23 Obstetric Trauma D. G. Evans and C. B-Lynch ACUTE UTERINE INVERSION Acute uterine inversion, defined as when the uterus is turned inside out, is a rare but serious complication of the third stage of labor. The estimated incidence is approximately 1 in 20–25 000 deliveries 1–3 . As the estimate of a later report was <1 : 2000 4 , the true incidence is unclear because some of the milder forms correct themselves spontaneously and are thus not recognized or reported. Classification Uterine inversion may be complete or incomplete, depending on whether the fundus has passed through the cervix 5 . When the uterine inversion occurs within the first 24 h post-delivery, it is classified as acute. In- version occurring after the first 24 h and up to 4 weeks postpartum is classified as sub-acute, and the rare chronic inversion occurs after the 4th week postpartum. Etiology The expulsion of the placenta was probably intended by Nature to occur as a result of gravitational forces, with the mother in the same squatting position that is often adopted for defecation. When the third stage is conducted in the dorsal position, however, help may be necessary for placental expulsion. Accordingly, the inappropriate management of the third stage of labor is often implicated in the etiology of acute uterine inver- sion. Indeed, Crede’s method of placental delivery with uncontrolled cord traction, referred to in most textbooks of midwifery and older textbooks of obstet- rics, may indeed increase the risk of acute uterine inversion. The firmly contracted uterus is used as a piston to push the placenta out, in the same manner that a piston is used to push fluid out of the barrel of a syringe. Pressure is applied with the palm of the hand in the axis of the pelvic inlet, in a downward and backward direction with the aim of forcing the pla- centa out through the lower genital tract. Unfortu- nately, application of Crede’s maneuver when the uterus is not contracted may well facilitate acute in- version. On the other hand, the Brandt Andrews maneuver, also mentioned in standard textbooks of midwifery and obstetrics, a modification of Aristotle’s method of delivering the placenta by cord traction, recommends applying tension, but not traction, to the umbilical cord with one hand, whilst the other hand is placed on the abdomen gently moving the uterus upwards and backwards. Today, controlled cord trac- tion is standard practice for the third stage of labor. Other etiological factors include forcibly attempt- ing to expel the placenta by using fundal pressure when the uterus is atonic, and traction on the umbili- cal cord in a fundally placed placenta when the uterus is relaxed. It may also be brought about by a local atony, more particularly of the fundal placental site together with active contractions of the rest of the uterus. Other etiological factors include macrosomia, polyhydramnios, multiple pregnancy, primiparity and oxytocin administration 5 . In other instances, however, the inversion occurs spontaneously from sudden increased abdominal pressure as a result of coughing, sneezing or straining. Chronic inversion may result from an acute inver- sion left unrecognized or from a sub-mucous fibroid which has prolapsed through the cervix. A placental polyp resulting from a retained cotyledon of the placenta may present in the same fashion. Diagnosis Symptoms are acute and pronounced. Generally, the mother is aware of something coming down and this is usually quickly followed by unanticipated profound shock. The uterus may appear at the introitus outside the vagina and the fundus is no longer palpable abdominally. In partial inversion, the fundus of the uterus may be indented and may or may not pass through the cervical os. In such instances, it is neither palpable abdominally nor visible at the vulva. Vaginal examination detects the inverted body of the uterus, and, above and encircling it, the ring of the cervix. In all instances, pain may be severe due to stretching of the infundibulo-pelvic ligaments and other viscera. Shock is the outstanding sign, and may in part be neurogenic due to stretching of the viscera and in part due to hemorrhage and hypovolemia. The degree of shock is proportional to blood loss and hemorrhage is variable, depending on whether any attempt has been made to remove the placenta. Some bleeding will always be present unless the placenta is completely adherent to the uterine wall. It is important to 185

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

23Obstetric TraumaD. G. Evans and C. B-Lynch
ACUTE UTERINE INVERSION
Acute uterine inversion, defined as when the uterus isturned inside out, is a rare but serious complication ofthe third stage of labor. The estimated incidence isapproximately 1 in 20–25 000 deliveries1–3. As theestimate of a later report was <1 : 20004, the trueincidence is unclear because some of the milder formscorrect themselves spontaneously and are thus notrecognized or reported.
Classification
Uterine inversion may be complete or incomplete,depending on whether the fundus has passed throughthe cervix5. When the uterine inversion occurs withinthe first 24 h post-delivery, it is classified as acute. In-version occurring after the first 24 h and up to 4 weekspostpartum is classified as sub-acute, and the rarechronic inversion occurs after the 4th week postpartum.
Etiology
The expulsion of the placenta was probably intendedby Nature to occur as a result of gravitational forces,with the mother in the same squatting position that isoften adopted for defecation. When the third stage isconducted in the dorsal position, however, help maybe necessary for placental expulsion. Accordingly, theinappropriate management of the third stage of labor isoften implicated in the etiology of acute uterine inver-sion. Indeed, Crede’s method of placental deliverywith uncontrolled cord traction, referred to in mosttextbooks of midwifery and older textbooks of obstet-rics, may indeed increase the risk of acute uterineinversion. The firmly contracted uterus is used as apiston to push the placenta out, in the same mannerthat a piston is used to push fluid out of the barrel of asyringe. Pressure is applied with the palm of the handin the axis of the pelvic inlet, in a downward andbackward direction with the aim of forcing the pla-centa out through the lower genital tract. Unfortu-nately, application of Crede’s maneuver when theuterus is not contracted may well facilitate acute in-version. On the other hand, the Brandt Andrewsmaneuver, also mentioned in standard textbooks ofmidwifery and obstetrics, a modification of Aristotle’smethod of delivering the placenta by cord traction,
recommends applying tension, but not traction, to theumbilical cord with one hand, whilst the other hand isplaced on the abdomen gently moving the uterusupwards and backwards. Today, controlled cord trac-tion is standard practice for the third stage of labor.
Other etiological factors include forcibly attempt-ing to expel the placenta by using fundal pressurewhen the uterus is atonic, and traction on the umbili-cal cord in a fundally placed placenta when the uterusis relaxed. It may also be brought about by a localatony, more particularly of the fundal placental sitetogether with active contractions of the rest of theuterus. Other etiological factors include macrosomia,polyhydramnios, multiple pregnancy, primiparity andoxytocin administration5. In other instances, however,the inversion occurs spontaneously from suddenincreased abdominal pressure as a result of coughing,sneezing or straining.
Chronic inversion may result from an acute inver-sion left unrecognized or from a sub-mucous fibroidwhich has prolapsed through the cervix. A placentalpolyp resulting from a retained cotyledon of theplacenta may present in the same fashion.
Diagnosis
Symptoms are acute and pronounced. Generally, themother is aware of something coming down and this isusually quickly followed by unanticipated profoundshock. The uterus may appear at the introitus outsidethe vagina and the fundus is no longer palpableabdominally. In partial inversion, the fundus of theuterus may be indented and may or may not passthrough the cervical os. In such instances, it is neitherpalpable abdominally nor visible at the vulva. Vaginalexamination detects the inverted body of the uterus,and, above and encircling it, the ring of the cervix. Inall instances, pain may be severe due to stretching ofthe infundibulo-pelvic ligaments and other viscera.
Shock is the outstanding sign, and may in part beneurogenic due to stretching of the viscera and in partdue to hemorrhage and hypovolemia. The degree ofshock is proportional to blood loss and hemorrhage isvariable, depending on whether any attempt has beenmade to remove the placenta. Some bleeding willalways be present unless the placenta is completelyadherent to the uterine wall. It is important to
185

recognize that severe hemorrhage will accompany anyattempt at removing the placenta before the uterus isreplaced5,6. This eventuality is a special risk if the birthhas been attended by a traditional birth attendant(TBA) in parts of the underdeveloped world.
Management
Acute uterine inversion is a true obstetric emergency6,and clearly one which may lead to severe postpartumhemorrhage. If present and available, a supportiveteam should be summoned to the delivery suite forresuscitation and protocol management. Uterotonics,if started, are to be stopped and manual replacementattempted under adequate and appropriate anesthesiafollowed by delivery of the placenta assisted by restartof oxytocin7.
Elevation of the foot of the delivery table or bedmay relieve the tension on the viscera and reduce thepain and shock. Immediate resuscitation with intra-venous fluids is indicated via large-gauge venousaccess. Adequate analgesia must be instituted prior toattempting replacement, and the bladder should becatheterized. Antibiotic prophylaxis is advisable.
Any delay increases the difficulty in replacing theuterus, and the first health-care professional presentshould make the initial attempt at replacement. Thiswill be aided if regional anesthetic is already in place8.The placenta should be left in situ and no attempt madeto remove it. The portion of the uterus that came downlast should go back first, that is, the lower segment ini-tially and the fundus later. The hand is lubricated withhibitane cream (or other suitable antiseptic if available)and placed inside the vagina. With gentle maneuvers ofthe fingers around the cervical rim and simultaneousupward pressure with the palm of the hand, the uterus isgradually replaced. The employment of force is danger-ous, as the thinned-out lower segment may be torn orotherwise traumatized. The vaginal vault may alreadyhave been torn in some cases. The degree of shock doesnot diminish until the uterus is replaced. In the majorityof instances, replacement of the uterus is successfulusing this conservative method9. If replacement issuccessful, the placenta should be manually removedwith the aid of ergometrine or an oxytocic infusion. Inunderdeveloped countries or in a home setting, boiledwater brought to a bearable temperature can be used tosoak clean towels or cloths to assist in pushing and pack-ing the vagina. This may facilitate replacement attemptsand control further blood loss. Bimanual massage of thefundus may improve contraction.
If replacement is unsuccessful, measures to relax thecervical retraction ring should be the next line oftherapy. Beta mimetics or amyl nitrite inhalation canoften relax the retraction ring sufficiently to allowuterine replacement9. A similar effect is seen with theadministration of halothane anesthesia, but, unfortu-nately, use of this agent in sufficient doses can result inthe unwanted and life-threatening complications ofuterine atony, hypotension and severe hemorrhage.
Halothane is no longer used for these and other reasons.A 2 g intravenous bolus of magnesium sulfate can beused in the hypotensive patient (0.25 mg of intravenousterbutaline in the stable patient) to relax the cervicalcontraction ring10. Intravenous nitroglycerine can betried although it is not commonly used.
Further attempts at replacement of the uterusshould take place under general anesthesia in an oper-ating theater equipped and ready to perform a laparo-tomy. Before resorting to a laparotomy, however, thetried and tested O’Sullivan hydrostatic technique11
should be attempted. Here, the patient is first resusci-tated to restore vital signs including adequate bloodvolume and pressure. The obstetric team and anesthe-tist are summoned.
Adequate analgesia is essential before:
(1) Attempt at repositioning without the use of uter-ine relaxant;
(2) If response is not imminent or sustained, an anes-thetist should provide uterine relaxation to facili-tate repositioning and the administration ofuterotonics;
(3) General anesthesia is preferable, administered byan obstetric anesthetist. Digital repositioningshould be maintained to support and establishgood uterine muscle tone;
(4) 1–2 liters of saline at body temperature should beinfused into the vagina through rubber tubesplaced in the posterior fornix, whilst obliteratingthe introitus with the obstetrician’s hand. As thevaginal walls distend, the fundus of the uterus risesand the inversion is usually promptly corrected.Once this is achieved, fluid is allowed to slowlyescape from the vagina whilst the placement of theuterine fundus is achieved and maintained.
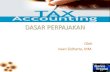
When O’Sullivan first described this technique, heused a douche-can and wide rubber tubing to deliverthe solution. More recently, a silastic vacuum cup hasbeen used to instil the sterile solution into thevagina12. Until replacement is effected, however,towels soaked in warm hypertonic saline solution anddraped over the inverted uterus may reduce the edemawhich will inevitably occur and which furtherimpedes replacement of the uterus. In extremely diffi-cult cases, replacement may require mid-line laparo-tomy, with the patient cleansed and draped in theLloyd Davis (frog-legged) position with a head-down(Trendelenberg) tilt. The patient is catheterized withan indwelling catheter and broad-spectrum antibioticsare administered. With the bowels packed upward andaway from the uterus, the obstetric surgeon places hishands in front and back of the lower segment with thefinger tips between and below the level of the invertedfundus. With progressive pressure on the fingertips ofboth hands which flip up simultaneously, the internaldimple is replaced progressively by the rising uterinefundus (Figure 1a–e)13. Uterine perfusion returns withre-establishment of uterine pulse pressure.
186
POSTPARTUM HEMORRHAGE

If this technique fails, then the mid-line abdominalincision can be extended upwards if necessary. Theinverted uterus resembles a funnel; it is best to exterio-rize the uterus. Instrumental upward traction is appliedto the round ligaments bilaterally using Allis or ringforceps, while the assistant exerts upward pressure onthe inverted parts from the vagina below. This maneu-ver is the Huntington technique14,15.
Failure at this stage warrants employing the Haultaintechnique whereby an incision is made vertically inthe posterior cervix via the abdominal route, follow-ing the dimple as a guide to relieve the constriction atthis level. The assistant exerts upward pressure fromthe vagina to effect reduction and replacement16.
On return of the uterus to its normal position, theplacenta should be removed manually from the vagina,and uterine contraction maintained abdominally by
187
Obstetric Trauma
Figure 1a Acute uterine inversion
Figure 1b Acute uterine inversion. Finger tips placed belowfundus of uterus to facilitate reduction
Figure 1c Acute uterine inversion. Progressive reduction withsome ischemia
Figure 1d Acute uterine inversion. Return of vascularity
Figure 1e Acute uterine inversion. Complete reduction andrevascularization with normal clinical features. (B-Lynch techniqueof non-instrumental reduction of acute uterine inversion atlaparotomy. ©Copyright ’05)

bi-manual stimulation. Ergometrine, oxytocic intra-venous infusion, or mesoprostyl can be administered.The posterior uterine incision, if used, is then repairedin layers, and the abdomen closed in the usual fashion.The patient should be monitored in the intensive careor the high-dependency unit for 24 h.
A sub-acute inversion is managed in a similarmanner but may resolve spontaneously as the uterusinvolutes4.
In chronic inversion, the uterus involutes in itsinverted position and remains in the vagina as a softswelling, which bleeds readily to touch and showsareas of superficial ulceration. Prolonged inversionmay result in conversion of the columnar epitheliumof the uterine wall into a stratified squamous epithe-lium. Replacement of a chronic inversion can proveextremely difficult, due partly to the inevitable edemapresent and the friable nature of the tissues. The tech-niques adopted for replacing the acutely inverteduterus are no longer helpful in this chronic situation.Bed rest, elevation of the foot of the bed, antibioticprophylaxis, and vaginal cleansing with hibitane packsmay be helpful to reduce the edema and treat anyinfections, but it may eventually be necessary to per-form a hysterectomy. If the chronic inversion is due tothe presence of a fibroid or a placental polyp, initialremoval of the polyp by ligating and cutting thepedicle as near to the base as possible may facilitatereplacement of the inverted uterus.
RUPTURED UTERUS
Uterine rupture is a serious obstetric complicationwith high morbidity and mortality. In developedcountries, the increasing number of cesarean sectionsperformed for minor degrees of disproportion, fetaldistress or pre-eclampsia in primiparae is of consider-able importance in calculating the long-term risksassociated with cesarean section, particularly in termsof the incidence and risk of uterine rupture. Both theshort- and long-term risks are accentuated in resource-poor countries.
Uterine rupture may be complete when the tearextends into the peritoneal cavity, or incompletewhen the serosa remains intact. The rupture may bespontaneous, traumatic or the result of scar dehiscenceand may occur either during pregnancy, early in laboror following a prolonged labor17.
In developed countries, the most common cause ofuterine rupture is dehiscence of a previous lower seg-ment transverse cesarean section scar. Rupture of aclassical scar is eight times more common than that ofa previous lower segment incision, and is far more aptto occur before rather than during labor. Previousrupture of a scar confers a 10–20-fold increase in riskof a subsequent rupture18,19.
Rupture of the uterus is generally sudden, accom-panied by severe abdominal pain and followed by vas-cular collapse. In many cases, however, asymptomaticdehiscence takes place during a vaginal delivery after aprevious cesarean section, when the dehiscence is
gradual and retraction of the uterus arrests hemorrhagefrom the wound. Because of this possibility, it isalways necessary to exclude silent dehiscence by man-ual exploration of the uterus after delivery of the fetuswhen a scar is present on the uterus.
A major factor in spontaneous uterine rupture isobstructed labor, especially in the developing worldwhen women routinely delivery without the benefitof the presence of trained health-care providers. Rup-ture may be due to maternal or fetal causes (generallymacrosomia). Examples of maternal causes are cepha-lopelvic disproportion from pelvic contraction due todevelopmental, constitutional or nutritional causes,abnormal presentation such as shoulder presentation,breech or brow, persistent mentoposterior face pre-sentation, transverse lie, fetal abnormality, hydro-cephalus, fetal tumor, fetal ascites, conjoined twins,maternal tumors, intrinsic cervical lesions, extrinsicfibroids or tumor, locked twins, and rarely uterinemisalignment such as incarcerated retroverted uterus,and pathological uterine anteversion. Additionally,grand multiparity, the use of uterotonic drugs to in-duce or augment labor, placenta percreta, and intra-uterine manipulation have all been implicated as causesof uterine rupture19,20.
The most common predisposing cause of ruptureduring pregnancy is a weak scar following a previouscesarean section20. Rarely, rupture can occur follow-ing unrecognized injury to the uterus at a previousdifficult delivery. It may present with sudden severeabdominal pains and collapse, or the symptoms maypresent gradually, when rupture is based on scar dehis-cence. If the onset is gradual, diagnosis may be difficultas the abdominal pain may be slight and accompaniedonly by alterations in the fetal heart tracing, maternaltachycardia and minimal vaginal bleeding. This triad isthen followed by patient collapse, cessation of fetalmovement and easy palpation of the fetal parts if thefetus has been expelled completely into the peritonealcavity. If the patient is in a hospital and the catastropherecognized at its onset, the outcome should be the safedelivery of the baby and repair of the uterus. If thepatient is not in a hospital, on the other hand, thecatastrophe is just that, a catastrophe of a dead childand its mother.
Uterine rupture during labor is also most com-monly due to dehiscence of a previous cesarean scarwith pain over the scar, followed by sudden severeabdominal pain and collapse. In grand multiparae witha friable inelastic uterine wall, rupture may occur inearly labor even where there has been no previous scaror difficult delivery, although this eventuality is notnearly as common as rupture in the previously scarreduterus. Here, however, diagnosis may be difficult ini-tially as the presentation may be confused with a smallaccidental hemorrhage and therefore missed.
Rupture after a prolonged labor is commonly dueto obstructed labor, with marked thinning of thelower segment and increased retraction of the uppersegment resulting in the formation of a retraction orBandl’s ring. The tear begins in the lower uterine
188
POSTPARTUM HEMORRHAGE

segment, may extend up to the fundus or down intothe vagina, or proceed laterally into the broad liga-ment. If the tear is posterior, it may go through theposterior vaginal fornix into the Pouch of Douglas(colporrhexis)20. If the rupture is in the lower anteriorsegment, the bladder is stripped from its attachment tothe lower segment. The peritoneum remains intactand so the rupture is characterized as incomplete. Amultiparous patient in obstructed labor will continueto have tetanic contractions until the uterus ruptures,whilst a primiparous patient will usually go out oflabor. Classical clinical signs of a rupture in a multi-parous patient can be dramatic; abdominal pain is con-stant, the contractions become virtually continuousinitially with only short intervals between them andlater no interval between contractile forces, with theformation of a Bandl’s ring followed by rupture andcollapse. The contractions then usually stop20–22, thefetus is expelled into the peritoneal cavity, the fetalparts are easily palpable and the uterus adopts analtered shape.
Rarely, the uterus may rupture during early to mid-pregnancy or during labor in patients who have had aprevious cornual ectopic pregnancy. Here also, therupture is dramatic, is located over the repair site ofthe ectopic and is characterized as a fundal blow-out.Sudden severe abdominal pain is experienced over thefundus of the uterus followed by collapse.
Rupture of a previously unscarred uterus is usually acatastrophic event resulting in death of the infant,extensive damage to the uterus and a very high risk ofmaternal death from blood loss. The damage to theuterus may be so extensive that repair is impossible anda hysterectomy is required. In developed countries,the incidence of ruptured uterus in an unscarred uterusis approximately 1 : 10 000 deliveries22; in the under-developed countries, the data are unknown. The inci-dence of rupture of a uterus with a previous cesareansection scar is 1%22,23. A trial of labor following a pre-vious cesarean section increases the risk of perinataldeath and rupture of the uterus compared to electiverepeat cesarean section. In one large Canadian study, atrial of labor following a previous cesarean section wasassociated with an increased risk of rupture (by 0.56%)but fewer maternal deaths than in an elective section(1.6 vs. 5.6 per 100 000)19.
In less developed countries, the incidence ofuterine rupture varies from 1.4% to 25%, with 25% inEthiopian women with obstructed labor23. Uterinerupture accounted for 9.3% of maternal mortality inone study from India and 6.2% in a study from SouthAfrica24.
A laparotomy is indicated when rupture of theuterus is suspected. The patient is anesthetized,cleansed, draped and the bladder catheterized with anindwelling catheter. A mid-line lower abdominal inci-sion should be used as this may be extended cephaladif necessary. The fetus should be delivered expedi-tiously and the uterus delivered from the abdominalincision to assist in controlling the bleeding and assess-ing the situation while resuscitative measures are
undertaken. In the series of over 1300 world-widereported successful applications of the B-Lynch(Brace) suture, 25 cases were applied for persistentuterine atony after repair of a uterine rupture. Inthese cases, successful bleeding control and hemostasiswere achieved (CBL world-wide communicationwww.CBLynch. com)25.
Hysterectomy may be necessary and should havebeen consented, if at all possible. It is not necessary toremove the ovaries merely because this is easier in acrisis. As with a cesarean hysterectomy performedin late labor, the cervix is no longer a discrete and cir-cumscribed solid structure, easily delineated and per-mitting accurate placement of vaginal clamps. In theacute situation, hemostasis and avoidance of furtherdissection are of paramount importance, and theremoval of the distal cervix is not critical. The mostdifficult surgical situation occurs when the rupture isextraperitoneal into the broad ligament, with a mas-sive hematoma distorting the anatomy and obscuringthe bleeding points. Here, it may be necessary to packthe space, the end of the pack being brought outthrough a gap in the uterine repair20. A balloon cathe-ter with light traction may be used for enhancedtamponade with or without the application of theB-Lynch (Brace) suture application26.
Other conservative surgery may be appropriate onoccasions, for example, when simple repair of the tearmay be preferable to hysterectomy. With an anteriorrupture, the bladder may be involved; the appearanceof hematuria is almost pathognomonic. Repair isundertaken and the bladder catheterized for 2 weeks.A posterior fornix rupture (colporrhexis) is relativelyeasy to repair. Incomplete rupture is not usually appar-ent until delivery has been achieved. It will commonlydeclare itself by intrapartum or postpartum hemor-rhage. It should always be excluded by manual explo-ration after delivery of the fetus. Both bladder tearsand colporrhexis may be missed if not anticipated. Ifthis is the case, bleeding may continue, to thesurgeon’s dismay.
BLUNT ABDOMINAL TRAUMA
The three main causes of serious blunt abdominaltrauma in pregnancy are motor vehicle accidents, fallsand domestic or intimate partner physical abuse. In thedeveloped world, the most common cause of bluntabdominal trauma is motor vehicle accidents27,28. Inthe less developed countries, the incidence of domes-tic physical abuse or intimate partner physical abusecan be as high as 13.5%29. Developed countries are notimmune from this problem, however, and a largereview of the prevalence of abuse during pregnancy inthe United States documented that between 0.9%and 20.1% of pregnant women were abused by theirpartners. This figure covers all forms of abuse, emo-tional, physical and sexual30.
Direct abdominal trauma by punching or kickingthe abdomen increases the risk of adverse outcome ofthe pregnancy. Adverse outcomes are more common
189
Obstetric Trauma

with direct physical assaults than with motor vehicleaccidents29,30. Partner abuse also tends to be a repeti-tive event, increasing the risk to the fetus31. In somecountries, partner abuse and violence against womenis accepted as a cultural norm, thus reducing thenumbers of reported cases. Even in the Chinese com-munity in Hong Kong and despite western socializa-tion, it is not uncommon for women to submit totheir husbands and endure humiliation for the sake ofkeeping their family together. Providing help for thesepregnant women is challenging32.
Motor vehicle accidents account for 60–75% ofcases of blunt trauma. Most injuries are minor, but, inthe United States, between 1300 and 3900 womeneach year suffer a fetal loss as a result of a motor vehicleaccident27,28. Despite the majority of the injuries beingminor, the fetus is always at risk and careful assessmentmust be carried out in all cases of blunt abdominaltrauma resulting from motor vehicle accidents. Assess-ments must be frequent and repeated with specialattention to conditions commonly seen after suchtrauma. These include abruptio placentae, pretermlabor, uterine rupture, fetomaternal hemorrhage,direct fetal injury and fetal demise33.
The pattern of injury following automobile acci-dents depends on the type of seat belt restraints. Anunbelted driver or passenger is usually ejected from thevehicle or sustains injuries when they hit the interiorof the car. The injuries are mainly to the face, head,chest, abdomen and pelvis. With shoulder and abdom-inal restraints, rib, sternum and clavicular fractures arecommon, whereas in the lap-only belted, lumbar spineand hollow viscus injuries are more frequent. Sharpobjects in the pockets of the clothing on the personcan cause additional trauma; a fountain pen may perfo-rate the lungs or heart. Even bulky outdoor over-clothing represents a hazard. With thick clothing,there is a short distance between the body of the per-son and the restraint. On impact, the weight of thebody causes acceleration forwards. The speed of con-tact between the person and the restraint can com-pound the damage sustained to the body.
During the first trimester, the uterus is well protectedwithin the pelvis and sustains very little damage fromblunt trauma. With advancing pregnancy, however, theuterus becomes an abdominal organ and therefore moresusceptible to trauma. The blood supply to the pelvis ismarkedly increased the more advanced the pregnancy,giving rise to retroperitoneal hemorrhage which can belife-threatening. Bowel injuries are less common, as thebowel occupies the upper abdominal space later inpregnancy, is a more movable entity and is not in thedirect line of the trauma.
Assessing the extent of trauma can be difficult, asclinical signs initially may be sparse. Patients should beassessed frequently to detect deterioration in their con-dition. The presence of bony injuries should raise sus-picion of intraperitoneal hemorrhage: rib fractures areassociated with liver and spleen injuries and pelvicfractures with retroperitoneal hemorrhage and injuryto the genitourinary system.
Difficulty is often encountered in detecting a smallamount of bleeding into the peritoneal cavity. Asblood may be non-irritant, ultrasound examinationmay be equivocal, and CT scanning exposes the fetusto a large radioactive dose. The decision to proceed toa laparotomy may therefore be entirely based on clini-cal judgement.
The most common cause of fetal death in non-fatalaccidents is abruptio placentae. In minor injuries, theincidence is between 1 and 5%, in contrast to majortrauma where the incidence may be as high as 30%. Atthe time of impact, the intrauterine pressure may be ashigh as ten times the pressure reached at the height of alabor contraction. Blunt trauma causes the uterus tocompress and then expand and the placenta shearsaway from the uterine wall. The degree of separationmay bear no relationship to the degree of trauma;abruption may occur with very little evidence ofinjury to the mother. It usually, but not always,follows soon after the trauma.
Vaginal bleeding, abdominal pain, increased uterinetone, uterine tenderness, high frequency contractions,and abnormal fetal cardiotocography are the classicalclinical signs of a placental abruption. In a posteriorlyinserted placenta, severe backache and vaginal bleed-ing may be significant symptoms. The bleeding maybe revealed or concealed within the uterus. If con-cealed, in severe cases, the uterus becomes woodyhard as described by Couvelaire, blood having beenextravasated into the muscular wall of the uterus. Fetalparts are impossible to feel and the patient’s conditionrapidly deteriorates due to hypovolemia and pain.
The management of abruptio placentae depends onthe severity of the abruption, the nature of the generalinjuries sustained, the condition of the fetus and theduration of the pregnancy. The trauma surgeon andthe obstetrician should work together in managing thepatient. Establishing wide-bore intravenous access isessential. The hematologist should also be involved. Acomplete thrombophilia screen should be requestedand cross-matched blood organized, together withfresh frozen plasma.
A preterm uncompromised fetus should beobserved by continuous cardiotocography for a mini-mum of 6–12 h or by a Pinard stethoscope in lessdeveloped communities and, if the gestation is under34 weeks, the mother should be given corticosteroidsto mimimize the adverse effect of prematurity on lungmaturation. If the fetus is previable and compromised,vaginal delivery is the safest for the mother.
In a term pregnancy with abruptio and an uncom-promised fetus, vaginal delivery is an option. How-ever, cesarean section is advised if the fetus iscompromised. If the fetus, on the other hand, has died,induction of labor and vaginal delivery are appropriateand safe for the mother.
Preterm labor following blunt abdominal traumamay be precipitated by extravasation of blood into themyometrium stimulating uterine contraction. Prosta-glandin release may stimulate uterine activity. Pretermlabor requiring tocolysis occurs in 10–30% of cases of
190
POSTPARTUM HEMORRHAGE

blunt abdominal trauma, but less than 1% deliverbefore 34 weeks. Tocolytics should be used guardedly,lest they mask the sign of abruption. Contractionsfollowing blunt abdominal trauma abate without treat-ment in 90% of cases. All tocolytics have side-effectswhich the obstetrician should be familiar with: betamimetics induce tachycardia and may mask the earlysigns of abruption; non-steroidal anti-inflammatoryagents affect platelet and renal function; and calciumchannel blockers cause hypertension. The fetal heartrate and the uterine contractions should be continu-ously monitored34.
Uterine rupture is a rare (1%) occurrence in bluntabdominal trauma; when it does occur, it is usually inassociation with a fractured pelvis. The site of ruptureis commonly the fundus of the uterus or the site of aprevious uterine scar. Fetal mortality in such cases is100%, and maternal mortality 10%35–38. Diagnosismay be difficult with vague abdominal pain, uterinetenderness, but with easily palpable fetal parts, and apoor trace or absence of a fetal heart on cardio-tocography. Fetal demise and maternal shock are moredramatic presentations.
If suspected, exploratory laparotomy in the pres-ence of the trauma surgeon is indicated. Uterine repairshould be undertaken only if the patient is hemo-dynamically stable. If not, hysterectomy should beperformed. However, the risk of a rupture in a subse-quent pregnancy is high, and the patient and herfamily should be advised this at an appropriate time.
Fetal injury occurs very infrequently followingblunt abdominal trauma. Fracture of the long bones orthe skull is the most common injury and occurs inapproximately 1% of cases. If the fetus is distressed,immediate delivery is called for. In the preterm non-compromised fetus, delivery may be delayed, but serialmonitoring is advised39,40.
Fetomaternal hemorrhage occurs in up to 30%of cases of blunt abdominal trauma, especially if theplacenta is situated anteriorly. Most fetuses will have anormal outcome, although anemia, supraventriculartachycardia and fetal demise can occur depending onthe extent of the fetomaternal hemorrhage41,42.Victims of blunt abdominal trauma should be screenedfor Rhesus factor, and all Rhesus-negative mothersgiven Anti-D immunoglobulin to prevent sensitiza-tion. Sensitization can occur as early as the 5th weekof pregnancy. A Kleihauer–Betke test is essential toassess the magnitude of the fetomaternal hemorrhageand adjust the dose of Anti-D immunoglobulinaccordingly.
In all cases of blunt abdominal injuries, fetal assess-ment is of paramount importance. Cardiotocographyis the most sensitive method of immediate fetal sur-veillance. Ultrasonography is only accurate in predict-ing 40% of cases of abruption. Uterine activity isthe most sensitive indicator for predicting abruptionfollowing blunt abdominal trauma. Frequent contrac-tions have an adverse effect on fetal outcome.
As a guideline, patients who have sustained bluntabdominal trauma, but have no abdominal tenderness,
no vaginal bleeding and no contractions should bemonitored 2-hourly for 6–12 hours. Patients withabdominal tenderness, vaginal bleeding and contrac-tions should be monitored continuously43,44.
References
1. Spain AW. Acute inversion of the uterus. J Obstet GynaecolBr Empire 1946;53:219
2. Das P. Inversion of the uterus. J Obstet Gynaecol Br Empire1940;47:525–48
3. Fahmy M. Acute inversion of the uterus. Int J Surg 1977;62:100
4. Watson P, Besch N, Bowes WA. Management of acute andsubacute puerperal inversion of the uterus. Obstet Gynecol1980;55:12
5. Brar HS, Greenspoon JS, Platt LD, Paul RH. Acute puerperaluterine inversion. J Reprod Med 1989;34:173–7
6. Wendel PJ, Cox SM. Emergent obstetric management ofuterine inversion. Obstet Gynecol Clin N Am 1995;22:261–74
7. Abouleish E, Ali V, Joumaa B, et al. Anaesthetic managementof acute puerperal uterine inversion. Br J Anaesth 1995;75:486–7
8. Catanzarite VA, Moffitt KD, Baker ML, et al. New approachto the management of acute puerperal uterine inversion.Obstet Gynecol 1986; 68(Suppl):7–10
9. Clark SL. Use of ritodrine in uterine inversion. Am J ObstetGynecol 1984;151:705
10. Grossman RA. Magnesium sulphate for uterine inversion.J Reprod Med 1981;26:261–2
11. O’Sullivan JV. Acute inversion of the uterus. Br Med J 1945;ii:282–3
12. Ogueh O, Ayida G. Acute uterine inversion: a new tech-nique of hydrostatic replacement. Br J Obstet Gynaecol 1997;104,951–2
13. B-Lynch C. Non instrumental atraumatic stepwise reductionof acute uterine inversion. In press
14. Huntington JL. Acute inversion of the uterus. Boston MedSurg J 1921;184:376–80
15. Huntington JL, Irving PC, Kellogg PS. Abdominal repositionin acute inversion of the puerperal uterus. Am J ObstetGynecol 1928;15:34–40
16. Haultain FWN. The treatment of chronic uterine inversionby abdominal hysterotomy with a successful case. Br Med J1901;ii:974
17. Schrinsky DC, Benson RC. Rupture of the pregnant uterus:a review. Obstet Gynaecol Surv 1978;33:217–32
18. Ritchie EH. Pregnancy after rupture of the pregnant uterus.J Obstet Gynaecol Br Commonwealth 1971;78:642–8
19. Aguero O, Kizer S. Obstetric prognosis of the repair ofuterine rupture. Surg Gynaecol Obstet 1968;127:528–30
20. Hudson CN. Obstructed labour and its sequelae. In LawsonJB, Harrison KA, Bergstrom S, eds. Maternity Care in Devel-oping Countries. London: RCOG Press, 2001
21. Wen SW, Rusen ID, Walker M, et al. Comparison of mater-nal mortality and morbidity between trial of labor and electiveCaesarean among women with previous caesarean delivery.Am J Obstet Gynecol 2004;19:1263–9
22. Miller DA, Goodwin TM, Cherman RB, Oaul RH.Intrapartum rupture of the unscarred uterus. Obstet Gynecol1997;89:671–3
23. Gaym A. Obstructed labour in a district hospital. Ethiop MedJ 2002;40:11
24. Rajaram P, Agarwal A, Swain S. Determinants of maternalmortality: a hospital based study from South India. Ind JMatern Child Health 1995;6:7–10
25. B-Lynch C. Persistent uterine atony after successful repair ofruptured uterus treated by Brace suture, world-wide reportsand personal communication. www.cblynch.com
191
Obstetric Trauma

26. Danso D, Reginald P. Intrauterine balloon catheter withB-Lynch suture. Br J Obstet Gynaecol 2002;109:963
27. Esposito TJ, Gens DR, Smith IG, Scorpio R, Buchman T.Trauma during pregnancy. A review of 79 cases. Arch Surg1991;126:1073–8
28. Hoff WS, D’Amelio LF, Tinkoff GH, et al. Maternal predic-tors of fetal demise in trauma during pregnancy. SurgGynecol Obstet 1991;172:175–80
29. Valladares E, Pena R, Oersson LA, Hogberg U. Violenceagainst pregnant women: prevalence and characteristics. Apopulation-based study in Nicaragua. Br J Obstet Gynaecol2005;112:1234–48
30. Gazmararian JA, Lazorick S, Spitz AM, Ballard TJ, SaltzmanLE, Marks JS. Prevalence of violence against women: areview of the literature. JAMA 1996;275:1915–20
31. Godwin TM, Breen MT. Pregnancy outcome and feto-maternal hemorrhage after non catastrophic trauma. Am JObstet Gynecol 1990;162:665–71
32. Tiwari A, Leung WC, Leung TW, Humphreys J, Parker B,Ho PC. A randomised controlled trial of empowermenttraining for Chinese abused pregnant women in Hong Kong.Br J Obstet Gynaecol 2005;112:1249–56
33. Connolly A, Katz VL, Bash KL, McMahon MJ, Hansen WF.Trauma and pregnancy. Am J Perinatol 1997;14:331–6
34. Elliott M. Vehicular accidents and pregnancy. Aust NZ JObstet Gynaecol 1966;6:279–86
35. Williams JK, McClain L, Rosemurgy AS, Colorado NM.Evaluation of blunt abdominal trauma in the third trimesterof pregnancy: maternal, and fetal considerations. ObstetGynecol 1990;75:33–7
36. American College of Obstetricians and Gynecologists.Trauma during pregnancy. ACOG Technical Bulletin No.161, November 1991, Washington DC
37. Mighty H. Trauma in pregnancy. Crit Care Clin 1994;10:623–34
38. Dahmus MA, Sibai BN. Blunt abdominal trauma. Are thereany predictive factors for abruptio placentae or maternal-fetaldistress. Am J Obstet Gynecol 1993;169:1054–9
39. Lavin JP, PolSky SS. Abdominal trauma during pregnancy.Clin Perinatol 1983;10:423–38
40. Goodwin TM, Breen MT. Pregnancy outcome and feto-maternal hemorrhage after non-catastrophic trauma. Am JObstet Gynecol 1990;162:665–71
41. Pearlman MD, Tintinalli JE, Lorenz RP. A prospective con-trolled study of outcome after trauma during pregnancy. Am JObstet Gynecol 1990;162:1502–10
42. Rose PG, Strohm PL, Zuspan FP. Fetomaternal hemorrhagefollowing trauma. Am J Obstet Gynecol 1985;153:844–7
43. Pearlman MD, Phillips ME. Safety belt use during pregnancy.Obstet Gynecol 1996;88:1026–9
44. Pearlman MD, Tintinalli JE, Lorenz RP. Blunt trauma duringpregnancy. N Engl J Med 1991;323:1609–13
192
POSTPARTUM HEMORRHAGE
Related Documents