.C. PSYCHOTHERAPIES 15
V.C.1. ______Exposure Therapy 16
Historically, cognitive-behavioral therapy (CBT) for OCD has been divided into two 17
forms: 1) CBT that relies primarily on behavioral techniques, such as exposure and 18
response (or ritual) prevention (Meyer 1966), and 2) CBT that relies primarily on 19
cognitive therapy techniques, such as identifying, challenging, and modifying faulty 20
beliefs (BECK 1976; Salkovskis 1985). Certain variants of exposure therapy routinely 21
include some informal cognitive therapy techniques (e.g, a discussion of fear-related 22
thoughts and beliefs), and many variants of cognitive therapy include behavioral 23
experiments, which can be similar to exposure techniques. Therefore, these two forms of 24
CBT, as administered in treatment trials, often overlap. In clinical practice, these two 25
forms are often combined. 26
Studies that have examined CBT consisting of exposure and response (or ritual) 27
prevention (hereinafter called ERP) for adults with OCD are reviewed in this section. 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
110
V.C.1.a. ____Randomized Controlled Trials Comparing Exposure 1
Therapy to a Non-Active Treatment 2
Several randomized controlled trials have examined whether exposure therapy is superior 3
to a nonactive treatment. Although the studies used different variants of exposure therapy 4
(e.g., therapist-supervised or self-controlled exposures), different formats (e.g., individual 5
sessions versus group therapy), different intensity (e.g., frequency and length of sessions 6
per week), and different control groups, all studies concluded that exposure therapy is 7
efficacious for the treatment of adults with OCD. 8
Several early controlled studies reported that exposure therapy was superior to 9
progressive muscle relaxation (PMR) (e.g., (Marks et al. 1975; Roper et al. 1975)). These 10
studies were limited by their small samples and the lack of standard diagnostic and 11
outcome measures. 12
Fals-Stewart (Fals-Stewart et al. 1993) compared the efficacy of 12 weeks of 13
random assignment individual exposure therapy (N=31), group exposure therapy (N=30), 14
or PMR (N=32), an attention control condition. Subjects were free of major depression 15
and Axis II disorders, and were treatment naïve. Individual exposure treatment was 16
delivered in 1-hour sessions twice a week; group exposure treatment consisted of 2-hour 17
sessions twice per week delivered in groups of 10. In both cases, treatment consisted of 18
exposure (imaginal and in vivo) and response prevention. In those who completed 19
treatment, both individual and group exposure treatments were superior to PMR but not 20
to each other in reducing OCD and depressive symptoms (Y-BOCS reduction in 21
completers: 40% for individual; 46% for group; 9% for PMR). However, group exposure 22
treatment took much less staff time. Patients receiving either individual or group 23
treatment maintained their gains at 6-month follow-up; however, whether patients 24
received additional treatment during follow-up is unclear. 25
Lindsay et al. (Lindsay et al. 1997) randomly assigned 18 patients to either 26
exposure therapy (N=9) or anxiety management (N=9). Both treatments involved about 27
15 hours of therapy over a 3-week period. Exposure therapy consisted of graded exposure 28
to feared situations and ritual prevention both in sessions and as homework. Anxiety 29
management consisted of breathing retraining, PMR, and problem-solving. All patients 30
completed the study. Exposure therapy was significantly superior to anxiety management 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
111
for both OCD and depressive symptoms (e.g., Y-BOCS: 62% reduction for exposure; 6% 1
increase for anxiety management). Five patients continued SRIs during the study that had 2
brought “no improvement” for at least 12 months. Study limitations include the small 3
sample, the lack of independent raters, and the very short-term duration of observation. 4
A large multisite trial (Greist et al. 2002) randomized 218 patients to 10 weeks of 5
exposure therapy guided by a therapist (N=69), exposure therapy guided by a computer 6
and workbook (N=74), or systematic relaxation guided by an audiotape and manual 7
(N=75). Exposure therapy guided by a therapist consisted of 11 weekly 1-hour sessions 8
in which therapists told patients how to conduct exposures at home, but did not supervise 9
in-session exposures. Exposure therapy guided by computer used BT STEPS, a 9-step 10
computer-driven interactive voice response system that allows patients to telephone from 11
home and progress through a self-paced workbook. Relaxation therapy consisted of an 12
audiotape and manual that directed the patient to practice PMR 1 hour daily. Of those 13
who entered, 55 completed exposure therapy, 55 completed BT STEPS, and 66 14
completed PMR. In ITT analyses, exposure therapy was superior to BT STEPS, and both 15
were superior to PMR (Y-BOCS reduction: 32% for exposure therapy; 23% for BT 16
STEPS; 7% for PMR). Significantly more patients receiving exposure therapy were CGI-17
I:1,2 responders (60%), compared to patients receiving either BT STEPS (38%) or PMR 18
(14%). Patients who adhered to exposure therapy (either guided by clinician or computer) 19
had a larger mean decrease in their symptoms than the overall mean decrease for that 20
condition. Patients were followed for an additional 14 weeks. However, the groups 21
received different follow-up treatment, confounding overall group comparisons. Of note, 22
nonresponders to BT STEPS switched to clinician-guided exposure therapy had a 23
significant decrease in OCD severity, whereas nonresponders to exposure therapy 24
switched to BT STEPS did not. The authors concluded that minimal exposure therapy 25
(i.e., 11 weekly 1-hour sessions in which a therapist provides instructions only) is 26
superior to BT STEPS, and PMR is ineffective for OCD. However, the reduction in OCD 27
symptoms was substantially less than that seen in other studies in which therapists 28
supervised in-session exposures (e.g., compare ITT results in Lindsay et al. 1997 29
(Lindsay et al. 1997) and Foa et al. 2005 (Foa et al. 2005)). 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
112
A Brazilian controlled trial of group exposure therapy (Cordioli et al. 2003) 1
randomized OCD patients to 12 weeks of either group exposure therapy (N=23) or wait-2
list control (N=24). Although 45% of patients were on medications at the time of therapy, 3
they had been on a stable dose for at least 3 months. The group exposure therapy was 4
conducted in weekly 2-hour sessions in groups of seven or eight; it included in-session 5
exposure, ritual prevention, and cognitive restructuring. In ITT analyses, group exposure 6
therapy was significantly superior to the wait-list condition (Y-BOCS reduction: group 7
exposure therapy 43%; wait-list 6%); 70% of group exposure therapy patients were 8
YBOCS-35% responders. Twenty-two exposure therapy patients reevaluated after 3 9
months had maintained their gains. However, whether patients received additional 10
treatment during follow-up is not stated. 11
A multisite trial (Foa et al. 2005) compared the efficacy of 12 weeks of exposure 12
therapy, clomipramine, their combination, and pill placebo in adults with OCD and 13
without co-occurring depression. Of 122 entering randomly assigned treatment, 87 14
completed the study. Exposure therapy was delivered intensively for the first 4 weeks 15
(i.e., five 2-hour sessions per week); it consisted of exposure (imaginal and in vivo), 16
ritual prevention, and relapse prevention. During exposures, feared consequences and 17
dysfunctional beliefs were discussed. For the remaining 8 weeks, patients received 45-18
minute maintenance sessions in which no in-session exposures were conducted. Patients 19
randomized to clomipramine or placebo were seen for 30 minutes weekly by a research 20
psychiatrist. They received clomipramine or placebo titrated up to 200 mg/day in the first 21
5 weeks, with an optional increase to 250 mg/day if needed. In ITT and completer 22
analyses, all active treatments were superior to placebo. Treated and completer response 23
rates (CGI-I:1,2) were, respectively, 62% and 86% for exposure therapy, 42% and 48% 24
for clomipramine, 70% and 79% for combination treatment, and 8% and 10% for 25
placebo. Post-hoc analyses (Simpson et al. 2005b) demonstrated that exposure therapy 26
with or without clomipramine produced a significantly higher proportion of patients 27
(>50%) with minimal symptoms (i.e., Y-BOCS ≤12) than either placebo (0%) or 28
clomipramine alone (25%). 29
In addition to these randomized controlled trials, several controlled trials 30
compared exposure therapy to different variants of cognitive therapy with and without 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
113
SRI medication. These studies are reviewed in the section on cognitive therapy for OCD 1
(Section V.C.2). Overall, these studies also found that exposure therapy significantly 2
reduced OCD symptoms, further supporting the efficacy of exposure therapy for OCD. 3
However, most of these studies lacked a placebo or nonactive control condition. Two 4
used a wait-list control: van Balkom (van Balkom et al. 1998) reported that gradual self-5
controlled exposure therapy was significantly superior to 8 weeks of wait-list control; and 6
McLean (McLean et al. 2001) found that group exposure therapy was superior to wait-list 7
control. 8
Open trials of exposure therapy (totaling hundreds of patients) also support the 9
efficacy of exposure treatment for OCD (e.g., (Foa et al. 1985; Franklin et al. 2000; 10
Rothbaum & Shahar 2000; Warren & Thomas 2001)). 11
V.C.1.b. ____Factors that Affect Outcome From Exposure Therapy 12
Several factors appear to affect the outcome of exposure therapy with relapse prevention. 13
These include patient adherence to the exposure procedures (Abramowitz et al. 2002), the 14
patient’s degree of insight into the irrationality of their fears (with poor insight leading to 15
worse outcome (Kozak & Foa 1994; Foa et al. 1999)), and certain co-occurring 16
conditions. For example, severe depression and some co-occurring anxiety disorders 17
(e.g., posttraumatic stress disorder, generalized anxiety disorder) (Abramowitz et al. 18
2000; Steketee et al. 2001; Gershuny et al. 2002) may negatively impact outcome. In 19
addition, some data suggest that certain subtypes of OCD patients may not benefit as 20
much from exposure therapy. Therefore, modifications of standard exposure therapy for 21
certain OCD subtypes (e.g., severe hoarders, patients without overt compulsions) have 22
been developed and are being investigated (e.g., (Freeston et al. 1997; Steketee & Frost 23
2003)). Whether the addition of formal cognitive therapy elements can improve exposure 24
outcome (either for all OCD patients or for patients with co-occurring conditions like 25
depression) is also under investigation (Sections II.B.1, II.B.3, II.B.4, and V.C.2). 26
Some data suggest that exposure therapy is most effective when delivered 27
intensively (e.g., five sessions per week (Abramowitz 1996; National Institute for Health 28
and Clinical Excellence 2005)). On the other hand, one study found that twice-weekly 29
exposure therapy with relapse prevention was comparable to intensive treatment 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
114
(Abramowitz et al. 2003), and good results have been achieved with weekly, 1-hour 1
sessions (Whittal et al. 2005). To date, no study has compared once or twice weekly 2
treatment with intensive treatment in a randomized controlled design. 3
It remains unclear whether the effects of exposure therapy achieved in 4
randomized controlled trials can be reproduced in routine clinical practice. However, 5
several large case series found that exposure treatment (even when delivered weekly) can 6
produce robust effects in fee-for-service settings, as long as the therapists are skilled (or 7
supervised by those skilled) in exposure therapy for OCD (Franklin et al. 2000; Warren 8
& Thomas 2001). 9
V.C.1.c._____Long-Term Outcome From Exposure Therapy 10
Studies examining the long-term outcome of adult OCD patients after exposure treatment 11
have generally concluded that most patients remain treatment responders at follow-up 12
(Cottraux et al. 1990; Fals-Stewart et al. 1993; Foa & Kozak 1996; de Haan et al. 1997; 13
McLean et al. 2001; Cordioli et al. 2003; Simpson et al. 2004). However, these findings 14
are inconclusive for reasons that include design limitations in some studies (e.g., 15
uncontrolled studies and/or naturalistic follow-up), methodological limitations in others 16
(e.g., lack of standardized assessment instruments and/or blind ratings), and/or 17
inconsistencies in whether additional treatment was received during follow-up. A small 18
controlled study suggested that the inclusion of relapse prevention techniques enhances 19
maintenance of gains from exposure therapy (Hiss et al. 1994). 20
Recently, Simpson et al. (Simpson et al. 2004) examined the post-treatment 21
effects of exposure therapy with relapse prevention after sustained treatment 22
discontinuation using evaluators blind to original treatment assignment. Twelve weeks 23
after treatment discontinuation, the relapse rate was significantly lower, and the time to 24
relapse was significantly longer for exposure therapy with relapse prevention responders 25
(with or without concomitant clomipramine, N=33, 12% relapse rate) than for responders 26
to clomipramine alone (N=11, 45% relapse rate). Limitations include the small sample 27
size and short period of observation after treatment discontinuation. 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
115
V.C.1.d. ____Can Exposure Therapy Augment SRI Response? 1
Data from open trials (Simpson et al. 1999; Tolin et al. 2004), a completed randomized 2
trial (N=96) (Tenneij et al. 2005), and another large (N>110) randomized controlled trial 3
nearing completion indicate that CBT consisting of exposure and response prevention can 4
successfully augment a partial response to an adequate SRI trial. An open trial also 5
suggests that the addition of CBT consisting of exposure, response prevention, and 6
cognitive therapy can help SRI nonresponders, although this trial lacked a control group 7
continuing on medication alone(Kampman et al. 2002). 8
V.C.2. ______Cognitive Therapy 9
This section reviews studies that have examined the efficacy of cognitive therapy (CT) in 10
the treatment of adults with OCD. For the purposes of this review, CT includes those 11
variants of CBT that rely primarily on cognitive therapy techniques as described in 12
Section V.C.1. The studies address three issues: whether CT without exposure is 13
effective, whether CT is as effective as exposure therapy and/or medication, and whether 14
the addition of cognitive procedures to exposure therapy leads to better outcome. 15
V.C.2.a. ____Is Cognitive Therapy (Without Exposure) Efficacious 16
for OCD? 17
In a small randomized trial, Jones and Menzies (Jones & Menzies 1998) compared the 18
efficacy of group cognitive therapy to a wait-list control for OCD patients with 19
contamination concerns. Eleven patients received 9 weeks of Danger Ideation Reduction 20
Therapy (DIRT), which consisted of eight 1-hour group therapy sessions, and included 21
cognitive restructuring, expert testimony and corrective information, and attentional 22
focusing; DIRT proscribed exposure, response prevention, and behavioral experiments. 23
Although DIRT led to significant greater changes than the wait-list control on several 24
self-report OCD and depression measures, the effects were small (e.g., a 20% mean 25
reduction in OCD symptoms on the Maudsley Obsessional Compulsive Inventory). Study 26
limitations include its small sample size, self-report measures, and use of a wait-list 27
control. 28

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
116
In an open trial enrolling 15 patients, Wilhelm et al. (Wilhelm et al. 2005) found 1
that individual CT in the absence of prolonged exposure led to significant improvement 2
on several self-report OCD and depression measures (including the Y-BOCS, OBQ, and 3
BDI). CT consisted of 14 weekly 60-minute sessions, and included psychoeduction, CT 4
procedures following Beck’s method, and relapse prevention. Behavioral experiments 5
were used to test and correct a patient’s belief, but did not involve prolonged exposure. 6
In sum, there is limited evidence to support the efficacy of pure CT (i.e., cognitive 7
restructuring without exposure or “behavioral experiments”) in the treatment of OCD. 8
V.C.2.b. ____Is Cognitive Therapy as Efficacious as Exposure 9
Therapy for OCD? 10
Most direct comparisons of CT and exposure therapy have found that these treatments 11
produce similar results. However, strong conclusions are difficult to reach for a number 12
of reasons. First, some variants of exposure therapy include informal cognitive 13
techniques (e.g., relapse prevention, cognitive restructuring during exposures) and some 14
forms of cognitive therapy include informal exposure (i.e., behavioral experiments), 15
blurring the distinction between these treatments. Second, the published studies have 16
differed in their designs and treatment procedures (e.g., duration and frequency of 17
treatment sessions). Third, only some studies formally monitored therapist adherence to 18
the treatment protocols. Fourth, some studies had limited power to detect differences. 19
Fifth, no study included a placebo group other than a waitlist control. Therefore, the 20
treatment recommendations gleaned from these studies are necessarily specific to the 21
procedures they used and limited by these methodological weaknesses. Together, the data 22
suggest that CT that includes behavioral experiments has similar efficacy to exposure 23
therapy based solely on habitation (i.e., without discussion of feared consequences or 24
dysfunctional beliefs). 25
Two early studies by Emmelkamp (Emmelkamp et al. 1988; Emmelkamp & 26
Beens 1991) examined the efficacy of rational-emotive therapy (RET) based on the work 27
of Ellis (Ellis 1962); this CT program included the identification and challenge of 28
irrational beliefs but no behavioral experiments. Both studies found that therapist-29
administered RET helped OCD patients and was similar in efficacy to self-controlled 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
117
exposure therapy. Emmelkamp and Beens (Emmelkamp & Beens 1991) concluded that 1
RET followed by self-controlled exposure therapy was no better than self-controlled 2
exposure therapy alone. However, both studies had small samples (i.e., N ≤11 per 3
condition) and used a less than optimal exposure therapy format (e.g., self-controlled as 4
opposed to therapist-guided exposure). 5
A larger randomized trial (van Oppen et al. 1995) compared the outcomes of 28 6
patients who received 16 weeks of CT based on the model of Beck (BECK 1976) and 7
Salkovskis (Salkovskis 1985) and 29 patients who received self-controlled exposure. This 8
CT program targeted dysfunctional beliefs believed to be central to OCD (i.e., the 9
overestimation of danger and inflated personal responsibility), and specifically included 10
behavioral experiments. For both conditions, therapy was delivered weekly in 45-minute 11
sessions. In treatment completers, both treatments led to significant and clinically 12
meaningful improvement in OCD. Although there were no significant group differences, 13
CT appeared somewhat superior (Y-BOCS reduction: 45% for CT, 32% for exposure 14
therapy). However, a less than optimal exposure therapy format (e.g., self-controlled 15
exposure) was used, and the CT program used behavioral experiments. Half the patients 16
in this study participated in a multicenter trial comparing fluvoxamine, behavioral 17
therapy, and CT, described below. 18
Van Balkom et al. (van Balkom et al. 1998) randomized 117 patients to one of 19
five conditions: fluvoxamine + exposure therapy, exposure therapy, CT, fluvoxamine + 20
CT, or wait-list control. At baseline, patients on average had mild depressive symptoms. 21
Full results are presented for the 70 patients who completed 16 weeks of active treatment 22
and the 16 patients who completed the 8-week wait-list condition. The mean week 16 23
dose in both fluvoxamine conditions was 197 (±82) mg/day. All therapy sessions were 45 24
minutes long. CT and exposure therapy were delivered as in the van Oppen study (van 25
Oppen et al. 1995) above. CT targeted dysfunctional OCD beliefs and included 26
behavioral experiments. Exposure therapy consisted of gradual self-controlled exposure 27
in vivo with gradual self-imposed response prevention. At week 16, all active treatments 28
led to a significant decrease on all OCD measures, with no significant differences 29
between the treatment groups (Y-BOCS reduction for completers: 46% for CT [N=19], 30
32% for exposure therapy [N=19], 43% for fluvoxamine + CT [N=14], 49% for 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
118
fluvoxamine + exposure therapy [N=18]). The authors concluded there was no reason to 1
combine SRIs and CBT in OCD adults without severe co-occurring mood disorder. 2
However, neither the exposure nor the fluvoxamine treatments were optimized. 3
Moreover, the combination groups received only 10 therapy sessions starting after 8 4
weeks of fluvoxamine treatment, whereas the groups receiving exposure or CT alone 5
received 16 therapy sessions. Some of these patients were followed naturalistically for 6 6
months, but the fact that they received varied treatment during this follow-up period 7
precludes strong conclusions (de Haan et al. 1997). 8
A French multisite randomized trial (Cottraux et al. 2001) compared the outcome 9
of patients who received 20 hours of either CT (N=32) or exposure therapy (N=33) over 10
16 weeks. CT treatment consisted of 20 1-hour individual sessions following the Beck 11
and Salkovskis model (i.e., challenging of dysfunctional beliefs); behavioral experiments 12
to “confront feared situations to modify thoughts” were also used. Exposure therapy 13
consisting of therapist-aided exposure with response prevention was delivered in an 14
intensive phase (4 weeks of two 2-hour individual sessions per week) and a maintenance 15
phase (12 weeks of one 40-minute booster session every 2 weeks). In treatment 16
completers, both treatments led to significant and substantial reductions in OCD 17
symptoms (Y-BOCS reduction: 44% for CT; 42% for exposure therapy), and many 18
patients were YBOCS-25% responders (CT 77%; exposure therapy 70%). There were no 19
significant group differences. Patients were followed after treatment to week 52, but 26% 20
of the patients were lost to follow-up, and whether those followed received additional 21
treatment is unclear. 22
A Canadian randomized trial (McLean et al. 2001) randomized OCD patients 23
(48% who were on a stable dose of medication and half of whom had a co-occurring Axis 24
I disorder) to 12 weeks of CT (N=18), exposure therapy (N=16), or wait-list control 25
(N=33). Patients in the wait-list condition were randomly assigned to receive CT or 26
exposure therapy after the 12-week delay, and their data were pooled with those who 27
received active treatment initially. Treatment was delivered in groups and consisted of 28
2.5-hour sessions delivered once per week. Based on the work of Salkovskis (Salkovskis 29
1996), Freeston et al. (Freeston et al. 1996), and van Oppen and Arntz (van Oppen & 30
Arntz 1994), the CT focused on challenging appraisals of intrusive thoughts; behavioral 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
119
experiments were used to collect evidence for and against alternative appraisals. 1
Exposure therapy consisted of in-session and between-session exposure and ritual 2
prevention focused on producing habituation, and relapse prevention; discussion of 3
cognitive beliefs was proscribed. In treatment completers, both treatments were superior 4
to wait-list control; however, group exposure therapy was superior to group CT in the 5
pooled sample (Y-BOCS decrease: 39% for exposure therapy; 26% for CT). Of the 63 6
patients who completed treatment, 16% of CT patients and 38% of exposure therapy 7
patients recovered (defined as a Y-BOCS score decrease ≥6 points and a total score <12). 8
Of note, 12 of 49 CT and 2 of 44 exposure patients dropped out of the study after 9
learning their randomization and before starting treatment. Moreover, nearly twice as 10
many patients taking medication received exposure than CT. At 3-month follow-up, there 11
was still a significant advantage for exposure therapy over CT. However, these data are 12
limited by the fact that patients were not prohibited from obtaining treatment during 13
follow-up. 14
Another Canadian controlled trial (Whittal et al. 2005) randomized patients to 15
individual CT (N=37) or exposure therapy (N=34). Both treatments consisted of 12 16
weekly 60-minute sessions and followed the same format as in the McLean et al. 17
(McLean et al. 2001) study described above. Specifically, the CT focused on challenging 18
faulty thoughts but included behavioral experiments; the exposure treatment included 19
exposure and relapse prevention but no cognitive restructuring. In those who completed, 20
there was significant improvement in OCD severity in both treatment groups, with no 21
significant group differences (Y-BOCS reduction: 56% for CT; 52% for exposure 22
therapy). Of the 59 patients who completed treatment, 67% of CT and 59% of exposure 23
therapy patients recovered (as defined above). Both groups also had a significant 24
decrease in depressive symptoms and in dysfunctional beliefs. The authors concluded that 25
individual exposure therapy based on habituation only was similar in efficacy to 26
individual CT that included behavioral experiments, and that both treatments change 27
OCD conditions. 28
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
120
V.C.2.c._____Does the Addition of Cognitive Therapy Make 1
Exposure Therapy More Effective? 2
Some data suggest that exposure therapy is more effective if it relies not just on 3
habituation but includes discussion of feared consequences and dysfunctional beliefs. 4
One small study suggests that the addition of relapse prevention helps patients maintain 5
their gains. Whether CT added to exposure therapy helps OCD patients with co-occurring 6
conditions (e.g., depression) is under investigation <<BS: reference?>> 7
An early study by Emmelkamp et al. (Emmelkamp et al. 1980) found that both 8
exposure therapy and exposure therapy plus “self-instructional” talk (i.e., emitting more 9
positive statements after imagining being exposed to some feared stimulus) led to 10
clinically significant improvement. However, the small sample (N=8 vs. N=7) and the 11
diagnostic uncertainty of the sample (given the lack of standard criteria at that time) 12
preclude strong conclusions. 13
A small randomized trial (Hiss et al. 1994) examined whether exposure therapy 14
with (N=10) or without (N=10) relapse prevention produced different outcomes. Both 15
groups received 3 weeks of intensive exposure therapy (i.e., 15 daily sessions of exposure 16
with 45 minutes devoted to imaginal exposure and 45 minutes to in vivo sessions) 17
followed by either four 90-minute sessions of relapse prevention (i.e., discussion of 18
stressors likely to trigger OCD, meeting with a significant other to discuss maintenance 19
of gains, and cognitive restructuring) or of associative therapy (i.e., free association about 20
OCD symptoms) combined with progressive muscle relaxation (AT-PMR). Those 21
receiving relapse prevention also received nine 15-minute phone calls over 12 weeks of 22
follow-up. Outcome was evaluated after intensive exposure therapy with relapse 23
prevention and after 6 months of follow-up. Both groups had dramatic decreases in OCD 24
symptoms after intensive exposure therapy, without a significant difference (Y-BOCS 25
decreases in completers: 66% for relapse prevention; 60% for AT-PMR). However, at 6-26
month follow-up the relapse prevention group showed significantly less relapse than the 27
AT-PMR group on most measures and a trend in this direction on the Y-BOCS. The 28
authors concluded that relapse prevention helps patients maintain their gains from 29
exposure therapy. Relapse prevention techniques are part of some standard exposure 30
protocols (Kozak & Foa 1997) 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
121
A Norwegian randomized trial (Vogel et al. 2004) examined whether the exposure 1
protocol of Kozak and Foa (Kozak & Foa 1997), which includes discussion of feared 2
consequences and dysfunctional beliefs during exposures, could be improved by the 3
addition of formal CT elements based on Beck (BECK 1976). Patients were randomized 4
to receive exposure therapy + CT, exposure therapy + relaxation training, or wait-list 5
control for 6 weeks. After 6 weeks, those randomized to wait-list control were 6
randomized to one of the active treatments. The final sample consisted of 16 patients who 7
received exposure + CT and 19 patients who received exposure + relaxation training; 8
34% were on a stable dose of medication during the trial. Therapy consisted of 2-hour 9
sessions twice weekly for a total of 12 sessions. Each session consisted of 1.5 hours of 10
exposure therapy and 30 minutes of either CT (based on the Beck model and focused on 11
either co-occurring conditions or faulty OCD beliefs) or relaxation training (i.e., 12
progressive muscle relaxation). ITT analysis indicated that both active groups did 13
significantly better than wait-list controls, with no differences between the two active 14
conditions (Y-BOCS reduction: 33% for exposure + CT, 28% for exposure + relaxation 15
training). However, more patients completed exposure + CT (15/16) than exposure + 16
relaxation (12/19). The authors concluded that the addition of CT to exposure therapy 17
(delivered as outlined in (Kozak & Foa 1997)) may reduce dropout but does not 18
necessarily enhance efficacy. However, the sample was relatively small and there were 19
other methodological limitations (e.g., wait list design, many ratings were done by the 20
therapist, patients who received exposure + relaxation training got more exposure time). 21
Two recent studies have also examined whether CT added to exposure therapy 22
can improve outcome. <<Placeholder for Rector study: randomized 87 patients to 23
exposure therapy + CT or exposure therapy alone and found better results for 24
combo.>><<Placeholder for Salkovskis study: apparently supports use of cognitive 25
techniques during exposures.>> 26
V.C.3. ______Group and Multifamily Behavioral Treatment 27
<<LK will add>>A limited number of studies have investigated both group and 28
multifamily behavioral treatments for OCD. 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
122
Fals-Stewart et al. (Fals-Stewart et al. 1993) compared group (N=30) and 1
individual behavioral therapy (N=31) to an active control (progressive muscle relaxation; 2
N=32) in a 12-week unblinded random allocation study. Patients with major depression 3
or Axis II disorders were excluded. Both active treatments were superior to the control 4
treatment, as reflected in changes in Y-BOCS, BDI, and Social Adjustment Scale scores. 5
However, response to treatment was faster with individual behavior therapy. The authors 6
concluded that group therapy was useful for less severe OCD. From an efficiency 7
standpoint, the individual treatment consumed 720 staff hours compared to 48 hours in 8
the group therapy component. 9
McLean et al. (McLean et al. 2001) <<LK will add>> conducted a randomized 10
controlled trial (consisting of 12 weeks of weekly 2.5-hour groups) comparing group 11
CBT (N=34) and group ERP (N=42) with a wait-list control group, who were later 12
randomly assigned to either active treatment. Subjects were diagnosed with DSM-IV 13
OCD of greater than one year’s duration, were between 18 and 65 years old and had been 14
on a stable medication regimen for ≥3 months. Ninety-three subjects entered the trial, 76 15
began and 63 completed treatment. Both active treatments were significantly superior to 16
the control condition based on change in Y-BOCS scores. The effect sizes were ERP = 17
1.62; CBT = 0.98. The difference between the active treatments in the proportions 18
“recovered” subjects (Y-BOCS score decrease >5 points and a final score <12), ERP 19
(38%) and CBT (16%), was not significant. At 3-month follow-up, ERP was associated 20
with a significantly greater recovery rate: ERP (45%) and CBT (13%). The ERP group 21
included more subjects using medication, but in the analyses this did not appear to affect 22
improvement. This group also experienced more drop-outs. This study suggested that 23
group ERP was marginally superior to CBT, but several cautions need to be taken in 24
interpreting these results. 25
Cardioli et al. (Cordioli et al. 2003) <<LK will add>> conducted a single-blind 26
randomized trial comparing 12 weeks of weekly cognitive behavioral group therapy 27
(CBGT) (n=23) with a wait-list control (n=24). Seventy percent of those in CBGT were 28
YBOCS-35% responders compared to 4% of controls. The Y-BOCS score effect sizes in 29
the ITT groups were 1.33 for the CBGT group and 0.43 for controls. The therapeutic 30
gains were maintained at three month follow-up. CBGT was associated with a significant 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
123
improvement in the quality of life as measured by the WHOQOL-BREF. Nearly half the 1
subjects were maintained on stable medication regimens not influencing the effect of 2
active treatment. These and other reports suggest the utility of group behavioral therapies 3
in the treatment of OCD, however, additional study is warranted. 4
Van Noppen et al. (Van Noppen et al. 1997) conducted an uncontrolled double-5
blind study, without random assignment, comparing group behavioral therapy (N=17) 6
and multi-family behavioral therapy (N=19). In each treatment there were 10 to 12 2-hour 7
sessions monthly. This small study found that both modalities were effective treatments, 8
with a significant decrement in the Y-BOCS score in both, and a significant decrease in 9
the Sheehan Disability Inventory in the group behavioral therapy component. This study 10
provides support for both group approaches. There are too few studies of multi-family 11
behavioral therapy to provide sufficient evidence to support its use. 12
Mehta et al. (Mehta 1990) conducted an unblinded random allocation study in 13
India, in patients aged 18 to 55, who had had no prior behavioral therapy, but who had 14
ostensibly failed pharmacological treatment. Fifteen patients were allocated to a group in 15
which family members functioned as co-therapists conducting desensitization and ERP, 16
and 15 patients received the same treatment without a family member as a co-therapist. 17
The treatment group with a family co-therapist showed significantly greater improvement 18
at 12 weeks and at 1-month follow-up on the MOC, Zung, neuroticism, and the GAS. 19
This small study suggests the utility of family-based co-therapists, but is limited because 20
of the absence of a control group, and may not be generalizable to other cultures. 21
V.C.4. ______Computer-Assisted Behavioral Therapy 22
See Greist 2002(Greist et al. 2002) in Section V.C.1.a 23
V.C.5. ______Kundalini Yoga 24
<<LK will add>>In a randomized study (Shannahoff-Khalsa 2004) eleven OCD patients 25
(with unspecified characteristics) were allocated to 12 weeks of treatment with the 26
Kundalini yoga (KY) method and 10 subjects to mental mindfulness and relaxation 27
response management. Seven subjects completed each teatment arm. The subjects 28
received 30 minutes of exercises weekly for 3 months followed by 12 additional months 29

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
124
of open KY. In the first 12 weeks, The KY intent-to-treat group experienced a mean 38% 1
Y-BOCS score decrease (9.4 points), compared to 14% (2.9 points) in the control group 2
(the change in Y-BOCS scores were 9.4 vs. 2.9 points). In both groups, an unspecified 3
number of subjects were taking anti-OCD medications; whether any concurrent behavior 4
therapy was underway is unclear. Further improvement was reported in the 12-month 5
open extension of the study. This small study requires replication by an independent 6
group in subjects more clearly described before any conclusion about the effectiveness of 7
KY can be drawn. KY was apparently well tolerated, but the reasons that some subjects 8
failed to complete the trial are unclear. 9
V.D. COMBINED THERAPY 10
Only six randomized trials directly address whether the combination of SRI and CBT is 11
superior to either treatment alone in adults with OCD, and limitations in their designs 12
and/or procedures prevent definitive conclusions. Some of the studies also compared SRI 13
monotherapy to CBT monotherapy. Few of the studies had adequate sample sizes to 14
detect small differences between treatments, even if they did exist. Moreover, some 15
studies excluded patients with significant comorbidity even though comorbidity is 16
common in OCD and these patients may be those who would show the greatest benefit 17
from combination treatment. Finally, certain design decisions (e.g., how the treatments 18
were delivered) may have prevented the detection of important differences between 19
combination treatment and monotherapy. 20
Despite these problems, the available data support the premise that combination 21
therapy can be superior to monotherapy in some OCD patients, but is not necessary for 22
all OCD patients. In particular, one study found that combination therapy is superior to 23
exposure monotherapy in OCD patients with co-occurring depression (Hohagen et al. 24
1998). In OCD patients without co-occurring depression, another study found that 25
combination therapy and intensive exposure therapy alone were each superior to SRI 26
monotherapy (Foa et al. 2005). 27
Marks et al. (Marks et al. 1980) compared the outcome of 40 OCD patients 28
randomly assigned to oral clomipramine or pill placebo plus 30 sessions of 29
psychotherapy. The study design was complex: during weeks 0–4, patients received 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
125
either clomipramine or placebo; during weeks 4–10, patients also received either 30 1
sessions of exposure therapy or 15 sessions of relaxation training followed by 15 sessions 2
of exposure therapy. A direct comparison of the effects of clomipramine + exposure, 3
exposure + placebo, clomipramine + relaxation training, and placebo + relaxation training 4
could only be made at week 7. At that time, patients receiving clomipramine + exposure 5
(n=10) had more improvement in rituals than patients receiving exposure therapy + 6
placebo (n=10) or clomipramine + relaxation training (n=10); however, there was no 7
significant interaction of clomipramine and exposure. The complex design, small sample, 8
lack of standard OCD measures, and treatment procedures (e.g., the effects of 9
clomipramine were likely underestimated at week 7) preclude strong conclusions. 10
A separate study (Marks et al. 1988) compared the outcome of 49 patients 11
randomly assigned to one of four treatments: 6 months of clomipramine and 23 weeks of 12
anti-exposure instructions (clomipramine + anti-exposure); 6 months of clomipramine 13
and 23 weeks of self-controlled exposure (clomipramine + exposure [self]), 6 months of 14
clomipramine and 8 weeks of self-controlled exposure, followed by therapist-aided 15
exposure from weeks 8 to 23 (clomipramine + exposure [self and therapist]); or 6 months 16
of placebo and 8 weeks of self-controlled exposure, followed by therapist-aided exposure 17
from weeks 8 to 23 (placebo + exposure [self and therapist]). At week 8, clomipramine + 18
exposure (self, n=25) produced significantly more improvement in rituals and depression 19
than placebo + exposure (self, n=12). However, at week 23, clomipramine + exposure 20
(self and therapist, n=10) showed no superiority over placebo + exposure (self and 21
therapist) + placebo (n=8). At week 8, clomipramine + exposure (self, n=13) also 22
produced significantly more improvement than clomipramine + anti-exposure (n=12) in 23
rituals and depression. Only three of the clomipramine + anti-exposure cases improved 24
enough to continue, precluding further comparisons. The authors concluded that the 25
combination of clomipramine and exposure therapy had a small transitory additive effect 26
compared to placebo + exposure therapy. However, the complex design, small sample, 27
lack of standard OCD measures, and treatment procedures (e.g., the clomipramine groups 28
only achieved doses ranging from 127–157 mg/day) preclude strong conclusions. 29
Cottraux et al. (Cottraux et al. 1990) randomized 60 adult patients with OCD to 30
24 weeks of fluvoxamine with exposure therapy (fluvoxamine + exposure), fluvoxamine 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
126
with instructions not to engage in exposure (fluvoxamine + anti-exposure), or placebo + 1
exposure. Of the 60 patients who entered, 44 completed all 24 weeks (n=16, 13, and 15, 2
respectively); of these 44, 43% entered with a major depressive or dysthymic disorder 3
(mean 17-item HAM-D score was 19). Exposure therapy consisted of eight weekly 4
sessions that included imaginal exposure during sessions and self-controlled exposure, 5
followed by 16 weeks of therapist-guided exposure. In treatment completers, all groups 6
improved on some measures of rituals and depression, but only the fluvoxamine + 7
exposure group improved on all measures at week 24. The combined fluvoxamine 8
treatment groups had the largest percent reduction in the duration of rituals per day 9
(fluvoxamine + exposure = 46%; fluvoxamine + anti-exposure = 42%; placebo + 10
exposure = 25%) and the largest percentage of patients who, by self-report, had more 11
than a 30% reduction in rituals per day (fluvoxamine + exposure = 69%; fluvoxamine + 12
anti-exposure = 54%; placebo + exposure = 40%); however, these group differences were 13
not statistically significant. Study limitations include the small sample, the lack of 14
standard OCD measures, and the limited information about the treatment procedures 15
(e.g., the exposure protocol consisted of weekly sessions of an unspecified duration, and 16
other psychosocial interventions were provided “as needed”). 17
Hohagen et al. (Hohagen et al. 1998) randomized 60 adults with OCD to 18
fluvoxamine + exposure therapy or placebo + exposure therapy. Many patients had co-19
occurring mood, anxiety, and personality disorders (mean 21-item HAM-D score was 20
19), and many (92%) had received prior treatment (84% had taken medication, 35% had 21
prior exposure therapy). The mean dose of fluvoxamine was 288 mg/day (range 250–300 22
mg/day). Exposure therapy was conducted weekly for at least 3 hours and included 23
therapist-aided exposure as well as cognitive restructuring. After 9 weeks of treatment, 24
both groups showed significant reductions in OCD severity. However, there were 25
significantly more YBOCS-35% responders in the fluvoxamine + exposure group 26
(87.5%) than in the placebo + exposure group (60%). Post-hoc analyses revealed: 1) both 27
groups improved significantly and comparably on compulsions, but the fluvoxamine + 28
exposure group improved significantly more on obsessions; and 2) patients with co-29
occurring depression fared better if they received fluvoxamine + exposure. The authors 30
concluded that combination therapy should be used when obsessions dominate the 31

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
127
clinical picture or when a secondary depression is present. Limitations include the lack of 1
data on whether the two groups differed in their response to prior treatment and the fact 2
that only 49 patients entered the final analysis because 9 were removed to equate baseline 3
Y-BOCS scores in the two groups and 2 dropped out for clinical reasons. 4
Van Balkom et al. (van Balkom et al. 1998) randomized 117 patients to one of 5
five conditions: fluvoxamine + exposure therapy, exposure therapy, CT, fluvoxamine + 6
CT, or wait-list control. At baseline, patients on average had mild depressive symptoms. 7
Full results are presented for the 70 patients who completed 16 weeks of active treatment 8
and the 16 patients who completed the 8-week wait-list condition. The mean fluvoxamine 9
dose at week 16 in both fluvoxamine conditions was 197 (± 82) mg/day. All therapy 10
sessions were 45 minutes long. Exposure therapy consisted of gradual self-controlled 11
exposure in vivo with gradual self-imposed response prevention. At week 16, all active 12
treatments led to a significant decrease on all OCD measures, and there were no 13
significant differences between the treatment groups. The authors concluded there was no 14
reason to combine SRIs and CBT in OCD adults without severe co-occurring mood 15
disorder. However, neither the exposure nor the fluvoxamine treatments were optimized. 16
Moreover, the combination group received only 10 exposure sessions, whereas the group 17
receiving exposure alone received 16 sessions. 18
Foa et al. (Foa et al. 2005) compared the outcome of 122 adult OCD patients 19
randomized to exposure therapy, clomipramine, their combination (clomipramine + 20
exposure therapy), or placebo. Patients with major depressive disorder (and a HAM-D 21
≥18) were excluded. Mean daily doses of clomipramine during the last study week for all 22
who entered and all who completed (respectively) were 196 and 235 mg/day for 23
clomipramine patients, and 163 and 194 mg/day for clomipramine + exposure patients. 24
Exposure therapy was delivered intensively for the first 4 weeks (i.e., two information-25
gathering sessions, fifteen 2-hour exposure sessions conducted over 3 weeks, two home 26
visits); this was followed by eight 45-minute weekly maintenance sessions over the next 27
8 weeks. Patients receiving clomipramine + exposure began both treatments 28
simultaneously. At week 12, all active treatments were superior to placebo at reducing 29
OCD symptoms. In addition, clomipramine + exposure and exposure therapy did not 30
significantly differ from each other, but each was superior to clomipramine alone. For all 31
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
128
who entered treatment and all who completed the 12-week trial, the CGI-I:1,2 response 1
rates were, respectively, 70% and 79% for clomipramine + exposure, 42% and 48% for 2
clomipramine, 62% and 86% for exposure, and 8% and 10% for placebo. The authors 3
concluded that clomipramine, exposure therapy, and their combination are all efficacious 4
treatments for OCD. In addition, in OCD patients without co-occurring depression, 5
intensive exposure therapy is superior to clomipramine. The authors noted several factors 6
that may have limited their ability to detect a superiority of combination treatment over 7
exposure monotherapy (e.g., the exclusion of patients with co-occurring depression, the 8
potency of intensive exposure therapy, the fact that the combination group did not 9
achieve maximum clomipramine doses). Study limitations include the lack of data on 10
patients who dropped out after randomization but before treatment started and the lack of 11
systematic data on subjects’ prior treatment history. 12
V.E._DISCONTINUATION OF ACTIVE TREATMENT 13
Four double-blind SRI discontinuation studies in adults with OCD have been published. 14
Each concerned a different SRI and used a different design (e.g., length of observation 15
and method of placebo substitution) and a different relapse definition. Each came to a 16
different conclusion. 17
Pato et al. (Pato et al. 1988) found that 89% of their 18 clomipramine responders 18
had “substantial recurrence” (not further defined) of OCD 7 weeks after they were 19
blindly switched (over 4 days) to placebo. Romano et al. (Romano et al. 2001) found no 20
significant differences in 1-year estimates of relapse rates between 36 fluoxetine 21
responders maintained on fluoxetine (21%) versus 35 fluoxetine responders switched to 22
placebo (32%); relapse was defined as a ≥50% loss of improvement on the Y-BOCS, a 23
Y-BOCS score of ≥19, and a GCI-I rating of much or very much worse relative to the end 24
of treatment. Koran et al. (Koran et al. 2002) found that sertraline responders rarely 25
relapsed over 28 weeks whether they were maintained on sertraline (3/108=3%) or 26
switched over 2 weeks to placebo (5/113=4%); relapse was defined as a Y-BOCS 27
increase of ≥5 points, a total Y-BOCS score of ≥20, and a ≥1 point increase in CGI-I 28
score relative to the end of acute treatment at three consecutive visits at 2-week intervals. 29
Finally, Hollander et al. (Hollander et al. 2003a) found that paroxetine responders 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
129
maintained on paroxetine for 6 months, compared to those switched immediately to 1
placebo, had a significantly lower relapse rate (37.7% vs. 58.8%) and longer time to 2
relapse (62.9 days vs. 28.5 days); relapse was defined as a return to the pretreatment Y-3
BOCS score or a ≥1 point increase on the CGI-severity (CGI-S) scale (Guy 1976) relative 4
to the end of treatment. In summary, using different SRIs, different study designs, and 5
different relapse criteria, double-blind discontinuation studies reported SRI relapse rates 6
ranging from a low of 4% over 28 weeks (Koran et al. 2002) to a high of 89% over 7 7
weeks (Pato et al. 1988). 8
An unblinded study of 130 OCD patients (Ravizza et al. 1996a), which instituted 9
drug discontinuation after response to six months of open treatment, reported 10
significantly higher 6-month relapse rates for the patients whose medication was 11
discontinued: 8% (clomipramine 150 mg/day) versus 46% (no drug), 0% (fluoxetine 40 12
mg/day) versus 40% (no drug), and 8% (fluvoxamine 300 mg/day) versus 62% (no drug) 13
(Ravizza et al. 1996a). Equally large or larger disparities were present after one and two 14
years of treatment versus no treatment, and relapse rates were higher. Relapse was 15
defined as a Y-BOCS increase of ≥25% plus a CGI-I of much or very much worse 16
relative to the end of treatment. These data suggest both that SRIs may not fundamentally 17
differ in the long-term durability of treatment response after treatment discontinuation 18
and that most patients will eventually relapse after stopping SRI treatment. 19
In a review of 16 ERP studies, Foa and Kozak (Foa & Kozak 1996) concluded 20
that patients receiving ERP (with and without concomitant medication) did well long-21
term. Of 376 treated patients, 76% were responders at follow-up (mean, 29 months; 22
range, 6–72 months). Of responders to acute ERP treatment (with or without medication), 23
the proportion losing their response during follow-up was 20% or less in most studies. 24
While suggestive, these findings are inconclusive because of the following: 1) design 25
limitations in some studies (e.g., uncontrolled studies with naturalistic follow-up); 2) 26
methodological limitations in others (e.g., lack of evaluators blind to original treatment 27
assignment); 3) differences in determining “response”; 4) inconsistencies in whether 28
treatment during follow-up was permitted (and reported); and 5) differences in length of 29
follow-up. Further complicating any comparison with SRI relapse rates is the fact that the 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
130
relapse definition employed in this review (i.e., loss of response) differs from that used in 1
the SRI studies. 2
A multi-site study that compared the effects of clomipramine and ERP after 12 3
weeks of treatment (Foa et al. 2005) and again 12 weeks after treatment discontinuation 4
(Simpson et al. 2004) found that ERP responders (with or without concomitant 5
clomipramine) had a significantly lower relapse rate (12%) and longer time to relapse 6
after treatment discontinuation than responders to clomipramine alone (45%); relapse was 7
defined as a return to baseline severity on the CGI-S scale. Post-hoc analyses of these 8
data using different relapse criteria generally supported these findings, since most of the 9
relapse criteria examined produced the same outcome, albeit with substantial variability 10
in observed relapse rates (Simpson et al. 2005a). 11
Together, these data suggest that ERP treatment response may be more durable, at 12
least in the short-run, than response to some SRIs once they are discontinued. However, 13
the observed differences could be explained by other factors, including clinical 14
characteristics of the subjects studied, differences in the length of follow-up, the intensity 15
of treatment prior to treatment discontinuation, the rate of medication taper, and the 16
relapse criteria. Because of these differences, no definitive conclusions about the relative 17
durability of SRI and ERP treatment effects can be drawn from these studies. 18
As noted above, for many different definitions of relapse, Simpson et al. 19
(Simpson et al. 2005a) found that ERP responders (with or without clomipramine) had a 20
significantly lower rate of relapse and longer time to relapse 12 weeks after treatment 21
discontinuation than responders to clomipramine alone. 22
PART C. FUTURE RESEARCH NEEDS 23
It is a most gratifying sign of the rapid progress of our time that our best text-books 24 become antiquated so quickly. 25
Theodor Billroth, 1829–1994 26 The Medical Sciences in the German Universities, Part II 27
28 There are no such things as incurable, there are only things for which man has not found 29 a cure. 30
Bernard Baruch, 1870–1965 31 32

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
131
1. Incorporate the CONSORT recommendations for trial design and reporting 1
(Moher et al. 2001; Altman et al. 2001) into planning future OCD treatment trials. 2
2. Find genetic markers (Nicolini et al. 1991; Alsobrook et al. 1999; Cavallini et al. 3
1999; Nestadt et al. 2000a; Hanna et al. 2005a) for: 4
a. the risk of developing OCD in the children of OCD patients; 5
b. predicting response to particular medications; 6
c. predicting side effects to particular medications, or to classes of medications. 7
3. Identify new neurochemical targets for pharmacotherapy in order to improve the 8
proportion of responders, and the degree, rapidity, and permanence of response. 9
4. Standardize the definitions of degrees of treatment response, resistance, 10
remission, and relapse following the models of the International Treatment 11
Refractory OCD Consortium (ITROC) (Pallanti et al. 2002a) and Simpson et al. 12
(Simpson et al. 2005a; Simpson et al. 2005b). 13
5. Examine whether faster SRI titration or higher doses will bring faster treatment 14
response and greater degrees of symptom relief. 15
6. Develop effective medication augmentation strategies for patients inadequately 16
responsive to first-line medications. 17
7. Conduct adequate treatment trials with medications for which preliminary data 18
suggest effectiveness either alone or as augmentation strategies, e.g., mirtazapine, 19
lithium, anticonvulsants, pindolol, stimulants, opiate-receptor agonists, glutamate 20
modulating agents, and others. 21
8. Investigate promising physical treatments, i.e., transcutaneous magnetic 22
stimulation and deep brain stimulation. 23
9. Find peripheral markers (in blood, EEG, or neurocognitive measures) of early 24
medication or psychotherapy effects that predict whether the treatment will be 25
effective for the patient. 26
10. Develop a valid animal model for OCD. 27
11. Identify subtypes of OCD that require specific treatments, e.g., hoarding, OCD 28
with co-occurring tics, OCD with co-occurring schizotypal personality disorder, 29
and develop effective treatments for these subtypes. 30

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
132
12. Determine the optimal schedule for administering CBT, and the relative 1
effectiveness of different CBT treatment elements. The optimal schedule and the 2
effective elements may differ by OCD symptom type, e.g., contamination versus 3
hoarding versus mental compulsions. 4
13. Determine the optimal schedule for continuation and maintenance of CBT 5
treatments after the patient has achieved marked improvement, i.e., what should 6
be done to sustain response? 7
14. Compare the cost-effectiveness of individual versus group CBT treatment 8
sessions. 9
15. Examine the role of family therapies in treating OCD. 10
16. Determine the optimal methods of combining medications and psychotherapies to 11
produce the fastest onset, greatest degree of response, and least likelihood of 12
relapse. 13
17. Determine the effect of combined pharmacotherapy and CBT on relapse rates 14
after the discontinuation of medication. 15
18. Determine the necessary length of psychotherapy and of pharmacotherapy before 16
treatment can be safely discontinued, and relapse prevention strategies that are 17
helpful. 18
19. Create a reliable and valid self-rating scale to measure OCD symptom intensity. 19
20. Develop a sensitive and specific OCD screening questionnaire, self-rated, for use 20
in primary care. 21
21. Determine the degree to which private insurance policies discriminate against 22
OCD in comparison with general medical illness, on a state-by-state basis, i.e., the 23
extent of OCD coverage under parity laws, state-by-state. 24
22. Determine the direct and indirect costs of OCD to the U.S. economy (via health 25
care, lost work time of relatives caring for an OCD patient, lost productivity of 26
OCD patients, and premature death). 27
ACKNOWLEDGMENTS 28
Andrea Allen, Ph.D., and Bernardo Dell’Osso, M.D., assisted in the research and 29
development of this guideline. 30
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
133
INDIVIDUALS AND ORGANIZATIONS THAT 1
SUBMITTED COMMENTS 2
<<AA to add after draft 2 is reviewed.>> 3
APPENDIX A 4
The American Psychiatric Association does not vouch for or endorse the accuracy of the 5
information contained in any of the publications or Web sites listed in this Appendix at 6
the time of writing or in the future, although they are believed to be generally trustworthy 7
at the time of writing. The clinician should review a book or visit a Web site before 8
recommending it to a patient. 9
10
Resources for OCD: 11
1. Baer L. Getting Control: Overcoming Your Obsessions and Compulsions. New 12
York: Plume Books, 2000. 13
2. Baer L. The Imp of the Mind: Exploring the Silent Epidemic of Obsessive Bad 14
Thoughts. New York: Plume Books, 2001. 15
3. Chansky RE. Freeing Your Child from Obsessive-Compulsive Disorder. New 16
York: Crown, 2000. 17
4. Ciarrocchi JW. The Doubting Disease: Help for Scrupulosity and Religious 18
Compulsions. Mahwah, NJ: Paulist Press, 1998. 19
5. Foa EB, Wilson R. Stop Obsessing! How to Overcome Your Obsessions and 20
Compulsions. New York: Bantam, 2001. 21
6. Gravitz HL. Obsessive Compulsive Disorder: New Help for the Family. Santa 22
Barbara, CA: Healing Visions Press, 1998. 23
7. Grayson J. Freedom from Obsessive Compulsive Disorder: A Personalized 24
Recovery Program for Living with Uncertainty. New York: Penguin (Tarcher), 25
2003. 26
8. Hyman BM, Pedrick C. The OCD Workbook: Your Guide to Breaking Free from 27
Obsessive Compulsive Disorder, 2nd Edition. Oakland, CA: New Harbinger 28
Publications, 2005. 29
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
134
9. Munford PR. Overcoming Obsessive Checking. Oakland, CA: New Harbinger 1
Publications, 2004. 2
10. Munford PR. Overcoming Obsessive Washing. Oakland, CA, New Harbinger 3
Publications, 2005. 4
11. Osborn I. Tormenting Thoughts and Secret Rituals. New York: Dell, 1999. 5
12. Penzel F. Obsessive-Compulsive Disorders: A Complete Guide to Getting Well 6
and Staying Well. New York: Oxford University Press, 2000. 7
13. Santa, TM. Understanding Scrupulosity: Helpful Answers for Those Who 8
Experience Nagging Questions and Doubts. Ligouri, MI: Ligouri Publications, 9
1999. 10
14. Schwartz JM. Brain Lock: Free Yourself from Obsessive Compulsive Disorder. 11
New York: Harper Collins, 1996. 12
15. Steketee GS. Overcoming Obsessive-Compulsive Disorder—Client Manual. 13
Oakland, CA: New Harbinger, 1999. 14
16. Waltz M. Obsessive-Compulsive Disorder: Help for Children and Adolescents. 15
Sebastopol, CA: O’Reilly Press, 2000. 16
17. Wilhelm S, Steketee G. Cognitive Therapy of Obsessive-Compulsive Disorder: A 17
Guide for Professionals. Oakland, CA: New Harbinger Publications, 2006. 18
19 OC Foundation 20 676 State Street 21 New Haven CT 06511 22 Tel: 203-401-2070 23 Fax: 203-401-2076 24 www.ocfoundation.org 25 26 Scrupulous Anonymous (for those with religious/moral questioning OCD) 27 http://mission.liguori.org/newsletters/scrupanon.htm 28 29 San Francisco Bay Area Resource & Internet Guide for Extreme Hoarding 30 Behavior 31 http://www.hoarders.org 32 33 Resources for Tic Disorders: 34 Tourette Syndrome Association, Inc. 35 42-40 Bell Boulevard 36 Bayside NY 11361 37 Tel: 718-224-2999 38

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
135
http://www.tsa-usa.org/ 1 2 The American Academy of Child and Adolescent Psychiatry has “fact sheets” for 3 families about OCD, Tourette's disorder, anxiety disorders, and other disorders as well as 4 information about locating treating clinicians. 5 6 3615 Wisconsin Ave., NW 7 Washington, D.C. 20016-3007 8 Tel: 202-966-7300 9 http://www.aacap.org/ 10 http://www.aacap.org/publications/factsfam/index.htm 11 12 Resources for Anxiety Disorders: 13
1. Zuercher-White, E. Overcoming Panic Disorder and Agoraphobia: Client Manual. 14
Oakland, CA: New Harbinger Publications, 1999. 15
2. Schneier F, Welkowitz L. The Hidden Face of Shyness. New York: Avon Books, 16
1996. 17
3. Stein, MB , Walker JR. Triumph over Shyness: Conquering Shyness and Social 18
Anxiety. Columbus, OH: McGraw Hill, 2002. 19
4. Zimbardo PG. Shyness: What It Is and What To Do About It. New York: 20
Addison-Wesley, 1999. 21
22 Anxiety Disorders Association of America 23 Tel: 301-231-9350 24 http://www.adaa.org 25 http://socialanxietysupport.com 26 27
Resources for Autism: 28
1. Hollander E. Autism Spectrum Disorders. New York: Marcel Dekker, 2003. 29
2. Volkmar FR, Paul R, Klin A, Cohen DJ. Handbook of Autism and Pervasive 30
Developmental Disorders, Two Volume Set. New York: John Wiley & Sons, 31
2005. 32
3. Ozonoff S, Rogers SJ, Hendren DO. Autism Spectrum Disorders: A Research 33
Review for Practitioners. Washington, DC: American Psychiatric Publishing, 34
2003. 35
36 Resources for Body Dysmorphic Disorder: 37
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
136
1. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic 1
Disorder. New York: Oxford University Press, 1996. 2
2. Claiborn J, Pedrick C. The BDD Workbook: Overcoming Body Dysmorphic 3
Disorder and End Body Obsessions. Oakland, CA: New Harbinger Press, 2002. 4
3. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: How to Identiry, Treat 5
and Prevent Body Obsession in Men and Boys. New York: Touchstone, 2002. 6
7 Resources for Compulsive Buying: 8
1. Mellan O and Christie S. Overcoming Overspending: A Winning Plan for 9
Spenders and Their Partners. New York: Barnes & Noble Books, 2004. 10
2. Wesson C. Women Who Shop Too Much: Overcoming the Urge to Splurge. New 11
York: St Martin’s Press, 1990. 12
13
Debtors Anonymous 14 General Service Office 15 PO Box 920888 16 Needham, MA 02492-0009 17 Tel: 781-453-2743 18 Fax: 781-453-2745 19 [email protected] 20 21 Resources for Nonparaphilic Sexual Disorders: 22
Sexaholics Anonymous 23
Provides publications and access to meetings across the United States, which are modeled 24 on the 12-step program of Alcoholics Anonymous. 25 http://www.sa.org 26 27 Sexual Addicts Anonymous 28 Provides access to publications and local chapter meetings. 29 http://www.sexaa.org 30 31 Sexual Compulsives Anonymous (SCA) 32 Provides a list of meetings and a pen pal program controlled by SCA. 33 http://www.sca-recovery.org/ 34 35 The National Council on Sexual Addiction and Compulsivity 36 Provides information about sexual compulsions, addresses of 12-step programs, and 37 recommended readings. 38 http://www.ncsac.org 39

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
137
1 Resources for Kleptomania: 2
Cleptomaniacs & Shoplifters Anonymous (CASA) 3 507 Lawrence 4 Ann Arbor, MI 48104 5 Tel: 313-913-6990 6 email: [email protected] 7 8 National Association for Shoplifting Prevention 9 380 N. Broadway, suite 306 10 Jericho, NY 11753-2109 11 Tel: 1-800-848-9595 12 Fax: 516-932-9393 13 email: [email protected] 14 http://www.shopliftingprevention.org 15 16 Resources for Pathological Gambling: 17
1. Blaszczynski A. Overcoming Compulsive Gambling: A Self-Help Guide Using 18
Cognitive Behavioral Techniques. London: Robinson, 1998 19
2. Grant JE, Kim SW. Stop Me Because I Can’t Stop Myself: Taking Control of 20
Impulsive Behavior. New York: McGraw Hill, 2003. 21
3. National Council on Problem Gambling and National Endowment for Financial 22
Education. Personal Financial Strategies for the Loved Ones of Problem 23
Gamblers. Greenwood Village, CO: National Endowment for Financial 24
Educations, 2000. 25
26 Gamblers Anonymous 27 Provides limited information on problematic gambling, access to local meetings, which 28 are modeled on the 12-step methods of Alcoholics Anonymous. 29 http://www.gamblersanonymous.org 30 31 Council On Compulsive Gambling of New Jersey 32 Provides articles for the public, a directory of other state Councils on Compulsive 33 Gambling and links to related sites. 34 35 3635 Quakerbrigdge Road 36 Hamilton, NJ 08619 37 Tel: 1-800-GAMBLER 38 Tel: 609-588-5515 39 email: CCGN2800Gambler.org 40 http://www.800gambler.org/ 41
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
138
1 Resources for Trichotillomania: 2
1. Keuthen NJ, Stein DJ, Christenson GA. Help for Hair Pullers: Understanding and 3
Coping with Trichotillomania. Oakland, CA: New Harbinger Publications, 2001. 4
2. Penzel F. The Hair-Pulling Problem: A Complete Guide to Trichotillomana. New 5
York: Oxford University Press 2003. 6
7 Trichotillomania Learning Center 8 Tel: 831-457-1004 9 http://www.trich.org 10 11 Information on the Use of Medication During Pregnancy and Breast Feeding 12
California Teratogen Information Service and Clinical Research 13 Tel: 1-800-532-3749 (CA only) or 610-543-2131 14 www.otispregnancy.org/ctis.html 15 16 MGH Women’s Mental Health Program 17 www.womensmentalhealth.com 18 19 Resources for General Information on Mental Disorders and Medications: 20
National Institute of Mental Health (NIMH) 21 Public Information and Communications Branch 22 6001 Executive Boulevard, Room 8184, MSC 9663 23 Bethesda, MD 20892-9663 24 Tel: 1-866-615-6464 25 Fax: 301-443-4279 26 27 National Alliance on Mental Illness 28 Tel: 1-800-950-6264; or, 703-524-7600 29 http://www.nami.org 30 31 National Mental Health Association 32 1021 Prince St. 33 Alexandria, VA 22314-2971 34 Tel: 1-800-969-6642 or 703-684-7722 35 Fax: 703-684-5968 36 www.nmha.org 37 38 Madison Institute of Medicine (also Lithium Information Center, Obsessive 39 Compulsive Information Center, Bipolar Disorders Treatment Information Center) 40 7617 Mineral Point Road, Suite 300 41 Madison, WI 53717 42 Tel: 608-827-2470 43

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
139
Fax: 608-827-2479 1 Email: [email protected] 2 3 National Library of Medicine 4 U.S. government online repository of articles published in peer-reviewed medical 5 journals. 6 www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=PubMed 7 8 NIH complementary medicine reviews 9 Access to abstracts of peer-reviewed articles concerning complementary medicine 10 www.nlm.nih.gov/nccam/camonpubmed.html 11 12 ConsumerLab.com 13 Tests herbal and vitamin products for purity and posts the results on the Web 14 www.consumerlab.com 15 16 Mental Health Net 17 Features thousands of resources on the Internet. 18 www.mhnet.org 19
APPENDIX B 20
<<Possible scale to be included: Y-BOCS>> 21
<<RK/AA to discuss with ECPG and request permission.>> 22
REFERENCES 23
The following coding system is used to indicate the nature of the supporting evidence in 24
the references: 25
[A] Randomized double-blind clinical trial. A study of an intervention in which subjects 26
are prospectively followed over time; there are treatment and control groups; subjects are 27
randomly assigned to the two groups; both the subjects and the investigators are blind to 28
the assignments. 29
[A–] Randomized clinical trial. Same as above but not double-blind. 30
[B] Clinical trial. A prospective study in which an intervention is made and the results of 31
that intervention are tracked longitudinally; study does not meet standards for a 32
randomized clinical trial. 33

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
140
[C] Cohort or longitudinal study. A study in which subjects are prospectively followed 1
over time without any specific intervention. 2
[D] Control study. A study in which a group of patients and a group of control subjects 3
are identified in the present and information about them is pursued retrospectively or 4
backward in time. 5
[E] Review with secondary data analysis. A structured analytic review of existing data, 6
e.g., a meta-analysis or a decision analysis. 7
[F] Review. A qualitative review and discussion of previously published literature without 8
a quantitative synthesis of the data. 9
[G] Other. Textbooks, expert opinion, case reports, and other reports not included above. 10
11 Abelson, J. L., Curtis, G. C., Sagher, O., Albucher, R. C., Harrigan, M., Taylor, S. F. et al. (2005). 12
Deep brain stimulation for refractory obsessive-compulsive disorder. Biol Psychiatry, 57, 510-516. [A-] 13
Abramowitz, J. S. (1996). Variants of exposure and response prevention in the treatment of 14 obsessive-compulsive disorder: A meta-analysis. Behav Ther, 27, 583-600. [BS: CODE?] 15
Abramowitz, J. S. (1997). Effectiveness of psychological and pharmacological treatments for 16 obsessive-compulsive disorder: a quantitative review. J.Consult Clin.Psychol., 65, 44-52. [E] 17
Abramowitz, J. S. (2005). Understanding and Treating Obsessive-Compulsive Disorder: A 18 Cognitive Behavioral Approach. (vols. IN PRESS) Mahwah, NJ: Lawrence Earlbaum Associates. [G] 19
Abramowitz, J. S. & Foa, E. B. (2000). Does comorbid major depressive disorder influence 20 outcome of exposure and response prevention for OCD? Behav Ther, 31, 795-800. [LK: CODE?] 21
Abramowitz, J. S., Foa, E. B., & Franklin, M. E. (2003). Exposure and ritual prevention for 22 obsessive-compulsive disorder: effects of intensive versus twice-weekly sessions. J.Consult Clin.Psychol., 23 71, 394-398. [B] 24
Abramowitz, J. S., Franklin, M. E., Street, G. P., Kozak, M. J., & Foa, E. B. (2000). Effects of 25 comorbid depression on response to treatment for obsessive-compulsive disorder. Behav Ther, 31, 517-528. 26 [LK: CODE?] 27
Abramowitz, J. S., Franklin, M. E., Zoellner, L. A., & DiBernardo, C. L. (2002). Treatment 28 compliance and outcome in obsessive-compulsive disorder. Behav.Modif., 26, 447-463. [B] 29
Ackerman, D. L. & Greenland, S. (2002). Multivariate meta-analysis of controlled drug studies for 30 obsessive-compulsive disorder. J.Clin.Psychopharmacol., 22, 309-317. [E] 31
Ackerman, D. L., Greenland, S., & Bystritsky, A. (1998). Clinical characteristics of response to 32 fluoxetine treatment of obsessive-compulsive disorder. J.Clin.Psychopharmacol., 18, 185-192. [A] 33
Albert, U., Aguglia, E., Maina, G., & Bogetto, F. (2002). Venlafaxine versus clomipramine in the 34 treatment of obsessive-compulsive disorder: a preliminary single-blind, 12-week, controlled study. 35 J.Clin.Psychiatry, 63, 1004-1009. [A] 36
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
141
Alonso, P., Pujol, J., Cardoner, N., Benlloch, L., Deus, J., Menchon, J. M. et al. (2001). Right 1 prefrontal repetitive transcranial magnetic stimulation in obsessive-compulsive disorder: a double-blind, 2 placebo-controlled study. Am.J.Psychiatry, 158, 1143-1145. [A] 3
Alsobrook, J. P., Leckman, J. F., Goodman, W. K., Rasmussen, S. A., & Pauls, D. L. (1999). 4 Segregation analysis of obsessive-compulsive disorder using symptom-based factor scores. 5 Am.J.Med.Genet., 88, 669-675. [LK: CODE?] 6
Altman, D. G., Schulz, K. F., Moher, D., Egger, M., Davidoff, F., Elbourne, D. et al. (2001). The 7 revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern.Med, 8 134, 663-694. [LK: CODE?] 9
American Academy of Pediatrics (2001). Transfer of drugs and other chemicals into human milk. 10 Pediatrics, 108, 776-789. [LK: CODE?] 11
American Diabetes Association (2004). Consensus development conference on antipsychotic 12 drugs and obesity and diabetes. Diabetes Care, 27, 596-601. [LK: CODE?] 13
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders. 14 (4th ed.) Washington, DC: American Psychiatric Association. [G] 15
American Psychiatric Association (1998). Practice guideline for the treatment of patients with 16 panic disorder. Am J Psychiatry, 155, 1-34. [G] 17
American Psychiatric Association (2000a). Practice guideline for the treatment of patients with 18 HIV/AIDS. Am J Psychiatry, 157, 1-62. [G] 19
American Psychiatric Association (2000b). Practice guideline for the treatment of patients with 20 major depressive disorder (revision). Am J Psychiatry, 157, 1-45. [G] 21
American Psychiatric Association (2001). A Task Force Report on the Practice of 22 Electroconvulsive Therapy: Recommendations for Treatment, Training and Privileging. (2nd ed.) 23 Washington, DC: American Psychiatric Association. [G] 24
American Psychiatric Association (2002). Practice guideline for the treatment of patients with 25 bipolar disorder (revision). Am J Psychiatry, 159, 1-50. [G] 26
American Psychiatric Association (2003). Practice guideline for the assessment and treatment of 27 patients with suicidal behaviors. Am J Psychiatry, 160, 1-60. [G] 28
American Psychiatric Association (2004). Practice guideline for the treatment of patients with 29 schizophrenia, second edition. Am J Psychiatry, 161, 1-56. [G] 30
American Psychiatric Association (2006a). Practice guideline for the psychiatric evaluation of 31 adults, second edition. Am J Psychiatry, IN PRESS. [G] 32
American Psychiatric Association (2006b). Practice guideline for the treatment of patients with 33 substance use disorders, second edition. Am J Psychiatry, IN PRESS. [G] 34
American Psychiatric Association & American Academy of Child and Adolescent Psychiatry 35 (2004a). The Use of Medication in Treating Childhood and Adolescent Depression: Information for 36 Patients and Families. Arlington, VA: American Psychiatric Association. 37 http://www.parentsmedguide.org. [G] 38

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
142
American Psychiatric Association & American Academy of Child and Adolescent Psychiatry 1 (2004b). The Use of Medication in Treating Childhood and Adolescent Depression: Information for 2 Physicians. Arlington, VA: American Psychiatric Association. http://www.parentsmedguide.org. [G] 3
Americans With Disabilities Act (1990). Americans With Disabilities Act of 1990. 42 USC 12101-4 12213. [G] 5
Anderson, D. & Ahmed, A. (2003). Treatment of patients with intractable obsessive-compulsive 6 disorder with anterior capsular stimulation. Case report. J.Neurosurg., 98, 1104-1108. [G] 7
Angst, J., Gamma, A., Endrass, J., Goodwin, R., Ajdacic, V., Eich, D. et al. (2004). Obsessive-8 compulsive severity spectrum in the community: prevalence, comorbidity, and course. Eur.Arch.Psychiatry 9 Clin.Neurosci., 254, 156-164. [LK: CODE?] 10
Aouizerate, B., Cuny, E., Martin-Guehl, C., Guehl, D., Amieva, H., Benazzouz, A. et al. (2004). 11 Deep brain stimulation of the ventral caudate nucleus in the treatment of obsessive-compulsive disorder 12 and major depression. Case report. J Neurosurg., 101, 682-686. [D] 13
Arnold, P. D., Rosenberg, D. R., Mundo, E., Tharmalingam, S., Kennedy, J. L., & Richter, M. A. 14 (2004). Association of a glutamate (NMDA) subunit receptor gene (GRIN2B) with obsessive-compulsive 15 disorder: a preliminary study. Psychopharmacology (Berl), 174, 530-538. [GN: CODE?] 16
Ashton, A. K. & Weinstein, W. L. (2002). Cyproheptadine for drug-induced sweating. Am J 17 Psychiatry, 159, 874-875. [LK: CODE?] 18
Atmaca, M., Kuloglu, M., Tezcan, E., & Gecici, O. (2002). Quetiapine augmentation in patients 19 with treatment resistant obsessive-compulsive disorder: a single-blind, placebo-controlled study. 20 Int.Clin.Psychopharmacol., 17, 115-119. [A-] 21
Baer, L., Jenike, M. A., Black, D. W., Treece, C., Rosenfeld, R., & Greist, J. (1992). Effect of axis 22 II diagnoses on treatment outcome with clomipramine in 55 patients with obsessive-compulsive disorder. 23 Arch.Gen.Psychiatry, 49, 862-866. [LK: CODE?] 24
Baer, L. & Minichiello, W. E. (2005). Behavior therapy for obsessive-compulsive disorder. In M. 25 A. Jenike, L. Baer, & W. E. Minichiello (Eds.), Obsessive-Compulsive Disorders: Practical Management 26 (3rd ed., pp. 337-367). St. Louis: Mosby. [G] 27
Baer, L., Rauch, S. L., Ballantine, H. T., Jr., Martuza, R., Cosgrove, R., Cassem, E. et al. (1995). 28 Cingulotomy for intractable obsessive-compulsive disorder. Prospective long-term follow-up of 18 29 patients. Arch.Gen.Psychiatry, 52, 384-392. [C] 30
BECK, A. T. (1976). Cognitive Therapy and the Emotional Disorders. New York: International 31 Universities Press. [G] 32
BECK, A. T., WARD, C. H., MENDELSON, M., MOCK, J., & ERBAUGH, J. (1961). An 33 inventory for measuring depression. Arch Gen Psychiatry, 4, 561-571. [LK: CODE?] 34
Beck, J. S. (1997). Cognitive approaches to personality disorders. In J. H. Wright & M. E. Thase 35 (Eds.), Cognitive Therapy Review of Psychiatry (pp. START PAGE?-END PAGE?). Washington, DC: 36 American Psychiatric Press. [G] 37
Bejerot, S. & Bodlund, O. (1998). Response to high doses of citalopram in treatment-resistant 38 obsessive-compulsive disorder. Acta Psychiatr.Scand., 98, 423-424. [LK: CODE?] 39
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
143
Bellodi, L., Sciuto, G., Diaferia, G., Ronchi, P., & Smeraldi, E. (1992). Psychiatric disorders in the 1 families of patients with obsessive-compulsive disorder. Psychiatry Res., 42, 111-120. [GH: CODE?] 2
Bergeron, R., Ravindran, A. V., Chaput, Y., Goldner, E., Swinson, R., van Ameringen, M. A. et 3 al. (2002). Sertraline and fluoxetine treatment of obsessive-compulsive disorder: results of a double-blind, 4 6-month treatment study. J.Clin.Psychopharmacol., 22, 148-154. [A] 5
Berrios, G. E. (1996). The History of Mental Symptoms: Descriptive Psychopathology Since the 6 Nineteenth Century. Cambridge: Cambridge University Press. [G] 7
Biondi, M. & Picardi, A. (2005). Increased maintenance of obsessive-compulsive disorder 8 remission after integrated serotonergic treatment and cognitive psychotherapy compared with medication 9 alone. Psychother Psychosom, 74, 123-128. [LK: CODE?] 10
Bisserbe, J. C., Lane, R., & Flament, M. F. (1997). Double-blind comparison of sertraline and 11 clomipramine in patients with obsessive-compulsive disorder <<LK: NEED ALL AUTHOR NAMES>>. 12 Eur Psychiatry, 12, 82-93. [LK: CODE?] 13
Black, D. W., Monahan, P., Gable, J., Blum, N., Clancy, G., & Baker, P. (1998). Hoarding and 14 treatment response in 38 nondepressed subjects with obsessive-compulsive disorder. J.Clin.Psychiatry, 59, 15 420-425. [LK: CODE?] 16
Black, K., Shea, C., Dursun, S., & Kutcher, S. (2000). Selective serotonin reuptake inhibitor 17 discontinuation syndrome: proposed diagnostic criteria. J Psychiatry Neurosci, 25, 255-261. [LK: 18 CODE?] 19
Blanco, C., Schneier, F. R., Schmidt, A., Blanco-Jerez, C. R., Marshall, R. D., Sanchez-Lacay, A. 20 et al. (2003). Pharmacological treatment of social anxiety disorder: a meta-analysis. Depress.Anxiety, 18, 21 29-40. [LK: CODE?] 22
Blier, P. & Bergeron, R. (1996). Sequential administration of augmentation strategies in treatment-23 resistant obsessive-compulsive disorder: preliminary findings. Int.Clin.Psychopharmacol., 11, 37-44. [GH: 24 CODE?] 25
Bogan, A. M., Koran, L. M., Chuong, H. W., Vapnik, T., & Bystritsky, A. (2005). Quetiapine 26 augmentation in obsessive-compulsive disorder resistant to serotonin reuptake inhibitors: an open-label 27 study. J Clin Psychiatry, 66, 73-79. [B] 28
Bourgeois, J. A. (2005). Compliance with psychiatric treatment in primary care: review and 29 strategies. Primary Psychiatry, 12, 40-47. [LK: CODE?] 30
Buecking, A., Vandeleur, C. L., Khazaal, Y., & Zullino, D. F. (2005). Mirtazapine in drug-31 induced excessive sweating. Eur J Clin Pharmacol, 61, 543-544. [LK: CODE?] 32
Burke, K. C., Burke, J. D., Jr., Regier, D. A., & Rae, D. S. (1990). Age at onset of selected mental 33 disorders in five community populations. Arch.Gen.Psychiatry, 47, 511-518. [LK: CODE?] 34
Burt, V. K., Suri, R., Altshuler, L., Stowe, Z., Hendrick, V. C., & Muntean, E. (2001). The use of 35 psychotropic medications during breast-feeding. Am J Psychiatry, 158, 1001-1009. [LK: CODE?] 36
Bystritsky, A., Ackerman, D. L., Rosen, R. M., Vapnik, T., Gorbis, E., Maidment, K. M. et al. 37 (2004). Augmentation of serotonin reuptake inhibitors in refractory obsessive-compulsive disorder using 38 adjunctive olanzapine: a placebo-controlled trial. J.Clin.Psychiatry, 65, 565-568. [A] 39

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
144
Bystritsky, A., Munford, P. R., Rosen, R. M., Martin, K. M., Vapnik, T., Gorbis, E. E. et al. 1 (1996). A preliminary study of partial hospital management of severe obsessive-compulsive disorder. 2 Psychiatr.Serv., 47, 170-174. [LK: CODE?] 3
Cannon, T. D., Kaprio, J., Lonnqvist, J., Huttunen, M., & Koskenvuo, M. (1998). The genetic 4 epidemiology of schizophrenia in a Finnish twin cohort. A population-based modeling study. Arch Gen 5 Psychiatry, 55, 67-74. [GN: CODE?] 6
Carey, G. & Gottesman, I. I. (1981). Twin and family studies of anxiety, phobic and obsessive 7 disorders. In D. F. Klein & J. Rabkin (Eds.), Anxiety: New Research and Changing Concepts (pp. 117-8 136). New York: Raven Press. [G] 9
Carey, P. D., Vythilingum, B., Seedat, S., Muller, J. E., Van Ameringen, M., & Stein, D. J. (2005). 10 Quetiapine augmentation of SRIs in treatment refractory obsessive-compulsive disorder: a double-blind, 11 randomised, placebo-controlled study [ISRCTN83050762]. BMC.Psychiatry, 5, 5. [A] 12
Carrasco, J. L., Hollander, E., Schneier, F. R., & Liebowitz, M. R. (1992). Treatment outcome of 13 obsessive compulsive disorder with comorbid social phobia. J Clin Psychiatry, 53, 387-391. [LK: 14 CODE?] 15
Casey, D. A. & Davis, M. H. (1994). Obsessive-compulsive disorder responsive to 16 electroconvulsive therapy in an elderly woman. South.Med.J., 87, 862-864. [D] 17
Cavallini, M. C., Pasquale, L., Bellodi, L., & Smeraldi, E. (1999). Complex segregation analysis 18 for obsessive compulsive disorder and related disorders. Am.J.Med.Genet., 88, 38-43. [LK: CODE?] 19
Chabane, N., Millet, B., Delorme, R., Lichtermann, D., Mathieu, F., Laplanche, J. L. et al. (2004). 20 Lack of evidence for association between serotonin transporter gene (5-HTTLPR) and obsessive-21 compulsive disorder by case control and family association study in humans. Neurosci.Lett., 363, 154-156. 22 [GN: CODE?] 23
Cheung, A. H., Emslie, G. J., & Mayes, T. L. (2005). Review of the efficacy and safety of 24 antidepressants in youth depression. J Child Psychol Psychiatry, 46, 735-754. [GH: CODE "F" or "G"?] 25
Ciraulo, D. A. (2005). Drug Interactions in Psychiatry. (3rd ed.) Baltimore: Lippincott, Williams 26 and Wilkins. [G] 27
Clayton, A. H., Pradko, J. F., Croft, H. A., Montano, C. B., Leadbetter, R. A., Bolden-Watson, C. 28 et al. (2002). Prevalence of sexual dysfunction among newer antidepressants. J Clin Psychiatry, 63, 357-29 366. [LK: CODE?] 30
Clayton, A. H., Warnock, J. K., Kornstein, S. G., Pinkerton, R., Sheldon-Keller, A., & McGarvey, 31 E. L. (2004). A placebo-controlled trial of bupropion SR as an antidote for selective serotonin reuptake 32 inhibitor-induced sexual dysfunction. J Clin Psychiatry, 65, 62-67. [LK: CODE?] 33
Clifford, C. A., Murray, R. M., & Fulker, D. W. (1984). Genetic and environmental influences on 34 obsessional traits and symptoms. Psychol Med, 14, 791-800. [D] 35
Connor, K. M., Payne, V. M., Gadde, K. M., Zhang, W., & Davidson, J. R. (2005). The use of 36 aripiprazole in obsessive-compulsive disorder: preliminary observations in 8 patients. J Clin Psychiatry, 66, 37 49-51. [B] 38
Cora-Locatelli, G., Greenberg, B. D., Martin, J., & Murphy, D. L. (1998). Gabapentin 39 augmentation for fluoxetine-treated patients with obsessive-compulsive disorder. J.Clin.Psychiatry, 59, 40 480-481. [LK: CODE?] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
145
Cordioli, A. V., Heldt, E., Bochi, D. B., Margis, R., Basso de Sousa, M., Tonello, J. F. et al. 1 (2003). Cognitive-behavioral group therapy in obsessive-compulsive disorder: a randomized clinical trial. 2 Psychother.Psychosom., 72, 211-216. [GN: CODE "A" or "A-"?] 3
Coric, V., Taskiran, S., Pittenger, C., Wasylink, S., Mathalon, D. H., Valentine, G. et al. (2005). 4 Riluzole augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. Biol 5 Psychiatry. [LK: CODE?] 6
Cottraux, J., Mollard, E., Bouvard, M., Marks, I., Sluys, M., Nury, A. M. et al. (1990). A 7 controlled study of fluvoxamine and exposure in obsessive-compulsive disorder. 8 Int.Clin.Psychopharmacol., 5, 17-30. [A-] 9
Cottraux, J., Note, I., Yao, S. N., Lafont, S., Note, B., Mollard, E. et al. (2001). A randomized 10 controlled trial of cognitive therapy versus intensive behavior therapy in obsessive compulsive disorder. 11 Psychother.Psychosom., 70, 288-297. [A-] 12
Cox, B. J., Swinson, R. P., Morrison, B., & Lee, P. S. (1993). Clomipramine, fluoxetine, and 13 behavior therapy in the treatment of obsessive-compulsive disorder: a meta-analysis. 14 J.Behav.Ther.Exp.Psychiatry, 24, 149-153. [E] 15
Crane, D. L. (2005). Ziprasidone as an augmenting agent in the treatment of anxiety-spectrum 16 disorders. CNS Spectr., 10, 176-179. [G] 17
Crino, R., Slade, T., & Andrews, G. (2005). The changing prevalence and severity of obsessive-18 compulsive disorder criteria from DSM-III to DSM-IV. Am J Psychiatry, 162, 876-882. [LK: CODE?] 19
D'Amico, G., Cedro, C., Muscatello, M. R., Pandolfo, G., Di Rosa, A. E., Zoccali, R. et al. (2003). 20 Olanzapine augmentation of paroxetine-refractory obsessive-compulsive disorder. 21 Prog.Neuropsychopharmacol.Biol.Psychiatry, 27, 619-623. [BS: CODE?] 22
Dale, R. C., Heyman, I., Giovannoni, G., & Church, A. W. (2005). Incidence of anti-brain 23 antibodies in children with obsessive-compulsive disorder. Br J Psychiatry, 187, 314-319. [LK: CODE?] 24
Dannon, P. N., Sasson, Y., Hirschmann, S., Iancu, I., Grunhaus, L. J., & Zohar, J. (2000). Pindolol 25 augmentation in treatment-resistant obsessive compulsive disorder: a double-blind placebo controlled trial. 26 Eur.Neuropsychopharmacol., 10, 165-169. [A] 27
Davidson, J. R., Foa, E. B., Huppert, J. D., Keefe, F. J., Franklin, M. E., Compton, J. S. et al. 28 (2004). Fluoxetine, comprehensive cognitive behavioral therapy, and placebo in generalized social phobia. 29 Arch Gen Psychiatry, 61, 1005-1013. [LK: CODE?] 30
Davidson, J. R., Potts, N., Richichi, E., Krishnan, R., Ford, S. M., Smith, R. et al. (1993). 31 Treatment of social phobia with clonazepam and placebo. J Clin Psychopharmacol, 13, 423-428. [LK: 32 CODE?] 33
de Haan, E., van Oppen, P., van Balkom, A. J., Spinhoven, P., Hoogduin, K. A., & van Dyck, R. 34 (1997). Prediction of outcome and early vs. late improvement in OCD patients treated with cognitive 35 behaviour therapy and pharmacotherapy. Acta Psychiatr.Scand., 96, 354-361. [A] 36
Debattista, C., Solvason, B., Poirier, J., Kendrick, E., & Loraas, E. (2005). A Placebo-Controlled, 37 Randomized, Double-Blind Study of Adjunctive Bupropion Sustained Release in the Treatment of SSRI-38 Induced Sexual Dysfunction. J Clin Psychiatry, 66, 844-848. [LK: CODE?] 39
Den Boer, J. A. (1997). Psychopharmacology of comorbid obsessive-compulsive disorder and 40 depression. J.Clin.Psychiatry, 58 Suppl 8, 17-19. [LK: CODE?] 41
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
146
Denys, D., Burger, H., van Megen, H., de Geus, F., & Westenberg, H. (2003a). A score for 1 predicting response to pharmacotherapy in obsessive-compulsive disorder. Int.Clin.Psychopharmacol., 18, 2 315-322. [LK: CODE?] 3
Denys, D., de Geus, F., van Megen, H. J., & Westenberg, H. G. (2004a). A double-blind, 4 randomized, placebo-controlled trial of quetiapine addition in patients with obsessive-compulsive disorder 5 refractory to serotonin reuptake inhibitors. J.Clin.Psychiatry, 65, 1040-1048. [A] 6
Denys, D., van der, W. N., van Megen, H. J., & Westenberg, H. G. (2003b). A double blind 7 comparison of venlafaxine and paroxetine in obsessive-compulsive disorder. J.Clin.Psychopharmacol., 23, 8 568-575. [A] 9
Denys, D., van Megen, H. J., van der, W. N., & Westenberg, H. G. (2004b). A double-blind 10 switch study of paroxetine and venlafaxine in obsessive-compulsive disorder. J.Clin.Psychiatry, 65, 37-43. 11 [A] 12
Diering, S. L. & Bell, W. O. (1991). Functional neurosurgery for psychiatric disorders: a historical 13 perspective. Stereotact.Funct.Neurosurg., 57, 175-194. [F] 14
Diniz, J. B., Rosario-Campos, M. C., Shavitt, R. G., Curi, M., Hounie, A. G., Brotto, S. A. et al. 15 (2004). Impact of age at onset and duration of illness on the expression of comorbidities in obsessive-16 compulsive disorder. J.Clin.Psychiatry, 65, 22-27. [LK: CODE?] 17
Dougherty, D. D., Baer, L., Cosgrove, G. R., Cassem, E. H., Price, B. H., Nierenberg, A. A. et al. 18 (2002). Prospective long-term follow-up of 44 patients who received cingulotomy for treatment-refractory 19 obsessive-compulsive disorder. Am.J.Psychiatry, 159, 269-275. [C] 20
Douglass, H. M., Moffitt, T. E., Dar, R., McGee, R., & Silva, P. (1995). Obsessive-compulsive 21 disorder in a birth cohort of 18-year-olds: prevalence and predictors. J.Am.Acad.Child Adolesc.Psychiatry, 22 34, 1424-1431. [LK: CODE?] 23
Dreessen, L., Hoekstra, R., & Arntz, A. (1997). Personality disorders do not influence the results 24 of cognitive and behavior therapy for obsessive compulsive disorder. J.Anxiety.Disord., 11, 503-521. [LK: 25 CODE?] 26
Drummond, L. M. (1993). The treatment of severe, chronic, resistant obsessive-compulsive 27 disorder. An evaluation of an in-patient programme using behavioural psychotherapy in combination with 28 other treatments. Br.J.Psychiatry, 163, 223-229. [LK: CODE?] 29
Eapen, V. & Robertson, M. M. (2000). Comorbid obsessive-compulsive disorder and Tourette 30 Syndrome: therapeutic interventions. CNS.Drugs, 13, 173-183. [LK: CODE?] 31
Eddy, K. T., Dutra, L., Bradley, R., & Westen, D. (2004). A multidimensional meta-analysis of 32 psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clin Psychol Rev, 24, 1011-1030. 33 [E] 34
Eichstedt, J. A. & Arnold, S. L. (2001). Childhood-onset obsessive-compulsive disorder: a tic-35 related subtype of OCD? Clin Psychol Rev, 21, 137-157. [LK: CODE?] 36
Einarson, T. R. & Einarson, A. (2005). Newer antidepressants in pregnancy and rates of major 37 malformations: a meta-analysis of prospective comparative studies. Pharmacoepidemiol Drug Saf. [LK: 38 CODE?] 39
Eisen, J. L., Phillips, K. A., Baer, L., Beer, D. A., Atala, K. D., & Rasmussen, S. A. (1998). The 40 Brown Assessment of Beliefs Scale: reliability and validity. Am J Psychiatry, 155, 102-108. [LK: CODE?] 41
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
147
Eisen, J. L., Rasmussen, S. A., Phillips, K. A., Price, L. H., Davidson, J., Lydiard, R. B. et al. 1 (2001). Insight and treatment outcome in obsessive-compulsive disorder. Compr.Psychiatry, 42, 494-497. 2 [LK: CODE?] 3
Ellis, A. (1962). Reason and Emotion in Psychotherapy. New York: Lyle-Stuart. [G] 4
Emmelkamp, P. M. & Beens, H. (1991). Cognitive therapy with obsessive-compulsive disorder: a 5 comparative evaluation. Behav.Res.Ther., 29, 293-300. [A-] 6
Emmelkamp, P. M., van der, H. M., van Zanten, B. L., & Plochg, I. (1980). Treatment of 7 obsessive-compulsive patients: the contribution of self-instructional training to the effectiveness of 8 exposure. Behav.Res.Ther., 18, 61-66. 9
Emmelkamp, P. M., Visser, S., & Hoekstra, R. J. (1988). Cognitive therapy vs exposure in vivo in 10 the treatment of obsessive-compulsives. Cognit Ther Res, 12, 103-114. [A-] 11
Endicott, J., Nee, J., Harrison, W., & Blumenthal, R. (1993). Quality of Life Enjoyment and 12 Satisfaction Questionnaire: a new measure. Psychopharmacol Bull, 29, 321-326. [LK: CODE?] 13
Erzegovesi, S., Cavallini, M. C., Cavedini, P., Diaferia, G., Locatelli, M., & Bellodi, L. (2001). 14 Clinical predictors of drug response in obsessive-compulsive disorder. J.Clin.Psychopharmacol., 21, 488-15 492. [B] 16
Erzegovesi, S., Guglielmo, E., Siliprandi, F., & Bellodi, L. (2005). Low-dose risperidone 17 augmentation of fluvoxamine treatment in obsessive-compulsive disorder: a double-blind, placebo-18 controlled study. Eur Neuropsychopharmacol, 15, 69-74. [A] 19
Evans, R. W. & Lipton, R. B. (2001). Topics in migraine management: a survey of headache 20 specialists highlights some controversies. Neurol Clin, 19, 1-21. [LK: CODE?] 21
Expert Consensus Panel (1997). Treatment of obsessive-compulsive disorder. The Expert 22 Consensus Panel for obsessive-compulsive disorder. J.Clin.Psychiatry, 58 Suppl 4, 2-72. [LK: CODE?] 23
Fallon, B. A., Liebowitz, M. R., Campeas, R., Schneier, F. R., Marshall, R., Davies, S. et al. 24 (1998). Intravenous clomipramine for obsessive-compulsive disorder refractory to oral clomipramine: a 25 placebo-controlled study. Arch.Gen.Psychiatry, 55, 918-924. [A] 26
Fals-Stewart, W., Marks, A. P., & Schafer, J. (1993). A comparison of behavioral group therapy 27 and individual behavior therapy in treating obsessive-compulsive disorder. J.Nerv.Ment.Dis., 181, 189-193. 28 [A-] 29
Fava, M., Judge, R., Hoog, S. L., Nilsson, M. E., & Koke, S. C. (2000). Fluoxetine versus 30 sertraline and paroxetine in major depressive disorder: changes in weight with long-term treatment. J Clin 31 Psychiatry, 61, 863-867. [LK: CODE?] 32
Fava, M., Thase, M. E., & Debattista, C. (2005). A multicenter, placebo-controlled study of 33 modafinil augmentation in partial responders to selective serotonin reuptake inhibitors with persistent 34 fatigue and sleepiness. J Clin Psychiatry, 66, 85-93. [LK: CODE?] 35
Feder, R. (1995). Clonidine treatment of excessive sweating. J Clin Psychiatry, 56, 35. [LK: 36 CODE?] 37
Fennig, S., Fennig, S. N., Pato, M., & Weitzman, A. (1994). Emergence of symptoms of Tourette's 38 syndrome during fluvoxamine treatment of obsessive-compulsive disorder. Br J Psychiatry, 164, 839-841. 39 [LK: CODE?] 40
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
148
Figueroa, Y., Rosenberg, D. R., Birmaher, B., & Keshavan, M. S. (1998). Combination treatment 1 with clomipramine and selective serotonin reuptake inhibitors for obsessive-compulsive disorder in 2 children and adolescents. J Child Adolesc Psychopharmacol, 8, 61-67. [LK: CODE?] 3
Fineberg, N. A., Sivakumaran, T., Roberts, A., & Gale, T. (2005). Adding quetiapine to SRI in 4 treatment-resistant obsessive-compulsive disorder: a randomized controlled treatment study. Int Clin 5 Psychopharmacol, 20, 223-226. [A] 6
Fireman, B., Koran, L. M., Leventhal, J. L., & Jacobson, A. (2001). The prevalence of clinically 7 recognized obsessive-compulsive disorder in a large health maintenance organization. Am.J.Psychiatry, 8 158, 1904-1910. [LK: CODE?] 9
Flament, M. F. & Bisserbe, J. C. (1997). Pharmacologic treatment of obsessive-compulsive 10 disorder: comparative studies. J.Clin.Psychiatry, 58 Suppl 12, 18-22. [LK: CODE?] 11
Flament, M. F., Whitaker, A., Rapoport, J. L., Davies, M., Berg, C. Z., Kalikow, K. et al. (1988). 12 Obsessive compulsive disorder in adolescence: an epidemiological study. J Am Acad Child Adolesc 13 Psychiatry, 27, 764-771. [LK: CODE?] 14
Foa, E. B., Abramowitz, J. S., Franklin, M. E., & Kozak, M. J. (1999). Feared consequences, fixity 15 of belief, and treatment outcome in patients with obsessive-compulsive disorder. Behav Ther, 30, 717-724. 16 [BS: CODE?] 17
Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic, R., Hajcak, G. et al. (2002). The 18 Obsessive-Compulsive Inventory: development and validation of a short version. Psychol.Assess., 14, 485-19 496. [LK: CODE?] 20
Foa, E. B. & Kozak, M. J. (1996). Psychological treatment for obsessive-compulsive disorder. In 21 M. R. Mavissakalian & R. F. Prien (Eds.), Long-Term Treatments of Anxiety Disorders (pp. 285-309). 22 Washington, DC: American Psychiatric Press. [G] 23
Foa, E. B., Kozak, M. J., Goodman, W. K., Hollander, E., Jenike, M. A., & Rasmussen, S. A. 24 (1995). DSM-IV field trial: obsessive-compulsive disorder. Am J Psychiatry, 152, 90-96. [LK: CODE?] 25
Foa, E. B., Kozak, M. J., Steketee, G. S., & McCarthy, P. R. (1992). Treatment of depressive and 26 obsessive-compulsive symptoms in OCD by imipramine and behaviour therapy. Br.J.Clin.Psychol., 31 ( Pt 27 3), 279-292. [A] 28
Foa, E. B., Liebowitz, M. R., Kozak, M. J., Davies, S., Campeas, R., Franklin, M. E. et al. (2005). 29 Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their 30 combination in the treatment of obsessive-compulsive disorder. Am J Psychiatry, 162, 151-161. [BS: 31 CODE?] 32
Foa, E. B., Steketee, G., Kozak, M. J., & Dugger, D. (1987). Effects of imipramine on depression 33 and obsessive-compulsive symptoms. Psychiatry Res., 21, 123-136. [A] 34
Foa, E. B., Steketee, G. S., & Ozarow, B. J. (1985). Behavior Therapy With Obsessive-35 Compulsives: From Theory to Treatment. In M. Mavissakalian, S. M. Turner, & L. Michelson (Eds.), 36 Obsessive-Compulsive Disorder: Psychological and Pharmacological Treatment (pp. 59-129). New York: 37 Plenum Press. [G] 38
Fontaine, D., Mattei, V., Borg, M., von Langsdorff, D., Magnie, M. N., Chanalet, S. et al. (2004). 39 Effect of subthalamic nucleus stimulation on obsessive-compulsive disorder in a patient with Parkinson 40 disease. Case report. J Neurosurg., 100, 1084-1086. [D] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
149
Fontaine, R. & Chouinard, G. (1986). An open clinical trial of fluoxetine in the treatment of 1 obsessive-compulsive disorder. J.Clin.Psychopharmacol., 6, 98-101. [B] 2
Fontenelle, L. F., Mendlowicz, M. V., Marques, C., & Versiani, M. (2003). Early- and late-onset 3 obsessive-compulsive disorder in adult patients: an exploratory clinical and therapeutic study. 4 J.Psychiatr.Res., 37, 127-133. [LK: CODE?] 5
Food and Drug Administration (2004). FDA public health advisory: suicidality in children and 6 adolescents being treated with antidepressant medications. 7 http://www.fda.gov/cder/drug/antidepressants/SSRIPHA200410.htm. [G] 8
Franklin, M. E., Abramowitz, J. S., Kozak, M. J., Levitt, J. T., & Foa, E. B. (2000). Effectiveness 9 of exposure and ritual prevention for obsessive-compulsive disorder: randomized compared with 10 nonrandomized samples. J.Consult Clin.Psychol., 68, 594-602. [B] 11
Freeman, C. P., Trimble, M. R., Deakin, J. F., Stokes, T. M., & Ashford, J. J. (1994). Fluvoxamine 12 versus clomipramine in the treatment of obsessive compulsive disorder: a multicenter, randomized, double-13 blind, parallel group comparison. J.Clin.Psychiatry, 55, 301-305. [A] 14
Freeston, M. H. & Ladouceur, R. (1997). What do patients do with their obsessive thoughts? 15 Behav Res Ther, 35, 335-348. [LK: CODE?] 16
Freeston, M. H., Ladouceur, R., Gagnon, F., Thibodeau, N., Rheaume, J., Letarte, H. et al. (1997). 17 Cognitive-behavioral treatment of obsessive thoughts: a controlled study. J.Consult Clin.Psychol., 65, 405-18 413. [A-] 19
Freeston, M. H., Rheaume, J., & Ladouceur, R. (1996). Correcting faulty appraisals of obsessional 20 thoughts. Behav.Res.Ther., 34, 433-446. [LK: CODE?] 21
Fricke, S., Moritz, S., Andresen, B., Jacobsen, D., Kloss, M., Rufer, M. et al. (2005). Do 22 personality disorders predict negative treatment outcome in obsessive-compulsive disorders? A prospective 23 6-month follow-up study. Eur Psychiatry. [LK: CODE?] 24
Fux, M., Benjamin, J., & Belmaker, R. H. (1999). Inositol versus placebo augmentation of 25 serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over 26 study. Int J Neuropsychopharmcol., 2, 193-195. [A] 27
Gabbard, G. O. (2005). Psychodynamic Psychiatry in Clinical Practice. (4th ed.) Washington, 28 DC: American Psychiatric Publishing. [G] 29
Gabbard, G. O. & Newman, C. F. (2005). Psychotherapy of obsessive-compulsive personality 30 disorder. In G. O. Gabbard, J. Beck, & J. A. Holmes (Eds.), Oxford Textbook of Psychotherapy (pp. PAGE 31 START?-PAGE END?). Oxford, UK: Oxford University Press. [G] 32
Gabriels, L., Cosyns, P., Nuttin, B., Demeulemeester, H., & Gybels, J. (2003). Deep brain 33 stimulation for treatment-refractory obsessive-compulsive disorder: psychopathological and 34 neuropsychological outcome in three cases. Acta Psychiatr.Scand., 107, 275-282. [EH: CODE?] 35
Geller, D. A., Biederman, J., Faraone, S., Agranat, A., Cradock, K., Hagermoser, L. et al. (2001). 36 Developmental aspects of obsessive compulsive disorder: findings in children, adolescents, and adults. 37 J.Nerv.Ment.Dis., 189, 471-477. [LK: CODE?] 38
Geller, D. A., Biederman, J., Jones, J., Shapiro, S., Schwartz, S., & Park, K. S. (1998). Obsessive-39 compulsive disorder in children and adolescents: a review. Harv.Rev Psychiatry, 5, 260-273. [LK: 40 CODE?] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
150
Gershuny, B. S., Baer, L., Jenike, M. A., Minichiello, W. E., & Wilhelm, S. (2002). Comorbid 1 posttraumatic stress disorder: impact on treatment outcome for obsessive-compulsive disorder. 2 Am.J.Psychiatry, 159, 852-854. [B] 3
Gillman, P. K. (1999). The serotonin syndrome and its treatment. J Psychopharmacol, 13, 100-4 109. [LK: CODE?] 5
Giulino, L., Gammon, P., Sullivan, K., Franklin, M., Foa, E., Maid, R. et al. (2002). Is parental 6 report of upper respiratory infection at the onset of obsessive-compulsive disorder suggestive of pediatric 7 autoimmune neuropsychiatric disorder associated with streptococcal infection? J.Child 8 Adolesc.Psychopharmacol., 12, 157-164. [LK: CODE?] 9
Goodman, W. K., Kozak, M. J., Liebowitz, M., & White, K. L. (1996). Treatment of obsessive-10 compulsive disorder with fluvoxamine: a multicentre, double-blind, placebo-controlled trial. 11 Int.Clin.Psychopharmacol., 11, 21-29. [A] 12
Goodman, W. K., Price, L. H., Delgado, P. L., Palumbo, J., Krystal, J. H., Nagy, L. M. et al. 13 (1990). Specificity of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder. 14 Comparison of fluvoxamine and desipramine. Arch.Gen.Psychiatry, 47, 577-585. [A] 15
Goodman, W. K., Price, L. H., Rasmussen, S. A., Delgado, P. L., Heninger, G. R., & Charney, D. 16 S. (1989a). Efficacy of fluvoxamine in obsessive-compulsive disorder. A double-blind comparison with 17 placebo. Arch.Gen.Psychiatry, 46, 36-44. [A] 18
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Delgado, P., Heninger, G. R. et al. 19 (1989b). The Yale-Brown Obsessive Compulsive Scale. II. Validity. Arch Gen Psychiatry, 46, 1012-1016. 20 [LK: CODE?] 21
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L. et al. 22 (1989c). The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch Gen 23 Psychiatry, 46, 1006-1011. [LK: CODE?] 24
Goodman, W. K., Ward, H., Kablinger, A., & Murphy, T. (1997). Fluvoxamine in the treatment of 25 obsessive-compulsive disorder and related conditions. J.Clin.Psychiatry, 58 Suppl 5, 32-49. [LK: CODE?] 26
Grady, T. A., Pigott, T. A., L'Heureux, F., Hill, J. L., Bernstein, S. E., & Murphy, D. L. (1993). 27 Double-blind study of adjuvant buspirone for fluoxetine-treated patients with obsessive-compulsive 28 disorder. Am.J.Psychiatry, 150, 819-821. [LK: CODE?] 29
Greenberg, B. D., George, M. S., Martin, J. D., Benjamin, J., Schlaepfer, T. E., Altemus, M. et al. 30 (1997). Effect of prefrontal repetitive transcranial magnetic stimulation in obsessive-compulsive disorder: a 31 preliminary study. Am.J.Psychiatry, 154, 867-869. [B] 32
Greenblatt, D. J., von Moltke, L. L., Harmatz, J. S., & Shader, R. I. (1998). Drug interactions with 33 newer antidepressants: role of human cytochromes P450. J Clin Psychiatry, 59 Suppl 15, 19-27. [LK: 34 CODE?] 35
Greist, J., Chouinard, G., DuBoff, E., Halaris, A., Kim, S. W., Koran, L. et al. (1995a). Double-36 blind parallel comparison of three dosages of sertraline and placebo in outpatients with obsessive-37 compulsive disorder. Arch.Gen.Psychiatry, 52, 289-295. [LK: CODE?] 38
Greist, J. H., Jefferson, J. W., Kobak, K. A., Chouinard, G., DuBoff, E., Halaris, A. et al. (1995b). 39 A 1 year double-blind placebo-controlled fixed dose study of sertraline in the treatment of obsessive-40 compulsive disorder. Int.Clin.Psychopharmacol., 10, 57-65. [A] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
151
Greist, J. H., Jenike, M. A., Robinson, D., & Rasmussen, S. A. (1995c). Efficacy of fluvoxamine 1 in obsessive-compulsive disorder: results of a multicentre, double blind, placebo controlled trial. Eur J Clin 2 Res, 7, 195-204. [EH: CODE?] 3
Greist, J. H., Marks, I. M., Baer, L., Kobak, K. A., Wenzel, K. W., Hirsch, M. J. et al. (2002). 4 Behavior therapy for obsessive-compulsive disorder guided by a computer or by a clinician compared with 5 relaxation as a control. J.Clin.Psychiatry, 63, 138-145. [GN: CODE: "A" or "A-"?] 6
Gunderson, J. G. (1988). Personality disorders. In A. M. Nicholi Jr. (Ed.), The New Harvard 7 Guide to Psychiatry (pp. 337-357). Cambridge, MA: Belknap Press. [G] 8
Guy, W. (1976). ECDEU Assessment Manual for Psychopharmacology, Revised. Rockville, MD: 9 DHEW Publication No. (ABM) 76-338. [LK: CODE?] 10
Haddad, P. M. (2001). Antidepressant discontinuation syndromes. Drug Saf, 24, 183-197. [LK: 11 CODE?] 12
Hall, D., Dhilla, A., Charalambous, A., Gogos, J. A., & Karayiorgou, M. (2003). Sequence 13 variants of the brain-derived neurotrophic factor (BDNF) gene are strongly associated with obsessive-14 compulsive disorder. Am.J.Hum.Genet., 73, 370-376. [GN: CODE?] 15
Hambrick, J. P., Weeks, J. W., Harb, G. C., & Heimberg, R. G. (2003). Cognitive-behavioral 16 therapy for social anxiety disorder: supporting evidence and future directions. CNS Spectr., 8, 373-381. 17 [LK: CODE?] 18
HAMILTON, M. (1960). A rating scale for depression. J Neurol Neurosurg.Psychiatry, 23, 56-62. 19 [LK: CODE?] 20
Hanna, G. L., Fingerlin, T. E., Himle, J. A., & Boehnke, M. (2005a). Complex Segregation 21 Analysis of Obsessive-Compulsive Disorder in Families with Pediatric Probands. Hum Hered., 60, 1-9. 22 [GH: CODE?] 23
Hanna, G. L., Himle, J. A., Curtis, G. C., & Gillespie, B. W. (2005b). A family study of obsessive-24 compulsive disorder with pediatric probands. Am J Med Genet B Neuropsychiatr.Genet, 134, 13-19. [GH: 25 CODE?] 26
Hanna, G. L., Veenstra-VanderWeele, J., Cox, N. J., Boehnke, M., Himle, J. A., Curtis, G. C. et al. 27 (2002). Genome-wide linkage analysis of families with obsessive-compulsive disorder ascertained through 28 pediatric probands. Am.J.Med.Genet., 114, 541-552. [GH: CODE?] 29
Haria, M., Fitton, A., & McTavish, D. (1994). Trazodone. A review of its pharmacology, 30 therapeutic use in depression and therapeutic potential in other disorders. Drugs Aging, 4, 331-355. [LK: 31 CODE?] 32
Hay, P., Sachdev, P., Cumming, S., Smith, J. S., Lee, T., Kitchener, P. et al. (1993). Treatment of 33 obsessive-compulsive disorder by psychosurgery. Acta Psychiatr.Scand., 87, 197-207. [C] 34
Hembree, E. A., Riggs, D. S., Kozak, M. J., Franklin, M. E., & Foa, E. B. (2003). Long-term 35 efficacy of exposure and ritual prevention therapy and serotonergic medications for obsessive-compulsive 36 disorder. CNS.Spectr., 8, 363-71, 381. [B] 37
Hermesh, H., Aizenberg, D., & Munitz, H. (1990). Trazodone treatment in clomipramine-resistant 38 obsessive-compulsive disorder. Clin.Neuropharmacol., 13, 322-328. [C] 39
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
152
Hermesh, H., Shahar, A., & Munitz, H. (1987). Obsessive-compulsive disorder and borderline 1 personality disorder. Am J Psychiatry, 144, 120-122. [LK: CODE?] 2
Hettema, J. M., Neale, M. C., & Kendler, K. S. (2001). A review and meta-analysis of the genetic 3 epidemiology of anxiety disorders. Am.J.Psychiatry, 158, 1568-1578. [E] 4
Hewlett, W. A., Schmid, S. P., & Salomon, R. M. (2003). Pilot trial of ondansetron in the 5 treatment of 8 patients with obsessive-compulsive disorder. J.Clin.Psychiatry, 64, 1025-1030. [LK: 6 CODE?] 7
Hewlett, W. A., Vinogradov, S., & Agras, W. S. (1992). Clomipramine, clonazepam, and 8 clonidine treatment of obsessive-compulsive disorder. J.Clin.Psychopharmacol., 12, 420-430. [A] 9
Heyman, I., Fombonne, E., Simmons, H., Ford, T., Meltzer, H., & Goodman, R. (2001). 10 Prevalence of obsessive-compulsive disorder in the British nationwide survey of child mental health. 11 Br.J.Psychiatry, 179, 324-329. [LK: CODE?] 12
Hiss, H., Foa, E. B., & Kozak, M. J. (1994). Relapse prevention program for treatment of 13 obsessive-compulsive disorder. J.Consult Clin.Psychol., 62, 801-808. [A-] 14
Hoehn-Saric, R., Ninan, P., Black, D. W., Stahl, S., Greist, J. H., Lydiard, B. et al. (2000). 15 Multicenter double-blind comparison of sertraline and desipramine for concurrent obsessive-compulsive 16 and major depressive disorders. Arch.Gen.Psychiatry, 57, 76-82. [A] 17
Hohagen, F., Winkelmann, G., Rasche-Ruchle, H., Hand, I., Konig, A., Munchau, N. et al. (1998). 18 Combination of behaviour therapy with fluvoxamine in comparison with behaviour therapy and placebo. 19 Results of a multicentre study. Br.J.Psychiatry Suppl, 71-78. [A] 20
Hollander, E., Allen, A., Steiner, M., Wheadon, D. E., Oakes, R., & Burnham, D. B. (2003a). 21 Acute and long-term treatment and prevention of relapse of obsessive-compulsive disorder with paroxetine. 22 J.Clin.Psychiatry, 64, 1113-1121. [A] 23
Hollander, E., Baldini, R. N., Sood, E., & Pallanti, S. (2003b). Risperidone augmentation in 24 treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. 25 Int.J.Neuropsychopharmacol., 6, 397-401. [A] 26
Hollander, E., Bienstock, C. A., Koran, L. M., Pallanti, S., Marazziti, D., Rasmussen, S. A. et al. 27 (2002). Refractory obsessive-compulsive disorder: state-of-the-art treatment. J.Clin.Psychiatry, 63 Suppl 6, 28 20-29. [F] 29
Hollander, E., Friedberg, J., Wasserman, S., Allen, A., Birnbaum, M., & Koran, L. M. (2003c). 30 Venlafaxine in treatment-resistant obsessive-compulsive disorder. J.Clin.Psychiatry, 64, 546-550. [B] 31
Hollander, E., Greenwald, S., Neville, D., Johnson, J., Hornig, C. D., & Weissman, M. M. (1996). 32 Uncomplicated and comorbid obsessive-compulsive disorder in an epidemiologic sample. 33 Depress.Anxiety., 4, 111-119. [LK: CODE?] 34
Hollander, E., Kaplan, A., & Stahl, S. M. (2003d). A double-blind, placebo-controlled trial of 35 clonazepam in obsessive-compulsive disorder. World J.Biol.Psychiatry, 4, 30-34. [A] 36
Hollander, E., Koran, L. M., Goodman, W. K., Greist, J. H., Ninan, P. T., Yang, H. et al. (2003e). 37 A double-blind, placebo-controlled study of the efficacy and safety of controlled-release fluvoxamine in 38 patients with obsessive-compulsive disorder. J.Clin.Psychiatry, 64, 640-647. [A] 39
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
153
Hollander, E. & Wong, C. M. (1995). Obsessive-compulsive spectrum disorders. J Clin 1 Psychiatry, 56 Suppl 4, 3-6. [LK: CODE?] 2
Holzer, J. C., Goodman, W. K., McDougle, C. J., Baer, L., Boyarsky, B. K., Leckman, J. F. et al. 3 (1994). Obsessive-compulsive disorder with and without a chronic tic disorder. A comparison of symptoms 4 in 70 patients. Br.J.Psychiatry, 164, 469-473. [LK: CODE?] 5
Huppert, J. D. & Franklin, M. E. (2005). Cognitive Behavioral Therapy for Obsessive-compulsive 6 Disorder: An Update. Curr Psychiatry Rep, 7, 268-273. [F] 7
Hussain, M. Z. & Ahad, A. (1970). Treatment of obsessive-compulsive neurosis. Can Med Assoc 8 J, 103, 648. [G] 9
INOUYE, E. (1965). SIMILAR AND DISSIMILAR MANIFESTATIONS OF OBSESSIVE-10 COMPULSIVE NEUROSES IN MONOZYGOTIC TWINS. Am J Psychiatry, 121, 1171-1175. [G] 11
Insel, T. R., Hamilton, J. A., Guttmacher, L. B., & Murphy, D. L. (1983a). D-amphetamine in 12 obsessive-compulsive disorder. Psychopharmacology (Berl), 80, 231-235. [LK: CODE?] 13
Insel, T. R., Murphy, D. L., Cohen, R. M., Alterman, I., Kilts, C., & Linnoila, M. (1983b). 14 Obsessive-compulsive disorder. A double-blind trial of clomipramine and clorgyline. Arch.Gen.Psychiatry, 15 40, 605-612. [A] 16
Isaacs, K. L., Philbeck, J. W., Barr, W. B., Devinsky, O., & Alper, K. (2004). Obsessive-17 compulsive symptoms in patients with temporal lobe epilepsy. Epilepsy Behav., 5, 569-574. [LK: CODE?] 18
Jacobsen, F. M. (1995). Risperidone in the treatment of affective illness and obsessive-compulsive 19 disorder. J Clin Psychiatry, 56, 423-429. [LK: CODE?] 20
Jenike, M. A. & Baer, L. (1988). An open trial of buspirone in obsessive-compulsive disorder. 21 Am.J.Psychiatry, 145, 1285-1286. [B] 22
Jenike, M. A., Baer, L., Ballantine, T., Martuza, R. L., Tynes, S., Giriunas, I. et al. (1991). 23 Cingulotomy for refractory obsessive-compulsive disorder. A long-term follow-up of 33 patients. 24 Arch.Gen.Psychiatry, 48, 548-555. [C] 25
Jenike, M. A., Baer, L., & Greist, J. H. (1990a). Clomipramine versus fluoxetine in obsessive-26 compulsive disorder: a retrospective comparison of side effects and efficacy. J.Clin.Psychopharmacol., 10, 27 122-124. [E] 28
Jenike, M. A., Baer, L., Minichiello, W. E., Rauch, S. L., & Buttolph, M. L. (1997). Placebo-29 controlled trial of fluoxetine and phenelzine for obsessive-compulsive disorder. Am.J.Psychiatry, 154, 30 1261-1264. [A] 31
Jenike, M. A. & Brotman, A. W. (1984). The EEG in obsessive-compulsive disorder. J Clin 32 Psychiatry, 45, 122-124. [LK: CODE?] 33
Jenike, M. A., Buttolph, L., Baer, L., Ricciardi, J., & Holland, A. (1989). Open trial of fluoxetine 34 in obsessive-compulsive disorder. Am.J.Psychiatry, 146, 909-911. [B] 35
Jenike, M. A., Hyman, S., Baer, L., Holland, A., Minichiello, W. E., Buttolph, L. et al. (1990b). A 36 controlled trial of fluvoxamine in obsessive-compulsive disorder: implications for a serotonergic theory. 37 Am.J.Psychiatry, 147, 1209-1215. [A] 38

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
154
Jenike, M. A., Surman, O. S., Cassem, N. H., Zusky, P., & Anderson, W. H. (1983). Monoamine 1 oxidase inhibitors in obsessive-compulsive disorder. J.Clin.Psychiatry, 44, 131-132. [C] 2
Joffe, R. T. & Swinson, R. P. (1987a). Carbamazepine in obsessive-compulsive disorder. Biol 3 Psychiatry, 22, 1169-1171. [LK: CODE?] 4
Joffe, R. T. & Swinson, R. P. (1987b). Methylphenidate in primary obsessive-compulsive 5 disorder. J.Clin.Psychopharmacol., 7, 420-422. [LK: CODE?] 6
Joffe, R. T., Swinson, R. P., & Levitt, A. J. (1991). Acute psychostimulant challenge in primary 7 obsessive-compulsive disorder. J.Clin.Psychopharmacol., 11, 237-241. [LK: CODE?] 8
Jones, M. K. & Menzies, R. G. (1998). Danger ideation reduction therapy (DIRT) for obsessive-9 compulsive washers. A controlled trial. Behav.Res.Ther., 36, 959-970. [A-] 10
Jonnal, A. H., Gardner, C. O., Prescott, C. A., & Kendler, K. S. (2000). Obsessive and compulsive 11 symptoms in a general population sample of female twins. Am.J.Med.Genet., 96, 791-796. [GH: CODE?] 12
Kamijima, K., Murasaki, M., Asai, M., Higuchi, T., Nakajima, T., Taga, C. et al. (2004). 13 Paroxetine in the treatment of obsessive-compulsive disorder: randomized, double-blind, placebo-14 controlled study in Japanese patients. Psychiatry Clin.Neurosci., 58, 427-433. [A] 15
Kampman, M., Keijsers, G. P., Hoogduin, C. A., & Verbraak, M. J. (2002). Addition of cognitive-16 behaviour therapy for obsessive-compulsive disorder patients non-responding to fluoxetine. Acta 17 Psychiatr.Scand., 106, 314-319. [B] 18
Karno, M., Golding, J. M., Sorenson, S. B., & Burnam, M. A. (1988). The epidemiology of 19 obsessive-compulsive disorder in five US communities. Arch.Gen.Psychiatry, 45, 1094-1099. [LK: 20 CODE?] 21
Katz, R. J., DeVeaugh-Geiss, J., & Landau, P. (1990). Clomipramine in obsessive-compulsive 22 disorder. Biol.Psychiatry, 28, 401-414. [A] 23
Keck, P. E., Jr. & Arnold, L. M. (2000). The serotonin syndrome. Psychiatric Ann, 30, 333-343. 24 [LK: CODE?] 25
Keijsers, G. P., Hoogduin, C. A., & Schaap, C. P. (1994). Predictors of treatment outcome in the 26 behavioural treatment of obsessive-compulsive disorder. Br.J.Psychiatry, 165, 781-786. [LK: CODE?] 27
Kendler, K. S. & Diehl, S. R. (1993). The genetics of schizophrenia: a current, genetic-28 epidemiologic perspective. Schizophr.Bull, 19, 261-285. [F] 29
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005a). 30 Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity 31 Survey Replication. Arch Gen Psychiatry, 62, 593-602. [LK: CODE?] 32
Kessler, R. C., Chiu, W. T., Demler, O., Merikangas, K. R., & Walters, E. E. (2005b). Prevalence, 33 severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. 34 Arch Gen Psychiatry, 62, 617-627. [LK: CODE?] 35
Khoury, M. J., Beaty, T. H., & Cohen, B. H. (1993). Fundamentals of Genetic Epidemiology. New 36 York: Oxford University Press. [G] 37
Kim, C. H., Chang, J. W., Koo, M. S., Kim, J. W., Suh, H. S., Park, I. H. et al. (2003). Anterior 38 cingulotomy for refractory obsessive-compulsive disorder. Acta Psychiatr.Scand., 107, 283-290. [C] 39

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
155
Kirchheiner, J., Brosen, K., Dahl, M. L., Gram, L. F., Kasper, S., Roots, I. et al. (2001). CYP2D6 1 and CYP2C19 genotype-based dose recommendations for antidepressants: a first step towards 2 subpopulation-specific dosages. Acta Psychiatr Scand, 104, 173-192. [LK: CODE?] 3
Kirchheiner, J., Nickchen, K., Bauer, M., Wong, M. L., Licinio, J., Roots, I. et al. (2004). 4 Pharmacogenetics of antidepressants and antipsychotics: the contribution of allelic variations to the 5 phenotype of drug response. Mol.Psychiatry, 9, 442-473. [LK: CODE?] 6
Kobak, K. A., Taylor, L. V., Bystritsky, A., Kohlenberg, C. J., Greist, J. H., Tucker, P. et al. 7 (2005). St John's wort versus placebo in obsessive-compulsive disorder: results from a double-blind study. 8 Int Clin Psychopharmacol, 20, 299-304. [LK: CODE?] 9
Koch, H. J., Raschka, C., & Hannak, D. (2000). Pindolol can be effectively given once or twice 10 daily for augmentation in psychiatric patients. Eur Neuropsychopharmacol, 10, 511-512. [GH: CODE?] 11
Koponen, H., Lepola, U., Leinonen, E., Jokinen, R., Penttinen, J., & Turtonen, J. (1997). 12 Citalopram in the treatment of obsessive-compulsive disorder: an open pilot study. Acta Psychiatr.Scand., 13 96, 343-346. [B] 14
Koran, L. M. (1999). Obsessive-Compulsive and Related Disorders in Adults: A Comprehensive 15 Clinical Guide. Cambridge: Cambridge University Press. [G] 16
Koran, L. M. (2000). Quality of life in obsessive-compulsive disorder. Psychiatr.Clin.North Am., 17 23, 509-517. 18
Koran, L. M., Aboujaoude, E., Bullock, K. D., Franz, B., Gamel, N., & Elliott, M. (2005a). 19 Double-blind treatment with oral morphine in treatment-resistant obsessive-compulsive disorder. J Clin 20 Psychiatry, 66, 353-359. [LK: CODE?] 21
Koran, L. M., Aboujaoude, E., Ward, H., Shapira, N., Sallee, F. R., Gamel, N. et al. (2005b). 22 Pulse-loaded intravenous clomipramine in treatment-unresponsive obsessive-compulsive disorder. J Clin 23 Psychopharmacol, IN PRESS. [LK: CODE?] 24
Koran, L. M., Cain, J. W., Dominguez, R. A., Rush, A. J., & Thiemann, S. (1996a). Are fluoxetine 25 plasma levels related to outcome in obsessive-compulsive disorder? Am.J.Psychiatry, 153, 1450-1454. 26 [LK: CODE?] 27
Koran, L. M., Gamel, N. N., Choung, H. W., Smith, E. H., & Aboujaoude, E. N. (2005c). 28 Mirtazapine for obsessive-compulsive disorder: an open trial followed by double-blind discontinuation. J 29 Clin Psychiatry, 66, 515-520. [LK: CODE?] 30
Koran, L. M., Hackett, E., Rubin, A., Wolkow, R., & Robinson, D. (2002). Efficacy of sertraline 31 in the long-term treatment of obsessive-compulsive disorder. Am.J.Psychiatry, 159, 88-95. [A] 32
Koran, L. M., McElroy, S. L., Davidson, J. R., Rasmussen, S. A., Hollander, E., & Jenike, M. A. 33 (1996b). Fluvoxamine versus clomipramine for obsessive-compulsive disorder: a double-blind comparison. 34 J.Clin.Psychopharmacol., 16, 121-129. [A] 35
Koran, L. M., Mueller, K., & Maloney, A. (1996c). Will pindolol augment the response to a 36 serotonin reuptake inhibitor in obsessive-compulsive disorder? J Clin Psychopharmacol, 16, 253-254. 37 [GH: CODE?] 38
Koran, L. M., Pallanti, S., Paiva, R. S., & Quercioli, L. (1998). Pulse loading versus gradual 39 dosing of intravenous clomipramine in obsessive-compulsive disorder. Eur.Neuropsychopharmacol., 8, 40 121-126. [B] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
156
Koran, L. M., Quirk, T., Lorberbaum, J. P., & Elliott, M. (2001). Mirtazapine treatment of 1 obsessive-compulsive disorder. J.Clin.Psychopharmacol., 21, 537-539. [LK: CODE = B?] 2
Koran, L. M., Sallee, F. R., & Pallanti, S. (1997). Rapid benefit of intravenous pulse loading of 3 clomipramine in obsessive-compulsive disorder. Am.J.Psychiatry, 154, 396-401. [A] 4
Kotler, M., Iancu, I., Kindler, S., Lefkifker, E., & Zohar, J. (1994). Clomipramine-induced 5 tourettism in obsessive-compulsive disorder: clinical and theoretical implications. Clin Neuropharmacol., 6 17, 338-343. [LK: CODE?] 7
Kozak, M. J. & Foa, E. B. (1994). Obsessions, overvalued ideas, and delusions in obsessive-8 compulsive disorder. Behav.Res.Ther., 32, 343-353. [F] 9
Kozak, M. J. & Foa, E. B. (1997). Mastery of Obsessive-Compulsive Disorder: A Cognitive-10 Behavioral Approach. New York: Oxford University Press. [G] 11
Kronig, M. H., Apter, J., Asnis, G., Bystritsky, A., Curtis, G., Ferguson, J. et al. (1999). Placebo-12 controlled, multicenter study of sertraline treatment for obsessive-compulsive disorder. 13 J.Clin.Psychopharmacol., 19, 172-176. [A] 14
Kulin, N. A., Pastuszak, A., Sage, S. R., Schick-Boschetto, B., Spivey, G., Feldkamp, M. et al. 15 (1998). Pregnancy outcome following maternal use of the new selective serotonin reuptake inhibitors: a 16 prospective controlled multicenter study. JAMA, 279, 609-610. [LK: CODE?] 17
Kurlan, R. (2003). Tourette's syndrome: are stimulants safe? Curr Neurol Neurosci Rep, 3, 285-18 288. [LK: CODE?] 19
Labad, J., Menchon, J. M., Alonso, P., Segalas, C., Jimenez, S., & Vallejo, J. (2005). Female 20 reproductive cycle and obsessive-compulsive disorder. J Clin Psychiatry, 66, 428-435. [LK: CODE?] 21
LaSalle, V. H., Cromer, K. R., Nelson, K. N., Kazuba, D., Justement, L., & Murphy, D. L. (2004). 22 Diagnostic interview assessed neuropsychiatric disorder comorbidity in 334 individuals with obsessive-23 compulsive disorder. Depress.Anxiety., 19, 163-173. [LK: CODE?] 24
Lavin, M. R. & Halligan, P. (1996). ECT for comorbid obsessive-compulsive disorder and 25 schizophrenia. Am.J.Psychiatry, 153, 1652-1653. [D] 26
Leckman, J. F., Riddle, M. A., Hardin, M. T., Ort, S. I., Swartz, K. L., Stevenson, J. et al. (1989). 27 The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child 28 Adolesc Psychiatry, 28, 566-573. [LK: CODE?] 29
Leckman, J. F., Zhang, H., Alsobrook, J. P., & Pauls, D. L. (2001). Symptom dimensions in 30 obsessive-compulsive disorder: toward quantitative phenotypes. Am.J.Med.Genet., 105, 28-30. [LK: 31 CODE?] 32
Lelliott, P. & Marks, I. (1987). Management of obsessive-compulsive rituals associated with 33 delusions, hallucinations and depression. Behav Psychother, 15, 77-87. [LK: CODE?] 34
Lelliott, P. T., Noshirvani, H. F., Basoglu, M., Marks, I. M., & Monteiro, W. O. (1988). 35 Obsessive-compulsive beliefs and treatment outcome. Psychol.Med., 18, 697-702. [LK: CODE?] 36
Leo, R. J., Kuldip, J., & Bakhai, Y. D. (2005). Nonadherence with psychopharmacologic 37 treatment among psychiatric patients. Primary Psychiatry, 12, 33-39. [LK: CODE?] 38

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
157
Leon, A. C., Shear, M. K., Portera, L., & Klerman, G. L. (1992). Assessing impairment in patients 1 with panic disorder: the Sheehan Disability Scale. Soc Psychiatry Psychiatr Epidemiol, 27, 78-82. [LK: 2 CODE?] 3
Leonard, H. L. & Rapoport, J. L. (1987). Relief of obsessive-compulsive symptoms by LSD and 4 psilocin. Am J Psychiatry, 144, 1239-1240. [LK: CODE?] 5
Lepola, U., Bergtholdt, B., St Lambert, J., Davy, K. L., & Ruggiero, L. (2004). Controlled-release 6 paroxetine in the treatment of patients with social anxiety disorder. J Clin Psychiatry, 65, 222-229. [LK: 7 CODE?] 8
Levine, J. (1997). Controlled trials of inositol in psychiatry. Eur.Neuropsychopharmacol., 7, 147-9 155. [GN: CODE?] 10
Liebowitz, M. R., Hollander, E., Schneier, F., Campeas, R., Hatterer, J., Papp, L. et al. (1989). 11 Fluoxetine treatment of obsessive-compulsive disorder: an open clinical trial. J.Clin.Psychopharmacol., 9, 12 423-427. [GH: CODE?] 13
Liebowitz, M. R., Mangano, R. M., Bradwejn, J., & Asnis, G. (2005). A randomized controlled 14 trial of venlafaxine extended release in generalized social anxiety disorder. J Clin Psychiatry, 66, 238-247. 15 [LK: CODE?] 16
Lindsay, M., Crino, R., & Andrews, G. (1997). Controlled trial of exposure and response 17 prevention in obsessive-compulsive disorder. Br.J.Psychiatry, 171, 135-139. [A-] 18
Lopez-Ibor, J. J., Jr., Saiz, J., Cottraux, J., Note, I., Vinas, R., Bourgeois, M. et al. (1996). Double-19 blind comparison of fluoxetine versus clomipramine in the treatment of obsessive compulsive disorder. 20 Eur.Neuropsychopharmacol., 6, 111-118. [A] 21
Lundberg, S., Carlsson, A., Norfeldt, P., & Carlsson, M. L. (2004). Nicotine treatment of 22 obsessive-compulsive disorder. Prog.Neuropsychopharmacol Biol Psychiatry, 28, 1195-1199. [LK: 23 CODE?] 24
Lykouras, L., Alevizos, B., Michalopoulou, P., & Rabavilas, A. (2003). Obsessive-compulsive 25 symptoms induced by atypical antipsychotics. A review of the reported cases. 26 Prog.Neuropsychopharmacol.Biol.Psychiatry, 27, 333-346. [LK:CODE?] 27
Maina, G., Albert, U., Salvi, V., & Bogetto, F. (2004). Weight gain during long-term treatment of 28 obsessive-compulsive disorder: a prospective comparison between serotonin reuptake inhibitors. 29 J.Clin.Psychiatry, 65, 1365-1371. [LK: CODE?] 30
Maina, G., Albert, U., Ziero, S., & Bogetto, F. (2003). Antipsychotic augmentation for treatment 31 resistant obsessive-compulsive disorder: what if antipsychotic is discontinued? Int.Clin.Psychopharmacol., 32 18, 23-28. [G] 33
Maletzky, B., McFarland, B., & Burt, A. (1994). Refractory obsessive compulsive disorder and 34 ECT. Convuls.Ther., 10, 34-42. [F] 35
Mansueto, C. S. & Keuler, D. J. (2005). Tic or Compulsion?: It's Tourettic OCD. Behav Modif., 36 29, 784-799. [LK: CODE?] 37
Mantovani, A., Lisanby, S. H., Fulvio, P., Ulivelli, M., Castrogiovanni, P., & Rossi, S. (2005). 38 Repetitive transcranial magnetic stimulation (rTMS) in the treatment of obsessive-compulsive disorder 39 (OCD) and Tourette's syndrome (TS). Int J Neuropsychopharmacol, 1-6. [EH: CODE?] 40
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
158
Marazziti, D. (2003). Venlafaxine treatment of obsessive-compulsive disorder: case reports. 1 CNS.Spectr., 8, 421-422. [B] 2
Marazziti, D., Dell'Osso, L., Gemignani, A., Ciapparelli, A., Presta, S., Nasso, E. D. et al. (2001). 3 Citalopram in refractory obsessive-compulsive disorder: an open study. Int.Clin.Psychopharmacol., 16, 4 215-219. [B] 5
Marazziti, D., Gemignani, A., & Dell'Osso, L. (1999). Trazodone augmentation in OCD: a case 6 series report. CNS Spectr., 4, 48-49. [G] 7
March, J. S., Frances, A., Carpenter, D., & Kahn, D. A. (1997). The expert consensus guideline 8 series: treatment of obsessive-compulsive disorder. J Clin Psychiatry, 58 (suppl 4), 3-72. [LK: CODE?] 9
Marcy, T. R. & Britton, M. L. (2005). Antidepressant-induced sweating. Ann Pharmacother., 39, 10 748-752. [LK: CODE?] 11
Marks, I. M., Baer, L., Greist, J. H., Park, J. M., Bachofen, M., Nakagawa, A. et al. (1998). Home 12 self-assessment of obsessive-compulsive disorder. Use of a manual and a computer-conducted telephone 13 interview: two UK-US studies. Br.J.Psychiatry, 172, 406-412. [GN: CODE?] 14
Marks, I. M., Hodgson, R., & Rachman, S. (1975). Treatment of chronic obsessive-compulsive 15 neurosis by in-vivo exposure. A two-year follow-up and issues in treatment. Br.J.Psychiatry, 127, 349-364. 16 [BS: CODE?] 17
Marks, I. M., Lelliott, P., Basoglu, M., Noshirvani, H., Monteiro, W., Cohen, D. et al. (1988). 18 Clomipramine, self-exposure and therapist-aided exposure for obsessive-compulsive rituals. Br J 19 Psychiatry, 152, 522-534. [A-] 20
Marks, I. M., Stern, R. S., Mawson, D., Cobb, J., & McDonald, R. (1980). Clomipramine and 21 exposure for obsessive-compulsive rituals: I. Br.J.Psychiatry, 136, 1-25. [A-] 22
Mashour, G. A., Walker, E. E., & Martuza, R. L. (2005). Psychosurgery: past, present, and future. 23 Brain Res Brain Res Rev, 48, 409-419. [F] 24
Mataix-Cols, D., Rauch, S. L., Manzo, P. A., Jenike, M. A., & Baer, L. (1999). Use of factor-25 analyzed symptom dimensions to predict outcome with serotonin reuptake inhibitors and placebo in the 26 treatment of obsessive-compulsive disorder. Am.J.Psychiatry, 156, 1409-1416. [LK: CODE?] 27
Matsunaga, H., Kiriike, N., Miyata, A., Iwasaki, Y., Matsui, T., Fujimoto, K. et al. (1999). 28 Prevalence and symptomatology of comorbid obsessive-compulsive disorder among bulimic patients. 29 Psychiatry Clin.Neurosci., 53, 661-666. [LK: CODE?] 30
McCabe, B. J. (1986). Dietary tyramine and other pressor amines in MAOI regimens: a review. J 31 Am Diet.Assoc, 86, 1059-1064. [LK: CODE?] 32
McCullough, P. K. & Maltsberger, J. T. (2001). Obsessive-compulsive personality disorder. In G. 33 O. Gabbard (Ed.), Treatments of Psychiatric Disorders, Vol 2 (3rd ed., pp. 2341-2352). Washington, DC: 34 American Psychiatric Press. 35
McDougle, C. J., Barr, L. C., Goodman, W. K., Pelton, G. H., Aronson, S. C., Anand, A. et al. 36 (1995). Lack of efficacy of clozapine monotherapy in refractory obsessive-compulsive disorder. 37 Am.J.Psychiatry, 152, 1812-1814. [B] 38
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
159
McDougle, C. J., Epperson, C. N., Pelton, G. H., Wasylink, S., & Price, L. H. (2000). A double-1 blind, placebo-controlled study of risperidone addition in serotonin reuptake inhibitor-refractory obsessive-2 compulsive disorder. Arch.Gen.Psychiatry, 57, 794-801. [A] 3
McDougle, C. J., Goodman, W. K., Leckman, J. F., Barr, L. C., Heninger, G. R., & Price, L. H. 4 (1993a). The efficacy of fluvoxamine in obsessive-compulsive disorder: effects of comorbid chronic tic 5 disorder. J.Clin.Psychopharmacol., 13, 354-358. [B] 6
McDougle, C. J., Goodman, W. K., Leckman, J. F., Holzer, J. C., Barr, L. C., McCance-Katz, E. et 7 al. (1993b). Limited therapeutic effect of addition of buspirone in fluvoxamine-refractory obsessive-8 compulsive disorder. Am.J.Psychiatry, 150, 647-649. [LK: CODE?] 9
McDougle, C. J., Goodman, W. K., Leckman, J. F., Lee, N. C., Heninger, G. R., & Price, L. H. 10 (1994). Haloperidol addition in fluvoxamine-refractory obsessive-compulsive disorder. A double-blind, 11 placebo-controlled study in patients with and without tics. Arch.Gen.Psychiatry, 51, 302-308. [A] 12
McDougle, C. J., Price, L. H., Goodman, W. K., Charney, D. S., & Heninger, G. R. (1991). A 13 controlled trial of lithium augmentation in fluvoxamine-refractory obsessive-compulsive disorder: lack of 14 efficacy. J.Clin.Psychopharmacol., 11, 175-184. [A] 15
McElroy, S. L., Phillips, K. A., & Keck, P. E., Jr. (1994). Obsessive compulsive spectrum 16 disorder. J Clin Psychiatry, 55 Suppl, 33-51. [LK: CODE?] 17
McLean, P. D., Whittal, M. L., Thordarson, D. S., Taylor, S., Sochting, I., Koch, W. J. et al. 18 (2001). Cognitive versus behavior therapy in the group treatment of obsessive-compulsive disorder. 19 J.Consult Clin.Psychol., 69, 205-214. [A-] 20
Mehta, M. (1990). A comparative study of family-based and patient-based behavioural 21 management in obsessive-compulsive disorder. Br.J.Psychiatry, 157, 133-135. [A-] 22
Mell, L. K., Davis, R. L., & Owens, D. (2005). Association between streptococcal infection and 23 obsessive-compulsive disorder, Tourette's syndrome, and tic disorder. Pediatrics, 116, 56-60. [LK: 24 CODE?] 25
Mellman, L. A. & Gorman, J. M. (1984). Successful treatment of obsessive-compulsive disorder 26 with ECT. Am.J.Psychiatry, 141, 596-597. [D] 27
Meyer, V. (1966). Modification of expectations in cases with obsessional rituals. Behav Res Ther, 28 4, 273-280. [LK: CODE?] 29
Miguel, E. C., Shavitt, R. G., Ferrao, Y. A., Brotto, S. A., & Diniz, J. B. (2003). How to treat 30 OCD in patients with Tourette syndrome. J.Psychosom.Res., 55, 49-57. [LK: CODE?] 31
Millet, B., Chabane, N., Delorme, R., Leboyer, M., Leroy, S., Poirier, M. F. et al. (2003). 32 Association between the dopamine receptor D4 (DRD4) gene and obsessive-compulsive disorder. 33 Am.J.Med.Genet., 116B, 55-59. [GH: CODE?] 34
Moher, D., Schulz, K. F., & Altman, D. G. (2001). The CONSORT statement: revised 35 recommendations for improving the quality of reports of parallel-group randomised trials. Lancet, 357, 36 1191-1194. [LK: CODE?] 37
Montgomery, S. A. & Asberg, M. (1979). A new depression scale designed to be sensitive to 38 change. Br J Psychiatry, 134, 382-389. [LK: CODE?] 39

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
160
Montgomery, S. A., McIntyre, A., Osterheider, M., Sarteschi, P., Zitterl, W., Zohar, J. et al. 1 (1993). A double-blind, placebo-controlled study of fluoxetine in patients with DSM-III-R obsessive-2 compulsive disorder. The Lilly European OCD Study Group. Eur.Neuropsychopharmacol., 3, 143-152. [A] 3
Montoya, A., Weiss, A. P., Price, B. H., Cassem, E. H., Dougherty, D. D., Nierenberg, A. A. et al. 4 (2002). Magnetic resonance imaging-guided stereotactic limbic leukotomy for treatment of intractable 5 psychiatric disease. Neurosurgery, 50, 1043-1049. [C] 6
Moreno, F. A. & Delgado, P. L. (1997). Hallucinogen-induced relief of obsessions and 7 compulsions. Am J Psychiatry, 154, 1037-1038. [LK: CODE?] 8
Moses-Kolko, E. L., Bogen, D., Perel, J., Bregar, A., Uhl, K., Levin, B. et al. (2005). Neonatal 9 signs after late in utero exposure to serotonin reuptake inhibitors: literature review and implications for 10 clinical applications. JAMA, 293, 2372-2383. [LK: CODE?] 11
Mrazek, D. A. (2004). New tool: genotyping makes prescribing safer, more effective. Current 12 Psychiatry, 3, 11-23. [LK: CODE?] 13
Mundo, E., Bianchi, L., & Bellodi, L. (1997). Efficacy of fluvoxamine, paroxetine, and citalopram 14 in the treatment of obsessive-compulsive disorder: a single-blind study. J.Clin.Psychopharmacol., 17, 267-15 271. [LK: CODE?] 16
Mundo, E., Guglielmo, E., & Bellodi, L. (1998). Effect of adjuvant pindolol on the antiobsessional 17 response to fluvoxamine: a double-blind, placebo-controlled study. Int.Clin.Psychopharmacol., 13, 219-18 224. [A] 19
Mundo, E., Maina, G., & Uslenghi, C. (2000). Multicentre, double-blind, comparison of 20 fluvoxamine and clomipramine in the treatment of obsessive-compulsive disorder. 21 Int.Clin.Psychopharmacol., 15, 69-76. [A] 22
Mundo, E., Richter, M. A., Zai, G., Sam, F., McBride, J., Macciardi, F. et al. (2002). 5HT1Dbeta 23 Receptor gene implicated in the pathogenesis of Obsessive-Compulsive Disorder: further evidence from a 24 family-based association study. Mol.Psychiatry, 7, 805-809. 25
Mundo, E., Rouillon, F., Figuera, M. L., & Stigler, M. (2001). Fluvoxamine in obsessive-26 compulsive disorder: similar efficacy but superior tolerability in comparison with clomipramine. Hum 27 Psychopharmacol, 16, 461-468. [A] 28
Muris, P., Merckelbach, H., & Clavan, M. (1997). Abnormal and normal compulsions. Behav Res 29 Ther, 35, 249-252. [LK: CODE?] 30
Murphy, P. A., Kern, S. E., Stanczyk, F. Z., & Westhoff, C. L. (2005). Interaction of St. John's 31 Wort with oral contraceptives: effects on the pharmacokinetics of norethindrone and ethinyl estradiol, 32 ovarian activity and breakthrough bleeding. Contraception, 71, 402-408. [LK: CODE?] 33
Murphy, T. K., Sajid, M., Soto, O., Shapira, N., Edge, P., Yang, M. et al. (2004). Detecting 34 pediatric autoimmune neuropsychiatric disorders associated with streptococcus in children with obsessive-35 compulsive disorder and tics. Biol.Psychiatry, 55, 61-68. [LK: CODE?] 36
Murray, C. L. & Lopez, A. D. (1996). The Global Burden of Disease: A Comprehensive 37 Assessment of Mortality and Disability from Diseases, Injuries, and Risk in 1990 and Projected. 38 Cambridge, MA: Harvard University Press. [G] 39
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
161
National Institute for Health and Clinical Excellence (2005). Obsessive Compulsive Disorder: 1 core interventions in the treatment of obsessive compulsive disorder and body dysmorphic disorder [NICE 2 Guideline]. IN PRESS. [G] 3
Nestadt, G., Bienvenu, O. J., Cai, G., Samuels, J., & Eaton, W. W. (1998). Incidence of obsessive-4 compulsive disorder in adults. J.Nerv.Ment.Dis., 186, 401-406. [C] 5
Nestadt, G., Lan, T., Samuels, J., Riddle, M., Bienvenu, O. J., III, Liang, K. Y. et al. (2000a). 6 Complex segregation analysis provides compelling evidence for a major gene underlying obsessive-7 compulsive disorder and for heterogeneity by sex. Am.J.Hum.Genet., 67, 1611-1616. [D] 8
Nestadt, G., Samuels, J., Riddle, M., Bienvenu, O. J., III, Liang, K. Y., LaBuda, M. et al. (2000b). 9 A family study of obsessive-compulsive disorder. Arch.Gen.Psychiatry, 57, 358-363. [D] 10
Newport, D. J., Fisher, A., Graybeal, S., & Stowe, Z. N. (2004). Psychopharmacology during 11 pregnancy and lactation. In A. F. Schatzberg & C. B. Nemeroff (Eds.), American Psychiatric Association 12 Textbook of Psychopharmacology (pp. 1109-1149). Washington, DC: American Psychiatric Association. 13 [G] 14
Neziroglu, F., Anemone, R., & Yaryura-Tobias, J. A. (1992). Onset of obsessive-compulsive 15 disorder in pregnancy. Am J Psychiatry, 149, 947-950. [LK: CODE?] 16
Nicolini, H., Hanna, G. L., Baxter, L., Schwartz, J., Weissbecker, K., & Spence, M. (1991). 17 Segregation analysis of obsessive compulsive and associated disorders: preliminary results. Ursus Medicus, 18 1, 25-28. [GH: CODE?] 19
Nordeng, H. & Spigset, O. (2005). Treatment with selective serotonin reuptake inhibitors in the 20 third trimester of pregnancy: effects on the infant. Drug Saf, 28, 565-581. [LK: CODE?] 21
Nulman, I., Rovet, J., Stewart, D. E., Wolpin, J., Pace-Asciak, P., Shuhaiber, S. et al. (2002). 22 Child development following exposure to tricyclic antidepressants or fluoxetine throughout fetal life: a 23 prospective, controlled study. Am J Psychiatry, 159, 1889-1895. [LK: CODE?] 24
Nurnberg, H. G., Gelenberg, A., Hargreave, T. B., Harrison, W. M., Siegel, R. L., & Smith, M. D. 25 (2001). Efficacy of sildenafil citrate for the treatment of erectile dysfunction in men taking serotonin 26 reuptake inhibitors. Am J Psychiatry, 158, 1926-1928. [LK: CODE?] 27
Nuttin, B., Cosyns, P., Demeulemeester, H., Gybels, J., & Meyerson, B. (1999). Electrical 28 stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet, 29 354, 1526. [A] 30
Nuttin, B. J., Gabriels, L., van Kuyck, K., & Cosyns, P. (2003). Electrical stimulation of the 31 anterior limbs of the internal capsules in patients with severe obsessive-compulsive disorder: anecdotal 32 reports. Neurosurg.Clin.N.Am., 14, 267-274. [EH: CODE?] 33
O'Regan, J. B. (1970). Treatment of obsessive--compulsive neurosis with haloperidol. Can.Med 34 Assoc J, 103, 167-168. [LK: CODE?] 35
Oliver, B., Gascon, J., Aparicio, A., Ayats, E., Rodriguez, R., Maestro De Leon, J. L. et al. (2003). 36 Bilateral anterior capsulotomy for refractory obsessive-compulsive disorders. Stereotact.Funct.Neurosurg., 37 81, 90-95. [C] 38
Ozaki, N., Goldman, D., Kaye, W. H., Plotnicov, K., Greenberg, B. D., Lappalainen, J. et al. 39 (2003). Serotonin transporter missense mutation associated with a complex neuropsychiatric phenotype. 40 Mol.Psychiatry, 8, 895, 933-895, 936. [G] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
162
Pallanti, S., Hollander, E., Bienstock, C., Koran, L., Leckman, J., Marazziti, D. et al. (2002a). 1 Treatment non-response in OCD: methodological issues and operational definitions. Int J 2 Neuropsychopharmacol, 5, 181-191. [F] 3
Pallanti, S., Quercioli, L., & Koran, L. M. (2002b). Citalopram intravenous infusion in resistant 4 obsessive-compulsive disorder: an open trial. J.Clin.Psychiatry, 63, 796-801. [B] 5
Pallanti, S., Quercioli, L., Paiva, R. S., & Koran, L. M. (1999). Citalopram for treatment-resistant 6 obsessive-compulsive disorder. Eur.Psychiatry, 14, 101-106. [B] 7
Pato, M. T., Pigott, T. A., Hill, J. L., Grover, G. N., Bernstein, S., & Murphy, D. L. (1991). 8 Controlled comparison of buspirone and clomipramine in obsessive-compulsive disorder. Am.J.Psychiatry, 9 148, 127-129. [A] 10
Pato, M. T., Zohar-Kadouch, R., Zohar, J., & Murphy, D. L. (1988). Return of symptoms after 11 discontinuation of clomipramine in patients with obsessive-compulsive disorder. Am.J.Psychiatry, 145, 12 1521-1525. [A] 13
Pauls, D. L. & Alsobrook, J. P. (1999). The inheritance of obsessive-compulsive disorder. Child 14 Adolesc Psychiatr Clin N Am, 8, 481-96, viii. [GH: CODE=F?] 15
Pauls, D. L., Alsobrook, J. P., Goodman, W., Rasmussen, S., & Leckman, J. F. (1995). A family 16 study of obsessive-compulsive disorder. Am.J.Psychiatry, 152, 76-84. [GH: CODE?] 17
Perry, J. C. (1992). Problems and considerations in the valid assessment of personality disorders. 18 Am J Psychiatry, 149, 1645-1653. [LK: CODE?] 19
Perugi, G., Akiskal, H. S., Gemignani, A., Pfanner, C., Presta, S., Milanfranchi, A. et al. (1998). 20 Episodic course in obsessive-compulsive disorder. Eur.Arch.Psychiatry Clin.Neurosci., 248, 240-244. [LK: 21 CODE?] 22
Perugi, G., Toni, C., Frare, F., Travierso, M. C., Hantouche, E., & Akiskal, H. S. (2002). 23 Obsessive-compulsive-bipolar comorbidity: a systematic exploration of clinical features and treatment 24 outcome. J.Clin.Psychiatry, 63, 1129-1134. [LK: CODE?] 25
Physicians Medical Economics (2005). Physicians' Desk Reference. Montvale, NJ: Thomson 26 Healthcare. [G] 27
Piccinelli, M., Pini, S., Bellantuono, C., & Wilkinson, G. (1995). Efficacy of drug treatment in 28 obsessive-compulsive disorder. A meta-analytic review. Br.J.Psychiatry, 166, 424-443. [E] 29
Pierre, J. M. & Guze, B. H. (2000). Benztropine for venlafaxine-induced night sweats. J Clin 30 Psychopharmacol, 20, 269. [LK: CODE?] 31
Pigott, T. A., L'Heureux, F., Hill, J. L., Bihari, K., Bernstein, S. E., & Murphy, D. L. (1992a). A 32 double-blind study of adjuvant buspirone hydrochloride in clomipramine-treated patients with obsessive-33 compulsive disorder. J.Clin.Psychopharmacol., 12, 11-18. [A] 34
Pigott, T. A., L'Heureux, F., Rubenstein, C. S., Bernstein, S. E., Hill, J. L., & Murphy, D. L. 35 (1992b). A double-blind, placebo controlled study of trazodone in patients with obsessive-compulsive 36 disorder. J.Clin.Psychopharmacol., 12, 156-162. [A] 37
Pigott, T. A., Pato, M. T., Bernstein, S. E., Grover, G. N., Hill, J. L., Tolliver, T. J. et al. (1990). 38 Controlled comparisons of clomipramine and fluoxetine in the treatment of obsessive-compulsive disorder. 39 Behavioral and biological results. Arch.Gen.Psychiatry, 47, 926-932. [A] 40

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
163
Pigott, T. A., Pato, M. T., L'Heureux, F., Hill, J. L., Grover, G. N., Bernstein, S. E. et al. (1991). A 1 controlled comparison of adjuvant lithium carbonate or thyroid hormone in clomipramine-treated patients 2 with obsessive-compulsive disorder. J.Clin.Psychopharmacol., 11, 242-248. [A] 3
Poyurovsky, M., Weizman, A., & Weizman, R. (2004). Obsessive-compulsive disorder in 4 schizophrenia: clinical characteristics and treatment. CNS.Drugs, 18, 989-1010. [LK: CODE?] 5
Rasmussen, S., Hackett, E., DuBoff, E., Greist, J., Halaris, A., Koran, L. M. et al. (1997a). A 2-6 year study of sertraline in the treatment of obsessive-compulsive disorder. Int.Clin.Psychopharmacol., 12, 7 309-316. [B] 8
Rasmussen, S. A., Baer, L., Eisen, J., & Shera, D. (1997b). Previous SRI treatment and efficacy of 9 sertraline for OCD: combined analysis of 4 multicenter trials. Poster presented at the 150th Annual 10 Meeting of the American Psychiatric Association, San Diego, CA, May 17-22, 1997. [LK: CODE] 11
Rasmussen, S. A. & Eisen, J. L. (1988). Clinical and epidemiologic findings of significance to 12 neuropharmacologic trials in OCD. Psychopharmacol Bull, 24, 466-470. [LK: CODE?] 13
Rauch, S. L., O'Sullivan, R. L., & Jenike, M. A. (1996). Open treatment of obsessive-compulsive 14 disorder with venlafaxine: a series of ten cases. J.Clin.Psychopharmacol., 16, 81-84. [B] 15
Ravi Kishore, V., Samar, R., Janardhan Reddy, Y. C., Chandrasekhar, C. R., & Thennarasu, K. 16 (2004). Clinical characteristics and treatment response in poor and good insight obsessive-compulsive 17 disorder. Eur Psychiatry, 19, 202-208. [LK: CODE?] 18
Ravizza, L., Barzega, G., Bellino, S., Bogetto, F., & Maina, G. (1995). Predictors of drug 19 treatment response in obsessive-compulsive disorder. J.Clin.Psychiatry, 56, 368-373. [LK: CODE?] 20
Ravizza, L., Barzega, G., Bellino, S., Bogetto, F., & Maina, G. (1996a). Drug treatment of 21 obsessive-compulsive disorder (OCD): long-term trial with clomipramine and selective serotonin reuptake 22 inhibitors (SSRIs). Psychopharmacol.Bull., 32, 167-173. [LK: CODE?] 23
Ravizza, L., Barzega, G., Bellino, S., Bogetto, F., & Maina, G. (1996b). Therapeutic effect and 24 safety of adjunctive risperidone in refractory obsessive-compulsive disorder (OCD). 25 Psychopharmacol.Bull., 32, 677-682. [B] 26
Rayburn, N. R. & Otto, M. W. (2003). Cognitive-behavioral therapy for panic disorder: a review 27 of treatment elements, strategies, and outcomes. CNS Spectr., 8, 356-362. [LK: CODE?] 28
Richelson, E. (1997). Pharmacokinetic drug interactions of new antidepressants: a review of the 29 effects on the metabolism of other drugs. Mayo Clin.Proc., 72, 835-847. [LK: CODE?] 30
Richter, E. O., Davis, K. D., Hamani, C., Hutchison, W. D., Dostrovsky, J. O., & Lozano, A. M. 31 (2004). Cingulotomy for psychiatric disease: microelectrode guidance, a callosal reference system for 32 documenting lesion location, and clinical results. Neurosurgery, 54, 622-628. [G] 33
Rivers-Bulkeley, N. & Hollender, M. H. (1982). Successful treatment of obsessive-compulsive 34 disorder with loxapine. Am.J.Psychiatry, 139, 1345-1346. [LK: CODE?] 35
Romano, S., Goodman, W., Tamura, R., & Gonzales, J. (2001). Long-term treatment of obsessive-36 compulsive disorder after an acute response: a comparison of fluoxetine versus placebo. 37 J.Clin.Psychopharmacol., 21, 46-52. [A] 38
Roper, G., Rachman, S., & Marks, I. (1975). Passive and participant modelling in exposure 39 treatment of obsessive-compulsive neurotics. Behav Res Ther, 13, 271-279. [BS: CODE?] 40

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
164
Rosario-Campos, M. C., Leckman, J. F., Mercadante, M. T., Shavitt, R. G., Prado, H. S., Sada, P. 1 et al. (2001). Adults with early-onset obsessive-compulsive disorder. Am.J.Psychiatry, 158, 1899-1903. 2 [LK: CODE?] 3
Rothbaum, B. O. & Shahar, F. (2000). Behavioral treatment of obsessive-compulsive disorder in a 4 naturalistic setting. Cognitive and Behavioural Practice, 7, 262-270. [G] 5
Rothschild, A. J. (1995). Selective serotonin reuptake inhibitor-induced sexual dysfunction: 6 efficacy of a drug holiday. Am J Psychiatry, 152, 1514-1516. [LK: CODE? B?] 7
Rubinstein, C. S., Pigott, T. A., L'Heureux, F., Hill, J. H., & Murphy, D. L. (1992). A preliminary 8 investigation of the lifetime prevalence of anorexia and bulimia nervosa in patients with obsessive-9 compulsive disorder. J Clin Psychiatry, 53, 309-314. [LK: CODE?] 10
Ryan, N. D. (2005). Treatment of depression in children and adolescents. Lancet, 366, 933-940. 11 [G] 12
Sachdev, P. S., McBride, R., Loo, C. K., Mitchell, P. B., Malhi, G. S., & Croker, V. M. (2001). 13 Right versus left prefrontal transcranial magnetic stimulation for obsessive-compulsive disorder: a 14 preliminary investigation. J.Clin.Psychiatry, 62, 981-984. [B] 15
Salkovskis, P. M. (1985). Obsessional-compulsive problems: a cognitive-behavioural analysis. 16 Behav Res Ther, 23, 571-583. [BS: CODE?] 17
Salkovskis, P. M. (1996). Cognitive-behavioral approaches to the understanding of obsessional 18 problems. In R. M. Rapee (Ed.), Current Controversies in the Anxiety Disorders (pp. START PAGE?-END 19 PAGE?). New York: Guilford Press. [G] 20
Salkovskis, P. M. & Harrison, J. (1984). Abnormal and normal obsessions--a replication. Behav 21 Res Ther, 22, 549-552. [LK: CODE?] 22
Salkovskis, P. M. & Warwick, H. M. (1985). Cognitive therapy of obsessive-compulsive disorder: 23 treating treatment failures. Behav Psychother, 13, 243-255. [LK: CODE?] 24
Saxena, S., Brody, A. L., Maidment, K. M., Smith, E. C., Zohrabi, N., Katz, E. et al. (2004). 25 Cerebral glucose metabolism in obsessive-compulsive hoarding. Am J Psychiatry, 161, 1038-1048. [LK: 26 CODE?] 27
Saxena, S. & Maidment, K. M. (2004). Treatment of compulsive hoarding. J Clin Psychol, 60, 28 1143-1154. [LK: CODE?] 29
Saxena, S., Maidment, K. M., Vapnik, T., Golden, G., Rishwain, T., Rosen, R. M. et al. (2002). 30 Obsessive-compulsive hoarding: symptom severity and response to multimodal treatment. 31 J.Clin.Psychiatry, 63, 21-27. [LK: CODE?] 32
Schwartz, J. M. (1996). Brain Lock: Free Yourself From Obsessive-Compulsive Behavior. New 33 York: Harper Collins. [G] 34
Seedat, S. & Stein, D. J. (1999). Inositol augmentation of serotonin reuptake inhibitors in 35 treatment-refractory obsessive-compulsive disorder: an open trial. Int.Clin.Psychopharmacol., 14, 353-356. 36 [B] 37
Seidman, S. N., Pesce, V. C., & Roose, S. P. (2003). High-dose sildenafil citrate for selective 38 serotonin reuptake inhibitor-associated ejaculatory delay: open clinical trial. J Clin Psychiatry, 64, 721-39 725. [LK: CODE?] 40

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
165
Sevincok, L. & Topuz, A. (2003). Lack of efficacy of low doses of quetiapine addition in 1 refractory obsessive-compulsive disorder. J.Clin.Psychopharmacol., 23, 448-450. [BS: CODE?] 2
Sevincok, L. & Uygur, B. (2002). Venlafaxine open-label treatment of patients with obsessive-3 compulsive disorder. Aust.N.Z.J.Psychiatry, 36, 817. [B] 4
Shannahoff-Khalsa, D. S. (2004). An introduction to Kundalini yoga meditation techniques that 5 are specific for the treatment of psychiatric disorders. J Altern.Complement Med, 10, 91-101. [A] 6
Shapira, N. A., Keck, P. E., Jr., Goldsmith, T. D., McConville, B. J., Eis, M., & McElroy, S. L. 7 (1997). Open-label pilot study of tramadol hydrochloride in treatment-refractory obsessive-compulsive 8 disorder. Depress.Anxiety., 6, 170-173. [C] 9
Shapira, N. A., Ward, H. E., Mandoki, M., Murphy, T. K., Yang, M. C., Blier, P. et al. (2004). A 10 double-blind, placebo-controlled trial of olanzapine addition in fluoxetine-refractory obsessive-compulsive 11 disorder. Biol.Psychiatry, 55, 553-555. [A] 12
Sheehan, D. V., Harnett-Sheehan, K., & Raj, B. A. (1996). The measurement of disability. Int Clin 13 Psychopharmacol, 11 Suppl 3, 89-95. [LK: CODE?] 14
Simon, G. E., Cunningham, M. L., & Davis, R. L. (2002). Outcomes of prenatal antidepressant 15 exposure. Am J Psychiatry, 159, 2055-2061. [LK: CODE?] 16
Simpson, H. B., Franklin, M. E., Cheng, J., Foa, E. B., & Liebowitz, M. R. (2005a). Standard 17 criteria for relapse are needed in obsessive-compulsive disorder. Depress.Anxiety, 21, 1-8. [G] 18
Simpson, H. B., Gorfinkle, K. S., & Liebowitz, M. R. (1999). Cognitive-behavioral therapy as an 19 adjunct to serotonin reuptake inhibitors in obsessive-compulsive disorder: an open trial. J.Clin.Psychiatry, 20 60, 584-590. [B] 21
Simpson, H. B., Huppert, J. D., & Petkova, E. (2005b). Response versus remission in obsessive-22 compulsive disorder [ADDITIONAL AUTHORS NEEDED]. J Clin Psychiatry, IN PRESS. [CODE?] 23
Simpson, H. B., Liebowitz, M. R., Foa, E. B., Kozak, M. J., Schmidt, A. B., Rowan, V. et al. 24 (2004). Post-treatment effects of exposure therapy and clomipramine in obsessive-compulsive disorder. 25 Depress.Anxiety., 19, 225-233. [BS: CODE?] 26
Skevington, S. M., Bradshaw, J., & Saxena, S. (1999). Selecting national items for the WHOQOL: 27 conceptual and psychometric considerations. Soc Sci Med, 48, 473-487. [LK: CODE?] 28
Skoog, G. & Skoog, I. (1999). A 40-year follow-up of patients with obsessive-compulsive 29 disorder [see comments]. Arch.Gen.Psychiatry, 56, 121-127. [LK: CODE?] 30
Smeraldi, E., Erzegovesi, S., Bianchi, I., Pasquali, L., Gocchi, S., & Ronchi, P. (1992). 31 Fluvoxamine vs clomopramine treatment in obsessive-compulsive disorder: a preliminary study. New 32 Trends Exp Clin Psychiatry, 8, 63-65. [A-] 33
Snider, L. A. & Swedo, S. E. (2003). Childhood-onset obsessive-compulsive disorder and tic 34 disorders: case report and literature review. J.Child Adolesc.Psychopharmacol., 13 Suppl 1, S81-S88. [LK: 35 CODE?] 36
Sobin, C., Blundell, M. L., & Karayiorgou, M. (2000). Phenotypic differences in early- and late-37 onset obsessive-compulsive disorder. Compr.Psychiatry, 41, 373-379. [LK: CODE?] 38
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
166
Sporn, J., Smith, M., Jersino, J. M., Greenberg, B., Cora-Locatelli, G., & Murphy, D. (2001). A 1 double-blind, placebo-controlled trial of gabapentin (GBP) augmentation of fluoxetine for treatment of 2 obsessive-compulsive disorder (OCD). Poster presented at New Clinical Drug Evaluation Unit Program, 3 May 28-31, 2001; Phoenix, AZ. [LK: CODE?] 4
Stein, D. J., Hollander, E., Mullen, L. S., DeCaria, C. M., & Liebowitz, M. R. (1992). Comparison 5 of clomipramine, alprazolam, and placebo in the treatment of Obsessive-Compulsive Disorder. Hum 6 Psychopharmacol, 7, 389-395. [LK: CODE?] 7
Stein, D. J., Kasper, S., Andersen, E. W., Nil, R., & Lader, M. (2004). Escitalopram in the 8 treatment of social anxiety disorder: analysis of efficacy for different clinical subgroups and symptom 9 dimensions. Depress.Anxiety, 20, 175-181. [LK: CODE?] 10
Stein, D. J., Montgomery, S. A., Kasper, S., & Tanghoj, P. (2001). Predictors of response to 11 pharmacotherapy with citalopram in obsessive-compulsive disorder. Int.Clin.Psychopharmacol., 16, 357-12 361. [LK: CODE?] 13
Stein, M. B., Forde, D. R., Anderson, G., & Walker, J. R. (1997). Obsessive-compulsive disorder 14 in the community: an epidemiologic survey with clinical reappraisal. Am.J.Psychiatry, 154, 1120-1126. 15 [LK: CODE?] 16
Stein, M. B., Fyer, A. J., Davidson, J. R., Pollack, M. H., & Wiita, B. (1999). Fluvoxamine 17 treatment of social phobia (social anxiety disorder): a double-blind, placebo-controlled study. Am J 18 Psychiatry, 156, 756-760. [LK: CODE?] 19
Steketee, G., Chambless, D. L., & Tran, G. Q. (2001). Effects of axis I and II comorbidity on 20 behavior therapy outcome for obsessive-compulsive disorder and agoraphobia. Compr Psychiatry, 42, 76-21 86. [B] 22
Steketee, G. & Frost, R. (2003). Compulsive hoarding: current status of the research. 23 Clin.Psychol.Rev., 23, 905-927. [LK: CODE?] 24
Steketee, G., Henninger, N. H., & Pollard, C. A. (2000). Predicting treatment outcome of 25 obsessive-compulsive disorder: effects of comorbidity. In W. K. Goodman, M. V. Rudorfer, & J. D. Maser 26 (Eds.), Obsessive-Compulsive Disorder: Contemporary Issues in Treatment (pp. 257-274). Mahwah, NJ: 27 Lawrence Erlbaum Associates. [G] 28
Steketee, G. S. (1993). Treatment of Obsessive Compulsive Disorder. New York: Guilford Press. 29 [G] 30
Steketee, G. S. (1999). Overcoming Obsessive-Compulsive Disorder--Client Manual. Oakland, 31 CA: New Harbinger. [G] 32
Steketee, G. S. & Van Noppen, B. L. (1998). Group and family treatment for obsessive-33 compulsive disorder. In M. A. Jenike, L. Baer, & W. E. Minichiello (Eds.), Obsessive-Compulsive 34 Disorders: Practical Management (3rd ed., pp. 443-468). St. Louis: Mosby. [LK: CODE?] 35
Stewart, S. E., Stack, D. E., Farrell, C., Pauls, D. L., & Jenike, M. A. (2005). Effectiveness of 36 intensive residential treatment (IRT) for severe, refractory obsessive-compulsive disorder. J Psychiatr Res, 37 39, 603-609. [LK: CODE?] 38
Stowe, Z. N., Hostetter, A. L., Owens, M. J., Ritchie, J. C., Sternberg, K., Cohen, L. S. et al. 39 (2003). The pharmacokinetics of sertraline excretion into human breast milk: determinants of infant serum 40 concentrations. J Clin Psychiatry, 64, 73-80. [LK: CODE?] 41

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
167
Strassnig, M., Riedel, M., & Muller, N. (2004). Electroconvulsive therapy in a patient with 1 Tourette's syndrome and co-morbid Obsessive Compulsive Disorder. World J Biol Psychiatry, 5, 164-166. 2 [D] 3
Substance Abuse and Mental Health Services Administration (2005). SAMHSA releases revised 4 and updated treatment improvement protocol on co-occurring disorders. Psychiatr Serv, 56, 371. [G] 5
Sweet, R. A., Brown, E. J., Heimberg, R. G., Ciafre, L., Scanga, D. M., Cornelius, J. R. et al. 6 (1995). Monoamine oxidase inhibitor dietary restrictions: what are we asking patients to give up? J Clin 7 Psychiatry, 56, 196-201. [LK: CODE?] 8
Szegedi, A., Wetzel, H., Leal, M., Hartter, S., & Hiemke, C. (1996). Combination treatment with 9 clomipramine and fluvoxamine: drug monitoring, safety, and tolerability data. J.Clin.Psychiatry, 57, 257-10 264. [C] 11
Tamam, L. & Ozpoyraz, N. (2002). Selective serotonin reuptake inhibitor discontinuation 12 syndrome: a review. Adv.Ther., 19, 17-26. [LK: CODE?] 13
Tamminga, C. A. (2003). Similarities and differences among antipsychotics. J Clin Psychiatry, 64 14 Suppl 17, 7-10. [F] 15
Taylor, L. H. & Kobak, K. A. (2000). An open-label trial of St. John's Wort (Hypericum 16 perforatum) in obsessive-compulsive disorder. J.Clin.Psychiatry, 61, 575-578. [LK: CODE?] 17
Taylor, S. (2000). Understanding and Treating Panic Disorder: Cognitive-Behavioural 18 Approaches. New York: Wiley. [G] 19
Tenneij, N. H., van Megen, H. J., Denys, D. A., & Westenberg, H. G. (2005). Behavior therapy 20 augments response of patients with obssesive-compulsive disorder responding to drug treatment. J Clin 21 Psychiatry, 66, 1169-1175. [A-] 22
Tesei, S., Antonini, A., Canesi, M., Zecchinelli, A., Mariani, C. B., & Pezzoli, G. (2000). 23 Tolerability of paroxetine in Parkinson's disease: a prospective study. Mov Disord, 15, 986-989. [LK: 24 CODE?] 25
The Clomipramine Collaborative Study Group (1991). Clomipramine in the treatment of patients 26 with obsessive-compulsive disorder. Arch.Gen.Psychiatry, 48, 730-738. [A] 27
Thiel, A., Broocks, A., Ohlmeier, M., Jacoby, G. E., & Schussler, G. (1995). Obsessive-28 compulsive disorder among patients with anorexia nervosa and bulimia nervosa. Am.J.Psychiatry, 152, 72-29 75. [LK: CODE?] 30
Thomas, S. G. & Kellner, C. H. (2003). Remission of major depression and obsessive-compulsive 31 disorder after a single unilateral ECT. J ECT, 19, 50-51. [D] 32
Thoren, P., Asberg, M., Cronholm, B., Jornestedt, L., & Traskman, L. (1980). Clomipramine 33 treatment of obsessive-compulsive disorder. I. A controlled clinical trial. Arch.Gen.Psychiatry, 37, 1281-34 1285. [A] 35
Tolin, D. F., Maltby, N., Diefenbach, G. J., Hannan, S. E., & Worhunsky, P. (2004). Cognitive-36 behavioral therapy for medication nonresponders with obsessive-compulsive disorder: a wait-list-controlled 37 open trial. J.Clin.Psychiatry, 65, 922-931. [B] 38
Tollefson, G. D., Birkett, M., Koran, L., & Genduso, L. (1994a). Continuation treatment of OCD: 39 double-blind and open-label experience with fluoxetine. J.Clin.Psychiatry, 55 Suppl, 69-76. [GH: CODE?] 40
OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
168
Tollefson, G. D., Rampey, A. H., Jr., Potvin, J. H., Jenike, M. A., Rush, A. J., kominguez, R. A. et 1 al. (1994b). A multicenter investigation of fixed-dose fluoxetine in the treatment of obsessive-compulsive 2 disorder. Arch.Gen.Psychiatry, 51, 559-567. [A] 3
TRETHOWAN, W. H. & SCOTT, P. A. (1955). Chlorpromazine in obsessive-compulsive and 4 allied disorders. Lancet, 268, 781-785. [B] 5
Trimble, M. R. (1990). Worldwide use of clomipramine. J Clin Psychiatry, 51 Suppl, 51-54. [F] 6
Trivedi, M. H., Rush, A. J., Ibrahim, H. M., Carmody, T. J., Biggs, M. M., Suppes, T. et al. 7 (2004). The Inventory of Depressive Symptomatology, Clinician Rating (IDS-C) and Self-Report (IDS-8 SR), and the Quick Inventory of Depressive Symptomatology, Clinician Rating (QIDS-C) and Self-Report 9 (QIDS-SR) in public sector patients with mood disorders: a psychometric evaluation. Psychol Med, 34, 73-10 82. [LK: CODE?] 11
Tukel, R., Ertekin, E., Batmaz, S., Alyanak, F., Sozen, A., Aslantas, B. et al. (2005). Influence of 12 age of onset on clinical features in obsessive-compulsive disorder. Depress.Anxiety, 21, 112-117. [LK: 13 CODE?] 14
Turner, S. M., Jacob, R. G., Beidel, D. C., & Himmelhoch, J. (1985). Fluoxetine treatment of 15 obsessive-compulsive disorder. J.Clin.Psychopharmacol., 5, 207-212. [GH: CODE?] 16
VA/DoD Evidence-Based Clinical Practice Guideline Working Group (2001). Management of 17 Substance Use Disorder in the Primary Care Setting. Washington, DC: VA/DoD Evidence-Based Clinical 18 Practice Guideline Working Group, Veterans Health Administration, Department of Veterans Affairs and 19 Health Affairs, Department of Defense, September 2001. Office of Quality and Performance publication 20 10Q-CPG/SUD-01. [G] 21
Vajda, F. J. & Solinas, C. (2005). Current approaches to management of depression in Parkinson's 22 Disease. J Clin Neurosci. [LK: CODE?] 23
Vallejo, J., Olivares, J., Marcos, T., Bulbena, A., & Menchon, J. M. (1992). Clomipramine versus 24 phenelzine in obsessive-compulsive disorder. A controlled clinical trial. Br.J.Psychiatry, 161, 665-670. [A] 25
Van Ameringen, M., Mancini, C., Patterson, B., & Bennett, M. (2005). Topiramate augmentation 26 in treatment-resistant obsessive-compulsive disorder: a retrospective, open-label case series. 27 Depress.Anxiety. [LK: CODE?] 28
van Ameringen, M. A., Lane, R. M., Walker, J. R., Bowen, R. C., Chokka, P. R., Goldner, E. M. 29 et al. (2001). Sertraline treatment of generalized social phobia: a 20-week, double-blind, placebo-controlled 30 study. Am J Psychiatry, 158, 275-281. [LK: CODE?] 31
van Balkom, A. J., de Haan, E., van Oppen, P., Spinhoven, P., Hoogduin, K. A., & van Dyck, R. 32 (1998). Cognitive and behavioral therapies alone versus in combination with fluvoxamine in the treatment 33 of obsessive compulsive disorder. J.Nerv.Ment.Dis., 186, 492-499. [A-] 34
Van Noppen, B., Steketee, G., McCorkle, B. H., & Pato, M. (1997). Group and multifamily 35 behavioral treatment for obsessive compulsive disorder: a pilot study. J.Anxiety.Disord., 11, 431-446. [GN: 36 CODE = B?] 37
van Oppen, P. & Arntz, A. (1994). Cognitive therapy for obsessive-compulsive disorder. 38 Behav.Res.Ther., 32, 79-87. [LK: CODE?] 39

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
169
van Oppen, P., de Haan, E., van Balkom, A. J., Spinhoven, P., Hoogduin, K., & van Dyck, R. 1 (1995). Cognitive therapy and exposure in vivo in the treatment of obsessive compulsive disorder. 2 Behav.Res.Ther., 33, 379-390. [A-] 3
Veenstra-VanderWeele, J., Kim, S. J., Gonen, D., Hanna, G. L., Leventhal, B. L., & Cook, E. H., 4 Jr. (2001). Genomic organization of the SLC1A1/EAAC1 gene and mutation screening in early-onset 5 obsessive-compulsive disorder. Mol.Psychiatry, 6, 160-167. [GH: CODE?] 6
Vogel, P. A., Stiles, T. C., & Gotestam, K. G. (2004). Adding cognitive therapy elements to 7 exposure therapy for obsessive compulsive disorder: a controlled study. Behavioural & Cognitive 8 Psychotherapy, 32, 275-290. [A-] 9
Voruganti, L., Cortese, L., Oyewumi, L., Cernovsky, Z., Zirul, S., & Awad, A. (2000). 10 Comparative evaluation of conventional and novel antipsychotic drugs with reference to their subjective 11 tolerability, side-effect profile and impact on quality of life. Schizophr.Res, 43, 135-145. [B] 12
Vulink, N. C., Denys, D., & Westenberg, H. G. (2005). Bupropion for patients with obsessive-13 compulsive disorder: an open-label, fixed-dose study. J Clin Psychiatry, 66, 228-230. [B] 14
Wanger, K. D. (2005). Pharmacotherapy for major depression in children and adolescents. Prog 15 Neuropsychopharmacol Biol Psychiatry, 29, 819-826. [GH: CODE?] 16
Warneke, L. (1997). A possible new treatment approach to obsessive-compulsive disorder. Can J 17 Psychiatry, 42, 667-668. [LK: CODE?] 18
Warren, R. & Thomas, J. C. (2001). Cognitive-behavior therapy of obsessive-compulsive disorder 19 in private practice: an effectiveness study. J.Anxiety.Disord., 15, 277-285. [G] 20
Weinrieb, R. M., Auriacombe, M., Lynch, K. G., & Lewis, J. D. (2005). Selective serotonin re-21 uptake inhibitors and the risk of bleeding. Expert Opin Drug Saf, 4, 337-344. [LK: CODE?] 22
Weiss, A. P. & Jenike, M. A. (2000). Late-onset obsessive-compulsive disorder: a case series. 23 J.Neuropsychiatry Clin.Neurosci., 12, 265-268. [LK: CODE?] 24
Weissman, A. M., Levy, B. T., Hartz, A. J., Bentler, S., Donohue, M., Ellingrod, V. L. et al. 25 (2004). Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants. Am J 26 Psychiatry, 161, 1066-1078. [LK: CODE?] 27
Weissman, M. M., Bland, R. C., Canino, G. J., Greenwald, S., Hwu, H. G., Lee, C. K. et al. 28 (1994). The cross national epidemiology of obsessive compulsive disorder. The Cross National 29 Collaborative Group. J.Clin.Psychiatry, 55 Suppl, 5-10. [LK: CODE?] 30
Whittal, M. L., Thordarson, D. S., & McLean, P. D. (2005). Treatment of obsessive-compulsive 31 disorder: Cognitive behavior therapy vs. exposure and response prevention. Behav Res Ther. [A-] 32
Wilhelm, S. & Steketee, G. (2006). Cognitive Therapy of Obsessive-Compulsive Disorder: A 33 Guide for Professionals. IN PRESS. [G] 34
Wilhelm, S., Steketee, G., Reilly-Harrington, N. A., Deckersbach, T., Buhlmann, U., & Baer, L. 35 (2005). Effectiveness of cognitive therapy for obsessive-compulsive disorder: an open trial. J Cog 36 Psychother, 19, 173-179. [B] 37
Williams, K. E. & Koran, L. M. (1997). Obsessive-compulsive disorder in pregnancy, the 38 puerperium, and the premenstruum. J.Clin.Psychiatry, 58, 330-334. [LK: CODE?] 39

OCD Practice Guideline Not for Distribution or Citation Draft 2, December 6, 2005
170
Willour, V. L., Yao, S. Y., Samuels, J., Grados, M., Cullen, B., Bienvenu, O. J., III et al. (2004). 1 Replication study supports evidence for linkage to 9p24 in obsessive-compulsive disorder. 2 Am.J.Hum.Genet., 75, 508-513. [GH: CODE?] 3
Winsberg, M. E., Cassic, K. S., & Koran, L. M. (1999). Hoarding in obsessive-compulsive 4 disorder: a report of 20 cases. J.Clin.Psychiatry, 60, 591-597. [LK: CODE?] 5
Wisner, K. L., Zarin, D. A., Holmboe, E. S., Appelbaum, P. S., Gelenberg, A. J., Leonard, H. L. et 6 al. (2000). Risk-benefit decision making for treatment of depression during pregnancy. Am J Psychiatry, 7 157, 1933-1940. [LK: CODE?] 8
Worthington, J. J., III, Simon, N. M., Korbly, N. B., Perlis, R. H., & Pollack, M. H. (2002). 9 Ropinirole for antidepressant-induced sexual dysfunction. Int Clin Psychopharmacol, 17, 307-310. [LK: 10 CODE?] 11
Yaryura-Tobias, J. A. (1981). Clinical observations on L-tryptophan in the treatment of obsessive-12 compulsive disorders. Biol Psychiatry, 16, 622-625. [LK: CODE?] 13
Yaryura-Tobias, J. A. & Bhagavan, H. N. (1977). L-tryptophan in obsessive-compulsive disorders. 14 Am J Psychiatry, 134, 1298-1299. [LK: CODE?] 15
Yaryura-Tobias, J. A. & Neziroglu, F. A. (1996). Venlafaxine in obsessive-compulsive disorder. 16 Arch.Gen.Psychiatry, 53, 653-654. [A] 17
Zai, G., Bezchlibnyk, Y. B., Richter, M. A., Arnold, P., Burroughs, E., Barr, C. L. et al. (2004). 18 Myelin oligodendrocyte glycoprotein (MOG) gene is associated with obsessive-compulsive disorder. Am J 19 Med Genet B Neuropsychiatr.Genet, 129, 64-68. [D] 20
Zajecka, J. (2001). Strategies for the treatment of antidepressant-related sexual dysfunction. J Clin 21 Psychiatry, 62 Suppl 3, 35-43. [LK: CODE?] 22
Zajecka, J., Tracy, K. A., & Mitchell, S. (1997). Discontinuation symptoms after treatment with 23 serotonin reuptake inhibitors: a literature review. J Clin Psychiatry, 58, 291-297. [LK: CODE?] 24
Zhang, H., Leckman, J. F., Pauls, D. L., Tsai, C. P., Kidd, K. K., & Campos, M. R. (2002). 25 Genomewide scan of hoarding in sib pairs in which both sibs have Gilles de la Tourette syndrome. Am J 26 Hum Genet, 70, 896-904. [LK: CODE?] 27
Zohar, J. & Judge, R. (1996). Paroxetine versus clomipramine in the treatment of obsessive-28 compulsive disorder. OCD Paroxetine Study Investigators. Br.J.Psychiatry, 169, 468-474. [A] 29
Zung, W. W. (1968). Evaluating treatment methods for depressive disorders. Am J Psychiatry, 30 124, Suppl-8. [LK: CODE?] 31
32
Related Documents











