8/25/2014 1 Dyspnea in Lung Cancer Jason Akulian, MD MPH Director, Interventional Pulmonology Assistant Professor of Medicine University of North Carolina at Chapel Hill Disclosures None Acknowledgements • David Feller-Kopman, MD • Lonny Yarmus, DO Objectives Etiology Diagnosis Initial stabilization Strategic considerations • modalities • multidisciplinary airway team

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/25/2014
1
Dyspnea in Lung Cancer
Jason Akulian, MD MPH Director, Interventional Pulmonology
Assistant Professor of Medicine University of North Carolina at Chapel Hill
Disclosures
None
Acknowledgements
• David Feller-Kopman, MD
• Lonny Yarmus, DO
Objectives
Etiology
Diagnosis
Initial stabilization
Strategic considerations
• modalities
• multidisciplinary airway team
8/25/2014
2
Etiology of dyspnea in lung cancer
Pneumonia
Stress/Anxiety
Pulmonary embolism
Radiation pneumonitis
Airway obstruction
Pleural/Pericardial effusions
Pneumonia
Cough
Sputum production
Fever
Pleuritic chest pain
Increased risk with some chemotherapeutics
Clinical diagnosis
Treated – Broad spectrum Abx
Stress/Anxiety
Hyperventilation
Often associated with “cardiac like” symptoms
• Feeling of doom or being overwhelmed
Very normal
Diagnosis of exclusion
Treated with anxiolytics and behavioral
modification
8/25/2014
3
Pulmonary embolism
Sudden onset dyspnea
Chest pain
Leg pain
Increased risk in malignancy
Diagnosed via clinical history and imaging studies
Treated with anticoagulants
Radiation pneumonitis
Cough (typically non-productive)
Delayed onset
Diagnosed via history and imaging
Treated with corticosteroids
Central Airway Obstruction: Symptoms
Depend on cause and comorbidities
Rapid onset vs. gradual
Wheezing • potential for misdiagnosis
• often refractory to bronchodilators, unilateral
Exacerbated by infections
Result in infection
Dyspnea on exertion: airway < 8 mm
Stridor: airway < 5 mm
Respiratory distress
Hollingsworth, Clin Chest Med 1987; 8: 231
8/25/2014
4
Non-malignant causes of central airway obstruction
Goiter
Lymphadenopathy
Granulation tissue
Infection
Amyloid
Vascular compression
Foreign bodies
Mucus plug
Sarcoidosis
Relapsing polychondritis
Iatrogenic
• stents
• stenosis post-intubation /
tracheostomy / XRT
Malignant causes of central airway obstruction
Bronchogenic CA • 20 – 30% will develop CAO
• up to 40% of deaths are due to loco-regional disease
Metastatic disease to airway • renal
• breast
• thyroid
• colon
• melanoma
• lymphadenopathy
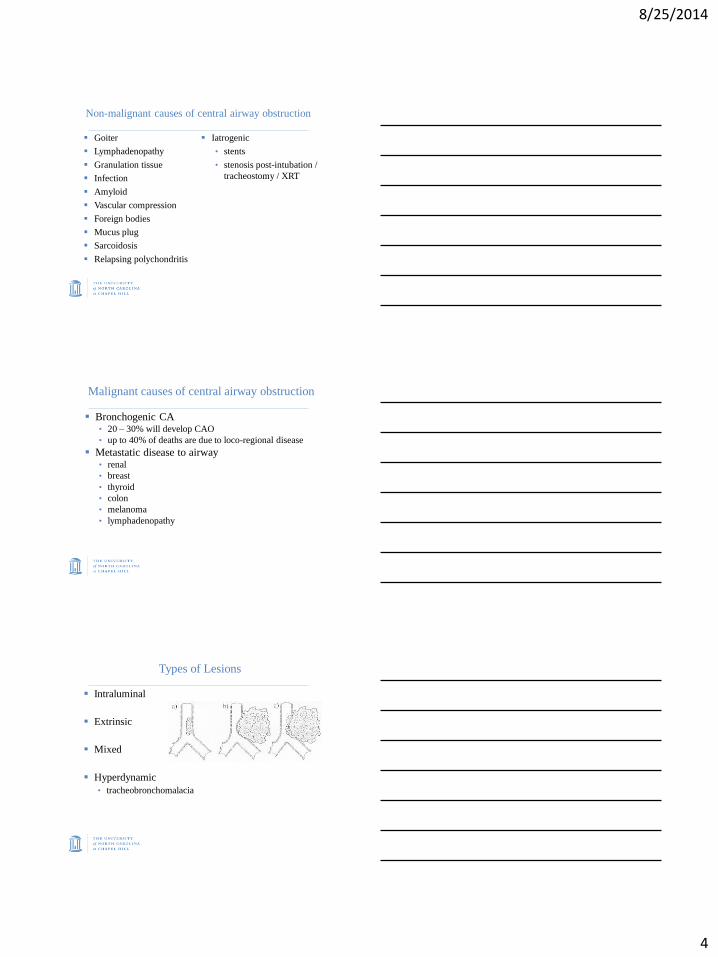
Types of Lesions
Intraluminal
Extrinsic
Mixed
Hyperdynamic
• tracheobronchomalacia
8/25/2014
5
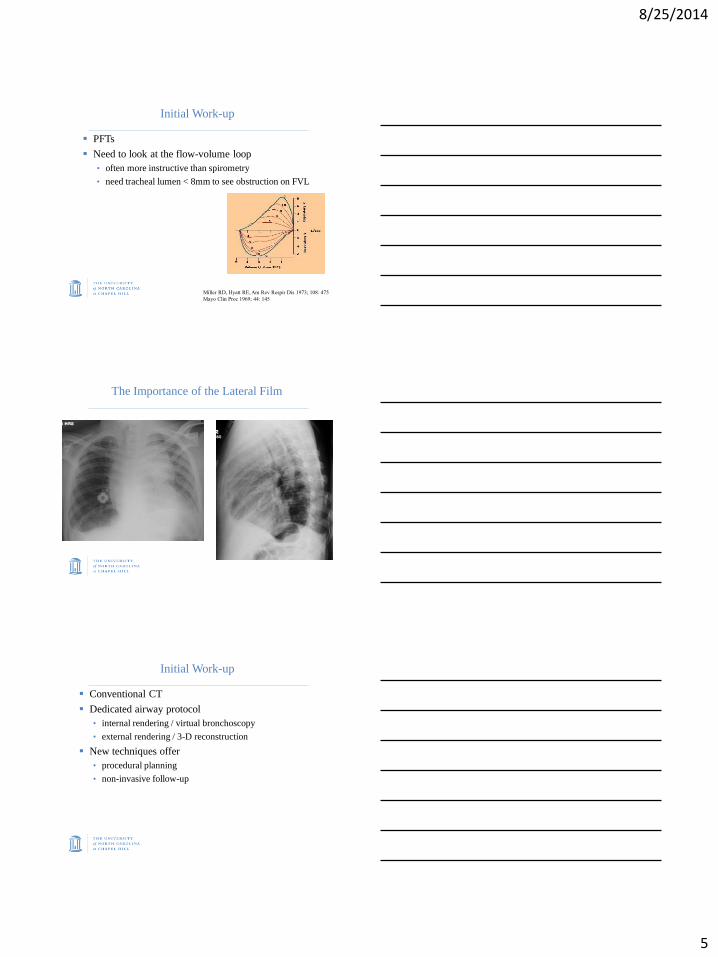
Initial Work-up
PFTs
Need to look at the flow-volume loop
• often more instructive than spirometry
• need tracheal lumen < 8mm to see obstruction on FVL
Miller RD, Hyatt RE, Am Rev Respir Dis 1973; 108: 475
Mayo Clin Proc 1969; 44: 145
The Importance of the Lateral Film
Initial Work-up
Conventional CT
Dedicated airway protocol
• internal rendering / virtual bronchoscopy
• external rendering / 3-D reconstruction
New techniques offer
• procedural planning
• non-invasive follow-up
8/25/2014
6
Initial Work-up: Flexible Bronchoscopy
Need:
• stable patient
• access to advanced airway management
More than complimentary to the CT
• can provide a tissue diagnosis
Main risk: conversion of relatively stable patient to an unstable patient
• therefore recommend its use only in patients with a secure airway
Initial Stabilization
Determine patient’s prognosis and wishes
Oxygen, morphine
Heliox at bedside
• lowers Reynolds number reduced tendency for turbulent
flow lower driving pressure to achieve a given flow /
increase in flow at same driving pressure
Bulk of data is in pediatric literature
Ho et al. Resuscitation; 52:297-300
Rigid Bronchoscopy
Gustav Killian, 1898
Ability to:
• oxygenate
• ventilate
• large bore suction
• dilate
• use other therapeutic
modalities
Mehta et.al., Chest 1993; 104: 673
Noppen et.al., Chest 1997; 112: 1136
Sheski et.al., Chest 1998; 114: 796
0
10
20
30
40
50
60
70
80
90
100
Per
cent
Years
Rigid
Flexible
8/25/2014
7
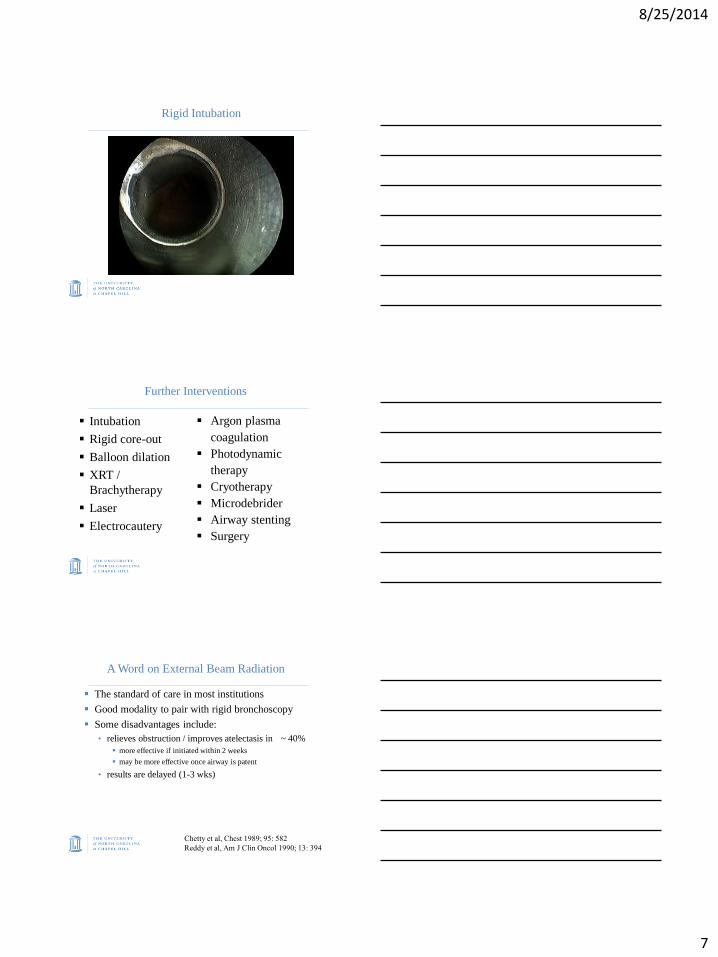
Rigid Intubation
Further Interventions
Intubation
Rigid core-out
Balloon dilation
XRT /
Brachytherapy
Laser
Electrocautery
Argon plasma
coagulation
Photodynamic
therapy
Cryotherapy
Microdebrider
Airway stenting
Surgery
A Word on External Beam Radiation
The standard of care in most institutions
Good modality to pair with rigid bronchoscopy
Some disadvantages include:
• relieves obstruction / improves atelectasis in ~ 40%
more effective if initiated within 2 weeks
may be more effective once airway is patent
• results are delayed (1-3 wks)
Chetty et al, Chest 1989; 95: 582
Reddy et al, Am J Clin Oncol 1990; 13: 394
8/25/2014
8
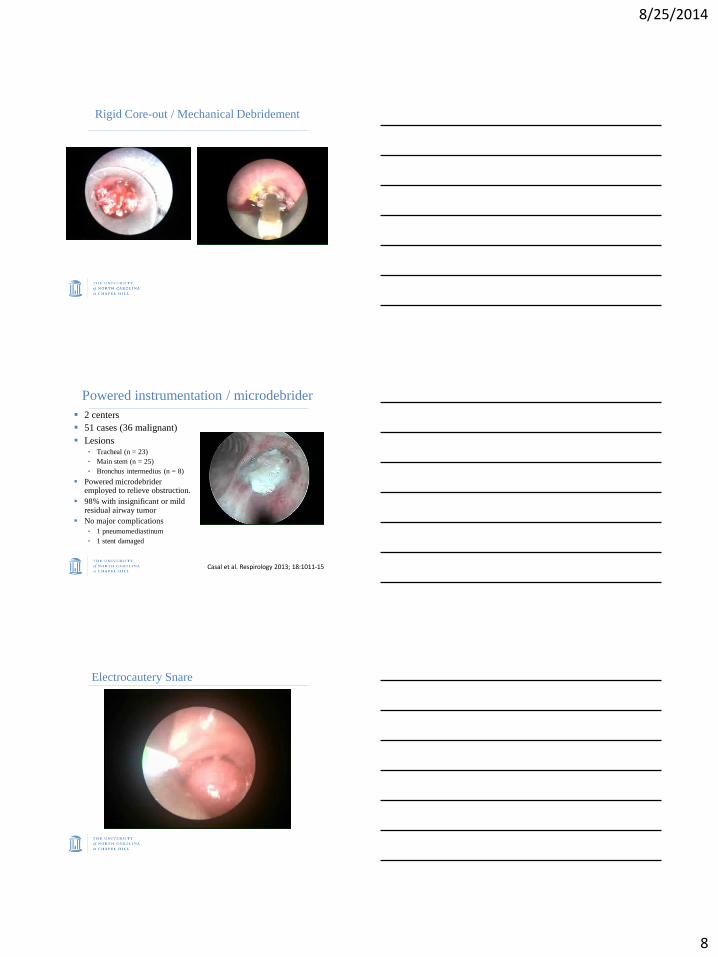
Rigid Core-out / Mechanical Debridement
Powered instrumentation / microdebrider
2 centers
51 cases (36 malignant)
Lesions • Tracheal (n = 23)
• Main stem (n = 25)
• Bronchus intermedius (n = 8)
Powered microdebrider employed to relieve obstruction.
98% with insignificant or mild residual airway tumor
No major complications
• 1 pneumomediastinum
• 1 stent damaged
Casal et al. Respirology 2013; 18:1011-15
Electrocautery Snare
8/25/2014
9
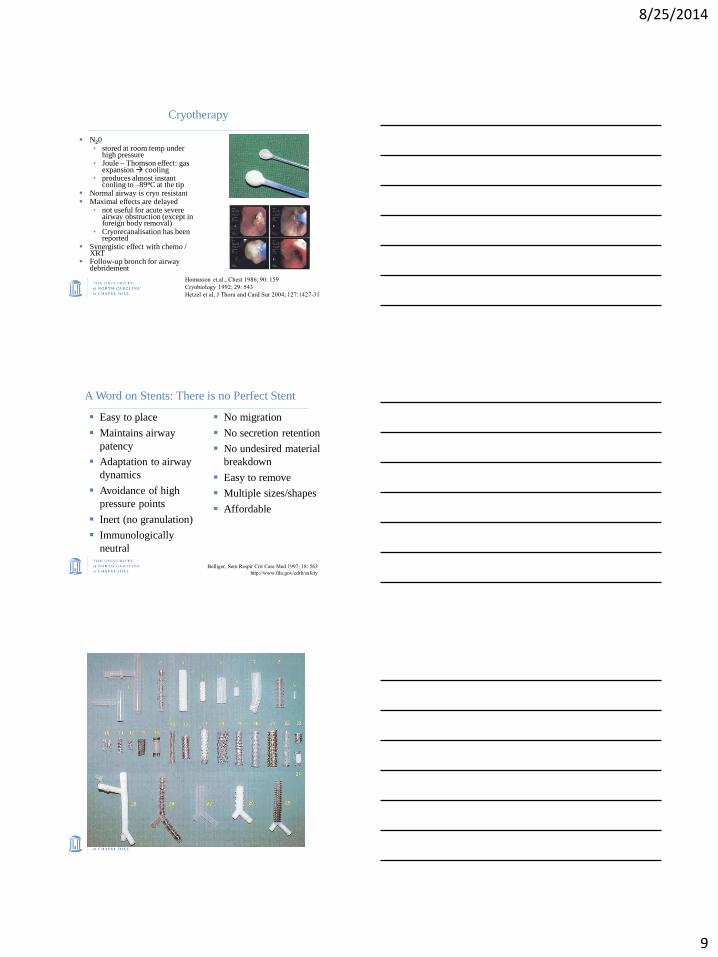
Cryotherapy
N20 • stored at room temp under
high pressure • Joule – Thomson effect: gas
expansion cooling • produces almost instant
cooling to –89oC at the tip Normal airway is cryo resistant Maximal effects are delayed
• not useful for acute severe airway obstruction (except in foreign body removal)
• Cryorecanalisation has been reported
Synergistic effect with chemo / XRT
Follow-up bronch for airway debridement
Homasson et.al., Chest 1986; 90: 159
Cryobiology 1992; 29: 543
Hetzel et al, J Thora and Card Sur 2004; 127:1427-31
A Word on Stents: There is no Perfect Stent
Easy to place
Maintains airway
patency
Adaptation to airway
dynamics
Avoidance of high
pressure points
Inert (no granulation)
Immunologically
neutral
No migration
No secretion retention
No undesired material
breakdown
Easy to remove
Multiple sizes/shapes
Affordable
Bolliger, Sem Respir Crit Care Med 1997; 18: 563
http://www.fda.gov/cdrh/safety
8/25/2014
10
56% of patients in respiratory failure can be
successfully extubated post procedure
Of those not intubated, 71% with immediate
reduction in level of care
Mortality is dependent on the success of airway
intervention
• 6m if airway patency restored c/w 1m if not
Outcomes
Colt et al, CHEST 1997; 112:202
Gelb et al, Ann Thorac Surg 1986; 43:164
Retrospective review of 12 patients.
Intubated and mechanically ventilated with inoperable or un-resectable CAO from NSCLC.
91% airway patency restored.
75% immediately extubated or removed from mechanical ventilation.
Median survival 228 days.
Median survival 313 days in patients extubated within 24 hours of therapeutic bronchoscopy.
Outcomes
Murgu et al. Respiration 2012; 84:55
Patients with ‘imminent suffocation’ due to CAO
that receive airway stents live a mean of 11 more
weeks.
• no increase in ‘prolonged suffering’
• 80% died at home
• majority from non-respiratory causes
Patient with CAO treated with rigid bronchoscopy
and standard Rx had similar outcomes to those
without CAO.
Outcomes cont.
Vonk-Noordegraaf et al, Chest 2001; 120:1811
Chhajed et al, Chest 2006; 130:1803
8/25/2014
11
36 patients underwent emergency airway
intervention for malignant obstruction.
Dyspnea relieved in 34/36 (94.4%).
61.8% underwent addition definitive therapeutic tx.
Patients who received additional definitive therapy
had significantly longer survival (38.2 vs. 6.2
months, p<0.001)
Outcomes
Jeon et al. J Thorac Oncol 2006; 1:319
74 patients with resectable disease and central
airway obstruction
• FEV1 1.7L 2.2L
• sleeve lobectomy or bi-lobectomy able to be
performed in 57% after rigid bronch
Therapeutic Bronchoscopy Can Allow for Surgical Cure
Chhajed et al, Ann Thorac Surg 2006; 81:1839
Surgical Resection / Reconstruction
Reserved for severe benign and relatively short
lesions
• Sleeve resection
• Lobectomy
Occasionally in malignant disease: carcinoid,
mucoepidermoid & adenocystic
Patient selection is crucial
• ‘surgeon selection’ just as important
8/25/2014
12
Malignant Effusions
2nd leading cause of exudative effusions
• ~ 200,000 / yr in US
75% are due to lung, breast and lymphoma
• 20% of patients with non-Hodgkin's and 30% of patients with Hodgkin's will develop an effusion during their illness
ATS, AJRCCM 2000; 162: 1987
Antunes et al, Thorax 2003; 58(sII): ii29
Heffner, Respirology 2008; 13:5
Prognosis
417 patients
• median survival 4.0 months
optimistic as all pts were candidates for pleurodesis
• most important predictor = primary tumor
2.3 months for GI primaries
3 months for lung CA
5.0 months for breast CA / unknown primary
6.0 months for mesothelioma
Heffner et al, Chest 2000; 117: 79
8/25/2014
13
Clinical Features
Dyspnea: up to 96%
• 1o due to large effusion alteration in chest wall P-V curve
Cough: 43%
• hemoptysis + effusion suggest bronchogenic CA
Chest pain
Weight loss
Fever
Up to 25% are asymptomatic (initially)
Chernow, Sahn, Am J Med 1977; 63: 695
Marel et al, Chest 1995; 107: 1598
Sahn, Clin Chest Med 1998; 19: 351
At Initial Thoracentesis:
Fully drain the pleural space
• no chest discomfort
• normal manometry
• use ultrasound
Does it relieve dyspnea ?
Does lung expand ?
How quickly does fluid return ?
• treat early
Feller-Kopman et al, Chest 2006; 129: 1556
Feller-Kopman et al, Ann Thorac Surg 2007;
Treatment: The Holy Grail
EARLY pleural palliation
• no further dyspnea
• no additional pleural procedures
Antunes et al, Thorax 2003; 58(suppl II): ii29
8/25/2014
14
Treatment Options
Palliation
• O2 / MSO4
Observation
• for asymptomatic patients, most will progress
Repeat thoracentesis
• relief of dyspnea, 100% recurrence at 1 month
• reserved for the sick ones
Antunes et al, Thorax 2003; 58(suppl II): ii29
ATS, AJRCCM 2000; 162: 1987
Light, Pleural Disease, 4th ed
Treatment Options
Chemo
• tap effusion first: accumulation of drugs can
increase toxicity
• intrapleural chemo
XRT
Pleurodesis
Tunneled pleural catheter
Antunes et al, Thorax 2003; 58(suppl II): ii29
ATS, AJRCCM 2000; 162: 1987
Light, Pleural Disease, 4th ed
Shoji et.al., Chest 2002; 121: 821
Talc
Success rates up to 95%
Inexpensive
Primary side effect: fever in 16 – 69%
• much less pain than tetracyclines
Schulze et.al., Ann Thorac Surg 2001; 71: 1809
de Campos et.al., Chest 2001; 119: 801
Viallat et.al., Chest 1996; 11: 1387
Cardillo et.al., Eur J Cardiothorac Surg 2002; 21: 302
8/25/2014
15
Talc: Mechanisms
Induces an inflammatory response
Induces expression of chemokines and ICAM-1
• IL-8 mediated neutrophil and monocyte influx
Increases bFGF
Induces apoptosis in tumor cells
Induces endostatin production by mesothelial cells
• inhibits angiogenesis
• induces apoptosis / reduces tumor growth
Weissberg et al, J Thorac Cardiovasc Surg 1993; 106: 689
Hamm, Light, Eur Respir J 1997; 10: 1648
Xie et al, Am J Respir Crit Care Med 1998; 157: 1441
Nasreen et al, Am J Respir Crit Care Med 1998; 158: 971
Nasreen et al, Am J Respir Crit Care Med 2000; 161: 595
Antony et al, Chest 2004; 126: 1522
Najmunnisa et al, Eur Respir J 2007; 29: 761
Medical Thoracoscopy vs VATS
‘Medical’ aka ‘pleuroscopy’ – in procedure suite with
moderate sedation and
supplemental O2
– single port
– avoids the lung and visceral
pleura
– single port
– less expensive
‘Surgical’ (VATS) – in OR with general
anesthesia (usually) single or double-lung
ventilation
– better for complex pleural
spaces
– single or multi-port
– can apply positive
pressure +/- decortication
Colt, Clin Chest Med 1995; 16: 505
Danby et.al., Chest 1998; 113: 739
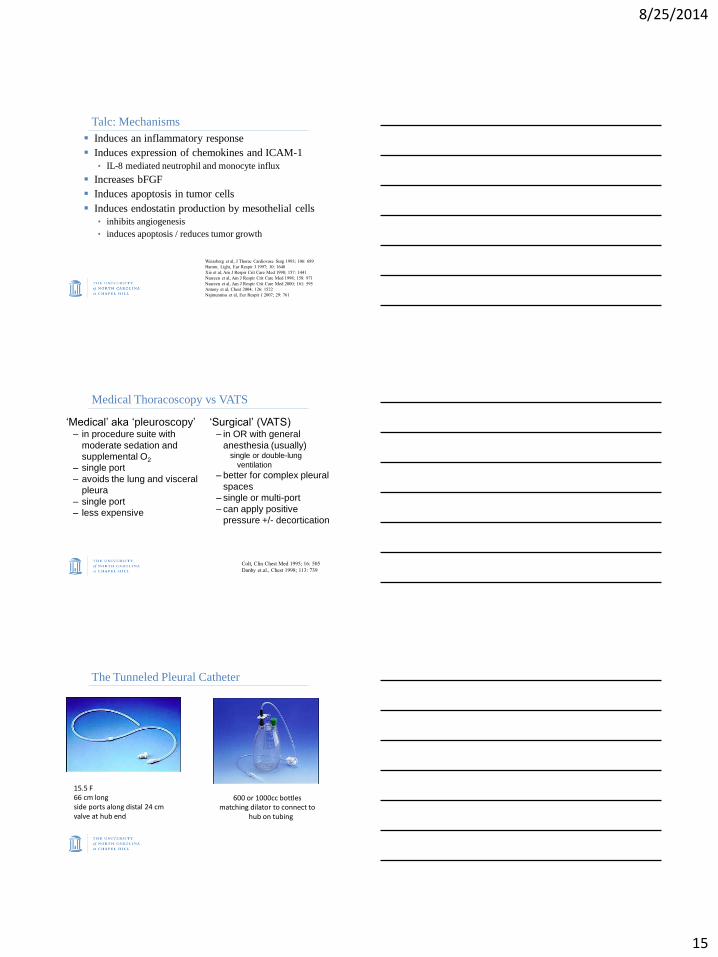
The Tunneled Pleural Catheter
15.5 F 66 cm long side ports along distal 24 cm valve at hub end
600 or 1000cc bottles matching dilator to connect to
hub on tubing
8/25/2014
16
Does it Work? 250 catheters placed in 223 patients
Complete or partial symptom control in 89%
Catheter duration: median of 56 days
Spontaneous pleurodesis occurred in 42.9%
• up to 72% in patients with breast / GYN CA
No further interventions in 90%
Risk of infection 2-4%
Tremblay, Chest 2006; 362-368
Warren et al, Eur J Cardiothorac Surg 2009; 33:89
Warren et al, Ann Thorac Surg 2008; 85:1049
Pros:
• effective
• minimally invasive
• one-stop shopping
Cons:
• 3-5d hospitalization
• need to prove full lung re-expansion prior to procedure
Pros:
• effective
• treatment of choice for lung entrapment
• outpatient procedure
Cons:
• need to care for / deal with the catheter
• potentially life long
Tunneled Pleural
Catheter Thoracoscopic Talc
Poudrage

8/25/2014
17
Combined Pleurx / Pleurodesis
30 patients: talc & pleurX
Chest tube removed at 24.4 hours
Median hospital LOS post procedure: 1.79d
Pleurodesis was achieved in 92%
PleurX removed: median 7.5 days
Mean Borg: 5.7 pre 1.5 post
Mean KPS: 56 pre 72 post
Reddy et.al.Chest 2011 [in press]
The Future: A Multi-pronged Approach
Target tumor cells with chemo +/- gene Rx
• replication-deficient recombinant adenovirus containing
HSVtk sensitivity to GCV
• adenoviral vector-INFβ in 7 pts with MPM and 3 with
MPE
Inhibit angiogenesis
• VEGF inhibitors
Augment anti-angiogenesis
• endostatin
Induce pleural fibrosis
• TGF- 2
Team Approach
Oncology
Interventional Pulmonologist
Thoracic Surgery
Chest Radiology
Radiation Oncology
ENT
8/25/2014
18
Conclusions
Dyspnea related to lung cancer is often
multifactorial
Common things are common
• Pulmonary embolism
• COPD exacerbation
• Pneumonia
Dyspnea from central airway obstruction and
malignant pleural effusions are often easily
palliated
Jason Akulian, MD MPH Director, Interventional Pulmonology
UNC Division of Pulmonary and Critical Care Medicine
8007 Burnett Womack Bldg.
Chapel Hill, NC 27599
(o) 919-966-2531
Related Documents











