2380 I dentification and treatment of atrial fibrillation (AF) is a key priority in the secondary stroke prevention manage- ment of patients with ischemic stroke or transient ischemic attack (TIA). One in every 4 patients with ischemic stroke has no specific cause evident after standard investigations (cryptogenic), and the usual treatment is antiplatelet therapy. 1 Paroxysmal AF is often suspected in patients with crypto- genic embolic strokes, but it routinely goes underdiagnosed and undertreated in practice because screening methods have typically been limited to short-duration (eg, 24 hours) ECG monitoring post stroke. 2 Prolonged ambulatory monitoring has become increas- ingly feasible with recent advances in ECG device tech- nologies, and it has now been shown in randomized trials to significantly improve AF detection and lead to increased anticoagulant treatment rates in patients with stroke or TIA. 2–4 However, its cost-effectiveness is uncertain and likely varies by device, monitoring duration, and patient characteristics. 5–8 Such data are needed to inform clinical practice and health policy decisions about the optimal monitoring strategies for secondary stroke prevention. Decision analytic modeling can provide insights into the comparative long-term clinical and Background and Purpose—Prolonged ambulatory ECG monitoring after cryptogenic stroke improves detection of covert atrial fibrillation, but its long-term cost-effectiveness is uncertain. Methods—We estimated the cost-effectiveness of noninvasive ECG monitoring in patients aged ≥55 years after a recent cryptogenic stroke and negative 24-hour ECG. A Markov model used observed rates of atrial fibrillation detection and anticoagulation from a randomized controlled trial (EMBRACE) and the published literature to predict lifetime costs and effectiveness (ischemic strokes, hemorrhages, life-years, and quality-adjusted life-years [QALYs]) for 30-day ECG (primary analysis) and 7-day or 14-day ECG (secondary analysis), when compared with a repeat 24-hour ECG. Results—Prolonged ECG monitoring (7, 14, or 30 days) was predicted to prevent more ischemic strokes, decrease mortality, and improve QALYs. If anticoagulation reduced stroke risk by 50%, 30-day ECG (at a cost of USD $447) would be highly cost-effective ($2000 per QALY gained) for patients with a 4.5% annual ischemic stroke recurrence risk. Cost- effectiveness was sensitive to stroke recurrence risk and anticoagulant effectiveness, which remain uncertain, especially at higher costs of monitoring. Shorter duration (7 or 14 days) monitoring was cost saving and more effective than an additional 24-hour ECG; its cost-effectiveness was less sensitive to changes in ischemic stroke risk and treatment effect. Conclusions—After a cryptogenic stroke, 30-day ECG monitoring is likely cost-effective for preventing recurrent strokes; 14-day monitoring is an attractive value alternative, especially for lower risk patients. These results strengthen emerging recommendations for prolonged ECG monitoring in secondary stroke prevention. Cost-effectiveness in practice will depend on careful patient selection. (Stroke. 2016;47:2380-2385. DOI: 10.1161/STROKEAHA.115.011979.) Key Words: anticoagulant ◼ atrial fibrillation ◼ electrocardiography ◼ secondary prevention ◼ stroke Potential Cost-Effectiveness of Ambulatory Cardiac Rhythm Monitoring After Cryptogenic Stroke Jean Hai Ein Yong, MASc; Kednapa Thavorn, PhD; Jeffrey S. Hoch, PhD; Muhammad Mamdani, PharmD, MPH; Kevin E. Thorpe, MMath; Paul Dorian, MD; Mike Sharma, MD; Andreas Laupacis, MD; David J. Gladstone, MD, PhD; on behalf of the EMBRACE Steering Committee Received October 27, 2015; final revision received June 8, 2016; accepted June 15, 2016. From the Centre for Excellence in Economic Analysis Research (CLEAR), Toronto, ON, Canada (J.H.E.Y, J.S.H.); Applied Health Research Centre, Toronto, ON, Canada (K.E.T.); HUB Research Solutions, Li Ka Shing Centre for Healthcare Analytics Research and Training (LKS-CHART) (M.M.), Li Ka Shing Knowledge Institute, Toronto, ON, Canada (A.L.); St. Michael’s Hospital, Toronto, ON, Canada (P.D.); Clinical Epidemiology Program, Ottawa Hospital Research Institute, The Ottawa Hospital; School of Epidemiology, Public Health and Preventive Medicine, University of Ottawa; Institute of Clinical and Evaluative Sciences (ICES UOttawa), ON, Canada (K.T.); Institute of Health Policy, Management, and Evaluation (J.S.H., M.M., A.L.), Dalla Lana School of Public Health (K.E.T.), Leslie Dan Faculty of Pharmacy (J.S.H., M.M.), Division of Neurology (D.J.G.), and Department of Medicine (M.M., P.D., A.L., D.J.G.), University of Toronto, ON, Canada; Department of Public Health Sciences and Center for Healthcare Policy and Research, University of California, Davis, CA (J.S.H.); Division of Neurology, Department of Medicine, McMaster University, Hamilton, ON, Canada (M.S.); and Division of Neurology, Department of Medicine, Hurvitz Brain Sciences Program, and Regional Stroke Centre, Sunnybrook Health Sciences Centre and Sunnybrook Research Institute, Toronto, ON, Canada (D.J.G.). The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 115.011979/-/DC1. Correspondence to David J. Gladstone, MD, PhD, Regional Stroke Prevention Clinic, Sunnybrook Health Sciences Centre, A442-2075 Bayview Ave, Toronto, ON, Canada M4N 3M5. E-mail [email protected] © 2016 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.115.011979 by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from by guest on June 30, 2018 http://stroke.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2380
Identification and treatment of atrial fibrillation (AF) is a key priority in the secondary stroke prevention manage-
ment of patients with ischemic stroke or transient ischemic attack (TIA). One in every 4 patients with ischemic stroke has no specific cause evident after standard investigations (cryptogenic), and the usual treatment is antiplatelet therapy.1 Paroxysmal AF is often suspected in patients with crypto-genic embolic strokes, but it routinely goes underdiagnosed and undertreated in practice because screening methods have typically been limited to short-duration (eg, 24 hours) ECG monitoring post stroke.2
Prolonged ambulatory monitoring has become increas-ingly feasible with recent advances in ECG device tech-nologies, and it has now been shown in randomized trials to significantly improve AF detection and lead to increased anticoagulant treatment rates in patients with stroke or TIA.2–4 However, its cost-effectiveness is uncertain and likely varies by device, monitoring duration, and patient characteristics.5–8 Such data are needed to inform clinical practice and health policy decisions about the optimal monitoring strategies for secondary stroke prevention. Decision analytic modeling can provide insights into the comparative long-term clinical and
Background and Purpose—Prolonged ambulatory ECG monitoring after cryptogenic stroke improves detection of covert atrial fibrillation, but its long-term cost-effectiveness is uncertain.
Methods—We estimated the cost-effectiveness of noninvasive ECG monitoring in patients aged ≥55 years after a recent cryptogenic stroke and negative 24-hour ECG. A Markov model used observed rates of atrial fibrillation detection and anticoagulation from a randomized controlled trial (EMBRACE) and the published literature to predict lifetime costs and effectiveness (ischemic strokes, hemorrhages, life-years, and quality-adjusted life-years [QALYs]) for 30-day ECG (primary analysis) and 7-day or 14-day ECG (secondary analysis), when compared with a repeat 24-hour ECG.
Results—Prolonged ECG monitoring (7, 14, or 30 days) was predicted to prevent more ischemic strokes, decrease mortality, and improve QALYs. If anticoagulation reduced stroke risk by 50%, 30-day ECG (at a cost of USD $447) would be highly cost-effective ($2000 per QALY gained) for patients with a 4.5% annual ischemic stroke recurrence risk. Cost-effectiveness was sensitive to stroke recurrence risk and anticoagulant effectiveness, which remain uncertain, especially at higher costs of monitoring. Shorter duration (7 or 14 days) monitoring was cost saving and more effective than an additional 24-hour ECG; its cost-effectiveness was less sensitive to changes in ischemic stroke risk and treatment effect.
Conclusions—After a cryptogenic stroke, 30-day ECG monitoring is likely cost-effective for preventing recurrent strokes; 14-day monitoring is an attractive value alternative, especially for lower risk patients. These results strengthen emerging recommendations for prolonged ECG monitoring in secondary stroke prevention. Cost-effectiveness in practice will depend on careful patient selection. (Stroke. 2016;47:2380-2385. DOI: 10.1161/STROKEAHA.115.011979.)
Key Words: anticoagulant ◼ atrial fibrillation ◼ electrocardiography ◼ secondary prevention ◼ stroke
Potential Cost-Effectiveness of Ambulatory Cardiac Rhythm Monitoring After Cryptogenic Stroke
Jean Hai Ein Yong, MASc; Kednapa Thavorn, PhD; Jeffrey S. Hoch, PhD; Muhammad Mamdani, PharmD, MPH; Kevin E. Thorpe, MMath; Paul Dorian, MD;
Mike Sharma, MD; Andreas Laupacis, MD; David J. Gladstone, MD, PhD; on behalf of the EMBRACE Steering Committee
Received October 27, 2015; final revision received June 8, 2016; accepted June 15, 2016.From the Centre for Excellence in Economic Analysis Research (CLEAR), Toronto, ON, Canada (J.H.E.Y, J.S.H.); Applied Health Research Centre,
Toronto, ON, Canada (K.E.T.); HUB Research Solutions, Li Ka Shing Centre for Healthcare Analytics Research and Training (LKS-CHART) (M.M.), Li Ka Shing Knowledge Institute, Toronto, ON, Canada (A.L.); St. Michael’s Hospital, Toronto, ON, Canada (P.D.); Clinical Epidemiology Program, Ottawa Hospital Research Institute, The Ottawa Hospital; School of Epidemiology, Public Health and Preventive Medicine, University of Ottawa; Institute of Clinical and Evaluative Sciences (ICES UOttawa), ON, Canada (K.T.); Institute of Health Policy, Management, and Evaluation (J.S.H., M.M., A.L.), Dalla Lana School of Public Health (K.E.T.), Leslie Dan Faculty of Pharmacy (J.S.H., M.M.), Division of Neurology (D.J.G.), and Department of Medicine (M.M., P.D., A.L., D.J.G.), University of Toronto, ON, Canada; Department of Public Health Sciences and Center for Healthcare Policy and Research, University of California, Davis, CA (J.S.H.); Division of Neurology, Department of Medicine, McMaster University, Hamilton, ON, Canada (M.S.); and Division of Neurology, Department of Medicine, Hurvitz Brain Sciences Program, and Regional Stroke Centre, Sunnybrook Health Sciences Centre and Sunnybrook Research Institute, Toronto, ON, Canada (D.J.G.).
The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 115.011979/-/DC1.
Correspondence to David J. Gladstone, MD, PhD, Regional Stroke Prevention Clinic, Sunnybrook Health Sciences Centre, A442-2075 Bayview Ave, Toronto, ON, Canada M4N 3M5. E-mail [email protected]
© 2016 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.115.011979
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Yong et al Cost-Effectiveness of ECG Monitoring After Cryptogenic Stroke 2381
cost-effectiveness of prolonged ECG monitoring by combin-ing available evidence.
Our primary objective was to estimate the potential cost-effectiveness of 30-day ECG monitoring (using an external auto-triggered event loop recorder) after a cryptogenic stroke or TIA and an initial negative 24-hour Holter ECG, compared with a repeat 24-hour ECG (Holter). Our secondary objectives were to assess the cost-effectiveness of 7-day and 14-day ECG against a repeat 24-hour ECG. We conducted an economic evaluation using data from the EMBRACE (30-Day Cardiac Event Monitor Belt for Recording Atrial Fibrillation After a Cerebral Ischemic Event) trial of 30-day noninvasive ECG monitoring in this population,3 combined with data from the published literature.
MethodsWe constructed a Markov cohort model to simulate disease progres-sion of patients who experienced a cryptogenic ischemic stroke or TIA within the preceding 6 months (Figure I in the online-only Data Supplement). Patient characteristics were based on the EMBRACE trial cohort (Table 1).3 In the base case, the analysis adopted a lifetime horizon. Patients entered the Markov model in the no event health state. The monitoring strategy determined the odds of detecting AF; patients’ AF and treatment status determined the clinical event rates (ischemic stroke, intracranial hemorrhage, major bleeding, and mortality). Patients’ quality of life declined after a clinical event. As patients moved through different health states every year, they accrued direct healthcare costs, life-years, and quality-adjusted life-years (QALYs). The risk of ischemic stroke and intracranial hemor-rhage increased with age.9,10 Stroke severity was classified according to the modified Rankin Scale. We discounted future clinical outcomes and costs at 5% per year.11
AssumptionsTo simplify the model, we made several assumptions that are con-sistent with those in previous cost-effectiveness analyses of antico-agulants for stroke prevention in AF9,12: (1) the efficacy of treatment remained constant over time unless patients discontinued treatment; (2) after an intracranial hemorrhage or major bleed, patients would switch to aspirin; and (3) patients who had a recurrent stroke or intra-cranial hemorrhage could only move to a health state with similar or greater disability; for example, patients with a mild stroke could develop a moderate stroke but not vice-versa.
AF Detection and Treatment RatesDetection rates were based on the observed primary outcome in EMBRACE: episodes of AF ≥30 s detected within 90 days after ran-domization (Table 1).3 In the EMBRACE intervention group, half of the AF cases were detected within the first 7 days of monitoring, and three quarters were detected within 14 days of monitoring.3 In that trial, 89% of patients with AF detected received an oral antico-agulant3; in sensitivity analysis, we varied this rate between 50% and 100%. We assumed 25% of anticoagulated patients received warfarin and 75% received a novel oral anticoagulant in the base case and varied novel oral anticoagulant use (25% to 100%) in sensitivity analyses.13 This assumption was based on recent practice patterns and expert opinion by clinicians to best reflect the current and future use of novel oral anticoagulants versus warfarin for such patients.
Clinical Event RatesEMBRACE detected mostly subclinical paroxysmal AF in patients with cryptogenic stroke.3 The annual risk of recurrent ischemic stroke in nonanticoagulated cryptogenic stroke patients is ≈3% to 8%1,14; the risk among those with subclinical AF is very likely higher than the average, but the exact rate is uncertain.15 In patients with previous
stroke or TIA and clinical AF (and similar CHADS2 scores as the
EMBRACE cohort) receiving aspirin, the estimated annual rate is ≈9%.3,16–18 We used a lower stroke risk (4.5% per year) for the base case, assuming that patients with subclinical AF have half the risk of ischemic stroke than patients with clinical AF.19,20 This estimate is also in line with the rate (4.8%) observed in subclinical AF patients with previous stroke or TIA (Jeff Healey, unpublished data, 2014).20 We varied this rate (2.5%–8.0%) in 1- and 2-way sensitivity analyses. Also, to reflect the uncertainty in this estimate, we assigned a larger confidence interval in probabilistic sensitivity analysis (Table I in the online-only Data Supplement).
For the base case, we estimated that oral anticoagulant therapy would reduce ischemic stroke risk by 50% over aspirin (Methods section in the online-only Data Supplement).17,21–23 The exact relative risk reduction is uncertain for subclinical AF because most patients with AF in anticoagulant trials had clinical AF; therefore, we var-ied the relative risk reduction (20%–60%) in sensitivity analyses and assigned a larger confidence interval in probabilistic sensitivity analysis.
Rates of intracranial hemorrhage (1.07% per year) and major bleeding (4.6% per year) for warfarin were estimated from patients with previous stroke or TIA receiving warfarin (Methods section in the online-only Data Supplement).24–27 Aspirin and novel oral anti-coagulants had lower risks of intracranial hemorrhage and major bleeding than warfarin.17,28,29 Mortality was age and sex specific.30 The target population had a higher risk of death than the general population (hazard ratio, 2.0); patients who had moderate to severe disability after stroke or intracranial hemorrhage had higher mortality risk than those with minor stroke or intracranial hemorrhage (hazard ratio, 2.0).31–34
Costs and UtilitiesThe analysis was undertaken from the perspective of a public health-care payer. In addition to AF monitoring costs, health state costs included costs of medication, international normalized ratio moni-toring, hospitalizations, physician services, emergency department visits, rehabilitation, home care, and long-term care (Methods sec-tion and Table II in the online-only Data Supplement). The first-year costs for ischemic stroke and intracranial hemorrhage came from studies of stroke costs35,36 and cost-effectiveness of anticoagulants for stroke prevention.12,33 Subsequent year costs were 60% of the first-year costs, based on long-term costing of stroke.33,37 The analysis used
Table 1. Model Inputs for the Base Case and Deterministic SA
Variable Base Case (SA)
Patient characteristics
Starting age, y 73 (55–80)
Sex (% female) 50%
CHADS2 distribution (2/3/4–6), % 16/42/42
Index event (ischemic stroke/TIA), % 67/33
Clinical event rates
AF detected at 90 d, 30-d ECG, % 16.1 (10.0–18.5)
AF detected at 90 d, 24-h repeat Holter, % 3.2 (1.5–6.0)
RR of intracranial hemorrhage (NOAC vs warfarin)
0.48 (0.40–0.55)
Odds ratio of intracranial hemorrhage (NOAC vs aspirin)
1.14 (1.00–2.00)
RR of overall major bleeding (NOAC vs warfarin) 0.86 (0.70–1.00)
RR of overall major bleeding (NOAC vs aspirin) 1.25 (1.00–1.50)
AF indicates atrial fibrillation; NOAC, new oral anticoagulants (apixaban, edoxaban, dabigatran, and rivaroxaban); RR, relative risk; SA, sensitivity analyses; and TIA, transient ischemic attack.
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

2382 Stroke September 2016
Canadian costs and converted the currency to US dollars using the rate of USD$1 to CAD$1.30. All costs were adjusted to 2014 dol-lars using the Consumer Price Index for health care.38 We estimated QALYs by weighting length of life with the general population utility score and health state–specific utility weight (Methods section and Table II in the online-only Data Supplement).
AnalysesTo assess cost-effectiveness, we calculated the incremental cost-effectiveness ratio, which is a ratio of incremental average costs between 2 strategies to the difference in their effect (QALYs). A strategy was considered highly cost-effective if it cost <$20 000 per QALY gained and low value if it cost ≥$100 000 per QALY gained.39 One- and 2-way sensitivity analyses were conducted by varying model inputs over a plausible range (Table 1; Tables I and II in the online-only Data Supplement) to assess their effects on the results. To validate our model, we performed logic checks by reviewing the results of 1-way sensitivity analyses. Probabilistic sensitivity analysis was performed to characterize uncertainty by randomly sampling the model inputs 10 000× from the assigned distribution (Tables III and IV in the online-only Data Supplement). The estimated 10 000 pairs of incremental costs and QALYs were plotted to show the probabil-ity that a strategy was cost-effective at different willingness-to-pay thresholds (eg, $100 000 per QALY gained).
ResultsBase Case AnalysisA strategy of 30-day ECG monitoring detected 129 more cases of AF and led to 104 more subclinical AF patients receiving anticoagulant therapy, for every 1000 patients screened. Our model predicted that 16 more ischemic strokes would be pre-vented at the expense of 2 more intracranial hemorrhages during a lifetime, for every 1000 patients screened. Overall,
30-day ECG monitoring was highly cost-effective (incremen-tal cost-effectiveness ratio: $2000 per QALY gained); it was predicted to gain 17 life-years and 13 QALYs at an additional cost of $28 000 in a cohort of 1000 patients (Table 2).
In secondary analyses evaluating shorter monitoring dura-tions, which lowered the AF detection rates and cost of moni-toring, both 7- and 14-day monitoring were cost saving and clinically effective in preventing ischemic stroke when com-pared with a repeat 24-hour Holter (Table V in the online-only Data Supplement). Among the monitoring strategies, 30-day monitoring was the most clinically effective (estimated num-bers needed to screen to prevent 1 ischemic stroke: 254, 102, and 63 for 7-, 14-, and 30-day monitoring, respectively).
Sensitivity AnalysesThe incremental costs and QALY gained associated with 30-day monitoring from 1-way sensitivity analyses were plot-ted (Figure 1). Thirty-day monitoring was either cost saving or cost <$100 000 per QALY gained in all but one scenario; it cost $120 000 per QALY gained when we assumed antico-agulation reduced ischemic stroke risk by only 20%. In sub-group analyses, 30-day monitoring was highly cost-effective for younger (55 years) patients; it was cost saving and more effective in patients with higher risks of AF (≥80 years of age or those with frequent atrial ectopy40).
The 2-way sensitivity analysis results (Figure 2) show how cost-effectiveness changed across a range of assumptions for annual ischemic stroke risk and effectiveness of antico-agulation in preventing ischemic stroke. For example, 30-day monitoring, at a cost of $447, would be considered low value in patients with an ischemic stroke recurrence risk of 3% or lower if anticoagulation only reduced ischemic stroke risk by 30%. The results were more sensitive to these assump-tions at higher monitoring costs. Cost-effectiveness of 7- and
Table 2. Results Comparing 30-Day ECG and Repeat 24-Hour Holter Monitoring, Base Case
30-d ECGRepeat 24-h
Holter Incremental
Ischemic stroke 0.195 0.211 −0.016
Intracranial hemorrhage 0.059 0.057 0.002
Major bleeding 0.233 0.227 0.007
Life-year 8.176 8.148 0.028
Life-year (discounted)* 6.137 6.119 0.017
QALY 5.857 5.837 0.020
QALY (discounted)* 4.467 4.454 0.013
Monitoring cost, $ 447 131 316
Cost of ischemic stroke, $ 17 604 18 960 −1356
Other costs, $ 41 661 40 707 954
Total cost, $ 59 712 59 798 −86
Total cost (discounted),$* 43 689 43 661 28
Number needed to screen to prevent 1 ischemic stroke
63
Incremental cost per QALY gained (discounted),* $/QALY
2166
QALY indicates quality-adjusted life-years.* Discounted at 5% per year.
Figure 1. Results of 117 sensitivity analyses. Detailed results of scenarios that 30-day monitoring cost of ≥$20 000/QALY are listed in Table VI in the online-only Data Supplement. A strategy was considered highly cost-effective if it cost <$20 000/QALY and moderately cost-effective if it cost <$100 000/QALY.39 ICER indicates incremental cost-effectiveness ratio, $/QALY gained. Less effective treatment: when the effectiveness of anticoagulant was reduced to 20% stroke risk reduction, 30-day monitoring cost $120 000 per quality-adjusted life-year (QALY) gained; lower stroke risk: in patients with stroke recurrence risk of 2.5% per year, 30-day monitoring cost $49 000 per QALY gained.
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Yong et al Cost-Effectiveness of ECG Monitoring After Cryptogenic Stroke 2383
14-day monitoring was less sensitive to changes in ischemic stroke risk and treatment effects (Figure II in the online-only Data Supplement). The probabilistic sensitivity analysis (Figure 3) shows that 30-day monitoring was more effective than repeat 24-hour monitoring 92% of the time. At a thresh-old of $100 000/QALY, 30-day monitoring was cost-effective 81% of the time when monitoring cost $447 (Figure III in the online-only Data Supplement) and 76% of the time when monitoring cost $800.
DiscussionOur findings suggest that noninvasive ECG monitoring for a target of 30 days is likely cost-effective among patients with a recent cryptogenic stroke or TIA. The results were sensi-tive to ischemic stroke risk and treatment benefit, especially at greater monitoring durations and costs.
This study is the first cost-effectiveness analysis of nonin-vasive monitoring for AF detection after cryptogenic stroke that uses effectiveness data from a randomized controlled trial, which minimizes the selection bias and confounding commonly present in observational studies. Our findings are consistent with previous cost-effectiveness analyses assessing
outpatient poststroke ECG monitoring that used detection rates from observational studies.41,42 One study found that 30-day intermittent ECG monitoring was cost saving and more effective than usual care in Sweden.42 Another study found that 7-day monitoring cost $13 000 per QALY gained in the United States.41 Their incremental cost was higher, partly because they assumed all patients with AF detected received β-blockers, and they were comparing their intervention to a strategy that had no cost of monitoring.
This study has limitations. First, the results are predicted from a decision analytic model rather than observed events. Second, the risk of recurrent ischemic stroke associated with low-burden subclinical paroxysmal AF in patients with crypto-genic stroke is uncertain.15 We acknowledge that the minimum duration of clinically significant AF remains controversial. In EMBRACE, the monitoring devices were limited to record-ing up to a maximum of 2.5 minutes of AF; >60% of the AF episodes detected lasted at least 2.5 minutes. If we assume that only patients with ≥2.5 minutes AF detected had an annual stroke recurrence risk of 4.5%, then the overall annual stroke risk would be 3.5%; 30-day monitoring would be considered low-value if anticoagulant therapy reduced ischemic stroke risk by <30% (apixaban reduced recurrent ischemic stroke rate by 71%).18 The untreated annual stroke recurrence risk is highly unlikely to be lower than 3.5% because the average annual stroke risk is ≈3% to 8% in studies of patients with cryptogenic stroke (without documented AF), and the risk seems higher in patients with AF detected versus those without AF detected.1,14,20 Third, the effectiveness of anticoagulation in this population is uncertain.43 Currently available, but limited, evidence suggests that the relative risk reduction with antico-agulation is likely similar across different patterns of AF.1,44 In two randomized trials of AF detection in stroke patients, fewer patients who received prolonged monitoring had recur-rent stroke or TIA; however, these trials were not powered for that end point.45 Trials underway will better inform us about this estimate.46 To address the concerns of both limitations, our 2-way sensitivity analysis results show the potential cost-effectiveness over a wide range of effectiveness estimates. In addition, our effectiveness estimate in the base case was more conservative than in similar cost-effectiveness analyses.41,42
Figure 2. Results from 2-way sensitivity analyses varying ischemic stroke recur-rence risk and effectiveness of antico-agulation at the same time when 30-day monitoring cost $447 (base case) and $800. Numbers on the table represent incremental cost-effectiveness ratios ($/QALY gained) for scenarios where 30-day monitoring cost $20 000 per quality-adjusted life-year (QALY) gained or more. *A strategy was considered low-value when it cost >$100 000/QALY.
Figure 3. Plot of 10 000 pairs of incremental costs and quality-adjusted life-years (QALYs) from probabilistic sensitivity analysis.
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

2384 Stroke September 2016
Our findings have implications for clinicians and policy-makers. Cryptogenic stroke is common in everyday stroke practice. With practice guidelines now starting to recommend longer than 24 hours of ECG monitoring to detect AF after cryptogenic stroke,5–7 our results support the recommendation that wearable devices enabling ≤30 days of monitoring be made available to the target population. Among the assessed strategies, 30-day monitoring was the most clinically effective, but 14-day monitoring can be an attractive alternative to poli-cymakers. In EMBRACE, 75% of the AF cases were detected within the first 14 days of monitoring. Comparing 30-day ver-sus 14-day monitoring, 30-day monitoring cost $28 000 per QALY gained, and there was less uncertainty around the cost-effectiveness of 14 days when the key assumptions (stroke risks and anticoagulant effectiveness) changed. In terms of generalizability, the AF detection rates were derived from an elderly and predominantly white Canadian secondary stroke prevention cohort who had nonlacunar, nonretinal, crypto-genic stroke events diagnosed by a stroke neurologist. The EMBRACE patients had mostly nondisabling strokes, and we assumed that they have long survival poststroke (8 years). Cost-effectiveness of monitoring in practice will depend on careful patient selection (especially given the tendency for overdiagnosis of TIAs), patients’ functional status and life expectancy, and adherence with monitoring and treatment.
SummaryAfter a recent cryptogenic stroke or TIA, 30-day ECG moni-toring is likely highly cost-effective for preventing recurrent strokes. A 14-day ECG protocol provides an attractive value alternative, especially for lower risk patients, as it seems cost saving and more effective than a repeat 24-hour ECG. These results lend support to emerging practice guidelines recom-mending longer (≥7 days) poststroke ECG monitoring in care-fully selected patients to optimize secondary stroke prevention. At greater monitoring durations and costs, cost-effectiveness depends on the stroke recurrence risk and effectiveness of anticoagulation, which remain uncertain. Future trials that clarify the stroke risk associated with subclinical AF and the effectiveness of anticoagulant therapy in this population will further inform the cost-effectiveness of prolonged monitoring strategies.
AcknowledgmentsWe thank Dr Jeff Healey, Population Health Research Institute, for sharing unpublished subgroup analysis results from ASSERT.
Sources of FundingThis work was supported by a national peer-reviewed grant from the Canadian Stroke Network and a provincial peer-reviewed grant from the Ontario Centres of Excellence (Advancing Health Program). Dr Gladstone has received support from the Bastable-Potts Chair in Stroke Research at Sunnybrook Health Sciences Centre, the Sam Sorbara Charitable Foundation, the Sunnybrook Department of Medicine, the University of Toronto Department of Medicine and Eaton Scholar Award, a Clinician-Scientist Award from the Heart and Stroke Foundation of Ontario, the Heart and Stroke Foundation Canadian Partnership for Stroke Recovery, and the Bril Chair in Neurology at the University of Toronto. Part of the project was con-ducted during Dr Kednapa Thavorn’s Applied Pharmacoeconomic
Fellowship supported by an unrestricted grant from Boehringer Ingelheim. Dr Laupacis is supported by a Canada Research Chair in Health Policy and Citizen Engagement.
DisclosuresDr Gladstone reports personal fees for lectures or advisory boards from Bayer, Boehringer Ingelheim, Bristol-Meyers Squibb, and Pfizer, outside the submitted work; Dr Gladstone is principal investi-gator of the EMBRACE trial that was funded by peer-reviewed oper-ating grants from the Canadian Stroke Network; coprincipal applicant with m-Health Solutions on a provincial peer-reviewed grant from the Ontario Centres of Excellence (Advancing Health competition); and principal investigator of the SCREEN-AF trial of atrial fibril-lation screening supported by the CIHR-funded Stroke Prevention Intervention Network (C-SPIN).
References 1. Hart RG, Diener HC, Coutts SB, Easton JD, Granger CB, O’Donnell MJ,
et al; Cryptogenic Stroke/ESUS International Working Group. Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol. 2014;13:429–438. doi: 10.1016/S1474-4422(13)70310-7.
2. Kishore A, Vail A, Majid A, Dawson J, Lees KR, Tyrrell PJ, et al. Detection of atrial fibrillation after ischemic stroke or transient ischemic attack: a systematic review and meta-analysis. Stroke. 2014;45:520–526. doi: 10.1161/STROKEAHA.113.003433.
3. Gladstone DJ, Spring M, Dorian P, Panzov V, Thorpe KE, Hall J, et al; EMBRACE Investigators and Coordinators. Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med. 2014;370:2467–2477. doi: 10.1056/NEJMoa1311376.
4. Sanna T, Diener HC, Passman RS, Di Lazzaro V, Bernstein RA, Morillo CA, et al; CRYSTAL AF Investigators. Cryptogenic stroke and underly-ing atrial fibrillation. N Engl J Med. 2014;370:2478–2486. doi: 10.1056/NEJMoa1313600.
5. Culebras A, Messé SR, Chaturvedi S, Kase CS, Gronseth G. Summary of evidence-based guideline update: prevention of stroke in nonvalvular atrial fibrillation: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2014;82:716–724. doi: 10.1212/WNL.0000000000000145.
6. Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, Demaerschalk BM, et al; American Heart Association Stroke Council; Council on Cardiovascular Nursing; Council on Peripheral Vascular Disease; Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare profession-als from the American Heart Association/American Stroke Association. Stroke. 2013;44:870–947. doi: 10.1161/STR.0b013e318284056a.
7. Verma A, Cairns JA, Mitchell LB, Macle L, Stiell IG, Gladstone D, et al; CCS Atrial Fibrillation Guidelines Committee. 2014 focused update of the Canadian Cardiovascular Society Guidelines for the management of atrial fibrillation. Can J Cardiol. 2014;30:1114–1130. doi: 10.1016/j.cjca.2014.08.001.
8. Loop Recorders to Detect Atrial Arrhythmias In Patients Post-Discharge Who Have Had a Cryptogenic Stroke: A Review of Clinical and Cost-Effectiveness. Ottawa, Canada: Canadian Agency for Drugs and Technologies in Health; 2014.
9. Kamel H, Easton JD, Johnston SC, Kim AS. Cost-effectiveness of apix-aban vs warfarin for secondary stroke prevention in atrial fibrillation. Neurology. 2012;79:1428–1434. doi: 10.1212/WNL.0b013e31826d5fe8.
10. Ariesen MJ, Claus SP, Rinkel GJ, Algra A. Risk factors for intracere-bral hemorrhage in the general population: a systematic review. Stroke. 2003;34:2060–2065. doi: 10.1161/01.STR.0000080678.09344.8D.
11. Guidelines for the Economic Evaluation of Health Technologies. Ottawa, Canada: Canadian Agency for Drugs and Technologies in Health; 2006.
12. Coyle D, Coyle K, Cameron C, Lee K, Kelly S, Steiner S, et al. Cost-effectiveness of new oral anticoagulants compared with warfarin in preventing stroke and other cardiovascular events in patients with atrial fibrillation. Value Health. 2013;16:498–506. doi: 10.1016/j.jval. 2013.01.009.
13. Xu Y, Holbrook AM, Simpson CS, Dowlatshahi D, Johnson AP. Prescribing patterns of novel oral anticoagulants following regulatory approval for atrial fibrillation in Ontario, Canada: a population-based descriptive analysis. CMAJ Open. 2013;1:E115–E119. doi: 10.9778/cmajo.20130032.
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Yong et al Cost-Effectiveness of ECG Monitoring After Cryptogenic Stroke 2385
14. Putaala J, Nieminen T, Haapaniemi E, Meretoja A, Rantanen K, Heikkinen N, et al. Undetermined stroke with an embolic pattern–a com-mon phenotype with high early recurrence risk. Ann Med. 2015;47:406–413. doi: 10.3109/07853890.2015.1057612.
15. Keach JW, Bradley SM, Turakhia MP, Maddox TM. Early detection of occult atrial fibrillation and stroke prevention. Heart. 2015;101:1097–1102. doi: 10.1136/heartjnl-2015-307588.
16. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33:1500–1510. doi: 10.1093/eurheartj/ehr488.
17. Connolly SJ, Eikelboom J, Joyner C, Diener HC, Hart R, Golitsyn S, et al; AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364:806–817. doi: 10.1056/NEJMoa1007432.
18. Diener HC, Eikelboom J, Connolly SJ, Joyner CD, Hart RG, Lip GY, et al; AVERROES Steering Committee and Investigators. Apixaban versus aspirin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a predefined subgroup analysis from AVERROES, a randomised trial. Lancet Neurol. 2012;11:225–231. doi: 10.1016/S1474-4422(12)70017-0.
19. Vanassche T, Lauw MN, Eikelboom JW, Healey JS, Hart RG, Alings M, et al. Risk of ischaemic stroke according to pattern of atrial fibrillation: analysis of 6563 aspirin-treated patients in ACTIVE-A and AVERROES. Eur Heart J. 2015;36:281–287a. doi: 10.1093/eurheartj/ehu307.
20. Healey JS, Connolly SJ, Gold MR, Israel CW, Van Gelder IC, Capucci A, et al; ASSERT Investigators. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med. 2012;366:120–129. doi: 10.1056/NEJMoa1105575.
21. Mant J, Hobbs FD, Fletcher K, Roalfe A, Fitzmaurice D, Lip GY, et al; BAFTA investigators; Midland Research Practices Network (MidReC). Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet. 2007;370:493–503. doi: 10.1016/S0140-6736(07)61233-1.
22. Assiri A, Al-Majzoub O, Kanaan AO, Donovan JL, Silva M. Mixed treat-ment comparison meta-analysis of aspirin, warfarin, and new anticoagu-lants for stroke prevention in patients with nonvalvular atrial fibrillation. Clin Ther. 2013;35:967–984.e2. doi: 10.1016/j.clinthera.2013.05.011.
23. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867.
24. Diener HC, Connolly SJ, Ezekowitz MD, Wallentin L, Reilly PA, Yang S, et al; RE-LY study group. Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE-LY trial. Lancet Neurol. 2010;9:1157–1163. doi: 10.1016/S1474-4422(10)70274-X.
25. Easton JD, Lopes RD, Bahit MC, Wojdyla DM, Granger CB, Wallentin L, et al; ARISTOTLE Committees and Investigators. Apixaban com-pared with warfarin in patients with atrial fibrillation and previ-ous stroke or transient ischaemic attack: a subgroup analysis of the ARISTOTLE trial. Lancet Neurol. 2012;11:503–511. doi: 10.1016/S1474-4422(12)70092-3.
26. Hankey GJ, Patel MR, Stevens SR, Becker RC, Breithardt G, Carolei A, et al; ROCKET AF Steering Committee Investigators. Rivaroxaban com-pared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of ROCKET AF. Lancet Neurol. 2012;11:315–322. doi: 10.1016/S1474-4422(12)70042-X.
27. Gomes T, Mamdani MM, Holbrook AM, Paterson JM, Hellings C, Juurlink DN. Rates of hemorrhage during warfarin therapy for atrial fibrillation. CMAJ. 2013;185:E121–E127. doi: 10.1503/cmaj.121218.
28. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383:955–962. doi: 10.1016/S0140-6736(13)62343-0.
29. Antithrombotic Agents for the Prevention of Stroke and Systemic Embolism in Patients With Atrial Fibrillation. Ottawa, Canada: Canadian Agency for Drugs and Technologies in Health; 2013.
30. Life Tables, Canada, Provinces and Territories 2009–2011. Ottawa, Canada: Statistics Canada; 2013. Catalogue no. 84-537-X-No. 005.
31. Anderson CS, Carter KN, Brownlee WJ, Hackett ML, Broad JB, Bonita R. Very long-term outcome after stroke in Auckland, New Zealand. Stroke. 2004;35:1920–1924. doi: 10.1161/01.STR.0000133130.20322.9f.
32. Hardie K, Hankey GJ, Jamrozik K, Broadhurst RJ, Anderson C. Ten-year survival after first-ever stroke in the perth community stroke study. Stroke. 2003;34:1842–1846. doi: 10.1161/01.STR.0000082382.42061.EE.
33. Sorensen SV, Kansal AR, Connolly S, Peng S, Linnehan J, Bradley-Kennedy C, et al. Cost-effectiveness of dabigatran etexilate for the pre-vention of stroke and systemic embolism in atrial fibrillation: a Canadian payer perspective. Thromb Haemost. 2011;105:908–919. doi: 10.1160/TH11-02-0089.
34. van Wijk I, Kappelle LJ, van Gijn J, Koudstaal PJ, Franke CL, Vermeulen M, et al; LiLAC study group. Long-term survival and vascular event risk after transient ischaemic attack or minor ischaemic stroke: a cohort study. Lancet. 2005;365:2098–2104. doi: 10.1016/S0140-6736(05)66734-7.
35. Goeree R, Blackhouse G, Petrovic R, Salama S. Cost of stroke in canada: A 1-year prospective study. J Med Econ. 2005;8:147–167.
36. Mittmann N, Seung SJ, Hill MD, Phillips SJ, Hachinski V, Coté R, et al. Impact of disability status on ischemic stroke costs in Canada in the first year. Can J Neurol Sci. 2012;39:793–800.
37. Meretoja A, Kaste M, Roine RO, Juntunen M, Linna M, Hillbom M, et al. Direct costs of patients with stroke can be continuously monitored on a national level: performance, effectiveness, and Costs of Treatment episodes in Stroke (PERFECT Stroke) Database in Finland. Stroke. 2011;42:2007–2012. doi: 10.1161/STROKEAHA.110.612119.
38. Consumer Price Index. Ottawa, Canada: Statistics Canada; 2014. Catalogue nos. 62-001-X and 62-010-X.
39. Laupacis A, Feeny D, Detsky AS, Tugwell PX. Tentative guide-lines for using clinical and economic evaluations revisited. CMAJ. 1993;148:927–929.
40. Gladstone DJ, Dorian P, Spring M, Panzov V, Mamdani M, Healey JS, et al; EMBRACE Steering Committee and Investigators. Atrial pre-mature beats predict atrial fibrillation in cryptogenic stroke: results from the EMBRACE trial. Stroke. 2015;46:936–941. doi: 10.1161/STROKEAHA.115.008714.
41. Kamel H, Hegde M, Johnson DR, Gage BF, Johnston SC. Cost-effectiveness of outpatient cardiac monitoring to detect atrial fibrilla-tion after ischemic stroke. Stroke. 2010;41:1514–1520. doi: 10.1161/STROKEAHA.110.582437.
42. Levin LÅ, Husberg M, Sobocinski PD, Kull VF, Friberg L, Rosenqvist M, et al. A cost-effectiveness analysis of screening for silent atrial fibril-lation after ischaemic stroke. Europace. 2015;17:207–214. doi: 10.1093/europace/euu213.
43. Passman R, Bernstein RA. New appraisal of atrial fibrillation bur-den and stroke prevention. Stroke. 2016;47:570–576. doi: 10.1161/STROKEAHA.115.009930.
44. Hohnloser SH, Pajitnev D, Pogue J, Healey JS, Pfeffer MA, Yusuf S, et al; ACTIVE W Investigators. Incidence of stroke in paroxysmal versus sustained atrial fibrillation in patients taking oral anticoagulation or com-bined antiplatelet therapy: an ACTIVE W Substudy. J Am Coll Cardiol. 2007;50:2156–2161. doi: 10.1016/j.jacc.2007.07.076.
45. Weber-Kruger M, Gelbrich G, Stahrenberg R, Liman J, Kerner P, Hamann GF, et al; FIND-AF (Randomised) Investigators. Finding atrial fibrillation in stroke patients: randomised evaluation of enhanced and prolonged Holter monitoring—FIND-AF (Randomised)—rationale and design. Am Heart J. 2014;168:438–445.
46. Apixaban for the reduction of thrombo-embolism in patients with device-detected sub-clinical atrial fibrillation (ARTESiA). ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT01938248. 2013. Accessed November 20, 2015.
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

on behalf of the EMBRACE Steering CommitteeThorpe, Paul Dorian, Mike Sharma, Andreas Laupacis and David J. Gladstone
Jean Hai Ein Yong, Kednapa Thavorn, Jeffrey S. Hoch, Muhammad Mamdani, Kevin E.Cryptogenic Stroke
Potential Cost-Effectiveness of Ambulatory Cardiac Rhythm Monitoring After
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2016 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.115.011979
2016;47:2380-2385; originally published online July 28, 2016;Stroke.
http://stroke.ahajournals.org/content/47/9/2380World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2016/07/28/STROKEAHA.115.011979.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from
ONLINE SUPPLEMENT
Yong JHE et al. “Potential Cost-Effectiveness of Ambulatory Cardiac Rhythm
Monitoring after Cryptogenic Stroke”
Contents EMBRACE Steering Committee ............................................................................................................ 2
Supplemental Methods ............................................................................................................................ 3
Clinical event rates .............................................................................................................................. 3
Costs and utilities ................................................................................................................................ 4
Supplemental Tables ............................................................................................................................... 6
Supplemental Table I. Additional clinical data input in base case and deterministic sensitivity
analysis (SA) 6
Supplemental Table II. Health utility weights and costs (2014 USD$) in base case and
deterministic sensitivity analyses (SA) ............................................................................................... 8
Supplemental Table III. Distributions for clinical estimates in probabilistic sensitivity analysis
(PSA) 10
Supplemental Table IV. Distributions for health state utilities and costs (2014 USD$) in
probabilistic sensitivity analysis ....................................................................................................... 13
Supplemental Table V. Cost-effectiveness of 7-, 14- and 30-day ECG monitoring (vs. repeat 24-
hour Holter monitoring) 15
Supplemental Table VI. Deterministic sensitivity analysis (SA) results for scenarios that 30-day
monitoring cost $20 000 per QALY gained or more ........................................................................ 16
Supplemental Figures ............................................................................................................................ 17
Supplemental Figure I. Schematic diagram of Markov model comparing cardiac monitoring
strategies to detect AF for secondary stroke prevention in cryptogenic stroke/TIA patients. .......... 18
Supplemental Figure II. Results of two-way sensitivity analysis for 7-, 14- and 30-day ECG
monitoring (against a repeat 24-hour Holter). .................................................................................. 19
Supplemental Figure III. Cost-effectiveness acceptability curves, generated from 10 000 Monte
Carlo simulations in probabilistic sensitivity analysis, show the probability that each strategy is
cost-effective at different willingness to pay thresholds. .................................................................. 20
Supplemental References ...................................................................................................................... 21

EMBRACE Steering Committee
R. Aviv, K. Boyle, J. Blakely, R. Cote, P. Dorian, D.J. Gladstone (chair), J. Hall, M.K.
Kapral, A. Laupacis, M. Mamdani, M. O'Donnell, V. Panzov, M. Sharma, A. Shuaib, M.
Spring, K. Thorpe.

Supplemental Methods
Clinical event rates
Relative risk of ischemic stroke, anticoagulant vs. aspirin, in subclinical AF: There are
limited data on the treatment effect of anticoagulant therapy for subclinical AF and
randomized trials currently underway will better inform us about this estimate.1 A recent
cohort study showed that anticoagulation was effective in preventing ischemic stroke in
patients with incidentally-detected subclinical AF.2 A subgroup analysis from the Warfarin-
Aspirin Recurrent Stroke Study (WARSS) also showed that warfarin reduced recurrent
ischemic stroke in patients with cryptogenic stroke.3 Subgroup analyses from large
anticoagulant trials did not show a statistically significant difference in relative risk between
permanent, persistent and paroxysmal AF.4, 5 While the absolute benefit of anticoagulation vs.
aspirin is likely less for patients with subclinical AF as compared with clinical AF due to
lower baseline risk, based on the above indirect evidence the relative risk reduction is likely
similar. To reflect the uncertainty in this estimate, we assigned a higher standard error than
reported in the meta-analyses of anticoagulant trials.6, 7
Stroke severity distribution for AF patients: The severity distribution of ischemic strokes
was derived from a Canadian cohort study of 1852 ischemic stroke patients with AF and
randomized controlled trials of anticoagulants for stroke prevention.8-10
Stroke recurrence in non-AF patients: Patients without AF had a lower stroke recurrence
rate (HR: 0.40) and less severe stroke distribution than patients with subclinical AF.2, 10, 11
Major bleeding: The annual intracranial hemorrhage rate in patients receiving warfarin
(1.07%) was estimated from patients with previous stroke or TIA receiving warfarin in recent
randomized controlled trials.8, 12, 13 The severity distribution of intracranial hemorrhage was
estimated from observational studies of warfarin-associated hemorrhage.14, 15 The risk of
overall major bleeding with warfarin and its case fatality rate (2%) was estimated from
population studies of patients receiving warfarin and subgroup analyses in patients with
previous stroke or TIA from large anticoagulant trials.8, 12-15
Costs and utilities
The 30-day ECG monitoring costs included technical and professional fees for interpreting
results from cardiac loop monitoring; the fees were for 14-day monitoring and we doubled
the fees for 30-day monitoring.16 We based our analysis on a centralized service model that is
currently operating in Ontario, whereby a company owns the devices and software, and only
charges the payer fees associated with interpreting the recorded ECG data. The 24-hour
Holter monitoring cost included device cost, recording and scanning fee, interpretation fee
and overhead cost.17-19
Costs of medication included prescription fees, assuming patients refill medication
every three months, and an 8% pharmacy markup.20 The cost of warfarin also included the
cost for monitoring the international normalized ratio, estimated from a costing study of
warfarin management across different clinic settings in Canada.21
The estimates of costs of ischemic stroke and intracranial hemorrhage were highly
variable across studies; we used the average for the base case and conducted sensitivity
analyses using the range. In EMBRACE, two-thirds of patients had a stroke as the index
event and one-third had a TIA. Therefore, we assumed that two-thirds of patients incurred
long-term costs associated with a minor stroke when they entered the model.
The general population utility score was estimated from a 10-year Canadian
longitudinal study (N=7915).22 The utility weights for stroke were derived from a study that
compared 5-year health state utility of patients after stroke or TIA with their matched

controls.23 Intracranial hemorrhage had the same utility as ischemic stroke at the same
severity, similar to other cost-effectiveness analyses.20, 24, 25 Patients who experienced major
bleeding had a utility of 0.80 for two weeks and returned to baseline utility for the rest of the
year.9

Supplemental Tables
Supplemental Table I. Additional clinical data input in base case and deterministic
sensitivity analysis (SA)
Variables Base case (SA)
Severity of ischemic stroke in patients with AF, %
Mild (mRS=0-2) 36.3 (30.0-45.0)
Disability (mRS=3-5) 43.4 (33.7-53.7)
Fatal (mRS=6) 20.3 (10.0-30.0)
% disabling stroke that is severe (mRS=5) 16.2 (5.0-27.0)
Anticoagulant treatment in patients without AF detected, %
30-day
24-hour
7.2 (5.0-10.0)
8.6 (7.0-15.0)
HR of ischemic stroke, no subclinical AF vs. subclinical AF 0.4 (0.17-0.67)
Severity of ischemic stroke in patients with no subclinical AF, %
Mild (mRS=0-2) 47.0 (37.5-57.5)
Moderate disability (mRS=3-4) 40.5 (30.0-50.0)
Severe disability (mRS=5) 4.3 (2.0-6.0)
Fatal (mRS=6) 8.2 (5.0-10.0)
HR of ischemic stroke per 10 year of life 1.4 (1.2-1.6)
Risk of intracranial hemorrhage with warfarin, %/year (among
patients with a prior ischemic stroke or TIA)
1.07 (0.8-1.5)
Case fatality rate for intracranial hemorrhage, % 42 (35-50)
% disabled among intracranial hemorrhage survivors 86 (60-85)
% disabling intracranial hemorrhage that is severe 68 (25-80)
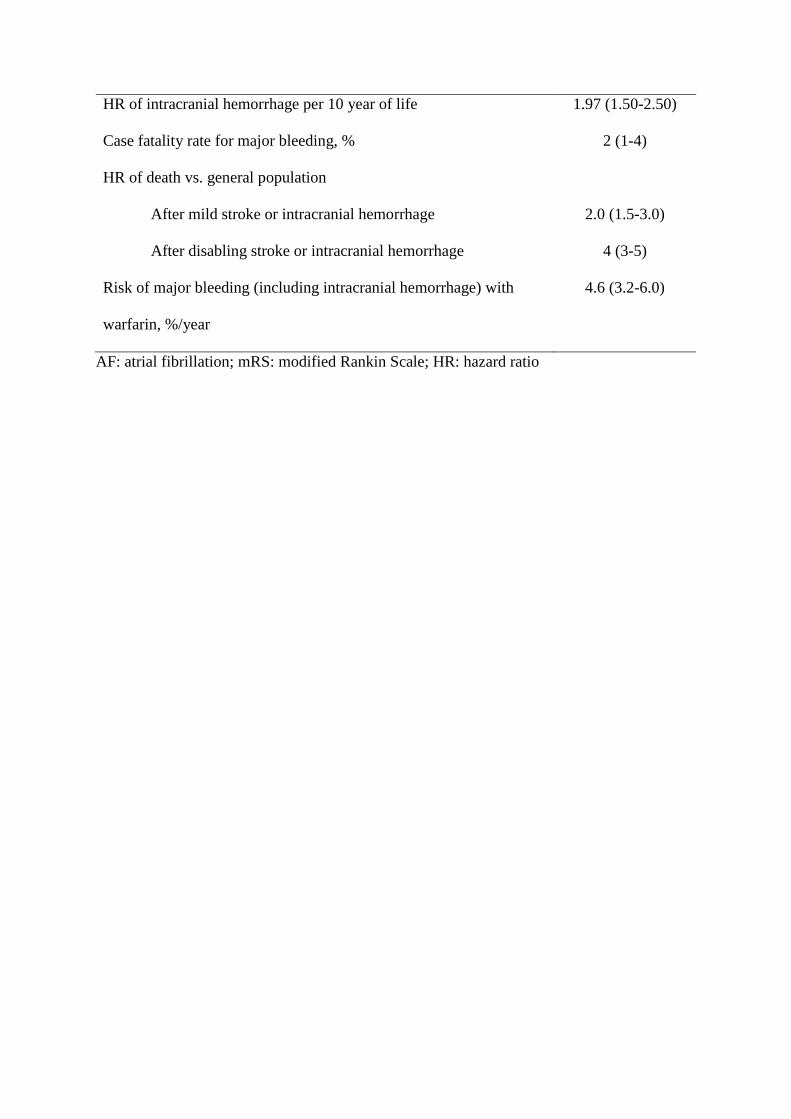
HR of intracranial hemorrhage per 10 year of life 1.97 (1.50-2.50)
Case fatality rate for major bleeding, % 2 (1-4)
HR of death vs. general population
After mild stroke or intracranial hemorrhage 2.0 (1.5-3.0)
After disabling stroke or intracranial hemorrhage 4 (3-5)
Risk of major bleeding (including intracranial hemorrhage) with
warfarin, %/year
4.6 (3.2-6.0)
AF: atrial fibrillation; mRS: modified Rankin Scale; HR: hazard ratio

Supplemental Table II. Health utility weights and costs (2014 USD$) in base case
and deterministic sensitivity analyses (SA)
Base case (SA)
Discount rates for costs, QALYs and life-years 5% (0-3%)
Health state utility weights
No event 0.93 (0.95)
Severe stroke (mRS=5) first year 0.30 (0.20-0.40)
Severe stroke subsequent years 0.48 (0.30-0.60)
Moderate stroke first year 0.67 (0.56-0.71)
Moderate stroke subsequent years 0.71 (0.67-0.80)
Mild stroke (first and subsequent years) 0.89 (0.80-0.93)
Disabling intracranial hemorrhage (first year) 0.42
Disabling intracranial hemorrhage (subsequent years) 0.55
Non-disabling intracranial hemorrhage 0.89
Major bleeding 0.8 (0.60) for 2 weeks*
Costs, $
30-day ECG monitoring 447 (538-692)
24-hour Holter monitoring 132 (93-170)
NOACs, per year 1000 (769-1231)
Warfarin, including INR monitoring, per year 235 (192-308)
Aspirin, per year 38 (23-54)
One-time or first year costs, $
Mild ischemic stroke (mRS=0-2) 13 385 (6692-20 077)
Moderate ischemic stroke (mRS=3-4) 57 942 (52 308-63 577)

Severe ischemic stroke (mRS=5) 105 385 (76 923-133
846)
Fatal ischemic stroke (mRS=6) 13 385 (6692-13 385)
Intracranial hemorrhage 42 234 (27 077-57 391)
Major bleeds 3413 (1707-5120)
No stroke or intracranial hemorrhage 4770 (4187-5354)
Long-term annual costs, $
Non-disabling ischemic stroke 7155 (6280-8031)
Moderate ischemic stroke 25 940 (13 734-38 146)
Severe ischemic stroke 53 125 (25 942-80 308)
Intracranial hemorrhage 26 832 (19 231-34 435)
* Returned to 0.93 after 2 weeks.

Supplemental Table III. Distributions for clinical estimates in probabilistic
sensitivity analysis (PSA)
Variable Mean (95%
CI)
Distribution Sourc
e
AF detection rates at 90 days, % 26
30-day ECG 16.1 Beta (45, 235)
24-hour Holter 3.2 Beta (9, 268)
Anticoagulant treatment rate, % 26
AF detected patients 89 Beta (49, 6)
Patients without AF detected, 30-day
ECG
7.2 Beta (17, 218)
Patients without AF detected, 24-hour
Holter
8.6 Beta (23, 245)
Proportion of patients who receive
anticoagulant receive warfarin
0.75 Beta (750, 250) 27
Ischemic stroke recurrence, aspirin (%/year) 4.5 (0.02-
0.09)
Beta 11, 28-30
HR of ischemic stroke, no subclinical AF vs.
subclinical AF
0.40 (0.20-
0.78)
Lognormal 11
RR of ischemic stroke (NOAC vs. warfarin) 0.92 (0.83-
1.02)
Lognormal 31
RR of ischemic stroke (NOAC vs. aspirin) 0.50 (0.25-
1.50)
Lognormal 7, 32, 33
Severity of ischemic stroke (%) in patients
with AF
8-10

Variable Mean (95%
CI)
Distribution Sourc
e
Mild (mRS=0-2) 36.3 Dirichlet (937)
Disability (mRS=3-5) 43.4
Fatal (mRS=6) 20.3 Dirichlet (524)
% disabling stroke that is severe (mRS=5) 16.2 Beta (159, 823) 9, 10
Severity of ischemic stroke (%) in patients
with no subclinical AF
10
Mild (mRS=0-2) 47.0
Moderate disability (mRS=3-4) 40.5 Dirichlet (3665)
Severe disability (mRS=5) 4.3 Dirichlet (389)
Fatal (mRS=6) 8.2 Dirichlet (742)
HR of ischemic stroke per 10 year of life 1.4 (1.0-2.0) Lognormal 25
Risk of intracranial hemorrhage with warfarin,
%/year
1.07 Beta (40, 6564) 8, 12, 13
RR of intracranial hemorrhage (NOAC vs.
warfarin)
0.48 (0.39-
0.59)
Lognormal 31
Odds ratio of intracranial hemorrhage (NOAC
vs. aspirin)
1.14 (0.38-
1.90)
Lognormal 34
Case fatality rate for intracranial hemorrhage,
%
42 Beta (257, 354) 14, 15
% disabled among intracranial hemorrhage
survivors
86 Beta (31, 5) 15
% disabling intracranial hemorrhage that is
severe
68 Beta (21, 10) 15

Variable Mean (95%
CI)
Distribution Sourc
e
RR of intracranial hemorrhage per 10 year of
life
1.97 (1.5-2.5) Lognormal 35
Risk of major bleeding (including intracranial
hemorrhage) in warfarin, %/year
4.6 Beta (4281, 88
779)
14 8, 12,
13
RR of major bleeding (NOAC vs. warfarin) 0.86 (0.73-
1.00)
Lognormal 31
RR of major bleeding (NOAC vs. aspirin) 1.25 (0.74-
1.75)
Lognormal 34
Case fatality rate for other major bleeding
(excluding intracranial hemorrhage), %
2.0 Beta (15, 599) 9, 15
HR of death after mild stroke or intracranial
hemorrhage (vs. general population)
2.0 (1.5-3.0) Lognormal 36-38
HR of death after disabling stroke or
intracranial hemorrhage (vs. general
population)
4.0 (3.0-5.0) Lognormal 24
NOAC: New oral anticoagulants (dabigatran, apixaban, rivaroxaban and edoxaban); RR:
relative risk; HR: hazard ratio; CI: confidence interval
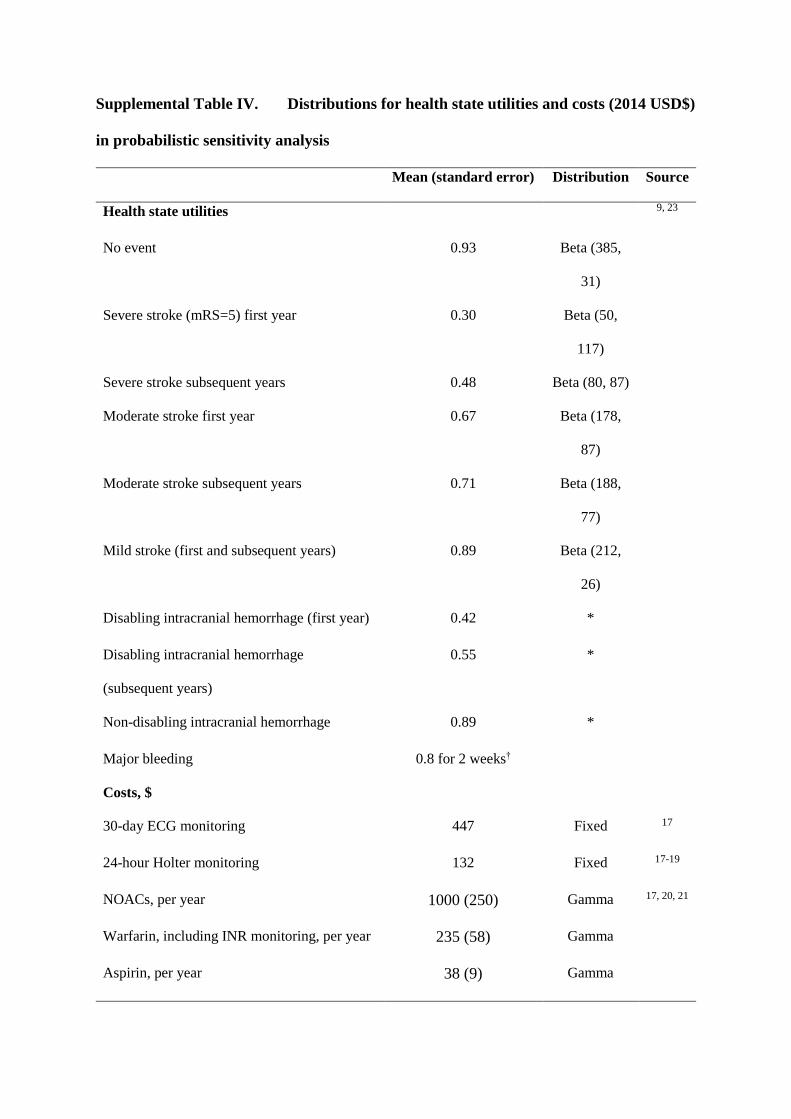
Supplemental Table IV. Distributions for health state utilities and costs (2014 USD$)
in probabilistic sensitivity analysis
Mean (standard error) Distribution Source
Health state utilities 9, 23
No event 0.93 Beta (385,
31)
Severe stroke (mRS=5) first year 0.30 Beta (50,
117)
Severe stroke subsequent years 0.48 Beta (80, 87)
Moderate stroke first year 0.67 Beta (178,
87)
Moderate stroke subsequent years 0.71 Beta (188,
77)
Mild stroke (first and subsequent years) 0.89 Beta (212,
26)
Disabling intracranial hemorrhage (first year) 0.42 *
Disabling intracranial hemorrhage
(subsequent years)
0.55 *
Non-disabling intracranial hemorrhage 0.89 *
Major bleeding 0.8 for 2 weeks†
Costs, $
30-day ECG monitoring 447 Fixed 17
24-hour Holter monitoring 132 Fixed 17-19
NOACs, per year 1000 (250) Gamma 17, 20, 21
Warfarin, including INR monitoring, per year 235 (58) Gamma
Aspirin, per year 38 (9) Gamma

Mean (standard error) Distribution Source
One-time or first year costs, $
Mild ischemic stroke (mRS=0-2) 13 385 (3346) Gamma 20, 24, 39
Moderate ischemic stroke (mRS=3-4) 57 942 (28 972) Gamma
Severe ischemic stroke (mRS=5) 105 385 (52 692) Gamma
Fatal ischemic stroke (mRS=6) 13 385 (3346) Gamma
Intracranial hemorrhage 42 234 (21 117) Gamma 39
Major bleeds 3413 (1707) Gamma 20
Long-term annual costs, $
Non-disabling ischemic stroke 7155 (3578) Gamma 24, 39, 40
Moderate ischemic stroke 25 940 (12 970) Gamma
Severe ischemic stroke 53 125 (26 562) Gamma
Intracranial hemorrhage 26 832 (13 416) Gamma
* We did not assign a distribution because we assumed intracranial hemorrhage has the same
utility as ischemic stroke, for the same severity.
† Utility returned to 0.93 after 2 weeks.

Supplemental Table V. Cost-effectiveness of 7-, 14- and 30-day ECG monitoring
(vs. repeat 24-hour Holter monitoring)
Changing input 30-day
(base case)
14-day 7-day
AF detected by prolonged monitoring, %* 16.1 11.6 7.0
AF detected by a repeat 24-hour Holter, % 3.2 3.2 3.2
Monitoring cost, USD$ 447 224 154
Incremental analysis (vs. a repeat 24-hour
Holter)
Ischemic strokes prevented 0.016 0.010 0.004
Number needed to screen to prevent 1 ischemic
stroke
63 102 254
Additional life years saved† 0.017 0.011 0.005
Additional QALYs gained† 0.013 0.008 0.004
Total incremental cost, † USD$ 28 -101 -74
Incremental cost per QALY gained,† $ 2166 Dominant§ Dominant§
* Estimates were obtained from EMBRACE.26
† Outcomes were discounted at 5% per year.
§ Prolonged monitoring is cost-saving and more effective than a repeat 24-hour Holter.

Supplemental Table VI. Deterministic sensitivity analysis (SA) results for scenarios
that 30-day monitoring cost $20 000 per QALY gained or more
Model input
Base
case
estimate
SA
estimate
Ischemic
stroke
QALY*
Cost
(USD$)*
ICER*
($/QALY)
Base case -0.016 0.013 28 2000
Atrial fibrillation
detected by 30-day
ECG
16.1% 10.0% -0.008 0.007 156 23 000
% receiving
anticoagulants among
AF-detected patients
89% 50% -0.008 0.007 161 24 000
Ischemic stroke
recurrence, aspirin,
per year
4.50% 2.5% -0.010 0.006 314 49 000
Anticoagulant
effectiveness
(ischemic stroke risk
reduction)
50% 20% -0.006 0.004 411 120 000
Cost of 30-day
monitoring
447 800 -0.016 0.013 381 29 000
Cost of 30-day
monitoring
447 1000 -0.016 0.013 581 45 000

Model input
Base
case
estimate
SA
estimate
Ischemic
stroke
QALY*
Cost
(USD$)*
ICER*
($/QALY)
Base case -0.016 0.013 28 2000
Time horizon (years) Lifetime 5 -0.009 0.003 207 63 000
* Discounted at 5% per year, unless stated otherwise; ICER: incremental cost-effectiveness
ratio; RR: relative risk
Supplemental Figures
Cost-effective (< $100 000/QALY) Low value (≥ $100 000/QALY)

Supplemental Figure I. Schematic diagram of Markov model comparing cardiac
monitoring strategies to detect AF for secondary stroke prevention in cryptogenic
stroke/TIA patients.
Note. Major bleeding is a temporary health state (lasts only one cycle), as indicated by the
dotted line.

Supplemental Figure II. Results of two-way sensitivity analysis for 7-, 14- and 30-day
ECG monitoring (against a repeat 24-hour Holter).

Supplemental Figure III. Cost-effectiveness acceptability curves, generated from 10 000
Monte Carlo simulations in probabilistic sensitivity analysis, show the probability that
each strategy is cost-effective at different willingness to pay thresholds.
0%
20%
40%
60%
80%
100%
0 50000 100000 150000 200000 250000
% cost-effective
Willingness to pay ($ per QALY)
30-day ECG
repeat 24-hour holter

Supplemental References
1. Healey J. Apixaban for the reduction of thrombo-embolism in patients with device-detected
sub-clinical atrial fibrillation.
2. Martinez C, Katholing A, Freedman SB. Adverse prognosis of incidentally detected
ambulatory atrial fibrillation. A cohort study. Thromb Haemost. 2014;112:276-286
3. Hart RG, Diener H-C, Coutts SB, Easton JD, Granger CB, O'Donnell MJ, et al. Embolic
strokes of undetermined source: The case for a new clinical construct. Lancet Neurol.
2014;13:429-438
4. Hohnloser SH, Pajitnev D, Pogue J, Healey JS, Pfeffer MA, Yusuf S, et al. Incidence of
stroke in paroxysmal versus sustained atrial fibrillation in patients taking oral anticoagulation
or combined antiplatelet therapy: An active w substudy. J Am Coll Cardiol. 2007;50:2156-
2161
5. Hohnloser SH, Shestakovska O, Eikelboom J, Franzosi MG, San Tan R, Zhu J, et al. The
effects of apixaban on hospitalizations in patients with different types of atrial fibrillation:
Insights from the averroes trial. European heart journal. 2013;34:2752-2759
6. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: Antithrombotic therapy to prevent stroke in
patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857-867
7. Assiri A, Al-Majzoub O, Kanaan AO, Donovan JL, Silva M. Mixed treatment comparison
meta-analysis of aspirin, warfarin, and new anticoagulants for stroke prevention in patients
with nonvalvular atrial fibrillation. Clin Ther. 2013;35:967-984 e962
8. Hankey GJ, Patel MR, Stevens SR, Becker RC, Breithardt G, Carolei A, et al. Rivaroxaban
compared with warfarin in patients with atrial fibrillation and previous stroke or transient
ischaemic attack: A subgroup analysis of rocket af. The Lancet Neurology. 2012;11:315-322
9. Dorian P, Kongnakorn T, Phatak H, Rublee DA, Kuznik A, Lanitis T, et al. Cost-
effectiveness of apixaban vs. Current standard of care for stroke prevention in patients with
atrial fibrillation. European Heart Journal. 2014

10. Saposnik G, Gladstone D, Raptis R, Zhou L, Hart RG, Investigators of the Registry of the
Canadian Stroke N, et al. Atrial fibrillation in ischemic stroke: Predicting response to
thrombolysis and clinical outcomes. Stroke. 2013;44:99-104
11. Healey JS, Connolly SJ, Gold MR, Israel CW, Van Gelder IC, Capucci A, et al. Subclinical
atrial fibrillation and the risk of stroke. N Engl J Med. 2012;366:120-129
12. Diener H-C, Connolly SJ, Ezekowitz MD, Wallentin L, Reilly PA, Yang S, et al. Dabigatran
compared with warfarin in patients with atrial fibrillation and previous transient ischaemic
attack or stroke: A subgroup analysis of the re-ly trial. Lancet Neurol. 2010;9:1157-1163
13. Easton JD, Lopes RD, Bahit MC, Wojdyla DM, Granger CB, Wallentin L, et al. Apixaban
compared with warfarin in patients with atrial fibrillation and previous stroke or transient
ischaemic attack: A subgroup analysis of the aristotle trial. Lancet Neurol. 2012;11:503-511
14. Gomes T, Mamdani MM, Holbrook AM, Paterson JM, Hellings C, Juurlink DN. Rates of
hemorrhage during warfarin therapy for atrial fibrillation. CMAJ. 2013;185:E121-E127
15. Fang MC, Go AS, Chang Y, Hylek EM, Henault LE, Jensvold NG, et al. Death and disability
from warfarin-associated intracranial and extracranial hemorrhages. The American journal of
medicine. 2007;120:700-705
16. Ontario Ministry of Health and Long-Term Care. Ontario health insurance (ohip) schedule of
benefits and fees.
17. Ontario Ministry of Health and Long-Term Care. Ontario drug benefit formulary/
comparative drug index.
18. Rockx MA, Hoch JS, Klein GJ, Yee R, Skanes AC, Gula LJ, et al. Is ambulatory monitoring
for "community-acquired" syncope economically attractive? A cost-effectiveness analysis of
a randomized trial of external loop recorders versus holter monitoring. Am Heart J.
2005;150:1065
19. Ontario Case Costing Initiatives. Occi ambulatory care 2010/2011, indirect cost (diagnosis:
Cardiac arrhythmia). 2011

20. Coyle D, Coyle K, Cameron C, Lee K, Kelly S, Steiner S, et al. Cost-effectiveness of new
oral anticoagulants compared with warfarin in preventing stroke and other cardiovascular
events in patients with atrial fibrillation. Value Health. 2013;16:498-506
21. Schulman S, Anderson DR, Bungard TJ, Jaeger T, Kahn SR, Wells P, et al. Direct and
indirect costs of management of long-term warfarin therapy in canada. J Thromb Haemost.
2010;8:2192-2200
22. Orpana HM, Ross N, Feeny D, McFarland B, Bernier J, Kaplan M. The natural history of
health-related quality of life: A 10 year cohort study. 2009
23. Luengo-Fernandez R, Gray AM, Bull L, Welch S, Cuthbertson F, Rothwell PM. Quality of
life after tia and stroke ten-year results of the oxford vascular study. Neurology.
2013;81:1588-1595
24. Sorensen SV, Kansal AR, Connolly S, Peng S, Linnehan J, Bradley-Kennedy C, et al. Cost-
effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in
atrial fibrillation: A canadian payer perspective. Thromb Haemost. 2011;105:908-919
25. Kamel H, Easton JD, Johnston SC, Kim AS. Cost-effectiveness of apixaban vs warfarin for
secondary stroke prevention in atrial fibrillation. Neurology. 2012;79:1428-1434
26. Gladstone DJ, Spring M, Dorian P, Panzov V, Thorpe KE, Hall J, et al. Atrial fibrillation in
patients with cryptogenic stroke. N Engl J Med. 2014;370:2467-2477
27. Xu Y, Holbrook AM, Simpson CS, Dowlatshahi D, Johnson AP. Prescribing patterns of novel
oral anticoagulants following regulatory approval for atrial fibrillation in ontario, canada: A
population-based descriptive analysis. Canadian Medical Association Open Access Journal.
2013;1:E115-E119
28. Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic
stroke and bleeding in 182 678 patients with atrial fibrillation: The swedish atrial fibrillation
cohort study. European heart journal. 2012:ehr488
29. Vanassche T, Lauw MN, Eikelboom JW, Healey JS, Hart RG, Alings M, et al. Risk of
ischaemic stroke according to pattern of atrial fibrillation: Analysis of 6563 aspirin-treated
patients in active-a and averroes. Eur Heart J. 2015;36:281-287a

30. Diener HC, Eikelboom J, Connolly SJ, Joyner CD, Hart RG, Lip GY, et al. Apixaban versus
aspirin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: A
predefined subgroup analysis from averroes, a randomised trial. Lancet Neurol. 2012;11:225-
231
31. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al.
Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients
with atrial fibrillation: A meta-analysis of randomised trials. Lancet. 2014;383:955-962
32. Mant J, Hobbs FD, Fletcher K, Roalfe A, Fitzmaurice D, Lip GY, et al. Warfarin versus
aspirin for stroke prevention in an elderly community population with atrial fibrillation (the
birmingham atrial fibrillation treatment of the aged study, bafta): A randomised controlled
trial. Lancet. 2007;370:493-503
33. Connolly SJ, Eikelboom J, Joyner C, Diener HC, Hart R, Golitsyn S, et al. Apixaban in
patients with atrial fibrillation. N Engl J Med. 2011;364:806-817
34. Canadian Agency for Drugs and Technologies in Health. Antithrombotic agents for the
prevention of stroke and systemic embolism in patients with atrial fibrillation. 2013
35. Ariesen M, Claus S, Rinkel G, Algra A. Risk factors for intracerebral hemorrhage in the
general population a systematic review. Stroke. 2003;34:2060-2065
36. Anderson CS, Carter KN, Brownlee WJ, Hackett ML, Broad JB, Bonita R. Very long-term
outcome after stroke in auckland, new zealand. Stroke. 2004;35:1920-1924
37. Hardie K, Hankey GJ, Jamrozik K, Broadhurst RJ, Anderson C. Ten-year survival after first-
ever stroke in the perth community stroke study. Stroke. 2003;34:1842-1846
38. van Wijk I, Kappelle LJ, van Gijn J, Koudstaal PJ, Franke CL, Vermeulen M, et al. Long-
term survival and vascular event risk after transient ischaemic attack or minor ischaemic
stroke: A cohort study. Lancet. 2005;365:2098-2104
39. Goeree R, Blackhouse G, Petrovic R, Salama S. Cost of stroke in canada: A 1-year
prospective study. J Med Econ. 2005;8:147-167
40. Meretoja A, Kaste M, Roine RO, Juntunen M, Linna M, Hillbom M, et al. Direct costs of
patients with stroke can be continuously monitored on a national level: Performance,

effectiveness, and costs of treatment episodes in stroke (perfect stroke) database in finland.
Stroke. 2011;42:2007-2012
Related Documents