3/2/2016 1 3/2/2016 Track 1 Breakout Session- Cost Effective Clinical Tools for Improved Diabetic Foot Outcomes (Hands- on session) R. Gary Sibbald, MD, M.Ed, D.Sc (Hons) FRCPC (Med, Derm), FAAD, MAPWCA Elizabeth A. Ayello, PhD, RN, ACNS-BC, CWON, MAPWCA, FAAN Kathya Zinszer, DPM, MPH FAPWCA Participants Will: Describe an evidence based 60- second screening tool for the high risk diabetic foot Demonstrate the use of infrared thermography in the care of persons with diabetes mellitus Identify areas of high pressure and shear on the diabetic foot that can lead to ulceration Global Type 2 Diabetes Tsunami IDF Atlas 5 th edition diabetes prevalence (age 20-79) Guyana 15% Year Persons with Diabetes Comment 2011 365 million • 4.6 million DM related deaths annually • Spending on DM 465 million US 2030 552 million • 50% increase • Additional 398 million at high risk 75% of people with diabetes now live in low-and middle-income countries 4th leading cause of death Lifestyle interventions to prevent diabetes Foot care for people at high risk Glycemic control if HbA1c > 9% Highest priorities for diabetes interventions Low-Middle Income Countries (LMIC) are? Dx and Rx Diabetic retinopathy © WoundPedia Diabetes Control Priorities in Developing Countries 1 Highest level priority: Cost saving AND Highly feasible Type 2 Diabetes • Foot care if high risk • Glycemic control to HbA1c < 9% • Blood pressure control to BP < 160/95 1) Narayan V, et al. Diabetes: The Pandemic and Potential Solutions. In: Jamison D, et al., editors. Disease Control Priorities in Developing Countries. 2nd ed. Washington, DC: World Bank; 2006. p. 591-603. Plantar Pressure Redistribution You do not need a lot of money or resources to make a big difference

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

3/2/2016
1
3/2/2016
Track 1 Breakout Session-
Cost Effective Clinical Tools
for Improved Diabetic Foot Outcomes
(Hands- on session)
R. Gary Sibbald, MD, M.Ed, D.Sc (Hons)
FRCPC (Med, Derm), FAAD, MAPWCA
Elizabeth A. Ayello, PhD, RN, ACNS-BC,
CWON, MAPWCA, FAAN
Kathya Zinszer, DPM, MPH FAPWCA
Participants Will:
Describe an evidence based 60- second screening tool for the high risk diabetic foot
Demonstrate the use of infrared thermography in the care of persons with diabetes mellitus
Identify areas of high pressure and shear on the diabetic foot that can lead to ulceration
Global Type 2 Diabetes Tsunami
IDF Atlas 5th edition diabetes
prevalence (age 20-79)
Guyana
15%
Year Persons with
Diabetes
Comment
2011 365 million • 4.6 million DM related deaths annually
• Spending on DM 465 million US
2030 552 million • 50% increase
• Additional 398 million at high risk
75% of people with diabetes now live in low-and middle-income countries
4th leading cause of death
Lifestyle interventions to prevent diabetes
Foot care for people at high risk
Glycemic control if HbA1c > 9%
Highest priorities for diabetes interventions
Low-Middle Income Countries (LMIC) are?
Dx and Rx Diabetic retinopathy
© WoundPedia
Diabetes Control Priorities in
Developing Countries1
Highest level priority:
Cost saving AND Highly feasible
Type 2 Diabetes
• Foot care if high risk
• Glycemic control to HbA1c < 9%
• Blood pressure control to BP < 160/95
1) Narayan V, et al. Diabetes: The Pandemic and Potential Solutions. In:
Jamison D, et al., editors. Disease Control Priorities in Developing
Countries. 2nd ed. Washington, DC: World Bank; 2006. p. 591-603.
Plantar Pressure Redistribution
You do not need a lot of money
or resources to make a big difference

3/2/2016
2
Plantar Pressure Redistribution
Standards of Care - Affordable
In Canada250 patients treated for
less than $7000 Canadian
In Guyana$150-200
$20-25
A Variety of Standard Offloading
Boots and shoes
$20-25
Darco Forefoot & Heel Offloading
Shoe & GlobalPed
$20-25
Forefoot OffloaderRearfoot Heel Offloader
Posterior Heel and Achilles Tendon offloader
Bledsoe & Pneumatic Walking Boots
$20-25
Total Contact Cast: Gold
Standard for Plantar Diabetic
Foot Ulcers
$20-25
Felted Foam: Lower risk for
Plantar Diabetic Foot Ulcers with
severe PDN
$20-25

3/2/2016
3
Every 20 seconds a lower limb is lost to diabetes somewhere in the world
Vast majority are preventable through patient centred interprofessional care (integrated, coordinated)
Diabetic foot screening (high risk foot) is one of the three most cost-savings diabetes interventions – yet the most neglected (others- HbA1c, blood pressure)
Diabetic Foot – Global View
Source: Williams, International Working Group for the Diabetic Foot & Narayan KV, Zhang P, Kanaya AM, DE, Engelgau MM, Imperatore G, et al. Diabetes: The Pandemic and Potential Solutions.
Disease Control Priorities in Developing Countries [Internet]. Washington D.C. World Bank; 2006 Available from: http://www.ncbi.nlm.nih.gov/books/NBK11777/
Benchmark HbA1c Data
• GPHC: 4302 1st tests – April 2010 to Feb
2013
• 295 F-up tests - 65% adherent to
protocol
• Percentage with HbA1c > 9%
o All persons with diabetes 38%
o Diabetic Foot patients 44%
Mean HbA1c from DFC patients 13% higher than from other facilities
High risk foot status is associated with poor glycemic control
Phase 1- Developed Center of Excellence at GPHC –
Diabetic Foot Centre
Interprofessional teams MD, Nurse, Rehab
Develop Key opinion leaders
4 levels of education – multi faceted,
longitudinal strategies
Focus on Prevention
Wound Bed Preparation Paradigm (Sibbald et al. 2011)
In clinic preceptorships:Doppler, infra-red thermometer, footwear
Conservative debridement
©
Major Amputations at GPHC
Risk Months Mean
St.
dev
95%
CI T test
Befor
e DFC 42 7.95 3.99 1.24 P <
0.0001After
DFC 42 4.14 2.36 0.73
48% reduction from pre-project levels
48 limbs saved each year = 192 limbs to July 2012
68% reduction in monthly proportion of DFU
despite 75% increase in DFU admissions
PLOS Med April 2015
Variable
Pre-DFC
(30months)
Post -DFC
(22 months)
Analysis
DF admissions
(ward records)
633 924
N Amputations 262 110 P<0.0001
Avg. Monthly
Proportion DFU
patient with Maj.
Amp.
41.4% 11.9% 71%
reduction
Diabetic Foot Ulcer Admissions and Amputation Rates at Georgetown Public Hospital Corporation
VariablePre-
Intervention
Post
InterventionTest-statistic p-value
Time in
months 42 48
N Above
knee amp124 113*
Mean (SD) 2.95 (2.44) 2.13 (1.81) -1.82 (t) 0.07
N Below
knee amp166 41*
Mean (SD) 3.95 (2.64) 0.77 (1.05) -7.35 (t) < 0.0001
Major Amputations by type at Georgetown Public Hospital Corporation
*Represents total with available dates. One AKA and 3 BKAs were not dated.

3/2/2016
4
Why were BKAs markedly lowered but AKAs were not?
Hypothesis:
Patients requiring AKAs are more likely to have associated peripheral vascular insufficiency (ischemia) which GDFP did not address.
Test:
Compare indices of PVD in patients with AKA and BKA
Reverse Innovation
…“innovation seen first, or likely to be
used first, in the developing world before
spreading to the industrialized world”.
Wikipedia
What innovations were applied in this project that
are not currently part of integrated coordinated care
in North America?
The 4 S’s of DM Ulcer Prevention
Screening Stop Smoking Shoes Shoes
© Sibbald & Ayello 2012
Skin Temperature
Screening – high risk status
Risk factor Ulcer yearly
incidence/ rate %
Odds ratio
(95%CI)
Group 0 (no PN, no PVD) 2%
Group 1
(PN, no PVD or deformity)
4.5% 2.4 (1.1.-5)
Group 2B (PVD) 13.8% 9.3 (5.7-15.2)
Group 3 PN/ PVD (history of
ulcer or amputation)
32.2% 52.7(27.2-109.8)
3/2/2016
Lavery LA, et al. … classification system of the International Working Group
on the Diabetic Foot. Diabetes Care 31(1):154-6, 2008.
Focus on Prevention:
60 Second Screening
•History
•Inspection abnormalities
•Palpate pulse
•Deformity
•Monofilament testing
(4 out 10 negative)
After Inlow 60 sec exam
Screening for the high risk diabetic foot: A 60-Second Tool (2012) ©
Sibbald
Name: _______________________________________________
ID#: ________ Phone #:_____________ Facility:____________
DOB (dd/mm/yy):_______/_______/_______
Gender: M □ F □ Years with diabetes:________
Ethnicity: Black □ Asian □ Caucasian □ Mixed □ Other □
Date of Exam (dd/mm/yy): ______/______/______
CHECK BOTH FEET
(Circle correct response)
“YES” on either foot = HIGH RISK
LEFT RIGHT
HISTORY 1. Previous ulcer NO YES NO YES
2. Previous amputation NO YES NO YES
PHYSICAL EXAM 3. Deformity NO YES NO YES
4. Absent pedal pulses
(Dorsalis Pedis and/ or Posterior Tibial) NO YES
NO YES
FOOT LESIONS Remember to check 4
th and
5th web spaces/nails for
fungal infection and check
for inappropriate footwear.
5. Active ulcer NO YES NO YES
6. Ingrown toenail NO YES NO YES
7. Calluses (thick plantar skin) NO YES NO YES
8. Blisters NO YES NO YES
9. Fissure (linear crack) NO YES NO YES
NEUROPATHY MORE THAN 4/10 SITES
LACKING FEELING =
“YES”
10. Monofilament exam (record negative reaction): a) Right______/10 negatives ( 4 negatives = Yes) b) Left_______/10 negatives ( 4 negatives = Yes)
NO YES
NO YES
Total # of YES:_____ Total # of YES: ____
PLAN
a) POSITIVE SCREEN- Results when there are one or more “Yes” responses. Refer to a foot specialist or team
for prevention, treatment and follow up. (Bony deformity, current ulcer, absent pulse are most urgent).
These individuals are at increased risk of a foot ulcer and/or infection. Patients should be educated on what
changes to observe and report, while waiting for the specialist appointment.
Referral to: ____________________________ Appointment time:_______________________
b) NEGATIVE SCREEN- Results when there are all “No” responses. No referral required.
Educate patient to report any new changes to their healthcare provider and re-examine in 1 year.
One Year Date for Re-Examination (dd/mm/yy):________/________/________
Completed By: __________________________ Date: _________________________________
Additional Note: See reverse side for recommendations from the International Diabetes Federation, & International Working
Group on the Diabetic Foot.
Local referral patterns may vary depending on expertise and available resources.
Available at
www.diabeticfootscreen.com
www.WoundPedia.com
What % persons with DM
have a high risk foot?
RED: 48%
YELLOW: 73%
PINK: 92%
GREEN: 27%
BLUE : 14%

3/2/2016
5
Profile: 1266 consecutive PWD
ITEM NO % YES %
Previous Ulcer 91 9
Previous Amp 96 4
Deformity 92.1 7.9
Absent pulse 88 12
Active DFU 92.3 9
Ingrown toenail 81.7 18.3
Callus 77.7 22.3
Fissure 89.5 10.5
Neuropathy 76.6 23.4
REFERRED DFC 52 48
PL0S Med. 2015 Apr; 12(4):
The Guyana Diabetes and Foot Care
Project: A Complex Quality
Improvement Intervention to
Decrease Diabetes-Related Major
Lower Extremity Amputations and
Improve Diabetes Care in a Lower-
Middle-Income Country
• Interprofessional team
• Center of excellence
• Footwear- Footcare + VIPs
• Reduced amputations 68-72%
Julia Lowe, R. Gary Sibbald,
Nashwah Y. Taha, Gerald Lebovic,
Carlos Martin,Indira Bhoj, Rolinda Kirton,
Brian Ostrow, and the
Guyana Diabetes and Foot Care Project Team¶
60 Second Screen - History
1. Previous Ulceration 2. Previous Amputation
3/2/2016
Simplified 60 Second Screen Tool (2012)©
Physical Examination
3. Deformity OR Charcot Change
© Sibbald 2012
60 Second Screen –
Physical Examination
4. Pulses absent
Dorsalis Pedis and /or Posterior Tibial
3/2/2016
60 Second Screen – Foot Lesions
5. Active Ulcer 6. Ingrown toenail
3/2/2016
60 Second Screen – Foot Lesions
7. Calluses =
increased pressure
3/2/2016

3/2/2016
6
60 Second Screen – Foot Lesions
4th – 5th Toe Web Space Nails- early fungus
3/2/2016
Also look for/ treat possible
fungus • 4th – 5th Toe Web Space
© Sibbald 2012
60 Second Screen – Neuropathy
10.Mono filament Exam
X for negative = 4/ 10
3/2/2016
X
X
X X
Lets go to the video tape!Simplified 60 Second Screen Tool (2012)©
International Diabetes Federation, International Working Group on the Diabetic Foot, 2008
Validation of the 60 second screening toolPLOS Medicine, June 2015 (Woodbury, Sibbald et.al)
• Multiple raters
– 6 Canadians
– 6 Guyanese KOL
• 18 subjects with various high risk diabetic foot features examined by all 12 rater clinicians
• Statistical analysis
– Cronbach's alpha as a measure of internal consistency
– Set of items= raters
– 0 to 1 (perfect agreement)
– Statistical cut off at 0.6
© WoundPedia
3/2/2016
7
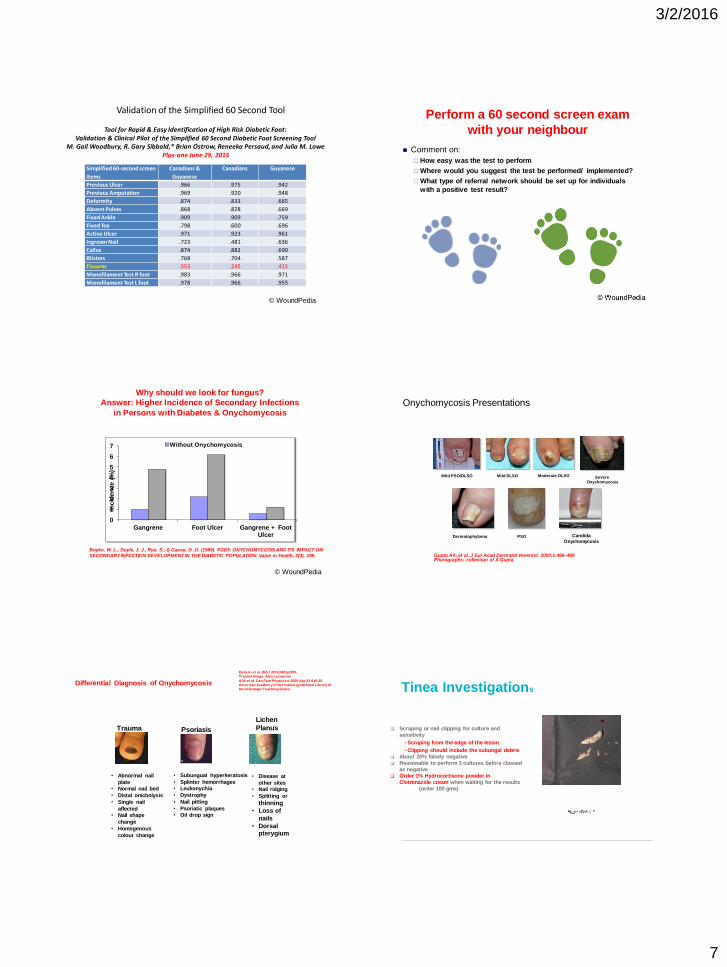
Validation of the Simplified 60 Second Tool
Simplified 60-second screen
items
Canadians &
Guyanese
Canadians Guyanese
Previous Ulcer .966 .975 .942
Previous Amputation .969 .920 .948
Deformity .874 .833 .665
Absent Pulses .868 .828 .669
Fixed Ankle .909 .909 .759
Fixed Toe .798 .600 .696
Active Ulcer .971 .923 .961
Ingrown Nail .723 .481 .636
Callus .874 .882 .690
Blisters .768 .704 .587
Fissures .553 .245 .415
Monofilament Test R foot .983 .966 .971
Monofilament Test L foot .978 .966 .955
Tool for Rapid & Easy Identification of High Risk Diabetic Foot: Validation & Clinical Pilot of the Simplified 60 Second Diabetic Foot Screening Tool
M. Gail Woodbury, R. Gary Sibbald,* Brian Ostrow, Reneeka Persaud, and Julia M. LowePlos-one June 29, 2015
© WoundPedia
Perform a 60 second screen exam
with your neighbour
Comment on:
How easy was the test to perform
Where would you suggest the test be performed/ implemented?
What type of referral network should be set up for individuals
with a positive test result?
Why should we look for fungus?
Answer: Higher Incidence of Secondary Infections
in Persons with Diabetes & Onychomycosis
0
1
2
3
4
5
6
7
Gangrene Foot Ulcer Gangrene + FootUlcer
Incid
en
ce (
%)
Without Onychomycosis
Boyko, W. L., Doyle, J. J., Ryu, S., & Gause, D. O. (1999). PDD5: ONYCHOMYCOSIS AND ITS IMPACT ON
SECONDARY INFECTION DEVELOPMENT IN THE DIABETIC POPULATION. Value in Health, 2(3), 199.
© WoundPedia
Onychomycosis Presentations
Mild PSO/DLSO Mild DLSO Moderate DLSO
Dermatophytoma
Severe Onychomycosis
Gupta AK, et al. J Eur Acad Dermatol Venereol. 2000;1:466–469Photographs: collection of A Gupta
PSO Candida
Onychomycosis
Differential Diagnosis of Onychomycosis
• Disease at
other sites
• Nail ridging
• Splitting or
thinning
• Loss of
nails
• Dorsal pterygium
Lichen
Planus
Eisman et al. BM J. 2014;348:g1800.
Trauma Image: Alex Lozupone
Afifi et al. Can Fam Physician. 2005 Apr;51:519-25.
American Academy of Dermatology National Library of
Dermatologic Teaching Slides.
Psoriasis
• Subungual hyperkeratosis
• Splinter hemorrhages
• Leukonychia
• Dystrophy
• Nail pitting
• Psoriatic plaques
• Oil drop sign
Trauma
• Abnormal nail
plate
• Normal nail bed
• Distal onicholysis
• Single nail
affected
• Nail shape
change
• Homogenous
colour change
Tinea Investigations
Scraping or nail clipping for culture and
sensitivity
• Scraping from the edge of the lesion
• Clipping should include the subungal debris
About 20% falsely negative
Reasonable to perform 3 cultures before classed
as negative
Order 1% Hydrocortisone powder in
Clotrimazole cream when waiting for the results
(order 100 gms)

3/2/2016
8
Fungal Nail Infections (L.I.O.N.)Evans EG, Sigurgeirsson B: Br Med J 99
Dose and Time Mycological Cure
Terbinefine 250 od for 3
months
75.7%
Terbinefine 250 od for 4
months
80.8%
Itraconazole 400 od x 1 wk
/mo x3
38.3%
Itraconazole 400 od x 1 wk
/mo x3
49.1%
A evidence: Double blind random study of more than 120 patients in each group
Dry Diabetic Foot: What cream should I use:
Fungus: X2 per day for 2 weeks
Cicloprox Rx – 60%
Azoles- 70%-80% Miconazole
Clotrimazole
Econazole
Ketoconazole
X1 per day for 1 week
Allylamines – 90%
Terbinefine Rx
naftifine
Recurrences 7-16% per year,
Use cream x 2 week to prevent recurrences
Dry Skin: Moisturizers
Humectants Urea
Lactic Acid
Glycerin
Ceramides
Lubricants Silicone, dimethacone
Lanolin, petrolatum
When in doubt, RX
1% hydrocortisone powder in Clotrimazole cream
Twice daily (BID) and give 100 grams
Pathway to the Prevention & Treatment of Toenail Onychomycosis
Detail: III Treatment strategies
1. Elewski B, et al. J Am Acad Dermatol 2013;68(4):600-8
2. Gupta AK, et al. J Drugs Dermatol. 2014
Topical efinaconazol e = Jublia, Valeant
Bacterial Soup
Compress a wound with saline or water
Do not use foot soaks or you are spreading any bacteria anywhere on the foot into the open areas (toe webs, nail folds, fissures or ulcers)
3/2/2016
How can you determine if shoes
are too small ?
No Smoking: Double indemnity
• Every cigarette will decrease the circulation in the leg or foot up to 30% for an hour or
increase sympathetic tone for 8 hours
Cigarette smoking decreases tissue oxygen. –Jensen JA - Arch Surg - 01-SEP-1991; 126(9): 1131-4 © Sibbald & Ayello 2012
3/2/2016
9
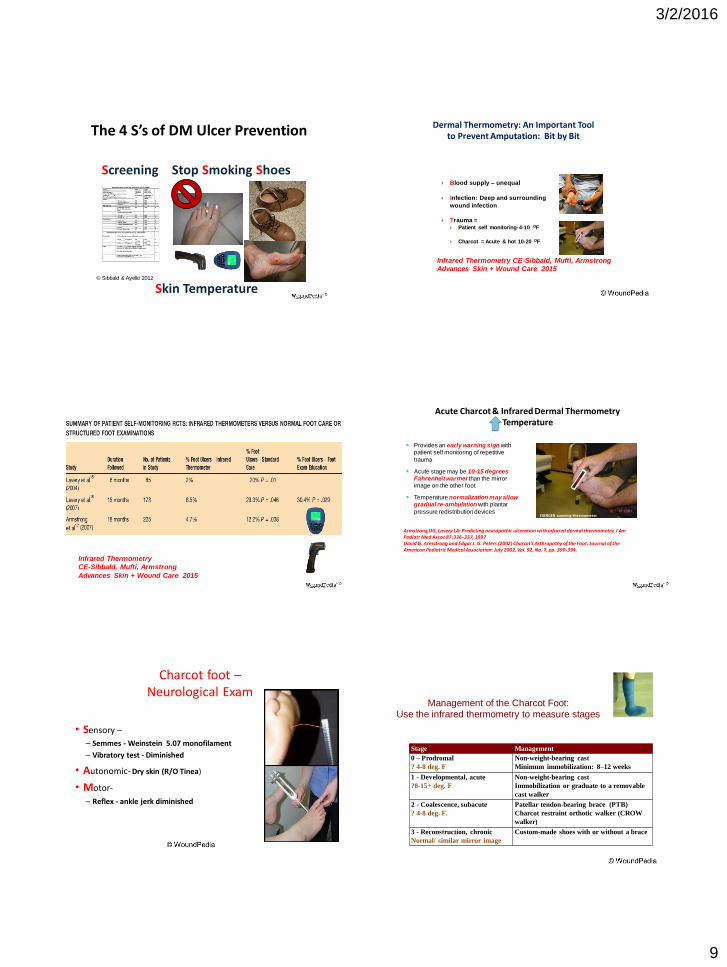
The 4 S’s of DM Ulcer Prevention
Screening Stop Smoking Shoes Shoes
© Sibbald & Ayello 2012
Skin Temperature
Dermal Thermometry: An Important Tool to Prevent Amputation: Bit by Bit
Blood supply – unequal
Infection: Deep and surrounding
wound infection
Trauma = Patient self monitoring-4-10 OF
Charcot = Acute & hot 10-20 OF
Infrared Thermometry CE-Sibbald, Mufti, Armstrong
Advances Skin + Wound Care 2015
Infrared Thermometry
CE-Sibbald, Mufti, Armstrong
Advances Skin + Wound Care 2015
Acute Charcot & Infrared Dermal ThermometryTemperature
Provides an early warning sign with patient self monitoring of repetitive
trauma
Acute stage may be 10-15 degrees Fahrenheit warmer than the mirror image on the other foot
Temperature normalization may allow gradual re-ambulation with plantar
pressure redistribution devices
Armstrong DG, Lavery LA: Predicting neuropathic ulceration with infrared dermal thermometry. J Am Podiatr Med Assoc 87:336–337, 1997David G. Armstrong and Edgar J. G. Peters (2002) Charcot’s Arthropathy of the Foot. Journal of the American Podiatric Medical Association: July 2002, Vol. 92, No. 7, pp. 390-394.
EXERGEN scanning thermometer
Charcot foot –Neurological Exam
• Sensory –
– Semmes - Weinstein 5.07 monofilament
– Vibratory test - Diminished
• Autonomic- Dry skin (R/O Tinea)
• Motor-
– Reflex - ankle jerk diminished
Stage Management
0 – Prodromal
? 4-8 deg. F
Non-weight-bearing cast
Minimum immobilization: 8–12 weeks
1 - Developmental, acute
?8-15+ deg. F
Non-weight-bearing cast
Immobilization or graduate to a removable
cast walker
2 - Coalescence, subacute
? 4-8 deg. F.
Patellar tendon-bearing brace (PTB)
Charcot restraint orthotic walker (CROW
walker)
3 - Reconstruction, chronic
Normal/ similar mirror image
Custom-made shoes with or without a brace54
Management of the Charcot Foot:Use the infrared thermometry to measure stages

3/2/2016
10
Pillars of Charcot Treatment
1. Early recognition
2. Off-loading to reduce
the deformity that will
result from continued
weight-bearing and
3. Management of
complications
Validation of Commercially Available Infrared Thermometers for Measuring Skin Surface
Temperature Associated with Deep and Surrounding Wound Infection
Asfandyar Mufti MD (c)Pat Coutts RN, IIWCCR. Gary Sibbald MD
Advances in Skin + Wound Care Jan 2015
Infrared Thermometer Screens
OBJECTIVE:
• Compare 4 less expensive, commercially available non-contact infrared thermometers to the scientifically accepted Exergen DermaTemp 1001™.
DESIGN, SETTING, AND PARTICIPANTS:
• observational study design• Consenting participants with open wounds were sequentially selected from a chronic wound clinic (n=108). • Skin temperatures were recorded using five non-contact infrared thermometers under consistent
environmental conditions.
MAIN RESULTS:
• No statistical difference was reported between the “ΔT” values for the five different thermometers (F(4, 514) = 0.339, p=0.852)
• intraclass correlation showed high reliability and agreement between raters, as the ICC values for all thermometers were >0.95.
Validation Commercially available low cost infrared thermometers
Device Measurement Range
Operating Range
Accuracy (Ambient
temperature = 25°Ca)
Distance to Size Ratio
Continuous Scanning
“Maximum” temperature
Cost
(US Dollars)
Exergen DermaTemp1001TM 18 to 43°C
(65 to 110°Fb)
16 to 43°C
(60 to 110°F)
± 0.1°C (0.2°F) 1:1 Yes Yes $650.00-750.00
Mastercraft Digital Temperature
ReaderTM
-30 to 480°C
(-22 to 896°F)
0 to 50°C
(32 to 122°F)
±2.0°C (4.0°F)c 8:1 Yes Yes $99.99
ATD Tools 70001 Infrared
Thermometer®
-60 to 550°C
(-76 to 1022°F)
0 to 50°C
(32 to 122°F)
±1.5°C (2.7°F) 12:1 Yes Yes $37.00-80.00
Pro Point Infrared Thermometer -60 to 500°C
(-76 to 932°F)
0 to 50°C
(32 to 122°F)
±1.0°C (1.8°F) 12:1 Yes Yes $99.99
Mastercool©
MSC52224-A-58 to 932°C
(-50 to 500°F)
0 to 40°C
(32 to 104°F)
±2.0°C (4.0°F) 12:1 Yes Yes $57.00 - $68.00
Device Specifications and Features
Neuropathic
Foot Ulcer
22%
Malignancy
3%
Infection
6%
Inflammation
10%
Venous/
Lymphatic
Ulcers
20%Post Surgical
Wound
8%
Pressure
Ulcer
7%
Trauma
11%
Arterial Ulcer
6%
Other
7%
STUDY PATIENT WOUND ETIOLOGYINFRARED THERMOMETER STUDY

3/2/2016
11
Thermometer Mean “ΔT”
Exergen DermaTemp 1001TM 2.39 °F (SD = 3.54)
Mastercool© MSC52224-A 2.68 °F (SD = 4.06)a
ATD Tools 70001 Infrared Thermometer®
2.67 °F (SD = 3.93)b
Mastercraft Digital Temperature ReaderT M
2.72 °F (SD = 4.26)c
Pro Point Infrared Thermometer 3.01 °F (SD = 3.90)d
a p = 0.987; b p = 0.985; c p = 0.972; d p = 0.774
RESULTS – “Mean Temperature Gradients”
N = 108P= 0.852
Thermometer ICCa
Exergen DermaTemp 1001TM 0.967 (0.92, 0.987)
ATD Tools 70001 Infrared Thermometer®
0.970 (0.925, 0.988)
Pro Point Infrared Thermometer 0.969 (0.922, 0.987)
Mastercool© MSC52224-A 0.968 (0.92, 0.987)
Mastercraft Digital Temperature ReaderT M
0.952 (0.884, 0.981)
a95% CI values stated in parenthesis.
RESULTS – “Inter- Rater Reliability”
N = 20
MastercraftDigital
Temperature ReaderTM
ATD Tools 70001 Infrared Thermometer®
Pro Point Infrared
Thermometer
Mastercool©
MSC52224-A
less expensive, industrial grade non-contact infrared thermometers have reliable temperature readings
Conclusion:
Asfandyar Mufti MD (c)Pat Coutts RN, IIWCCR. Gary Sibbald MD
Advances in Skin + Wound Care Jan 2015
Wound Bed Preparation 2015Person
with a Chronic Wound
Identify & Treat the cause
Patient/Family Centered Concerns
Determine Healability for patient outcomes &
local wound care
DebridementInflammation/
InfectionNERDS/STONEES
Moisture Balance
Edge Effect© Sibbald , Elliott, Ayello, Sumayaji -Advances in Skin – Wound Care- Oct. 2015
Levine Technique
Speaker, Title, Hospital
• Non-healing
• Exudate
• Red + Bleeding
• Debris
• Smell
NERDS Superficial
critical colonization :
Treat topically
• Size is bigger
• Temperature ↑
• Os (probes, exposed)
• New breakdown
• Exudate,
• Erythema, Edema
• Smell
STONEES
Deep
+ Surrounding
Treat Systemically
PAIN AND WOUND
Superficial Critical Colonization Deep / Surrounding Infection
Sibbald, Woo, Ayello 06
Woo, Sibbald 09

3/2/2016
12
NERDS STONEES
NERDS and STONEESWoo & Sibbald 2009
Critical Colonization Deeper infection
N 0.42 (0.18-0.97)* by history S 5.00 (1.82-13.76)
E 5.36 (0.54-53.66) T 8.05 (2.90-22.38)
R 5.07 (1.7-14.83) O 2.76 (1.04-7.31)
D 5.63 (2.19-14.45) N 5.71 (1.79-18.21)
S 3.59 (1.22-10.58)
E 4.88 (1.79-13.27)
E 4.13 (1.72-9.91)
S 3.59 (1.22-10.58)
Clinicians often need to triangulate and look for 2 or 3 of these signs and symptoms
before they make a diagnosis of increased superficial bacterial burden.
Infection vs. peri-wound skin temperature
Skin Temperatures group II a & b
-2
0
2
4
6
8
10
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
One way AVOVA
between and within
wounded non-
infected
and infected
groups:
F = 44.238
Significance =
.000
0.5˚F 6.4˚F
Range
-0.5 -
8.7˚F
Mean
4.3 ˚F
+/-2.44
Range
-1.0-
3.0˚F
Mean
.383 ˚F
+/-.893
Fierheller Advances 2010
4 Point Technique Whole Wound Technique
3/2/2016
13
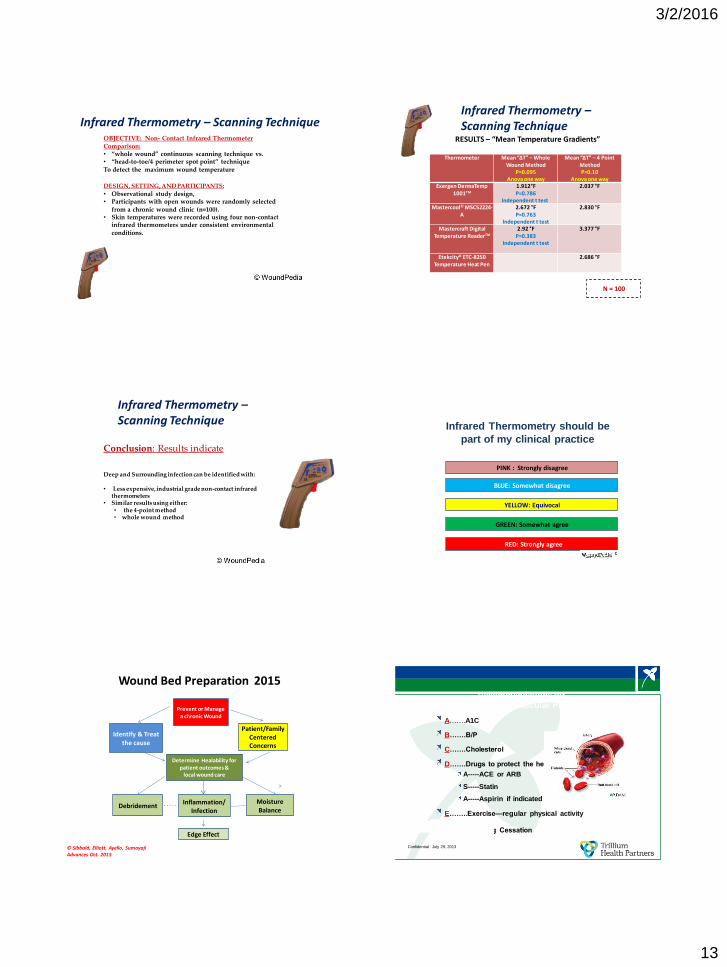
OBJECTIVE: Non- Contact Infrared Thermometer Comparison: • “whole wound” continuous scanning technique vs. • “head-to-toe/4 perimeter spot point” technique To detect the maximum wound temperature
DESIGN, SETTING, AND PARTICIPANTS:• Observational study design, • Participants with open wounds were randomly selected
from a chronic wound clinic (n=100). • Skin temperatures were recorded using four non-contact
infrared thermometers under consistent environmental conditions.
Infrared Thermometry – Scanning TechniqueRESULTS – “Mean Temperature Gradients”
Thermometer Mean “ΔT” – Whole Wound Method
P=0.095 Anova one way
Mean “ΔT” – 4 Point MethodP=0.10
Anova one way Exergen DermaTemp
1001TM
1.912°FP=0.786
Independent t test
2.037 °F
Mastercool© MSC52224-A
2.672 °FP=0.763
Independent t test
2.830 °F
Mastercraft Digital Temperature ReaderTM
2.92 °FP=0.383
Independent t test
3.377 °F
Etekcity® ETC-8250 Temperature Heat Pen
2.686 °F
N = 100
Infrared Thermometry –Scanning Technique
Conclusion: Results indicate
Deep and Surrounding infection can be identified with:
• Less expensive, industrial grade non-contact infrared thermometers
• Similar results using either:• the 4-point method • whole wound method
Infrared Thermometry –Scanning Technique
Infrared Thermometry should be
part of my clinical practice
YELLOW: Equivocal
GREEN: Somewhat agree
?RED: Strongly agree
BLUE: Somewhat disagree
PINK : Strongly disagree
Wound Bed Preparation 2015
Prevent or Manage a chronic Wound
Identify & Treat the cause
Patient/Family Centered Concerns
Determine Healability for patient outcomes &
local wound care
DebridementInflammation/
Infection
Moisture Balance
Edge Effect
© Sibbald, Elliott, Ayello, SumayajiAdvances Oct. 2015
Confidential July 29, 2013
Recommendations for
Treat the Cause: Vascular Protection
A…….A1C
B…….B/P
C…….Cholesterol
D…….Drugs to protect the heart
A-----ACE or ARB
S-----Statin
A-----Aspirin if indicated
E……..Exercise—regular physical activity
S……..Smoking Cessation

3/2/2016
14
What is HbA1c and what does it reflect?
• average blood sugar over 3 month period– Lifespan of red blood cell
(RBC)
• Glycation of hemoglobin irreversible– average level of glucose to
which RBC exposed
Nathan DM et al. Diabetes Care 31 (8): 1473–8
What is the A1C?
Blood test
which shows
average blood
sugar over
past 3 months
What is
your
A1C (%) ?
Your Average Blood Sugar
13 18 - 19 324-342
12 16 - 17 288-301
11 14 - 15 252-270
10 13 - 14 234-252
9 11 - 12 198-216
8 10 - 11 180-198
7 8 - 9 144-162
6 7 126
mmol/L mg/dl
Translating the hemoglobin A1c assay into estimated av erage glucose v alues
Dav id M. Nathan, Judith Kuenen, Rikke Borg, Hui Zheng, Dav id Schoenf eld, and Robert J. Heine, f or the A1c-Deriv ed Av erage Glucose
(ADAG) Study Group. Diabetes Care 2008 . Av erage Blood Glucose (mmol) = 1.59 x A1C - 2.59
MH CCACCWCA 2012-Diabetes Related Data
19.3
25.655
Client with Foot Ulcers: Has the client had HbA1c
assessment in the last year
Yes
No
Toronto Regional Wound Healing Clinic Inc2016-03-02
HbA1c blood test measures the percentageof red blood cells that have glucose attached. Normal levels for people with Diabetes is <7.0%.HbA1c should be monitored regularly by physician and patient.
VIPS of Treat the Cause
Vascular
Insufficiency
Inflammation and /
or Infection
Pressure
downloading
Sharp Surgical
debridement
3/2/2016
Diagnostic tests VASCULAR SUPPLY AND HEALING ABILITY
Palpable pulse >80 mm Hg
Ankle-brachial
pressure index
(ABPI)
>0.5 and <1.3
Transcutaneous
O2 tension>30 mm Hg
Toe pressure >55 mm Hg
Audible hand
held Doppler
Triphasic,
Biphasic Sound

3/2/2016
15
AUDIBLE HAND HELD DOPPLER ULTRASOUND DETERMINES RELIABLE & INEXPENSIVE EXCLUSION OF SIGNIFICANT PVD
ALAVI A, SIBBALD RG, NABAVIZADEH R, VALAEI F, COUTTS P, MAYER DVASCULAR. 2015 JAN 27. PII: 1708538114568703. EPUB AHEAD OF PRINT
• Accuracy audible hand held
Doppler ultrasound (AHHD)to identify PVD
• 200 patients, 379 legs
• All had ABPI, toe pressures at
certified vascular lab
(Gold Standard)
Criteria Meaning Result PT/ DP
Specificity No PVD 98.6%/ 97.8%
Sensitivity PVD identified 37.5% / 30.19%
+ Pre.Value (PPV) Abn. AHHD
+ PVD
81.2%/ 72.75%
- Pre. Value (NPV) Normal AHHD/
no PVD
90.91%/ 88.10%
Conclusion: AHHD reliable, simple, rapid,
inexpensive bedside exclusion test
PVD in Diabetic/ non-diabetic subjects
The gold standard of plantar pressure
redistribution is:
YELLOW: Irremovable cast walker
PINK: Contact cast
?RED: Deep toed shoes and custom
orthotics
BLUE: Orthopedic plaster of Paris cast
GREEN: Removable Cast Walker
Plantar Pressure Redistribution
Group A: Walking casts
Pneumatic walker
Contact cast
Group B: Special Shoes
Med- Surg. Shoe
Rocker soles
Special half shoes
Group C: Home Made
Simple materials/ modifications
Option D: With Caution
Surgical pressure
offloading
Group A
Group B
Group C
Downloading % healed Time (days)
RCW 51.9 58.0 +/- 15.2
ITCC 82.6 41.6 +/- 18.7
MH CCACCWCA 2012
Toronto Regional Wound Healing Clinic Inc
139/240 clients with Foot Ulcers were without plantar pressure redistribution.
Examples- Demonstrations of Foot Wear
90
3/2/2016
16
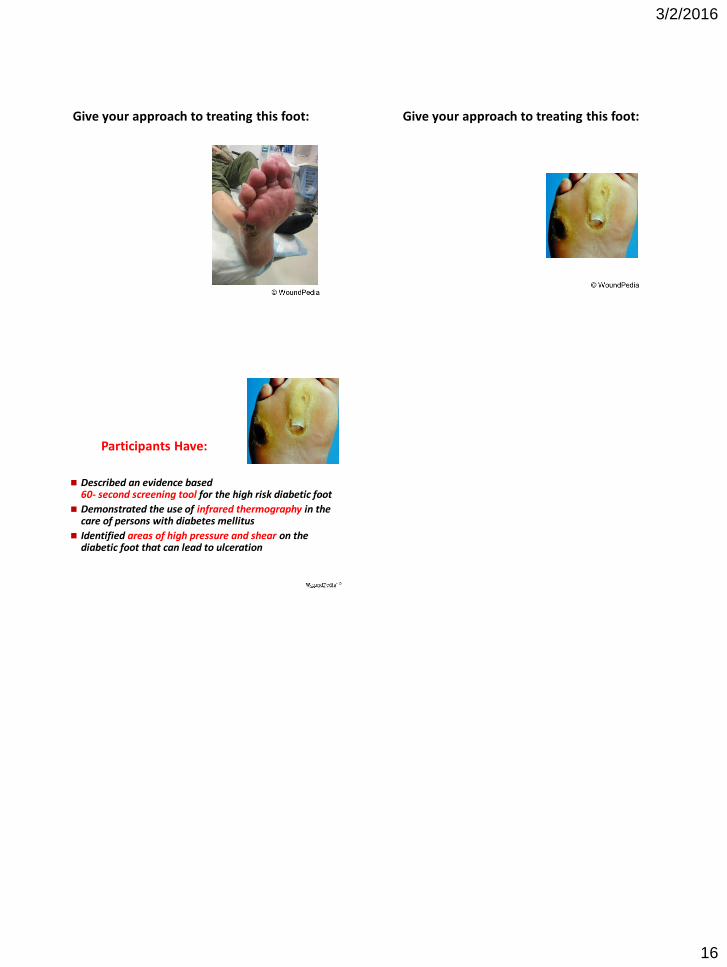
Give your approach to treating this foot: Give your approach to treating this foot:
Participants Have:
Described an evidence based 60- second screening tool for the high risk diabetic foot
Demonstrated the use of infrared thermography in the care of persons with diabetes mellitus
Identified areas of high pressure and shear on the diabetic foot that can lead to ulceration
Related Documents











